
Physical Activity in Daily Life 1 Year After Lung Transplantation
7
Physical Activity in Daily Life 1 Year After Lung Transplantation Daniel Langer, PT, MSc, a,b Rik Gosselink, PT, PhD, a,b Fabio Pitta, PT, PhD, c Chris Burtin, PT, MSc, a,b Geert Verleden, MD, PhD, b Lieven Dupont, MD, PhD, b Marc Decramer, MD, PhD, b and Thierry Troosters, PT, PhD a,b Background: Reduced physical fitness has been reported to occur after lung transplantation. Pre- and post- transplant factors, including an inactive lifestyle, have been proposed as possible causes. However, daily physical activity has not been objectively assessed so far in lung recipients. The purpose of this study was to objectively measure daily physical activity in lung recipients. Methods: Twenty-two clinically stable patients with single (n 7) and bilateral lung grafts (n 15) underwent measurements of physical activity with activity monitors at least 12 months after surgery. Results were compared with findings from 22 healthy, age- and gender-matched control subjects. Results: Substantial and statistically significant differences in daily activity were observed. Steps, standing time and moderate-intensity activity of lung recipients were reduced by 42%, 29% and 66%, respectively, relative to controls. Daily sedentary time was increased by 30%. Daily steps correlated with self-reported physical functioning (r 0.81), 6-minute walk distance (r 0.68), quadriceps force (r 0.66) and maximum workload (r 0.63). Conclusions: This study has shown for the first time that daily activity is substantially reduced after lung transplantation and related to measures of physical fitness and health-related quality of life. Future studies need to examine whether physical activity can be modified to improve functional recovery after lung transplantation. J Heart Lung Transplant 2009;28:572– 8. Copyright © 2009 by the International Society for Heart and Lung Transplantation. Lung transplantation (LTx) has gained widespread ac- ceptance as a therapeutic option for end-stage lung disease. 1 Survival rates have improved in successive years with a current worldwide survival half-life of about 5 years. 2 Patients have continued to report limitations in phys- ical functioning despite substantial improvements in general quality of life. 3,4 Persisting limitations in exer- cise capacity and skeletal muscle weakness have also been reported. 5–11 Inactivity prior to transplantation 12 and resulting pre-transplant deconditioning 6,13 are likely to influence functional recovery after surgery. Repeated episodes of infection and rejection, use of anti- inflammatory and immunosuppressive drugs and a sed- entary lifestyle are possible post-transplant contributors to limitations in physical fitness. 5,6,9 Daily physical activity (PA) has been studied in heart and liver recipients, but with ambiguous results. Heart recipients were classified as either “moderately active” (1,100 kcal/week spent in recreational activities), based on self-report, 14 or very sedentary, based on accelerome- ter measurements. 15 No statistically significant differences between liver recipients and healthy controls were re- ported for accelerometer measurements of daily PA. 16 To our knowledge, no data on daily PA after lung transplan- tation have been published. Given this absence of data and the contradictory findings in other study populations after transplantation, the purpose of the present investigation was to objectively measure daily PA in lung recipients. The main research questions were: (1) Do stable lung recipients reach levels of daily PA comparable to those of healthy, age-matched control subjects 1 year after LTx? (2) Is daily PA in lung recipients related to measures of exercise capacity, muscle force and health-related quality of life? METHODS Subjects Our experimental protocol was approved by the ethics review board of the University Hospital Leuven. Criteria for participation in our study were: (1) age 40 years; From the a Department