Parasitic Zoonoses - Patologi
151
Parasitic Zoonoses B. B. Singh Dhaliwal Prayag Dutt Juyal
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Parasitic Zoonoses - Patologi

Parasitic Zoonoses
B. B. Singh DhaliwalPrayag Dutt Juyal

Parasitic Zoonoses

B. B. Singh DhaliwalPrayag Dutt Juyal
Parasitic Zoonoses
123

B. B. Singh DhaliwalSchool of Public Health and ZoonosesGuru Angad Dev Veterinary
and Animal Sciences UniversityLudhiana, PunjabIndia
Prayag Dutt JuyalVeterinary ParasitologyGuru Angad Dev Veterinary
and Animal Sciences UniversityLudhiana, PunjabIndia
ISBN 978-81-322-1550-9 ISBN 978-81-322-1551-6 (eBook)DOI 10.1007/978-81-322-1551-6Springer New Delhi Heidelberg New York Dordrecht London
Library of Congress Control Number: 2013942660
� Springer India 2013This work is subject to copyright. All rights are reserved by the Publisher, whether the whole orpart of the material is concerned, specifically the rights of translation, reprinting, reuse ofillustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way,and transmission or information storage and retrieval, electronic adaptation, computer software,or by similar or dissimilar methodology now known or hereafter developed. Exempted from thislegal reservation are brief excerpts in connection with reviews or scholarly analysis or materialsupplied specifically for the purpose of being entered and executed on a computer system, forexclusive use by the purchaser of the work. Duplication of this publication or parts thereof ispermitted only under the provisions of the Copyright Law of the Publisher’s location, in itscurrent version, and permission for use must always be obtained from Springer. Permissions foruse may be obtained through RightsLink at the Copyright Clearance Center. Violations areliable to prosecution under the respective Copyright Law.The use of general descriptive names, registered names, trademarks, service marks, etc. in thispublication does not imply, even in the absence of a specific statement, that such names areexempt from the relevant protective laws and regulations and therefore free for general use.While the advice and information in this book are believed to be true and accurate at the date ofpublication, neither the authors nor the editors nor the publisher can accept any legalresponsibility for any errors or omissions that may be made. The publisher makes no warranty,express or implied, with respect to the material contained herein.
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)

Preface
The book ‘‘Parasitic Zoonoses’’ is intended for higher undergraduate
and graduate students of zoonoses and public health, veterinary para-
sitology, parasite epidemiology; public health workers; public health
veterinarians; field veterinarians; medical professionals and all others
interested in the subject. The main objective of writing this book is to
provide source of information on zoonotic parasites.
The book describes definition of zoonoses and parasitic zoonoses.
Parasitic zoonoses are the combination of two subjects, i.e., parasitology
and zoonoses where knowledge of both the fields comes into play for the
study of zoonotic parasites. Parasitic zoonoses are the most diversified
group of zoonotic diseases representing all the classes mentioned in
zoonotic diseases classification. They have been classified and discussed
based on etiological agents, transmission cycle, reservoir hosts and
principal host involved along with examples. Important topics such as
food borne, vector borne and occupation-related parasitic zoonoses have
also been covered in the introduction. We have also discussed factors
responsible for emergence of zoonotic parasites viz. climatic change
associated with global warming, increased vector populations, world
tourism, the demand for livestock food products, changing socio-eco-
nomic conditions, poverty, lack of safe drinking water, the large number
of stray animals, changed cooking practices, defecating outdoors, poor
personal hygiene and the high population density in the tropics.
More than 15 protozoa and 50 other parasitic diseases are zoonotic in
nature and all these diseases have been discussed in detail. Each disease
has been divided in different sections viz. synonyms/common names,
etiology, epidemiology, life cycle, mode of transmission, clinical signs in
man and animals, diagnosis and their prevention and control. Life cycle
charts and coloured photographs of these parasites have been included
wherever required. An alphabetical bibliography for every disease has
also been included so that readers have access to further information.
There are few diseases which are rare in occurrence or their zoonotic
potential is still being questioned but they have also been given some
space to update the knowledge of the readers. We hope this book will
prove beneficial to the students and others interested in the subject.
B. B. Singh Dhaliwal
P. D. Juyal
v

Acknowledgments
First of all with great humility, we dedicatedly accord our sincere
gratitude to Almighty God for His benign blessing hand and bestowing
a creative and healthy environment throughout this work.
We feel humbled and acknowledge our indebtedness to the authors of
the research articles whose work has been consulted and cited in this
book. We also thank authors of several source books from where we
took guidance and inspiration for this publication.
We particularly value the mentorship provided by Dr. Alvin A.
Gajadhar and are thankful to professional and technical staff with
Canadian Food Inspection Agency’s Centre for Food Borne and Ani-
mal Parasitology for incessant encouragement and invaluable advice
which enabled us to accomplish the hard task of completing this text
book and making it worth presenting.
We are thankful to faculty members of the School of Public Health
and Zoonoses and Department of Veterinary Parasitology, Guru Angad
Dev Veterinary and Animal Sciences University (GADVASU), Ludhi-
ana (India) for their ever-willing help and scholastic guidance
throughout the writing of this book. We also thank authorities of
GADVASU, Ludhiana, for providing excellent academic atmosphere to
pen this book.
Mere words of acknowledgement will never express the sense of
regards and indebtedness towards our families who are the source of our
strength and inspiration. Their unconditional love, patience, compro-
mises and sacrifice can never be forgotten.
The cooperation and help of Springer India Pvt. Ltd. to bring out this
book is highly appreciated. The authors welcome valuable suggestions
from the readers so as to improve the contents of the book in revised
editions if any published in the future.
B. B. Singh Dhaliwal
P. D. Juyal
vii

Contents
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.1 Classification of Parasitic Zoonoses . . . . . . . . . . . . . . . 2
1.1.1 Based on Etiological Agents . . . . . . . . . . . . . 21.1.2 Based on Transmission Cycle . . . . . . . . . . . . 21.1.3 Based on Reservoir Hosts . . . . . . . . . . . . . . . 31.1.4 Based on Principal Host Involved . . . . . . . . . 3
1.2 Animal-Related Parasitic Zoonoses . . . . . . . . . . . . . . . 41.2.1 Livestock-Related Parasitic Zoonoses . . . . . . . 41.2.2 Wildlife-Related Parasitic Zoonoses . . . . . . . . 41.2.3 Domiciliated Animals . . . . . . . . . . . . . . . . . . 51.2.4 Pet Animal-Related Parasitic Zoonoses . . . . . . 51.2.5 Fish, Shellfish and Mollusc-Borne
Parasitic Zoonoses . . . . . . . . . . . . . . . . . . . . 61.3 Occupational Parasitic Zoonoses . . . . . . . . . . . . . . . . . 7
1.3.1 Prevention and Control . . . . . . . . . . . . . . . . . 71.4 Food Borne Parasitic Zoonoses . . . . . . . . . . . . . . . . . . 7
1.4.1 Fish, Shellfish and Mollusc-BorneParasitic Zoonoses . . . . . . . . . . . . . . . . . . . . 10
1.4.2 Meat-Borne Parasitic Zoonoses . . . . . . . . . . . 101.4.3 Water-Borne Parasitic Zoonoses. . . . . . . . . . . 111.4.4 Milk-Borne Parasitic Zoonoses . . . . . . . . . . . 121.4.5 Raw Vegetables/Plant-Borne Parasitic
Zoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.4.6 Reptile, Amphibian-Borne Parasitic
Zoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . 131.4.7 Poultry-Related Parasitic Zoonoses . . . . . . . . . 13
1.5 Soil-Transmitted Parasitic Zoonoses . . . . . . . . . . . . . . . 131.5.1 Prevention and Control . . . . . . . . . . . . . . . . . 13
1.6 Vector-Borne Parasitic Zoonoses . . . . . . . . . . . . . . . . . 131.6.1 Prevention and Control . . . . . . . . . . . . . . . . . 14
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
2 Protozoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152.1 African Trypanosomiasis. . . . . . . . . . . . . . . . . . . . . . . 15
2.1.1 Common Name/Synonyms . . . . . . . . . . . . . . 152.1.2 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152.1.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 16
ix

2.1.4 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 162.1.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 162.1.6 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 162.1.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 162.1.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 162.1.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 162.1.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
2.2 Amoebiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172.2.1 Common Name/Synonyms . . . . . . . . . . . . . . 172.2.2 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172.2.3 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 172.2.4 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 172.2.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 182.2.6 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 182.2.7 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 182.2.8 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 182.2.9 Clinical Signs in Animals . . . . . . . . . . . . . . . 182.2.10 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 182.2.11 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.3 Babesiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.3.1 Common Name/Synonyms . . . . . . . . . . . . . . 182.3.2 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . 182.3.3 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.3.4 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 192.3.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 192.3.6 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 192.3.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 192.3.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 192.3.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 192.3.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
2.4 Balantidiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202.4.1 Common Name/Synonyms . . . . . . . . . . . . . . 202.4.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 202.4.3 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.4.4 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 212.4.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 212.4.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 212.4.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 212.4.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 212.4.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 212.4.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
2.5 Chagas Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.5.1 Common Name/Synonyms . . . . . . . . . . . . . . 212.5.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 212.5.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 212.5.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 222.5.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 222.5.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 222.5.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 22
x Contents

2.5.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 222.5.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
2.6 Cryptosporidiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222.6.1 Common Name/Synonyms . . . . . . . . . . . . . . 232.6.2 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.6.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 232.6.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 242.6.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 242.6.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 242.6.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 242.6.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 242.6.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
2.7 Giardiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242.7.1 Common Name/Synonyms . . . . . . . . . . . . . . 242.7.2 Etiological Agent . . . . . . . . . . . . . . . . . . . . . 252.7.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 252.7.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 252.7.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 252.7.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 262.7.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 262.7.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 262.7.9 Prevention and Control . . . . . . . . . . . . . . . . . 26
2.8 Leishmaniasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262.8.1 Visceral Leishmaniasis . . . . . . . . . . . . . . . . . 272.8.2 Cutaneous Leishmaniasis. . . . . . . . . . . . . . . . 28
2.9 Sarcocystosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 302.9.1 Common Name/Synonyms . . . . . . . . . . . . . . 302.9.2 Etiological Agent . . . . . . . . . . . . . . . . . . . . . 302.9.3 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 302.9.4 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 302.9.5 Clinical Signs in Animals . . . . . . . . . . . . . . . 302.9.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 312.9.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 31
2.10 Toxoplasmosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.10.1 Synonyms . . . . . . . . . . . . . . . . . . . . . . . . . . 322.10.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.10.3 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 322.10.4 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 322.10.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 332.10.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 332.10.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 332.10.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 332.10.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
2.11 Other Protozoan Zoonotic Diseases . . . . . . . . . . . . . . . 332.11.1 Cyclosporiasis . . . . . . . . . . . . . . . . . . . . . . . 332.11.2 Infections Caused by Free-Living Amoebae. . . 352.11.3 Malaria in Non-human Primates. . . . . . . . . . . 35
Contents xi

2.11.4 Microsporidiosis. . . . . . . . . . . . . . . . . . . . . . 352.11.5 Atypical Human Trypanosomiasis . . . . . . . . . 35
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
3 Trematode Zoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 413.1 Cercarial Dermatitis . . . . . . . . . . . . . . . . . . . . . . . . . . 41
3.1.1 Common Name/Synonyms . . . . . . . . . . . . . . 413.1.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 423.1.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 423.1.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 423.1.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 423.1.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 423.1.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 423.1.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 433.1.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 433.1.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3.2 Dicrocoeliasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.2.1 Common Name/Synonyms . . . . . . . . . . . . . . 433.2.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 433.2.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 433.2.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 433.2.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 433.2.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 443.2.7 Clinical Signs in Man and Animals . . . . . . . . 443.2.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 443.2.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
3.3 Echinostomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453.3.1 Common Name/Synonyms . . . . . . . . . . . . . . 453.3.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 453.3.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 453.3.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 453.3.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 453.3.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 453.3.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 453.3.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 463.3.9 Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . 463.3.10 Control and Prevention . . . . . . . . . . . . . . . . . 46
3.4 Fascioliasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 463.4.1 Common Name/Synonyms . . . . . . . . . . . . . . 463.4.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 463.4.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 463.4.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 463.4.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 463.4.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 473.4.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 473.4.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 473.4.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
xii Contents
3.5 Fasciolopsiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 473.5.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 483.5.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 483.5.3 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 483.5.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 483.5.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 483.5.6 Disease in Man . . . . . . . . . . . . . . . . . . . . . . 483.5.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 483.5.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
3.6 Gastrodisciasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 483.6.1 Common Name/Synonyms . . . . . . . . . . . . . . 483.6.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 493.6.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 493.6.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 493.6.5 Clinical Signs in Man and Animals . . . . . . . . 493.6.6 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 49
3.7 Heterophyiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 493.7.1 Common Name/Synonyms . . . . . . . . . . . . . . 493.7.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 493.7.3 Metagonimiasis . . . . . . . . . . . . . . . . . . . . . . 493.7.4 Heterophyiasis Due to Heterophyes Species. . . 503.7.5 Haplorchiasis . . . . . . . . . . . . . . . . . . . . . . . . 51
3.8 Nanophyetus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513.8.1 Common Name/Synonyms . . . . . . . . . . . . . . 513.8.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 513.8.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 513.8.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 513.8.5 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 523.8.6 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 523.8.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 523.8.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 523.8.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 523.8.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
3.9 Other Liver Flukes . . . . . . . . . . . . . . . . . . . . . . . . . . . 523.9.1 Clonorchiasis . . . . . . . . . . . . . . . . . . . . . . . . 523.9.2 Opisthorchiasis. . . . . . . . . . . . . . . . . . . . . . . 533.9.3 Metorchiosis (Canadian Liver Fluke) . . . . . . . 53
3.10 Paragonimiasis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 533.10.1 Common Name/Synonyms . . . . . . . . . . . . . . 533.10.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 543.10.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 543.10.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 543.10.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 543.10.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 543.10.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 553.10.8 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 553.10.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 563.10.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Contents xiii

3.11 Schistosomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 563.11.1 Common Name/Synonyms . . . . . . . . . . . . . . 563.11.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 563.11.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 563.11.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 563.11.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 573.11.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 573.11.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 583.11.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 583.11.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 583.11.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
4 Cestode Zoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 654.1 Coenurosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
4.1.1 Common Name/Synonyms . . . . . . . . . . . . . . 664.1.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 664.1.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 664.1.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 664.1.5 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 664.1.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 674.1.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 674.1.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
4.2 Diphyllobothriasis . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.2.1 Common Name/Synonyms . . . . . . . . . . . . . . 674.2.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 674.2.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 674.2.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 684.2.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 684.2.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 684.2.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 684.2.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 684.2.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
4.3 Dipylidiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 684.3.1 Common Name/Synonyms . . . . . . . . . . . . . . 684.3.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 694.3.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 694.3.4 Life Cycle and Transmission in Man . . . . . . . 704.3.5 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 704.3.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 704.3.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 704.3.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
4.4 Echinococcosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 714.4.1 Common Name/Synonyms . . . . . . . . . . . . . . 714.4.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 714.4.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 714.4.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 714.4.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 714.4.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 72
xiv Contents

4.4.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 724.4.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 734.4.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73
4.5 Sparganosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 744.5.1 Common Name/Synonyms . . . . . . . . . . . . . . 744.5.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 744.5.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 744.5.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 744.5.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 744.5.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 754.5.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 754.5.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 754.5.9 Prevention and Control . . . . . . . . . . . . . . . . . 75
4.6 Taeniasis and Cysticercosis . . . . . . . . . . . . . . . . . . . . . 764.6.1 Common Name/Synonyms . . . . . . . . . . . . . . 764.6.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 764.6.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 764.6.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 764.6.5 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 764.6.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 774.6.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 774.6.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
4.7 Other Cestode Zoonoses . . . . . . . . . . . . . . . . . . . . . . . 784.7.1 Bertiellosis . . . . . . . . . . . . . . . . . . . . . . . . . 784.7.2 Hymenolepiosis . . . . . . . . . . . . . . . . . . . . . . 794.7.3 Inermicapsiferosis. . . . . . . . . . . . . . . . . . . . . 794.7.4 Mesocestoidosis . . . . . . . . . . . . . . . . . . . . . . 794.7.5 Raillietinosis . . . . . . . . . . . . . . . . . . . . . . . . 79
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
5 Nematode Zoonoses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 835.1 Acanthocephalus . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
5.1.1 Common Name/Synonyms . . . . . . . . . . . . . . 835.1.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 835.1.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 845.1.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 845.1.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 845.1.6 Clinical Signs in Man and Animals . . . . . . . . 845.1.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 855.1.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
5.2 Angiostrongylosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . 855.2.1 Common Name/Synonyms . . . . . . . . . . . . . . 855.2.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 855.2.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 855.2.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 855.2.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 855.2.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 865.2.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 86
Contents xv

5.2.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 865.2.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
5.3 Anisakiosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 865.3.1 Common Name/Synonyms . . . . . . . . . . . . . . 875.3.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 875.3.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 875.3.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 875.3.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 875.3.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 875.3.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 875.3.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 885.3.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
5.4 Ascariosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 885.4.1 Common Name/Synonyms . . . . . . . . . . . . . . 885.4.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 885.4.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 895.4.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 895.4.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 895.4.6 Clinical Signs in Man and Animals . . . . . . . . 895.4.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 895.4.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89
5.5 Baylisascariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 895.5.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 895.5.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 905.5.3 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 905.5.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 905.5.5 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 905.5.6 Clinical Signs in Animals . . . . . . . . . . . . . . . 905.5.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 905.5.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
5.6 Capillariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 915.6.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 915.6.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 915.6.3 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 915.6.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 915.6.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 925.6.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 925.6.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 925.6.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 925.6.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
5.7 Cutaneous Larva Migrans . . . . . . . . . . . . . . . . . . . . . . 925.7.1 Common Name/Synonyms . . . . . . . . . . . . . . 925.7.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 925.7.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 925.7.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 935.7.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 935.7.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 935.7.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 935.7.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 93
xvi Contents

5.7.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 935.7.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
5.8 Dioctophymosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 935.8.1 Common Name/Synonyms . . . . . . . . . . . . . . 935.8.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 935.8.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 935.8.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 945.8.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 945.8.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 945.8.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 945.8.8 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 945.8.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 945.8.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
5.9 Dracunculiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 945.9.1 Common Name/Synonyms . . . . . . . . . . . . . . 945.9.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 955.9.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 955.9.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 955.9.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 955.9.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 955.9.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 955.9.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 955.9.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 955.9.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
5.10 Gnathostomiasis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 965.10.1 Common Name/Synonyms . . . . . . . . . . . . . . 965.10.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 965.10.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 965.10.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 965.10.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 965.10.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 975.10.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 975.10.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 975.10.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 975.10.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
5.11 Gongylonemosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 975.11.1 Common Name/Synonyms . . . . . . . . . . . . . . 975.11.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 975.11.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 985.11.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 985.11.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 985.11.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 985.11.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 995.11.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 995.11.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 995.11.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99
5.12 Lagochilascariosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 995.12.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 995.12.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 99
Contents xvii

5.12.3 Reservoir and Transmission of the Disease . . . 995.12.4 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 995.12.5 Disease in Man . . . . . . . . . . . . . . . . . . . . . . 1005.12.6 Disease in Animals. . . . . . . . . . . . . . . . . . . . 1005.12.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1005.12.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
5.13 Mammomonogamus . . . . . . . . . . . . . . . . . . . . . . . . . . 1005.13.1 Common Name/Synonyms . . . . . . . . . . . . . . 1005.13.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1005.13.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1005.13.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.13.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1015.13.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.13.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1015.13.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1015.13.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.13.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101
5.14 Micronemosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.14.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.14.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1015.14.3 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1015.14.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1025.14.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1025.14.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1025.14.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 1025.14.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1025.14.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
5.15 Oesophagostomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . 1025.15.1 Common Name/Synonyms . . . . . . . . . . . . . . 1025.15.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1025.15.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1025.15.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1035.15.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1035.15.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1035.15.7 Clinical Signs in Man and Animals . . . . . . . . 1035.15.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1035.15.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
5.16 Strongyloidiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1035.16.1 Common Name/Synonyms . . . . . . . . . . . . . . 1035.16.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1035.16.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1045.16.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1045.16.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1045.16.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1045.16.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1045.16.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1045.16.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1045.16.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
xviii Contents

5.17 Thelaziasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1045.17.1 Common Name/Synonyms . . . . . . . . . . . . . . 1055.17.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.17.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1055.17.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.17.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1055.17.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.17.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1055.17.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1055.17.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.17.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
5.18 Trichinosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.18.1 Common Name/Synonyms . . . . . . . . . . . . . . 1065.18.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1065.18.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1065.18.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1065.18.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1065.18.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1065.18.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1075.18.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1075.18.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1075.18.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 107
5.19 Trichostrongylosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 1085.19.1 Common Name/Synonyms . . . . . . . . . . . . . . 1085.19.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1085.19.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1095.19.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1095.19.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1095.19.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1095.19.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1095.19.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1095.19.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1095.19.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 109
5.20 Trichuriasis of Animal Origin . . . . . . . . . . . . . . . . . . . 1095.20.1 Common Name/Synonyms . . . . . . . . . . . . . . 1095.20.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1095.20.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1105.20.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1105.20.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1105.20.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1105.20.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1105.20.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1105.20.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1105.20.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 110
5.21 Visceral Larva Migrans . . . . . . . . . . . . . . . . . . . . . . . 1105.21.1 Common Name/Synonyms . . . . . . . . . . . . . . 1105.21.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1105.21.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1115.21.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 111
Contents xix

5.21.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1115.21.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1115.21.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1115.21.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1115.21.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1115.21.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
5.22 Zoonotic Ancylostomiasis . . . . . . . . . . . . . . . . . . . . . . 1125.22.1 Common Name/Synonyms . . . . . . . . . . . . . . 1125.22.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1125.22.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1125.22.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1135.22.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1135.22.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1135.22.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1135.22.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1135.22.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1135.22.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113
5.23 Zoonotic Filariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . 1145.23.1 Common Name/Synonyms . . . . . . . . . . . . . . 1145.23.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1145.23.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1145.23.4 Reservoir. . . . . . . . . . . . . . . . . . . . . . . . . . . 1145.23.5 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1145.23.6 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1145.23.7 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1145.23.8 Clinical Signs in Animals . . . . . . . . . . . . . . . 1155.23.9 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1155.23.10 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 115
6 Arthropod Zoonoses. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1236.1 Myiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
6.1.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1236.1.2 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1246.1.3 Clinical Signs in Animals . . . . . . . . . . . . . . . 1246.1.4 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1246.1.5 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1246.1.6 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124
6.2 Pentastomiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1246.2.1 Common Name/Synonyms . . . . . . . . . . . . . . 1246.2.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1246.2.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1256.2.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1256.2.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1256.2.6 Clinical Signs in Man . . . . . . . . . . . . . . . . . . 1256.2.7 Clinical Signs in Animals . . . . . . . . . . . . . . . 1256.2.8 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1256.2.9 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125
xx Contents

6.3 Tungiasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.1 Synonyms . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.3 Epidemiology. . . . . . . . . . . . . . . . . . . . . . . . 1266.3.4 Transmission . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.5 Life Cycle . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.6 Clinical Signs in Man and Animals . . . . . . . . 1266.3.7 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.3.8 Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126
6.4 Zoonotic Dermatitis . . . . . . . . . . . . . . . . . . . . . . . . . . 1266.4.1 Zoonotic Scabies . . . . . . . . . . . . . . . . . . . . . 1266.4.2 Tick Infestations. . . . . . . . . . . . . . . . . . . . . . 1276.4.3 Dermatitis Due to Acarid Parasites Belonging
to Families Cheyletiellidae, Dermanyssidaeand Macronyssidae . . . . . . . . . . . . . . . . . . . . 128
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129
About the Authors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 133
Contents xxi

1Introduction
Abstract
Parasitism is basically association between two species: Parasite (firstspecies) and the host (second species). Parasitic diseases cause significantproblems in the developing world. At present, there are more than 15protozoa and 50 other parasitic diseases that are zoonotic in nature.Zoonotic parasites are important due to their human and animal health,food safety and economic concerns. Emergence and re-emergence ofmany zoonotic parasites have been reported across the globe. Contam-inated water and food significantly increase the transmission of theseparasites. Factors influencing prevalence of these parasites includeresurgence in vector population, climate change coupled with globalwarming, international food trade, poverty and lack of safe drinkingwater in non-industrialised countries, etc. Most of the animals which livein close contact with man could harbour and transmit zoonotic parasitesto human beings. Livestock, pets, domiciliated, wild animals, fish andsome other animals; all of them could transmit zoonotic parasites. Anupdate on current status of zoonotic parasites has been provided.
Parasitism is basically association between twospecies: Parasite (first species) and the host(second species). In this association, parasitelives on the host or its tissue for certain periods oftime. This association can be of different types,viz. symbiosis, commensalism, mutualism,phoresis, predation or parasitism. Such hostparasite relationship could lead to pathologicaldisorders and disease in the host. In animals andman, many important diseases occur due to par-asites. Parasitic diseases cause significant prob-lems particularly in the developing world.Approximately 370 parasitic species (300 hel-minths and 70 protozoa) have been found inhuman beings (Ashford and Crewe 1998;
Cox 2002). Out of these, some parasites causeimportant parasitic diseases in man. The para-sites are generally classified under the categories:Protozoa, helminths and arthropods (Fig. 1.1).
At present, there are more than 15 protozoaand 50 other parasitic diseases that are zoonoticin nature. Zoonotic parasites are important dueto their human and animal health, food safetyand economic concerns.
As per World Health Organization (Acha andSzyfres 2006), zoonoses are defined as ‘‘thosediseases and infections (the agents of) which arenaturally transmitted between (other) vertebrateanimals and man’’. Many new zoonotic diseaseshave been recognised in the recent past to further
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_1, � Springer India 2013
1

expand the existing list of zoonotic diseases.Zoonotic parasitology is the study of phenome-non of parasites which are zoonotic in nature. Inother words, parasitic zoonoses are the combi-nation of two subjects: Parasitology and zoono-ses where knowledge of both the fields comesinto play for study of zoonotic parasites.
Parasitic zoonotic diseases are prevalentworldwide. First reports, emergence andre-emergence of zoonotic parasites, have beenrecorded in human and animal populations in thepast decades (Singh et al. 2010). Importantfactors that influence the occurrence of zoonoticparasites, particularly in the developing world,include climate change and global warming,vector populations, poverty, lack of safe drink-ing water, presence of stray animals, defecatingoutdoors, poor personal hygiene and the highpopulation density (Singh et al. 2011).
Parasitic zoonoses can be classified intodifferent categories as in case of zoonoses(Schwabe 1984). Parasitic zoonoses are the mostdiversified group of zoonotic diseases repre-senting all classes of zoonotic diseases classifiedon different bases.
1.1 Classification of ParasiticZoonoses
1.1.1 Based on Etiological Agents
1. Protozoonoses: cryptosporidiosis, giardiasis,toxoplasmosis, etc.
2. Trematode zoonoses: clonorchiosis, para-gonimiasis, etc.
3. Cestode zoonoses: hydatidosis, taeniosis,cysticercosis, etc.
4. Nematode zoonoses: larva migrans, trichi-nosis, zoonotic ancylostomiasis, etc.
5. Arthropod zoonoses: myiases, zoonotic sca-bies, etc.
1.1.2 Based on Transmission Cycle
The parasitic zoonotic diseases can be classifieddepending upon the life cycle of the zoonoticpathogens.
1. Direct parasitic zoonoses: The parasite istransmitted by direct contact or indirectly
Fig. 1.1 Classification of parasites
2 1 Introduction

through food, e.g. scabies, trichinellosis,giardiasis, etc.
2. Cyclozoonoses: The diseases caused byzoonotic parasites require two or more ver-tebrate hosts to complete life cycle of theparasite. Cyclozoonoses are further classi-fied under two categories:(a) Obligatory cyclozoonoses: Human
beings must act as host to complete lifecycle of the parasite, e.g. Taenia soliumand Taenia saginata taeniosis.
(b) Non-obligatory cyclozoonoses: Humanbeings are not required to completelifecycle of the parasite but could act asaccidental host, e.g. human hydatidosis.
3. Metazoonoses: The diseases caused bythose zoonotic parasites which require bothvertebrate and invertebrate species tocomplete life cycle of the parasite. Meta-zoonoses are further classified under fourcategories:(a) Metazoonoses type I: The diseases caused
by those zoonotic parasites which requireone invertebrate and one vertebrate host,e.g. Dipylidium caninum dipylidiasis.
(b) Metazoonoses type II: The diseasescaused by those zoonotic parasiteswhich require two invertebrate and onevertebrate hosts, e.g. paragonimiasis.
(c) Metazoonoses type III: The diseasescaused by those zoonotic parasiteswhich require one invertebrate and twovertebrate hosts, e.g. clonorchiosis.
(d) Metazoonoses type IV: The diseasescaused by those zoonotic parasiteswhich require transovarian transmis-sion, e.g. Babesia divergens babesiosis.
4. Saprozoonoses: The diseases caused bythose zoonotic parasites which require non-animate material in addition to their hostsfor completion of life cycle. Saprozoonosesare further classified under three categories:(a) Saproanthropozoonoses: Animals princi-
pally act as reservoir host and the etio-logical agents are transmitted from
animals to man through inanimate mate-rial, e.g. cutaneous larva migrans, myiasis.
(b) Saproamphixenoses: Both animals andhumans could act as reservoir hosts andthe etiological agents are transmittedthrough inanimate objects, e.g. probablymicronemosis.
(c) Saprometanthropozoonoses: Sapromet-anthropozoonoses require vertebratehost, invertebrate host and inanimatesubstance for transmission of disease,e.g. fasciolosis.
1.1.3 Based on Reservoir Hosts
1. Anthropozoonoses: The diseases in whichanimals act as reservoir hosts and humansbecome accidentally infected, e.g. hydatido-sis, visceral larvae migrans.
2. Zooanthroponoses: These diseases are nor-mally present in humans but could be trans-mitted to animals, e.g. amoebosis.
3. Amphixenosis: The diseases in which bothman and animals could act as reservoir hosts,e.g. clonorchiosis.
1.1.4 Based on Principal HostInvolved
1. Cattle-related parasitic zoonoses: T. saginatataeniosis, cryptosporidiosis.
2. Sheep-related parasitic zoonoses: fasciolosis,hydatidosis.
3. Pig-related parasitic zoonoses: ascariasis,swine taeniosis.
4. Fish-related parasitic zoonoses: diphyllo-bothriosis.
5. Dog-related parasitic zoonoses: ancylosto-miasis, echinococcosis.
6. Cat-related parasitic zoonoses: toxoplas-mosis.
7. Racoon-related parasitic zoonoses: baylisa-scariosis.
1.1 Classification of Parasitic Zoonoses 3

1.2 Animal-Related ParasiticZoonoses
Most of the animals which are in close contactwith man could harbour and transmit zoonoticparasites to human beings. Livestock, pets,domiciliated, wild animals, fish and some otheranimals, all of them could transmit zoonoticparasites (Parija 1990).
1.2.1 Livestock-Related ParasiticZoonoses
Livestock is an essential component of humanactivities particularly for dairy farmers, veteri-narians and other related occupations. The foodof animal origin, viz. meat, milk and theirproducts are essential components of humandiet. The human and livestock populations livein close association with each other. This closeassociation and dependence for food can resultin transmission of zoonotic parasites whenproper hygienic measures are not taken. Thesediseases can be transmitted either through food,contaminated water or by vector population.
Livestock transmitted parasitic zoonoses canbe classified either on the basis of speciesinvolved or on the basis of mode of their trans-mission (Figs. 1.2, 1.3, 1.4, 1.5, 1.6, 1.7).
Based on the animal species involved, theycan be classified into:1. Cattle-related parasitic zoonoses: B. divergens
babesiosis, cryptosporidiosis, sarcocystosis,fasciolosis, T. saginata taeniosis.
2. Pig-related parasitic zoonoses: balantidiasis,sarcocystosis, toxoplasmosis, gastrodiscoi-dosis, T. solium taeniosis, ascariosis, gna-thostomosis, trichinosis.
3. Sheep-related parasitic zoonoses: toxoplas-mosis, fasciolosis.
4. Goat related parasitic zoonoses: toxoplas-mosis.
1.2.2 Wildlife-Related ParasiticZoonoses
Human beings, particularly hunters, forestworkers, agricultural workers, army personnel,tourists and other related occupational workers,may be exposed to wild animal-related parasiticzoonoses. The wild animal reservoir hosts ofsome diseases may also enter human anddomestic animal habitations leading to theirtransmission and occurrence in human beings.
Examples of wildlife-related parasiticzoonoses
Opossums (Didelphis albiventris, Didelphis mar-supialis): Trypanosoma cruzi trypanosomosis.
Fig. 1.2 Zoonoticparasites of pig
4 1 Introduction

Monkeys: malaria of simian origin.Wild cats: toxoplasmosis.Wild felids: baylisascariosis.Wild boar: trichinosis.Racoons: baylisascariosis.
1.2.3 Domiciliated Animals
Domiciliated animals live in close associationwith human habitats. They may be partly depen-dent on man for food and shelter. Resultantly, theycan always transmit zoonotic parasitic diseases.
Examples of Domiciliated animal-relatedparasitic zoonoses
Rodents: Babesia microti babesiosis, leishmani-osis, angiostrongylosis.
Reptile/amphibian borne: sparganosis, gnathos-tomosis.
1.2.4 Pet Animal-Related ParasiticZoonoses
Pet animals are kept by man for companionship,security and enjoyment. Dogs and cats are themost common and popular pets kept worldwide.
Fig. 1.3 Zoonoticparasites of cattle
Fig. 1.4 Zoonoticparasites of sheep and goat
1.2 Animal-Related Parasitic Zoonoses 5

Poor animal hygiene may result in transmissionof such diseases to the human population.
Examples of Pet animal-related parasiticzoonoses
Dogs: T. cruzi trypanosomosis, leishmaniosis,diplydiasis, echinococcosis, cutaneous larvamigrans, gnathostomosis, toxocariasis.
Cats: T. cruzi trypanosomosis, toxoplasmosis,diplydiasis, cutaneous larvae migrans,gnathostomosis.
1.2.5 Fish, Shellfish and Mollusc-Borne Parasitic Zoonoses
Fish are aquatic vertebrates and are essentialcomponent of human diet. Fish is an importantsource of protein for man. Ingestion of con-taminated raw fish may transmit importantzoonotic infections.
Examples of Fish, shellfish, craband mollusc-borne parasitic zoonoses
Fig. 1.5 Zoonoticparasites of rodents
Fig. 1.6 Zoonoticparasites of cat
6 1 Introduction

Angiostrongylosis, paragonimiasis, anisakiosis,clonorchiosis, diphyllobothriosis, echinosto-mosis, Heterophyes heterophyes infections,Haplorchis spp. infections, Matagonimusyokogamai infections (Figs. 1.8, 1.9).
1.3 Occupational ParasiticZoonoses
Occupational parasitic zoonoses are the zoonoticparasitic diseases which may occur due to theoccupational environment in persons relatedwith specific occupation. There is increased riskof contacting such diseases in persons workingin specific occupational areas. In addition tooccupational zoonoses, immunocompromisedpersons are always at higher risk of beinginfected with zoonotic parasites such as Cryp-tosporidium parvum, Toxoplasma gondii, etc.There is also a strong correlation between
occurrence of zoonotic babesiosis among sple-nectomized individuals (Fig. 1.10).
1.3.1 Prevention and Control
• To generate better awareness regardingtransmission and prevention of occupationalzoonoses among related occupational groups.
• Monitoring and surveillance of occupationallyrelated zoonotic parasites among risk groups.
• Control of such disease in their animal hosts.
1.4 Food Borne Parasitic Zoonoses
The food animals, viz. cattle, buffalo, sheep,goat and pigs consume fodder crops and convertthem into animal protein. The meat from theseanimals is an important source of protein andnutrients (Gracey and Collins 1992). Fish and
Fig. 1.7 Zoonoticparasites of dog
1.2 Animal-Related Parasitic Zoonoses 7

other sea foods also make a vital contribution toprovide essential nourishment for human popu-lation. The meat of wild animals is also used as a
part of human diet in many parts of the world.Poultry are another important meat producingspecies. Besides fish and meat, milk and rawvegetables also form important components ofhuman food. Food and water are the twoessential components of human diet. The food ofanimal origin is a rich source of proteins, energy,vitamins and minerals. The food especially ofanimal origin is essential for growth and devel-opment of human beings.
However, presence of zoonotic parasites insuch food and contaminated water could lead totheiroccurrenceinmanandanimals.Transmissionof zoonoses of parasitic origin through food haspublic health as well as socio-economic signifi-cance (Slifko et al. 2000). Transmission of zoo-notic parasites through contaminated water, food,plants, vegetables and soil assumes great impor-tance (Slifko et al. 2000; Zhou et al. 2008). Foodsecurity is an important issue due to increasinghuman populations, income levels, changing foodpreferences and urbanisation. The demand forfood of animal origin is increasing worldwide.
Food and water act as an important route oftransmission for parasites from one host toanother. Food and water are also important fortransmission of parasites which require morethan one host to complete their life cycle
Fig. 1.8 Zoonotic parasites of some other animals
Fig. 1.9 Zoonotic parasites of man
8 1 Introduction

(Bhatia 1991). The important parasites trans-mitted through food and water includes T. soli-um, Echinococcus granulosus, T. gondii, etc.Parasites exploit behavioural patterns of theirhosts for further transmission among animals andhumans (Gajadhar et al. 2006). Further, parasitelife cycle stages such as eggs and oocysts havethe ability to resist and survive adverse envi-ronmental conditions (Gajadhar et al. 2006).Many factors have lead to an increased risk forthe occurrence of food borne zoonotic parasites.Climate change and increased food trade havemanifold increased the risk of food borne para-sitic zoonoses. Increased demand for animal fooddue to rapid urbanisation, increase in humanpopulation and high income indicates need formore emphasis on food safety issues (Gajadhar
et al. 2006). Many emerging zoonotic parasitesare food borne in nature (WHO 2002)(Fig. 1.11).
Prevention and control strategies shouldinclude use of advanced serological and molec-ular diagnostic techniques, continuous monitor-ing of zoonotic parasites, health education,social and economic development particularly inthe developing world; and prompt treatment ofcases (Dorny et al. 2009). Many importantparasites shed their eggs in the faeces whichserve as an important source of infection leadingto contamination of environment particularlywater and food supplies (Slifko et al. 2000).One or more life cycle stages of the parasitecan transmit the infection. For example, inges-tion of only infectious oocysts leads to
Fig. 1.10 Occupational parasitic zoonoses
Fig. 1.11 Food borne parasitic zoonoses
1.4 Food Borne Parasitic Zoonoses 9

cryptosporidiosis, whereas both oocysts andtissue cysts of T. gondii can cause infection inman (Slifko et al. 2000).
1.4.1 Fish, Shellfish and Mollusc-Borne Parasitic Zoonoses
Fish and related zoonoses can be classified intotrematode, cestode and nematode zoonoses.Trematode diseases can be further sub-classifiedinto liver and intestinal flukes. As perWHO (1995), fish-borne trematodes infect morethan 18 million people and globally more thanhalf a billion people are at risk from these dis-eases (Chai et al. 2005) (Fig. 1.12).
1.4.1.1 Prevention and Control• Avoid eating raw or improperly cooked fish.• Interruption in the transmission cycle of the
parasite.• Health education and environmental
sanitation.• Use of clean water in slaughtering operations
to avoid contamination with other water-bornezoonotic parasites.
1.4.2 Meat-Borne Parasitic Zoonoses
Many important parasitic zoonotic diseases aremeat-borne in nature, e.g. toxoplasmosis, taeni-osis, trichinellosis, etc. Most of the food pro-ducing animals (except poultry), viz. cattle,
Fig. 1.12 Fish-shellfish and mollusc-borne parasitic zoonoses
Fig. 1.13 Meat-borne parasitic zoonoses
10 1 Introduction

buffalo, pig, sheep and goat could transmitzoonotic parasites. Meat-borne parasitic diseasescan be further classified either on the basis ofanimal host involved or into protozoan, trema-tode, cestode and nematode meat-borne parasiticzoonoses (Figs. 1.13, 1.14).
1.4.2.1 Prevention and Control• Avoid consumption of raw or under cooked
meat.• Provide safe food and water to livestock.
• Use of best hygienic practices during slaugh-tering operations to avoid contamination withother water-borne zoonotic parasites.
1.4.3 Water-Borne Parasitic Zoonoses
These parasites are prevalent worldwide andpose a significant threat particularly in thedeveloping world (Gajadhar and Allen 2004).The non-availability of clean and hygienicdrinking water is an important risk in thedeveloping world. The parasite stages that canbe transmitted through water range from uni-cellular amoebae to complex metazoans such astrematodes and cestodes (Gajadhar andAllen 2004). The life cycle stages of these par-asites are well adapted for their survival in theenvironment and further dissemination by water(Gajadhar and Allen 2004). Many importantzoonotic parasites such as C. parvum, T. gondii,could be transmitted through contaminatedwater. Transport hosts such as swine can also
Fig. 1.14 Meat-borne parasitic zoonoses
Fig. 1.15 Water-borne parasitic zoonoses
Fig. 1.16 Vector-borne parasitic zoonoses
1.4 Food Borne Parasitic Zoonoses 11

play an important role in collection and con-centration of resistant exogenous stages (Gaja-dhar and Allen 2004) of many parasites.Important water-borne parasitic zoonoses can beclassified through protozoa, trematode and ces-tode zoonoses, but protozoan zoonoses are morecommon and significant (Fig. 1.15).
1.4.3.1 Prevention and Control• Use properly filtered water for drinking
purpose.• Routine monitoring of drinking water.
• Regular deworming of reservoir and animalhosts.
• Avoid surface contamination of swimmingpools.
1.4.4 Milk-Borne Parasitic Zoonoses
Although milk is considered as safer food inrelation to zoonotic parasites, but milk of cap-rine and ovine can cause toxoplasmosis in man ifthe animal is infected with the disease and rawmilk is consumed. Additionally, external faecal
Fig. 1.17 Classification of vector-borne parasitic zoonoses as per Colwell et al. (2011)
12 1 Introduction

contamination during or after milking couldpose additional risks for transmission of someimportant zoonotic parasites.
1.4.5 Raw Vegetables/Plant-BorneParasitic Zoonoses
The role of raw vegetables/salad in transmissionof zoonotic parasites gets attention particularly incases of neurocysticercosis in humans wherehuman sewage has been used for irrigation pur-poses for farmland used to grow vegetables and ithas been found to be an important risk fortransmission of the disease. Fasciolosis is anotherimportant disease which can be transmittedthrough ingestion of contaminated plants. Thecontamination of vegetables could also help intransmission of parasites such as Ascaris suumand Toxocara species (Slifko et al. 2000).
1.4.6 Reptile, Amphibian-BorneParasitic Zoonoses
Sparganosis and Gnathostomosis are twoimportant cestode and nematode diseases,respectively which can occur in human beingsdue to consumption of raw or under cookedreptiles or amphibians.
1.4.7 Poultry-Related ParasiticZoonoses
No zoonotic parasites are present in poultry meatand it is generally free from zoonotic parasitesexcept that clean water should be used inslaughtering operations. However, free rangingchicken could serve as important reservoir fortoxoplasmosis. A recent study has demonstratedthat poultry may serve as a minor reservoir forfish borne trematodes (Anh et al. 2010).
1.5 Soil-Transmitted ParasiticZoonoses
Soil-transmitted zoonotic parasites include hel-minth infections, viz. ascariosis due to Ascarislumbricoides, hookworm infections dueto Ancylostoma spp. and toxocarosis due toToxocara canis and Toxocara cati under moistconditions. The parasite eggs are generallyfound in soil of tropical and sub-tropical coun-tries (Bethony et al. 2006). These parasites maylead to anaemia and growth retardation.
1.5.1 Prevention and Control
• Periodic deworming with anthelmintic drugs.• To generate awareness regarding soil-
transmitted helminths in school children.• Improved personal hygiene.• Control of disease in animal hosts.
1.6 Vector-Borne ParasiticZoonoses
Vector-borne parasitic zoonoses (VBPZ) are thediseases in which zoonotic parasites are trans-mitted from an infected animal to human beingsby an arthropod or other vector. Climate changeand global warming could affect occurrence,intensity and seasonality of many vector-bornezoonotic parasites. VBPZ are important as theyaffect human and animal health (WHO 2004)and cause economic losses (Bram et al. 2001).Factors responsible for emergence of VBPZinclude climate change (Lindgren and Gustaf-son 2001; Rosenthal 2009), increased tourism,animal transport and international food trade(Weijden et al. 2007), drug resistance in parasiteand vector (Takken and Knols 2007), and chan-ges in land-use pattern (Colwell et al. 2011).
VBPZ can be classified either on the basis ofvector involved or into protozoa, cestode andnematode vector-borne zoonoses. Under VBPZ,
1.4 Food Borne Parasitic Zoonoses 13

protozoan-related zoonoses are most importantand significant.
Depending upon the vector involved, VBPZcan be classified into fly, mosquito, mites, bugs,flea and tick-borne parasitic zoonoses(Figs. 1.16, 1.17).
1.6.1 Prevention and Control
1. Use of physical barriers such as mosquitonets.
2. Biological control of vector population.3. Destroy or modify vector breeding grounds.4. Use of chemicals and herbal insecticides as
repellant/killer, etc.5. Reduction in the reservoir hosts of infection.6. Personal prevention strategies.
References
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals. Scientific andtechnical publication No. 580. World Health Organi-zation, Geneva
Anh NTL, Madsen H, Dalsgaard A, Phuong NT, ThanhDTH, Murrell KD (2010) Poultry as reservoir hostsfor fishborne zoonotic trematodes in Vietnamese fishfarms. Vet Parasitol 169:391–394
Ashford RW, Crewe W (1998) The parasites of Homosapiens. Liverpool School of Tropical Medicine,Liverpool
Bethony JR, Brooker S, Albonico M, Geiger SM, LoukasA, Diemert D, Hotez PZ (2006) Soil-transmittedhelminth infections: ascariasis, trichuriasis, and hook-worm. Lancet 367:1521–1532
Bhatia BB (1991) Current status of food-borne parasiticzoonoses in India. In: Cross JH (ed) Emergingproblems in food-borne parasitic zoonosis: impact onagriculture and public health. Proceedings of the 33rdSEAMEO-TROPMED regional seminar. SoutheastAsian J Trop Med Public Health 22:36–41
Bram RA, George JE, Reichard RE, Tabachnick WJ(2001) Threat of foreign arthropod borne pathogens tolivestock in the United States. J Med Entomol39:405–416
Chai JY, Murell KD, Lymbery AJ (2005) Fish-borneparasitic zoonoses: status and issues. Int J Parasitol35:1233–1254
Colwell DD, Torres FD, Otranto D (2011) Vectorborneparasitic zoonoses: emerging scenarios and newperspectives. Vet Parasitol 182:14–21
Cox FEG (2002) History of human parasitology. ClinMicrobiol Rev 15(4):595–612. doi:10.1002/9780470688618.taw0166
Dorny P, Praet N, Deckers N, Gabriel S (2009) Emergingfood-borne parasites. Vet Parasitol 163:196–206
Gajadhar AA, Allen JR (2004) Factors contributing to thepublic health and economic importance of waterbornezoonotic parasites. Vet Parasitol 126:3–14
Gajadhar AA, Scandrett WB, Forbes LB (2006) Over-view of food and water borne zoonotic parasites atthe farm level. Rev Sci Tech Off Int Epiz25(2):595–606
Gracey JF, Collins DS (1992) Meat hygiene (9th edn).Published by Bailliere Tindall educational lowpriced book scheme funded by the Britishgovernment
Lindgren E, Gustafson R (2001) Tickborne encepha-litis in Sweden and climate change. Lancet358:16–18
Parija SC (1990) Review of parasitic zoonoses. AITBSPublishers Distributors, New Delhi
Rosenthal J (2009) Climate change and the geographicdistribution of infectious diseases. EcoHealth6:489–495
Schwabe CW (1984) Veterinary Medicine and HumanHealth, 3rd edn. Williams and Wilkins, USA 428 EastPreston Street
Singh BB, Sharma R, Sharma JK, Juyal PD (2010)Parasitic zoonoses in India: an overview. Rev SciTech Off Int Epiz 29(3):629–637
Singh BB, Sharma R, Gill JPS, Aulakh RS, Banga HS(2011) Climate change, zoonoses and India. Rev SciTech Off Int Epiz 30(3):779–788
Slifko TR, Smith VH, Rose JB (2000) Emerging parasitezoonoses associated with water and food. Int JParasitol 30:379–393
Takken W, Knols BGJ (2007) Emerging pests and vectorborne diseases in Europe. Wageningen AcademicPublishers, Wageningen
van der Weijden WJ, Marcelis RAL, Reinhold W (2007)Invasions of vectorborne diseases driven by transporta-tion and climate change. In:Takken W, Knols BGJ (eds)Emerging pests and vectorborne diseases in Europe.Wageningen Academic Publishers, Wageningen
WHO (1995) Control of foodborne trematode infections.WHO Tech Rep 849:1–157
WHO (2002) Foodborne diseases, emerging.http://www.who.int/mediacentre/factsheets/fs124/en/print.html
WHO (2004) Changing history. World Health Organiza-tion, Geneva
Zhou P, Chen N, Zhang RL, Lin RQ, Zhu XQ (2008)Food-borne parasitic zoonoses in China: perspectivefor control. Trends Parasitol 24(4):190–196
14 1 Introduction

