twelve minor prophets. - Commentaries on the four last books ...

© 2014 S. Karger AG, Basel1420–8008/14/0384–0234$39.50/0
Original Research Article
Dement Geriatr Cogn Disord 2014;38:234–244
Galantamine versus Risperidone forAgitation in People with Dementia:A Randomized, Twelve-Week,Single-Center Study
Yvonne Freund-Levi a, b Victor Bloniecki a Bjørn Auestad c, d Ann Christine Tysen Bäckström b Marie Lärksäter b Dag Aarsland a, b
a Department of Neurobiology, Caring Sciences and Society (NVS), Division of Clinical Geriatrics, Karolinska Institutet, and b Department of Geriatric Medicine, Karolinska University Hospital Huddinge, Stockholm , Sweden; c Research Department, Stavanger University Hospital, and d Department of Mathematics and Natural Sciences, University of Stavanger, Stavanger , Norway
Key Words Neuropsychiatric symptoms · Agitation · Dementia · Behavioral and psychologicalsymptoms of dementia · Galantamine · Risperidone
Abstract Aims: To examine the effects of galantamine and risperidone on agitation in patients with dementia. Methods: A total of 100 patients with dementia and neuropsychiatric symptoms (mean age ± SD: 78.6 ± 7.5 years; 67% female) were included in this 12-week, randomized, parallel-group, controlled, single-center trial. The participants received galantamine (n = 50; target dose: 24 mg) or risperidone (n = 50; target dose: 1.5 mg) for 12 weeks. Results: Both galantamine and risperidone treatment resulted in reduced agitation. However, risperidone showed a significant advantage over galantamine both at week 3 (mean difference in total Cohen-Mansfield Agitation Inventory score: 3.7 points; p = 0.03) and at week 12 (4.3 points; p = 0.01). Conclusions: Agitation improved in both groups, even if the treatment effects were more pronounced in the risperidone group; however, the effects on cognition and other as-pects of tolerability were stronger with galantamine. © 2014 S. Karger AG, Basel
Accepted: March 13, 2014 Published online: June 25, 2014
Yvonne Freund-Levi Department of Neurobiology, Caring Sciences and Society (NVS) Division of Clinical Geriatrics, Karolinska Institutet SE–146 86 Stockholm (Sweden) E-Mail Yvonne.Freund-Levi @ ki.se
www.karger.com/dem
DOI: 10.1159/000362204
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

235Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
Introduction
Agitation is common in people with all types of dementia and is manifest in approxi-mately 25% of all dementia patients [1] . It can appear in home-dwelling patients but is partic-ularly common in nursing homes [2] , especially amongst patients with moderate or severe dementia [1, 3] . Agitation has important clinical consequences, such as a reduced quality of life and an increased burden to formal or family caregivers, and furthermore causes 30% of the associated treatment costs [2, 4–6] . The underlying neuronal mechanisms of agitation in dementia are unknown, but there are some indications that prefrontal lesions and neuro-chemical deficits involving monoaminergic and cholinergic neurotransmission contribute to its occurrence [7] .
Management of agitation consists of the identification and removal of factors which might contribute to or maintain agitation, such as physical diseases, pain or psychosocial determinants [8] . Psychotropic drugs are frequently used to treat agitation in dementia, and there is evidence that atypical antipsychotics, including neuroleptics such as risperidone or olanzapine, can be successful in reducing agitation [9–13] . However, the use of atypical anti-psychotics is associated with side effects such as an increased risk of cerebrovascular inci-dents as well as a possible deterioration of cognitive functions [14, 15] . Thus, there is an urgent need for improved pharmacological options for the treatment of agitation in dementia as agitation represents a big clinical challenge to patients, caregivers and the society.
Preliminary evidence suggests that cholinesterase inhibitors may reduce agitation in dementia [16, 17] . In a post hoc analysis of three large trials, galantamine was shown to generate reduced agitation as compared with placebo [18] . In addition to this effect, galan-tamine also has nicotinic-receptor-modulating effects, which might be relevant due to a potential association between nicotinic receptor activity and some neuropsychiatric symptoms [19] .
The use of cholinesterase inhibitors is interesting from a clinical point of view, since these drugs also have beneficial effects on cognition and good tolerability in the elderly, even though some conflicting results have been reported regarding their effects in the treatment of agitation. A large placebo-controlled trial did not find any evidence supporting that donepezil is effective against agitation in patients with dementia [20] . Only few studies have compared cholinesterase inhibitors and antipsychotic agents for the treatment of agitation in dementia. In the only placebo-controlled study, neither rivastigmine nor quetiapine improved agitation; however, quetiapine was associated with greater cognitive decline [21] .
