
Mitochondria and cardioprotection
12
Mitochondria and cardioprotection Fabio Di Lisa Marcella Canton Roberta Menabo ` Nina Kaludercic Paolo Bernardi Published online: 22 May 2007 Ó Springer Science+Business Media, LLC 2007 Abstract Major factors linking mitochondrial dysfunc- tion with myocardial injury are analyzed along with pro- tective mechanisms elicited by endogenous processes and pharmacological treatments. In particular, a reduced rate of ATP hydrolysis and a slight increase in ROS formation appear to represent the prevailing components of self-de- fense mechanisms, especially in the case of ischemic pre- conditioning. These protective processes are activated by signaling pathways, which converge on mitochondria activating the mitochondrial K ATP channels and/or inhib- iting the mitochondrial permeability transition pore. These pathways can also be stimulated by pharmacological treatments. Another major goal for cardioprotection is decreasing the burst in mitochondrial ROS formation that characterizes post-ischemic reperfusion. Finally, mito- chondrial targets for therapeutic intervention may include the switch of substrate being utilized, because inhibition of fatty acid oxidation is associated with cardioprotective effects. Keywords Mitochondria Á Metabolism Á Ischemia Á Permeability Transition Á Reactive oxygen species Abbreviations AIF Apoptosis inducing factor BH BCL-2 homology CPT Carnitine palmitoyl transferase CsA Cyclosporin A Cx43 Connexin 43 CyP Cyclophilin Dp Protonmotive force Dw m Mitochondrial membrane potential ER Endoplasmic reticulum FAO Fatty acid oxidation IMM Inner mitochondrial membrane IMS Intermembrane space IPC Ischemic preconditioning MAO Monoamine oxidase mitoK ATP Mitochondrial K ATP channel Pi Inorganic phosphate OMM Outer mitochondrial membrane PDH Pyruvate dehydrogenase PTP Permeability transition pore ROS Reactive oxygen species SOD Superoxide dismutase PLA 2 Phospholipase A 2 TPP Triphenylphosphonium Introduction The heart is especially vulnerable to mitochondrial derangements owing to its strict dependence on aerobic metabolism [1–3]. A wide variety of cardiomyopathies Fabio Di Lisa and Paolo Bernardi are recipients of grants from CNR and MIUR. F. D. Lisa (&) Á M. Canton Á N. Kaludercic Dipartimento di Chimica Biologica, Universita ` di Padova, Viale G. Colombo 3, Padova 35121, Italy e-mail: [email protected] P. Bernardi Dipartimento di Scienze Biomediche Sperimentali, Universita ` di Padova, Viale G. Colombo 3, Padova 35121, Italy F. D. Lisa Á R. Menabo ` Á P. Bernardi Istituto di Neuroscienze del CNR, Universita ` di Padova, Viale G. Colombo 3, Padova 35121, Italy 123 Heart Fail Rev (2007) 12:249–260 DOI 10.1007/s10741-007-9028-z
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Mitochondria and cardioprotection

Mitochondria and cardioprotection
Fabio Di Lisa Æ Marcella Canton Æ Roberta Menabo ÆNina Kaludercic Æ Paolo Bernardi
Published online: 22 May 2007
� Springer Science+Business Media, LLC 2007
Abstract Major factors linking mitochondrial dysfunc-
tion with myocardial injury are analyzed along with pro-
tective mechanisms elicited by endogenous processes and
pharmacological treatments. In particular, a reduced rate of
ATP hydrolysis and a slight increase in ROS formation
appear to represent the prevailing components of self-de-
fense mechanisms, especially in the case of ischemic pre-
conditioning. These protective processes are activated by
signaling pathways, which converge on mitochondria
activating the mitochondrial KATP channels and/or inhib-
iting the mitochondrial permeability transition pore. These
pathways can also be stimulated by pharmacological
treatments. Another major goal for cardioprotection is
decreasing the burst in mitochondrial ROS formation that
characterizes post-ischemic reperfusion. Finally, mito-
chondrial targets for therapeutic intervention may include
the switch of substrate being utilized, because inhibition of
fatty acid oxidation is associated with cardioprotective
effects.
Keywords Mitochondria � Metabolism � Ischemia �Permeability Transition � Reactive oxygen species
Abbreviations
AIF Apoptosis inducing factor
BH BCL-2 homology
CPT Carnitine palmitoyl transferase
CsA Cyclosporin A
Cx43 Connexin 43
CyP Cyclophilin
Dp Protonmotive force
Dwm Mitochondrial membrane potential
ER Endoplasmic reticulum
FAO Fatty acid oxidation
IMM Inner mitochondrial membrane
IMS Intermembrane space
IPC Ischemic preconditioning
MAO Monoamine oxidase
mitoKATP Mitochondrial KATP channel
Pi Inorganic phosphate
OMM Outer mitochondrial membrane
PDH Pyruvate dehydrogenase
PTP Permeability transition pore
ROS Reactive oxygen species
SOD Superoxide dismutase
PLA2 Phospholipase A2
TPP Triphenylphosphonium
Introduction
The heart is especially vulnerable to mitochondrial
derangements owing to its strict dependence on aerobic
metabolism [1–3]. A wide variety of cardiomyopathies
Fabio Di Lisa and Paolo Bernardi are recipients of grants from CNR
and MIUR.
F. D. Lisa (&) � M. Canton � N. Kaludercic
Dipartimento di Chimica Biologica, Universita di Padova, Viale
G. Colombo 3, Padova 35121, Italy
e-mail: [email protected]
P. Bernardi
Dipartimento di Scienze Biomediche Sperimentali, Universita di
Padova, Viale G. Colombo 3, Padova 35121, Italy
F. D. Lisa � R. Menabo � P. Bernardi
Istituto di Neuroscienze del CNR, Universita di Padova, Viale G.
Colombo 3, Padova 35121, Italy
123
Heart Fail Rev (2007) 12:249–260
DOI 10.1007/s10741-007-9028-z
have been reported as direct consequences of inborn errors
of mitochondrial metabolism [4–6]. In addition, alterations
of mitochondrial bioenergetics are likely to play a crucial
role in myocardial failure [7–9]. However, most of the
current knowledge on mitochondrial contribution to myo-
cardial pathology derives from studies on ischemia/reper-
fusion injury. The present article analyzes the mechanisms
of cardioprotection underlying both self-defense processes
and therapeutic strategies, and tries to sort causes from
consequences of mitochondrial impairment in the ischemic
heart.
Mitochondrial derangements in ischemia and
reperfusion
Oxygen is the main acceptor of electrons harvested from
nutrients, mainly carbohydrates and lipids through the
activity of NAD- and FAD-dependent dehydrogenases. The
reduced forms of these coenzymes are reoxidized at the
level of Complex I and II of the respiratory chain and the
electrons are funneled to complex IV where more than 90%
of the intracellular oxygen is reduced to water. Thus,
oxygen is for the most part utilized in a single reaction and
this explains the profound metabolic changes occurring
when oxygen supply is no longer sufficient for the activity
of cytochrome oxidase. In fact, the very first and immediate
consequence of an insufficient cellular oxygenation is the
inhibition of electron flow along the respiratory chain that
inevitably impairs both energy conservation and oxidative
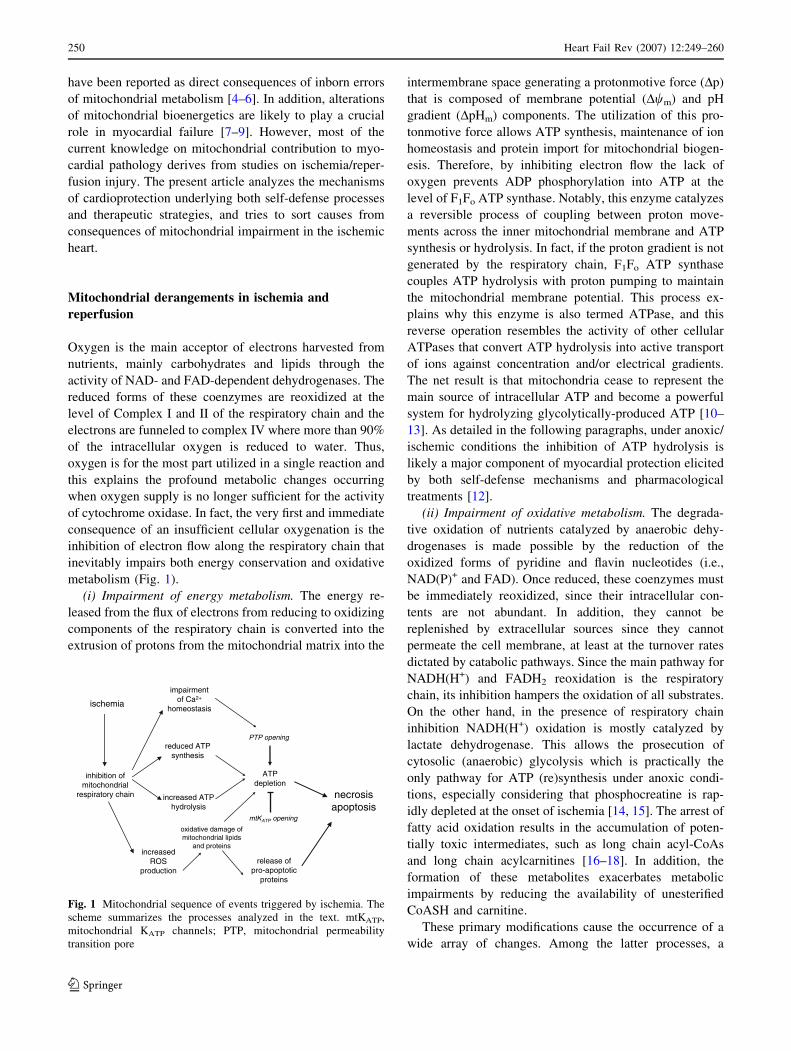
metabolism (Fig. 1).
