
Maternal Olfaction Differentially Modulates Oxytocin and Prolactin Release during Suckling in Goats
Upload
independentCategory
view
1download
0
PHARMACOI<INETICS AND DRUG DISPOSITION
Pharmacolunetics of the novel antipsychotic agent risperidone and the prolactin response in healthy subjects
The pharmacokinetics of a novel antipsychotic agent, risperidone, and the prolactin response were stud- ied in 12 dextromethorphan-phenotyped healthy men after administration of 1 mg risperidone intrave- nously, intramuscularly, and orally. The formation of the equipotent major metabolite, 9-hydroxy- risperidone, exhibited CYP2D6-related polymorphism. The plasma area under the concentration-time curve from time zero to infinity ratio of 9-hydroxyrisperidone to risperidone averaged 3 (intravenous and intramuscular) and 6 (oral administration) in the extensive metabolizers and 0.2 in the poor metab- olizers. Risperidone half-life was about 3 hours in extensive metabolizers and 22 hours in poor metabo- lizers. Risperidone absolute oral bioavailability was 66%. The pharmacokinetics of the active moiety (risperidone plus 9-hydroxyrisperidone) varied little among subjects (mean terminal half-life, 20 + 2% hours; absolute oral and intramuscular bioavailability, 100%). The prolactin response correlated best with the plasma active moiety, which showed little hysteresis. I t is concluded that risperidone metabolic polymorphism on increased plasma prolactin is minimal and that the active moiety is clinically relevant. (CLIN PHARMACOL THER 1993;54:257-68.)
May-Lynn Huang, PhD, Achiel Van Peer, PhD, Robert Woestenborghs, MSc, Roland De Coster, DVM, Jos Heykants, PhD, Arno A. I. Jansen, MS, Zbigniew Zylicz, MD, Hendrik W. Visscher, MSc, and Jan H. G. Jonkman, PhD Beerse, Belg-ium, and Tilburg and Zuidlaren, The Netherlands
Risperidone (see Structure) is a novel antipsychotic agent chemically classified as a benzisoxazole deriva- tive. It is a selective monoaminergic antagonist with high affinity for serotonergic 5-HT, and dopaminergic D, receptors.' Clinical trials in psychotic patients
From the Janssen Research Foundation, Beerse; Janssen Pharma- ceutica B.V., Tilburg; and Pharma Bio-Research, Zuidlaren.
Presented in part at a clinical pharmacologic meeting organized by the Belgian and Dutch Societies of Clinical Pharmacology and Biopharmaceutics, Ghent, Belgium, April 3, 1992, and as a poster at the Fifth European Congress of Biopharmaceutics and Pharmacokinetics, B N S S ~ ~ S , Belgium, April 20-22, 1993.
Received for publication Feb. 10, 1993; accepted May 7, 1993. Reprint requests: May-Lynn Huang, PhD, Department of Pharma-
cokinetics and Drug Metabolism, Janssen Research Foundation, Beerse, Belgium.
Copyright O 1993 by Mosby-Year Book, Inc. 0009-9236/931$1 .OO + 0.10 1311148442
Chemical structure of risperidone.
have shown risperidone to be effective in the treat- ment of the positive, negative, and affective symp- toms of s c h i ~ o ~ h r e n i a . ~ - ~ Furthermore, risperidone therapy is associated with reduced extrapyramidal symptoms. Patients with chronic schizophrenia receiv-
257

2 5 8 Huan. et al. CLINICAL PHARMACOLOGY & THERAPEUTICS
SEPTEMBER 1993
Table I. Subject characteristics
Subject No. Age (yr) Sex Weight (kg) Height (cm) Smoker Dextromethorphanlmetabolic ratio
1 22 Male 74 179 No 0.004 2 23 Male 73 183 Yes 0.015 3 23 Male 7 1 185 Yes 0.002 4 20 Male 72 186 Yes 0.0002 5 22 Male 76 187 No 0.002 6 23 Male 69 180 Yes 5.355 7 24 Male 78 176 No 0.002 8 20 Male 79 192 No 0.004 9 19 Male 62 177 No 0.005
10 26 Male 71 183 Yes 0.001 11 24 Male 76 190 No 6.463 12 4 1 Male 76 189 No 0.122
Mean ? SD 24 * 6 - 73 2 5 184 ? 5 - - Minimum 19 - 62 176 - 0.0002 Maximum 4 1 - 79 192 - 6.463
ing risperidone treatment required 10 times less anti- parkinsonian medication compared with those receiv- ing haloperidol treatment.4
In humans, risperidone is metabolized mainly by the liver. The major pathways (in order of preference) include 9-hydroxylation (at the alicyclic site of the py- rimidinone ring), N-dealkylation (at the piperidine ni- trogen), and 7-hydroxylation (also at the alicyclic site of the pyrimidinone ring). An earlier study in three healthy volunteers indicated that the formation of 9-hydroxyrisperidone is related to the debrisoquin ox- idative status of the subjects (Mannens G, et al. Un- published data, February 1993).
Standard pharmacology tests performed in rats and dogs showed 9-hydroxyrisperidone to be about as equipotent as ri~peridone.~ Other metabolites did not exhibit significant pharmacologic activities. Thus, in vivo, both risperidone and 9-hydroxyrisperidone (the sum of which is hereafter referred to as the active moiety) could account for the pharmacologic re- sponses after the administration of risperidone.
Therefore one of the aims of this study was to ex- amine the relationship of risperidone and the active moiety with respect to the debrisoquin-type metabolic polymorphism. The subjects in this study were pheno- typed to include poor, intermediate, and extensive me- tabolizers of dextromethorphan because this substance has been shown to be an alternative to debrisoquin for phenotyping the cytochrome P450 IID6-related meta- bolic status of the subject^.^ Furthermore, because prolactin release from the anterior pituitary is mainly under the tonic inhibitory control of d ~ ~ a m i n e , ~ we also studied the prolactin responses in these subjects. This could provide a direct assessment of the impact
of metabolic polymorphism on one of the pharmaco- logic responses of risperidone.
