Lung Transplantation - UI Health Care
27
1 Lung Transplantation 2020 Tahuanty Peña, MD, MS Division of Pulmonary, Critical Care and Occupational Medicine I will not discuss off label use and/or investigational use of the following drugs/devices. NO relevant financial relationships exist related to this presentation. Relevant Financial Relationship Disclosure Statement 1 2
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Lung Transplantation - UI Health Care
1
Lung Transplantation2020Tahuanty Peña, MD, MSDivision of Pulmonary, Critical Care and Occupational Medicine
I will not discuss off label use and/or investigational use of the following drugs/devices.
NO relevant financial relationships exist related to this presentation.
Relevant Financial Relationship Disclosure Statement
1
2

2
Objectives
Overview of Lung Transplantation
Lung Transplant at UIHC
Case Studies
Objectives
Overview of Lung Transplantation
Lung Transplant at UIHC
Case Studies
3
4

3
Who needs a transplant?Severe end stage lung disease
Ineffective/maximal medical therapy
Limited life expectancy (< 2 yrs)
Capable of full rehabilitation post transplantation
Adequate psychosocial profile
Recipient Selection Diseases
Obstructive: Emphysema, Alpha 1 anti-trypsin, COPD
Suppurative: Cystic fibrosis, bronchiectasis
Restrictive: interstitial lung diseases
Vascular: Pulmonary hypertension
5
6

4
Lung function after transplant
4/13/2016 6/6/2018
FVC 1.25 3.36
FVC %Predicted
35% 100%
FEV1 0.29 3.03
FEV1% Predicted
10% 113%
FEV1/FVC 23 90
FEF 25-75% 0.10 3.34
FEF 25-75% % Predicted
4 122
Recipient Selection
J Heart Lung Transplant. 2015 Jan;34(1):1-15. doi: 10.1016/j.healun.2014.06.014. Epub 2014 Jun 26
Absolute Contraindications Recent history of Malignancy.
Untreatable significant organ system dysfunction (heart, liver, kidney, brain) Combined transplantation.
CAD non amenable to revascularization.
Acute Medical instability (non-pulmonary).
Uncorrectable bleeding diathesis.
Chronic infection with highly virulent/resistant microbes.
7
8

5
Recipient Selection
J Heart Lung Transplant. 2015 Jan;34(1):1-15. doi: 10.1016/j.healun.2014.06.014. Epub 2014 Jun 26
Absolute Contraindications Class II or III obesity (BMI>35).
Non-adherence to medical therapy.
Uncontrolled Psychiatric/Psychological conditions.
Absence of reliable social support.
Poor rehabilitation potential.
Substance abuse or dependence.
Recipient Selection
J Heart Lung Transplant. 2015 Jan;34(1):1-15. doi: 10.1016/j.healun.2014.06.014. Epub 2014 Jun 26
Relative Contraindications Age >65 Class I obesity (BMI 30-35) Malnutrition, Osteoporosis Prior chest surgery Mechanical Ventilation or ECLS Infections Hepatitis B or C HIV B. Cepacia M. Abscessus
9
10

6
Surgical Choices
Bilateral TransplantMandatory for suppurative lung disease
Preferred for pulmonary HTN
Better choice for younger patients.
Single TransplantExtends a limited donor pool
Shorter operation with fewer peri operative complications
Lung Allocation Score
Replaced prior time-based system.
Active as of May 2005.
Intended to facilitate allocation of available donors (short supply) to individuals with more urgent need.
Patients ≥ 12 years of age.
Has reduced waitlist mortality in IPF, COPD, CF.
11
12
7
Lung Allocation Score
FVC Pulmonary Hemodynamics O2 at rest Age BMI DM Functional status 6MW distance Assisted ventilation Creatinine Diagnosis PCO2 Bilirubin
Lung Allocation Score
Score from 0 to 100.
Tries to balance severity of illness (risk of mortality) and chances of success following transplant (survival probability).
Provides a rank on waitlist based on blood group.
13
14
8
Lung Allocation Score
Lung Allocation Score
Donor identified family consents for donation.
Organ offered to programs in a 250 nautical miles radius (Zone A).
1 Offered to patients listed in Zone A, ABO identical.
2 Offered to patients listed in Zone A, ABO compatible.
3 Zone B, ABO identical.
4 Zone B, ABO compatible.
Etc…
15
16