of Rehabilitation Sciences, Katholieke Univer- siteit Leuven, and b Respiratory Rehabilitation and Respiratory Divi- sion, University Hospital Leuven, Leuven, Belgium; and c Department of Physiotherapy, Universidade Estadual de Londrina, Londrina, Brazil. Submitted October 10, 2008; revised March 4, 2009; accepted March 6, 2009. Supported by the International Society for Heart and Lung Transplanta- tion Nursing and Social Science Award 2005 a grant from the Research Foundation Flanders Project G0523.06 and KAN 1.5.139.06N, and a grant from the Brazilian National Council for Scientific and Technological Development (CNPq, Brazil) to F.P. Reprint requests: Thierry Troosters, PT, PhD, Department of Rehabil- itation Sciences, Katholieke Universiteit Leuven, Tervuursevest 101, Leuven 3000, Belgium. Telephone: 32-16-347107. Fax: 32-347126. E-mail: [email protected] Copyright © 2009 by the International Society for Heart and Lung Transplantation. 1053-2498/09/$–see front matter. doi:10.1016/ j.healun.2009.03.007 572
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Physical Activity in Daily Life 1 Year After Lung Transplantation

PDGT
B
M
R
C
Lcdya
igcbat
Fsso
MStFfD
iLECTj
5
hysical Activity in Daily Life 1 Year After Lung Transplantationaniel Langer, PT, MSc,a,b Rik Gosselink, PT, PhD,a,b Fabio Pitta, PT, PhD,c Chris Burtin, PT, MSc,a,b
eert Verleden, MD, PhD,b Lieven Dupont, MD, PhD,b Marc Decramer, MD, PhD,b andhierry Troosters, PT, PhDa,b
ackground: Reduced physical fitness has been reported to occur after lung transplantation. Pre- and post-transplant factors, including an inactive lifestyle, have been proposed as possible causes. However,daily physical activity has not been objectively assessed so far in lung recipients. The purpose of thisstudy was to objectively measure daily physical activity in lung recipients.
ethods: Twenty-two clinically stable patients with single (n � 7) and bilateral lung grafts (n � 15)underwent measurements of physical activity with activity monitors at least 12 months after surgery.Results were compared with findings from 22 healthy, age- and gender-matched control subjects.
esults: Substantial and statistically significant differences in daily activity were observed. Steps, standingtime and moderate-intensity activity of lung recipients were reduced by 42%, 29% and 66%,respectively, relative to controls. Daily sedentary time was increased by 30%. Daily steps correlatedwith self-reported physical functioning (r � 0.81), 6-minute walk distance (r � 0.68), quadricepsforce (r � 0.66) and maximum workload (r � 0.63).
onclusions: This study has shown for the first time that daily activity is substantially reduced after lung transplantationand related to measures of physical fitness and health-related quality of life. Future studies need toexamine whether physical activity can be modified to improve functional recovery after lungtransplantation. J Heart Lung Transplant 2009;28:572–8. Copyright © 2009 by the International Society
for Heart and Lung Transplantation.eiet
ar(otbpotttw
rhIeo
MS
Or
ung transplantation (LTx) has gained widespread ac-eptance as a therapeutic option for end-stage lungisease.1 Survival rates have improved in successiveears with a current worldwide survival half-life ofbout 5 years.2
Patients have continued to report limitations in phys-cal functioning despite substantial improvements ineneral quality of life.3,4 Persisting limitations in exer-ise capacity and skeletal muscle weakness have alsoeen reported.5–11 Inactivity prior to transplantation12
nd resulting pre-transplant deconditioning6,13 are likelyo influence functional recovery after surgery. Repeated
rom the aDepartment of Rehabilitation Sciences, Katholieke Univer-iteit Leuven, and bRespiratory Rehabilitation and Respiratory Divi-ion, University Hospital Leuven, Leuven, Belgium; and cDepartmentf Physiotherapy, Universidade Estadual de Londrina, Londrina, Brazil.Submitted October 10, 2008; revised March 4, 2009; acceptedarch 6, 2009.