METHODS Subjects and treatment plan. Twelve healthy male
subjects participated in the study after each signed an informed consent form. The study was approved by the Medical Ethics Committee in Assen, The Nether- lands. Before the trial, the subjects took 22 mg dex- tromethorphan to determine their dextromethorphan metabolic ratios (MR), which were calculated as the 8-hour urinary recovery ratios of dextromethorphan to de~trorphan.~ The bimodal distribution of the dextro- methorphan metabolic ratio has an antimode of MR at about 0.3 in a white population.6 Two of our subjects (Nos. 6 and 11) who each had an MR > 1 were clas- sified as poor metabolizers. One subject (No. 12) had an MR of 0.12, close to the antimode was classified as an intermediate metabolizer. Nine of the subjects who each had an MR between 0.0002 and 0.015 were clas- sified as extensive metabolizers. Average age (+SD) of the subjects was 24 + 6 years (age range, 19 to 41 years); average body weight was 73 + 5 kg (weight range, 62 to 79 kg), and average body height was 184 + 5 cm (height range, 176 to 192 cm). Details of subject characteristics are listed in Table I.
According to a randomized crossover scheme, sub- jects received three treatments (intravenous, intramus- cular, and oral administration) of 1 mg risperidone. The washout period between treatments was 2 weeks. Before each treatment, subjects underwent an over- night fast of at least 10 hours. The intravenous infu- sion (over 30 minutes) was performed with use of an IVAC 700 syringe pump (IVAC Corp., San Diego,

CLINICAL PHARMACOLOGY & TIIERAPEUTICS VOLUME 54, NUMBER 3 Huang e t al. 259
100 - 1m 100
E : - P : - E ai E p 10 F lo ai c 0
i? .- n L ? $ 1 V)
1 ,- .- s Y
1 1 0 12 24 36 48 60 72 0 12 24 36 48 60 72 0 12 24 36 48 60 72
Hours Hours Hours
Fig. 1. Plasma concentrations of risperidone (left graph), 9-hydroxyrisperidone (middle graph), and active moiety (i.e., risperidone plus 9-hydroxyrisperidone) (right graph) in 12 healthy sub- jects after an intravenous infusion (30 minutes) of 1 mg risperidone. Subjects 6 (squares) and 11 (triangles) are poor metabolizers and subject 12 (circles) is an intermediate metabolizer of dextro- methorphan. The extensive metabolizers are shown by solid lines.
Table 11. Essential pharmacokinetic parameters of risperidone based on compartmental analysis in healthy volunteers after an intravenous infusion of 1 mg risperidone
Poor metabolizers (n = 2)* Parameters Extensive metabolizers (n = 9)" Intermediate metabolizer (n = I)* Subject 6 Subject 11
V, (L) 20.9 L 7.3 Vss (L) 80.6 ? 10.1 VSS (Llkg) 1.1 * 0.2 Vma (L) 91.8 * 14.1 v,, ( L k ) 1.3 ? 0.2 CL (mllmin) 394 2 107 CL (mllminlkg) 5.4 ? 1.4
V,, Volume of the central compartment; V,,, steady-state volume of distribution; V,,, area-based volume of distribution; CL, total plasma clearance *The dextromethorphan metabolic ratios of the subjects are listed in Table I.
Calif.). A 2 mglml sterile risperidone solution was re- constituted with sterile isotonic saline solution just be- fore the intravenous and intramuscular administration. For oral administration, subjects took an oral solution of risperidone and 200 ml water. Each medication was administered at approximately 8 AM in the morning. Subjects fasted until 2 hours after administration when a standard breakfast was given. A lunch was served 5 hours and a dinner 10 hours after administration. In addition, subjects fasted overnight before each of the morning blood samplings at 24, 48, and 72 hours after administration. As a precautionary measure for ortho- static hypotension, subjects remained in the supine po- sition until 4 hours after drug administration.
Blood sampling and urine collection. Blood sam- ples (8 ml each) for drug and prolactin measurements were collected in heparinized tubes just before drug administration and at 8, 15, 30 minutes and at 1, 1 %, 2, 3, 5, 8, 12, 16, 24, 36, 48, and 72 hours after drug
administration. For the intravenous infusion, addi- tional blood samples were collected at 10, 20, and 30 minutes after the start of infusion. Urine was collected from - 12 to 0 hour and at several time intervals up to 72 hours after drug administration. Aliquots of urine collection were frozen at -20" C until analysis.
