Ortho+Regional - FRCA Headstart
80
Orthopedic & Regional Chris Smales
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Ortho+Regional - FRCA Headstart

Orthopedic & Regional
Chris Smales

Introduction• Orthopeadics – General principles• Emergencies• The tourniquet• Regional – General principles• ‘Stop before you block’• Upper limb blocks• Trunk blocks• Lower limb• Recent past questions

Ortho
• >160,000 Major joints/ year in UK• Shift towards minimally invasive, early mobilisation, shorter stays
• Diverse population but often elderly, obese, poor functional status (?arthritis vs Cardioresp), multisystem comorbidities (RA)
• High risk VTE• Painful surgeries (regional)

Enhanced recovery for joint arthroplasty
• 4 key elements• Improve pre-‐op care• Reduce physical stress of op• Decreased post-‐op discomfort• Improve post op mobility• Pre-‐op Gabapentin/ Dex, minimise fasting• Intraop – low dose spinal/ opioid free, TXA, avoid drains, sensible fluid, large vol LA infiltration
• Post-‐op – multimodal analgesia, early mobilisation/ physio

Benefits of Regional in Ortho
• Good post-‐op pain relief and decreased PONV• Decreased risk of VTE (alone or with GA)• Reduced bleeding at surgical site (particularly neuroaxial blocks – surgeons prefer as can get better fixation)
• If no sedation then decreased post op cognitive impairment

Emergencies
• Fat Embolism Syndrome (FES)• Embolisation of fat common, FES rare• Rate reduced by early fixation and avoidance of IM nailing
• Usually patients with long bone fractures

FES
• Major – Resp – tachypnoea/dyspnoea, bilat creps, haemoptysis, bilat shadowing on CXR
Neuro – confusion, drowsinessPetechial rash• Minor – Tachycardia, retinal signs (petechiae), Jaundice, oliguria
• Lab tests – thrombocytopenia, sudden ~20% decrease Hb, raised ESR, fat macroglobulaemia

FES Treatment
• Supportive• Early oxygen may prevent onset of syndrome• 10-‐40% may need mechanical ventilation• Debate about use of steroids• Takes around 7 days to resolve

Bone cement implantation syndrome (BCIS)
• Acrylic polymer cements• Hypoxia, hypotension, cardiovascular collapse• Aetiology still not certain, likely fat embolism• BCIS classification – Grade 1-‐3 (3 worst)• Usually happens just after cementing• Ability of patient to withstand should be anticipated
• Worsened by hypovolaemia, Anaesthetic technique make no difference

Prevention/ Treatment
• Suction of bone cavity (remove fat/air) during cementing drastically reduced incidence
• Increased BP measurement frequency + react• Hydrate prior to cement• Increase Fi02, stop N20• Some suggestion alpha agonists superior to adrenaline in resuscitating these patients

Compartment Syndrome
• Increased pressure in closed compartment compromises blood flow leading to ischaemia, necrosis and loss of function
• Irreversible damage can occur in under 4 hours. Initially limb threatening but can lead to systemic organ dysfunction
• Suspect in an significant limb trauma (event w/o fracture). Care in patients with concurrent spinal injuries – may mask symptoms

Signs & Symptoms
• Pain over affected compartment – worse on passive stretching
• Tense swelling / drum like skin• Parasthesia in distribution of nerves traversing compartment
• Weakness/ paralysis is a late sign• Distal pulses usually present• Compartment pressure within 30mmHg of DBP diagnostic

Special considerations• Can occur with open fractures• Do not elevate limb, will further decrease perfusion
• Release all bandages, casts etc to see if decreases symptoms, urgent fasciotomies may be required
• Care with bleeding post fasciotomy• Ensure well hydrated + good urine output (Myoglobulinuriamaximal post reperfusion)
• Avoid regional in high risk patients (high tibial/ forearm fractures) as masks early symptoms

Tourniquets• Produce bloodless field +/-‐ expressive exsanguination (contraindicated in infection, tumour, DVT)
• Pneumatic safer than mechanical (lower pressure)
• PVD is relative contraindication• Avoid in severe crush injuries• Controversial in Sickle cell – sickling in anoxic conditions so exsanguinate limb first and reduce tourniquet time as much as able if needed.

