
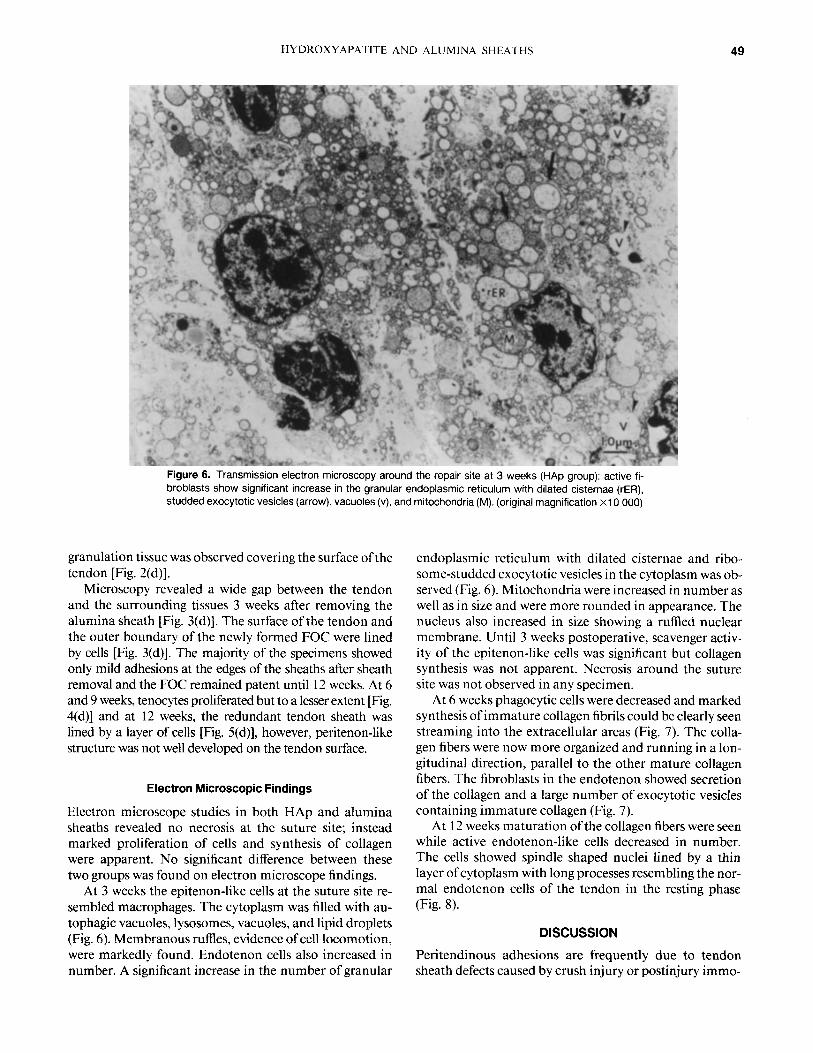
Postoperative complications and hospital costs following small ...

Effects of Hydroxyapatite and Alumina Sheaths on Postoperative Peritendinous Adhesions in Chickens
Najam A. Siddiqi,* Yoshiki Hamada,t Takatoshi Ide,t and Noriya Akamatsut
*Department of Orthopedic Surgery, Johns Hopkins University School of Medicine, Baltimore, Maryland and +Department of Orthopedic Surgery, Yamanashi Medical University, Japan
Two experimental methods for restoring flexor tendon sheath integrity and preventing adhe- sions around traumatized flexor tendons utilizing artificial tendon sheaths made of either hy- droxyapatite (HAp) or alumina were studied in a flexor tendon-trauma model and compared to a standard tendon sheath repair and a control. Eighty toes were divided equally into a control group, a sheath repair group, an HAp group, and an alumina group. Profundus tendons in zone I1 were divided and repaired after sublimis excision in all groups. In the sheath repair group, the flexor sheath was also repaired after suturing the tendon. In artificial sheath groups, sheaths made of HAP and alumina were placed over the repair sites to protect them from the surrounding tissues. In the control group, after repairing the tendon, the flexor sheath was excised and no artificial sheaths were used. Each toe was immobilized in a plaster cast for 3 weeks. After three weeks, the plaster cast was removed followed by the removal of the sheaths in the artificial sheath groups through a small incision in the skin in zone 11. Active mobilization was encouraged in each group. Postoperative adhesions were examined at 3,6,9, and 12 week intervals by using light microscopic techniques. To further explore the effects of artificial sheaths on tendon healing, transmission electron microscopy was done for the HAp and alu- mina groups at 3,6, and 12 week intervals. Results demonstrated decreased severity of postop- erative adhesions in the HAp as well as in the alumina groups in comparison with the sheath repair and controls. A space resembling the fibro-osseous canal was formed around the tendon after removing the sheaths. This space remained patent until 12 weeks, 9 weeks after removing the sheaths, and a newly formed tendon sheath-like structure lined by synovial cells and with a peritenon-like structure over the tendon surface was observed. In the sheath repair and control groups, the severity of adhesions was decreased with the passage of time, to some extent due to unrestricted mobility. However, a newly formed tendon sheath or peritenon-like structure was not observed. Electron microscopic studies confirmed good healing at the suture in the HAp and alumina groups with no evidence of necrosis. These results are qualitative in nature as no statistical tests were performed. From these results we conclude that if the tendon is separated from the surrounding granulation tissue by a barrier with good biocompatibility, the tendon can heal with fewer adhesions. Artificial sheaths may be used to reduce adhesions in severe injuries of the hand where postoperative immobilization is necessary due to fractures, vascular, or nerve injuries. 0 1995 John Wiley & Sons, Inc.
INTRODUCTION
Hand injuries often result in lacerated flexor tendons and sheaths in zone 11. The restoration of normal function af- ter these injuries is often unsatisfactory because of the for- mation of adhesions around the repair site that restrict the gliding of the tendons. These peritendinous adhesions de- velop due to the healing of the tendon, subcutaneous tis- sue, and the skin as a single compartment because there is no barrier between these tissues. The result is contracture
Requests for reprints should be sent to Najam A. Siddiqi, M.D., Ph.D., Dept. of Orthopedic Surgery, Johns Hopkins University School of Medicine, The Ross Research Building, 720 Rutland Ave., Baltimore, MD 2 1205.