Radioimmunoassay of risperidone and Phydroxy- risperidone. To measure the very low plasma concen- trations of risperidone and to measure the concentra- tions of active moiety, two radioimmunoassays (RIA) were developed and used for the analysis of the plasma samples. The plasma samples were either ex- tracted at pH 10 by use of heptanelisoamyl alcohol (98.5 : 1.5, vol/vol) and analyzed by use of a specific antiserum for the determination of the unchanged drug (RIA-I), or analyzed by a direct RIA with use of the antiserum against 9-hydroxyrisperidone for the mea- surement of the active moiety, that is, risperidone plus 9-hydroxyrisperidone (RIA-11). The plasma concentra-
CLINICAL. PHARMACOLOGY &THERAPEUTICS SEFTEMBER 1993
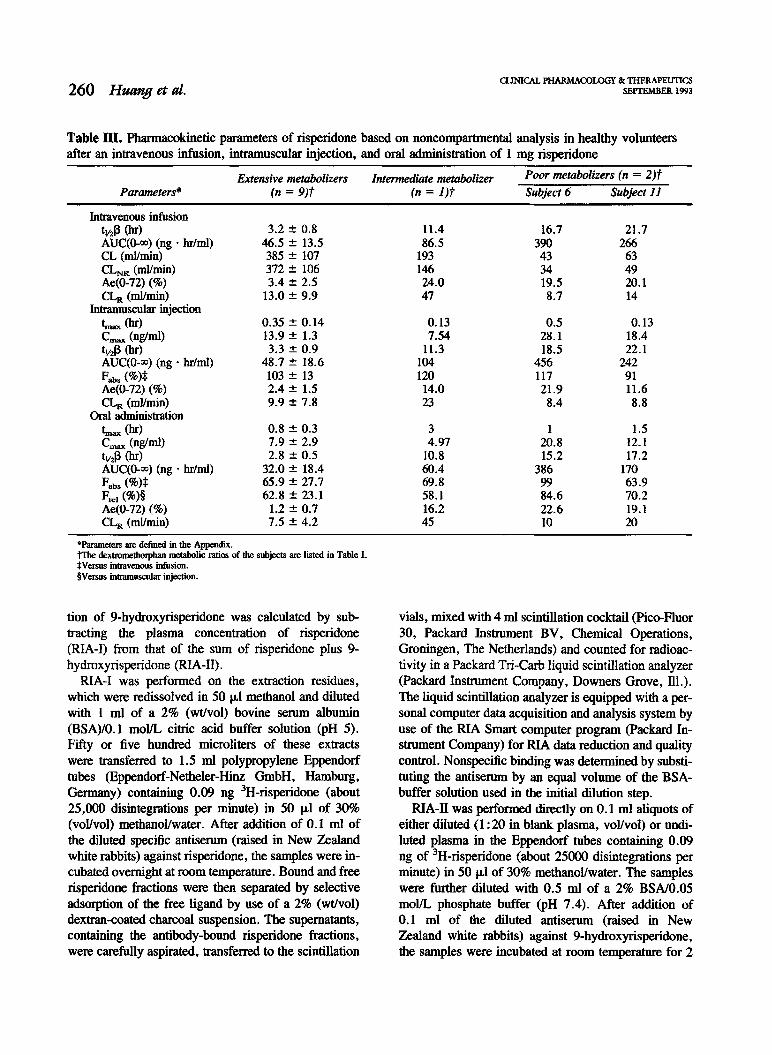
Table 111. Pharmacokinetic parameters of risperidone based on noncompartmental analysis in healthy volunteers after an intravenous infusion, intramuscular injection, and oral administration of 1 mg risperidone
Extensive metabolizers Intermediate metabolizer Poor metabozizers fn = 2)f Parameters* (n = 9)f fn = I )? Subject 6 Subject 11
*Parameters are defined in the Appendix. trip dextromethorphan metabolic ratios of the subjects are listed in Table I. $Versus intravenous infusion. Oversus intramuscular injection.
tion of 9-hydroxyrisperidone was calculated by sub- tracting the plasma concentration of risperidone (RIA-I) from that of the sum of risperidone plus 9- hydroxyrisperidone (RIA-11) .
RIA-I was performed on the extraction residues, which were redissolved in 50 p1 methanol and diluted with 1 ml of a 2% (Wvol) bovine serum albumin (BSA)/O.l mom citric acid buffer solution (pH 5). Fifty or five hundred microliters of these extracts were transferred to 1.5 ml polypropylene Eppendorf tubes (Eppendorf-Netheler-Hinz GmbH, Hamburg, Germany) containing 0.09 ng 3~-risperidone (about 25,000 disintegrations per minute) in 50 p1 of 30% (voYvol) methanollwater. After addition of 0.1 ml of the diluted specific antisem (raised in New Zealand white rabbits) against risperidone, the samples were in- cubated overnight at room temperature. Bound and free risperidone fractions were then separated by selective adsorption of the free ligand by use of a 2% (wt/vol) dextran-coated charcoal suspension. The supernatants, containing the antibody-bound risperidone fractions, were carefully aspirated, transferred to the scintillation
vials, mixed with 4 ml scintillation cocktail (Pico-Fluor 30, Packard Instrument BV, Chemical Operations, Groningen, The Netherlands) and counted for radioac- tivity in a Packard Tri-Carb liquid scintillation analyzer (Packard Instrument Company, Downers Grove, Ill.). The liquid scintillation analyzer is equipped with a per- sonal computer data acquisition and analysis system by use of the RIA Smart computer program (Packard In- strument Company) for RIA data reduction and quality control. Nonspecific binding was determined by substi- tuting the antiserum by an equal volume of the BSA- buffer solution used in the initial dilution step.
RIA-II was performed directly on 0.1 ml aliquots of either diluted (1 :20 in blank plasma, vollvol) or undi- luted plasma in the Eppendorf tubes containing 0.09 ng of 3~-risperidone (about 25000 disintegrations per minute) in 50 pl of 30% methanol/water. The samples were further diluted with 0.5 ml of a 2% BSAlO.05 mom phosphate buffer (pH 7.4). After addition of 0.1 ml of the diluted antiserum (raised in New Zealand white rabbits) against 9-hydroxyrisperidone, the samples were incubated at room temperature for 2

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 54, NUMBER 3 Huan. et al. 26 1
Table IV. Pharmacokinetic parameters of 9-hydroxyrisperidone based on noncompartmental analysis in healthy volunteers after an intravenous infusion, intramuscular injection, and oral administration of 1 mg risperidone
Extensive metabolizers Intermediate metabolizer metabO1izers (n = 2)f Parameters* (n = 9 ) f (n = 1)f Subject 6 Subject I1
Intravenous infusion C,,, (nglml) tmax (hr) tl/2P (hr) AUC(0-w) (ng . hrlml) AUC(0-w) ratio* Ae(0-72) (%) CL, (mllmin)
Intramuscular injection Lax (hr) C,,, (nglml) f l/2P (hr) AUC(0-w) (ng . hrlml) AUC(0-30) ratio* Ae(0-72) (%) CL, (mllmin)
Oral administration Lax (hr) C,,, (nglml) tl/2P (hr) AUC(0-m) (ng , hrlml) AUC(0-a) ratio* Ae(0-72) (%) CL, (mllmin)
NA, Not assessable. *Parameters are defined in the Appendix. tThe dextromethorphan metabolic ratios of the subjects are listed in Table I . $Plasma AUC(0-m) ratio of 9-hydroxyrisperidone to risperidone.