(i) Impairment of energy metabolism. The energy re-
leased from the flux of electrons from reducing to oxidizing
components of the respiratory chain is converted into the
extrusion of protons from the mitochondrial matrix into the
intermembrane space generating a protonmotive force (Dp)
that is composed of membrane potential (Dwm) and pH
gradient (DpHm) components. The utilization of this pro-
tonmotive force allows ATP synthesis, maintenance of ion
homeostasis and protein import for mitochondrial biogen-
esis. Therefore, by inhibiting electron flow the lack of
oxygen prevents ADP phosphorylation into ATP at the
level of F1Fo ATP synthase. Notably, this enzyme catalyzes
a reversible process of coupling between proton move-
ments across the inner mitochondrial membrane and ATP
synthesis or hydrolysis. In fact, if the proton gradient is not
generated by the respiratory chain, F1Fo ATP synthase
couples ATP hydrolysis with proton pumping to maintain
the mitochondrial membrane potential. This process ex-
plains why this enzyme is also termed ATPase, and this
reverse operation resembles the activity of other cellular
ATPases that convert ATP hydrolysis into active transport
of ions against concentration and/or electrical gradients.
The net result is that mitochondria cease to represent the
main source of intracellular ATP and become a powerful
system for hydrolyzing glycolytically-produced ATP [10–
13]. As detailed in the following paragraphs, under anoxic/
ischemic conditions the inhibition of ATP hydrolysis is
likely a major component of myocardial protection elicited
by both self-defense mechanisms and pharmacological
treatments [12].
(ii) Impairment of oxidative metabolism. The degrada-
tive oxidation of nutrients catalyzed by anaerobic dehy-
drogenases is made possible by the reduction of the
oxidized forms of pyridine and flavin nucleotides (i.e.,
NAD(P)+ and FAD). Once reduced, these coenzymes must
be immediately reoxidized, since their intracellular con-
tents are not abundant. In addition, they cannot be
replenished by extracellular sources since they cannot
permeate the cell membrane, at least at the turnover rates
dictated by catabolic pathways. Since the main pathway for
NADH(H+) and FADH2 reoxidation is the respiratory
chain, its inhibition hampers the oxidation of all substrates.
On the other hand, in the presence of respiratory chain
inhibition NADH(H+) oxidation is mostly catalyzed by
lactate dehydrogenase. This allows the prosecution of
cytosolic (anaerobic) glycolysis which is practically the
only pathway for ATP (re)synthesis under anoxic condi-
tions, especially considering that phosphocreatine is rap-
idly depleted at the onset of ischemia [14, 15]. The arrest of
fatty acid oxidation results in the accumulation of poten-
tially toxic intermediates, such as long chain acyl-CoAs
and long chain acylcarnitines [16–18]. In addition, the
formation of these metabolites exacerbates metabolic
impairments by reducing the availability of unesterified
CoASH and carnitine.
These primary modifications cause the occurrence of a
wide array of changes. Among the latter processes, a
tnemriapmiaC fo +2
sisatsoemoh
desaercniSOR
noitcudorp
PTAnoitelped
fo noitibihnilairdnohcotim
niahc yrotaripser
aimehcsi
PTA decudersisehtnys
PTA desaercnisisylordyh
gninepo PTP
Ktm PTA gninepo
fo egamad evitadixo sdipil lairdnohcotim
snietorp dna
fo esaelercitotpopa-orp
snietorp
sisorcensisotpopa
Fig. 1 Mitochondrial sequence of events triggered by ischemia. The
scheme summarizes the processes analyzed in the text. mtKATP,
mitochondrial KATP channels; PTP, mitochondrial permeability
transition pore
250 Heart Fail Rev (2007) 12:249–260
123

prominent role is attributed to impaired Ca2+ homeostasis
and increased ROS formation.
(iii) [Ca2+] increase. Since both mitochondrial Ca2+
uptake and release depend on Dp [19, 20], respiratory chain
inhibition results in profound alterations of mitochondrial
Ca2+ homeostasis that can trigger and be further exacer-
bated by opening of the mitochondrial permeability tran-
sition pore (PTP), as discussed in the following paragraphs
and in many reviews (see for instance [19, 21–24]). It is
generally accepted that during ischemia and/or reperfusion
mitochondrial [Ca2+] ([Ca2+]m) increases, yet it must be
pointed out that quite different mechanisms underlie
[Ca2+]m rise or overload. In fact, during ischemia Dp is
abolished because of respiratory chain inhibition and
[Ca2+]m may passively follow the occurrence of elevations
of cytosolic Ca2+. On the other hand, upon reperfusion, Dp
is recovered along with the capacity of mitochondria to
take up huge amounts of Ca2+. Therefore, only under the
latter conditions active accumulation of Ca2+ takes place
within the matrix, which is more likely to cause PTP
opening, mitochondrial depolarization, impairment of ATP
synthesis and initiation of massive hydrolysis of ATP. In
any case [Ca2+]m elevation is the consequence of a pre-
ceding rise in cytosolic [Ca2+] ([Ca2+]c). Therefore, the
abrupt release of Ca2+ from an overloaded matrix is not
likely to determine per se intracellular Ca2+ overload. The
lack of adequate pharmacological or genetic tools to inhibit
mitochondrial Ca2+ uptake in situ has so far prevented a
clear assessment of its role in myocardial physiology and
pathology. Relevant questions, such as mitochondrial
involvement in excitation-contraction coupling or the
relationships between mitochondrial Ca2+ uptake and cell
injury, remain indeed unanswered. Nevertheless, strategies
aimed at decreasing cytosolic Ca2+ overload are likely to
prevent or delay alterations in mitochondrial structure and
function.
(iv) Increased ROS formation. Reactive oxygen specie
(ROS) are formed within mitochondria under physiological
and pathological conditions, especially during post-ische-
mic reperfusion [25–27]. The common estimate that 2–4%
of oxygen utilized by the respiratory chain undergoes
univalent reduction becoming superoxide anion (O2–•) is
probably too high, and it has been suggested that a correct
estimate might be one order of lower magnitude [28, 29].
O2–• formed at the level of Complex I and III is rapidly
transformed into hydrogen peroxide (H2O2) by a family of
metalloenzymes, superoxide dismutases (SOD) [30]. The
inhibition of the respiratory chain favors ROS formation
lending support to the concept that respiratory complexes,
especially Complex I, are the main intracellular sites for
ROS formation. However, mitochondrial sites other than
the inner mitochondrial membrane are capable of gener-
ating H2O2 at significant rates. A relevant role in this re-
spect is likely played by monoamine oxidases (MAO).
These outer membrane flavoproteins catalyze electron
transfer from various amine compounds (including cate-
cholamines) to O2, thus producing large amounts of H2O2
[31, 32].
Another example of mitochondrial ROS generation at
sites other than the respiratory chain is provided by
p66Shc. This protein, which localizes in part within mito-
chondria, catalyzes electron transfer from cytochrome c to
oxygen. The consequent ROS formation has been linked to
PTP opening and apoptosis [33]. Indeed, fibroblasts lacking
p66Shc displayed a reduced formation of ROS in response
to oxidative stress-inducing agents. Conversely, p66Shc
overexpression resulted in enhanced stress-induced apop-
tosis [33–35]. Interestingly, life span is extended by ab-
lating p66Shc gene expression [36]. More recent work
suggests that PKC b induced phosphorylation of p66Shc on
Ser36 could cause its translocation to mitochondria [37].
Therefore, the increase in mitochondrial ROS formation
caused by p66Shc appears to amplify PKC b signaling
triggered by an initial oxidative stress.
The above-mentioned alterations trigger and underlie all
the deleterious consequences of ischemia, and their rele-
vance is likely to be crucial for any myocardial disease.
Considering mechanisms involved in cell death, PTP
opening and release of apoptogenic proteins represent the
most relevant processes.
(v) PTP opening. A central role in cell death is attributed
to PTP opening as related to a wide range of pathologies
extending far beyond myocardial injury ([21] and refer-
ences therein). This paragraph briefly summarizes the rel-
evance of PTP in myocardial ischemia. Additional details
have been addressed by numerous reviews [10, 22–24, 38]
The permeability transition describes a sudden increase of
the inner membrane permeability to solutes with molecular
weights up to 1500 Daltons (reviewed in [19, 20, 39, 40])
caused by the opening of a voltage-dependent, high-con-
ductance channel located in the inner mitochondrial
membrane defined as the permeability transition pore
(PTP). PTP opening can be induced by all the factors
analyzed above, i.e., [Ca2+]m increase, Dwm fall and oxi-
dative stress, and represents a major cause of mitochondrial
dysfunction creating conditions hardly compatible with cell
survival. This especially holds true in the case of prolonged
openings [41] that cause collapse of Dwm, depletion of ATP
and NAD+, matrix swelling, rupture of the outer membrane
followed by release of proteins of the intermembrane
space, such as cytochrome c.