9
Lung Allocation Score
17
18

10
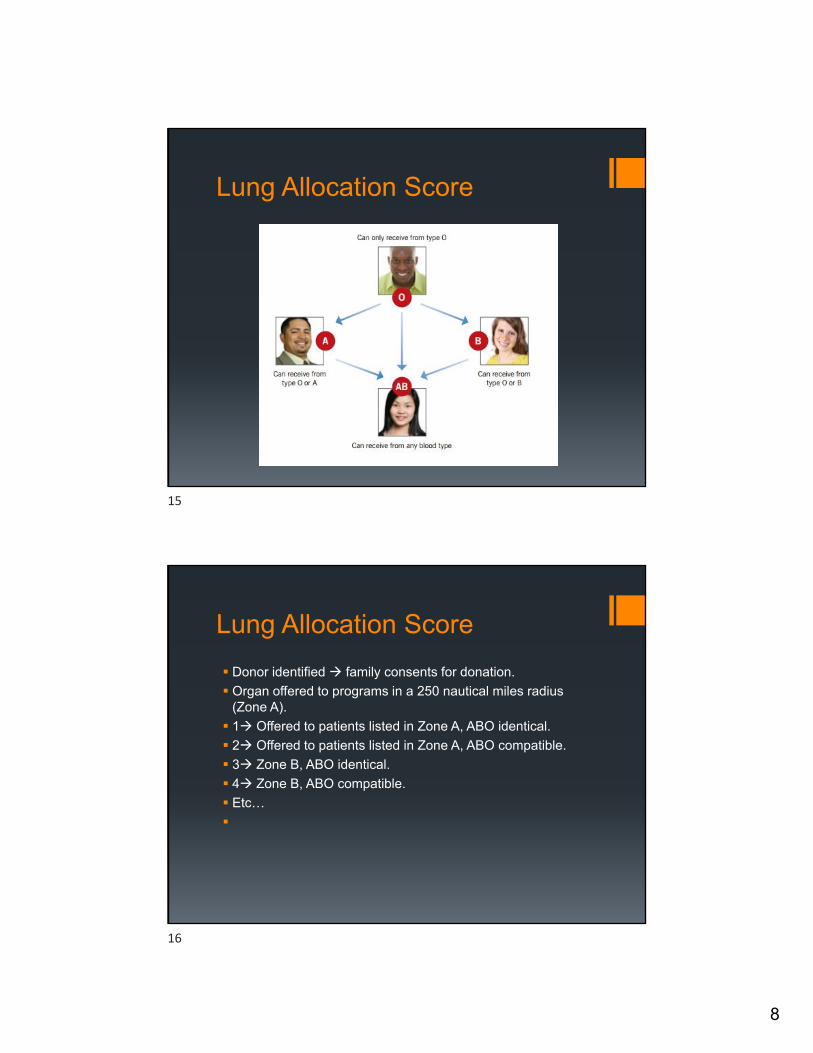
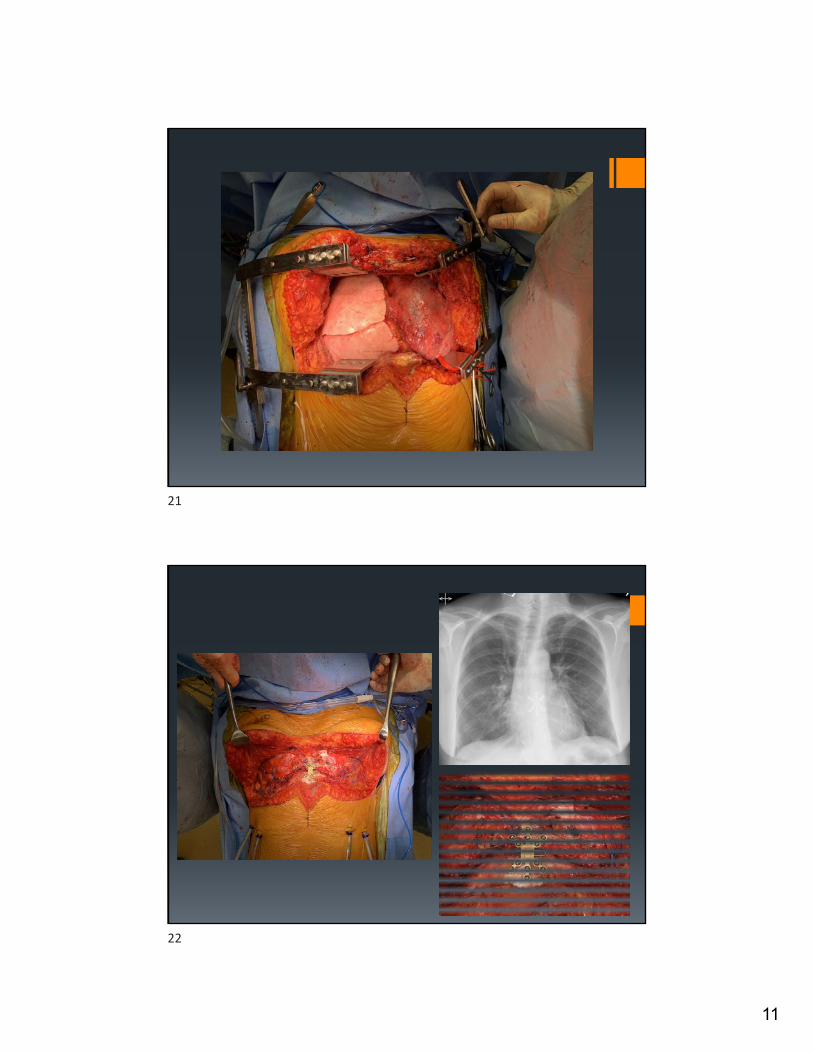
Surgery
19
20
11
21
22
12
23
24