upported by the International Society for Heart and Lung Transplanta-ion Nursing and Social Science Award 2005 a grant from the Researchoundation Flanders Project G0523.06 and KAN 1.5.139.06N, and a grantrom the Brazilian National Council for Scientific and Technologicalevelopment (CNPq, Brazil) to F.P.Reprint requests: Thierry Troosters, PT, PhD, Department of Rehabil-
tation Sciences, Katholieke Universiteit Leuven, Tervuursevest 101,euven 3000, Belgium. Telephone: �32-16-347107. Fax: �32-347126.-mail: [email protected] © 2009 by the International Society for Heart and Lungransplantation. 1053-2498/09/$–see front matter. doi:10.1016/
f.healun.2009.03.007
72
pisodes of infection and rejection, use of anti-nflammatory and immunosuppressive drugs and a sed-ntary lifestyle are possible post-transplant contributorso limitations in physical fitness.5,6,9
Daily physical activity (PA) has been studied in heartnd liver recipients, but with ambiguous results. Heartecipients were classified as either “moderately active”1,100 kcal/week spent in recreational activities), basedn self-report,14 or very sedentary, based on accelerome-er measurements.15 No statistically significant differencesetween liver recipients and healthy controls were re-orted for accelerometer measurements of daily PA.16 Tour knowledge, no data on daily PA after lung transplan-ation have been published. Given this absence of data andhe contradictory findings in other study populations afterransplantation, the purpose of the present investigationas to objectively measure daily PA in lung recipients.The main research questions were: (1) Do stable lung
ecipients reach levels of daily PA comparable to those ofealthy, age-matched control subjects 1 year after LTx? (2)s daily PA in lung recipients related to measures ofxercise capacity, muscle force and health-related qualityf life?
ETHODSubjects
ur experimental protocol was approved by the ethicseview board of the University Hospital Leuven. Criteria
or participation in our study were: (1) age �40 years;
(iacmoifgsdt
A
Dasiw
tadwassisDs
uimmbfl(pmemwTrbop
H
Tttl
adgupa
O
Pti(p
S
GSuasssmp
RS
EsbdFFmn(hTbl
w(d(hplTtts0N
The Journal of Heart and Lung Transplantation Langer et al. 573Volume 28, Number 6
2) status �12 months post-transplantation; and (3) nonfection or acute allograft rejection requiring hospitaldmission within the preceding 30 days. Exclusionriteria were: (1) retransplantation; (2) heart–lung orultiple-organ transplantation; and (3) signs of bronchi-
litis obliterans syndrome (Stage �1), as defined by thenitial diagnostic criteria from the International Societyor Heart and Lung Transplantation (ISHLT).17 Age- andender-matched volunteers were included as controlubjects. Healthy individuals were all relatives of stu-ents from the Department of Rehabilitation Sciences athe Katholieke Universiteit Leuven.
ssessment of Daily Physical Activity
aily PA was assessed with two activity monitors. Bothctivity monitors were worn simultaneously on 4 con-ecutive days during 12 waking hours. Subjects werenstructed not to change their daily routine while
earing the devices.The DynaPort activity monitor (DynaPort) quantifies
ime spent in different postures (i.e., standing, sittingnd lying), time spent walking and daily steps. Aetailed description of the device can be found else-here.18 In previous validation studies the device was
ble to accurately detect postures and movements inlowly moving subjects.12,19 Daily walking time, dailyteps (computed from walking time and average walk-ng frequency), standing time and sedentary time (timepent lying and sitting) were the parameters from theynaPort that were chosen to characterize daily PA of
tudy subjects.The SenseWear Pro activity monitor (Armband) was
sed to estimate energy expenditure during daily activ-ties. The Armband integrates monitoring of body move-
ent by a biaxial accelerometer with non-invasive sensorseasuring the following physical parameters: changes in
ody temperature; near-body ambient temperature; heatux; and galvanic skin resistance. The provided softwareSENSEWEAR Professional, version 6.0.2.1444) uses pro-rietary algorithms to provide minute-by-minute esti-ates of energy expenditure, expressed in metabolic
quivalents (METs). Time spent in activities of at leastoderate intensity was used as main outcome. Theseere defined as activities requiring at least 3 METs.hirty minutes of moderately intense PA are known toesult in health benefits when performed on a dailyasis.20 Energy estimates of the Armband were previ-usly validated in patients with chronic obstructiveulmonary disease (COPD).21
ealth-related Quality of Life
he Medical Outcomes Study Short Form (SF-36) ques-ionnaire was used to evaluate self-reported domains ofhe health-related quality of life (HRQoL) measure in
ung recipients.22 The SF-36 questionnaire was not mdministered in healthy control subjects. Instead, stan-ard reference scores23 and population norms from theeneral Dutch population were used as reference val-es.24 The SF-36 was previously validated in COPDatients25 and has been used in patients before andfter LTx.3,4,26,27
ther Measurements
ulmonary function, maximal inspiratory and expira-ory pressures, quadriceps force, handgrip force, max-mal exercise capacity and 6-minute walking distance6MWD) were assessed in our laboratory according torotocols described previously in more detail.12
tatistical Methods
roup means were compared using unpaired t-tests.F-36 domain scores were compared with Dutch pop-lation norms,24 derived from a sample with similar agend gender distribution. Physical and mental SF-36ummary scores were calculated for comparison withtandard reference values with a mean of 50 and atandard deviation (SD) of 10.23 Pearson product-mo-ent correlation coefficients were calculated betweenarameters of PA, physical fitness and HRQoL.