Continued…• Preferably apply to upper arm or thigh (better pressure distribution)
• Calf only is healthy patient and for <1 hour• Cuff width 20% > than upper limb circumference, 40% > thigh, apply over area of greatest limb circumference
• Pressures – UL = SBP + 50mmHg, LL = 2XSBP• Deflate every 1 hour if poss, do not exceed 2• Increased HR + DBP common under GA after 1-‐2 hours, less with neuroaxial blocks

Regional Anaesthesia• Know your anatomy• Use Ultrasound +/-‐ nerve stimulation to improve accuracy/ decrease complications
• 4 key elements to US:• Image capture• Image optimisation• Image interpretation• Needling techniques• NB. Always use highest frequency transducer available for the depth of your target

Ultrasound
• Once transducer lightly applied to skin 4 hand movements to optimise image (P.A.R.T.)
• P – Pressure – don’t press to hard + distort anatomy (artery non-‐compressible)
• A – Align – slide across skin tracking structures/nerves to find optimal injection point
• R – Rotate – twist to see short-‐axis view• T – Tilt – rock side to side and heal-‐toe to get best reflection of nerve

• Never advance needle if you cant see tip• Never deliberately contact the nerve• Observe injection – if cant see LA spreading ?Intravascular or needle tip not in scan plane
• Injection should be low pressure and painless – stop and reposition if not
• If nerve swells, stop and reposition

For any Block question
• S – Sterile equipment• L – Light source• I – IV access• M – Monitoring• R – Resusitation equipment• A – Assistant trained in RA• G – Ability to convert to GA• Get easy marks, pre-‐assess and consent patient

Stop before you block
• Wrong sided peripheral nerve blocks rare but potentially serious consequences
• Can cause nerve injury, LA toxicity, delayed discharge due to poor mobility, may even lead to wrong side surgery!
• SALG 2010 – analysed 67 cases and recommended surgeons marked surgical site prior to PNB as per WHO checklist

Causes
• Distraction in Anaesthetic room• Time delay between WHO and performing block (e.g. Femoral blocked performed after difficult spinal)
• Covering surgical marks with blankets to keep patients warm
• Personnel performing PNB not doing regular block lists

• Patient requires turning (e.g. Femoral then posterior approach sciatic block)
• No stop immediately before needle insertion. Anaesthetist and ODP should double check by visualising surgical arrow, ask patients to confirm side if awake or double check with consent form if not

Upper limb blocks
• The brachial plexus


Interscalene
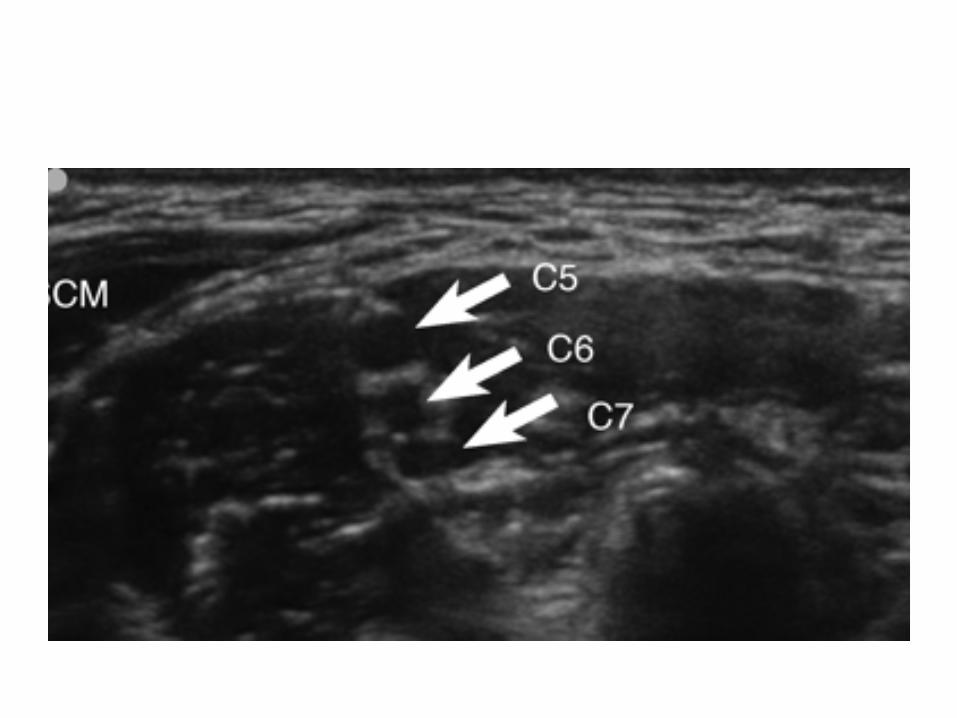
• Shoulder + upper arm surgery• C5,6,7 nerve ROOTS travel superficially through the interscalene groove (between scalenus anterior + medius)
• Traffic light appearance on US• C7 lies close to vertebral artery


