Oral leiomyosarcomas: report of two cases with immunohistochemical profile
6
Oral leiomyosarcomas: report of two cases with immunohistochemical profile Camila Oliveira Rodini, DDS, MSc, a Flávia Sirotheau Corrêa Pontes, DDS, MSc, b Hélder Antônio Rebelo Pontes, DDS, MSc, b Paulo Sérgio da Silva Santos, DDS, MSc, a Marina Gallottini Magalhães, DDS, PhD, a and Décio Santos Pinto, Jr., DDS, PhD, a São Paulo and Pará, Brazil UNIVERSITY OF SÃO PAULO AND FEDERAL UNIVERSITY OF PARÁ Leiomyosarcoma of the oral cavity is a very rare tumor associated with aggressive clinical behavior and low survival. In this paper, we report 2 cases of leiomyosarcoma, affecting the gingival mucosa of a 54-year-old female and the maxillary bone of a 63-year-old male. Histologically, the tumors were composed of variably oriented fascicles of spindle-shaped cells with cigar-shaped nuclei and eosinophilic cytoplasm. The lesions were treated by surgical resection. Immunoreactivity to anti-vimentin, anti–smooth muscle actin, anti-desmin, anti-laminin, and anti–muscle- specific actin antibodies were found; conversely, the tumor cells were negative for anti-S100 and AE1/AE3 proteins. This report emphasizes the role of immunohistochemical study for correct diagnosis of leiomyosarcoma. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:e50-e55) Leiomyosarcoma (LMS) is a relatively uncommon ma- lignant mesenchymal neoplasm that exhibits smooth muscle differentiation. 1 Smooth muscle tumors are most commonly found in the soft tissues or in a visceral location, including the gastrointestinal, urinary, and female genital tracts. Leiomyosarcomas occurring in the head and neck region, including the oral cavity, are exceptionally rare. 2 Leiomyosarcomas usually show distinctive morpho- logic and architectural features, being composed of spindle-shaped cells with elongated nuclei and eosino- philic cytoplasm. The presence of frequent and atypical mitotic figures and necrotic foci indicates aggressive behavior. The prognosis of LMS is usually poor, owing to high recurrence and metastatic rates. 3,4 The purpose of the present report is to describe 2 cases of LMS in the oral region and their immunohis- tochemical features, which were useful for final diag- nosis. CASE REPORT 1 The patient was a 54-year-old white woman who presented with a 2-month history of a painful swelling of the gingiva distal to the mandibular right second molar. There was no regional lymphadenopathy, and general physical examination was unremarkable. Clinically, the neoplasm presented as a painful pericoronal gingival swelling that mimicked an acute periodontal infec- tion (Fig. 1, A). On panoramic radiographic examination, the affected alveolar bone demonstrated an ill-defined area of resorption (Fig. 1, B). The lesion was managed accordingly, with curettage, debridement, and antibiotics prescription. When the lesion failed to respond to this treatment approach, excision was performed under local anesthesia. Microscopic examination showed a neoplasm composed of interlacing fascicles of spindle-shaped tumor cells mostly exhibiting blunt-ended (cigar-shaped) oval to elongated shaped centrally located nuclei and abundant eosinophilic cytoplasm. Scat- tered mitoses were observed, but cellular pleomorphism was not a dominant feature (Fig. 2, A-D). Consecutive sections were used for the histochemical and immunohistochemical studies, which were performed by Masson’s trichrome and avidin-biotin/peroxidase techniques, respectively. Masson’s trichrome staining demonstrated red longitudinally oriented parallel fibrils within the cytoplasm (Fig. 2, E). Immunohistochemical reactions were also performed for anti-vimentin (1:200; Dako, Glostrup, Denmark), anti-desmin (1:100; Dako), anti–smooth muscle actin (1:50; Dako; Fig. 2, G), anti-laminin (1:3000; Dako; Fig. 2, H), and anti-S100 (1:400; Dako) proteins. The cytoplasm of the tumor cells was positive for all of these intermediate filaments except for the anti-S100 protein. These findings were consistent with the diagnosis of low-grade LMS. The pattern of bone loss was interpreted to be consistent with direct extension of the low- grade malignant process. The tumor was successfully removed en bloc under general anesthesia. Surgical margins were free of tumor. No signs of local recurrence or distant metastasis were noted 14 months after the definitive surgical procedure. a Department of Stomatology (Oral Pathology), Dental School, Uni- versity of São Paulo. b Department of Pathology, Dental School, Federal University of Pará; and Barros Barreto University Hospital. Received for publication Feb 9, 2007; returned for revision May 4, 2007; accepted for publication May 10, 2007. 1079-2104/$ - see front matter © 2007 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2007.05.005 e50
