Intrauterine Fetal Demise After Uncomplicated COVID-19 - MDPI
Upload
independentCategory
view
1download
0
AMERICAN JOURNAL OF PHYSICAL ANTHROPOLOGY 91215-224 (1993)
Protection From Intrauterine Growth Retardation in Tibetans at High Altitude
STACY ZAMUDIO, TARSHI DROMA, KUNDU Y. NORKYEL, GANESH ACHARYA, JOSEPH A. ZAMUDIO, SUSAN N. NIERMEYER, AND LORNA G. MOORE Cardiovascular Pulmonary Research Laboratory, University of Colorado Health Sciences Center, Denuer CO 80262 (S.Z., L.G.M.); Tibet Institute for Medical Science, Lhasa, Tibet Autonomous Region, 850000, China (T.D.); Department of Obstetrics and Gynecology, Patan Hospital, Kathmandu, Nepal (K.N., G.A.); Cooperative Institute for Research in Environmental Sciences, University of Colorado at Boulder, Boulder CO 80309 (J.A.Z.); Department of Pediatrics, University of Colorado Health Sciences Center, Denver, CO 80262 (S.N.N.1; Department of Anthropology, University of Colorado at Denver, Denver CO 8021 7 (S.Z., L.G.M.)
KEY WORDS tion, Comparison of North and South American populations
Fetal growth, Low birth weight, Genetic adapta-
ABSTRACT Intrauterine growth retardation has long been recognized at high altitude. Since growth-retarded babies have a decreased chance of sur- vival, intrauterine growth retardation would be expected to have been se- lected against in populations long resident at high altitude. We have previ- ously reported that Tibetan babies born at 3,658 m weighed more than their North or South American altitude counterparts. This study sought to deter- mine whether Tibetans were protected from altitude-associated intrauterine growth retardation. We compared birth weights in Tibetans living at low altitude in Kathmandu, Nepal (elevation 1,200 m), or at high altitude in Lhasa, Tibet Autonomous Region, China (elevation 3,658 m). Birth weights were similar in 45 low-altitude and 34 high-altitude Tibetan births regardless of whether all infants or only full-term births were considered, or whether birth weight was adjusted for variation in maternal parity, gestational age, and infant sex. In comparison with literature observations, the altitude-asso- ciated difference in birth weight was smallest in Tibetans, intermediate in South America, and greatest in North America. These data support the hy- pothesis that Tibetans are protected from altitude-associated intrauterine growth retardation and suggest that selection for optimization of birth weight at high altitude has occurred in Tibetans. o 1993 Wiley-Liss, Inc.
Altitude-associated intrauterine growth retardation has long been recognized in North and South America (Lichty et al., 1957; McCullough et al., 1977; Haas et al., 1980; Beall, 1981; Moore and Regensteiner, 1983; Yip, 1987). Since growth-retarded ba- bies have a decreased chance of survival at both low and high altitude (Karn and Pen- rose, 1951; Haas et al., 1987; Unger et al., 1988), natural selection would be expected to stabilize birth weight at values associated with the lowest mortality risk. Because
birth weight is subject to genetic control (Nance, 19761, we reason that populations long resident at high altitude would have undergone natural selection for adaptations that permit normal fetal growth.
Received January 10,1992; accepted October 14,1992. Address reprint requests to Stacy Zamudio, Ph.D., Cardiovas-
cular Pulmonary Research Laboratory (B1331, University of Col- orado Health Sciences Center, 4200 East 9th Avenue, Denver, CO 80262.
Q 1993 WILEY-LISS. INC
216 S. ZAMUDIO ET AL
We hypothesized that Tibetans, a long resident high-altitude population (Senshui, 1981), have birth weights similar to those observed at low altitude and greater than those of other high-altitude populations. In a previous report, we observed that a small sample of Tibetan babies born at 3,658 m weighed more than their North or South American altitude counterparts (Moore, 1990). However, in the absence of birth weights from Tibetans at low altitude, we were not able to determine whether Tibet- ans were protected from altitude-associated intrauterine growth retardation.
We undertook the present study in order to determine whether birth weight differs in Tibetans born a t low compared with high altitude. Information on birth weight and associated infant and maternal characteris- tics was collected from 45 births to healthy Tibetan women living at low altitude in Kathmandu, Nepal (elevation 1,200 m), and from 34 Tibetan births to healthy high-alti- tude residents of Lhasa, Tibet Autonomous Region, China (elevation 3,658 m). These data were compared with birth weight re- ductions previously reported for North and South American high-altitude populations to determine whether Tibetans were pro- tected from altitude-associated intrauterine growth retardation. Because it is likely that Tibetans have lived at high altitude for a longer period of time than the high-altitude inhabitants of North and South America (Senshui, 1981; Zhimin et al., 1982; Nunez, 1983; MacNeish and Berger, 1970; Lynch, 1978), we hoped that this comparison would enable us to determine whether time-depen- dent selection for optimization of birth weight a t high altitude is likely to have oc- cured.