Table V. Pharmacokinetic parameters of the active moiety (i.e., risperidone plus 9-hydroxyrisperidone) based on noncompartmental analysis in 12 subjects after an intravenous infusion, intramuscular injection, and oral administration of 1 mg risperidone
Parameters* Intravenous infusion Intramuscular injection Oral administration
*Parameters are defined in the Appendix. Wersus intravenous infusion. $Versus intramuscular injection.
hours. Bound and free ligands were separated by se- lective adsorption of the free ligand as described in RIA-I. The supernatants, containing the antibody- bound risperidone and 9-hydroxyrisperidone fractions, were transferred to the scintillation vials and subject to the same subsequent treatments as described in RIA-I.
Standard calibration curves (obtained by four- parameter logistic curve-fitting) were generated for
RIA-I and RIA-11, each with use of blank plasma and plasma standards spiked with risperidone ranging from 0.02 to 50 ngtml. The concentrations in the plasma samples were calculated by interpolation from these daily calibration curves. The cross-reactivities of the 9-hydroxyrisperidone (relative to risperidone) in RIA-I and RIA-I1 were 11150 and 111, respectively. The ab- solute detection limit (10% inhibition of tracer bind-

262 Huang et al. CLINICAL PHARMACOLOGY & THERAPEUTICS
SEMEMBER 1993
.001-1 . ......., . ......., . ......., . . . . . . . . . ...- .0001 .001 .01 .1 1 10
Dextromethorphan metabolic ratios
Fig. 2. Correlation between the logarithm of the nonrenal plasma clearance of risperidone (upper graph) and the log- arithm of the urinary recovery ratio of risperidone to 9- hydroxyrisperidone (lower graph) and the logarithm of the dextromethorphan metabolic ratio of the subjects after intra- venous (open squares), intramuscular (closed circles), and oral administration (open circles). The solid lines are the best-fitted lines for the regressions (see text).
ing) was about 20 pg for both RIA-I and RIA-11. The practical quantification limits were 0.10 nglml for RIA-I and 0.20 ng/ml for RIA-11. The accuracy and reproducibility of both methods were calculated by replicate analysis of quality control samples. For RIA-I, the mean interassay coefficient of variation was 14.9% at 0.205 ng/ml and 12.3% at 2.56 nglml. For RIA-11, the mean interassay coefficients of varia-
tion were 15.9% and 12.5% at 2.26 and 7.69 ng/ml, respectively. Intra-assay coefficients of variation for both assays ranged from 6.8% to 11.8%. The mean relative errors at 0.205 and 2.56 nglml were +9.1% and -2.4% for RIA-I and -1.4% and -2.9% for RIA-11.
HPLC determination of risperidone and 9-hydroxy- risperidone. The concentrations of risperidone and 9-hydroxyrisperidone in the urine samples were mea- sured by an HPLC m e t h ~ d . ~ The urine samples were extracted and injected onto a reversed-phase CI8 col- umn coupled with an ultraviolet detector operating at 280 nm. The detection limits of the HPLC assay were 2.5 ng/ml for risperidone and 10 nglml for 9-hydroxy- risperidone. The overall assay precision for the quality control samples was less than 10%.
Prolactin determination. Plasma prolactin was de- termined by a direct time-resolved immunofluoromet- ric assay by use of a commercially available kit (Delfia Pharmacia, Brussels, Belgium). The dynamic range of the assay was 0.25 to 250 nglml. The intra- assay variabilities (coefficient of variation) of the quality control samples were between 8.2% and 12%.
Pharmacokinetic analysis. The plasma concentra- tion- time data of risperidone after the intravenous ad- ministration were fitted to an open multicompartment model with a zero-order input into the central com- partment (i.e., a 30-minute, constant-rate infusion) by use of the nonlinear regression program EL SF IT.^ The program applies extended least-squares in data fitting to estimate the parameters of the model. A variance model that includes the inverse square of the observed plasma concentration was used to define the weighting scheme. The Marquardt algorithm was used for the numeric iteration during fitting. The initial estimates of the model parameters were calculated by use of the method of residuals.1° Goodness of fit was judged by the standard deviations of the estimated parameters and by visual inspection of the weighted residuals be- tween observed and predicted plasma concentrations. The volume of the central compartment (Vc), steady- state and area-based volumes of distribution (V,, and V,,), and total plasma clearance (CL) were calcu- lated by use of the following equations, which were derived from a two-compartment model (in which plasma concentration [C] as a function of time [t] were described as C = Ae-"' + ~ e - ~ ' ) " :

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 54, NUMRER 3 Huang et al. 263
Intravenous Intramuscular Oral administration
Dextromethorphan metabolic ratios
Fig. 3. Correlation between the logarithm of the area under the plasma concentration-time curve extrapolated to infinity [AUC(O-m)] of risperidone (open symbols) and risperidone plus 9-hydroxy- risperidone (i.e., the active moiety, closed symbols) and the logarithm of dextromethorphan met- abolic ratio of the subject after intravenous (left graph), intramuscular (middle graph), and oral administration (right graph). The solid and broken lines are the best-fitted lines for the regres- sions (see text).
0 -1 I I 1
0 6 12 18 24 30 36 42 48 54 60 66 72
Hours
Fig. 4. Average plasma concentration of prolactin in 12 healthy subjects after intravenous (trian- gles), intramuscular (squares), and oral (circles) administration of 1 mg risperidone.
