
MIAMI UNIVERSITY - OhioLINK ETD Center
100
MIAMI UNIVERSITY The Graduate School Certificate for Approving the Dissertation We hereby approve the Dissertation of Julia Simone Kaufman Candidate for the Degree DOCTOR OF PHILOSOPHY ______________________________________ Terri Messman-Moore, PhD, Director ______________________________________ Elise Clerkin, PhD, Reader ______________________________________ Aaron Luebbe, PhD, Reader ______________________________________ Kevin Bush, PhD, Graduate School Representative
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of MIAMI UNIVERSITY - OhioLINK ETD Center

MIAMI UNIVERSITY The Graduate School
Certificate for Approving the Dissertation
We hereby approve the Dissertation
of
Julia Simone Kaufman
Candidate for the Degree
DOCTOR OF PHILOSOPHY
______________________________________ Terri Messman-Moore, PhD, Director
______________________________________ Elise Clerkin, PhD, Reader
______________________________________ Aaron Luebbe, PhD, Reader
______________________________________ Kevin Bush, PhD, Graduate School Representative

ABSTRACT
PSYCHOLOGICAL MALTREATMENT SUBTYPES AND ASSOCIATED LONG-
TERM EFFECTS: A PERSON-CENTERED ANALYSIS
by
Julia S. Kaufman
Despite evidence indicating that psychological maltreatment (PM) has pernicious, long-
lasting effects, research on this form of child maltreatment has been slow to progress. PM
in childhood has been found to be a predictor of adult symptoms of anxiety and
depression, substance use, and substance-related problems. Although a range of abusive
and neglectful parenting behaviors can be considered psychological maltreatment,
different subtypes of PM are rarely assessed. The available research examining subtypes
of PM suggests that children experience distinct, and perhaps predictable, combinations
of PM subtypes. Yet, research has not explored how subtypes of PM naturally co-occur
or how these subtypes may differentially affect adult psychological functioning. Using
latent profile analysis, the present study explored the natural co-occurrence of PM
subtypes (i.e., terrorizing, spurning, exploiting/corrupting, isolating, and denying
emotional responsiveness) and differences in adult psychological functioning in a
community sample of 491 young women. Results indicated the best fit was a three-class
model reflecting exposure to low, moderate, and high PM, across PM subtypes. Distinct
PM groups were characterized by severity, but not subtype. Results also revealed
statistically significant differences between the three PM groups on symptoms of anxiety
and depression, substance use, and substance-related problems such that exposure to
more severe PM tended to be associated with greater symptom severity. Importantly, PM
did not occur in isolation as participants in the moderate and high PM groups reported
high rates of child physical and sexual abuse. Research and clinical implications are
discussed.

PSYCHOLOGICAL MALTREATMENT SUBTYPES AND ASSOCIATED LONG-
TERM EFFECTS: A PERSON-CENTERED ANALYSIS
A DISSERTATION
Presented to the Faculty of
Miami University in partial
fulfillment of the requirements
for the degree of
Doctor of Philosophy
Department of Department of Psychology
by
Julia S. Kaufman
The Graduate School
Miami University
Oxford, Ohio
2020
Dissertation Director: Terri L. Messman-Moore, Ph.D.

©
Julia Simone Kaufman
2020
iii
TABLE OF CONTENTS
List of Tables.......................................................................................................................v
List of Figures.....................................................................................................................vi
Dedication..........................................................................................................................vii
Acknowledgements..........................................................................................................viii
Introduction..........................................................................................................................1
Defining Psychological Maltreatment......................................................................1
Measurement and incidence of psychological maltreatment........................4
Evidence for subtypes of psychological maltreatment..................................6
Effects of Psychological Maltreatment.....................................................................7
Anxiety and depression................................................................................8
Substance use...............................................................................................9
Differential effects for different types of psychological maltreatment.......10
Purpose...................................................................................................................12
Study Aims.................................................................................................12
Hypotheses.................................................................................................13
Method...............................................................................................................................13
Participants.............................................................................................................13
Procedures..............................................................................................................14
Measures................................................................................................................14
Psychological maltreatment.......................................................................14
Physical abuse, sexual abuse, and neglect.................................................15
Anxiety and depression..............................................................................16
Substance use.............................................................................................16
Results................................................................................................................................18
Confirmatory Factor Analysis................................................................................18
Person-Centered Analysis of Childhood Psychological Maltreatment..................19
Examination of Characteristics of the Three PM Groups.......................................21
Demographic characteristics......................................................................22
Co-occurrence of other types of child maltreatment..................................22
Intercorrelation of Variables..................................................................................24

iv
Depression and Anxiety.........................................................................................25
Substance Use........................................................................................................26
Alcohol use................................................................................................26
Drug use.....................................................................................................27
Controlling for Other Types of Child Maltreatment..............................................28
Discussion..........................................................................................................................30
Adult Psychological Functioning...........................................................................31
Depression and anxiety..............................................................................31
Substance use.............................................................................................33
Alcohol use.....................................................................................33
Cannabis and nicotine use..............................................................33
Drug use.........................................................................................34
Co-Occurrence of Other Types of Child Maltreatment..........................................35
Child maltreatment type versus severity.....................................................36
Isolating effects of PM...............................................................................37
Strengths and Limitations.......................................................................................42
Implications............................................................................................................44
Conclusion.........................................................................................................................47
References..........................................................................................................................48
Tables.................................................................................................................................67
Figures................................................................................................................................86

v
LIST OF TABLES
1. Confirmatory Factor Analysis of the CAMI Psychological Maltreatment Scale..........66
2. Fit Indices for Latent Profile Models 1 – 4....................................................................67
3. Characteristics of Psychological Maltreatment Subtypes.............................................68
4. Demographic Characteristics.......................................................................................69
5. Co-occurrence of Other Types of Child Maltreatment.................................................70
6. Binomial Logistic Regression Predicting Sexual and Physical Abuse..........................71
7. Intercorrelations, Means, and Standard Deviations for Outcome Variables.................72
8. Bivariate Correlations for Outcomes Variables and Demographic Characteristics......73
9. Depression and Anxiety Between the Psychological Maltreatment Groups.................74
10. Crosstabulation of Psychological Maltreatment Groups and Depression Severity.......75
11. Crosstabulation of Psychological Maltreatment Groups and Anxiety Severity............76
12. Alcohol Use Between the Psychological Maltreatment Groups...................................77
13. Crosstabulation of Psychological Maltreatment Group and Alcohol Use.....................78
14. Cannabis and Nicotine Use Between Psychological Maltreatment Groups..................79
15. Crosstabulation of Psychological Maltreatment Groups and Drug Use Frequency......80
16. Crosstabulation of Psychological Maltreatment Groups and Drug Use Problems.......81
17. Depression and Anxiety Between Groups Controlling for CSA and CPA...................82
18. Alcohol Use Between Groups Controlling for CSA and CPA Victim Status..............83
19. Cannabis and Nicotine Use Between Groups Controlling for CSA and CPA..............84

vi
LIST OF FIGURES
1. Subtypes of Psychological Maltreatment.....................................................................85
2. Severity of Other Types of Child Maltreatment ..........................................................86
3. Percent of Physical and Sexual Abuse Victims.............................................................87
4. Percent of Physical and/or Sexual Abuse Victims.. .....................................................88
5. Characteristics of Child Sexual Abuse Experiences.....................................................89
6. Characteristics of Child Physical Abuse Experiences..................................................90

vii
DEDICATION
To my parents, without whom none of this would have been possible. Thank you for your
endless guidance and support.

viii
ACKNOWLEDGEMENTS
I would like to express my gratitude for the support and guidance I received throughout
this project. I want to thank my advisor, Dr. Terri Messman-Moore, for welcoming me
into her research lab. The time we spent thinking out loud together is something I will
truly miss. I also want to thank my dissertation committee members, Drs. Aaron Luebbe,
Elise Clerkin, and Kevin Bush, for their enthusiasm and guidance on this project.
To my peers, Alex McConnell, Lee Eshelman, Kathryn Mancini, Prachi Bhuptani, Selime
Salim, Bethany Walker, who provided endless support over the years, thank you for
listening to my ideas, reading my drafts, and for your friendship. To my partner, Dave,
thank you for incredible support and patience. I do not know how I could have done it
without you.
Lastly, I thank the women who participated in this study for sharing their stories.

1
A Person-Centered Approach to Identifying Common and Unique Impacts of Different
Psychological Maltreatment Experiences
Psychological maltreatment (PM) has received the least research attention of all forms of
child maltreatment (Barnett et al., 2005; Finkelhor, Ormrod, Turner, & Hamby, 2005; Hart &
Glaser, 2011) despite the fact that it may be the most commonly occurring (Armour, Elklit, &
Christoffersen, 2014; Barnett, Miller-Perrin, & Perrin, 2005; Hart, Binggeli, & Brassard, 1998).
PM refers to patterns of caregiver behavior that communicate to children that they are worthless,
unloved, or endangered (American Professional Society on the Abuse of Children [APSAC],
1995). PM is associated with negative outcomes such as anxiety, depression, emotion
dysregulation, and substance use (Banducci, Hoffman, Lejuez, & Koenen, 2014; Binggeli, Hart,
& Brassard, 2001; Hart et al., 1998; Norman et al., 2012; Spinazzola et al., 2014; Taillieu,
Brownridge, Sareen, & Afifi, 2016). In empirical work, PM is frequently examined as a unitary
construct despite evidence demonstrating its multidimensional nature (Paul & Eckenrode, 2015;
White, English, Thompson, & Roberts, 2016). Although PM can be conceptualized as an
umbrella term for a range of abusive and neglectful parenting behaviors, different subtypes of
PM are rarely assessed. In fact, researchers have yet to apply a person-centered approach to
examine how subtypes of PM co-occur and few studies have assessed differential effects of PM
subtypes (Allen, 2008; Shin, Lee, Jeon, & Wills, 2015; Taussig & Culhane, 2010). The available
research suggests differences in rates of PM across PM subtypes (Baker & Ben-Ami, 2011;
Taussig & Culhane, 2010) as well as differential effects of PM subtypes (e.g., Allen, 2008;
Egeland, Sroufe, & Erickson, 1983; English, Thompson, White, & Wilson, 2015; Taillieu et al.,
2016). Therefore, there is a need to investigate specific experiences of PM and associated effects
on adult functioning (Hart et al., 1998; Taussig & Culhane, 2010). The present study addresses
this gap in the literature by exploring the natural co-occurrence of PM subtypes and associated
differences in adult psychological functioning in a sample of young women.
Defining Psychological Maltreatment
Since the first national law on child abuse was enacted in the United States (Child Abuse
Prevention and Treatment Act [CAPTA], 1974) and PM received vague recognition (as “mental
injury”) in the definition of child maltreatment, a range of terms to describe PM has been used
interchangeably (Navarre, 1987; Taussig & Culhane, 2010). Today, the term PM is often
preferred because it encompasses the cognitive, affective, and interpersonal dimensions of
2
maltreatment as well as acts of omission (i.e., neglect) and acts of commission (i.e., abuse;
APSAC, 1995; Glaser, 2011; Hart & Brassard, 1987). Many definitions of PM, including the
APSAC (1995) definition, imply that emotional abuse is subsumed by PM (e.g., Hart et al.,
1998; Hart, Germain, & Brassard, 1987), although there are exceptions to this perspective (e.g.,
O’Hagan, 1995). Others have stated that the decision to use the term emotional or psychological
is a matter of convention as distinctions between these terms is often not clear (English et al.,
2015).
In a review of the literature, Brassard and Donovan (2006) concluded that there is
considerable agreement among researchers regarding what parenting behaviors constitute this
type of maltreatment. The disagreement largely concerns the following: (1) whether a behavior
should be labeled as PM or another form of abuse/neglect, (2) which subtype of PM a specific
behavior falls under, and (3) which behaviors are severe enough to be called PM as opposed to
poor parenting (Brassard & Donovan, 2006). As noted by Taussig and Culhane (2010), PM
might be defined as harsh parenting and witnessing marital violence in one study, verbal abuse or
aggression (i.e., spurning) in another, and a third study might include exploitation and
abandonment. The lack of definitional clarity impedes progress in the study of PM and limits
comparisons that can be made across studies.
PM constitutes a unique form of child maltreatment, which can be experienced in
isolation (e.g., Armour et al., 2014; Egeland et al., 1983; Garbarino & Vondra, 1987), but
frequently co-occurs with other types of child maltreatment (Bifulco, Moran, Baines, Bunn, &
Stanford, 2002; Cicchetti & Rogosch, 2001; McGee, Wolfe, & Wilson, 1997; Taillieu et al.,
2016; Trickett, Mennen, Kim, & Sang, 2009). The rates of co-occurrence are especially high for
PM and physical abuse (Clausen & Crittenden, 1991; Crittenden, Claussen, & Sugarman, 1994;
Dong et al., 2004; Hodgdon et al., 2018; McGee et al., 1997; Rice et al., 2001). Some researchers
suggest that PM may be the “core component” of child maltreatment (e.g., Hart et al., 1998; Hart
et al., 2011), “embedded in and interact[ing] with” all types of abuse and neglect (Binggeli et al.,
2001, p. xi). In fact, PM in combination with other types of child maltreatment may amplify the
effects of maltreatment (Edwards, Holden, Felitti, & Anda, 2003; McGee et al., 1997; Spinazzola
et al., 2014).
At this time, the APSAC (1995) definition of PM is the most widely utilized and agreed
upon. The APSAC (1995) guidelines define PM as “a repeated pattern of caregiver behavior or

3
extreme incident(s) that convey to children that they are worthless, flawed, unloved, unwanted,
endangered, or only of value in meeting another’s needs” (p. 2). There is general agreement
among researchers that PM reflects a wide range of parenting behaviors including acts of
commission and acts of omission. It has been suggested that, “No two cases of psychological
maltreatment will contain exactly the same elements, and many will be quite different from one
another” (Binggeli et al., 2001, p. 17). The APSAC (1995) guidelines identified and defined five
categories of PM which included spurning, terrorizing, isolating, exploiting/corrupting, and
denying emotional responsiveness. Spurning includes both verbal and non-verbal acts that reject
and degrade a child, such as demeaning, shaming, humiliating, and excessively criticizing a child
(e.g., swearing at or calling a child names; APSAC, 1995; Barnett, Miller-Perrin, & Perrin, 2011;
Hart et al., 1998). Terrorizing is defined as caregiver behavior that threatens or is likely to
physically hurt, kill, or abandon the child or the child’s loved ones or objects (e.g., threatening
suicide, threatening to physically hurt a child). In addition, behaviors that place a child or child’s
loved ones or objects in unpredictable or dangerous situations, exploit a child’s vulnerabilities
with threats, and set unrealistic expectations with threats of loss or harm if not met are
conceptualized as terrorizing. Isolating includes acts that consistently deny the child
opportunities to meet needs for interacting or communicating with peers or adults, outside or
inside the home. This can include behaviors that confine or place unreasonable limitations on the
child’s movement inside the home (e.g., locking a child in a room) and behaviors that limit social
interactions in the home or community (Barnett et al., 2011; Hart et al., 1998).
Exploiting/corrupting includes acts that encourage inappropriate, self-destructive, antisocial,
deviant or other maladaptive behaviors (e.g., encouraging alcohol or drug use, allowing a child to
watch adults have sex, and encouraging prostitution; Barnett et al., 2011; Hart et al., 1998).
Denying emotional responsiveness occurs when caretakers display no emotion in interactions
with the child and ignore the child’s attempts to interact by failing to express affection (e.g., only
interacting with a child if absolutely necessary; Barnett et al., 2011; Hart et al., 1998). While
rejection does not constitute its own category of PM, it is a relevant aspect of all categories
(Hart, Brassard, Binggeli, & Davidson, 2002; Rohner & Rohner, 1980). Rejection is most clearly
reflected in spurning and denying emotional responsiveness. With regard to spurning, rejection is
expressed through behavioral acts of hostility and aggression (i.e., acts of commission).
Rejection is conveyed in denying emotional responsiveness as “the mental attitude of

4
indifference is manifested behaviorally in a caretaker’s neglect of a child’s emotional needs”
(i.e., acts of omission; Hart et al., 2002, p. 81). The APSAC definition of PM included a sixth
category, mental health, medical, and educational neglect; however, this category was derived
from the first five and is not typically included as a separate area of research (APSAC, 1995;
Binggeli et al., 2001; Hart et al., 1998).
Measurement and incidence of psychological maltreatment. Efforts to research and
measure the incidence of PM have been challenging for several reasons. Child maltreatment has
frequently been treated as a dichotomous variable based on the presence or absence of a
maltreatment history. For example, studies that use Child Protective Service (CPS) reports as an
indicator of maltreatment typically dichotomize the variable, using CPS records to assess
whether or not maltreatment occurred. According to Newcomb and Locke (2001), treating child
maltreatment as a dichotomous variable is “blindly avoiding the reality that childhood
maltreatment exists to degree, along various continua” (p. 1221). Therefore, many researchers
advocate for measuring the severity of maltreatment while also accounting for the variety of
maltreatment types experienced (Clemmons, Walsh, DiLillo, & Messman-Moore, 2007;
Litrownik et al., 2005). Another reason to avoid the use of a dichotomous indicator of PM is that
it may be the most difficult form of child maltreatment to dichotomize by defining a cut-off or
threshold level (Wekerle, 2011).
Self-report measures of PM have presented similar challenges. Given the lack of
consistency in conceptual definitions of PM, it is not surprising that there is variability in
operational definitions applied to self-report measures. Available research in the domain of PM
has tended to focus on some subtypes of PM (e.g., terrorizing and spurning), while overlooking
others. For example, the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, 1998;
Bernstein et al., 2003) is a widely used measure that assesses different subtypes of child
maltreatment. Some researchers use the Emotional Abuse subscale of the CTQ to assess PM
(e.g., Shin et al., 2015) while others combine the Emotional Abuse and Emotional Neglect
subscales (e.g., Hamilton et al., 2013; Potthast, Neuner, & Catani, 2014). According to Baker
(2009), these two subscales of the CTQ contain four items reflecting spurning and one item for
terrorizing. The CTQ does not assess isolating, exploiting/corrupting, or denying emotional
responsiveness. Thus, the CTQ is not truly a measure of PM as defined by the APSAC (1995),
even though researchers might identify the construct as such. Baker (2009) examined 15 scales

5
that have been created to assess childhood experiences of PM. Through examination of these
self-report measures, Baker (2009) concluded that only four measures included items referencing
all five APSAC categories of PM. Examination of available self-report measures reveals that the
majority of self-report measures focus on spurning (Baker, 2009). In a review of the literature,
Brassard and Donovan (2006) concluded that parent- and self-report instruments were in need of
improvement. Thus, rates of PM vary based on the definition and measurement used.
According to CPS records, there were an estimated 674,000 victims of abuse and neglect
in 2017 in the United States, of which 5.7% were psychologically maltreated (U.S. Department
of Health and Human Services [USDHHS], 2019). However, CPS records are the most stringent
measurement of maltreatment (Finkelhor et al., 2005; Sedlak et al., 2010; USDHHS, 2019;
White et al., 2016) and tend to significantly underestimate the rate of PM (Schneider, Ross,
Graham, & Zielinski, 2005; Sedlak et al., 2010; Trickett et al., 2009). In addition, the criteria for
substantiation and the definitions of PM, if included in a state’s definition of abuse and neglect at
all, vary considerably from state to state (Newcomb & Locke, 2001; USDHHS, 2019).
Relative to CPS records, other measurements yield higher rates of PM. The National
Incidence Studies (NIS), which estimate rates of child maltreatment based on data from CPS
agencies as well as reports from a national sample of community professionals, likely provide
more accurate estimates of maltreatment rates. According to the Fourth National Incidence Study
of Child Abuse and Neglect (NIS-4), nearly 3 million children or approximately 39.5 per 1,000
children in the United States experienced maltreatment during the study year (2005-2006; Sedlak
et al., 2010). The NIS-4 emotional abuse codes closely correspond to the APSAC (1995)
categories of terrorizing, spurning, and isolating. Emotional neglect is less closely related to the
APSAC (1995) definition of PM, although several of the emotional neglect codes reflect denying
emotional responsiveness and exploiting/corrupting (Paul & Eckenrode, 2015; Sedlak et al.,
2010). Of children who were abused, 36% (4.1 per 1,000 children) were emotionally abused (an
estimated 302,600 children; Sedlak et al., 2010). Of children who were neglected, 52% (15.9 per
1,000 children) were emotionally neglected (an estimated 1,173,800 children; Sedlak et al.,
2010).
Rates of child maltreatment in community surveys are even higher. An overall
maltreatment rate of 138 per 1,000 children was obtained from a nationally representative sample
of children and youth who reported maltreatment experiences during the past year (Finkelhor et

6
al., 2005). Emotional abuse (i.e., spurning) was the most frequent type of child maltreatment
experienced, at a rate of 103 per 1,000 (Finkelhor et al., 2005). In another large, community
survey with a nationally representative sample of 4,549 children and youth, Finkelhor, Turner,
Ormrod, and Hamby (2009) found a past-year rate of psychological abuse by an adult (i.e.,
spurning) of 6.4% (64 per 1,000) and a lifetime rate of 11.9% (119 per 1,000). Among
adolescents aged 14 to 17 years, 22.6% (226 per 1,000) had experienced spurning over their
lifetime (Finkelhor et al., 2009).
Rates of childhood PM retrospectively reported by adults vary. A sample of 8,613 adults
who attended a primary care clinic in California completed a survey, and 10.2% reported a
history of emotional abuse (i.e., spurning and terrorizing; Dube et al., 2003). In a study of parents
reporting their own parenting behaviors, Straus and Field (2003) found that by the time their
child had reached age two, 90% of parents in a national telephone survey reported using
psychological aggression (i.e., spurning) toward their child in the previous year. The “true
prevalence” of PM is not known, as the majority of incidents remain unreported (Hart et al.,
2011, p. 131); however, many researchers agree that PM is the most frequently occurring form of
child maltreatment (Hart et al., 1998; Armour et al., 2014; Barnett et al., 2005). The best estimate
of the overall rate of PM is approximately 30% of the population (Binggeli et al., 2001).
Evidence for subtypes of psychological maltreatment. Theory and research indicate
that PM is a multidimensional construct; nonetheless, most studies treat PM as unidimensional
(Paul & Eckenrode, 2015; White et al., 2016). Few published studies examine different
experiences of PM, despite widespread recognition of the vast range of abusive and neglectful
parenting behaviors that constitute this form of maltreatment (e.g., Baker, 2009; Binggeli et al.,
2001; Brassard & Donovan, 2006). Available research examining subtypes of PM indicates that
the rate and co-occurrence of the subtypes vary (e.g., Baker & Verrocchio, 2015; de la Vega, de
la Osa, Ezpeleta, Granero, & Domènech, 2011; Taussig & Culhane, 2010; Trickett et al., 2009).
For example, Baker and Ben-Ami (2011) examined subtypes of PM in a sample of 118 adult
children of divorced parents. Of participants who endorsed experiencing at least one type of PM
in childhood, 85.7% reported they were denied emotional responsiveness, 60.3% were spurned,
41.3% were isolated, 34.9% terrorized, and 30.2% exploited/corrupted. In addition, of
participants reporting a PM history, over one-fourth (27.0%) endorsed two PM subtypes, over
one-fifth (23.8%) endorsed four subtypes, and 6.3% endorsed all five subtypes (Baker & Ben-
7
Ami, 2011). Studies that have examined different subtypes of PM have found that some subtypes
tend to co-occur more than others. For example, the combination of terrorizing and spurning may
be the most common co-occurring type of PM, with one study finding that 78.9% of children
who experienced spurning or terrorizing also experienced the other (Trickett et al., 2009). In
addition, children who experience terrorizing/spurning may be more likely to experience
abandonment than not (Taussig & Culhane, 2010). Experiences of exploiting/corrupting and
isolating also frequently co-occur, with one study reporting that 65.0% of the children who
experienced one subtype also experienced the other (Trickett et al., 2009). Together, this
research suggests that some PM subtypes are more common than others, and that children
experience unique and perhaps predictable combinations of PM subtypes.
Effects of Psychological Maltreatment
PM is associated with a range of negative outcomes including symptoms of depression
and anxiety, risky behavior including substance use, and interpersonal problems (Hart et al.,
1998; Norman et al., 2012; Spinazzola et al.; 2014; Taillieu et al., 2016). In fact, with the
exception of child maltreatment that results in death, PM may produce the most destructive and
long-lasting effects (Berzenski & Yates, 2011; Binggeli et al., 2001; Ney, Fung, & Wickett,
1994) through broad impairments in social and emotional development, which can be observed
beginning in early childhood (Egeland & Sroufe, 1981; Egeland et al., 1983; McGee et al.,
1997). For example, studies using data from the Minnesota Longitudinal Study of Parents and
Children revealed that by 18 months of age, children who were denied emotional responsiveness
displayed a decline in social and emotional functioning that was more striking and devastating
than that observed in children exposed to other types of maltreatment (Egeland & Sroufe, 1981;
Egeland et al., 1983). In older children and adolescents, effects of PM are similarly devastating.
For instance, verbal abuse (i.e., terrorizing/spurning) and emotional neglect (i.e., denying
emotional responsiveness) were found to significantly impact development as measured by
children’s perceptions of themselves and their future (Ney et al., 1994).
The experience of PM in childhood continues to confer risk for mental health problems in
adulthood, although research on the effects of PM in adults is limited both in terms of the
number of studies and the outcomes examined. Some researchers posit that relative to other types
of child maltreatment, PM is equally or even more strongly associated with later psychological
functioning (Barnett et al., 2011; Berzenski & Yates, 2011; Hart et al., 1998). For example,