13
Adult and Pediatric Lung TransplantsNumber of Transplants by Year and Location
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000N
um
ber
of
tran
spla
nts
Other
North America
Europe
2018JHLT. 2018 Oct; 37(10): 1155-1206
NOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
Adult and Pediatric Lung TransplantsNumber of Transplants by Year and Procedure Type
5 7 35 74167
408
709923
110512131391
13921512
15501568
1708178519792018
2228
2583
281129503025
3313
3587
38693852
417740984261
4661
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Nu
mb
er o
f Tr
ansp
lan
ts
Bilateral/Double Lung
Single Lung
NOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
2018JHLT. 2018 Oct; 37(10): 1155-1206
25
26

14
42
30
45
2819
1015
0
6
12
18
24
30
36
0
10
20
30
40
50
60
1-4 5-9 10-19 20-29 30-39 40-49 50+
% o
f Tr
ansp
lan
ts (
red
lin
e)
Nu
mb
er o
f C
ente
rs
Average number of lung transplants per year
Number of centers Percentage of transplants
Adult and Pediatric Lung TransplantsAverage Center Volume (Transplants: January 2004 – June 2017)
2018JHLT. 2018 Oct; 37(10): 1155-1206
Adult Lung TransplantsMajor Diagnoses by Year (Number)
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
Nu
mb
er o
f Tr
ansp
lan
ts
Transplant Year
COPD A1ATD CF IIP ILD-not IIP Retransplant
2018JHLT. 2018 Oct; 37(10): 1155-1206
27
28

15
Europe North America Other0%
20%
40%
60%
80%
100%
% o
f Tr
ansp
lan
ts
Other
Sarcoidosis
Retransplant
Non CF-bronchiectasis
IPAH
ILD-not IIP
IIP
COPD
CF
A1ATD
Adult Lung TransplantsDiagnosis Distribution by Location
(Transplants: January 2004 – June 2017)
2018JHLT. 2018 Oct; 37(10): 1155-1206
Objectives
Overview of Lung Transplantation
Lung Transplant at UIHC
Case Studies
29
30