We here report results from a randomized, open, single-center trial of galantamine and risperidone over 12 weeks including patients with dementia and neuropsychiatric symptoms. The current study represents a secondary analysis of data collected as part of a recently published trial [22] . The original trial involved the same study population and data collection with the intent to investigate the effect of galantamine and risperidone on behavioral and psychological symptoms of dementia as assessed by the Neuropsychiatric Inventory (NPI) [23] and global function. In that trial, both treatments led to a reduction in total scores, but with significantly more improvement with risperidone than with galantamine on the two subitems agitation and irritation. In contrast, Mini-Mental State Examination (MMSE) scores improved significantly more in the galantamine group than in the risperidone group, although the scores improved in both groups.
In the present study, our objective was to compare the treatment effect of a cholines-terase inhibitor (galantamine) and an atypical antipsychotic drug (risperidone) on agitation in the same trial and in more detail, based on scores from the Cohen-Mansfield Agitation Inventory (CMAI) [24] . Based on our previous findings, we hypothesized that both treatments would reduce agitation, but that risperidone would be more effective than galantamine.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

236Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
Patients and Methods
Patients Patients were recruited from the Memory Clinic at the Department of Geriatrics at the Karolinska
University Hospital Huddinge (Stockholm, Sweden) between 2003 and 2006. A total of 145 patients were screened ( fig. 1 ). The inclusion criteria were the presence of dementia according to the Diagnostic and Statis-tical Manual of Mental Disorders, 4th edition (DSM-IV) or the presence of mild cognitive impairment (MCI) [25] . Furthermore, the patients were also required to be ≥ 45 years of age and to have displayed neuropsy-chiatric symptoms (defined as a total score of ≥ 10 on the NPI) for ≥ 2 weeks prior to inclusion.
Patients were excluded if they had other psychiatric or neurological disorders or clinically significant medical disorders. The participants had to have a caregiver who was capable of and committed to assisting the subject in complying with the trial protocol and willing to provide the information required at the assessment interviews.
A total of 100 patients were included, with the following diagnoses: 34% had Alzheimer’s disease (AD), 27% mixed AD, 18% vascular dementia (VaD), 3% frontal lobe dementia, 2% Parkinson’s disease (PD), 4% unspecified dementia and 12% MCI.
Assessment The participants were assessed at baseline, after 2 weeks and at the end of the study at week 12. A
medical examination was conducted, including psychiatric and neurological examinations such as the MMSE [26] and NPI. The participants were home-dwelling but were admitted to the inpatient geriatric ward for
Assessed for eligibility(n = 145)
Randomized(n = 100)
Excluded (n = 45): Not meeting the inclusion criteria (n = 6) Refused to participate (n = 9) Other reason (n = 30)
Allocated to galantamine (n =50) Received galantamine (n = 50)
Enrolment
Allocation
Analyzed (n = 47)Excluded from analysis: Withdrawn informed consent (n = 1) Hyponatremia (n = 1) Death due to cardiac failure (n = 1)
Analysis
Analyzed (n = 44)Excluded from analysis: Withdrawn informed consent (n = 1) Cardiac failure (n = 1) Syncope (n = 1) Death due to cardiac failure (n = 1), suicide (n = 1) and pneumonia (n = 1)
Allocated to risperidone (n = 50)Received risperidone (n = 50)
Fig. 1. Design of the study and trial profile. Reasons for withdrawal are also shown.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

237Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
completion of the screening procedures. For the galantamine group, the length of the hospital stay was 15.3 ± 5.9 days, and for the risperidone group, it was 14.8 ± 4.6 days.
In this study, the primary efficacy measure was the change in total score on the CMAI. The CMAI was developed to systematically assess agitation in people with dementia. It consists of 29 descriptions of agitated behaviors, each rated on a 7-point scale based on frequency, ranging from never manifesting the behavior (score of 1) to manifesting the behavior several times an hour (score of 7), with a possible score range of 29–203. The CMAI has been shown to be the most reliable rating scale for agitation, superior to the NPI for the detection of changes in levels of agitation [27] .
Four different agitation factor subscores on the CMAI have been identified and were used as secondary outcome measures: (1) aggressive physical behavior (hitting, kicking, pushing, scratching, tearing things and cursing); (2) nonaggressive physical behavior (pacing, inappropriate robing or disrobing, repetitious sentences or questions, trying to get to a different place, general restlessness, handling things inappropri-ately and repetitious mannerisms); (3) verbally aggressive behavior (complaining, constant request for attention), and (4) verbally nonaggressive behavior (negativism, repetitious sentences or questions and complaining).
Randomization and Intervention The subjects admitted to the trial were consequently allocated to one of the two treatment groups
according to a predefined randomization code in blocks of 4, receiving either galantamine or risperidone (produced by Janssen Pharmaceuticals, Stockholm, Sweden). A fixed dose regimen was used for the two medications. Subjects randomized to galantamine received 1 tablet twice daily, preferably taken with food (breakfast at approx. 8 a.m. and a snack or meal at approx. 6 p.m.). The starting dose of galantamine was4 mg twice daily; after 1 week, the dose was increased to 8 mg twice daily, and to 12 mg twice daily at the start of week 3. Subjects randomized to risperidone received 0.25 mg twice daily at the beginning, which was increased to 0.5 mg twice daily after 1 week and to the final dose of 1.5 mg daily at the start of week 3. Compliance was monitored by quantifying unused medication and via self-reports of the patients and care-givers. To increase independence, the study clinician administering the rating scales (Y.F.-L.) was unaware of the study drug at the time of rating, and the statistical analyses were performed blinded to the study drug.