8
controlling for other types of child maltreatment, adolescents’ and adults’ perceptions of
childhood experiences of PM are associated with psychological distress (Crawford & Wright,
2007; McGee et al., 1997; Spertus, Yehuda, Wong, Halligan, & Seremetis, 2003; Wright,
Crawford, and Del Castillo, 2009). Similarly, Greenfield and Marks (2010) found that a history
of psychological violence (i.e., terrorizing/spurning) was associated with more negative affect
and less psychological well-being in adults, regardless of whether or not participants had
experienced physical abuse.
Anxiety and depression. Across samples, the evidence for PM as a risk for anxiety and
depression is consistently strong (Crow, Cross, Powers, & Bradley, 2014; McGee et al., 1997;
Nelson, Klumparendt, Doebler, & Ehring, 2017; Norman et al., 2012). In a large national sample
of clinic-referred youth, Spinazzola et al. (2014) found that compared to physical and sexual
abuse, PM was the strongest and most consistent predictor of internalizing problems including
depression, generalized anxiety, and social anxiety. In college student and adult samples, PM
continues to predict anxiety and depression (e.g., Briere & Runtz, 1988), and these effects
remain even when other types of child maltreatment are considered (Crow et al., 2014; Gibb,
Chelminski, & Zimmerman, 2007; Gross & Keller, 1992; Miller-Perrin, Perrin, & Kocur, 2009;
Spertus, Yehuda, Wong, Halligan, & Seremetis, 2003; Taillieu et al., 2016). For example, Miller-
Perrin et al. (2009) identified parental psychological aggression (i.e., spurning and terrorizing)
during childhood as the most unique predictor of depression severity scores in college students,
above and beyond the impact of physical abuse, the frequency of corporal punishment, and
demographic characteristics. In adult psychiatric patients, Martins, Von Werne Baes, Tofoli, and
Juruena (2014) found that patients with a history of emotional abuse (i.e., spurning and
terrorizing) had more severe symptoms of depression, hopelessness, suicidal ideation, and
anxiety compared to patients without a history of spurning. Further, approximately 70% of
patients diagnosed with a depressive disorder reported a history of spurning and terrorizing
(Martins et al., 2014). In a systematic review of the literature on non-sexual child maltreatment,
Norman et al. (2012) found that individuals with histories of emotional abuse (defined differently
across studies, but often reflecting spurning) had a higher risk of developing depressive and
anxiety disorders compared to individuals with histories of physical abuse and neglect and those
with no childhood maltreatment history. In addition, research suggests a dose-response
relationship between the severity of PM experiences and the likelihood of chronic or recurrent

9
major depression (Bifulco et al., 2002). Therefore, there is strong evidence for an association
between childhood experiences of PM and symptoms of anxiety and depression in adulthood;
however, this evidence is predominantly based on studies focusing on spurning/terrorizing and
on assessment of PM as a unidimensional construct.
Substance use. In contrast to the evidence for an association between PM and symptoms
of anxiety and depression, the evidence for substance use and substance-related problems is far
less clear. In a systematic review of the literature, Norman et al. (2012) concluded that the
evidence was not consistent across studies or across types of substances. Norman et al. (2012)
identified PM as a strong risk factor for drug use, but the evidence for alcohol problems and
tobacco smoking was weaker and inconsistent. However, since Norman et al.’s (2012) review,
several studies have presented evidence suggesting the relation between PM and alcohol use and
alcohol use problems (Duke, 2018; Hayre, Goulter, & Moretti, 2019; Taillieu et al., 2016) and
tobacco or nicotine use (Duke, 2018; Elliott, et al., 2014; Hayre et al., 2019; Taha, Galea, Hien,
& Goodwin, 2014) may be stronger than previously believed. Among cocaine dependent women,
severity of emotional abuse (i.e., spurning and terrorizing) is associated with a greater severity of
substance abuse and with younger age of first alcohol use, but not significantly associated with
age of onset of regular alcohol, nicotine, or cocaine use or age of first nicotine or cocaine use
(Hyman, Garcia, & Sinha, 2006). However, in non-treatment seeking samples, PM has been
identified as a predictor of alcohol use and alcohol-related problems (Dube, Anda, Felitti,
Edwards, & Croft, 2002; Mandavia, Robinson, Bradley, Ressler, & Powers, 2016; Mezquita,
Ibáñez, Moya, Villa, & Ortet, 2014; White et al., 2016). Moran, Vuchinich, and Hall (2004)
examined the relation between different types of child maltreatment and substance use among
high school students. Although all maltreatment types were associated with tobacco, alcohol, and
illicit drug use, emotional abuse (i.e., spurning) was associated with lower risk of substance use
compared to other types of maltreatment. It is worth noting that Moran et al. (2004) assessed
each type of child maltreatment with a single item, and the assessment of spurning was
particularly weak as it was not behaviorally specific, and it required participants to assume
intentionality on the part of perpetrator(s). In other studies, PM has emerged as a stronger
predictor of substance use and/or substance use problems than other types of child maltreatment
(Rosenkranz, Muller, & Henderson, 2012; Scheidell et al., 2017; Shin et al., 2015; Spinazzola et
al., 2014; Taillieu et al., 2016; White et al., 2016). For example, Potthast et al. (2014) explored

10
the impact of child maltreatment on alcohol dependence in a sample of treatment-seeking adults.
Results indicated that emotional maltreatment (i.e., spurning and terrorizing) was the strongest
predictor of alcohol dependence severity, above and beyond the effect of child sexual abuse
(CSA), child physical abuse (CPA), and peer victimization. Among non-treatment-seeking
adults, emotional abuse (i.e., spurning and terrorizing) is associated with frequency of alcohol
use, binge drinking (i.e., heavy episodic drinking), alcohol-related problems, and alcohol use
disorders, controlling for demographic characteristics, psychological distress, and other types of
child maltreatment (Shin et al., 2015).
Differential effects for different types of psychological maltreatment. There is
growing evidence to suggest that different subtypes of PM have different short- and long-term
effects. However, it is worth noting that research has tended to focus on children and adolescents
and on experiences of terrorizing and spurning, often excluding other subtypes of PM. Research
on young children has demonstrated the particularly devastating impact of psychologically
unavailable or emotionally unresponsive caregivers (i.e., denying emotional responsiveness) on
development, even when children are receiving adequate physical care (Brassard & Donovan,
2006; Egeland & Sroufe, 1981; Egeland et al., 1983). In middle childhood and adolescence,
research indicates that caregiving characterized by denying emotional responsiveness and
spurning has a negative impact on development. For example, Shaffer, Yates, and Egeland
(2009) found that emotional abuse (i.e., spurning) and emotional neglect (e.g., denying emotional
responsiveness) were associated with increased social withdrawal in middle childhood and lower
ratings of socioemotional competence in early adolescence. The relation between spurning, but
not denying emotional responsiveness, and adolescent socioemotional competence was mediated
by social withdrawal in middle childhood (Shaffer et al., 2009). In a longitudinal study
examining the impact of marital violence on children, Stuewig and McCloskey (2005) found that
parental rejection (i.e., spurning) and parental warmth (i.e., emotional responsiveness) assessed
when the youth were approximately 15 years old, were correlated with symptoms of depression
two years later. Spurning in adolescence was associated with the adolescent’s shame proneness,
which was in turn associated with depression (Stuewig & McCloskey, 2005). Paul and
Eckenrode (2015) found gender differences in the association between PM and adolescent
depressive symptoms. For adolescent girls, caregiver degradation (i.e., spurning) was predictive
of increased depressive symptoms, controlling for experiences of physical and sexual abuse. On

11
the other hand, for adolescent boys, isolation was predictive of depressive symptoms (Paul &
Eckenrode, 2015).
With regard to older adolescents, White et al. (2016) used data from the Longitudinal
Studies of Child Abuse and Neglect (LONGSCAN) to explore the relation between childhood
experiences of PM and psychological symptoms and substance use at age 18. Measurement of
PM was based on self-report and CPS allegations of maltreatment that were coded using the
Maltreatment Classification System modified by LONGSCAN (MMCS). White et al. (2016)
found that both self-reports and CPS reports of failure to support psychological safety and
security (i.e., terrorizing) predicted anxiety, depression, and use of illegal drugs other than
marijuana, controlling for demographic characteristics and other types of child maltreatment.
Self-reports of terrorizing, but not official reports, predicted cigarette smoking. CPS reports of
failure to provide acceptance and self-esteem (i.e., spurning) emerged as a unique predictor of
problem drinking. Other PM subtypes including failure to allow age-appropriate autonomy (i.e.,
exploiting/corrupting) and restriction (i.e., isolating) did not emerge as significant predictors of
anxiety, depression, or any substance use (White et al., 2016).
Research examining the long-term effects of different PM subtypes in adults is quite
limited. In a sample of 256 undergraduate psychology students, Allen (2008) found that anxiety
and depression were significantly correlated with perceptions of childhood experiences of
degradation (i.e., spurning), terrorizing, ignoring (i.e., denying emotional responsiveness), and
witnessing family violence, but not with isolating. Regression analyses that included four
subtypes of PM, physical abuse, and gender, revealed differential effects of PM subtypes.
Specifically, terrorizing emerged as a unique predictor of anxiety and denying emotional
responsiveness emerged as a unique predictor of depression (Allen, 2008). Taillieu et al. (2016)
used cross-sectional data from the National Epidemiological Survey on Alcohol and Related
Conditions, which used a large, representative sample of adults living in the United States to
examine associations between child maltreatment and psychiatric disorders. Direct comparison
of a history of emotional neglect (i.e., other/denying emotional responsiveness) and emotional
abuse (i.e., spurning/terrorizing) revealed that spurning/terrorizing was associated with higher
odds of a lifetime diagnosis of psychiatric disorders including depression, anxiety disorders, and
any substance use disorder, controlling for other types of child maltreatment. Taken together,

12
available research suggests that different experiences of PM may differentially affect adult
psychological functioning.
Purpose
Research suggests that PM has powerful and persistent effects on psychological
functioning. Although PM can be conceptualized as an umbrella term for a range of abusive and
neglectful parenting behaviors, different subtypes of PM are rarely assessed. In fact, most studies
treat PM as a unitary construct despite theory and evidence supporting a multidimensional
construct (Paul & Eckenrode, 2015; White et al., 2016). Moreover, while research indicates that
the rate and co-occurrence of subtypes of PM varies, research has yet to explore how these
subtypes naturally co-occur. There is very little research on the differential impacts of subtypes
of PM (Allen, 2008; Taussig & Culhane, 2010) and researchers have tended to assess PM using
measures that only capture experiences of spurning and terrorizing. When PM subtypes have
been studied, differential effects of the different subtypes have emerged (e.g., Allen, 2008; Paul
& Eckenrode, 2015; Schneider et al., 2005). Researchers including Hart and colleagues (1998)
have called for additional studies examining the relations between the severity of different
subtypes of PM and associated effects. Taussig and Culhane (2010) have emphasized the
importance of understanding the differential impacts of the different subtypes of PM in order to
truly understand the impact of PM on psychosocial development and adult functioning.
Study aims. The purpose of the present study was to examine childhood experiences of
PM in a sample of young women. The primary aim was to use a person-centered analytic
approach to empirically identify naturally occurring subgroups or profiles of women based on
subtypes of PM experienced in childhood. Prior to conducting the person-centered analysis, I
tested the fit of the data with the APSAC model, examining whether the CAMI PM items loaded
adequately onto the factors or PM subscales. Given the high co-occurrence of PM with other
types of child maltreatment (i.e., sexual abuse, physical abuse, and neglect), I planned to
investigate whether certain derived PM profiles are more strongly associated with the presence
and/or severity of other types of child maltreatment. The second aim of the present study was to
examine associations between specific PM experiences and adult outcomes. Specifically, I
examined whether PM profiles were differentially associated with indicators of psychological
functioning including depression, anxiety, and substance use.

13
Hypotheses. The person-centered analysis of naturally occurring profiles of different PM
experiences was exploratory in nature, as this was the first study to conduct such an analysis
using subtypes of PM. Therefore, there were no a priori hypotheses regarding the number of
latent profiles. I expected to find a derived latent profile of participants who reported relatively
low levels of all PM subtypes and at least one latent profile of participants who reported
experiencing PM during childhood.
In terms of the co-occurrence of other types of child maltreatment, certain PM profiles
were hypothesized to be differentially associated with the presence/absence and severity of
different types of child maltreatment. The hypothesized low PM profile was expected to have a
lower prevalence and lower levels of severity of all other types of child maltreatment (i.e.,
physical abuse, sexual abuse, and neglect). In addition, previous research suggests that physically
abusive parents are likely to also terrorize and spurn their children (Berzenski & Yates, 2011;
Kim, Mennen, & Trickett, 2016; Ney et al., 1994; Trickett et al., 2009). Therefore, a PM profile
characterized by high levels of terrorizing/spurning was hypothesized to have relatively higher
rates and levels of severity of child physical abuse compared to profiles with lower levels of
terrorizing/spurning. Given previous research suggesting that children who are neglected in one
domain are highly likely to be neglected in other domains (Claussen & Crittenden, 1991), a
derived PM profile characterized by having been denied emotional responsiveness was expected
to be more strongly associated with neglect than profiles with lower levels of denying emotional
responsiveness. It was also hypothesized that compared to a low PM profile, PM profiles with
more severe PM experiences would be more strongly associated with indicators of poor adult
psychological functioning (i.e., depressive and anxiety symptoms, substance use).
Method
Participants
Participants were 491 community women between the ages of 18 and 25 (M = 21.74, SD
= 2.23) who were part of a larger, multi-site study examining mechanisms underlying sexual
revictimization. One participant was removed from analyses as all child maltreatment data was
missing. Approximately two-thirds of participants (61.3%) identified as White, 35% as African
American, 4.3% Asian/Pacific Islander, 3.1% Native American, and 2.6% other, and 5.7% of
participants identified at Latina/Hispanic. Over half of participants were students (61.7%; full- or
part-time) at the time of the study. The median household income was between $10,000 and
14
$20,000. Two hundred two participants (41.2%) reported an annual household income under
$10,000, 79 participants (16.1%) reported income between $10,000 and $20,000, 19% reported
income between $20,000 and $40,000, 12.7% reported income between $40,000 and $75,000,
and 9.8% reported income above $75,000. The majority of participants had never been married
(83.3%), 13.6% were married or in a long-term relationship (defined as three or more years) and
cohabitating, and 2.6% were separated or divorced. One-fifth (20.2%) of participants had
children.
Procedures
Data were collected as part of the baseline assessment of a larger, multi-site prospective
study. The Project WISE data were collected at four geographic locations (Lincoln and Omaha,
Nebraska; Jackson, Mississippi; Oxford, Ohio). The larger study focused on emotion
dysregulation and sexual revictimization in young adult women. All procedures were approved
by the Institutional Review Board of the participating institutions. The larger study included a
community sample of young women from the four study locations. All women between ages of
18 and 25 within the specified geographic regions (zip codes) were mailed a letter notifying them
of study. Women were also recruited through advertisements in newspaper and on Craigslist,
fliers posted in the communities, and university mass emails. The consent process was completed
in person and all participants provided written informed consent for study participation. At the
baseline assessment, participants completed diagnostic interviews as well as a series of self-
report questionnaires. Self-report questionnaires were completed online on a computer in the
laboratory of one of the study sites. Participants were reimbursed $75 upon completion of the
baseline assessment.
Measures
Psychological maltreatment. The Computer Assisted Maltreatment Inventory (CAMI;
DiLillo, 2003; DiLillo et al., 2010) is a computer-based, self-report measure that was developed
to assess five types of child maltreatment (sexual abuse, physical abuse, exposure to domestic
violence, psychological maltreatment, and neglect). The CAMI uses specific behavioral criteria,
based on acts commonly defined as abuse in the child maltreatment literature. The CAMI has
been shown to have good test-retest reliability and good criterion-related validity compared to a
standard measure of childhood maltreatment (DiLillo et al., 2010). The psychological
maltreatment (PM) scale was developed from an initial pool of 57 items generated by a team of

15
researchers. The items were thought to represent the major domains of psychological
maltreatment based on the APSAC (1995) definition (i.e., terrorizing, spurning, isolating,
exploiting or corrupting, and denying emotional responsiveness). The CAMI PM scale was
reduced from 57 items to 24 items based on results of an exploratory factor analysis (EFA; Nash,
Hayes-Skelton, & DiLillo, 2012). The revised CAMI PM scale consisting of 24 items was used
in the present study. For the purpose of the present study, the number of CAMI PM items
referencing each APSAC (1995) category of PM was determined based on examination of each
item’s content, examination of Nash et al.’s (2012) EFA, and in consultation with my research
advisor. For the CAMI PM scale, participants were instructed to indicate how much they agree
or disagree with each statement using a 5-point Likert scale ranging from 1 (strongly disagree) to
5 (strongly agree). Items in the emotional responsiveness subscale were reverse scored.
Instructions for the PM scale read as follows: “Please indicate by using the scale below how
much you agree or disagree with each statement. By ‘parents’ we mean any parent, stepparent,
foster parent, or other primary caregiver who took care of you as a child, even if they were not
biologically related to you.” Mean scores were calculated for each PM subscale. Reliability
coefficients have been high for the 24-item PM scale, α = .91 (Nash et al., 2012).
Physical abuse, sexual abuse, and neglect. The CAMI (DiLillo, 2003; DiLillo et al.,
2010) was also used to assess childhood experiences of physical abuse (CPA), sexual abuse
(CSA), and neglect. The physical and sexual abuse scales were scored in two different ways,
continuously as a measure of severity and dichotomously as an indicator of the presence or
absence of both types of child maltreatment. The physical and sexual abuse scales begin with
behaviorally specific screener questions that reveal whether or not participants experienced or
were exposed to various abusive acts before age 18. The screener questions are followed by
questions that inquire about the details of such events. The presence of certain features of the
events, which were empirically determined to reflect greater severity of CPA and CSA (e.g.,
frequency of the acts, nature of the acts, duration of the acts, whether injury resulted from the
acts, number of perpetrators, relationship to perpetrator[s]) are assigned a weighted score
reflecting abuse severity. The neglect scale was developed from an initial pool of 38 items and a
revised version of the CAMI neglect scale consisting of 20 items was created based on results of
an exploratory factor analysis (Nash et al., 2012). The revised CAMI neglect scale was used in
the present study and was scored continuously with higher mean scores indicating greater
16
severity. The CAMI has demonstrated excellent internal consistency for child sexual abuse (α =
.96) and child physical abuse (α = .86; DiLillo et al., 2009) and good internal consistency for
neglect (α = .88; Nash et al., 2012). Cronbach’s alpha for the neglect subscale of the CAMI in
the present sample was .93. The CAMI has demonstrated adequate test-retest reliability, with
kappa coefficients ranging from .74 to .95 for sexual abuse and .66 to .82 for physical abuse.
Good criterion validity is suggested by strong correlations with corresponding scores on the CTQ
(Bernstein & Fink, 1998; r = .55 for sexual abuse and r = .53 for physical abuse; DiLillo et al.,
2010).
Anxiety and depression. The short form version of the Depression, Anxiety, and Stress
Scale (DASS-21; P. F. Lovibond & Lovibond, 1995) is a 21-item self-report measure of
depression, anxiety, and stress symptom severity. The DASS-21 is designed to measure
symptoms that are common to depression and anxiety. Respondents are asked to indicate the
presence of symptoms over the previous week on a 4-point scale ranging from 0 (did not apply to
me at all over the last week) to 3 (applied to me very much or most of the time over the past
week). Each of the three subscales consists of 7 items and total subscale scores are calculated by
summing responses of each item. Higher scores indicate greater levels of distress. The subscales
of the DASS-21 have demonstrated adequate internal consistency (range = .80 to 93; Henry &
Crawford, 2005; Sinclair, Siefert, Slavin-Mulford, Stein, Renna & Blais, 2012). Cut-off scores
for the subscales of the DASS-21 have been established to characterize degree of severity
relative to the general population. The cut-off scores define severity categories for normal, mild
(i.e., above the population mean, not a mild level of a disorder), moderate, severe, and extremely
severe. The depression and anxiety subscales were used in the present study. Cronbach’s alphas
for the DASS-21 depression and anxiety subscales in this sample are .89 and .80, respectively.
Substance use. The Alcohol Use Disorders Identification Test (AUDIT; Saunders,
Aasland, Babor, de la Fuente, & Grant, 1993) is a 10-item self-report measure designed to
identify individuals with hazardous and harmful patterns of alcohol consumption. The AUDIT is
frequently used as a screening tool for detection of high-risk drinking, and researchers often use
the AUDIT as a continuous measure of hazardous or problematic alcohol use (e.g., Watkins,
Maldonado, & DiLillo, 2014). The AUDIT assesses three aspects of problematic drinking
including quantity and frequency of alcohol use, symptoms of alcohol use disorder, and
problems caused by alcohol use. Each item is scored using a scale ranging from 0 to 4. Total
17
scores range from 0 to 40 with higher scores indicating greater problematic alcohol use. Two
scores were used in the present study: (1) a sum score consisting of all 10 items, reflecting
problematic alcohol use and, (2) a dichotomous score using a cutoff of 8 or more indicating
problematic alcohol use (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001; Saunders et al.,
1993). The AUDIT has high internal consistency and it has been shown reliably identify patients
with hazardous drinking patterns (Babor et al., 2001; Saunders et al., 1993). Cronbach’s alpha
for the AUDIT in this sample is .83.
Heavy episodic drinking (HED) in the past year was assessed with four items. The items
assessed past year frequency of heavy drinking (four or more alcoholic drinks on a single
occasion), alcohol intoxication, being unable to remember things from the night before, and
being unable to consent to sexual activity due to alcohol consumption. Participants responded to
each item using a 5-point Likert scale ranging from 0 to 4 (0 = Never; 1 = Monthly or less; 2 = 2-
4 times per month; 3 = 2-3 times per week; 4 = 4 or more times a week). The four items were
highly correlated with each other, with correlations ranging between .41 and .81, so items were
averaged to create a single score of HED.
The Drug Use Questionnaire (DUQ; Hien & First, 1991) is an 18-item self-report
measure that assesses frequency and problems associated with drug use in the past year. For
items assessing the frequency of drug use, participants responded to each item using a 6-point
Likert scale ranging from 0 to 5 (0 = Never; 1 = One time; 2 = Monthly or less; 3 = 2-4 times a
month; 3 = 2-3 times a week; 4 = 4 or more times a week). For items assessing problems
associated with drug use, participants indicated how frequently they experienced each problem
using a 5-point Likert scale ranging from 0 to 4 (0 = Never; 1 = Less than monthly; 2 = Monthly;
3 = Weekly; 4 = Daily or almost daily). Cronbach’s alpha for the DUQ in the present sample was
.82. Three frequency scores (i.e., nicotine use, cannabis use, and drug use other than cannabis)
and a score for problems associated with drug use were computed. Nicotine and cannabis use
were each one item. Item responses were summed to create composite indices of the frequency
of drug use other than cannabis and drug use problems. The distribution of the drug use
frequency and drug use problems scores were highly skewed and the differences between
intervals on the scales were not equal, ruling out the possibility of treating them as interval
scales. These two composite scores were transformed into ordinal scales. For the frequency of
drug use other than cannabis, original scores were recoded into three categories (0 = no drug use;

18
1-2 = low drug use; ≥ 3 = moderate to high drug use). The ordinal scale for drug use problems
also contained three categories (0 = no drug use problems; 1-2 = mild drug use problems; ≥ 3 =
moderate to severe drug use problems).
Results
A Missing Value Analysis (MVA; SPSS 2016) was used to determine the pattern of the
missing data. According to Little’s MCAR test (Little, 1988), data were not consistent with a
pattern of missing completely at random, χ2 (332) = 454.06, p < .001. Examination of the
missing data revealed that only 0.35% of values were missing and there no clear patterns of
missingness. Widaman (2006) recommended the use of single imputation when the amount of
missing data is relatively low (i.e., 1-2%). Given the lack of patterns of missingness and the
small amount of missing data, single imputation was used. Missing data were singly imputed at
the scale level using the expected maximization algorithm with 25 iterations (Graham, 2009;
Little & Rubin, 1987). Scale scores were calculated only if participants had complete data for at
least 80% of the measure (Graham, 2009).
All study variables were examined for statistical normality. All variables with the
exception of the DUQ drug use frequency and drug use problems fulfilled the statistical
assumption of normality. Drug use frequency other than cannabis and drug use problem severity
scores were transformed into categorical variables.
For all one-way MANOVAs in the present study, the assumption of homogeneity of
covariance matrices was violated as indicated by Box’s M statistic (ps < .001). Pillai’s Trace is
more robust than other test statistics and it is recommended when there is heterogeneity of
covariance matrices and group sizes are unequal (Olson, 1974; Pillai & Jayachandran, 1967). For
all follow up one-way ANOVAs, the assumption of homogeneity of variances was not met as
indicated by Levine’s Test (ps < .001). The Games-Howell post hoc test for pairwise
comparisons is robust to non-normality and controls Type I error rate when there are unequal
size groups with unequal variances (Games & Howell, 1976; Sauder & DeMars, 2019; Shingala
& Rajyaguru, 2015). Therefore, the Pillai’s Trace statistic and Games-Howell post hoc procedure
were used in the present study.
Confirmatory Factor Analysis
The CAMI PM scale was submitted to confirmatory factor analysis (CFA) to determine
whether the APSAC (1995) model fit the data. A CFA was performed using robust weighted