IS Block• Supine, head facing contralateral (sniff to see interscalene groove)
• Depth 1-‐4cm• 25-‐50mm short beveled, faceted, echogenic needle (e.g. stimiplex)
• In-‐plane (usually in UK)• Post SCM boarder at level of cricoid for injection• 15-‐20mls of LA (less for analgesia)• Phrenic nerve palsy very likely (less if inject near C6)• Pec + deltoid twitch is using nerve stimulator (0.2-‐0.5mA)

Supraclavicular block
• Arm and hand surgery• TRUNKS and DIVISIONS pass over 1st rib, posterolateral to subclavian artery
• Beware pneumothorax• Don’t miss inferior plexus beneath artery• Distal top up may be required (otherwise takes a long time)

Supra-‐clavicular

SC Block
• Supine, arm adducted resting on abdomen• Transducer parallel to clavicle in supra-‐clavicular fossa
• 50mm Stimiplex• In-‐plane• 10-‐20mls of LA (ensure good spread)• Nerve stimulator will cause finger flexion and extension in the inferior trunks

Infra-‐clavicular
• Arm and hand surgery• Trunks and divisions pass over 1st rib and under mid-‐point of clavicle to form CORDS
• 3 cords lie medial, posterior and lateral in relation to axillary artery deep to Pec Minor
• Beware pneumothorax• Beware vessel puncture – cant compress!


IC block
• Position as for SC block• Transducer parallel to clavicle but beneath it• 50mm Stimiplex, in-‐plave• 15-‐20mls of LA• Quicker onset than SC block in theory

Axillary Brachial Plexus Block
• Forearm and hand surgery• The cords divide into TERMINAL BRANCHES in the axilla
• Block MN, UN & RN + Musculocutaneous nerve (leaves plexus high and lies in choracobrachialis)
• Axillary artery is again the reference structure
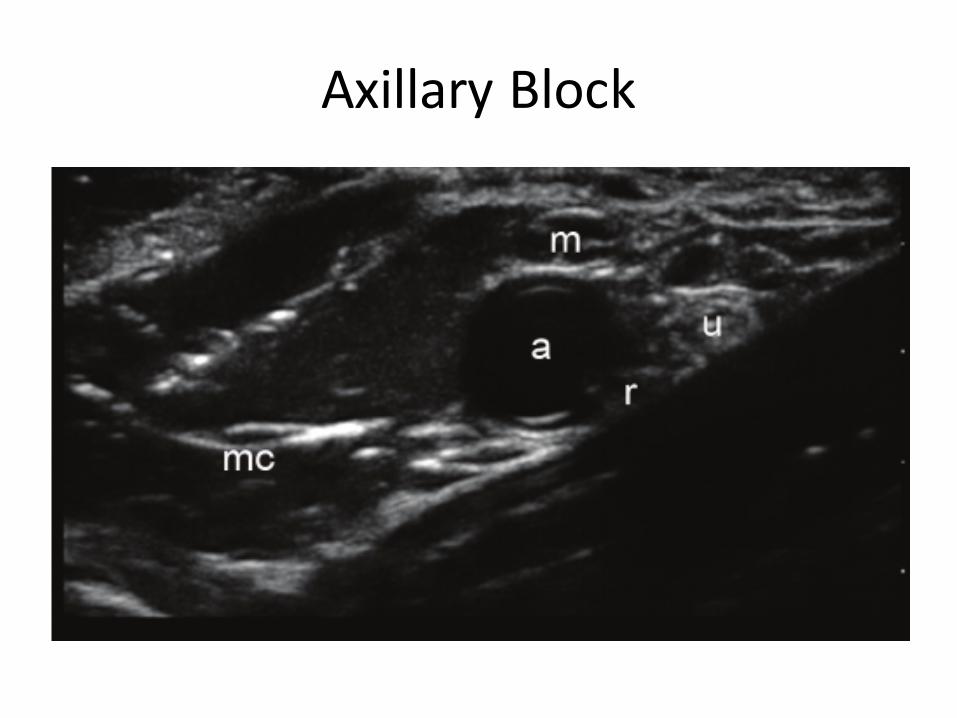
Axillary Block