2Protozoonoses
Abstract
Protozoan zoonoses could be defined as ‘‘those protozoan diseases whichare naturally transmitted between (other) vertebrate animals and man’’.Diseases such as toxoplasmosis and cryptosporidiosis are worldwide inoccurrence. Toxoplasma gondii, Cryptosporidium parvum and Sarcocys-tis suihominis are the most significant coccidian parasites affectinganimals and man. Immunocompromised persons are always at higher riskof being infected with zoonotic parasites such as C. parvum, T. gondii,etc. Cryptosporidiosis is an emerging water-borne protozoan disease ofpublic health significance. The parasite Sarcocystis suihominis isprevalent in pigs in Asian countries such as India and China. Africantrypanosomiasis, Chagas disease, leishmaniasis and zoonotic babesiosisare the important vector borne protozoan zoonotic diseases. Africantrypanosomiasis is still a priority zoonosis for the people in sub-SaharanAfrica. The wild rodent P. leucopus acts as an important reservoir forB. microti human infections. Chagas disease is an important medical andeconomic concern in Latin America. Leishmaniasis has been reportedfrom more than 80 countries.
2.1 African Trypanosomiasis
Order: KinestoplastoridaFamily: Trypanosomatidae
2.1.1 Common Name/Synonyms
Nagana (meaning powerless/useless) disease(Winkle 2005) is the common name for thedisease in animals (African animal trypanoso-miasis) and sleeping sickness is the common
name for the disease in humans (human Africantrypanosomiasis).
2.1.2 History
The parasite is present and infecting the people insub-Saharan Africa since many centuries in thepast (Steverding 2008; Cox 2004). T. brucei wasfirst discovered by David Bruce (1855–1931,Scottish microbiologist and pathologist) as thecause of cattle trypanosomiasis (cattle nagana) in1895 (Bruce 1895). After 6 years, trypanosomeswere observed in the human blood for the first
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_2, � Springer India 2013
15

time in 1901 (Forde 1902). The parasite specieswere later identified and proposed as Trypano-soma gambiense (now T. b. gambiense) (Dutton1902). The second trypanosome species patho-genic to human beings, T. rhodesiense (nowT. b. rhodesiense), was later recovered in 1910(Stephens and Fantham 1910).
2.1.3 Epidemiology
The disease is particularly endemic in Africa.Human epidemics due to severe sleeping sick-ness occurred in Africa in the twentieth century(Steverding 2008). T. brucei gambiense is pres-ent in central and western Africa and T. bruceirhodesiense is present in eastern Africa.
2.1.4 Etiology
Two subspecies of T. brucei, T. brucei rhodes-iense and T. brucei gambiense (Bales 1991;Acha and Szyfres 2006) are responsible forhuman African trypanosomiasis (sleeping sick-ness). T. brucei brucei, the third subspecies onlycauses infection in animals. The chronic andepidemic form of sleeping sickness generallyoccurs due to T. b. gambiense, whereasT. b. rhodesiense infection is responsible for theacute form of the disease.
2.1.5 Reservoir
Human beings act as important reservoirs ofT. b. gambiense. Wild and domestic animalscould also act as important parasite reservoirs forhuman trypanosomiasis (WHO 2006; Njiokouet al. 2006; Simo et al. 2006; Steverding 2008).
2.1.6 Transmission
The bite of an infected tsetse fly belonging togenus Glossina transmits the infection from onehost to the other (Fig. 2.1).
2.1.7 Clinical Signs in Man
The bite of an infected fly leads to eruption ofred sores at the region of the bite. Symptomssuch as fever, swollen lymph glands, headachesand irritability and aching muscles and joints,could arrive within a few weeks.
The disease progresses through two distinctstages. During the initial stage or haemolymphaticphase, the parasite infects the blood and lymphsystem (WHO 2006). The corresponding symp-toms include fever, headache, joint pain and itch-ing. In the later stages (neurological phase), theinvolvement of nervous system leads to symptomssuch as changes in personality, alteration of thebiological clock (the circadian rhythm), confusion,slurred speech, seizures and difficulty in walkingand talking (WHO 2006). This is generally char-acterised by the presence of trypanosomes in thecerebrospinal fluid (WHO 2006). Death may occurin untreated patients within months (in case ofT. b. rhodesiense infections) or within years(in case of T. b. gambiense infections) dependingupon the species involved.
2.1.8 Clinical Signs in Animals
Infections due to T. b. rhodesiense are gener-ally asymptomatic in domestic (cattle andsheep), wild and laboratory animals (Acha andSzyfres 2006). The second parasite species,T. b. gambiense has been occasionally isolatedfrom laboratory animals with no evidence thatit causes disease (Acha and Szyfres 2006).
2.1.9 Diagnosis
The disease may be diagnosed from clinicalsigns; demonstration of the parasite from lymphgland and cerebrospinal fluids, bone marrow andblood; mice inoculation and culture in specialmedia such as glucose, lactoalbumin or GLSH.Serological tests such as card agglutination,ELISA, indirect hemagglutination may also beused but they are of limited value.
16 2 Protozoonoses

2.1.10 Control
The control of the disease includes reduction inthe reservoir host and vector population, che-motherapy and chemoprophylaxis.
2.2 Amoebiasis
Subphylum: SarcodinaOrder: AmoebidoridaFamily: Endamoebidae
2.2.1 Common Name/Synonyms
The disease is known as amoebiasis, amoebicdysentery and entamoebiasis.
2.2.2 History
The amoebae were first found in faecal samples byFeder Losch in 1875 in Saint Petersburg, but he didnot regard them as a cause for dysentery (Pinillaet al. 2008). Later, E. histolytica were pointed out
to be a species complex by Emile Brumpt in 1925,comprising two morphologically similar species,E. dysenteríae and E. dispar found in symptomaticand asymptomatic carriers, respectively (Pinillaet al. 2008). In 1993, Diamond and Clark alsoagreed to Brumpt’s original 1925 hypothesis, withsimilar conclusions (Pinilla et al. 2008). Thishypothesis was accepted by the World HealthOrganisation in 1997 (Pinilla et al. 2008).
2.2.3 Etiology
E. histolytica and E. polecki are of zoonoticimportance. Knowledge regarding E. dispar isquite limited. Most of the asymptomatic amoe-bic infections occur due to E. dispar, althoughE. histolytica asymptomatic colonisation is alsonot uncommon (Braga et al. 1996; Haque et al.1997; Cantellano and Palomo 2000).
2.2.4 Epidemiology
Amoebiasis due to Entamoeba histolytica has aworldwide distribution (WHO 1969, WHO 1985).
Fig. 2.1 Life cycle of T.b. rhodesience
2.1 African Trypanosomiasis 17

Most of the infections have been reported in thedeveloping countries of Central and SouthAmerica, Africa and Asia.
2.2.5 Reservoir
Man is an important reservoir of E. histolytica.
2.2.6 Transmission
Food and water contaminated with faecal matterserve as important sources of infection. Addi-tionally, flies could act as vectors and carry thecysts (Acha and Szyfres 2006).
2.2.7 Life Cycle
The life cycle involves trophozoites which arepresent in host’s large intestine and cysts whichare shed in the faeces of the host. Humansbecome infected by ingesting cysts, throughcontaminated food or water.
2.2.8 Clinical Signs in Man
According to WHO, 50 million cases of colitisand liver abscess and 100,000 deaths resultannually from infection by this organism (WHO1995).
In most cases, the infection remains asymp-tomatic as the parasite lives in the intestine anddoes not cause disease, or causes mild disease.Symptoms of this form include loose or waterystools, abdominal discomfort and stomachcramps. Sometimes, a severe form amoebicdysentery could develop leading to stomachpain, bloody stools and fever. In rare cases, theparasite reaches the liver and forms abscesses.
2.2.9 Clinical Signs in Animals
The disease due to E. histolytica could occur innon-human primates. The parasite has also been
reported from dogs, rats, cats, swine and cattle(Levine 1985). E. polecki has been commonlyreported in swine (Pakandl 1994).
2.2.10 Diagnosis
The disease may be diagnosed from directdemonstration of the parasite (trophozoites andcysts) from faeces, or using specific trichrome oriron hematoxylin staining techniques (Fotedaret al. 2007). The advanced diagnostic testsinclude identification of the parasite based ondetection of E. histolytica-specific antigen andDNA in stool and other clinical samples.Molecular diagnostic tests, such as conventionaland real-time PCR, have also been developed forthe detection and differentiation of E. histolyticaand E. dispar in recent years.
2.2.11 Control
The control of the disease includes improvedpersonal hygiene and avoiding contamination offood and water with infected faeces.
2.3 Babesiosis
Class: PiroplasmidaFamily: Babesiidae
2.3.1 Common Name/Synonyms
The disease is known as babesiasis, piroplas-mosis.
2.3.2 History
Babesia divergens was first described and namedPiroplasma divergens in 1911 (M’Fadyean andStockman 1911). Later, the parasite B. divergenswas identified as the causative agent of the dis-ease in splenectomised humans (Fitzpatrick et al.1968).
18 2 Protozoonoses

The first human case was reported fromCroatia (then Yugoslavia) in 1956. B. divergens(cattle parasite) was believed to be the cause forthis infection. This parasite is mainly responsi-ble for zoonotic babesiosis in Europe (Zintl et al.2003). Another authenticated case due toB. microti has also been recorded from Europe(Hildebrandt et al. 2007).
2.3.3 Etiology
B. microti (Gorenflot et al. 1998; Homer et al.2000; Kjemtrup and Conrad 2000; Telford et al.1993; Telford and Spielman 1997) andB. divergens (Beattie et al. 2002; Herwaldt et al.1996; Olmeda et al. 1997) are the two importantspecies responsible for zoonotic babesiosis.
2.3.4 Epidemiology
In Europe, most cases of human babesiosis arecaused by Babesia divergens (Genchi 2007).Epidemiological surveys have revealed the pres-ence of B. divergens throughout Europe and mayextend beyond Europe into North Africa (Zintlet al. 2003). Human babesiosis due to B. microtiwas reported in the USA in 1969 (Westernet al. 1970). Thirty-one human cases of Babesiainfections have been reported from splenecto-mised individuals in Europe (Gorenflot et al.1998; Marsaudon et al. 1995; Hunfeld et al. 2002).
2.3.5 Reservoir
Infected rodents and animals can serve asimportant reservoirs for other animals. The wildrodent P. leucopus acts as an important reservoirfor B. microti human infections.
2.3.6 Transmission
Ixodes ricinus transmits Babesia divergens andI. scapularis transmits B. microti (Hunfeld andBrade 2004). The adult I. ricinus female
acquires the infection from the infected host andcan transmit transovarially to larvae (Beckeret al. 2009; Zintl et al. 2003) (Fig. 2.2).
2.3.7 Clinical Signs in Man
In immunocompromised patients, acute illnessdue to B. divergens appears suddenly, with hae-moglobinuria as important symptom (Telfordet al. 1993). Persistent high fever (40–41 �C),chills, intense sweats, headaches, myalgia andlumbar and abdominal pain are the other impor-tant symptoms. Vomiting and diarrhoea may alsooccur in a few cases (Gorenflot et al. 1998).Haemolysis could lead to jaundice (Hunfeld et al.2008). Anoxia and toxic waste products couldresult in further complications such as respira-tory, cardiac, renal or hepatic failure.
B. microti might result in acute and mildinfections in immunocompromised and immu-nocompetent individuals, respectively. Asymp-tomatic infections are also not uncommon. Thereported case of an immunocompromised indi-vidual showing symptoms such as fever andchest pain was successfully treated (Hildebrandtet al. 2007). In immunocompromised humans,this parasite may cause medical emergencies dueto rapid fulmination and parasitemias that mayexceed 70 % (Zintl et al. 2003).
2.3.8 Clinical Signs in Animals
In severe cases, there may be fever, anaemia,anorexia, depression and increased respiratoryand heart rate. The mucous membranes becomepale and may be jaundiced (Christensson 1989;Collins et al. 1970; Gray and Murphy 1985;Sherlock et al. 2000). Erythrocyte destructionleads to haemoglobinuria. Death generallyoccurs due to cardiac failure, hepatic or renalinsufficiency (Collins et al. 1970).
2.3.9 Diagnosis
The preliminary diagnosis can be done fromclinical signs such as high fever with
2.3 Babesiosis 19

haemoglobinuria. Definitive diagnosis can bedone with the detection of the parasite in theerythrocytes. Single round or oval forms aregenerally seen in both species. Advanced diag-nostics include serological tests such as IFATand PCR analysis followed by sequencing of thePCR product. Inoculation of infected materialinto splenectomised calves or gerbils is anothersensitive method for detection of the parasite(Gray et al. 1989; Joyner and Davies 1967;L’Hostis et al. 1995).
For detecting B. divergens in ticks, micro-scopic examination of Giemsa-stained smears ofgut or other tick tissues (Gern and Brossard1986; Koch 1906), xenodiagnosis and PCR (Duhet al. 2001) are of great diagnostic value.
2.3.10 Control
Avoid contact with ticks as the infection occursthrough tick bites. Asplenic and immunocom-promised individuals are at the greatest risk and
should take extra care particularly when visitingendemic areas.
2.4 Balantidiosis
Phylum: CiliophoraOrder: TrichostomatoridaFamily: Balantidiidae
2.4.1 Common Name/Synonyms
Balantidiosis is also known as balantidiasis,balantidial or ciliary dysentery.
2.4.2 Etiology
The disease occurs due to Balantidium coli. It isthe largest ciliate protozoan and can infectswine, primates, man and rarely rats, guinea pigsand dogs.
Fig. 2.2 Life cycle of B. microti /B. divergens
20 2 Protozoonoses

2.4.3 History
Malmsten reported B. coli from two patientswith severe diarrhoea in 1857 (Kean et al. 1978).
2.4.4 Epidemiology
The disease is endemic and prevalent world-wide, mostly prevalent in temperate and tropicalregions (Arean and Koppisch 1956). B. coli canbe found in many primates (Nakauchi 1999).
2.4.5 Transmission
Pigs and rat are important sources of infectionfor human beings (Esteban et al. 1998). Man-to-man transmission could occur due to poor per-sonal/environmental hygiene (Giacometti et al.1997). Non-human primates could also transmitthe infection. Humans generally act as asymp-tomatic carriers of B. coli (Esteban et al. 1998).Contaminated water or food containing cystsserve as an important source of infection forhuman beings.
2.4.6 Life Cycle
The cysts shed in the faeces by infected hostscause infection in the susceptible host throughfaecal oral route after ingestion of cyst con-taminated water or food.
2.4.7 Clinical Signs in Man
Balantidiosis at times may resemble intestinalamoebiasis. The acute form is recognised byrapid onset of diarrhoea or dysentery (Castroet al. 1983) and other signs like abdominal colic,nausea and vomiting. In the chronic form, thereare episodes of intermittent diarrhoea alternatingwith normal bowel movements or constipation.Other signs like headache, anorexia, weight lossor muscular weakness could also be present.
2.4.8 Clinical Signs in Animals
The parasite is generally non-pathogenic or cau-ses asymptomatic disease in swine or primates.
2.4.9 Diagnosis
The disease may be diagnosed from direct dem-onstration of the parasite (trophozoites and cysts)from faeces or intestinal scrapings, in wet mountsof fresh faeces. Trophozoites are usually presentin diarrhoeic stools and cysts in solid stools.
2.4.10 Control
The control of the disease includes avoidingcontamination of food and water with infectedfaeces and treatment of infected cases
2.5 Chagas Disease
Order: KinestoplastoridaFamily: Trypanosomatidae
2.5.1 Common Name/Synonyms
The disease is also known as American try-panosomiasis or Chagas mazza disease.
2.5.2 Etiology
American trypanosomiasis/chagas disease iscaused by the protozoan Trypanosoma cruzi.The parasite multiplication generally occursinside the heart and smooth muscle cells.
2.5.3 Epidemiology
Chagas disease is an important medical andeconomic concern in Latin America (Miles et al.2003). According to a survey, more than 10
2.4 Balantidiosis 21

million people act as carriers of Trypanosomacruzi (Collier et al. 1997).
2.5.4 Transmission
Many species of triatomine bug are known(Carcavallo et al. 1998) to carry T. cruzi. Theparasite is transmitted by many species of triato-mine bugs, due to deposition of faeces by infectedvector on the mucous membranes or abraded skin(Miles et al. 2003). Triatomine bugs do not fly tohosts to take a blood meal as in the case of tsetsefly vectors of African trypanosomiasis (Fig. 2.3).The infection occurs when some species oftriatomine bugs colonise houses in large numbersleading to feeding from humans, domestic mam-mals and chickens. The chickens are not suscep-tible to infection, but could serve as an importantsource of blood meal (Miles et al. 2003).
2.5.5 Reservoir
Infected mammals such as armadillo, carnivo-rous animals (dog and cat) and rodents couldserve as reservoirs of infection.
2.5.6 Clinical Signs in Man
Chagas disease is an important cause for heartdisease in Latin America (Tanowitz et al. 1992,Amorin 1979). As per estimates, approximately50,000 deaths have been found associated withthe infection (Espinosa et al. 1985, Garcia-Zapata and Marsden 1986).
2.5.6.1 Acute Clinical Chagas DiseaseThe disease may remain asymptomatic or pres-ent clinical signs. Inflammatory lesion which isalso known as a chagoma may develop at thesite of entry of the T. cruzi (Tanowitz et al.1992). It is generally followed by fever, myal-gia, cephalalgia and unilateral eyelid swelling(Acha and Szyfres 2006).
2.5.6.2 Chronic ChagasCardiomyopathy
Chronic chagas disease may lead to symptomssuch as arrhythmias, thromboembolic events(Oliveira et al. 1983) or congestive heart failure(Tanowitz et al. 1992).
2.5.7 Clinical Signs in Animals
The disease is generally asymptomatic amongwild animals. Symptoms such as fever, palpebraledema, hepatomegaly and alterations in nervoussystem could occur in dogs (Acha and Szyfres2006).
2.5.8 Diagnosis
The disease may be diagnosed from clinicalsigns, demonstration of the parasite from blood,serological testing, laboratory animal inocula-tions and molecular techniques such as PCR.
2.5.9 Control
Combined international efforts have led to sig-nificant reductions in the adverse impact ofchagas disease in the recent years in the Amer-icas (Dias et al. 2002). Use of pesticides such asorganochlorines (dieldrin and gamma-BHC) andother synthetic pyrethroids have effectivelycontrolled vector populations (Dias et al. 2002).Successful implementation of control measuresfor chronic chagas disease have led to themoving of age-specific mortality from the clas-sical 35–55 years to age groups higher than60 years (Dias 2000).
2.6 Cryptosporidiosis
Subclass: CoccideaFamily: Cryptosporidiidae
22 2 Protozoonoses

2.6.1 Common Name/Synonyms
The disease is also known as Cryptosporidiuminfection.
2.6.2 History
Cryptosporidium is recognised as an importanthuman parasite since 1976 (Current and Garcia1991, Fraser et al. 1997). C. parvum has beenresponsible for several water-borne outbreaks(Hayes et al. 1989, MacKenzie et al. 1994).Since 1982, cryptosporidiosis has been increas-ingly recognised as a cause for severe and life-threatening diarrhoea in AIDS patients (Current1983).
2.6.3 Epidemiology
Cryptosporidiosis is an emerging water-borneprotozoan disease of public health significanceworldwide. Cryptosporidium parvum has theability to cause gastrointestinal illness in a widevariety of mammals, including humans, cattle,sheep, goat, pig and horses across the globe(Fayer 1997). C. parvum has been associatedwith neonatal calf diarrhoea (Nydam et al. 2001;Singh et al. 2006) and 1- to 3-week-old calvesare most susceptible (Leek and Fayer 1984;Singh et al. 2006). The parasite has also beenreported in cattle over 2 years of age (Henriksenand Krogh 1985). C. parvum is identified as acommon cause for diarrhoea in immunocompe-tent individuals. In immunodeficient individuals,
Fig. 2.3 Life cycle of T. cruzi
2.6 Cryptosporidiosis 23

the parasite may lead to life-threatening chronicdiarrhoea. In Acquired Immuno DeficiencySyndrome (AIDS) endemic areas in the devel-oping world, the parasite poses a significantpublic health problem (Casemore and Wright1997; Griffiths 1998; O’Donoghue 1995).Infection rates are predicted to be highest indeveloping countries and in children (Fayer1997).
2.6.4 Transmission
The disease occurs through the faecal oral routewhen oocysts excreted by infected man/animalscontaminate food and water. The contaminatedfood and water when ingested leads to infectionin other susceptible hosts.
2.6.5 Reservoir
Neonatal calves are an important source ofinfection to man.
2.6.6 Clinical Signs in Animals
The disease in calves is characterised by weightloss and watery diarrhoea. But it is necessary todistinguish the infection from many other causesof calf diarrhoea. Calves 7- to 21-days old seemto be most susceptible to this infection (Aiello1998; OIE 2005).
2.6.7 Clinical Signs in Man
Clinical signs mainly include watery diarrhoea,stomach cramps and slight fever. Immunocompromised individuals are not able to clearthe parasite (Angus 1983). In immunodeficienthuman beings, Cryptosporidium could lead tolife-threatening chronic diarrhoea.
2.6.8 Diagnosis
The disease can be diagnosed by identifying theoocyst stage of the parasite in host faeces (Garciaet al. 1983; Casemore et al. 1985) or in histo-logical sections taken during necropsy (Current1985). Detection of the parasite in the faeces canbe done by using acid fast or immunofluores-cence staining of unconcentrated faecal smears.Appropriate concentration methods could beused when small numbers of oocysts are present.The parasite can be detected in mucosal scrap-ings of fresh intestine. Concentration techniquessuch as faecal flotation in sucrose or zinc sul-phate solutions could be used. Polymerase chainreaction (PCR) could be used to detect crypto-sporidiosis in water supplies or asymptomaticcarriers. The World Organisation for AnimalHealth (OIE) recommends modified Ziehl-Neelson (mZn) acid fast staining and sheather’ssucrose floatation method for detection ofoocysts from faeces (OIE 2005) (Figs. 2.4, 2.5).
2.6.9 Control
Prevention and control measures include use ofboiled, filtered or bottled water. Maintain goodpersonal hygiene and wash hands thoroughlyafter any contact with stools. Persons withweakened immune system must take extraprecautions.
2.7 Giardiosis
Class: ZoomastigophoraOrder: DiplomonadidaFamily: Diplomonadida
2.7.1 Common Name/Synonyms
Giardia enteritis
24 2 Protozoonoses

2.7.2 Etiological Agent
Giardia intestinalis (syn. duodenalis or lamblia)is a water-borne pathogen and can infect allmammals. The presence of zoonotic genotypes(assemblages A and B) in animals such as dogsand cattle is of public health significance(Hamnes et al. 2006). Cattle are susceptible toinfection with three genotypes of G. intestinalis,the zoonotic genotypes of assemblages A and B(Lalle et al. 2005) and the hoofed livestockgenotype of assemblage E (Thompson 2004).
2.7.3 Epidemiology
The intestinal flagellate Giardia intestinalis isglobally distributed and commonly infects manyanimal species and man (Xiao 1994; Kulda andNohykova 1995). Giardiosis is worldwide andoccurs in both developed and developing coun-tries (Fraser et al. 1997; Gilman et al. 1988;Islam et al. 1983; Addiss et al. 1991; Rauch et al.1990; White et al. 1989; Birkhead and Vogt1989; Singh et al. 2008).
2.7.4 Reservoir
Humans act as the main reservoir of infection forhumans. The parasite is prevalent in bovinepopulations (Buret et al. 1990; Iburg et al. 1996;Olson et al. 1997) which could serve as a sourceof contamination to water supplies as Giardiacyst travels through the environment (Barwicket al. 2003). It has been suggested that the fewoutbreaks in humans might have resulted due tocontamination of drinking water by dairy pasturerunoff (Degerli et al. 2005). There is evidencesuggesting it to be a zoonosis (Buret et al. 1990).Thus farmers, veterinarians and techniciansworking in close contact with infected animalsmay be at risk of contacting the disease. Sinceinfected calves excrete high numbers of Giardiacysts, they are considered to be the mostimportant source of contamination for theirspecies (Xiao and Herd 1994; Xiao et al. 1993).Although Giardia is more prevalent in calves,adult animals serve as reservoirs of infection(McAllister et al. 2005).
2.7.5 Transmission
Infection takes place through faecal oral route.Cysts of G intestinalis, shed by faeces, areingested orally via water, milk and feed (Gozet al. 2006).
Fig. 2.4 Cryptosporidium oocysts from a Sheather’sfloation of faecal samples (with kind permission from Dr.Alvin A Gajadhar, Research Scientist cum Head, Centrefor Food-Borne and Animal Parasitology, Canadian FoodInspection Agency Saskatoon Lab, Canada)
Fig. 2.5 Cryptosporidium oocysts from modified Ziehl-Neelson’s staining of faecal samples
2.7 Giardiosis 25

2.7.6 Clinical Signs in Man
The disease is generally asymptomatic or sub-clinical (Farthing 1996). The important symp-toms include diarrhoea, bloating and abdominalpain. Recurring diarrhoea and flatulence mightpersist in some patients.
2.7.7 Clinical Signs in Animals
The severity of G. intestinalis infections variesfrom asymptomatic to clinical disease (Xiaoet al. 1993; Quilez et al. 1996). The symptoms incalves include mucoid and fatty stool, weightloss and growth retardation (Dwight 1999; Xiaoand Herd 1994). An infected animal shedsmicroscopic cysts with the faeces and intermit-tent cyst shedding can continue for severalweeks in calves (Xiao and Herd 1994).
2.7.8 Diagnosis
Faecal samples can be examined by wet mount(native lugol) and Wheatley’s trichrome (Modifi-cation of Gomori Trichrome) staining technique(Garcia 2001; Wheatley 1951). If the number ofoocysts in faecal material is fairly low or absent,then sucrose floatation should be followed bystaining techniques. For trichrome staining, mod-erately thick faecal smears should be prepared andimmediately fixed in Schaudinn’s fixative for aminimum of 30 min. Microscopic examinationshould be done at magnification(s) of 40X and100X. Morphometric studies of Giardia cysts andtrophozoites can also be carried out (Fig. 2.6).
2.7.9 Prevention and Control
Avoid contamination of drinking water withfaecal matter.
2.8 Leishmaniasis
Class: ZoomastigophoraFamily: TrypanosomatidaeGenus: Leishmania
Leishmaniasis is a complex group of diseasesendemic in many parts of the world. Leish-maniasis could occur due to more than 20Leishmania species. The parasite is transmittedto human beings by many species of phleboto-mine sand flies (Chappuis et al. 2007; Herwaldt1999; Pearson and Sousa 1996).
Leishmaniasis has been reported from 88countries. Ninety percent of visceral leishmani-asis cases have been reported from five coun-tries: India, Bangladesh, Nepal, Sudan andBrazil (NICD 2006). Some workers believeIndian kala-azar to be anthroponotic due toabsence of animal reservoirs.
Leishmaniasis occurs in four clinical forms:Cutaneous leishmaniasis; muco-cutaneousleishmaniasis; visceral leishmaniasis and post-kala-azar dermal leishmaniasis.
Fig. 2.6 Giardia cysts from a zinc sulphate flotation offaecal samples (with kind permission from Dr. Alvin AGajadhar, Research Scientist cum Head, Centre for Food-Borne and Animal Parasitology, Canadian Food Inspec-tion Agency Saskatoon Lab, Canada)
26 2 Protozoonoses

2.8.1 Visceral Leishmaniasis
2.8.1.1 Common Name/SynonymsBlack fever, Kala-azar, dumdum fever, post-kala-azar dermal leishmaniasis.
2.8.1.2 EtiologyThe disease occurs due to Leishmania donovanicomplex—L. donovani sensu stricto in Indiansubcontinent, East Africa and the L. infantum inNorth Africa, Europe and Latin America (Lukes2007; Chappuis et al. 2007; Mauricio et al.2000). The disease occurs due to L. chagasi inthe American continent. L. donovani causes an-throponotic, whereas L. infantum is responsiblefor zoonotic visceral leishmaniasis. The diseasecould become fatal if not properly treated.
2.8.1.3 ReservoirDogs principally act as reservoir hosts for spreadof zoonotic visceral leishmaniosis (VL) whichmainly occurs due to transmission of L. Infantum(Chappuis et al. 2007; Alvar et al. 2004).
2.8.1.4 TransmissionThe transmission of the parasite occurs due tobite of sand flies belonging to either Phleboto-mus or Lutzomyia spp.
2.8.1.5 EpidemiologyThe parasite L. infantum mostly infects childrenand immunosuppressed individuals, whereasL. donovani could infect all age groups(Chappuis et al. 2007). Estimated 500,000 newcases and more than 50,000 deaths occur due tovisceral leishmaniasis every year (Chappuiset al. 2007; Desjeux 2004a, b).
From a total of approximately 500,000 vis-ceral leishmaniasis cases occurring annuallyacross the globe, more than 23,000 cases arereported from India. The present foci of thedisease in India are Bihar, West Bengal, Uttar
Pradesh and Jharkhand (Sutherst 1993). Spo-radic cases have also been reported from Gujarat(west India) (Munshi et al. 1972), Tamil Naduand Kerala (south India) and sub-Himalayanparts of north India including Uttar Pradesh,Himachal Pradesh and Jammu and Kashmir(Kesavan et al. 2003). It was a common beliefthat western India has become a VL free zone,but recent studies (Sharma et al. 2007) havereported that the population of Gujarat state isagain at risk of kala-azar after about 20 years.
The disease is a serious problem in Bihar,West Bengal and eastern Uttar Pradesh states ofIndia where there is under-reporting of kala-azarand post-kala-azar dermal leishmaniasis inwomen and children 0–9 years of age (Bora1999). The parasite and the disease were firstreported in India in the 1820s in undividedBengal. The disease almost disappeared in the1950s but resurgence was reported in the 1970sin north Bihar (NICD 2006). Recent outbreaksof VL in India and the epidemic of humanimmunodeficiency virus (HIV) makes VL are-emerging problem in India. Outbreaks andepidemics have been associated with climatechange, urban development, deforestation andhuman migration. The prevalence of HIV sero-positivity in VL patients was found to be 5.7 %(6/104) at a tertiary care centre in northern India(Mathur et al. 2006). Four of the six (67 %)VL/HIV co-infected patients had a chronic/relapsing course, not responding to antileish-manial treatment.
The first indigenous case of visceral leish-maniasis in a 7-year-old girl from central India(Dey et al. 2007) indicated that more than onegenetic variant of L. donovani is circulating indifferent parts of India. The co-existence ofmalaria and kala-azar poses difficulties in dif-ferential diagnosis and results in lower reportingof the disease. Examination of Leishmania-stained blood smears of 450 asymptomatichealthy individuals residing in an endemic vil-lage in Bihar (Sharma et al. 2000), showed thepresence of Leishmania amastigotes in six per-sons (1.3 %).
2.8 Leishmaniasis 27

2.8.1.6 Clinical Signs in ManThe incubation period of the disease is between2 and 6 months. The symptoms mainly resultdue to systemic infections. Symptoms includeloss of appetite, fever, fatigue, weakness andweight loss. Due to invasion of the parasite inthe blood and reticuloendothelial system,enlargement of lymph nodes, spleen and livercould occur. The feet, hands, abdomen and skinmay take a grey hue particularly in Indianpatients.
2.8.1.7 Clinical Signs in AnimalsThe disease can occur in dogs and could causecutaneous or systemic lesions. Cutaneoussymptoms include alopecia and inflammationleading to formation of nodules, scabs andulcers. Systemic symptoms include fever, anae-mia, splenomegaly and lymphadenopathy.
2.8.1.8 Diagnosis• Microscopic examination of blood, lymph
nodes, bone marrow or spleen aspirates for theidentification of amastigote form of theparasite.
• Serological tests.• Molecular techniques such as Polymerase
chain reaction.
2.8.1.9 ControlThe control measures for visceral leishmaniasisinclude control of the disease in reservoir andvector, use of insecticide impregnated materialsand active detection and treatment of cases(Chappuis et al. 2007; Boelaert 2000; Davieset al. 2003).
2.8.2 Cutaneous Leishmaniasis
2.8.2.1 Common Name/SynonymsDelhi sore, Oriental sore, Baghdad ulcer, Uta,Buba.
2.8.2.2 EtiologyCutaneous Leishmaniasis can occur due to manyLeishmania species and sand flies transmit theinfection to human beings and animals(Reithinger et al. 2007). Most Leishmania spe-cies could cause cutaneous leishmaniasis inhuman beings.
L. braziliensis complex, L. mexicana com-plex, L. lainsoni, L. naiffi and L. lindenbergicause the disease in the new world. L. tropicacomplex (L. tropica, L. major and L. aethiopica)species cause the disease in old world. Somestrains of L. infantum can also cause cutaneousleishmaniasis. With the exception of L. tropica,all the other organisms are zoonotic in nature.
2.8.2.3 EpidemiologyCutaneous leishmaniasis endemic in the tropicsand neotropics (Reithinger et al. 2007). Cuta-neous leishmaniasis is endemic in more than70 countries worldwide. Ninety percent of casesoccur in countries such as Afghanistan, Pakistan,Saudi Arabia, Algeria, Brazil, Peru and Syria(Desjeux 2004a, b). The disease is spreading tonew areas as a result of urbanisation and defor-estation (Desjeux 2001). In India, initially thedisease was reported from hot dry northwesternregion and was endemic in western Thar desertof Rajasthan (NICD 2006). Sporadic cases werealso reported from Punjab, Delhi, Haryana andGujarat (Shahi 1941; Lysenko 1971). New fociof infection have been reported from differentparts of India (Bora et al. 1996; Sharma et al.2003). Kerala remained free from cutaneousleishmaniasis (CL) since 1988, many cases havebeen recorded afterwards (Bora et al. 1996;Kumaresan and Kumar 2007). This is animportant public health issue in view of a newlyrecognised reservoir area of CL in South India.
2.8.2.4 ReservoirMany domestic animals could serve as potentialreservoirs (Davies et al. 2000; Reithinger et al.2003). Both dogs and rodents serve as the zoo-notic reservoirs for cutaneous leishmaniasis in
28 2 Protozoonoses
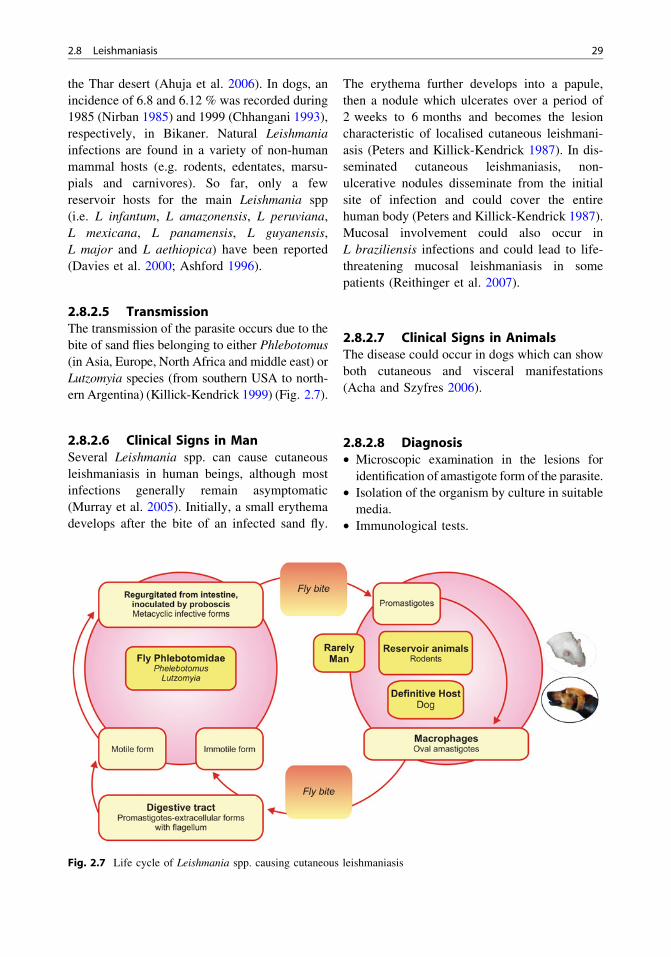
the Thar desert (Ahuja et al. 2006). In dogs, anincidence of 6.8 and 6.12 % was recorded during1985 (Nirban 1985) and 1999 (Chhangani 1993),respectively, in Bikaner. Natural Leishmaniainfections are found in a variety of non-humanmammal hosts (e.g. rodents, edentates, marsu-pials and carnivores). So far, only a fewreservoir hosts for the main Leishmania spp(i.e. L infantum, L amazonensis, L peruviana,L mexicana, L panamensis, L guyanensis,L major and L aethiopica) have been reported(Davies et al. 2000; Ashford 1996).
2.8.2.5 TransmissionThe transmission of the parasite occurs due to thebite of sand flies belonging to either Phlebotomus(in Asia, Europe, North Africa and middle east) orLutzomyia species (from southern USA to north-ern Argentina) (Killick-Kendrick 1999) (Fig. 2.7).
2.8.2.6 Clinical Signs in ManSeveral Leishmania spp. can cause cutaneousleishmaniasis in human beings, although mostinfections generally remain asymptomatic(Murray et al. 2005). Initially, a small erythemadevelops after the bite of an infected sand fly.
The erythema further develops into a papule,then a nodule which ulcerates over a period of2 weeks to 6 months and becomes the lesioncharacteristic of localised cutaneous leishmani-asis (Peters and Killick-Kendrick 1987). In dis-seminated cutaneous leishmaniasis, non-ulcerative nodules disseminate from the initialsite of infection and could cover the entirehuman body (Peters and Killick-Kendrick 1987).Mucosal involvement could also occur inL braziliensis infections and could lead to life-threatening mucosal leishmaniasis in somepatients (Reithinger et al. 2007).
2.8.2.7 Clinical Signs in AnimalsThe disease could occur in dogs which can showboth cutaneous and visceral manifestations(Acha and Szyfres 2006).
2.8.2.8 Diagnosis• Microscopic examination in the lesions for
identification of amastigote form of the parasite.• Isolation of the organism by culture in suitable
media.• Immunological tests.
Fig. 2.7 Life cycle of Leishmania spp. causing cutaneous leishmaniasis
2.8 Leishmaniasis 29

2.8.2.9 ControlThe control measures for cutaneous leishmani-asis include control of infection in reservoir andvector and the use of insecticides.
2.9 Sarcocystosis
Subclass: CoccidiaOrder: EucoccidioridaFamily: Sarcocystidae
2.9.1 Common Name/Synonyms
Sarcosporidiosis
2.9.2 Etiological Agent
Sarcocystosis is a protozoan disease of almostall species of domestic animals caused by Sar-cocystis sp. Cattle and pig act as the mainsources of human disease. Three species ofSarcocystis have been recognised in cattle, ofthese, S. cruzi has the dog as its definitive host,S. hirsuta the cat and S. hominis the man. Pigharbours three species of Sarcocystis namely,S. miescheriana, S. porcifelis, and S. suihominiswith their definitive hosts as dog, cat and man,respectively. Sarcocysts have been commonlyfound in retailed foods and can remain viable forseveral days under refrigeration conditions.
2.9.3 Life Cycle
Human beings act as definitive host for S. homi-nis, S suihominis and get infected by eating rawor undercooked beef and pork, respectively.Meat with visible sarcocysts is unacceptable tothe consumer and the condemnation of carcassesleads to considerable losses to the meat industry.In intermediate hosts, signs are evident at thetime when vascular endothelium is parasitised byschizonts. Later, the schizonts disappear withinabout a month and lead to formation of cysts inthe muscles (Fig. 2.8).
2.9.4 Epidemiology
Previous studies indicate high incidence of sar-cocystosis all over the world (Carvalho 1993,Dubey et al. 1989, Foggin 1980; Shi and Zhao1987; Stalheim et al. 1980; Singh et al. 2003,2004; Avapal et al. 2002, 2004; Juyal et al. 1982;Juyal 1991; Juyal and Bhatia 1989). Studies usingconventional techniques have reported the pres-ence of S. suihominis in India (Banerjee et al.1994; Bhatia 1991). Sarcocystis species has beenreported from many countries. In India, S. cruzihas been reported from Uttranchal, MadhyaPradesh, Bihar and Assam, whereas S. hominishas been reported from Uttar Pradesh andMadhya Pradesh states only (Devi et al. 1998;Jain and Shah 1988; Pandit et al. 1994; Salequeand Bhatia 1991; Singh 2001; 2002). Sarcocystisspecies mainly infect skeletal and cardiacmuscles. Sarcocystis species has been found inthe muscles of oesophagus, thigh, cardiac, dia-phragm, eye, tongue and tail.
2.9.5 Clinical Signs in Animals
The disease is also of economic importance, as itcauses both direct and indirect economic losses.Direct losses arise through losses incurred indetaining or condemning carcasses and indirectlosses arise from delayed growth and productionlosses on the farm. In heavy infections ofintermediate host (cattle), important symptomsinclude anorexia, pyrexia (42 �C or more),anaemia, cachexia, enlarged palpable lymphnodes, excessive salivation, nervousness, lame-ness and hair loss on the extremities.
Hair loss is noticed especially at the end ofthe tail and complete loss of the switch gives theanimals a ‘‘rat tail’’ appearance. The cystic stageof sarcocystosis is virtually non-pathogenic.Pathological changes observed at necropsyinclude eosinophilic myositis (Jensen et al.1986), generalised lymphadenopathy, erosionsand ulcerations in the oral cavity and oesopha-gus and severe laminitis. Histologically, there islymphadenitis, myositis, myocarditis and
30 2 Protozoonoses

glomerulonephritis. Schizonts of Sarcocystisspecies may be found in the endothelial cells ofblood vessels in many organs. Abortions mayoccur in breeding stocks.
2.9.6 Clinical Signs in Man
Human sarcocystosis is reviewed under two sec-tions: Intestinal sarcocystosis, where man acts as adefinitive host and muscular sarcocystosis, whereman acts as an intermediate host for various Sar-cocystis species. Intestinal sarcocystosis is mainlycharacterised by abdominal pain and diarrhoea.The muscular form of the disease is characterisedby pain, swelling, stiffness and displacement ofmyofibrils in the affected muscles.
2.9.7 Diagnosis
Samples of the animal’s muscle tissues like thigh,cardiac, jaw, tail, diaphragm, neck, eye muscles,oesophagus and brain should be collected inpolythene bags containing ice at 4 �C. Theyshould be first examined grossly and then sub-jected to pepsin digestion method (Jacob et al.1960) after removing fat and connective tissue.The diagnosis from muscles can be done using thefollowing methods: (Figs. 2.9, 2.10, 2.11)• Isolation of intact microsarcocysts from
muscles (Juyal et al. 1989).• Pepsin digestion technique.• Histopathological examination (Luna 1968).• Serological tests like ELISA, etc.• Electron microscopic studies (Mehlhorn et al.
1976).
Fig. 2.8 Life cycle of S. hominis and S. suihominis
2.9 Sarcocystosis 31

Control: Avoid consumption of raw or under-cooked pork or beef.
2.10 Toxoplasmosis
Subclass: CoccidiaOrder: EucoccidioridaFamily: Sarcocystidae
2.10.1 Synonyms
Congenital toxoplasmosis.
2.10.2 Etiology
Toxoplasmosis is a coccidial disease whichoccurs due to the parasite Toxoplasma gondii.
2.10.3 Reservoir
T. gondii is a protozoan parasite offlies with manyintermediate hosts, e.g. sheep, goat, pig, cattle,etc., including man (Dubey and Beattie 1988).
2.10.4 Epidemiology
Toxoplasmosis in man and sheep is prevalentworldwide including India (Dubey and Beattie1988; Dubey 1987; Chhabra and Mahajan 1982).In the first national serological prevalence ofT. gondii in India (Dhumne et al. 2007), 23,094serum samples were tested for T. gondii IgG andIgM antibodies using a solid-phase immunocap-ture ELISA. Antibodies IgG and IgM were foundin 24.3 and 2 % samples, respectively. The lowestseroprevalences were reported from the northern
Fig. 2.9 Transmission electron microscopy of S. cruzi,thin walled S. cruzi showing zoites in the granulomataand hair-like projections on the cyst wall (with kindpermission from Dr. Alvin A Gajadhar, Research Scien-tist cum Head, Centre for Food-Borne and AnimalParasitology, Canadian Food Inspection Agency Saska-toon Lab, Canada)
Fig. 2.10 Ultrastructure of Sarcocyst wall showingvillar projections (VP) arising from the S. cruzi cystwall. No microtubules are seen in VP and a zone ofground substance (GS) can also be seen (with kindpermission from Dr. Alvin A Gajadhar, Research Scien-tist cum Head, Centre for Food-Borne and AnimalParasitology, Canadian Food Inspection Agency Saska-toon Lab, Canada)
Fig. 2.11 Thick-walled Sarcocystis cyst in diaphrag-matic muscles of pig (H & E stain, 40X)
32 2 Protozoonoses

parts of the country, with the highest in the south.The data probably indicate the effects of signifi-cantly drier conditions and their related negativeimpact on the survivability of T. gondii oocysts innorthern India. It has also been observed that theseroprevalence of T. gondii in humans in India islow compared to that of western countries (Dubeyand Beattie 1988). Many other workers have alsoreviewed human toxoplasmosis in India (Parija2004; Dubey 1987).
2.10.5 Transmission
Human beings can become infected either aftereating raw or undercooked contaminated meatinfected with cysts of the parasite or from catfaeces infected with T. gondii oocysts. Theinfection can further be transmitted from aninfected mother to the foetus through the pla-centa. Although rare, organ transplant frominfected persons could also lead to infection.Transplacental transmission may also take place.Persons with weakened immune systems are athigh risk of being infected. Cat acts as thedefinitive host and shed oocysts in the faeces.The sporulated oocysts can be ingested by man,animals and mice (Fig. 2.12).
2.10.6 Clinical Signs in Man
In healthy persons, the disease is generallyasymptomatic. The symptoms generally appear7–14 days after the exposure. The parasite caninfect many vital organs such as brain, eye, liver,lung and heart. Symptoms generally includeheadache, fever, enlarged lymph nodes, partic-ularly of the neck and sore throat, and musclepain. In congenital toxoplasmosis, eye infectioncould lead to blindness. Congenital toxoplas-mosis could lead to mental retardation, multipleorgan failure, hydrocephalus or foetal death(Hohlfeld et al. 1989). Toxoplasmic encephalitis(TE) is the most frequent cause for focal nervoussystem disorder complicating AIDS. There havebeen various reports of TE from India (Chaddha
et al. 1999). Although Toxoplasma infectiondoes not cause repeated foetal losses, this is themost common indication for investigation oftoxoplasmosis in India.
2.10.7 Clinical Signs in Animals
The parasite remains asymptomatic most of thetime. The disease is particularly important insheep and goat where it may lead to abortions inpregnant animals. Congenital infections can alsooccur with young ones having problems inmuscle coordination.
2.10.8 Diagnosis
In intermediate hosts, the disease can be diag-nosed by molecular and serological tests, miceinoculation, histological and other tests such asMRI, CT scan, etc. Giemsa-stained microscopicexamination of impression smears can also bedone. In cat (definitive host), faecal examinationusing flotation techniques or serological testscan be performed (Figs. 2.13, 2.14).
2.10.9 Control
For prevention of the disease, consume properlycooked meat. Persons involved in slaughteringshould handle raw meat carefully and wash theirhands properly. Children should avoid access tocat faeces, particularly in playgrounds and parks.Pregnant women should not handle cat litter.
2.11 Other Protozoan ZoonoticDiseases
2.11.1 Cyclosporiasis
Cyclosporiasis occurs due to coccidium parasiteCyclospora cayetanensis. The human disease isworldwide in occurrence. The occurrence of thedisease in animals is unknown. The parasite
2.10 Toxoplasmosis 33

Fig. 2.12 Life cycle of Toxoplasma gondii
Fig. 2.13 Toxoplasma cyst, toludine stained (100 X)(with kind permission from Dr. Alvin A Gajadhar,Research Scientist cum Head, Centre for Food-Borne andAnimal Parasitology, Canadian Food Inspection AgencySaskatoon Lab, Canada)
Fig. 2.14 Transmission electron microscopy showingultrastructure of Toxoplasma cyst (with kind permissionfrom Dr. Alvin A Gajadhar, Research Scientist cum Head,Centre for Food-Borne and Animal Parasitology, Cana-dian Food Inspection Agency Saskatoon Lab, Canada)
34 2 Protozoonoses

could cause watery diarrhoea in human subjects.The double-walled oocysts can be detected infaeces using oocyst concentration and stainingtechniques (Fig. 2.15).
2.11.2 Infections Caused by Free-LivingAmoebae
The free-living amoebae belonging to the genusNaegleria, Acanthamoeba and Balamuthia couldcause the disease in man and some other mam-mals. The parasite Naegleria fowleri could causeamoebic meningoencephalitis in man. Acantha-moeba spp. could cause granulomatous amoebicencephalitis in man. The important sources ofinfection include contaminated water and soil.
2.11.3 Malaria in Non-human Primates
The disease occurs due to parasites belonging tothe genus Plasmodium (Phylum Apicomplexa)which affect non-human primates. Mosquitoesbelonging to the genus Anopheles act as vectorsof the disease. The infection due to plasmodia ofnon-human primates has been rarely recorded inhuman beings.
2.11.4 Microsporidiosis
The disease primarily occurs due to Enterocyto-zoon bieneusi, Encephalitozoon intestinalis,E. cuniculi and some other species. Microsporid-iosis is an important disease in immunodeficientindividuals. The important symptoms in maninclude diarrhoea and watery stools. Contamina-tion of water with infected faeces and stools couldserve as a source of infection for other persons.
2.11.5 Atypical HumanTrypanosomiasis
Although the zoonotic potential of trypanosomi-asis in humans due to animal trypanosomes is notcertain, 19 (T. lewisi-8, T. evansi-5, T. brucei-4,T. vivax-1, T. congolense-1) atypical human try-panosomiasis cases have been reported in theliterature (Joshi 2013).
References
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals, 3rd edn, vol IIIparasitoses. World health organisation, Geneva
Addiss DG, Stewart JM, Finton RJ, Wahlquist SR,Williams RB, Dickerson JW, Spencer HC, JuranekDD (1991) Giardia lamblia and Cryptosporidiuminfections in child day-care centers in Fulton County,Georgia. Pediatr Infect Dis J 10:907–911
Ahuja A, Gahlot AK, Purohit SK, Bumb RA, Mehta RD(2006) Zoonotic significance of cutaneous leishman-iasis- an important zoonosis of western Rajasthan.Intas Polivet 7(2):437–443
Aiello E (1998) Cryptosporidiosis. In: The MerckVeterinary Manual, 8th edn, pp 145–146
Alvar J, Canavate C, Molina R, Moreno J, Nieto J (2004)Canine leishmaniasis. Adv Parasitol 57:1–88
Amorin DS (1979) Chagas’ disease. Prog Cardiol8:235–279
Angus KW (1983) Cryptosporidiosis in man, domesticanimals and birds: a review. J R Soc Med 76(1):62–70
Arean VM, Koppisch E (1956) Balantidiasis: a reviewand report of cases. Am J Pathol 32:1089–1115
Ashford RW (1996) Leishmaniasis reservoirs and theirsignificance in control. Clin Dermatol 14:523–532
Avapal RS, Sharma JK, Juyal PD (2004) Pathologicalchanges in Sarcocystis infection in domestic pigs (Susscrofa). Vet J 168:358–361
Fig. 2.15 Cyclospora cayetanensis from Sheather’sflotation of faecal sample (with kind permission fromDr. Alvin A Gajadhar, Research Scientist cum Head,Centre for Food-Borne and Animal Parasitology, Cana-dian Food Inspection Agency Saskatoon Lab, Canada)
2.11 Other Protozoan Zoonotic Diseases 35