Concomitant Drugs Other antipsychotics, cholinesterase inhibitors or memantine were not allowed. Antidepressants were
allowed if the treatment had been stable for a period of 3 months, and a new treatment could be initiated if needed during the course of the trial. Drugs without anticholinergic potency had to be chosen. Except for eyedrops, the administration of drugs with anticholinergic potency was stopped at least 1 week prior to inclusion. If possible, the medication for somatic disorders remained unaltered during the trial period.
Rescue Medication If needed, oxazepam at 5–45 mg/day or clomethiazole at 300–600 mg/day was allowed for anxiety or
insomnia. In the galantamine group, risperidone could be added as a rescue medication if agitation worsened. The use of these drugs was recorded.
Adverse Events Adverse event reporting followed standard guidelines. At the 3 assessment points, motor side effects
were assessed by the Simpson and Angus scale [28] , a rating scale for evaluating drug-related extrapyramidal syndromes with 10 items scored as 0–4, with a possible range from 0 to 40, higher scores meaning more severe symptoms. Cognition was assessed using the MMSE. The numbers of dropouts and hospitalizations due to adverse events were recorded.
Ethics Approval The study was conducted according to good clinical practice and the ethical principles of the Declaration
of Helsinki. The protocol was approved by the Ethics Committee at the Karolinska University Hospital Huddinge (study ID: 20100039). Prior to entry in the trial, the investigator explained the full procedures to potential subjects or their legal representatives, and described the trial and the implications of participation to the subjects’ informal caregivers. An informed consent form was signed by the patients and their care-givers before entering the study.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

238Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
Statistical Analyses Sample size calculations were based on the NPI, as described in our primary paper [22] . Between-group
differences in outcome measures over time were analyzed using ANCOVA, adjusting for the baseline score to handle the repeated structure of the data. Age and sex were used as covariates. Also adjustment for diagnosis was checked. The number of dropouts was analyzed using the χ 2 test; Fisher’s exact test was used if it was <5 in any of the groups.
The primary efficacy population was a modified intention-to-treat subpopulation of the total popu-lation, i.e. all participants with ≥ 1 postbaseline assessment, using the last-observation-carried-forward (LOCF) procedure to account for missing data. p < 0.05 was considered statistically significant.
To further test the robustness of the findings, t tests comparing scores at weeks 3 and 12 and changes from baseline to weeks 3 and 12 were performed for each group. To adjust for the nonnormality of the data, we also performed bootstrap comparisons of the means at week 12. Furthermore, we analyzed the data using multiple imputation to account for missing data. Finally, we also analyzed the data in observed cases and in patients with agitation at baseline, i.e. with a CMAI score of ≥ 39.
Results
Of the 100 randomized participants, 9 dropped out of the study between the assessments at week 3 and week 12 (3 in the galantamine and 6 in the risperidone group; Fisher’s exact test, two-sided: p = 0.5; fig. 1 ). All 100 patients were therefore included in the primary intention-to-treat/LOCF analysis. The two groups were well balanced regarding their demo-graphic and clinical characteristics ( table 1 ).
Efficacy The CMAI total scores declined during treatment in both groups. Using ANCOVA and
adjusting for baseline CMAI total score, age and sex, the change from baseline to follow-up was significantly greater in the risperidone group than in the galantamine group at week 3 (mean difference: –3.7; p = 0.03) and also at week 12 (LOCF data; mean difference: –4.3; p = 0.01). The mean CMAI values of the two patient groups during the trial are shown in figure 2 . Analyzing the CMAI subscores, subitem 1 (aggressive physical behavior) was the only subscale demonstrating a significant difference between the groups at week 12 (ANCOVA adjusted for baseline, sex and age, LOCF data: p < 0.05), whereas the other three subscale scores did not differ significantly. However, in the observed cases, the ANCOVA did not show any significant between-group difference at week 3 (p = 0.052) or week 12 (p = 0.16).
All patients Galantamine Risperidone
Age, years 78.7 ± 7.5 79.6 ± 6.8 77.8 ± 8.0Female, % 67 68 66BMI 24.3 ± 4.3 23.5 ± 4.3 25.1 ± 4.2NPI scorea 51.0 ± 25.8 51.5 ± 22.6 50.54 ± 28.8MMSE scoreb 20.1 ± 4.6 19.5 ± 4.9 20.7 ± 4.3CDR scorec 1.5 ± 0.6 1.5 ± 0.7 1.4 ± 0.6
All values are shown as means ± SD, except where indicated otherwise. BMI = Body mass index; CDR = Clinical Dementia Rating scale.
a Range: 0 – 144 points. b Range: 0 – 30 points. c Global; range: 0 – 3 points.