16
Lung Transplantation at the University of Iowa
First and only lung transplant program in Iowa
Originally active 1988-1996
Reactivated May 2007
198 lung transplants and counting…
UNOS Zones
73 centers doing adult lung transplants
31
32

17
Multidisciplinary Approach to Transplantation
Pulmonary MedicineThoracic Surgery PharmacyNursingRespiratory TherapyPulmonary RehabilitationSocial WorkNutritionTransplant Financial
University of Iowa Lung Transplantation Program
Thoracic SurgeryKalpaj Parekh, Surgical DirectorJohn KeechEvgeny Arshava
Pulmonary MedicineJulia Klesney-Tait, Medical DirectorMichael EberleinTahuanty PeñaLakshmi Durairaj
Lung Transplant CoordinatorsAbigail MackRebecca HoranDani Slaughter
Transplant PharmacySarah MinnerHeather Bream-Rouwenhorst
Transplant Social WorkEmily MathewsStephanie Rauckhorst
Pulmonary RehabilitationCarol McCaffertyKim EppenJane GreinerJulie Wiebold
Transplant OfficeDebbie HunterKent BeckerRob Huber
Organ Transplant CenterHeart and Vascular Center
33
34
18
— 35 —
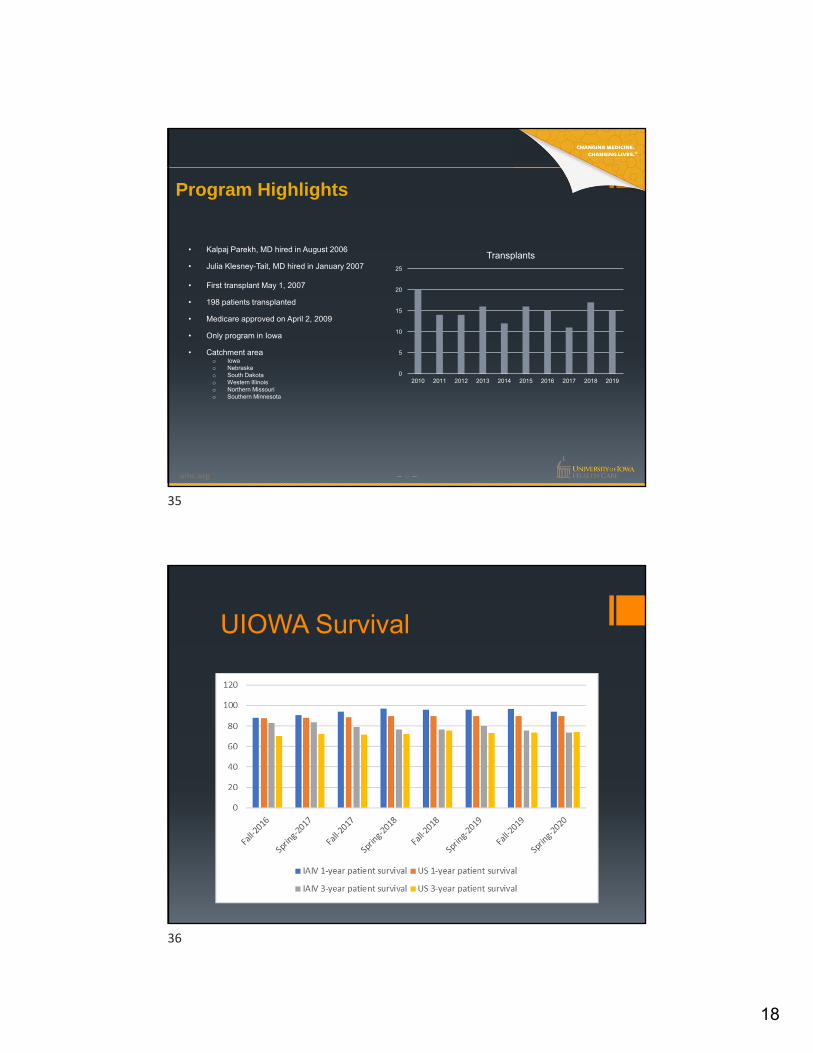
Program Highlights
• Kalpaj Parekh, MD hired in August 2006
• Julia Klesney-Tait, MD hired in January 2007
• First transplant May 1, 2007
• 198 patients transplanted
• Medicare approved on April 2, 2009
• Only program in Iowa
• Catchment areao Iowao Nebraskao South Dakotao Western Illinoiso Northern Missourio Southern Minnesota
0
5
10
15
20
25
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019
Transplants
UIOWA Survival
35
36
19
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Su
rviv
al (
%)
Years
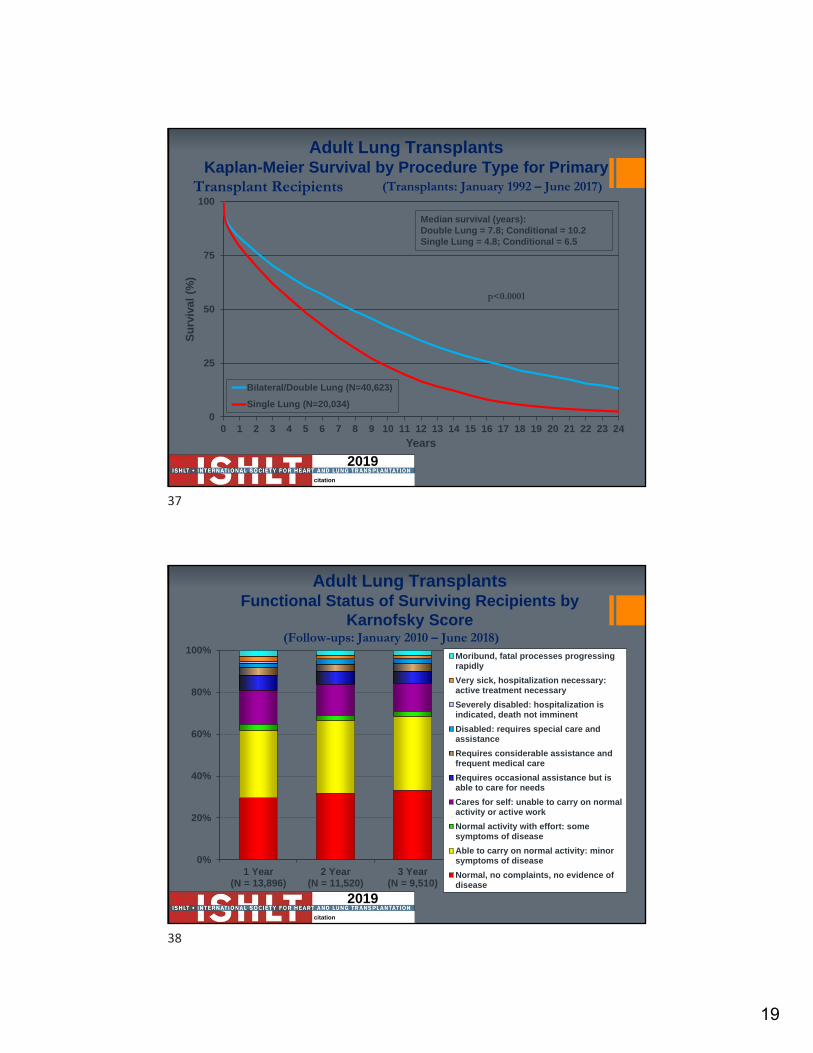
Bilateral/Double Lung (N=40,623)
Single Lung (N=20,034)
Adult Lung TransplantsKaplan-Meier Survival by Procedure Type for Primary
Transplant Recipients
Median survival (years): Double Lung = 7.8; Conditional = 10.2 Single Lung = 4.8; Conditional = 6.5
p<0.0001
(Transplants: January 1992 – June 2017)
2019citation
2019citation
Adult Lung TransplantsFunctional Status of Surviving Recipients by