Avapal RS, Singh BB, Sharma JK, Juyal PD (2002)Seroprevalence of sarcocystosis in swine. J ParasiticDis 26(2):109–110
Bales JD (1991) African trypanosomiasis. In: StricklandGT (ed) Hunter’s tropical medicine, 7th edn. Saun-ders, Philadelphia, pp 617–628
Banerjee PS, Bhatia BB, Pandit BA (1994) Sarcocystissuihominis infection in human being in India. J VetParasitol 8(1):57–58
Barwick RS, Mohammed HO, White ME, Bryant RB(2003) Prevalence of Giardia spp. and Cryptospori-dium spp. on dairy farms in southeastern New YorkState. Prev Vet Med 59:1–11
Beattie JF, Michelson ML, Holman PJ (2002) Acutebabesiosis caused by Babesia divergens in a residentof Kentucky. N Engl J Med 347:697–698
Becker CAM, Agnès B-A, Maggy J, Alain C, LaurenceM (2009) Natural transmission of zoonotic Babesiaspp. by Ixodes ricinus ticks. Emerg Infect Dis15(2):320–322
Bhatia BB (1991) Current status of food-borne parasiticzoonoses in India. In: Cross JH (ed) Emergingproblems in food-borne parasitic zoonosis: impacton agriculture and public health. Proceedings of the33rd SEAMEO-TROPMED regional seminar. South-east Asian J Trop Med Public Hlth 22:36–41
Birkhead G, Vogt RL (1989) Epidemiologic surveillancefor endemic Giardia lamblia infection in vermont.Am J Epi Demiol 129:762–768
Boelaert M (2000) Visceral leishmaniasis control: apublic health perspective. Trans R Soc Trop Med Hyg94:465–471
Bora D (1999) Epidemiology of visceral leishmaniasis inIndia. Natl Med J India 12(2):62–68
Bora D, Khera AK, Mittal V, Kaul SM, Sharma RS (1996)New focus of cutaneous leishmaniasis in India. IndianJ Dermatol Venereol Leprol 62(1):19–21
Braga LL, Lima AAM, Sears CL, Newman RD, WuhibT, Paiva CA, Guerrant RL, Mann BJ (1996) Seroep-idemiology of Entamoeba histolytica in a slum inNortheastern Brazil. Am J Trop Med Hyg 55:693–697
Bruce D (1895) Preliminary report on the tsetse flydisease or nagana in Zululand. Bennett and Davis,Durban
Buret A, Den Hollander N, Wallis PM, Befus D, OlsonME (1990) Zoonotic potential of giardiasis indomestic ruminants. J Infect Dis 162:231–237
Cantellano ME, Palomo AM (2000) Pathogenesis ofintestinal amebiasis: from molecules to disease. ClinMicrobiol Rev 13(2):318–333
Carcavallo RU, Galindez Giron I, Jurberg J, Lent H(1998) Atlas of Chagas disease vectors in theAmericas. Rio de Janeiro: Editora Fiocruz
Carvalho SP (1993) Prevalence and identity of Sarco-cystis sp. cysts in cattle slaughtered at Lisbon. RevistaPortuguessa de Ciencias–Veterinarians 88:36–41
Casemore DP, Armstrong M, Sands RL (1985) Labora-tory diagnosis of cryptosporidiosis. J Clin Pathol38:1337–1341
Casemore SE, Wright CL (1997) Cryptosporidiosis–human and animal epidemiology. In: Fayer R (ed)Cryptosporidium and cryptosporidiosis. CRC press,Boca Raton, pp 65–92
Castro J, Vazquez-Iglesias JL, Arnal-Monreal F (1983)Dysentery caused by Balantidium coli—report of twocases. Endoscopy 15:272–274
Chaddha DS, Kalra SP, Singh AP (1999) Toxoplasmicencephalitis in acquired immunodeficiency syndrome.J Assoc Physician India 47:680–684
Chappuis F, Sundar S, Hailu A, Ghalib H, Rijal S,Peeling RW, Alvar J, Boelaert M (2007) Visceralleishmaniasis: What are the needs for diagnosis,treatment and control? Nature Rev Microbiol5:873–882
Chhabra MB, Mahajan RC (1982) Toxoplasmosis inIndia: prevalence of serum antibodies in sheep andgoats. Indian J Anim Hlth 21:5–8
Chhangani SK (1993) Investigation on cutaneous leish-maniasis in men and dogs in Bikaner, Rajasthan.M.V.Sc Thesis, Rajasthan Agricultural University
Christensson DA (1989) Inverse age resistance to exper-imental Babesia divergens infection in cattle. ActaVet Scand 30:453–464
Collier L, Balows A, Sussman M, Miles MA (1997) Newworld trypanosomiasis. In: Collier L, Balows A,Sussman M (eds) Topley and Wilson’s microbiologyand microbial infections, vol 5. Arnold, London,pp 283–302
Collins JD, Nuallain TO, Ferguson AR (1970) Observa-tions of bovine babesiosis in Ireland. Ir Vet J24:42–51
Cox FEG (2004) History of sleeping sickness (Africantrypanosomiasis). Infect Dis Clin N Am 18:231–245
Current WL (1983) Human cryptosporidiosis. N Engl JMed 309:1325–1327
Current WL (1985) Cryptosporidiosis. J Am Vet MedAssoc 187:1334–1338
Current WL, Garcia LS (1991) Cryptosporidiosis. ClinMicro Biol Rev 4:325–358
Davies CR, Kaye P, Croft SL, Sundar S (2003) Leish-maniasis: new approaches to disease control. BMJ326:377–382
Davies CR, Reithinger R, Campbell-Lendrum D, Felic-iangeli D, Borges R, Rodriguez N (2000) Theepidemiology and control of leishmaniasis in Andeancountries. Cad Saúde Publica 16:925–950
Degerli S, Celikrez A, Kalkan K, Ozecelik S (2005)Prevalence of Cryptosporidium spp. and Giardia spp.in cows and calves in sivas. Turk J Vet Anim Sci29:995–999
Desjeux P (2001) The increase in risk factors forleishmaniasis worldwide. Trans R Soc Trop MedHyg 95:239–243
Desjeux P (2004a) Leishmaniasis. Nat Rev Mirobiol2:692
Desjeux P (2004b) Leishmaniasis: current situation andnew perspectives. Comp Immunol Microbiol InfectDis 27:305–318
36 2 Protozoonoses

Devi PP, Sarmah PC, Saleque A (1998) Sarcocystsis sppinfection in carcasses of domestic pigs in GuwahatiAssam. J Vet Parasitol 12(1):56–57
Dey A, Sharma U, Singh S (2007) First case ofindigenous visceral leishmaniasis from central India.Am J Trop Med Hyg 77(1):95–98
Dhumne M, Sengupta C, Kadival G, Rathinaswamy A,Velumani A (2007) National seroprevalence of Tox-oplasma gondii in India. J Parasitol 93(6):1520–1521
Dias JCP (2000) Chagas disease control and the naturalhistory of human Chagas disease: a possible interac-tion? Mem Inst Oswaldo Cruz 95:14–20
Dias JCP, Silveira AC, Schofield CJ (2002) The impactof chagas disease control in Latin America—areview. Mem Inst Oswaldo Cruz 97(5):603–612
Dubey JP (1987) Toxoplasmosis in domestic animals inIndia: present and future. J Vet Parasitol 1:13–18
Dubey JP, Beattie CP (1988) Toxoplasma and toxoplas-mosis in animals including man. CRC Press, Florida
Dubey JP, Speer CA, Fayer R (1989) Sarcocystosis ofanimals and man. CRC Press, Boca Raton, pp 1–215
Duh D, Petrovec M, Avsic-Zupanc T (2001) Diversity ofbabesia infecting European sheep ticks (Ixodes rici-nus). J Clin Microbiol 39:3395–3397
Dutton JE (1902) Preliminary note upon a trypanosomeoccurring in the blood of man. Thompson Yates LabRep 4:455–468
Dwight DB (1999) Georgi’s parasitology for veterinar-ians. WB. Saunders Co, New York
Espinosa R, Carrasco HA, Belandria F, Fuenmayor AM,Molina C, Gonzalez R, Martinez O (1985) Lifeexpectancy analysis in patients with Chagas’ disease:prognosis after one decade (1973–1983). Int J Cardiol8:45–56
Esteban JG, Aguirre C, Angles R, Ash LR, Mas-Coma S(1998) Balantidiasis in Aymara children from thenorthern Bolivian Altiplano. Am J Trop Med Hyg59:922–927
Farthing MJ (1996) Giardiasis. Gastroenterol Clin NorthAm 25(3):493–515
Fayer R (1997) Cryptosporidium and cryptosporidiosis.CRC Press, Boca Raton, p 251
Fitzpatrick JE, Kennedy CC, McGeown MG, OreopoulosDG, Robertson JH, Soyannwo MA (1968) Human caseof piroplasmosis (babesiosis). Nature 217:861–862
Foggin CM (1980) Sarcocystis infection and granulom-atous myositis in cattle in Zimbabwe. Zimb Vet J11:8–13
Forde RM (1902) Some clinical notes on a Europeanpatient in whose blood a trypanosome was observed.J Trop Med 5:261–263
Fotedar R, Stark D, Beebe N, Marriott D, Ellis J,Harkness J (2007) Laboratory diagnostic techniquesfor Entamoeba species. Clin Microbiol Rev20(3):511–532
Fraser D, Dagan R, Naggan L, Greene V, El-on J, RbiahYA, Deckelbaum RJ (1997) Natural history ofGiardia lamblia and Cryptosporidium infections ina cohort of Israeli bedouin infants: a study of a
population in transition. Am J Trop Med57(5):544–549
Garcia LS (2001) Diagnostic medical parasitology, 4thedn. ASM Press, Washington, DC, p 723
Garcia LS, Bruckner DA, Brewer TC, Shimizu RY(1983) Techniques for the recovery and identificationof Cryptosporidium oocysts from stool specimens.J Clin Microbiol 18:185–190
Garcia-Zapata MTA, Marsden PD (1986) Chagas’disease. Clin Trop Med Commun Dis 1:537–585
Genchi C (2007) Human babesiosis, an emerging zoo-nosis. Parassitologia 49(1):29–31
Gern L, Brossard M (1986) Evolution annuelle del’infestation de bovins par la tique Ixodes ricinus L.et de l’infection de ces ectoparasites par Babesiadivergens dans le Clos du Doubs Jura. Suisse SchweizArchiv Tierheilkd 128:361–363
Giacometti A, Cirioni O, Balducci M (1997) Epidemi-ologic features of intestinal parasitic infections inItalian mental institutions. Eur J Epidemiol13:825–830
Gilman RH, Marquis GS, Miranda E, Vestegui M,Martinez H (1988) Rapid reinfection of Giardialamblia after treatment in a hyperendemic third worldcommunity. Lancet 1:343–345
Gorenflot A, Moubri K, Precigout E, Carcy B, SchettersTPM (1998) Human babesiosis. Ann Trop MedParasitol 92:489–501
Goz Y, Altug N, Yuksek N, Ozkan C (2006) Parasitesdetected in neonatal and young calves with diarrhea.Bull Vet Inst Pulawy 50:345–348
Gray JS, Langley RJ, Brophy PO, Gannon P (1989)Vaccination against bovine babesiosis with drug-controlled live parasites. Vet Rec 125:369–372
Gray JS, Murphy TM (1985) Bovine babesiosis inIreland. Ir Vet News, 9–14
Griffiths JK (1998) Human cryptosporidiosis: epidemiol-ogy, transmission, clinical disease, treatment anddiagnosis. Adv Parasitol 40:37–85
Hamnes IS, Gjerde B, Robertson L (2006) Prevalence ofGiardia and Cryptosporidium in dairy calves in threeareas of Norway. Vet Parasitol 140:204–216
Haque R, Faruque ASG, Hahn P, Lyerly DM, Petri WA(1997) Entamoeba histolytica and Entamoeba disparinfection in children in Bangladesh. J Infect Dis175:734–736
Hayes EB, Matte TD, O’Brien TR, McKinley TW,Logsdon GS (1989) Large community outbreak ofcryptosporidiosis due to contamination of a filteredpublic water supply. N Engl J Med 320:1372–1376
Henriksen SVA, Krogh HV (1985) Bovine cryptosporid-iosis in Denmark 1. Prevalence, age distribution, andseasonal variation. Nord Vet Med 37:34–41
Herwaldt BL (1999) Leishmaniasis. Lancet 354:1191–1199Herwaldt BL, Persing DH, Precigout EA, Goff WL,
Mathiesen DA, Taylor PW, Eberhard ML, GorenflotAF (1996) A fatal case of babesiosis in Missouri:identification of another piroplasm that infectshumans. Ann Intern Med 124:643–650
References 37

Hildebrandt A, Hunfeld KP, Baier M, Krumbholz A,Sachse S, Lorenzen T, Kiehntopf M, Fricke HJ,Straube E (2007) First confirmed autochthonous caseof human Babesia microti infection in Europe. Eur JClin Microbiol Infect Dis 26:595–601
Hohlfeld P, Daffos F, Thulliez P, Aufrant C, Couvreur J,MacAleese J (1989) Fetal toxoplasmosis: outcome ofpregnancy and infant follow-up after in utero treat-ment. J Pediatr 115:765–769
Homer MJ, Aguilar-Delfin I, Telford SR, Krause PJ,Persing DH (2000) Babesiosis. Clin Microbiol Rev13:451–469
Hunfeld KP, Brade V (2004) Zoonotic Babesia: possiblyemerging pathogens to be considered for tick-infestedhumans in Central Europe. Int J Med Microbiol37:93–103
Hunfeld KP, Hildebrandt A, Gray JS (2008) Babesiosis:recent insights into an ancient disease. Int J Parasitol38:1219–1237
Hunfeld KP, Lambert A, Kampen H, Albert S, Epe C,Brade V, Tenter AM (2002) Seroprevalence ofBabesia infections in humans exposed to ticks inmidwestern Germany. J Clin Microbiol 40:2431–2436
Iburg T, Gasser RB, Henriksen SA (1996) First record ofGiardia in cattle in Denmark. Acta Vet Scand37:337–341
Islam A, Stoll BJ, Ljungstrom I, Biswas J, Nazrul H,Huldt G (1983) Giardia lamblia infections in a cohortof Bangladeshi mothers and infants followed for oneyear. J Pediatr 103:996–1000
Jacob L, Jack RS, Marjorie ML (1960) The resistance ofthe encysted form of Toxoplasma gondii. J Parasitol8:11–21
Jain PC, Shah HL (1988) A comparative morphologicalstudy of Sarcocysts of three species of Sarcocystisinfecting cattle in Madhya Pradesh. Indian J Anim Sci58:8–13
Jensen R, Alexander AP, Dahegren RR, Jolley WR,Masquardt WC, Flack DE, Bennet BW, Cox MP,Harris CW (1986) Eosinophilic myositis and muscu-lar sarcocystosis in the carcasses of slaughtered cattleand lambs. Am J Vet Res 36:587–593
Joshi PP (2013) Human trypanosomiasis in India: Is it anemerging new zoonosis? Section 1: infectious dis-eases. Med Update 23:10–13 (Published by theassociation of physicians of India)
Joyner LP, Davies SFM (1967) Acquired resistance toBabesia divergens in experimental calves. J Protozool14:260–262
Juyal PD, Bhatia BB (1989) Sarcocystosis: an emergingzoonosis. Indian Vet Medical J 13:66–69
Juyal PD, Ruprah NS, Chhabra MB (1989) Rapidisolation of intact micro Sarcocystis (Protozoa-Api-complexa) cysts from muscular tissues. Ind J AnimalHlth 28(1):69–70
Juyal PD, Sahai BN, Srivastava PS, Sinha SRP (1982)Heavy sarcocystosis in ocular musculature of cattleand buffaloes. Vet Res Commun 5:337–342
Juyal PD (1991) Sarcocystis and sarcocystosis in India.South-East Asian J Trop Med Pub Hlth 22:138–141
Kean BH, Mott KE, Russell AJ (1978) Tropical medicineand parasitology classic investigations, vol 1. CornellUniversity Press, Ithaca, NY, 173–177
Kesavan A, Parvathy VK, Thomas S, Sudha SP (2003)Indigenous visceral leishmaniasis: two cases fromKerala. Indian J Pediatr 40:373–374
Killick-Kendrick R (1999) The biology and control ofphlebotomine sandflies. Clin Dermatol 17:279–289
Kjemtrup AM, Conrad PA (2000) Human babesiosis: anemerging tick-borne disease. Int J Parasitol30:1323–1337
Koch R (1906) Beiträge zur Entwicklungsgeschichte derPiroplasmen. Z Hyg Infektionskrankh 54:1–9
Kulda J, Nohykova E (1995) Giardia in humans andanimals. In: Kreier JP (ed) Parasitic protozoa, vol 10,2nd edn. Academic Press, San Diego, pp 225–430
Kumaresan M, Kumar P (2007) Localized cutaneousleishmaniasis in South India: successful treatmentwith ketoconazole. Indian J Dermatol VenereolLeprol 73(5):361–362
Lalle M, Pozio E, Capelli G, Bruschi F, Crotti D, CaccioSM (2005) Genetic heterogeneity at the b- giardinlocus among human and animal isolates of Giardiaduodenalis and identification of potentially zoonoticsubgenotypes. Int J Parasitol 35:207–213
Leek RG, Fayer R (1984) Prevalence of cryptosporidiuminfections and their relation to diarrhea in calves on12 dairy farms in Maryland. Proc Helminthol SocWash 51:360–361
Levine ND (1985) Veterinar protozoology. Iowa stateUniversity Press, Ames
L’Hostis M, Chauvin A, Valentin A, Marchand A,Gorenflot A (1995) Large scale survey of bovinebabesiosis due to Babesia divergens in France. VetRec 14:36–38
Lukes J (2007) Evolutionary and geographical history ofthe Leishmania donovani complex with a revision ofcurrent taxonomy. Proc Natl Acad Sci USA 104:9375–9380
Luna LG (1968) Manual of histological staining meth-ods. Armed forces institute of pathology, 3rd edn.Mcgraw Hill Book Company, New York, pp 34–157
Lysenko AJA (1971) Distribution of leishmaniasis in thewhole world. Bull World Health Organ 44:515
MacKenzie WR, Hoxie NJ, Proctor ME, Gradus MS.Blair KA, Peterson DE, Kazmierczak JJ, Addiss DG,Fox KR, Rose JB, Davis JP (1994) A massiveoutbreak in Milwaukee of Cryptosporidium infectiontransmitted through the public water supply. N Engi JMed 331:161–167
Marsaudon E, Camenen J, Testou D, Bourree P, SamsonP, Luneau F (1995) Une babésiose humaine a Babesiacanis, responsable d’une anurie de 40 jours. Ann MedIntern 146:451–452
Mathur P, Samantaray JC, Vajpayee M, Samanta P (2006)Visceral leishmaniasis/human immunodeficiency
38 2 Protozoonoses

virus co-infection in India: the focus of two epidemics.J Med Microbiol 55:919–922
Mauricio IL, Stothard JR, Miles MA (2000) The strangecase of Leishmania chagasi. Parasitol Today16:188–189
McAllister TA, Olson ME, Fletch A, Wetzstein M, EntzT (2005) Prevalence of Giardia and Cryptosporidiumin beef cows in Southren Ontario and in beef cows inSouthren British Columbia. Can Vet J 46:47–55
Mehlhorn H, Hartley WJ, Heydorn AO (1976) Acomparative ultrastructure study of cyst wall of 13Sarcocystis species. Prostologica 12:451–467
M’Fadyean J, Stockman S (1911) A new species ofpiroplasm found in the blood of British cattle. J CompPathol 24:340–354
Miles MA, Dora Feliciangeli M, Antonieta Rojas deArias (2003) American trypanosomiasis (Chagas’disease) and the role of molecular epidemiology inguiding control strategies. Br Med J 326(7404):1444–1448
Munshi CP, Vaidya PM, Buranpuri JJ, Gulati OD (1972)Kalaazar in Gujarat. J Indian Med Assoc 59:287–293
Murray HW, Berman JD, Davies CR, Saravia NG (2005)Advances in leishmaniasis. Lancet 366:1561–1577
Nakauchi K (1999) The prevalence of Balantidium coliinfection in fifty-six mammalian species. J Vet MedSci 61:63–65
NICD (2006) Leishmaniasis and its control. Natl InstCommun Diseases Bull 10(1):1–8
Nirban VK (1985) Incidence of Leishmania tropicainfection in and around Bikaner, and preliminarytrials of its cultivation on artificial media. M.V.Sc.Thesis, Sukhadia University, Udaipur
Njiokou F, Laveissière C, Simo G, Nkinin S, Grébaut P,Cuny G, Herder S (2006) Wild fauna as a probableanimal reservoir for Trypanosoma brucei gambiensein Cameroon. Infect Genet Evol 6:147–153
Nydam DV, Wade SE, Schaaf SL, Mohammed HO(2001) Number of Cryptosporidium parvum oocystsshed by dairy calves after natural infection. Am J VetRes 62:1612–1615
O’Donoghue PJ (1995) Cryptosporidium and cryptospo-ridiosis in man and animals. Int J Parasitol25:139–195
OIE (2005) Cryptosporidiosis. In: Manual of diagnostictests and vaccines for terrestrial animals
Oliveira JSM, Correa De Araujo RRC, Navarro MA,Muccillo G (1983) Cardiac thrombosis and thrombo-embolism in chronic Chagas’ heart disease. Am JCardiol 52:147–151
Olmeda AS, Armstrong PM, Rosenthal BM, ValladaresB, Del Castillo A, De Armas F, Miguelez M,Gonzalez A, Rodriguez JA, Spielman A, Telford SR(1997) A subtropical case of human babesiosis. ActaTrop 67:229–234
Olson ME, Thorlakson CL, Deselliers L (1997) Giardiaand Cryptosporidium in Canadian farm animals. VetParasitol 68:375–381
Pakandl M (1994) The prevalence of intestinal protozoain wild and domestic pigs. Vet Med 39:377–380
Pandit BA, Bhatia BB, Banerjee PS (1994) Comparativemorphology of sarcocysts of three species of Sarco-cystis in cattle from Tarai region of Uttar Pradesh.J Vet Parasitol 8:59–63
Parija SC (2004) Review of emerging parasitic zoonosesin India. In: Summer school ‘‘Current trends andstrategies in diagnosis and control of parasiticdiseases of domestic animals and poultry’’ 25 Aug–14 Sep 2004, Veterinary College and ResearchInstitute Namakkal, pp 140–159
Pearson RD, Sousa AQ (1996) Clinical spectrum ofLeishmaniasis. Clin Infect Dis 22:1–13
Peters W, Killick-Kendrick R (1987) The leishmaniasesin biology and medicine. Clinical aspects and control,vol 2. Published by Academic Press, London
Pinilla AE, López MC, Viasus DF (2008) History of theEntamoeba histolytica protozoan. Rev Med Chil136(1):118–124
Quilez J, Sanchez-Acedo C, Cacho E, Clavel A, CausapeAC (1996) Prevalence of Cryptosporidium and Giar-dia infections in cattle in Aragon (Northeast Spain).Vet Parasitol 66:139–146
Rauch AM, Van Rory MT, Bartlett AV, Pickering LK(1990) Longitudinal study of Giardia lamblia infec-tion in a day care center population. Pediatr Infect Dis9:186–189
Reithinger R, Dujardin JC, Louzir H, Pirmez C, Alex-ander B, Brooker S (2007) Cutaneous leishmaniasis.Lancet Infect Dis 7:581–596
Reithinger R, Espinoza JC, Davies CR (2003) Thetransmission dynamics of canine American cutaneousleishmaniasis in Huanuco, Peru. Am J Trop Med Hyg69:473–480
Saleque A, Bhatia BB (1991) Prevalence of sarcocystsisin domestic pigs in India. Vet Parasitol 40:151–153
Shahi MM (1941) Report on the epidemic of oriental sorein Delhi. Indian Med Gaz 76:449
Sharma MC, Gupta AK, Das VNR, Verma N, Kumar N,Saran R, Kar SK (2000) Leishmania donovani inblood smears of asymptomatic persons. Acta Trop76(2):195–196
Sharma RC, Mahajan VK, Sharma NL, Sharma A (2003)A new focus of cutaneous leishmaniasis in HimachalPradesh (India). Indian J Dermatol Venereol Leprol69:170–172
Sharma U, Redhu NS, Mathur P, Singh S (2007) Reemergence of visceral leishmaniasis in Gujarat, India.J Vect Borne Dis 44:230–232
Sherlock M, Healy A, Larkin HA, Doherty ML (2000)Bovine babesiosis: clinical assessment and transfu-sion therapy. Irish Vet J 53:572–578
Shi LZ, Zhao HY (1987) Evaluation of an enzymeimmunoassay for the detection of antibodies againstSarcocystis sp. in naturally infected cattle in China.Vet Parasitol 24:185–194
Simo G, Asonganyi T, Nkinin SW, Njiokou F, Herder S(2006) High prevalence of Trypanosoma bruceigambiense group 1 in pigs from the Fontem sleepingsickness focus in Cameroon. Vet Parasitol139:57–66
References 39

Singh BB (2001) Prevalence and immunodiagnosis ofSarcocystis sp. of public health signifance in cattle.M.V.Sc. Thesis, Punjab Agricultural University,Ludhiana
Singh BB, Sharma JK, Juyal PD, Aulakh RS (2003)Prevalence and comparative morphology of Sarco-cystis species recovered from cattle in Punjab. J ResPAU 40(3–4):456–458
Singh BB, Sharma JK, Juyal PD, Gill JPS (2004)Seroprevalence of Sarcocystis species of cattle inPunjab. J Vet Parasitol 18(1):75–76
Singh BB, Sharma R, Kumar H, Banga HS, Aulakh RS,Gill JPS, Sharma JK (2006) Prevalence of Cryptos-poridium parvum infection in Punjab (India) and itsassociation with diarrhea in neonatal dairy calves. VetParasitol 140(1–2):162–165
Singh BB, Sharma R, Sharma JK, Banga HS, Kumar H,Aulakh RS, Gill JPS (2008) Prevalence of Giardiaintestinalis infection in cattle. J Vet Parasitol22(2):91–92
Singh R (2002) Prevalence and immunodiagnosis ofSarcocystis sp. of public health significance in swine.M.VSc Thesis, Punjab Agricultural University,Ludhiana
Stalheim OH, Fayer R, Hubbert WT (1980) Update onbovine toxoplasmosis and sarcocystosis with empha-sis on their role in bovine abortions. J Am Vet MedAss 176:299–302
Stephens JWW, Fantham HB (1910) On the peculiarmorphology of a trypanosome from a case of sleepingsickness and the possibility of its being a new species(T. rhodesiense). Proc R Soc Lond B 83:28–33
Steverding D (2008) The history of African trypanoso-miasis. Parasites Vectors 1:3
Sutherst RW (1993) Arthropods as disease vectors in achanging environment. In: Lake JV, Bock GR,Ackrill K (eds) Environmental change and humanhealth. Ciba Foundation Symposium. AcademicPress, London, pp 124–145
Tanowitz HB, Kirchhoff LV, Simon D, Morris SA, WeissLM, Witfner M (1992) Chagas’ disease. Clin Micro-biol Rev, pp 400–419
Telford SR, Gorenflot A, Brasseur P, Spielman A (1993)Babesial infections in humans and wildlife. In: Kreier
JP (ed) Parasitic protozoa. Academic Press, SanDiego, pp 1–45
Telford SR, Spielman A (1997) Babesiosis of humans.In: Cox FEG, Kreier JP, Wakelin D (eds) Topley andWilson’s microbiology and microbial infections, 9thedn. Arnold, London, pp 349–359
Thompson RCA (2004) The zoonotic significance andmolecular epidemiology of Giardia and giardiasis.Vet Parasitol 126:15–35
Western KA, Benson GD, Gleason NN, Healy GR,Schultz MG (1970) Babesiosis in a Massachusettsresident. N Engl J Med 283:854–856
Wheatley W (1951) A rapid staining procedure forintestinal amoebae and flagellates. Am J Clin Pathol21:990–991
White KE, Hedberg CW, Edmonson LM, Jones DBW,Oster holm MT, MacDonald KL (1989) An outbreakof giardiasis in a nursing home with evidence formultiple modes of transmission. J Infect Dis160:298–304
WHO (1969) WHO technical report series, no. 421,(Amoebiasis: report of a WHO Expert Committee)
WHO (1985) Amoebiasis and its control. Bull WorldHealth Organ 63(3):417–426
WHO (1995) Division of diarrhoeal and acute respiratorydisease control, interim report, 1994. World HeathOrganization, Geneva
WHO (2006) African trypanosomiasis (sleeping sick-ness). Available at http://www.who.int/mediacentre/factsheets/fs259/en/
Winkle S (2005) Geißeln der Menschheit. Kulturgeschichte der Seuchen. Artemis & Winkler, Düsseldorf
Xiao L (1994) Giardia infection in farm animals.Parasitol Today 10:436–438
Xiao L, Herd RP (1994) Infection patterns of Cryptos-poridium and Giardia in calves. Vet Parasitol55:257–262
Xiao L, Herd RP, Rings DM (1993) Concurrent infec-tions of Giardia and Cryptosporidium on two Ohiofarms with calf diarrhea. Vet Parasitol 51:41–48
Zintl A, Mulcahyxc G, Skerrett HE, Taylor SM, Gray JS(2003) Babesia divergens, a bovine blood parasite ofveterinary and zoonotic importance. Clin Rev Micro-biol 16:622–636
40 2 Protozoonoses

3Trematode Zoonoses
Abstract
Trematode zoonoses could be defined as ‘‘those trematode diseases whichare naturally transmitted between (other) vertebrate animals and man’’.Many neglected trematode zoonotic diseases are being considered asimportant human infections. The penetration of human skin by cercariae ofavian schistosomes leads to cercarial dermatitis. Metagonimus yokogawaiand Heterophes heterophes are the important heterophyids which couldcause zoonotic disease. Pigs appear to be natural definitive host forGastrodiscus hominis, which causes disease in human beings. Fasciolosisis mainly important in livestock but human cases have been reported from42 countries. The parasite Fasciolopsis buski is prevalent in manySoutheast Asian countries. Accidental ingestion of ants infected withDicrocoelium dendriticum could cause human disease. Among all the liverflukes, Clonorchis sinensis is the most important fish-borne zoonosesprevalent in East Asia. The parasite Paragonimus westermani is found inAsia, Africa and South America. In Africa, the public health burden ofschistosomiasis, caused by Schistosoma mansoni, S. hematobium andS. intercalatum is enormous.
3.1 Cercarial Dermatitis
Subclass: DigeneaFamily: Schistosomatidae
3.1.1 Common Name/Synonyms
Schistosome dermatitis, Swimmer’s itch, ricefarmer’s itch or clam digger’s itch
Cercarial dermatitis occurs due to penetra-tion of human skin generally with cercariae ofavian schistosome parasites. The diseaseoccurs across the globe mostly near freshwaterhabitats. Swimmer’s itch is a commonnon-communicable water-borne disease andhas been recently regarded as an emerginginfection (De Gentile et al. 1996; Kolarova2007). Cercarial dermatitis is an occupationalzoonosis in certain populations.
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_3, � Springer India 2013
41

3.1.2 Etiology
The disease primarily occurs due to larvae of 20species of Schistosome genera such as Aus-trobilharzia, Dendritobilharzia, Gigantobilharzia,Trichobilharzia and Orientobilharzia.
3.1.3 Epidemiology
Cercarial dermatitis is trematode zoonosis andworldwide in occurrence (Farahnak and Essalat2003). The disease has been reported from manycountries in Europe and America (De Gentile et al.1996; Bastert et al. 1998; Folster-Holst et al. 2001;Kolarova et al. 1999; Chamot et al. 1998; Lind-blade 1998). The parasite has also been detected insnails in Germany (Loy and Haas 2001). The caseshave been reported in North America, Canada,Europe, Africa, the Far East (Hoeffler 1977;Mulvihill and Burnett 1990) and Taiwan (Wangand Chang 2008). Several outbreaks of cercarialdermatitis have also been reported in Quebec,Canada, Germany, France, Thailand and along theHuaihe River of China (Levesque et al. 2002;Kullallavanijaya and Wongwaisayawan 1993;Verbrugge et al. 2004; Li et al. 1998).
The schistosome larvae develop in freshwatersnails leading to association of the disease in lakesor ponds where cercariae of bird schistosomes areusually reported as the causative agent of thedisease (Horák et al. 2002; Kolarova 2007). Fewoutbreaks from salt or brackish waters have alsobeen reported (Horák et al. 2002; Kolarova 2007).
3.1.4 Reservoir
The cercaria’s normal hosts are birds, rodents andvarious other small mammals and human beingsact as an accidental host (Wang and Chang 2008).
3.1.5 Transmission
Humans become infected when cercariae presentin water bodies attach and enter through the skinof the human accidental host.
3.1.6 Life Cycle
The adult parasites live in the mesenteric bloodvessels of birds or mammals and produce eggswhich are released in faeces of the host. Theeggs released through faeces into the waterbodies hatch and release miracidia. The mira-cidia penetrate an appropriate species of inter-mediate snail host. In snail they further developinto multiple sporocysts. Numerous fork-tailedcercariae develop in the snail host throughasexual multiplication (Bastert et al. 1998;Folster-Holst et al. 2001; Farahnak and Essalat2003). The cercariae are released in the waterwhere they penetrate a vertebrate definitive oraccidental (Brant et al. 2010) host’s skin usingoral suckers and release a proteolytic enzymewhich facilitates their penetration (Wang andChang 2008).
3.1.7 Clinical Signs in Man
The clinical disease was first reported by Fujiiin 1887 (Oda 1973). The schistosome larvae(cercariae) were identified as the causativeagent by Cort in 1928 in the USA. Thisfollowed the reporting of the causative agentsfrom United Kingdom (Matheson 1930) andFrance (Brumpt 1931). Christensen and Green(1928) used the word swimmers’ itch for thedisease. Clinical signs in man include a strongmaculo-papulovesicular skin eruption andintensive itching affecting areas exposed towater (Horák et al. 2002; Kolarova 2007).
The cercaria of non-human schistosomiasiscould occasionally penetrate the epidermis, butare unable to reach the bloodstream and toinduce systemic infection (Haas and van deRoemer 1998; Wang and Chang 2008). Theseparasites induce Type I hypersensitivity reactionand finally die due to histolysis (Wang andChang 2008). The residual cercarial proteincould induce Type IV hypersensitivity reactionand diffused skin eruptions (Kourilova et al.2004).
42 3 Trematode Zoonoses

3.1.8 Clinical Signs in Animals
Although cercarial dermatitis is mainly related tohuman infections, symptoms have been reportedin animals such as rabbits and dogs (Herber1938; Augustine and Weller 1949; Olivier 1953).
3.1.9 Diagnosis
History of exposure to the contaminated fresh-water and clinical signs give preliminary indi-cation for the disease (Scrimgeour and Daar2000). The parasite could be detected bymicroscopic observation of schistosome larvaefrom water snails (Kolarova 2007).
3.1.10 Control
Use of personnel protective measures could helpprevent the disease in human beings.
3.2 Dicrocoeliasis
Subclass: DigeneaOrder: PlagiorchiidaFamily: Dicrocoeliidae
3.2.1 Common Name/Synonyms
Lancet liver fluke disease
3.2.2 Etiology
The disease occurs due to D. dendriticum andD. hospes. The parasite resides in the bile ducts ofsheep, cattle and other mammals including man.
3.2.3 Epidemiology
The parasite is distributed in Europe (Mediterra-nean area), Asia (Middle East, Indonesia, Japan,Malaysia, People’s Republic of China), former
Soviet Union, North Africa, South America andsome foci in North America (Jeandron et al. 2011;Le Bailly and Bouchet 2010). Although theinfection is common in livestock, it has been rarelyreported in human beings (Jeandron et al. 2011).Human infections by D. dendriticum, a zoonoticliver fluke are not common and rare in occurrence.Most reports concern autochthonous populationsin Europe, Middle East and immigrants fromNorth Africa (Gualdieri et al. 2011; Ashrafi 2010).D. dendriticum has also been reported in humansfrom Canada (Schweiger and Kuhn 2008).Samalia et al. (2009) reported the disease in a7-year-old child presented with recurrent rightflank subcutaneous nodules containing a liverfluke on excision, and tissue histology showedcharacteristic brown operculated ova of D. den-driticum. El-Shafie et al. (2011) reported zoonoticdicrocoeliasis among a farmer’s family and hisdomestic animals. The human infection is mainlyasymptomatic or subclinical, but clinical cases ofhuman dicrocoeliasis have also been reportedfrom different parts of the world, including Iran(Ashrafi 2010) and Turkey (Cengiz et al. 2010).Cases of dicrocoeliasis in patients infected withthe human immunodeficiency virus (HIV) havealso been reported (Drabick et al. 1988; Zaliet al. 2004). D. dendriticum eggs have also beenfound in the stool of a patient with Crohn’s disease(Schweiger and Kuhn 2008). In Egypt, Helmyand Al-Mathal (2003) found that 121/1196patients were positive for D. dendriticum.
3.2.4 Reservoir
D. dendriticum is a small lancet fluke infectingdomestic and wild ruminants (e.g., buffalo, cattle,goat, sheep and deer), rabbits, and, occasionally,dogs, horses, pigs and humans. The parasite isfound in the small bile duct and gall bladder of themammalian host (Jeandron et al. 2011).
3.2.5 Transmission
Humans become infected after accidental inges-tion of infected ants (containing the metacercariae)
3.1 Cercarial Dermatitis 43

present on fruits, vegetables, grass or in drinkingwater (Haridy et al. 2003).
3.2.6 Life Cycle
Life cycle of the parasite involves two interme-diate hosts’ viz. land snails and ants (Fig. 3.1).
3.2.7 Clinical Signs in Manand Animals
The disease is generally asymptomatic in humanbeings. The clinical signs and pathology isgenerally similar to other liver trematodes suchas Clonorchis sinensis, Fasciola hepatica, and
Opisthorchis viverrini, and may include chronicdiarrhoea, constipation, right upper abdominalpain, vomiting, weight loss and fatigue(Jeandron et al. 2011). Hepatomegaly, peripheraleosinophilia, biliary obstruction and cholangitiscould also occur (Rana et al. 2007; Jeandronet al. 2011). Acute urticaria (Singh et al. 2008)has also been reported.
3.2.8 Diagnosis
The disease is difficult to diagnose from clinicalsigns. The disease can be diagnosed by identi-fication of the parasite eggs in the faecal sam-ples, while a living or dead fluke could be rarelyseen.
Fig. 3.1 Life cycle of Dicrocoelium dendriticum
44 3 Trematode Zoonoses
3.2.9 Control
Control of intermediate host population viz.snail and ants, health education can help in theprevention of the disease.
3.3 Echinostomiasis
Subclass: DigeneaFamily: Echinostomatidae
3.3.1 Common Name/Synonyms
Echinostomatidiasis
3.3.2 Etiology
These are intestinal parasites which can infectbirds and mammals. There are 15 species whichcan infect humans (Chai et al. 2005a, b;Yamashita 1964; Huffman and Fried 1990).Echinostoma hortense, Echinochasmus japoni-cus, E. echinatum are important species from 11fish-borne echinostomes (Chai et al. 2005a, b;Yu and Mott 1994; Chai and Lee 2002; Carney1991; Ujiie 1963).
3.3.3 Epidemiology
Human infections have been reported from Asia,Western Pacific and Africa (Chai et al. 2005a, b;Yu and Mott 1994; Haseeb and Eveland 2002).E. hortense has been reported from humans androdents in the Republic of Korea (Chai and Lee2002) and China (Yu and Mott 1994; Yu et al.1994). The parasite is endemic in Southeast Asiaand the Far East, i.e. mainland China, Taiwan,India, Korea, Malaysia, Philippines and Indonesia(Fried et al. 2004; Bandyopathy and Nandy 1986).
3.3.4 Life Cycle
Freshwater snail act as first intermediate hostwhere cercariae develop and may encyst asmetacercariae in another snail, mollusk, tadpoleor freshwater fish (second intermediate hosts)(Acha and Szyfres 2006).
3.3.5 Transmission
Ingestion of raw or undercooked second inter-mediate host (fish) can cause infection in humanbeings.
3.3.6 Clinical Signs in Man
The symptoms are generally related to the levelof parasitemia (Fried et al. 2004; Bandyopathyand Nandy 1986; Chai et al. 1994). Clinical signsare generally not evident but ulcerations andbleeding in the stomach or duodenum may occurin E. hortense infection (Chai et al. 1994). Inlight to moderate infections, anaemia, headache,dizziness, slight stomach ache, gastric pain andloose stools have been reported (Chattopadyayet al. 1990; Bundy et al. 1991). Heavy infectionsare associated with eosinophilia, abdominal pain,profuse watery diarrhoea, anaemia, oedema andanorexia (Chattopadyay et al. 1990). Severeulcerative lesions with bleeding in the duodenumhave also been reported in some cases (Chai et al.1994).
3.3.7 Clinical Signs in Animals
The experimental infections in rats have lead todecrease in villus/crypt ratio, villous atrophy,crypt hyperplasia and inflammation of thestroma (Chai et al. 2005a, b; Chai and Lee2002).
3.2 Dicrocoeliasis 45

3.3.8 Diagnosis
The disease can be diagnosed by identificationof characteristic operculate, non-embryonated,ellipsoidal, yellow to yellow–brown eggs and bythe morphology of the adult parasite (Fried et al.2004; Bandyopathy and Nandy 1986). Inrodents, the infections can be diagnosed on thebasis of serological tests (Graczyk and Fried1994, 1995; Graczyk 1997).
3.3.9 Treatment
Praziquantel @ 10–20 mg/kg in a single oralregimen can be used to treat the infections (Chaiand Lee 2002).
3.3.10 Control and Prevention
The human disease can be controlled by inter-rupting the life cycle of the parasite (Graczykand Fried 1998). Avoiding consumption of rawor undercooked meat of molluscs, fish, crusta-ceans and amphibians can help prevent the dis-ease in humans (Graczyk and Fried 1998).
3.4 Fascioliasis
Subclass: DigeneaSuperfamily: Fasciolidae
3.4.1 Common Name/Synonyms
Sheep liver fluke disease
3.4.2 Etiology
The disease occurs due to liver fluke F. hepaticaand F. gigantica.
3.4.3 Epidemiology
The fascioliasis is mainly important in livestock(Malek 1980; Boray 1982). Human cases havebeen reported from 42 countries (Chen and Mott1990; Esteban et al. 1998; Mas-Coma et al.1999a, b) and up to 2.4 million people arebelieved to be infected with this parasite (Rim1994; WHO 1995a). F. hepatica mainly occursin Europe, Asia, Africa, Americas and Oceania.F. gigantica has been reported in Asia and Africa(Ashrafi et al. 2006). Human fascioliasis isbecoming an important public health problemthese days (Chen and Mott 1990; WHO 1995b;Mas-Coma et al. 1999a, b). Health problems dueto human fascioliasis have been reported in manycountries such as Bolivia, Peru, Chile, Ecuador,Cuba, Egypt, Portugal, France and Spain and Iran(Mas-Coma et al. 2004, 2005a, b).
3.4.4 Transmission
Sheep and cattle mainly act as reservoir hosts forF. hepatica. The infection in human beings canoccur directly through drinking contaminatedwater or through ingestion of contaminatedfreshwater plants or vegetables (Chen and Mott1990; Mas-Coma et al. 1999a; Cadel 1996).
3.4.5 Life Cycle
The parasite needs two hosts to complete theirlife cycle. The definitive hosts mainly includeherbivorous animals such as sheep, cattle andhuman beings. In the definitive hosts, eggs passthrough bile duct and are excreted in the faeces.Eggs develop outside the host to miracidialstage. Miracidia enters the freshwater snails. Thesnails of the family Lymnaeidae act as inter-mediate hosts. Miracidia develop to rediae in thesporocyst which further develop to cercariaewhich swim in water and attaches to freshwateraquatic plants. Encystation of cercaria occursand humans and other definitive hosts become
46 3 Trematode Zoonoses

infected after ingestion of infective metacerca-riae (Mas-Coma et al. 2005a, b) (Fig. 3.2).
3.4.6 Clinical Signs in Animals
There is development of haemorrhagic tracts,swelling in the liver. Fibrosis of the liver couldresult in bile duct blockage and inflammationwhich can result in death during chronic phaseof the disease. The occurrence of submandibularoedema (Bottle jaw) is a typical symptomnoticed in fasciolosis.
3.4.7 Clinical Signs in Man
Hepatic involvement results in inflammation andswelling of the liver. Additional symptomsinclude abdominal pain, anaemia, fever, chole-cystitis and cholelithiasis.
3.4.8 Diagnosis
The disease can be diagnosed through clinicalsigns, identification of the eggs, during PMexamination and by immunological tests.
3.4.9 Control
Prevention and control of animal fasciolosis,vector population can help control the disease inhuman beings (Roberts and Suhardono 1996;Torgerson and Claxton 1999; Spithill et al.1999). Avoid ingestion of contaminated plants inendemic areas.
3.5 Fasciolopsiasis
Subclass: DigeneaFamily: Fasciolidae
Fig. 3.2 Life cycle of Fasciola hepatica
3.4 Fascioliasis 47
3.5.1 Etiology
The disease occurs due to F. buski, which is thelargest fluke affecting human being (Kuntz andLo 1967).
3.5.2 Epidemiology
The parasite is prevalent in many countries ofsouth and East Asia including Thailand, China,Taiwan, Vietnam, Bangladesh and India(Mas-Coma et al. 2005a, b; Lo and Lee 1996;Wiwanitkit et al. 2002; Gilman et al. 1982; Leet al. 2004). Fasciolopsiasis has been reviewedin detail by Mas-Coma et al. (2005a, b).
3.5.3 Reservoir
Pigs act as important reservoirs of infection(Rim 1982a, b, c).
3.5.4 Transmission
Human beings become infected through ingestionof metacercariae by drinking contaminated wateror due to consumption of infected plants. Fascio-lopsiasis generally occurs near freshwater habitatswith stagnant or slow moving waters (Mas-Comaet al. 2005a, b). Cultivation of freshwater plantsand pollution with human and animal (mainly pig)excreta are important factors for the transmissionof the disease (Mas-Coma et al. 2005a, b).
3.5.5 Life Cycle
The adult parasite is present in the intestine of thehuman and pig host. The parasite inhabits duo-denum and jejunum but could be found in otherparts of the intestinal tract in heavy infections.Eggs released in the faeces embryonate in waterin 3–7 weeks (Weng et al. 1989). After hatching,miracidia infect snails of the genera Segmentina,Hippeutis and Gyraulus which shed cercariaeafter 4–6 weeks (Graczyk et al. 2000). Cercariae
encyst on the surface of freshwater plants (Wenget al. 1989). Ingestion of metacercariae lead toinfection in human and pig hosts.
3.5.6 Disease in Man
High morbidity occurs due to fasciolopsiasis inendemic areas (Graczyk et al. 2001; Weng et al.1989) and the disease may become fatal in heavyinfections (Graczyk et al. 2001 and Weng et al.1989). In light infections, anaemia, headache,dizziness, stomach ache, gastric pain and loosestools (Gilman et al. 1982) may be seen. Heavyinfections could result in severe epigastric andabdominal pain, diarrhoea or bowel obstruction,nausea, acute ileus, anasarca and markedeosinophilia and leucocytosis (Gilman et al.1982). Malnutrition (Graczyk et al. 2001; Wenget al. 1989) is an important factor associatedwith heavy infections.
3.5.7 Diagnosis
The disease may be diagnosed by faecal sampleexamination for presence of eggs and adultparasite (Mas-Coma et al. 2005a, b). Moleculartechniques could also be used in future.
3.5.8 Control
Control can be achieved by proper diagnosis,treatment of people and livestock, preventingreinfection and instituting modern pig farmingand avoiding consumption of freshwater plants(Mas-Coma et al. 2005a, b).
3.6 Gastrodisciasis
Subclass: DigeneaFamily: Paramphistomatidae
3.6.1 Common Name/Synonyms
Gastrodiscoidosis, Amphistomiasis
48 3 Trematode Zoonoses

3.6.2 Etiology
Gastrodiscoides species are approximately8–14 mm in length (Fried et al. 2004).Gastrodiscoides hominis causes disease in humanbeings. The parasite has a pharynx, tandem, lobedtestes, a post-testicular ovary, an ascendinguterus and a ventral genital pore (Kumar 1999).
3.6.3 Epidemiology
The parasite has been reported primarily fromIndia but cases have been reported fromBangladesh and East Asian countries (Acha andSzyfres 2006).
3.6.4 Transmission
The transmission of the disease occurs when rawor undercooked vegetation, crustaceans, mol-luscs or amphibians contaminated with encystedmetacercariae are consumed.
3.6.5 Clinical Signs in Manand Animals
Swine appears to be natural definitive host. Thedisease condition associated with G. hominis isalso referred to as gastrodisciasis. The flukesexcyst from metacercariae and descend in theintestinal tract to reach the cecum and colonwhere they mature and live as adults (Kumar1999). The parasite infects humans and hogs,e.g. hogs in Africa (Goldsmid 1975; Hira 1983)and India (Murty and Reddy 1980). Disease isgenerally inapparent but could cause mucoiddiarrhoea (Strickland 1991).
3.6.6 Diagnosis
Morphological identification of trematode flukeand detection of parasite eggs in faecal samplescan help in diagnosis of the disease.
3.7 Heterophyiasis
Subclass: DigeneaFamily: Heterophyidae
3.7.1 Common Name/Synonyms
Heterophyes infection
3.7.2 Etiology
Heterophyids are minute intestinal flukesbelonging to the family Heterophyidae (Chaiet al. 2005a, b). These parasites infect birds andmammals (Chai et al. 2005a, b). Although 35heterophyid species can infect man (Chai et al.2005a, b), but from zoonotic point of view,Metagonimus yokogawai and Heterophyesheterophyes are the important species (Yu andMott 1994). Studies have been carried out fromPhilippines (Belizario et al. 2001) and Thailandon Haplorchis taichui (Waikagul 1991;Sukontason et al. 2001) and from Korea on sev-eral species including Heterophyes nocens andMetagonimus species (Chai and Lee 1991; Chaiand Lee 1990, 2002; Chai et al. 2005a, b). Aquaticsnails and fresh or brackish-water fish acts as firstand second intermediate hosts, respectively.
3.7.3 Metagonimiasis
The genus Metagonimus is identified by a lat-erally deviated ventral sucker and absenceof ventrogenital apparatus or genital sucker(Chai and Lee 2002).
3.7.3.1 EtiologyThe disease occurs due to M. yokogawai,Metagonimus takahashii, M. minutus andMetagonimus miyatai.
3.7.3.2 TransmissionThe molluscan freshwater snail acts as an inter-mediate host (Chai and Lee 2002). The species
3.6 Gastrodisciasis 49

has rather broad fish host specificity, but thesweet fish Plecoglossus altivelis is an importantfish host in Korea and Japan (Chai et al. 2005a, b).
3.7.3.3 EpidemiologyThe disease is endemic in Korea (Chai et al.1977; Seo et al. 1981; Chai and Lee 2002; Chaiet al. 1993). The human infections have alsobeen recorded from Siberia, Europe, China,Japan, Russia and Taiwan (Chai et al. 2005a, b;Yu and Mott 1994; Ito et al. 1991).
3.7.3.4 Clinical Signs in ManThe parasite affects the mucosa of the middle partof the small intestine (Chai 1979) and could leadto villous atrophy, crypt hyperplasia and inflam-matory reactions (Chai 1979). Gastrointestinalproblems such as epigastric pain, diarrhoea,anorexia and fatigue could occur in mild infec-tions. Heavy infections may lead to abdominalcramps, malabsorption and weight loss.
3.7.3.5 DiagnosisThe disease may be diagnosed by identificationof the parasite eggs by faecal examination.
3.7.3.6 TreatmentPraziquantel @ dose of 10–20 mg/kg orally maybe used for treatment of the infection (Chai andLee 2002).
Other Metagonimus species
Other Metagonimus species infecting humansinclude M. takahashii Suzuki (Chai and Lee2002) and M. miyatai (Saito et al. 1997; Chaiand Lee 2002) which can be differentiated fromM. yokogawai using PCR-based-restrictionfragment length polymorphism (PCR–RFLP)patterns, karyotypes, simple sequence repeat-PCR (SSR–PCR) patterns (Chai and Lee 2002)and amplification of mitochondrial cytochrome coxidase subunit I and 28S ribosomal DNAsequences (Lee et al. 2004).
3.7.4 Heterophyiasis Dueto Heterophyes Species
The genus Heterophyes is characterised by themedian location of the ventral sucker and thepresence of a genital sucker armed with gonotyl(Chai and Lee 2002).
3.7.4.1 EtiologyThe disease occurs due to Heterophyiasis het-erophyes (v. Siebold, 1852, Stiles and Hassall,1900), Heterophyes dispar and H. nocens (syn.Heterophyes katsuradai), (Yu and Mott 1994;Chai et al. 1986; Chai and Lee 2002). The adultflukes measure 1.0–1.7 mm long, 0.3–0.4 mmwide, and possess large median ventral suckerand a genital sucker with gonotyl armed with60–90 multidigitate spines (Beaver et al. 1984).
3.7.4.2 EpidemiologyThe adult parasites are found in fish-eating birdsand mammals in addition to humans (Radomyoset al. 1994; Kumar 1999). The parasite is frag-mented in distribution in parts of the world (Chaiet al. 2005a, b; Yu and Mott 1994). Humandisease has been recorded from Egypt, Japan(Kagei et al. 1980) and Republic of Korea (Chaiet al. 1986; Chai and Lee 2002).
3.7.4.3 TransmissionConsumption of raw, undercooked or inade-quately processed freshwater, brackish or marinefishes (Radomyos et al. 1994) and mullet Mugilcephalus (Yu and Mott 1994) are importantsources of infection.
3.7.4.4 Life CycleDogs, cats, foxes, jackals and other fish-eatingmammals act as important reservoirs (Radomyoset al. 1994). Pirenella conica and Cerilbida cengu-lata are the important gastropod first intermediatehosts of these heterophyids. The second intermedi-ate hosts include brackish-water fishes in the genusMugil (mullets), Aphanius and Acanthogobius.
50 3 Trematode Zoonoses

