The importance of venous Doppler velocimetry for evaluation of intrauterine growth restriction
17
The Importance of Venous Doppler Velocimetry for Evaluation of Intrauterine Growth Restriction he aim of fetal and maternal surveillance in the case of fetal growth restriction may be summarized as the need to opti- mize the timing of delivery before death of the fetus in the uterus or before it undergoes permanent damage. Fetuses with in- trauterine growth restriction (IUGR) are usually delivered on the basis of abnormal results from a nonstress test such as fetal heart rate monitoring, a biophysical profile, or the presence of maternal distress. During the last 25 years, Doppler velocimetry has become a routine part of fetal surveillance in complicated pregnancies. Circulatory adaptation of the human fetus in the presence of utero- placental insufficiency in IUGR fetuses leads to preferential perfu- sion of vital organs such as the brain, heart, 1 adrenal glands, 2 and spleen. 3,4 Changes in flow velocity waveforms are observed in various fetal vascular beds, and Doppler surveillance is based on the rela- tionship between circulatory changes and the fetal condition. 5 In obstetrics, Doppler sonography has largely been used to examine the arterial system. There is a vast amount of literature on umbilical artery and fetal arterial blood flow. Elevated impedance to blood flow in the placenta is reflected by abnormal umbilical artery ve- locimetric findings (early-stage Doppler abnormalities and an ele- vated pulsatility index). 6 In such situations, growth restriction due to placental insufficiency occurs, and there may also be a change in the fetal cerebral waveforms that suggests increased blood flow to the brain (brain-sparing effect). Apostolos Kaponis, MD, PhD, Takashi Harada, MD, George Makrydimas, MD, Tomoiki Kiyama, MD, Kazuya Arata, MD, George Adonakis, MD, Vasilis Tsapanos, MD, Tomio Iwabe, MD, Theodoros Stefos, MD, George Decavalas, MD, Tasuku Harada, MD, PhD, DMSci Received November 12, 2010, from the Depart- ment of Obstetrics and Gynecology, Patra Uni- versity School of Medicine, Patra, Greece (A.K., G.A., V.T., G.D.); Department of Obstetrics and Gynecology, Tottori University Faculty of Medi- cine, Yonago, Japan (A.K., Tak.H., T.K., K.A., T.I., Tas.H.); and Department of Obstetrics and Gy- necology, Ioannina University School of Medicine, Ioannina, Greece (G.M., T.S.). Revision requested December 4, 2010. Revised manuscript accepted for publication December 9, 2010. Address correspondence to Apostolos Kapo- nis, MD, PhD, Department of Obstetrics and Gy- necology, Tottori University Faculty of Medicine, 36-1 Nishimachi, Yonago 683-8504, Japan. E-mail: [email protected] Abbreviations IUGR, intrauterine growth restriction T ©2011 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2011; 30:529–545 | 0278-4297/11/$3.50 | www.aium.org REVIEW ARTICLE The management of growth-restricted fetuses requires accurate diagnosis to optimize the timing of delivery. Doppler velocimetry is the only noninvasive method for assess- ing the fetoplacental hemodynamic status. This review will give a critical overview of the current knowledge on fetal venous blood flow in pregnancies complicated by in- trauterine growth-restricted fetuses. Adaptation of the circulation in intrauterine growth- restricted fetuses is described. Normal and abnormal venous Doppler waveforms are presented. Correlations of abnormal waveforms with the presence of acidemia and peri- natal outcomes are emphasized. Limitations of venous Doppler velocimetry for opti- mizing the time for delivery and the perinatal outcome are also presented. Key Words—ductus venosus; fetal venous system; intrauterine growth restriction; peri- natal outcome; venous Doppler velocimetry
Transcript of The importance of venous Doppler velocimetry for evaluation of intrauterine growth restriction

The Importance of Venous Doppler Velocimetry for Evaluation of IntrauterineGrowth Restriction
he aim of fetal and maternal surveillance in the case of fetalgrowth restriction may be summarized as the need to opti-mize the timing of delivery before death of the fetus in the
uterus or before it undergoes permanent damage. Fetuses with in-trauterine growth restriction (IUGR) are usually delivered on thebasis of abnormal results from a nonstress test such as fetal heartrate monitoring, a biophysical profile, or the presence of maternaldistress. During the last 25 years, Doppler velocimetry has becomea routine part of fetal surveillance in complicated pregnancies. Circulatory adaptation of the human fetus in the presence of utero-placental insufficiency in IUGR fetuses leads to preferential perfu-sion of vital organs such as the brain, heart,1 adrenal glands,2 andspleen.3,4
Changes in flow velocity waveforms are observed in variousfetal vascular beds, and Doppler surveillance is based on the rela-tionship between circulatory changes and the fetal condition.5In obstetrics, Doppler sonography has largely been used to examinethe arterial system. There is a vast amount of literature on umbilicalartery and fetal arterial blood flow. Elevated impedance to bloodflow in the placenta is reflected by abnormal umbilical artery ve-locimetric findings (early-stage Doppler abnormalities and an ele-vated pulsatility index).6 In such situations, growth restriction dueto placental insufficiency occurs, and there may also be a change inthe fetal cerebral waveforms that suggests increased blood flow tothe brain (brain-sparing effect).
Apostolos Kaponis, MD, PhD, Takashi Harada, MD, George Makrydimas, MD, Tomoiki Kiyama, MD,Kazuya Arata, MD, George Adonakis, MD, Vasilis Tsapanos, MD, Tomio Iwabe, MD, Theodoros Stefos, MD,George Decavalas, MD, Tasuku Harada, MD, PhD, DMSci
Received November 12, 2010, from the Depart-ment of Obstetrics and Gynecology, Patra Uni-versity School of Medicine, Patra, Greece (A.K.,G.A., V.T., G.D.); Department of Obstetrics andGynecology, Tottori University Faculty of Medi-cine, Yonago, Japan (A.K., Tak.H., T.K., K.A., T.I.,Tas.H.); and Department of Obstetrics and Gy-necology, Ioannina University School of Medicine,Ioannina, Greece (G.M., T.S.). Revision requestedDecember 4, 2010. Revised manuscript acceptedfor publication December 9, 2010.
Address correspondence to Apostolos Kapo-nis, MD, PhD, Department of Obstetrics and Gy-necology, Tottori University Faculty of Medicine,36-1 Nishimachi, Yonago 683-8504, Japan.
E-mail: [email protected]
AbbreviationsIUGR, intrauterine growth restriction
T
©2011 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2011; 30:529–545 | 0278-4297/11/$3.50 | www.aium.org
REVIEW ARTICLE
The management of growth-restricted fetuses requires accurate diagnosis to optimizethe timing of delivery. Doppler velocimetry is the only noninvasive method for assess-ing the fetoplacental hemodynamic status. This review will give a critical overview ofthe current knowledge on fetal venous blood flow in pregnancies complicated by in-trauterine growth-restricted fetuses. Adaptation of the circulation in intrauterine growth-restricted fetuses is described. Normal and abnormal venous Doppler waveforms arepresented. Correlations of abnormal waveforms with the presence of acidemia and peri-natal outcomes are emphasized. Limitations of venous Doppler velocimetry for opti-mizing the time for delivery and the perinatal outcome are also presented.
Key Words—ductus venosus; fetal venous system; intrauterine growth restriction; peri-natal outcome; venous Doppler velocimetry
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 529

Fetal middle cerebral artery velocimetry has been sug-gested as a predictor of fetal hypoxemia when a character-istic increase in diastolic blood velocities was present as asign of fetal brain-sparing.7 However, abnormal early um-bilical artery abnormalities and middle cerebral arterysignals do not necessarily predict the outcome in growth-restricted fetuses. In addition, examination of middle cere-bral artery velocimetry in complicated pregnancies hasindicated that the brain-sparing effect is an early sign offetal hypoxemia in fetuses who still have adequate reversesto cope with the stress of labor and vaginal delivery8 andtherefore is of limited value for the prediction of the fetaloutcome and the optimal time for delivery.9,10
More recently, research on the fetomaternal circula-tion has focused on the venous side of the fetal circulation.The first clinical venous flow measurements in the fetalumbilical vein and the right branch of the portal vein wereperformed by Gill11 and these preliminary measurementswere published in 1979. Laurin et al12 stated that the diag-nostic accuracy of umbilical venous flow assessment wasbetter than that of umbilical artery Doppler evaluation foridentifying fetuses at increased risk of adverse neonatal out-comes. In addition, because absent end-diastolic or re-versed flow in the ductus venosus and pulsation in theumbilical vein are less frequent findings in IUGR fetusesthan abnormal arterial Doppler waveforms that are asso-ciated with a high risk of perinatal death,13 it seems that thepresence of alterations of the venous system could consti-tute a sufficient and adequate reason to optimize the tim-ing of delivery. This review will give a critical overview ofthe current knowledge on fetal venous blood flow in preg-nancies complicated by IUGR fetuses.
Physiologic Characteristics of the Fetal Venous Circulation
Blood flow coming from the placenta returns to the heartvia the umbilical vein, ductus venosus, and inferior venacava. The umbilical vein conveys oxygenated blood fromthe placenta to the liver. The liver is the first fetal organ toreceive well-oxygenated blood from the placenta, whichalso is richest in amino acids and glucose.14 The umbilicalvein joins the left portal vein, perfusing the left liver lobeand giving rise to the ductus venosus, a trumpet-shapedvein, which bypasses the liver and shunts blood to the fetalheart. In physiologic human pregnancies, the umbilicalvein first supplies the left liver lobe and then the ductusvenosus (20%–30%).15,16 The ductus venosus plays amajor role in regulating the circulation of oxygenatedblood from the placenta. The other 70% to 80% of blood
flows through the liver, mainly into the right heart and viathe ductus arteriosus and the descending aorta back to theplacenta.