19
least squares (WLSMV) using MPlus Version 7.3 (Muthén & Muthén, 1998-2012). Multiple
indices of model fit were used and models are thought to fit the data well with the following:
non-significant chi-square, root mean square error of approximation (RMSEA; < .06; Hu &
Bentler, 1999; Steiger & Lind, 1980), weighted root-mean-square residual (WRMR; < 1.0;
Muthén & Muthén, 1998-2012; Yu, 2002), Tucker-Lewis index (TLI; > .95; Tucker & Lewis,
1973), and comparative fit index (CFI; > .95; Bentler, 1990; Hu & Bentler, 1999).
The initial CFA specified a five-factor model with 5 items indicating the Terrorizing
factor, 3 items indicating the Spurning factor, 5 items indicating the Exploiting/Corrupting
factor, 2 items indicating the Isolating factor, and 6 items indicating the Denying Emotional
Responsiveness factor. Correlations were allowed among the five factors. Three CAMI PM items
(items 1, 5, and 13) that did not clearly fit into any of the APSAC theoretical categories were
allowed to load freely onto the factors. This model acceptable fit to the data, 2 (227, N = 490) =
790.73, p < .001; CFI = .97; TLI = .96; RMSEA = .07; WRMR = 1.23. In this model, the three
items allowed to load freely did not load onto any of the factors (factor loadings were low).
Examination of these three items revealed they were three of the four CAMI PM items that
comprised a factor identified by Nash et al. (2012; Demanding/Rigid) that was not one of the PM
subtypes in the APSAC (1995) definition of PM. Examination of the fourth item in Nash et al.’s
(2012) Demanding/Rigid factor, item 9, revealed adequate, although not optimal, factor loading
(.76) onto the Exploiting/Corrupting factor. Elimination of the four items determined by Nash et
al. (2012) to comprise the Demanding/Rigid factor resulted in a model with acceptable fit to the
data, 2 (160, N = 490) = 481.05, p < .001; CFI = .98; TLI = .98; RMSEA = .06; WRMR = 1.06,
and all factor loadings were substantial (>.72). Results of the CFA indicated the CAMI PM items
loaded adequately onto the PM subtypes as defined by APSAC (1995). Therefore, I determined
the CAMI PM accurately measured the APSAC (1995) model. Table 1 displays the standardized
factor loadings for the final model, which was used in subsequent analyses.
Person-Centered Analysis of Childhood Psychological Maltreatment
In order to identify naturally occurring groups of participants based on their exposure to
different subtypes of PM in childhood, I conducted a latent profile analysis (LPA) using MPlus
Version 7.3 (Muthén & Muthén, 1998-2012). LPA is a person-centered approach to analysis that
focuses on similarities and differences among individuals rather than variables (Berlin, Williams,
& Parra, 2014). LPA allows for simultaneous examination of multiple PM subtypes, accounting
20
for the complexity of PM experiences. LPA is a statistical approach that can be used to classify
individuals with similar patterns into unobserved groups (Berlin et al., 2014). Thus, in LPA a
person-centered categorical latent variable is derived. Participants are assigned to one mutually
exclusive profile based on their responses to observed variables of interest (i.e., PM variables;
Berlin et al., 2014; Hazen, Connelly, Roesch, Hough, & Landsverk, 2009).
The groups or latent profiles were determined using multiple indicators of model fit as
well as theoretical justification. Indicators of fit that were used included entropy (Ramaswamy,
DeSarbo, Reibstein, & Robinson, 1993), Akaike Information Criterion (AIC; Akaike, 1974;
1987), Bayesian Information Criteria (BIC; Schwarz, 1978), sample-size adjusted BIC (Sclove,
1987), Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMR; Lo, Mendell, & Rubin, 2001),
Vuong-Lo-Mendell-Rubin Likelihood Ratio Test (VLMR; Lo et al., 2001), and Bootstrap
Likelihood Ratio Test (BLRT; McLachlan & Peel 2000). Entropy assesses classification
accuracy and can range from 0 to 1. Higher scores indicate greater classification accuracy (i.e.,
the probability that a participant would be in one class versus another; Berlin et al., 2014). The
AIC, BIC, and sample-size adjusted BIC are measures of relative fit, which allow for comparison
of models with different numbers of classes. Lower values on these fit indices indicate better
model fit. LMR, VLMR, and BLRT are likelihood ratio tests that compare the estimated model
with k classes to a model with k – 1 classes. Significant p-values on these tests indicate that the
model with k classes reflects a statically significant improvement in fit than the model with k – 1
classes.
Maximum likelihood estimation with robust standard errors (i.e., MLR) was used. LPA
models were estimated using 100 initial stage random starts and 20 final stage optimizations to
determine if the best log-likelihood value was obtained and replicated. Additionally, 100
bootstrap draws with 100 random stage starts and 20 final stage optimizations were used for
BLRTs. Several models were fit to the data in a hierarchical fashion, beginning with specifying a
1-class model and adding classes hierarchically until adding an additional class no longer
resulted in improved model fit. Model fit indices are displayed in Table 2.
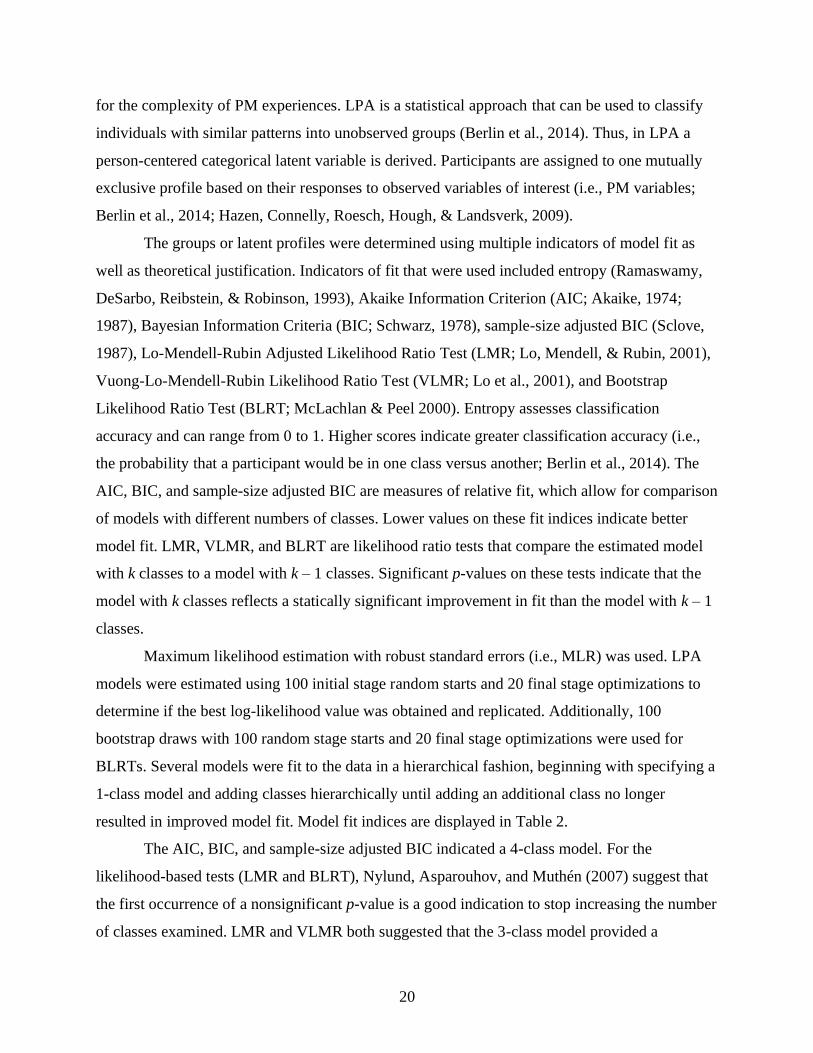
The AIC, BIC, and sample-size adjusted BIC indicated a 4-class model. For the
likelihood-based tests (LMR and BLRT), Nylund, Asparouhov, and Muthén (2007) suggest that
the first occurrence of a nonsignificant p-value is a good indication to stop increasing the number
of classes examined. LMR and VLMR both suggested that the 3-class model provided a

21
significantly better fit than the 2-class model, and that the 4-class model did not provide a
statistically significant improvement over the 3-class model. The BLRT, however, indicated that
a 3-class model provided a significantly better fit than the 2-class model and that the 4-class
model provided a significantly better fit than the 3-class model. While simulation studies suggest
that the BLRT outperforms other likelihood ratio tests, simulations with sample sizes similar to
the present sample size indicate similar performance of the BLRT and the LMR (Nylund et al.,
2007). Examination of the 4-class model indicated that two of the four classes each contained
less than 6% of the sample (n = 29 and n = 28). These two small classes comprised one class in
the 3-class model. Researchers have suggested that small classes (i.e., classes with 5% or less of
the total sample) are too small and potentially unstable for the purpose of comparisons (McCrae,
Chapman, & Christ, 2006; Pears, Kim, & Fisher, 2008). The best entropy value was for the 4-
class model. Given the relatively small number of members in two of the classes in the 4-class
model and that these two classes appeared to be subgroups of one of the classes in the 3-class
model, I chose the 3-class model as the best fitting model.
The patterns of PM experiences for the three latent classes are displayed in Table 3 and
Figure 1; 62.0% (n = 304) of the sample was classified into Class 1, 27.1% (n = 133) were
classified into Class 2, and 10.8% (n = 53) were classified into Class 3. As can be seen in Figure
1, Class 1 had a high probability of reporting low levels of childhood PM, across all five PM
subtypes. Class 2 had a high probability of reporting moderate levels of PM and Class 3 had a
high probability of endorsing high PM exposure, particularly for terrorizing, spurning, and
emotional nonresponsiveness. Thus, the three latent classes were labeled the low, moderate, and
high PM groups, based on the average PM exposure of the group members.
Examination of Characteristics of the Three PM Groups
A one-way MANOVA1 was conducted to examine whether the three PM groups differed
significantly on the five subtypes of PM (see Table 3 and Figure 1). Results revealed a statistically
significant difference between the groups on the combined dependent variables, Pillai’s Trace = .96,
F(10, 968) = 89.03, p < .001, ηp2 = .48. Follow up univariate one-way ANOVAs were conducted. A
Bonferroni adjustment was made such that statistical significance was accepted when p < .01. There
1. Analyses were run with demographic characteristics as control variables. A similar pattern of
results was found with and without demographic variables. Results for analyses without control
variables are presented.

22
were statistically significant differences in adjusted means for terrorizing, F(2, 487) = 788.38, p <
.001, ηp2 = .76, spurning, F(2, 487) = 750.97, p < .001, ηp2 = .76, exploiting/corrupting, F(2, 487) =
115.03, p < .001, ηp2 = .32, isolating, F(2, 487) = 188.24, p < .001, ηp2 = .44, and emotional
nonresponsiveness, F(2, 487) = 215.10, p < .001, ηp2 = .47. Games-Howell post hoc comparisons
were made for all three PM groups. Results indicated that the three groups were significantly
different from each other on all five subtypes of PM (see Table 3). The low PM group had the lowest
levels of PM, the high PM group had the highest levels of PM, and the moderate PM group fell in
between the low and high PM groups.
Demographic characteristics. One-way ANOVA and chi-square or Fisher’s exact tests
were used to examine demographic differences among the three PM groups (see Table 4).
Results revealed no significant differences in demographic characteristics between the groups.
Co-Occurrence of other types of child maltreatment. A one-way MANOVA was
conducted to examine whether the three PM groups differed significantly on the severity of other
types of child maltreatment (i.e., neglect, CPA, and CSA; Table 5). Results revealed a
statistically significant difference between the PM groups on the combined dependent variables,
Pillai’s Trace = .50, F(6, 934) = 52.22, p < .001, ηp2 = .25. Follow up univariate one-way
ANOVAs were conducted, and a Bonferroni adjustment was made such that statistical
significance was accepted when p < .0167. There were statistically significant differences in
adjusted means for neglect severity, F(2, 468) = 148.96, p < .001, ηp2 = .39, CPA severity, F(2,
468) = 59.93, p < .001, ηp2 = .20, and CSA severity, F(2, 468) = 43.01, p < .001, ηp2 = .16.
Games-Howell post hoc comparisons were made for all three child maltreatment variables.
Results indicated that the three classes were significantly different from each other on neglect,
CPA, and CSA severity such that the low PM group had the lowest severity and the high PM
group had the highest severity on these three other types of child maltreatment. Figure 2 displays
standardized neglect, CPA, and CSA severity scores for the three PM groups.
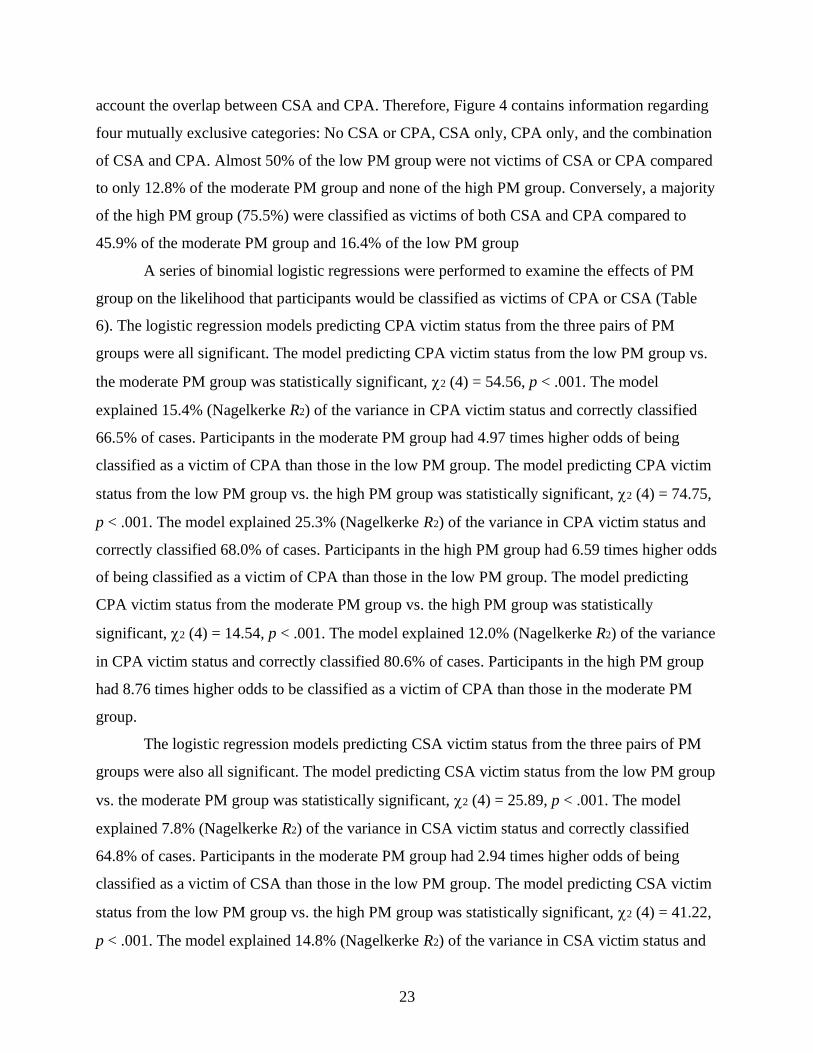
Figure 3 displays the percent of participants in each PM group categorized as victims of
CSA and CPA. Approximately one-third of the low PM group was categorized as CSA and CPA
victims. Over half of the participants in the moderate PM group were victims of CSA and
approximately three-fourths were victims of CPA. Of the participants in the high PM group,
almost 80% were victims of CSA and over 95% were victims of CPA. Figure 4 displays the
percent of participants in the PM groups categorized as CSA and/or CPA victims, taking into
23
account the overlap between CSA and CPA. Therefore, Figure 4 contains information regarding
four mutually exclusive categories: No CSA or CPA, CSA only, CPA only, and the combination
of CSA and CPA. Almost 50% of the low PM group were not victims of CSA or CPA compared
to only 12.8% of the moderate PM group and none of the high PM group. Conversely, a majority
of the high PM group (75.5%) were classified as victims of both CSA and CPA compared to
45.9% of the moderate PM group and 16.4% of the low PM group
A series of binomial logistic regressions were performed to examine the effects of PM
group on the likelihood that participants would be classified as victims of CPA or CSA (Table
6). The logistic regression models predicting CPA victim status from the three pairs of PM
groups were all significant. The model predicting CPA victim status from the low PM group vs.
the moderate PM group was statistically significant, 2 (4) = 54.56, p < .001. The model
explained 15.4% (Nagelkerke R2) of the variance in CPA victim status and correctly classified
66.5% of cases. Participants in the moderate PM group had 4.97 times higher odds of being
classified as a victim of CPA than those in the low PM group. The model predicting CPA victim
status from the low PM group vs. the high PM group was statistically significant, 2 (4) = 74.75,
p < .001. The model explained 25.3% (Nagelkerke R2) of the variance in CPA victim status and
correctly classified 68.0% of cases. Participants in the high PM group had 6.59 times higher odds
of being classified as a victim of CPA than those in the low PM group. The model predicting
CPA victim status from the moderate PM group vs. the high PM group was statistically
significant, 2 (4) = 14.54, p < .001. The model explained 12.0% (Nagelkerke R2) of the variance
in CPA victim status and correctly classified 80.6% of cases. Participants in the high PM group
had 8.76 times higher odds to be classified as a victim of CPA than those in the moderate PM
group.
The logistic regression models predicting CSA victim status from the three pairs of PM
groups were also all significant. The model predicting CSA victim status from the low PM group
vs. the moderate PM group was statistically significant, 2 (4) = 25.89, p < .001. The model
explained 7.8% (Nagelkerke R2) of the variance in CSA victim status and correctly classified
64.8% of cases. Participants in the moderate PM group had 2.94 times higher odds of being
classified as a victim of CSA than those in the low PM group. The model predicting CSA victim
status from the low PM group vs. the high PM group was statistically significant, 2 (4) = 41.22,
p < .001. The model explained 14.8% (Nagelkerke R2) of the variance in CSA victim status and

24
correctly classified 69.2% of cases. Participants in the high PM group had 2.81 times higher odds
of being classified as a victim of CSA than those in the low PM group. The model predicting
CSA victim status from the moderate PM group vs. the high PM group was statistically
significant, 2 (4) = 7.43, p < .001. The model explained 5.4% (Nagelkerke R2) of the variance in
CSA victim status and correctly classified 64.5% of cases. Participants in the high PM group had
2.69 times higher odds of being classified as a victim of CSA than those in the moderate PM
group.
Figures 5 and 6 depict descriptive characteristics of CSA and CPA experiences,
respectively, of participants in the three PM groups identified as CSA or CPA victims. For each
abuse characteristic, the most severe category was identified, and participants received a code (0
= absent, 1 = present) for each characteristic. Many of the CSA victims in the high PM group
were exposed to the most severe forms of CSA. For example, 66.7% were abused by a family
member, 71.4% experienced penetration, 64.3% were physically held down by their
perpetrator(s), and 45.2% were abused over ten times. Of CSA victims in the low and moderate
PM groups, 29.3% and 46.2% were abused by a family member, 55.6% and 66.7% experienced
penetration, 47.5% and 47.4% were physically held down by their perpetrator(s), and 21.2% and
32.1% were abused over ten times, respectively.
Examination of the characteristics of CPA experienced by participants in this sample
revealed that almost all of the participants in the three PM groups who were physically abused
reported they were abused by a parent (96.0% - 97.3%). Across PM groups, a majority of CPA
victims experienced at least two years of physical abuse (over 90% for the moderate and high
PM groups and almost 85% for the low PM group). Similar to the findings for CSA, many of the
CPA victims in the high PM group were exposed to the most severe forms of CPA. For example,
almost 95% of CPA victims in the high PM group were choked, beaten, or burned while
approximately 80% of the moderate PM group and 50% of the low PM group experienced this
type of abuse. In addition, over 20% of CPA victims in the high PM group were seriously injured
(e.g., bone fractures, burns, internal injuries, paralysis) while 7.1% of the moderate PM group
and less than 1% of the low PM group were seriously injured.
Intercorrelation of Variables
Table 7 contains bivariate correlations, means, and standard deviations for the continuous
outcome variables of adult psychological functioning for the entire sample (i.e., depression,

25
anxiety, problematic alcohol use, heavy episodic drinking, cannabis use frequency, nicotine use
frequency). All outcome variables were significantly correlated with each other. Table 8 contains
bivariate correlations between the continuous outcome variables and demographic
characteristics. Age was not significantly correlated with any of the outcome variables.
Identifying as White was significantly positively correlated with problematic alcohol use, heavy
episodic drinking, and nicotine use frequency. Identifying as African American was negatively
correlated with problematic alcohol use, heavy episodic drinking, nicotine use frequency, and
depression. Identifying as Latina was positively correlated with depression and anxiety.
Identifying as Native American was negatively correlated with heavy episodic drinking.
Identifying as another racial/ethnic identity was negatively correlated with problematic alcohol
use and heavy episodic drinking. Being a student was negatively correlated with all outcome
variables except anxiety. Having children was positively correlated with anxiety and nicotine use
frequency and negatively correlated with problematic alcohol use and heavy episodic drinking.
Depression and Anxiety
A one-way MANOVA was conducted to examine whether the three PM groups differed
significantly on symptoms of depression and anxiety. Results revealed a statistically significant
difference between the groups on the combined dependent variables, Pillai’s Trace = .12, F(4,
974) = 14.89, p < .001, ηp2 = .06. Follow up univariate one-way ANOVAs were conducted. A
Bonferroni adjustment was made such that statistical significance was accepted when p < .025.
There were statistically significant differences in adjusted means for symptoms of depression,
F(2, 487) = 19.55, p < .001, ηp2 = .07, and symptoms of anxiety, F(2, 487) = 29.98, p < .001, ηp2
= .11. Games-Howell post hoc comparisons were made for depression and anxiety. Results
indicated that symptoms of depression and anxiety were both significantly lower for the low PM
group compared to the moderate and high PM groups, but there was no significant difference
between the moderate and the high PM groups (see Table 9).
The association between the PM groups and symptoms of depression and anxiety were
also examined utilizing the categorical severity indicators for depression and anxiety. Using
previously defined cut-off scores (S. H. Lovibond & Lovibond, 1995), scores for depression and
anxiety were categorized as normal, mild to moderate, and severe to extremely severe.
Examination of depression severity scores for the full sample revealed 68.0% (n = 333) reported
symptoms in the normal range, 21.6% (n = 106) reported symptoms in the mild to moderate
26
range, and 10.4% (n = 51) reported symptoms in the severe to extremely severe range. For
symptoms of anxiety, 64.9% (n = 318) of the full sample reported anxiety in the normal range,
21.0% (n = 103) reported symptoms falling the mild to moderate range, and 14.1% (n = 69)
reported symptoms in the severe to extremely severe range. Chi-square tests of independence
were conducted between PM group and depression and anxiety scored categorically (Tables 10
and 11). For both analyses, all expected cell frequencies were greater than five. Results revealed
a statistically significant association between the PM groups and depression severity, 2(4) =
49.34, p < .001, and between the PM groups and anxiety severity, 2(4) = 45.04, p < .001,
although the associations were small (Cohen, 1988), Cramer’s V = .22 and .21, respectively. For
depression severity, examination of adjusted residuals indicated that participants in the low PM
group were more likely than expected to report symptoms of depression in the normal range. The
low PM group was more likely than expected to have participants with depression in the normal
range than the moderate and high PM groups. The moderate PM group was more likely than
expected to have participants who reported symptoms in the mild to moderate range. Finally, the
high PM group was more likely to have participants with symptoms in the severe to extremely
severe range. For anxiety, examination of adjusted residuals indicated that the low PM group was
more likely than expected to have participants who reported symptoms of anxiety in the normal
range and less likely to have participants with mild to moderate and severe to extremely severe
anxiety. On the other hand, the moderate and high PM groups were more likely than expected to
have participants with anxiety in the severe to extremely severe range.
Substance Use
Alcohol use. A one-way MANOVA was conducted to examine whether the three PM
groups differed significantly on problematic alcohol use and heavy episodic drinking. Results
revealed a statistically significant difference between the groups on the combined dependent
variables, Pillai’s Trace = .04, F(4, 974) = 4.63, p = .001, ηp2 = .02. Follow-up univariate one-
way ANOVAs were conducted, and a Bonferroni adjustment was made such that statistical
significance was accepted when p < .025. There were statistically significant differences in
adjusted means for problematic alcohol use, F(2, 487) = 8.21, p < .001, ηp2 = .03, and heavy
episodic drinking, F(2, 487) = 6.23, p = .002, ηp2 = .03 (Table 12). Games-Howell post hoc
comparisons indicated that problematic alcohol use scores were significantly different for the
low versus the moderate and high PM groups, such that the low PM group had lower problematic

27
alcohol use scores. Problematic alcohol use was not significant different for the moderate
compared to the high PM group. Heavy episodic drinking scores were significantly lower in the
low PM group compared to the high PM group, but were not significantly different for the low
versus the moderate or the moderate versus the high PM group.
A chi-square test of independence (Table 13) was conducted between the PM groups and
the AUDIT scored dichotomously based on the recommended cutoff ( 8) indicating the
presence or absence of problematic alcohol use. All expected cell frequencies were greater than
five. There was a statistically significant association between the PM groups and problematic
alcohol use, 2(2) = 8.96, p = .011. The association was small (Cohen, 1988), Cramer’s V = .14.
Results revealed that the low PM group was less likely than expected to have problematic
alcohol use, with only 17.5% of the low PM group obtaining AUDIT scores greater than or equal
to eight. A trend suggested that the moderate and high PM groups may have been more likely
than expected to report problematic alcohol use, although results did not reach statistical
significance.
Drug Use. A one-way MANOVA was conducted to examine whether the three PM
groups differed significantly on cannabis and nicotine use frequency in the past year. Results
revealed a statistically significant difference between the groups on the combined dependent
variables, Pillai’s Trace = .07, F(4, 974) = 8.69, p < .001, ηp2 = .03. Follow up univariate one-
way ANOVAs were conducted. A Bonferroni adjustment was made such that statistical
significance was accepted when p < .025. There were statistically significant differences in
adjusted means for cannabis use frequency, F(2, 487) = 6.72, p = .001, ηp2 = .03, and nicotine use
frequency, F(2, 487) = 16.96, p < .001, ηp2 = .07. Games-Howell post hoc comparisons were
made for cannabis and nicotine use frequency (see Table 14). The moderate PM group reported
significantly more frequent cannabis use than the low PM group. The high PM group did not
differ from the low or moderate PM groups; however, the pattern of results was in the expected
direction. In addition, Games-Howell is affected by group size and within group variance such
that power is the lowest for the smallest groups with the largest variance (Sauder & DeMars,
2019). Nicotine use frequency was significantly higher in the moderate and high PM groups
compared to the low PM group. While the difference between the moderate and high PM groups
on nicotine use did not reach statistical significance, the pattern was consistent with what one