ESULTSubjects
ighty-nine patients underwent surgery at the Univer-ity Hospital Leuven between March 2005 and Decem-er 2006. Seventy-seven of these patients were still aliveuring the inclusion period between January 2007 andebruary 2008. Forty-seven of them met the age criteria.ive additional patients were excluded because of noteeting other inclusion criteria. Pre-transplant diag-oses of the 42 eligible patients were lung emphyseman � 30), interstitial lung disease (n � 7), pulmonaryypertension (n � 3) and bronchiectasis (n � 2).wenty patients were not included in our sampleecause they either refused to participate (n � 7) or
ived far away from our center (n � 13).Twenty-two patients agreed to participate and under-ent measurements at an average of 15.5 months
range 12 to 24 months) after surgery. Pre-operativeiagnoses of included patients were emphyseman � 18), interstitial lung disease (n � 2), pulmonaryypertension (n � 1) and bronchiectasis (n � 1). Sevenatients received single-lung and 15 received bilateral
ung grafts. All lung recipients were clinically stable.hree of 22 patients followed a structured rehabilita-
ion program at the University Hospital Leuven afterransplantation. All patients received a daily dose ofteroids (methylprednisolone) ranging between 0.2 and.4 mg/kg/day during the first year after transplantation.one had returned to work by the time of their
easurements. Twenty-two healthy, age- and gender-
mtr
D
Ntatvejt3�tm(��mmti(tc[0(pt9
H
STDrdncsmv
M
Dspcgf
FdctcaM
T
LC
B
T
S
S
D
574 Langer et al. The Journal of Heart and Lung TransplantationJune 2009
atched control subjects were included. All were re-ired by the time of their measurements. Anthropomet-ic data of study subjects are shown in Table 1.
aily Physical Activity
umber of steps, standing time, sedentary time andime spent in moderately intense PA of study subjectsre shown in Figure 1. Data of transplant recipients inhese plots are expressed as a percentage of the averagealue of healthy controls. Only a few lung recipientsxceeded average levels of PA in healthy control sub-ects. Average daily step count was 4,977 (SD 2,332) inhe transplant group as compared with 8,645 (SD,491) in healthy controls (difference between means:2,636 steps [�42%]; 95% confidence interval: �5,475
o �1,861; p � 0.000). Daily walking time averaged 55inutes (SD 25) in the transplant group and 81 minutes
SD 26) in healthy controls (difference between means:26 minutes [�32%]; 95% confidence interval: �41 to10; p � 0.002). Daily standing time averaged 201inutes (SD 76) in the transplant group and 283inutes (SD 99) in healthy controls (difference be-
ween means: �82 minutes [�29%]; 95% confidencenterval: �135 to �29; p � 0.004). Daily sedentary timelying or sitting averaged 447 minutes [SD 76] in theransplant group and 358 minutes [SD 112] in healthyontrols; difference between means: 104 minutes�30%]; 95% confidence interval: 40 to 168; p �.002). Daily time spent in moderately intense activity�3 METs) averaged 67 minutes (SD 61) in the trans-lant group and 154 minutes (SD 96) in healthy con-rols (difference between means: �87 minutes [�66%];5% confidence interval: �136 to �38; p � 0.001).
