
Quantitative EEG in Alzheimer's disease: Cognitive state, resting state and association with disease...
8
Quantitative EEG in Alzheimer's disease: Cognitive state, resting state and association with disease severity Heinrich Garn a,1 , Markus Waser a , Manfred Deistler b , Reinhold Schmidt f , Peter Dal-Bianco d , Gerhard Ransmayr e , Josef Zeitlhofer d , Helena Schmidt f , Stephan Seiler f , Guenter Sanin c , Georg Caravias e , Peter Santer d , Dieter Grossegger g , Wolfgang Fruehwirt g , Thomas Benke c, ⁎ a AIT Austrian Institute of Technology GmbH, A-1220 Vienna, Austria b Vienna University of Technology, A-1220 Vienna, Austria c Department of Neurology, Innsbruck Medical University, A-6020 Innsbruck, Austria d Department of Neurology, Vienna Medical University, A-1090 Vienna, Austria e Department of Neurology, Linz General Hospital, A-4020 Linz, Austria f Department of Neurology, Graz Medical University, A-8036 Graz, Austria g Dr. Grossegger & Drbal GmbH, A-1190 Vienna, Austria abstract article info Article history: Received 22 March 2014 Received in revised form 3 June 2014 Accepted 6 June 2014 Available online xxxx Keywords: Alzheimer's disease Quantitative EEG Cognitive state Resting state Background: Quantitative electroencephalogram (qEEG) recorded during cognitive tasks has been shown to differentiate between patients with Alzheimer's disease (AD) and healthy individuals. However, the association between various qEEG markers recorded during mnestic paradigms and clinical measures of AD has not been studied in detail. Objective: To evaluate if ‘cognitive’ qEEG is a useful diagnostic option, particularly if memory paradigms are used as cognitive stimulators. Methods: This study is part of the Prospective Registry on Dementia in Austria (PRODEM), a multicenter dementia research project. A cohort of 79 probable AD patients was included in a cross-sectional analysis. qEEG recordings performed in resting states were compared with recordings during cognitively active states. Cognition was evoked with a face–name paradigm and a paired-associate word list task, respectively. Relative band powers, co- herence and auto-mutual information were computed as functions of MMSE scores for the memory paradigms and during rest. Analyses were adjusted for the co-variables age, sex, duration of dementia and educational level. Results: MMSE scores explained 36–51% of the variances of qEEG-markers. Face–name encoding with eyes open was superior to resting state with eyes closed in relative theta and beta1 power as well as coherence, whereas relative alpha power and auto-mutual information yielded more significant results during resting state with eyes closed. The face–name task yielded stronger correlations with MMSE scores than the verbal memory task. Conclusion: qEEG alterations recorded during mnestic activity, particularly face–name encoding showed the highest association with the MMSE and may serve as a clinically valuable marker for disease severity. © 2014 Elsevier B.V. All rights reserved. 1. Introduction Alzheimer's disease (AD) is a progressive neurological disorder which can be diagnosed in advanced disease stages with high diagnostic accuracy. However, early AD is more difficult to detect and currently requires the use of costly technical diagnostic facilities, such as MRI, FDG-PET or laboratory based investigations (Dubois et al., 2007). Alternatively, several previous studies have employed quantitative electroencephalogram (qEEG) as an economical, noninvasive tool to differentiate normal controls (NC) or subjects with preclinical disease stages from patients with manifest AD (for reviews, see: Drago et al., 2011; Sakkalis, 2011; Platt and Riedel, 2001; Leiser et al., 2001; Santos et al., 2010; Dauwels et al., 2010; Giannakopoulos et al., 2009; Rossini et al., 2007; Uhlhaas and Singer, 2006; Menendez, International Journal of Psychophysiology xxx (2014) xxx–xxx ⁎ Corresponding author at: Klinik für Neurologie, Anichstr. 35, A-6020 Innsbruck, Austria. Fax: +43 51250423852. E-mail addresses: [email protected] (H. Garn), [email protected] (M. Waser), [email protected] (M. Deistler), [email protected] (R. Schmidt), [email protected] (P. Dal-Bianco), [email protected] (G. Ransmayr), [email protected] (J. Zeitlhofer), [email protected] (H. Schmidt), [email protected] (S. Seiler), [email protected] (G. Sanin), [email protected] (G. Caravias), [email protected] (P. Santer), offi[email protected] (D. Grossegger), [email protected] (W. Fruehwirt), [email protected] (T. Benke). 1 Tel.: +43 505504103; fax: +43 505504125. INTPSY-10807; No of Pages 8 http://dx.doi.org/10.1016/j.ijpsycho.2014.06.003 0167-8760/© 2014 Elsevier B.V. All rights reserved. Contents lists available at ScienceDirect International Journal of Psychophysiology journal homepage: www.elsevier.com/locate/ijpsycho Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimer's disease: Cognitive state, resting state and association with disease severity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho.2014.06.003
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Quantitative EEG in Alzheimer's disease: Cognitive state, resting state and association with disease...

International Journal of Psychophysiology xxx (2014) xxx–xxx
INTPSY-10807; No of Pages 8
Contents lists available at ScienceDirect
International Journal of Psychophysiology
j ourna l homepage: www.e lsev ie r .com/ locate / i jpsycho
Quantitative EEG in Alzheimer's disease: Cognitive state, resting state andassociation with disease severity
Heinrich Garn a,1, Markus Waser a, Manfred Deistler b, Reinhold Schmidt f, Peter Dal-Bianco d,Gerhard Ransmayr e, Josef Zeitlhofer d, Helena Schmidt f, Stephan Seiler f, Guenter Sanin c, Georg Caravias e,Peter Santer d, Dieter Grossegger g, Wolfgang Fruehwirt g, Thomas Benke c,⁎a AIT Austrian Institute of Technology GmbH, A-1220 Vienna, Austriab Vienna University of Technology, A-1220 Vienna, Austriac Department of Neurology, Innsbruck Medical University, A-6020 Innsbruck, Austriad Department of Neurology, Vienna Medical University, A-1090 Vienna, Austriae Department of Neurology, Linz General Hospital, A-4020 Linz, Austriaf Department of Neurology, Graz Medical University, A-8036 Graz, Austriag Dr. Grossegger & Drbal GmbH, A-1190 Vienna, Austria
⁎ Corresponding author at: Klinik für Neurologie, AnAustria. Fax: +43 51250423852.
E-mail addresses: [email protected] (H. Garn), m(M. Waser), [email protected] (M. Deistler),[email protected] (R. Schmidt), peter.dal-(P. Dal-Bianco), [email protected] (G. [email protected] (J. Zeitlhofer), helena.s(H. Schmidt), [email protected] (S. Seiler), gu(G. Sanin), [email protected] (G. Caravias), peter.(P. Santer), [email protected] (D. Grossegger), w.fruehw(W. Fruehwirt), [email protected] (T. Benke).
1 Tel.: +43 505504103; fax: +43 505504125.
http://dx.doi.org/10.1016/j.ijpsycho.2014.06.0030167-8760/© 2014 Elsevier B.V. All rights reserved.