At the median fissure of the liver, the umbilical veinjoins the right branch of the portal vein. At this point, themain portal vein joins the right branch of the portal vein,which carries deoxygenated blood from the spleen andfetal gut, thus supplying the right liver lobe.17 The 3 (left,middle, and right) hepatic veins reach the inferior venacava just below the diaphragm in the same funnel-likestructure as the ductus venosus.18
Animal experiments have shown that there is a stream-lining of blood flow within the thoracic inferior vena cava.19
Blood from the distal inferior vena cava and the right lobeof the liver together with blood from the superior vena cavais directed toward the right atrium and through the tricus-pid valve into the right ventricle and to the pulmonary ar-tery. Most of it is shunted through the ductus arteriosusinto the descending aorta. Blood from the ductus venosusand the left hepatic vein is directed toward the foramenovale, thereby delivering well-oxygenated blood to the leftheart and via the ascending aorta to the myocardium andbrain.19,20
Adaptation of the Fetal Circulation in IUGR
Restriction of placentation leads to impaired fetal growthin sheep.21 In human fetuses, IUGR and a compromisedplacenta are usually linked with abnormal Doppler vari-ables. One of these parameters is the proportion of fetal car-diac output distributed to the placenta. Human fetusesnormally direct one-third of their cardiac output to the pla-centa during the second half of pregnancy and one-fifth dur-ing the last couple of months.22 In contrast, IUGR fetuseswith early umbilical artery abnormalities direct a reducedvolume of blood toward the placenta, both in absolute andrelative terms, while maintaining relatively normal cardiacoutput.22 This reduction was found by another group in ear-lier pregnancies (20th–24th gestational weeks) in humanIUGR fetuses before the development of early umbilical artery abnormalities.23 Low cardiac output to the placentamay already be present at a stage of the disease that pre-cedes the appearance of clinical evidence of a reduction infetal growth and changes in impedance to flow in the fetalarterial and venous circulation.23 This condition may sug-gest that, at an early stage of placental compromise, the vol-ume of fetal blood flow toward the placenta is reduced, andmore extensive recirculation of umbilical blood in the fetalbody develops in an attempt to achieve more efficient ex-traction of oxygen and nutrients.22–24
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545530
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 530

Animal studies using invasive techniques and nonin-vasive studies using Doppler sonography in the humanfetus have shown that intrauterine hypoxemia is associatedwith redistribution of cardiac output in favor of the leftventricle, providing preferential perfusion of the brain,myocardium, and other vital organs (brain- and heart-sparing effects).25,26 This condition results in a doublingof umbilical vein–derived oxygen delivery to the myo -cardium and increased delivery to the fetal brain. Accord-ing to an animal study, hypoxemia alone has little if anyrole in influencing liver and ductus venosus blood flow inthe fetal lamb.27 However, the conclusion of most ani-mal studies is that the combination of severe hypoxemiawith acidemia causes redistribution of umbilical veinblood toward the ductus venosus at the expense of he-patic blood flow.20,27,28 Because fetal proteins are pre-dominantly synthesized in the liver, it is suggested thatthe low fetal body weight of IUGR fetuses is partiallycaused by impairment of protein biosynthesis after re-duction of fetal liver blood flow.29 By blocking the duc-tus venosus blood flow in fetal sheep near term, the samegroup of authors showed that the hepatic blood flow wasincreased and the cell proliferation rate was also increasedsubstantially (2-fold) in heart muscle, skeletal muscle, andkidneys and 6-fold in the liver. It was concluded that in-creases in hepatic blood flow stimulate cell proliferation inmajor organs of the ovine fetus.30
The ductus venosus is 1 of the 3 physiologic shuntsresponsible for circulatory adaptation to intrauterine life.Well-oxygenated blood is directed from the umbilical veinthrough the ductus venosus into the left atrium throughthe foramen ovale, without mixing with poorly oxygenatedblood. Experimental animal data suggested that the volume of blood shunted through the ductus venosus in-creased during hypovolemia and hypoxia and couldreach as much as 70% of the umbilical blood flow.19,28
In human fetuses, Bellotti et al31 estimated that the meanblood flow through the ductus venosus increased substan-tially (>70%) with high dilatation of the vessel comparedwith steady conditions, the end result of which was redis-tribution of cardiac output. Nowadays, ductus venosusflow is the strongest Doppler predictor of perinatal mor-tality in preterm IUGR fetuses.32,33
This shunt is responsible for maintaining a well- oxygenated supply to essential organs such as the brain,heart, and adrenal glands, and liver perfusion is reduced to30%, as shown in animal studies and in the humanfetus.19,34 This diversion of oxygenated blood and re-duced flow to less important organs such as muscles,bowel, and kidneys enables the fetus to survive for a con-
siderable period. If the oxygen supply to the myocardiumreaches its limit, the myocardium stiffens, and the centralvenous pressure increases.35
Adaptation of the fetal circulation to hypoxemia ischaracterized by decreased cerebral impedance to flowwith increased impedance to flow in the peripheral vesselsof the lower body. The former reduces the left ventricularafterload, whereas the latter increases the right ventricularafterload. Persistent uteroplacental insufficiency is associ-ated with a progressive fall of combined cardiac output, in-dicating decreasing cardiac function.36 Because the rightventricle has an increased afterload, there is an increase inthe diameter at the atrioventricular ring of the right fetalheart. This finding coexists with absent or reversed dias-tolic flow in the umbilical artery (late abnormalities),37 in-dicating that there is right ventricular dysfunction withhigh umbilical artery resistance. Right atrioventricular ringdilatation causes tricuspid regurgitation, increasing theend-diastolic volume of the right atrium. The latter is re-sponsible for increased reversed flow in the inferior venacava during atrial systole.38
Successive distal progression of flow patterns in thevenous beds presumably reflects progressive stages of my-ocardial dysfunction. Hypoxemic impairment of ventricu-lar function contributes to the high end-diastolic pressurein the right ventricle and right atrium and subsequently tohigh central venous pressure.4 Elevated right ventricularend-diastolic pressure, which is transmitted to the rightatrium, increases right atrial pressure and impairs the for-ward flow of blood during atrial systole. Reversal of bloodflow during atrial systole initially observed in the inferiorvena cava, if transmitted through the ductus venosus,eventually results in end-diastolic pulsation in the left por-tal vein and umbilical vein.4,39–41 Pulsation in the umbili-cal vein associated with late umbilical artery abnormalities(absent or reversed diastolic flow) is considered a sign ofimminent fetal asphyxia accompanied by acidemia, hy-poxemia, and an adverse perinatal outcome.4,42,43 More-over, decreased antegrade flow in the ductus venosus isassociated with considerable worsening of the hypoxemiaand axidemia,4,42,43 resulting in impaired delivery of well-oxygenated blood to the already compromised my-ocardium. This condition could provide a potent stimulusfor coronary vasodilatation to enhance myocardial bloodflow (heart-sparing effect).44,45
Visualization of coronary blood flow in IUGR fetusesconsistently coincides with deterioration of venous flow,45
increasing impedance to the middle cerebral artery re-sulting in a high left ventricular afterload,46 and atrioven-tricular valve insufficiencies with relatively low-velocity
J Ultrasound Med 2011; 30:529–545 531
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 531

regurgitant jets.45,47 Normalization of cerebral flow indicescorrelates with cerebral edema. It can be inferred from pre-vious studies that such a progression coincides with thedevelopment of abnormal venous flow.4,34,47 This incre-mental progression strongly supports the use of multives-sel Doppler surveillance in the assessment of severelyIUGR fetuses.46,48 We suggest that a normal middle cere-bral artery pulsatility index correlated with late umbilicalartery Doppler abnormalities (absent or reversed end- diastolic flow) should preferably be interpreted by lookingat the venous system because abnormal flow velocity wave-forms there are strongly suggestive of a centralized circu-lation that has deteriorated. Cardiovascular collapse is themain cause of intrauterine death in IUGR fetuses.
Normal Doppler Findings in the Fetal Venous System
The first studies on the fetal venous system by Dopplersonography were concerned with the quantitative flow ofblood in the umbilical vein. The umbilical vein became afocus of Doppler investigations as early as the 1980s.49,50
These pioneering studies combined pulsed Dopplersonography with conventional B-mode probes at a fixedangle, which enabled quantitative evaluation of volumeblood flow in the intra-abdominal part of the umbilicalvein. These studied reported an average volume blood flowequal to 110 to 120 mL/kg/min in uncomplicated third-trimester pregnancies.
Generally, flow volume measurements and absolutevelocity measurements have considerably higher inaccu-racies and intrapatient variations compared with velocityratios.20,49 Quantitative flow studies have been neglectedbecause of this relative inaccuracy due to dependence onthe sampling site, fetal breathing activity, angle of in-sonation, vessel diameter, and gestational age.
Hecher et al51 established reference ranges with ges-tation for blood flow velocities and indices of pulsatility forflow in the fetal venous system. Two indices that were in-dependent of the angle of insonation were calculated: thepeak velocity index for veins and pulsatility index for veins.Blood velocities increased, whereas the peak velocity pul-satility indices for veins decreased with advancing gesta-tion.51 Because of the above-mentioned limitations forevaluation of quantitative parameters in the fetal venoussystem, qualitative waveform analyses are used extensivelyfor monitoring the fetal condition.
The physiologic umbilical vein Doppler patterns showlinear forward flow (Figures 1A and 2A). During early ges-tation, pulsations were always seen in the umbilical vein
until the eighth gestational week and they progressivelydisappeared between 9 and 12 weeks.52 Other investiga-tors found umbilical vein pulsations synchronous with thefetal heart rate in healthy fetuses between 34 and 38weeks.53 They were present in 20% of measurements in afree-floating loop of the cord, in 33% of intra-abdominalumbilical vein measurements, and in 78% of waveformsfrom the umbilical sinus and left portal vein,53 suggestingthat the sampling site is also of crucial importance in ve-nous Doppler studies. It is of paramount importance to dis-tinguish these pulsations from pulsations occurring in casesof severe fetal compromise and nonimmune hydrops.
The ductus venosus flow velocity waveform displayscontinuous forward flow throughout the cardiac cycle,consisting of 2 surges of velocity peaks, the first corre-sponding to ventricular systole (S wave) and the secondto ventricular diastole (D wave). These are followed by areduction in velocity during atrial systole (A wave; Figures1B and 2C).54 Kiserud et al55 reported that velocities at theinlet of the ductus venosus immediately above the umbil-ical vein are higher than at the outlet into the inferior venacava and suggested standardizing the sampling site at theinlet.