Axillary block
• Supine with arm abducted, hand behind head• Transducer over the anterior axillary fold (pec major insertion)
• 50mm Stimiplex• 15-‐25mls of LA

Distal blocks of M, U, R
• Radial – block over lateral humerus lower 1/3rd of arm deep to triceps
• Median – supinate arm and block mid forearm, lie medial to brachial artery (trace down from antecubital fossa)
• Ulnar – abduct arm and block just beneath medial condyl of elbow. Sits next to the ulnar artery beneath flexor carpi ulnaris
• 2-‐5mls of LA per nerve sufficient

How to block Anterior Neck
• Superficial cervical plexus block• Classically for carotid surgery• Will be blocked with interscalene block• Supine patient, head turned to contralateral side
• Palpate posterior boarder of SCM at level of cricoid cartilage (as per ISBPB) then scan cranially observing C5 & 6 nerve roots move towards their respective transverse processes

SCP
• At the level of C5 the cervical plexus is seen as hyperechoic beads in the fascial plane just beneath SCM
• 4 nerves blocked:• Greater Auricular• Lesser Occipital• Transverse cervical• Supraclavicular

• Can do deep cervical plexus block – high risk of vertebral artery or subarachnoid injection + not necessary
• 10% require LA supplementation by surgeon (around angle of jaw if high bifurcation or large retraction needed)
• Don’t press to hard (carotid plaque)• Inject around carotid sheath (NOT within), vagus lies within

Trunk Blocks
• Anterior Rami of T6-‐L1 supply sensation to anterior abdo wall
• Intercostal nerves run between internal oblique and transversus abdominus then pierce rectus sheath to supply abdo wall
• Deeper blocks so use 100mm needle


Rectus sheath Block
• For midline abdo surgery• Transducer placed transversely across abdomen superior and lateral to umbilicus
• Pass needle directly through rectus muscle and inject LA between the muscle and the posterior rectus sheath
• High volume blocks


Transversus abdominal plane (TAP)
• Typically for surgery below umbilicus (unilateral e.g. open appendix or bilateral for midline incision/ LSCS)
• Place transducer transversely at midpoint between inferior costal boarder and iliac crest posterior to the mid-‐axillary line


Ilioinguinal & Iliohypogastric
• Post-‐op analgesia for inguinal hernia repair• Anterior ramus of L1 divides into above nerves which pass close to the ASIS in the same plane before piercing the internal oblique to supply the superficial tissues of the inguinal and pubic regions
• Place transducer next to ASIS pointing towards umbilicus. 2-‐10mls of LA


Pec + Serratus blocks
• Pec 1 – LA infiltrated between Pec Major & Pec Minor (breast augmentation pain)
• Pec 2 – between Pec minor & Serratus Anterior (mastectomy + axillary surgery)
• Serratus block – Lat dorsi + Serratus anteriour (move extensive surgery e.g. Lat dorsi flap reconstruction)