Please cite this article as: Garn, H., et al., Quseverity, Int. J. Psychophysiol. (2014), http://
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 22 March 2014Received in revised form 3 June 2014Accepted 6 June 2014Available online xxxxKeywords:Alzheimer's diseaseQuantitative EEGCognitive stateResting state
Background: Quantitative electroencephalogram (qEEG) recorded during cognitive tasks has been shown todifferentiate between patients with Alzheimer's disease (AD) and healthy individuals. However, the associationbetween various qEEG markers recorded during mnestic paradigms and clinical measures of AD has not beenstudied in detail.Objective: To evaluate if ‘cognitive’ qEEG is a useful diagnostic option, particularly if memory paradigms are usedas cognitive stimulators.Methods: This study is part of the Prospective Registry onDementia in Austria (PRODEM), amulticenter dementiaresearch project. A cohort of 79 probable AD patients was included in a cross-sectional analysis. qEEG recordingsperformed in resting states were compared with recordings during cognitively active states. Cognition wasevokedwith a face–name paradigm and a paired-associate word list task, respectively. Relative band powers, co-
herence and auto-mutual information were computed as functions of MMSE scores for the memory paradigmsand during rest. Analyses were adjusted for the co-variables age, sex, duration of dementia and educational level.Results:MMSE scores explained 36–51% of the variances of qEEG-markers. Face–name encoding with eyes openwas superior to resting state with eyes closed in relative theta and beta1 power as well as coherence, whereasrelative alpha power and auto-mutual information yielded more significant results during resting state witheyes closed. The face–name task yielded stronger correlations with MMSE scores than the verbal memory task.Conclusion: qEEG alterations recorded during mnestic activity, particularly face–name encoding showed thehighest association with the MMSE and may serve as a clinically valuable marker for disease severity.© 2014 Elsevier B.V. All rights reserved.
ichstr. 35, A-6020 Innsbruck,
[email protected]),[email protected]@[email protected]@alphatrace.at
antitative EEG in Alzheimer'dx.doi.org/10.1016/j.ijpsycho
1. Introduction
Alzheimer's disease (AD) is a progressive neurological disorderwhich can be diagnosed in advanced disease stageswith high diagnosticaccuracy. However, early AD is more difficult to detect and currentlyrequires the use of costly technical diagnostic facilities, such as MRI,FDG-PET or laboratory based investigations (Dubois et al., 2007).Alternatively, several previous studies have employed quantitativeelectroencephalogram (qEEG) as an economical, noninvasive tool todifferentiate normal controls (NC) or subjects with preclinical diseasestages from patients with manifest AD (for reviews, see: Drago et al.,2011; Sakkalis, 2011; Platt and Riedel, 2001; Leiser et al., 2001;Santos et al., 2010; Dauwels et al., 2010; Giannakopoulos et al.,2009; Rossini et al., 2007; Uhlhaas and Singer, 2006; Menendez,
s disease: Cognitive state, resting state and association with disease.2014.06.003

2 H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
2005; Jeong, 2004). It has been shown that the essential qEEG hall-marks of AD are (i) slowing of the frequency spectrum, (ii) changingsynchrony between sites across the cortex, particularly with diseaseprogression, and (iii) reduced signal complexity. Thus, AD was foundto be associated with an increase of spectral power at low frequencies(delta and theta waves) and a decrease of power at higher frequencies(alpha and beta waves). Furthermore, synchrony between EEG chan-nels as measured by coherence increases during the first years of ADand decreases in later disease stages. Signal complexity generally de-creases with disease progression, as evident from an increase of automutual information.
Although previous research has found AD-specific markers in qEEG,this technique is presently not among the recommended standard diag-nostic tools of AD. Since impairments of cognitive functions (e.g. amne-sia) are typical and early symptoms of AD, qEEG recorded during activecognitive performancemay containmore and better diagnosticmarkersthan recordings during rest. We investigated a large cohort of patientswith early and moderate AD using a comprehensive analysis of qEEGand cognitive parameters. In particular, we aimed to evaluate a)wheth-er recording of qEEGduring or immediately after cognitive effort revealsmore significant findings than during the unengaged resting state,b) how well brain dynamics of qEEG can serve as surrogate markers ofAD, and c) which of the cognitive tasks administered evokes the mostprominent qEEG changes. Based on previous studies our tentativehypotheses were that early and moderate AD is associated with severalpathological qEEG markers, that cognitive activity related to a memorytask is accompanied by abnormal qEEG, and that active cognition pro-vides more diagnostic clues in qEEG than resting states (Klimesch,1999).
2. Materials and methods
2.1. Study and participants
The Prospective Registry on Dementia in Austria (PRODEM Austria)is a longitudinal multicenter study of AD and other dementias in a rou-tine clinical setting (Seiler et al., 2012; Benke et al., 2013). Participantswere recruited prospectively in 4 tertiary-referral memory clinics. Thestudy was approved by the Ethic Committees of the individual researchsites, and patients gave their written informed consent to participate inthe study. AD was diagnosed according to the NINCDS-ADRDA criteria(McKhann et al., 1984). Additional inclusion criteria were non-institutionalization, no need for 24-hour care, and availability of acaregiver who agreed to provide information on the patient. Durationof disease (inmonths)was estimated by the caregiver who also gave in-formation regarding the patient's education, disease stage as assessedby Clinical Dementia Rating (CDR, Berg, 1988), and basic and instru-mental activities of daily living (Gelinas et al., 1999). The MMSE(Folstein et al., 1975) was used as a global measure of cognition andstaging of dementia. In the present study, 79 patients (50 females)with a diagnosis of probable ADwere included. Important demographicand disease variables of the study population are summarized inTables 1 and 2. As evident from their CDR and MMSE scores the cohort
Table 1Group characteristics for the whole group of 79 patients.
Median Median absolutedeviation
Range
Age (years) 75 6 52–88Level of education (scale 1–6) 2 1 1–6Duration of illness (months) 23 13 2–120MMSE (max. 30) 22 2 26–15CDR (max. 3) 0.5 0.5 0–2DAD (max. 100) 90 10 30–100
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimerseverity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
was in an early to moderate disease stage of AD. About 49% of the pa-tients were treated with cholinergic substitution treatment. Five pa-tients received antipsychotics.
2.2. Experimental procedure
The rationale for the current study was to record, analyze and com-pare qEEG during periods of rest and cognitive activity, and to explorewhich period and qEEG markers best predict the concurrent MMSEscore. With regard to the earliest and most frequent cognitive impair-ment of AD, two episodic memory paradigms were chosen as disease-relevant tasks, one visual–verbal and one strictly verbal. Details of thetest procedure and qEEG recording are shown in Table 3.