Karnofsky Score (Follow-ups: January 2010 – June 2018)
0%
20%
40%
60%
80%
100%
1 Year(N = 13,896)
2 Year(N = 11,520)
3 Year(N = 9,510)
Moribund, fatal processes progressingrapidly
Very sick, hospitalization necessary:active treatment necessary
Severely disabled: hospitalization isindicated, death not imminent
Disabled: requires special care andassistance
Requires considerable assistance andfrequent medical care
Requires occasional assistance but isable to care for needs
Cares for self: unable to carry on normalactivity or active work
Normal activity with effort: somesymptoms of disease
Able to carry on normal activity: minorsymptoms of disease
Normal, no complaints, no evidence ofdisease
37
38
20
Objectives
Overview of Lung Transplantation
Lung Transplant at UIHC
Case Studies
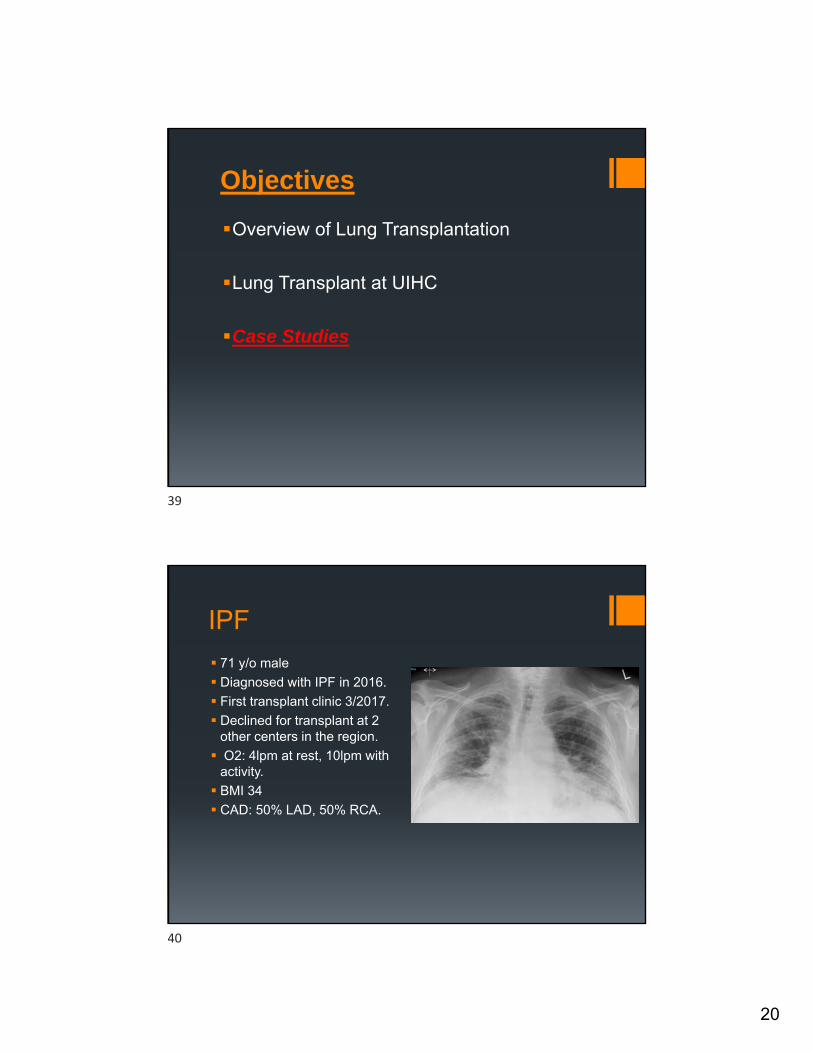
IPF
71 y/o male
Diagnosed with IPF in 2016.
First transplant clinic 3/2017.
Declined for transplant at 2 other centers in the region.
O2: 4lpm at rest, 10lpm with activity.
BMI 34
CAD: 50% LAD, 50% RCA.
39
40