Journal of Applied Biomaterials. Vol. 6.43-53 (1995) 0 1995 John Wiley & Sons, Inc. CCC 1045-4861/95/010043-1 I
formation and decreased range of motion of the digit. Al- though anatomic repair of the tendon sheath would seem to restore the normal environment for tendon gliding, nar- rowing of the fibro-osseous canal (FOC) restricts tendon gliding.'-4 Sometimes repairing the sheath is not possible either due to large defects in the substance of the sheath after injury or it is crushed so badly that it has to be re- sected.
Attempts have been made in the past to protect the te- norrhaphy site by using many types of barriers such as fas- cia,' fat, pentenon, stainless steel sheaths, silastic sheaths,6 veins, polyethylene tubes,' cellulose filter tubes (Milli- pore-Microweb sheaths),8 Teflon,@,' silicone rubber enve- lopes," tantalum foil, synthetic polytetraflorethylene (PTFE) surgical membrane3 etc., but none of these meth- ods proved to be clinically successful.
This study attempts to decrease postoperative flexor tendon adhesions by using tunnel shaped barriers made of
43

44 SIDDIQI ET AL.
4.0mm
Alumina artificial Hydroxyapatite artificial tendon sheath tendon sheath
Figure 1. Hydroxyapatite and alumina sheaths.
either HAp or alumina and to compare these results to controls of flexor sheath repair or excision. Synthetic hy- droxyapatite ceramic was chosen for this experiment be- cause it has been recently developed as a biomaterial and has been noted for its excellent biocompatibility and os- teoconduction when employed in bone tissue. ' '-I4 Peri- tendinous adhesions were evaluated by studying the inter- faces between the artificial sheaths, tendons, and the sub- cutaneous tissues. Furthermore, to assess the degree of healing at the suture site, electron microscopic studies were also conducted.
MATERIALS AND METHODS
Tunnel-shaped HAp (Bone cearum-P) and alumina test pieces were prepared (Sumotomo Pharmaceutical Com- pany) measuring 15 mm in length, 1 mm in thickness and 2 mm in inner diameter (Fig. l), according to the size of the chicken tendon. The HAp was prepared by the wet method by mixing (H,PO,) into a container containing calcium hydroxide (CA(OH)2).
10Ca(OH)2 + 6H3P04 --t Ca 10(P04)6(OH)2 + 18H20.
The mixture was thoroughly mixed with the help of a pro- peller and the HAp was then collected on a mesh filter. The powder was dried to obtain HAp and the powder was
then filled under compression in special containers shaped like a tunnel to form the test pieces. Pores were obtained by mixing polymethylmethacrylate (PMMA) in the HAp powder. After the tunnel was formed, the PMMA was burned under high temperature to form pores. The size of the pores (200-250 pm) depended on the size of the PMMA. The test pieces were then sintered at 1 150 "C for 3 h.
Eighty tendons (40 chickens) of the middle digits of white, adult female Leghorn chickens weighing an average of 1.2 kg were randomly selected for this experiment. Each tendon was assigned to the specific group according to the nature of the treatment it received. No blinding was in- volved either at the time of surgery nor at the evaluation.
Operative Technique
Anesthesia was achieved with pentobarbital 1 mL/kg body weight (Nembutal 50 mg/mL), administered intramuscu- larly and the operation was conducted using aseptic tech- niques. A zigzag volar incision was made on the planter surface of the foot starting from zone I11 and extending to the distal interphalangeal joint. Subcutaneous tissues were dissected to expose the flexor sheath. Eighty digits were equally divided into four groups: control group, 20 toes: sheath repair group, 20 toes; HAp group, 20 toes; and alu- mina group, 20 toes. In the control group the flexor sheath was excised between the proximal and distal pulleys in
HYDROXYAPATITE AND ALUMINA SHEATHS 45
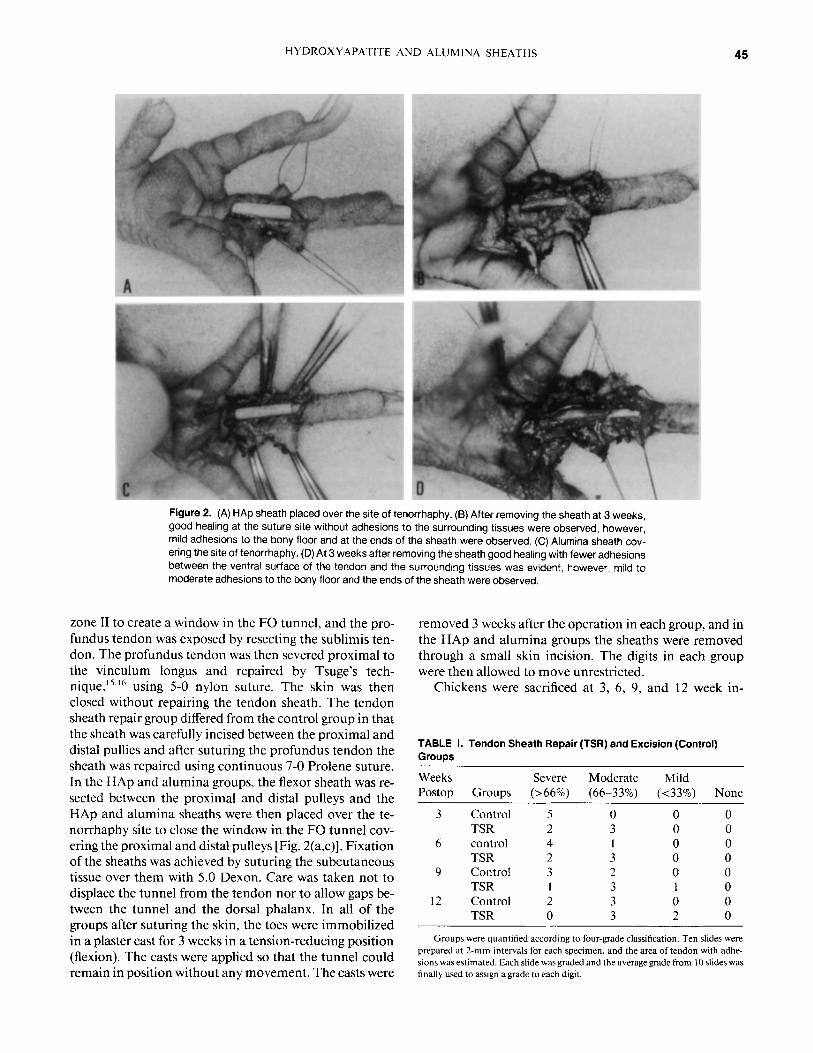
Figure 2. (A) HAp sheath placed over the site of tenorrhaphy. (B) After removing the sheath at 3 weeks, good healing at the suture site without adhesions to the surrounding tissues were observed, however, mild adhesions to the bony floor and at the ends of the sheath were observed. (C) Alumina sheath cov- ering the site of tenorrhaphy. (D) At 3 weeks after removing the sheath good healing with fewer adhesions between the ventral surface of the tendon and the surrounding tissues was evident, however, mild to moderate adhesions to the bony floor and the ends of the sheath were observed.