The flow velocity waveform of the inferior vena cavadisplays a biphasic flow profile with 2 peaks during ven-tricular systole and diastole and retrograde flow duringatrial contraction (Figure 1C).54 The reversed flow maybe absent in 10% to 36% of healthy fetuses if the measure-ments are performed in the distal portion of the inferiorvena cava.56 Recordings in the inferior vena cava at the en-trance to the right atrium have a large SD for various wave-form parameters56; therefore, the sample volume shouldbe placed in the fetal abdomen between the entrance of therenal vein and the ductus venosus (Figure 3).57
Improvements in Doppler technology have allowedinvestigation of hepatic vein35 (similar to the inferior venacava waveform with higher pulsatility and a characteristicreversed A wave), portal vein (continuous forward flow),pulmonary vein58,59 (similar to the ductus venosus wave-form), and internal jugular vein60 flow velocity waveforms.The internal jugular vein blood flow pattern consists of 2forward venous waves during ventricular systole and earlydiastole and 1 backward venous wave during late diastolewith atrial contraction.60 During early gestation, the sys-tolic and diastolic waves are almost equal, and the reversedwave is present, whereas during late gestation, the systolicwave is higher than the diastolic wave, and there is no re-versed wave.60 Finally, the cerebral venous system has recently become a subject of investigation. In healthy fe-tuses, the vein of Galen and straight sinus do not have the
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545532
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 532
characteristics pulsations observed in the systemic venouscirculation.61 In contrast, the transverse sinus waveform istriphasic, consisting of a rise in velocities with systolic flowduring ventricular systole and early diastolic flow due topassive ventricular filling, with the lowest velocities corre-sponding to atrial contraction.61
Venous Doppler Measurements in Growth-Restricted Fetuses
Intrauterine growth restriction is mainly attributed to pla-cental insufficiency, and many growth-restricted fetusesmay be hypoxemic and acidemic. The fetal hemodynamicadaptation to hypoxia can be summarized as a decrease incardiac output and the heart rate, an increase in arterialpressure and the associated afterload, and major redistri-bution of the blood flow by selective peripheral vasocon-striction.54 Doppler velocimetry, therefore, could be usedin clinical assessment of fetal responses to intrauterine hy-poxemia. Doppler sonography in IUGR fetuses describesdownstream vascular resistance (umbilical artery), pref-erential organ blood flow (middle cerebral artery), andthe filling capacity of the fetal heart (precordial veins).Worsening arterial Doppler results do parallel a worseningfetal status, but only the addition of venous Doppler ve-locimetry has allowed a comprehensive understanding ofcardiovascular deterioration.62,63
With accumulating data and experience, it has be-come evident that fetal venous Doppler velocimetry couldbe a useful tool for the determination of fetal well-being.Blood velocity waveforms in the central veins normallypulsate in response to central venous pressure.64 Hecheret al4 showed that there were no significant differences inarterial pulsatility index values between fetuses with nor-mal and abnormal biophysical assessment parameters (ex-cept for the aorta and abnormal fetal heart rate trace),whereas venous pulsatility was significantly increased incompromised fetuses compared with the noncompro-mised group. However, in the late third-trimester fetusesthe venous Doppler findings were not as reliable as duringthe late second and early third trimesters.4
Changes in venous blood flow are preceded bychanges in fetal arterial flow. In a study by Ozcan et al,13 ar-terial Doppler indices did not reveal significant associa-tions with adverse perinatal outcomes. A low pulsatilityindex in the middle cerebral artery, reflecting the brain-sparing effect, is an early sign of hypoxemia in IUGR fe-tuses.7 Venous Doppler waveforms become abnormalafter the brain-sparing effect and correlate better withacidemia than do those of the peripheral arteries.65
Velocimetric modifications in the fetal venous com-partment constitute a relevant prognostic sign in the pre-diction of perinatal mortality and neonatal resuscitation.66
The farther the compromised venous vessels are from theheart, the higher the relative risk for perinatal mortality,and it is 5 times greater than normal when pulsations arerecorded at the inferior vena cava level, 8 times greater at
J Ultrasound Med 2011; 30:529–545 533
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
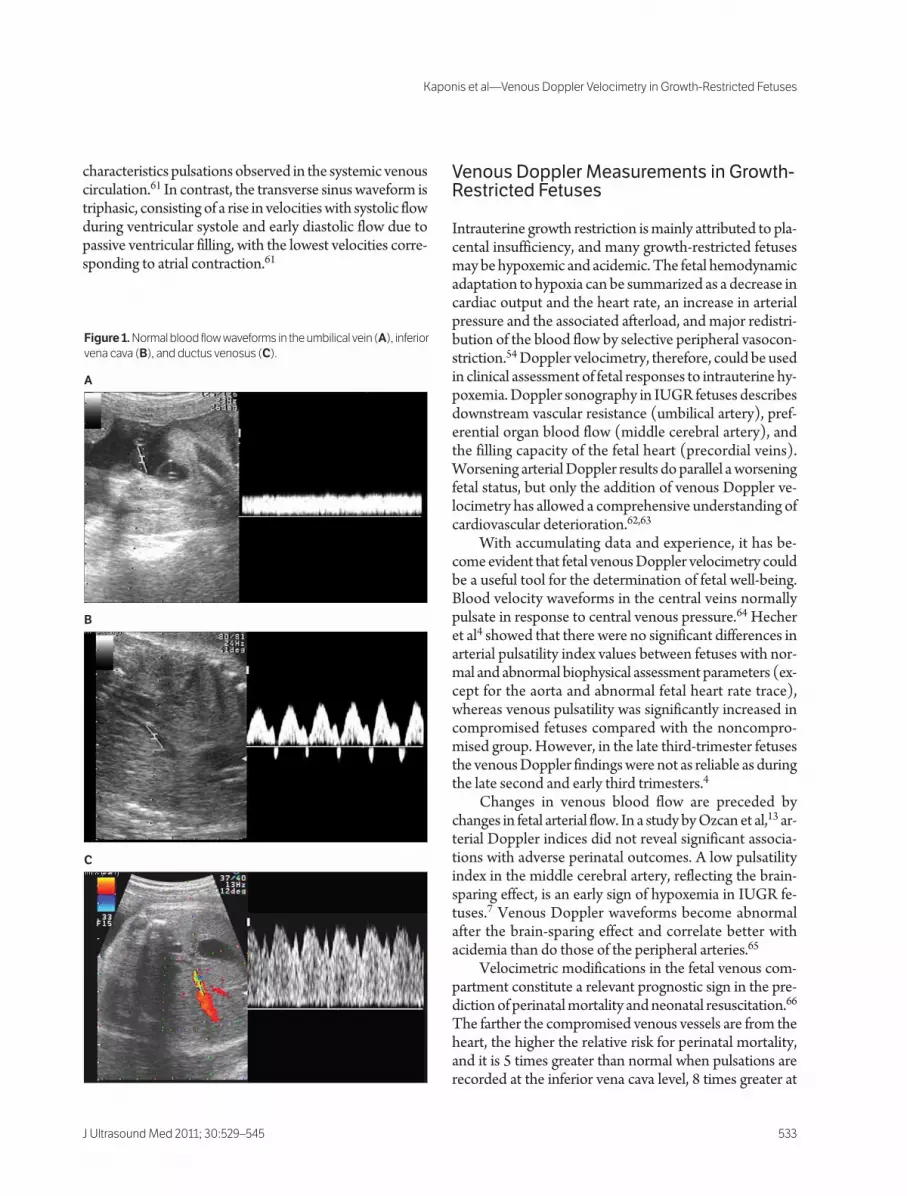
Figure 1. Normal blood flow waveforms in the umbilical vein (A), inferior
vena cava (B), and ductus venosus (C).
A
B
C
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 533

the ductus venosus level, and 18 times greater when pul-sations are present at the umbilical vein level.66
Umbilical VeinUmbilical vein pulsations with moderate to severe notchessynchronous with atrial contraction have been described asominous signs associated with various conditions of fetaldisease such as twin-twin transfusion syndrome,67 severeIUGR in fetuses with absent-end diastolic flow in the um-bilical arteries,68 abnormal fetal heart rates,68 and other fetaland placental abnormalities (Table 1).71,72 Pulsatile bloodflow in the umbilical vein is considered the dominant fac-tor determining the interval between the first occurrence ofabsent end-diastolic velocities in the umbilical artery (lateDoppler abnormalities) and the development of late heartrate decelerations and delivery.73
Umbilical vein pulsations have been considered a conse-quence of ductus venosus reversed flow.4,40,41,74 Pulsationscan even occur in normal pregnancies.72,75 These pulsa-tions may result from the transmission of pulse waves fromthe umbilical arteries.72 However, umbilical vein pulsationsafter the first trimester of pregnancy (at that time, pulsa-tions are attributable to the large reflux component duringatrial contraction) are sporadic and possibly intermittentphenomena, and they may be related to fetal arrhythmia.75
Types of Umbilical Vein PulsationsThere are 2 different types of umbilical vein pulsations at-tributed to a single or double decrease in blood velocityduring a single heart cycle. In most IUGR fetuses, umbili-cal vein pulsations tend to be monophasic (Figure 2B).The large amount of reversed flow causes umbilical veinpulsations manifested as a single peaked waveform.38 More
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545534
Figure 2. Normal (A and C) and abnormal (B and D) umbilical vein and abnormal ductus venosus flow waveforms. Abnormal umbilical vein wave-
forms (B) show monophasic-type pulsations. Abnormal ductus venosus waveforms (D) show a decreased A wave during atrial systole.
A B
C D
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 534
rarely, a biphasic flow pattern with systolic and diastolicpeaks is seen with progressive circulatory deterioration.4,48
The double-pulsating pattern of the umbilical vein hasbeen considered an ominous sign related to perinatal mor-tality.76 It is associated with congestive cardiac failure andtricuspid regurgitation caused by relatively long-standinghigh umbilical artery resistance due to placental insuffi-ciency and intrauterine hypoxia.77 Baschat and Gem-bruch44 reported a case of a singleton pregnancy withsevere IUGR in which the venous flow pattern in the um-bilical vein was triphasic. The fetus survived for 8 days afterthe finding of triphasic blood flow in the umbilical vein.The authors speculated that the prolonged survival was at-
tributed to remodeling of the myocardial vasculature dueto early onset of hypoxemia and/or to coronary vasodi-latation and enhanced myocardial blood flow and oxy-genation that may have restricted the onset of intrauterinecardiac failure and fetal death.44
The sampling site of the umbilical vein may have animportant role in evaluation of the severity of fetal growthrestriction. Hofstaetter et al76 suggested that pulsationsrecorded only in the intra-abdominal part of the umbilicalvein might be relatively early indicators of a worsening fetalcondition, with a better prognosis than when pulsationsextend out to the cord.
Quantitative Parameters of Umbilical Vein Blood FlowQuantitative parameters of the umbilical vein were alsoused for the diagnosis of IUGR. Umbilical vein blood flowis lower in IUGR fetuses. In a longitudinal study, Di Naroet al78 showed that there is a progressive reduction of theumbilical vein blood flow over time in IUGR fetuses evenin the presence of normal umbilical artery Doppler pa-rameters. This finding is in accordance with a study by Fer-razzi et al,79 who showed that the umbilical vein blood flowwas reduced in IUGR fetuses on a weight-specific basis. DiNaro et al78 proposed that because the umbilical vein sizedoes not change substantially, the reduction of blood flowin IUGR fetuses might be explained by an increased vis-cosity in the umbilical cord blood and by a decreased bloodflow velocity compared with appropriate-for-gestational-age fetuses. The former speculation is in agreement with afinding by Baschat et al,80 who showed that IUGR fetuseshave an increased nucleated red blood cell count at birth.This circumstance is supported by the finding that inhealthy fetuses, umbilical blood flow velocity measure-ments increase normally with advancing gestation, whereasin IUGR fetuses, this finding does not occur.81 However,the reduced flow and the lower-velocity waveform in theumbilical vein cannot be used alone as reliable markers ofthe severity of IUGR because a considerable overlap existswith normal ranges.82,83
Rigano et al84 observed that the umbilical vein bloodflow per unit of fetal tissue in IUGR fetuses was reducedin fetuses with normal umbilical artery Doppler veloci-metric parameters. This finding suggests that in contrastto the umbilical vein pulsations, the reduced blood flowcoming from the placenta to the fetus might represent anearly event in the pathogenesis of IUGR, playing an im-portant role in the nutrients and fetal oxygen deprivationthat finally compromise the natural fetal growth potential.Moreover, when the blood flow was corrected according tothe abdominal circumference, this finding proved to be a
J Ultrasound Med 2011; 30:529–545 535
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
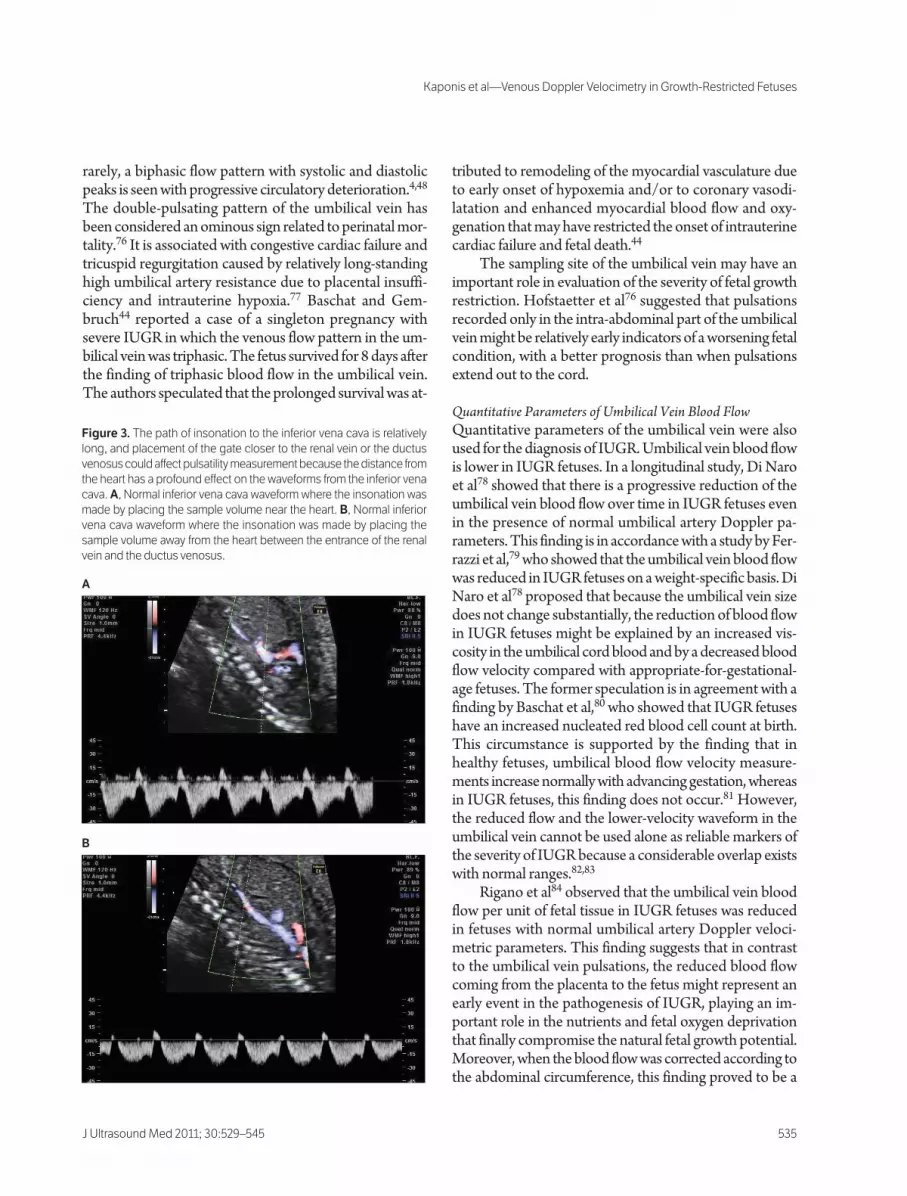
Figure 3. The path of insonation to the inferior vena cava is relatively
long, and placement of the gate closer to the renal vein or the ductus
venosus could affect pulsatility measurement because the distance from
the heart has a profound effect on the waveforms from the inferior vena
cava. A, Normal inferior vena cava waveform where the insonation was
made by placing the sample volume near the heart. B, Normal inferior
vena cava waveform where the insonation was made by placing the
sample volume away from the heart between the entrance of the renal
vein and the ductus venosus.