28
would expect given previous research finding positive associations between PM and increased
tobacco or nicotine use (Duke, 2018; Hayre et al., 2019; Moran et al., 2004).
A chi-square test of independence was conducted between PM group and drug use
frequency scored categorically (see Table 15). One cell had expected count of less than five,
otherwise all expected cell frequencies were greater than five, which meets the statistical
assumption that at least 80% of cells have expected values of five or more (e.g., McHugh, 2013).
Results revealed a statistically significant association between PM group and drug use frequency
2(4) = 23.29, p < .001, although the strength of the association was small (Cohen, 1988),
Cramer’s V = .15. The low PM group was more likely than expected to report no drug use and
less likely to report moderate to high drug use in the past year. The moderate and high PM
groups were both less likely than expected to have no drug use in the past year and more likely to
have moderate to high drug use. Approximately 20% of the high PM group reported moderate to
high drug use compared to only 5.9% of the low PM group.
A chi-square test of independence was conducted between PM group and drug use
problems scored categorically (Table 16). All expected cell frequencies were greater than five.
There was a statistically significant association between PM group and drug use problems 2(4)
= 39.22, p < .001. The association was small (Cohen, 1988), Cramer’s V = .20. The low PM
group was more likely than expected to report no drug use problems in the past year and less
likely than expected to report any drug use problems (i.e., mild and moderate to high drug use
problems). The moderate and high PM groups were less likely than expected to report no drug
use problems and more likely to report moderate to high drug use problems. The moderate PM
group was also more likely to report mild drug use problems than expected. Approximately 80%
of the low PM group reported no drug use problems compared to 58.0% and 50.9% of the
moderate and high PM groups, respectively.
Controlling for Other Types of Child Maltreatment
Other types of child maltreatment were included in the models examining differences
between the three PM groups on different indicators of adult psychological functioning. Given
that the PM group variable was categorical, I chose to use CSA and CPA victim status as control
variables instead of using CSA and CPA severity scores. When CSA and CPA victim status were
included as control variables in the one-way MANCOVAs examining differences between PM

29
groups on the dependent variables, some group differences still emerged, but the magnitude of
the differences decreased.
The one-way MANCOVA with depression and anxiety as dependent variables revealed a
statistically significant difference between the PM groups on the combined dependent variables,
Pillai’s Trace = .05, F(4, 968) = 6.08, p < .001, ηp2 = .02. Follow up univariate one-way
ANOVAs with a Bonferroni adjustment revealed a significant difference among the PM groups
on depression, F(2, 484) = 5.27, p = .005, ηp2 = .02, and anxiety, F(2, 484) = 12.03, p < .001, ηp2
= .05 (see Table 17). Games-Howell post hoc comparisons indicated that the low PM group was
significantly different from the high PM group on depression. For anxiety, the low PM group
was significantly lower than the moderate and high PM group. There was also a statistically
significant difference between victims and nonvictims of both CSA, Pillai’s Trace = .05, F(2,
483) = 11.43, p < .001, ηp2 = .05, and CPA, Pillai’s Trace = .02, F(2, 483) = 3.63, p = .027, ηp2 =
.02, on the combined dependent variables (depression and anxiety). Results of follow up
univariate one-way ANOVAs with a Bonferroni adjustment revealed that being a victim of CSA
was associated with higher levels of depression, F(1, 484) = 14.30, p < .001, ηp2 = .03, and
anxiety, F(1, 484) = 21.75, p < .001, ηp2 = .04. Being a victim of CPA was associated with higher
levels of depression, F(1, 484) = 7.20, p = .008, ηp2 = .02, but not with anxiety, F(1, 484) = 2.20,
p = .139, ηp2 = .01.
The one-way MANCOVA with problematic alcohol use and heavy episodic drinking as
dependent variables revealed a statistically significant difference between the PM groups on the
combined alcohol use variables, Pillai’s Trace = .02, F(4, 968) = 2.56, p = .037, ηp2 = .01. Follow
up univariate one-way ANOVAs with a Bonferroni adjustment revealed a significant difference
among the PM groups on problematic alcohol use, F(2, 484) = 3.86, p = .022, ηp2 = .02, but
results of Games-Howell post hoc comparisons did not reach statistical significance (see Table
18). There was no significant difference among the PM groups on heavy episodic drinking, F(2,
484) = 3.63, p = .027, ηp2 = .02. In addition, CSA and CPA victim status were not significantly
associated with problematic alcohol use, Pillai’s Trace = .00, F(2, 483) = .54, p = .582, ηp2 = .00,
and Pillai’s Trace = .00, F(2, 483) = .71, p = .492, ηp2 = .00, respectively.
For cannabis and nicotine use frequency, results of the one-way MANCOVA controlling
for CSA and CPA victim status revealed a statistically significant difference between the PM
groups on the combined dependent variables, Pillai’s Trace = .03, F(4, 968) = 3.13, p = .014, ηp2

30
= .01. Table 23 displays results of follow up univariate one-way ANOVAs with a Bonferroni
adjustment. Results revealed a significant difference among the PM groups for nicotine use
frequency, F(2, 484) = 5.42, p = .005, ηp2 = .02, but no significant difference emerged among the
PM groups for cannabis use frequency, F(2, 484) = 2.70, p = .068, ηp2 = .01. Games-Howell post
hoc comparisons indicated there was a significant difference between the low and high PM
groups on nicotine use frequency, but not between the low and moderate or the moderate and
high PM groups. Results also indicated that being a victim of CSA was associated with greater
frequency of nicotine use, F(1, 484) = 10.75, p = .001, ηp2 = .02, but being a victim of CSA was
not associated with cannabis use frequency, F(1, 484) = 4.17, p = .04, ηp2 = .01. Being a victim
of CPA was not significantly associated with either nicotine use frequency, F(1, 484) = 4.42, p =
.036, ηp2 = .01, or cannabis use frequency, F(1, 484) = .67, p = .414, ηp2 = .00.
Discussion
The present study explored the natural co-occurrence of psychological maltreatment
subtypes experienced in childhood and associated indicators of adult psychological functioning
in a geographically diverse sample of young women. To my knowledge, this is the first study to
use a person-centered approach to examine the co-occurrence of PM subtypes. According to the
most widely used and agreed upon definition of PM outlined by APSAC (1995), PM consists of
five distinct subtypes: spurning, terrorizing, exploiting/corrupting, isolating, and denying
emotional responsiveness. Results of the CFA in the present study supported the use of the
CAMI PM scale to adequately measure the five PM subtypes based on the APSAC (1995)
model. Using a person-centered analysis, I explored the experiences of different PM subtypes
and severity levels reported by women in the current sample. Based on previous research
indicating differences in the rate and co-occurrence of PM subtypes (e.g., Baker & Ben-Ami,
2011; Taussig & Culhane, 2010; Trickett et al., 2009), I expected to find groups of participants
based on exposure to different PM subtypes and levels of severity. In contrast to hypotheses,
however, I found evidence of a unitary construct of PM that differed by severity of PM exposure,
but not by subtype of PM experienced. Results indicated the best fit for the data was a three-class
model, with the three latent classes reflecting exposure to low, moderate, and high PM severity
across subtypes such that the high PM group was exposed to severe spurning, terrorizing,
exploiting/corrupting, isolating, and denying emotional responsiveness. I did not find evidence of
different types of PM experiences, instead I found participants were exposed to different levels

31
of PM severity across all five subtypes. Therefore, differences between the PM groups on
indicators of adult psychological functioning were driven by differences in PM severity rather
than by exposure to different PM subtypes.
While previous studies have found evidence to suggest that different subtypes of PM
have different psychological effects (e.g., Allen, 2008; Brassard & Donovan, 2006; Shaffer et al.,
2009; White et al., 2016), the current results cannot be directly compared to these past studies
due to important methodological differences. First, no prior studies have used a person-centered
analysis to explore participants’ experiences of different subtypes of PM. In addition, the vast
majority of research on PM has failed to include all five PM subtypes. Research has tended to
focus on terrorizing and spurning, while neglecting other subtypes (Baker, 2009; Hamilton et al.,
2013; Potthast et al., 2014; Shin et al., 2015). Measures of PM have typically been combined into
a single PM variable (e.g., Dubowitz et al., 2016; Lewis et al., 2019), obscuring effects of any
specific PM subtype. Furthermore, researchers have often used dichotomous indicators of the
presence/absence of PM or PM subtypes (e.g., Taussig & Culhane, 2010; Trickett et al., 2009),
ignoring the fact that PM exists along a continuum of severity. As discussed earlier, many
researchers advocate for measuring the severity of child maltreatment exposure and this is
especially true for PM as it may be the most difficult form of maltreatment to dichotomize
(Clemmons et al., 2007; Litrownik et al., 2005; Newcomb & Locke, 2001; Wekerle, 2011). In
light of the current findings of PM groups based on severity across all subtypes, discussion of
results cannot address effects of specific PM subtypes.
Adult Psychological Functioning
Results of the present study are consistent with previous research finding that PM is
associated with decreased psychological functioning in adulthood (e.g., Hart et al., 1998; Miller-
Perrin et al., 2009; Norman et al., 2012; Spinazzola et al., 2014). Results generally suggest a
positive association between PM severity and psychological symptoms. Participants in the low
PM group tended to report the least distress while participants in the high PM group tended to
report the most distress and the most severe outcomes (i.e., more severe symptoms of depression
and anxiety, greater substance use, and more severe substance use problems).
Depression and anxiety. Results of the present study revealed significant differences in
symptoms of depression and anxiety between the PM groups. Using continuous severity scores
for depression and anxiety, results indicated that scores were significantly lower for the low PM

32
group compared to both the moderate and high PM groups. The low PM group reported very low
levels of depression and anxiety, with scores that have been categorized as falling in the normal
range, indicating that the scores are similar to the population mean (S. H. Lovibond & Lovibond,
1995). Depression and anxiety scores for the high PM group fall in the high end of the mild
range, suggesting symptoms are above the population mean but are mild compared to people
typically seeking treatment. The lack of significant differences between the moderate and high
groups on symptoms of depression and anxiety may have been due to a lack of power given the
small sample size and relatively small number of participants in the high PM group. The pattern
of results, which suggests a positive association between PM severity and symptoms of
depression and anxiety, is in the expected direction and is consistent with previous research (e.g.,
Crow et al., 2014; Norman et al., 2012; Spinazzola et al., 2014).
When the distribution of scores was maintained with the use of categorical indicators of
depression, a more nuanced picture emerged. Specifically, the high PM group reported more
severe to extremely severe depression than expected while the moderate group was more likely
to report mild to moderate depression. Comparison of the severity of depression and anxiety
symptoms obtained in the present study to those obtained in previous studies using the DASS
(Crawford & Henry, 2003; Wardenaar et al., 2018) indicates a larger percentage of participants
in the current sample reported any symptoms (mild and above) of depression and anxiety. In a
general population sample of adults in the UK, Crawford and Henry (2003) found that 18.3%
reported symptoms of depression that were at least mild and 11% reported anxiety that was in the
mild range or greater. Similarly, in a sample of almost 8,000 Dutch adults, 26.1% reported
depression in the mild range and above and 15.2% reported anxiety that was in the mild range or
greater (Wardenaar et al., 2018). The high PM group seems to stand out with regard to symptoms
of depression and anxiety as approximately 30% of participants in the high PM group reported
depression and anxiety in the severe to extremely severe range compared to rates of 5.8% and
7.2% for depression and 5.2% and 4.6% for anxiety reported by adults in Europe (Crawford &
Henry, 2003; Wardenaar et al., 2018, respectively). Examination of the frequencies of depression
scores obtained by participants in the current study suggests that more severe PM is associated
with more severe depression in almost a gradient of severity for some individuals. Current results
seem to support findings of Bifulco et al. (2002) who found that PM severity was associated with
chronic or recurrent major depression in a community sample of women. For anxiety, the

33
analysis using the categorical severity variable indicated that women in the moderate and high
PM groups reported more severe to extremely severe anxiety than expected. This finding may
suggest a threshold level of PM exposure (i.e., somewhere between moderate and severe PM) is
associated with an increased likelihood of severe anxiety in adulthood.
Substance use. Given the inconsistent findings regarding the relation between PM and
substance use in the literature, the current study sought to clarify this relation by examining
different PM subtypes and several substance use variables. In general, results for substance use
were largely consistent with previous studies that have found a positive association between PM
and substance use (e.g., Dube et al., 2002; Rosenkranz et al., 2012; Spinazzola et al., 2014;
Taillieu et al., 2016).
Alcohol use. With regard to alcohol use, participants in the moderate and high PM groups
reported more severe problematic drinking than those in the low PM group. Similarly, when
problematic alcohol use was scored dichotomously, participants in the low PM group were less
likely than expected to report problematic alcohol use. Although not reaching statistical
significance, trend-level results suggest the moderate and high PM groups may have been more
likely than expected to have participants with problematic alcohol use. For heavy episodic
drinking, participants in the high PM group reported engaging in heavy episodic drinking more
frequently in the past year than those in the low PM group. Interestingly, participants in the
moderate group did not differ significantly from those in either the low or high group. These
findings may be evidence for a threshold level of PM exposure above which women are at
increased risk for alcohol use problems in early adulthood. On the other hand, similar to the
findings for depression and anxiety, the lack of significant differences may be due to a lack of
power. The pattern of results does suggest that the severity of PM exposure is positively
associated with the severity of alcohol problems and the frequency of heavy episodic drinking.
This pattern is consistent with previous research demonstrating an association between alcohol
use or alcohol-related problems and PM severity (Potthast et al., 2015; Schwandt, Heilig,
Hommer, George, & Ramchandani, 2013).
Cannabis and nicotine use. Examination of the pattern of results for cannabis and
nicotine use suggests that more severe PM is associated with more frequent cannabis and
nicotine use. Although not all of the comparisons between groups reached statistical significance,
the pattern of results was in the expected direction based on previous research finding positive
34
associations between PM and cannabis use (Banducci, Felton, Bonn-Miller, & Lejuez, 2018;
Duke, 2018; Hayre et al., 2019) and tobacco or nicotine use (Duke, 2018; Hayre et al., 2019;
Moran et al., 2004). The ability to make direct comparisons across studies is limited, however,
as the majority of previous studies (e.g., Banducci et al., 2018; Duke, 2018; Hayre et al., 2019;
Moran et al., 2004) did not include all PM subtypes, instead they included only spurning and/or
terrorizing. In addition, previous studies have tended to use adolescent samples (Banducci et al.,
2018; Duke, 2018; Hayre et al., 2019; Moran et al., 2004) and dichotomous indicators of PM
exposure (Duke, 2018; Moran et al., 2004). One recent study by Dubowitz et al. (2016) found
contradicting evidence indicating that PM (i.e., terrorizing and spurning) was not associated with
adolescent marijuana use; however, all subtypes of PM were not included and measurement of
child maltreatment was based on CPS reports, which tend to underestimate the prevalence and
extent of PM exposure (Sedlak et al., 2010; Trickett et al., 2009). Thus, the pattern of results for
cannabis and nicotine use seems to be consistent with the majority of previous research, which
has revealed positive associations between PM and increased cannabis and nicotine use.
Drug use. The association between PM and drug use has been largely neglected in the
literature. The available literature suggests that PM is associated with increased drug use and
increased drug use problems. However, past studies have typically combined drug use with the
use of cannabis and other types of substances (e.g., alcohol, nicotine) to create a single substance
use frequency or problems variable (e.g., Moran et al., 2004; Rosenkranz et al., 2012; Taillieu et
al., 2016). In addition, a majority of previous research has used dichotomous variables for PM as
well as for drug use (Dube et al., 2003; Post et al., 2015; Taillieu et al., 2016). In the present
study, participants in the moderate and high PM groups were more likely than expected to report
moderate to high frequency of drug use other than cannabis in the past year (e.g., use of one drug
2-4 times per month to 4 or more times per week), while those in the low PM group were more
likely to report no drug use. Results suggest that exposure to moderate or high PM severity does
not increase risk of occasional or experimental drug use (e.g., use of one drug once in the past
year). In contrast, exposure to moderate or high PM does increase the chance of past year regular
or frequent drug use (i.e., use of three drugs one time each, use of one drug 2-4 times per month,
or multiple drugs four or more times per week). Examination of drug use problems revealed a
slightly different pattern of results. Participants in the low PM group were more likely than
expected to report no drug use problems. Those in the moderate PM group were more likely than

35
expected to report mild drug use problems and moderate to severe drug use problems. Finally,
participants in the high PM group were more likely than expected to report moderate to severe
drug use problems. These results suggest that the severity of PM exposure is positively
associated with the severity of drug use problems in early adulthood. Taken together, these
results suggest that exposure to moderate or high PM severity increases the risk of regular to
frequent drug use, which increases the risk of drug use problems; however, individuals with the
most severe PM are at increased risk of the most severe drug use problems.
Co-Occurrence of Other Types of Child Maltreatment
In the current study, PM did not occur in isolation, as the women who reported exposure
to PM also reported experiencing neglect, CSA, and CPA. Different types of child maltreatment
are highly correlated and frequently co-occur (Cecil et al., 2017; Dong et al., 2004; Higgins &
McCabe, 2000), that maltreated children frequently experience more than one type of
maltreatment (Cecil et al., 2017; Herrenkohl & Herrenkohl, 2009), and exposure to one type of
child maltreatment increases the likelihood of exposure to another type of maltreatment (Arata,
Langhinrichsen-Rohling, Bowers, & O’Brien, 2007; Finkelhor et al., 2009; Herrenkohl and
Herrenkohl, 2009; Higgins & McCabe, 2001). In the current study, a majority of participants in
the moderate and high PM groups were victims of CPA and/or CSA, which is consistent with
research finding that PM has a particularly high rate of co-occurrence with other types of child
maltreatment (Berzenski et al., 2019; Bifulco et al., 2002; Cicchetti & Rogosch, 2001; McGee et
al., 1997; Taillieu et al., 2016; Trickett et al., 2009). In addition, the likelihood of being a victim
of CPA and/or CSA increased from the low to the moderate to the high PM group. The relation
between PM and CPA was particularly noteworthy. The odds of being a victim of CPA increased
by 5 times from the low to the moderate group and over 8.5 times from the moderate to the high
group. The rate of CPA in the moderate and high PM groups supports previous research finding
a particularly high co-occurrence between PM and CPA (Claussen & Crittenden, 1991;
Crittenden et al., 1994; Dong et al., 2004; Hodgdon et al., 2018; McGee et al., 1997; Rice et al.,
2001). Thus, for the women in the current sample, as the severity of PM exposure increased, the
likelihood of experiencing CPA and/or CSA also increased.
In the present study, the increasing rate of CPA and CSA across PM groups corresponded
to a decrease in psychological functioning. This finding can be conceptualized as the effect of
cumulative abuse, in which the number of types of maltreatment that are experienced is

36
associated with worse mental health correlates (Cecil et al., 2017; Martin, Cromer, DePrince, &
Freyd, 2011; Scott-Storey, 2011). Researchers have found associations between the number of
different types of adverse or traumatic experiences and depression and/or anxiety (Arata,
Langhinrichsen-Rohling, Bowers, & O’Farrill-Swails, 2005; Bifulco et al., 2002; Chapman et al.,
2004; Edwards et al., 2003; Schilling, Aseltine, & Gore, 2007; Shin, McDonald, & Conley,
2018; Teicher, Tomoda, & Anderson, 2006), alcohol use and/or alcohol use problems (Dube et
al., 2002; Hughes et al., 2017), drug use and/or drug use problems (Dube et al., 2003; Hughes et
al., 2017; Scheidell et al., 2018; Schilling et al., 2007; Vilhena-Churchill & Goldstein, 2014),
trauma symptoms (Clemmons et al., 2007; Sundermann & DePrince, 2015), and emotion
dysregulation (Sundermann & DePrince, 2015; Vilhena-Churchill & Goldstein, 2014). Results of
the current study provide further support for the adverse effect of cumulative abuse on adult
psychological functioning.
In the current study, not only did the rate of exposure to other types of child maltreatment
increase across PM groups, the severity of neglect, CPA, and CSA also increased from the low to
the moderate to the high PM group. Given that results generally suggested a positive relation
between PM severity and negative outcome, results were largely consistent with literature
indicating that more severe child maltreatment is associated with decreased psychological
functioning (e.g., Chapman et al., 2004; Higgins, 2004; Norman et al., 2012). Participants in the
high PM group were exposed to the most severe PM as well as the most severe neglect, CPA,
and CSA compared to the moderate and low PM groups. The severity of CPA and CSA was
observed in the continuous severity scores and in the specific trauma characteristics (Figures 5
and 6). The characteristics of CPA and CSA experiences appeared to increase in severity as PM
severity increased from the low to the moderate to the high PM group. The relation between PM
group and the severity of neglect, CPA, and CSA in combination with the rate of CPA and CSA
exposure in the PM groups, suggests an association between maltreatment severity and
cumulative abuse or exposure to multiple types of child maltreatment. This pattern of results is
consistent with those found by Clemmens et al. (2007), who identified a positive association
between the number of child maltreatment types and more severe maltreatment.
Child maltreatment type versus severity. While some researchers have debated the
relative importance of specific child maltreatment experiences versus the number of types of
abuse experienced, others have posited that child maltreatment severity, regardless of
37
maltreatment type, best characterizes individuals’ experiences. Results of the present study
suggest child maltreatment severity may better capture experiences of maltreatment than
maltreatment type, providing support for the argument that child maltreatment types should be
assessed and analyzed as a unitary construct. Higgins (2004) explored whether maltreatment
experiences were best classified based on exposure to distinct types of maltreatment or a single,
overarching construct of child maltreatment. Higgins (2004) found evidence to suggest that
experiences of child maltreatment are better characterized by overall severity of maltreatment
experiences (low, moderate, and high) than by maltreatment type. In comparing results from the
current study to those reported by Higgins (2004), it is important to note several differences in
methodology. First, I did not include other types of child maltreatment in analyses aimed at
identifying underlying groups of participants (i.e., LPA). In addition, Higgins’ (2004) study did
not include PM subtypes and used cluster analysis rather than a person-centered approach to
characterize participants’ experiences. Several studies have used person-centered approaches
(i.e., latent class and latent profile analyses) and identified groups of participants based on child
maltreatment severity across maltreatment types (e.g., Cecil, Viding, Barker, Guiney, &
McCrory, 2014; Lin et al., 2016), although none have included PM subtypes. Lin et al. (2016)
used LPA to classify 256 Chinese children with oppositional defiant disorder into groups based
on exposure to emotional abuse (i.e., spurning), emotional neglect (i.e., terrorizing), and physical
abuse. In another study, Cecil and colleagues (2014) used LPA to categorize experiences of
participants from a community sample of high-risk adolescents and young adults based on
exposure to emotional (i.e., spurning), physical, and sexual abuse and physical and emotional
neglect (i.e., terrorizing). The results of both studies revealed three profiles of child maltreatment
reflecting exposure to low, moderate, and high maltreatment severity across maltreatment types.
While the aim of the present study was not to identify groups based on the severity of exposure
to different types of child maltreatment, results nonetheless appear to support past findings
indicating that people may be best classified based on the severity rather than type of
maltreatment exposure.
Isolating effects of PM. It is not clear what accounts for the differences in outcomes
between the PM groups due to the co-occurrence of other types of child maltreatment in the
current sample. The differences in adult psychological functioning may be due to the effect of
PM alone, the effect of another type of child maltreatment (i.e., neglect, CSA, or CPA), or the
38
effect of exposure to multiple types of maltreatment (i.e., cumulative abuse). One approach to
identifying which child maltreatment experience is contributing the most to negative outcomes is
to statistically control for other types of maltreatment in an attempt to isolate the unique effects
of a single maltreatment type. Researchers have pointed out that failure to consider other types of
child maltreatment can lead to an overestimation of the effects of one type of maltreatment
(Cecil et al., 2017; Thibodeau et al., 2017). In the present study, controlling for CSA and CPA
victim status attenuated, but did not eliminate, the effects of PM. In general, when controlling for
CSA and CPA, the magnitude of the difference between the PM groups on indicators of
psychological functioning decreased. For most substance-related variables (i.e., problematic
alcohol use, heavy episodic drinking, and cannabis use frequency), the previously significant
differences between the PM groups in the unadjusted model ceased to exist. This finding is in
contrast to those of previous studies, which found that PM continued to predict indicators of
problematic alcohol use after controlling for other types of child maltreatment (Mandavia et al.,
2016; Potthast et al., 2014; Rosenkranz et al., 2012; Shin et al., 2015; White et al., 2016). Few
studies have examined the effect of PM on cannabis use and the available research is
inconsistent. White et al. (2016) found that PM (based on official and self-reports) was not a
significant predictor of cannabis use for adolescents after controlling for demographic
characteristics and other types of maltreatment. Also using a sample of adolescents and official
reports for measures of child maltreatment, Dubowitz et al. (2016) found that maltreated youth
were more likely to report cannabis use than non-maltreated youth; however, PM did not predict
cannabis use above and beyond the effects of demographic characteristics and other types of
maltreatment. On the other hand, Scheidell et al. (2017) did find a significant effect of PM on
cannabis use. Scheidell et al. (2017) examined the longitudinal relations between self-reported
childhood trauma and later drug use. Controlling for sociodemographic characteristics and a
range of childhood traumas, PM predicted past year cannabis use in emerging adulthood, but
CPA, CSA, and neglect did not.
For depression and nicotine use frequency in the present study, after controlling for CSA
and CPA, the low and moderate PM groups were no longer significantly different from each
other and only the difference between the low and high PM group remained statistically
significant. These results suggest the effect of PM was attenuated after controlling for CSA and
CPA, but PM continued to contribute significantly to the model. Similarly, Taillieu et al. (2016)