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Oral leiomyosarcomas: report of two cases with immunohistochemical profile

Oral leiomyosarcomas: report of two cases withimmunohistochemical profileCamila Oliveira Rodini, DDS, MSc,a Flávia Sirotheau Corrêa Pontes, DDS, MSc,b
Hélder Antônio Rebelo Pontes, DDS, MSc,b Paulo Sérgio da Silva Santos, DDS, MSc,a
Marina Gallottini Magalhães, DDS, PhD,a
and Décio Santos Pinto, Jr., DDS, PhD,a São Paulo and Pará, BrazilUNIVERSITY OF SÃO PAULO AND FEDERAL UNIVERSITY OF PARÁ
Leiomyosarcoma of the oral cavity is a very rare tumor associated with aggressive clinical behavior and lowsurvival. In this paper, we report 2 cases of leiomyosarcoma, affecting the gingival mucosa of a 54-year-old femaleand the maxillary bone of a 63-year-old male. Histologically, the tumors were composed of variably oriented fasciclesof spindle-shaped cells with cigar-shaped nuclei and eosinophilic cytoplasm. The lesions were treated by surgicalresection. Immunoreactivity to anti-vimentin, anti–smooth muscle actin, anti-desmin, anti-laminin, and anti–muscle-specific actin antibodies were found; conversely, the tumor cells were negative for anti-S100 and AE1/AE3 proteins.This report emphasizes the role of immunohistochemical study for correct diagnosis of leiomyosarcoma. (Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 2007;104:e50-e55)Leiomyosarcoma (LMS) is a relatively uncommon ma-lignant mesenchymal neoplasm that exhibits smoothmuscle differentiation.1 Smooth muscle tumors aremost commonly found in the soft tissues or in a viscerallocation, including the gastrointestinal, urinary, andfemale genital tracts. Leiomyosarcomas occurring inthe head and neck region, including the oral cavity, areexceptionally rare.2
Leiomyosarcomas usually show distinctive morpho-logic and architectural features, being composed ofspindle-shaped cells with elongated nuclei and eosino-philic cytoplasm. The presence of frequent and atypicalmitotic figures and necrotic foci indicates aggressivebehavior. The prognosis of LMS is usually poor, owingto high recurrence and metastatic rates.3,4
The purpose of the present report is to describe 2cases of LMS in the oral region and their immunohis-tochemical features, which were useful for final diag-nosis.
CASE REPORT 1The patient was a 54-year-old white woman who presented
with a 2-month history of a painful swelling of the gingivadistal to the mandibular right second molar. There was no
aDepartment of Stomatology (Oral Pathology), Dental School, Uni-versity of São Paulo.bDepartment of Pathology, Dental School, Federal University ofPará; and Barros Barreto University Hospital.Received for publication Feb 9, 2007; returned for revision May 4,2007; accepted for publication May 10, 2007.1079-2104/$ - see front matter© 2007 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2007.05.005e50
regional lymphadenopathy, and general physical examinationwas unremarkable.
Clinically, the neoplasm presented as a painful pericoronalgingival swelling that mimicked an acute periodontal infec-tion (Fig. 1, A). On panoramic radiographic examination, theaffected alveolar bone demonstrated an ill-defined area ofresorption (Fig. 1, B). The lesion was managed accordingly,with curettage, debridement, and antibiotics prescription.When the lesion failed to respond to this treatment approach,excision was performed under local anesthesia. Microscopicexamination showed a neoplasm composed of interlacingfascicles of spindle-shaped tumor cells mostly exhibitingblunt-ended (cigar-shaped) oval to elongated shaped centrallylocated nuclei and abundant eosinophilic cytoplasm. Scat-tered mitoses were observed, but cellular pleomorphism wasnot a dominant feature (Fig. 2, A-D). Consecutive sectionswere used for the histochemical and immunohistochemicalstudies, which were performed by Masson’s trichrome andavidin-biotin/peroxidase techniques, respectively. Masson’strichrome staining demonstrated red longitudinally orientedparallel fibrils within the cytoplasm (Fig. 2, E).