A
B
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 535

better indicator for expressing umbilical vein blood flowchanges compared with the estimated fetal weight.84 Thelatter longitudinal study revealed that the blood flow re-duction was not a transient phenomenon but persistedthroughout the pregnancy, and it could differentiate IUGRfetuses in midgestation from constitutionally small fetuses.According to these data, we suggest that abnormalities inthe umbilical vein waveform have to be combined with ar-terial Doppler indices for a better indication of the severityof fetal growth restriction.
Estimation of the fetal brain volume in utero and itsrelationship with liver volume and umbilical vein volumeflow measurements has been used to detect IUGR fe-tuses.85 A substantially increased fetal brain to liver volumeratio was found in IUGR compared with appropriate-for-gestational-age fetuses, and additionally, there was a con-siderable inverse relationship between this ratio and fetalweight-related umbilical vein volume flow.85 The authorsof that study suggested that the fetal brain to liver vol-ume ratio is a predictor of the outcome in IUGR fetuses.However, the clinical importance of this finding remainsquestionable.
Inferior Vena CavaBecause fetal oxygenation depends on blood returningfrom the placenta via the inferior vena cava to the fetalheart, alterations in the pattern of inferior vena cava flowhave the potential to affect the fetal condition. In compro-mised fetuses, a decrease in forward flow during the S andD waves and accentuated reversed flow in the A wave willbe present.83 Areias et al86 analyzed inferior vena cava pat-terns in conjunction with tricuspid flow velocities. Theysuggested that with decreased right ventricular complianceand elevated filling pressures, the pressure increase in theright ventricle is greater and more rapid than in the rightatrium. This increase shortens the duration of initial for-ward tricuspid flow. When atrial contraction occurs against
a high–end-diastolic pressure ventricle, there is an increaseof reversed flow in the venous system.86 In addition, duringatrial contraction, the foramen ovale is closed.87 The resultis a pulsatile inferior vena cava blood flow pattern. The ex-tension of pulsations in the ductus venosus and umbilicalvein is accompanied by a worsening of the fetal condition.
Mori et al88 found 2 different abnormal waveforms inthe inferior vena cava of IUGR fetuses: 1 with a high- pulsatile pattern and the other with a shallow and low- pulsatile pattern. Both groups had considerably worseoutcomes than fetuses with normal flow in the inferior venacava. Fetuses in the low-pulsatile group were the most se-verely compromise, presenting with late heart rate decel-eration. The authors suggested that impaired contractilityand reduced ventricular output with concomitantly re-duced ventricular filling were responsible for this abnor-mal pattern.88 This finding could be representative of abreakdown of blood flow redistribution comparable tothe return of low-resistance middle cerebral artery wave-forms to high-resistance waveforms.20
Correlation With Doppler Waveforms in the Umbilical Artery In IUGR fetuses with high-resistance flow patterns in theumbilical artery studied longitudinally, a progressivechange in inferior vena cava and ductus venosus wave-forms preceded the onset of late heart rate decelerations,but these changes were not related to concomitant alter-ations in arterial vessels.89,90 In IUGR fetuses with late um-bilical artery Doppler abnormalities, there was a decreasedproportion of blood flow during diastole and increased re-versed flow during atrial contraction in the inferior venacava.38 Fetal morbidity appears to be associated with an in-crease in reversed flow in the inferior vena cava during atrialcontraction.
A correlation in velocity waveforms between the infe-rior vena cava and superior vena cava in growth-restrictedfetus with late umbilical artery Doppler abnormalities was
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545536
Table 1. Representative Studies Evaluating Abnormal Umbilical Vein Transverse Sinus Waveforms With Perinatal Outcomes
Abnormal Neonatal
Study n Waveforms PNM IUFD Death NEC RDS IVH
Ozcan et al13 22 Pulsation 1 4 4 8
Schwarze et al69 74 Pulsation 8 6 6
Cheema et al70 16 Pulsation 3
Cheema et al70 102 Abnormal 2,2
TS PIV,
abnormal
TS PLI
IUFD indicates intrauterine fetal death; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; PIV, pulsatility index for veins; PLI,
preload index; PNM, perinatal mortality; RDS, respiratory distress syndrome; and TS, transverse sinus.
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 536

made by Fouron et al.91 They showed that a reciprocal shiftexisted in the waveforms between the two vessels. The flowprofile in the inferior vena cava resembled the one ob-served in the superior vena cava in healthy fetuses and viceversa. In healthy fetuses, the velocity at the end of systolewas always higher in the inferior vena cava than the supe-rior vena cava, but in growth-restricted fetuses, the veloc-ity at the end of systole was always lower and close to 0 inthe inferior vena cava.91 This complete inversion of flowpatterns suggests that the fall in umbilical venous returndue to the elevated placental resistance and the rise in vas-cular impedance of the lower limbs and mesenteric circu-lation induced by the secondary hypoxemia combine toreduce the volume flow through the inferior vena cava. Thecerebral vasodilatation secondary to hypoxemia increasesthe superior vena cava blood flow. These changes are he-modynamic manifestations of blood flow redistribution to-ward the brain in the presence of placental circulatoryinsufficiency.
In contrast, in a study conducted by Gudmundssonet al,43 only 1 of 17 fetuses with absent or reversed end- diastolic flow in the umbilical artery had abnormal bloodflow in the inferior vena cava. Baschat et al92 suggested thatchanges in inferior vena cava pulsatility are indeterminatein IUGR fetuses.
Inferior Vena Cava Waveforms and Blood Gas AnalysisThe utility of impedance indices from the inferior venacava for predicting acidemia and hypoxia in IUGR fetuseswas evaluated by Rizzo et al.93 According to their results,the preload index of the inferior vena cava was the best pre-dictor of fetal acidemia. They proposed that there is a moredirect relationship between the inferior vena cava flow ve-locity waveform and the severity of fetal compromise dueto the proximity of this vessel to the heart.93 On the otherhand, Hecher et al42 could not find any association be-tween inferior vena cava pulsatility and blood gas analysisresults. The most likely explanation for this discrepancy isthe lack of a landmark for accurate and reproducible place-ment of the sample volume in the inferior vena cava.42
LimitationsHuisman et al56 recorded inferior vena cava signals at theentrance to the right atrium and found a large SD for vari-ous flow velocity waveform parameters. Rizzo et al57 re-ported that the highest reproducibility of inferior vena cavaflow velocity waveforms was achieved by placing the sam-ple volume in the fetal abdomen, between the entrance ofthe renal vein and the ductus venosus. However, the pathof insonation is relatively long, and placement of the gate
closer to one or the other vessel could affect pulsatilitymeasurement because the distance from the heart has aprofound effect on the waveforms from the inferior venacava (Figure 3).42 According to these data, we suggest thatthere are conflicting results in the international literaturefor the validity of inferior vena cava flow indices to diag-nose and monitor IUGR fetuses. The extension of venouspulsatility to the ductus venosus and umbilical vein is a bet-ter indicator for the severity of fetal growth restriction.
Sonographic measurement of inferior vena cava wallmovements (diameter pulse waveforms) have opened upnew possibilities for evaluation of this vessel.94 A low- pulsatility waveform may reflect depressed myocardialfunction and indicate fetal cardiac dysfunction in utero.94
However, larger longitudinal studies are needed to clarify allof the parameters involved for altering the inferior vena cavawaveforms and to define the mode of change correspondingto the chronologically deteriorating fetal cardiac function.
Ductus VenosusIn contrast to the inferior vena cava, ductus venosus ve-locity measurements have acceptable reproducibility, thewithin-patient coefficient of variation varying from 8% to10%.95 The introduction of Doppler velocimetry of theductus venosus74 in human fetuses has opened a new era ofprenatal fetal assessment.54 The impedance in the ductusvenosus and the pressure gradient between the umbilicalvein and central venous pressure produced in the heart andinferior vena cava regulate the oxygenated blood flow re-turning from the placenta to the fetus. The pressure gradi-ent across the ductus venosus is estimated to vary between0 and 3 mm Hg.96 Any change in the pressure gradient, ascan be observed in IUGR fetuses, may alter the ductusvenosus blood flow. Altered fetal hemodynamics mani-fested by increased central venous pressure may be pre-ceded by changes in ductus venosus flow velocities.20,51
Normal Ductus Venosus Waveform in IUGR FetusesThe first study evaluating ductus venosus waveforms in se-verely IUGR fetuses was performed by Kiserud et al.34 Toensure the oxygen supply to the fetus, the blood flow in theductus venosus is maintained within normal ranges as longas possible, despite the obvious impairment of the umbil-ical circulation.54 Various studies have shown that despitemarked changes in the umbilical circulation in fetuses withsevere IUGR, a normal peak velocity in the ductus venosusis maintained.97–99 The blood flow in the ductus venosus isa preferential bloodstream in the fetus and may indicateredistribution of umbilical vein blood through the ductusvenosus at the expense of hepatic blood flow. A substan-tial increase in ductus venosus shunting associated with
J Ultrasound Med 2011; 30:529–545 537
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 537

vein dilatation in IUGR fetuses compared with healthy fe-tuses has been found.24,99 These results show that in fetuseswith severe IUGR, ductus venosus shunting is higher, andthe umbilical blood flow to the liver is lower, particularly infetuses with the most severe umbilical hemodynamic com-promise.99 The isthmic portion of the ductus venosus con-tains less smooth muscle tissue and α-adrenergic receptorscompared with the intrahepatic branches of the portalvein.100 The increase in the ductus venosus shunting rate isa general mechanism of adaptation to fetal distress and isobserved in IUGR fetuses.