MATERIALS AND METHODS Study sites and samples
The low-altitude sample was comprised of 45 Tibetan residents of Kathmandu, Nepal (1,200 m), who gave birth at the Patan Hos- pital between January-December 1990. The high-altitude sample was comprised of 34 Tibetan residents of Lhasa, Tibet Autono- mous Region, China (3,658 m), who gave birth a t the Peoples' Provincial Hospital be- tween September-November 1987, Octo-
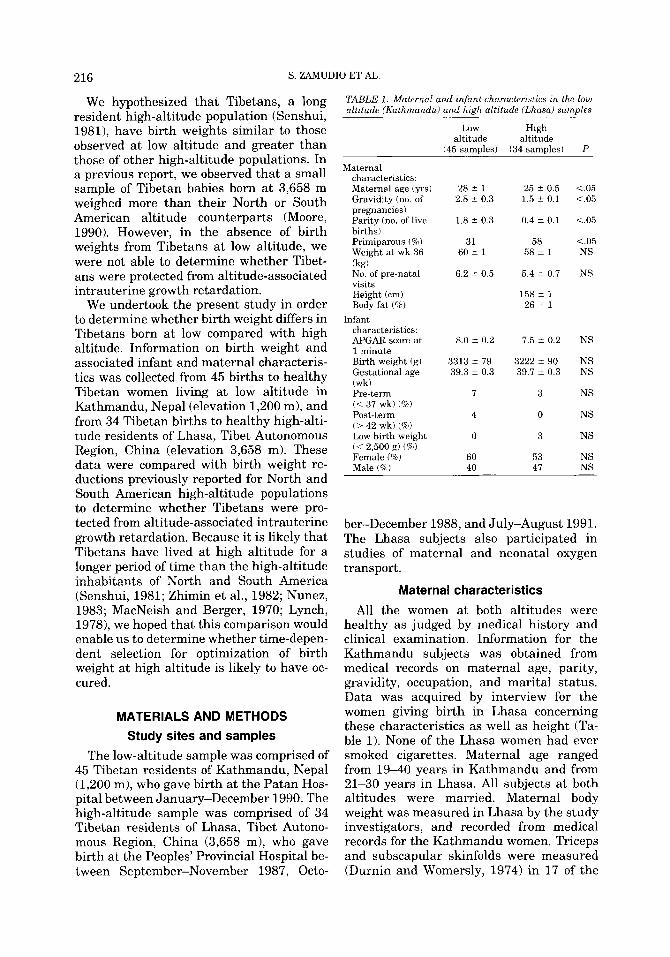
TABLE 1. Maternal and infant characteristics in the low altitude (Kathmandu) arid high altztude (Lhasai samules
Maternal characteristics: Maternal age (yrs) Gravidity (no. of pregnancies) Parity (no. of live births) Primiparous (8) Weight a t wk 36 (kg) No. of pre-natal visits Height (cm) Body fat (Q)
characteristics: APGAR score a t 1 minute Birth weight (g) Gestational age (wk) Pre-term (< 37 wk) ("70) Post-term (> 42 wk) (96) Low birth weight (< 2,500 g) (%) Female (%) Male ('%)
Infant
Low High altitude altitude
(45 samples) (34 samples)
28 i 1 2.8 2 0.3
1.8 -+ 0.3
25 2 0.5 1.5 t 0.1
0.4 i 0.1
31 58 60 lr 1
6.2 i 0.5
58 i 1
5.4 i 0.7
158 ? 1 26 i 1
8.0 i 0.2
3313 2 79
7.5 i 0.2
3222 i 90 39.3 i 0.3 39.7 i- 0.3
7 3
4 0
0 3
60 53 40 47
P ~
<.05 <.05
<.05
<.05 NS
NS
NS
NS NS
NS
NS
NS
NS NS
ber-December 1988, and July-August 1991. The Lhasa subjects also participated in studies of maternal and neonatal oxygen transport.
Maternal characteristics All the women at both altitudes were
healthy as judged by medical history and clinical examination. Information for the Kathmandu subjects was obtained from medical records on maternal age, parity, gravidity, occupation, and marital status. Data was acquired by interview for the women giving birth in Lhasa concerning these characteristics as well as height (Ta- ble 1). None of the Lhasa women had ever smoked cigarettes. Maternal age ranged from 1 9 4 0 years in Kathmandu and from 21-30 years in Lhasa. All subjects a t both altitudes were married. Maternal body weight was measured in Lhasa by the study investigators, and recorded from medical records for the Kathmandu women. Triceps and subscapular skinfolds were measured (Durnin and Womersly, 1974) in 17 of the
TIBETAN BIRTH WEIGHT 217
Lhasa subjects for an estimate of percent body fat. Body weights were obtained in 4 of the Lhasa women 2 years postpartum. None of the Kathmandu women reported having an occupation outside of the home while the Lhasa subjects were most commonly em- ployed in the home, clerical workers, or tradeswomen.
The Patan Hospital in Kathmandu is lo- cated adjacent to the large Tibetan immi- grant community of Jawalakhel, thus many Tibetan women attend prenatal clinics a t Patan Hospital. Kathmandu subjects were identified as Tibetan by a two-step proce- dure devised by Kundu Norkyel, M.D., Vice- Director of the Department of Obstetrics and Gynecology, and herself a Tibetan im- migrant. First, the birth registry a t Patan Hospital was reviewed for the period March 1987 to July 1991. Of the 11,150 total births, 6% or 665 infants were born to women who identified themselves as Tibetan (i.e., sub- ject name preceded by the ethnic designa- tion Lama). Because the father’s name was not recorded in the birth registry and hence there was no way to exclude births to Ti- betan mothers and non-Tibetan fathers, the second step was review of medical records for 5 randomly selected deliveries per month during the 1990 calendar year. Decisions regarding inclusion or exclusion were re- viewed by Dr. Norkyel. Of the 56 charts available, 9 (16%) of the infants had non- Tibetan fathers as judged by name, caste designation, and/or Hindu religion. For the remaining 47 infants both parents were Ti- betan as judged by the designation Lama, Tibetan surname, and Buddhist religion. Two subjects were excluded for maternal disease leaving 45 women and infants in the study. Information on place of birth or dura- tion of residence in Kathmandu was not available.
The women giving birth in Lhasa were identified as Tibetan on the basis of primary language spoken, self-identified ethnicity, and absence of any known non-Tibetan an- cestor. All the Lhasa women were born and had lived all their lives at elevations 3 3,600 m.