Immunohistochemical reactions were also performed foranti-vimentin (1:200; Dako, Glostrup, Denmark), anti-desmin(1:100; Dako), anti–smooth muscle actin (1:50; Dako; Fig. 2,G), anti-laminin (1:3000; Dako; Fig. 2, H), and anti-S100(1:400; Dako) proteins. The cytoplasm of the tumor cells waspositive for all of these intermediate filaments except for theanti-S100 protein. These findings were consistent with thediagnosis of low-grade LMS. The pattern of bone loss wasinterpreted to be consistent with direct extension of the low-grade malignant process.
The tumor was successfully removed en bloc under generalanesthesia. Surgical margins were free of tumor. No signs oflocal recurrence or distant metastasis were noted 14 months
after the definitive surgical procedure.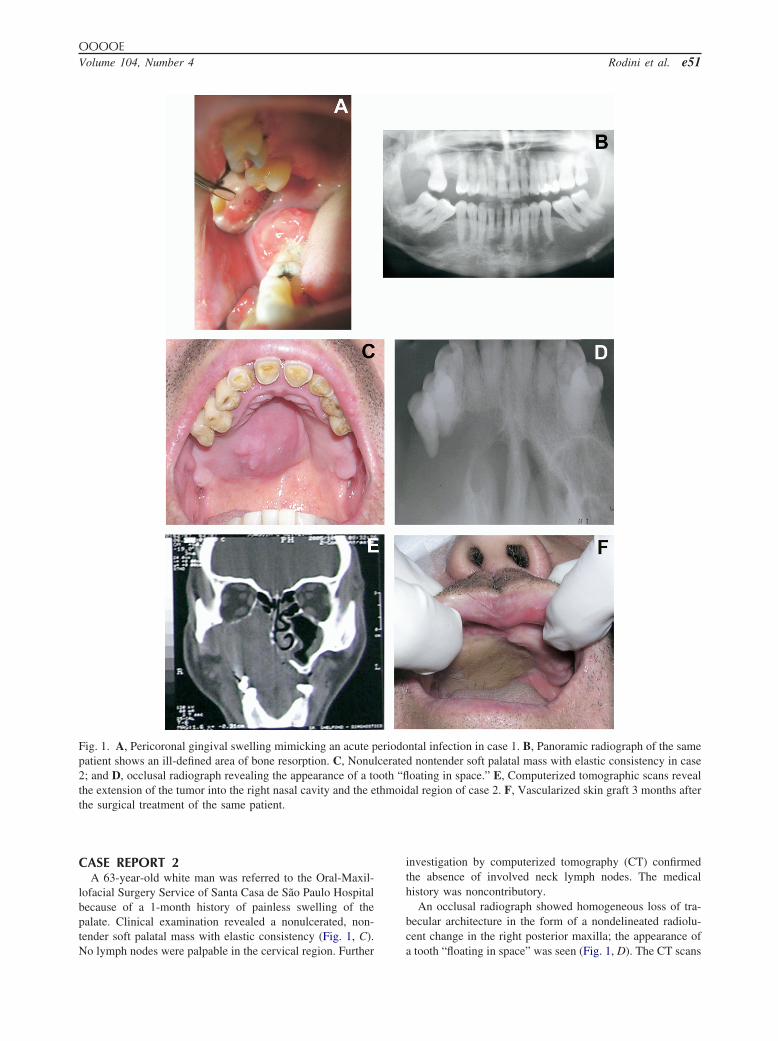
OOOOEVolume 104, Number 4 Rodini et al. e51
CASE REPORT 2A 63-year-old white man was referred to the Oral-Maxil-
lofacial Surgery Service of Santa Casa de São Paulo Hospitalbecause of a 1-month history of painless swelling of thepalate. Clinical examination revealed a nonulcerated, non-tender soft palatal mass with elastic consistency (Fig. 1, C).