in which k,, and k,, are micro-rate constants of drug transfer to and from the peripheral compartment and AUC(0-m) is the area under the best-fitted curve of the plasma concentration-time data. The calculation of the micro-rate constants and the parameters for one- and three-compartment models are described by Gibaldi and Perrier.1°
Noncompartmental parameters (see Appendix) are also analyzed for risperidone, 9-hydroxyrisperidone, and the active moiety. Selected noncompartmental pa-
rameters (maximum concentration [C,,,], time to reach C,,, [t,,,], and AUC) were calculated for the plasma concentration-time profiles of prolactin. Statis- tical analyses were performed by means of linear re- gression (for log-transformed parameters versus log of MR) and ANOVA (for comparison of parameters from the three treatments) of the SAS computer soft- ware." A general linear model that included subject, period, first-order carryover (sequence), and treatment as factors was used in the ANOVA. The significant
264 Huang e t al. CLINICAL PHARMACOLOGY & THERAPEUTICS
SEITEMBER 1993
0.0001 0.001 0.01 0.1 1 10
Dextromethorphan metabolic ratios
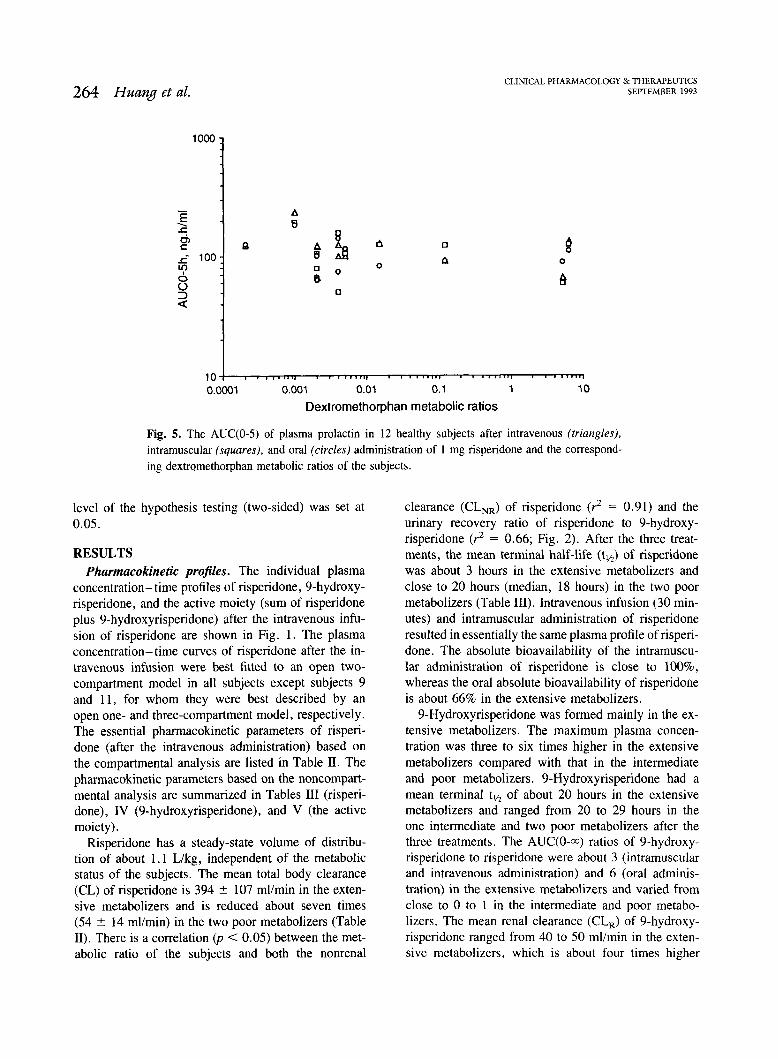
Fig. 5. The AUC(0-5) of plasma prolactin in 12 healthy subjects after intravenous (triangles), intramuscular (squares), and oral (circles) administration of 1 mg risperidone and the correspond- ing dextr~methorphan metabolic ratios of the subjects.
level of the hypothesis testing (two-sided) was set at 0.05.
RESULTS Pharmacokinetic profiles. The individual plasma
concentration- time profiles of risperidone, 9-hydroxy- risperidone, and the active moiety (sum of risperidone plus 9-hydroxyrisperidone) after the intravenous infu- sion of risperidone are shown in Fig. 1. The plasma concentration- time curves of risperidone after the in- travenous infusion were best fitted to an open two- compartment model in all subjects except subjects 9 and 11, for whom they were best described by an open one- and three-compartment model, respectively. The essential pharmacokinetic parameters of risperi- done (after the intravenous administration) based on the compartmental analysis are listed in Table 11. The pharmacokinetic parameters based on the noncompart- mental analysis are summarized in Tables I11 (risperi- done), IV (9-hydroxyrisperidone), and V (the active moiety).
Risperidone has a steady-state volume of distribu- tion of about 1.1 Llkg, independent of the metabolic status of the subjects. The mean total body clearance (CL) of risperidone is 394 & 107 mllmin in the exten- sive metabolizers and is reduced about seven times (54 2 14 mllmin) in the two poor metabolizers (Table 11). There is a correlation ( p < 0.05) between the met- abolic ratio of the subjects and both the nonrenal
clearance (CL,,) of risperidone (? = 0.91) and the urinary recovery ratio of risperidone to 9-hydroxy- risperidone (r2 = 0.66; Fig. 2). After the three treat- ments, the mean terminal half-life (t,/,) of risperidone was about 3 hours in the extensive metabolizers and close to 20 hours (median, 18 hours) in the two poor metabolizers (Table 111). Intravenous infusion (30 min- utes) and intramuscular administration of risperidone resulted in essentially the same plasma profile of risperi- done. The absolute bioavailability of the intramuscu- lar administration of risperidone is close to loo%, whereas the oral absolute bioavailability of risperidone is about 66% in the extensive metabolizers.