2.2.1. Tests and administrationA memory test was designed to compare mnestic activity with the
resting state. Test materials contained verbal and figural informationand were adapted to patients with dementia. Details of the testing pro-cedure are summarized in Table 3. The face–name taskwas started aftera rest interval (360 s, rest 1with eyes closed and rest 2with eyes open);then, 3 face–name pairs were presented (encoding 1). Next, the threefaceswere shown alone, and the corresponding names had to be report-ed (name recall 1), followed by a second presentation of the three face–name pairs (encoding 2). After a 90 s consolidation interval, duringwhich participants were asked to close their eyes and keep faces andnames inmind, the three encoded faces had to be recognized and distin-guished from 6 distracter faces (recognition). Next, the names of thethree target faces had to be retrieved again (name recall 2). The word-pair task consisted of an encoding period (encoding 3) during which 3word pairs were visually presented twice, and a recall trial (word recall,completion of the paired associate as response to a given single word).Maximum possible scores were 18 for the face–name test, and 3 forthe word-pair test. qEEG was recorded both during resting states andduring cognitive activity when patients learned and recalled new infor-mation. qEEGmarkerswere calculated separately for the eleven periodsof the test. Intervals of rest and cognitive activity were compared as totheir corresponding qEEG activity.
2.3. EEG recordings
Patients sat in upright position on a comfortable chairwith neck rest.A 21 inch computer screen was placed in convenient distance to thepatient's head. The room was normally illuminated with no dazzlinglight and disturbances were held off during the recordings. EEG datawere collected from 19 monopolar electrode sites of the international10/20 system. Data acquisition was performed on an AlphaEEG amplifi-er with NeuroSpeed software (Alpha Trace Medical systems, Vienna,Austria). Electrodes for the horizontal electrooculogram (H-EOG) wereplaced on the right side of the right eye and on the left side of the lefteye. Electrodes for the vertical electrooculogram (V-EOG) were placedvertically above and below the left eye. The ground electrode wasplaced at FCz. Connected mastoid electrodes were used as reference.Electrode contacts were arranged to achieve impedances below 10 kΩ.
Table 2Group characteristics for 40 medication-free patients.
Median Median absolutedeviation
Range
Age (years) 74 7 54–87Level of education (scale 1–6) 2 1 1–4Duration of illness (months) 14 8.5 2–60MMSE (max. 30) 23 2 26–15CDR (max. 3) 0.5 0 0–2DAD (max. 100) 92.5 7.5 45–100
's disease: Cognitive state, resting state and association with disease.2014.06.003

Table 3Timeline, sequence and materials of the cognitive qEEG.
Phase Duration (s) Test and materials Eyes Sum score
Rest 1 180 None ClosedRest 2 180 None OpenFace–name test Encoding 1 3 × 10 Sequential presentation of 3 face–name pairs Open
Name recall 1 3 × 10 Faces alone, matching of corresponding names Open 3Encoding 2 3 × 10 Same as encoding 1 OpenConsolidation 90 Silent rehearsal of face–name pairs ClosedRecognition Unlimited Pseudorandom presentation of 3 target faces and 6 distractors,
yes–no recognition of original facesOpen 12
Name recall 2 3 × 10 Same as name recall 1 Open 3Paired word learning test Encoding 3 140 Presentation of 3 word pairs, 2 times Open
Word recall 60 First words shown alone, second words to be matched Open 3Rest 3 150 None Closed
3H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
The EEG amplifiers had a bandpass from0.3 to 70Hz (3 dB points),witha 50 Hz notch filter. Data were sampled at a rate of 256 s−1 with 16 bitresolution. The electrocardiographic (ECG) signal was recorded viaclamp electrodes that were put at both wrists.
3. Theory/calculation
3.1. qEEG markers
EEG signal preprocessing included (1) visual selection of usableepochs to exclude artifacts, (2) elimination of interferences from eyemovements and blinks by linear regression using the horizontal andvertical electrooculogram (H-EOG, V-EOG) signals, and (3) detectionand correction of interferences from the heart beat by using a modifiedPan–Tompkins algorithmand linear regression (Waser andGarn, 2013).A 2 Hertz high pass filter was used to eliminate fluctuations caused bysweating. Finally, a sliding window was moved automatically over theartifact-free, interference-corrected sections of the EEG to determineseries of 4-second epochs with an overlap of 2 s. These epochs wereused to calculate the EEG-markers for each phase.
Analyses were performed on 19 electrodes in the 2–20 Hz frequencyrange. The electrodes T7, T8, F7, F8, P7, and P8 were limited to 15 Hz toavoid the inclusion of muscle activity. In addition, the markers werecalculated on the first and second principal components of electrodeclusters. Clusters were defined as follows (Dauwels et al., 2010): central(Ce): Fz, Cz, Pz, C3, and C4; temporal (Te): F7, T7, and P7 (left side) andF8, T8, and P8 (right side), respectively; posterior (Po): P3, P4, O1, andO2; parietal–occipital (Pa-Oc): P7, P3, O1, P8, P4, and O2; left (L): FP1,F3, F7, C3, T7, P3, P7, and O1. For each electrode or cluster, results forall selected epochs were averaged within each period of the paradigm.
We calculated relative band powers as measures of frequencyslowing in the delta (2–4 Hz), theta (4–8 Hz), alpha (8–13 Hz), andbeta1 (13–20Hz) bands using an indirect spectral estimator to estimatethe spectral density for each of the visually selected epochs as demon-strated in (Waser et al., 2013). Thereby, Fourier transformation wasnot applied on the original time signal, but on its covariance function.By using a so-called lag-window, sample points with greater time lagswereweighted less than sample points that are close to each other. Hav-ing estimated the spectral density, the power in a certain frequencybandwas calculated from the amplitude sumwithin border frequencies.Values for each frequency band were expressed as percentage of thepower in the total 2–20 Hz range.
Coherences were calculated as measures of synchrony in thefrequency ranges delta (2–4 Hz), theta (4–8 Hz), alpha (8–13 Hz), andbeta1 (13–20 Hz) between the following pairs of electrode clusters:anterior–central, anterior–posterior, anterior-temporal/left, anterior-temporal/right, central–posterior, central-temporal/left, central-temporal/right, posterior-temporal/left, posterior-temporal/right, tem-poral/left–temporal/right, anterior/temporal–parietal/occipital, left–right.
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimer'severity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
Auto-mutual information was calculated as a measure of signalcomplexity in the frequency range of 2–15 Hz.
3.2. Statistical analysis
Computations were performed using Matlab R 2011a. All qEEGmarkers were calculated for each patient and for each period of theparadigm.
We used scatterplots to visualize the correlation between qEEGmarkers andMMSE scores. Univariate, quadratic regressionswere fittedto these graphs. Fisher's F-testswere used to determine statistical signif-icance in the regressions. Analyses were adjusted for the co-variablesage, sex, duration of dementia, and educational level. Age and durationof dementiawere introduced via both linear and quadratic terms. Treat-ment with anti-dementia drugs (yes/no), APOE (one or two e4 allelesversus no e4 allele) as well as cross-terms between the confoundingvariables were not significant. Coefficients of determination (R2) werecalculated to evaluate to what extent the variations in qEEG markerscould be explained by MMSE scores.