Fig. 1. A, Pericoronal gingival swelling mimicking an acute ppatient shows an ill-defined area of bone resorption. C, Nonu2; and D, occlusal radiograph revealing the appearance of a tothe extension of the tumor into the right nasal cavity and the ethe surgical treatment of the same patient.
No lymph nodes were palpable in the cervical region. Further
investigation by computerized tomography (CT) confirmedthe absence of involved neck lymph nodes. The medicalhistory was noncontributory.
An occlusal radiograph showed homogeneous loss of tra-becular architecture in the form of a nondelineated radiolu-cent change in the right posterior maxilla; the appearance of
ntal infection in case 1. B, Panoramic radiograph of the samed nontender soft palatal mass with elastic consistency in caseoating in space.” E, Computerized tomographic scans revealal region of case 2. F, Vascularized skin graft 3 months after
eriodolcerateoth “flthmoid
a tooth “floating in space” was seen (Fig. 1, D). The CT scans

OOOOEe52 Rodini et al. October 2007
of the area revealed a tumor extending into the right nasalcavity as well as into the ethmoidal region (Figs. 1, E).
An incisional biopsy of the intraoral mass was performedunder local anesthesia. Histopathologic examination of hema-toxylin and eosin–stained sections of the biopsy sampleshowed an infiltrating cellular neoplasm composed of rela-tively uniform interlacing fascicles of spindle-shaped lesionalcells. These cells exhibited eosinophilic condensation of thecytoplasm, rare atypical mitotic figures, and several areas ofnecrosis. The preliminary diagnosis of a spindle cell malignancywas made. A panel of antibodies was applied to additional tissue
Fig. 2. Microscopic examination showing interlacing fasciclecentrally located nuclei and abundant eosinophilic cytoplaneoplasm. E, Masson’s trichrome staining demonstrating red limmunopositivity against HHF35 (F), smooth muscle actin (�400 (B, E, F, G, and H), and �1000 (C and D).
sections using routine immunohistochemical techniques; these
included antibodies directed against muscle-specific actin (cloneHHF35, 1:100; Novocastra; Fig. 2, F), smooth muscle actin(1:50; Dako), vimentin (1:200; Dako), desmin (1:100; Dako),S100 protein (1:400; Dako), pancytokeratin (AE1/AE3, 1:50;Dako), and epithelial membrane antigen (EMA, 1:75; Dako).The immunohistochemical studies indicated that the tumor cellswere reactive to antibodies directed against desmin, vimentin,muscle-specific actin, and smooth muscle actin, but nonreactiveto anti-S100 protein, pancytokeratin, and EMA. Based on im-munohistochemical and histopathologic findings, a diagnosis oflow-grade LMS was made. Subsequent imaging studies of the
indle-shaped cells (A and B) with blunt-ended (cigar-shaped)). D, Atypical mitoses observed scattered throughout thedinally oriented parallel fibrils within the cytoplasm. Note thed laminin antigens (H). Original magnifications: �250 (A),
s of spsm (CongituG), an
lungs and brain showed no evidence of metastatic disease.

; �, ne
OOOOEVolume 104, Number 4 Rodini et al. e53
Surgical treatment consisted of a hemimaxillectomy pro-cedure performed by the Head and Neck Surgery team ofSanta Casa de São Paulo Hospital under general anesthesia.The maxilla was resected from the right canine to the entiremaxillary tuberosity, and an immediate vascularized skingraft was performed (Fig. 1, F). The postoperative course wasuneventful. Follow-up 1 year after treatment did not revealany indication of tumor recurrence.