• Supine patient with arm abducted to 90 degrees
• Transducer at level of 2nd rib perpendicular to rib just medial to acromioclavicular joint
• Identify axillary artery + vein deep to muscles• 50-‐100mm Needle• 20-‐30 mls of LA

• Image of pec 1 and 2 block

Pec 2 block


Lower limb blocks
• The lumbar plexus


Lumbar plexus Block• Unilateral analgesia for hip, anterior thigh or knee surgery
• Ventral rami L1-‐4 pass into psoas to form lumbar plexus which gives rise to:-‐
• Ilioinguinal + iliohypogastric (L1 + some T12 for iliohypogastric)
• Genitofemoral (L1-‐2)• Lateral femoral cutaneous (L2-‐3)• Femoral (L2-‐4)• Obturator (L2-‐4)

How to block
• Tuffier’s line (L4). Psoas deep to transverse processes of L2-‐4 approx 2-‐5cm lateral to midline
• Position patient lateral, operative site up• Transducer placed along Tuffier’s line• In-‐plane injection of 10-‐30mls of LA, 100mm needle required


Femoral nerve block
• Femoral or knee surgery analgesia (need to combine with obturator and sciatic block for knee anaesthesia)
• NAVY• Transducer over femoral artery parallel and just beneath inguinal ligament
• 100mm needle, 10-‐20mls of LA


Sciatic nerve blocks• Exam favourite as many different places to block• Continuation of the sacral plexus (formed by anterior divisions of L4-‐5 + S1-‐3)
• Exits pelvis via greater sciatic foramen anterior to the Piriformis muscle. Runs deep to gluteus maximus
• Passes into the thigh between the ischialtuberosity and the greater trocanter. Divides at the apex of the popliteal fossa into tibial and common peroneal nerves (supply posterior knee, foot and ankle)

Sciatic blocks
• 1 anterior (Beck’s) and 4 posterior approaches described
• Posterior approaches are parasacral(Mansour), transgluteal(Labat), subgluteal(Raj) and popliteal (if it hasn’t divided yet)
• Parasacral and transgluteal rarely done as nerve lies deep and offers no real benefit

Subgluteal (Raj Approach)
• In subgluteal region the Sciatic lies medial to Biceps Femoris, lateral to semitendinosus and posterior to adductor magnus

Popliteal
• Scan in popliteal crease, lies medially to popliteal artery, scan distally to see bifurcation into tibial + common peroneal

Beck’s (Anterior) approach

Becks
• Draw line from ASIS to pubic tubercle (represents inguinal ligament)
• Draw a parallel line from the greater trochanter
• Draw a perpendicular line from first to second line and this is the injection point
• Hit lesser trochanter with needle and walk of it medially advancing 2cm then inject

Ankle block
• 5 nerves to block: -‐• Tibial (Sciatic)• Deep peroneal (Sciatic – common peroneal)• Superficial peroneal (Sciatic – common peroneal)
• Sural (Sciatic – from tibial and common peroneal)
• Saphenous (Femoral)


Landmarks for block• Posterior tibial – LA next to posterior tibial artery behind medial malleolus
• Sural – inject LA in a band between Achilles tendon and lateral malleolus
• Superficial peroneal – subcut band of LA from lateral malleolus to extensor hallucis longus tendon
• Deep peroneal – needl;e 1cm above medial malleolus aiming to inject under extensor hallucis longus
• Saphenous – subcut injection between medial malleolus + anterior tibial tendon

Recent Questions – Chairman’s report
March ‘17•Question 2: Wrong side block and never events Pass rate 39.0% This question related to an important safety initiative. Candidates did not have adequate knowledge of the factors contributing to the performance of a wrong side block such as distraction, the patient being lateral or prone or site mark being covered by blankets.