To determine statistical significance of the differences foundbetween markers in resting states and markers in cognitive states,we first tested the squared deviations of the data points from theregressions for normal distribution using the one-sample Kolmogorov–Smirnov test. To test for equality or inequality of variances, the two-sample F-test for equal variances (normal distribution) or the Ansari–Bradley test (no normal distribution) was applied.
4. Results
4.1. Behavioural results
Fig. 1 provides an overview of the sum scores of the face–name test(Fig. 1a) and the word-pair test (Fig. 1b). The majority of AD patientsscored in the upper range of both tests. As evident from their recalland recognition accuracy it can be assumed that the cohort understoodthe test procedure and actively participated in both tests.
4.2. qEEG
The resulting R2 were compared between resting states and cogni-tive states. Fig. 2 shows examples of differential results for two selectedmarkers: For relative delta band power (left column, 2a, 2c, 2e), signif-icant results (p b 0.01) occurred in resting state with eyes closed, butnot during recall of faces or word pairs with eyes open. For coherence(right column, 2b, 2d, 2e), significant results (p b 0.01) occurred duringrecall of faces and word pairs, but not in resting state with eyes closed.Table 4 presents an overview of selected (best) results for the coeffi-cients of determination (R2) for each qEEG measure in its optimal cog-nitive state. Table 5 presents results for the medication-free patients
s disease: Cognitive state, resting state and association with disease.2014.06.003
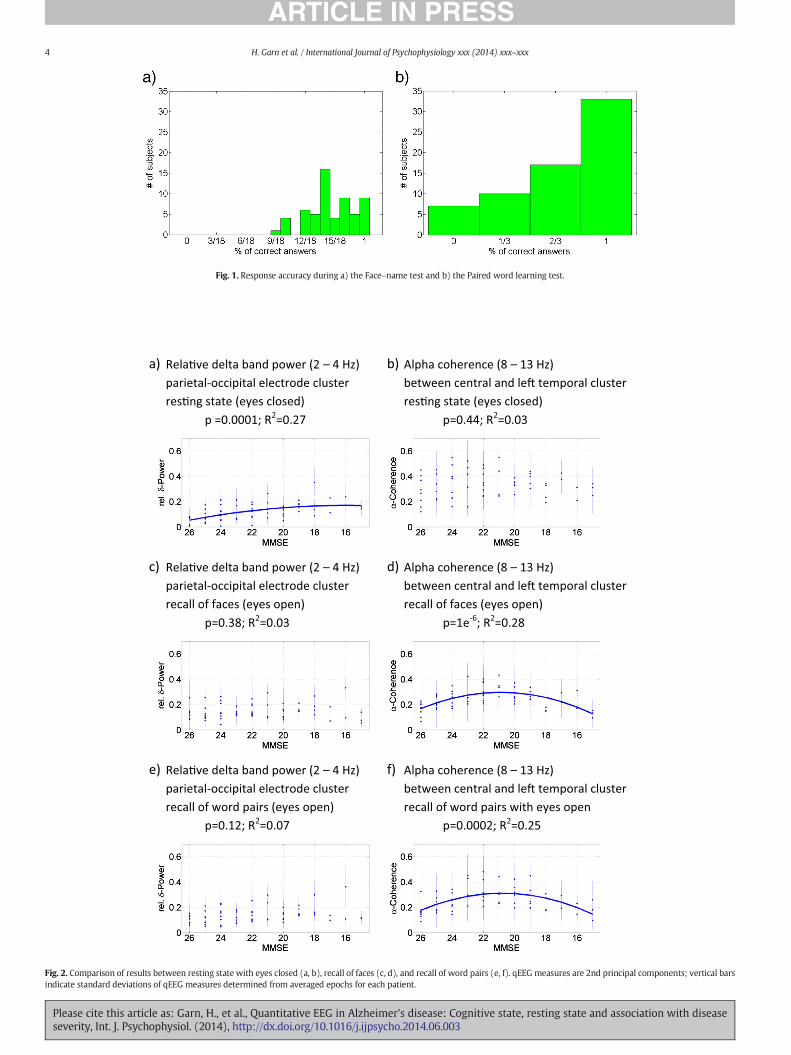
Fig. 1. Response accuracy during a) the Face–name test and b) the Paired word learning test.
a) Rela�ve delta band power (2 – 4 Hz) b) Alpha coherence (8 – 13 Hz)parietal-occipital electrode cluster between central and le� temporal cluster res�ng state (eyes closed) res�ng state (eyes closed)
p =0.0001; R2=0.27 p=0.44; R2=0.03
c) Rela�ve delta band power (2 – 4 Hz) d) Alpha coherence (8 – 13 Hz)parietal-occipital electrode cluster between central and le� temporal cluster recall of faces (eyes open) recall of faces (eyes open)
p=0.38; R2=0.03 p=1e-6; R2=0.28
e) Rela�ve delta band power (2 – 4 Hz) f) Alpha coherence (8 – 13 Hz)parietal-occipital electrode cluster between central and le� temporal clusterrecall of word pairs (eyes open) recall of word pairs with eyes open
p=0.12; R2=0.07 p=0.0002; R2=0.25
Fig. 2. Comparison of results between resting state with eyes closed (a, b), recall of faces (c, d), and recall of word pairs (e, f). qEEG measures are 2nd principal components; vertical barsindicate standard deviations of qEEG measures determined from averaged epochs for each patient.
4 H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimer's disease: Cognitive state, resting state and association with diseaseseverity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho.2014.06.003
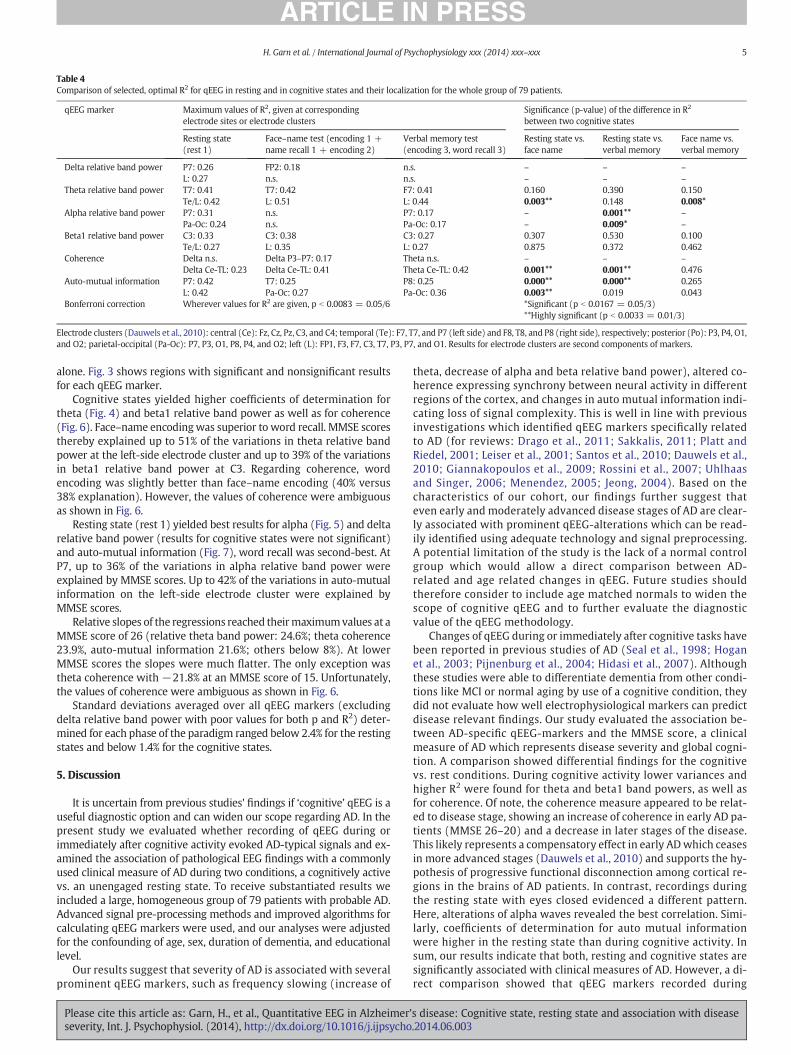
Table 4Comparison of selected, optimal R2 for qEEG in resting and in cognitive states and their localization for the whole group of 79 patients.