Importance of an Abnormal Ductus Venosus WaveformAbnormal ductus venosus waveforms can be seen in hy-poxemic and hypovolemic fetuses. Absence or reversal ofblood flow during atrial contraction (A wave) implies fail-ure of fetal circulatory compensation to supply well-oxygenated blood to vital organs.101 Ductus venosusDoppler velocimetry effectively identifies preterm IUGRfetuses that are at the highest risk of adverse outcomes atleast 1 week before delivery, independent of the umbilicalartery waveform.102 Progressive escalation of the ductusvenosus Doppler index is associated with a high stillbirthrate. Kiserud et al34 found that 34% of severely IUGR fe-tuses had a reduced minimum velocity in the ductus veno-sus, whereas reversed blood flow during atrial contractionwas found in 16% of cases. Among the fetuses with reducedductus venosus blood flow velocity during atrial contrac-tion, 69% were associated with umbilical vein pulsations.34
The reduction of the forward flow has been attributed toincreased end-diastolic pressure and cardiac failure in IUGR
fetuses (Figure 2D). Bellotti et al31 suggested that thesechanges may partially be attributed to active dilatation of theductus venosus. The decrease in the flow velocity during theatrial contraction may be caused by the lower umbilical veinpressure during vasodilatation of the ductus venosus.31
Absent or reversed flow in the ductus venosus indi-cates a poor prognosis, with a high probability of perinatalmortality. Hecher et al4 showed that 5 of 8 fetuses with ab-sent or reversed flow in the ductus venosus on the day ofdelivery died. Moreover, Rizzo et al90 found significantlyhigher ductus venosus peak velocity values and a higherratio between systolic and atrial peak velocities in IUGRfetuses. The perinatal outcome was worse among thosewith a systolic to atrial ratio above the 95% confidence in-terval. Baschat et al5 suggested that the only statisticallysignificant relationship between Doppler indices and peri-natal outcome is the association between ductus venosusflow and fetal death. In a study by Figueras et al,103 the pos-itive predictive values of an abnormal ductus venosuswaveform for admission to the neonatal intensive care unit,major neonatal morbidity, the need for neonatal intuba-tion, and an umbilical artery pH of less than 7.10 were81.5%, 26%, 48%, and 55%, respectively. It seems thatthere is a consensus among scientists that the presence ofreversed flow in the ductus venosus has been associatedwith higher perinatal mortality (Table 2).4,43,68,74,89
However, Hofstaetter et al8 found that the abnormalductus venosus velocity waveforms recorded in 26 preg-nancies were not correlated well to the perinatal outcome,except for a low Apgar score at 1 minute of life. In a differ-ent study, the same group reported that the sensitivity of re-
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545538
Table 2. Representative Studies Evaluating Abnormal Ductus Venosus Waveforms and Perinatal Outcomes
Abnormal Neonatal
Study n Waveforms PNM IUFD Death NEC RDS IVH
Hecher et al4 8 A/RAV 5
Hofstaetter et al8 22 Elevated DV
index
Ozcan et al13 5 A/RAV 4 1 3 4
Bilardo et al33 37 Elevated DV 6
index
Schwarze et al69 74 A/RAV 8 6 4
Figueras et al103 27 Elevated DV 7 7 1
index
Cosmi et al104 145 A/RAV 34
Alves et al105 20 A/RAV 13 1 10
Baschat et al106 132 A/RAV 20 18
Bilardo et al107 17 A/RAV 5
Müller et al108 12 A/RAV 3 2 1 1 8 5
A/RAV indicates absent/reversed A-wave; DV, ductus venosus; IUFD, intrauterine fetal death; IVH, intraventricular hemorrhage; NEC, necro-
tizing enterocolitis; PNM, perinatal mortality; and RDS, respiratory distress syndrome.
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 538

versed flow in the ductus venosus for the prediction of peri-natal mortality was very low: 53% in all cases with perina-tal mortality, 67% in cases with absent or reversed flow inthe umbilical artery, and 79% when the velocity in the duc-tus venosus during atrial contraction was below the fifthpercentile.35 According to the authors, a longitudinal studyof the pulsatility index for veins and the systolic toatrial/systolic ratio in the right hepatic vein and ductusvenosus seems to be the most useful index, as well as thepresence of double umbilical venous pulsations, for opti-mizing the timing of intervention.35
Correlation With Blood Gas AnalysisIn human IUGR fetuses with placental insufficiency, a sub-stantial negative correlation between the umbilical vein pHand ductus venosus pulsatility index (pulsatility index forveins) has been found.42 In this cross-sectional study of 23severely IUGR fetuses, moderate acidemia was associatedwith individual ductus venosus Doppler index results,with most measurements still within the referenceranges.42 With increasing severity of hypoxemia andacidemia, the ductus venosus pulsatility indices in-creased, and velocities with atrial contraction were re-duced to 0 or became negative in the most severecases.20,42 Rizzo et al93 also found significant relationshipsbetween acidemia and all of the venous Doppler indices,whereas hypoxemia was significantly associated with onlythe systolic to atrial ratio in the ductus venosus and thepreload index in the inferior vena cava. In human IUGRfetuses with abnormal umbilical artery Doppler findings,it has been shown that inferior vena cava, ductus venosus,and umbilical vein Doppler parameters were predictive ofan umbilical artery pH of less than 7.20.109
In an experimental sheep model, fetal hypoxemia in-creased the pulsatility of the ductus venosus blood veloc-ity waveform pattern. However, in fetuses with elevatedplacental vascular resistance, the pulsatility on ductus veno-sus velocimetry did not increase further in the presence ofsevere and worsening fetal acidemia and impending fetaldeath.110 Different groups have proposed the study of var-ious Doppler indices to predict acidemia at birth. The duc-tus venosus systolic to atrial ratio, systolic to atrial/systolicratio, and pulsatility index for veins were all good predictorsof fetal acidemia.111 Another group suggested that com-bining the pulsatility indices of the umbilical artery andthose of the ductus venosus provided the greatest accuracyin predicting IUGR neonates with acidemia.112 It seemsthat combination rather than single-vessel assessment pro-vides the best predictive accuracy for acidemia in a sub-stantial proportion of IUGR neonates.
Limitations The necessity of extensive repetition of Doppler samplingto confirm the finding that the recorded flow velocity wave-forms are truly representative of ductus venosus flow mayhamper the accuracy of these investigations and conse-quently affect their clinical relevance.107 Gestational ageaffects the blood flow volume through the ductus venosus. In one study, the absolute blood flow volume increasedwith gestational age, whereas blood flow normalized forestimated fetal body weight decreased with gestationalage.29 Accurate measurement of the vessel diameter with a2-dimensional sonography is regarded as a major problem.Flow measurements and calculation of the ductus venosusshunt rate should be regarded with caution, especiallywhen determined in IUGR fetuses.
Hepatic and Portal VeinsThe hepatic vein, although easy to sample, is only infre-quently used as a parameter in IUGR studies.83 A declinein forward velocities during atrial systole, usually associ-ated with a reversed A wave in the inferior vena cava andthe hepatic vein, indicates abnormalities in forward cardiacfunction. Only in cases with severely compromised fetusesand fetuses with hydrops has the hepatic vein velocimetrybeen used to predict perinatal mortality.35,113 According tothe authors of that study, the hepatic vein was an earlier pre-dictor of impending mortality than the ductus venosus.35
The portal vein directs poorly oxygenated blood fromthe splanchnic circulation to the right liver. Under normalconditions, a substantial portion of umbilical vein bloodflows steadily forward through the left portal vein. Placen-tal insufficiency causes venous hypoperfusion of the fetalliver and an increased contribution of poorly oxygenatedblood from the portal vein.114 In IUGR fetuses, an associ-ation was found between reversed flow in the left portalvein and increased resistance in the umbilical artery.115
Fetuses with absent or reversed end-diastolic flow in theumbilical artery and normal flow in the umbilical vein hadnormal left portal vein flow in mild cases, pulsatile left por-tal vein flow in cases with increased resistance or zero flowin the umbilical artery, and reversed left portal vein flow infetuses with reversed flow in the umbilical artery.115 How-ever, the role of the left portal vein for evaluating fetal com-promise has been questioned by a longitudinal studyperformed in healthy fetuses during the second trimester ofpregnancy, showing that the occurrence of pulsations inthe left portal branch is a normal phenomenon, as is rever-sal of flow, albeit rare and occurring only during the finaldays of pregnancy or during fetal breathing (intermittedflow reversal).116
J Ultrasound Med 2011; 30:529–545 539
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 539

Cerebral VeinsIntrauterine growth-restricted fetuses have incrementalbrain venous blood flow velocities, a reduced pulsatilityindex for veins in the transverse sinus, and increased pul-sations in the vein of Galen. Pulsations and a maximum ve-locity in the vein of Galen in high-risk pregnancies wereseen more frequently than pulsations in the umbilical veinand correlated well with adverse perinatal outcomes, in-cluding perinatal mortality.70 An abnormal transverse sinuspulsatility index for veins and a preload index and straightsinus maximum velocity were very infrequent and relatedonly to perinatal mortality, suggesting that are late signs offetal compromise, even later than pulsations in the umbil-ical vein.70 Senat et al117 found a significant association be-tween an increased transverse sinus pulsatility index forveins and low Apgar scores. In contrast, all other veinsshowed similar pulsatility index values between IUGR andappropriate-for-gestational-age fetuses.118 All cerebralveins of IUGR fetuses showed significantly increased max-imum and mean velocities. An increased pulsatile patternin the vein of Galen and straight sinus was noted in IUGRcases.118 It seems that larger longitudinal studies areneeded to verify the validity of cerebral veins for evaluatingIUGR fetuses.
Internal Jugular VeinIn a longitudinal study, Weiner et al60 found a significantlylower peak velocity ratio and velocity time integral ratio inthe internal jugular vein of IUGR fetuses with absent end-diastolic flow at the umbilical artery compared with healthyfetuses at 28 to 32 weeks’ gestation. The internal jugularvein blood flow pattern in these IUGR fetuses showedequal S and D waves with an absent reversed wave. All ofthe fetuses at that time had normal inferior vena cavaDoppler indices, whereas umbilical vein pulsations and ab-normal flow patterns in the ductus venosus and inferiorvena cava were not observed.60 These changes could be at-tributed to increased cerebral venous blood flow (brain-sparing effect) and appear early in the development ofgrowth restriction. The clinical importance of this obser-vation is still not clear.