Infant characteristics Infants were weighed a t birth on a beam-
balance scale in Kathmandu (Continental Scale, model 322KG, Bridgeview, IL) and on
a spring-counterforce mechanical scale in Lhasa (Toledo Sentinel Mechanical New- born Scale, Model 1361, Toledo, OH). The scale in Lhasa was provided and calibrated by the authors. The Kathmandu scales were calibrated monthly with standard weights. In Kathmandu infant sex and 1 minute AP- GAR score was obtained from medical records. Gestational age was determined by weeks from the last menstrual period for both the Lhasa and Kathmandu deliveries. For 15 of the 34 deliveries in Lhasa, one of us (SN) determined gestational age using the modified-Ballard clinical exam (Ballard et al., 1977) and assigned APGAR scores at 1 and 5 minutes. The clinical estimate of ges- tational age agreed closely with estimates based on weeks from the last menstrual pe- riod (39.7 vs. 39.4 respectively, P = NS). In two of the 45 Kathmandu deliveries, gesta- tional age was estimated using ultrasound.
Statistics Data are reported as mean & standard er-
ror of the mean (SEM) in the text, tables, and figures. Maternal and infant character- istics were compared at low and high alti- tude using unpaired Students t-tests or chi- square tests. Analysis of variance was used to test for mean differences when three or more groups were considered, The relation- ship between birth weight and gestational age was assessed using linear regression techniques. Analysis of covariance was used to compare birth weights between the low- and high-altitude samples while controlling for variation in parity, gestational age, and infant sex. Comparisons are considered sig- nificant when P < .05.
RESULTS The women giving birth a t low altitude
were older and of higher gravidity and par- ity than the women at high altitude. Body weight a t week 36 and the number of prena- tal visits were similar in the low- and high- altitude residents (Table 1). Weight for height and estimated percent body fat in the Lhasa women were within normal values (Table 1). Pregnancy weight gain averaged 9 & 2 kg in the four Lhasa women for whom body weights were obtained in the nonpreg- nant state.
218 S. ZAMUDIO ET AL
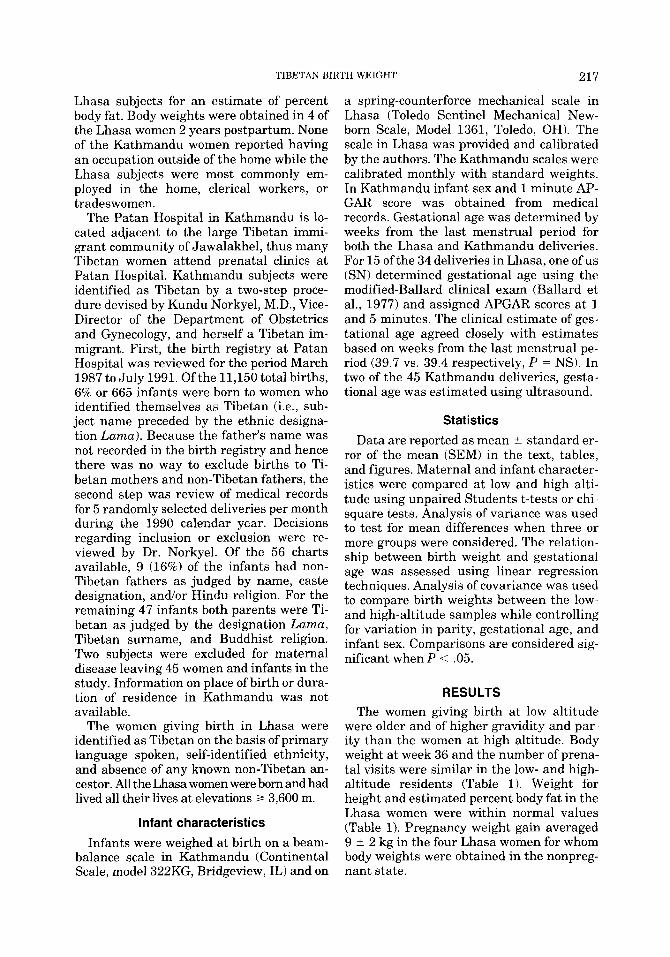
LOW ALTITUDE BIRTHS (3299 5 79 gm)
(39.7 A 0.3 weeks)
9 .i 7
-2499 2500- 2750 3000- 3250- 3500- 3750-4000- ,4250 2749 3000 3249 3499 3749 3999 4249
HIGH ALTITUDE BIRTHS (3236 5 76 gm)
(39.8 5 0.3 weeks) "I1 7 e, B
3 LT w m
z
~ 2 4 9 9 2500- 2750- 3000- 3250- 3500- 3750- 4000- ,4250 2749 3000 3249 3499 3749 3999 4249
BIRTH WEIGHT (gm)
Fig. 1. (P = NS).