The PTP opening is favored by [Ca2+]m elevation,
depolarization, increases in ROS and inorganic phosphate
(Pi). These factors are counteracted by physiological PTP
antagonists, such as elevated values of Dwm and high
concentrations of H+, Mg2+ and adenine nucleotides,
Heart Fail Rev (2007) 12:249–260 251
123

especially ADP [19, 23]. This explains the evidence ob-
tained in many laboratories that PTP opening occurs during
post-ischemic reperfusion. In fact during ischemia, intra-
cellular acidosis along with high levels of Mg2+ and ADP
overrides the PTP promoting conditions established by
Dwm decrease and increases in Ca2+ and Pi levels. Con-
versely, upon reperfusion the recovery of pH together with
a burst in ROS formation in the presence of high-matrix
concentrations of Ca2+ and Pi create the perfect scenario
for PTP opening despite the antagonizing effect of Dwm
recovery (Fig. 2).
In isolated mitochondria PTP opening is usually ob-
tained by additions of Ca2+ exceeding 0.1 mM. Such high
Ca2+ concentrations are hardly achieved in viable cells
suggesting that Ca2+ does not cause PTP opening directly,
and PTP is sensitized to Ca2+ by several processes, such as
formation of ROS or metabolites generated by Ca2+-
dependent enzymes. For instance, a recent report suggests
that PTP onset is due to a deadly mixture of ROS gener-
ation and pH normalization, whereas intracellular Ca2+
overload would be the consequence and not the cause of
bioenergetic failure [42]. On the other hand, the activation
of Ca2+-dependent enzymes could signal the occurrence of
cell damage to mitochondria by converting and amplifying
initial Ca2+-related signals into Ca2+-dependent derange-
ments. Among the possible signaling pathways we have
characterized the activation of cytosolic phospholipase A2
resulting in the formation of arachidonic acid which in-
duces apoptosis by promoting PTP opening [43]. Several
reports indicate the relevance of calpains. The relationship
between these Ca2+ dependent proteinases and cell death
involves multiple processes and cellular sites [44, 45]. The
involvement of mitochondria is suggested by evidence of
intramitochondrial localization especially of the l isoform
[46], and by the reports that calpains may be involved in
PTP opening [47], mitochondrial release of the apoptosis
inducing factor (AIF) [48] and cleavage of Bid, a proa-
poptotic member of the BCL-2 family [49]. Interestingly,
calpain activation within mitochondria appears to be trig-
gered by interaction with its natural activator, acyl CoA
binding protein [46]. Therefore, counteracting [Ca2+]i rise
and/or activation of Ca2+ dependent enzymes should rep-
resent an effective strategy for preventing PTP opening
(Fig. 3).
(vi) Release of proapoptotic proteins. Besides changes
occurring at the level of IMM and matrix space, changes in
the permeability of the outer mitochondrial membrane
(OMM) allow the efflux of proteins of the intermembrane
space (IMS) into the cytosol [50, 51]. Several of these
proteins, such as cytochrome c, AIF, endonuclease G,
SMAC-Diablo are pivotal factors for the executioner phase
of apoptosis [51–53].
The mechanisms linking impairment of mitochondrial
bioenergetics with structural changes causing IMS protein
release are subjects of ongoing studies and debates. Two
major hypotheses have been proposed highlighting pro-
cesses occurring at the IMM or at the OMM, respectively.
As far as IMM is concerned, PTP-induced mitochondrial
swelling could cause OMM rupture allowing the release of
IMS proteins. This sequence of events is easily detectable
in isolated mitochondria, but it might not be a necessary
consequence of PTP opening in situ, especially in the case
of transient openings [54]. Nevertheless, PTP-dependent
swelling of mitochondria has been observed in ischemic
tissues [55, 56]. Notably, matrix swelling is likely to be
required for releasing a large fraction of cytochrome c [57].
In fact, under physiological conditions the majority of
cytochrome c is sequestered within spaces delimited by
mitochondrial cristae, so that in the absence of matrix
swelling OMM permeabilization per se would result in the
release of only a minor fraction (about 15%) of cytochrome
c [54, 58, 59].
Hypotheses supporting a pivotal role of OMM permea-
bilization are centered on a large group of proteins related
to BCL-2 that includes pro and antiapoptotic members.
This family of proteins share up to four regions known as
BCL-2 homology (BH) domains [50, 51]. Antiapoptotic
members, such BCL-2 and BCL-XL contain all four do-
DESOLC NEPO
Hp wolgM hgih +2
SOR wol
ψ∆ m llaf
esaercni HpaC[ +2 esaercni ]
SOR hgihiP hgih
gM[ +2 esaerced ]
DESOLC NEPO
ψ∆ m yrevocer
AIMEHCSI NOISUFREPER
Fig. 2 PTP agonists vs. antagonists in ischemia and reperfusion
ralullecartnIaC[ +2 daolrevo ]
gninepo PTP
ralullecartni thgilSaC[ +2 noitavele ]
gninepo PTP
fo noitavitcAaC +2 semyzne tnedneped-
ytivitisnes desaercnIaC ot PTP fo +2
TCERID TCERIDNI
SOR
Fig. 3 Relationships between intracellular [Ca2+] elevation and PTP
opening
252 Heart Fail Rev (2007) 12:249–260
123

mains. Based upon structural features, the proapoptotic
group is divided into multidomain members that contain
BH1–3 domains, and BH3-only members. The former
subgroup includes BAX and BAK that are required for
ensuing apoptosis. In fact, in the absence of these proteins
cells become resistant to apoptogenic stimuli [60]. The
proapoptotic action of BAX and BAK appears to be
facilitated by BH3-only proteins and counteracted by an-
tiapoptotic members.
Far from being mutually exclusive, IMM and OMM
processes are likely to be coordinated and integrated. For
instance, an initial OMM permeabilization can be followed
by or trigger a PTP-dependent widening of tubular cristae
allowing rapid and complete release of IMS proteins. In
addition, it has to be pointed out that several BCL-2 family
members are also located at cellular sites other than the
OMM. Antiapoptotic members have been reported to re-
duce [Ca2+] within the endoplasmic reticulum (ER),
whereas proapoptotic members appear to promote ER Ca2+
release. Due to the close proximity of ER and mitochon-
dria, the latter event may lead to an increased probability of
PTP opening [61]. Additional evidence that BCL-2 pro-
teins and the PTP are connected is provided by the
observation that PTP is sensitized to opening in isolated
mitochondria and cells treated with compounds that share
the ability to bind the BH3 domain of BCL-2 and thus
displace BAX causing apoptosis [62]. These compounds
may be beneficial in the treatment of leukemia, suggesting
that the opposite strategy, i.e., stimulating BCL-2 interac-
tions with proapoptotic members could be effective in
decreasing the occurrence of apoptosis in diseased hearts.
Mitochondrial self-defense mechanisms
Owing to their multifaceted relationship with cell death,
mitochondria appear to be ideal targets for interventions
aimed at preserving cardiomyocyte viability. Obviously, in
the absence of oxygen mitochondrial ATP synthesis cannot
be restored or increased, yet protection results from
decreasing ATP hydrolysis. This goal can be achieved
through several mechanisms that are also a part of self-
defense mechanisms triggered by ischemic preconditioning
(IPC). For instance, mitochondrial depolarization promotes
F1Fo ATPase binding to its natural inhibitor IF(1). This
direct inhibition has been proposed to play a relevant role
in both classical and pharmacological IPC [63, 64]. Mito-
chondrial ATP hydrolysis also appears to be modulated by
BCL-2, since its overexpression in mouse hearts was found
to both increase cardiomyocyte survival upon reperfusion
and reduce the decline in ATP during ischemia. This effect
was attributed to a direct inhibition of F1Fo ATPase, since
the addition of oligomycin did not cause any additional
effect [65]. This finding extends the role of BCL-2 to
modulation of mitochondrial metabolism [12]. Interest-
ingly, BCL-2 is upregulated in preconditioned hearts, while
it is downregulated by ischemia/reperfusion [66]. In addi-
tion, its downregulation by means of antisense oligonu-
cleotides abolished IPC cardioprotection in perfused rat
hearts [67].
ATP hydrolysis could also be prevented by PTP inhi-
bition, a beneficial effect that would add the ATP sparing
effect to a wider range of protective actions, such as pre-
vention of NAD+ depletion, preservation of Ca2+ homeo-
stasis and lack of release of proapoptotic proteins [22–24].
The probability of PTP opening is reduced in precondi-
tioned hearts upon post-ischemic reperfusion which confers
a stress-tolerant state to cardiomyocytes [68, 69]. The re-
duced probability of PTP opening in preconditioned car-
diomyocytes is likely to be contributed by the activation of
signaling pathways [70–72]. The analysis of these pro-
cesses goes beyond the scope of this review and is covered
by other articles in this same issue.
In addition to the protection afforded by PTP inhibition,
numerous studies attribute a protective role to opening of
the mitochondrial KATP channel (mitoKATP) [73–75]. Upon
mitoKATP opening the electrophoretic influx of K+ into the
matrix causes mitochondrial depolarization along with
matrix swelling and alkalinization [76]. It has been sug-
gested that the matrix contraction caused by the Dwm de-
crease occurring during anoxia would be compensated by
the matrix swelling resulting from mitoKATP opening. This
type of swelling might both increase the efficiency of en-
ergy metabolism in the normoxic myocyte and accelerate
the recovery of optimal ATP concentrations during post-
ischemic reperfusion by preventing the loss of substrate
channeling otherwise caused by matrix contraction and
expansion of the intermembrane space [77].