ealth-related Quality of Life
cores on the 8 subscales of the SF-36 are shown inable 2 in comparison with reference values from theutch general population.24 Domains of the SF-36
eflecting physical health components were all re-uced, whereas items reflecting mental health compo-ents were similar to reference values. The mentalomponent summary score (MCS) of the SF-36 waslightly higher, whereas the physical component sum-ary score (PCS) was lower than standard reference
alues.23
able 1. Anthropometric Characteristics of Study Subjects
Gender(M/F)
Age(y)
Height(cm)
Weight(kg)
FEV1
(%pred)
ung recipients 12/10 59 � 5 168 � 7 66 � 14 79 � 18a
ontrols 12/10 58 � 7 169 � 8 66 � 10 110 � 17
MI, body mass index; FEV , forced expiratory volume in 1 second.
1aStatistically significant difference between groups (p � 0.01).uscle Force and Exercise Capacity
ata on muscle force and exercise capacity of studyubjects are presented in Table 3. These indicators ofhysical fitness were all reduced in lung recipientsompared with healthy controls. Differences betweenroups were not statistically significant for handgriporce (�10%), maximal inspiratory pressure (�16%)
igure 1. Daily physical activity in lung recipients (Post-LTX) stan-ardized as a percentage of the average value (� 100%) in healthyontrols (Healthy). Abbreviations: DynaPort � DynaPort activity moni-or; Armband � SenseWear armband; (A) Step Count � daily stepount; (B) Standing � daily standing time; (C) Sedentary � daily sittingnd lying time; (D) MIPA � moderately intense physical activity (�3ETs). *Statistically significant difference between groups (p � 0.01).
able 2. HRQoL Scores From the SF-36 for Lung Recipients
Lung recipients Reference valuea
F-36 scalesb
Physical function 64.0 � 19.8 83.0Role—physical 68.8 � 33.5 76.4Bodily pain 69.2 � 22.5 74.9General health 59.3 � 23.9 70.7Vitality 64.4 � 17.5 68.6Social function 83.6 � 20.3 84.0Role—emotional 91.7 � 19.2 82.3Mental health 76.5 � 18.8 76.8
F-36 summary scalesc
Physical component (PCS) 42.8 � 11.2Mental component (MCS) 53.8 � 10.9
ata expressed as mean � SD.aDutch general population.25
bScore range: 0 to 100; higher scores indicate better HRQoL.cTransformed scores for comparison to general norm scores with mean �
SD � 50 � 10; higher scores indicate better HRQoL.24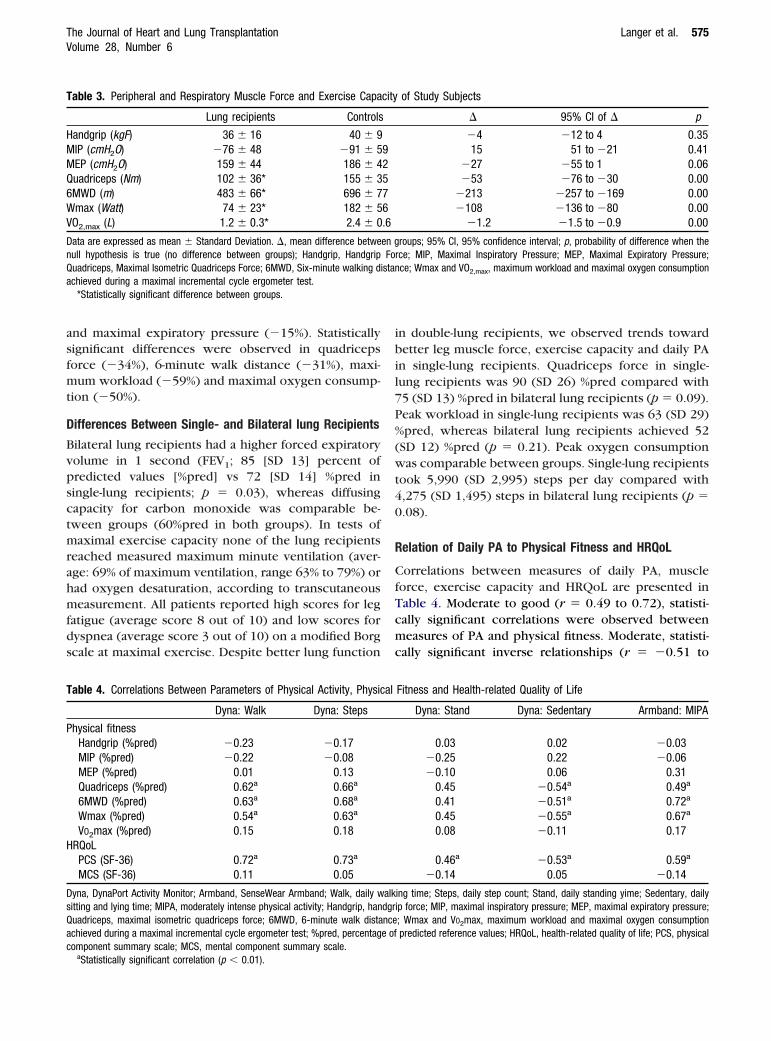
asfmt
D
Bvpsctmrahmfds
ibil7P%(wt40
R
CfTcmc
T
HMMQ6WV