Histogram of the birth weights of term infants (37-42 weeks) at low and high altitude
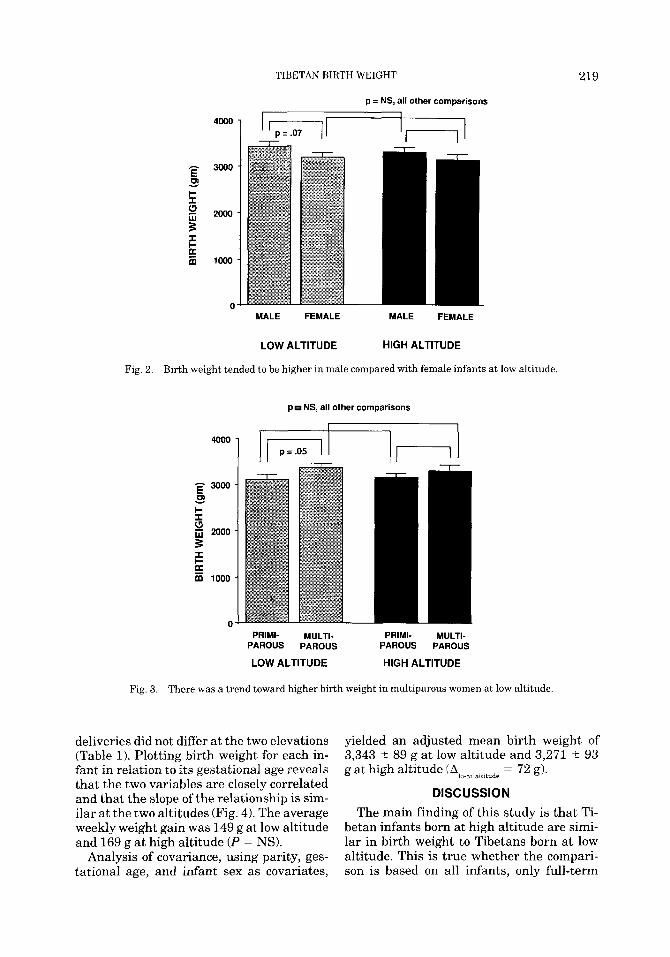
The APGAR scores of the low- and high- altitude infants were similar (Table 1). The average birth weight of Tibetan infants born at low altitude did not differ from that of the high-altitude Tibetan infants (Table 1, Alo.hi altitude = 69 g, P = NS). The birth weights were also similar when only term births (37-42 wk) were considered (Fig. 1). Male babies weighed the same whether born at low or high altitude. Likewise, birth weights of female infants did not differ a t low and
high altitude (Fig. 2). At low altitude, males were heavier than females (Fig. 2) and mul- tiparous women tended to have larger ba- bies than primiparous women (Fig. 3). At high altitude, male and female birth weights were similar (Fig. 2). In addition, birth weights did not differ in babies born to mul- tiparous compared with primiparous women at high altitude (Fig. 3).
Mean gestational age and the frequency of pre-term, post-term, and low birth weight
TIBETAN BIRTH WEIGHT 219
p = NS, all other comparisons I
- 3000 E m 1
5 $ 2000
E 1000
3 I I-
0 MALE FEMALE MALE FEMALE
LOW ALTITUDE HIGH ALTITUDE
Fig. 2. Birth weight tended to be higher in male compared with female infants at low altitude.
p NS, all other comparisons
I I I
PRIMI- MULTI- PRIMI- MULTI- PAROUS PAROUS PAROUS PAROUS
LOW ALTITUDE HIGH ALTITUDE
Fig. 3. There was a trend toward higher birth weight in multiparous women at low altitude.
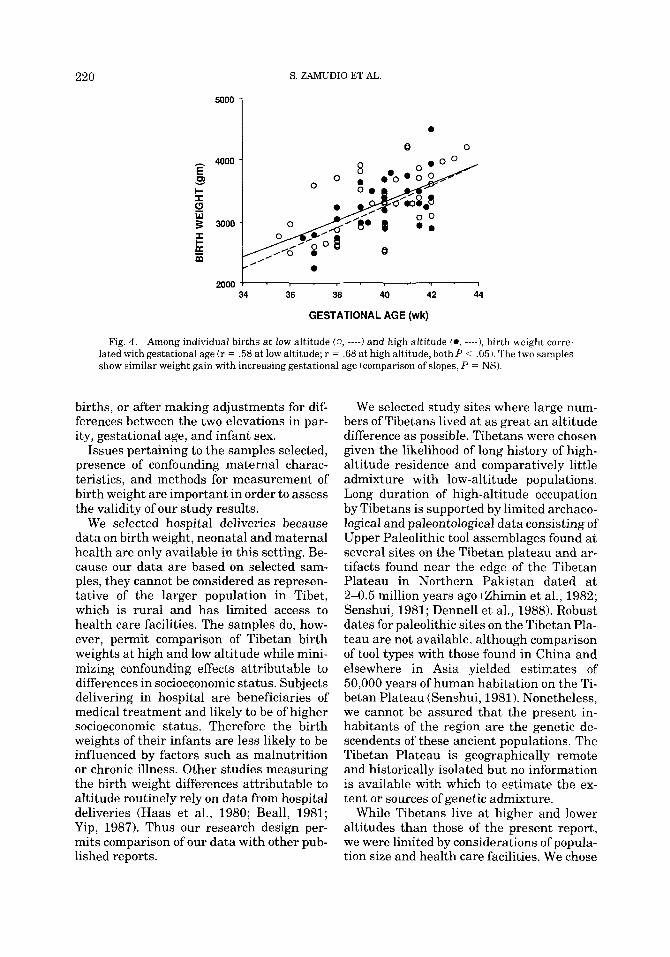
deliveries did not differ at the two elevations (Table 1). Plotting birth weight for each in- fant in relation to its gestational age reveals that the two variables are closely correlated and that the slope of the relationship is sim- ilar at the two altitudes (Fig. 4). The average weekly weight gain was 149 g at low altitude and 169 g at high altitude (P = NS).
Analysis of covariance, using parity, ges- tational age, and infant sex as covariates,
yielded an adjusted mean birth weight of 3,343 ? 89 g at low altitude and 3,271 ? 93 g a t high altitude
alt,iudp = 72g). DISCUSSION
The main finding of this study is that Ti- betan infants born at high altitude are simi- lar in birth weight to Tibetans born at low altitude. This is true whether the compari- son is based on all infants, only full-term