21
IPF
Decision to list for a SLT.
Weight loss to a BMI<30.
Listed 8/2017, Txp 9/2017
CF 32 y/o male with CF (2008)
BMI 20
Multiple exacerbations per year
2lpm at rest, 4lpm with activity
Listed for BLT
Transplanted on Jan/2008
41
42

22
CF
COPD
54 y/o female with COPD
FEV1 0.56L
PCO2 – 62
4lpm at rest, 6lpm with activity
CAD: 80% occlusion of LAD, stent placed.
Hepatitis C positive, underwent treatment.
Listed for txp on 4/2014, transplanted on 8/2015.
43
44
23
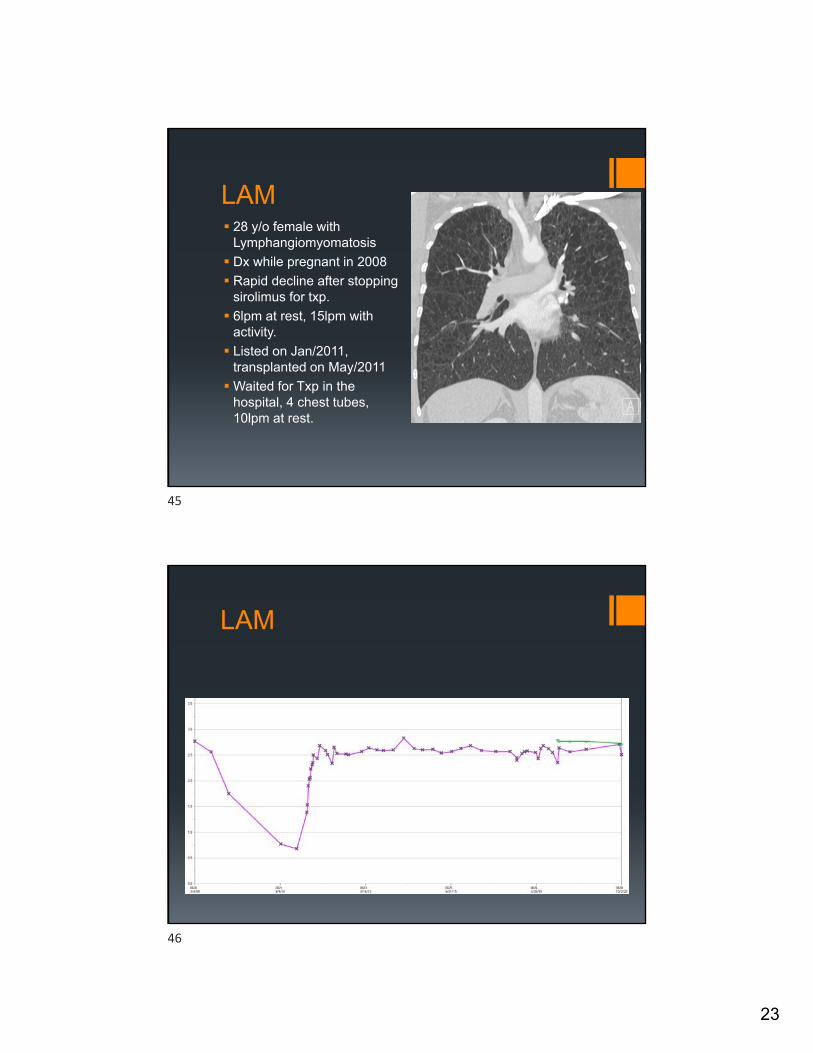
LAM 28 y/o female with
Lymphangiomyomatosis
Dx while pregnant in 2008
Rapid decline after stopping sirolimus for txp.
6lpm at rest, 15lpm with activity.
Listed on Jan/2011, transplanted on May/2011
Waited for Txp in the hospital, 4 chest tubes, 10lpm at rest.
LAM
45
46

24
Melanie P. Lung Transplant 2011
Andrea S. Lung Transplant 2011Lance S. Lung Transplant 2014
Andrea S. Lung Transplant 2011Lance S. Lung Transplant 2014
47
48

25
Don R. Lung Transplant 2013
Destiny R. Lung Transplant 2009
49
50

26
2016 Annual Picnic- Lung recipients
51
52

27
Thank You
53