Since cardioprotection is elicited by both PTP inhibition
and mitoKATP opening, the two processes are likely to be
related. Mitochondrial depolarization and ROS formation
have been suggested as plausible links rendering mitoKATP
an additional mode for modulating the PTP. The decrease
in mitochondrial membrane potential caused by mitoKATP
opening could reduce the driving force for mitochondrial
Ca2+ uptake, thus decreasing the probability of PTP
opening [78, 79]. On the other hand, matrix alkalinization
has been suggested to be responsible for the increase in
H2O2 formation observed in cardiomyocytes treated with
the mitoKATP opener diazoxide [80–82]. The increased
formation of ROS might reduce the probability of PTP
opening by affecting the redox state of critical thiol groups
[83]. In addition, a recent report suggests that PKCe acti-
vates mitoKATP resulting in a slight elevation of ROS
which eventually cause PTP inhibition [84], as also docu-
mented in a previous study [85]. The ROS-mediated link
Heart Fail Rev (2007) 12:249–260 253
123

between PKCe and mitoKATP might involve additional
factors. For instance, the increase in ROS formation in-
duced by diazoxide is blunted in cardiomyocytes and hearts
of heterozygous connexin 43 deficient (C·43+/–) mice [81].
This protein that forms gap junctions within the sarco-
lemma has been reported to accumulate within the IMM as
a result of IPC [86], while IPC protection is lost in C·43+/–
mice [87]. Therefore, it is tempting to speculate that C·43
favors PKCe interaction with mitoKATP or modulates di-
rectly mitoKATP activity.
Mitochondrially targeted cardioprotective approaches
Besides self-defense mechanisms pharmacological ap-
proaches have been developed to tackle myocardial injury
directly at the mitochondrial level. The majority of com-
pounds proposed so far can be grouped into three major
cardioprotective strategies, namely PTP inhibition, de-
creased ROS formation, and inhibition of fatty acid oxi-
dation (FAO).
PTP inhibition
Opening of the PTP is inhibited by cyclosporin (Cs) A after
binding to cyclophilin (CyP)-D, a matrix peptidyl-prolyl
cis-trans isomerase [88]. The very high-affinity binding
CsA to CyP-D is displaced by Ca2+ [89] implying that
under conditions of intracellular Ca2+ overload CsA might
not prevent PTP opening. In fact, in mitochondria devoid
of CyP-D, CsA sensitivity is lost, yet PTP opening can be
obtained although at higher [Ca2+] [90–92]. A relevant
implication of these results is that the effect of CsA is best
described as ‘‘desensitization’’ rather than inhibition of the
PTP [21]. This concept holds valid also for all the other
available PTP ‘‘inhibitors,’’ such as Sanglifehrin A and
NIM811 [93, 94]. Despite the fact that it is not a PTP
blocker, CsA represented an invaluable tool for the
advancement in our knowledge of PTP role in myocardial
ischemia. Indeed, CsA largely attenuates reperfusion in-
jury. The initial evidence obtained by using a pharmaco-
logical approach [95, 96] has also been validated by
developing direct assays for detecting PTP opening in
isolated cells and perfused hearts [97–100]. More recently,
PTP inhibition has been shown to limit the loss of viability
even when administered only at the time of reperfusion
[68, 101]. Definite support to the role of PTP desensitiza-
tion through modulation of its interaction with CyP-D was
recently provided by the reduced susceptibility to ischemic
injury observed in mice lacking CyP-D [90, 102]. All
together these findings demonstrate that PTP opening is
causally related to the loss of viability and represents a
crucial target for cardioprotection.
Antioxidants and MAO inhibition
Any antioxidant treatment is likely to be cardioprotective at
the mitochondrial level based upon the deleterious roles of
ROS on mitochondrial function and structure. However,
since mitochondria are the main intracellular source of
ROS, antioxidants acting at other cellular sites might have
a limited efficacy. This possible limitation has prompted
the development of ‘‘mitochondriotropic’’ compounds
[103, 104]. The strategy adopted in the design of these
molecules resembles that used for assessing mitochondrial
membrane potential whereby fluorescent lipophilic cations
are electrophoresed into the negatively charged mito-
chondrial matrix [105]. An example of this strategy is the
synthesis of triphenylphosphonium (TPP)-based com-
pounds, which were demonstrated to be effective antioxi-
dants in several cell types [106–108]. A TPP+-linked
analogue of ubiquinone, MitoQ, decreased reperfusion-in-
duced heart dysfunction, cell death, and mitochondrial
damage, whereas ubiquinone or TPP+ were ineffective
[109].
Besides scavenging ROS once they are formed an
alternative and perhaps more efficacious strategy is to
prevent their generation or at least the large increase
occurring under pathological conditions. This goal can be
achieved by mild uncoupling. In fact, mitochondrial
depolarization decreases ROS generation that is exponen-
tially dependent on Dwm [110, 111]. A decreased ROS
formation associated with myocardial protection has been
demonstrated by using uncouplers [112] or overexpressing
uncoupling proteins [113, 114]. On the other hand deple-
tion of uncoupling proteins reduces IPC protection and
increases ROS formation in cardiac myoblasts [115]. It
must be pointed out that also a severe uncoupling reduces
the loss of viability [116, 117]. This paradoxical finding
has been explained as resulting from a decreased avail-
ability of ATP for the generation of irreversible hyper-
contracture, which jeopardizes sarcolemma integrity upon
post-ischemic reperfusion [1, 118–121].
A third possibility for reducing mitochondrially gener-
ated oxidative stress is to inhibit mitochondrial processes
generating ROS at sites other than the respiratory chain.
For instance, MAO-A has been shown to represent an
important source of hydrogen peroxide in rat heart [122],
and MAO-A induced ROS formation resulted in cardio-
myocyte apoptosis [123, 124]. Quite interestingly, a recent
study demonstrated that MAO-A inhibition reduces myo-
cardial damage induced by 30 min of ischemia followed by
60 min of reperfusion in the rat heart [125]. Both in the
case of isolated cardiomyocytes and intact heart MAO-A
stimulation has been attributed to an increased availability
of its substrate serotonin. Besides investigating whether
MAO-A activity is modulated by factors other than an
254 Heart Fail Rev (2007) 12:249–260
123

increased supply of exogenous substrates, the specificity of
MAO inhibitors should be ascertained by comparing
pharmacological evidence with results from a genetic ap-
proach based on loss of function studies.
Metabolic approaches
The inhibition of fatty acid oxidation is the common
denominator of several, if not the majority of metabolic
approaches aimed at protecting the ischemic heart. The
expected goal of this strategy is the stimulation of pyruvate
dehydrogenase (PDH). In fact, acetyl-CoA produced in
large amounts by b-oxidation inhibits PDH thus hampering
the oxidation of pyruvate, while favoring its reduction to
lactate. It must be pointed out that this scenario is not likely
to occur under conditions of anoxia or severe ischemia,
since the absence of oxygen prevents b-oxidation. How-
ever, when oxygen supply no longer matches oxygen de-
mand or upon post-ischemic reperfusion when b-oxidation
and anaerobic (cytosolic) glycolysis are stimulated, the
excess FAO results in an increased lactate formation at the
expense of a decrease in the complete oxidation of glucose
into CO2 and H2O [126, 127] (Fig. 4).
It has been proposed that lactate accumulation by means
of intracellular pH decrease plays a relevant role in func-
tional and structural alterations of cardiomyocytes [126,
128]. Under these conditions, FAO inhibition decreases
lactate formation by restoring pyruvate oxidation [129].
This metabolic shift is likely to explain the protective ef-
fects of compounds reducing the mitochondrial uptake of
long chain acyl-CoAs by means of inhibition of carnitine
palmitoyl transferase (CPT, [130–132]) or by inhibiting
enzymes of b-oxidation [133–135]. At present, the greatest
clinical experience is with trimetazidine [136, 137] which
inhibits the last step of b-oxidation, namely b-keto acyl
CoA thiolase [133].
Alternatively, PDH can be directly stimulated by di-
chloroacetate [138, 139] or its inhibition can be removed
by reducing the acyl-CoA/CoASH ratio. This goal is effi-
ciently achieved by L-carnitine. It might seem paradoxical
that a substance known for its essential role in promoting
FAO mimics the protective effects of FAO inhibitors.
However, it is frequently overlooked that L-carnitine is the
substrate of several transferases that also transforms med-
ium-chain and short-chain acyl-CoAs into the corre-
sponding acylcarnitines. For instance, an increased supply
of carnitine promotes pyruvate oxidation by transforming
acetyl-CoA into acetylcarnitine which does not affect PDH
oxidation [140, 141]. This explains the apparent paradox
whereby the administration of L-carnitine to perfused rat
heart increases glucose oxidation while decreasing FAO
[142]. This biochemical rationale underlies the clinical
evidence of L-carnitine protection [143–145].
The maintenance of an optimal acyl-CoA/CoASH ratio
expands the role of carnitine in the metabolism of phos-
pholipids adding anabolic functions to the abovementioned
involvement in the oxidative catabolism of energy sub-
strates. Indeed, membrane phospholipid fatty acid turnover
and repair depend on LCACoA availability. In this respect
the role of carnitine and CPT is two fold: provide acyl-units
at no ATP-cost and buffer the harmful decrease in cellular
CoASH levels [146]. Supporting this concept, CPT inhi-
bition has been shown to result in a marked depression of
the reacylating capability in both human erythrocytes and
neuronal cells [147, 148].
The functions of carnitine in both energy metabolism
and phospholipid turnover indicate a general role of this
compound in the maintenance of cell viability. This cyto-
protective role is likely to be contributed by the inhibitory
effects on ceramide synthesis [149] and caspase activities
[150]. In cardiac myocytes exposed to doxorubicin, carni-
tine administration reduced the degree of apoptotic death
by preventing the increase in intracellular levels of cera-
mide, a powerful endogenous promoter of apoptosis [149].