zone I1 to create a window in the FO tunnel, and the pro- fundus tendon was exposed by resecting the sublimis ten- don. The profundus tendon was then severed proximal to the vinculum longus and repaired by Tsuge's tech- n i q ~ e , ' ~ . ' ~ using 5-0 nylon suture. The skin was then closed without repairing the tendon sheath. The tendon sheath repair group differed from the control group in that the sheath was carefully incised between the proximal and distal pullies and after suturing the profundus tendon the sheath was repaired using continuous 7-0 Prolene suture. In the HAp and alumina groups, the flexor sheath was re- sected between the proximal and distal pulleys and the HAP and alumina sheaths were then placed over the te- norrhaphy site to close the window in the FO tunnel cov- ering the proximal and distal pulleys [Fig. 2(a,c)]. Fixation of the sheaths was achieved by suturing the subcutaneous tissue over them with 5.0 Dexon. Care was taken not to displace the tunnel from the tendon nor to allow gaps be- tween the tunnel and the dorsal phalanx. In all of the groups after suturing the skin, the toes were immobilized in a plaster cast for 3 weeks in a tension-reducing position (flexion). The casts were applied so that the tunnel could remain in position without any movement. The casts were
removed 3 weeks after the operation in each group, and in the HAp and alumina groups the sheaths were removed through a small skin incision. The digits in each group were then allowed to move unrestricted.
Chickens were sacrificed at 3 , 6, 9, and 12 week in-
TABLE 1. Tendon Sheath Repair (TSR) and Excision (Control) Groups
Weeks Severe Moderate Mild Postop Groups (>66%) (66-33%) (<33%) None
3 Control 5 0 0 0 TSR 2 3 0 0
6 control 4 1 0 0 TSR 2 3 0 0
9 Control 3 2 0 0 TSR 1 3 1 0
12 Control 2 3 0 0 TSR 0 3 2 0
Groups were quantified according to four-grade classification. Ten slides were prepared at 2-mm intervals for each specimen, and the area of tendon with adhe- sions was estimated. Each slide was graded and the average grade from 10 slides was finally used to assign a grade to each digit.
46 SIDDIQI ET AL.
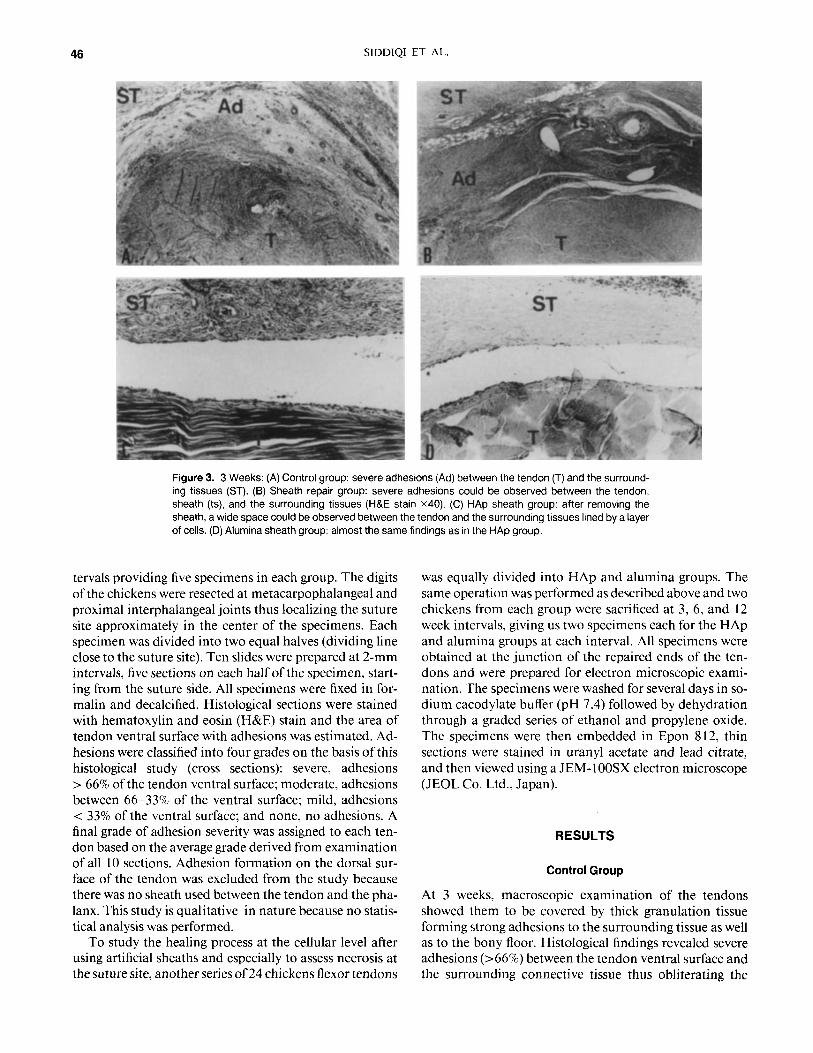
Figure 3. 3 Weeks: (A) Control group: severe adhesions (Ad) between the tendon (T) and the surround- ing tissues (ST). (B) Sheath repair group: severe adhesions could be observed between the tendon, sheath (ts), and the surrounding tissues (H&E stain x40). (C) HAp sheath group: after removing the sheath, a wide space could be observed between the tendon and the surrounding tissues lined by a layer of cells. (D) Alumina sheath group: almost the same findings as in the HAp group.