DISCUSSIONIntraoral LMS is an extremely uncommon neoplasm,
with fewer than 80 cases reported in the English-lan-guage literature to date, probably because of the paucityof smooth muscle tissue. Leiomyosarcoma occurring inareas with scanty smooth muscle such as the oral andmaxillofacial region have been considered to arise fromthe tunica media of the blood vessels or from pluripo-tential undifferentiated mesenchymal cells.4 Althoughunusual, the possibility of a LMS metastasizing to theoral cavity from another primary site should always beruled out before a diagnosis of primary oral LMS isgiven.3,5 Oral LMS tends to metastasize to the cervicalnodes and to the lung and liver, unlike LMS in softtissue, whose nodal involvement is extremely rare.5-7
Oral LMS does not display any significant genderpredilection and has been reported to occur over a wideage range, with most patients in the third and sixth orseventh decade of life. Jawbones appear to be thepreferred site for oral LMS; approximately 70% ofthese tumors arise in the maxilla and mandible.1,8 Othercases with intraoral locations include the tongue, softand hard palate, floor of the mouth, buccal mucosa,gingiva, and upper lip.3
The present case 1 showed mandible gingival in-volvement, and case 2 developed in the maxilla. Thedistinction between central and peripheral LMS in the
Table I. Immunohistochemical profile useful in the di
85 Lesion SMA HHF35 Vimentin AE1/AE3 EM
Leiomyosarcoma �d �d �d �af �Rhabdomyosarcoma � �d � � �Spindle cell
carcinoma�af � � � �
Solitary fibroustumor
� �f � � �
Angiosarcoma � � � � �Melanoma � � � � �Neural tumor � � � � �Myofibroblastic
tumor�f � � � �
HHF35, muscle-specific actin; AE1/AE3, pancytokeratin; �, positive
oral cavity depends on the radiographic and clinical
features of the tumor.7 Both of the present cases re-vealed no involved neck lymph nodes as well as anabsence of metastasis. Accordingly, Vilos et al.,1 in areview of 50 cases, showed that 91% of the patients didnot show evidence of neck involvement after clinicalexamination or imaging studies on presentation, and95.6% presented with no detectable distant metastasis.
Radical surgery is the treatment of choice. Radio-therapy and chemotherapy had little effect when ap-plied in recurrent tumors. The unfavorable prognosis ofmaxillary LMS is probably related to more advanceddisease at the time of diagnosis and greater difficulty inresecting maxillary lesions.3,6,8 In the LMS of the headand neck, 5-year survival accounts for 62% of cases.2
The patients reported here showed clinical signs sug-gestive of malignancy, such as radiographically detect-able bone destruction. Radical surgery was promptlyplanned and performed. This may influence the rela-tively favorable prognosis. Because the course is un-predictable, long-term follow-up of patients with thislesion is mandatory.9
The definitive histologic diagnosis of oral LMS isdifficult, because of its similarity with other spindle celllesions, poor differentiation of neoplastic cells in somecases, and the rarity of these lesions in the oral andmaxillofacial locations.3,9 Differential diagnosis ofspindle cell proliferations should include LMS, rhab-domyosarcoma, spindle cell carcinoma, fibrosarcoma,malignant schwannoma, myofibrosarcoma, solitary fi-brous tumor, fibroblastic osteosarcoma, angiosarcoma,malignant fibrous histiocytoma, and melanoma.1,4,5 Adefinitive diagnosis of LMS is generally established onthe basis of light microscopy, but histochemical andimmunohistochemical findings (Table I) as well aselectron microscopy are widely accepted as useful tools
tial diagnosis of leiomyosarcomaAntibodies
smin CD146Myogenin and
myoglobin CD34 CD31 HMB45 S100
ad � � � � � �d NS � � � � �
� � � � � � �
f NS � � � � �
� � � � � � �� � � � � � �� a � � � � �� NS � � � � �
gative; d, diffuse; f, focal; a, variable; NS, not surveyed in literature.