220 S. ZAMUDIO ET AL.
h
v k I- I
W
I I-
P 3
%
4000
3000
2000 34 36 38 40 42 44
GESTATIONAL AGE (wk)
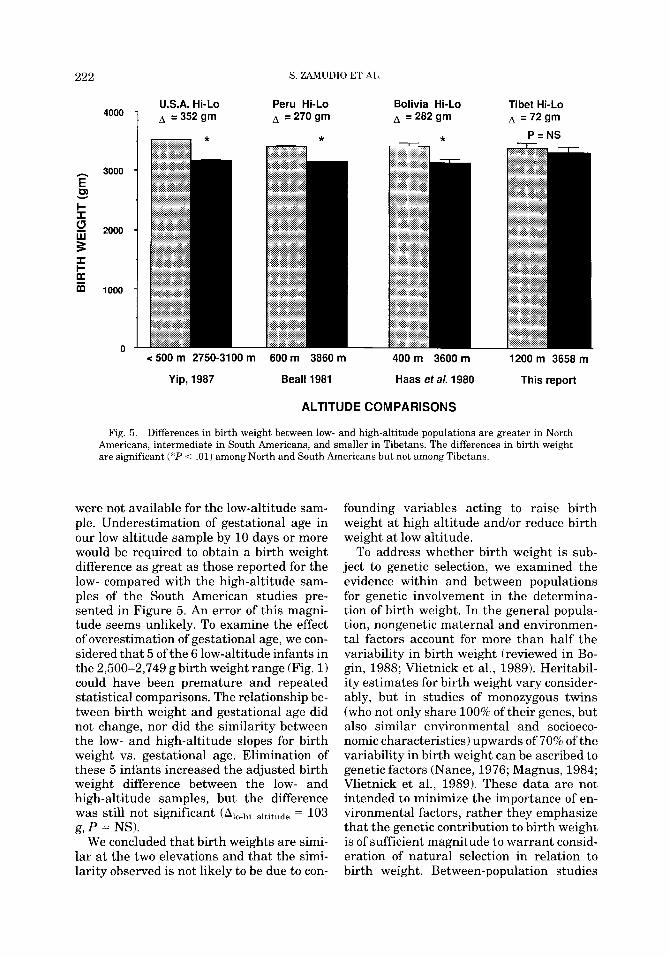
Fig. 4. Among individual births at low altitude (0, ----) and high altitude (0, ----I, birth weight corre- lated with gestational age (r = .58 at low altitude; r = .68 at high altitude, both P < .05). The two samples show similar weight gain with increasing gestational age (comparison of slopes, P = NS).
births, or after making adjustments for dif- ferences between the two elevations in par- ity, gestational age, and infant sex.
Issues pertaining to the samples selected, presence of confounding maternal charac- teristics, and methods for measurement of birth weight are important in order to assess the validity of our study results.
We selected hospital deliveries because data on birth weight, neonatal and maternal health are only available in this setting. Be- cause our data are based on selected sam- ples, they cannot be considered as represen- tative of the larger population in Tibet, which is rural and has limited access to health care facilities. The samples do, how- ever, permit comparison of Tibetan birth weights a t high and low altitude while mini- mizing confounding effects attributable to differences in socioeconomic status. Subjects delivering in hospital are beneficiaries of medical treatment and likely to be of higher socioeconomic status. Therefore the birth weights of their infants are less likely to be influenced by factors such as malnutrition or chronic illness. Other studies measuring the birth weight differences attributable to altitude routinely rely on data from hospital deliveries (Haas et al., 1980; Beall, 1981; Yip, 1987). Thus our research design per- mits comparison of our data with other pub- lished reports.
We selected study sites where large num- bers of Tibetans lived at as great an altitude difference a s possible. Tibetans were chosen given the likelihood of long history of high- altitude residence and comparatively little admixture with low-altitude populations. Long duration of high-altitude occupation by Tibetans is supported by limited archaeo- logical and paleontological data consisting of Upper Paleolithic tool assemblages found a t several sites on the Tibetan plateau and ar- tifacts found near the edge of the Tibetan Plateau in Northern Pakistan dated at 2-0.5 million years ago (Zhimin et al., 1982; Senshui, 1981; Dennell et al., 1988). Robust dates for Paleolithic sites on the Tibetan Pla- teau are not available, although comparison of tool types with those found in China and elsewhere in Asia yielded estimates of 50,000 years of human habitation on the Ti- betan Plateau (Senshui, 1981). Nonetheless, we cannot be assured that the present in- habitants of the region are the genetic de- scendents of these ancient populations. The Tibetan Plateau is geographically remote and historically isolated but no information is available with which to estimate the ex- tent or sources of genetic admixture.
While Tibetans live at higher and lower altitudes than those of the present report, we were limited by considerations of popula- tion size and health care facilities. We chose
TIBETAN BIRTH WEIGHT 221
Lhasa and Kathmandu since they have the greatest Tibetan population concentration and best health care facilities in their re- spective regions. Our high-altitude subjects identified themselves and their ancestors as Tibetan and were born and raised in Lhasa or at a similar elevation. We could not ques- tion our low-altitude subjects regarding their ancestry or altitude of origin. Because the hospital is adjacent to a large commu- nity of Tibetan immigrants and because subjects identified themselves and their husbands as Tibetan (rather than as one of the other Buddhist minorities of Nepal) they were most likely migrants from Tibet. While documentation of the genetic history of the Lhasa and Kathmandu Tibetan populations awaits study, the age of the Kathmandu women and the lack of immigration from Ti- bet to Nepal in recent years (Goldstein, 1991) makes it likely that a majority of our study subjects either were born and raised in Nepal to parents that had been born and raised in Tibet, or had immigrated to Nepal as children. We may speculate that a major- ity of Tibetan immigrants came from the Lhasa area, which was and still is the larg- est population center in Tibet (Sharma, 1983).
All the women in the study were judged healthy on the basis of clinical exam, prior medical history, and absence of recognized complications during pregnancy. That the women at the two altitudes were likely to be equally healthy was supported by a similar number of prenatal visits in the two sam- ples, similar body weight near term, and an absence of cigarette smoking in the Lhasa women and in all likelihood, since cigarette smoking among Tibetan women in Nepal is rare, in the Kathmandu women as well (Norkyel, personal communication). The Lhasa residents had a normal nonpregnant weight for height (Statistical Bulletin, 1983) and estimated percent body fat (Durnin and Womersly, 1974) by Western standards. Their absolute weight increase during preg- nancy was at the low end of the recom- mended range (National Research Council, 1981), but their 18% relative weight gain was within the 16-25% proportional weight gain associated with the most favorable ma- ternal and neonatal outcome (Shepard et al.,
1986). While Tibetans in Nepal have emi- grated from Tibet, they are not a “refugee” population in the sense of being recently ar- rived and in poor health. In fact, Tibetans living in Kathmandu may be advantaged relative to the Lhasa Tibetans with respect to the greater abundance and variety of foods available, a higher standard of living, and better quality of health care.