tervals providing five specimens in each group. The digits of the chickens were resected at metacarpophalangeal and proximal interphalangeal joints thus localizing the suture site approximately in the center of the specimens. Each specimen was divided into two equal halves (dividing line close to the suture site). Ten slides were prepared at 2-mm intervals, five sections on each half of the specimen, start- ing from the suture side. All specimens were fixed in for- malin and decalcified. Histological sections were stained with hematoxylin and eosin (H&E) stain and the area of tendon ventral surface with adhesions was estimated. Ad- hesions were classified into four grades on the basis of this histological study (cross sections): severe, adhesions > 66% of the tendon ventral surface; moderate, adhesions between 66-33% of the ventral surface; mild, adhesions < 33% of the ventral surface; and none, no adhesions. A final grade of adhesion severity was assigned to each ten- don based on the average grade derived from examination of all 10 sections. Adhesion formation on the dorsal sur- face of the tendon was excluded from the study because there was no sheath used between the tendon and the pha- lanx. This study is qualitative in nature because no statis- tical analysis was performed.
To study the healing process at the cellular level after using artificial sheaths and especially to assess necrosis at the suture site, another series of 24 chickens flexor tendons
was equally divided into HAp and alumina groups. The same operation was performed as described above and two chickens from each group were sacrificed at 3 , 6, and 12 week intervals, giving us two specimens each for the HAp and alumina groups at each interval. All specimens were obtained at the junction of the repaired ends of the ten- dons and were prepared for electron microscopic exami- nation. The specimens were washed for several days in so- dium cacodylate buffer (pH 7.4) followed by dehydration through a graded series of ethanol and propylene oxide. The specimens were then embedded in Epon 812, thin sections were stained in uranyl acetate and lead citrate, and then viewed using a JEM- 1 OOSX electron microscope (JEOL Co. Ltd., Japan).
RESULTS
Control Group
At 3 weeks, macroscopic examination of the tendons showed them to be covered by thick granulation tissue forming strong adhesions to the surrounding tissue as well as to the bony floor. Histological findings revealed severe adhesions (>66%) between the tendon ventral surface and the surrounding connective tissue thus obliterating the
HYDROXYAPATITE AND ALUMINA SHEATHS 47
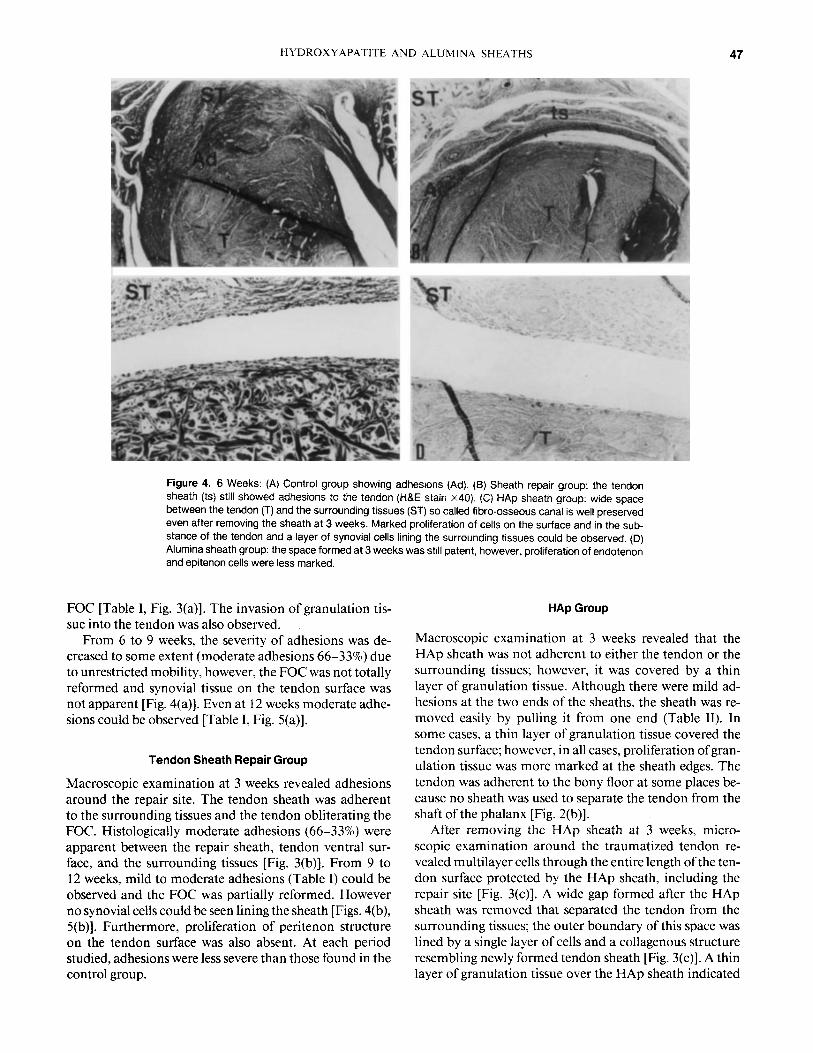
Figure 4. 6 Weeks: (A) Control group showing adhesions (Ad). (8) Sheath repair group: the tendon sheath (ts) still showed adhesions to the tendon (H&E stain x40). (C) HAp sheath group: wide space between the tendon (T) and the surrounding tissues (ST) so called fibro-osseous canal is well preserved even after removing the sheath at 3 weeks. Marked proliferation of cells on the surface and in the sub- stance of the tendon and a layer of synovial cells lining the surrounding tissues could be observed. (D) Alumina sheath group: the space formed at 3 weeks was still patent, however, proliferation of endotenon and epitenon cells were less marked
FOC [Table I, Fig. 3(a)]. The invasion of granulation tis- sue into the tendon was also observed.