DnQa
T
P
H
DsQac
The Journal of Heart and Lung Transplantation Langer et al. 575Volume 28, Number 6
nd maximal expiratory pressure (�15%). Statisticallyignificant differences were observed in quadricepsorce (�34%), 6-minute walk distance (�31%), maxi-um workload (�59%) and maximal oxygen consump-
ion (�50%).
ifferences Between Single- and Bilateral lung Recipients
ilateral lung recipients had a higher forced expiratoryolume in 1 second (FEV1; 85 [SD 13] percent ofredicted values [%pred] vs 72 [SD 14] %pred iningle-lung recipients; p � 0.03), whereas diffusingapacity for carbon monoxide was comparable be-ween groups (60%pred in both groups). In tests ofaximal exercise capacity none of the lung recipients
eached measured maximum minute ventilation (aver-ge: 69% of maximum ventilation, range 63% to 79%) orad oxygen desaturation, according to transcutaneouseasurement. All patients reported high scores for leg
atigue (average score 8 out of 10) and low scores foryspnea (average score 3 out of 10) on a modified Borgcale at maximal exercise. Despite better lung function
able 3. Peripheral and Respiratory Muscle Force and Exercise Capa
Lung recipients Controls
andgrip (kgF) 36 � 16 40 � 9IP (cmH2O) �76 � 48 �91 � 5EP (cmH2O) 159 � 44 186 � 4uadriceps (Nm) 102 � 36* 155 � 3MWD (m) 483 � 66* 696 � 7max (Watt) 74 � 23* 182 � 5
O2,max (L) 1.2 � 0.3* 2.4 � 0
ata are expressed as mean � Standard Deviation. �, mean difference betweull hypothesis is true (no difference between groups); Handgrip, Handgripuadriceps, Maximal Isometric Quadriceps Force; 6MWD, Six-minute walking dchieved during a maximal incremental cycle ergometer test.
*Statistically significant difference between groups.
able 4. Correlations Between Parameters of Physical Activity, Physic
Dyna: Walk Dyna: Steps
hysical fitnessHandgrip (%pred) �0.23 �0.17MIP (%pred) �0.22 �0.08MEP (%pred) 0.01 0.13Quadriceps (%pred) 0.62a 0.66a
6MWD (%pred) 0.63a 0.68a
Wmax (%pred) 0.54a 0.63a
VO2max (%pred) 0.15 0.18RQoLPCS (SF-36) 0.72a 0.73a
MCS (SF-36) 0.11 0.05
yna, DynaPort Activity Monitor; Armband, SenseWear Armband; Walk, daily witting and lying time; MIPA, moderately intense physical activity; Handgrip, hanuadriceps, maximal isometric quadriceps force; 6MWD, 6-minute walk distachieved during a maximal incremental cycle ergometer test; %pred, percentagomponent summary scale; MCS, mental component summary scale.