Concerning the determination of birth weight, all the infants were weighed a t birth by hospital personnel using calibrated, beam-balance or spring-counterforce me- chanical newborn scales. We transported the mechanical scales to Lhasa, calibrated them on site, and trained personnel in their use in order to obtain the birth weights re- ported here. The determination of birth weight was overseen by one of us in approxi- mately half the Lhasa deliveries and the val- ues obtained were confirmed. In support of the accuracy of the birth weights obtained, values correlated closely with gestational age at both locations and the late third tri- mester weekly weight gain observed was in- distinguishable from the 132-176 glweek re- ported for Western populations (Gruenwald, 1975; Lockwood and Weiner, 1986). Fur- thermore, the low altitude sample demon- strated the expected relationship between parity, infant sex and birth weight (Karn and Penrose 1951; Lockwood and Weiner 1986). Infant birth weight increases with each successive pregnancy (Karn and Pen- rose, 1951). The absence of a relationship between birth weight and parity at high alti- tude is likely to be an artifact of the uni- formly low parity of the Lhasa women. Whereas the number of prior births in the 34 multiparous women at low altitude aver- aged 4 and ranged from 1 to 12, only one of the 14 multiparous women athigh altitude had borne more than one child. Haas et al. (1980) reported that male and female birth weights are similar at high altitude as the result of a greater depressant effect of alti- tude upon male than female values.
Gestational age was calculated from the mother’s last menstrual period. Clinical es- timates of gestational age were available for nearly half the high-altitude infants and did not differ from gestational age calculated from maternal dates. Similar comparisons
222 S. ZAMUDIO ET AL.
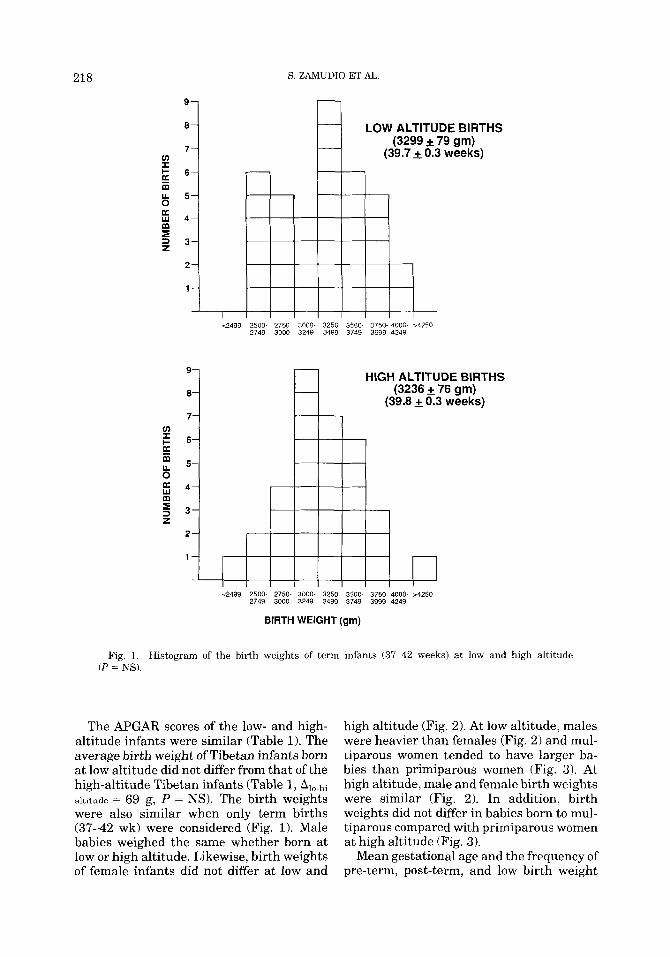
U.S.A. Hi-Lo Peru Hi-Lo Bolivia Hi-Lo Tibet Hi-Lo A = 270 gm A =282gm A =72gm
3000
v &
$
F I (3 2000
I F E m 1000
n
* P = N S
< 500 m 2750-3100 m 600 rn 3860 m 400m 3600m 1200 m 3658 m
Yip, 1987 Beall 1981 Haas et a/. 1980 This report
ALTITUDE COMPARISONS
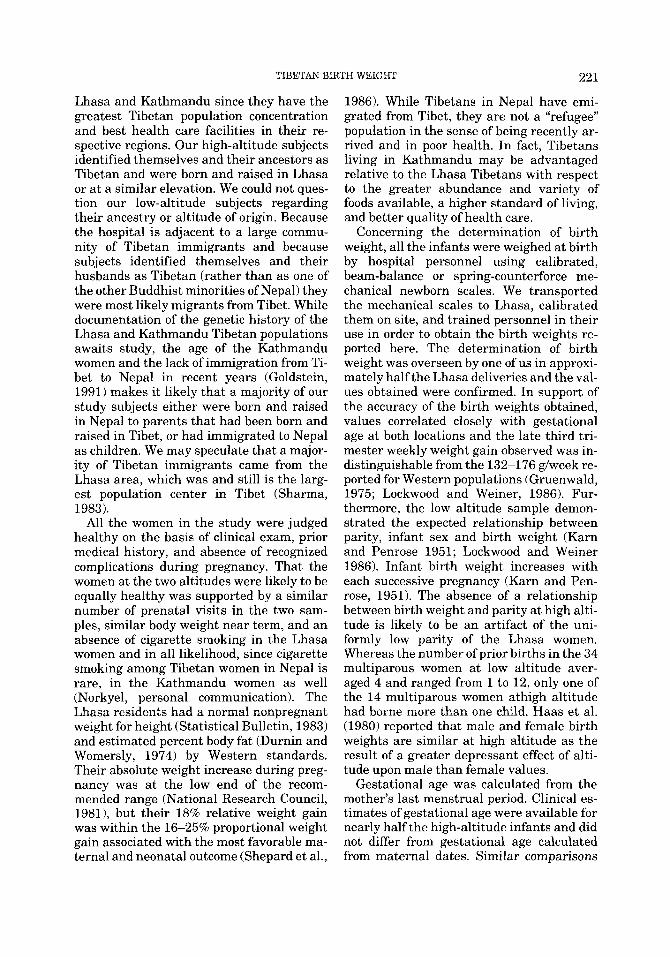
Fig. 5. Differences in birth weight between low- and high-altitude populations are greater in North Americans, intermediate in South Americans, and smaller in Tibetans. The differences in birth weight are significant (*P < .01) among North and South Americans but not among Tibetans.