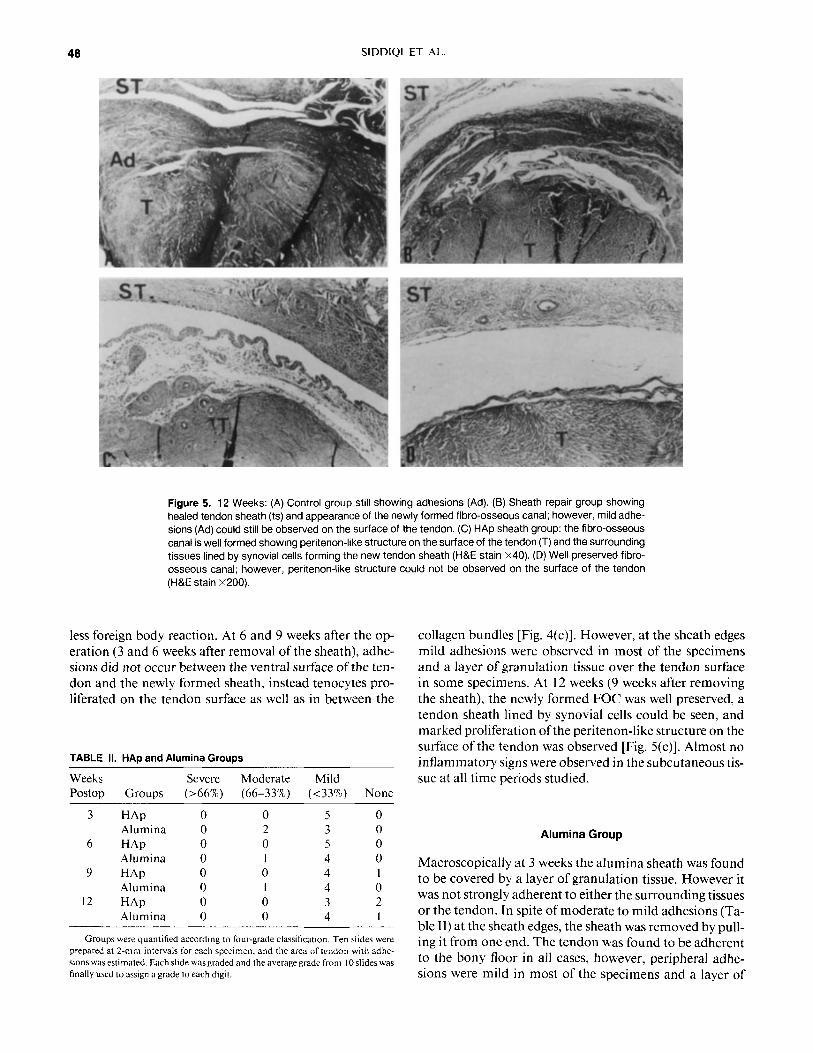
From 6 to 9 weeks, the severity of adhesions was de- creased to some extent (moderate adhesions 66-33%) due to unrestricted mobility, however, the FOC was not totally reformed and synovial tissue on the tendon surface was not apparent [Fig. 4(a)]. Even at 12 weeks moderate adhe- sions could be observed [Table I, Fig. 5(a)].
Tendon Sheath Repair Group
Macroscopic examination at 3 weeks revealed adhesions around the repair site. The tendon sheath was adherent to the surrounding tissues and the tendon obliterating the FOC. Histologically moderate adhesions (66-33%) were apparent between the repair sheath, tendon ventral sur- face, and the surrounding tissues [Fig. 3(b)]. From 9 to 12 weeks, mild to moderate adhesions (Table I ) could be observed and the FOC was partially reformed. However no synovial cells could be seen lining the sheath [Figs. 4(b), 5(b)]. Furthermore, proliferation of peritenon structure on the tendon surface was also absent. At each period studied, adhesions were less severe than those found in the control group.
HAp Group
Macroscopic examination at 3 weeks revealed that the HAp sheath was not adherent to either the tendon or the surrounding tissues; however, it was covered by a thin layer of granulation tissue. Although there were mild ad- hesions at the two ends of the sheaths, the sheath was re- moved easily by pulling it from one end (Table 11). In some cases, a thin layer of granulation tissue covered the tendon surface; however, in all cases, proliferation of gran- ulation tissue was more marked at the sheath edges. The tendon was adherent to the bony floor at some places be- cause no sheath was used to separate the tendon from the shaft of the phalanx [Fig. 2(b)].
After removing the HAp sheath at 3 weeks, micro- scopic examination around the traumatized tendon re- vealed multilayer cells through the entire length of the ten- don surface protected by the HAp sheath, including the repair site [Fig. 3(c)]. A wide gap formed after the HAp sheath was removed that separated the tendon from the surrounding tissues; the outer boundary of this space was lined by a single layer of cells and a collagenous structure resembling newly formed tendon sheath [Fig. 3(c)]. A thin layer of granulation tissue over the HAp sheath indicated
48 SIDDIQI ET AL.
Figure 5. 12 Weeks: (A) Control group still showing adhesions (Ad). (B) Sheath repair group showing healed tendon sheath (ts) and appearance of the newly formed fibro-osseous canal; however, mild adhe- sions (Ad) could still be observed on the surface of the tendon. (C) HAp sheath group: the fibro-osseous canal is well formed showing peritenon-like structure on the surface of the tendon (T) and the surrounding tissues lined by synovial cells forming the new tendon sheath (H&E stain X40). (D) Well preserved fibro- osseous canal; however, peritenon-like structure could not be observed on the surface of the tendon (H&E stain x200).