qEEG marker Maximum values of R2, given at correspondingelectrode sites or electrode clusters
Significance (p-value) of the difference in R2
between two cognitive states
Resting state(rest 1)
Face–name test (encoding 1 +name recall 1 + encoding 2)
Verbal memory test(encoding 3, word recall 3)
Resting state vs.face name
Resting state vs.verbal memory
Face name vs.verbal memory
Delta relative band power P7: 0.26 FP2: 0.18 n.s. – – –
L: 0.27 n.s. n.s. – – –
Theta relative band power T7: 0.41 T7: 0.42 F7: 0.41 0.160 0.390 0.150Te/L: 0.42 L: 0.51 L: 0.44 0.003** 0.148 0.008*
Alpha relative band power P7: 0.31 n.s. P7: 0.17 – 0.001** –
Pa-Oc: 0.24 n.s. Pa-Oc: 0.17 – 0.009* –
Beta1 relative band power C3: 0.33 C3: 0.38 C3: 0.27 0.307 0.530 0.100Te/L: 0.27 L: 0.35 L: 0.27 0.875 0.372 0.462
Coherence Delta n.s. Delta P3–P7: 0.17 Theta n.s. – – –
Delta Ce-TL: 0.23 Delta Ce-TL: 0.41 Theta Ce-TL: 0.42 0.001** 0.001** 0.476Auto-mutual information P7: 0.42 T7: 0.25 P8: 0.25 0.000** 0.000** 0.265
L: 0.42 Pa-Oc: 0.27 Pa-Oc: 0.36 0.003** 0.019 0.043Bonferroni correction Wherever values for R2 are given, p b 0.0083 = 0.05/6 *Significant (p b 0.0167 = 0.05/3)
**Highly significant (p b 0.0033 = 0.01/3)
Electrode clusters (Dauwels et al., 2010): central (Ce): Fz, Cz, Pz, C3, and C4; temporal (Te): F7, T7, and P7 (left side) and F8, T8, and P8 (right side), respectively; posterior (Po): P3, P4, O1,and O2; parietal-occipital (Pa-Oc): P7, P3, O1, P8, P4, and O2; left (L): FP1, F3, F7, C3, T7, P3, P7, and O1. Results for electrode clusters are second components of markers.
5H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
alone. Fig. 3 shows regions with significant and nonsignificant resultsfor each qEEG marker.
Cognitive states yielded higher coefficients of determination fortheta (Fig. 4) and beta1 relative band power as well as for coherence(Fig. 6). Face–name encodingwas superior to word recall. MMSE scoresthereby explained up to 51% of the variations in theta relative bandpower at the left-side electrode cluster and up to 39% of the variationsin beta1 relative band power at C3. Regarding coherence, wordencoding was slightly better than face–name encoding (40% versus38% explanation). However, the values of coherence were ambiguousas shown in Fig. 6.
Resting state (rest 1) yielded best results for alpha (Fig. 5) and deltarelative band power (results for cognitive states were not significant)and auto-mutual information (Fig. 7), word recall was second-best. AtP7, up to 36% of the variations in alpha relative band power wereexplained by MMSE scores. Up to 42% of the variations in auto-mutualinformation on the left-side electrode cluster were explained byMMSE scores.
Relative slopes of the regressions reached theirmaximumvalues at aMMSE score of 26 (relative theta band power: 24.6%; theta coherence23.9%, auto-mutual information 21.6%; others below 8%). At lowerMMSE scores the slopes were much flatter. The only exception wastheta coherence with −21.8% at an MMSE score of 15. Unfortunately,the values of coherence were ambiguous as shown in Fig. 6.
Standard deviations averaged over all qEEG markers (excludingdelta relative band power with poor values for both p and R2) deter-mined for each phase of the paradigm ranged below 2.4% for the restingstates and below 1.4% for the cognitive states.
5. Discussion
It is uncertain from previous studies' findings if ‘cognitive’ qEEG is auseful diagnostic option and can widen our scope regarding AD. In thepresent study we evaluated whether recording of qEEG during orimmediately after cognitive activity evoked AD-typical signals and ex-amined the association of pathological EEG findings with a commonlyused clinical measure of AD during two conditions, a cognitively activevs. an unengaged resting state. To receive substantiated results weincluded a large, homogeneous group of 79 patients with probable AD.Advanced signal pre-processing methods and improved algorithms forcalculating qEEG markers were used, and our analyses were adjustedfor the confounding of age, sex, duration of dementia, and educationallevel.
Our results suggest that severity of AD is associated with severalprominent qEEG markers, such as frequency slowing (increase of
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimer'severity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
theta, decrease of alpha and beta relative band power), altered co-herence expressing synchrony between neural activity in differentregions of the cortex, and changes in auto mutual information indi-cating loss of signal complexity. This is well in line with previousinvestigations which identified qEEG markers specifically relatedto AD (for reviews: Drago et al., 2011; Sakkalis, 2011; Platt andRiedel, 2001; Leiser et al., 2001; Santos et al., 2010; Dauwels et al.,2010; Giannakopoulos et al., 2009; Rossini et al., 2007; Uhlhaasand Singer, 2006; Menendez, 2005; Jeong, 2004). Based on thecharacteristics of our cohort, our findings further suggest thateven early and moderately advanced disease stages of AD are clear-ly associated with prominent qEEG-alterations which can be read-ily identified using adequate technology and signal preprocessing.A potential limitation of the study is the lack of a normal controlgroup which would allow a direct comparison between AD-related and age related changes in qEEG. Future studies shouldtherefore consider to include age matched normals to widen thescope of cognitive qEEG and to further evaluate the diagnosticvalue of the qEEG methodology.