were not available for the low-altitude sam- ple. Underestimation of gestational age in our low altitude sample by 10 days or more would be required to obtain a birth weight difference as great as those reported for the low- compared with the high-altitude sam- ples of the South American studies pre- sented in Figure 5. An error of this magni- tude seems unlikely. To examine the effect of overestimation of gestational age, we con- sidered that 5 of the 6 low-altitude infants in the 2,500-2,749 g birth weight range (Fig. 1) could have been premature and repeated statistical comparisons. The relationship be- tween birth weight and gestational age did not change, nor did the similarity between the low- and high-altitude slopes for birth weight vs. gestational age. Elimination of these 5 infants increased the adjusted birth weight difference between the low- and high-altitude samples, but the difference was still not significant (Alo-hi altitude = 103 g, P = NS).
We concluded that birth weights are simi- lar a t the two elevations and that the simi- larity observed is not likely to be due to con-
founding variables acting to raise birth weight a t high altitude and/or reduce birth weight a t low altitude.
To address whether birth weight is sub- ject to genetic selection, we examined the evidence within and between populations for genetic involvement in the determina- tion of birth weight. In the general popula- tion, nongenetic maternal and environmen- tal factors account for more than half the variability in birth weight (reviewed in Bo- gin, 1988; Vlietnick et al., 1989). Heritabil- ity estimates for birth weight vary consider- ably, but in studies of monozygous twins (who not only share 100% of their genes, but also similar environmental and socioeco- nomic characteristics) upwards of 70% of the variability in birth weight can be ascribed to genetic factors (Nance, 1976; Magnus, 1984; Vlietnick et al., 1989). These data are not intended to minimize the importance of en- vironmental factors, rather they emphasize that the genetic contribution to birth weight is of sufficient magnitude to warrant consid- eration of natural selection in relation to birth weight. Between-population studies
TIBETAN BIRTH WEIGHT 223
have also revealed differences which have been ascribed to the operation of genetic in- fluences on birth weight. For instance, birth weights of babies born to Chinese women have been shown to be 200 g below values in the general United States white population regardless of whether the Chinese women lived in mainland China, Taiwan, or the United States (Yip et al., 1991). Further- more, infants born to one Chinese and one white parent were intermediate between the values observed in the Chinese and general United States white populations. It has also been reported that Amerindian women have larger babies than European women regard- less of altitude and despite smaller body size (Haas et al., 1980).
Birth weight has long been regarded as the classic example of stabilizing selection insofar as infants with birth weights above or below a normal range are subjected to increased mortality. The intensity of selec- tion against low birth weight varies with the cause of reduced size a t birth (Haas et al., 1987). Nonetheless, the selective pressure against low birth weight infants is greater than that against high birth weight infants; reductions in birth weight are associated with an exponential increase in mortality risk whereas the mortality risk experienced by high birth weight infants increases lin- early (Williams et al., 1982). Growth-re- tarded infants have higher mortality rates than normal birth weight infants regardless of whether the babies are born at low or high altitude (Haas et al., 1987; Unger et al., 1988). The intensity of selection against low birth weight infants can be assessed by the difference between the optimal birth weight, defined as that which is associated with the lowest mortality risk, and the mean birth weight observed. At low altitude, optimal birth weight is usually higher than the ac- tual mean birth value, with differences av- eraging 150-200 g (Karn and Penrose, 1951; Williams et al., 1982). At 3,860 m, the differ- ence between the optimal and mean birth weight was 322 g, while in a similar popula- tion at 600 m, the difference was 222 g (Beall, 19811, suggesting that low-altitude populations are closer than high-altitude populations to their optimal birth weight.
We compared the birth weights of the present study with those obtained previ-
ously by the same investigators at low and high altitudes in North and South America (Fig. 5). The altitude-associated differences of 352 and 270-282 g observed in the United States and South America, respectively, are statistically significant whereas the 72 g dif- ference observed in the present report is not significant. Whether the raw birth weight data were considered or were adjusted for variation in gestational age and ethnicity, or birth weights were considered in relation to the altitude differences observed, the effect of altitude appeared greatest in North America, intermediate in South America, and smallest in Tibetans. No demonstrable reduction in birth weight occurs at altitudes below 1,500 m, thus the somewhat lesser magnitude of altitude difference in the Ti- betan sample is not a likely contributor to the smaller birth weight difference (Yip, 1987). Available archaeological evidence supports the possibility that Tibetans have resided longer a t high altitude than North or South American populations (Zhimin et al., 1981; Senshui, 1981; Nunez, 1983; Mac- Neish and Berger, 1970; Lynch, 1978). It is unknown whether European admixture in South American Andean populations has contributed to the birth weight reductions reported in studies comparing low- and high-altitude populations. Nonetheless, the magnitude of the birth weight differences appears to be inversely related to the duration of high-altitude residence sug- gesting that time-dependent selection for normal birth weight has occurred at high altitude.