3.7.4.5 Clinical Signs in Animalsand Man
The disease is generally asymptomatic but highparasitemia could lead to irritation of intestinalmucosa, increased mucus, chronic diarrhoea,colic and nausea (Acha and Szyfres 2006).Aberrant eggs may produce granulomatous foci inmyocardium and brain (Acha and Szyfres 2006).
3.7.4.6 DiagnosisMorphological identification of adult fluke anddetection of parasite eggs in faecal samples canhelp in diagnosis (Radomyos et al. 1994).
3.7.4.7 Prevention and controlControl measures include avoidance of eatingraw or undercooked fish, personnel hygienemeasures, treatment of infected people, envi-ronmental sanitation, proper excreta disposaland disease awareness.
3.7.5 Haplorchiasis
Haplorchis species have a single testis and ventro-genital sucker complex with gonotyl and chitinousspines (Chai et al. 2005a, b; Yamaguti 1958).Human disease can occur due to H. taichui,Haplorchis pumilio, Haplorchis yokogawai,Haplorchiasis pleurolophocerca and Haplorchisvanissimus (Yu and Mott 1994; Chai et al. 2005a, b);the first three parasites are the most important (Chaiet al. 2005a, b). The Haplorchis species are foundthroughout Asia (Velasquez 1982) among humans.H. taichui Chen 1936 was first reported from birdsand mammals from central Taiwan (Faust andNishigori 1926). H. pumilio is distributed in Asia(Velasquez 1982; Yu and Mott 1994) in birds andmammals. H. yokogawai human infections havealso been reported from many Asian countries,Australia and Egypt (Velasquez 1982; Yu and Mott1994).
3.8 Nanophyetus
Subclass: DigeneaFamily: Troglotrematidae
3.8.1 Common Name/Synonyms
Salmon poisoning (in animals), Elokomin flukefever
3.8.2 Etiology
The disease occurs due to trematode flukeNanophyetus salmincola Chapin, 1927 (syn.Troglotrema salmincola Witenberg 1932)belonging to the family Nanophyetidae (Chaiet al. 2005a, b). Nanophyetus schikhobalowi, isanother species described from natives of far-eastern Siberia and is regarded as a subspeciesN. salmincola schikhobalowi (Millemann andKnapp 1970; Kumar 1999).
3.8.3 Epidemiology
Eastburn et al. (1987) recorded 10 cases ofNanophyetus from North West America. Ferrelet al. (1974) also detected cases of Nanophyetussalmincola in kippered salmon in America. Thedisease is endemic in the far-eastern part ofRussia (Yu and Mott 1994). In USA, the prev-alence in local ethnic minorities could reach upto 60 % (Eastburn et al. 1987).
3.8.4 Life Cycle
The snail Oxytrema silicula acts as the firstintermediate host in USA and Semisulcospiracancellata and S. laevigata in Siberia. The sal-monid (trout, salmon) and non-salmonid fish(Millemann and Knapp 1970) act as secondintermediate hosts. The non-embryonated eggsare released in the faeces of the mammalianhost. Miracidia develop within the egg in about4 months and hatches and penetrates in the firstintermediate host. Cercariae develop and emergefrom the snail to penetrate skin and gills ofsalmonid fish. This is followed by encystation inthe muscles and connective tissues of secondintermediate host (Fried et al. 2004). The adultparasite develops in the intestine of definitive
3.7 Heterophyiasis 51

host after consumption of infected fish (Schell1985). The adult resides in the small intestine ofmammals (Schell 1985).
3.8.5 Reservoir
The fishes Oncorhynchus species, Salmo spe-cies, Cottus perplexus, Dicamptodin ensatus andSalvelinus fortinalis transmit the infection tohumans in the United States (Fried et al. 2004).
3.8.6 Transmission
Consumption of raw or undercooked infectedfish is an important source of infection.
3.8.7 Clinical Signs in Man
Clinical signs include gastrointestinal symptomssuch as peripheral blood eosinophilia, increasedfrequency of bowel movements or diarrhoea,abdominal discomfort, nausea, vomition, weightloss and fatigue (Eastburn et al. 1987).
3.8.8 Clinical Signs in Animals
The parasite can infect different mammalsincluding dogs, cat, raccoon and foxes. The par-asite also affects three species of birds on thePacific coast of North America, Canada andEastern Siberia (Chai et al. 2005a, b; Millemannand Knapp 1970; Beaver et al. 1984). In dogs,foxes and coyotes, this fluke is particularlyimportant as it acts as the vector of a rickettsia,Neorickettsia helmintheca, which causes a seriousand often fatal systemic infection known as ‘sal-mon poisoning’, which has not been reported inhumans (Chai et al. 2005a, b). The mortality due torickettsia in dogs may reach 90 % (Schell 1985).
3.8.9 Diagnosis
The disease can be diagnosed by detection ofeggs typical for N. salmincola from stool
samples. Eggs of the parasite are operculate andnot embryonated.
3.8.10 Control
Avoid eating raw or undercooked fish.
3.9 Other Liver Flukes
Subclass: DigeneaFamily: Opisthorchiidae
These liver flukes belong to the familyOpisthorchiidae. These include clonorchiasis,opisthorchiasis and Metorchis infections. Theseparasites generally have similar life cycles andsymptoms (Chai et al. 2005a, b). As per WHO,17 million people are infected with liver flukes(WHO 1995a, b, c).
3.9.1 Clonorchiasis
3.9.1.1 Common Name/SynonymsChinese Liver fluke disease
3.9.1.2 EtiologyThe disease occurs due to C. sinensis. Among allthe liver flukes, C. sinensis is the most importantfish-borne zoonosis prevalent in East Asia (Chaiet al. 2005a, b; Rim 1990; Chen et al. 1994;Hong 2003; Yoshida 2012).
3.9.1.3 EpidemiologyThis parasite causes serious disease in manyparts of the world (Chai et al. 2005a, b) partic-ularly in China, Japan, Korea and countries ofSoutheast Asia (Shekhar et al. 1995).
3.9.1.4 ReservoirThe cats, dogs and pigs are believed to act asreservoirs but their role as reservoirs has notbeen well studied (Chen et al. 1994; WHO1995a, b, c).
52 3 Trematode Zoonoses

3.9.1.5 TransmissionThe definitive hosts become infected throughconsumption of raw or undercooked infectedfish.
3.9.1.6 Life CycleThe parasite lives in the biliary tract of defin-itive host (man and fish-eating animals) andsheds eggs through bile duct and intestines(Chai et al. 2005a, b). Freshwater snails(Parafossarulus manchouricus and otherhydrobid snails) ingest these eggs. The mira-cidia hatches in the snail and develop intosporocysts (Rim 1982a). Rediae are formedwithin the sporocyst and cercariae furtherdevelop within the rediae (Chai et al. 2005a, b;Kaewkes 2003). In water, free swimming cer-caria penetrates beneath the fish’s scales and istransformed into an encysted metacercaria(Chai et al. 2005a, b). Many species of thefreshwater fishes and shrimp can act as thesecond intermediate host (Chen et al. 1994;Park et al. 2004). The metacercariae developinto the adult in the definitive host (Rim 1986).Humans and fish-eating mammals and birds canact as definitive hosts (Fig. 3.3).
3.9.1.7 Clinical Signs in Animalsand Man
Most important symptoms include calculi for-mation, cholangitis, cholecystitis and cholan-giohepatitis. Infection of pancreas could lead topancreatitis or obstruction of pancreatic duct.Chronic infections can also lead to cholangio-carcinoma (Flavell 1981; Chai et al. 2005a, b).
3.9.1.8 DiagnosisThe disease can be diagnosed by multiple stoolexaminations for identification of parasite eggsin faeces. The eggs may also be diagnosed fromduodenal aspirates. Specialised techniques suchas cellophane thick smear (Chai et al. 1982) orKato-Katz techniques (Hong et al. 2003) may beused. Serological tests such as ELISA may alsobe done (Choi et al. 2003).
3.9.1.9 ControlThe prevention and control relies on avoidingconsumption of raw or undercooked fish, vectorcontrol and prompt diagnosis and treatment ofthe infection.
3.9.2 Opisthorchiasis
Four species of the parasite viz. O. viverrini,Opisthorchis felineus, O. noverca and O. guaya-quilensis could infect humans (Kaewkes 2003).Out of these, O. viverrini is prevalent in SoutheastAsia (Chai et al. 2005a, b; Shekhar et al. 1995)and particularly causes serious disease (Chai et al.2005a, b; Rim 1982b; Kaewkes 2003). O. felineusis a parasite of dogs, cats, foxes and pigs in Europeand the Asiatic parts of Russia, Turkey andSiberia (Chai et al. 2005a, b; Beaver et al. 1984;Rim 1982b). The life cycles, symptoms anddiagnosis are similar to that of C. sinensis.
3.9.3 Metorchiosis (Canadian LiverFluke)
The disease occurs due to Metorchis conjunctus.The parasite is found in carnivorous animals
in Canada and USA (MacLean et al. 1996).Human infections have also been reported inCanada (Yamaguti 1958; MacLean et al. 1996;Behr et al. 1998). Mode of transmission, symp-toms are similar as for other liver fluke infec-tions (Rim 1982b; Beaver et al. 1984).Carcinoma of the infected parts may lead todeath in some cases.
3.10 Paragonimiasis
Subclass: DigeneaFamily: Troglotrematidae
3.10.1 Common Name/Synonyms
Lung fluke disease, pulmonary distomatosis,endemic hemoptysis and oriental hemoptysis.
3.9 Other Liver Flukes 53
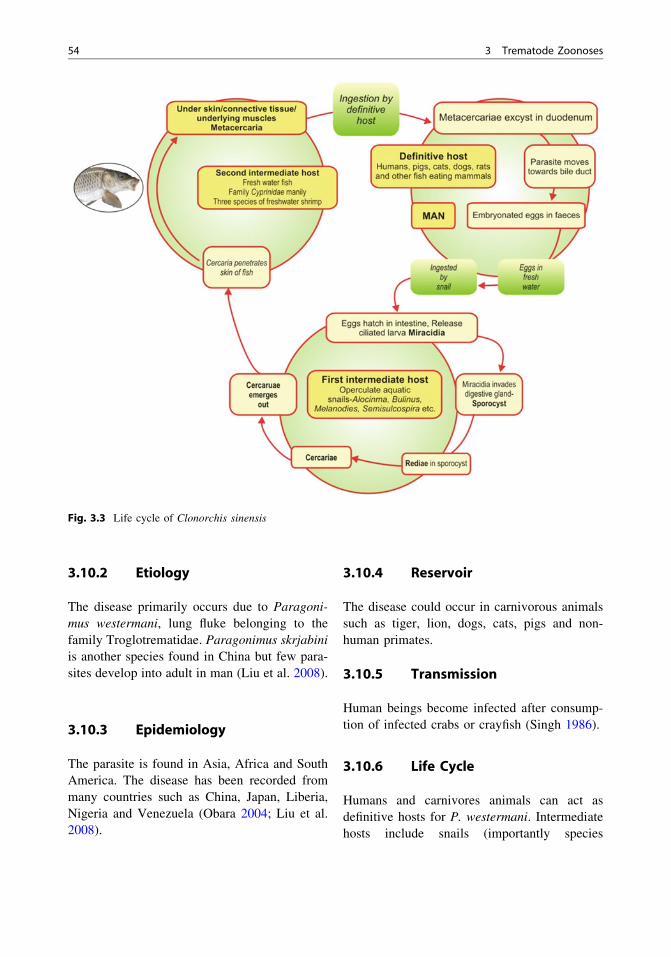
3.10.2 Etiology
The disease primarily occurs due to Paragoni-mus westermani, lung fluke belonging to thefamily Troglotrematidae. Paragonimus skrjabiniis another species found in China but few para-sites develop into adult in man (Liu et al. 2008).
3.10.3 Epidemiology
The parasite is found in Asia, Africa and SouthAmerica. The disease has been recorded frommany countries such as China, Japan, Liberia,Nigeria and Venezuela (Obara 2004; Liu et al.2008).
3.10.4 Reservoir
The disease could occur in carnivorous animalssuch as tiger, lion, dogs, cats, pigs and non-human primates.
3.10.5 Transmission
Human beings become infected after consump-tion of infected crabs or crayfish (Singh 1986).
3.10.6 Life Cycle
Humans and carnivores animals can act asdefinitive hosts for P. westermani. Intermediatehosts include snails (importantly species
Fig. 3.3 Life cycle of Clonorchis sinensis
54 3 Trematode Zoonoses

Semisulcospira, Melanopides) and crabs orcrayfish (Velez 2003). In humans and carnivoresanimals, lungs are important site of predilectionand harbour the adult parasite (Liu et al. 2008;Guan 2005). The eggs are coughed up from therespiratory system and passed in faeces. Con-tamination of freshwater with faeces of thedefinitive host leads to embryonation andhatching of the eggs. Free swimming miracidiaenters the first intermediate host. Miracidiadevelops to sporocyst to redia to cercaria in thefirst intermediate host. Crabs or cray fish ingeststhe snail and cercariae encysts and develops intometacercariae in the vessels of the gills, liverand muscles of the cephalothorax. Humans andcarnivores animals become infected after theingestion of raw or undercooked infected
crustacean host. Metacercariae excyst in intes-tinal tract and reach through abdominal cavity todiaphragm to pleural cavity and finally to thelungs (Obara 2004; Guan 2005) (Fig. 3.4).
3.10.7 Clinical Signs in Animals
The involvement of respiratory system may leadto formation of granulomata and abscess cavities.
3.10.8 Clinical Signs in Man
The respiratory system infections could result insymptoms such as chest pain, cough, blood-stained sputum and dyspnea. If gastrointestinal
Fig. 3.4 Life cycle of Paragonimus westermani
3.10 Paragonimiasis 55
system is infected, symptoms include abdominalpain, or diarrhoea and eggs can be seen in thestools (Waikagul 1989). Extrapulmonary para-gonimiasis mostly result in involvement ofcentral nervous system (Huang 2000).
3.10.9 Diagnosis
The disease may be diagnosed from clinicalsigns, detection of eggs from sputum or faecesand CT, MRI or serological techniques.
3.10.10 Control
Control measures include avoiding consump-tion of raw or undercooked crab or crayfish, control of intermediate host (snail) pop-ulations and avoiding contamination of surfacewater with faeces of definitive host (Liu et al.2008).
3.11 Schistosomiasis
Subclass: DigeneaOrder: StrigeididaFamily: Schistosomatidae
3.11.1 Common Name/Synonyms
Bilharziasis, snail fever
3.11.2 Etiology
The disease occurs due to Schistosoma haemat-obium (urinary schistosomiasis), S. mansoni,S. japonicum, S. mekongi and S. malayi, (gas-trointestinal and hepatosplenic schistosomiasis)and S. intercalatum, which also affects the GItract but with lower morbidity (Almeda et al.1994; Corachan 2002).
3.11.3 Epidemiology
More than 300 million people are believed to beinfected worldwide, the parasite being morecommon in children aged between 5 to 15 years(WHO 1993; Standley et al. 2009; Fenwick et al.2009). Schistosomiasis has been reported in mostAfrican countries, limited areas of SouthAmerica, Caribbean, Middle East and Asia(Corachan 2002; Standley et al. 2012; Hotez et al.2008). Schistosoma japonicum is the causativeagent of schistosomiasis in China, Philippinesand in small pockets of Indonesia (Gray et al.2008; Ross et al. 2001, 2002). In Africa,the public health burden of schistosomiasis,caused by S. mansoni, S. haematobium andS. intercalatum/guineensis, is enormous (Hotezand Fenwick 2009). The losses occurring due tohuman schistosomiasis caused by S. mansoni,S. haematobium and S. japonicum have beenestimated to be 1.7–4.5 million disability adjustedlife years (McManus et al. 2010) (DALYs). Thetrue burden was found to be substantially greaterthan previous estimates (Finkelstein et al. 2008;Jia et al. 2007; King et al. 2005; Van der Werfet al. 2003). In China, zoonotic schistosomiasisjaponica, also called ‘‘snail fever,’’ is a significanthealth risk for human and livestock populations(McManus et al. 2010, 2009; Ross et al. 2001;Utzinger et al. 2005; Wang et al. 2006; Zhou et al.2005, 2007).
3.11.4 Reservoir
The zoonotic nature of S. japonicum furthercomplicates parasite transmission and control. Theparasite has ability to infect more than 40 speciesof wild and domestic animals (WHO 1993). Ear-lier studies indicated public health importance ofrats, dogs, pigs, sheep and goats, cattle and waterbuffalo hosts (Johansen et al. 2000; WHO 1993).In China, however, water buffaloes (Bubalusbubalis) could play a significant role in the trans-mission of S. japonicum (Johansen et al. 2000;WHO 1993; Gray et al. 2008).
56 3 Trematode Zoonoses
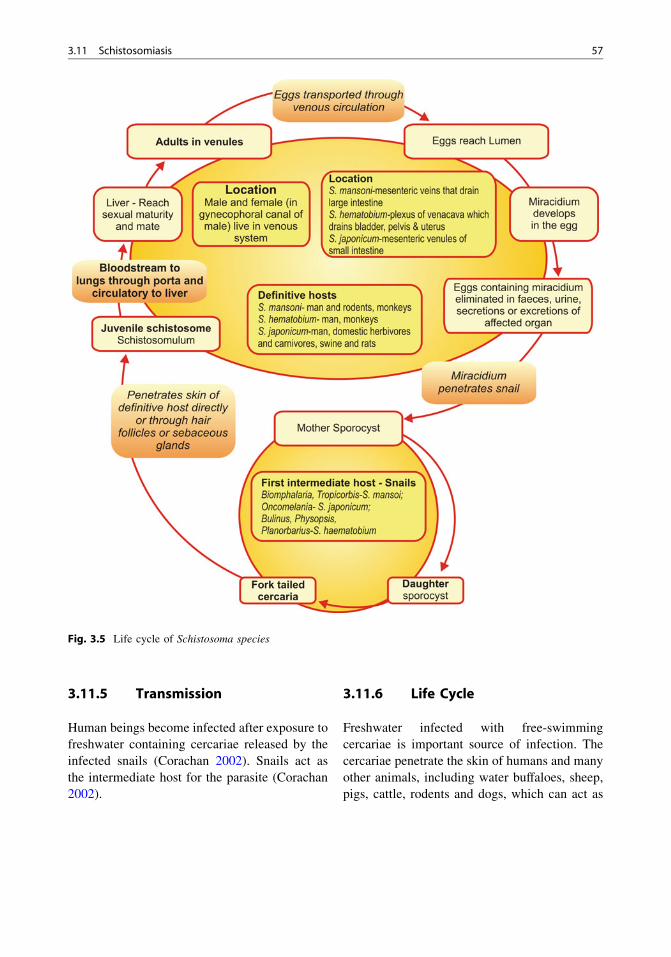
3.11.5 Transmission
Human beings become infected after exposure tofreshwater containing cercariae released by theinfected snails (Corachan 2002). Snails act asthe intermediate host for the parasite (Corachan2002).
3.11.6 Life Cycle
Freshwater infected with free-swimmingcercariae is important source of infection. Thecercariae penetrate the skin of humans and manyother animals, including water buffaloes, sheep,pigs, cattle, rodents and dogs, which can act as
Fig. 3.5 Life cycle of Schistosoma species
3.11 Schistosomiasis 57

important reservoirs for human infection (Rosset al. 2001; Zhou et al. 2007) (Fig. 3.5).
3.11.7 Clinical Signs in Man
The disease is generally asymptomatic in humanbeings. In infections due to S. japonicum,S. mansoni; early lesions occur in small intestinefollowed by portal hypertension due to Schisto-soma eggs retained in the portal spaces, ascitisand spleenomegaly. Clinical symptoms due toS. haematobium schistosomiasis include hae-maturia, proteinuria and leukocyturia accompa-nied by dysuria and nocturia (Corachan 2002).Chronic infections could lead to obstructiveuropathy and hydronephrosis (Corachan 2002).S. japonicum infection may lead to fever,headache and lethargy, portal hypertension,ascites and hepatosplenomegaly, which cancause premature death (Ross et al. 2002).
Rare CNS involvement due to embolization ofeggs to the brain and spinal cord may occur inS. japonicum and S. mansoni infections (Alfred1996). Early infection in childhood can causegrowth retardation and anaemia (Ross et al. 2002).
3.11.8 Clinical Signs in Animals
The disease is common in animals. The symp-toms generally are similar to as that in man.
3.11.9 Diagnosis
The disease can be diagnosed by detection of eggsin human stool samples, tissue biopsy examina-tions or ultrasonography (Corachan 2002), clini-cal signs, serologicalormolecular techniques. Theeggs of S. japonicum are round and have a shellwith reduced lateral spine (McManus et al. 2010).
3.11.10 Control
Control measures include health education,control of snails, water hygiene and treatment ofinfected cases.
References
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals. vol III (Para-sitosis), Pan American health Organisation, USA
Alfred BPL (1996) Schistosomiasis. In: Shakir RA,Newman PK, Poser CM (eds) Tropical neurology.WB Saunders, Philadelphia, pp 295–316
Almeda J, Corachan M, Sousa A (1994) Schistosomiasisin the Republic of Sao Tome and Principe: humanstudies. Trans R Soc Trop Med Hyg 88:406–409
Ashrafi K (2010) Human dicrocoeliasis in northern Iran:two case reports from Gilan province. Annals TropMed Parasitol 104:351–353
Ashrafi K, Valero MA, Massoud J, Sobhani A, Moham-madi SS, Conde P, Khoubbane M, Bargues MD, Mas-Coma S (2006) Plant-borne human contamination byfascioliasis. Am J Trop Med Hyg 75(2):295–302
Augustine DL, Weller TH (1949) Experimental studieson the specificity of skin tests for the diagnosis ofschistosomiasis. J Parasitol 35:461–466
Bandyopathy AK, Nandy A (1986) A preliminaryobservation on the prevalence of echinostomes in atribal community near Calcutta. Ann Trop MedParasitol 80:3016–3034
Bastert J, Sing A, Wollenberg A, Korting HC (1998)Aquarium dermatitis: cercarial dermatitis in anaquarist. Dermatology 197:84–86
Beaver PC, Jung RC, Cupp EW (1984) Clinical parasi-tology, 9th edn. Lea and Febiger, Philadelphia
Behr MA, Gyorkos TW, Kokoskin E, Ward BJ, MacLeanJD (1998) North American liver fluke (Metorchisconjunctus) in a Canadian aboriginal population: asubmerging human pathogen? Can J Public Health89:258–259
Belizario VY, Bersabe MJ, de Leon WU, Hilomen VY,Paller GV, de Guzman AD, Bugayon MG (2001)Intestinal heterophyidiasis: an emerging fish-borneparasitic zoonosis in southern Philippines. SoutheastAsian J Trop Med Public Health 32:36–42
Boray JC (1982) Fascioliasis. In: Hillyer GV, Hopla CE(eds) Handbook series in zoonoses, section C. Para-sitic zoonoses, vol 3. CRC Press, Boca Raton,pp 71–88
Brant SV, Cohen AN, James D, Hui L, Hom A, Loker ES(2010) Cercarial dermatitis transmitted by exoticmarine snail. Emerg Infect Dis 16(9):1357–1365
Brumpt E (1931) Cercaria ocellata déterminant ladermatite des nageurs, provient d’une bilharzie descanards. CR Acad Sci (Paris) 193:612–614
Bundy DA, Chandiwana SK, Homeida MM, Yoon S,Mott KE (1991) The epidemiological implications ofa multiple-infection approach to the control of humanhelminth infections. Trans Roy Soc Trop Med Hyg85:274–276
Cadel S (1996) Eighteen cases of human fascioliasis inBasse-Normandie, 1994–1995. Bulletin de la SocieÂte FrancË aise de Parasitologie 14:39–43 (in French)
58 3 Trematode Zoonoses

Carney WP (1991) Echinostomiasis—a snail-borne intes-tinal trematode zoonosis. Southeast Asian J Trop MedPublic Health 22:206–221
Cengiz ZT, Ylmaz H, Dulger AC, Cicek M (2010)Human infection with Dicrocoelium dendriticum inTurkey. Annals Saudi Med 30:159–161
Chai JY, Murell KD, Lymbery AJ (2005a) Fish-borneparasitic zoonoses: status and issues. Int J Parasitol35:1233–1254
Chai JY (1979) Study on Metagonimus yokogawai(Katsurada 1912) in Korea V. Intestinal pathologyin experimentally infected albino rats. Seoul J Med20:104–117
Chai JY, Cho SY, Seo BS (1977) Study on Metagonimusyokogawai (Katsurada 1912) in Korea. IV. An epide-miological investigation along Tamjin River Basin,SouthChollaDo. Korea. Korean JParasitol 15:115–120
Chai JY, Hong ST, Lee SH, Lee GC, Min YI (1994) Acase of echinostomiasis with ulcerative lesions in theduodenum. Korean J Parasitol 32:201–204
Chai JY, Huh S, Yu JR, Kook J, Jung KC, Park EC, SohnWM, Hong ST, Lee SH (1993) An epidemiologicalstudy of metagonimiasis along the upper reaches ofthe Namhan River. Korean J Parasitol 31:99–108
Chai JY, Lee SH (1990) Intestinal trematodes of humansin Korea: metagonimus, heterophyids and echinosto-mes. Korean J Parasitol 28:S103–S122
Chai JY, Lee SH (1991) Intestinal trematodes infectinghumans in Korea. Southeast Asian J Trop Med PublicHealth 22:163–170
Chai JY, Lee SH (2002) Food-borne intestinal trematodeinfections in the Republic of Korea. Parasitol Int51:129–154
Chai JY, Murell KD, Lymbery AJ (2005b) Fish-borneparasitic zoonoses: status and issues. Int J Parasitol35:1233–1254
Chai JY, Seo BS, Lee SH, Hong SJ, Sohn WM (1986)Human infections by Heterophyes heterophyes and H.dispar imported from Saudi Arabia. Korean J Paras-itol 24:82–88
Chai JY, Yang YT, Lee SH, Seo BS (1982) Thedetectability of helminth eggs from feces by cello-phane thick smear technique. Korean J Parasitol20:14–20
Chamot E, Toscani L, Rougemont A (1998) Public healthimportance and risk factors for cercarial dermatitisassociated with swimming in Lake Leman at Geneva,Switzerland (abstract). Epidemiology Infect120:305–314
Chattopadyay UK, Das MS, Pal D, Das S, Mukherjee A(1990) A case of echinostomiasis in a tribal commu-nity in Bengal. Ann Trop Med Parasitol 84:193
Chen MG, Lu Y, Hua X, Mott KE (1994) Progress inassessment of morbidity due to Clonorchis sinensisinfection: a review of recent literature. Trop Dis Bull91:R7–R65
Chen MG, Mott KE (1990) Progress in assessment ofmorbidity due to Fasciola hepatica infection: areview of recent literature. Trop Dis Bull 87(4):R1–R38
Choi MH, Park IC, Li S, Hong ST (2003) Excretory-secretory antigen is better than crude antigen for theserodiagnosis of clonorchiasis by ELISA. Korean JParasitol 41:35–39
Christensen RO, Green WP (1928) Studies on biologicaland medical aspects of ‘swimmeritch’. Schistosomedermatitis in Minnesota. Minnesota Med 11:573–575
Corachan (2002) Schistosomiasis and internationaltravel. Clin Infect Dis 35:446–450
De Gentile L, Picot H, Bourdeau P, Bardet R, Kerjan A,Piriou M, Le Guennic A, Bayssade-Dufour C, Cha-basse D, Mott KE (1996) Cercarial dermatitis inEurope: a new public health problem? Bull WorldHealth Organ 74:159–163
Drabick JJ, Egan JE, Brown SL, Vick RG, Sandman BM,Neafie RC (1988) Dicrocoeliasis (lancet fluke dis-ease) in an HIV seropositive man. J Am Med Assoc259:567–568
Eastburn RL, Tritsche TR, Terhune CA Jr (1987) Humanintestinal infection with Nanophyetus salmincolafrom salmonid fishes. Am J Trop Med Hyg36:586–591
El-Shafie AM, Fouad MA, Khalil MF, Morsy TA (2011)Zoonotic Dicrocoeliasis dendriticum in a farmer’sfamily at Giza Governorate, Egypt. J Egypt SocParasitol. 41(2):327–336
Esteban JG, Bargues MD, Mas-Coma S (1998) Geograph-ical distribution, diagnosis and treatment of humanfascioliasis: a review. Res Rev Parasitol 58:13–48
Farahnak A, Essalat M (2003) A study on cercarialdermatitis in Khuzestan province, south western Iran.BMC Public Health 3:35
Faust EC, Nishigori M (1926) The life cycles of two newspecies of Heterophyidae parasitic in mammals andbirds. J Parasitol 13:91–131
Fenwick A, Webster JP, Bosque-Oliva E, Blair L,Fleming FM, Zhang Y, Garba A, Stothard JR,Gabrielli AF, Clements AC, Kabatereine NB, ToureS, Dembele R, Nyandindi U, Mwansa J, KoukounariA (2009) The Schistosomiasis Control Initiative(SCI): rationale, development and implementationfrom 2002–2008. Parasitol 136:1719–1730
Ferrel KR, Soave OA, Johnston SD (1974) Nanophetussalmincola infections in kippered salmon. PublicHealth Briefs 64(8):808–809
Finkelstein JL, Schleinitz MD, Carabin H, McGarvey ST(2008) Decision-model estimation of the age-specificdisability weight for schistosomiasis japonica: asystematic review of the literature. PLoS Negl TropDis 2:e158
Flavell DJ (1981) Liver fluke infection as an aetiologicalfactor in bile duct carcinoma of man. Trans Roy SocTrap Med Hyg 75:815–823
Folster-Holst R, Disko R, Rowert J, Bockeler W,Kreiselmaier I, Christophers E (2001) Cercarialdermatitis contracted via contact with an aquarium:case report and review. Br J Dermatol 145:638–640
Fried B, Graczyk TK, Tamang L (2004) Food-borneintestinal trematodiases in humans. Parasitol Res93:159–170
References 59

Gilman RH, Mondal G, Maksud M, Alam K, RutherfordE, Gilman JB (1982) Endemic focus of Fasciolopsisbuski infection in Bangladesh. Am J Trop Med Hyg31:796–802
Goldsmid JM (1975) Ecological and cultural aspects ofhuman trematodiasis excluding schistosomiasis inAfrica. Cent Afr J Med 21:49–53
Graczyk TK, Gilman RH, Fried B (2001) Fasciolopsiasis:is it a controllable food borne disease? Parasitol Res87:80–83
Graczyk TK (1997) Trematode immunobiology in thevertebrate host. In: Fried B, Graczyk TK (eds)Advances in trematode biology. ICR Press, BocaRaton, pp 383–404
Graczyk TK, Alam K, Gilman RH, Mondal G, Ali S(2000) Development of Fasciolopsis buski (Trema-toda; Fasciolidae) in Hippeutis umbilicalis and Seg-mentina trochoideus (Gastropoda: Pulmonata).Parasitol Res 86:324–326
Graczyk TK, Fried B (1994) ELISA method for detectinganti- Echinostoma caproni (Trematoda: Echinostom-atidae) antibodies in experimentally infected ICRmice. J Parasitol 80:544–549
Graczyk TK, Fried B (1995) An ELISA for detectinganti-Echinostoma trivolvis (Trematoda) immunoglob-ulins in experimentally infected ICR mice: cross-reactivity with Echinostoma caproni. Parasitol Res81:710–712
Graczyk TK, Fried B (1998) Echinostomiasis: a commonbut forgotten food-borne disease. Am J Trop MedHyg 58:501–504
Gray DJ, Williams GM, Li Y, McManus DP (2008)Transmission Dynamics of Schistosoma japonicum inthe Lakes and Marshlands of China. PLoS ONE3(12):e4058. doi:10.1371/journal.pone.0004058
Gualdieri L, Rinaldi L, Petrullo L, Morgoglione ME,Maurelli MP, Musella V, Piemonte M, Caravano L,Coppola MG, Cringoli G (2011) Intestinal parasites inimmigrants in the city of Naples (southern Italy). ActaTrop 117:196–201
Guan XH (2005) Paragonimiasis. In: Li YL, Guan XH(eds) Human Parasitology. People’s Public HealthPress, pp 109–113
Haas W, van de Roemer A (1998) Invasion of thevertebrate skin by cercariae of Trichobilharzia ocel-lata: penetration processes and stimulating hostsignals. Parasitol Res 84:787–795
Haridy FM, Morsy TA, Ibrahim BB, Abdel-Aziz A(2003) A preliminary study on dicrocoeliasis inEgypt, with a general review. J Egyptian SocParasitol 33:85–96
Haseeb MA, Eveland LK (2002) Human echinostomasis:mechanisms of pathogenesis and host resistance. In:Fried B, Graczyk TK (eds) Echinostomes as modelsfor biological research. Kluwer, Dordrecht, pp 83–98
Helmy MM, Al-Mathal EM (2003) Human infection withDicrocoelium dendriticum in Riyadh district (SaudiArabia). J Egypt Soc Parasitol 33(1):139–144
Herber EC (1938) Schistosome dermatitis in dog.J Parasitol 24:474–475
Hira PR (1983) Further spurious parasitic infestations ofman in Zambia. Cent Afr J Med 29:33–40
Hoeffler DF (1977) Swimmer’s itch (cercarial dermati-tis). Cutis 19:461–467
Hong ST (2003) Clonorchis sinensis. In: Miliotis MD,Bier JW (eds) International Handbook of FoodbornePathogens. Marcel Dekker, Inc., New York, Basel,pp 581–592
Hong ST, Choi MH, Kim CH, Chung BS, Li Z (2003)The Kato-Katz method is reliable for diagnosis ofClonorchis sinensis infection. Diagn Microbiol InfectDis 47:345–347
Horák P, Kolárová L, Adema CM (2002) Biology of theschistosome genus Trichobilharzia. Adv Parasitol52:155–232
Hotez PJ, Bottazzi ME, Franco-Paredes C, Ault SK,Periago MR (2008) The neglected tropical diseases oflatin america and the caribbean: a review of diseaseburden and distribution and a roadmap for control andelimination. PLoS Neglected Trop Dis 2:e300
Hotez PJ, Fenwick A (2009) Schistosomiasis in Africa:an emerging tragedy in our new global health decade.PLoS Neglected Trop Dis 3:e485
Huang AQ (2000) Clinical analysis of cerebral paragon-imiasis. Chin J Zoonoses 16:115–116
Huffman JE, Fried B (1990) Echinostoma and echino-stomiasis. Adv Parasitol 29:215–269
Ito J, Mochizuki H, Ohno Y, Ishiguro M (1991) On theprevalence of Metagonimus sp. among the imhabit-ants at Hamamatsu basin in Shizuoka Prefecture.Japan. Jpn J Parasitol 40:274–278 (in Japanese)
Jeandron A, Rinaldi L, Abdyldaieva G, Usubalieva J,Steinmann P, CringoliI G, Utzinger J (2011) Humaninfections with Dicrocoelium dendriticum in Kyrgyz-stan: the tip of the iceberg? J Parasitol97(6):1170–1172
Jia TW, Zhou XN, Wang XH, Utzinger J, Steinmann P,Wu XH (2007) Assessment of the age-specificdisability weight of chronic schistosomiasis japonica.Bull World Health Organ 85:458–465
Johansen MV, Bøgh HO, Nansen P, Christensen NO(2000) Schistosoma japonicum infection in the pig asa model for human schistosomiasis japonica. ActaTrop 76:85–99
Kaewkes S (2003) Taxonomy and biology of liver flukes.Acta Trop 88:177–186
Kagei N, Hayashi S, Kato K (1980) On the heterophyidtrematode (Heterophyes heterophyes) infection casesimported from Egypt to Japan. Jpn J Trop Med Hyg8:1–7 (in Japanese)
King CH, Dickman K, Tisch DJ (2005) Reassessment ofthe cost of chronic helminthic infection: a meta-analysis of disability-related outcomes in endemicschistosomiasis. Lancet 365:1561–1569
Kolarova L (2007) Schistosomes causing cercarial der-matitis: a mini-review of current trends in systematics
60 3 Trematode Zoonoses

and of host specificity and pathogenicity. FoliaParasitol 54:81–87
Kolarova L, Skirnisson K, Horak P (1999) Schistosomecercariae as the causative agent of swimmer’s itch inIceland. J Helminthol 73:215–220
Kourilova P, Hogg KG, Kolarova L, Mountford AP(2004) Cercarial dermatitis caused by bird schisto-somes comprises both immediate and late phasecutaneous hypersensitivity reaction. J Immunol172:3766–3774
Kullallavanijaya P, Wongwaisayawan H (1993) Outbreakof cercarial dermatitis in Thailand. Int J Dermatol32:113–115
Kumar V (1999) Trematode infections and diseases ofman and animals. Kluwer, Dordrecht
Kuntz RE, Lo CT (1967) Preliminary studies on Fasci-olopsis buski (Lankester, 1857) (giant Asian intestinalfluke) in the United States. Trans Amer Microsc Soc86:163–166
Le Bailly M, Bouchet F (2010) Ancient dicrocoeliosis:occurrence, distribution and migration. Acta Trop115:175–180
Le TH, Nguyen VD, Phan BU, Blair D, McManus DP(2004) Case report: unusual presentation of Fascio-lopsis buski in a Vietnamese child. Trans R Soc TropMed Hyg 98:193–194
Lee SU, Huh S, Sohn WM, Chai JY (2004) Sequencecomparisons of 28S ribosomal DNA and mitochon-drial cytochrome c oxidase I of Metagonimus yokog-awai, M. takahashii and M. miyatai. Korean JParasitol 42:129–135
Levesque B, Giovenazzo P, Guerrier P, Laverdiere D,Prud’Homme H (2002) Investigation of an outbreakof cercarial dermatitis. Epidemiol Infect 129:379–386
Li C, Ma C, Gu J, Lu W (1998) An epidemiologicalsurvey of schistosome cercarial dermatitis among theresidents living along the banks of the Huaihe Riversystem. Zhongguo Ji Sheng Chong Xue Yu Ji ShengChong Bing Za Zhi 16:384–387
Lindblade KA (1998) The epidemiology of cercarialdermatitis and its association with limnologicalcharacteristics of a northern Michigan lake. J Parasitol1998(84):19–23
Liu Q, Wei F, Liu W, Yang S, Zhang X (2008)Paragonimiasis: an important food-borne zoonosis inChina. Trends Parasitol 24(7):318–323
Lo CT, Lee KM (1996) Intestinal parasites among theSoutheast Asian laborers in Taiwan during1993–1994. Zhonghua Yi Xue Za Zhi (Taipei)57:401–404
Loy C, Haas W (2001) Prevalence of cercariae fromLymnaea stagnalis snails in a pond system inSouthern Germaney. Parasitol Res 87:878–882
MacLean JD, Arthur JR, Ward BJ, Gyorkos TW, CurtisMA, Kokoskin E (1996) Common-source outbreak ofacute infection due to the North American liver flukeMetorchis conjunctus. Lancet 347:154–158
Malek EA (1980) Snail-transmitted parasitic diseases.vols 1 and 2. CRC Press, Boca Raton, 1–334
Mas-Coma S, Bargues MD, Valero MA (2005a) Fasci-oliasis and other plant-borne trematode zoonoses. IntJ Parasitol 35:1255–1278
Mas-Coma S, Bargues MD, Esteban JG (1999a) HumanFasciolosis. In: Dalton JP (ed) Fasciolosis. CABInternational Publishing, Wallingford, Oxon,pp 411–434
Mas-Coma S, Bargues MD, Esteban JG (2004) Humanfasciolosis. In: Cotruvo JA, Dufour A, Rees G,Bartram J, Carr R, Cliver DO, Craun GF, Fayer R,Gannon VPJ (eds) Waterborne zoonoses: identifica-tion, causes and control. World Health Organizationand IWA Publishing, London, pp 305–322
Mas-Coma S, Bargues MD, Valero MA (2005b) Fasci-oliasis and other plantborne trematode zoonoses. Int JParasitol 35:1255–1278
Mas-Coma S, Esteban JG, Bargues MD (1999b) Epide-miology of human fascioliasis: a review and proposednew classification. Bull WHO 77:340–346
Matheson S (1930) Notes on Cercaria elvae Miller as theprobable cause of an outbreak of dermatitis in Cardiff.Trans R Soc Trop Med Hyg 23:421
McManus DP, Gray DJ, Li Y, Feng Z, Williams GM,Stewart D, ReyLadino J, Ross AG (2010) Schistoso-miasis in the People’s Republic of China: the era ofthe Three Gorges Dam. Clin Microbiol Rev23:442–466
McManus DP, Li Y, Gray DJ, Ross AG (2009)Conquering ‘snail fever’: schistosomiasis and itscontrol in China. Expert Rev. Anti-Infect Ther7:473–485
Millemann RE, Knapp SE (1970) Biology of Nanophy-etus salmincola and ‘salmon poisoning’ disease. AdvParasitol 8:1–41
Mulvihill CA, Burnett JW (1990) Swimmer’s itch:a cercarial dermatitis. Cutis 46:211–213
Murty CV, Reddy CR (1980) A case report of Gastro-discoides hominis infestation. Indian J Pathol Micro-biol 23:303–304
Obara A (2004) Paragonimiasis cases recently foundamong immigrants in Japan. Intern Med 43:388–392
Oda T (1973) Schistosome dermatitis in Japan. ProgrMed Parasitol 2:5–53
Olivier L (1953) Observations on the migration of avianschistosomes in mammals previously unexposed tocercariae. J Parasitol 39:237–243
Park JH, Guk SM, Kim TY, Shin EH, Lin A, Park JY,Kim JL, Hong ST, Chai JY (2004) Clonorchissinensis metacercarial infection in the pond smeltHypomesus olidus and the minnow Zacco platypuscollected from the Soyang and Daechung Lakes.Korean J Parasitol 42:41–44
Radomyos P, Radomyos B, Tungtrongchitr A (1994)Multi-infection with helminths in adults from north-east Thailand as determined by posttreatment fecal
References 61

examination of adult worms. Trop Med Parasitol45:133–135
Rana SS, Bhasin DK, Nanda M, Singh K (2007) Parasiticinfestations of the biliary tract. Current GastroenterolReports 9:156–164
Rim HJ (1982a) Fasciolopsiasis. In: Hillyer GV, HoplaCE (eds) Handbook Series in Zoonoses. Section C.Parasitic Zoonoses, vol 3. CRC Press, Boca Raton,pp 89–97
Rim HJ (1982b) Clonorchiasis. In: Steele JH (ed) CRChandbook series in zoonoses, Section C: parasiticzoonoses (Trematode Zoonoses), vol III. CRC Press,Boca Raton, pp 17–32
Rim HJ (1982c) Opisthorchiasis. In: Steele JH (ed) CRChandbook series in zoonoses, Section C: parasiticzoonoses (Trematode Zoonoses), vol III. CRC Press,Boca Raton, pp 109–121
Rim HJ (1986) Current pathobiology and chemotherapyof clonorchiasis. Korean J Parasitol 24:1–141
Rim HJ (1990) Clonorchiasis in Korea. Korean JParasitol 28:63–78
Rim HJ (1994) Food-borne trematodes: ignored oremerging? Parasitol Today 10:207–209
Roberts JA, Suhardono (1996) Approaches to the controlof fasciolosis in ruminants. Int J Parasitol 26:971–981
Ross AGP, Bartley PB, Sleigh AC, Olds RG, Li Y (2002)Schistosomiasis. N Eng J Med 346:1212–1219
Ross AGP, Sleigh AC, Li Y, Davis GM, Williams GW(2001) Schistosomiasis in the People’s Republic ofChina: prospects and challenges for the 21st century.Clin Microbiol Rev 14:270–295
Saito S, Chai JY, Kim KH, Lee SH, Rim HJ (1997)Metagonimus miyatai sp. nov. (Digenea: Heterophy-idae), a new intestinal trematode transmitted byfreshwater fishes in Japan and Korea. Korean JParasitol 35:223–232
Samalia MO, Shehu SM, Abubaker N, Mohammed U,Jabo B (2009) Human dicrocoeliasis presenting as asubcutaneous mass. BMJ Case Reports. doi:10.1136/bcr.02.2009.1622
Schell SC (1985) Trematodes of North America, north ofMexico. University Press Idaho, Moscow
Schweiger F, Kuhn M (2008) Dicrocoelium dendriticuminfection in a patient with Crohn’s disease. Can JGastroenterol 22:571–573
Scrimgeour EM, Daar AS (2000) Schistosomiasis: clin-ical relevance to surgeons in Australasia and diag-nostic update. Aust N Z J Surg 70:157–161
Seo BS, Lee SH, Cho SY, Chai JY, Hong ST, Han IS,Shon JS, Cho BH, Ahn SR, Lee SK, Chung SC, KangKS, Shim HS, Hwang IS (1981) An epidemiologicstudy on clonorchiasis and metagonimiasis in river-side areas in Korea. Korean J Parasitol 19:137–150
Shekhar KC, Nazarina M, Lee SH, Pathmanathan R(1995) Clonorchiasis/Opisthorchiasis in Malaysians,case reports and review. Med J Malaysia50(2):182–186
Singh A, Tybus K, Fackler I (2008) Acute urticariaassociated with Dicrocoelium dendriticum infestation.Indian J Med Microbiol 26:97–98
Singh TD (1986) Pulmonary paragonimiasis: clinicalfeatures, diagnosis and treatment of 39 cases inManipur. Trans R Soc Trop Med Hyg 80:967–971
Spithill TW, Smooker PM, Copeman DB (1999) Fasci-ola gigantica: epidemiology, control, immunologyand molecular biology. In: Dalton JP (ed) Fasciolosis.CAB International Publishing, UK, pp 465–525
Standley CJ, Adriko M, Alinaitwe M, Kazibwe F,Kabatereine NB, Stothard JR (2009) Intestinal schis-tosomiasis and soil-transmitted helminthiasis inUgandan School children: a rapid mapping assess-ment. Geospatial Health 4:39–53
Standley CJ, Dobson AP, Stothard JR (2012) Out ofanimals and back again: schistosomiasis as a zoonosisin Africa, Schistosomiasis, Prof. Mohammad BagherRokni (ed), ISBN: 978-953-307-852-6, InTech, Chap-ter 11, pp 219–230
Strickland GT (1991) Hunter’s Tropical medicine, 7thedn. Saunders, Philadelphia
Sukontason KL, Sukontason K, Piangjai S, Pungpak S,Radomyos P (2001) Prevalence of Opisthorchisviverrini infection among villagers harboring Opis-thorchis-like eggs. Souteast Asian J Trop Med PublicHealth 32:23–26
Torgerson P, Claxton J (1999) Epidemiology and control.In: Dalton JP (ed) Fasciolosis. CAB InternationalPublishing, UK, pp 113–149
Ujiie N (1963) On the structure and development ofEchinochasmus japonicus and its parasitism in man.J Med Assoc Formosa 35:525–546
Utzinger J, Zhou XN, Chen MG, Bergquist R (2005)Conquering schistosomiasis in China: the longMarch. Acta Trop 96:69–96
Van der Werf MJ, de Vlas SJ, Brooker S, Looman CW,Nagelkerke NJ, Habbema JD, Engels D (2003)Quantification of clinical morbidity associated withschistosome infection in sub-Saharan Africa. ActaTrop 86:125–139
Velasquez CC (1982) Heterophyidiasis. In: Steele JH(ed) CRC handbook series in zoonoses, Section C:parasitic zoonoses (trematode zoonoses), vol III. CRCPress, Boca Raton, pp 99–107
Velez I (2003) Morphological description and life cycleof Paragonimus spp. (Trematoda: Troglotrematidae):causal agent of human paragonimiasis in Colombia.J Parasitol 89:749–755
Verbrugge LM, Rainey JJ, Reimink RL, Blankespoor HO(2004) Swimmer’s itch: incidence and risk factors.Am J Public Health 94:738–741
Waikagul J (1991) Intestinal fluke infections in SoutheastAsia. Southeast Asia J Trop Med Public Health22:158–162
Waikagul J (1989) Paragonimus siamensis: subcutaneousinfection with excysted metacercariae. Med Lab Sci6:370–371
Wang CH, Chang CH (2008) Cercarial Dermatitis. TzuChi Med J 20(1):63–66
Wang T, Zhang S, Wu W, Zhang G, Lu D, Ornbjerg N,Johansen MV (2006) Treatment and reinfection ofwater buffaloes and cattle infected with Schistosoma
62 3 Trematode Zoonoses

japonicum in Yangtze River valley, Anhui Province,China. J Parasitol 92:1088–1091
Weng YL, Zhuang ZL, Jiang HP, Lin GR, Lin JJ (1989)Studies on ecology of Fasciolopsis buski and controlstrategy of fasciolopsiasis. Chin J Parasitol Parasit Dis7:108–111
WHO (1993) The control of schistosomiasis. Secondreport of the WHO Expert Committee. World HealthOrgan. Tech Rep Ser 830:1–86
WHO (1995a) Control of foodborne trematode infections.WHO Tech Rep Ser No. 849, pp 1–157
WHO (1995b) Control of foodborne trematode infec-tions. Report of a WHO Expert Committee. Geneva,World Health Organization 1995 (WHO TechnicalReport Series, No. 849)
WHO (1995c) Control of foodborne trematode infections.WHO Tech Rep Ser 849:1–157
Wiwanitkit V, Suwansaksri J, Chaiyakhun Y (2002) Highprevalence of Fasciolopsis buski in an endemic areaof liver fluke infection in Thailand. Med Gen Med 4:6
Yamaguti S (1958) Part I. The digenetic trematodes ofvertebrates, Systema helminthum, vol I. IntersciencePublishers Inc, New York
Yamashita J (1964) Echinostome. Prog Med ParasitolJapan 1:287–313
Yoshida Y (2012) Clonorchiasis—A historical review ofcontributions of Japanese parasitologists. Parasitol Int61:5–9
Yu S, Hu L, Jiang Z (1994) Report of the first nationwidesurvey of the distribution of human parasites inChina. Regional distribution of parasite species. ChinJ Parasitol Parasit Dis 12:241–247
Yu SH, Mott KE (1994) Epidemiology and morbidity offood-borne intestinal trematode infections. Trop DisBull 91:R125–R152
Zali MR, Mehr AJ, Rezaian M, Meamar AR, Vaziri S,Mohraz M (2004) Prevalence of intestinal parasiticpathogens among HIV-positive individuals in Iran.Japanese J Infect Dis 57:268–270
Zhou XN, Guo J, Wu XH, Jiang QW, Zheng J, Dang H,Wang XH, Xu J, Zhu HQ, Wu GL, Li YS, Xu XJ,Chen HG, Wang TP, Zhu YC, Qiu DC, Dong XQ,Zhao GM, Zhang SJ, Zhao NQ, Xia G, Wang LY,Zhang SQ, Lin DD, Chen MG, Hao Y (2007)Epidemiology of schistosomiasis in the Peoples’Republic of China, 2004. Emerg Infect Dis13:1470–1476
Zhou XN, Wang LY, Chen MG, Wu XH, Jiang QW,Chen XY, Zheng J, Utzinger J (2005) The publichealth significance and control of schistosomiasis inChina—then and now. Acta Trop 96:97–105
References 63