Changes of qEEG during or immediately after cognitive tasks havebeen reported in previous studies of AD (Seal et al., 1998; Hoganet al., 2003; Pijnenburg et al., 2004; Hidasi et al., 2007). Althoughthese studies were able to differentiate dementia from other condi-tions like MCI or normal aging by use of a cognitive condition, theydid not evaluate how well electrophysiological markers can predictdisease relevant findings. Our study evaluated the association be-tween AD-specific qEEG-markers and the MMSE score, a clinicalmeasure of AD which represents disease severity and global cogni-tion. A comparison showed differential findings for the cognitivevs. rest conditions. During cognitive activity lower variances andhigher R2 were found for theta and beta1 band powers, as well asfor coherence. Of note, the coherence measure appeared to be relat-ed to disease stage, showing an increase of coherence in early AD pa-tients (MMSE 26–20) and a decrease in later stages of the disease.This likely represents a compensatory effect in early ADwhich ceasesin more advanced stages (Dauwels et al., 2010) and supports the hy-pothesis of progressive functional disconnection among cortical re-gions in the brains of AD patients. In contrast, recordings duringthe resting state with eyes closed evidenced a different pattern.Here, alterations of alpha waves revealed the best correlation. Simi-larly, coefficients of determination for auto mutual informationwere higher in the resting state than during cognitive activity. Insum, our results indicate that both, resting and cognitive states aresignificantly associated with clinical measures of AD. However, a di-rect comparison showed that qEEG markers recorded during
s disease: Cognitive state, resting state and association with disease.2014.06.003
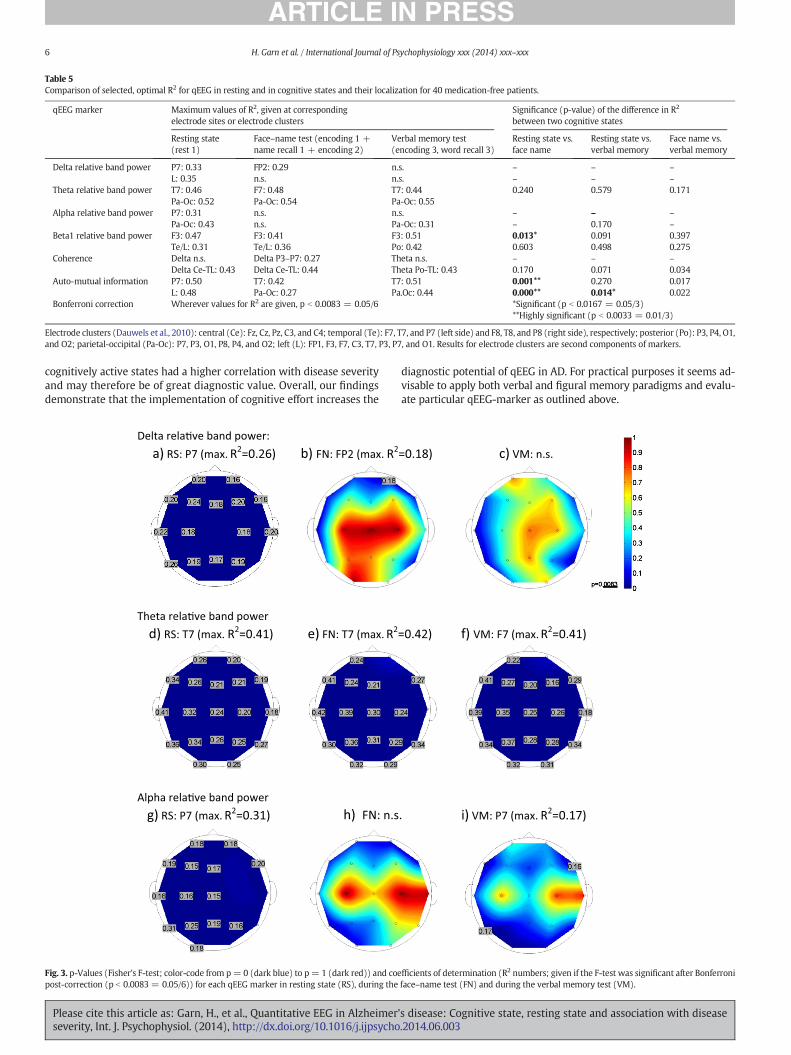
Table 5Comparison of selected, optimal R2 for qEEG in resting and in cognitive states and their localization for 40 medication-free patients.
qEEG marker Maximum values of R2, given at correspondingelectrode sites or electrode clusters
Significance (p-value) of the difference in R2
between two cognitive states
Resting state(rest 1)
Face–name test (encoding 1 +name recall 1 + encoding 2)
Verbal memory test(encoding 3, word recall 3)
Resting state vs.face name
Resting state vs.verbal memory
Face name vs.verbal memory
Delta relative band power P7: 0.33 FP2: 0.29 n.s. – – –
L: 0.35 n.s. n.s. – – –
Theta relative band power T7: 0.46 F7: 0.48 T7: 0.44 0.240 0.579 0.171Pa-Oc: 0.52 Pa-Oc: 0.54 Pa-Oc: 0.55
Alpha relative band power P7: 0.31 n.s. n.s. – – –
Pa-Oc: 0.43 n.s. Pa-Oc: 0.31 – 0.170 –
Beta1 relative band power F3: 0.47 F3: 0.41 F3: 0.51 0.013* 0.091 0.397Te/L: 0.31 Te/L: 0.36 Po: 0.42 0.603 0.498 0.275
Coherence Delta n.s. Delta P3–P7: 0.27 Theta n.s. – – –
Delta Ce-TL: 0.43 Delta Ce-TL: 0.44 Theta Po-TL: 0.43 0.170 0.071 0.034Auto-mutual information P7: 0.50 T7: 0.42 T7: 0.51 0.001** 0.270 0.017
L: 0.48 Pa-Oc: 0.27 Pa.Oc: 0.44 0.000** 0.014* 0.022Bonferroni correction Wherever values for R2 are given, p b 0.0083 = 0.05/6 *Significant (p b 0.0167 = 0.05/3)
**Highly significant (p b 0.0033 = 0.01/3)
Electrode clusters (Dauwels et al., 2010): central (Ce): Fz, Cz, Pz, C3, and C4; temporal (Te): F7, T7, and P7 (left side) and F8, T8, and P8 (right side), respectively; posterior (Po): P3, P4, O1,and O2; parietal-occipital (Pa-Oc): P7, P3, O1, P8, P4, and O2; left (L): FP1, F3, F7, C3, T7, P3, P7, and O1. Results for electrode clusters are second components of markers.
6 H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
cognitively active states had a higher correlation with disease severityand may therefore be of great diagnostic value. Overall, our findingsdemonstrate that the implementation of cognitive effort increases the
Delta rela�ve band power:a) RS: P7 (max. R2=0.26) b) FN: FP2 (max. R2
Theta rela�ve band powerd) RS: T7 (max. R2=0.41) e) FN: T7 (max. R2
Alpha rela�ve band powerg) RS: P7 (max. R2=0.31) h) FN: n.s
Fig. 3. p-Values (Fisher's F-test; color-code from p= 0 (dark blue) to p= 1 (dark red)) and coepost-correction (p b 0.0083 = 0.05/6)) for each qEEG marker in resting state (RS), during the
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimerseverity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
diagnostic potential of qEEG in AD. For practical purposes it seems ad-visable to apply both verbal and figural memory paradigms and evalu-ate particular qEEG-marker as outlined above.