Because of the small, selected samples used in this report, these data must be inter- preted cautiously. Needed are larger sam- ples of births from across an altitude gradi- ent within Tibet. The similarity in birth weights observed in infants born to Tibetan mothers residing at low and high altitudes supports our hypothesis that Tibetans are protected from altitude-associated growth retardation. This similarity contrasts with the birth weight differences previously re- ported for North and South America. We postulate that for Tibetans, long history of high-altitude residence has permitted natu- ral selection for factors which increase fetal oxygen availability and permit normal fetal growth. Further work is required to define
224 S. ZAMUDIO ET AL.
the physiological and genetic mechanisms involved.
ACKNOWLEDGMENTS The authors gratefully acknowledge the
assistance of Dr. Drolkar, Dr. Tshering Drolkar, Dr. Robin Houston, Mr. Michael Keller, Dr. Li, Dr. Sylvia Schulz and the staff of the Patan Hospital, Dr. Shamina, Mr. Karma Tashi, Dr. Thubten, Dr. Yang Ping and Dr. Zhu. Support for this work was provided by NSF BNS 8903554, NSF BNS 8919645, NIH HL07171, NIH CHD 000681, and NIH HLBI 14985.
LITERATURE CITED Ballard JL et al. (1977) A simplified assessment of ges-
tational age. Pediatric Res. 11:374-377. Beall CM f 1981) Optimal birthweights in Peruvian pop-
ulations at high and low altitudes. Am. J. Phys. An- thropol. 56r209-216.
Bogin B. (1988) Patterns of Human Growth. Cambridge: Cambridge University Press, p 21.
Dennell RW, Rendell HM, and Hailwood E (1988) Late Pliocene artifacts from Northern Pakistan. Curr. An- thropol. 29:495-498.
Durnin JVGA, and Womersley J (1974) Body fat as- sessed from total body density and its estimation from skinfold thickness: Measurements on 481 men and women aged from 16-72 years. Br. J. Nutr. 32:77-97.
Goldstein MC (1991) The Dragon and the Snow Lion: The Tibet question in the 20th century. Unpublished manuscript.
Gruenwald P (1975) The supply line of the fetus; defini- tions relating to fetal growth. In P Gruenwald fed.): The Placenta and its Maternal Supply Line.: Univer- sity Park Press, Baltimore, Md., pp. 1-17.
Haas JD, Frongillo EA Jr. , Stepcik CD, Beard JL, and Hurtado LG (1980) Altitude, ethnic and sex difference in birth weight and length in Bolivia. Hum. Biol. 52t459-477.
Haas JD, Balcazar H, and Caulfield L (1987) Variation in early neonatal mortality for different types of fetal growth retardation. Am. J. Phys. Anthropol. 73:467- 473.
Karn MN, and Penrose LS (1951) Birth weight and ges- tation time in relation to maternal age, parity and infant survival. Eugenics 16:147-164.
Lichty JA, Ting RY, Bruns PD, and Dyar E 11957) Stud- ies of babies born a t high altitude. Am. J . Dis. Child. 93366-678.
Lockwood CJ, and Weiner S (1986) Assessment of fetal growth. Clin Perinatol13t3-11.
Lynch TF (1978) The paleo-indians. In JD Jennings (ed.): Ancient South Americans.: W.H. Freeman and Co., San Francisco, pp. 87-137.
MacNeish RS, and Berger RP (1970) Megafauna and man from Ayacucho, Highland Peru. Science 166: 975-977.
Magnus P (1984) Causes of variation in birth weight: A study of offspring of twins. Clin. Genet. 25:15-24.
McCullough RE, Reeves JT, and Liljegren RL (1977) Fetal growth retardation and increased infant mortal- ity a t high altitude. Arch. Env. Health 32t36-39.
Moore LG (1990) Maternal 0, transport and fetal growth in Colorado, Peru, and Tibet high-altitude res- idents. Am. J . Hum. Biol. 2:627-637.
Moore LG, and Regensteiner JG (1983) Adaptation to high altitude. Ann. Rev. Anthropol. 12:285-304.
Nance WE (1976) Genetic studies of the offspring of identical twins. Acta Genet. Med. Gemellol. 25tlOZL113.
National Research Council (1981) Nutritional Services in Perinatal Care. Washington D.C.: National Acad- emy Press.
Nunez L (1983) Paleoindian and archaic cultural peri- ods in the arid and semiarid regions of Northern Chile. Adv. World Archaeol. 2r161-203.
Senshui Z (1981) Uncovering prehistoric Tibet. China Reconstruc. January:64-65.
Sharma JC (1983) Dental morphology and odontometry of the Tibetan immigrants. Am. J. Phys. Anthropol.
Shepard MJ, Hellenbrand KG, and Bracken MB (1986) Proportional weight gain and complications of preg- nancy, labor, and delivery in healthy women of nor- mal prepregnant stature. Am. J . Obstet. Gynecol. 155t947-954.
Statistical Bulletin (1983) Metropolitan Height and Weight Tables. JanJuner3-9.
Unger C, Weiser JK, McCullough RE, Keefer S, and Moore LG (1988) Altitude, low birth weight, and in- fant mortality in Colorado. JAMA 259:3427-3432.
Vlietnick R, Derom R, Neale MC, Maes H, van Loon H, Derom C, and Thiery M (1989) Genetic and environ- mental variation in the birth weight of twins. Behav- ior Genetics 19:151-161.
Williams RL, Creasy RK, Cunningham GC, Hawes WE, Norris FD, and Tashiro M (1982) Fetal growth and perinatal viability in California. Obstet. Gynecol. 59:624-632.
Yip R (1987) Altitude and birth weight. J. Pediatr. 111:869-876.
Yip R, Li Z, and Chong WH (1991) Race and birth weight: The Chinese example. Pediatrics 87:68%93.
Zhimin A et al. (1982) Paleoliths and microliths from Sheja and Shuanghu, Northern Tibet. Curr. Anthro- pol. 23t493-499.
61,495-505.
Copyright © 2022 FDOKUMEN