39
found that exposure to PM was associated with an increased odds of major depression,
dysthymia, panic disorder, and generalized anxiety disorder in a large sample of US adults, and
these relations were attenuated after controlling for other experiences of child maltreatment.
Other studies have also found that PM predicts depression over and above the effects of other
types of child maltreatment (e.g., Bifulco et al., 2002; Gibb et al., 2007; White et al., 2016).
Several researchers have examined the effect of PM on the combination of depression and
anxiety and found that PM is a significant predictor over and above the effects of other types of
child maltreatment (Cecil et al., 2017; Spertus et al., 2003). With regard to nicotine use, studies
examining the relation between PM and nicotine use are scarce. However, the available literature
indicates that PM predicts nicotine/tobacco use after controlling for other maltreatment (Elliott et
al., 2014; White et al., 2016). For example, in a large sample of adults with nicotine dependence,
PM, CSA, and CPA predicted the persistence of nicotine dependence approximately three years
later, controlling for demographics, other adverse experiences, and other types of child
maltreatment (Elliott et al., 2014).
Overall, the current results suggest that even when accounting for exposure to CSA and
CPA, more severe PM tends to be associated with worse psychological functioning in early
adulthood. While the inclusion of CSA and CPA in the models decreased the magnitude of the
differences between PM groups, CSA and CPA victim status emerged as significantly associated
with only a few indicators of psychological functioning. Being a victim of CSA was significantly
associated with higher levels of depression, anxiety, and nicotine use. On the other hand, being a
victim of CPA was only significantly associated with higher levels of depressive symptoms,
which may be due to the fact that PM and CPA are highly co-occurring and conceptually
overlapping. While research has demonstrated an association between CPA and CSA and adult
psychological functioning (Amado, Arce, & Herraiz, 2015; Dube et al., 2005; Elliott et al., 2014;
Lindert et al., 2014; Mandavia et al., 2016), studies that have accounted for PM have tended to
find the effects of CSA and/or CPA are weaker in comparison to those of PM (e.g., Cecil et al.,
2017; Gibb et al., 2007; Infurna et al., 2015; White et al., 2016).
It has been suggested that PM may be the context within which all child maltreatment
occurs (Edwards et al., 2003). Some researchers have conceptualized PM as an indicator of
family environment and the background upon which other types of child maltreatment are
experienced (Edwards et al., 2003). While controlling for other types of child maltreatment

40
allows researchers to statistically isolate unique effects of PM, it may not be ecologically valid as
it may not reflect people’s actual experiences. Characteristics common among maltreating
families include a chaotic and unstable family system, anger, and conflict (Cicchetti &
Valentino, 2006). Hodgdon et al. (2018) suggested that PM is especially likely to occur with
non-responsive caregivers in a chaotic and unpredictable home environment. In a study
examining the differential effects of different types of maltreatment with a large sample of clinic-
referred youth, Hodgdon and colleagues (2018) found that youth with PM had experienced more
co-occurring trauma types, such as exposure to domestic violence, impaired caregiving, and
neglect, than youth with CSA or CPA without PM. In the present study, every participant in the
high PM group was a victim of CPA and/or CSA and three-fourths of participants in this group
were victims of both CPA and CSA. This finding supports the theory that PM may be the
environmental context within which child maltreatment occurs. Other researchers posit that PM
is an underlying component of all types of child maltreatment, and it may even be the driving
force or common factor accounting for the negative effects of all types of maltreatment (Binggeli
et al., 2001; Hart et al., 1998; Hart et al., 2011). Further, types of child maltreatment experienced
during a single incident of abuse are not mutually exclusive. Price-Robertson, Higgins, and
Vassallo (2013) noted that “some individual acts of violence against children involve multiple
forms of maltreatment” (p. 85). For example, a parent who hits their child (CPA) may also curse
at the child (spurning) and threaten to become increasingly violent if unrealistic expectations are
not met (terrorizing). Given several different conceptualizations of how PM may be inherently
intertwined in all child maltreatment experiences, statistically controlling for other maltreatment
types may be overly conservative, leading to an underestimation of the effect of PM.
Results of the current study suggest that participants, rarely, if ever, experienced PM in
the absence of other types of child maltreatment. Given the substantial co-occurrence among
child maltreatment types, we cannot conclude that PM alone is driving group differences in
outcome. In fact, when controlling for other types of child maltreatment, PM seemed to have
little effect outside the context of these other types of maltreatment. The present findings are
consistent with previous research indicating that PM rarely occurs in isolation (Arata et al., 2007;
Arata et al., 2005; Dong et al., 2004; Ney et al., 1994). However, other researchers have
identified individuals exposed to PM with no other maltreatment histories (e.g., Lewis et al.,
2019; Moran et al., 2004; Spinazzola et al., 2014). In the present sample, a PM only group does
41
not seem to exist. For the high PM group in particular, the different types of child maltreatment
appear to be occurring together. Comparison of the current study to studies that found
individuals who had only experienced PM reveals important differences in the study designs. In
contrast to the present study, which used a young adult sample of women, continuous measures
of PM, and all five APSAC (1995) subtypes of PM, previous studies were focused on youth,
used dichotomous measures of the presence/absence of PM, and included only partial definitions
of PM (Lewis et al., 2019; Moran et al., 2004; Spinazzola et al., 2014).
Perhaps increased psychological distress is not due to a single type of child maltreatment,
but rather the co-occurrence or combination of different types of maltreatment. For example,
Lewis et al. (2019) found that individuals who had experienced PM (i.e., denying emotional
responsiveness and spurning) plus physical and/or sexual abuse were more likely to smoke
cigarettes. PM alone did not predict smoking, nor did physical and/or sexual abuse alone. It was
the specific combination of PM and physical and/or sexual abuse that predicted smoking.
Researchers have found evidence of an interactive effect of PM with other types of child
maltreatment such that the impact of exposure to maltreatment is worsened in the context of PM
(Berzenski & Yates, 2011; Edwards et al., 2003; McGee et al., 1997; Spinazzola et al., 2014). In
a large sample of adult members of a health maintenance organization, Edwards et al. (2003)
found that the presence of PM (i.e., spurning) heightened the effect of child maltreatment (CPA,
CSA, and witnessing of maternal battering) on depression and anxiety. Similarly, Spinazzola et
al. (2014) found that the co-occurrence of PM with CSA or CPA was associated with greater
internalizing, externalizing, and PTSD symptoms compared to CSA or CPA alone in a large
national sample of clinic-referred youth. Using the same sample of youth, Hodgdon et al. (2018)
found there was something particularly potent about the combination of PM and CPA. Youth
with exposure to PM and CPA had the youngest age of abuse onset, the greatest proportion of
lifetime abuse exposure, and the highest number of co-occurring traumas compared to youth with
PM, CPA, or CSA alone or any other combination of maltreatment types (i.e., CSA and CPA,
PM and CSA). Thus, it may not be possible to determine whether PM alone is responsible for
group differences in outcomes in the current study. Pursuing these findings may even be
counterproductive as isolating individual types of child maltreatment may cease to reflect
children’s actual experiences.

42
Strengths and Limitations
Strengths of the present study lie within the novel approach to identifying maltreatment
groups based on the severity of PM subtypes (i.e., spurning, terrorizing, isolating,
exploiting/corrupting, denying emotional responsiveness) within a racially/ethnically and
geographically diverse community sample of women. However, findings should be interpreted
with consideration of several limitations. The current study’s sample was entirely female, over
half students, and relatively homogeneous in terms of age, which limits the generalizability of
results. Future research should include male and female participants given research finding
gender differences in the effects of PM (Banducci et al., 2018; Berzenski & Yates, 2011; Harper
& Arias, 2004; Hyman et al., 2006; Paul & Eckenrode, 2015; Taussig & Culhane, 2010). While
the current sample had some racial and ethnic diversity, African American and Latina
participants were underrepresented relative to national statistics (U.S. Census Bureau, 2019). In
addition, the sample size precluded examination of the effect of race on variables of interest.
Given past research finding racial/ethnic differences in the effect of child maltreatment on adult
mental health outcomes (e.g., Lee & Chen, 2017; Schilling et al. 2007), future studies with
larger, diverse samples are needed.
The assessment of PM and other types of child maltreatment was a considerable strength
of the current study. The PM scale of the CAMI (DiLillo et al., 2010) was created to reflect all
five major domains of the APSAC (1995) model. The CAMI also utilizes behaviorally specific
descriptions, which increase the reliability of reports. In a review of the literature, Hardt and
Rutter (2004) found that retrospective reports of details of childhood maltreatment experiences
and reports that required judgment or interpretation tended to be less reliable than those with
those with clearly defined definitions of maltreatment. Nonetheless, retrospective self-report
measures of child maltreatment are subject to retrospective recall and social desirability biases
and tend to produce underestimates of maltreatment experienced (Widom, 1989; Widom &
Morris, 1997; Widom & Shepard, 1996).
The measures used to assess substance use in the present study presented some
limitations. Cannabis and nicotine use were assessed with a single item. While this is standard in
the literature (e.g., Banducci et al., 2018), future research would benefit from using a more
comprehensive assessment. In addition, the drug use frequency and drug use problems scores
were highly skewed, so the two variables were transformed into ordinal scales to maintain the

43
general distribution of scores and increase ease of interpretation. The rate of past year drug use in
this sample was also quite low. Future research should use a larger sample or oversample for
higher levels of drug use.
The lack of specific, detailed information about the nature of the participants’
experiences of PM was a limitation of the current study. The CAMI PM does not assess for the
relationship to the perpetrator(s), number of perpetrators, age(s) of PM initiation and exposure,
or duration of the maltreatment. Researchers have found associations between specific trauma
characteristics and outcomes. Access to data on the specific trauma characteristics would have
allowed for a more complex understanding of the PM experiences and might have provided a
richer picture of the relation between PM and other types of child maltreatment. For example, the
moderate and high PM groups might have different from each other by factors such as the
number of abusive caretakers. Davis et al. (2019) identified latent classes based on child
maltreatment experiences and trauma characteristics in a sample of adolescents entering
substance use treatment. Davis and colleagues (2019) found that youth with the highest
probability of exposure to PM, CPA, and CSA also endorsed the highest rates of theoretically-
harmful trauma characteristics, such as being abused by a family member or other trusted
individual, experiencing abuse over a long period of time, and experiencing negative reactions
upon abuse disclosure. Some researchers have suggested that one reason PM may be so powerful
is that it tends to be associated with an earlier age of onset and a longer duration of exposure than
other types of child maltreatment. Hodgdon et al. (2018) examined specific trauma
characteristics within maltreatment groups and found that youth who experienced PM alone or in
combination with other types of maltreatment (i.e., CSA and CPA) had an earlier age of abuse
onset and a higher lifetime proportion of exposure compared to youth without PM. Age of abuse
onset, which often signifies duration or chronicity of maltreatment, may be a better predictor of
symptoms than other trauma characteristics (Sundermann & DePrince, 2015). Other research has
suggested that the relation between child maltreatment and outcomes may be more complex than
previously thought. Research indicates there are sensitive developmental periods during which
exposure to child maltreatment is particularly damaging (Teicher & Samson, 2016). For
example, Cowell et al. (2015) found that children who were maltreated during infancy
demonstrated worse inhibitory control and working memory performance than children
maltreated later in childhood. Research on the neurobiological effects of maltreatment have

44
demonstrated the importance of maltreatment type and the developmental timing of exposure.
For instance, Pechtel, Lyons-Ruth, Anderson, and Teicher (2014) examined amygdala volume as
this “stress-susceptible brain region” (Teicher & Samson, 2016, p. 243) may be particularly
sensitive to the effects of child maltreatment. Using a sample of adults with a history of child
maltreatment and healthy controls, Pechtel and colleagues (2014) found that the severity of child
maltreatment exposure at 10-11 years of age was the strongest predictor of greater right
amygdala volume, which is believed to be associated with self-referential processing of negative
emotional stimuli. Thus, future research should assess for the specific characteristics of PM as
this would allow for a more complex understanding of PM experiences and the associated long-
term effects.
Implications
The present findings have important implications for future research and clinical work. The
conceptualization of PM and the five primary subtypes as defined by the APSAC (1995) model (i.e.,
spurning, terrorizing, exploiting/corrupting, isolating, denying emotional responsiveness) is strongly
grounded in theory and supported by research (Brassard & Donovan, 2006). The APSAC (1995) model
was further supported by results from the current study; however, participants were best classified
based on the severity of all PM experiences and there was no evidence for PM groups based on the
specific subtype(s) of PM. This finding raises questions about the conceptualization of PM as a
multidimensional construct and suggests the distinction among subtypes may not translate into people’s
actual experiences. It is possible that distinct PM subtypes exist but tend to co-occur at similar levels of
severity. The highly traumatized nature of the present sample is noteworthy and suggests the
participants’ experiences of maltreatment may differ from that of the general population. Perhaps the
participants’ experience of PM speaks to the context within which the maltreatment occurred. For
example, once maltreatment has reached a certain level of severity, the PM subtypes might not occur
outside the context of one another.
Examination of previous research providing evidence of differences in rates across PM subtypes
reveals the sample and measurement of PM subtypes differed from those in the current study. Past
research was largely based on samples of children (e.g., de la Vega et al., 2011; Taussig & Culhane,
2010; Trickett et al., 2009) and unlike the current study, did not utilize self-report measures of PM.
Instead, past studies used official case records (Taussig & Culhane, 2010; Trickett et al., 2009) or an
interview with the participant’s mother (de la Vega et al., 2011). The present study’s use of self-report

45
measures might have impacted results as it may be difficult for adults to retrospectively recall and
differentiate exposure to specific PM subtypes in childhood. While the CAMI PM was designed to be a
behaviorally specific measure, PM is much more difficult to quantify than other forms of maltreatment,
especially compared to those consisting of acts of commission that tend to cause immediate and visible
harm (Barnett et al., 2011; Wekerle, 2011). In addition, PM subtypes are not entirely mutually
exclusive as a single parenting behavior could fit the definition of more than one PM subtype (Perrin-
Miller & Perrin, 2007). For example, locking a child in a closet, which is a form of isolating, could be
considered terrorizing if it induces extreme fear and/or involves an element of threat and it could also
be considered a form of denying emotional responsiveness when it is done without expressed affection
and the child’s cries are ignored. Given evidence supporting the APSAC (1995) model of PM and
multiple explanations for the present findings, results should not be interpreted as evidence that PM is a
unidimensional construct without further research.
Results of the current study suggest a close connection between PM and other types of
child maltreatment. Participants who reported the most severe PM also reported high levels of
exposure to neglect, CSA, and CPA. On the other hand, participants who reported minimal
exposure to PM experienced relatively low levels of other types of child maltreatment. In an
attempt to better understand the relation between PM and other types of child maltreatment,
future research should explore whether it is possible to experience other types of maltreatment
without PM. For decades researchers have proposed that PM may be embedded within all other
types of child maltreatment (Binggeli et al., 2001; Hart et al., 1998; Hart et al., 2011). Therefore,
future research should attempt to determine precisely how PM relates to other types of
maltreatment.
The present findings also provide support for utilizing continuous measures of PM rather
than dichotomous indicators of PM exposure. If PM had been dichotomized in the present study,
participants in the moderate PM group would have been grouped with either the low or high PM
group, which would have obscured a more nuanced understanding of the impact of PM. In future
research on PM, it will be important to use consistent definitions and reliable measurements that
assess all PM subtypes according to the APSAC (1995) model. The sixth subtype of PM defined
by APSAC (1995), mental health, medical, and educational neglect, should be considered for
inclusion in future research as this subtype has received minimal research attention to date (e.g.,
Binggeli et al., 2001; Brassard & Donovan, 2006; Hart et al., 1998). In addition, future research
46
should determine whether witnessing intimate partner violence should be included as an aspect
of PM. While witnessing intimate partner violence is not explicitly included in the APSAC
(1995) definition, some researchers have conceptualized it as a subtype of PM (Kairys &
Johnson, 2002) and others have identified witnessing intimate partner violence as a form of
terrorizing and corrupting (Somer & Braunstein, 1999). In addition, some CPS definitions of
emotional maltreatment include witnessing intimate partner violence (Sedlak et al., 2010).
Results of the current study highlight the importance of assessing exposure to PM
regardless of exposure to other types of child maltreatment. Results suggest a positive
association between PM severity and decreased psychological functioning in early adulthood,
and this association remained for several outcomes even when controlling for other types of child
maltreatment. Thorough assessment and early identification of PM may provide the opportunity
for earlier intervention and perhaps the prevention of other types of child maltreatment. Previous
research has found that PM is associated with an earlier age of onset than other types of child
maltreatment (e.g., Hodgdon et al., 2018), suggesting PM may be a precursor and an early
indication of later exposure to other types of maltreatment. Clinicians working with children
experiencing PM may want to regularly assess and monitor for exposure to other types of
maltreatment. For participants in the current study, we do not know whether their exposure to
PM predated their exposure to other types of maltreatment. However, participants with the most
severe PM reported extremely high rates of CSA and CPA, suggesting individuals exposed to
severe PM may be more likely to experience other types of child maltreatment as well.
It is important that clinicians are aware of the breadth of PM experiences that can occur
as many aspects of PM do not fit into commonly known definitions of emotional or verbal abuse
and emotional neglect. The current results suggest that if a child or adolescent is experiencing
one subtype of PM, it is likely they are also experiencing other subtypes. Some researchers have
suggested that interventions for PM would be more effective if they targeted specific subtypes of
PM (Brassard & Hardy, 1997; Glaser, 2002; 2011). Results of the current study do not appear to
support this assertion as participants reported exposure to all PM subtypes at similar levels.
However, this finding does not eliminate the possibility that a particular PM subtype could result
in different outcomes for different people.
Finally, researchers have been calling for increased attention on PM by CPS agencies
(English et al., 2015) as CPS records grossly underestimate the rate of PM (Schneider et al.,

47
2005; Sedlak et al., 2010). Trickett et al. (2009) examined CPS records of 303 adolescents with
substantiated child maltreatment and found that almost half of the adolescents had experienced
PM, although less than 10% were identified as having experienced PM at the time they were
referred to CPS. Hodgdon and colleagues (2018) suggested that the adverse effects of PM are
made worse by disagreement and confusion about how to define, assess, and intervene in cases
of PM. CPS agencies across the country would be better equipped to identify cases of PM with
clearly defined criteria for PM exposure. Accurate and consistent identification of PM by CPS
agencies would improve if researchers defined a threshold level of severity at which poor
parenting becomes PM and children are placed at increased risk for negative outcomes.
Conclusion
Psychological maltreatment is associated with devasting, long-lasting effects (Berzenski
& Yates, 2011; Binggeli et al., 2001; Ney et al., 1994), yet it is the least studied form of child
maltreatment (Barnett et al., 2005; Finkelhor et al., 2005; Hart & Glaser, 2011). In the current
study, PM was associated with decreases in adult psychological functioning as evidenced by
differences between the low, moderate, and high PM severity groups on symptoms of depression
and anxiety, substance use, and substance-related problems. Furthermore, this association
remained for some outcomes even when controlling for other types of child maltreatment, which
were highly co-occurrent with participants’ experiences of PM. The current study also provided
further support for the APSAC (1995) model of PM with PM subtypes existing as distinct
constructs, even though the young women in this sample experienced all subtypes at similar
levels. Despite evidence that a range of parenting behaviors can be considered psychological
maltreatment, different subtypes of PM are rarely assessed (Paul & Eckenrode, 2015; White et
al., 2016). Researchers need to come to a consensus on the definition and conceptualization of
PM, which includes determining whether PM is a separate type of child maltreatment or an
inherent part of all other types of maltreatment. These perspectives are not mutually exclusive.
PM can both constitute a distinct type of maltreatment that can occur independent of other types
of maltreatment and reflect core contextual elements found in all types of child maltreatment. As
a core component of all types of child maltreatment, it is essential that we continue to develop
our understanding of all forms of PM.

48
References
Akaike, H. (1974). A new look at the statistical model identification. IEEE Transactions on
Automatic Control, 19, 716-723. doi:10.1109/TAC.1974.1100705
Akaike, H. (1987). Factor analysis and AIC. Psychometrika, 52, 317-332. doi:10.1007/BF02294359
Allen, B. (2008). An analysis of the impact of diverse forms of childhood psychological
maltreatment on emotional adjustment in early adulthood. Child Maltreatment, 13, 307-
312. doi:10.1177/1077559508318394
Amado, B. G., Arce, R., & Herraiz, A. (2015). Psychological injury in victims of child sexual
abuse: A meta-analytic review. Psychosocial Intervention, 24, 49-62.
doi:10.1016/j.psi.2015.03.002
American Professional Society on the Abuse of Children (APSAC; 1995). Guidelines for
psychosocial evaluation of suspected psychological maltreatment in children and
adolescents. Chicago: Author.
Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., & O’Brien, N. (2007). Differential
correlates of multi-type maltreatment among urban youth. Child Abuse & Neglect, 31,
393-415. doi:10.1016/j.chiabu.2006.09.006
Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., & O’Farrill-Swails, L. (2005). Single
versus multi-type maltreatment: An examination of the long-term effects of child abuse.
Journal of Aggression, Maltreatment & Trauma, 11, 29-52. doi:10.1300/J146v11n04
Armour, C., Elklit, A., & Christoffersen, M. N. (2014). A latent class analysis of childhood
maltreatment: Identifying abuse typologies. Journal of Loss and Trauma, 19, 23-39.
doi:10.1080/15325024.2012.734205
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). AUDIT. The
Alcohol Use Disorders Identification Test: Guidelines for use in primary health care (2nd
ed.). Geneva, Switzerland: World Health Organization.
Baker, A. J. L. (2009). Adult recall of childhood psychological maltreatment: Definitional
strategies and challenges. Children and Youth Services Review, 31, 703-714.
doi:10.1016/j.childyouth.2009.03.001
Baker, A. J. L., & Ben-Ami, N. (2011). Adult recall of childhood psychological maltreatment in
“adult children of divorce”: Prevalence and associations with concurrent measures of well-

49
being. Journal of Divorce & Remarriage, 52, 203-219.
doi:10.1080/10502556.2011.556973
Baker, A. J. L., & Verrocchio, M. C. (2015). Parental bonding and parental alienation as
correlates of psychological maltreatment in adults in intact and non-intact families.
Journal of Child and Family Studies, 24, 3047-3057. doi:10.1007/s10826-014-0108-0
Banducci, A. N., Felton, J. W., Bonn-Miller, M. O., & Lejuez, C. W. (2018). An examination of
the impact of childhood emotional abuse and gender on cannabis use trajectories among
community youth. Translational Issues in Psychological Science, 4, 85-98.
doi:10.1037/tps0000142
Banducci, A. N., Hoffman, E. M., Lejuez, C. W., & Koenen, K. C. (2014). The impact of
childhood abuse on inpatient substance users: Specific links with risky sex, aggression,
and emotion dysregulation. Child Abuse & Neglect, 38, 928-938.
doi:10.1016/j.chiabu.2013.12.007
Barnett, O. W., Miller-Perrin, C. L., & Perrin, R. D. (2005). Family violence across the lifespan:
An introduction (2nd ed.). Thousand Oaks, CA: Sage.
Barnett, O. W., Miller-Perrin, C. L., & Perrin, R. D. (2011). Family violence across the lifespan:
An introduction (3rd ed.). Thousand Oaks, CA: Sage.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107,
238-246. doi:10.1037/0033-2909.107.2.238
Berlin, K. S., Williams, N. A., & Parra, G. R. (2014). An introduction to latent variable mixture
modeling (Part 1): Overview and cross-sectional latent class and latent profile
analyses. Journal of Pediatric Psychology, 39, 174-187. doi:10.1093/jpepsy/jst084
Bernstein, D. P., & Fink, L. (1998). Childhood Trauma Questionnaire: A retrospective self-
report manual. New York: The Psychological Corporation.
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., Ahluvalia, T., Stokes, J.,
Handelsman, L., Medrano, M., Desmond, D., & Zule, W. (2003). Development and
validation of a brief screening version of the Childhood Trauma Questionnaire. Child
Abuse & Neglect, 27, 169-190. doi:10.1016/S0145-2134(02)00541-0
Berzenski, S. R., Madden, A. R., & Yates, T. M. (2019). Childhood emotional abuse
characteristics moderate associations with adult psychopathology and caregiving. Child
Abuse & Neglect, 87, 77-87. doi:10.1016/j.chiabu.2018.06.004

50
Berzenski, S. R., & Yates, T. M. (2011). Classes and consequences of multiple maltreatment: A
person-centered analysis. Child Maltreatment, 16, 250-261.
doi:10.1177/1077559511428353
Bifulco, A., Moran, P. M., Baines, R., Bunn, A., & Stanford, K. (2002). Exploring psychological
abuse in childhood: II. Association with other abuse and adult clinical depression.
Bulletin of the Menninger Clinic, 66, 241-258. doi:10.1521/bumc.66.3.241.23366
Binggeli, N. J., Hart, S. N., & Brassard, M. R. (2001). Psychological maltreatment of children:
The APSAC study guides 4. Thousand Oaks, CA: Sage.
Brassard, M. R., & Donovan, K. L. (2006). Defining psychological maltreatment. In M. M.
Feerick, J. F. Knutson, P. K. Trickett, & S. M. Flanzer (Eds.), Child abuse and neglect:
Definitions, classifications, & a framework for research (pp. 151-197). Baltimore, MD:
Paul H. Brookes.
Brassard, M. R., & Hardy, D. D. (1997). Psychological maltreatment. In M. Helfer, R. Kempe, &
R. Krugman (Eds.), The battered child (pp. 392-412). Chicago, IL: University of Chicago
Press.
Briere, J., & Runtz, M. (1988). Multivariate correlates of childhood psychological and physical
maltreatment among university women. Child Abuse & Neglect, 12, 331-341.
doi:10.1016/0145-2134(88)90046-4
Cecil, C. A. M., Viding, E., Barker, E. D., Guiney, J., & McCrory, E. J. (2014). Double
disadvantage: The influence of childhood maltreatment and community violence
exposure on adolescent mental health. Journal of Child Psychology and Psychiatry and
Allied Disciplines, 55, 839-848. doi:10.1111/jcpp.12213
Cecil, C. A. M., Viding, E., Fearon, P., Glaser, D., & McCrory, E. J. (2017). Disentangling the
mental health impact of childhood abuse and neglect. Child Abuse & Neglect, 63, 106-
119. doi:10.1016/j.chiabu.2016.11.024
Chapman, D. P., Whitfield, C. L., Felitti, V. J., Dube, S. R., Edwards, V. J., & Anda, R. F.
(2004). Adverse childhood experiences and the risk of depressive disorders in adulthood.
Journal of Affective Disorders, 82, 217-225. doi:10.1016/j.jad.2003.12.013
Child Abuse Prevention and Treatment Act. (1974). Pub. L. No. 93-247, 42. U.S.C. 5101, sec. 3.