Table 1. Baseline characteristics of all patients as well as the galantamine and risperidone treatment groups
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

239Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
Further analyses showed that the CMAI scores at week 3 (p = 0.037) and week 12 (p = 0.017) were significantly lower in the risperidone group than in the galantamine group ( table 2 ). The changes within each group from baseline to week 3 and week 12 (using the LOCF method) were significant both for the risperidone group (mean change ± SD at week 3: –10.6 ± 13.3, d.f. = 49, p < 0.0005; at week 12: –7.0 ± 11.6, d.f. = 49, p < 0.0005) and the galan-tamine group (mean change at week 3: –8.7 ± 12.7, d.f. = 49, p < 0.0005; at week 12: –4.3 ± 10.9, d.f. = 49, p = 0.008).
In the final analyses, we included only those patients with a baseline CMAI score of ≥ 39 (n = 73). ANCOVA adjusting for baseline CMAI total score, age and sex showed a significant difference in favor of risperidone at week 3 (p = 0.012) and, using the LOCF sample, at week 12 (p = 0.007). Again, in the analysis of the observed cases, there was no significant between-group difference at week 12 (p = 0.051). The ANCOVA of the CMAI scores were also checked with adjustment for diagnosis (AD and mixed AD vs. no AD), resulting in practically unchanged effect estimates and p values.
To explore why the results differed between the LOCF subpopulation and the observed cases, we analyzed the course of the 9 dropouts individually ( fig. 1 ). Five of the 6 dropouts in the risperidone group had a relatively large improvement in CMAI score between baseline and week 3 (range: 8–35 points), whereas 2 of the 3 dropouts in the galantamine group had
30
Baseline 3 12 Follow-up (weeks)
35
40
45
50
CMAI
sco
re
Fig. 2. Plot of mean CMAI scores for both patient groups at base-line, week 3 and week 12. Dashed line: risperidone; solid line: galantamine.
Table 2. CMAI total scores during treatment period
Galantamine (n = 50) Risperidone (n = 50) p value
Baseline 47.5 ± 11.1 (44.4 – 50.5) 45.6 ± 12.5 (44.2 – 491) 0.439Week 3 38.7 ± 10.3 (35.9 – 41.6) 35.0 ± 6.7 (33.2 – 36.9) 0.037Week 12 (LOCF) 43.2 ± 10.5 (40.3 – 46.1) 38.6 ± 8.5 (36.2 – 40.9) 0.017Changea from baseline to week 3 –8.7 ± 12.7 –10.6 ± 13.3 <0.0005b; <0.0005c
Changea from baseline to week 12 –4.3 ± 10.9 –7.0 ± 11.6 0.008b; <0.0005c
Numbers represent means ± SD with confidence intervals in parentheses. Scores at week 12 are based on the LOCF population. Results from t test.
a Negative value means reduced score, i.e. improvement. b p values for change within the galantamine group. c p values for change within the risperidone group.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M
240Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
improved moderately (4 and 13 points), and marked worsening was observed in 1 patient. Thus, in the risperidone group, the relatively great change in participants who withdrew after the assessment at week 3 contributed to the reduction in CMAI scores for this group in the LOCF subpopulation analysis, whereas these cases were not included in the analysis of the observed cases.
Using the bootstrap technique, the difference between the groups at week 12 did not reach significance either for the observed cases or the LOCF subpopulation (both p values approx. 0.07). Similarly, in the analysis of the data using multiple imputation to account for missing data, the difference between the groups was not significant either (ANCOVA week 12: p = 0.18).
Rescue Medication during the First Two Weeks The proportion of patients using oxazepam or clomethiazole did not differ between the
galantamine group (54%) and the risperidone group (58%; χ 2 test: 0.7, d.f. = 1, p = 0.7). Only 2 of the patients in the galantamine group received additional risperidone during the first 2-week period.