fferen
A De
�
�
for confirming the diagnosis.3,8,9

OOOOEe54 Rodini et al. October 2007
At the light microscopy level, the presence of 2 ormore mitotic figures per 10 high-power fields is cur-rently considered the most reliable criterion of smoothmuscle cell tumors. Intracytoplasmatic glycogen can bedemonstrated with the periodic acid–Schiff stainingwith and without diastase digestion, supporting themyogenous differentiation of the tumor. The Gomorisilver impregnation technique reveals figures of finereticulin fibers, which are considered characteristic ofLMS,7 and Masson’s trichrome stain demonstrates redlongitudinally oriented parallel fibrils within the cyto-plasm, helping to distinguish this neoplasm.1
Regarding the use of immunohistochemistry as anancillary technique to differentiate spindle cell neo-plasms, the LMS spindle cells that comprise the neo-plastic proliferation react positively with antibodiestargeted against smooth muscle antigenic epitopes ofmesenchymal origin, such as smooth muscle actin,muscle-specific actin, vimentin, and laminin1,5,9-12;however, rhabdomyosarcoma and, inconstantly, spindlecell carcinoma may display similar immunoprofile.8
Pancytokeratin and EMA negativity rules out the diag-nosis of spindle cell carcinoma. On the other hand,spindle cell carcinomas may show focal actin positivitybut no immunostaining for desmin, whereas LMS maybe positive for pancytokeratin, in either a diffuse orperinuclear dot-like pattern; however, this staining istypically focal and strong diffuse staining for desminand/or actin is invariably present in such cases.5,13
Accurate search for typical rhabdomyoblasts or forareas with small/round cell differentiation, suggestiveof embryonal rhabdomyosarcoma, is mandatory to dif-ferential diagnosis from LMS. However, the search forspecific morphologic indicators of skeletal muscle dif-ferentiation, e.g., cross-striations, may be frustrating.Besides, it is not easy to distinguish LMS from rhab-domyosarcoma by immunoreaction. Both neoplasmsshare almost identical immunoprofile, desmin positivitybeing more consistently detectable in rhabdomyosarco-ma.8 In case of primary oral LMS, desmin immuno-staining may be either positive or negative.1,8 Leiomy-osarcoma and rhabdomyosarcoma can be differentiatedby smooth muscle actin12 and CD14614 immunoexpres-sion (both positive in LMS), nuclear myogenin (skele-tal muscle myogenin), myoglobin, and sarcomeric actin(positive in rhabdomyosarcoma).15
Immunohistochemically, solitary fibrous tumors(SFT) consistently express immunoreactivity with vi-mentin, CD34, and, focally, muscle-specific actin anddesmin. This immunophenotypic feature of SFT reli-ably allows its differentiation from LMS.8 The immu-nohistochemical expressions of CD31 and CD34 anti-gens in angiosarcomas, and of HMB45 and S100
proteins in melanomas allow adequate characterizationof these neoplasms.5 Malignant peripheral nerve sheathtumor exhibits S100 protein and vimentin positivity.8
Finally, immunoreactivity for desmin and muscle-specific actin may not necessarily be adequate to indi-cate the diagnosis of LMS, because fibrosarcoma cellsoften undergo myogenic or myofibroblastic differenti-ation.9 Within this context, Sedghizadeh et al.2 reportedthat most actin antibodies commercially available arepan-actin moieties that cluster around 45 kD, so theyare not muscle epitope specific enough to demonstrate“pure” myogenous differentiation. Therefore, these an-tibodies can react with many other cell types besidesmuscle, as seen by actin positivity in reactive lesionsand in non–smooth muscle tumors such as synovialsarcoma, malignant fibrous histiocytoma, fibromatosis,and nodular fascitis. The myofibroblastic tumor is typ-ically at least focally reactive to smooth muscle–spe-cific actin and generally negative for desmin and S100protein.5 A critical discriminatory feature in the myo-fibroblastic tumor of infancy is the lack of cellularpleomorphism and atypia that are seen in LMS; anotherfeature is the presence of few, if any, mitotic figures,which are not atypical mitoses. This is in contrast to thehigh mitotic rate seen in LMS.7
Nikitakis et al.3 evaluated the diagnostic and prog-nostic value of the expression of p53, bcl-2, MDM2,PCNA, and CDK4 in 2 cases of primary LMS of thejawbones. The results revealed p53 protein overexpres-sion, MDM2, PCNA, and bcl-2-positive immunophe-notypes, and CDK4 immunopositivity and overexpres-sion in both cases and MDM2 overexpression in thesecond case. The clinical relevance of this findingsincludes the possible use of p53, CDK4, and PCNApositivity and overexpression in distinguishing betweenbenign and malignant smooth muscle tumors and intheir association with aggressive clinical behavior andnegative outcome of the tumor. Both cases described inthat study were operated and successful, and locore-gional control of the disease was achieved. The secondpatient, however, had an unfavorable long-term outcomeowing to distant metastatic spread. Despite the potentialprognostic and diagnostic usefulness of MDM2 andbcl-2 remains controversial, the authors suggested thatMDM2 amplification can happen in a subset of oralLMS and that the adverse clinical outcome of thesecond case might be assigned to aberrations in theexpression of the aforementioned proteins, especiallyMDM2 protein.