The inhibition of ceramide production is the result of two
different actions of carnitine. In fact the subtraction of
palmitoyl CoA which is diverted from ceramide synthesis
to oxidative metabolism [151] is reinforced by the inhibi-
tory effect on acid sphyngomyelinase, which generates
ceramide in response to a host of apoptotic stimuli [149]. In
addition, carnitine has been shown to inhibit the activity of
caspases 3 and 8 [150], which act as initiator and execu-
tioner of apoptosis, respectively. Since the action of car-
nitine is reversed by palmitoylcarnitine. The free/esterified
AoCACL
enitinraclyteca
enitinrac-L
AoC-lytecaetavuryp
OAFsrotibihni
β-ox
idat
ion
HDP
esoculg
etatcal
AoCACL
OC 2 H + 2O
raCACL
AFF
I TPCsrotibihni
ACD
Fig. 4 Interventions favoring glucose oxidation while reducing
lactate formation. Inhibited processes are indicated by dashed lines.
CPT, carnitine palmitoyl transferase; DCA, dicholoroacetate; FAO,
fatty acid oxidation; FFA, free fatty acids; LCACoA, long-chain acyl-
Coa; LCACar, long-chain acylcarnitines; PDH, pyruvate dehydroge-
nase
Heart Fail Rev (2007) 12:249–260 255
123

carnitine ratio has been suggested to play a relevant role in
the cell commitment to apoptosis [150].
Concluding remarks
Although countless cellular processes are involved, mito-
chondria take center stage in determining the fate of
ischemic cardiomyocytes. It is now widely accepted that
both necrosis and apoptosis can be antagonized pharma-
cologically by drugs acting primarily or exclusively at the
level of mitochondria. In this respect, the PTP appears to be
the most relevant target to prevent the detrimental conse-
quences of myocardial ischemia. Although the significant
growth of information on mitochondrial processes related
to cell death and the availability of protective compounds
encourage some optimism, several relevant issues are far
from being solved. For instance, the molecular identity of
mitochondrial channels is still elusive hindering their
characterization as pharmaceutical targets. As discussed
above, the compounds available for reducing the proba-
bility of PTP opening act by interacting with Cyp-D and
not with pore components. On the other hand, our current
understanding of the role of mitoKATP is undermined by
lack of direct methods for cellular studies and scarce
specificity of available agonists and antagonists.
Elucidating the mitochondrial switches that control the
evolution of the ischemic injury toward recovery or loss of
viability remains an exciting challenge. The results will
help translating experimental strategies into the clinical
arena.
Acknowledgements This work was supported by grants from CNR,
FIRB, and MIUR.
References
1. Di Lisa F, Menabo R, Canton M, Petronilli V (1998) The role of
mitochondria in the salvage and the injury of the ischemic
myocardium. Biochim Biophys Acta 1366:69–78
2. Halestrap AP, Kerr PM, Javadov S, Woodfield KY (1998)
Elucidating the molecular mechanism of the permeability tran-
sition pore and its role in reperfusion injury of the heart. Bio-
chim Biophys Acta 1366:79–94
3. Jennings RB, Ganote CE (1976) Mitochondrial structure and
function in acute myocardial injury. Circ Res 38:80–91
4. Bennett MJ, Rinaldo P, Strauss AW (2000) Inborn errors of
mitochondrial fatty acid oxidation. Crit Rev Clin Lab Sci 37:1–44
5. Smeitink JA, Zeviani M, Turnbull DM, Jacobs HT (2006)
Mitochondrial medicine: a metabolic perspective on the
pathology of oxidative phosphorylation disorders. Cell Metab
3:9–13
6. Wallace DC (2000) Mitochondrial defects in cardiomyopathy
and neuromuscular disease. Am Heart J 139:S70–S85
7. Marin-Garcia J, Goldenthal MJ, Moe GW (2001) Mitochondrial
pathology in cardiac failure. Cardiovasc Res 49:17–26
8. Russell LK, Finck BN, Kelly DP (2005) Mouse models of
mitochondrial dysfunction and heart failure. J Mol Cell Cardiol
38:81–91
9. Trifunovic A, Wredenberg A, Falkenberg M, Spelbrink JN,
Rovio AT, Bruder CE, Bohlooly Y, Gidlof S, Oldfors A, Wibom
R, Tornell J, Jacobs HT, Larsson NG (2004) Premature ageing
in mice expressing defective mitochondrial DNA polymerase.
Nature 429:417–423
10. Di Lisa F, Bernardi P (1998) Mitochondrial function as a
determinant of recovery or death in cell response to injury. Mol
Cell Biochem 184:379–391
11. Di Lisa F, Blank PS, Colonna R, Gambassi G, Silverman HS,
Stern MD, Hansford RG (1995) Mitochondrial membrane po-
tential in single living adult rat cardiac myocytes exposed to
anoxia or metabolic inhibition. J Physiol 486:1–13
12. Murphy E, Steenbergen C (2007) Preconditioning: the mito-
chondrial connection. Annu Rev Physiol 69:51–67
13. Rouslin W, Erickson JL, Solaro RJ (1986) Effects of oligomycin
and acidosis on rates of ATP depletion in ischemic heart muscle.
Am J Physiol 250:H503–H508
14. Allen DG, Orchard CH (1987) Myocardial contractile function
during ischemia and hypoxia. Circ Res 60:153–168
15. Jennings RB, Steenbergen C (1985) Nucleotide metabolism and
cellular damage in myocardial ischemia. Annu Rev Physiol
477:727–749
16. Corr PB, Gross RW, Sobel BE (1984) Amphipathic metabolites
and membrane dysfunction in ischemic myocardium. Circ Res
55:135–154
17. Idell Wenger JA, Grotyohann LW, Neely JR (1978) Coenzyme
A and carnitine distribution in normal and ischemic hearts. J
Biol Chem 253:4310–4318
18. Katz AM, Messineo FC (1981) Lipid-membrane interactions
and the pathogenesis of ischemic damage in the myocardium.
Circ Res 48:1–16
19. Bernardi P (1999) Mitochondrial transport of cations: channels,
exchangers, and permeability transition. Physiol Rev 79:1127–
1155
20. Gunter TE, Pfeiffer DR (1990) Mechanisms by which mito-
chondria transport calcium. Am J Physiol 258:C755–C786
21. Bernardi P, Krauskopf A, Basso E, Petronilli V, Blalchy-Dyson
E, Di Lisa F, Forte MA (2006) The mitochondrial permeability
transition from in vitro artifact to disease target. FEBS J
273:2077–2099
22. Di Lisa F, Bernardi P (2006) Mitochondria and ischemia-rep-
erfusion injury of the heart: fixing a hole. Cardiovasc Res
70:191–199
23. Halestrap AP, Clarke SJ, Javadov SA (2004) Mitochondrial
permeability transition pore opening during myocardial reper-
fusion-a target for cardioprotection. Cardiovasc Res 61:372–385
24. Weiss JN, Korge P, Honda HM, Ping P (2003) Role of the
mitochondrial permeability transition in myocardial disease.
Circ Res 93:292–301
25. Balaban RS, Nemoto S, Finkel T (2005) Mitochondria, oxidants,
and aging. Cell 120:483–495
26. Droge W (2002) Free radicals in the physiological control of cell
function. Physiol Rev 82:47–95
27. Turrens JF (2003) Mitochondrial formation of reactive oxygen
species. J Physiol 552:335–344
28. Fridovich I (2004) Mitochondria: are they the seat of senes-
cence? Aging Cell 3:13–16
29. St-Pierre J, Buckingham JA, Roebuck SJ, Brand MD (2002)
Topology of superoxide production from different sites in the
mitochondrial electron transport chain. J Biol Chem 277:44784–
44790
30. Fridovich I (1995) Superoxide radical, superoxide dismutases.
Annu Rev Biochem 64:97–112
256 Heart Fail Rev (2007) 12:249–260
123

31. Cadenas E, Davies KJ (2000) Mitochondrial free radical gen-
eration, oxidative stress, and aging. Free Radic Biol Med
29:222–230
32. Shih JC, Chen K, Ridd MJ (1999) Monoamine oxidase: from
genes to behavior. Annu Rev Neurosci 22:197–217
33. Giorgio M, Migliaccio E, Orsini F, Paolucci D, Moroni M,
Contursi C, Pelliccia G, Luzi L, Minucci S, Marcaccio M,
Pinton P, Rizzuto R, Bernardi P, Paolucci F, Pelicci PG (2005)
Electron transfer between cytochrome c and p66Shc generates
reactive oxygen species that trigger mitochondrial apoptosis.