51
Cicchetti, D., & Rogosch, F. A. (2001). The impact of child maltreatment and psychopathology
on neuroendocrine functioning. Development and Psychopathology, 13, 783-804.
doi:10.1017/S0954579401004035
Cicchetti, D., & Valentino, K. (2006). An ecological-transactional perspective on child
maltreatment: Failure of the average expectable environment and its influence on child
development. In D. Cicchetti & D. Cohen (Eds.), Handbook of developmental
psychopathology (2nd ed., Vol. 1, pp. 129-201). Hoboken, NJ: Wiley.
Claussen, A. H., & Crittenden, P. M. (1991). Physical and psychological maltreatment: Relations
among types of maltreatment. Child Abuse & Neglect, 15, 5–18. doi:10.1016/0145-
2134(91)90085-R
Clemmons, J. C., Walsh, K., DiLillo, D., & Messman-Moore, T. L. (2007). Unique and
combined contributions of multiple child abuse types and abuse severity to adult trauma
symptomatology. Child Maltreatment, 12, 172-181. doi:10.1177/1077559506298248
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ:
Lawrence Erlbaum Associates.
Cowell, R. A., Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2015). Childhood maltreatment and
its effect on neurocognitive functioning: Timing and chronicity matter. Development and
Psychopathology, 27, 521-533. doi:10.1017/S0954579415000139
Crawford, J. R., & Henry, J. D. (2003). The Depression Anxiety Stress Scales (DASS):
Normative data and latent structure in a large non-clinical sample. British Journal of
Clinical Psychology, 42, 111-131. doi:10.1348/014466503321903544
Crawford, E., & Wright, M. O. (2007). The impact of childhood psychological maltreatment on
interpersonal schemas and subsequent experiences of relationship aggression. Journal of
Emotional Abuse, 7, 93-116. doi:10.1300/J135v07n02_06
Crittenden, P. M. (1992). Children’s strategies for coping with adverse home environments: An
interpretation using attachment theory. Child Abuse and Neglect, 16, 329-343.
doi:10.1016/0145-2134(92)90043-Q
Crittenden, P. M., Claussen, A. H., & Sugarman, D. B. (1994). Physical and psychological
maltreatment in middle childhood and adolescence. Development and Psychopathology,
6, 145-164. doi:10.1017/S0954579400005927

52
Crow, T., Cross, D., Powers, A., & Bradley, B. (2014). Emotion dysregulation as a mediator
between childhood emotional abuse and current depression in a low-income African
American sample. Child Abuse & Neglect, 38, 1590-1598.
doi:10.1016/j.chiabu.2014.05.015
Davis, J. P., Dworkin, E. R., Helton, J., Prindle, J., Patel, S., Dumas, T. M., & Miller, S. (2019).
Extending poly-victimization theory: Differential effects of adolescents’ experiences of
victimization on substance use disorder diagnoses upon treatment entry. Child Abuse &
Neglect, 89, 165-177. doi:10.1016/j.chiabu.2019.01.009
de la Vega, A., de la Osa, N., Ezpeleta, L., Granero, R., & Domènech, J. M. (2011). Differential
effects of psychological maltreatment on children of mothers exposed to intimate partner
violence. Child Abuse & Neglect, 35, 524-531. doi:10.1016/j.chiabu.2011.03.006
DiLillo, D. (2003). The Computer Assisted Maltreatment Inventory (CAMI). Unpublished
measure.
DiLillo, D., Hayes-Skelton, S. A., Fortier, M. A., Perry, A. R., Evans, S. E., Messman-Moore, T.
L., Walsh, K., Nash, C. & Fauchier, A. (2010). Development and initial psychometric
properties of the Computer Assisted Maltreatment Inventory (CAMI): A comprehensive
self-report measure of child maltreatment history. Child Abuse & Neglect, 34, 305-317.
doi:10.1016/j.chiabu.2009.09.015
DiLillo, D., Peugh, J., Walsh, K., Panuzio, J., Trask, E., & Evans, S. (2009). Child maltreatment
history among newlywed couples: A longitudinal study of marital outcomes and
mediating pathways. Journal of Consulting and Clinical Psychology, 77, 680-692.
doi:10.1037/a0015708
Dong, M., Anda, R. F., Felitti, V. J., Dube, S. R., Williamson, D. F., Thompson, T. J., Loo, C.
M., & Giles, W. H. (2004). The interrelatedness of multiple forms of childhood abuse,
neglect, and household dysfunction. Child Abuse & Neglect, 28, 771-784.
doi:10.1016/j.chiabu.2004.01.008
Dube, S. R., Anda, R. F., Felitti, V. J., Edwards, V. J., & Croft, J. B. (2002). Adverse childhood
experiences and personal alcohol abuse as an adult. Addictive Behaviors, 27, 713-725.
doi:10.1016/S0306-4603(01)00204-0
Dube, S. R., Anda, R. F., Whitfield, C. L., Brown, D. W., Felitti, V. J., Dong, M., & Giles, W. H.
(2005). Long-term consequences of childhood sexual abuse by gender of victim.

53
American Journal of Preventive Medicine, 28, 430-438.
doi:10.1016/j.amepre.2005.01.015
Dube, S. R., Felitti, V. J., Dong, M., Chapman, D. P., Giles, W. H., & Anda, R. F. (2003).
Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The
Adverse Childhood Experiences Study. Pediatrics, 111, 564-572.
doi:10.1542/peds.111.3.564
Dubowitz, H., Thompson, R., Arria, A. M., English, D., Metzger, R., & Kotch, J. B. (2016).
Characteristics of child maltreatment and adolescent marijuana use: A prospective study.
Child Maltreatment, 21, 16-25. doi:10.1177/1077559515620853
Duke, N. N. (2018). Adolescent adversity and concurrent tobacco, alcohol, and marijuana use.
American Journal of Health Behavior, 42(5), 85-99. doi:10.5993/AJHB.42.5.8
Edwards, V. J., Holden, G. W., Felitti, V. J., & Anda, R. F. (2003). Relationship between
multiple forms of childhood maltreatment and adult mental health in community
respondents: Results from the Adverse Childhood Experiences Study. American Journal
of Psychiatry, 160, 1453-1460. doi:10.1176/appi.ajp.160.8.1453
Egeland, B., & Sroufe, L. A. (1981). Developmental sequelae of maltreatment in infancy. New
Directions for Child Development, 11, 77-92. doi:10.1002/cd.23219811106
Egeland, B., Sroufe, L. A., & Erickson, M. (1983). The developmental consequence of different
patterns of maltreatment. Child Abuse & Neglect, 7, 459-469. doi:10.1016/0145-
2134(83)90053-4
Elliott, J. C., Stohl, M., Wall, M. M., Keyes, K. M., Goodwin, R. D., Skodol, A. E., Krueger, R.
F., Grant, B. F., & Hasin, D. S. (2014). The risk for persistent adult alcohol and nicotine
dependence: The role of childhood maltreatment. Addiction, 109, 842-850.
doi:10.1111/add.12477
English, D., Thompson, R., White, C. R., & Wilson, D. (2015). Why should child welfare pay
more attention to emotional maltreatment? Children and Youth Services Review, 50, 53-
63. doi:10.1016/j.childyouth.2015.01.010
Finkelhor, D., Ormrod, R. K., Turner, H. A., & Hamby, S. L. (2005). The victimization of
children and youth: A comprehensive, national survey. Child Maltreatment, 10, 5-25.
doi:10.1177/1077559504271287

54
Finkelhor, D., Turner, H., Ormrod, R., & Hamby, S. L. (2009). Violence, abuse, and crime
exposure in a national sample of children and youth. Pediatrics, 124, 1411-1423.
doi:10.1542/peds.2009-0467
Games, P. A., & Howell, J. F. (1976). Pairwise multiple comparison procedures with unequal
N’s and/or variances: A Monte Carlo study. Journal of Educational Statistics, 1, 113-125.
doi:10.2307/1164979
Garbarino, J., & Vondra, J. (1987). Psychological maltreatment: Issues and perspectives. In M.
R. Brassard, R. Germain, & S. N. Hart (Eds.), Psychological maltreatment of children
and youth (pp. 24-44). New York, NY: Pergamon Press.
Gibb, B. E., Chelminski, I., & Zimmerman, M. (2007). Childhood emotional, physical, and
sexual abuse and diagnoses of depressive and anxiety disorders in adult psychiatric
outpatients. Depression and Anxiety, 24, 256-263. doi:10.1002/da.20238
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment): A conceptual
framework. Child Abuse & Neglect, 26, 697-714. doi:10.1016/S0145-2134(02)00342-3
Glaser, D. (2011). How to deal with emotional abuse and neglect – Further development of a
conceptual framework (FRAMEA). Child Abuse & Neglect, 25, 866-875.
doi:10.1016/j.chiabu.2011.08.002
Graham, J. W. (2009). Missing data analysis: Making it work in the real world. Annual Review of
Psychology, 60, 549-576. doi:10.1146/annurev.psych.58.110405.085530
Greenfield, E. A., & Marks, N. F. (2010). Identifying experiences of physical and psychological
violence in childhood that jeopardize mental health in adulthood. Child Abuse & Neglect,
34, 161-171. doi:10.1016/j.chiabu.2009.08.012
doi:10.1016/j.comppsych.2008.04.005
Gross, A. B., & Keller, H. R. (1992). Long-term consequences of childhood physical and
psychological maltreatment. Aggressive Behavior, 18, 171-185. doi:10.1002/1098-
2337(1992)18:3<171::AID-AB2480180302>3.0.CO;2-I
Hamilton, J. L., Shapero, B. G., Stange, J. P., Hamlat, E. J., Abramson, L. Y., & Alloy, L. B.
(2013). Emotional maltreatment, peer victimization, and depressive versus anxiety
symptoms during adolescence: Hopelessness as a mediator. Journal of Clinical Child &
Adolescent Psychology, 42, 332-347. doi:10.1080/15374416.2013.777916

55
Harper, F. W. K., & Arias, I. (2004). The role of shame in predicting adult anger and depressive
symptoms among victims of child psychological maltreatment. Journal of Family
Violence, 19, 367-375. doi:10.1007/s10896-004-0681-x
Hart, S. N., Binggeli, N. J., & Brassard, M. R. (1998). Evidence for the effects of psychological
maltreatment. Journal of Emotional Abuse, 1, 27-58. doi:10.1300/J135v01n01_03
Hart, S. N., & Brassard, M. R. (1987). A major threat to children’s mental health: Psychological
maltreatment. American Psychologist, 42, 160-165. doi:10.1037/0003-066X.42.2.160
Hart, S. N., Brassard, M.R., Davidson H. A., Rivelis, E., Diaz, V., & Binggeli, N. J. (2011).
Psychological maltreatment. In J. E. B. Myers (Ed.), The APSAC handbook on child
maltreatment (3rd ed., pp. 125-144). Thousand Oaks, CA: Sage.
Hart, S. N., Brassard, M. R., Binggeli, N. J., & Davidson, H. A. (2002). Psychological
maltreatment. In J. E. B. Myers, L. Berliner, J. Briere, C. T. Hendrix, C. Jenny, & T. A.
Reid (Eds.), The APSAC handbook on child maltreatment (2nd ed., pp. 79-103).
Thousand Oaks, CA: Sage.
Hart, S. N., Germain, R. B., & Brassard, M. (1987). The challenge: To better understand and
combat psychological maltreatment of children and youth. In M. R. Brassard, R.
Germain, & S. N. Hart (Eds.), Psychological maltreatment of children and youth (pp. 3-
24). New York, NY: Pergamon.
Hart, S. N., & Glaser, D. (2011). Psychological maltreatment - Maltreatment of the mind: A
catalyst for advancing child protection toward proactive primary prevention and
promotion of personal well-being. Child Abuse & Neglect, 35, 758-766.
doi:10.1016/j.chiabu.2011.06.002
Hayre, R. S., Goulter, N., & Moretti, M. M. (2019). Maltreatment, attachment, and substance use
in adolescence: Direct and indirect pathways. Addictive Behaviors, 90, 196-203.
doi:10.1016/j.addbeh.2018.10.049
Hazen, A. L., Connelly, C. D., Roesch, S. C., Hough, R. L., & Landsverk, J. A. (2009). Child
maltreatment profiles and adjustment problems in high-risk adolescents. Journal of
Interpersonal Violence, 24, 361–378. doi:10.1177/0886260508316476
Henry, J. D., & Crawford, J. R. (2005). The short-form version of the Depression Anxiety Stress
Scales (DASS-21): Construct validity and normative data in a large non-clinical sample.
British Journal of Clinical Psychology, 44, 227-239. doi:10.1348/014466505X29657

56
Herrenkohl, R. C., & Herrenkohl, T. I. (2009). Assessing a child’s experience of multiple
maltreatment types: Some unfinished business. Journal of Family Violence, 24, 485-496.
doi:10.1007/s10896-009-9247-2
Hien, D.A., & First, M. (1991). Drug use questionnaire. Unpublished scale, Columbia College of
Physicians and Surgeons, New York State Psychiatric Institute, New York, New York.
Higgins, D. J. (2004). The importance of degree versus type of maltreatment: A cluster analysis
of child abuse types. Journal of Psychology, 138, 303-324. doi:10.3200/JRLP.138.4.303-
324
Higgins, D. J., & McCabe, M. P. (2001). The development of the Comprehensive Child
Maltreatment Scale. Journal of Family Studies, 7, 7-28. doi:10.5172/jfs.7.1.7
Hodgdon, H. B., Spinazzola, J., Briggs, E. C., Liang, L.-J., Steinberg, A. M., & Layne, C. M.
(2018). Maltreatment type, exposure characteristics, and mental health outcomes among
clinic referred trauma-exposed youth. Child Abuse & Neglect, 82, 12-22.
doi:10.1016/j.chiabu.2018.05.021
Hu, L.-T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure
analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6,
1-55. doi:10.1080/10705519909540118
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., Jones, L., &
Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: A
systematic review and meta-analysis. Lancet Public Health, 2, e356–e366.
doi:10.1016/S2468-2667(17)30118-4
Hyman, S. M., Garcia, M., & Sinha, R. (2006). Gender specific associations between types of
childhood maltreatment and the onset, escalation and severity of substance use in cocaine
dependent adults. The American Journal of Drugs and Alcohol Abuse, 32, 655-664.
doi:10.1080/10623320600919193
Infurna, M. R., Reichl, C., Parzer, P., Schimmenti, A., Bifulco, A., & Kaess, M. (2016).
Associations between depression and specific childhood experiences of abuse and
neglect: A meta-analysis. Journal of Affective Disorders, 190, 47-55.
doi:10.1016/j.jad.2015.09.006

57
Kairys, S. W., Johnson, C. F., & Committee on Child Abuse and Neglect. (2002). The
psychological maltreatment of children - Technical Report. Pediatrics, 109, e68-e72.
doi:10.1542/peds.109.4.e68
Kim, J., Mennen, F. E., & Trickett, P. K. (2016). Patterns and correlates of co-occurrence among
multiple types of child maltreatment. Child & Family Social Work, 22, 492-502.
doi:10.1111/cfs.12268
Lee, R. D., & Chen, J. (2017). Adverse childhood experiences, mental health, and excessive
alcohol use: Examination of race/ethnicity and sex differences. Child Abuse & Neglect,
69, 40-48. doi:10.1016/j.chiabu.2017.04.004
Lewis, T., Kotch, J., Proctor, L., Thompson, R., English, D., Smith, J., Zolotor, A., Block, S., &
Dubowitz, H. (2019). The role of emotional abuse in youth smoking. American Journal
of Preventive Medicine, 56, 93-99. doi:10.1016/j.amepre.2018.08.020
Lindert, J., von Ehrenstein, O. S., Grashow, R., Gal, G., Braehler, E., & Weisskopf, M. G.
(2014). Sexual and physical abuse in childhood is associated with depression and anxiety
over the life course: Systematic review and meta-analysis. International Journal of
Public Health, 59, 359-372. doi:10.1007/s00038-013-0519-5
Lin, X., Li, L., Chi, P., Wang, Z., Heath, M. A., Du, H., & Fang, X. (2016). Child maltreatment
and interpersonal relationship among Chinese children with oppositional defiant disorder.
Child Abuse & Neglect, 51, 192-202. doi:10.1016/j.chiabu.2015.10.013
Litrownik, A. J., Lau, A., English, D. J., Briggs, E., Newton, R. R., Romney, S., & Dubowitz, H.
(2005). Measuring the severity of child maltreatment. Child Abuse & Neglect, 29, 553-
573. doi:10.1016/j.chiabu.2003.08.010
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing
values. Journal of the American Statistical Association, 83, 1198-1202.
doi:10.2307/2290157
Little, R. J., & Rubin, D. B. (1987). Statistical analysis with missing data (Vol. 4). New York:
Wiley.
Lo, Y, Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal
mixture. Biometrika, 88, 767-778. doi:10.1093/biomet/88.3.767

58
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states:
Comparison of the depression anxiety stress scales (DASS) with the Beck Depression and
Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343. doi:10.1016/0005-
7967(94)00075-U
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the Depression Anxiety & Stress Scales.
(2nd ed.). Sydney: Psychological Foundation.
Mandavia, A., Robinson, G. G. N., Bradley, B., Ressler, K. J., & Powers, A. (2016). Exposure to
childhood abuse and later substance use: Indirect effects of emotion dysregulation and
exposure to trauma. Journal of Traumatic Stress, 29, 422-429. doi:10.1002/jts
Martin, C. G., Cromer, L. D., DePrince, A. P., & Freyd, J. J. (2013). The role of cumulative
trauma, betrayal, and appraisals in understanding trauma symptomatology. Psychological
Trauma, 52, 110-118. doi:10.1037/a0025686
Martins, C. M., Von Werne Baes, C., Tofoli, S. M., & Juruena, M. F. (2014). Emotional abuse in
childhood is a differential factor for the development of depression in adults. Journal of
Nervous and Mental Disorders, 202, 774-782. doi:10.1097/NMD.0000000000000202
McCrae, J. S., Chapman, M. V., & Christ, S. L. (2006). Profiles of children investigated for
sexual abuse: Association with psychopathology symptoms and services. American
Journal of Orthopsychiatry, 76, 468-481. doi:10.1037/0002-9432.76.4.468
McGee, R. A., & Wolfe, D. A. (1991). Psychological maltreatment: Toward an operational
definition. Development and Psychopathology, 3, 3-18.
doi:10.1017/S0954579400005034
McGee, R. A., Wolfe, D. A., & Wilson, S. K. (1997). Multiple maltreatment experiences and
adolescent behavior problems: Adolescents’ perspectives. Development and
Psychopathology, 9, 131-149. doi:10.1017/S0954579497001107
McHugh, M. L. (2013). The chi-square test of independence. Biochemia Medica, 23, 143-149.
doi:10.11613/bm.2013.018
McLachlan, G., & Peel, D. (2000). Finite mixture models. New York, NY: Wiley.
Mezquita, L., Ibáñez, M. I., Moya, J., Villa, H., & Ortet, G. (2014). A longitudinal examination
of different etiological pathways to alcohol use and misuse. Alcoholism: Clinical and
Experimental Research, 38, 1770-1779. doi:10.1111/acer.12419

59
Miller-Perrin, C. L., Perrin, R. D., & Kocur, J. L. (2009). Parental physical and psychological
aggression: Psychological symptoms in young adults. Child Abuse & Neglect, 33, 1-11.
doi:10.1016/j.chiabu.2008.12.001
Moran, P. B., Vuchinich, S., & Hall, N. K. (2004). Associations between types of maltreatment
and substance use during adolescence. Child Abuse & Neglect, 28, 565–574.
doi:10.1016/j.chiabu.2003.12.002
Muthén, L. K., & Muthén, B. O. (1998-2012). Mplus user’s guide (7th ed.). Los Angeles, CA:
Muthén & Muthén.
Nash, C. L., Hayes-Skelton, S. A., & DiLillo, D. (2012). Reliability and factor structure of the
psychological maltreatment and neglect scales of the Computer Assisted Maltreatment
Inventory (CAMI). Journal of Aggression, Maltreatment & Trauma, 21, 583-607.
doi:10.1080/10926771.2012.680574
Navarre, E. L. (1987). Psychological maltreatment: The core component of child abuse. In M. R.
Brassard, R. Germaine, & S. N. Hart (Eds.), Psychological maltreatment of children and
youth (pp. 45-88). New York, NY: Pergamon Press.
Nelson, J., Klumparendt, A., Doebler, P., & Ehring, T. (2017). Childhood maltreatment and
characteristics of adult depression: Meta-analysis. British Journal of Psychiatry, 210, 96-
104. doi:10.1192/bjp.bp.115.180752
Newcomb, M. D., & Locke, T. F. (2001). Intergenerational cycle of maltreatment: A popular
concept obscured by methodological limitations. Child Abuse & Neglect, 25, 1219-1240.
doi:10.1016/S0145-2134(01)00267-8
Ney, P. G., Fung, T., & Wickett, A. R. (1994). The worst combinations of child abuse and
neglect. Child Abuse & Neglect, 18, 705-714. doi:10.1016/0145-2134(94)00037-9
Norman, R. E., Byambaa, M., De, R., Butchart, A., Scott, J., & Vos, T. (2012). The long-term
health consequences of child physical abuse, emotional abuse, and neglect: A systematic
review and meta-analysis. PLOS Medicine, 9. doi:10.1371/journal.pmed.1001349
Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in
latent class analysis and growth mixture modeling: A Monte Carlo simulation study.
Structural Equation Modeling, 14, 535-569. doi:10.1080/10705510701575396
O’Hagan, K. P. (1995). Emotional and psychological abuse: Problems of definition. Child Abuse
& Neglect, 19, 449-461. doi:10.1016/0145-2134(95)00006-T

60
Olson, C. L. (1974). Comparative robustness of six tests in multivariate analysis of variance.
Journal of the American Statistical Association, 69, 894-908.
doi:10.1080/01621459.1974.10480224
Paul, E., & Eckenrode, J. (2015). Childhood psychological maltreatment subtypes and adolescent
depressive symptoms. Child Abuse & Neglect, 47, 38-47. doi:10.1016/j.chiabu.2015.05.018
Pears, K. C., Kim, H. K., & Fisher, P. A. (2008). Psychosocial and cognitive functioning of
children with specific profiles of maltreatment. Child Abuse & Neglect, 32, 958-971.
doi:10.1016/j.chiabu.2007.12.009
Pechtel, P., Lyons-Ruth, K., Anderson, C. M., & Teicher, M. H. (2014). Sensitive periods of
amygdala development: The role of maltreatment in preadolescence. NeuroImage, 97,
236-244. doi:10.1016/j.neuroimage.2014.04.025
Perrin-Miller, C. L., & Perrin, R. D. (2007). Child maltreatment: An introduction (2nd ed.).
Thousand Oaks, CA: Sage.
Pillai, S., & Jayachandran, K. (1967). Power comparisons of tests of two multivariate hypotheses
based on four criteria. Biometrika, 54, 195-210. doi:10.2307/2333863
Post, R. M., Altshuler, L. L., Kupka, R., Mcelroy, S. L., Frye, M. A., Rowe, M., Leverich, G. S.,
Grunze, H., Suppes, T., Keck, P. E. Jr., & Nolen, W. A. (2015). Verbal abuse, like
physical and sexual abuse, in childhood is associated with an earlier onset and more
difficult course of bipolar disorder. Bipolar Disorders, 17, 323-330.
doi:10.1111/bdi.12268
Potthast, N., Neuner, F., & Catani, C. (2014). The contribution of emotional maltreatment to
alcohol dependence in a treatment-seeking sample. Addictive Behaviors, 39, 949-958.
doi:10.1016/j.addbeh.2014.01.015
Price-Robertson, R., Higgins, D., & Vassallo, S. (2013). Multi-type maltreatment and
polyvictimization: A comparison of two research frameworks. Family Matters, 93, 84-98.
Retrieved from https://aifs.gov.au/publications/family-matters
Ramaswamy, V., DeSarbo, W. S., Reibstein, D. J., & Robinson, W. T. (1993). An empirical
pooling approach for estimating marketing mix elasticities with PIMS data. Marketing
Science, 12, 103-124. doi: 10.1287/mksc.12.1.103