less foreign body reaction. At 6 and 9 weeks after the op- eration ( 3 and 6 weeks after removal of the sheath), adhe- sions did not occur between the ventral surface of the ten- don and the newly formed sheath, instead tenocytes pro- liferated on the tendon surface as well as in between the
collagen bundles [Fig. 4(c)]. However, at the sheath edges mild adhesions were observed in most of the specimens and a layer of granulation tissue over the tendon surface in some specimens. At 12 weeks (9 weeks after removing the sheath), the newly formed FOC was well preserved, a tendon sheath lined by synovial cells could be seen, and marked proliferation of the pentenon-like structure on the surface of the tendon was observed [Fig. 5(c)]. Almost no inflammatory signs were observed in the subcutaneous tis- TABLE II. HAp and Alumina Groups
Weeks Severe Moderate Mild sue at all time periods studied. Postop Groups (>66%) (66-33’70) (<33%) None
3 HAp
6 HAp
9 HAp
12 HAp
Alumina
Alumina
Alumina
Alumina
0 5 2 3 0 5 1 4 0 4 1 4 0 3 0 4
Groups were quantified according to four-grade classification. Ten slides were prepared at 2-mm intervals for each specimen. and the area of tendon with adhe- sions was estimated. Each slide was graded and the average grade from I0 slides was finally used to assign a grade lo each digit.
Alumina Group
Macroscopically at 3 weeks the alumina sheath was found to be covered by a layer of granulation tissue. However it was not strongly adherent to either the surrounding tissues or the tendon. In spite of moderate to mild adhesions (Ta- ble 11) at the sheath edges, the sheath was removed by pull- ing it from one end. The tendon was found to be adherent to the bony floor in all cases, however, peripheral adhe- sions were mild in most of the specimens and a layer of
6P SHLV3HS VNlMinlV aNV XLILVdVAXO8aAH

50 SIDDIQI ET AL.
Figure 7. Transmission electron microscopy around the repair site at 6 weeks (alumina group): metabol- ically active fibroblasts within the endotenon and marked secretion of extracellular new collagen fibrils in the extracellular matrix (arrow) in various stages of polymerization. Exocytotic vesicles could also be seen. (original magnification x16 000)
bilization necessitated by tendon lacerations, phalanx fracture, vascular, or nerve injury. In these cases, an arti- ficial barrier or tendon sheath to protect the tenorrhaphy site from the “one wound one scar” type of healing as stated by Peacock would appear to be useful. In the past it was believed that tendons are passive organs that depend on digital sheath or surrounding vascular granulation tis- sue for healing’.* and the tenocytes of the tendon proper play no active role in tendon repair. This type of healing, called extrinsic repair, results in peritendinous adhesions thus limiting the mobility ofthe tendon. In the recent past, through in vitro as well as in vivo experiments, it has be- come apparent that tendons are dynamic have intrinsic repair potential, and do not depend on extrinsic cells for healing. The repair process of the tendon after trauma is explained by the proliferation of epitenon cells that phagocytize debris at the suture site while the endo- tenon cells proliferate later and secrete collagen to bridge the gap at the suture site.21 Either vascular or synovial nu- tritional supply is enough for tendon healing after trauma26 and all the connective tissue cells comprising a tendon are capable of producing immature cells in a syno- vial fluid environment.” Furthermore, the diffusion path- way from the synovial fluid was sufficient for the superfi- cial layers of the tendon cells to proliferate and produce collagen fibers. 18.26
Role of Barriers in Tendon Surgery
There has been a lot of controversy over the use of artificial sheaths or tubes. It was reported in the past that wrapping the tendon with a membrane-like barrier or using blocking tubes would result in necrosis of the suture This could be due to the obstruction ofthe flow ofsynovial fluid to the suture site because of tight wrapping of the mem- brane. Moreover, wrapping might also prevent the extrin- sic helper cells from reaching the suture site resulting in necrosis. From the concept of intrinsic tendon-healing ca- pability, Manske et reported that peripheral adhe- sions do not appear to be essential for tendon repair and that if the suture site is protected by a barrier, postopera- tive peritendinous adhesions could be decreased. How- ever, Potenza’ reported that blocking tubes placed around the repair sites prevent invasion of blood vessels thereby jeopardizing sound healing. The vascular elements from the sheath grow beneath the tubes to reach the wound site. Thus healing of the tendon is delayed, prevented, or both, resulting in degeneration of the repair site. Potenza there- fore concluded that searching for an ideal blocking mate- rial to create a so-called artificial tendon sheath to prevent adhesions is of doubtful value. Later Ashley et aL2* re- ported that there is a need for an artificial tendon sheath material that could be successful in both preventing
HYDROXYAPATITE AND ALUMINA SHEATHS 51
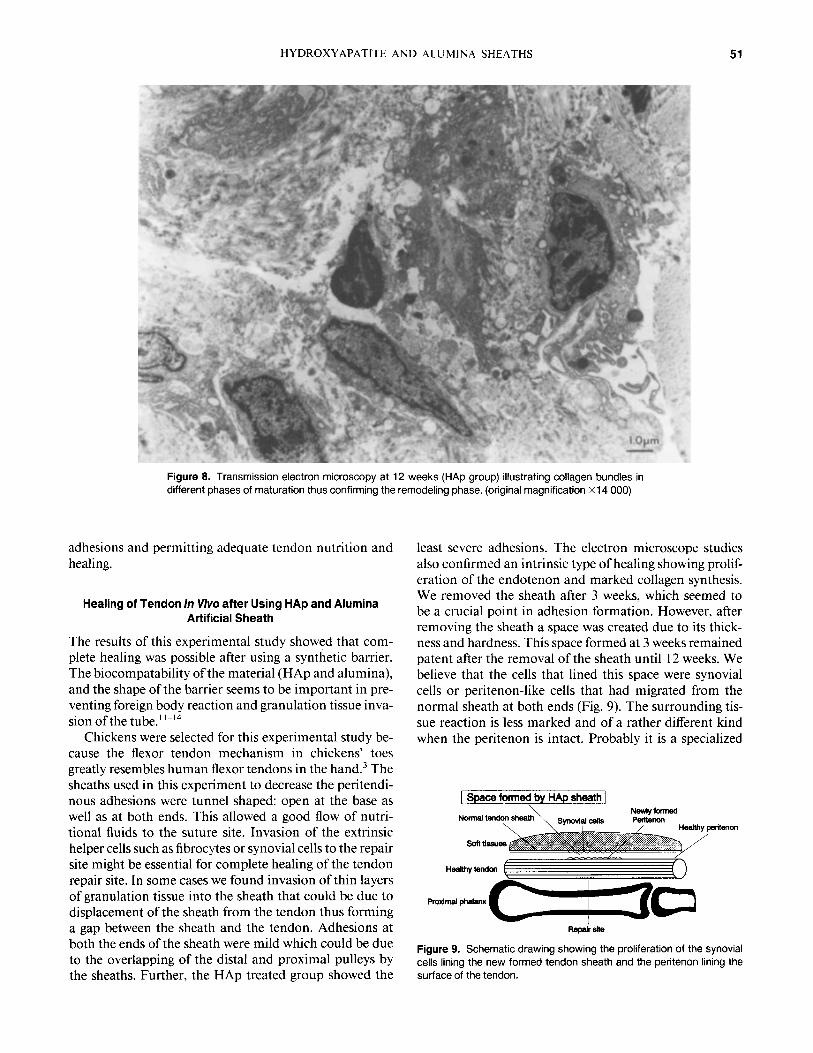
Figure 8. Transmission electron microscopy at 12 weeks (HAP group) illustrating collagen bundles in different phases of maturation thus confirming the remodeling phase. (original magnification x14 000)
adhesions and permitting adequate tendon nutrition and healing.