Cell 122:221–233
34. Orsini F, Migliaccio E, Moroni M, Contursi C, Raker VA,
Piccini D, Martin-Padura I, Pelliccia G, Trinei M, Bono M, Puri
C, Tacchetti C, Ferrini M, Mannucci R, Nicoletti I, Lanfrancone
L, Giorgio M, Pelicci PG (2004) The life span determinant
p66Shc localizes to mitochondria where it associates with
mitochondrial heat shock protein 70 and regulates trans-mem-
brane potential. J Biol Chem 279:25689–25695
35. Trinei M, Giorgio M, Cicalese A, Barozzi S, Ventura A,
Migliaccio E, Milia E, Padura IM, Raker VA, Maccarana M,
Petronilli V, Minucci S, Bernardi P, Lanfrancone L, Pelicci PG
(2002) A p53-p66Shc signalling pathway controls intracellular
redox status, levels of oxidation-damaged DNA and oxidative
stress-induced apoptosis. Oncogene 21:3872–3878
36. Migliaccio E, Giorgio M, Mele S, Pelicci G, Reboldi P, Pandolfi
PP, Lanfrancone L, Pelicci PG (1999) The p66shc adaptor
protein controls oxidative stress response and life span in
mammals. Nature 402:309–313
37. Pinton P, Rimessi A, Marchi S, Orsini F, Migliaccio E, Giorgio
M, Contursi C, Minucci S, Mantovani F, Wieckowski MR, Del
SG, Pelicci PG, Rizzuto R (2007) Protein kinase C beta and
prolyl isomerase 1 regulate mitochondrial effects of the life-span
determinant p66Shc. Science 315:659–663
38. Hausenloy DJ, Yellon DM (2003) The mitochondrial permeabil-
ity transition pore: its fundamental role in mediating cell death
during ischaemia and reperfusion. J Mol Cell Cardiol 35:339–341
39. Crompton M (1999) The mitochondrial permeability transition
pore and its role in cell death. Biochem J 341:233–249
40. Zoratti M, Szabo I (1995) The mitochondrial permeability
transition. Biochim Biophys Acta 1241:139–176
41. Petronilli V, Penzo D, Scorrano L, Bernardi P, Di Lisa F (2001)
The mitochondrial permeability transition, release of cyto-
chrome c and cell death. Correlation with the duration of pore
openings in situ. J Biol Chem 276:12030–12034
42. Kim JS, Jin Y, Lemasters JJ (2006) Reactive oxygen species, but
not Ca2+ overloading, trigger pH- and mitochondrial perme-
ability transition-dependent death of adult rat myocytes after
ischemia-reperfusion. Am J Physiol Heart Circ Physiol
290:H2024–H2034
43. Penzo D, Petronilli V, Angelin A, Cusan C, Colonna R, Scorr-
ano L, Pagano F, Prato M, Di Lisa F, Bernardi P (2004) Ara-
chidonic acid released by phospholipase A(2) activation triggers
Ca(2+)-dependent apoptosis through the mitochondrial pathway.
J Biol Chem 279:25219–25225
44. Goll DE, Thompson VF, Li H, Wei W, Cong J (2003) The
calpain system. Physiol Rev 83:731–801
45. Orrenius S, Zhivotovsky B, Nicotera P (2003) Regulation of cell
death: the calcium-apoptosis link. Nat Rev Mol Cell Biol 4:552–
565
46. Shulga N, Pastorino JG (2006) Acyl coenzyme A-binding pro-
tein augments bid-induced mitochondrial damage and cell death
by activating mu-calpain. J Biol Chem 281:30824–30833
47. Aguilar HI, Botla R, Arora AS, Bronk SF, Gores GJ (1996)
Induction of the mitochondrial permeability transition by pro-
tease activity in rats: a mechanism of hepatocyte necrosis.
Gastroenterology 110:558–566
48. Polster BM, Basanez G, Etxebarria A, Hardwick JM, Nicholls
DG (2005) Calpain I induces cleavage and release of apoptosis-
inducing factor from isolated mitochondria. J Biol Chem
280:6447–6454
49. Chen M, Won DJ, Krajewski S, Gottlieb RA (2002) Calpain and
mitochondria in ischemia/reperfusion injury. J Biol Chem
277:29181–29186
50. Breckenridge DG, Xue D (2004) Regulation of mitochondrial
membrane permeabilization by BCL-2 family proteins and
caspases. Curr Opin Cell Biol 16:647–652
51. Danial NN, Korsmeyer SJ (2004) Cell death: critical control
points. Cell 116:205–219
52. Gustafsson AB, Gottlieb RA (2007) Bcl-2 family members and
apoptosis, taken to heart. Am J Physiol Cell Physiol 292:C45–
C51
53. Kroemer G, Galluzzi L, Brenner C (2007) Mitochondrial
membrane permeabilization in cell death. Physiol Rev 87:99–
163
54. Forte M, Bernardi P (2006) The permeability transition and
BCL-2 family proteins in apoptosis: co-conspirators or inde-
pendent agents? Cell Death Differ 13:1287–1290
55. Hino K, Nishikawa M, Sato E, Inoue M (2005) L-carnitine
inhibits hypoglycemia-induced brain damage in the rat. Brain
Res 1053:77–87
56. Nakai A, Shibazaki Y, Taniuchi Y, Miyake H, Oya A, Takeshita
T (2004) Role of mitochondrial permeability transition in fetal
brain damage in rats. Pediatr Neurol 30:247–253
57. Bernardi P, Petronilli V, Di Lisa F, Forte M (2001) A mito-
chondrial perspective on cell death. Trends Biochem Sci
26:112–117
58. Bernardi P, Azzone GF (1981) Cytochrome c as an electron
shuttle between the outer and inner mitochondrial membranes. J
Biol Chem 256:7187–7192
59. Scorrano L, Ashiya M, Buttle K, Weiler S, Oakes SA, Mannella
CA, Korsmeyer SJ (2002) A distinct pathway remodels mito-
chondrial cristae and mobilizes cytochrome c during apoptosis.
Dev Cell 2:55–67
60. Wei MC, Zong WX, Cheng EH, Lindsten T, Panoutsakopoulou
V, Ross AJ, Roth KA, MacGregor GR, Thompson CB, Kors-
meyer SJ (2001) Proapoptotic BAX and BAK: a requisite
gateway to mitochondrial dysfunction and death. Science
292:727–730
61. Scorrano L, Oakes SA, Opferman JT, Cheng EH, Sorcinelli MD,
Pozzan T, Korsmeyer SJ (2003) BAX and BAK regulation of
endoplasmic reticulum Ca2+: a control point for apoptosis.
Science 300:135–139
62. Milanesi E, Costantini P, Gambalunga A, Colonna R, Petronilli
V, Cabrelle A, Semenzato G, Cesura AM, Pinard E, Bernardi P
(2006) The mitochondrial effects of small organic ligands of
BCL-2: sensitization of BCL-2-overexpressing cells to apoptosis
by a pyrimidine-2,4,6-trione derivative. J Biol Chem
281:10066–10072
63. Comelli M, Metelli G, Mavelli I (2007) Downmodulation of
mitochondrial F0F1 ATP synthase by diazoxide in cardiac
myoblasts: a dual effect of the drug. Am J Physiol Heart Circ
Physiol 292:H820–H829
64. Ylitalo K, Ala-Rami A, Vuorinen K, Peuhkurinen K, Lepojarvi
M, Kaukoranta P, Kiviluoma K, Hassinen I (2001) Reversible
ischemic inhibition of F(1)F(0)-ATPase in rat and human
myocardium. Biochim Biophys Acta 1504:329–339
65. Imahashi K, Schneider MD, Steenbergen C, Murphy E (2004)
Transgenic expression of Bcl-2 modulates energy metabolism,
prevents cytosolic acidification during ischemia, and reduces
ischemia/reperfusion injury. Circ Res 95:734–741
66. Zhao ZQ, Velez DA, Wang NP, Hewan-Lowe KO, Nakamura
M, Guyton RA, Vinten-Johansen J (2001) Progressively devel-
Heart Fail Rev (2007) 12:249–260 257
123

oped myocardial apoptotic cell death during late phase of rep-
erfusion. Apoptosis 6:279–290
67. Hattori R, Hernandez TE, Zhu L, Maulik N, Otani H, Kaneda Y,
Das DK (2001) An essential role of the antioxidant gene Bcl-2
in myocardial adaptation to ischemia: an insight with antisense
Bcl-2 therapy. Antioxid Redox Signal 3:403–413
68. Hausenloy DJ, Maddock HL, Baxter GF, Yellon DM (2002)
Inhibiting mitochondrial permeability transition pore opening: a
new paradigm for myocardial preconditioning? Cardiovasc Res
55:534–543
69. Javadov SA, Clarke S, Das M, Griffiths EJ, Lim KH, Halestrap
AP (2003) Ischaemic preconditioning inhibits opening of
mitochondrial permeability transition pores in the reperfused rat
heart. J Physiol 549:513–524
70. Hausenloy DJ, Yellon DM (2004) New directions for protecting
the heart against ischaemia-reperfusion injury: targeting the
Reperfusion Injury Salvage Kinase (RISK)-pathway. Cardiovasc
Res 61:448–460
71. Juhaszova M, Zorov DB, Kim SH, Pepe S, Fu Q, Fishbein KW,
Ziman BD, Wang S, Ytrehus K, Antos CL, Olson EN, Sollott SJ
(2004) Glycogen synthase kinase-3beta mediates convergence
of protection signaling to inhibit the mitochondrial permeability
transition pore. J Clin Invest 113:1535–1549
72. Schulz R, Cohen MV, Behrends M, Downey JM, Heusch G
(2001) Signal transduction of ischemic preconditioning. Car-
diovasc Res 52:181–198
73. Garlid KD, Paucek P, Yarov-Yarovoy V, Murray HN, Dar-