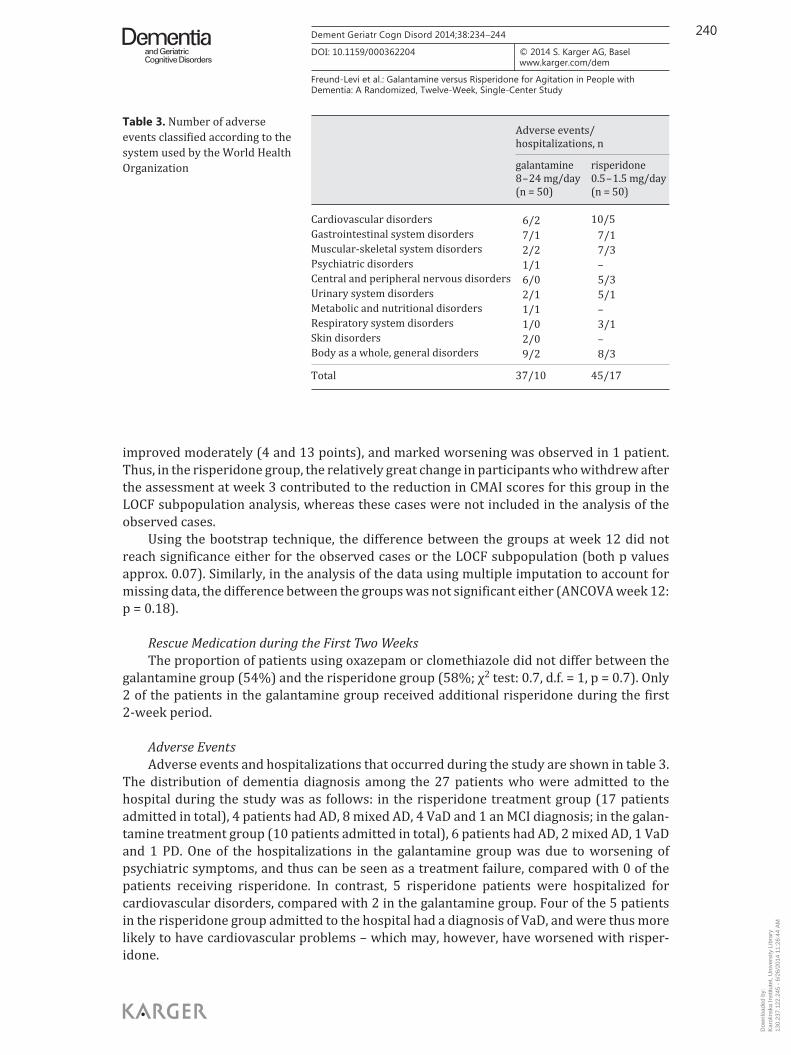
Adverse Events Adverse events and hospitalizations that occurred during the study are shown in table 3 .
The distribution of dementia diagnosis among the 27 patients who were admitted to the hospital during the study was as follows: in the risperidone treatment group (17 patients admitted in total), 4 patients had AD, 8 mixed AD, 4 VaD and 1 an MCI diagnosis; in the galan-tamine treatment group (10 patients admitted in total), 6 patients had AD, 2 mixed AD, 1 VaD and 1 PD. One of the hospitalizations in the galantamine group was due to worsening of psychiatric symptoms, and thus can be seen as a treatment failure, compared with 0 of the patients receiving risperidone. In contrast, 5 risperidone patients were hospitalized for cardiovascular disorders, compared with 2 in the galantamine group. Four of the 5 patients in the risperidone group admitted to the hospital had a diagnosis of VaD, and were thus more likely to have cardiovascular problems – which may, however, have worsened with risper-idone.
Adverse events/hospitalizations, n
gala ntamine8 – 24 mg/day(n = 50)
risperidone0.5 – 1.5 mg/day(n = 50)
Cardiovascular disorders 6/2 10/5Gastrointestinal system disorders 7/1 7/1Muscular-skeletal system disorders 2/2 7/3Psychiatric disorders 1/1 –Central and peripheral nervous disorders 6/0 5/3Urinary system disorders 2/1 5/1Metabolic and nutritional disorders 1/1 –Respiratory system disorders 1/0 3/1Skin disorders 2/0 –Body as a whole, general disorders 9/2 8/3
Total 37/10 45/17
Table 3. Number of adverse events classified according to the system used by the World Health Organization
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

241Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
The baseline Simpson and Angus scale score tended to be higher in the galantamine group than in the risperidone group (p = 0.06). Although the scores became more similar during the study period, the difference in change between the two groups was not significant (ANCOVA adjusting for baseline score, gender and age at week 3: p = 0.29; at week 12: p = 0.87).
Discussion
We analyzed the change in agitation during a 12-week trial comparing risperidone with galantamine. The main finding was that the levels of agitation decreased in both treatment groups, but the main analyses suggested that the improvement was significantly larger in the risperidone group. However, this was counterbalanced by better tolerability in the galan-tamine group, with a numerically smaller proportion of patients discontinuing treatment and a larger cognitive improvement.
Our findings are consistent with those from previous clinical trials and meta-analyses reporting evidence that risperidone has a beneficial effect on agitation in people with dementia [29, 30] , albeit at the cost of frequent side effects such as an increased risk of cerebrovascular incidents and mortality [14, 29] . There is some evidence suggesting that cholinesterase inhib-itors may modestly reduce agitation and other psychiatric symptoms in dementia [15, 17, 31] , although in the most systematic clinical trial, donepezil did not show an improved treatment outcome compared with placebo [20] . However, in that study, patients were included only if they did not respond to a 4-week course of a behavioral intervention, possibly suggesting that these patients have a more persistent and treatment-resistant type of agitation.