Healing of Tendon In Vivo after Using HAp and Alumina Artificial Sheath
The results of this experimental study showed that com- plete healing was possible after using a synthetic barrier. The biocompatability of the material (HAP and alumina), and the shape of the barrier seems to be important in pre- venting foreign body reaction and granulation tissue inva- sion of the tube.''-I4
Chickens were selected for this experimental study be- cause the flexor tendon mechanism in chickens' toes greatly resembles human flexor tendons in the hand.3 The sheaths used in this experiment to decrease the peritendi- nous adhesions were tunnel shaped: open at the base as well as at both ends. This allowed a good flow of nutri- tional fluids to the suture site. Invasion of the extrinsic helper cells such as fibrocytes or synovial cells to the repair site might be essential for complete healing of the tendon repair site. In some cases we found invasion of thin layers of granulation tissue into the sheath that could be due to displacement of the sheath from the tendon thus forming a gap between the sheath and the tendon. Adhesions at both the ends of the sheath were mild which could be due to the overlapping of the distal and proximal pulleys by the sheaths. Further, the HAp treated group showed the
least severe adhesions. The electron microscope studies also confirmed an intrinsic type of healing showing prolif- eration of the endotenon and marked collagen synthesis. We removed the sheath after 3 weeks, which seemed to be a crucial point in adhesion formation. However, after removing the sheath a space was created due to its thick- ness and hardness. This space formed at 3 weeks remained patent after the removal of the sheath until I2 weeks. We believe that the cells that lined this space were synovial cells or peritenon-like cells that had migrated from the normal sheath at both ends (Fig. 9). The surrounding tis- sue reaction is less marked and of a rather different kind when the peritenon is intact. Probably it is a specialized
[ Space formed by HAp sheath]
Figure 9. Schematic drawing showing the proliferation of the synovial cells lining the new formed tendon sheath and the peritenon lining the surface of the tendon.

52 SIDDIQI ET AL.
connective tissue capsule. I This capsule itself does not show a tendency to invade the collagenous bundles of the tendon; but if destruction of peritenon occurs, it results in profuse invasion of the vascular tissue from the surround- ing tissue.' These synovial cells and peritenon protected the newly formed FOC and prevented adhesion forma- tion. The space formed after the removal of the sheath helped the migration of these cells.
CLINICAL SIGNIFICANCE AND CONCLUSION
This study supports the concept that tendons are dynamic organs and possess an intrinsic healing mechanism for their repair. However in clinical practice or in v i v a it seems to be that the tendon heals by extrinsic repair." This direct invasion of extrinsic fibroblasts and capillaries results in peritendinous adhesions, a frequent postopera- tive complication in hand injuries. By using artificial HAp and alumina sheaths the severity of peritendinous adhe- sions was decreased. HAP sheaths provided a better envi- ronment for tendon healing resulting in significant prolif- eration of tendon cells and formation of peritenon-like tis- sue at 12 weeks. Electron microscope studies confirmed these findings by showing marked collagen formation at 6 weeks. The alumina group showed less cellular prolifera- tion and almost no peritenon-like structure at 12 weeks. From this experimental study we conclude that HAp and alumina sheaths were successful in decreasing postopera- tive adhesions if placed around the repair site for 3 weeks. HAp having better biocompatability, HAp sheaths could be further studied for clinical use in hand injury cases. However, as this study is qualitative in nature, and no blinding was involved at the time of surgery or during op- eration, further quantitative analysis and improvement in the design and material of the sheath is necessary before any clinical trials should be conducted.
The authors wish to express gratitude to Professor Akira Kawaoi, Department of Pathology I1 for his guidance and academic advice regarding histological and electron microscopic techniques. The author also thanks Mrs. Mikiko Yoda for her technical assistance. This article was presented at the 1 Ith Japanese Biomaterial Conference at Kyoto in October 1989.
REFERENCES
1. Skoog, T.; Persson, B. H. An experiment study of the early healing of the tendons. Plast. Reconst. Surg. 13384-399; 1954.
2. Potenza, A. D. Critical evaluation of flexor-tendon healing and adhesion formation within artificial digital sheaths, an experimental study. J. Bone Jt. Surg. 45A:1217-1233; 1963.