benzio RB, D’Alonzo AJ, Lodge NJ, Smith MA, Grover GJ
(1997) Cardioprotective effect of diazoxide and its interaction
with mitochondrial ATP-sensitive K+ channels. Possible
mechanism of cardioprotection. Circ Res 81:1072–1082
74. O’Rourke B (2000) Myocardial K(ATP) channels in precondi-
tioning. Circ Res 87:845–855
75. Oldenburg O, Cohen MV, Yellon DM, Downey JM (2002)
Mitochondrial K(ATP) channels: role in cardioprotection. Car-
diovasc Res 55:429–437
76. Costa AD, Quinlan CL, Andrukhiv A, West IC, Jaburek M,
Garlid KD (2006) The direct physiological effects of mi-
toK(ATP) opening on heart mitochondria. Am J Physiol Heart
Circ Physiol 290:H406–H415
77. Kowaltowski AJ, Seetharaman S, Paucek P, Garlid KD (2001)
Bioenergetic consequences of opening the ATP-sensitive K(+)
channel of heart mitochondria. Am J Physiol 280:H649–H657
78. Holmuhamedov EL, Wang L, Terzic A (1999) ATP-sensitive
K+ channel openers prevent Ca2+ overload in rat cardiac
mitochondria. J Physiol 519 Pt 2 :347–360
79. Korge P, Honda HM, Weiss JN (2002) Protection of cardiac
mitochondria by diazoxide and protein kinase C: implications
for ischemic preconditioning. Proc Natl Acad Sci U S A
99:3312–3317
80. Andrukhiv A, Costa AD, West IC, Garlid KD (2006) Opening
mitoKATP increases superoxide generation from complex I of
the electron transport chain. Am J Physiol Heart Circ Physiol
291:H2067–H2074
81. Heinzel FR, Luo Y, Li X, Boengler K, Buechert A, Garcia-
Dorado D, Di Lisa F, Schulz R, Heusch G (2005) Impairment of
diazoxide-induced formation of reactive oxygen species and loss
of cardioprotection in connexin 43 deficient mice. Circ Res
97:583–586
82. Pain T, Yang XM, Critz SD, Yue Y, Nakano A, Liu GS, Heusch
G, Cohen MV, Downey JM (2000) Opening of mitochondrial
K(ATP) channels triggers the preconditioned state by generating
free radicals. Circ Res 87:460–466
83. Costantini P, Chernyak BV, Petronilli V, Bernardi P (1995)
Selective inhibition of the mitochondrial permeability transition
pore at the oxidation-reduction sensitive dithiol by monobro-
mobimane. FEBS Lett 362:239–242
84. Costa AD, Jakob R, Costa CL, Andrukhiv K, West IC, Garlid
KD (2006) The mechanism by which the mitochondrial ATP-
sensitive K+ channel opening and H2O2 inhibit the mitochon-
drial permeability transition. J Biol Chem 281:20801–20808
85. Baines CP, Song CX, Zheng YT, Wang GW, Zhang J, Wang
OL, Guo Y, Bolli R, Cardwell EM, Ping P (2003) Protein kinase
Cepsilon interacts with and inhibits the permeability transition
pore in cardiac mitochondria. Circ Res 92:873–880
86. Boengler K, Dodoni G, Rodriguez-Sinovas A, Cabestrero A,
Ruiz-Meana M, Gres P, Konietzka I, Lopez-Iglesias C, Garcia-
Dorado D, Di Lisa F, Heusch G, Schulz R (2005) Connexin 43
in cardiomyocyte mitochondria and its increase by ischemic
preconditioning. Cardiovasc Res 67:234–244
87. Schwanke U, Konietzka I, Duschin A, Li X, Schulz R, Heusch G
(2002) No ischemic preconditioning in heterozygous connex-
in43-deficient mice. Am J Physiol Heart Circ Physiol
283:H1740–H1742
88. Halestrap AP, Davidson AM (1990) Inhibition of Ca2+-induced
large-amplitude swelling of liver and heart mitochondria by
cyclosporin is probably caused by the inhibitor binding to
mitochondrial-matrix peptidyl-prolyl cis- trans isomerase and
preventing it interacting with the adenine nucleotide translocase.
Biochem J 268:153–160
89. McGuinness O, Yafei N, Costi A, Crompton M (1990) The
presence of two classes of high-affinity cyclosporin A binding
sites in mitochondria. Evidence that the minor component is
involved in the opening of an inner-membrane Ca2+-dependent
pore. Eur J Biochem 194:671–679
90. Baines CP, Kaiser RA, Purcell NH, Blair NS, Osinska H,
Hambleton MA, Brunskill EW, Sayen MR, Gottlieb RA, Dorn
GW, Robbins J, Molkentin JD (2005) Loss of cyclophilin D
reveals a critical role for mitochondrial permeability transition
in cell death. Nature 434:658–662
91. Basso E, Fante L, Fowlkes J, Petronilli V, Forte MA, Bernardi P
(2005) Properties of the permeability transition pore in mito-
chondria devoid of Cyclophilin D. J Biol Chem 280:18558–18561
92. Schinzel AC, Takeuchi O, Huang Z, Fisher JK, Zhou Z, Rubens
J, Hetz C, Danial NN, Moskowitz MA, Korsmeyer SJ (2005)
Cyclophilin D is a component of mitochondrial permeability
transition and mediates neuronal cell death after focal cerebral
ischemia. Proc Natl Acad Sci U S A 102:12005–12010
93. Clarke SJ, McStay GP, Halestrap AP (2002) Sanglifehrin A acts as
a potent inhibitor of the mitochondrial permeability transition and
reperfusion injury of the heart by binding to cyclophilin-D at a
different site from cyclosporin A. J Biol Chem 277:34793–34799
94. Waldmeier PC, Feldtrauer JJ, Qian T, Lemasters JJ (2002)
Inhibition of the mitochondrial permeability transition by the
nonimmunosuppressive cyclosporin derivative NIM811. Mol
Pharmacol 62:22–29
95. Griffiths EJ, Halestrap AP (1993) Protection by Cyclosporin A
of ischemia/reperfusion-induced damage in isolated rat hearts. J
Mol Cell Cardiol 25:1461–1469
96. Nazareth W, Yafei N, Crompton M (1991) Inhibition of anoxia-
induced injury in heart myocytes by cyclosporin A. J Mol Cell
Cardiol 23:1351–1354
97. Di Lisa F, Menabo R, Canton M, Barile M, Bernardi P (2001)
Opening of the mitochondrial permeability transition pore cau-
ses depletion of mitochondrial and cytosolic NAD+ and is a
causative event in the death of myocytes in postischemic rep-
erfusion of the heart. J Biol Chem 276:2571–2575
98. Griffiths EJ, Halestrap AP (1995) Mitochondrial non-specific
pores remain closed during cardiac ischaemia, but open upon
reperfusion. Biochem J 307:93–98
258 Heart Fail Rev (2007) 12:249–260
123

99. Nieminen AL, Saylor AK, Tesfai SA, Herman B, Lemasters JJ
(1995) Contribution of the mitochondrial permeability transition
to lethal injury after exposure of hepatocytes to t-butylhydrop-
eroxide. Biochem J 307(Pt 1):99–106
100. Petronilli V, Miotto G, Canton M, Brini M, Colonna R, Bernardi
P, Di Lisa F (1999) Transient and long-lasting openings of the
mitochondrial permeability transition pore can be monitored
directly in intact cells by changes in mitochondrial calcein flu-
orescence. Biophys J 76:725–734
101. Argaud L, Gateau-Roesch O, Raisky O, Loufouat J, Robert D,
Ovize M (2005) Postconditioning inhibits mitochondrial per-
meability transition. Circulation 111:194–197
102. Nakagawa T, Shimizu S, Watanabe T, Yamaguchi O, Otsu K,
Yamagata H, Inohara H, Kubo T, Tsujimoto Y (2005) Cyclo-
philin D-dependent mitochondrial permeability transition regu-
lates some necrotic but not apoptotic cell death. Nature
434:652–658
103. Brookes PS, Yoon Y, Robotham JL, Anders MW, Sheu SS
(2004) Calcium, ATP, and ROS: a mitochondrial love-hate tri-
angle. Am J Physiol Cell Physiol 287:C817–C833
104. Smith RA, Porteous CM, Gane AM, Murphy MP (2003)
Delivery of bioactive molecules to mitochondria in vivo. Proc
Natl Acad Sci U S A 100:5407–5412
105. Bernardi P, Scorrano L, Colonna R, Petronilli V, Di Lisa F
(1999) Mitochondria and cell death. Mechanistic aspects and
methodological issues. Eur J Biochem 264:687–701
106. Jauslin ML, Meier T, Smith RA, Murphy MP (2003) Mito-
chondria-targeted antioxidants protect Friedreich Ataxia fibro-
blasts from endogenous oxidative stress more effectively than
untargeted antioxidants. FASEB J 17:1972–1974
107. Kelso GF, Porteous CM, Coulter CV, Hughes G, Porteous WK,
Ledgerwood EC, Smith RA, Murphy MP (2001) Selective tar-
geting of a redox-active ubiquinone to mitochondria within
cells: antioxidant and antiapoptotic properties. J Biol Chem
276:4588–4596
108. Smith RA, Porteous CM, Coulter CV, Murphy MP (1999)
Selective targeting of an antioxidant to mitochondria. Eur J
Biochem 263:709–716
109. Adlam VJ, Harrison JC, Porteous CM, James AM, Smith RA,
Murphy MP, Sammut IA (2005) Targeting an antioxidant to
mitochondria decreases cardiac ischemia-reperfusion injury.