=0.18) c) VM: n.s.
=0.42) f) VM: F7 (max. R2=0.41)
. i) VM: P7 (max. R2=0.17)
fficients of determination (R2 numbers; given if the F-test was significant after Bonferroniface–name test (FN) and during the verbal memory test (VM).
's disease: Cognitive state, resting state and association with disease.2014.06.003
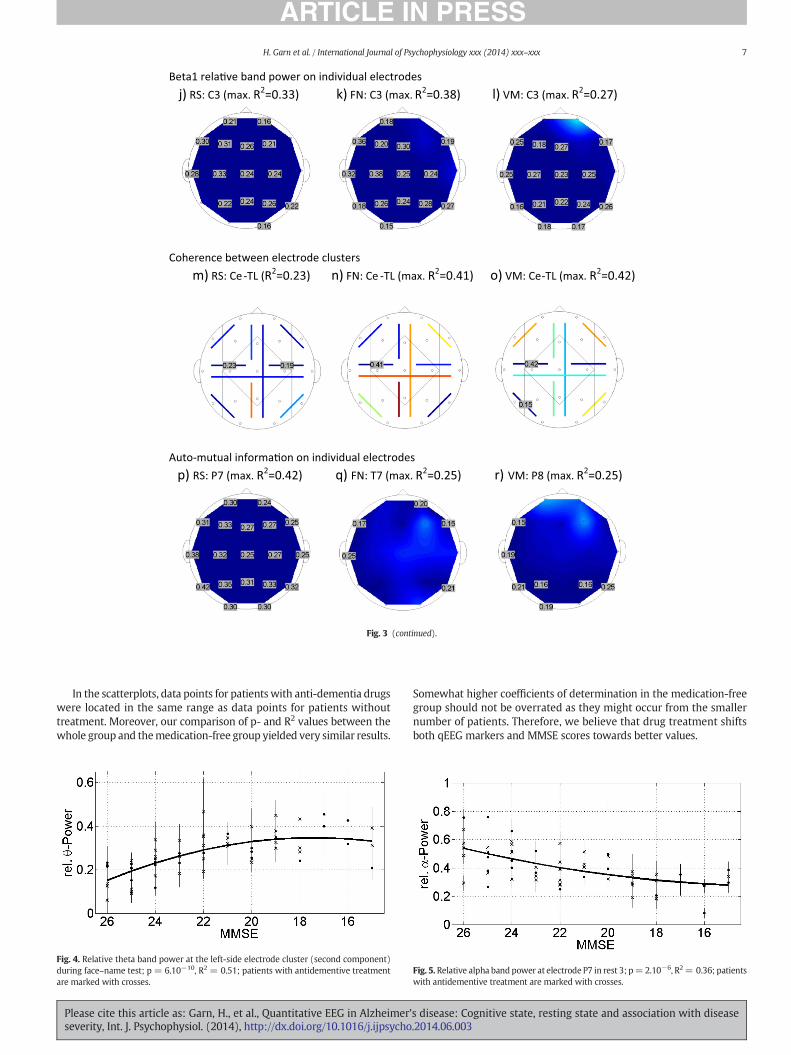
Beta1 rela�ve band power on individual electrodes j) RS: C3 (max. R2=0.33) k) FN: C3 (max. R2=0.38) l) VM: C3 (max. R2=0.27)
Coherence between electrode clusters m) RS: Ce-TL (R2=0.23) n) FN: Ce -TL (max. R2=0.41) o) VM: Ce-TL (max. R2=0.42)
Auto-mutual informa�on on individual electrodes p) RS: P7 (max. R2=0.42) q) FN: T7 (max. R2=0.25) r) VM: P8 (max. R2=0.25)
Fig. 3 (continued).
7H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
In the scatterplots, data points for patients with anti-dementia drugswere located in the same range as data points for patients withouttreatment. Moreover, our comparison of p- and R2 values between thewhole group and themedication-free group yielded very similar results.
Fig. 4. Relative theta band power at the left-side electrode cluster (second component)during face–name test; p = 6.10−10, R2 = 0.51; patients with antidementive treatmentare marked with crosses.
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimer'severity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
Somewhat higher coefficients of determination in the medication-freegroup should not be overrated as they might occur from the smallernumber of patients. Therefore, we believe that drug treatment shiftsboth qEEG markers and MMSE scores towards better values.
Fig. 5. Relative alpha band power at electrode P7 in rest 3; p=2.10−6, R2= 0.36; patientswith antidementive treatment are marked with crosses.
s disease: Cognitive state, resting state and association with disease.2014.06.003

Fig. 6. Theta coherence between central and left temporal electrode cluster (secondcomponent) during encoding 3; p = 9.10−8, R2 = 0.40; patients with antidementivetreatment are marked with crosses.
8 H. Garn et al. / International Journal of Psychophysiology xxx (2014) xxx–xxx
Previous cognitive qEEG studies of AD have mainly employed taskstapping attention (Seal et al., 1998; Hidasi et al., 2007) and workingmemory (Pijnenburg et al., 2004, Karrasch 2006). In the present studywe used two episodic memory tasks during EEG recordings tappingthe ability to learn, retain, and recall new information. Both, the verbalmemory and the face–name task were associated with marked qEEG-abnormalities, and MMSE scores explained up to 51% of the variance.We assume that this effect reflects an attempt to utilize defective neuralnetworks engaged in episodic memory functions which are commonlyimpaired in AD. However, the face–name task yielded even strongercorrelations with MMSE scores than the verbal memory task. Severalstudies agree that forming conjunctions of stimuli as in face–nameassociation learning is already impaired in early AD (Werheid andClare, 2007; Sperling R, 2007; Della Sala et al., 2012). This task maytherefore represent a sensitive method to detect disease specific alter-ations of cognitive qEEG recordings in AD. We conclude that someqEEG markers more than others appear to be associated with diseaseseverity and cognitive decline and may therefore serve as severity-related markers.
Acknowledgment
This study was supported by the Austrian Research PromotionAgency (FFG) (project no. 827462), Dr. Grossegger & Drbal GmbH andby the Austrian Alzheimer Society, http://www.alzheimer-gesellschaft.at/.
References
Benke, T., Delazer, M., Sanin, G., Schmidt, H., Seiler, S., Ransmyer, G., Dal-Bianco, P.,Uranüs, M., Marksteiner, J., Leblhuber, F., Kapeller, P., Bancher, C., Schmidt, R., 2013.Cognition, gender, and functional abilities in Alzheimer's disease: how are they relat-ed? J. Alzheimer's Dis. 35 (2), 247–252.
Fig. 7. Auto-mutual information on the left-side electrode cluster (second component)during rest 1; p= 5.10−8, R2 = 0.42; patients with antidementive treatment are markedwith crosses.