March 2017• Question 12: Early management of hip fractures and use of fascia iliaca
block Pass rate 22.2% It is disappointing that this question concerning a very commonly seen clinical
scenario and accompanying anaesthetic technique, was answered so poorly. In part a many candidates failed to mention assessment of pain as part of preoperative optimization. There was general lack of knowledge of anatomy in part b. In part c some candidates failed to read the question correctly and described a technique using a nerve stimulator rather than ultrasound, or described a femoral nerve block rather than a fascia iliaca block. Some candidates still wrote about assistance and emergency equipment despite being told in the question that this was unnecessary. Many of the answers were somewhat brief but it is unclear whether this reflects a lack of knowledge or a lack of time.
Fascia Iliaca Block
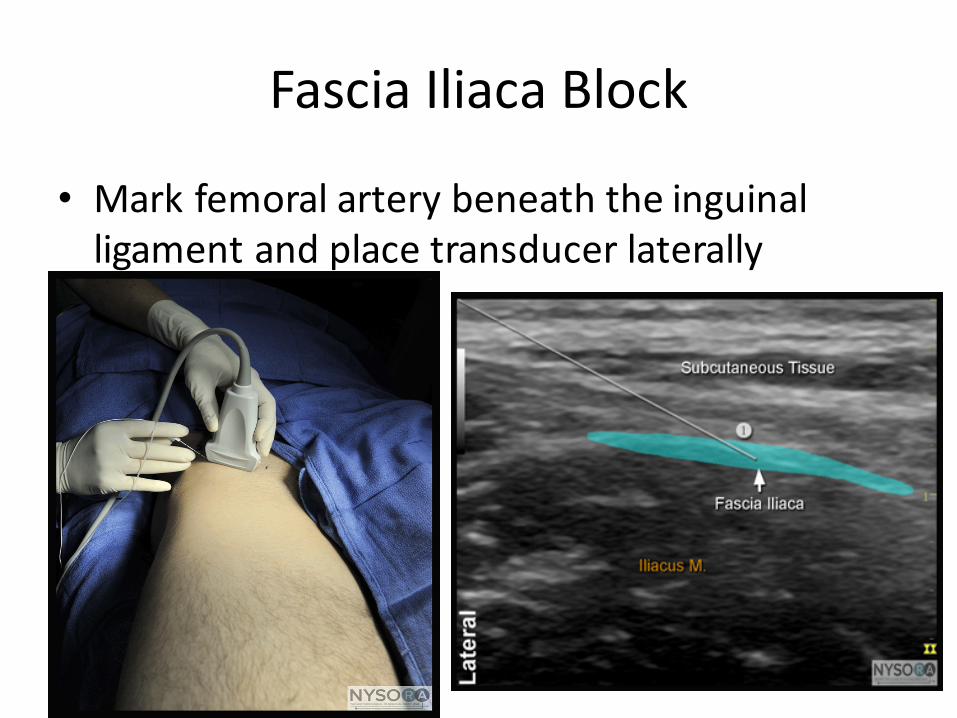
• Mark femoral artery beneath the inguinal ligament and place transducer laterally

• The femoral and femoral lateral cutaneous lie underneath the fascia iliaca
• Get ‘double pop’ as the needle passess through the fascia lata and the fascia iliaca
• Large volume of weak LA used (20-‐40mls)

September 2017
• 63 year old with COPD presents with 9th/10th/11th rib fractures. Inadequate analgesia with paracetamol and codeine. Give other options…
• Pass rate 74.8%. Chairman happy with candidates knowledge

March 2017
• Wrong side peripheral nerve blocks. Implications for patients.
• Summarise ‘stop before you block’ recommendations and factors leading to wrong side blocks
• Define never events

September 2016
• Question 9: Orthopaedics -‐ enhanced recovery in orthopaedic surgery
• Pass rate 59.4% • This was predicted to be an easy question and whilst most candidates answered it well, some did not appear to know the reasons for having an enhanced recovery program nor what the elements of it would be. This is surprising given that most hospitals now run such programs for their patients in various surgical areas.

March 2015
• Question 4 (Pink Book) • A 56-‐year-‐old man is listed for carotid endarterectomy 10 days after
suffering a cerebrovascular accident. • a) What are the advantages (4 marks) and disadvantages (4 marks) of
performing the procedure under regional anaesthesia? • b) What local or regional anaesthetic techniques may be used? (3 marks) • c) How can his risk of perioperative cerebrovascular accident be
minimised? (6 marks) • d) Following this procedure what other specific postoperative
complications may occur? (3 marks)