61
Rice, C., Mohr, C. D., Del Boca, F. K., Mattson, M. E., Young, L., Brady, K., & Nickless, C.
(2001). Self-reports of physical, sexual and emotional abuse in an alcoholism treatment
sample. Journal of Studies on Alcohol, 62, 114-123. doi:10.15288/jsa.2001.62.114
Rohner, R. P., & Rohner, E. C. (1980). Antecedents and consequences of parental rejection: A
theory of emotional abuse. Child Abuse & Neglect, 4, 189-198. doi:10.1016/0145-
2134(80)90007-1
Rosenkranz, S. E., Muller, R. T., & Henderson, J. L. (2012). Psychological maltreatment in
relation to substance use problem severity among youth. Child Abuse & Neglect, 36, 438-
448. doi:10.1016/j.chiabu.2012.01.005
Sanders, B., & Becker-Lausen, E. (1995). The measurement of psychological maltreatment:
Early data on the Child Abuse and Trauma Scale. Child Abuse & Neglect, 19, 315-323.
doi:10.1016/S0145-2134(94)00131-6
Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R., & Grant, M. (1993).
Development of the alcohol use disorders identification test (AUDIT): WHO
collaborative project on early detection of persons with harmful alcohol consumption: II.
Addiction, 88, 791-804. doi:10.1111/j .13600443.1993.tb02093.x
Scheidell, J. D., Quinn, K., McGorray, S. P., Frueh, B. C., Beharie, N. N., Cottler, L. B., &
Khan, M. R. (2017). Childhood traumatic experiences and the association with marijuana
and cocaine use in adolescence through adulthood. Addiction, 113, 44-56.
doi:10.1111/add.13921
Schilling, E. A., Aseltine, R. H., Jr., & Gore, S. (2007). Adverse childhood experiences and
mental health in young adults: A longitudinal survey. BMC Public Health, 7, 7-30.
doi:10.1186/1471-2458-7-30
Schneider, M. W., Ross, A., Graham, J. C., & Zielinski, A. (2005). Do allegations of emotional
maltreatment predict developmental outcomes beyond that of other forms of
maltreatment? Child Abuse & Neglect, 29, 513-532. doi:10.1016/j.chiabu.2004.08.010
Schwarz, G. (1978). Estimating the dimension of a model. The Annals of Statistics, 6, 461-464.
doi:10.1214/aos/1176344136
Schwandt, M. L., Heilig, M., Hommer, D. W., George, D. T., & Ramchandani, V. A. (2013).
Childhood trauma exposure and alcohol dependence severity in adulthood: Mediation by
62
emotional abuse severity and neuroticism. Alcoholism: Clinical and Experimental
Research, 37, 984-992. doi:10.1111/acer.12053
Sclove, S. L. (1987). Application of model-selection criteria to some problems in multivariate
analysis. Psychometrika, 52, 333-343. doi:10.1007/BF02294360
Scott-Storey, K. (2011). Cumulative abuse: Do things add up? An evaluation of the
conceptualization, operationalization, and methodological approaches in the study of the
phenomenon of cumulative abuse. Trauma, Violence, & Abuse, 12, 135-150.
doi:10.1177/1524838011404253
Sedlak, A. J., Mettenburg, J., Basena, M., Petta, I., McPherson, K., Greene, A., & Li, S. (2010).
Fourth national incidence study of child abuse and neglect (NIS-4). Washington, DC:
U.S. Department of Health and Human Services, Administration for Children and
Families.
Shaffer, A., Yates, T. M., & Egeland, B. R. (2009). The relation of emotional maltreatment to
early adolescent competence: Developmental processes in a prospective study. Child
Abuse & Neglect, 33, 36-44. doi:10.1016/j.chiabu.2008.12.005
Shin, S. H., Lee, S., Jeon, S.-M., & Wills, T. A. (2015). Childhood emotional abuse, negative
emotion-driven impulsivity, and alcohol use in young adulthood. Child Abuse &
Neglect, 50, 94-103. doi:10.1016/j.chiabu.2015.02.010
Shin, S. H., McDonald, S. E., & Conley, D. (2018). Patterns of adverse childhood experiences
and substance use among young adults: A latent class analysis. Addictive Behaviors, 78,
187-192. doi:10.1016/j.addbeh.2017.11.020
Shingala, M. C., & Rajyaguru, A. (2015). Comparison of post hoc tests for unequal variance.
International Journal of New Technologies in Science and Engineering, 2(5), 22-23.
https://www.ijntse.com/
Sinclair, S. J., Siefert, C. J., Slavin-Mulford, J. M., Stein, M. B., Renna, M., & Blais, M. A.
(2012). Psychometric evaluation and normative data for the Depression, Anxiety, and
Stress Scales-21 (DASS-21) in a nonclinical sample of U.S. adults. Evaluation & the
Health Professions, 35, 259-279. doi:10.1177/0163278711424282
Somer, E., & Braunstein, A. (1999). Are children exposed to interparental violence being
psychologically maltreated? Aggression and Violent Behavior, 4, 449-456.
doi:10.1016/S1359-1789(98)00023-8
63
Spertus, I. L., Yehuda, R., Wong, C. M., Halligan, S., & Seremetis, S. V. (2003). Childhood
emotional abuse and neglect as predictors of psychological and physical symptoms in
women presenting to a primary care practice. Child Abuse & Neglect, 27, 1247-1258.
doi:10.1016/j.chiabu.2003.05.001
Spinazzola, J., Hodgdon, H., Liang, L. J., Ford, J. D., Layne, C. M., Pynoos, R., Briggs, E. C.,
Stolbach, B., & Kisiel, C. (2014). Unseen wounds: The contribution of psychological
maltreatment to child and adolescent mental health and risk outcomes. Psychological
Trauma: Theory, Research, Practice, and Policy, 6(Suppl 1), S18-S28.
doi:10.1037/a0037766
Steiger, J. H., & Lind, J. C. (1980, June). Statistically based tests for the number of common
factors. Paper presented at the Psychometric Society annual meeting, Iowa City, IA.
Straus, M. A., & Field, C. J. (2003). Psychological aggression by American parents: National
data on prevalence, chronicity, and severity. Journal of Marriage and Family, 65, 795-
808. doi:10.1111/j.1741-3737.2003.00795.x
Stuewig, J., & McCloskey, L. A. (2005). The relation of child maltreatment to shame and guilt
among adolescents: Psychological routes to depression and delinquency. Child
Maltreatment, 10, 324-336. doi:10.1177/1077559505279308
Sundermann, J. M., & DePrince, A. P. (2015). Maltreatment characteristics and emotion
regulation (ER) difficulties as predictors of mental health symptoms : Results from a
community-recruited sample of female adolescents. Journal of Family Violence, 30, 329-
338. doi:10.1007/s10896-014-9656-8
Taha, F., Galea, S., Hien, D., & Goodwin, R. D. (2014). Childhood maltreatment and the
persistence of smoking: A longitudinal study among adults in the US. Child Abuse &
Neglect, 38, 1995-2006. doi:10.1016/j.chiabu.2014.10.022
Taillieu, T. L., Brownridge, D. A., Sareen, J., & Afifi, T. O. (2016). Childhood emotional
maltreatment and mental disorders: Results from a nationally representative adult sample
from the United States. Child Abuse & Neglect, 59, 1-12.
doi:10.1016/j.chiabu.2016.07.005
Taussig, H. N., & Culhane, S. E. (2010). Emotional maltreatment and psychosocial functioning
in preadolescent youth placed in out-of-home care. Journal of Aggression, Maltreatment
& Trauma, 19, 52-74. doi:10.1080/10926770903476008

64
Teicher, M. H., & Samson, J. A. (2016). Annual research review: Enduring neurobiological
effects of childhood abuse and neglect. Journal of Child Psychology and Psychiatry, 57,
241-266. doi:10.1111/jcpp.12507
Teicher, M. H., Tomoda, A., & Andersen, S. L. (2006). Neurobiological consequences of early
stress and childhood maltreatment: Are results from human and animal studies
comparable? Annals of the New York Academy of Sciences, 1071, 313-323.
doi:10.1196/annals.1364.024
Thibodeau, M.-E., Lavoie, F., Hébert, M., & Blais, M. (2017). Childhood maltreatment and
adolescent sexual risk behaviors: Unique, cumulative and interactive effects. Child Abuse
& Neglect, 72, 411-420. doi:10.1016/j.chiabu.2017.09.002
Trickett, P. K., Mennen, F. E., Kim, K., & Sang, J. (2009). Emotional abuse in a sample of
multiply maltreated, urban young adolescents: Issues of definition and identification.
Child Abuse & Neglect, 33, 27-35. doi:10.1016/j.chiabu.2008.12.003
Tucker, L. R., & Lewis, C. (1973). A reliability coefficient for maximum likelihood factor
analysis. Psychometrika, 38, 1-10. doi:10.1007/BF02291170
U.S. Department of Health and Human Services, Administration for Children and Families,
Administration on Children, Youth, and Families, Children’s Bureau. (2019). Child
maltreatment 2017. http://www.acf.hhs.gov/cb/research-data-technology/statistics-
research/child-maltreatment
U.S. Census Bureau. (2019). QuickFacts: United States. http://www.census.gov/quickfacts/fact/
table/us/PST045219#
Vilhena-Churchill, N., & Goldstein, A. L. (2014). Maltreatment and marijuana problems in
young adults: Examining the role of motives and emotion dysregulation. Child Abuse &
Neglect, 38, 962-972. doi:10.1016/j.chiabu.2013.10.009
Wardenaar, K. J., Wanders, R. B. K., Jeronimus, B. F., & de Jonge, P. (2018). The psychometric
properties of an internet-administered version of the Depression Anxiety and Stress
Scales (DASS) in a sample of Dutch adults. Journal of Psychopathology and Behavioral
Assessment, 40, 318-333. doi:10.1007/s10862-017-9626-6
Watkins, L. E., Maldonado, R. C., & DiLillo, D. (2014). Hazardous alcohol use and intimate
partner aggression among dating couples: The role of impulse control
difficulties. Aggressive Behavior, 40, 369-381. doi:10.1002/ab.21528

65
Wekerle, C. (2011). Emotionally maltreated: The under-current of impairment? Child Abuse &
Neglect, 35, 899-903. doi:10.1016/j.chiabu.2011.09.002
White, C. R., English, D., Thompson, R., & Roberts, Y. H. (2016). Youth self-report of
emotional maltreatment: Concordance with official reports and relation to outcomes.
Children and Youth Services Review, 62, 111-121. doi:10.1016/j.childyouth.2016.02.004
Widaman, K. F. (2006). Missing data: What to do with or without them. Monographs of the
Society for Research in Child Development, 71(3), 42-64. doi:10.1111/j.1540-
5834.2006.00404.x
Widom, C. S. (1989). Does violence beget violence? A critical examination of the literature.
Psychology Bulletin, 106, 3-28. doi:10.1037/0033-2909.106.1.3
Widom, C. S., & Morris, S. (1997). Accuracy of adult recollections of childhood victimization:
Part 2. Childhood sexual abuse. Psychological Assessment, 9, 34-46. doi:10.1037/1040-
3590.9.1.34
Widom, C. S., & Shepard, R. L. (1996). Accuracy of adult recollections of childhood
victimization: Part 1. Childhood physical abuse. Psychological Assessment, 8, 412-421.
doi:10.1037/1040-3590.8.4.412
Wright, M. O., Crawford, E., & Del Castillo, D. (2009). Childhood emotional maltreatment and
later psychological distress among college students: The mediating role of maladaptive
schemas. Child Abuse & Neglect, 33, 59-68. doi:10.1016/j.chiabu.2008.12.007
Yu, C. Y. (2002). Evaluating cutoff criteria of model fit indices for latent variable models with
binary and continuous outcomes. (Unpublished doctoral dissertation). University of
California Los Angeles, Los Angeles, CA. doi:10.1.1.310.3956

66
Table 1
Standardized Factor Loadings for the CFA for the Final Model of the CAMI PM
Item Factor Loading
Terrorizing
2. My parents put me in situations that frightened me. .74
6. My parents threatened to leave me somewhere so that I could never come home. .80
14. My parents sometimes got angry and destroyed things that were mine. .81
19. My parents threatened to leave me and never come back. .84
23. My parents threatened to hit or physically hurt me when I was a child. .81
Spurning
4. My parents often made me cry for no good reason. .83
20. My parents purposely embarrassed me in front of my friends. .72
22. I was cursed or sworn at as a child by my parents. .79
Exploiting/Corrupting
3. My parents didn’t really care when I did things that were wrong. .69
7. I used illegal drugs with my parents before I was 18 years old. .83
11. I saw my parents do illegal things like use drugs or steal. .89
21. My parents encouraged me to do things that some might consider illegal or
immoral.
.91
Isolating
10. My parents often sent me to bed without dinner. .87
16. My parents punished me by confining me to a closet or other small places. .79
Denying Emotional Responsiveness
8. My parents often asked me about my day. .83
12. My parents liked spending time with me. .89
15. My childhood achievements were acknowledged by my parents. .84
17. My parents paid attention to me when I talked to them. .90
18. My parents showed a lot of interest in me as a child. .92
24. As a child I felt loved by my parents. .90
2 = 481.05***
RMSEA = .06 (.06, .07)
CFI = .98
TLI = .98
Note. CFA = confirmatory factor analysis; CAMI PM = Computer Assisted Maltreatment Inventory
Psychological Maltreatment scale. N = 490. Factors are in bold. Deleted items include items 1
(“Being second best was never good enough for my parents”), 5 (“My parents were very
controlling”), 9 (“I felt like my parents used me to meet their own emotional needs”), and 13
(“When I was in school, only A’s were good enough for my parents”).
*p < .05. **p < .01. ***p < .001.

67
Table 2
Fit Indices for Latent Profile Models 1 – 4
Model AIC BIC ABIC LMR (p) VLMR (p) BLRT (p) Entropy
1 6407.06 6449.01 6417.27 --- --- --- ---
2 5403.35 5470.46 5417.68 989.10 (.003) 1015.71 (.002) 1015.71 (<.001) 0.917
3 5083.23 5175.50 5105.68 323.42 (<.001) 332.13 (<.001) 332.13 (<.001) 0.919
4 4967.22 5084.66 4995.79 124.657 (.53) 128.01 (.53) 128.01 (<.001) 0.931
Note. AIC = Akaike information criteria; BIC = Bayesian information criteria; ABIC = Sample-size
adjusted BIC; LMR = Lo-Mendell-Rubin adjusted likelihood ratio test; VLMR = Vuong-Lo-Mendell-
Rubin likelihood ratio test; BLRT = Bootstrap likelihood ratio test.

68
Table 3
Characteristics of Psychological Maltreatment (PM) Subtypes for the PM Groups
Psychological maltreatment group
Full sample
(N = 490)
Low
(n = 304)
Moderate
(n = 133)
High
(n = 53)
PM subtypes M (SD) M (SD) M (SD) M (SD) F (2, 487) η2partial
Terrorizing 1.81 (.92) 1.27 (.36)a 2.29 (.51)b 3.72 (.67)c 736.45** .76
Spurning 2.12 (1.12) 1.41 (.47)a 2.95 (.68)b 4.17 (.66)c 711.37** .75
Exploiting/corrupting 1.47 (.77) 1.14 (.33)a 1.83 (.86)b 2.38 (1.14)c 105.90** .31
Isolating 1.38 (.71) 1.09 (.27)a 1.56 (.68)b 2.58 (1.02)c 182.79** .43
Denying ER 2.00 (1.00) 1.54 (.62)a 2.36 (.85)b 3.66 (.95)c 202.03** .46
Note. All p-values are Bonferroni adjusted. Denying ER = denying emotional responsiveness.
aWithin each row, means with different subscripts are significantly different at p < .01.
*p < .05. **p < .01.

69
Table 4
Demographic Characteristics of Psychological Maltreatment Groups
Psychological maltreatment group
Full
sample
(N = 490)
Low
(n = 304)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) M (SD) F (df) ηp2
Age 21.73
(2.23)
21.66
(2.26)
21.84
(2.17)
21.83
(2.18)
.37 (2,
487) .00
n (%) n (%) n (%) n (%) 2
Race/ethnicity
White 301 (61.4) 178 (58.6) 89 (66.9) 34 (64.2) 2.92
African American 171 (34.9) 113 (37.2) 45 (33.8) 13 (24.5) 3.27
Latina 28 (5.7) 14 (4.6) 8 (6.0) 6 (11.3) −
Native American 15 (3.1) 8 (2.6) 3 (2.3) 4 (7.5) −
Asian 21 (4.3) 12 (3.9) 6 (4.5) 3 (5.7) −
Other 13 (2.7) 6 (2.0) 5 (3.8) 2 (3.8) −
Student 303 (61.8) 198 (65.1) 81 (60.9) 24 (45.3) 6.87
Children 98 (20.0) 50 (16.4) 33 (24.8) 15 (28.3) 6.86
Note. All p-values are Bonferroni adjusted. There were no significant differences. For cells n < 5,
Fisher’s Exact Test was used in place of the Chi-square. Other = other race/ethnicity; Student =
participant was a student; Children = participant had children. Demographic characteristics, with the
exception of age, were coded 0 = no, 1 = yes. Percentages for race/ethnicity add up to over 100%
because participants could select more than one race/ethnicity.

70
Table 5
Co-occurrence of Other Types of Child Maltreatment
Psychological maltreatment group
Full sample
(N = 490)
Low
(n = 291)
Moderate
(n = 131)
High
(n = 49)
M (SD) M (SD) M (SD) M (SD) F (2, 460) η2partial
Neglect severity 1.57 (.62) 1.30 (.35)a 1.78 (.59)b 2.48 (.72)c 148.96** .39
CPA severity 9.07 (6.20) 6.98 (6.15)a 11.52 (5.00)b 14.80 (1.49)c 59.93** .20
CSA severity 5.10 (6.19) 3.36 (5.30)a 6.94 (6.27)b 10.59 (6.43)c 43.01** .16
Note. All p-values are Bonferroni adjusted. CPA = child physical abuse; CSA = child sexual abuse.
aWithin each row, means with different subscripts are significantly different at p < .05.
*p < .05. **p < .01.
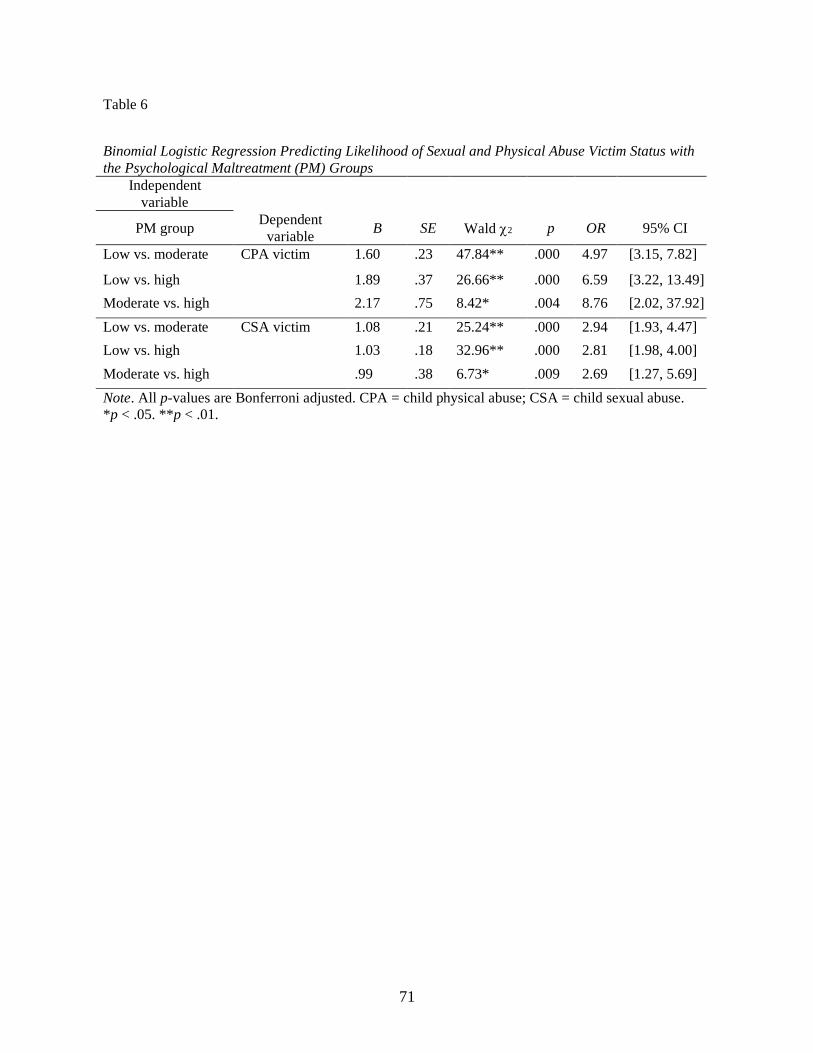
71
Table 6
Binomial Logistic Regression Predicting Likelihood of Sexual and Physical Abuse Victim Status with
the Psychological Maltreatment (PM) Groups
Independent
variable
PM group Dependent
variable B SE Wald 2 p OR 95% CI
Low vs. moderate CPA victim 1.60 .23 47.84** .000 4.97 [3.15, 7.82]
Low vs. high 1.89 .37 26.66** .000 6.59 [3.22, 13.49]
Moderate vs. high 2.17 .75 8.42* .004 8.76 [2.02, 37.92]
Low vs. moderate CSA victim 1.08 .21 25.24** .000 2.94 [1.93, 4.47]
Low vs. high 1.03 .18 32.96** .000 2.81 [1.98, 4.00]
Moderate vs. high .99 .38 6.73* .009 2.69 [1.27, 5.69]
Note. All p-values are Bonferroni adjusted. CPA = child physical abuse; CSA = child sexual abuse.
*p < .05. **p < .01.

72
Table 7
Intercorrelations, Means, and Standard Deviations for Outcome Variables for the Full Sample
Depression Anxiety
Problematic
alcohol use
Heavy episodic
drinking
Cannabis use
frequency
Nicotine Use
Frequency
Depression
(DASS-21)
−
Anxiety
(DASS-21)
.67** −
Problematic alcohol use
(AUDIT)
.30** .26** −
Heavy episodic drinking
(HED)
.25** .22** .84** −
Cannabis use frequency
(DUQ)
.22** .26** .42** .41** −
Nicotine use frequency
(DUQ)
.20** .26** .38** .31** .50** −
M 3.75 3.34 4.85 .66 1.04 1.20
SD 4.50 3.81 5.13 .69 1.64 1.93
Note. DASS-21= Depression, Anxiety, and Stress Scale; AUDIT = Alcohol Use Disorders Identification
Test; HED = Heavy Episodic Drinking; DUQ = Drug Use Questionnaire.
*p < .05. **p < .01.

73
Table 8
Bivariate Correlations for Outcomes Variables and Demographic Characteristics for the Full Sample
Age White
African
American Latina
Native
American Asian Other Student Children
Depression
(DASS-21) .02 .07 -.10* .11* .00 .01 -.01 -.09* .08
Anxiety
(DASS-21) -.05 .01 -.05 .14** .02 .03 .03 -.04 .12**
Problematic alcohol use
(AUDIT) .00
.26*
* -.25** .04 -.03 -.01 -.10* -.11* -.13**
Heavy episodic drinking
(HED) .00
.24*
* -.23** .04 -.09* .00 -.09* -.10* -.12**
Cannabis use frequency
(DUQ) -.05 .09 -.06 .01 .07 -.05 -.07 -.12** -.04
Nicotine use frequency
(DUQ) .06
.25*
* -.24** -.03 .01 .02 -.07 -.24** .09*
Note. DASS-21= Depression, Anxiety, and Stress Scale; AUDIT = Alcohol Use Disorders
Identification Test; HED = Heavy Episodic Drinking; DUQ = Drug Use Questionnaire. Other = other
race/ethnicity; Student = participant was a student; Children = participant had children. Demographic
characteristics, with the exception of age, were coded 0 = no, 1 = yes.
*p < .05. **p < .01

74
Table 9
Depression and Anxiety Between the Psychological Maltreatment Groups
Psychological maltreatment groups
Full sample
(N = 490)
Low
(n = 304)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) M (SD) F (df) ηp2
Depression 3.75 (4.50) 2.88 (3.96)a 4.66 (4.31)b 6.47 (6.12)b 19.55 (2, 487)** .07
Anxiety 3.34 (3.81) 2.41 (3.20)a 4.45 (4.00)b 5.91 (4.62)b 29.98 (2, 487)** .11
Note. All p-values are Bonferroni adjusted. Depression and anxiety were assessed with the Depression,
Anxiety, and Stress Scale (DASS-21).
aWithin each row, means with different subscripts are significantly different at p < .01.
*p < .05. **p < .01.