In summary, predicting the clinical behavior of LMSin any location is notoriously difficult. Mitoses andnecrosis appear to be the best histologic predictors ofmalignant behavior.7 Long-term follow-up after opera-
tion is needed.
OOOOEVolume 104, Number 4 Rodini et al. e55
REFERENCES1. Vilos GA, Rapidis AD, Lagogiannis G, Apostolidis C. Leiomy-
osarcoma of the oral tissues: clinicopathologic analysis of 50cases. J Oral Maxillofac Surg 2005;63:1461-77.
2. Sedghizadeh PP, Angiero F, Allen CM, Kalmar JR, Rawal Y,Albright EA. Post-irradiation leiomyosarcoma of the maxilla:report of a case in a patient with prior radiation treatment forretinoblastoma. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2004;97:726-31.
3. Nikitakis NG, Lopes MA, Bailey JS, Blanchaert RM Jr, Ord RA,Sauk JJ. Oral leiomyosarcoma: review of the literature and reportof two cases with assessment of the prognostic and diagnosticsignificance of immunohistochemical and molecular markers.Oral Oncol 2002;38:201-8.
4. Sumida T, Hamakawa H, Otsuka K, Tanioka H. Leiomyosar-coma o the maxillary sinus with cervical lymph node metastasis.J Oral Maxillofac Surg 2001;59:568-71.
5. Dry SM, Lorgensen JL, Fletcher CDM. Leiomyosarcomas of theoral cavity: an unusual topographic subset easily mistaken fornonmesenchymal tumours. Histopathology 2000;36:210-20.
6. Schenber ME, Slootweg PJ, Koole R. Leiomyosarcoma of theoral cavity. Report of four case and review of the literature. JCraniomaxillofac Surg 1993;21:342-7.
7. Carter LC, Aguirre A, Boyd B, DeLacure M. Primary leiomyo-sarcoma of the mandible in a 7-year-old girl. Report of a case andreview of the literature. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1999;87:477-84.
8. Muzio LL, Favia G, Mignogna MD, Piattelli A, Maiorano E.Primary intraoral leiomyosarcoma of the tongue: an immunohis-tochemical study and review of the literature. Oral Oncol
2000;36:519-24.9. Izumi K, Maeda T, Cheng J, Saku T. Primary leiomyosarcoma ofthe maxilla with regional lymph node metastasis: report of a caseand review of the literature. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1995;80:310-9.
10. Yang SW, Chen TM, Tsai CY, Lin CY. A peculiar site ofleiomyosarcoma: the tongue tip—report of a case. Int J OralMaxillofac Surg 2006;35:469-71.
11. Goldschmidt PR, Goldschmidt JD, Leblich SE, Elsenberg E.Leiomyosarcoma present as a mandibular gingival swelling: casereport. J Periodontol 1999;70:84-9.
12. Jundt G, Moll C, Nidecker A, Schilt R, Remagen W. Primaryleiomyosarcoma of bone: report of eight cases. Hum Pathol1994;25:1205-12.
13. Miettinen M. Immunoreactivity for cytokeratin and epithelialmembrane antigen in leiomyosarcoma. Arch Pathol Lab Med1988;112:637-40.
14. Shih IM, Nesbit M, Herlyn M, Kurman RJ. A new Mel-CAM(CD146)-specific monoclonal antibody, MN-4, on paraffin-em-bedded tissue. Mod Pathol 1998;11:1098-6.
15. Hasegawa T, Matsuno Y, Nike T, Hirohashi S, Shimoda T,Takayama J, et al. Second primary rhabdomyosarcomas in pa-tients with bilateral retinoblastoma: a clinicopathologic and im-munohistochemical study. Am J Surg Pathol 1998;22:1351-60.
Reprint requests:
Camila Oliveira RodiniRua Professor Luiz Braga, n° 3-17517016-050 BauruSão PauloBrasil
[email protected]