We are aware of only two studies that have directly compared the effects of a cholines-terase inhibitor and an antipsychotic for agitation in dementia. In the larger study, neither the atypical antipsychotic quetiapine nor the cholinesterase inhibitor rivastigmine was superior to placebo in improving agitation, and a worsening of cognition was observed in the quetiapine group [21] . In the smaller study, similar findings to those of our study were reported: risper-idone, but not rivastigmine (6 mg/day), was more effective than placebo in reducing agitation [32] . In these two studies, however, the patients were institutionalized and had more severe dementia and neuropsychiatric symptoms than the current study cohort.
According to current recommendations, antipsychotics for agitation should only be considered for the most severely disturbed patients [8, 29] , whereas drugs with a better toler-ability, such as memantine, citalopram and even carbamazepine, are recommended for patients with mild or moderate neuropsychiatric symptoms [8, 33] . Other treatment options for agitation in dementia, such as omega-3 fatty acid supplementation, have also been proposed [34] . The current findings suggest that cholinesterase inhibitors, with their better tolerability profile, might also be considered as a treatment option for dementia patients with less severe agitation, although the improvement was significantly smaller than that in the antipsychotic group, an approach supported by long-term studies of cholinesterase inhibitors against agitation [35, 36] .
The main limitations of this study are its nonblinded design and the lack of a placebo group, which together make the interpretation of the findings more difficult. The open design might have influenced scoring due to expectations. However, attempts were made to keep the rater unaware of the study drug used. The lack of a placebo group means that we do not know whether the observed improvements are beyond the effect of placebo alone. Previous studies have found a considerable response in their placebo groups [20, 21] , probably due to both a Hawthorne effect (i.e. residents in an unstimulating environment respond positively to the increased interaction which is part of the study procedures) and regression to the mean. Such
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

242Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
effects might be particularly strong in the current study, since all patients were admitted to a hospital with special expertise in treating psychiatric disturbances in people with dementia during the first 2 weeks. However, the improvement from baseline values was sustained even after the 10 weeks of outpatient treatment following discharge from the hospital.
The dose of risperidone administered to the patients was 1.5 mg/day, which is higher than the dose used in the majority of studies on risperidone (1 mg/day). This could be a possible explanation for the increased number of adverse effects in the risperidone group, as adverse effects have been shown to be dose related [37] . On the other hand, this may also have led to a stronger effect on agitation.
Using the LOCF method has its limitations, and if multiple imputation was applied, there were no significant differences between the groups concerning agitation. Similarly, there were no between-group differences if adjusting for the nonnormality of the data. The number of dropouts was higher in the risperidone group than in the galantamine group. Of note, several of the dropouts in the risperidone group showed marked improvements after 3 weeks. Thus, the dropout pattern supported the main conclusion, i.e. that risperidone seems to be more effective in reducing agitation but at the cost of poorer tolerability. The number of adverse events leading to withdrawal was higher in the risperidone group than in the galantamine group, although this difference was not significant. Similarly, the frequency of hospitalizations due to adverse events did not differ significantly between the two groups, even though the reasons for these hospitalizations tended to be adverse events in the risper-idone group in contrast to treatment failures in the galantamine group.
The main conclusion is also supported by the cognitive scores. However, it is noteworthy that although the cognitive response was significant in the galantamine but not in the risper-idone patients, there was no significant worsening of cognition as measured by the MMSE in the risperidone group.
In summary, agitation was reduced in both groups, but more so in the risperidone group. On the other hand, a significant cognitive improvement was observed in the galantamine group but not in the risperidone group. These findings suggest that for patients with dementia and modest agitation, galantamine treatment might be considered before initiating antipsy-chotic medication, whereas risperidone should be considered in cases with persistent or severe agitation. Adequately powered, double-blind, placebo-controlled studies with a head-to-head comparison between antidementia drugs and antipsychotics are warranted.
Acknowledgments
The present study is an academically initiated study financed by an independent grant from Janssen Pharmaceuticals, Stockholm, Sweden. The company was represented in the trial steering committee with regard to the study design and provided the galantamine and risperidone preparations. The company has not been involved in patient and data collection. The support for this work by grants from the Petrus and Augusta-Hedlunds Foundation, Demensförbundet and Loo and Hans Osterman Foundation Karolinska Insti-tutet as well as Demensförbundet Stockholm is also gratefully acknowledged. There was a Regional Agreement on Medical Training and Clinical Research (ALF) between the Stockholm County Council and Karolinska Insti-tutet (20110263, 20110604).
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M
243Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
References
1 Lyketsos CG, Steinberg M, Tschanz JT, Norton MC, Steffens DC, Breitner JC: Mental and behavioral disturbances in dementia: findings from the Cache County Study on Memory in Aging. Am J Psychiatry 2000; 157: 708–714.