75
Table 10
Crosstabulation of Psychological Maltreatment Groups and Depression Severity Category
Psychological maltreatment group
Depression severity
(DASS-21 score multiplied by 2) Low
n = 304
Moderate
n = 133
High
n = 53
Full sample
(N = 490)
Normal
(0 – 9)
77.3%
n = 235
(5.7)
54.1%
n = 72
(-4.0)
49.1%
n = 26
(-3.1)
68.0%
n = 333
Mild – moderate
(10 – 20)
16.1%
n = 49
(-3.8)
34.6%
n = 46
(4.3)
20.8%
n = 11
(-.2)
21.6%
n = 106
Severe – extremely severe
(11 – 42)
6.6%
n = 20
(-3.5)
11.3%
n = 15
(.4)
30.2%
n = 16
(5.0)
10.4%
n = 51
Note. Adjusted residuals appear in parentheses below observed frequencies. Adjusted residuals
exceeding ±1.96 are significant at p < .05. Depression was assessed with the Depression, Anxiety, and
Stress Scale (DASS-21).
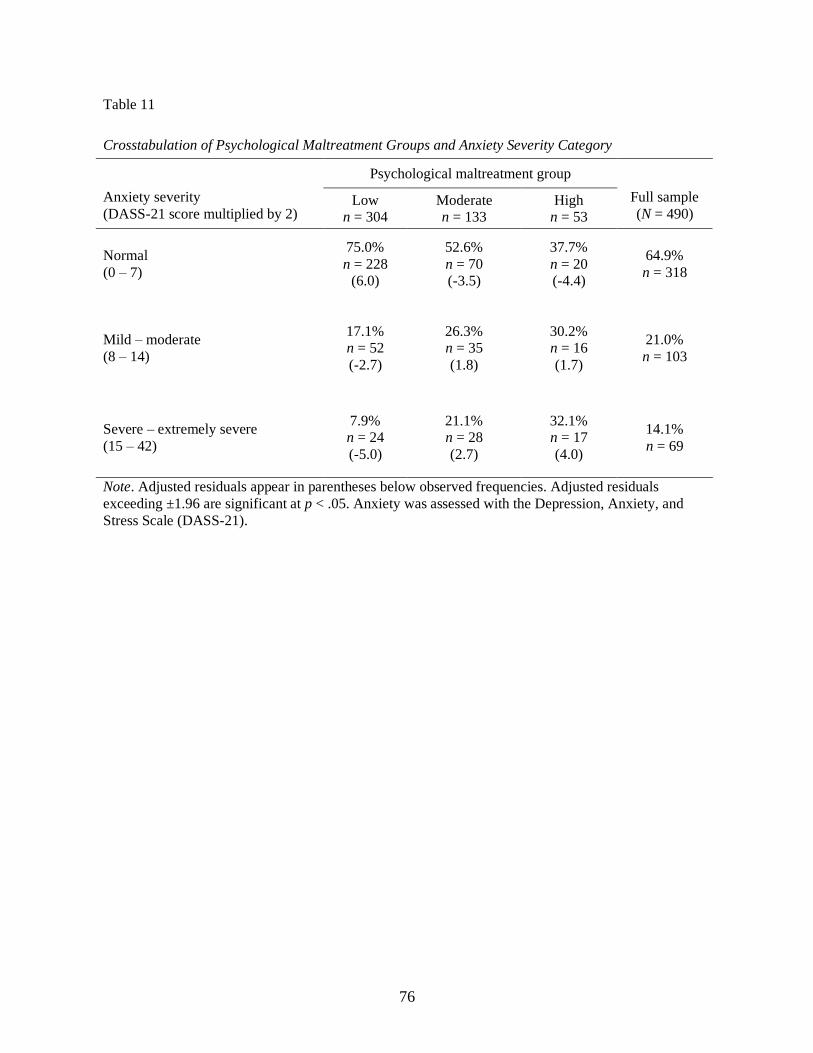
76
Table 11
Crosstabulation of Psychological Maltreatment Groups and Anxiety Severity Category
Psychological maltreatment group
Anxiety severity
(DASS-21 score multiplied by 2) Low
n = 304
Moderate
n = 133
High
n = 53
Full sample
(N = 490)
Normal
(0 – 7)
75.0%
n = 228
(6.0)
52.6%
n = 70
(-3.5)
37.7%
n = 20
(-4.4)
64.9%
n = 318
Mild – moderate
(8 – 14)
17.1%
n = 52
(-2.7)
26.3%
n = 35
(1.8)
30.2%
n = 16
(1.7)
21.0%
n = 103
Severe – extremely severe
(15 – 42)
7.9%
n = 24
(-5.0)
21.1%
n = 28
(2.7)
32.1%
n = 17
(4.0)
14.1%
n = 69
Note. Adjusted residuals appear in parentheses below observed frequencies. Adjusted residuals
exceeding ±1.96 are significant at p < .05. Anxiety was assessed with the Depression, Anxiety, and
Stress Scale (DASS-21).

77
Table 12
Alcohol Use Between the Psychological Maltreatment Groups
Psychological maltreatment group
Full sample
(N = 490)
Low
(n = 304)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) M (SD) F (df) ηp2
AUDIT 4.85 (5.13) 4.15 (4.39)a 5.75 (5.57)b 6.61 (6.96)b 8.21 (2, 487)** .03
HED .66 (.69) .59 (.62)a .73 (.70)ab .92 (.94)b 6.23 (2, 487)* .03
Note. AUDIT = Alcohol Use Disorder Identification Test; HED = Heavy Episodic Drinking. All p-
values are Bonferroni adjusted.
aWithin each row, means with different subscripts are significantly different at p < .05.
*p < .05. **p < .01.

78
Table 13
Crosstabulation of Psychological Maltreatment Group and Problematic Alcohol Use
Psychological maltreatment group
Low
n = 302
Moderate
n = 131
High
n = 53
Full sample
(N = 486)
Non-problematic alcohol use
(AUDIT scores < 8)
82.5%
n = 249
(2.9)
72.5%
n = 95
(-1.8)
67.9%
n = 36
(-1.9)
78.2%
n = 380
Problematic alcohol use
(AUDIT scores 8)
17.5%
n = 53
(-2.9)
27.5%
n = 36
(1.8)
32.1%
n = 17
(1.9)
21.8%
n = 106
Note. Adjusted residuals appear in parentheses below observed frequencies. AUDIT = Alcohol Use
Disorders Identification Test. Adjusted residuals exceeding ±1.96 are significant at p < .05.
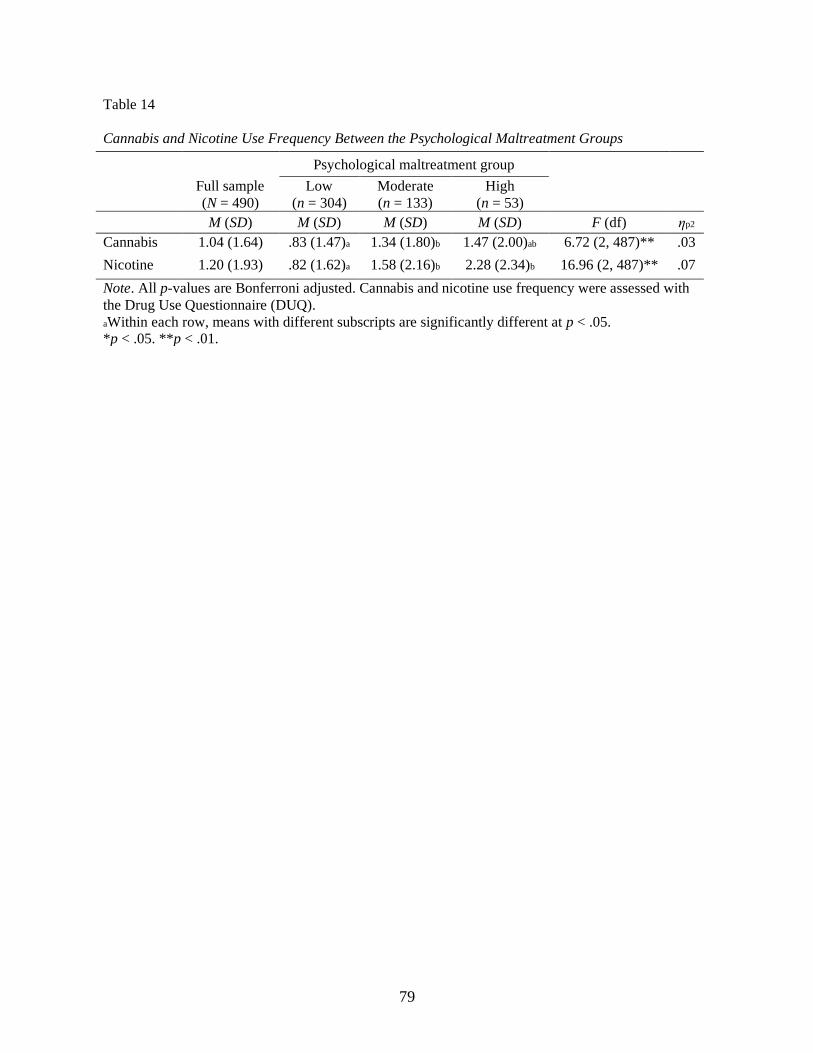
79
Table 14
Cannabis and Nicotine Use Frequency Between the Psychological Maltreatment Groups
Psychological maltreatment group
Full sample
(N = 490)
Low
(n = 304)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) M (SD) F (df) ηp2
Cannabis 1.04 (1.64) .83 (1.47)a 1.34 (1.80)b 1.47 (2.00)ab 6.72 (2, 487)** .03
Nicotine 1.20 (1.93) .82 (1.62)a 1.58 (2.16)b 2.28 (2.34)b 16.96 (2, 487)** .07
Note. All p-values are Bonferroni adjusted. Cannabis and nicotine use frequency were assessed with
the Drug Use Questionnaire (DUQ).
aWithin each row, means with different subscripts are significantly different at p < .05.
*p < .05. **p < .01.

80
Table 15
Crosstabulation of Psychological Maltreatment Groups and Drug Use Frequency
Psychological maltreatment group
Drug use frequency
Low
n = 304
Moderate
n = 132
High
n = 53
Full sample
(N = 489)
None
85.9%
n = 261
(4.2)
70.5%
n = 93
(-3.2)
69.8%
n = 37
(-2.0)
80.0%
n = 391
Low
8.2%
n = 25 (-.8)
10.6%
n = 14 (.8)
9.4%
n = 5 (.1)
9.0%
n = 44
Moderate – high
5.9%
n = 18
(-4.6)
18.9%
n = 25
(3.4)
20.8%
n = 11
(2.4)
11.0%
n = 54
Note. Adjusted residuals appear in parentheses below observed frequencies. Adjusted residuals
exceeding ±1.96 are significant at p < .05. Drug use frequency was assessed with the Drug Use
Questionnaire (DUQ).

81
Table 16
Crosstabulation of Psychological Maltreatment Groups and Drug Use Problems
Psychological maltreatment group
Drug use problem severity
Low
n = 302
Moderate
n = 131
High
n = 53
Full sample
(N = 489)
None
80.5%
n = 243
(5.8)
58.0%
n = 76
(-3.9)
50.9%
n = 27
(-3.4)
80.0%
n = 391
Mild
11.9%
n = 36
(-2.6)
21.4%
n = 28
(2.3)
18.9%
n = 10
(.8)
9.0%
n = 44
Moderate – severe
7.6%
n = 23
(-4.9)
20.6%
n = 27
(2.7)
30.2%
n = 16
(3.7)
11.0%
n = 54
Note. Adjusted residuals appear in parentheses below observed frequencies. Adjusted residuals
exceeding ±1.96 are significant at p < .05. Drug use problem severity was assessed with the Drug Use
Questionnaire (DUQ).

82
Table 17
Depression and Anxiety Between the Psychological Maltreatment Groups Controlling for CSA and CPA Victim Status
Psychological maltreatment groups
Low
(n = 303)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) F (df) ηp2
Depression 2.88 (3.97)a 4.66 (4.31)ab 6.47 (6.12)b 5.27 (2, 484)* .02
Anxiety 2.38 (3.16)a 4.45 (4.00)b 5.91 (4.62)b 12.03 (2, 484)** .05
Note. All p-values are Bonferroni adjusted. CSA = child sexual abuse; CPA = child physical abuse.
Depression and anxiety were assessed with the Depression, Anxiety, and Stress Scale (DASS-21).
aWithin each row, means with different subscripts are significantly different at p < .01.
*p < .05. **p < .01.

83
Table 18
Alcohol Use Between the Psychological Maltreatment Groups Controlling for CSA and CPA Victim Status
Psychological maltreatment groups
Low
(n = 303)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) F (df) ηp2
AUDIT 4.16 (4.40)a 5.75 (5.57)a 6.61 (6.96)a 3.86 (2, 484)* .02
HED .59 (.62) .73 (.70) .92 (.94) 3.63 (2, 484) .02
Note. AUDIT = Alcohol Use Disorder Identification Test; HED = Heavy Episodic Drinking; CSA =
child sexual abuse; CPA = child physical abuse. All p-values are Bonferroni adjusted.
aWithin each row, means with different subscripts are significantly different at p < .05.
*p < .05.
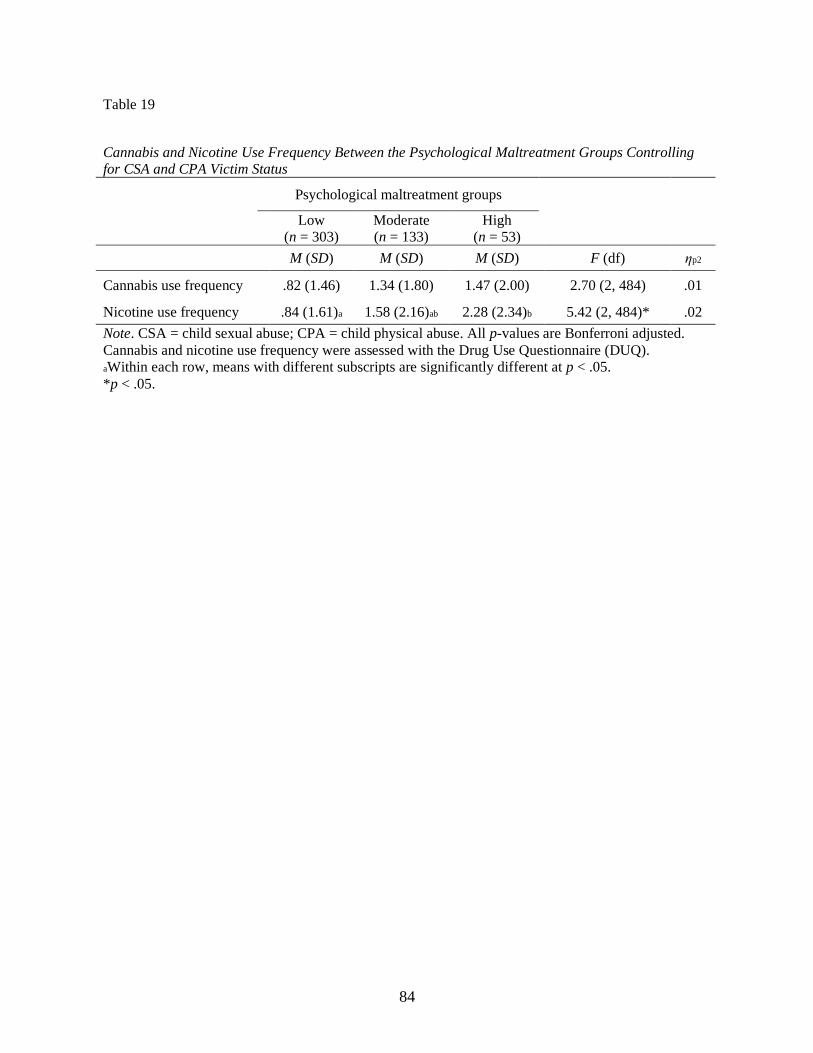
84
Table 19
Cannabis and Nicotine Use Frequency Between the Psychological Maltreatment Groups Controlling for CSA and CPA Victim Status
Psychological maltreatment groups
Low
(n = 303)
Moderate
(n = 133)
High
(n = 53)
M (SD) M (SD) M (SD) F (df) ηp2
Cannabis use frequency .82 (1.46) 1.34 (1.80) 1.47 (2.00) 2.70 (2, 484) .01
Nicotine use frequency .84 (1.61)a 1.58 (2.16)ab 2.28 (2.34)b 5.42 (2, 484)* .02
Note. CSA = child sexual abuse; CPA = child physical abuse. All p-values are Bonferroni adjusted.
Cannabis and nicotine use frequency were assessed with the Drug Use Questionnaire (DUQ).
aWithin each row, means with different subscripts are significantly different at p < .05.
*p < .05.
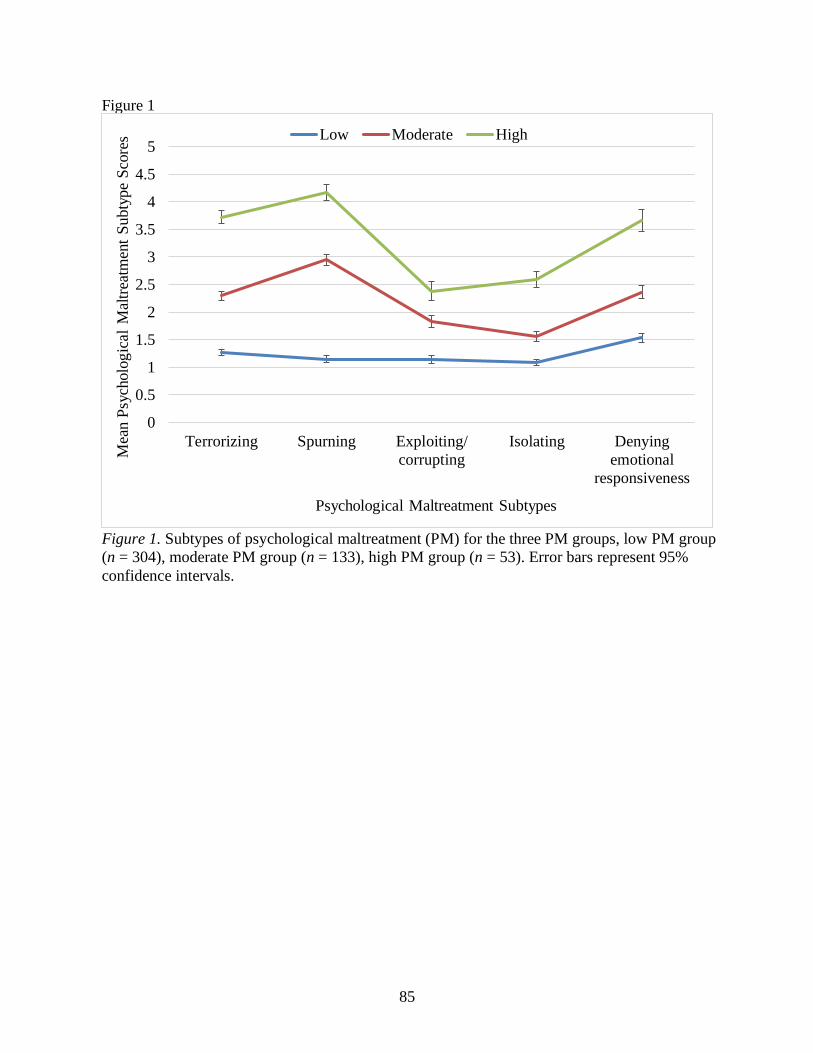
85
Figure 1
Figure 1. Subtypes of psychological maltreatment (PM) for the three PM groups, low PM group
(n = 304), moderate PM group (n = 133), high PM group (n = 53). Error bars represent 95%
confidence intervals.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Terrorizing Spurning Exploiting/
corrupting
Isolating Denying
emotional
responsiveness
Mea
n P
sych
olo
gic
al
Mal
trea
tmen
t S
ubty
pe
Sco
res
Psychological Maltreatment Subtypes
Low Moderate High
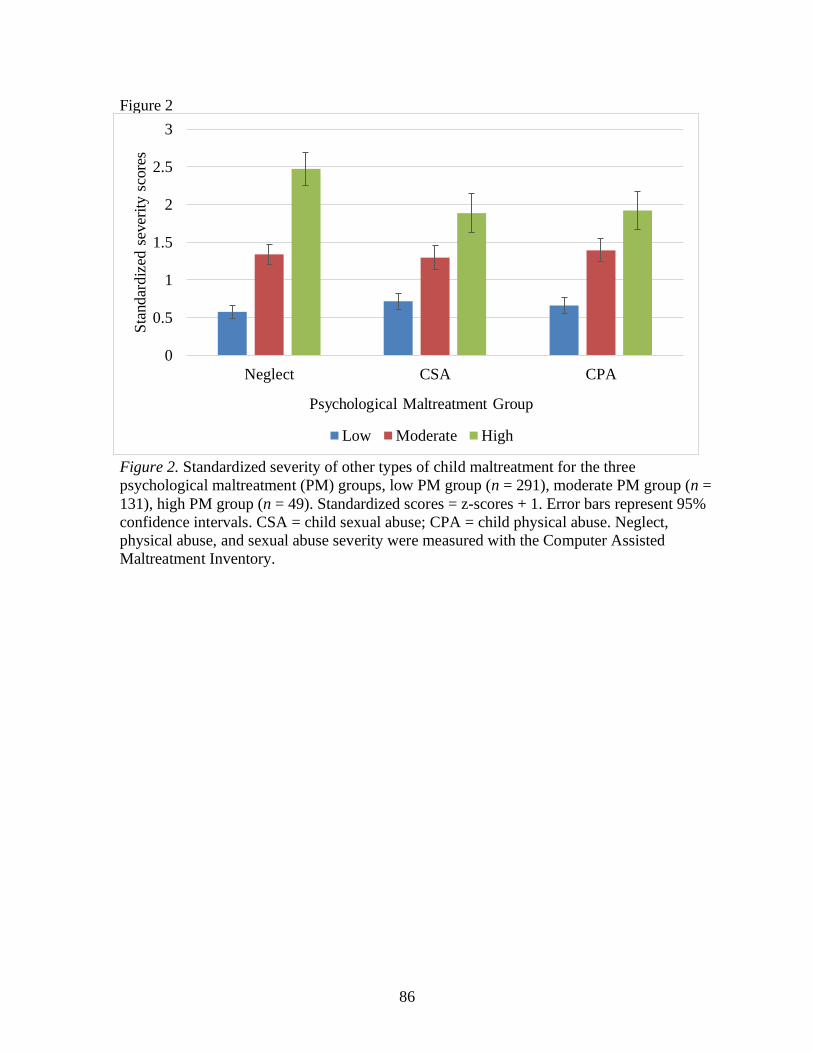
86
Figure 2
Figure 2. Standardized severity of other types of child maltreatment for the three
psychological maltreatment (PM) groups, low PM group (n = 291), moderate PM group (n =
131), high PM group (n = 49). Standardized scores = z-scores + 1. Error bars represent 95%
confidence intervals. CSA = child sexual abuse; CPA = child physical abuse. Neglect,
physical abuse, and sexual abuse severity were measured with the Computer Assisted
Maltreatment Inventory.
0
0.5
1
1.5
2
2.5
3
Neglect CSA CPA
Sta
ndar
diz
ed s
ever
ity s
core
s
Psychological Maltreatment Group
Low Moderate High

87
Figure 3
Figure 3. Percent of participants who were victims of CSA and CPA in each of the three
psychological maltreatment (PM) groups, low PM group (CSA: n = 304, CPA: n = 303),
moderate PM group (CSA: n = 133, CPA: n = 133), high PM group (CSA: n = 53, CPA: n =
53). CSA = child sexual abuse; CPA = child physical abuse. Physical abuse and sexual abuse
victim status were assessed using the Computer Assisted Maltreatment Inventory.
32.6%
58.6%
79.2%
36.8%
74.4%
96.2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Low Moderate High
Per
cent
Vic
tim
s
Psychological Maltreatment Group
CSA
CPA

88
Figure 4
Figure 4. Percent of participants who were victims of CSA and/or CPA in each of the three
psychological maltreatment (PM) groups, low PM group (CSA: n = 304, CPA: n = 303),
moderate PM group (CSA: n = 133, CPA: n = 133), high PM group (CSA: n = 53, CPA: n = 53).
CSA = child sexual abuse; CPA = child physical abuse. Physical abuse and sexual abuse victim
status were assessed using the Computer Assisted Maltreatment Inventory.
Low Moderate High
No CSA or CPA 47.4% 12.8% 0.0%
CSA Only 20.4% 28.6% 20.8%
CPA Ony 15.8% 12.8% 3.8%
CSA & CPA 16.4% 45.9% 75.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%P
erce
nt
Vic
tim
s
Psychological Maltreatment Group

Figure 5
Figure 5. Characteristics of child sexual abuse (CSA) experiences by psychological maltreatment (PM) group. Only CSA victims
were included, low PM group (n = 99), moderate PM group (n = 78), high PM group (n = 42). Characteristics of sexual abuse were
assessed using the Computer Assisted Maltreatment Inventory. For each characteristic, the most severe category (or maximum
value) was identified and coded as present or absent for each participant.
Intrafamilial
perpetrator
Number of
perpetrators:
≥ 3
Nature:
Penetration
Tactic:
Physically held
down
Frequency:
> 10 timesDuration:
≥ 2 years
Total sample 42.5% 21.9% 62.6% 50.7% 29.7% 34.7%
Low PM group 29.3% 15.2% 55.6% 47.5% 21.2% 27.3%
Moderate PM group 46.2% 23.1% 66.7% 47.4% 32.1% 38.5%
High PM group 66.7% 35.7% 71.4% 64.3% 45.2% 45.2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Per
cent
Characteristics of CSA

90
Figure 6
Figure 6. Characteristics of child physical abuse (CPA) experiences by psychological maltreatment (PM) group. Only CPA victims
were included, low PM group (n = 112), moderate PM group (n = 99), high PM group (n = 51). Characteristics of physical abuse
were assessed using the Computer Assisted Maltreatment Inventory. For each characteristic, the most severe category (or maximum
value) was identified and coded as present or absent for each participant.
Perpetrator
type: Parent
Number of
perpetrators:
≥ 3
Nature:
Choked, beaten,
burned
Injury:
Bone fractures,
burns, internal
injury, paralysis
Frequency:
> 10 timesDuration:
≥ 2 years
Total sample 96.6% 25.2% 71.0% 7.3% 42.4% 88.9%
Low PM group 97.3% 21.4% 50.9% 0.9% 35.7% 83.0%
Moderate PM group 96.0% 24.2% 81.8% 7.1% 37.4% 92.9%
High PM group 96.1% 35.3% 94.1% 21.6% 66.7% 94.1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Per
cent
Characteristics of CPA




