3. Peterson, W. W.; Manske, P. R.; Dunlap, J.; Horwitz, D. S.; Kahn, B. Effects of various methods of restoring flexor sheath integrity on the formation of adhesions after tendon injury. J. Hand Surg. I5:48-56; 1990.
4. Umeda, H.; Ishii, S.; Minami, M.; et al. Studies on the adhe- sions of the digital flexor tendon (Part 3). Tendon healing and adhesion releasing process from its surrounding tissues. J. Jpn. Orthop. Assoc. 50:391-400; 1976 (in Japanese).
5. Kessler, F. B.; Epstein, M. J.; Lannik, D.; Maher, D.; Pappu,
S. Facia patch graft for a digital flexor sheath defect over primary tendon repair in the chicken. J. Hand Surg. 59:908- 913: 1986.
6. Stark, H. H.; Boyer, J. H.; Johnson, L. The use of paratenon polyethylene film or silastic sheeting to prevent restricting adhesions to tendon in the hand. J. Bone Jt. Surg. 59:908- 913; 1977.
7. Gonzalez, R. I. Experimental tendon repair within the flexor tunnels: use of polyethylene tubes for improvement of func- tional results in the dog. Surgery 26: 18 1-198; 1949.
8. Ashley, F. L.; Stones, R. S.; Alonsoartieda, M.; Syverud, J. M.; Edwards, J. W. Experimental and clinical studies on the application of monomolecular cellulose filter tubes to create artificial tendon sheaths in digits. Plast. Reconstr. Surg. 23536-534; 1959.
9. Gonzalez, R. I. Experimental use of Teflon in tendon sur- gery. Plast. Reconstr. Surg. 23535; 1959.
10. Hunter, J . M.; Salisbury, R. E. Flexor tendon reconstruction in severely damaged hands. A two stage procedure using a silicone-dacron reinforced gliding prosthesis prior to tendon grafting. J. Bone Jt. Surg. 53:829-858; 197 I .
I I . Donath, K. Tissue reaction to Ca-phosphate ceramics. Oo- nishi, H.; Aoki, H.; Sawai, K. eds. Bioceramics 1. Tokyo: Ishiyaku EuroAmerica. Inc.; 1989:96-101.
12. Negami, S. Histological observation on muscle tissue reac- tion to porous hydroxyapatite sintered body in rats. J. Jpn. Orthop. Assoc. 62235-94; 1988.
13. Shinjo, K.; Makiyama. T.; Sugiura, I.: Kondo, K. Clinical application of the hydroxyapatite implants. Oonishi, H.; Aoki, H.; Sawai, K., eds. Bioceramics I . Tokyo: Ishiyaku EuroAmerica, Inc.; 1989: 124-1 29.
14. Takashima, F.; Kurokawa, F.: Katayama, T.; Takuma, M.; Miyauchi, S.; Maruyama, T. An experimental study of soft tissue reactions to methacrylate resin, hydroxyapatite and titanium alloy. J. Jpn. Prosthodont. SOC. 3 I : 1202-1207; 1987.
15. Tsuge, K.; Ikuta, Y.; Matsuishi, Y . Intra-tendinous tendon suture in the hand, a new technique. The Hand 7:259-255; 1975.
16. Tsuge, K.; Ikuta, Y.; Matsuishi, Y. Repair of flexor tendons by intratendinous tendon suture. J. Hand Surg. 2:436-440; 1977.
17. Furlow, L. T. The role of tendon tissue in tendon healing. Plast. Reconstr. Surg. 57:39-49; 1976.
18. Gelberman, R. H.: Manske, P. R.: Akeson, W. H.; Woo, S. L.-Y.; Lundborg, G.; Amiel, D. Flexortendon healingand restoration of the gliding surface. J. Bone Jt. Surg. (A) 65:
19. Gelberman, R. H.; Manske, P. R.: Akeson, W. H.; Woo, S. L.-Y.; Lundborg, G.; Amiel, D. Flexor tendon repair. J. Orthop. Res. 4: I 19- 128: 1986.
20. Lundborg, G.; Rank, F. Experimental intrinsic healing of the flexor tendons based upon synovial fluid nutrition. J. HandSurg. 3:21-31; 1978.
2 1. Manske, P. R.; Gelberman, R. H.; Vande Berg, J. S.; Lesker, P. A. Intrinsic flexor-tendon repair. J. Bone Jt. Surg. (A ) 66:
22. Mass, D. P.; Tuel. R. Human flexor tendon participate in the in vitro repair process. J. Hand Surg. 14:64-71; 1989.
23. Schepel, S. J. Intrinsic healing of flexor tendons in primates. Hunter, J. M.; Schneider, L. H.; Mackin, E. J., eds. Tendon surgery in the hand. New York: C. V. Mosby; 1987:6 1-66.
24. Ishii, S.: Umeda, H. Role of tendon in healing: a morpho- logical study in vitro and in viva Hunter, J. M.; Schneider, L. H.; Mackin, E. J., eds. Tendon surgery in the hand. New York: C. V. Mosby; 1987:79-85.
25. Umeda, H. An experimental study on the intrinsic healing
70-80; 1983.
385-396: 1984.

HYDROXYAPATITE AND ALUMINA SHEATHS 53
mechanisms of digital flexor tendons. J. Jpn. Orthop. Assoc. 52:9 17-929; 1978.
26. Lundborg, G.; Holm, S.; Myrhage, R. The role of the syno- vial fluid and tendon sheath for flexor tendon nutrition. Scand. J. Plast. Reconstr. Surg. 14:99-107; 1980.
27. Lindsay, W. K.; Thomson, H. G. Digital flexor tendon: an
Marmor, L. An evaluation of the healing process in avian digital flexor tendons and grafts following the application of an artificial tendon sheath. Plast. Reconstr. Surg. 33:411- 421; 1959.
experimental study. Br. J. Plast. Surg. 12:289-3 16; 1959. 28. Ashley, F. L.; McConnell, D. V.; Polak, T.; Stone, R. S.;
Received May 14. 1993 Accepted October 28, 1994
Copyright © 2022 FDOKUMEN




