2 Morley JE: Dementia-related agitation. J Am Med Dir Assoc 2011; 12: 611–612. 3 Selbaek G, Kirkevold O, Engedal K: The prevalence of psychiatric symptoms and behavioural disturbances and
the use of psychotropic drugs in Norwegian nursing homes. Int J Geriatr Psychiatry 2007; 22: 843–849. 4 Allegri RF, Sarasola D, Serrano CM, Taragano FE, Arizaga RL, Butman J, Loñ L: Neuropsychiatric symptoms as
a predictor of caregiver burden in Alzheimer’s disease. Neuropsychiatr Dis Treat 2006; 2: 105–110. 5 Schnaider Beeri M, Werner P, Davidson M, Noy S: The cost of behavioral and psychological symptoms of
dementia (BPSD) in community dwelling Alzheimer’s disease patients. Int J Geriatr Psychiatry 2002; 17: 403–408.
6 Wetzels RB, Zuidema SU, de Jonghe JF, Verhey FR, Koopmans RT: Determinants of quality of life in nursing home residents with dementia. Dement Geriatr Cogn Disord 2010; 29: 189–197.
7 Cerejeira J, Lagarto L, Mukaetova-Ladinska EB: Behavioral and psychological symptoms of dementia. Front Neurol 2012; 3: 73.
8 Ballard CG, Gauthier S, Cummings JL, Brodaty H, Grossberg GT, Robert P, Lyketsos CG: Management of agitation and aggression associated with Alzheimer disease. Nat Rev Neurol 2009; 5: 245–255.
9 Brodaty H, Ames D, Snowdon J, Woodward M, Kirwan J, Clarnette R, Lee E, Lyons B, Grossman F: A randomized placebo-controlled trial of risperidone for the treatment of aggression, agitation, and psychosis of dementia. J Clin Psychiatry 2003; 64: 134–143.
10 Schneider LS, Dagerman K, Insel PS: Efficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials. Am J Geriatr Psychiatry 2006; 14: 191–210.
11 Profenno LA, Tariot PN: Pharmacologic management of agitation in Alzheimer’s disease. Dement Geriatr Cogn Disord 2004; 17: 65–77.
12 Maher A, Maglione M, Bagley S, et al: Efficacy and comparative effectiveness of atypical antipsychotic medica-tions for off-label uses in adults: a systematic review and meta-analysis. JAMA 2011; 306: 1359–1369.
13 Sultzer DL, Davis SM, Tariot PN, Dagerman KS, Lebowitz BD, Lyketsos CG, Rosenheck RA, Hsiao JK, Lieberman JA, Schneider LS; CATIE-AD Study Group: Clinical symptom responses to atypical antipsychotic medications in Alzheimer’s disease: phase 1 outcomes from the CATIE-AD effectiveness trial. Am J Psychiatry 2008; 165: 844–854.
14 Vigen CLP, Mack WJ, Keefe RSE, Sano M, Sultzer DL, Stroup TS, Dagerman KS, Hsiao JK, Lebowitz BD, Lyketsos CG, Tariot PN, Zheng L, Schneider LS: Cognitive effects of atypical antipsychotic medications in patients with Alzheimer’s disease: outcomes from CATIE-AD. Am J Psychiatry 2011; 168: 831–883.
15 Sink KM, Holden KF, Yaffe K: Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA 2005; 293: 596–608.
16 Rodda J, Morgan S, Walker Z: Are cholinesterase inhibitors effective in the management of the behavioral and psychological symptoms of dementia in Alzheimer’s disease? A systematic review of randomized, placebo-controlled trials of donepezil, rivastigmine and galantamine. Int Psychogeriatr 2009; 21: 813–824.
17 Trinh N, Hoblyn J, Mohanty S, Yaffe K: Efficacy of cholinesterase inhibitors in the treatment of neuropsychiatric symptoms and functional impairment in Alzheimer disease: a meta-analysis. JAMA 2003; 289: 210–216.
18 Herrmann N, Rabheru K, Wang J, Binder C: Galantamine treatment of problematic behavior in Alzheimer disease: post-hoc analysis of pooled data from three large trials. Am J Geriatr Psychiatry 2005; 13: 527–534.
19 O’Brien JT, Colloby SJ, Pakrasi S, Perry EK, Pimlott SL, Wyper DJ, McKeith IG, Williams ED: Nicotinic α 4 β 2 -receptor binding in dementia with Lewy bodies using 123I-5IA 85380 SPECT demonstrates a link between occipital changes and visual hallucinations. Neuroimage 2008; 40: 1056–1063.
20 Howard RJ, Juszczak E, Ballard CG, Bentham P, Brown RG, Bullock R, Burns AS, Holmes C, Jacoby R, Johnson T, Knapp M, Lindesay J, O’Brien JT, Wilcock G, Katona C, Jones RW, DeCesare J, Rodger M; CALM-AD Trial Group: Donepezil for the treatment of agitation in Alzheimer’s disease. N Engl J Med 2007; 357: 1382–1392.