Coronary Blood Flow and Venous Flow In contrast, the heart-sparing effect in IUGR fetuses man-ifested by visualization of coronary blood flow is a sign ofsevere fetal compromise associated with a poor perinataloutcome. Visualization of coronary blood flow consistentlycoincides with deterioration of venous flow.45 The eleva-tion of the peak velocity index in the inferior vena cava andductus venosus is substantially higher in fetuses with the
heart-sparing effect.47,51 These fetuses show Doppler sono-graphic findings associated with fetal acidemia and a poorperinatal outcome, including umbilical vein pulsations,normalization of the middle cerebral artery pulsatilityindex, and atrioventricular valve insufficiencies with rela-tively low-velocity regurgitant jets.45
Cardiovascular Parameters for Evaluation ofIUGR Fetuses
Improvements in ultrasound technology allow evaluationof IUGR fetuses earlier than the classic Doppler waveformsallow. Umbilical vein flow and placental/left and right car-diac output fractions were found to be reduced by 20 to 24gestational weeks.23 This reduction occurred earlier thanmodifications in the fetal size and arterial and venous pul-satility index values.23
In recent years, new cardiovascular parameters havealso been proposed for fetal assessment. An abnormal aor-tic isthmus flow pattern has been associated with adverseperinatal outcomes and a later neurodevelopmental statusin several experimental and clinical studies.119,120 The aor-tic wall thickness was found to be significantly increased inIUGR compared with appropriate-for-gestational-age fe-tuses.104 In addition, aortic intima-media thickness meas-urements in fetuses with IUGR were inversely related to theestimated fetal weight, showing that a low birth weight andDoppler abnormalities may be correlated with an alteredvascular structure causing possible endothelial damage.104
The myocardial performance index, a Doppler indexof combined systolic and diastolic function, has beenshown to be correlated with the presence of cardiac- andbrain-sparing effects.121 The myocardial performanceindex increased in IUGR fetuses, having a linear correla-tion with the hemodynamic severity stage.121,122 In a re-cent study, the myocardial performance index and ductusvenosus pulsatility index variables were found to be inde-pendent predictors of perinatal mortality in preterm(24th–34th gestational week) IUGR fetuses.123 In thesame study, the risk for intrauterine death in IUGR fetusesbefore the 28th gestational week with present atrial flow inthe ductus venosus and a normal myocardial performanceindex was 18%.123 When 1 of these 2 variables was abnor-mal, the risk was 70% to 73%, and when both variableswere abnormal, the risk was 97%.123 In IUGR fetuses afterthe 28th gestational week, the risks of death were 0.1%, 6%to 7%, and 45%, respectively.123 A combination of ductusvenosus flow with the myocardial performance index maybetter stratify the estimated probability of death in IUGRfetuses. However, we have to emphasize that larger longi-
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545540
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 540

tudinal studies are needed to evaluate the potential clinicalvalue of these new Doppler variables and to clarify their as-sociation and potential interaction with other classicDoppler indices.
Validity of Venous Doppler Studies to Optimize the Timing of Delivery in Growth-Restricted Fetuses
The decision to deliver a preterm IUGR fetus still remainsone of the great challenges in obstetrics. Fetal venousDoppler studies represent valuable diagnostic techniquesthat can influence the management of IUGR fetuses. Onthe basis of the current literature, we suggest that longitu-dinal monitoring of venous flow velocity waveforms inIUGR fetuses is a logical approach to optimize the timingof delivery rather than watching and waiting for changesin fetal heart patterns, which, moreover, correlate poorlywith the neonatal outcome.124 Abnormal venous Dopplerresults would appear to indicate fetal deterioration and afetus who will not be able to cope much longer in the in-trauterine environment. Most of the longitudinal studiesdiscussed in this review showed that alterations of venousflow volume waveforms precede fetal heart rate decelera-tions and therefore offer warning signs to act before a fetallife-threatening situation occurs.
However, in clinical practice, it is difficult to accuratelyestimate the duration of fetal compromise. In most IUGRfetuses, the deterioration of uteroplacental function is man-ifested by the following longitudinal progression of abnor-mal Doppler waveforms: elevated umbilical artery bloodflow resistance and a decrease in the umbilical vein flowvolume per kilogram of fetal body weight, both of whichprecede the onset of a growth delay.84,102 Decreased mid-dle cerebral artery impedance and increased brain venousblood flow velocities assist in the appearance of the brain-sparing effect. These “early responses” are physiologicallyfollowed by late-onset Doppler abnormalities such as absent/reversed umbilical artery end-diastolic velocity,
absent/reversed inferior vena cava and ductus venosus A waves, and umbilical vein pulsation (Table 3).4,5,83,102,117,125
Venous Doppler abnormalities may persist for a variableperiod in the preterm IUGR fetus.97,126,127 Impacts on theperinatal outcome become important with escalation of ve-nous flow abnormalities. These Doppler indices have to beevaluated together with the gestational age and biophysi-cal profile scores to make a decision for intervention.
In most cases (70%), the Doppler deterioration wascomplete 24 hours before biophysical profile score de-clines. In the face of severe Doppler deterioration, main-tenance of a normal biophysical profile would allowappropriate preparation for delivery, whereas when bothsystems fail, the need for urgent delivery is certain.92 Thecombination of longitudinal multivessel monitoring andbiophysical profile scores together with the gestational agecould provide a definitive indication for action in the man-agement of severely IUGR fetuses. However, there is stillthe need for well-designed longitudinal trials to approachthe reference standard for management of fetuses withIUGR.
References
1. Campbell S, Vyas S, Nicolaides KH. Doppler investigation of fetal circu-lation. J Perinat Med 1991; 19:21–26.
2. Mari G, Uerpairojkit B, Abuhamad AZ, Copel JA. Adrenal artery velocitywaveforms in the appropriate and small-for-gestational-age fetuses. Ultrasound Obstet Gynecol 1996; 8:82–86.
3. Abuhamad AZ, Mari G, Bogdan D, Evans ET. Doppler flow velocimetryof the splenic artery in the human fetus: is it a matter of chronic hypoxia?Am J Obstet Gynecol 1995; 172:820–825.
4. Hecher K, Campbell S, Doyle P, Harrington K, Nicolaides K. Assessmentof fetal compromise by Doppler ultrasound investigation of the fetal circulation: arterial, intracardiac, and venous blood flow velocity studies.Circulation 1995; 91:129–138.
5. Baschat AA, Gembruch U, Reiss I, Gortner L, Weiner CP, Harman CR.Relationship between arterial and venous Doppler and perinatal outcomein fetal growth restriction. Ultrasound Obstet Gynecol 2000; 16:407–413.
J Ultrasound Med 2011; 30:529–545 541
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
Table 3. Representative Studies Evaluating Abnormal Venous Waveforms and Perinatal Outcomes
Abnormal Neonatal
Study n Waveforms PNM IUFD Death NEC RDS IVH
Baschat et al5 50 DV AAV, UV 18 11 7 6 33 6
pulsations
Hofstaetter et al35 28 Abnormal veins 15 12 3
Schwarze et al69 74 Abnormal DV 2 3 6
and UV
AAV indicates absent A-wave; DV, ductus venosus; IUFD, intrauterine fetal death; IVC, inferior vena cava; IVH, intraventricular hemorrhage;
NEC, necrotizing enterocolitis; PNM, perinatal mortality; PVI, peak velocity index; RDS, respiratory distress syndrome; and UV, umbilical vein.
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 541

6. Divon MY. Umbilical artery Doppler velocimetry: clinical utility in high-risk pregnancies. Am J Obstet Gynecol 1996; 174:10–14.
7. Mari G, Deter RL. Middle cerebral artery flow velocity waveforms in nor-mal and small-for-gestational-age fetuses. Am J Obstet Gynecol 1992;166:1262–1270.
8. Hofstaetter C, Gudmundsson S, Dubiel M, Marsál K. Ductus venosusvelocimetry in high-risk pregnancies. Eur J Obstet Gynecol Reprod Biol 1996;70:135–140.
9. Gudmundsson S, Dubiel M, Gunnarson G, Stale H, Maesel A, Marsál K.Middle cerebral artery velocimetry as a predictor of hypoxemia in fetuseswith increased pulsatility index in the umbilical artery. J Matern Fetal In-vest 1994; 4(suppl):19.
10 Dubiel M, Gudmundsson S, Gunnarson G, Marsál K. Middle cerebralartery velocimetry as a predictor of hypoxemia in fetuses with increased re-sistance to blood flow in the umbilical artery. Early Hum Dev 1997;47:177–184.
11. Gill RW. Pulsed Doppler with B-mode imaging for quantitative bloodflow measurement. Ultrasound Med Biol 1979; 5:223–235.
12. Laurin J, Lingman G, Marsál K, Persson PH. Fetal blood flow in preg-nancies complicated by intrauterine growth retardation. Obstet Gynecol1987; 69:895–902.
13. Ozcan T, Sbracia M, d’Ancona RL, Copel JA, Mari G. Arterial and ve-nous Doppler velocimetry in the severely growth-restricted fetuses andassociations with adverse perinatal outcome. Ultrasound Obstet Gynecol1998; 12:39–44.
14. Tchirikov M, Kertschanska S, Stürenberg HJ, Schröder HJ. Liver bloodperfusion as a possible instrument for fetal growth regulation. Placenta2002; 23(suppl A):S153–S158.
15. Bellotti M, Pennati G, De Gasperi C, Battaglie FC, Ferrazzi E. Role of duc-tus venosus in distribution of umbilical blood flow in human fetuses dur-ing second half of pregnancy. Am J Physiol Heart Circ Physiol 2000;279:H1256–H1263.
16. Kiserud T, Rasmussen S, Skulstad S. Blood flow and the degree of shunt-ing through the ductus venosus in the human fetus. Am J Obstet Gynecol2000; 182:147–153.
17. Fasouliotis SJ, Achiron R, Kivilevitch Z, Yagel S. The human fetal venoussystem: normal embryologic, anatomic, and physiologic characteristicsand developmental abnormalities. J Ultrasound Med 2002; 21:1145–1158.
18. Huisman TWA, Gittenberger-De Groot AC, Wladimiroff JW. Recogni-tion of a fetal subdiaphragmatic venous vestibulum essential for fetal ve-nous Doppler assessment. Pediatr Res 1992; 32:338–341.
19. Edelstone DI, Rudolph AM. Preferential streaming of ductus venosusblood to the brain and heart in fetal lambs. Am J Physiol 1979; 237:H724–H729.
20. Hecher K, Campbell S. Characteristics of fetal venous blood flow undernormal circumstances and during fetal disease. Ultrasound Obstet Gynecol1996; 7:68–83.
21. Robinson JS, Kingston EJ, Jones CT, Thorburn GD. Studies on experi-mental growth retardation in sheep: the effect of removal of endometrialcaruncles on fetal size and metabolism. J Dev Physiol 1979; 1:379–398.
22. Kiserud T, Ebbing C, Kessler J, Rasmussen S. Fetal cardiac output, distri-bution to the placenta and impact of placental compromise. UltrasoundObstet Gynecol 2006; 28:126–136.
23. Rizzo G, Capponi A, Cavicchioni O, Vendola M, Arduini D. Low cardiacoutput to the placenta: an early hemodynamic adaptive mechanism inintrauterine growth restriction. Ultrasound Obstet Gynecol 2008; 32:155–159.
24. Bellotti M, Pennati G, De Gasperi C, Bozzo M, Battaglia FC, Ferrazzi E.Simultaneous measurements of umbilical venous, fetal hepatic, and duc-tus venosus blood flow in growth-restricted human fetuses. Am J ObstetGynecol 2004; 190:1347–1358.
25. Sheldon RE, Peeters LLH, Jones MD, Makowski EL, Meschia G. Redis-tribution of cardiac output and oxygen delivery in the hypoxemic fetallamb. Am J Obstet Gynecol 1979; 135:1071–1078.
26. al-Ghazali W, Chita SK, Chapman MC, Allan LD. Evidence of redistrib-ution of cardiac output in asymmetrical growth retardation. Br J ObstetGynaecol 1987; 96:697–704.
27. Reuss ML, Rudolph AM. Distribution and recirculation of umbilical andsystemic venous blood flow in fetal lambs during hypoxia. J Dev Physiol1980; 2:71–84.
28. Edelstone DI, Rudolph AM, Heymann MA. Effects of hypoxemia anddecreasing umbilical flow on liver and ductus venosus blood flows in fetallambs. Am J Physiol 1980; 238:H656–H663.