9-Hydroxyrisperidone was formed mainly in the ex- tensive metabolizers. The maximum plasma concen- tration was three to six times higher in the extensive metabolizers compared with that in the intermediate and poor metabolizers. 9-Hydroxyrisperidone had a mean terminal tl,, of about 20 hours in the extensive metabolizers and ranged from 20 to 29 hours in the one intermediate and two poor metabolizers after the three treatments. The AUC(0-a) ratios of 9-hydroxy- risperidone to risperidone were about 3 (intramuscular and intravenous administration) and 6 (oral adminis- tration) in the extensive metabolizers and varied from close to 0 to 1 in the intermediate and poor metabo- lizers. The mean renal clearance (CL,) of 9-hydroxy- risperidone ranged from 40 to 50 mllmin in the exten- sive metabolizers, which is about four times higher
CLINICAL. PHARMACOLOGY & THERAPEUTICS VOLUME 54. NUMBER 3 Huang. et al. 265
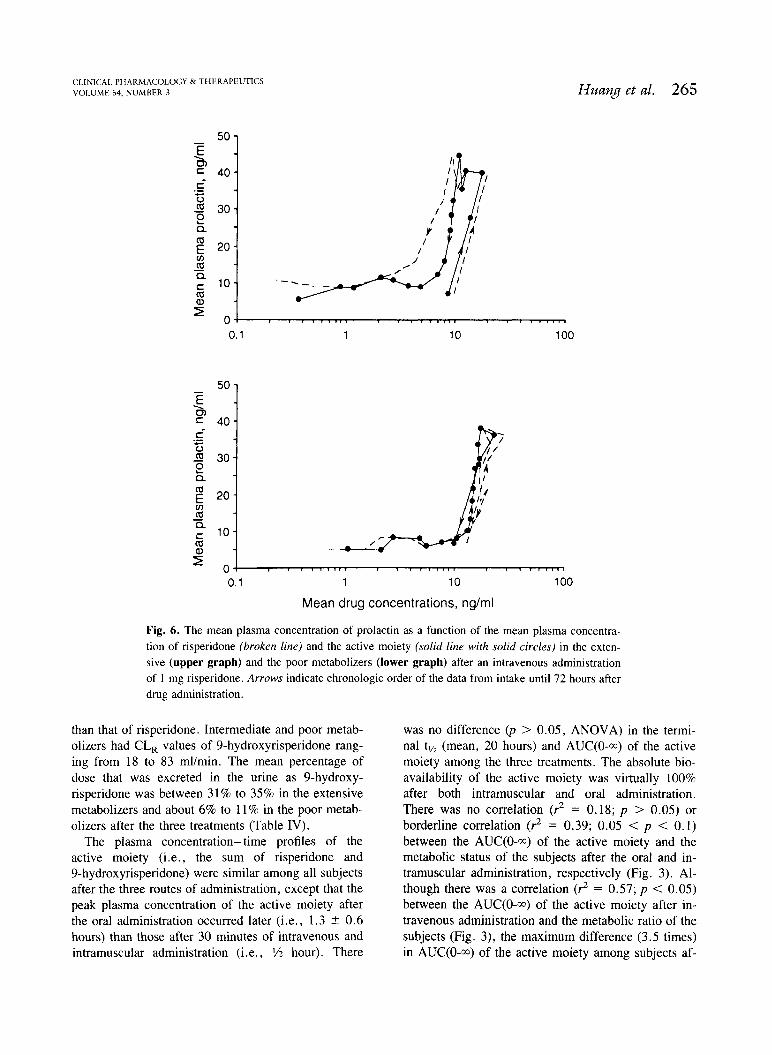
Mean drug concentrations, nglml
Fig. 6 . The mean plasma concentration of prolactin as a function of the mean plasma concentra- tion of risperidone (broken line) and the active moiety (solid line with solid circles) in the exten- sive (upper graph) and the poor metabolizers (lower graph) after an intravenous administration of 1 mg risperidone. Arrows indicate chronologic order of the data from intake until 72 hours after drug administration.
than that of risperidone. Intermediate and poor metab- olizers had CL, values of 9-hydroxyrisperidone rang- ing from 18 to 83 mllmin. The mean percentage of dose that was excreted in the urine as 9-hydroxy- risperidone was between 31% to 35% in the extensive metabolizers and about 6% to 11% in the poor metab- olizers after the three treatments (Table IV).
The plasma concentration-time profiles of the active moiety (i.e., the sum of risperidone and 9-hydroxyrisperidone) were similar among all subjects after the three routes of administration, except that the peak plasma concentration of the active moiety after the oral administration occurred later (i.e., 1.3 t- 0.6 hours) than those after 30 minutes of intravenous and intramuscular administration (i.e., 1/2 hour). There
was no difference ( p > 0.05, ANOVA) in the termi- nal tl/, (mean, 20 hours) and AUC(0-m) of the active moiety among the three treatments. The absolute bio- availability of the active moiety was virtually 100% after both intramuscular and oral administration. There was no correlation (3 = 0.18; p > 0.05) or borderline correlation (2 = 0.39; 0.05 < p < 0.1) between the AUC(0-m) of the active moiety and the metabolic status of the subjects after the oral and in- tramuscular administration, respectively (Fig. 3). Al- though there was a correlation (3 = 0.57; p < 0.05) between the AUC(0-a) of the active moiety after in- travenous administration and the metabolic ratio of the subjects (Fig. 3), the maximum difference (3.5 times) in AUC(0-m) of the active moiety among subjects af-

CLINICAL PHARMACOLOGY & THERAPEUTICS SEPTEMBER 1993
.1 1 10 100 Mean active moiety, ng/ml
Fig. 7. The mean * SD plasma concentration of prolactin as a function of the mean plasma concentration of the ac- tive moiety in all 12 subjects after intravenous (triangles), intramuscular (squares), and oral (circles) administration of 1 mg risperidone.
ter intravenous administration was half of the average difference in AUC(0-m) of risperidone between poor and extensive metabolizers.
Plasma proluctin profiles. Except for a slightly later onset after the oral risperidone intake, the plasma concentration- time profiles of prolactin were similar among all subjects after the three routes of administra- tion (Fig. 4). In general, the prolactin increase was rapid. Mean maximum concentrations of prolactin (about 40 ng/ml) occurred at the same time as that of the active moiety for each route of administration. It returned to the upper limit of the normal range (16 r?g/ml) within 5 hours after the drug administration. There was no correlation ( p > 0.05) between the AUC(0-5) of prolactin and the metabolic ratio of the subjects (Fig. 5). Furthermore, no difference ( p > 0.05, ANOVA) was found in either C,,, or AUC(0-5) among the three treatments.
Fig. 6 shows prolactin as a function of the plasma concentration of risperidone and the active moiety in the extensive and poor metabolizers after the intrave- nous administration. The anticlockwise hysteresis seen in the extensive metabolizers when the prolactin con- centration was plotted against the plasma concentra- tion of risperidone diminished when it was plotted against the plasma concentration of the active moiety. In poor metabolizers, very little hysteresis was seen
whether prolactin was plotted against risperidone or the active moiety. Pooling all subjects from the three routes of administration together, the drug concentra- tion-response curve of prolactin rises above an active moiety concentration of about 7 ng/ml (Fig. 7). Within the concentration range seen in the study, no plateauing of the response was reached.