4Cestode Zoonoses
Abstract
Cestode Zoonoses could be defined as ‘‘those cestode diseases which arenaturally transmitted between (other) vertebrate animals and man.’’ Thezoonotic cestodes belonging to family Taeniidae are of paramountimportance in the developing world. Most of the food producing animalsviz. cattle, buffalo, sheep, goat and pigs along with some other mammalsact as intermediate hosts for Echinococcus granulosus. Human beingscould become infected after accidental consumption of Echinococcusspecies eggs shed in the faeces of the definitive carnivorous host/animal.Taeniasis is a true zoonotic infection (Euzoonoses) where pig and cattleact as intermediate host for Taenia solium and Taenia saginata,respectively and human beings act as definitive/final hosts. Neurocystic-ercosis is an important public health issue and is responsible forneurological disorders worldwide. Besides important animal and humanhealth concern; the economic losses arising due to these infections areenormous. Coenurosis is a rare zoonosis and more than 100 human caseshave been reported across the globe. Other important cestodes includeparasites such as Diphyllobothrium latum and Spirometra mansoni.Different epidemiological trends have been reported across the globe fordiphyllobothriasis. The parasite Dipylidium caninum can cause disease indomestic dogs, cats, some wild carnivores and occasionally man.Sparganosis is a rare cestode zoonosis that can infect man. The parasitehas been recorded across the globe but is commonly found in easternAsia. The important cestodes transmitted through food and waterincludes T. solium, E. granulosus and D. latum.
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_4, � Springer India 2013
65
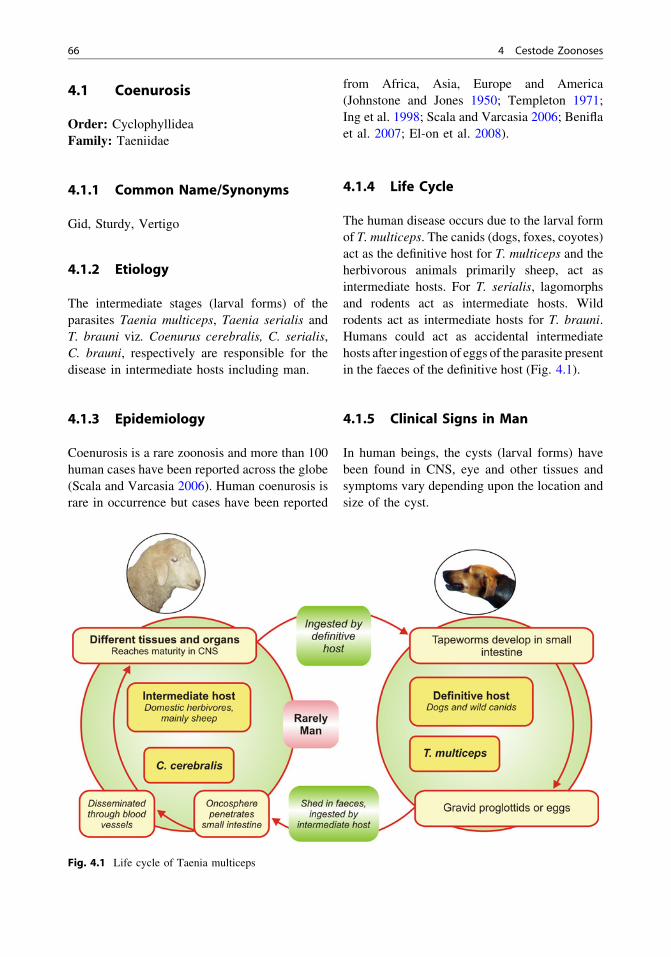
4.1 Coenurosis
Order: CyclophyllideaFamily: Taeniidae
4.1.1 Common Name/Synonyms
Gid, Sturdy, Vertigo
4.1.2 Etiology
The intermediate stages (larval forms) of theparasites Taenia multiceps, Taenia serialis andT. brauni viz. Coenurus cerebralis, C. serialis,C. brauni, respectively are responsible for thedisease in intermediate hosts including man.
4.1.3 Epidemiology
Coenurosis is a rare zoonosis and more than 100human cases have been reported across the globe(Scala and Varcasia 2006). Human coenurosis israre in occurrence but cases have been reported
from Africa, Asia, Europe and America(Johnstone and Jones 1950; Templeton 1971;Ing et al. 1998; Scala and Varcasia 2006; Beniflaet al. 2007; El-on et al. 2008).
4.1.4 Life Cycle
The human disease occurs due to the larval formof T. multiceps. The canids (dogs, foxes, coyotes)act as the definitive host for T. multiceps and theherbivorous animals primarily sheep, act asintermediate hosts. For T. serialis, lagomorphsand rodents act as intermediate hosts. Wildrodents act as intermediate hosts for T. brauni.Humans could act as accidental intermediatehosts after ingestion of eggs of the parasite presentin the faeces of the definitive host (Fig. 4.1).
4.1.5 Clinical Signs in Man
In human beings, the cysts (larval forms) havebeen found in CNS, eye and other tissues andsymptoms vary depending upon the location andsize of the cyst.
Fig. 4.1 Life cycle of Taenia multiceps
66 4 Cestode Zoonoses
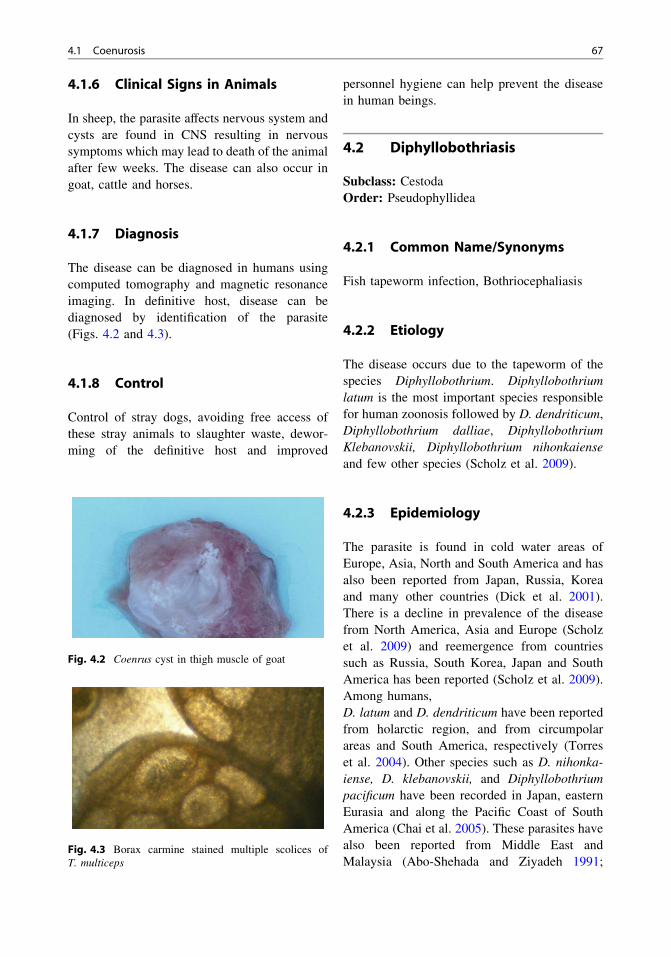
4.1.6 Clinical Signs in Animals
In sheep, the parasite affects nervous system andcysts are found in CNS resulting in nervoussymptoms which may lead to death of the animalafter few weeks. The disease can also occur ingoat, cattle and horses.
4.1.7 Diagnosis
The disease can be diagnosed in humans usingcomputed tomography and magnetic resonanceimaging. In definitive host, disease can bediagnosed by identification of the parasite(Figs. 4.2 and 4.3).
4.1.8 Control
Control of stray dogs, avoiding free access ofthese stray animals to slaughter waste, dewor-ming of the definitive host and improved
personnel hygiene can help prevent the diseasein human beings.
4.2 Diphyllobothriasis
Subclass: CestodaOrder: Pseudophyllidea
4.2.1 Common Name/Synonyms
Fish tapeworm infection, Bothriocephaliasis
4.2.2 Etiology
The disease occurs due to the tapeworm of thespecies Diphyllobothrium. Diphyllobothriumlatum is the most important species responsiblefor human zoonosis followed by D. dendriticum,Diphyllobothrium dalliae, DiphyllobothriumKlebanovskii, Diphyllobothrium nihonkaienseand few other species (Scholz et al. 2009).
4.2.3 Epidemiology
The parasite is found in cold water areas ofEurope, Asia, North and South America and hasalso been reported from Japan, Russia, Koreaand many other countries (Dick et al. 2001).There is a decline in prevalence of the diseasefrom North America, Asia and Europe (Scholzet al. 2009) and reemergence from countriessuch as Russia, South Korea, Japan and SouthAmerica has been reported (Scholz et al. 2009).Among humans,D. latum and D. dendriticum have been reportedfrom holarctic region, and from circumpolarareas and South America, respectively (Torreset al. 2004). Other species such as D. nihonka-iense, D. klebanovskii, and Diphyllobothriumpacificum have been recorded in Japan, easternEurasia and along the Pacific Coast of SouthAmerica (Chai et al. 2005). These parasites havealso been reported from Middle East andMalaysia (Abo-Shehada and Ziyadeh 1991;
Fig. 4.2 Coenrus cyst in thigh muscle of goat
Fig. 4.3 Borax carmine stained multiple scolices ofT. multiceps
4.1 Coenurosis 67
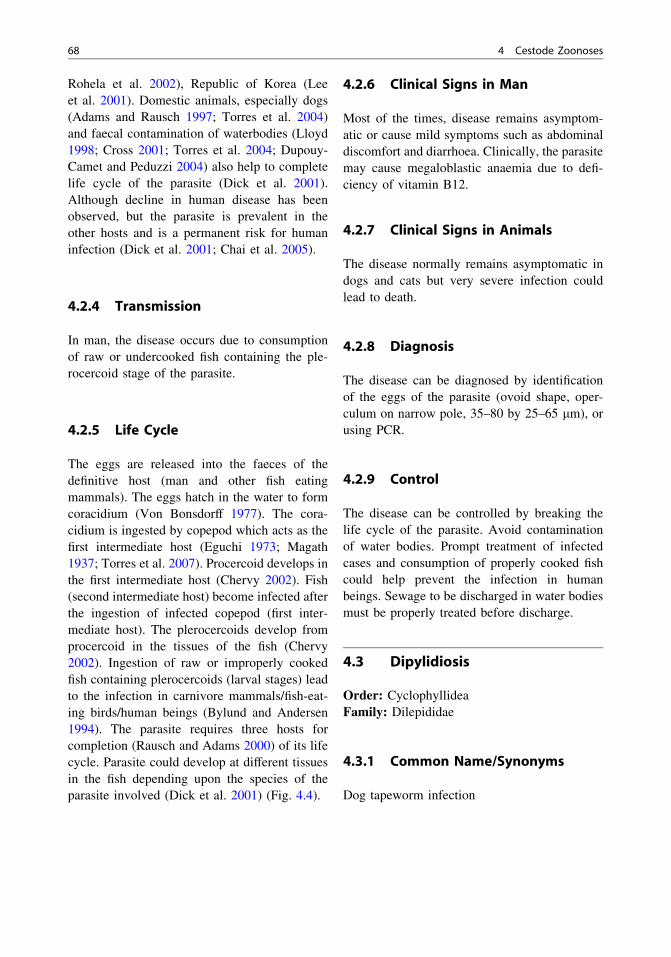
Rohela et al. 2002), Republic of Korea (Leeet al. 2001). Domestic animals, especially dogs(Adams and Rausch 1997; Torres et al. 2004)and faecal contamination of waterbodies (Lloyd1998; Cross 2001; Torres et al. 2004; Dupouy-Camet and Peduzzi 2004) also help to completelife cycle of the parasite (Dick et al. 2001).Although decline in human disease has beenobserved, but the parasite is prevalent in theother hosts and is a permanent risk for humaninfection (Dick et al. 2001; Chai et al. 2005).
4.2.4 Transmission
In man, the disease occurs due to consumptionof raw or undercooked fish containing the ple-rocercoid stage of the parasite.
4.2.5 Life Cycle
The eggs are released into the faeces of thedefinitive host (man and other fish eatingmammals). The eggs hatch in the water to formcoracidium (Von Bonsdorff 1977). The cora-cidium is ingested by copepod which acts as thefirst intermediate host (Eguchi 1973; Magath1937; Torres et al. 2007). Procercoid develops inthe first intermediate host (Chervy 2002). Fish(second intermediate host) become infected afterthe ingestion of infected copepod (first inter-mediate host). The plerocercoids develop fromprocercoid in the tissues of the fish (Chervy2002). Ingestion of raw or improperly cookedfish containing plerocercoids (larval stages) leadto the infection in carnivore mammals/fish-eat-ing birds/human beings (Bylund and Andersen1994). The parasite requires three hosts forcompletion (Rausch and Adams 2000) of its lifecycle. Parasite could develop at different tissuesin the fish depending upon the species of theparasite involved (Dick et al. 2001) (Fig. 4.4).
4.2.6 Clinical Signs in Man
Most of the times, disease remains asymptom-atic or cause mild symptoms such as abdominaldiscomfort and diarrhoea. Clinically, the parasitemay cause megaloblastic anaemia due to defi-ciency of vitamin B12.
4.2.7 Clinical Signs in Animals
The disease normally remains asymptomatic indogs and cats but very severe infection couldlead to death.
4.2.8 Diagnosis
The disease can be diagnosed by identificationof the eggs of the parasite (ovoid shape, oper-culum on narrow pole, 35–80 by 25–65 lm), orusing PCR.
4.2.9 Control
The disease can be controlled by breaking thelife cycle of the parasite. Avoid contaminationof water bodies. Prompt treatment of infectedcases and consumption of properly cooked fishcould help prevent the infection in humanbeings. Sewage to be discharged in water bodiesmust be properly treated before discharge.
4.3 Dipylidiosis
Order: CyclophyllideaFamily: Dilepididae
4.3.1 Common Name/Synonyms
Dog tapeworm infection
68 4 Cestode Zoonoses

4.3.2 Etiology
The disease occurs due to Dipylidium caninum(cyclophyllidean cestode). The parasite D.caninum (Linnaeus 1758, Cyclophyllidea,Dipylidiidae) can cause disease in domesticdogs, cats, some wild carnivores, and occasion-ally human beings (Schmidt and Roberts 2000).
4.3.3 Epidemiology
The disease occurs across the globe and humancases have been reported in many Europeancountries, India, China, Japan, etc. The humaninfection mostly occurs in young children asthey often play with dogs and cats (Marx 1991).
Fig. 4.4 Life cycle of Diphyllobothrium latum
4.3 Dipylidiosis 69

4.3.4 Life Cycle and Transmissionin Man
Intermediate hosts include cat and dog(Ctenocephalides felis and Ctenocephalidescanis) flea but dog lice (Trichodectes canis andHeterodoxus spiniger) and human flea (Pulexirritans) can also transmit the parasite (Craigand Ito 2007; Chappell and Penn 1990).Definitive hosts (dogs and cats) become infec-ted after ingestion of the flea and lice infectedwith cysticercoids (Robertson and Thompson2002). Accidental infection occurs in humanbeings after ingestion of the infected cat anddog flea or food contaminated with infectedflea (Turner 1962). The intermediate hostsbecome infected after ingesting contaminatedanimal faeces (Fig. 4.5).
4.3.5 Clinical Signs in Man
The disease has been reported from infants andyoung children (Tsumura et al. 2007; Reddy1982; Claudia et al. 2003; Reid et al. 1992). Inhuman beings, the disease is rarely seen and
often remains asymptomatic but symptoms suchas abdominal pain, diarrhoea and increasedirritability of anus and intestinal obstruction maybe seen. Proglottids (rice grain like) are excretedin the faeces of the host.
4.3.6 Clinical Signs in Animals
The infection generally remains asymptomaticin dogs, but few typical signs such as crawlingand rubbing around the anus could result due toperianal pruritus (Dantas-Torres 2008). Pro-glottids (rice grain like) can also be seen aroundperianal area (Dantas-Torres 2008).
4.3.7 Diagnosis
The disease can be diagnosed after microscopicidentification of parasite eggs or observing ricegrain-like proglottids in faeces. The gravid pro-glottids contain eggs packed in embryonicmembrane. The eggs are 20–40 lm in diameterand contain a hexacanth embryo (Neira et al.2008; Ramana et al. 2011).
Fig. 4.5 Life cycle of Dipylidium caninum
70 4 Cestode Zoonoses

4.3.8 Control
Control of the flea vectors from dog, cat and theirsurroundings, personnel hygiene (washing handsof children after they play with pets), proper dis-posal of cat and dog faeces and regular dewor-ming of pet animals can help control the infection.
4.4 Echinococcosis
Class: CestodaOrder: CyclophyllideaFamily: Taeniidae
4.4.1 Common Name/Synonyms
Hydatidosis, dwarf dog tapeworm
4.4.2 Etiology
Echinococcosis is a very important cestodezoonosis. The infection occurs due to the para-sites belonging to the species Echinococcus(Family Taeniidae). E. granulosus, Echinococ-cus multilocularis, Echinococcus oligarthrusand Echinococcus vogeli (Rausch 1975 andThompson 1995) are the species of the genusEchinococcus responsible for the disease.Among these, E. granulosus zoonosis is partic-ularly significant due to many domestic, man-made life-cycle patterns and involvement ofnumber of intermediate hosts (Eckert 1998;Schantz et al. 1995). Further, there are ninerecognised strains of E. granulosus (Thompsonet al. 1995). The metacestode infection is com-monly known as hydatidosis.
4.4.3 Epidemiology
E. granulosus is worldwide in occurrence(Eckert et al. 2001; Singh et al. 2012a, b, Juyalet al. 2005; Bhatia and Pathak 1990) and human
cases have been reported throughout the worldwhereas E. multilocularis is mainly prevalent innorthern hemisphere. The other two parasites arefound in central and south America (Acha andSzyfres 2006).
4.4.4 Transmission
The carnivorous animals act as definitive hosts,and shed eggs in their faeces. The ingestion ofthese eggs by the intermediate host animals andoccasionally man leads to development of met-acestode stage in their visceral organs primarilyliver and lungs (WHO and OIE 2001).
4.4.5 Life Cycle
Most of the food producing animals viz. cattle,buffalo, sheep, goat and pigs along with someother mammals act as intermediate hosts forE. granulosus (Rausch 1986; Rausch 1995;Thompson and Allsopp 1988; WHO 1984).Dog and foxes act as definitive hosts forE. granulosus and E. multilocularis, respectivelyfor most of the times.
E. granulosus—Definitive host: Dogs and wildcanidsIntermediate host: Sheep, pig, cattle, buffalo,goat, horses, camels, other herbivorous animalsand manE. multilocularis—Definitive host: Arctic fox(Alopex lagopus) and red fox (Vulpes vulpes)Intermediate host: Wild rodentsE. oligarthrus—Definitive host: Wild felids(Jaguars, Pumas etc.)Intermediate host: RodentsE. vogeli—Definitive host: Wild canid (Speothosvenaticus)Intermediate host: Rodent Cuniculus paca
Life cycle of other Echinococcus species isalmost similar to E. granulosus involving theirrespective intermediate and definitive hosts(Fig. 4.6).
4.3 Dipylidiosis 71

4.4.6 Clinical Signs in Man
Human beings could become infected afteraccidental consumption of eggs of the parasiteshed in the faeces of the definitive carnivoroushost/animal. Depending upon the parasiteinvolved, three types of the disease could occurin human beings (WHO and OIE 2001).
Cystic echinococcosis (CE): The diseaseoccurs due to metacestode of E. granulosus.C. echinococcosis is an important disease prob-lem in many parts of the world (WHO and OIE2001). Unilocular cysts occur in liver, lung andfew other organs.
Alveolar echinococcosis (AE): The diseaseoccurs due to metacestode of E. multilocularisand produces alveolar hydatidosis. Althoughrare, but disease is malignant and highly fatalamong infected human beings.
Polycystic echinococcosis (PE): The diseaseoccurs due to metacestode of E. vogeli orE. oligarthrus.
The clinical signs in these forms varydepending upon the type of visceral organinvolved. Liver and lungs are parasitised most ofthe times and the related clinical signs are seenaccordingly.
4.4.7 Clinical Signs in Animals
4.4.7.1 Intermediate HostsThe symptoms generally do not appear and thedomestic animals remain asymptomaticthroughout their life, but the disease causessignificant economic losses in most of the foodproducing animals at the time of slaughter due to
Fig. 4.6 Life cycle of Echinococcus granulosus
72 4 Cestode Zoonoses

condemnation of infected organs. Large-sizedhydatid cysts can cause symptoms in the animalsdue to pressure atrophy of the affected organ(s)(Schwabe 1986). The cysts are mainly found inliver and lung but can be present in spleen, heart,kidney and other organs (Orlando 1997; WHOand OIE 2001). The cysts are responsible forreduced growth and milk production especiallyin dairy animals.
4.4.7.2 Definitive HostThe infected carnivorous animals generally donot present any clinical symptoms.
4.4.8 Diagnosis
In intermediate host animals, the disease can bediagnosed at the time of post mortem inspectionof the infected organs, radiographic techniques,ultra sonography, PCR and serological tech-niques. In carnivorous animals, detection of eggsusing conventional parasitological techniquesand later confirmation by PCR and serologicaltechniques can be used. In human beings, radi-ography along with serological confirmation isroutinely used for diagnosis of the parasite(Figs. 4.7, 4.8, 4.9, 4.10, 4.11, 4.12 and 4.13).
4.4.9 Control
Control of stray dogs, prevention of illegalslaughter (with free access to dogs) and treatmentof infected dogs are important steps to be takenFig. 4.7 Hydatid cysts in liver of sheep
Fig. 4.8 Hydatid cysts in lungs of sheep
Fig. 4.9 Hydatid cysts in liver of pig
Fig. 4.10 Fully mature invaginative forms of protosco-lices at 10 X
4.4 Echinococcosis 73

particularly for the control of E. granulosusrelated echinococcosis.
4.5 Sparganosis
Subclass: CestodaOrder: PseudophyllideaFamily: Diphyllobothriidae
4.5.1 Common Name/Synonyms
Spirometrosis, Larval diphyllobothriasis
4.5.2 Etiology
Several species of the Spirometra, such asSpirometra mansoni, S. mansonoides andS. erinaceieuropaei can cause the disease.
4.5.3 Epidemiology
Sparganosis is a rare cestode zoonosis that caninfect man. The parasite has been recordedacross the globe but is commonly found ineastern Asia (Viroj 2005) viz. countries such asChina, Korea, Japan, and from Southeast Asia.The parasite has also been reported from adomestic cat in India (Saleque et al. 1989).
4.5.4 Life Cycle
Humans can act as accidental secondary inter-mediate host where plerocercoid (metacestodestage) develop and results in sparganosis(Beaver et al. 1984; Andersen 1983; Cho et al.1990; Tesacharoen 1980). Frogs act as thesecond intermediate hosts. Ingestion of larvaefrom cyclops (copepod; first intermediate host)or frogs can lead to infection in humans, pigsand mice (Fukushima and Yamane 1999;Nithiuthai et al. 2004). Second stage larvae(spargana) during their migration in these hosts(reptiles-snakes; mammals such as pigs andhuman beings) cause the disease (Mueller 1974;Bearup 1953; Daly 1982; Acha and Szyfres1987). The animals belonging to the familycanidae and felidae act as definitive hosts(Fig. 4.14).
4.5.5 Transmission
The disease is transmitted to man throughingestion of infected copepods in drinking water,
Fig. 4.11 Alternate arrangement of large and smallhooks in the rostella (E. granulosus) at 100X
Fig. 4.12 Taenia spp. eggs seen at 10X
Fig. 4.13 Taenia spp. eggs at 100X
74 4 Cestode Zoonoses

ingesting lightly cooked frogs and snakes,poultry and pork. Use of infected frog as abandage and pressing it on the ulcers, skin andeye could lead to transmission of the parasitethrough mucous membranes (Mueller 1974;Acha and Szyfres 1987).
4.5.6 Clinical Signs in Man
The spargana can enter brain, eye, subcutaneoustissues, abdominal cavity, and rarely spinal cordwhich can result in blindness, paralysis anddeath (Yoon et al. 2004; Cho et al. 2000). Theparasite has the ability to infect cerebral, ocular,subcutaneous and other visceral organs depend-ing upon the migration of the parasite (Holodniyet al. 1991).
4.5.7 Clinical Signs in Animals
The infection generally remains asymptomaticin intermediate and definitive hosts but couldcause weight loss and emaciation in cats.
4.5.8 Diagnosis
The disease can be diagnosed from clinicalsigns, identification of parasitic stages andserological tests.
4.5.9 Prevention and Control
For preventing the disease, clean drinking waterand properly cooked meat of the concernedspecies should always be consumed.
Fig. 4.14 Life cycle of Spirometra species
4.5 Sparganosis 75
4.6 Taeniasis and Cysticercosis
Order: CyclophyllideaFamily: Taeniidae
Taeniasis is a true zoonotic infection(Euzoonoses) where pig and cattle act as inter-mediate host for Taenia solium and Taeniasaginata, respectively and human beings act asdefinitive hosts. Taenia asiatica (from pigs),much related to T. saginata could also infecthuman beings (Li et al. 2007).
4.6.1 Common Name/Synonyms
T. solium taeniasis, T. saginata taeniasis, cysti-cercosis, measly pork, measly beef, neurocys-ticercosis (NCC)
4.6.2 Etiology
The infection occurs due to T. solium andT. saginata in pigs and cattle, respectively. Thelarval forms of T. solium and T. saginata areknown as Cysticercus cellulosae and C. bovis inpigs and cattle, respectively.
4.6.3 Epidemiology
T. saginata, T. solium, and T. asiatica are pre-valent worldwide. Taeniasis swine is an impor-tant public health issue particularly indeveloping countries (Pathak et al. 1984; Juyalet al. 2008) and 20 million persons are believedto be infected with T. solium cysticerci (Bernet al. 1999) and as per WHO, adult parasites areprevalent among 2 million people worldwide(Shandera et al. 1994; White 2000; Yanagidaet al. 2012; Del Brutto 1999; Murrell 2005).Neurocysticercosis is an important public healthissue and is responsible for neurological disor-ders worldwide (White 2000; Flisser et al.2005). T. asiatica is distributed in east Asia(Anantaphruti et al. 2007).
4.6.4 Transmission
Humans and pigs act as definitive and interme-diate hosts, respectively for T. solium. But acci-dental ingestion of eggs of the parasite(T. solium) by human beings can also lead toserious disease such as neurocysticercosis.So both the taeniasis and cysticercosis due toT. solium can occur in human beings. Humanbeings become infected after ingestion of raw orpartially cooked measly pork (Singh et al. 2002).Pigs and human beings can become infected afteringestion of eggs shed by human carriers. Tae-niasis infected person (Taenia carriers) act asimportant risk factor for neurocysticercosis forthe other members of the family (Flisser 1994).Poor sanitary conditions and feeding of pigs ongarbage and human waste are important factorsresponsible for the spread of the disease (Li et al.2007; Sarti et al. 1992; Pawlowski and Murrell2001; Burneo and Garcia 2002). Sewage farmingis another important risk factor for neurocystic-ercosis even for the vegetarians and non-porkeaters. The consumption of measly beef couldlead to T. saginata taeniasis in man (Fig. 4.15).
4.6.5 Clinical Signs in Man
The important symptoms due to taeniasis includeabdominal pain, nausea, diarrhoea but the diseasemay remain asymptomatic at times (Garcia et al.2003). But the prompt diagnosis of T. solium tae-niasis is important so as to avoid the risk of auto-infection through faecal contamination leading toneurocysticercosis in human beings. In case ofcysticercosis, cysticerci may be present in the sub-cutaneous tissue beneath the skin, skeletal or cardiacmuscles. Rare eye infections leading to blindness(Cardenas et al. 1992) and tongue infections (Eliaset al. 2005) can also occur. The cysticerci havetendency to develop in the brain tissue leading toneurocysticercosis (Garcia et al. 2003). Dependingupon the location and number of cysticerci in thecentral nervous system, the symptoms such as sei-zures and headaches, vision problems, late-onset/
76 4 Cestode Zoonoses

adult/acquired epilepsy (Medina et al. 1990; White2000) and death can occur. T. saginata taeniasisusually remain asymptomatic but very high parasiteloads can result in abdominal pain, diarrhoea,weight loss and intestinal obstruction.
4.6.6 Clinical Signs in Animals
No symptoms are usually seen in pigs even ifthousands of cysts are present (Garcia et al.2003). Small cysts can be seen in many organssuch as skeletal muscles and some visceralorgans, but the disease generally remains
asymptomatic. However, T. solium cysticercosiscauses huge economic losses to the pig industry(Garcia et al. 2003).
4.6.7 Diagnosis
Detection of Taenia eggs from faecal samples,immunodiagnostic tools such as ELISA, coproantigen detection assays, CT and MRI can beused for diagnosis of the disease from humanbeings (Garcia et al. 2003; Allan et al. 2007).Cysticercosis is mainly diagnosed at the time ofpost mortem examination in pigs (Figs. 4.16,4.17, 4.18 and 4.19).
Fig. 4.15 Life Cycle of Taenia solium
4.6 Taeniasis and Cysticercosis 77

4.6.8 Control
Elimination of human carriers is highly impor-tant for prevention of neurocysticercosis (CDC1992). The T. solium carriers should be treatedwith anthelmintics such as praziquantel (Flisseret al. 2005; Garcia 2001). Interdisciplinaryapproaches (Engels et al. 2003), use of anthel-mintics (Roman et al. 2000) in endemic areas,avoiding free access of human faeces to pigs,education of lower socioeconomic populationcan help reduce the incidence of the disease(Juyal et al. 2008). Consumption of properlycooked pork, implementation of meat inspectionpractices and freezing of pork for appropriatetime before consumption can help prevent thedisease.
4.7 Other Cestode Zoonoses
4.7.1 Bertiellosis
Bertiellea species cestode commonly occurs inchimpanzees and rodents. The two speciesB. studri and B. macronata have also beenreported from human beings (Feldman et al.1983; Denegri and Perez-Serrano 1997; Denegriet al. 1998). Oribatid mites act as intermediatehost where cysticercoid stage occurs. Humanbeings can become infected after accidental
Fig. 4.17 Cysticercus cellulosae in striated muscles ofpig
Fig. 4.18 Cysticercus cellulosae in striated muscles ofpig
Fig. 4.19 Pig brain infected with Cysticercus cellulosae
Fig. 4.16 Cysticercus cellulosae in striated muscles ofpig
78 4 Cestode Zoonoses

ingestion of these mites. The disease remainsasymptomatic but there might be abdominalpain, diarrhoea and general fatigue in somehuman patients (Denegri and Perez-Serrano1997).
4.7.2 Hymenolepiosis
The disease occurs due to Hymenolepis nana orH. diminuta which have zoonotic significance(Waugh et al. 2006). Rodents act as principalhost for these parasites but the parasite couldinfect humans, particularly children (Goswamiet al. 2011). The parasite has been recorded frommany parts of the world (Marangi et al. 2003)particularly from India (Watwe and Dardi 2008).The life cycle of parasite is direct with theinfection through faecal oral route in humans, butrat may play role in the transmission of the dis-ease due to contamination of human food with ratfaeces. The parasite infects gastrointestinal sys-tem and remains asymptomatic but can causeabdominal pain, diarrhoea, weakness, etc.
4.7.3 Inermicapsiferosis
The infection occurs due to Inermicapsifermadagascariensis found in rodents in Africa(Acha and Szyfres 2006). The parasite rarelyinfects man through rodent-arthropod-man cycle(Acha and Szyfres 2006).
4.7.4 Mesocestoidosis
The disease occurs due to Mesocestoides linea-tus and M. variablis (Acha and Szyfres 2006).The parasite has been reported from Japan,China and Korea (Eom et al. 1992). The lifecycle of the parasite is not clear but dogs, catsand other carnivores may act as definitive hostand coprophagous arthropod as first intermediatehost and rodents, birds, amphibians, reptiles assecond intermediate host (Acha and Szyfres2006). Consumption of undercooked meat ofamphibians, reptiles, etc. may cause the disease
in man. The parasite infects gastrointestinalsystem and may cause abdominal pain, diar-rhoea, weakness, etc.
4.7.5 Raillietinosis
The infection occurs due to Raillietina celeb-ensis and Raillietina demerariensis and fewother species found in rodents. Insects act asintermediate hosts where cysticercoids developand rare human infections occur after acciden-tal ingestion of food contaminated with infectedarthropod (Acha and Szyfres 2006). The para-site generally remains asymptomatic but couldaffect circulatory, nervous or digestive systemin man.
References
Abo-Shehada MN, Ziyadeh Y (1991) Prevalence ofendoparasites in dog faecal deposits in Jordan.J Helminthol 65:313–314
Acha PN, Szyfres B (1987) Zoonoses and communicablediseases common to man, 2nd edn. Pan Amer HealthOrg, pp 744–749
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals, 3rd edn, volIII. Parasitoses, published by World Health Organi-sation, Geneva
Adams AM, Rausch RL (1997) Diphyllobothriasis. In:Connor DH, Chandler FW, Schwartz DA, Manz HJ,Lack ED (eds) Pathology of infectious diseases, vol 2.Appleton and Lange, Stanford, pp 1377–1389
Allan JC, Wilkins PP, Tsang VCW, Craig PS (2007)Immunodiagnostic tools for taeniasis. Acta Trop87(2003):87–93
Anantaphruti MT, Yamasaki H, Nakao M, Waikagul J,Watthanakulpanich D, Nuamtanong S, Maipanich W,Pubampen S, Sanguankiat S, Muennoo C, Nakaya K,Sato MO, Sako Y, Okamoto M, Ito A (2007)Sympatric occurrence of Taenia solium, T. saginata,and T. asiatica. Emerg Infect Dis 13(9):1413–1416
Andersen KL (1983) Description of musculature differ-ences in spargana of Spirometra (Cestoda; Pseudo-phyllidea) and tetrathyridia of Mesocestoides(Cestoda; Cyclophyllidea) and their value in identi-fication. J Helminthol 57:331–334
Bearup AJ (1953) Life history of a Spirometrid tape-worm, causing Sparganosis in feral pigs. Aust Vet J29:217–224
Beaver PC, Jung RC, Cupp EW (1984) Clinical Parasi-tology, 9th edn. Lea and Febiger, Philadelphia
4.7 Other Cestode Zoonoses 79

Benifla M, Barrelly R, Shelef I, El-on J, Cohen MD,Cagnano E (2007) Huge hemispheric intraparenchy-mal cyst caused by Taenia multiceps in a child.J Neurosurg Pediatr 107(6):511–514
Bern C, Garcia HH, Evans C, Gonzalez AE, VerasteguiM, Tsang VC, Gilman RH (1999) Magnitude of thedisease burden from neurocysticercosis in a develop-ing country. Clin Infect Dis 29:1203–1209
Bhatia BB, Pathak KLM (1990) Echinococcosis. In:Parija SC (ed) Review of Parasitic Zoonoses. AITBSPublishers and Distributors, New Delhi, pp 212–219
Burneo JG, Garcia HH (2002) Neurocysticercosis. Med J3:1–20
Bylund G, Andersen K (1994) Thirty years of Diphyl-lobothrium research and future trends. Bull Scand SocParasitol 4:47–56
Cardenas F, Quiroz H, Plancarte A, Meza A, Dalma A,Flisser A (1992) Taenia solium ocular cysticercosis:findings in 30 cases. Ann Ophthalmol 24:25–28
CDC (1992) International task force for disease eradica-tion. Morb Mortal Wkly Rep 41:697–698
Chai JY, Murrell KD, Lymbery AJ (2005) Fish-borneparasitic zoonoses: status and issues. Int J Parasitol35:1233–1254
Chappell CL, Penn HM (1990) Dipylidium caninum,an underrecognized infection in infants and children.Pediatr Infect Dis J 9:745–747
Chervy L (2002) The terminology of larval cestodes ormetacestodes. Syst Parasitol 52:1–33
Cho SY, Kang SY, Kong Y (1990) Purification ofantigenic protein of sparganum by immune affinitychromatography using a monoclonal antibody. Kor-ean J Parasitol 280:135–142
Cho JH, Lee KB, Yong TS, Kim BS, Park HB, Ryu KN(2000) Subcutaneous and musculoskeletal spargano-sis: imaging characteristics and pathologic correlation.Skeletal Radiol 29:402–408. doi:10.1007/s002560000206
Claudia PM, James O, Patrick A (2003) Infection byDipylidium caninum in an infant. Arch Pathol LabMed 127:e157–e159
Craig P, Ito A (2007) Intestinal cestodes. Curr OpinInfect Dis 20:524–532
Cross JH (2001) Fish-and invertebrate-borne helminthes.In: Hui YH, Sattar SA, Murrell KD, Nip WK,Stanfield PS (eds) Foodborne disease handbook, vol2. Marcel Dekker, New York, pp 631–634
Daly JJ (1982) Sparganosis. In: Steele JH, Jacobs L,Arambul P (eds) CRC handbook series in zoonosis,section C: parasitic zoonoses, vol 1. CRC Press Inc,Boca Raton, pp 293–312
Dantas-Torres F (2008) Canine vector-borne diseases inBrazil. Parasites Vectors 1(25):1–17
Del Brutto OH (1999) Neurocysticercosis: a review. RevNeurol 29:456–466
Denegri G, Perez-Serrano J (1997) Bertielliasis in man:a review of cases. Rev Med Trop S Paulo39(2):123–127
Denegri G, Bernadina W, Perez-Serrano J, Rodriguez-Caabeiro F (1998) Anoplocephalid cestodes of
veterinary and medical significance: a review. FoliaParasitol 45:1–8
Dick TA, Nelson PA, Choudhury A (2001) Diphyllo-bothriasis: update on human cases, foci, patterns andsources of human infections and future consider-ations. Southeast Asian J Trop Med Public Health32(2):59–76
Dupouy-Camet J, Peduzzi R (2004) Current situation ofhuman diphyllobothriasis in Europe. Eurosurveillance9:31–35
Eckert J (1998) Alveolar echinococcosis (Echinococcusmultilocularis) and other forms of echinococcosis(E. vogeli and E. oligarthrus). In: Palmer SR, SoulsbyEJL, Simpson DIH (eds) Zoonoses. Oxford Univer-sity Press, Oxford, pp 689–716
Eckert J, Schantz PM, Gasser RB, Torgerson PR,Bessonov AS, Movses-sian SO, Thakur A, GrimmF, Nikogossian MA (2001) Geographic distributionand prevalence. In: Eckert J, Gemmell MA, MeslinFX, Pawlowski ZS (eds) WHO/OIE manual onechinococcosis in humans and animals: a publichealth problem of global concern. World Organisa-tion for Animal Health, Paris, pp 100–142
Eguchi S (1973) Diphyllobothrium latum (Linnaeus,1758). Proc Med Parasitol Jpn 5:127–144
Elias FM, Martins MT, Foronda R, Jorge WA, Araujo NS(2005) Oral cysticercosis: case report and reviewof the literature. Rev Inst Med Trop Sao Paulo47:95–98
El-on J, Shelef I, Cagnano E, Benifla M (2008) Taeniamulticeps: a rare human cestode infection in Israel.Veterinaria Italiana 44(4):621–631
Engels D, Urbani C, Belotto A, Meslin F, Savioli L(2003) The control of human (neuro) cysticercosis:which way forward? Acta Trop 87:177–182
Eom KS, Kim S, Rim HJ (1992) Second case of humaninfection with Mesocestoides lineatus in Korea. TheKorean J Parasitol 30(2):147–150
Feldman R, Denegri G, Avolio J, Cantu N (1983) Nuevocaso humano de teniasis por Bertiellea mucronataMeyner, 1895 en la Argentina I. Diagnostico ytratamiento. Acta Bioq Clin Latinoam 17:571–578
Flisser A (1994) Taeniasis and Cysticercosis due toTaenia solium. Prog Clin Parasitol 4:77–116
Flisser A, Vazquez-Mendoza A, Martinez-Ocana J,Gomez-Colin E, Leyva RS, Medina- Santillan R(2005) Evaluation of a self-detection tool for tape-worm carriers for use in public health. Am J TropMed Hyg 72:510–512
Fukushima T, Yamane Y (1999) How does the sparga-nosis occur? Parasitol Today 15:124. doi:10.1016/S0169-4758(99)01405-2
Garcia LS (2001) Diagnostic medical parasitology, 4thedn. ASM Press, Washington, DC
Garcia HH, Gonzalez AE, Evans CA, Gilman RH (2003)Taenia solium cysticercosis. Lancet 362:547–556
Goswami R, Singh SM, Kataria M, Somvanshi R (2011)Clinicopathological sudies on spontaneous Hymenol-epis diminuta infection in wild and laboratory rats.Braz J Vet Pathol 4(2):103–111
80 4 Cestode Zoonoses

Holodniy M, Almenoff J, Loutit J (1991) CerebralSparganosis: Case report and review. Rev Infec Dis13:155–159
Ing MB, Schantz PM, Turner JA (1998) Human Coenu-rosis in North America: Case Reports and Review.Clinical Infect Dis 27:519–523
Johnstone HG, Jones OW (1950) Cerebral coenurosis inan infant. Am J Trop Med 30:431–441
Juyal PD, Singh NK, Kaur P (2005) Hydatidosis in India:a review on veterinary perspectives. J Parasitic Dis29(2):97–102
Juyal PD, Sharma R, Singh NK, Singh G (2008)Epidemiology and control strategies against cysticer-cosis (due to Taenia solium) with special reference toswine and human in Asia. J Vet Animal Sci 1:1–10
Lee KW, Suhk HC, Pai KS, Shin HJ, Jung SY, Han ET,Chai JY (2001) Diphyllobothrium latum infectionafter eating domestic salmon flesh. Korean J Parasitol39:319–321
Li T, Ito A, Craig PS, Chen X, Qiu D, Zhou X, Xiao N,Qiu J (2007) Taeniasis/cysticercosis in China. South-east Asian J Trop Med Public Health 38(1):131–139
Lloyd S (1998) Other cestode infections. In: Palmer SR,Soulsby L, Simpson DIH (eds) Zoonoses: Biology,Clinical Practice and Public Health Control. OxfordUniversity Press, Oxford, pp 653–656
Magath TB (1937) Factors influencing the geographicdistribution of D. latum. In: Schulz RES, GnyedinaMP (ed) Papers on helminthology. K. I. Skrjabin,Moscow, Russia, p 366–379
Marangi M, Zechini B, Fileti A, Quaranta G, Aceti A(2003) Hymenolepis diminuta infection in a childliving in the urban area of Rome, Italy. J ClinMicrobiol 41:3994–3995
Marx MB (1991) Parasites, Pets, and People. Prim Care18(1):153–165
Medina MT, Rosas E, Rubio-Donnadieu F, Sotelo J(1990) Neurocysticercosis as the main cause of late-onset epilepsy in Mexico. Arch Intern Med150:325–327
Mueller JF (1974) The biology of Spirometra. J Parasitol60:3–14
Murrell KD (2005) Epidemiology of taeniosis andcysticercosis. In: Murrell KD (ed) WHO/FAO/OIEGuidelines for the surveillance, prevention and con-trol of taeniosis. OIE, Paris, pp 27–32
Neira OP, Jofre ML, Munoz SN (2008) Dipylidiumcaninum infection in a 2 year old infant. Case reportand literature review. Rev Cil Infectol 25(6):465–471
Nithiuthai S, Anantaphruti MT, Waikagul J, Gajadhar A(2004) Waterborne zoonotic helminthiases. VetParasitol 126:167–193. doi:10.1016/j.vetpar.2004.09.018
Orlando DF (1997) Evolution of the programme for thecontrol of hydatidosis in Uruguay. Archivos Interna-cionales de la hidatidosis 32:69–72
Pathak KML, Gaur SNS, Kumar D (1984) The epidemi-ology of strobillar and cystic phase of Taenia soliumin certain parts of Uttar Pradesh (India). Indian VetMed J 4:17–18
Pawlowski ZS, Murrell KD (2001) Taeniasis and cysti-cercosis. In: Hui YH, Sattar SA, Murrell KD et al(eds) Foodborne disease handbook: viruses, parasites,pathogens, and HACCP, vol 2. Marcel Dekker,New York, pp 217–227
Ramana KV, Rao SD, Rao R, Mohanty SK, Wilson CG(2011) Human dipylidiasis: a case report of Dipylid-ium caninum infection in teaching hospital at Kar-imnagar. OJHAS 10(2) (Apr–Jun 2011)
Rausch RL (1975) Taeniidae. In: Hubbert WF, McCul-loch WF, Schurrenberger PR (eds) Diseases trans-mitted from animals to man. Thomas, Springfield,pp 678–707
Rausch RL (1986) Life cycle patterns and geographicdistribution of Echinococcus species. In: ThompsonRCA, Allen GA, Unwin (ed) The biology of Echino-coccus and hydatid disease. London, pp 44–80
Rausch RL (1995) Life cycle patterns and geographicdistribution of Echinococcus species. In: ThompsonRCA, Allen GA (eds) Echinococcus and hydatiddisease. CAB International, Wallingford, pp 88–134
Rausch RL, Adams AM (2000) Natural transfer ofhelminths of marine origin to freshwater fishes withobservation on the development of Diphyllobothriumalascense. J Parasitol 86:319–327
Reddy SB (1982) Infestation of a five-month-old infantwith Dipylidium caninum. Del Med J 54(8):455–456
Reid CJD, Perry FM, Evans N (1992) Dipylidiumcaninum in an infant. Eur J Pediatr 151:502–503
Robertson ID, Thompson RC (2002) Enteric parasiticzoonoses of domesticated dogs and cats. MicrobesInfect 4:867–873
Rohela M, Jamaiah I, Chan KW, Yosoff WS (2002)Diphyllobothriasis: the first case report from Malay-sia. Southeast Asian J Trop Med Public Health33:229–230
Roman G, Sotelo J, Del Brutto O, Flisser A, Dumas M,Wadia N, Botero D, Cruz M (2000) A proposal todeclare neurocysticercosis an international reportabledisease. Bull World Health Organ 78:399–406
Saleque A, Juyal PD, Bhatia BB (1989) Spirometra sp. indomestic cat in India. Vet Parasitol 35:273–276
Sarti E, Schantz PM, Plancarte A (1992) Prevalence andrisk factors for Taenia solium taeniosis and cysticer-cosis in humans and pigs in a village in Morelos,Mexico. Am J Trop Med Hyg 46:677–685
Scala A, Varcasia A (2006) Updates on morphobiology,epidemiology and molecular characterization of coe-nurosis in sheep. Parassitologia 48(1–2):61–63
Schantz PM, Chai J, Craig PS, Eckert J, Jenkins DJ,Macpherson CNL, Thakur A (1995) Epidemiologyand control of hydatid disease. In: Thompson RCA,Lymbery AJ (eds) Echinococcus and hydatid disease.CAB International, Wallingford, pp 233–331
Schmidt GD, Roberts LS (2000) Foundations of Parasi-tology, 6th edn. McGraw-Hill, Boston, p 670
Scholz TS, Garcia HH, Kuchta R, Wich B (2009) Updateon the human broad tapeworm (Genus Diphylloboth-rium), including clinical relevance. Clin MicrobiolRev 146–160
References 81