21 Ballard C, Margallo-Lana M, Juszczak E, Douglas S, Swann A, Thomas A, O’Brien J, Everratt A, Sadler S, Maddison C, Lee L, Bannister C, Elvish R, Jacob R: Quetiapine and rivastigmine and cognitive decline in Alzheimer’s disease: randomised double blind placebo controlled trial. BMJ 2005; 330: 874.
22 Freund-Levi Y, Jedenius E, Tysen-Bäckström AN, Lärksäter M, Wahlund LO, Eriksdotter M: Galantamine versus risperidone treatment of neuropsychiatric symptoms in patients with probable dementia: an open randomized trial. Am J Geriatr Psychiatry 2014; 22: 341–348.
23 Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J: The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 1994; 44: 2308–2314.
24 Cohen-Mansfield J, Billig N: Agitated behaviors in the elderly. I. A conceptual review. J Am Geriatr Soc 1986; 34: 711–721.
25 American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, ed 4. Washington, American Psychiatric Association, 1995.
26 Folstein MF, Folstein SE, McHugh PR: ‘Mini-mental state’: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189–198.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M

244Dement Geriatr Cogn Disord 2014;38:234–244
DOI: 10.1159/000362204
Freund-Levi et al.: Galantamine versus Risperidone for Agitation in People with Dementia: A Randomized, Twelve-Week, Single-Center Study
www.karger.com/dem© 2014 S. Karger AG, Basel
27 Zuidema SU, Buursema AL, Gerritsen MG, Oosterwal KC, Smits MM, Koopmans RT, de Jonghe JF: Assessing neuropsychiatric symptoms in nursing home patients with dementia: reliability and Reliable Change Index of the Neuropsychiatric Inventory and the Cohen-Mansfield Agitation Inventory. Int J Geriatr Psychiatry 2011; 26: 127–134.
28 Simpson GM, Angus JW: A rating scale for extrapyramidal side effects. Acta Psychiatr Scand Suppl 1970; 212: 11–19.
29 Ballard CG, Waite J: The effectiveness of atypical antipsychotics for the treatment of aggression and psychosis in Alzheimer’s disease. Cochrane Database Syst Rev 2006; 1:CD003476.
30 Carson S, McDonagh MS, Peterson K: A systematic review of the efficacy and safety of atypical antipsychotics in patients with psychological and behavioral symptoms of dementia. J Am Geriatr Soc 2006; 54: 354–361.
31 Holmes C, Wilkinson D, Dean C, Vethanayagam S, Olivieri S, Langley A, Pandita Gunawardena ND, Hogg F, Clare C, Damms J: The efficacy of donepezil in the treatment of neuropsychiatric symptoms in Alzheimer disease. Neurology 2004; 63: 214–219.
32 Holmes C, Wilkinson D, Dean C, Clare C, El-Okl M, Hensford C, Moghul S: Risperidone and rivastigmine and agitated behaviour in severe Alzheimer’s disease: a randomised double blind placebo controlled study. Int J Geriatr Psychiatry 2007; 22: 380–381.
33 Wilcock GK, Ballard CG, Cooper JA, Loft H: Memantine for agitation/aggression and psychosis in moderately severe to severe Alzheimer’s disease: a pooled analysis of 3 studies. J Clin Psychiatry 2008; 69: 341–348.
34 Freund-Levi Y, Basun H, Cederholm T, Faxén-Irving G, Garlind A, Grut M, Vedin I, Palmblad J, Wahlund LO, Eriksdotter-Jönhagen M: Omega-3 supplementation in mild to moderate Alzheimer’s disease: effects on neuropsychiatric symptoms. Int J Geriatr Psychiatry 2008; 23: 161–169.
35 Rösler M, Retz W, Retz-Junginger P, Dennle H-J: Effects of two-year treatment with the cholinesterase inhibitor rivastigmine on behavioural symptoms in Alzheimer’s disease. Behav Neurol 1998; 4: 211–216.
36 Cummings JL, Koumaras B, Chen M, Mirski D; Rivastigmine Nursing Home Study Team: Effects of rivastigmine treatment on the neuropsychiatric and behavioral disturbances of nursing home residents with moderate to severe probable Alzheimer’s disease: a 26-week, multicenter, open-label study. Am J Geriatr Pharmacother 2005; 3: 137–148.
37 Katz IR, Jeste DV, Mintzer JE, Clyde C, Napolitano J, Brecher M: Comparison of risperidone and placebo for psychosis and behavioral disturbances associated with dementia: a randomized, double-blind trial. Risper-idone Study Group. J Clin Psychiatry 1999; 60: 107–115.
Dow
nloa
ded
by:
Kar
olin
ska
Inst
itute
t, U
nive
rsity
Lib
rary
13
0.23
7.12
2.24
5 -
6/26
/201
4 11
:26:
44 A
M
Copyright © 2022 FDOKUMEN




