FASEB J 19:1088–1095
110. Boveris A, Oshino N, Chance B (1972) The cellular production
of hydrogen peroxide. Biochem J 128:617–630
111. Turrens JF (2003) Mitochondrial formation of reactive oxygen
species. J Physiol 552:335–344
112. Ganote CE, Armstrong SC (2003) Effects of CCCP-induced
mitochondrial uncoupling and cyclosporin A on cell volume,
cell injury and preconditioning protection of isolated rabbit
cardiomyocytes. J Mol Cell Cardiol 35:749–759
113. Bienengraeber M, Ozcan C, Terzic A (2003) Stable transfection
of UCP1 confers resistance to hypoxia/reoxygenation in a heart-
derived cell line. J Mol Cell Cardiol 35:861–865
114. Teshima Y, Akao M, Jones SP, Marban E (2003) Uncoupling
protein-2 overexpression inhibits mitochondrial death pathway
in cardiomyocytes. Circ Res 93:192–200
115. McLeod CJ, Aziz A, Hoyt RF Jr., McCoy JP Jr., Sack MN
(2005) Uncoupling proteins 2 and 3 function in concert to
augment tolerance to cardiac ischemia. J Biol Chem 280:33470–
33476
116. Elz JS, Nayler WG (1988) Calcium gain during postischemic
reperfusion. The effect of 2,4- dinitrophenol. Am J Pathol
131:137–145
117. Ganote CE, McGarr J, Liu SY, Kaltenbach JP (1980) Oxygen-
induced enzyme release. Assessment of mitochondrial function
in anoxic myocardial injury and effects of the mitochondrial
uncoupling agent 2,4-dinitrophenol (DNP). J Mol Cell Cardiol
12:387–408
118. Altschuld RA, Wenger WC, Lamka KG, Kindig OR, Capen CC,
Mizushira V, Vander-Heide RS, Brierley GP (1985) Structural
and functional properties of adult rat heart myocytes lysed with
digitonin. J Biol Chem 260:14325–14334
119. Ganote CE, Armstrong SC (1993) Ischaemia and the myocyte
cytoskeleton: review and speculation. Cardiovasc Res 27:1387–
1403
120. Siegmund B, Klietz T, Schwartz P, Piper HM (1991) Temporary
contractile blockade prevents hypercontracture in anoxic-reox-
ygenated cardiomyocytes. Am J Physiol 260:H426–H435
121. Silverman HS, Stern MD (1994) Ionic basis of ischaemic car-
diac injury: insights from cellular studies. Cardiovasc Res
28:581–597
122. Maurel A, Hernandez C, Kunduzova O, Bompart G, Cambon C,
Parini A, Frances B (2003) Age-dependent increase in hydrogen
peroxide production by cardiac monoamine oxidase A in rats.
Am J Physiol Heart Circ Physiol 284:H1460–H1467
123. Bianchi P, Pimentel DR, Murphy MP, Colucci WS, Parini A
(2005) A new hypertrophic mechanism of serotonin in cardiac
myocytes: receptor-independent ROS generation. FASEB J
19:641–643
124. Pchejetski D, Kunduzova O, Dayon A, Calise D, Seguelas MH,
Leducq N, Seif I, Parini A, Cuvillier O (2007) Oxidative stress-
dependent sphingosine kinase-1 inhibition mediates monoamine
oxidase A-associated cardiac cell apoptosis. Circ Res 100:
41–49
125. Bianchi P, Kunduzova O, Masini E, Cambon C, Bani D, Rai-
mondi L, Seguelas MH, Nistri S, Colucci W, Leducq N, Parini A
(2005) Oxidative stress by monoamine oxidase mediates
receptor-independent cardiomyocyte apoptosis by serotonin and
postischemic myocardial injury. Circulation 112:3297–3305
126. Stanley WC, Lopaschuk GD, Hall JL, McCormack JG (1997)
Regulation of myocardial carbohydrate metabolism under nor-
mal and ischaemic conditions. Potential for pharmacological
interventions. Cardiovasc Res 33:243–257
127. Taegtmeyer H, King LM, Jones BE (1998) Energy substrate
metabolism, myocardial ischemia, and targets for pharmaco-
therapy. Am J Cardiol 82:54K–60K
128. Stanley WC, Recchia FA, Lopaschuk GD (2005) Myocardial
substrate metabolism in the normal and failing heart. Physiol
Rev 85:1093–1129
129. Stanley WC, Sabbah HN (2005) Metabolic therapy for ischemic
heart disease: the rationale for inhibition of fatty acid oxidation.
Heart Fail Rev 10:275–279
130. Chandler MP, Chavez PN, McElfresh TA, Huang H, Harmon
CS, Stanley WC (2003) Partial inhibition of fatty acid oxidation
increases regional contractile power and efficiency during de-
mand-induced ischemia. Cardiovasc Res 59:143–151
131. Kennedy JA, Kiosoglous AJ, Murphy GA, Pelle MA, Horowitz
JD (2000) Effect of perhexiline and oxfenicine on myocardial
function and metabolism during low-flow ischemia/reperfusion
in the isolated rat heart. J Cardiovasc Pharmacol 36:794–801
132. Lopaschuk GD, Wall SR, Olley PM, Davies NJ (1988) Etom-
oxir, a carnitine palmitoyltransferase I inhibitor, protects hearts
from fatty acid-induced ischemic injury independent of changes
in long chain acylcarnitine. Circ Res 63:1036–1043
133. Kantor PF, Lucien A, Kozak R, Lopaschuk GD (2000) The
antianginal drug trimetazidine shifts cardiac energy metabolism
from fatty acid oxidation to glucose oxidation by inhibiting
mitochondrial long-chain 3-ketoacyl coenzyme A thiolase. Circ
Res 86:580–588
134. McCormack JG, Barr RL, Wolff AA, Lopaschuk GD (1996)
Ranolazine stimulates glucose oxidation in normoxic, ischemic,
and reperfused ischemic rat hearts. Circulation 93:135–142
Heart Fail Rev (2007) 12:249–260 259
123

135. Pantos C, Bescond-Jacquet A, Tzeis S, Paizis I, Mourouzis I,
Moraitis P, Malliopoulou V, Politi ED, Karageorgiou H, Varo-
nos D, Cokkinos DV (2005) Trimetazidine protects isolated rat
hearts against ischemia-reperfusion injury in an experimental
timing - dependent manner. Basic Res Cardiol 100:154–160
136. Bertomeu-Gonzalez V, Bouzas-Mosquera A, Kaski JC (2006)
Role of trimetazidine in management of ischemic cardiomyop-
athy. Am J Cardiol 98:19J–24J
137. Sabbah HN, Stanley WC (2005) Metabolic therapy for heart
disease: impact of trimetazidine. Heart Fail Rev 10:281–288
138. McVeigh JJ, Lopaschuk GD (1990) Dichloroacetate stimulation
of glucose oxidation improves recovery of ischemic rat hearts.
Am J Physiol 259:H1079–H1085
139. Taniguchi M, Wilson C, Hunter CA, Pehowich DJ, Clanachan
AS, Lopaschuk GD (2001) Dichloroacetate improves cardiac
efficiency after ischemia independent of changes in mitochon-
drial proton leak. Am J Physiol Heart Circ Physiol 280:H1762–
H1769
140. Huelsmann WC, Siliprandi D, Ciman M, Siliprandi N (1964)
Effect of carnitine on the oxidation of alpha-ketoglutarate to
succinate in the presence of acetoacetate or pyruvate. Biochim
Biophys Acta 93:166–168
141. Lysiak W, Lilly K, Di Lisa F, Toth PP, Bieber LL (1988)
Quantitation of the effect of L-carnitine on the levels of acid-
soluble short-chain acyl-CoA and CoASH in rat heart and liver
mitochondria. J Biol Chem 263:1151–1156
142. Broderick TL, Quinney HA, Lopaschuk GD (1992) Carnitine
stimulation of glucose oxidation in the fatty acid perfused iso-
lated working rat heart. J Biol Chem 267:3758–3763
143. Brevetti G, Di Lisa F, Perna S, Menabo R, Barbato R, Martone
VD, Siliprandi N (1996) Carnitine-related alterations in patients
with intermittent claudication: indication for a focused carnitine
therapy. Circulation 93:1685–1689
144. Ferrari R, Cucchini F, Visioli O (1984) The metabolical effects
of L-carnitine in angina pectoris. Int J Cardiol 5:213–216
145. Iliceto S, Scrutinio D, Bruzzi P, D’Ambrosio G, Boni L, Di BM,
Biasco G, Hugenholtz PG, Rizzon P (1995) Effects of L-carni-
tine administration on left ventricular remodeling after acute
anterior myocardial infarction: the L-Carnitine Ecocardiografia
Digitalizzata Infarto Miocardico (CEDIM) Trial. J Am Coll
Cardiol 26:380–387
146. Ramsay RR, Arduini A (1993) The carnitine acyltransferases
and their role in modulating acyl-CoA pools. Arch Biochem
Biophys 302:307–314
147. Arduini A, Denisova N, Virmani A, Avrova N, Federici G,
Arrigoni ME (1994) Evidence for the involvement of carnitine-
dependent long-chain acyltransferases in neuronal triglyceride
and phospholipid fatty acid turnover. J Neurochem 62:1530–
1538
148. Arduini A, Mancinelli G, Radatti GL, Dottori S, Molajoni F,
Ramsay RR (1992) Role of carnitine and carnitine palmitoyl-
transferase as integral components of the pathway for membrane
phospholipid fatty acid turnover in intact human erythrocytes. J
Biol Chem 267:12673–12681
149. Andrieu AN, Jaffrezou JP, Hatem S, Laurent G, Levade T,
Mercadier JJ (1999) L-carnitine prevents doxorubicin-induced
apoptosis of cardiac myocytes: role of inhibition of ceramide
generation. FASEB J 13:1501–1510
150. Mutomba MC, Yuan H, Konyavko M, Adachi S, Yokoyama CB,
Esser V, McGarry JD, Babior BM, Gottlieb RA (2000) Regu-
lation of the activity of caspases by L-carnitine and palmitoyl-
carnitine. FEBS Letters 478:19–25
151. Paumen MB, Ishida Y, Muramatsu M, Yamamoto M, Honjo T
(1997) Inhibition of carnitine palmitoyltransferase I augments
sphingolipid synthesis and palmitate-induced apoptosis. J Biol
Chem 272:3324–3329
260 Heart Fail Rev (2007) 12:249–260
123




