Schwabe CW (1986) Current status of hydatid disease:a zoonosis of increasing importance. In: ThompsonRCA, Allen G, Unwin (ed) The biology of Echino-coccus and hydatid disease. London, pp 81–113
Shandera WX, White AC, Chen JC, Diaz P, Armstrong R(1994) Neurocysticercosis in Houston, Texas. Areport of 112 cases. Med (Baltimore) 73:37–52
Singh G, Prabhakar S, Ito A (2002) Taenia solium taeniasisand cysticercosis in Asia. In: Singh G, Prabhakar S(eds) Taenia solium cysticercosis: from basic to clinicalscience. CABI, Cambridge, pp 111–127
Singh BB, Sharma JK, Ghatak S, Sharma R, Bal MS,Tuli A, Gill JPS (2012a) Molecular epidemiology ofechinococcosis from food producing animals in northIndia. Vet Parasitol 186:503–506
Singh BB, Sharma JK, Tuli A, Sharma R, Bal MS,Aulakh RS, Gill JPS (2012b) Prevalence and mor-phological chracterisation of Echinococcus granulo-sus from north India. J Parasitic Dis. doi:10.1007/s12639-012-0189-x
Templeton AC (1971) Anatomical and geographicallocation of human coenurus infection. Trop GeogrMed 23:105–108
Tesacharoen S (1980) Sparganum in Thai people. J MedCouncil 9:255–262
Thompson RCA (1995) Biology and systematics ofEchinococcus. In: Thompson RCA, Lymbery AJ(eds) Echinococcus and hydatid disease. CAB Inter-national, Wallingford, pp 1–50
Thompson RCA, Allsopp CE (1988) Hydatidosis. Vet-erinary perspectives and annotated bibliography.CAB International, Wallingford, p 246
Thompson RCA, Lymbery AJ, Constantine CC (1995)Variation in Echinococcus: towards a taxonomicrevision of the genus. Adv Parasitol 35:145–176
Torres P, Cuevas C, Tang M, Barra M, Franjola R,Navarrete N, Montefusco A, Otth L, Wilson G, PugaS, Figeroa L, Cerda O (2004) Introduced and nativefishes as infection foci of Diphyllobothrium spp. inhumans and dogs from two localities at Lake
Panguipulli in Southern Chile. Comp Parasitol70:111–117
Torres P, Villalobos L, Woelfl S (2007) Experimentalinfection of copepods from four lakes in southernChile with Diphyllobothrium latum (Linnaeus, 1758)coracidia. Comp Parasitol 74:167–170
Tsumura N, Koga H, Hidaka H, Mukai F, Ikenaga M,Otsu Y, Masunaga K, Nagai K, Yoneda Y, Fukuma T,Ishimoto K (2007) Dipylidium caninum infection inan infant. Kansenshogaku Zasshi 81(4):456–458
Turner JA (1962) Human dipylidiasis (dog tapeworminfection) in the United States. J Pediatr 61:763
Viroj W (2005) A review of human sparganosis inThailand. Int J Infect Dis 9:312–316
Von Bonsdorff B (1977) Diphyllobothriasis in man.Academic Press, New York
Watwe S, Dardi CK (2008) Hymenolepis diminuta in achild from rural area. Indian J Path Microbiol51:149–151
Waugh CA, Lindo JF, Foronda P, Angeles-Santana M,Lorenzo-Morales J, Robinson RD (2006) Populationdistribution and zoonotic potential of gastrointestinalhelminths of wild rats Rattus rattus and Rattusnorvegicus from Jamaica. J Parasitol 92:1014–1018
White AC (2000) Neurocysticercosis: Updates on epide-miology, pathogenesis, disease and management.Annu Rev Med 51:187–206
WHO (1984) Guidelines for surveillance, prevention andcontrol of echinococcosis/hydatidosis. Eckert J,Gemmell M, Matyas Z and Soulsby EJL (eds). WorldHealth Organization, Geneva, pp 1–147
WHO and OIE (2001) WHO/OIE Manual on Echino-coccosis in humans and animals: a public healthproblem of global concern. France, Paris
Yanagida T, Sako Y, Nakao M, Nakaya K, Ito A (2012)Taeniasis and cysticercosis due to Taenia solium inJapan. Parasites Vectors 5:18
Yoon KC, Seo MS, Park SW, Park YG (2004) Eyelidsparganosis. Am J Ophthalmol 2004(138):5–873. doi:10.1016/j.ajo.2004.05.055
82 4 Cestode Zoonoses

5Nematode Zoonoses
Abstract
Nematode Zoonoses could be defined as ‘‘those nematode diseases whichare naturally transmitted between (other) vertebrate animals and man’’.Zoonotic nematodes infect millions of people worldwide. An overview ofthe epidemiology, transmission, clinical manifestations and diagnosis ofzoonotic nematodes is presented, along with methods of prevention andcontrol. Angiostrongylosis is endemic in south Asia, Pacific islands,Australia, China and Caribbean islands. Zoonotic ascariasis due toAscaris suum has been widely reported in North America and someEuropean countries. Baylisascaris procyonis, the intestinal roundworm ofraccoons has been reported to cause severe neurologic disease in man.Subcutaneous migration of the animal hookworms could lead tocutaneous larva migrans (CLM) in man. Gnathostomiasis is a food-borne zoonosis of public health significance. Trichinellosis has beenreported in most parts of the world except the deserts. The provision ofsafe food and water in the non-industrialised countries is of utmostimportance for the prevention and control of these diseases.
5.1 Acanthocephalus
Phylum: AcanthocephalaFamily: Oligacanthorhynchidae
5.1.1 Common Name/Synonyms
MacracanthorhynchusThese parasites are spiny-headed worms and
at times are included in the same phylum
with nematodes (Garcia 2001). They are pseu-docoelomate endoparasites and have manyunique morphological and biological features(Marquards et al. 2000; Garcia 2001).
5.1.2 Etiology
Acanthocephalus primarily occurs due to fol-lowing species of parasites:
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_5, � Springer India 2013
83

5.1.3 Epidemiology
Acanthocephalus is not common and has beenrarely reported in man. Till date, seven cases ofacanthocephlus have been reported (Robertsand Janovy 2005; Berenji et al. 2007). Theseparasites include Acanthocephalus bufonis,Corynosoma strumosum, Acracanthorhynchuahirudinaceus, Moniliformis moniliformis, Bolb-soma sp. (Counselman et al. 1989; Marquardset al. 2000; Roberts and Janovy 2005), Macra-canthorhynchua ingens (Counselman et al. 1989,Roberts and Janovy 2005) and Acanthocephalusrauschi (Marquards et al. 2000; Roberts andJanovy 2005). The parasite M. moniliformis hasbeen reported from many parts of the world(Ikeh et al. 1992; Roberts and Janovy 2005).Human infections due to M. moniliformis havebeen reported from Africa, Asia, Australia,Europe, and America (Muller 1975; Beaver et al.1984; Ikeh et al. 1992; Baker et al. 2000; Berenjiet al. 2007). The morphological parameters ofthe parasite have been described in detail bydifferent authors (Lawlor et al. 1990; Beaveret al. 1984; Roberts and Janovy 2005).
5.1.4 Transmission
Man gets the infection after consumption of rawparatenic host (Roberts and Janovy 2005) or dueto incidental consumption of intermediate host(Berenji et al. 2007).
5.1.5 Life Cycle
Humans are the incidental hosts, and the wormresides in the small intestine. The definitivehosts become infected after eating the interme-diate host (Ikeh et al. 1992).
5.1.6 Clinical Signs in Manand Animals
The symptoms of the disease are not well defined.High parasitemia may lead to vomition, abdominalpain, perforation of the intestine, fatigue, diar-rhoea, anorexia, irritability and intermittent burn-ing sensations around the umbilicus (Beaver et al.1984; Counselman et al. 1989; Ikeh et al. 1992;
Name of the parasite Definitive host Intermediate host References
MacracanthorhynchushirudinaceusSynonym: Gigantorhynchushirudinaceus, G. gigas,Echinorhynchus gigas
Swine, wild boar and occasionallyrodents, bovine, dog, monkey and man
Dung beetle of thefamilyScarabaeidae
Acha andSzyfres(2006)
Moniliformis moniliformis Rats and small rodents Beetles andcockroaches
Corynosoma strumosum Arctic fox (Alopex lagopus), dog, seaotter (Enhydra lutris) and species ofcetaceans and pinnipeds
Amphipodcrustacean(Pontoporeiaaffinis)Many species offish could act asparatenic host
Acanthocephalus rauschi,A. bufonis (A. sinensis)
Crustaceans –
Bolbosoma spp. Cetaceans Juvenile state foundin fish
84 5 Nematode Zoonoses

Marquards et al. 2000; Roberts and Janovy 2005).The penetration of proboscis and release andreattach tendency of the parasite could lead toinflammation, ulcer and haemorrhages in thedefinitive host (Marquards et al. 2000; Garcia2001; Roberts and Janovy 2005). It has beenobserved that M. moniliformis infected cockroachmove more slowly and travel shorter distances(Moore et al. 1994; Libersat and Moore 2000;Roberts and Janovy 2005). This might be respon-sible for the parasite’s predation by the definitivehost (Libersat and Moore 2000). The morbidity isgenerally high among mammals infected withacanthocephalans. However, fish may remainasymptomatic even after high intensities of wormsdeeply penetrated into their intestinal wall(Taraschewski 2000). The high heavy metalsabsorbance capacity indicates the usefulness ofacanthocephalans as bioindicators (Taraschewski2000).
5.1.7 Diagnosis
The disease can be diagnosed by identificationof the thick-shelled eggs containing first larvalstage in the faecal samples, while a living ordead fluke is rarely seen.
5.1.8 Control
Humans should avoid ingestion of intermediateor paratenic host.
5.2 Angiostrongylosis
Order: StrongylidaSuperfamily: Metastrongyloidea
5.2.1 Common Name/Synonyms
Intestinal angiostrongyliasis, eosinophilic menin-gitis
5.2.2 Etiology
The rat lung worm, Angiostrongylus cantonensiswas first time reported in China (Chen 1935)from domestic rat. This is a food-borne zoonoticnematode parasite of significant public healthimportance. Angiostrongylus costaricensis cau-ses abdominal eosinophilic granulomas in Cen-tral and South America (Pien and Pien 1999).
5.2.3 Epidemiology
Angiostrongylosis due to A. cantonensis isendemic in south Asia, Pacific islands, Australia,China and Caribbean islands (Wang et al. 2008;Lv et al. 2008).
5.2.4 Transmission
Human beings become infected after consump-tion of intermediate (raw snails) or paratenichosts (freshwater prawns, crabs, frogs), or veg-etables contaminated with the infected larvae(Alicata 1991).
5.2.5 Life Cycle
For A. cantonensis, rats and molluscs act as thedefinitive and intermediate host for this parasite,respectively. The crustaceans (prawns and landcrabs), predacious land planarians (flatworms inthe genus Platydemus), frogs and monitor lizards(Wang et al. 2008) are the important paratenichosts. The parasite A. cantonensis is present in the(pulmonary arteries) rat lungs. Larvae hatch andmigrate through trachea and gastrointestinal tractto rat faeces. These first stage larvae are eaten upby snails and slugs, and further develop intoinfective larvae (third stage). Man and ratsbecome infected after consuming infected snail orcontaminated vegetables. Larvae migratetowards the brain in human beings and could leadto brain abscess and haemorrhage (Koo et al.1988). The parasite A. costaricensis resides inmesenteric arteries of caecum of cotton rat. The
5.1 Acanthocephalus 85

first stage larvae penetrate slugs and develop tosecond and third stage larvae. The cycle is com-pleted when definitive host ingest infective larvaereleased from slugs (Fig. 5.1).
5.2.6 Clinical Signs in Man
In A. cantonensis angiostrongylosis, the parasiteinfects brain (Cross 1978; Chotmongkol andSawanyawisuth 2002). The other importantsymptoms include headache, neck stiffness,paraesthesia, vomition and nausea (Wang et al.2008). Symptoms due to A. costaricensis includeabdominal pain, vomition and rarely gastroin-testinal bleeding (Hulbert et al. 1992; Silveraet al. 1989).
5.2.7 Clinical Signs in Animals
The infected rodents may show sneezing,coughing, fibrosis in the lungs and occasionallygastrointestinal lesions.
5.2.8 Diagnosis
The disease can be diagnosed after detection ofthe parasite from cerebrospinal fluid or ocularchamber (Wang et al. 2008). History, clinicalsigns and serological tests are also useful in thediagnosis. Diagnosis of human angiostrongylosis(A. cantonensis) is based on clinical features aswell as laboratory findings (Eamosobhana andYong 2009; Eamsobhana 2006).
5.2.9 Control
Prevention and control measures primarily relyupon health education, avoidance of eating rawor undercooked intermediate and paratenichosts, unwashed vegetables and rodent control.
5.3 Anisakiosis
Order: AscarididaFamily: Anisakidae
Fig. 5.1 Life cycle of Angiostrongylus cantonensis
86 5 Nematode Zoonoses
Anisakiosis is parasitic zoonosis whichoccurs due to accidental ingestion of the parasitelarvae (Sakanari and Mckerrow 1989).
5.3.1 Common Name/Synonyms
Herring worm disease, Cod worm disease
5.3.2 Etiology
The disease can occur due to Anisakis, Pseudo-terranova and Contracaecum species, butAnisakis is primarily important. A. simplex isparticularly associated with gastroallergic ani-sakiosis (Audicana et al. 2002).
5.3.3 Epidemiology
The scientist ‘Van Thiel’ for first time recognizedAnisakiosis in 1960 (Van Theil 1960). The dis-ease is common in Japan (about 2000 cases/year)but cases have also been recorded from northernEurope (Scandinavia, Holland) and Pacific coastof South America (Caramello et al. 2003). Gastricanisakiosis is more common in Japan, whileintestinal anisakiosis has been mainly reportedfrom Europe (Audicana et al. 2002).
5.3.4 Transmission
Human beings become infected after eating raw orlightly cooked marinated seafood such as Japanesesushi and sashimi, Dutch salted or smoked herring,Scandinavian gravlax, Hawaiian lomi–lomi andLatin American ceviche (Chai et al. 2005).
5.3.5 Life Cycle
The adult parasites are present in stomach ofmarine fish (whales and dolphins). Crustaceans
act as first intermediary hosts. Fish and somecuttlefish act as paratenic hosts (Caramello et al.2003). Human beings become infected afterconsumption of third stage larvae present ininfected salt-water fish or cephalopod molluscspecies, including mackerel, squid, sardine,horse mackerel, salmon and bonito (Yasunagaet al. 2010; Karasawa et al. 2008). In fish, larvaegenerally localise on the surface of visceralorgans, body cavity and occasionally on themuscles. In man, the parasites do not mature, butthey cause the disease. Other definitive hostsinclude birds, reptiles and amphibians (Fig. 5.2).
5.3.6 Clinical Signs in Man
The symptoms could arise due to both gastricand intestinal anisakiosis. Clinical signs arerelated to allergic reactions and tissue damage.Presence of Anisakis allergens in the humanfood cause gastroallergic anisakiosis which maylead to urticaria, angioedema and anaphylacticshock associated with other gastrointestinalsymptoms (Caramello et al. 2003; LopezSerrano et al. 2000). Acute gastric anisakiosisoccurs suddenly 12–72 h after ingestion of rawseafood and leads to severe abdominal pain(Sugimachi et al. 1985). The tissue damage bythe larvae causes intestinal anisakiosis. Furtherchanges include invasion of the gut wall, andeosinophilic granuloma, or perforation whichmay lead to symptoms such as fever, abdominalpain, vomition and bloody stools.
5.3.7 Clinical Signs in Animals
The parasite larvae may lead to liver atrophy,perforations of the stomach wall, visceral adhe-sions and muscle damage (Smith and Wootten1978). In marine mammals, parasites have beenfound embedded in gastric mucosa tumours(Acha and Szyfres 2006).
5.3 Anisakiosis 87

5.3.8 Diagnosis
The disease can be diagnosed by upper gastro-intestinal endoscopy for visualisation of theworm (McCarthy and Moore 2000) or usingmolecular techniques (Mattiucci et al. 2011).
5.3.9 Control
Prevention and control measures include healtheducation; avoid eating raw or undercookedfish and heating or freezing of fish at appro-priate time–temperature combinations beforeconsumption.
5.4 Ascariosis
Order: AscarididaSuperfamily: Ascaridoidea
5.4.1 Common Name/Synonyms
Ascaridiasis
5.4.2 Etiology
Ascariosis occurs due to Ascaris lumbricoidesand Ascaris suum; two closely related speciesresponsible for the disease in humans and pigs,respectively (Dold and Holland 2010). Thesespecies are morphologically indistinguishablewith few molecular variations (Anderson et al.1993). Albeit both the parasites are specific totheir hosts (Crompton 2001), experimentalstudies have shown that they can infect both thehosts (Takata 1951; Galvin 1968). In personsliving in low prevalence areas of human para-sites, A. suum could cause zoonotic infections(Crewe and Smith 1971; Jaskoski 1961; Lordand Bullock 1982; Nejsum et al. 2005). Theparasite A. suum has also been found among zoochimpanzees (Nejsum et al. 2010).
Fig. 5.2 Life cycle of Anisakis, Pseudoterranova, or Contracaecum species
88 5 Nematode Zoonoses

5.4.3 Epidemiology
A. lumbricoides is a common human parasiteworldwide and more than 1.2 billion people arebelieved to be infected globally (de Silva et al.2003). A. lumbricoides has been commonlyreported from sub-Saharan Africa, Americas,China and East Asia (WHO 2006). A. suum isanother parasite prevalent across the globeand infects pigs with high prevalence rates(Roepstorff et at. 1998; Nansen and Roepstorff1999). Zoonotic ascariosis due to A. suum hasbeen reported in North America, Denmark(Anderson 1995; Nejsum et al. 2005) andthe United Kingdom (Nejsum et al. 2010).Chimpanzees in the Copenhagen Zoo werefound infected with A. suum from pigs bymolecular analysis (Nejsum et al. 2005).
5.4.4 Transmission
Human beings become infected after accidentalingestion of Ascaris eggs through contaminatedfood, water or soil.
5.4.5 Life Cycle
The disease is transmitted via faecal-oral route.After ingestion of infective eggs, L3 larvaehatches in the intestine (Geenen et al. 1999).This is followed by movement of larvae fromsmall to large intestine and further penetration ofthe mucosa (Murrell et al. 1997). Later, thelarvae reach the liver via blood circulation andshed L2 cuticle and finally migrates to the lungs(Roepstorff et al. 1997). The larvae penetratealveolar space and move towards pharynx wherethey are swallowed. The larvae again return tosmall intestine where they mature and reachsexual maturity (Pilitt et al. 1981; Roepstorffet al. 1997). The eggs are shed in faeces anddevelop to infective larvae under favourableconditions.
5.4.6 Clinical Signs in Manand Animals
Clinical symptoms may range from asymptom-atic to severe coughing and wheezing. The lowerage groups are usually affected. Ascaris pnu-monia could result due to damage caused bylarvae. Heavy worm loads may lead to intestinalblockage and obstruction in children. Furthercomplications include intussusception, perfora-tion and gangrene of the bowel. In endemicareas, biliary and pancreatic disease could leadto biliary colic, acute cholecystitis, acute cho-langitis, acute pancreatitis and hepatic abscess.
5.4.7 Diagnosis
The disease can be diagnosed by detection of theparasitic eggs during the intestinal phase of thedisease. Clinical signs such as laboured breath-ing, stunting etc. can also aid in the diagnosis.Serological, molecular (Zhu et al. 1999) tech-niques can provide some help during themigratory phase of the larvae.
5.4.8 Control
Prevention and control measures includeimproved personnel hygiene, health education,improved sanitary measures and chemotherapy(Hotez et al. 2006).
5.5 Baylisascariasis
Order: AscarididaSuperfamily: Ascaridoidea
5.5.1 Etiology
The disease occurs due to Baylisascaris procy-onis, the intestinal roundworm of raccoons,
5.4 Ascariosis 89

which has been regarded as a cause of severeneurologic disease among humans (Sorvilloet al. 2002) since last 2–3 decades.
5.5.2 Epidemiology
This parasite is found in raccoons from NorthAmerica and has also been recorded in othercountries from Europe and Asia (Snyder 1987;Wirtz 1982). Fourteen confirmed human casesdue to B. procyonis have been cited in the lit-erature (Wise et al. 2005; Gavin et al. 2005).
5.5.3 Transmission
Human beings become infected after ingestionof infective eggs from environment contami-nated with racoon faeces.
5.5.4 Life Cycle
The North American raccoon (Procyon lotor)acts as the definitive host for B. procyonis.Intermediate hosts include small birds andmammals (particularly rodents). Humans act asaccidental intermediate hosts. The importantrisks for human infection include young childrenwith pica or geophagia (Kazacos 2000). Rac-coons become infected with B. procyonis throughtwo ways: either through ingestion of infectiveeggs from contaminated environment or afterconsumption of paratenic hosts (Wise et al. 2005;Kazacos 2001). The larvae are released betweeneggs and they develop into male and female adultworms (Kazacos 2001). Gravid females againstart releasing eggs into the faeces. The eggsundergo embryonation and become infective(Kazacos 2001). The paratenic hosts such assquirrels and rodents play an important role in thecompletion of the life cycle. After they ingesteggs, larvae are released which penetrate anddisseminate in different organs and tissues. Lar-vae often migrate to the central nervous system(CNS) (Tiner 1953) and these paratenic hosts are
consumed by racoons. The larvae mature inracoon to become male and female adults andshed eggs (Kazacos 1983, 2001) (Fig. 5.3).
5.5.5 Clinical Signs in Man
B. procyonis could rarely lead to fatal or neuro-logically devastating neural larva migrans(NLM). This results in acute eosinophilicmeningoencephalitis in infants and young chil-dren (Goldberg et al. 1993; Kazacos et al. 1985;Gavin et al. 2005). Pica, exposure to infectedraccoons and contaminated environments withracoon faeces are the three significant risk factorsfor infection (Gavin et al. 2005). The parasitemay occasionally lead to ocular larva migrans(OLM) usually in healthy adults. Clinical symp-toms are not fully understood but could includevisceral, neural and ocular larva migrans.
5.5.6 Clinical Signs in Animals
The infection in raccoons is generally subclini-cal. B. procyonis is considered as the mostcommon cause of clinical larva migrans in someother animals such as rodents, particularly NLM(Gavin et al. 2005). The case reports of infectionin dogs and cats have also been reported(Kazacos 2001; Greve and O’Brien 1989;Averbeck et al. 1995).
5.5.7 Diagnosis
The disease can be diagnosed from clinical signsand history, brain biopsy or serological tests andidentification of ellipsoidal and dark brownB. procyonis eggs (Kazacos 2001).
5.5.8 Control
Avoid contact with raccoons or their faeces andpractice good sanitary measures.
90 5 Nematode Zoonoses

5.6 Capillariasis
Superfamily: TrichuroideaFamily: Capillariidae
5.6.1 Etiology
The nematodes Capillaria hepatica, C. aerophilaand C. philippinensis are responsible for hepatic,pulmonary and intestinal capillariasis in man(Cross 1992). Out of these, C. philippinensisrelated intestinal capillariasis is most importantdisease in human beings.
5.6.2 Epidemiology
Epidemics due to C. philippinensis have beenreported from Philippine islands, Thailand andTaiwan (Cross 1992). In Philippines and Thai-land, more than 2,000 cases have been reported.
Sporadic cases have also been reported frommany other countries such as Korea, Japan,Taiwan, India, Iran, Egypt, Italy, United ArabEmirates, Spain and United Kingdom (Cross1998; El Hassan and Mikhail 1992; Austin et al.1999). Increasing number of cases of Intestinalcapillariasis are being reported from Asia (Hongand Cross 2005).
5.6.3 Reservoir
Fish-eating birds act as the reservoir hosts(Cross 1998) for intestinal capillariasis. Rodentsserve as reservoir for C. hepatica infections.
5.6.4 Transmission
Human beings become infected after consump-tion of tiny freshwater and brackish-water fish(Cross 1998).
Fig. 5.3 Life cycle of Baylisascaris procyonis
5.6 Capillariasis 91

5.6.5 Life Cycle
For C. philippinensis, fish act as intermediatehost and fish-eating birds or man are the defin-itive host for intestinal capillariasis (Bhaibulayaand Indra-Ngarm 1979; Cross and Basaca-Sevilla 1983). Human beings become infectedafter accidental consumption of the tiny fishwhich are normally consumed by birds.
5.6.6 Clinical Signs in Man
The symptoms of intestinal capillariasis includesevere enteropathy and abdominal pain, intermit-tent diarrhoea, weight loss and occasionally deathinhuman beings (Cross 1992,1998) if the cases arenot properly treated. Hepatic capillariasis couldresult in hepatomegaly, abdominal discomfort,diarrhoea, constipation etc. C. aerophila causespulmonary capillariasis and related symptoms.
5.6.7 Clinical Signs in Animals
C. hepatica capillariasis and C. aerophilacapillariasis can cause clinical disease in rodentsand foxes, respectively.
5.6.8 Diagnosis
The disease can be diagnosed by stool examina-tion. Capillaria spp. eggs should be differentiatedfromothercloselyrelatedspeciessuchasTrichurisand Trichinella. If eggs, larvae or adult ofC. philippinensis are not found in the stool sam-ples, biopsy specimens could help in the diagnosis.
5.6.9 Control
Avoid eating raw or undercooked fish in ende-mic areas.
5.7 Cutaneous Larva Migrans
Superfamily: Ancylostomatoidea
5.7.1 Common Name/Synonyms
Creeping eruption, serpiginous eruption, larvacurrens (Strongyloides spp. infection)
5.7.2 Etiology
Cutaneous larva migrans (CLM) occurs due tosubcutaneous migration of the nematode larvae,especially animal hookworms. The etiologicalagents include Ancylostoma braziliense, Ancy-lostoma caninum, Ancylostoma ceylanicum,A. tubaeforme, Uncinaria stenocephala orBunostomum phlebotomum. A. braziliense ismostly responsible for the occurrence of diseasein human beings (Caumes 2000). Many otherparasites such as Strongyloides papillosus,S. westeri, S. stercoralis, S. procyonis andS. myopotami can occasionally cause a similardisease but they move more rapidly than animalhookworms. Moving Gnathostoma spinigerumand Dirofilaria repens could also cause a similartype of dermatitis.
5.7.3 Epidemiology
A. braziliense is endemic in tropical and sub-tropical areas, whereas A. caninum and B. phle-botomum more commonly occur in temperateareas. Human cases have been reported acrossthe globe from many countries (Shinkar et al.2005; Yoshida et al. 1973). Travellers visitingendemic areas are at particular risk of theinfection.
92 5 Nematode Zoonoses

5.7.4 Reservoir
Carnivorous animals act as reservoir for theinfection.
5.7.5 Transmission
Human beings become infected due to penetra-tion of the parasite larvae present in the soilcontaminated by infected animal faeces.
5.7.6 Life Cycle
In carnivorous animals, the larvae present in thesoil penetrate the skin and migrate through thetissue to reach small intestine of the host wherethey mature into adults. In human beings, althoughlarva penetrates and migrates through skin, but itdo not develop further and cause the disease.
5.7.7 Clinical Signs in Man
These migrating larvae produce erythematous,serpiginous, pruritic, cutaneous track also knownas creeping eruption (Caumes et al. 2002;Beaver 1956; Bryceson and Hay 1998; Lucchinaand Wilson 1999) due to percutaneous penetra-tion and subsequent migration of larvae of manynematode parasites (Knight 2003).
5.7.8 Clinical Signs in Animals
The disease occurs in carnivorous (dogs and cat)animals. The symptoms include diarrhoea,anaemia and allergic dermatitis.
5.7.9 Diagnosis
The disease can be diagnosed by clinicalsymptoms, successful treatment or by histopa-thological confirmation (Purdy et al. 2011).
5.7.10 Control
For prevention and control, one should not walkbarefoot and use a mattress while lying in sandyareas particularly in disease endemic tropicaland subtropical areas.
5.8 Dioctophymosis
Superfamily: DioctophymatoideaFamily: Dioctophymidae
5.8.1 Common Name/Synonyms
Dioctophymiasis
5.8.2 Etiology
Dioctophymosis occurs due to Dioctophymarenale, a large nematode also known as the giantkidney worm (Soulsby 1978; Bowman 1999).
5.8.3 Epidemiology
The parasite has been reported across the globebarring Africa and Oceania (Soulsby 1978;Freitas 1980; Kommers et al. 1999). The parasitebasically infects domestic and wild fish-eatingcarnivores (Soulsby 1978; Maxie 1993;Bowman 1999; Nakagawa et al. 2007) but hasthe ability to cause the disease in human beings(Sun et al. 1986; Acha and Szyfres 2006).Among domestic animals, the parasite is morecommonly found in dogs than cats, horses andcattle (Maxie 1993; Nakagawa et al. 2007). Theadult parasite is usually found in kidney but canalso occur in abdominal cavity, uterus, ovary,mammary gland, urethra, subcutaneous tissuesof the inguinal region and mesenteric lymphnodes (Freitas 1980; Maxie 1993).
5.7 Cutaneous Larva Migrans 93

5.8.4 Reservoir
The mink (Mustela vison) is considered to be themain reservoir and definite host (Bowman1999), and humans and dogs are thought to beterminal or accidental hosts (Acha and Szyfres2006; Nakagawa et al. 2007).
5.8.5 Transmission
Human beings become infected after eatinginfected raw fish, frogs or by drinking watercontaminated with the mud-worm infected byD. renale in its larval form.
5.8.6 Life Cycle
The life cycle of the parasite involves differentkind of hosts (Soulsby 1978; Freitas 1980;Bowman 1999). The eggs of the parasite arepassed in the urine and are ingested by interme-diate hosts viz. mud-worms (aquatic oligochae-tes). The nematode develop into third stage larva(Freitas 1980) in mud worms and then these areeaten by fishes or frogs which act as paratenichosts and the larvae become ingested in tissuewithout further development (Bowman 1999).Wild fish eating carnivores act as the definite hostsand become infected after consuming infectedintermediate or paratenic host (Soulsby 1978;Bowman 1999). The larva migrates to the kidneyin the definitive host (Freitas 1980; Bowman1999; Nakagawa et al. 2007).
5.8.7 Clinical Signs in Animals
In dogs, most cases generally remain asymp-tomatic (Soulsby 1978; Maxie 1993) or theclinical signs are not conclusive for the defini-tive diagnosis of the disease. Right kidney andabdominal cavity are more commonly affectedin case of dogs (Freitas 1980; Maxie 1993;
Bowman 1999; Kommers et al. 1999). Theinfection could lead to renal parenchyma atro-phy, dilation of the renal pelvis and urethralobstruction (Soulsby 1978; Maxie 1993). Othersigns such as renal failure, haematuria, abdom-inal distention and peritonitis may also beobserved.
5.8.8 Clinical Signs in Man
The parasitic infection could lead to similar kindof symptoms in man.
5.8.9 Diagnosis
The disease can be diagnosed using imagingtechniques such as radiology (Nakagawa et al.2007), sonography (Soler et al. 2008) anddetection of parasite ova or eggs (Birchard andSherding 1994) in the urine. Postmortem-baseddetection of the parasite is another method rou-tinely employed for detection of the parasite(Pereira et al. 2006).
5.8.10 Control
Avoid consumption of raw or undercooked fishand frog or water contaminated with infectedmud worms.
5.9 Dracunculiasis
Class: SecerenteaSuborder: CamallinidaSuperfamily: Dracunculoidea
5.9.1 Common Name/Synonyms
Guinea worm disease, Dracontiasis
94 5 Nematode Zoonoses

5.9.2 Etiology
The disease occurs due to guinea wormDracunculus medinensis, one of the longest tis-sue nematode which can infect human beings.
5.9.3 Epidemiology
The parasite was prevalent in southern Asia andNorth, West and East Africa for past two dec-ades (Tiben and Hopkins 2006). After the end of2007, the disease remains endemic only in fewcountries viz. Sudan, Ghana, Mali and Niger dueto successful implementation of dracunculiasiseradication programme (Hopkins et al. 2008).
5.9.4 Reservoir
Human being acts as the reservoir ofD. medinensis.
5.9.5 Transmission
Human beings become infected after drinkingwater from stagnant ponds, pools, cisterns oropen wells containing fresh water copepods(Cyclops or water fleas) harbouring infectivelarvae of the parasite (Tiben and Hopkins 2006).
5.9.6 Life Cycle
The first stage larvae are released by femaleworm when they emerge from the human body.The released larvae remain in the water and areingested by an intermediate host, copepod.Larvae develop into third stage in the copepod(Cairncross et al. 2002; Muller 1971). Humanbeings become infected after drinking watercontaining infected copepods. In human beings,gastric juices digest the vector and release larva.The larvae migrate through thoracic cavity and
enter connective tissues to reach maturity. Mat-ing occurs, female continue their developmentand emerge from lower part of the human body(Karam and Tayeh 2006). Blister formationoccurs and female worm releases thousands oflarvae after contact with cold water (Muller1971) (Fig. 5.4).
5.9.7 Clinical Signs in Man
In human beings, the symptoms start with theformation of cutaneous blister. There is intenseburning sensation and symptoms could extend toerythema, urticarial rash, intense pruritus, nau-sea and vomiting, diarrhoea, dyspnoea, giddi-ness and syncope (Muller 1971). After the blisterbursts, symptoms start to disappear slowly. If thelarvae are released inside the joint, it may lead tosevere arthritis and ankylose.
5.9.8 Clinical Signs in Animals
Clinical manifestations are similar as in man.Few presumed zoonotic cases have been reportedin Japan, Korea and Indonesia, where disease isnot endemic and these infections might haveoccurred from animal reservoirs (Hashikura1927; Kobayashi et al. 1986; Van Heutsz 1926).Possibly, the infection occurred after consump-tion of raw freshwater fishes as paratenic hosts(Cairncross et al. 2002). Emerging female wormshave also been recovered occasionally from awide range of mammals from both endemic andnon-endemic areas (Cairncross et al. 2002).
5.9.9 Diagnosis
The disease can be diagnosed from the clinicaland allergic symptoms or using immunodiag-nostic/serological tests (Bloch et al. 1993, 1998;Bapna and Renapurkar 1996).
5.9 Dracunculiasis 95

5.9.10 Control
The ponds and shallow or step wells are theimportant sources of the disease. The provisionof clean drinking water is a must for preventionand control of the disease.
5.10 Gnathostomiasis
Superfamily: SpiruroideaFamily: Gnathostomatidae
5.10.1 Common Name/Synonyms
Gnathostomiasis, larva migrans (Gnathostoma)
5.10.2 Etiology
Gnathostomiasis is important food-borne zoono-sis of public health significance. The diseaseoccurs due to 12 species of Gnathostoma(Guitierrez2000;HermanandChiodini2009).Outof these, 4 species have been recorded in humanbeings viz. G. spinigerum (reported from wild anddomestic cats and dogs in India, China, Japan andsoutheast Asia), G. hispidum (reported from wild
and domestic pigs in Europe, Asia and Australia),G. doloresi (reported from wild boars) andG. nipponicum (reported from weasels in Japan)(Guitierrez 2000; Herman and Chiodini 2009).
5.10.3 Epidemiology
The disease is endemic in Japan, Thailand andparts of Southeast Asia (Rusnak and Lucey 1993).The disease has also been reported from Centraland South America, Cambodia, Laos, Myanmar,Indonesia, Philippines, Malaysia, China, SriLanka and India (Rusnak and Lucey 1993).
5.10.4 Reservoir
In endemic areas, cats, dogs and pigs can serveas important reservoirs of infection (Daensvang1980; Moore et al. 2003),
5.10.5 Transmission
Human beings become infected after consump-tion of raw or undercooked infected freshwaterfish or snakes, frogs, chickens and pigs. Inges-tion of water containing infected copepod
Fig. 5.4 Life cycle of Dracunculus medinensis
96 5 Nematode Zoonoses

is another important risk for the infection(Daengsvang 1981).
5.10.6 Life Cycle
The adult parasites live in the stomach wall of fishconsuming carnivores and shed the eggs in theirfaeces. When eggs are shed in freshwater, firststage swimming larvae form which are consumedby first intermediate host small crustaceancyclops. Fish consume these hosts and infectivelarvae develop in fish muscle tissue as L3 larvae. Indefinitive host, adult parasite develops after con-sumption of infected fish. For G. spinigerum, feralcats and dogs mainly act as definitive host, butinfections have also been recorded from tigers,leopards, lions, racoons, minks, opossums andotters (McCarthyandMoore2000).Human beingsaccidentally become infected after consumptionof infected fish. Additionally, pigs, frogs, snails,chickens and snakes can also act as intermediatehosts (McCarthy and Moore 2000) (Fig. 5.5).
5.10.7 Clinical Signs in Man
The symptoms include malaise, fever, urticaria,anorexia, nausea, vomition, diarrhoea, and epi-gastric pain (Rusnak and Lucey 1993). Theparasite migrates through skin and subcutaneoustissue leading to painful swelling and cutaneousgnathostomiasis (Rusnak and Lucey 1993).Occasionally, parasite may migrate to othervisceral organs and could lead to pulmonary,ocular, genitourinary, gastrointestinal, auditoryand central nervous gnathostomiasis with fatalconsequences (Rusnak and Lucey 1993).
5.10.8 Clinical Signs in Animals
In their respective definitive hosts, the parasiteproduces clinical symptoms. Necrotic tunnels invisceral organs (such as liver, pancreas),abdominal tissues and peritonitis can occur incat and dogs due to G. spinigerum infections
(Acha and Szyfres 2006). Stomach ulcers andother abdominal symptoms could also be seen inpigs infected with G. hispidum and G. doloresi(Acha and Szyfres 2006).
5.10.9 Diagnosis
Clinical signs, history and serological tests canhelp in diagnosis of the disease.
5.10.10 Control
Avoid eating raw or undercooked intermediatehosts such as fish, snakes, frogs, chicken etc. anddrink clean water. Freezing of meat to -20 �Cfor 3 to 5 days can also render meat safe forconsumption (Herman and Chiodini 2009).
5.11 Gongylonemosis
Order: SpiruridaSuperfamily: SpiruroideaFamily: Thelaziidae
5.11.1 Common Name/Synonyms
Gongylonematosis
5.11.2 Etiology
The disease primarily occurs due to Gongylo-nema pulchrum, Molin 1857, a spiuroid nema-tode although many other species ofGongylonema, could also affect mammals andbirds (Soulsby 1982; Yamaguti 1961; Cappucciet al. 1982). Ruminants, pigs and wild boar arethe main definitive hosts of this parasite, but ithas also been reported from nonhuman primates,carnivores and rodents. Human beings becomeaccidentally infected after ingestion of interme-diate host or drinking contaminated water.
5.10 Gnathostomiasis 97

5.11.3 Epidemiology
Although a rare zoonosis, but the disease inhumans is wide in distribution. More than 50human cases have been reported from China,Middle East, Australia, Italy, United States,Europe, Sri Lanka, New Zealand, Japan andSoutheast Asia (Wilde et al. 2001; Cappucciet al. 1982).
5.11.4 Reservoir
Existence of large number of definitive andintermediate hosts serves as source of infection.
5.11.5 Transmission
Accidental ingestion of small beetles possiblythrough contaminated salad and vegetablescould serve as source of infection in man.
5.11.6 Life Cycle
Approximately fifty species of arthropodcoprophagous insects such as dung beetles,cockroaches, etc. act as intermediate hosts forG.pulchrum (Cappucci et al. 1982; Illescas-Gomez et al. 1988; Soulsby 1965). Embryo-nated eggs are shed in the faeces of definitive
Fig. 5.5 Life cycle of Gnathostoma spinigerum
98 5 Nematode Zoonoses

host and they are further consumed by inter-mediate hosts. The third stage larva develops inthe intermediate host. Definitive hosts becomeinfected after ingestion of these intermediatehosts, whereas swine mostly become infecteddue to coprophagia (Wilde et al. 2001;Cappucci et al. 1982).
5.11.7 Clinical Signs in Man
In human beings, sensation occurs due to themovements of the worm. The parasite can pro-duce irritation in buccal mucosa, and occasion-ally may cause bloody expectoration, tarrystools, numbness of tongue, pain in chest andabdomen, vomiting, bloating, pharyngitis andstomatitis (Cappucci et al. 1982; Kudo et al.2008). Association between oesophageal squa-mous cell carcinoma and gongylonemosis hasalso been reported (Bleier et al. 2005).
5.11.8 Clinical Signs in Animals
In animals, the lesions include mild or chronicinflammatory changes in the affected parts. Theinfection may also lead to occlusions of theoesophagus due to reflex action produced byirritation.
5.11.9 Diagnosis
The disease can be diagnosed by history ofmoving worm followed by further parasiteidentifications.
5.11.10 Control
Improved personnel and environmental hygienecan help to prevent the disease.
5.12 Lagochilascariosis
Order: AscarididaSuperfamily: Ascaridoidea
5.12.1 Etiology
There are five species of genus Lagochilascaris:L. minor, L. major, L. buckleyi, L. turgida andL. sprenti (Leiper 1909; Sprent 1971). The humandisease occurs due to the nematode L. minor (Pacoet al. 1999).
5.12.2 Epidemiology
L. minor lagochilascariosis is present in Neo-tropical areas (from Mexico to Brazil), Uruguay(Sakamoto and Cabrera 2002). It is an emergingzoonotic disease in Brazil (Fraiha et al. 1989;Barbosa et al. 2006; Prudente et al. 2008; Freire-Filha et al. 2001). Rural and low socioeconomicstatus populations are at the high risk of infec-tion in endemic areas.
5.12.3 Reservoir and Transmissionof the Disease
Natural reservoirs and transmission of the dis-ease are not clear. Ingestion of embryonatedeggs released by another species might be thecause of disease in man.
5.12.4 Life Cycle
Albeit, the life cycle is not fully understood,but there is strong belief that cats act as thedefinitive host for this parasite. The adultworms are present in the upper portion of the
5.11 Gongylonemosis 99

respiratory or digestive tract and eggs are pas-sed through faeces of the cat. Synanthropic ratsand other rodents ingest the infective eggscontaining third stage larvae and act as theintermediate hosts for this parasite. Further,larvae hatch in the intermediate host andmigrate to different organs such as liver, lungsand form cysts in the muscle and subcutaneoustissue (deMoura et al. 2012; Campos et al.1992; Volcan et al. 1992). Humans and thecanids, act as accidental hosts after consump-tion of raw or undercooked infected rodentmeat (Campos et al. 1992). Rodents (Paco et al.1999) capybara (Hidrochaeris hidrochaeris)and agouti (Dasyprocta aguti) are particularlyimportant. The developmental stages could befound in cat or other accidental definitive hosts(Leão et al. 2005).
5.12.5 Disease in Man
Important clinical signs in humans include puru-lent subcutaneous tissue abscess in ear, neck, jaw,orbit, mastoid process, head and presence of eggs,larval and adult parasites in retropharyngeal tissue(Leiper 1909; Olle-Goig et al. 1996; Moncadaet al. 1998). In rare cases, the parasite may affectpulmonary tissue or central nervous system(Rosemberg et al. 1986; Veloso et al. 1992)leading to death (Sakamoto and Cabrera 2002).
5.12.6 Disease in Animals
The symptoms in the definitive host are notmuch clear. Two reported cases in cat revealedpresence of fistulated abscesses (deFreitas et al.2008; Amato et al. 1990).
5.12.7 Diagnosis
The disease can be diagnosed by identificationof eggs in the faeces or from identification of theparasite in affected lesions.
5.12.8 Control
No specific control measures are known for thisdisease.
5.13 Mammomonogamus
Order: StrongylidaSuperfamily: StrongyloideaFamily: Syngamidae
5.13.1 Common Name/Synonyms
Syngamiasis
5.13.2 Etiology
The disease occurs due to Mammomonogamuslaryngeus (Syngamus laryngeus). This parasiteis generally present in laryngotracheal region ofcattle and some other bovines (Gutierrez 1999;Anderson et al. 1980). The other parasiteM. nasicola is present in nasal fossa of bovids.These parasites are found in the larynx of cattle(Anderson et al. 1980) and are found rarely inhuman beings (Beaver et al. 1984).
5.13.3 Epidemiology
More than 100 human infections due toM. larygeus (Gutierrez 1999; Nosanchuk et al.1995; da Costa et al. 2005; Angheben et al.2009) have been reported from different coun-tries such as Caribbean Islands, South America(especially Brazil), Australia, Canada, the Uni-ted States, France, United Kingdom (Cunnacet al. 1988), Philippines (Beaver et al. 1984),Thailand (Pipitogool et al. 1992), Italy (Anghe-ben et al. 2009) and Korea (Kim et al. 1998).The parasite is mainly found in the Caribbeanand South America and other cases have beenreported from tourists visiting these areas(da Costa et al. 2005).
100 5 Nematode Zoonoses

5.13.4 Reservoir
Ruminants act as reservoirs for M. laryngeus andM. nasicola.
5.13.5 Transmission
The transmission cycle of the parasite is notclearly known. It is thought that infection occurseither after ingestion of embryonated egg, hat-ched larvae or paratenic host such as earth-worms, snails, or arthropods. Contaminated rawvegetables or drinking water could also serve asa source of infection.
5.13.6 Life Cycle
Life cycle of the parasite is not fully understoodbut it is assumed that it penetrates the intestinalwall and then migrates to the tracheolaryngealregion through the body (Gutierrez 1999; Severoet al. 1988). The eggs are produced by theparasite in the tracheal mucosa, which areswallowed and are then passed through thefaeces.
5.13.7 Clinical Signs in Man
The symptoms primarily include chronic cough,fever and occasionally hemoptysis. Addition-ally, parasite may cause irritation of the larynxand asthma.
5.13.8 Clinical Signs in Animals
The disease is not symptomatic in animals.Ruminant infections have been recorded fromtropical America, Africa, India, Malaysia, Viet-nam and Philippines (Acha and Szyfres 2003).
5.13.9 Diagnosis
The disease can be diagnosed by brochoscopicor expectorated identification of the parasite(Gutierrez 1999). Eggs may also be seen insputum or faeces of infected persons.
5.13.10 Control
Improved personnel hygiene can help preventinfection in human beings.
5.14 Micronemosis
Order: RhabditidaSuperfamily: Rhabditoidea
5.14.1 Etiology
The disease occurs due to Micronema deletrix(Synonym: Halicephalobus gingivalis), a smallfree living nematode. The parasite is mostcommonly found in brain but could be found inkidneys, oral and nasal cavities, lymph nodes,spinal cord and adrenal glands (Spalding et al.1990; Rames et al. 1995).
5.14.2 Epidemiology
Micronemosis has been reported from UnitedStates (Anderson and Bemrick 1965; Rubin andWoodard 1974; Alstad et al. 1979; Simpsonet al. 1988), Switzerland (Pohlenz et al. 1981)and Netherlands (Keg et al. 1984) in horses.
5.14.3 Reservoir
This parasite is found in close association withdecaying humus (Anderson and Bemrick 1965;
5.13 Mammomonogamus 101

Poinar 1983). The opportunistic parasitedepends for food on bacteria, but may becomeindependent for its development (Poinar 1983).
5.14.4 Transmission
The route of transmission is not fully understoodbut it is believed to be through contamination oforal or nasal wounds, due to common parasiteinfestation of these sites. The manure contami-nation of cutaneous lacerations or decubitalulcers was also found responsible for two humancases with CNS involvement (Gardiner et al.1981; Rames et al. 1995).
5.14.5 Life Cycle
M. deletrix is a facultative parasite of man andanimals as all the developmental stages havebeen found in the environment outside the bodyof human and animal hosts (Shadduck et al.1979; Acha and Szyfres 2003).
5.14.6 Clinical Signs in Man
In humans, three cases of M. deletrix microne-mosis responsible for parasitic meningoenceph-alitis have been recorded in Canada (Hoogstratenand Young 1975) and the United States(Shadduck et al. 1979; Gardiner et al. 1981).
5.14.7 Clinical Signs in Animals
Among horses, the parasite was found to causeinfection in nasal passages, lung, lymph nodes,stomach, maxillae, mandible, brain, kidney,adrenal glands and femur (Gordon et al. 1990).
5.14.8 Diagnosis
The diagnosis can be done at the time of post-mortem using histological examination of theaffected organs.
5.14.9 Control
Improved personnel hygiene can help preventinfection in human beings.
5.15 Oesophagostomiasis
Order: StrongylidaSuperfamily: StrongyloideaFamily: Trichonematidae
5.15.1 Common Name/Synonyms
Esophagostomiasis, Ternidensiasis
5.15.2 Etiology
Oesophagostomiasis occurs due to strongylidintestinal parasites Oesophagostomum bifurcum,O. stephanostomum, O. aculeatum and Terni-dens derminutus of non-human primates andhumans (Remfry 1978; McCarthy and Moore2000). Out of these, O. bifurcum was considereda rare zoonosis. The zoonotic potential ofO. bifurcum is still not fully understood. Recently,epidemiological, molecular and morphologicalstudies on O. bifurcum from humans and variousmonkeys clarified that different strains ofO. bifurcum are prevalent in humans and monkeysand they are specific to their respective hostsindicating a non-zoonotic transmission betweenthese species (Polderman et al. 2010). However,another study carried out in western Ugandaindicates that O. bifurcum are prevalent in chim-panzees which have potential for zoonotic trans-mission of these species (Krief et al. 2010).
5.15.3 Epidemiology
O. bifurcum is widely prevalent in West Africa,but a few cases have also been reported fromother parts of Africa, Asia and South America(Bogers et al. 2001).
102 5 Nematode Zoonoses

5.15.4 Reservoir
Non-human primates are thought to be theimportant reservoir hosts.
5.15.5 Transmission
Humans become infected after ingestion ofinfective larvae from soil contaminated withfaeces of non-human primates.
5.15.6 Life Cycle
Humans or primates become infected afteringestion of L3 larvae. The larvae penetratecolon and some of these larvae develop andreturn to the bowel lumen, while others becomeimmature worms and lead to formation ofabscess in the bowl lumen. Adult mature wormsmate and shed eggs in the faeces. The eggs hatchin soil and develop from L1 to L3 infectivelarvae (Polderman and Blotkamp 1995).
5.15.7 Clinical Signs in Manand Animals
Most of the times, infections are not symptom-atic. Two forms of the disease viz. multinodularand uninodular (Dapaong tumour) can occur(Polderman and Blotkamp 1995). Clinical signsinclude ‘Dapaong tumour’, named after thecapital of Togo’s northernmost province. In thisan inflammatory mass develop around juvenileworms in the colonic wall or abdominal cavity.Adhesions develop around the abdominal walland this may lead to occasional obstruction ofcolon (Storey et al. 2000; Polderman et al.1999). Heavy infections can lead to diarrhoea,weight loss, weakness and death in man.
5.15.8 Diagnosis
The disease can be diagnosed after parasiticidentification and stool culture on stool charcoalmixture (Polderman et al. 1991), PCR–RFLPand Random Amplified Polymorphic DNA—Gel—electrophoresis.
5.15.9 Control
Improved personnel hygiene, chemotherapy ofinfected animals can help control the infection.
5.16 Strongyloidiasis
Order: RhabditidaSuperfamily: RhabditoideaFamily: Strongyloididae
5.16.1 Common Name/Synonyms
Strongyloidiasis, threadworm infection
5.16.2 Etiology
The disease occurs due to the parasite Strongy-loides stercoralis and S. fuelleborni. Role of theanimal hosts dogs and cats for S. stercoraliszoonotic infections is not clearly understood. It isbelieved that they might be contributing to humaninfections in some parts of the world. The zoo-notic potential of S. fuelleborni is believed to bemuch higher than S. stercoralis. It mainly infectsnon-human primates but can cause zoonotic dis-ease in Africa and Southeast Asia or at least have azoonotic origin (Ashford and Barnish 1989; Olsenet al. 2009). Other Strongyloid infections can alsocause dermatitis in man which can be zoonotic innature.
5.15 Oesophagostomiasis 103