Please cite this article as: Garn, H., et al., Quantitative EEG in Alzheimerseverity, Int. J. Psychophysiol. (2014), http://dx.doi.org/10.1016/j.ijpsycho
Berg, L., 1988. Clinical Dementia Rating (CDR). Psychopharmacol. Bull. 24 (4), 637–639.Dauwels, J., Vialette, F., Musha, T., Cichocki, A., 2010. A comparative study of synchrony
measures for the early diagnosis of Alzheimer's disease based on EEG. Neuroimage49, 668–693.
Della Sala, S., Parra, M.A., Fabi, K., Luzzi, S., Abrahams, S., 2012. Short-term memory bind-ing is impaired in AD but not in non-AD dementias. Neuropsychologia 50 (5),833–840.
Drago, V., Babiloni, C., Bartrés-Faz, D., Caroli, A., Bosch, B., Hensch, T., Didic, M., Klafki, H.-W., Pievani, M., Jovicich, J., Venturi, L., Spitzer, P., Vecchio, F., Schoenknecht, P.,Wiltfang, J., Redolfi, A., Forloni, G., Blin, O., Irving, E., Davis, C., Hardemark, H.-G.,Frisoni, G.B., 2011. Disease tracking markers for Alzheimer's disease at the prodromal(MCI) stage. J. Alzheimer's Dis. 26, 159–1999.
Dubois, B., Feldman, H., Jacova, C., DeKosky, S.T., Barberger-Gateau, P., Cummings, J.,Delacourte, A., Galasko, D., Gauthier, S., Jicha, G., Meguro, K., O'brien, J., Pasquier, F.,Robert, P., Rossor, M., Salloway, S., Stern, Y., Visser, P.J., Scheltens, P., 2007. Researchcriteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria.Lancet Neurol. 6, 734–746.
Folstein, M.F., Folstein, S.E., McHugh, P.R., 1975. Mini-mental state A practical method forgrading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198.
Gelinas, I., Gauthier, L., McIntyre, M., Gauthier, S., 1999. Development of a functional mea-sure for persons with Alzheimer's disease: the Disability Assessment for Dementia.Am. J. Occup. Ther. 53, 471–481.
Giannakopoulos, P., Missonnier, P., Koevari, E., Gold, G., Michon, A., 2009. Electrophysio-logical markers of rapid cognitive decline in mild cognitive impairment. Front NeurolNeurosci 24, 39–46.
Hidasi, Z., Czigler, B., Salacz, P., Csibri, E., Molnar, M., 2007. Changes of EEG spectra and co-herence following performance in a cognitive task in Alzheimer's disease. Int. J.Psychophysiol. 65, 252–260.
Hogan, M.J., Swanwick, G.R.J., Kaiser, J., Rowan, M., Lawlor, B., 2003. Memory-related EEGpower and coherence reductions inmild Alzheimer's disease. Int. J. Psychophysiol. 49,147–163.
Jeong, J., 2004. EEG dynamics in patients with Alzheimer's disease. Clin. Neurophysiol.115, 1490–1505.
Karrasch, M., Laine, M., Rinne, J.O., Rapinoja, P., Sinervä, E., Krause, C.M., 2006. Brain oscil-latory responses to an auditory-verbal working memory task in mild cognitive im-pairment and Alzheimer's disease. Int J Psychophysiol 59, 168–178.
Klimesch,W., 1999. EEG alpha and theta oscillations reflect cognitive andmemory perfor-mance: a review and analysis. Brain Res. Rev. 29, 169–195.
Leiser, S.C., Dunlop, J., Bowlby, M.R., Devilbiss, D.M., 2001. Aligning strategies for usingEEG as a surrogate biomarker: a review of preclinical and clinical research. Biochem.Pharmacol. 81, 1408–1421.
McKhann, G., Drachmann, D., Folstein, M., Katzman, R., Price, D., Stadlan, E.M., 1984. Clin-ical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Groupunder the auspices of Department of Health and Human Services Task Force onAlzheimer's Disease. Neurology 34, 939–944.
Menendez, M., 2005. Down syndrome, Alzheimer's disease and seizures. Brain Dev. 27,246–252.
Pijnenburg, Y.A.L., Made, Y.V.D., van Cappellen vonWalsum, A.M., Knol, D.L., Scheltens, P.,Stam, C.J., 2004. EEG synchronization likelihood in mild cognitive impairment andAlzheimer's disease during a working memory task. Clin. Neurophysiol. 115,1332–1339.
Platt, B., Riedel, G., 2001. The cholinergic system, EEG and sleep. Behav. Brain Res. 221,499–504.
Rossini, P.M., Rossi, S., Babiloni, C., Polich, J., 2007. Clinical neurophysiology of aging brain:from normal aging to neuro-degeneration. Prog. Neurobiol. 83, 375–400.
Sakkalis, V., 2011. Review of advanced techniques for the estimation of brain connectivitymeasured with EEG/MEG. Comput. Biol. Med. 41, 1110–1117.
Santos, S.F., Pierrot, N., Octave, J.N., 2010. Network excitability dysfunction in Alzheimer'sdisease: insights from in vitro and in vivo models. Rev. Neurosci. 21 (3), 153–171.
Seal, E.C., van Hintum, C.J., Pierson, J.M., Helme, R.D., 1998. Quantitative electroencepha-lography, with serial subtraction and odour detection in the differentiation ofAlzheimer's disease and vascular dementia. Arch. Gerontol. Geriatr. 27 (2), 115–126.
Seiler, S., Schmidt, H., Lechner, A., Benke, T., Sanin, G., Ransmayr, G., Lehner, R., Dal-Bianco,P., Santer, P., Linortner, P., Eggers, C., Haider, B., Uranues, M., Marksteiner, J.,Leblhuber, F., Kapeller, P., Bancher, C., Schmidt, R., 2012. Driving cessation and de-mentia: results of the Prospective Registry on Dementia in Austria (PRODEM). PLoSONE 7 (12), e52710.
Sperling, R., 2007. Functional MRI studies of associative encoding in normal aging, mildcognitive impairment, and Alzheimer's disease. Ann. N. Y. Acad. Sci. 1097, 146–155.
Uhlhaas, P.J., Singer, W., 2006. Neural synchrony in brain disorders: relevance for cogni-tive dysfunction and pathophysiology. Neuron 52, 155–168.
Waser, M., Garn, H., 2013. Removing cardiac interference from the electroencephalogramusing a modified Pan–Tompkins algorithm and linear regression. 35th IEEE Int'l. Conf.Engineering in Medicine & Biology, Proc 2028-2031.
Waser, M., Deistler, M., Garn, H., Benke, T., Dal-Bianco, P., Ransmayr, G., Grossegger, D.,Schmidt, R., 2013. EEG in the diagnostics of Alzheimer's disease. Stat. Pap. 54 (4),1095–1107.
Werheid, K., Clare, L., 2007. Are faces special in Alzheimer's disease? Cognitive conceptu-alisation, neural correlates, and diagnostic relevance of impaired memory for facesand names. Cortex 43 (7), 898–906.
's disease: Cognitive state, resting state and association with disease.2014.06.003



