DISCUSSION Many drug compounds have been reported to be
metabolized by the genetically polymorphic cyto- chrome P450 IID6 system.'* The metabolism of a drug must show a rather high degree of specificity for one enzyme or isozyme that exhibits genetic polymor- phism before such a polymorphism could be observed in the kinetics of the drug itself.13 In our study, the CL,, (i.e., metabolic clearance) of risperidone ac- counted for more than 80% of the CL in the exten- sive metabolizers. Furthermore, 9-hydroxyrisperidone, which amounts to about 35% of the total dose in our study (Table IV), was found to be the most abundant species in the urine of the extensive metabolizers in an earlier study (Mannens G, et al. Unpublished data, February 1993). In contrast, poor metabolizers, lack- ing or having insufficient quantity of the enzyme in question, had a sevenfold smaller CL of risperidone compared with the extensive metabolizers (Table 11). It is clear that other routes of elimination for risperidone, including N-dealkylation and renal excretion, were far less efficient than the 9-hydroxylation process.
9-Hydroxyrisperidone, on the other hand, was re- moved mainly by renal excretion, inasmuch as very little or no further metabolism or conjugation products were found in the urine or feces of volunteers in an earlier study (Mannens G, et al. Unpublished data, February 1993). The renal clearance of 9-hydroxy- risperidone observed in most subjects was about three to four times that of risperidone and approximates the CL of risperidone observed in poor metabolizers (Tables I1 and IV). Although no administration of 9-hydroxy- risperidone was performed for a direct assessment of its kinetics, the terminal tl/, of 9-hydroxyrisperidone in the extensive metabolizers after the administration of risperidone (between 20 and 22 hours) is comparable to that of risperidone in the poor metabolizers. The exact tissue distribution profile may differ between risperi- done and 9-hydroxyrisperidone5; however, based on kinetic principles,1° one could infer that the volume of distribution of 9-hydroxyrisperidone may approximate, in order of magnitude, that of risperidone (1.1 Wkg).
As a result of the kinetic properties of risperidone and 9-hydroxyrisperidone discussed above, intersub-
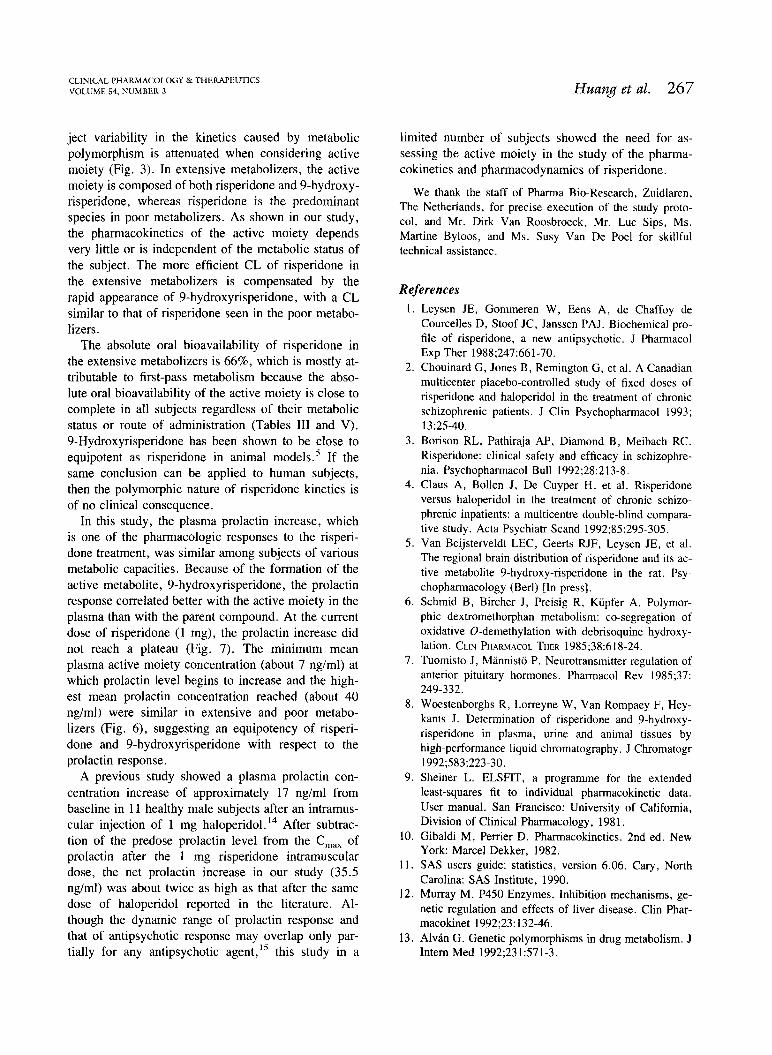
CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 54, NUMBER 3 Huang et al. 267
ject variability in the kinetics caused by metabolic polymorphism is attenuated when considering active moiety (Fig. 3). In extensive metabolizers, the active moiety is composed of both risperidone and 9-hydroxy- risperidone, whereas risperidone is the predominant species in poor metabolizers. As shown in our study, the pharmacokinetics of the active moiety depends very little or is independent of the metabolic status of the subject. The more efficient CL of risperidone in the extensive metabolizers is compensated by the rapid appearance of 9-hydroxyrisperidone, with a CL similar to that of risperidone seen in the poor metabo- lizers.
The absolute oral bioavailability of risperidone in the extensive metabolizers is 66%, which is mostly at- tributable to first-pass metabolism because the abso- lute oral bioavailability of the active moiety is close to complete in all subjects regardless of their metabolic status or route of administration (Tables I11 and V). 9-Hydroxyrisperidone has been shown to be close to equipotent as risperidone in animal models.' If the same conclusion can be applied to human subjects, then the polymorphic nature of risperidone kinetics is of no clinical consequence.