5.16.3 Epidemiology
S. stercoralis infections could be seen across theglobe but is particularly endemic in tropical andsubtropical areas viz. Southeast Asia, sub-SaharanAfrica, Latin America, and the south-easternUnited States (Berk et al. 1987). The parasite isbelieved to be affecting 100–200 million personsworldwide (Genta 1989). S. fullerborni infectionsoccur in non-human primates of Africa and Asia.S. stercoralis infection can occur for very longperiods of time due to the ability of the parasite tocause autoinfection which result in persistentchronic infections (Grove 1996). Poor sanitaryconditions are important factor for S. stercoralisinfections (Hall et al. 1994).
5.16.4 Reservoir
Humans are reservoir for S. stercoralis infec-tions. For S. fuelleborni infections, African andAsian simians serve as important reservoirs.
5.16.5 Transmission
The disease occurs through direct skin contactwith contaminated soil particularly in agricul-tural and recreational activities.
5.16.6 Life Cycle
The parasite has both free-living and parasiticstages. The female parasite present in the smallintestine lays eggs in the intestinal mucosa. Theeggs develop into larvae and are shed in the fae-ces. In suitable environment, larvae develop intoinfective filariform larvae or develop into free-living adults. The sexual reproduction of theparasite occurs in the free-living adult stage (Neva1994). The parasite generally enters the humanbody through cutaneous route, enters the blood-stream and reaches through lungs finally to thegastrointestinal tract (Keiser and Nutman 2004).
5.16.7 Clinical Signs in Man
The infection primarily remains asymptomatic(Grove 1989) but can cause symptoms related tocutaneous (pruritus, urticaria), respiratory(cough, chronic bronchitis) and intestinal(abdominal pain, intermittent or persistent diar-rhoea) systems. However, in immune compro-mised individuals, the parasite can cause afulminant fatal disease (Keiser and Nutman2004) viz. hyperinfection (uncontrolled multi-plication) and dissemination of larvae to all thevisceral organs (Olsen et al. 2009).
5.16.8 Clinical Signs in Animals
The disease in dogs and cats is not long lastingand generally infects young puppies. The symp-toms are self limiting and generally resemble asin healthy human beings. Among non-humanprimates, mild to severe haemorrhagic diarrhoeacould occur particularly in young or weakenedanimals (Acha and Szyfres 2003).
5.16.9 Diagnosis
The parasite can be detected using faecal con-centration or culture techniques (Cheesbrough1987). Immunological tests such as Western blot,ELISA and IFAT can also be used in the diag-nosis (Silva et al. 2003; Rodrigues et al. 2007).
5.16.10 Control
Proper disposal of human faeces, treatment ofinfected persons and using protective measuresin endemic areas can help control the disease.
5.17 Thelaziasis
Order: SpiruridaSuperfamily: SpiruroideaFamily: Thelaziidae
104 5 Nematode Zoonoses

5.17.1 Common Name/Synonyms
Oriental eye-worm, thelaziasis, eye worminfections, conjunctival spirurosis
5.17.2 Etiology
Thelazia callipaeda is a helminth responsible forcausing eye infection in humans and animalssuch as domestic cats and dogs (Otranto andEberhard 2011). T. callipaeda causes insect-borne zoonosis in man. Some other species suchas T. californiensis and T. rhodesii could alsocause the disease.
5.17.3 Epidemiology
Among humans, the parasite is distributed inerstwhile Soviet Union and Asian countries suchas China, Korea, Japan, Indonesia, Thailand,Taiwan and India (Otranto and Eberhard 2011).More than 157 cases have been reported acrossthe globe in addition to 100 cases reported fromJapan (Koyama et al. 2000; Kitano et al. 1996;Singh and Singh 1993). Children and old personare at higher risk of being infected. The parasiteis also widespread in domestic and wild animalsin Asia, Italy, France and Germany (Miyazaki1991; Otranto et al. 2003a; Kosin et al. 1989;Shen et al. 2006; Sohn et al. 2011).
5.17.4 Reservoir
Domestic and wild mammals serve as importantreservoirs of disease.
5.17.5 Transmission
The disease is transmitted by secretophagous flieswhich deposit it in the eye orbit of human beings(Otranto and Traversa 2005) and other animals.
5.17.6 Life Cycle
The secretophagous flies play central role intransmission of this disease. These flies feed onthe lachrymal secretions of man and other infec-ted animals and thus ingest first stage larvae in theprocess. The third stage larva develops in the flyand is deposited back into the orbit of the eye.
5.17.7 Clinical Signs in Man
Clinical signs in man include lachrymation,epiphora, conjunctivitis, keratitis and cornealulcers in severe cases (Anderson 1992).
5.17.8 Clinical Signs in Animals
Domestic dogs, cats and wild carnivores (e.g.foxes, wolves and wild cats) are primarilyaffected (Otranto et al. 2009). Symptoms aregenerally similar as in the human infections.
5.17.9 Diagnosis
The disease can be diagnosed after removal ofthe worm from the eye followed by morpho-logical identification of the parasite (Otrantoet al. 2003b).
5.17.10 Control
Avoidance of eye contact with intermediatehosts can prove beneficial for prevention of thedisease.
5.18 Trichinosis
Order: EnoplidaSuperfamily: TrichuroideaFamilly: Trichinellidae
5.17 Thelaziasis 105

5.18.1 Common Name/Synonyms
Trichinellosis, Trichiniasis, Trichinelliasis
5.18.2 Etiology
The disease occurs due to the parasites of genusTrichinella. At present, two clads are recognised:One that contain species which encapsulate inhost muscle cell (T. spiralis, T. nativa, T. britovi,T. murrelli, T. nelsoni and Trichinella T6, T8, T9and T12) and second that do not encapsulate inhost muscle cell (T. psudospiralis, T. papuae,T. zimbabwensis). All the species present in thefirst clad only infect mammals, whereas in sec-ond clad, T. pseudospiralis infects mammals andbirds; and T. papuae, T. zimbabwensis both infectmammals and reptiles (Gajadhar et al. 2009).
5.18.3 Epidemiology
The parasite causes serious zoonosis and as manyas 11 million people may be infected (Dupouy-Camet 2000). Numerous outbreaks of trichinel-losis have been reported in different parts of theworld (Dupouy-Camet 2000). Trichinella infec-tion has been reported in domestic (mainly pigs)and wild life species of 43 and 66 countries,respectively (Pozio 2007). Trichinellosis is aworldwide prevalent nematode zoonotic diseaseof medical, veterinary and economic significance(Dupouy-Camet 2000). Trichinella is one of themost wide spread parasites infecting people andother mammals across the globe in most climates,except for deserts (Dupouy-Camet 2000).Domestication of pigs some 10,000 years ago inAsia created a permanent reservoir of parasitesfor humans, limited by the use of fire and Mosaiclaws (Dupouy-Camet 2000). Trichinellosis sig-nificantly impact national economies due to rea-sons of public health, socioeconomics and trade(Todd 1989; Roberts and Murrell 1993; Ortega-Pierres et al. 2000). The occurrence of significanttransmission from scavenged animal carcasses
suggests that environmental temperature andhumidity play an important role in the transmis-sion of Trichinella among wild life (Pozio 2000).Environmental contamination with Trichinella-infected meat scraps could lead to infectionamong herbivores, particularly in horses (Pozio2000). Unhygienic slaughtering of food animals,roaming behaviour of stray pigs, lack of struc-tured meat inspection, commonly used garbageand kitchen practices for pigs, free access of dogsand cats to slaughter houses, socioeconomicconditions, culinary habits etc. undoubtedlyenhances perpetuation of the transmission cycle.
5.18.4 Reservoir
Wild boar or other animals are important reser-voirs of infection.c
5.18.5 Transmission
Consumption of raw or undercooked pork orwild boar meat is important source for trans-mission of the disease in man.
5.18.6 Life Cycle
Trichinella spp. can complete its life cycle in asingle host. After ingestion of infected meatcontaining first stage infective larvae, digestionof meat in the stomach releases larva whichmature in small intestine in few days (Gajadharet al. 2006) (Fig. 5.6).
The adult female starts shedding larvae. Thelarvae enter blood circulation and reach skeletalmuscles and encapsulate and usually live therefor 3–5 years or more (Gajadhar et al. 2006).The infected meat when consumed by anotherhost restarts the life cycle of the parasite. Highnumbers of Trichinella larvae are present indiaphragm, tongue and massetar muscles(Gajadhar et al. 2006).
106 5 Nematode Zoonoses

5.18.7 Clinical Signs in Man
The number of larvae present, genotype involvedand host immunity determine the severity of dis-ease in man. Clinical signs vary from asymp-tomatic infections to diarrhoea, gastrointestinaldisturbances, periorbital and facial oedema,myalgia, fever, conjunctivitis, headache and skinrash (Gajadhar et al. 2006). In extreme cases, lifethreatening encephalitis, endocarditis, myocar-ditis may also be seen (Gajadhar et al. 2006).
5.18.8 Clinical Signs in Animals
The disease is generally asymptomatic in animals.Among animals, pigs, bear, canids, rodents, skunks,raccoon, walrus, opossum and seals can act as hosts.
5.18.9 Diagnosis
The disease can be diagnosed using trichinos-copy, Trichinella artificial digestion assay,serological, histological, bioassay and moleculartechniques. The digestion assay is more reliableand recommended test to trichinoscopy(Figs. 5.7, 5.8).
5.18.10 Control
Proper meat inspection practices, rodent control,avoiding garbage feeding to pigs, proper carcassdisposal can help control the disease.Consumption of properly cooked meat can avoidinfection in man (Gajadhar et al. 2006).
Fig. 5.6 Life cycle of Tichinella spiralis
5.18 Trichinosis 107

5.19 Trichostrongylosis
Order: StrongylidaSuperfamily: TrichostrongyloideaFamily: Trichostrongylidae
5.19.1 Common Name/Synonyms
Trichostrongyliasis
5.19.2 Etiology
There are several species of the genus which caninfect sheep, goat and bovines. For humaninfections, cases due to Trichostrongylus orien-talis, T. axei, T. colubriformis, T. skrjabini,T. vitrinus, T. probolurus, T. capricola, T. brevis,T. affinis and T. calcaraus have been recorded(Acha and Szyfres 2003).
Fig. 5.7 Numerous coiledinfective Trichinella larvaeseen using trichinelloscopy(with kind permission fromDr. Alvin A Gajadhar,Research Scientist cumHead, Center for Food-Borne and AnimalParasitology, CanadianFood Inspection AgencySaskatoon Lab, Canada)
Fig. 5.8 Coiled infectiveTrichinella larvaerecovered from horse meatusing pepsin HCl digestionassay (with kindpermission from Dr. AlvinA Gajadhar, ResearchScientist cum Head, Centerfor Food-Borne andAnimal Parasitology,Canadian Food InspectionAgency Saskatoon Lab,Canada)
108 5 Nematode Zoonoses

5.19.3 Epidemiology
The disease has been reported across the globe.Sporadic human cases have been reported fromAsian countries such as Thailand, South Korea,China, Laos; United States and Australia (Satoet al. 2011; Beaver et al. 1984; Boreham et al.1995; Panasoponkul et al. 1985; Yong et al.2007; Wall et al. 2011). Farmers and otherpersons involved in dairy farming are at risk ofbeing infected particularly in the developingworld and endemic areas (Adams et al. 2005).Among animals, high prevalence has beenrecorded in Asia and Middle East (Youn 2009;Giboda et al. 1991; Poirriez et al. 1984).
5.19.4 Reservoir
Herbivorous animals act as reservoirs for mostof the Trichostrongylus species.
5.19.5 Transmission
Human beings become infected after consump-tion of contaminated food and water particularlyin the places where animal faeces are used forsoil fertilisation.
5.19.6 Life Cycle
The host species releases eggs in the faeces.These eggs develop into first stage larva. Afterfeeding on organic matter, these larvae furtherdevelop into third stage larva which is infective tothe host. After ingestion of third stage larva, itmature into adult and start releasing eggs in thefaeces of the host.
5.19.7 Clinical Signs in Man
Disease generally remains asymptomatic but inhigh parasitemia, clinical symptoms may includeeosinophilia, bloating diarrhoea, abdominal pain,weight loss and some other abdominal disorders.
5.19.8 Clinical Signs in Animals
The disease is responsible for production lossesin animals.
5.19.9 Diagnosis
The disease can be diagnosed using identifica-tion of eggs followed by faecal culture so as toidentify larvae for species differentiation.
5.19.10 Control
For prevention and control of the disease, pas-ture management, stock rotation and regularde-worming of animals particularly in endemicareas should be practised. For human beings,improved personnel and environmental hygienecan help to prevent the disease.
5.20 Trichuriasis of Animal Origin
Order: EnoplidaSuperfamily: TrichuroideaFamily: Trichridae
5.20.1 Common Name/Synonyms
Whipworm disease, trichocephaliasis
5.20.2 Etiology
The zoonotic trichuriasis occurs due to Trichurisvulpis and Trichuris suis which can be occa-sionally present in intestine of man. Rarely,T. vulpis is responsible for causing VLM in man.T. vulpis primarily infects domestic and wildcanids, whereas T. suis causes infection indomestic pigs and wild boars. T. trichuria isanother parasite which could cause infection inman (Acha and Szyfres 2003).
5.19 Trichostrongylosis 109

5.20.3 Epidemiology
Both the parasites are distributed across theglobe. Malnourished 5–6 year old children intropical areas are at high risk of being infected(Márquez-Navarro et al. 2012).
5.20.4 Reservoir
Dogs, wild canids and swine could act asimportant reservoirs of infection.
5.20.5 Transmission
Trichuriasis of animal origin is a soil transmittednematode infection. The infection is transmitteddirectly through faecal oral route due to con-taminated soil or water.
5.20.6 Life Cycle
The animal or human host becomes infected afteringestion of infective eggs. After gastric passage,larvae are released in the small intestine from theseeggs. First stage larva reaches the large intestineand after multiple moults develops into the adults.
5.20.7 Clinical Signs in Man
The disease is mostly asymptomatic but diar-rhoea, dysentery, rectal prolapse, abdominalpain, vomiting, headache etc. may be seen inheavy infections.
5.20.8 Clinical Signs in Animals
The disease is generally asymptomatic but heavyinfections can cause symptoms related to gas-trointestinal system, such as diarrhoea and sec-ondary disease complications.
5.20.9 Diagnosis
The disease can be diagnosed by identificationof eggs in the faeces of the host.
5.20.10 Control
Improved personnel and environmental hygiene,proper disposal of excreta, hand washing, con-sumption of hygienic food and water can help toprevent the infection in children.
5.21 Visceral Larva Migrans
Order: AscarididaSuperfamily: AscaridoideaFamily: Ascarididae
Beaver et al. (1952) for the first time reportedmigration of Toxocara larvae to the liver. Afterthat, many cases of these larvae migrating toliver, lungs and other visceral organs have beenreported (Inoue et al. 2002; Roig et al. 1992;Morimatsu et al. 2006).
5.21.1 Common Name/Synonyms
Toxocariasis, Toxocarosis, Larval granulomato-sis, OLM.
5.21.2 Etiology
The human disease occurs due to the larvae ofToxocara sp. roundworms. The human diseaseoccurs due to Toxocara canis and T. cati. In addi-tion to these, T. vitulorum has also been recognisedas rare cause of this zoonosis. The zoonoticpotential of T. pteropodis is being questioned.T. canis toxocariasis is considered to be moreimportant than T. cati infections. For T. canis, dogsand some other canids act as definitive host,whereas cats act as definitive host for T. cati.
110 5 Nematode Zoonoses
5.21.3 Epidemiology
The disease is distributed across the globe andeggs have been found in soil from most parts ofthe world. High seroprevalences have beenrecorded from tropical countries.
5.21.4 Reservoir
Dogs act as important reservoir for humaninfections.
5.21.5 Transmission
The parasite normally affects young childrenafter accidental ingestion of infective eggs fromcontaminated soil, unwashed hands, contami-nated food and water or through ingestion of rawor undercooked tissues (particularly liver). Theinfection occurs through contamination of soiland direct contact with pets is not likely to causeinfection in human beings. Occurrence of casesafter ingestion of meat from quails, cows andchickens (Sakakibara et al. 2002) suggests itsimportance as food-borne parasitic zoonosis.
5.21.6 Life Cycle
The adult parasite sheds un-embryonated eggs inthe faeces of the definitive host. The eggs becomeinfective to third stage larvae within 7–14 days inthe environment under favourable conditions.The larvae enter the host through ingestion ofthird stage larvae present in the contaminated soilor water. The larvae hatch in the digestive systemand migrate towards the liver and then dissemi-nate to other organs, such as lungs and heart (Mok1968; Woodruff 1970). In definitive hosts, somelarvae again reach intestine through lungs anddevelop into adult worms and start releasing theeggs. For kittens, T. cati toxocariasis is nottransmitted in utero but can be transmittedthrough milk or colostrum (Fig. 5.9).
5.21.7 Clinical Signs in Man
The disease is generally not symptomatic.Clinical symptoms in man can be discussedunder four different forms viz. visceral or sys-temic, ocular, neural and covert toxocariasis(Acha and Szyfres 2003). In visceral form,symptoms could vary from asymptomatic tochronic eosinophilia, hepatomegaly, pneumoni-tis, fever and digestive disorders (Acha andSzyfres 2003). The ocular form could lead tovariety of symptoms such as retinal granulomas,retinal detachment, Keratitis and can cause lossof vision and blindness. Neurological form maylead to meningoencephalitis. The covert form isnot uncommon, and may produce symptomssuch as malaise, abdominal pain and eosino-phillia (Acha and Szyfres 2003).
5.21.8 Clinical Signs in Animals
Adult cat and dogs generally do not showsymptoms for the disease. Young puppies andkittens may show symptoms such as diarrhoea,vomiting and other digestive disturbances.
5.21.9 Diagnosis
The human infections can be diagnosed based onclinical signs, ophthalmoscopic examination,eosinophilia, other clinical pathology findings,serological tests, histologically or isolation oflarva (Aragane et al. 1999). The disease in ani-mal hosts can be diagnosed by detection of theeggs.
5.21.10 Control
For prevention and control, regular de-wormingof definitive hosts, especially their puppies andkittens must be done. Health education of per-sons in close contact with these animals shouldalso prove helpful.
5.21 Visceral Larva Migrans 111

5.22 Zoonotic Ancylostomiasis
Order: StrongylidaSuperfamily: AncylostomatoideaFamily: Ancylostomatidae
5.22.1 Common Name/Synonyms
Hookworm disease, necatoriasis, uncinariasis
5.22.2 Etiology
The disease occurs due to A. ceylanicum (catnematode) and A. caninum (dog nematode).
5.22.3 Epidemiology
Human infections are rare but have beenreported from many parts of the world. Theseparasites are endemic in India (Traub et al.2007, 2008, 2004) and south East Asia (Chooet al. 2000; Setasuban et al. 1976; Yoshidaet al. 1968). Detailed publications on humanancylostomiasis due to A. ceylanicum werepublished between the mid 1960s and early1970s (Anten and Zuidema 1964; Areekul et al.1970; Chowdhury and Schad 1972; Yoshidaet al. 1968). Recent studies by Ngui et al.(2012), Traub et al. (2008) revealed using thecombination of epidemiological, conventionaldiagnostic and molecular tools that A. ceylanicumis common in endemic areas particularly where
Fig. 5.9 Life cycle of Toxocara canis
112 5 Nematode Zoonoses

there is close contact between human and cat, dogpopulations. A. caninum is responsible for humaneosinophilic enteritis (EE) and has been reportedfrom Australia (Loukas et al. 1992; Croese et al.1994a; Landmann and Prociv 2003), UnitedStates (Khoshoo et al. 1995), Egypt (Bahgat et al.1999), Philippines, South America and Israel(Croese et al. 1994b). A. ceylanicum is able toproduce patent infections in human beings bothnaturally and experimentally (Ngui et al. 2012;Wijers and Smit 1966; Carroll and Grove 1986).Human infections due to A. ceylanicum have alsobeen reported from West New Guinea (Anten andZuidema 1964), Philippines (Velasquez andCabrera 1968), Taiwan (Yoshida et al. 1968),Thailand (Areekul et al. 1970; Traub et al. 2008;Jiraanankul et al. 2011), Laos (Sato et al. 2011)and India (Chowdhury and Schad 1972).
5.22.4 Reservoir
Dogs can act as reservoir hosts for humanhookworm infections.
5.22.5 Transmission
Ingestion of contaminated soil or food like veg-etables could transmit infection in human beings.
5.22.6 Life Cycle
The parasite A. ceylanicum has a direct life cycle.This parasite is present in small intestine of dogs,cats and humans. The infection occurs due toingestion or percutaneous migration of infectiousthird stage larvae from the soil. The host animalpasses un-embryonated eggs in the faeces after14 days of entry into the host (Yoshida et al.1974). The infectious larvae usually develop in2–8 days under favourable conditions.
5.22.7 Clinical Signs in Man
A. ceylanicum can develop into adult in humanbeings (Tu et al. 2008; Anten and Zuidema1964) and produces natural patent infectionscausing anaemia (Anten and Zuidema 1964;Velasquez and Cabrera 1968; Chowdhury andSchad 1972; Traub et al. 2008). A. caninumoccasionally reaches adulthood in humans(Landmann and Prociv 2003; Prociv and Croese1990; Croese et al. 1994a, b) and can causeeosinophilic enteritis (Prociv and Croese 1996).
5.22.8 Clinical Signs in Animals
Heavy infections due to A. ceylanicum can causediarrhoea, bloody and mucoid stool and irondeficiency anaemia (Carroll and Grove 1984) indogs. Migrating larva in heavy infections canaffect and cause symptoms in cutaneous, respi-ratory and intestinal systems.
5.22.9 Diagnosis
The disease can be diagnosed by identificationof parasite eggs, from clinical signs in animalssuch as anaemia (pale mucus membranes), roughhair coat, by use of serological tests such asELISA, western blot and molecular techniques(Sato et al. 2010).
5.22.10 Control
Control measures for non-zoonotic humanancylostomiasis such as prophylactic and thera-peutic treatment and improved sanitation foranimals also work well for control of zoonoticancylostomiasis.
5.22 Zoonotic Ancylostomiasis 113
5.23 Zoonotic Filariasis
Order: SpiruridaSuborder: FilariinaSuperfamily: Filariroidea
5.23.1 Common Name/Synonyms
Brugia malayi filariasis
5.23.2 Etiology
Many species of animal filariasis are reported tocause disease in man (Addario 1885; Gutierrez1990; Orihel and Ash 1995).
Zoonotic filariasis could primarily occur dueto the following etiological agents:1. Dirofilaria spp. viz. D. immitis, D. tenuis,
D. repens2. Onchocerca spp. viz. O. cervicalis,
O. gutturosa3. Brugia spp. viz. B. malayi, B. pahangi,
B. leporis4. Other species such as Loaina sp., Meningo-
nema sp., and some unidentified species
5.23.3 Epidemiology
Cases due to zoonotic filariasis have beenreported across the globe (Orihel and Eberhard1998; Thomas and Mark 1998). Zoonotic filari-asis has been reviewed in detail by Orihel andEberhard (1998). Different species of Brugiainfect animals such as tree shrews and monkeysin Southeast Asia, and raccoons and rabbits inthe United States (Eberhard 1984; Orihel 1966;Orihel and Pacheco 1966). Human infectionsdue to D. repens have been reviewed byPampiglione et al. (1995) and reported 400 casesfrom 30 countries in Europe, Asia and Africa.Most human infections have been reported fromtemperate zones (Orihel and Eberhard 1998).
5.23.4 Reservoir
Monkeys, cats and wild carnivores act as reser-voir for subperiodic brugiasis in Southeast Asia(Acha and Szyfres 2003). Other wild anddomestic animals might also act as reservoirs forthe disease.
5.23.5 Transmission
The disease is transmitted by the bite of bloodsucking insects such as mosquitoes belonging tothe genra Mansonia.
5.23.6 Life Cycle
Zoonotic filariasis is a vector borne disease andblood sucking insects act as biological vectors fortransmissionof thedisease.Theadultparasite livesin vertebrate host’s tissues. The female releasesembryos (microfilariae) which can be found inblood, lymph or skin. The vectors transmit theinfection by feeding previously on an animalinfected with a patent filaria infection (Anderson1992). The arthropod vector ingests microfilariaepresent in blood, lymph or skin. The microfilariaefurtherdevelopinto infectious thirdstage larvaandmigrate towards the mouthparts of the arthropod.The insect vector then transmits the infectionwhile feeding on another new vertebrate host.
5.23.7 Clinical Signs in Man
Brugia spp. infects lymphatic system and pro-duces symptoms such as lymphadenopathy andlymphangitis. Dirofilaria spp. generally infectsskin and subcutaneous tissue and produce rela-ted symptoms such as nodules and swellings.D. immitis can infect heart, pulmonary and otherblood vessels and produce related symptoms.
114 5 Nematode Zoonoses
5.23.8 Clinical Signs in Animals
The disease is generally asymptomatic but largenumber of parasites could pose problems such asstenosis of pulmonary vessels, obstruction in flowof blood.
5.23.9 Diagnosis
Blood smear examinations and Millipore filterconcentration techniques, PCR, ELISA can beused for diagnosis of parasites present in thehuman blood.
5.23.10 Control
Control of vector populations can help preventand control these infections.
References
Acha PN, Szyfres B (2003) Zoonoses and communicablediseases common to man and animals. Washington(DC): Pan American Health Organization; Scientificand Technical Publication No. 580
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals, vol III.Parasitosis. Published by Pan American HealthOrganization, USA
Adams VJ, Markus MB, Adams JF (2005) Paradoxicalhelminthiasis and giardiasis in Cape Town, SouthAfrica: epidemiology and control. Afr Health Sci5:276–280
Addario C (1885) Su un nematode dell’occhio umano.Ann Ottalmolog 13:135–147
Alicata JE (1991) The discovery of Angiostrongyluscantonensis as a cause of human eosinophilic men-ingitis. Parasitol Today 7:151–153
Alstad AD, Berg IE, Samuel C (1979) DisseminatedMicronema deletrix infection in the horse. J Am VetMed Assoc 174:264–266
Amato JF, Girsi L, Pimentel-Nato M (1990) Two cases offistulated abscesses caused by Lagochilascaris majorin the domestic cat. Mem Inst Oswaldo Cruz85(4):471–473
Anderson TJC (1995) Ascaris infections in humans fromNorth America: molecular evidence for cross-infec-tion. Parasitology 110:215–219
Anderson RC (1992) Nematode parasites of vertebrates,their development and transmission. CAB Interna-tional, Wallingford
Anderson RV, Bemrick WJ (1965) Micronema deletrix n.sp., a saprophagous nematode inhabiting a nasaltumor of a horse. Proc Helminthol Soc Wash 32:4–75
Anderson RC, Chabaud AG, Willmott S (1980) CIH keysto the nematode parasites of vertebrates, no.7. Keys tothe genera of the superfamily Strongyloidea. Com-monwealth Agricultural Bureau, Farrham Royal,Bucks, England
Anderson TJC, Romero-Abal ME, Jaenike J (1993)Genetic structure and epidemiology of Ascaris pop-ulations: patterns of host affiliation in Guatemala.Parasitology 107:319–334
Angheben A, Gobbo M, Gobbi F, Bravin A, Toneatti F(2009) Human syngamosis: an unusual cause ofchronic cough in travellers. BMJ Case Reports2009, doi:10.1136/bcr.12.2008.1305
Anten JF, Zuidema PJ (1964) Hookworm infection inDutch servicemen returning from West New Guinea.Trop Geogr Med 64(756):216–224
Aragane K, Akao N, Matsuyama T, Sugita M, NatsuakiM, Kitada O (1999) Fever, cough, and nodules onankles. Lancet 354:1892
Areekul S, Radomyos P, Viravan C (1970) Preliminaryreport of Ancylostoma ceylanicum infection in Thaipeople. J Med Assoc Thai 53:315–321
Ashford RW, Barnish G (1989) Strongyloides fuelleborniand similar parasites in animals and man. In: GroveDI (ed) Strongyloidiasis—a major roundworm infec-tion of man. Taylor and Francis, London, pp 271–286
Audicana MT, Ansotegui IJ, de Corres LF, Kennedy MW(2002) Anisakis simplex: dangerous—dead and alive?Trends Parasitol 18(1):20–25
Austin DN, Mikhail MG, Chiodini PL, Murray-Lyon LM(1999) Intestinal capillariasis acquired in Egypt. Eur JGastroenterol Hepatol 11:935–936
Averbeck G, Vanek J, Stromberg B, Laursen J (1995)Differentiation of Baylisascaris species, Toxocaracanis, and Toxascaris leonina infections in dogs.Compendium 17(475–478):511
Bahgat MA, El Gindy AE, Mahmoud LA, Hegab MH,Shahin AM (1999) Evaluation of the role of Ancy-lostoma caninum in human as a cause of acute andrecurrent abdominal pain. J Egypt Soc Parasitol29:873–882
Baker JR, Muller R, Rollinson D (eds) (2000) Advancesin Parasitology. Academic Press, USA, pp 1–179
Bapna S, Renapurkar DM (1996) Immunodiagnosis ofearly dracunculiasis. J Commun Dis 28:33–37
Barbosa AP, Campos DMB, Semerene AR, TeixeiraARL, Santana JM (2006) Lagochilascaris minorthird-stage larvae secrete metalloproteases with spec-ificity for fibrinogen and native collagen. MicrobesInfect 8:2725–2732
Beaver AC (1956) Larva migrans: a review. ExpParasitol 5:587–621
5.23 Zoonotic Filariasis 115

Beaver PC, Synder CH, Carrera GM, Dent JH, LaffertyJW (1952) Chronic eosinophilia due to visceral larvamigrans. Pediatrics 9:7–9
Beaver PC, Jung RC, Cupp EW (1984) Clinical parasi-tology, 9th edn. Lea and Febiger, Philadelphia,pp 544–547
Berenji F, Fata A, Hosseininejad Z (2007) A case ofMoniliformis moniliformis (Acanthocephala) infec-tion in Iran. Korean J Parasitol 45(2):145–148
Berk SL, Verghese A, Alvarez S, Hall K, Smith B (1987)Clinical and epidemiologic features of strongyloidiasis.A prospective study in rural Tennessee. Arch InternMed147:1257–1261.doi:10.1001/archinte.147.7.1257
Bhaibulaya M, Indra-Ngarm S (1979) Amaurornisphoenicurus and Ardeola Bacchus as experimentaldefinitive hosts for Capillaria philippinensis in Thai-land. Int J Parasitol 9:321–322
Birchard SJ, Sherding RG (1994) Manual Saunders:Clı0nica de Pequenos Animais, first ed. Roca, SaoPaulo, pp 815–816
Bleier T, Hetzel U, Nat R, Bauer C, Behlert O, BurkhardtE (2005) Gongylonema pulchrum infection andesophageal squamous cell carcinoma in a vari (Lemurmacaco variegata; Kehr 1792). J Zoo Wildlife Med36(2):342–345
Bloch P, Simonsen PE, Vennervald BJ (1993) Theantibody response to Dracunculus medinensis in anendemic human population of northern Ghana. J Hel-minthol 67:37–48
Bloch P, Vennervald BJ, Simonsen PE (1998) Studies onimmunodiagnosis of dracunculiasis. II. Search forcirculating antigens. Acta Trop 70:303–315
Bogers JJ, Storey PA, Faile G, Hewitt E, Yelifari E,Polderman A, Van Marck EA (2001) Human oesoph-agostomiasis: a histomorphometric study of 13 newcases in northern Ghana. Virchows Arch 439:21–26
Boreham RE, McCowan MJ, Ryan AE, Allworth AM,Robson JM (1995) Human trichostrongyliasis inQueensland. Pathology 27:182–185
Bowman DW (1999) Georgis’ parasitology for veteri-narians. W.B. Saunders, Philadelphia, p 215
Bryceson ADM, Hay RJ (1998) Parasitic worms andprotozoa. In: Champion RH, Burton JL, Burns DA,Breathnach SM (eds) Textbook of sermatology, 6thedn. Blackwell Science, Oxford, pp 1377–1422
Cairncross S, Muller R, Zagaria N (2002) Dracunculiasis(Guinea Worm Disease) and the eradication initiative.Microbiol Rev 15:223–246
Campos DMB, Freire-Filha LG, Vieira MA, Paco JM,Maia MA (1992) Experimental life cycle of Lago-chilascaris minor Leiper, 1909. Revista do Institutode Medicina Tropical de São Paulo 34:277–287
Cappucci DT, Augsburg JK, Klinck PC (1982) Gongy-lonemiasis. In: Steele JH (ed) CRC handbook seriesin Zoonoses Sect. C: Parasitic Zoonoses, vol 2. CRCPress, Boca Raton. pp 181–192
Caramello P, Vitali A, Canta F, Caldana A, Santi F,Caputo A, Lipani F, Balbiano R (2003) Intestinal
localization of anisakiasis manifested as acute abdo-men. Clin Microbiol Infect 9:734–737
Carroll SM, Grove DI (1984) Parasitological, hemato-logic, and immunologic responses in acute andchronic infections of dogs with Ancylostoma ceylan-icum: a model of human hookworm infection. J InfectDis 150:284–294
Carroll SM, Grove DI (1986) Experimental infection ofhuman with Ancylostoma ceylanicum: clinical, para-sitological, haematological and immunological find-ings. Trop Geogr Med 38:38–45
Caumes E (2000) Treatment of cutaneous larva migrans.Clin Infect Dis 30:811–814
Caumes E, Ly F, Bricaire F (2002) Cutaneous larvamigrans with folliculitis: report of seven cases andreview of the literature. Br J Dermatol 146:314–316
Chai JY, Darwin Murrell K, Lymbery AJ (2005) Fish-borne parasitic zoonoses: status and issues. Int JParasitol 35:1233–1254
Cheesbrough M (1987) Medical laboratory manual fortropical countries, vol 1, 2nd edn. Tropical HealthTechnology and Butterworths, Cambridge
Chen HT (1935) A new pulmonary nematode of rats,Pulmonema cantonensis ng, nsp from Canton. AnnParasitol 13:312–317 (in French)
Choo J, Pang E, Prociv P (2000) Hookworms in dogs ofKuching, Sarawak (north Borneo). Trans R Soc TropMed Hyg 94:21–22
Chotmongkol V, Sawanyawisuth K (2002) Clinicalmanifestations and outcome of patients with severeeosinophilic meningoencephalitis presumably causedby Angiostrongylus cantonensis. Southeast Asian JTrop Med Public Health 33:231–234
Chowdhury AB, Schad GA (1972) Ancylostoma ceylan-icum: a parasite of man in Calcutta and environs. AmJ Trop Med Hyg 21:300–301
Counselman K, Field C, Lea G, Nickol B, Neafie R(1989) Moniliformis moniliformis from a child inFlorida. Am J Trop Med Hyg 41:88–90
Crewe W, Smith DH (1971) Human infection with pigAscaris (A. suum). Ann Trop Med Parasitol 65:85
Croese J, Loukas A, Opdebeeck J, Fairley S, Prociv P(1994a) Human enteric infection with canine hook-worms. Ann Intern Med 120:369–374
Croese J, Loukas A, Opdebeeck J, Prociv P (1994b)Occult enteric infection by Ancylostoma caninum: apreviously unrecognized zoonosis. Gastroenterology106:3–12
Crompton DWT (2001) Ascaris and ascariasis. AdvParasit 48:285–375
Cross JH (1978) Clinical manifestations and laboratorydiagnosis of eosinophilic meningitis syndrome asso-ciated with angiostrongyliasis. Southeast Asian JTrop Med Public Health 9:161–170
Cross JH (1992) Intestinal capillariasis. Clin MicrobiolRev 5(2):120–129
Cross JH (1998) Capillariasis. In: Palmer SR, Soulsby L,Simpson DIH (eds) Zoonoses: biology, clinical
116 5 Nematode Zoonoses

practice, and public health control, 1st edn. OxfordUniversity Press, New York, pp 759–772
Cross JH, Basaca-Sevilla V (1983) Experimental trans-mission of Capillania philippinensis to birds. Trans RSoc Trop Med Hyg 77:511–514
Cunnac M, Magnaval JF, Cayarci D, Leophonte P (1988)A propos de 3 cas de syngamose humaine enGuadeloupe. Rev Pneumol Clin 44:140–142
da Costa JC, Delgado ML, Vieira P, Afonso A, Conde B,Cross JH (2005) Syngamoniasis in tourist (letter).Emerg Infect Dis 11(12):1976–1977
Daengsvang S (1981) Gnathostomiasis in Southeast Asia.Southeast Asian J Trop Med Public Health 12:319–332
Daensvang S (1980) A monograph on the genusGnathostoma and gnathostomiasis in Thailand.Southeast Asian Medical Information Center/Interna-tional Medical Foundation of Japan, Tokyo
de Silva NR, Brooker S, Hotez PJ, Montresor A, EngelsD, Savioli L (2003) Soiltransmitted helminth infec-tions: updating the global picture. Trends Parasitol19:547–551
deFreitas JG, Prudente MFS, Spadafora-Ferreira M,Kipnis APJ, dePaula EC, Tambourgi DV, Lino-JúniorRS, Carvalhaes MS (2008) Lagochilascaris minor:experimental infection of C57BL/6 and BALB/cisogenic mice reveals the presence of adult worms.Exp Parasitol 119:325–331
deMoura MQ, Jeske S, Gallina T, Borsuk S, Berne MEA,Villela MM (2012) First report of Lagochilascaris(Nematoda: Ascarididae) eggs in a public park inSouthern Brazil. Vet Parasitol 184:359–361
Dold C, Holland CV (2010) Ascaris and ascariasis.Microbes and Infection. doi: 10.1016/j.micinf.2010.09.012
Dupouy-Camet J (2000) Trichinellosis: a worldwidezoonosis. Vet Parasitol 93:191–200
Eamosobhana P, Yong HS (2009) Immunological diag-nosis of human angiostrongyliasis due to Angiostron-gylus cantonensis (Nematoda: Angiostrongylidae). IntJ Infect Dis 13:425–431
Eamsobhana P (2006) The rat lungworm Parastrongylus(Angiostrongylus) cantonensis: parasitology, immu-nology, eosinophilic meningitis, epidemiology andlaboratory diagnosis. Wankaew (IQ) Book Center,Bangkok
Eberhard ML (1984) Brugia lepori sp.n. (Filarioidea:Onchocercidae) from rabbits (Sylvilagus aquaticus,S. floridanus) in Louisiana. J Parasitol 70:576–579
El Hassan SE, Mikhail WE (1992) Malabsorption due toCapillaria philippinensis in an Egyptian woman livingin Dubai, United Arab Emirates. Trans R Soc TropMed Hyg 89:79
Fraiha H, Leão RNQ, Costa FSA (1989) Lagochilascar-iase humana e dos animais domésticos. Vet IntZoonoses 1:25–33
Freire-Filha LG, Junqueira-Kipnis AP, Ribeiro WR,Campos DMB (2001) Avaliacão cito-hematológicaem camundongos isogênicos da linhagem C57BL/6
infectados com ovos de Lagochilascaris minor (Lei-per, 1909). Revista de Patologia Tropical 30:225–234
Freitas MG (1980) Helmintologia Veterina0ria. fourth ed.Gra0fica Rabelo, Belo Horizonte, pp 267–270
Gajadhar AA, Scandrett WB, Forbes LB (2006) Overviewof food- and water-borne zoonotic parasites at the farmlevel. Rev Sci Tech Off Int Epiz 25(2):595–606
Gajadhar AA, Pozio E, Gamble HR, Nockler K, Maddox-Hyttel C, Forbes LB, Vallee I, Rossi P, Marinculic A,Boireau P (2009) Trichinella diagnostics and control:mandatory and best practices for ensuring food safety.Vet Parasitol 159:197–205
Galvin TJ (1968) Development of human and pig Ascarisin the pig and rabbit. J Parasitol 54:1085–1091
Garcia LS (2001) Diagnostics medical parasitology, 4thedn. ASM press, Washington, pp 477–501
Gardiner CH, Koh DS, Cardella TA (1981) Micronemain man: third fatal infection. Am J Trop Med Hyg30:586–589
Gavin PJ, Kazacos KR, Shulman ST (2005) Baylisasca-riasis. Clin Microbiol Rev 18(4):703–718
Geenen PL, Bresciani J, Boes J, Pedersen A, Eriksen L,Fagerholm HP, Nansen P (1999) The morphogenesisof Ascaris suum to the infective third-stage larvaewithin the egg. J Parasitol 85:616–622
Genta RM (1989) Global prevalence of strongyloidiasis:critical review with epidemiologic insights into theprevention of disseminated disease. Rev Infect Dis11:755–767. doi:10.1093/clinids/11.5.755
Giboda M, Viengsay M, Bouaphan S, Ditrich O (1991)Epidemiology of intestinal parasitosis in Laos (withantiamoebic antibody levels). Bull Soc Pathol Exot84:184–193
Goldberg MA, Kazacos KR, Boyce WM, Ai E, Katz B(1993) Diffuse unilateral subacute neuritis. Morpho-metric, serologic and epidemiologic support forBaylisascaris as a causative agent. Ophthalmology100:1695–1701
Gordon AC, Murray JK, Martin WB, Wilhelm FE (1990)Micronema deletrix in the kidney of a horse. Can VetJ 31:451–452
Greve JH, O’Brien S (1989) Adult Baylisascaris infec-tion in two dogs. Comp Anim Pract 19:41–43
Grove DI (1989) Clinical manifestations. In: Grove DI(ed) Strongyloidiasis: a major roundworm infection ofman. Taylor and Francis, Philadelphia, pp 155–173
Grove DI (1996) Human strongyloidiasis. Adv Parasitol38:251–309
Guitierrez Y (2000) Diagnostic pathology of parasiticinfections with clinical correlations, 2nd edn. OxfordUniversity Press, Oxford
Gutierrez Y (1990) Diagnostic pathology of parasiticinfections with clinical correlations. Lea and Febiger,Philadelphia
Gutierrez Y (1999) Other tissue nematode infections. In:Guerrant RL, Walker DH, Weller PF (eds) Tropicalinfectious diseases: principles, pathogens, and prac-tice. Churchill Livingstone, London, pp 933–948
References 117

Hall A, Conway DJ, Anwar KS, Rahman ML (1994)Strongyloides stercoralis in an urban slum commu-nity in Bangladesh: factors independently associatedwith infection. Trans R Soc Trop Med Hyg88:527–530
Hashikura T (1927) A case of Filaria medinensis inChosen (Korea). Jpn Med World 7:145–146
Herman JS, Chiodini PL (2009) Gnathostomiasis,another emerging imported disease. Clin MicrobiolRev 22(3):484–492
Hong ST, Cross JH (2005) Capillaria philippinensisinfection in Asia. In: Arizono N, Chai JY, Nawa Y,Takahashi Y (eds) Asian parasitology vol. 1 Food-borne helminthiasis in Asia. Federation of AsianParasitologists, Chiba, pp 225–259
Hoogstraten J, Young WG (1975) Meningo-encephalo-myelitis due to the saprophagous nematode, Micro-nema deletrix. Can J Neurol Sci 2:121–126
Hopkins DR, Tiben ER, Downs P, Withers PC, Roy S(2008) Dracunculiasis eradication: neglected nolonger. Am J Trop Med Hyg 79(4):474–479
Hotez PJ, Bundy DAP, Beegle K, Brooker S, Drake L, deSilva NR, Montresor A, Engels D, Jukes M (2006)Helminth infections: soil-transmitted helminth infec-tion and schistosomiasis. In: Jamison DT, Breman JG,Measham AR, Alleyne G, Claeson M, Evans DB, JhaP, Mills A, Musgrove P (eds) Disease controlpriorities in developing countries. World Bank Group,Washington, pp 467–478
Hulbert TV, Larson RA, Chandrasoma PT (1992)Abdominal angiostrongyliasis mimicking acuteappendicitis and Meckel’s diverticulum: report of acase in the United States and review. Clin Infect Dis14:836–840
Ikeh Z, Anosike J, Okon E (1992) Acanthocephalaninfection in man in northern Nigeria. J Helminthol66:241–242
Illescas-Gomez MP, Osorio MR, Garcia VG, GomezMorales MA (1988) Human Gongylonema infectionin Spain. Am J Trop Med Hyg 38:363–365
Inoue K, Inoue Y, Arai T, Nawa Y, Kashiwa Y,Yamamoto S, Sakatani M (2002) Chronic eosino-philic pneumonia due to visceral larva migrans. InternMed 41:478–482
Jaskoski BJ (1961) An apparent swine Ascaris infectionof man. J Am Vet Med Assoc 138:504–505
Jiraanankul V, Aphijirawat W, Mungthin M, Khositnithi-kul R, Rangsin R et al (2011) Incidence and riskfactors of hookworm infection in a rural communityof central Thailand. Am J Trop Med Hyg 84:594–598
Karam M, Tayeh A (2006) Dracunculiasis eradication.Bull Soc Pathol Exot 99(5):377–385
Karasawa Y, Karasawa G, Kamiya K, Hoshi K (2008)Current situation of anisakiasis: the second nationalsurvey. Nihon Iji Shimpo 4386:68–74
Kazacos KR (1983) Raccoon roundworms (Baylisascarisprocyonis): a cause of animal and human disease.Purdue University Agricultural Experiment StationBulletin No. 422
Kazacos KR (2000) Protecting children from helminthiczoonoses. Contemp Pediatr 17:1–24
Kazacos KR (2001) Baylisascaris procyonis and relatedspecies. In: Samuels WM, Pybus MJ, Kocans AA(eds) Parasitic diseases of wild mammals, 2nd edn.Lowa State University Press, Ames, pp 301–341
Kazacos KR, Raymond LA, Kazacos EA, Vestre WA(1985) The raccoon ascarid. A probable cause ofhuman ocular larva migrans. Ophthalmology92:1735–1743
Keg PR, Mirck MH, Dik KJ, Vos JH (1984) Micronemadeletrix infection in a Shetland pony stallion. EquineVet J 16:471–475
Keiser PB, Nutman TB (2004) Strongyloides stercoralisin the immunocompromised population. Clin Micro-biol Rev 17(1):208–217
Khoshoo V, Craver R, Schantz P, Loukas A, Prociv P(1995) Abdominal pain, pan-gut eosinophilia, and doghookworm infection. J Pediatr Gastroenterol 21:481
Kim HY, Lee SM, Joo JE, Na MJ, Ahn MH, Min DY(1998) Human syngamosis: the first case in Korea.Thorax 53:717–718
Kitano H, Uni S, Iseki M (1996) Case of humanthelaziasis in Nara Prefecture. Jpn Ganka RinsyouIhou 90:1551–1554 (in Japanese)
Knight R (2003) The hookworms. In: Cox TM, Firth JD,Warrell DA (eds) Oxford textbook of medicine.Oxford University Press, Oxford, pp 799–800
Kobayashi A, Katatura A, Hamada A, Suzuki T (1986)Human case of dracunculiasis in Japan. Am J TropMed Hyg 35:159–161
Kommers DG, Ilha MRS, Barros CSL (1999) Dioctofi-mose em caes: 16 casos. Ciencia Rural 29:517–522
Koo J, Pien F, Kliks MM (1988) Angiostrongylus(Parastrongylus) eosinophilic meningitis. Rev InfectDis 10:1155–1162
Kosin E, Kosman ML, Depary AA (1989) First case ofhuman thelaziasis in Indonesia. Southeast Asian JTrop Med Public Health 20:233–236
Koyama Y, Ohira A, Kono T, Shimane T, Yoneyama T,Shiwaku K (2000) Five cases of thelaziasis. Br JOphthalmol 84:439–442
Krief S, Vermeulen B, Lafosse S, Kasenene JM, Niegu-itsila A (2010) Nodular worm infection in wildchimpanzees in Western Uganda: a risk for humanhealth? PLoS Negl Trop Dis 4(3):e630. doi:10.1371/journal.pntd.0000630
Kudo N, Kubota H, Gotoh H, Ishida H, Ikadai H,Oyamada T (2008) Efficacy of thiabendazole, meben-dazole, levamisole and ivermectin against gulletworm, Gongylonema pulchrum: In vitro and in vivostudies. Vet Parasitol 151:46–52
Landmann JK, Prociv P (2003) Experimental humaninfection with the dog hookworm, Ancylostomacaninum. Med J Aust 178(2):69–71
Lawlor B, Read A, Keymer A, Parveen G, Crompton D(1990) Non-random mating in a parasitic worm: matechoice by males? Anim Behav 40:870–876
118 5 Nematode Zoonoses

Leão RNQ, Fraiha-Neto H, Dias LB (2005) Lagoquila-scaríase. In: Focaccia R (ed) Tratado de Infectologia.Atheneu, São Paulo, pp 1781–1785
Leiper RT (1909) A new nematode worm from Trinidad.Lagochilascaris minor. Proc Zool Soc Lond 4:742–743
Libersat F, Moore J (2000) The parasite Moniliformismoniliformis alters the escape response of its cock-roach host Periplaneta americana. J Insect Behav13:103–110
Lopez Serrano MC, Alonso-Gomez A, Moreno-AncilloA, Daschner A, Suarez de Parga J (2000) Gastroal-lergic anisakiasis: immediate hypersensitivity due toAnisakis simplex infestation. Allergol Immunol Clin15:230–236
Lord WD, Bullock WL (1982) Swine Ascaris in humans.N Engl J Med 306:1113
Loukas A, Croese J, Opdebeeck J, Prociv P (1992)Detection of antibodies to secretions of Ancylostomacaninum in human eosinophilic enteritis. Trans R SocTrop Med Hyg 86:650–653
Lucchina LC, Wilson ME (1999) Cysticercosis and otherhelminthic infections. In: Freedberg IM, Eisen AZ,Wolff K et al (eds) Fitzpatrick’s dermatology ingeneral medicine, 5th edn. McGraw-Hill, New York,pp 2619–2654
Lv S, Zhang Y, Steinmann P, Zhou XN (2008) Emergingangiostrongyliasis in mainland China. Emerg InfectDis 14(1):161–164
Marquards WC, Demaree RS, Grieve RB (2000) Para-sitology and vector biology, 2nd edn. Harcourtacademic Press, San Diego, p 491. doi:499
Márquez-Navarro A, García-Bracamontes G, Álvarez-Fernández BE, Ávila-Caballero LP, Santos-Aranda I,Díaz-Chiguer DL, Sánchez-Manzano RM, Rodrí-guez-Bataz E, Nogueda-Torres B (2012) Trichurisvulpis (Froelich, 1789) Infection in a Child: A CaseReport. Korean J Parasitol 50(1):69–71
Mattiucci S, Paoletti M, Borrini F, Palumbo M, PalmieriRM, Gomes V, Casati A, Nasce G (2011) Firstmolecular identification of the zoonotic parasiteAnisakis pegreffii (Nematoda: Anisakidae) in a par-affin-embedded granuloma taken from a case ofhuman intestinal anisakiasis in Italy. BMC InfectDis 11:82
Maxie MG (1993) The kidney. In: Jubb KVF, KennedyPC, Palmer N (eds) The pathology of domesticanimals, vol 2, 4th edn. Academic Press, San Diego,pp 447–538 (Chapter 5)
McCarthy J, Moore TA (2000) Emerging helminthzoonoses. Int J Parasitol 30:1351–1360
Miyazaki I (1991) Section III. Nematode zoonoses. 32.Thelaziasis. An illustrated book of helminthic zoo-noses. Tokyo, Japan. International Medical Founda-tion of Japan. pp 362–368
Mok CH (1968) Visceral larva migrans. A discussionbased on review of the literature. Clin Pediatr7:565–573
Moncada LI, Alvarez CA, Castellanos C, Caceres E,Nicholls S, Corredor A (1998) Logochilascaris minor
in a patient from the Colombian Amazon: a casereport. Rev Inst Med Trop Sao Paulo 40:387–389
Moore J, Freehling M, Gotelli NJ (1994) Alteredbehavior in two species of blattid cockroachesinfected with Moniliformis moniliformis (Acantho-cephala). J Parasitol 80:220–223
Moore DAJ, McCroddan J, Dekumyoy P, Chiodini PL(2003) Gnathostomiasis: an emerging imported dis-ease. Emerg Infect Dis 9(6):647–650
Morimatsu Y, Akao N, Akiyoshi H, Kawazu T, Okabe Y,Aizawa H (2006) A familial case of visceral larvamigrans after ingestion of raw chicken livers: appear-ance of specific antibody in broncho alveolar lavagefluid of the patients. Am J Trop Med Hyg75(2):303–306
Muller R (1971) Dracunculus and dracunculiasis. AdvParasitol 9:73–151
Muller R (1975) Worm and disease, a manual of medicalhelminthology, 1st edn. William Heinemann MedicalBook Ltd, London, p 64
Murrell KD, Eriksen L, Nansen P, Slotved HC, Rasmus-sen T (1997) Ascaris suum: a revision of its earlymigratory path and implications for human ascariasis.J Parasitol 83:255–260
Nakagawa TLDR, Bracarense APFRL, dos Reis ACF,Yamamura MH, Headley SA (2007) Giant kidneyworm (Dioctophyma renale) infections in dogs fromNorthern Parana’, Brazil. Vet Parasitol 145:366–370
Nansen P, Roepstorff A (1999) Parasitic helminths of thepig: factors influencing transmission and infectionlevels. Int J Parasitol 29:877–891
Nejsum P, Parker ED, Frydenberg J, Roepstorff A, BoesJ, Haque R, Astrup I, Prag J, Sensen UBS (2005)Ascariasis is a zoonosis in Denmark. J Clin Microbiol43:1142–1148
Nejsum P, Bertelsen MF, Betson M, Stothard JR, MurrellKD (2010) Molecular evidence for sustained trans-mission of zoonotic Ascaris suum among zoo chim-panzees (Pan troglodytes). Vet Parasitol 171:273–276
Neva FA (1994) Intestinal nematodes of human beings.In: Neva FA (ed) Basic clinical parasitology. Apple-ton and Lange, Norwalk, pp 123–128
Ngui R, Lim YAL, Traub R, Mahmud R, Mistam MS(2012) Epidemiological and genetic data supportingthe transmission of ancylostoma ceylanicum amonghuman and domestic animals. PLoS Negl Trop Dis6(2):e1522. doi:10.1371/journal.pntd.0001522
Nosanchuk JS, Wade SE, Landolf M (1995) Case reportof and description of parasite in Mammomonogamuslaryngeus (human syngamosis). J Clin Microbiol33:998–1000
Olle-Goig JE, Recacoechea M, Feeley T (1996) First caseof Lagochilascaris minor infection in Bolivia. TropMed Int Health 1:851–853
Olsen A, van Lieshout L, Marti H, Polderman T, PolmanK, Steinmanne P, Stothard R, Thybo S, Verweij JJ,Magnussen P (2009) Strongyloidiasis—the mostneglected of the neglected tropical diseases? TransR Soc Trop Med Hyg 103:967–972
References 119