29. Tchirikov M, Rybakowski C, Hüneke B, Schröder HJ. Blood flow throughthe ductus venosus in singleton and multifetal pregnancies and in fetuseswith intrauterine growth retardation. Am J Obstet Gynecol 1998; 178:943–949.
30. Tchirikov M, Kertschanska S, Schröder HJ. Obstruction of ductus veno-sus stimulates cell proliferation in organs of fetal sheep. Placenta 2001;22:24–31.
31. Bellotti M, Pennati G, Pardi G, Fumero R. Dilatation of the ductus veno-sus in human fetuses: ultrasonographic evidence and mathematical mod-eling. Am J Physiol 1998; 275:H1759–H1767.
32. Baschat AA, Cosmi E, Bilardo CM, et al. Predictors of neonatal outcomein early-onset placental dysfunction. Obstet Gynecol 2007; 109:253–261.
33. Bilardo CM, Wolf H, Stigter RH, et al. Relationship between monitoringparameters and perinatal outcome in severe, early intrauterine growth re-striction. Ultrasound Obstet Gynecol 2004; 23:119–125.
34. Kiserud T, Eik-Nes SH, Blaas HG , Hellevic LR, Simensen B. Ductusvenosus blood velocity and the umbilical circulation in the seriouslygrowth-retarded fetus. Ultrasound Obstet Gynecol 1994; 4:109–114.
35. Hofstaetter C, Gudmundsson S, Hausmann M. Venous Doppler ve-locimetry in the surveillance of severely compromised fetuses. UltrasoundObstet Gynecol 2002; 20:233–239.
36. Rizzo G, Capponi A, Pietropolli A, Bufalino LM, Arduini D, Romanini C.Fetal cardiac and extracardiac flows preceding intrauterine death. Ultra-sound Obstet Gynecol 1994; 4:139–142.
37. Reed KL, Anderson CF, Shenker L. Changes in intracardiac Dopplerblood flow velocities in fetuses with absent umbilical artery diastolic flow.Am J Obstet Gynecol 1987; 157:774–779.
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545542
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 542

38. Reed KL, Appleton CP, Anderson CF, Shenker L, Sahn DJ. Doppler stud-ies of vena cava flows in human fetuses. Circulation 1990; 81:498–505.
39. Rizzo G, Arduini D, Romanini C. Doppler cardiographic assessment offetal cardiac function. Ultrasound Obstet Gynecol 1992; 2:434–445.
40. Kiserud T, Crowe C, Hanson M. Ductus venosus agenesis prevents trans-mission of central venous pulsations to the umbilical vein in fetal sheep. Ul-trasound Obstet Gynecol 1998; 11:190–194.
41. Kiserud T, Kilavuz O, Hellevic LR. Venous pulsation in the fetal left por-tal branch: the effect of pulse and flow direction. Ultrasound Obstet Gynecol2003; 21:359–364.
42. Hecher K, Snijders R, Campbell S, Nicolaides K. Fetal venous, intracar-diac, and arterial blood flow measurements in intrauterine growth retar-dation: relationship with fetal blood gases. Am J Obstet Gynecol 1995;173:10–15.
43. Gudmundsson S, Tulzer G, Huhta JC, Marsál K. Venous Doppler in thefetus with absent end-diastolic flow in the umbilical artery. Ultrasound Ob-stet Gynecol 1996; 7:262–267.
44. Baschat AA, Gembruch U. Triphasic umbilical venous blood flow withprolonged survival in severe intrauterine growth retardation: a case report.Ultrasound Obstet Gynecol 1996; 8:201–205.
45. Baschat AA, Gembruch U, Harman CR. Coronary blood flow in fetuseswith intrauterine growth restriction. J Perinat Med 1998; 26:143–156.
46. Rowlands DJ, Vyas SK. Longitudinal study of fetal middle cerebral arteryflow velocity waveforms preceding fetal death. Br J Obstet Gynaecol 1995;102:888–890.
47. Baschat AA, Gembruch U, Reiss I, Gortner L, Diedrich K. Demonstra-tion of fetal coronary blood flow by Doppler ultrasound in relation to ar-terial and venous flow velocity waveforms and perinatal outcome: the“heart-sparing effect.” Ultrasound Obstet Gynecol 1997; 9:162–172.
48. Gembruch U, Baschat AA. Demonstration of fetal coronary blood flow bycolor-coded and pulsed wave Doppler sonography: a possible indicatorof severe compromise and impending demise in intrauterine growth re-tardation. Ultrasound Obstet Gynecol 1996; 7:10–16.
49. Eik-Nes SH, Brubakk AO, Ulstein MK. Measurement of human fetalblood flow. Br Med J 1980; 280:283–284.
50. Gill RW, Trudinger BJ, Garrett WJ, Kossoff G, Warren PS. Fetal umbili-cal venous flow measured in utero by pulsed Doppler and B-mode ultra-sound in normal pregnancies. Am J Obstet Gynecol 1981; 139:720–725.
51. Hecher K, Campbell S, Snijders R, Nicolaides K. Reference range for fetalvenous and atrioventricular blood flow parameters. Ultrasound Obstet Gy-necol 1994; 4:381–390.
52. Rizzo G, Arduini D, Romanini C. Umbilical vein pulsations: a physiologicfinding in early gestation. Am J Obstet Gynecol 1992; 167:675–677.
53. van Splunder IP, Huisman TWA, Stijnen T, Wladimiroff JW. Presenceof pulsations and reproducibility of waveform recording in the umbilicaland left portal vein in normal pregnancies. Ultrasound Obstet Gynecol 1994;4:49–53.
54. Tekay A, Campbell S. Doppler ultrasonography in obstetrics. In: CallenPW (ed). Ultrasonography in Obstetrics and Gynecology. 4th ed. Philadel-phia, PA: WB Saunders Co; 2000:677–723.
55. Kiserud T, Eik-Nes SH, Hellevic LR, Blaas HG. Ductus venosus: a longi-tudinal Doppler velocimetric study of the human fetus. J Matern Fetal Invest 1992; 2:5–11.
56. Huisman TWA, Stewart PA, Wladimiroff JW. Flow velocity waveformsin the fetal inferior vena cava during the second half of normal pregnancy.Ultrasound Med Biol 1991; 17:679–682.
57. Rizzo G, Arduini D, Caforio L, Romanini C. Effects of sampling sites oninferior vena cava flow velocity waveforms. J Matern Fetal Invest 1992;2:153–156.
58. Brezinca C, Laudy JA, Ursem NT, Hop WC, Wladimiroff JW. Fetal pul-monary venous flow into the left atrium relative to diastolic and systoliccardiac time intervals. Ultrasound Obstet Gynecol 1999; 13:191–195.
59. Laudy JA, Ursem NT, Mulder PG, Wladimiroff JW. Doppler velocime-try of normal human fetal venous intrapulmonary branches. UltrasoundObstet Gynecol 1999; 13:247–254.
60. Weiner Z, Goldberg Y, Shalev E. Internal jugular vein blood flow in nor-mal and growth-restricted fetuses. Obstet Gynecol 2000; 96:167–171.
61. Laurichesse-Delmas H, Grimaud O, Moscoso G, Ville Y. Color Dopplerstudy of the venous circulation in the fetal brain and hemodynamic studyof the cerebral transverse sinus. Ultrasound Obstet Gynecol 1999; 13:34–42.
62. James DK, Parker MJ, Smoleniec JS. Comprehensive fetal assessmentwith three ultrasonographic characteristics. Am J Obstet Gynecol 1992;166:1486–1495.
63. Arduini D, Rizzo G, Romanini C. Changes of pulsatility index from fetalvessels preceding the onset of late decelerations in growth-retarded fe-tuses. Obstet Gynecol 1992; 79:605–610.
64. Reuss ML, Rudolph AM, Dae MW. Phasic blood flow patterns in the su-perior and inferior venae cavae and umbilical vein of fetal sheep. Am J Ob-stet Gynecol 1983; 145:70–78.
65. Rizzo G, Capponi A, Arduini D, Romanini C. The value of fetal arterial,cardiac and venous flow in predicting pH and blood gases in umbilicalblood at cordocentesis in growth-retarded fetuses. Br J Obstet Gynaecol1995; 102:963–969.
66. Gramellini D, Piantelli G, Verrotti C, Fieni S, Delle Chiaie L, Kaihura C.Doppler velocimetry and non-stress test in severe fetal growth restriction.Clin Exp Obstet Gynecol 2001; 28:33–39.
67. Tsuzaki T, Miura H, Maeda K. The study on the individual physical con-dition of the fetuses in multiple pregnancies by pulsed Doppler and non-stress test. Jpn J Med Ultrason 1990; 17(suppl 1):651–652.
68. Indik JK, Chen V, Reed KL. Association of umbilical venous with inferiorvena cava blood flow velocities. Obstet Gynecol 1991; 77:551–557.
69. Schwarze A, Gembruch U, Krapp M, Katalinic A, Germer U, Axt-Flied-ner R. Qualitative venous Doppler flow waveform analysis in preterm in-trauterine growth-restricted fetuses with ARED flow in the umbilicalartery: correlation with short-term outcome. Ultrasound Obstet Gynecol2005; 25:573–579.
70. Cheema R, Dubiel M, Breborowicz G, Gudmundsson S. Fetal cerebral ve-nous Doppler velocimetry in normal and high-risk pregnancy. UltrasoundObstet Gynecol 2004; 24:147–153.
J Ultrasound Med 2011; 30:529–545 543
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 543

71. Gudmundsson S, Huhta JC, Wood DC, Tulzer G, Cohen AW, WeinerS. Venous Doppler ultrasonography in the fetus with nonimmune hy-drops. Am J Obstet Gynecol 1991; 164:33–37.
72. Nakai Y, Miyazaki Y, Matsuoka Y, Matsumoto M, Imanaka M, Ogita S.Pulsatile umbilical venous flow and its clinical significance. Br J Obstet Gy-naecol 1992; 99:977–980.
73. Arduini D, Rizzo G, Romanini C. The development of abnormal heartrate patterns after absent end-diastolic velocity in umbilical artery: analy-sis of risk factors. Am J Obstet Gynecol 1993; 168:43–50.
74. Kiserud T, Eik-Nes SH, Blaas HG, Hellevic LR. Ultrasonographic ve-locimetry of the fetal ductus venosus. Lancet 1991; 338:1412–1414.
75. Heyl W, Funk A, Reineke T, Rath W. Pulsation of blood flow in the um-bilical vein during the second trimester of pregnancy correlated to fetalmalformation and chromosomal aberration. J Perinat Med 1998; 26:278–283.
76. Hofstaetter C, Dubiel M, Gudmundsson S. Two types of umbilical ve-nous pulsations and outcome of high-risk pregnancies. Early Hum Dev2001; 61:111–117.
77. Mitra SC. Umbilical venous Doppler waveform without fetal breathing:its significance. Am J Perinatol 1995; 12:217–219.
78. Di Naro E, Raio L, Ghezzi F, Franchi M, Romano F, d’Addario V. Longi-tudinal umbilical vein blood flow changes in normal and growth-retardedfetuses. Acta Obstet Gynecol Scand 2002; 81:527–533.
79. Ferrazzi E, Rigano S, Bozzo M, et al. Umbilical vein blood flow in growth-restricted fetuses. Ultrasound Obstet Gynecol 2000; 16:432–438.
80. Baschat AA, Gembruch U, Reiss I, Gortner L, Harman CR, Weiner MD.Neonatal nucleated red blood cell counts in growth-restricted fetuses: re-lationship to arterial and venous Doppler studies. Am J Obstet Gynecol1999; 181:190–195.