In this study, the plasma prolactin increase, which is one of the pharmacologic responses to the risperi- done treatment, was similar among subjects of various metabolic capacities. Because of the formation of the active metabolite, 9-hydroxyrisperidone, the prolactin response correlated better with the active moiety in the plasma than with the parent compound. At the current dose of risperidone (1 mg), the prolactin increase did not reach a plateau (Fig. 7). The minimum mean plasma active moiety concentration (about 7 nglml) at which prolactin level begins to increase and the high- est mean prolactin concentration reached (about 40 nglml) were similar in extensive and poor metabo- lizers (Fig. 6), suggesting an equipotency of risperi- done and 9-hydroxyrisperidone with respect to the prolactin response.
A previous study showed a plasma prolactin con- centration increase of approximately 17 nglml from baseline in 11 healthy male subjects after an intramus- cular injection of 1 mg haloperidol.14 After subtrac- tion of the predose prolactin level from the C,,, of prolactin after the 1 mg risperidone intramuscular dose, the net prolactin increase in our study (35.5 nglml) was about twice as high as that after the same dose of haloperidol reported in the literature. Al- though the dynamic range of prolactin response and that of antipsychotic response may overlap only par- tially for any antipsychotic agent,15 this study in a
limited number of subjects showed the need for as- sessing the active moiety in the study of the pharma- cokinetics and pharmacodynamics of risperidone.
We thank the staff of Pharma Bio-Research, Zuidlaren, The Netherlands, for precise execution of the study proto- col, and Mr. Dirk Van Roosbroeck, Mr. Luc Sips, Ms. Martine Byloos, and Ms. Susy Van De Poel for skillful technical assistance.
References Leysen JE, Gommeren W, Eens A, de Chaffoy de Courcelles D, Stoof JC, Janssen PAJ. Biochemical pro- file of risperidone, a new antipsychotic. J Pharmacol Exp Ther 1988;247:661-70. Chouinard G, Jones B, Remington G, et al. A Canadian multicenter placebo-controlled study of fixed doses of risperidone and haloperidol in the treatment of chronic schizophrenic patients. J Clin Psychopharmacol 1993; l3:25-40. Borison RL, Pathiraja AP, Diamond B, Meibach RC. Risperidone: clinical safety and efficacy in schizophre- nia. Psychopharmacol Bull 1992;28:213-8. Claus A, Bollen J, De Cuyper H, et al. Risperidone versus haloperidol in the treatment of chronic schizo- phrenic inpatients: a multicentre double-blind compara- tive study. Acta Psychiatr Scand 1992;85:295-305. Van Beijste~eldt LEC, Geerts RJF, Leysen JE, et al. The regional brain distribution of risperidone and its ac- tive metabolite 9-hydroxy-risperidone in the rat. Psy- chopharmacology (Berl) [In press]. Schmid B, Bircher J, Preisig R, Kiipfer A. Polymor- phic dextromethorphan metabolism: co-segregation of oxidative 0-demethylation with debrisoquine hydroxy- lation. CLIN PHARMACOL THER 1985;38:618-24. Tuornisto J, Mannisto P. Neurotransmitter regulation of anterior pituitary hormones. Pharmacol Rev 1985;37: 249-332. Woestenborghs R, Lorreyne W, Van Rompaey F, Hey- kants J. Determination of risperidone and 9-hydroxy- risperidone in plasma, urine and animal tissues by high-performance liquid chromatography. J Chromatogr 1992;583:223-30. Sheiner L. ELSFIT, a programme for the extended least-squares fit to individual pharmacokinetic data. User manual. San Francisco: University of California, Division of Clinical Pharmacology, 198 1. Gibaldi M, Perrier D. Pharmacokinetics. 2nd ed. New York: Marcel Dekker, 1982. SAS users guide: statistics, version 6.06. Cary, North Carolina: SAS Institute, 1990. Murray M. P450 Enzymes. Inhibition mechanisms, ge- netic regulation and effects of liver disease. Clin Phar- macokinet l992;23: 132-46. Alvin G. Genetic polymorphisms in drug metabolism. J Intern Med l992;23 1 :57 1-3.

268 Huang et al. CLINICAL PHARMACOLOGY & THERAPEUTICS
SEPTEMBER 1993
14. Langer G, Sachar EJ, Halpern FS, Gruen PH, Solomon M. The prolactin response to neuroleptic drugs. A test of dopaminergic blockade: neuroendocrine studies in normal men. J Clin Endocrinol Metab 1977;45:996- 1002.
15. Van Putten T, Marder SR, Mintz J. Serum prolactin as a correlate of clinical response to haloperidol. J Clin Psychopharmacol 1991;11:357-61.
APPENDIX Description of the noncompartmental parameters
Cmax Peak plasma concentration, determined as the highest concentration of the plasma concen- tration-time data.
L a x Time to reach C,,. ~ V Z P Terminal half-life, defined as 0.693lP in
which P is the elimination rate constant, which is the slope of the terminal log (natural logarithm)/linear concentration- time curve.
AUC(0-t) Area under the plasma concentration-time curve, calculated by trapezoidal summation up to time point t.
AUC(0-m) Area under the plasma concentration-time
Absolute bioavailability, defined as the AUC(0-m) ratio ( X 100%) of intramuscular and oral administration to intravenous admin- istration. Relative bioavailability, defined as the AUC(0-m) ratio ( X 100%) of oral to intra- muscular administration Total plasma clearance (only for risperidone after a 1 mg intravenous dose), calculated as the ratio of the intravenous dose (1 mg) to the plasma AUC(0-m) after the 1 mg intrave- nous dose.
CLR Renal clearance, calculated as the ratio of the cumulative amount excreted in the urine to AUC(0-t) at the last time point t with a detectable concentration in both plasma and urine.
C ~ N R Nonrenal clearance, calculated as the differ- ence between CL and CL,.
Ae(0-72) Percentage of dose excreted in urine as the unchanged drug or as 9-hydroxyrisperidone up to 72 hours after drug administration.
curve extrapolated to time infinity taking into account the terminal half-life.
Copyright © 2022 FDOKUMEN




