Orihel TC (1966) Brugia tupaiae sp.n. (Nematoda:Filarioidea) in tree shrews (Tupaia glis) from Malay-sia. J Parasitol 52:162–165
Orihel TC, Ash LR (1995) Parasites in human tissues. AmSoc Clin Pathologists, ASCP Press, Chicago, p 111
Orihel TC, Eberhard ML (1998) Zoonotic fiariasis. ClinMicrobiol Rev 11(2):366–381
Orihel TC, Pacheco G (1966) Brugia malayi in thePhilippine macaque. J Parasitol 52:394
Ortega-Pierres MG, Arriaga C, Yepez-Mulia L (2000)Epidemiology of trichinellosis in Mexico, Central andSouth America. Vet Parasitol 93:201–225
Otranto D, Eberhard ML (2011) Zoonotic helminthsaffecting the human eye. Parasites Vectors 4:41
Otranto D, Traversa D (2005) Thelazia eyeworm: anoriginal endo- and ectoparasitic nematode. TrendsParasitol 21:1–4
Otranto D, Ferroglio E, Lia R, Traversa D, Rossi L (2003a)Current status and epidemiological observations ofThelazia callipaeda (Spirurida, Thelaziidae) in dogs,cats and foxes in Italy: a ‘coincidence’ or a parasiticdisease of the old continent? Vet Parasitol 116:315–325
Otranto D, Lia RP, Traversa D, Giannetto S (2003b)Thelazia callipaeda (Spirurida, Thelaziidae) of car-nivores and humans: morphological study by lightand scanning electron microscopy. Parassitologia45:125–133
Otranto D, Dantas-Torres F, Mallia E, DiGeronimo PM,Brianti E, Testini G, Traversa D, Lia P (2009)Thelazia callipaeda (Spirurida, Thelaziidae) in wildanimals: report of new host species and ecologicalimplications. Vet Parasitol 166:262–267
Paco JM, Campos DMB, Araújo de Oliveira J (1999)Wild rodents as experimental intermediate hosts ofLagochilascaris minor Leiper, 1909. Memórias doInstituto Oswaldo Cruz 94:441–449
Pampiglione S, Canestri Trotti G, Rivasi F (1995) Humandirofilariasis due to Dirofilaria (Nochtiella) repens: areview of world literature. Parassitologia 37:149–193
Panasoponkul C, Radomyos P, Singhasivanon V (1985)Trichostrongylus infection in a Thai boy. SoutheastAsian J Trop Med Public Health 16:513–514
Pereira BJ, Girardeli GL, Trivilin LO, Lima VR, NunesLC, Martins IVF (2006) Ocorrencia de dioctofimoseem caes do municı0pio de Cachoeiro de Itapemirim,Espı0rito Santo, Brasil, no perı0odo de maio a dezem-bro de 2004. Ver Bras Parasitol Vet 15:123–125
Pien FD, Pien BC (1999) Angiostrongylus cantonensisEosinophilic Meningitis. Int J Infect Dis 3:161–163
Pilitt PA, Lichtenfels JR, Tromba FG, Madden PA (1981)Differentiation of late fourth and early fifth stages ofAscaris suum Goeze, 1782 (Nematoda: Ascaridoidea)in swine. P Helm Soc Wash 48:1–7
Pipitogool V, Chaisiri K, Visetsuspakarn P, Srigan V,Maleewong W (1992) Mammomonogamus (synga-mus) laryngeus. First case report in Thailand. South-east Asian J Trop Med Public Health 23:336–337
Pohlenz J, Eckert J, Minder HP (1981) Zentralnervosestorungen beim Pferd, verursacht durch Nematoden
der Gattung Micronema (Rhabdita). Berl MuenchTieraerztl Wochenschr 94:216–220
Poinar GO (1983) The natural history of nematodes.Prentice-Hall Inc, Englewood Cliffs, pp 114–115
Poirriez J, Dei-Cas E, Guevart E (1984) Human infes-tation by Trichostrongylus vitrinus in Morocco. AnnParasitol Hum Comp 59:636–638
Polderman AM, Blotkamp J (1995) Oesophagostomuminfection in humans. Parasitol Today 11:451–456
Polderman AM, Krepel HP, Baeta S, Blotkamp J, GigaseP (1991) Oesophagostomiasis, a common infection ofman in northern Togo and Ghana. Am J Trop MedHyg 44:336–344
Polderman AM, Anemana SD, Asigri V (1999) Humanoesophagostomiasis: a regional public health problemin Africa. Parasitol Today 15:129–130
Polderman AM, Eberhard M, Baeta S, Gasser RB, vanLieshout L, Magnussen P, Olsen A, Spannbrucker N,Ziem J, Horton J (2010) The rise and fall of humanoesophagostomiasis. Adv Parasitol 71:93–155
Pozio E (2000) Factors affecting the flow amongdomestic, synanthropic and sylvatic cycles of Trich-inella. Vet Parasitol 93:241–262
Pozio E (2007) World distribution of Trichinella spp.infections in animals and humans. Vet Parasitol149:3–21
Prociv P, Croese J (1990) Human eosinophilic enteritiscaused by dog hookworm Ancylostoma caninum.Lancet 335(8701):1299–1302
Prociv P, Croese J (1996) Human enteric infection withAncylostoma caninum: hookworms reappraised in thelight of a ‘‘new’’ zoonosis. Acta Trop 62:23–44
Prudente MFS, Lima KC, Carvalhaes MS (2008) Perfilhematológico, bioquímico sérico e sorológico de Felisdomesticus com lagochilascariose experimental. RevSoc Bras Med Trop 41:496–501
Purdy KS, Langley RG, Webb AN, Walsh N, Haldane D(2011) Cutaneous larva migrans. Lancet 377:1948
Rames DS, Miller DK, Barthel R, Craig TM, Dziezyc J,Helman RG, Mealey R (1995) Ocular Halicephalobus(syn. Micronema) deletrix in a Horse. Vet Pathol32:540
Remfry J (1978) The incidence, pathogenesis andtreatment of helminth infections in rhesus monkeys(Macaca mulatta). Lab Anim 12:213–218
Roberts L, Janovy JR (2005) Foundation of parasitology,7th edn. McGraw-Hill, Boston, pp 493–509
Roberts T, Murrell KD (1993) Economic losses caused byfood-borne parasitic diseases. In: Proceedings of thesymposium on cost-benefits aspects of food irradiationprocessing. IAEA/FAO/WHO, Alix-En Provence, 1–5Mar. IAEA, SM-328/66, Vienna, pp 51–75
Rodrigues RM, De Oliveira MC, Sopelete MC, Silva DA,Campos DM, Taketomi EA (2007) IgG1, IgG4, andIgE antibody responses in human strongyloidiasis byELISA using Strongyloides ratti saline extract asheterologous antigen. Parasitol Res 101:1209–1214
Roepstorff A, Eriksen L, Slotved HC, Nansen P (1997)Experimental Ascaris suum infection in the pig: worm
120 5 Nematode Zoonoses

population kinetics following single inoculations withthreedoses of infectiveeggs.Parasitology 115:443–452
Roepstorff A, Nilsson O, Oksanen A, Gjerde B, RichterSH, Örtenberg E, Christensson D, Martinsson KB,Bartlett PC, Nansen P (1998) Intestinal parasites inswine in the Nordic countries: prevalence and geo-graphical distribution. Vet Parasitol 76:305–319
Roig J, Romeu J, Riera C, Texido A, Domingo C, MoreraJ (1992) Acute eosinophilic pneumonia due totoxocariasis with bronchoalveolar lavage findings.Chest 102:294–296
Rosemberg MB, Lopes Z, Campos R, Vieira Bressan MC(1986) Fatal encephalopathy due to Lagochilascarisminor infection. Am J Trop Med Hyg 35:575–578
Rubin HL, Woodard JC (1974) Equine infection withMicronema deletrix. J Am Vet Med Assoc 165:256–258
Rusnak JM, Lucey DR (1993) Clinical gnathostomiasis:case report and review of the English-languageliterature. Clin Infect Dis 16:33–50
Sakakibara A, Baba K, Niwa S, Yagi T, Wakayama H,Yoshida K, Kobayashi T, Yokoi T, Hara K, Itoh M,Kimura E (2002) Visceral larva migrans due toAscaris suum which presented with eosinophilicpneumonia and multiple intra-hepatic lesions withsevere eosinophil infiltration—outbreak in a Japanesearea other than Kyushu. Intern Med 41:574–579
Sakamoto T, Cabrera PA (2002) Subcutaneous infectionof Lagochilascaris minor in domestic cats fromUruguay. Vet Parasitol 108:145–152
Sakanari JA, Mckerrow JH (1989) Anisakiasis. ClinMicrobiol Rev 2:278–284
Sato M, Sanguankiat S, Yoonuan T, Pongvongsa T,Keomoungkhoun M (2010) Copro-molecular identi-fication of infections with hookworm eggs in ruralLao PDR. Trans R Soc Trop Med Hyg 104:617–622
Sato M, Yoonuan T, Sanguankiat S, Nuamtanong S,Pongvongsa T, Phimmayoi I, Phanhanan V, BouphaB, Moji K, Waikagul J (2011) Human Trichostron-gylus colubriformis infection in a rural village inLaos. Am J Trop Med Hyg 84(1):52–54
Setasuban P, Vajrasthira S, Muennoo C (1976) Preva-lence and zoonotic potential of Ancylostoma ceylan-icum in cats in Thailand. Southeast Asian J Trop MedPublic Health 7:534–539
Severo LC, Conci LMA, Camargo JJP, Andre-Alves MR,Palombini BC (1988) Syngamosis: two new Braziliancases and evidence of possible pulmonary cycle.Trans R Soc Trop Med Hyg 82:467–468
Shadduck IA, Ubelaker J, Telford VQ (1979) Micronemadeletrix meningoencephalitis in an adult man. Am JClin Pathol 72:640–643
Shen J, Gasser RB, Chu D, Wang Z, Yuan X, CantacessiC, Otranto D (2006) Human thelaziosis-A neglectedparasitic disease of the eye. J Parasitol 92:872–876
Shinkar RM, Stocks R, Thomas E (2005) Cutaneouslarva migrans, creeping eruption, sand worm. ArchDis Child 90:998
Silva LP, Barcelos ISC, Passos-Lima AB, Espindola FS,Campos DMB, Costa-Cruz JM (2003) Western blot-ting using Strongyloides ratti antigen for the detection
of IgG antibodies as confirmatory test in humanstrongyloidiasis. Mem Inst Oswaldo Cruz 98:687–691
Silvera CT, Ghali VS, Roven S (1989) Angiostrongyli-asis: a rare case of gastrointestinal hemorrhage. Am JGastroenterol 84:329–332
Simpson RM, Hodgin EC, Cho DY (1988) Micronemadeletrixinduced granulomatous osteoarthritis in alame horse. J Comp Pathol 99:347–351
Singh TS, Singh KN (1993) Thelaziasis: report of twocases. Br J Ophthalmol 7:528–529
Smith JW, Wootten R (1978) Anisakis and anisakiasis.Adv Parasitol 16:93–163
Snyder DE (1987) Contaminative potential, egg preva-lence, and intensity of Baylisascaris procyonis-infected raccoons (Procyon lotor) from Illinois, witha comparison to worm intensity. Proc HelminthiolSoc Wash 54:141–145
Sohn WM, Na BK, Yoo JM (2011) Two cases of humanThelaziasis and brief review of Korean cases. KoreanJ Parasitol 49(3):265–271
Soler M, Cardose L, Teixeira M, Agu A (2008) Imagingdiagnosis—Dioctophyma renale in a dog. Vet RadiolUltrasound 49:307–308
Sorvillo F, Ash LR, Berlin OG, Morse SA (2002)Baylisascaris procyonis: an emerging helminthiczoonosis. Emerg Infect Dis 8:355–359
Soulsby ELJ (1965) Textbook of veterinary clinicalparasitology, vol 1. Lippincott Williams and Wil-liams, Philadelphia
Soulsby EJL (1978) Helminths, arthropods and protozoaof domestic animals, 6th edn. Baillie’re Tindall andCassell, London, pp 326–327
Soulsby EJL (1982) Arthropods and protozoa andhelminthes of domesticated animals, 7th edn. Bail-liere Tindall, London, pp 296–298
Spalding MG, Greiner EC, Green SL (1990) Haliceph-alobus (Micronema) deletrix infection in two half-sibling foals. Am Vet Med Assoc 196(7):1127–1129
Sprent JFA (1971) Speciation and development in thegenus Lagochilascaris. Parasitology 62:71–112
Storey PA, Anemana S, van Oostayen JA (2000)Ultrasound diagnosis of oesophagostomiasis. Br JRadiol 73:328–332
Sugimachi K, Inokuchi K, Ooiwa T, Fujino T, Ishii Y(1985) Acute gastric anisakiasis, analysis of 178cases. JAMA 253(7):1012–1013
Sun T, Turnbull A, Lieberman PH, Sternberg SS (1986)Giant kidney worm (Dioctophyma renale) infectionmimicking retroperitoneal neoplasm. Am J Surg Pathol10:508–512
Takata I (1951) Experimental infection ofman with Ascarisof man and the pig. Kitasato Arch Exp Med 23:151
Taraschewski H (2000) Host-parasite interactions inAcanthocephala: a morphological approach. AdvParasitol 46:1–179
Thomas CO, Mark LE (1998) Zoonotic Filariasis. ClinMicrobiol Rev 11(2):366–381
Tiben ER, Hopkins DR (2006) Dracunculiasis (GuineaWorm Disease) Eradication. Adv Parasitol61:275–309
References 121

Tiner JD (1953) The migration, distribution in the brain,and growth of ascarid larvae in rodents. J Infect Dis92:105–113
Todd ECD (1989) Preliminary estimates of cost of food-borne disease in the United States. J Food Prod52:595–601
Traub RJ, Robertson ID, Irwin P, Mencke N, ThompsonRC (2004) Application of a species-specific PCR-RFLP to identify Ancylostoma eggs. Vet Parasitol123:245–255
Traub RJ, Hobbs RP, Adams PJ, Behnke JM, Harris PD,Thompson RC (2007) A case of mistaken identity—reappraisal of the species of canid and felid hook-worms (Ancylostoma) present in Australia and India.Parasitology 134:113–119
Traub RJ, Inpankaew T, Sutthikornchai C, Sukthana Y,Thompson RCA (2008) PCR-based coprodiagnostictools reveal dogs as reservoirs of zoonotic ancylosto-miasis caused by Ancylostoma ceylanicum in templecommunities in Bangkok. Vet Parasitol 155:67–73
Tu CH, Liao WC, Chiang TH, Wang HP (2008) Petparasites infesting the human colon. GastrointestEndosc 67(1):159–160
Van Heutsz (1926) One indigenous and two importedcases of Dracunculus in Java. Geneeskd. TijdschrNed.-Indie 66:25 (In Dutch)
Van Thiel PH (1960) A nematode parasitic to herringcausing acute abdomen syndromes in man. TropGeogr Med 2:97–113
Velasquez CC, Cabrera BC (1968) Ancylostoma ceylan-icum (Looss 1911) in a Filipino woman. J Parasitol54:430–431
Veloso MGP, Faria MCAR, Freitas JD, Moraes MAP,Gorini DF, Mendonc JLF (1992) Lagochilascaríasehumana sobre três casos encontrados no DistritoFederal, Brasil. Rev Inst Med Trop Sao Paulo34:587–591
Volcan GS, Medrano CE, Payares G (1992) Experimen-tal heteroxenous cycle of Lagochilascaris minorLeiper, 1909 (Nematoda: Ascarididae), in white miceand cats. Memórias do Instituto Oswaldo Cruz87:532–535
Wall EC, Bhatnagar N, Watson J, Doherty T (2011) Anunusual case of hypereosinophilia and abdominalpain: an outbreak of Trichostrongylus Imported fromNew Zealand. J Travel Med 18(1):59–60
Wang QP, Lai DH, Zhu XQ, Chen XG, Lun ZR (2008)Human angiostrongyliasis. Lancet Infect Dis8:621–630
WHO (2006) Preventative chemotherapy in humanhelminthiases: coordinated use of anthelminthic drugsin control interventions: a manual for health profes-sionals and programme managers. World HealthOrganisation, Geneva
Wijers DJ, Smit AM (1966) Early symptoms after exper-imental infection of man with Ancylostoma braziliensevar. ceylanicum. Trop Geogr Med 18:48–52
Wilde H, Suankratay C, Thongkam C, Chaiyabutr N(2001) Human gongylonema infection in SoutheastAsia. J Travel Med 8:204–206
Wirtz WL (1982) Cerebrospinal nematodiasis due to theraccoon ascarid Baylisascaris procyonis. MS Thesis,Purdue University
Wise ME, Sorvillo FJ, Shafir SC, Ash LR, Berlin G(2005) Severe and fatal central nervous systemdisease in humans caused by Baylisascaris procyonis,the common roundworm of raccoons: a review ofcurrent literature. Microbes Infect 7:317–323
Woodruff AW (1970) Toxocariasis. BMJ 3:663–669Yamaguti S (1961) Systema helminthum. Interscience,
New York, pp 612–614Yasunaga H, Horiguchi H, Kuwabara K, Hashimoto H,
Matsuda S (2010) Clinical features of bowel anisa-kiasis in Japan. Am J Trop Med Hyg 83(1):104–105
Yong TS, Lee JH, Sim S, Lee J, Min DY, Chai JY, EomKS, Sohn WM, Lee SH, Rim HJ (2007) Differentialdiagnosis of Trichostrongylus and hookworm eggsvia PCR using ITS-1 sequence. Korean J Parasitol45:69–74
Yoshida Y, Okamoto K, Chiu JK (1968) Ancylostomaceylanicum infection in dogs, cats, and man inTaiwan. Am J Trop Med Hyg 17:378–381
Yoshida Y, Okamoto K, Matsuo K, Kwo EH, Retnas-abapathy A (1973) The occurrence of Ancylostomabraziliense (de Faria, 1910) and Ancylostoma cey-lanicum (Looss, 1911) in Malaysia. Southeast Asian JTrop Med Public Health 4:498–503
Yoshida Y, Kondo K, Kurimoto H, Fukutome S,Shirasaka S (1974) Comparative studies on Ancylos-toma braziliense and Ancylostoma ceylanicum. 3. Lifehistory in the definitive host. J Parasitol 60:636–641
Youn H (2009) Review of zoonotic parasites in medicaland veterinary fields in the republic of Korea. KoreanJ Parasitol 47:133–141
Zhu X, Chilton NB, Jacobs DE, Boes J, Gasser RB(1999) Characterisation of Ascaris from human andpig hosts by nuclear ribosomal DNA sequences. Int JParasitol 29:469–478
122 5 Nematode Zoonoses

6Arthropod Zoonoses
Abstract
Arthropod Zoonoses could be defined as ‘‘those arthropod diseases whichare naturally transmitted between (other) vertebrate animals and man’’.Infestation of dipteran fly larva could cause myiasis in animals and man.Pentastomiasis is a zoonotic disease which can occur in human beings.The disease occurs due to Armillifer and Linguatula species (FamiliesPorocephalidae and Linguatulidae); endoparasites of reptiles, birds andmammals. Tungiasis occurs due to the infestation of female sand fleaTunga (Sarcopsylla) penetrans and could result in tungiasis in dogs, cats,pigs, non-human primates and occasionally man. Tungiasis has beenreported from many countries. Zoonotic scabies occurs due to Sarcoptesscabiei which affects many mammal and marsupial species.
6.1 Myiasis
Class: InsectaOrder: Diptera
The disease occurs due to dipteran fly larvawhich infests live vertebrates viz. animals andhumans (Zumpt 1965). These larvae feed on theliving/dead tissue/body fluids of the host or oningested food (Francesconi and Lup 2012). Thelarvae can infest different locations and producespectrum of symptoms depending upon the lar-vae species and the host involved (Noutsis andMillikan 1994; Francesconi and Lup 2012).
6.1.1 Etiology
Although many species can cause the disease,the important etiological agents include:
6.1.1.1 Specific Parasites• Larvae of Cochliomyia hominivorax (screw
worm)• Larvae of Chrysoma bezziana• Furuncular myiasis due to larva of Cordylobia
anthropophaga• Furuncular myiasis due to larvae of Derma-
tobia hominis• Furuncular myiasis due to Cuterebra spp.• Larvae of Hypoderma spp.• Larvae of Oestrus ovis and Rhinoestrus
purpureus• Larvae of Gasterophilus spp.• Furuncular myiasis due to Wohlfahrtia spp.
6.1.1.2 Facultative or Semi SpecificMyiasis
• Due to larvae of Lucilia sericata, Sarcophaga,Parasarcophaga, Phormia, Paraphrominaspecies
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6_6, � Springer India 2013
123

6.1.1.3 Accidental Myiasis• Due to larvae of Musca domestica, Musca
stabulans, Fannia canicularis, F. scalaris
6.1.2 Epidemiology
The disease is worldwide in distribution. Highprevalence has been recorded from poor socio-economic regions of tropical and subtropicalcountries (Francesconi and Lup 2012). Animalsplay an important role and man generally acts asan accidental host. Poor hygiene and lowsocioeconomic status are the important risks forthe occurrence of the disease (Fernandes et al.2009; Marquez et al. 2007).
6.1.3 Clinical Signs in Animals
Myiasis could lead to severe production lossessuch as reduced milk yield, inferior quality ofhide, decreased weight and fertility losses(Francesconi and Lup 2012).
6.1.4 Clinical Signs in Man
Depending upon symptoms, human myiasis hasbeen discussed under following headings.
6.1.4.1 Cutaneous MyiasisThis is most frequently encountered form ofmyiasis (Diaz 2009).1. Furuncular myiasis: It occurs when dipteran
larvae penetrate healthy skin. Symptomsinclude erythematous, furuncle-like nodulecontaining one or more maggots in it. It mainlyoccurs due to Dermatobia hominis andCordylobia anthropophaga. Important clinicalsymptoms include pruritus, pain, and move-ment sensation (Mahal and Sperling 2012).
2. Migratory (creeping) myiasis: It occurs dueto aimless migration of dipteran larvathrough burrows in the skin. It producesmigratory patterns of the lesions. Clinical
symptoms include painful and migratoryswelling.
3. Wound myiasis: It results due to local tissuedestruction and further invasion into deeptissues.
6.1.4.2 Cavitary MyiasisCavitary myiasis occurs due to infestation ofbody cavities by the larvae. The symptoms varydepending upon the cavity or organ affected orinvolved. For example in ophthalmomyiasis,important clinical symptoms include vision lossand eye pain.
6.1.5 Diagnosis
The disease can be diagnosed from clinicalsigns, ultrasound examination or by detection ofthe larva.
6.1.6 Control
Improved personnel and environmental sanita-tion, measures for control of flies, maggot ther-apy and reducing animal myiasis can helpcontrol the infection.
6.2 Pentastomiasis
Class: PentastomidaFamily: Porocephalidae
6.2.1 Common Name/Synonyms
Porocephaliasis, Tongue worm infection, golfcaddy’s disease, halzoun, marrara
6.2.2 Etiology
Pentastomiasis is a zoonotic disease whichcan infect human beings. These parasites are
124 6 Arthropod Zoonoses

endoparasites of reptiles, birds and mammals.The disease occurs due to parasites belonging tofamilies Porocephalidae and Linguatulidae viz.Armillifer and Linguatula species. The diseasecan occur in two forms viz. visceral or naso-pharyngeal pentastomiasis. The visceral formoccurs when humans ingest infective eggs ofArmillifer armillatus or L. serrata and act asintermediate host.
Nasopharyngeal pentastomiasis occurs whenman ingests raw or undercooked infected inter-mediate host (e.g. sheep or goat) containingencysted nymphs of the parasite L. serrata.
6.2.3 Epidemiology
The disease is worldwide in distribution withmany reports from Asia and tropical Africa.A. armillatus is primarily found in Africa whereashuman cases due to L. serrata have been reportedfrom North Africa, Europe and Middle East(Acha and Szyfres 2006; Aynimode et al. 2010).Pentastomiasis among humans in China havebeen found to be associated with the ingestion ofraw or undercooked snakes (Min et al. 2008).
6.2.4 Transmission
Vertebrate animals including primates andhumans act as intermediate hosts (Lang et al.1987). Human beings become infected either afterconsumption of contaminated water or vegetablescontaminated by faeces of definitive host or due tothe naso bronchial secretions of infected snakes orcarnivores, or by eating raw or undercooked snakeor lizard (Machado et al. 2006).
6.2.5 Life Cycle
For Armillifier species, snakes act as definitivehosts and rodents and other wild mammals act asintermediate hosts. For Linguatula spp., herbiv-orous animals such as sheep, goat act as inter-mediate hosts and dogs, canids and some felids
act as definitive hosts. Intermediate hosts becomeinfected after the ingestion of the egg containedeither in faeces or in the sputum of the definitivehosts. The eggs develop to larva in the interme-diate host and then burrow towards the abdominalcavity. Larvae mature to nymphs and remain inthe viscera in an encysted form. Definitive hostsbecome infected after consumption of the inter-mediate host containing the encysted nymphs.
6.2.6 Clinical Signs in Man
The disease is generally not symptomatic butcould produce symptoms when encysted larvaeenlarge through molting and cause pressure orduring larval migration in vital organs. There arereports of vital organ collapse viz. lung (Stock1946), intestinal obstruction (Cannon 1942),peritonitis (Herzog et al. 1985) and glaucoma(Lang et al. 1987). Liver is another commonlyaffected organ.
6.2.7 Clinical Signs in Animals
In definitive hosts, Linguatula infections couldproduce symptoms such as nasal catarrah,sneezing and epistaxis (Acha and Szyfres 2006).In general, the infections remain asymptomaticin intermediate hosts.
6.2.8 Diagnosis
In definitive hosts, the disease can be diagnosedby the identification of the characteristic thick-shelled eggs containing an embryo with rudi-mentary legs. Intermediate host infections aredifficult to diagnose and may be diagnosed eitherby X-rays or histopathological examination.
6.2.9 Control
Improved personnel hygiene and avoid eatingraw or undercooked infected meat for preventionof the disease.
6.2 Pentastomiasis 125

6.3 Tungiasis
Order: SiphonapteraFamily: Tungidae
6.3.1 Synonyms
Chigoe, jigger flea infestation sand fleainfestation
6.3.2 Etiology
The disease occurs due to the infestation offemale sand flea Tunga (Sarcopsylla) penetrans.
6.3.3 Epidemiology
This flea could infest warm-blooded animalsincluding dogs, cats, pigs, non-human primatesand man. The disease has been reported fromCentral, South and Latin America, Caribbean,Africa and India (Leung et al. 2007).
6.3.4 Transmission
In endemic areas, human beings could becomeinfected when they walk barefoot on the soilcontaining the fleas.
6.3.5 Life Cycle
The fleas are hematophagous (Eisele et al. 2003;Fein et al. 2001) and male dies quickly after thecopulation. The female flea penetrates in thehost epidermis and lay eggs for 2–3 weeksbefore death. The eggs fall and mature intolarvae on the soil (Fein et al. 2001). The larvaedevelop to pupae and finally develop intoadult flea. The whole cycle is completed in18 days under favourable conditions (Leunget al. 2007).
6.3.6 Clinical Signs in Manand Animals
Clinical symptoms range from asymptomatic topruritic, painful ulceration having papular ornodular lesion with a central dark spot. The fleacommonly infests feet but could affect any partwhich comes in contact with the soil (Leunget al. 2007). The symptoms could be furtherdeteriorated with secondary bacterial infections.
6.3.7 Diagnosis
The disease can be diagnosed from clinicalsymptoms or by identification of flea fromcharacteristic lesions.
6.3.8 Control
Flea control measures, avoidance of walkingbarefoot can help prevent the infection.
6.4 Zoonotic Dermatitis
Zoonotic dermatitis occur in man primarily dueto three parasites1. Sarcoptes scabiei causing zoonotic scabies2. Tick infestations due to ticks of various
species3. Other acarid parasites such as parasites of the
families Cheyletiellidae, Dermanyssidae andMacronyssidae
6.4.1 Zoonotic Scabies
Phylum: ArthropodaClass: ArachnidaFamily: Sarcoptidae
6.4.1.1 Common Name/SynonymsAcariasis, Mange, sarcoptic itch
126 6 Arthropod Zoonoses

6.4.1.2 EtiologyThe disease occurs due to Sarcoptes scabieiwhich affects many mammal and marsupialspecies. There are many subtypes of the parasitewhich could be host specific. Important subtypesinclude S. scabiei var hominis which primarilyinfect humans, S. scabiei var. canis, S. scabieivar bovis, S. scabiei var. equi, S. scabiei var suisand S. scabiei var ovis. Humans could alsobecome infected by many of these subtypes. Inaddition to these, humans can also becomeinfected with Notoedres cati (notoedric mange)present in cats and Trixacarus caviae (guineapig mite) affecting guinea pigs.
6.4.1.3 EpidemiologyThe parasite S. scabies is worldwide in distri-bution. Human disease particularly occurs inpersons belonging to poor and lower socioeco-nomic groups.
6.4.1.4 TransmissionHuman beings become infected either throughdirect contact with infected animal or by indirectcontact with fomites (Arlian et al. 1984).
6.4.1.5 Life CycleThe parasite burrows tunnels in the skin andlives there. The parasite completes its life cycleon the host skin and cannot survive in theenvironment for long period of time. Males dieafter copulation. The female form tunnels in theskin and lay eggs. The larvae hatch and migratetowards the surface of the skin. Larvae furthermolt to nymphal and adult parasite.
6.4.1.6 Clinical Signs in ManHuman cases due to S. scabiei var. canis havebeen reported (Arlian et al. 1984; Weese et al.2002). Zoonotic scabies is generally a self lim-iting disease in human beings. In humans, theparasite may cause intense pruritus commonlyaffecting arms, legs, thoracic and abdominal
regions. The zoonotic infections normally do notcause burrows and produce symptoms such asdermatitis, vesicles and papules.
6.4.1.7 Clinical Signs in AnimalsClinical symptoms in animals include intensepruritus and are commonly found on legs, faceand trunk (Arlian et al. 1984).
6.4.1.8 DiagnosisThe disease can be diagnosed from clinical signsand identification of the mite from the lesions.
6.4.1.9 ControlPrevention and control of the parasite in animalsand using protective measures can help preventinfection in human beings.
6.4.2 Tick Infestations
Class: ArachnidaOrder: Acarina
6.4.2.1 FamilyArgasidae (soft ticks) and Ixodidae (hard ticks)
6.4.2.2 EtiologyMany species can cause tick infestations in man.There are approximately 12 argasid (Argasand Ornithodos), 20 ixodid (4 Amblyomma,7 Dermacentor species, 3 Haemaphysalis spe-cies, 2 Hyalomma species and 6 Ixodes species)tick species which can infest man (Estrada-Penand Jongejan 1999). The detailed reviews ontick infestations in human beings are available inthe literature (Estrada-Pen and Jongejan 1999).
6.4.2.3 EpidemiologyThe ticks are distributed across the globevarying with species and regions. Many human
6.4 Zoonotic Dermatitis 127

cases have been recorded in the literature(Estrada-Pen and Jongejan 1999).
6.4.2.4 TransmissionInfected animals shed adult or larvae in theenvironment from where they can infect humanbeings.
6.4.2.5 Clinical Signs in ManAccidental infections normally occur in humanbeings. Tick infestations could lead to paralyses,toxicities and allergic reactions (Estrada-Pen andJongejan 1999; Gauci et al. 1989). Additionally,ticks can also transmit many important vectorborne zoonotic diseases in animals and man(Sonenshine 1991). Paralysis due to bite ofOtobius megnini (Peacock 1958), ear infesta-tions (Chellappa 1973), allergic reactions (Gauciet al. 1989), irritation (Eads and Campos 1984;Uilenberg et al. 1980) and toxic reactions fol-lowing the bites of A. brumpti and O. moubata(Sonenshine 1993) have been reported.
6.4.2.6 Clinical Signs in AnimalsClinical symptoms are generally similar as inman. Additionally, ticks can transmit manyimportant vector borne zoonotic diseases inanimals and man (Sonenshine 1991).
6.4.2.7 DiagnosisThe disease can be diagnosed by removal andidentification of tick species involved.
6.4.2.8 ControlImproved personnel habitat and control of ticksin animals can help prevent human infections.
6.4.3 Dermatitis Due to AcaridParasites Belonging to FamiliesCheyletiellidae, Dermanyssidaeand Macronyssidae
Class: ArachnidaOrder: Acarina
6.4.3.1 Etiology
1. Cheyletiella parasitovorax (rabbit parasite),C. yasguri (dog parasite) and C. blakei (catparasite)
2. Dermanyssus gallinae (chicken, turkeys,pigeons, canaries, wild fowl parasite)
3. Liponyssoides sanguineus (small rodentparasite)
4. Ornithonyssus bacoti (rodents and small mar-supials parasite), O. bursa and O. sylvarium(birds parasite)
6.4.3.2 EpidemiologyMost of these mites are worldwide indistribution.
6.4.3.3 TransmissionClose contact with respective animal hosts isresponsible for transmission of the disease.
6.4.3.4 Life CycleThe female mite lays eggs in burrows, nests orcracks or attached to animal hairs dependingupon the host involved. These eggs hatch andrelease larvae which further develop to becomeadults.
6.4.3.5 Clinical Signs in ManThe primary sign is dermatitis and parasite mayinfect different body parts such as thorax, arms,thighs, etc. Bite of these mites could producesevere symptoms such as intense pruritis, aller-gic dermatitis, urticaria and skin irritationdepending upon the species involved (Acha andSzyfres 2003).
6.4.3.6 Clinical Signs in AnimalsIn the animal hosts, symptoms such as dandruff,alopecia, pruritis, scaly condition, anemiaand irritation could be seen varying upon thehost and species involved (Acha and Szyfres2003).
128 6 Arthropod Zoonoses

6.4.3.7 DiagnosisIdentification of causative agents using micro-scopic or skin scrapings can help diagnose thedisease.
6.4.3.8 ControlThe infected animals should be properly treatedwith acaricides (Acha and Szyfres 2003).
References
Acha PN, Szyfres B (2006) Zoonoses and communicablediseases common to man and animals, vol III.Parasitosis. Pan American Health Organization, USA
Acha PN, Szyfres B (2003) Zoonoses and communicablediseases common to man and animals. Volume 3.Parasitoses, 3rd ed. Scientific and Technical Publica-tion No. 580, Washington DC
Arlian LG, Runyan RA, Estes SA (1984) Cross infectiv-ity of Sarcoptes scabiei. J Am Acad Dermatol10:979–986
Ayinmode AB, Adedokun AO, Aina A, Taiwo V (2010)The zoonotic implications of pentastomiasis in theroyal python (Python regius). Ghana Med J44(3):115–118
Cannon DA (1942) Linguatulid infestation of man. AnnTrop Med Parasitol 36:160–167
Chellappa DJ (1973) Note on spinose ear tick infestationin man and domestic animals in India and its control.Madras Agric J 60:656–658
Diaz JH (2009) Myiasis and tungiasis. In: Mandell GL,Bennett JE, Dolin R (eds) Mandell, Douglas, andBennett’s principles and practice of infectious dis-eases, vol 2. Elsevier, Philadelphia
Eads RB, Campos EG (1984) Human parasitism byOtobius megnini (Acari: Argasidae) in New Mexico,USA. J Med Entomol 21:244
Eisele M, Heukelbach J, Van Marck E (2003) Investi-gations on the biology, epidemiology, pathology andcontrol of Tunga penetrans in Brazil: I. Naturalhistory of tungiasis in man. Parasitol Res 90(2):87–99
Estrada-Pen AA, Jongejan F (1999) Ticks feeding onhumans: a review of records on human-bitingIxodoidea with special reference to pathogen trans-mission. Expt Appl Acarol 23:685–715
Fein H, Naseem S, Witte D (2001) Tungiasis in NorthAmerica: a report of 2 cases in internationallyadopted children. J Pediatr 139:744–746
Fernandes LF, Pimenta FC, Fernandes FF (2009) Firstreport of human myiasis in Goia S state, Brazil:
frequency of different types of myiasis, their variousetiological agents, and associated factors. J Parasitol95:32–38
Francesconi F, Lup O (2012) Myiasis. Clin MicrobiolRev 25(1):79–105
Gauci M, Loh RK, Stone BF, Thong YH (1989) Allergicreactions to the Australian paralysis tick, Ixodesholocyclus: diagnostic evaluation by skin test andradioimmunoassay. Clin Exp Allergy 19:279–283
Herzog U, Marty P, Zak F (1985) Pentastomiasis: casereport of an acute abdominal emergency. Acta Trop42:261–271
Lang Y, Garzozi H, Epstein Z, Barkay S, Gold D, LengyJ (1987) Intraocular pentastomiasis causing unilateralglaucoma. Br J Ophthalmol 71:391–395
Leung AKC, Woo T, Robson WLM, Trotter MJ (2007) Atourist with tungiasis. Can Med Assoc J177(4):343–344
Machado MAC, Makdissi FF, Canedo LF, Martino RB,Crescentini F, Chieffi PP, Bacchella T, MachadoMCC (2006) Unusual case of pentastomiasis mim-icking liver tumor. J Gastroenterol Hepatol21:1218–1220
Mahal JJ, Sperling JD (2012) Furuncular myiasis fromDermatobia hominus: a case of human botfly infes-tation. J Emerg Med 43(4):618–621
Marquez AT, Mattos MD, Nascimento SB (2007)Myiasis associated with some socioeconomic factorsin five urban areas of the State of Rio de Janeiro. RevSoc Bras Med Trop 40:175–180
Min HY, Fang W, Lan FT (2008) Human pentastomiasisin China: case report and literature review. J Parasitol94(6):1295–1298
Noutsis C, Millikan LE (1994) Myiasis. Dermatol Clin12:729–736
Peacock PB (1958) Tick paralysis or poliomyelitis. SouthAfr J Med Sci 32:201–202
Sonenshine DE (1991) Biology of ticks, vol 1. OxfordUniversity Press, Oxford
Sonenshine DE (1993) Biology of ticks, vol 2. OxfordUniversity Press, Oxford
Stock FE (1946) Collapse of the lung and porocephalosis.Trans R Soc Trop Med Hyg 40:101–102
Uilenberg G, Hoogstraal H, Klein JM (1980) Les tiques(Ixodoidea) de Madagascar et leur role vecteur. ArchInst Pasteur de Madagascar, Special Number,pp 1–153
Weese JS, Peregrine AS, Armstrong J (2002) Occupa-tional health and safety in small animal veterinarypractice: part II—parasitic zoonotic diseases. Can VetJ 43:799–802
Zumpt F (1965) Myiasis in man and animals in the oldWorld. Butterworths, London
6.4 Zoonotic Dermatitis 129

About the Authors
Dr. B. B. Singh DhaliwalDr. Balbir Bagicha Singh Dhaliwal (Ph.D.) isworking as Assistant Professor (VeterinaryPublic Health) with Guru Angad Dev Veterinary& Animal Sciences University’s School ofPublic Health & Zoonoses (Ludhiana, India). Heparticipated as Visiting Scientist at Centre forFood Borne & Animal Parasitology, OIE Ref-erence Lab (Trichinella) & Collaborating Centre(Food Borne & Zoonotic Parasites), CanadianFood Inspection Agency, Saskatoon (Canada)for a period of six months. He is working in thefield of Food Borne & Zoonotic Parasitologysince the last 13 years. He is a recipient of Dr.V. S. Alwar memorial award (2004), TheFlemish Vlaamse Interuniversitaire Raad—Uni-versity Development Corporation (VLIR–UOS)grant (2007) and the World Association forAdvancement of Veterinary ParasitologyScholarship funding (2013). He has severalresearch publications in the field of Food Borne& Zoonotic Parasitology in international andnational journals of repute.
Dr. P. D. JuyalDr. P.D. Juyal served at RAU, Pusa (Bihar),GBPU&T, Pantnagar and PAU, Ludhiana and as
Professor and Head Department of VeterinaryParasitology at Guru Angad Dev Veterinary &Animal Sciences University, Ludhiana (India).Presently, Dr. Juyal is working as Registrar,GADVASU, Ludhiana (India). He has publishedmore than 189 research and extension papersand six practical manuals for UG students. He isEx-Vice-President of Indian Society for Parasi-tology and General Secretary of Indian Associ-ation for Advancement of VeterinaryParasitology (IAAVP). He is national fellow ofIAAVP and fellow of National Academy ofVeterinary Sciences (NAVSc). He is also amember of the editorial board of Journal ofParasitic Diseases, Journal of Laboratory Phy-sicians (New Delhi), and Pakistan J. Vet. &A. Sc. (Lahore). Besides, he is also a nominee/representative of CPCSEA for many pharmacycolleges in Punjab. He is a recipient of the Prof.B.V. Rao Gold Medal (1998) for research pub-lications in journals.
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6, � Springer India 2013
131

Index
AAcanthocephalus, 83Accidental myiasis, 124African trypanosomosis, 15Amebiosis, 17Amphixenosis, 3Ancylostoma braziliense, 92Ancylostoma caninum, 92Ancylostoma ceylanicum, 92Ancylostoma tubaeforme, 92Angiostrongylosis, 85Angiostrongylus cantonensis, 85Anisakiosis, 86Anisakis, 87Anthropozoonoses, 3Argas, 127Armillifer, 125Armillifer armillatus, 125Ascariosis, 88Ascaris lumbricoides, 88Ascaris suum, 88Atypical human trypanosomosis, 35Austrobilharzia, 42
BBabesia divergens, 19Babesia microti, 19Babesiosis, 19Balantidiosis, 21Balantidium coli, 21Baylisascariasis, 89Baylisascaris procyonis, 89Bertiellosis, 78
CCapillaria aerophila, 91Capillaria hepatica, 91Capillaria philippinensis, 91Capillariasis, 91Corynebacterium bovis, 76
Cattle related parasitic zoonoses, 3Cercarial dermatitis, 41Chagas disease, 21Cheyletiella parasitovorax, 128Chrysoma bezziana, 123Classification of parasitic zoonoses, 2Clonorchiosis, 52Clonorchis sinensis, 52Cochilomyia hominivorax, 123Coenurosis, 63Coenurus brauni, 66Coenurus cerebralis, 63Coenurus serialis, 63Contracaecum, 87Cordylobia anthropophaga, 123, 124Cryptosporidiosis, 22Cryptosporidium parvum, 22Cutaneous larva migrans, 92Cutaneous Leishmaniosis, 28Cyclospora cayetanensis, 33Cyclosporosis, 33Cyclozoonoses, 3Cysticercus cellulosae, 76
DDermacentor, 127Dermanyssus gallinae, 128Dermatobia hominis, 124Dendritobilharzia, 42Dicrocoeliasis, 43Dicrocoelium dendriticum, 44Dioctophyma renale, 93Dioctophymosis, 93Diphyllobothriosis, 67Diphyllobothrium, 67Diphyllobothrium hospes, 43Diphyllobothrium latum, 67Diphyllobothrium nihonkaiense, 67Dipylidiosis, 68Dipylidium caninum, 69Direct parasitic zoonoses, 2
B. B. S. Dhaliwal and P. D. Juyal, Parasitic Zoonoses,DOI: 10.1007/978-81-322-1551-6, � Springer India 2013
133

Dracunculiasis, 94Dracunculus medinensis, 95
EEchinochasmus japonicus, 45Echinococcus, 71Echinostoma hortense, 45Echinococcus echinatum, 45Echinococcus granulosus, 71Echinococcus multilocularis, 71, 72Echinococcus oligarthrus, 71, 72Echinococcus vogeli, 71, 72Echinococcosis, 71Echinostomosis, 45Entamoeba histolytica, 17Entamoeba polecki, 17
FFannia canicularis, 124Fasciola gigantica, 46Fasciola hepatica, 46Fasciolopsiosis, 47Fasciolopsis buski, 48Fasciolosis, 46Fish related parasitic zoonoses, 3Fish, shellfish and mollusc borne parasitic
zoonoses, 6Food borne parasitic zoonoses, 9
GGastrodiscoides hominis, 49Gastrodiscoidosis, 49Giardia intestinalis, 25Giardiosis, 25Gigantobilharzia, 42Gnathostoma, 96Gnathostoma nipponicum, 96Gnathostoma spinigerum, 96Gnathostomosis, 96Gongylonema pulchrum, 97Gongylonemosis, 97
HHaemaphysalis, 127Halicephalobus gingivalis, 101Haplorchiosis, 51Heterophyosis, 49Heterophyosis due to Heterophyes species, 50Hymenolepiosis, 79
IInermicapsiferosis, 79Infections caused by free-living amoebae, 33
LLagochilascariosis, 99Lagochilascaris, 99Leishmania, 28Leishmania braziliensis, 28Leishmaniasis donovani, 27Leishmaniasis infantum, 27Leishmaniasis major, 99Leishmaniasis mexicana, 28Leishmaniasis minor, 99Leishmaniasis sprenti, 99Leishmaniasis tropica, 28Leishmaniasis turgida, 99Leishmaniosis, 26Linguatula, 124Linguatula serrata, 124Liponyssoides sanguineus, 128Livestock related parasitic
zoonoses, 4
MMalaria in nonhuman primates, 35Mammomonogamus, 100Mammomonogamus laryngeus, 100Meat borne parasitic zoonoses, 10Mesocestoidosis, 79Metagonimosis, 49Metagonimus miyatai, 49Metagonimus takahashii, 49Metagonimus yokogawai, 49Metazoonoses, 3Metorchiosis (Canadian liver fluke), 53Micronema deletrix, 101Micronemosis, 101Microsporidiosis, 35Milk borne parasitic zoonoses, 12Musca domestica, 124Myiasis, 124
NNanophyetosis, 51Nanophyetus salmincola, 51Nanophyetus schikhobalowi, 51
OOccupational parasitic zoonoses, 7Oesophagostomiasis aculeatum, 102Oesophagostomiasis, 102Oesophagostomum bifurcum, 102Opisthorchiosis, 52Ornithodos, 127Ornithonyssus bacoti, 128Other cestode zoonoses, 78Other Liver flukes, 52Other Metagonimus species, 50
134 Index

PParagonimosis, 53Paragonimus westermani, 54Parasitism, 1Pentastomiosis, 124Pet animal related parasitic zoonoses, 5Pig related parasitic zoonoses, 3Poultry related parasitic zoonoses, 13Pseudoterranova, 87
RRaillietinosis, 79Raw vegetables/plant borne parasitic zoonoses, 13Reptile, amphibian borne parasitic zoonoses, 13Rhinoestrus purpureus, 123
SSarcocystiosis, 30Sarcoptes scabiei, 126Sarcocystis hominis, 30Sarcocystis miescheriana, 30Sarcocystis suihominis, 30Saprozoonoses, 3Schistosoma japonicum, 56Schistosoma malayi, 56Schistosoma mansoni, 56Sheep related parasitic zoonoses, 3Soil transmitted parasitic zoonoses, 13Spirometra erinaceieuropaei, 74Sparganosis, 74Spirometra mansoni, 74Spirometra mansonoides, 74Strongyloides fuelleborni, 103Strongyloides stercoralis, 103Strongyloidiasis, 103
TTaenia axei, 108Taenia serialis, 66Taenia solium, 76Taeniidae saginata, 76Taeniosis and cysticercosis, 76Ternidens derminutus, 102Thelazia callipaeda, 105Thelaziidae californiensis, 105Thelaziidae callipaeda, 105Thelaziidae rhodesii, 105Thelaziasis, 104Tick Infestations, 127Toxocara, 110Toxocara canis, 110
Toxocara cati, 110Toxocara pteropodis, 110Toxocara vitulorum, 110Toxoplasma gondii, 32Toxoplasmosis, 32Trematosaurus brauni, 66Trichinella, 106Trichinella multiceps, 66Trichinella murrelli, 106Trichinella nativa, 106Trichinella nelsoni, 106Trichinella papuae, 106Trichinella psudospiralis, 106Trichinella spiralis, 106Trichinella britovi, 106Trichinosis, 105Trichobilharzia, 42Trichostrongylosis, 108Trichostrongylus brevis, 108Trichostrongylus capricola, 108Trichostrongylus colubriformis, 108Trichostrongylus orientalis, 108Trichostrongylus probolurus, 108Trichostrongylus skrjabini, 108Trichostrongylus vitrinus, 108Trichuriosis of animal origin, 109Trichuris suis, 109Trichuris vulpis, 109Trypanosoma cruzi, 21Trypanosomatidae brucei gambiense, 16Trypanosomatidae brucei rhodesiense, 16Tunga (Sarcopsylla) penetrans, 126Tungosis, 126
VVector borne parasitic zoonoses, 13Visceral larva migrans, 110Visceral Leishmaniosis, 27
WWater borne parasitic zoonoses, 11Wildlife related parasitic zoonoses, 4Wohlfahrtia spp, 123
ZZooanthroponoses, 3zoonoses, 1Zoonotic ancylostomiasis, 112Zoonotic dermatitis, 126Zoonotic filariasis, 114
Index 135