81. Lees C, Albaiges G, Deane C, Parra M, Nicolaides KH. Assessment ofumbilical arterial and venous flow using color Doppler. Ultrasound ObstetGynecol 1999; 14:250–255.
82. Kiserud T. Venous flow in intrauterine growth restriction and cardiac de-compensation. In: Yagel S, Silverman NH, Gembruch U (eds). Fetal Car-diology. 2nd ed. New York, NY: Informa Healthcare; 2009:547–560.
83. Yagel S, Kivilevitch Z, Cohen SM, et al. Ultrasound evaluation of the fetalvenous system, part II: the fetus with congenital venous system malfor-mation or developing circulatory compromise. Ultrasound Obstet Gynecol2010; 36:93–111.
84. Rigano S, Bozzo M, Ferrazzi E, Bellotti M, Battaglia FC, Galan HL. Earlyand persistent reduction in umbilical vein blood flow in the growth-re-stricted fetus: a longitudinal study. Am J Obstet Gynecol 2001; 185:834–838.
85. Boito S, Struijk PC, Ursem NTC, Fedele L, Wladimiroff JW. Fetalbrain/liver volume ratio and umbilical volume flow parameters relativeto normal and abnormal human development. Ultrasound Obstet Gynecol2003; 21:256–261.
86. Areias JC, Matias A, Montenegro N. Venous return and right ventriculardiastolic function in ARED flow fetuses. J Perinat Med 1998; 26:157–167.
87. Van Eyck TC, Stewart PA, Wladimiroff JW. Human fetal foramen ovale
flow velocity waveforms related to behavioral states in normal term preg-nancy. Am J Obstet Gynecol 1990; 163:1239–1242.
88. Mori A, Trudinger B, Mori R, Reed V, Takeda Y. The fetal central venouspressure waveform in normal pregnancy and in umbilical placental in-sufficiency. Am J Obstet Gynecol 1995; 172:51–57.
89. Rizzo G, Capponi A, Arduini D, Romanini C. Ductus venosus velocitywaveforms in appropriate and small-for-gestational-age fetuses. Early HumDev 1994; 39:15–26.
90. Rizzo G, Arduini D, Romanini C. Inferior vena cava flow velocity wave-forms in appropriate and small-for-gestational-age fetuses. Am J Obstet Gy-necol 1992; 166:1271–1280.
91. Fouron JC, Absi F, Skoll A, Proulx F, Gosselin J. Changes in flow velocitypatterns of the superior and inferior venae cavae during placenta circula-tory insufficiency. Ultrasound Obstet Gynecol 2003; 21:53–56.
92. Baschat AA, Gembruch U, Harman CR. The sequence of changes inDoppler and biophysical parameters as severe fetal growth restrictionworsens. Ultrasound Obstet Gynecol 2001; 18:571–577.
93. Rizzo G, Capponi A, Talone E, Arduini D, Romanini C. Doppler indicesfrom inferior vena cava and ductus venosus in predicting pH and oxygentension in umbilical blood at cordocentesis in growth-restricted fetuses.Ultrasound Obstet Gynecol 1996; 7:401–410.
94. Mori A, Uchida N, Inomo A, Ishiguro Y, Atsuko T, Mikio M. Normal andabnormal diameter pulse waveforms in the fetal inferior vena cava. PrenatDiagn 2007; 27:244–250.
95. Huisman TWA, Brezinka C, Stewart PA, Stijnen T, Wladimiroff JW. Duc-tus venosus flow velocity waveforms in relation to fetal behavioural states.Br J Obstet Gynaecol 1994; 101:220–224.
96. Kiserud T, Hellevic LR, Eik-Nes SH, Anglesen BAJ, Blaas HG. Estima-tion of the pressure gradient across the fetal ductus venosus based onDoppler velocimetry. Ultrasound Med Biol 1994; 20:225–232.
97. Hecher K, Bilardo M, Stigter RH, et al. Monitoring of fetuses with in-trauterine growth restriction: a longitudinal study. Ultrasound Obstet Gy-necol 2001; 18:564–570.
98. Ferrazzi E, Bozzo M, Rigano S, et al. Temporal sequence of abnormalDoppler changes in the peripheral and central circulatory systems of theseverely growth-restricted fetus. Ultrasound Obstet Gynecol 2002; 19:140–146.
99. Kiserud T, Kessler J, Ebbing C, Rasmussen S. Ductus venosus shunting ingrowth-restricted fetuses and the effect of umbilical circulatory compro-mise. Ultrasound Obstet Gynecol 2006; 28:143–149.
100. Tchirikov M, Schröder HJ, Hecher K. Ductus venosus shunting in thefetal venous circulation: regulatory mechanisms, diagnostic methods andmedical importance. Ultrasound Obstet Gynecol 2006; 27:452–461.
101. Baschat AA, Gembruch U, Weiner CP, Harman CR. Qualitative venousDoppler waveform analysis improves prediction of critical perinatal out-comes in premature growth-restricted fetuses. Ultrasound Obstet Gynecol2003; 22:240–245.
102. Baschat AA. Doppler application in the delivery timing of the pretermgrowth-restricted fetus: another step in the right direction. Ultrasound Ob-stet Gynecol 2004; 23:111–118.
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
J Ultrasound Med 2011; 30:529–545544
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 544
103. Figueras F, Martínez JM, Puerto D, Coll O, Cararach V, Vanrell JA. Con-traction stress test versus ductus venosus Doppler evaluation for the pre-diction of adverse perinatal outcome in growth-restricted fetuses withnon-reassuring non-stress test. Ultrasound Obstet Gynecol 2003; 21:250–255.
104. Cosmi E, Visentin S, Fanelli T, Mautone AJ, Zanardo V. Aortic intima-media thickness in fetuses and children with intrauterine growth restric-tion. Obstet Gynecol 2009; 114:1109–1114.
105. Alves SK, Francisco RP, Miyadahira S, Krebs VL, Vaz FA, Zugaib M. Duc-tus venosus Doppler and postnatal outcomes in fetuses with absent or re-versed end-diastolic flow in the umbilical arteries. Eur J Obstet GynecolReprod Biol 2008; 141:100–103.
106. Baschat AA, Galan HL, Bhide A, et al. Doppler and biophysical assess-ment in growth restricted fetuses: distribution of test results. UltrasoundObstet Gynecol 2006;27:41–47.
107. Bilardo CM, Müller MA, Zikulnig L, Schipper M, Hecher K. Ductusvenosus studies in fetuses at high risk for chromosomal or heart abnor-malities: relationship with nuchal translucency measurements and fetaloutcome. Ultrasound Obstet Gynecol 2001; 17:288–294.
108. Müller MA, Pajkrt E, Bleker OP, Bonsel GJ, Bilardo CM. Disappearanceof enlarged nuchal translucency before 14 weeks’ gestation: relationshipwith chromosomal abnormalities and pregnancy outcome. UltrasoundObstet Gynecol 2004; 24:169–174.
109. Baschat AA, Guclu S, Kush ML, Gembruch U, Weiner CP, Harman CR.Venous Doppler in the prediction of acid-base status of growth-restrictedfetuses with elevated placental blood flow resistance. Am J Obstet Gynecol2004; 191:277–284.
110. Mäkikallio K, Acharya G, Erkinaro T, et al. Ductus venosus velocimetry inacute fetal acidemia and impending fetal death in a sheep model of in-creased placental vascular resistance. Am J Physiol Heart Circ Physiol 2010;298:H1229–H1234.
111. Carvalho FHC, Moron AF, Mattar R, et al. Ductus venosus Doppler ve-locimetry in the prediction of acidemia at birth: which is the best param-eter? Prenat Diagn 2005; 25:1212–1216.
112. Hung JH, Fu CY, Hung J. Combination of fetal Doppler velocimetric re-sistance values predict acidemic growth-restricted neonates. J UltrasoundMed 2006; 25:957–962.
113. Hofstaetter C, Gudmundsson S. Venous Doppler in the evaluation offetal hydrops. Obstet Gynecol Int 2010; 2010:430157.
114. Kessler J, Rasmussen S, Godfrey K, Hanson M, Kiserud T. Fetal growthrestriction is associated with prioritization of umbilical blood flow to theleft hepatic lobe at the expense of the right lobe. Pediatr Res 2009; 66:113–117.
115. Kilavuz O, Vetter K, Kiserud T, Vetter P. The left portal vein is the water-shed of the fetal venous system. J Perinat Med 2003; 31:184–187.
116. Kessler J, Rasmussen S, Kiserud T. The left portal vein as an indicator ofwatershed in the fetal circulation: development during the second half ofpregnancy and a suggested method of evaluation. Ultrasound Obstet Gy-necol 2007; 30:757–764.
117. Senat MV, Schwarzler P, Alcais A, Ville Y. Longitudinal changes in theductus venosus, cerebral transverse sinus and cardiotocogram in fetalgrowth restriction. Ultrasound Obstet Gynecol 2000; 16:19–24.
118. Figueroa-Diesel H, Hernandez-Andrade E, Benavides-Serralde A, et al.Cerebral venous blood flow in growth-restricted fetuses with an abnormalblood flow in the umbilical artery before 32 weeks’ gestation. Eur J ObstetGynecol Reprod Biol 2008; 140:201–205.
119. Del Rio M, Martinez JM, Figueras F, et al. Doppler assessment of the aor-tic isthmus and perinatal outcome in preterm fetuses with severe in-trauterine growth restriction. Ultrasound Obstet Gynecol 2008; 31:41–47.
120. Fouron JC, Gosselin J, Raboisson MJ, et al. The relationship between anaortic isthmus blood flow velocity index and the postnatal neurodevel-opmental status of fetuses with placental circulatory insufficiency. Am JObstet Gynecol 2005; 192:497–503.
121. Ichizuka K, Matsuoka R, Hasegawa J, et al. The Tei index for evaluationof fetal myocardial performance in sick fetuses. Early Hum Dev 2005;81:273–279.
122. Crispi F, Hernandez-Andrade E, Pelsers MM, et al. Cardiac dysfunctionand cell damage across clinical stages of severity in growth-restricted fe-tuses. Am J Obstet Gynecol 2008; 199:254.e1–254.e8.
123. Hernandez-Andrade E, Crispi F, Benavides-Serralde JA, et al. Contribu-tion of the myocardial performance index and aortic isthmus blood flowindex to predicting mortality in preterm growth-restricted fetuses. Ultra-sound Obstet Gynecol 2009; 34:430–436.
124. Black RS, Campbell S. Cardiotocography versus Doppler. Ultrasound Ob-stet Gynecol 1997; 9:148–151.
125. Soothill PW, Ajayi RA, Campbell S, Nicolaides KH. Prediction of mor-bidity in small and normally grown fetuses by fetal heart rate variability,biophysical profile score and umbilical artery Doppler studies. Br J ObstetGynaecol 1993; 100:742–745.
126. Turan OM, Turan S, Gungor S, Progression of Doppler abnormalities inintrauterine growth restriction. Ultrasound Obstet Gynecol 2008; 32:160–167.
127. Arduini D, Rizzo G. Prediction of fetal outcome in small-for-gestational-age fetuses: comparison of Doppler measurements obtained from differ-ent fetal vessels. J Perinat Med 1992; 20:29–38.
J Ultrasound Med 2011; 30:529–545 545
Kaponis et al—Venous Doppler Velocimetry in Growth-Restricted Fetuses
304jumvonline.qxp:Layout 1 3/18/11 12:02 PM Page 545




