aStatistically significant correlation (p � 0.01).
n double-lung recipients, we observed trends towardetter leg muscle force, exercise capacity and daily PA
n single-lung recipients. Quadriceps force in single-ung recipients was 90 (SD 26) %pred compared with5 (SD 13) %pred in bilateral lung recipients (p � 0.09).eak workload in single-lung recipients was 63 (SD 29)pred, whereas bilateral lung recipients achieved 52
SD 12) %pred (p � 0.21). Peak oxygen consumptionas comparable between groups. Single-lung recipients
ook 5,990 (SD 2,995) steps per day compared with,275 (SD 1,495) steps in bilateral lung recipients (p �.08).
elation of Daily PA to Physical Fitness and HRQoL
orrelations between measures of daily PA, muscleorce, exercise capacity and HRQoL are presented inable 4. Moderate to good (r � 0.49 to 0.72), statisti-ally significant correlations were observed betweeneasures of PA and physical fitness. Moderate, statisti-
ally significant inverse relationships (r � �0.51 to
of Study Subjects
� 95% CI of � p
�4 �12 to 4 0.3515 51 to �21 0.41
�27 �55 to 1 0.06�53 �76 to �30 0.00
�213 �257 to �169 0.00�108 �136 to �80 0.00
�1.2 �1.5 to �0.9 0.00
roups; 95% CI, 95% confidence interval; p, probability of difference when therce; MIP, Maximal Inspiratory Pressure; MEP, Maximal Expiratory Pressure;ce; Wmax and VO2,max, maximum workload and maximal oxygen consumption
Fitness and Health-related Quality of Life
Dyna: Stand Dyna: Sedentary Armband: MIPA
0.03 0.02 �0.03�0.25 0.22 �0.06�0.10 0.06 0.31
0.45 �0.54a 0.49a
0.41 �0.51a 0.72a
0.45 �0.55a 0.67a
0.08 �0.11 0.17
0.46a �0.53a 0.59a
�0.14 0.05 �0.14
ing time; Steps, daily step count; Stand, daily standing yime; Sedentary, dailyip force; MIP, maximal inspiratory pressure; MEP, maximal expiratory pressure;; Wmax and VO2max, maximum workload and maximal oxygen consumptionpredicted reference values; HRQoL, health-related quality of life; PCS, physical
city
92576.6
en gFo
istan
al
alkdgrncee of

�fi
pTsPspof
rfe0s
D
TpOdisdsp
P
Tdtcd
thpacoaalg
mmslmarcat
R
Rcpatwcltiemtnmmai
PHsw
Fpt(m
576 Langer et al. The Journal of Heart and Lung TransplantationJune 2009
0.55) were found between parameters of physicaltness and daily time spent sedentary (sitting or lying).Domains of the SF-36 reflecting physical health com-
onents were most closely related to parameters of PA.his resulted in moderate to good (r � 0.46 to 0.73),tatistically significant relations between PA and theCS of the SF-36 (Table 4). A moderate inverse relation-hip (r � �0.53) between this domain of HRQoL and aarameter of inactivity (daily time spent sedentary) wasbserved. No statistically significant correlations wereound between the MCS and indicators of PA.
Representative scatterplots of statistically significantelations (all p � 0.01) between daily steps and physicalunctioning subscale of the SF-36 (r � 0.81), functionalxercise capacity (r � 0.68), quadriceps force (r �.66) and maximum workload (Wmax) (r � 0.63) arehown in Figure 2.
ISCUSSION
his study is the first controlled trial to investigatehysical inactivity in patients after lung transplantation.ur data show a significant reduction in the amount ofaily activities and a major reduction in moderately
ntense activities in stable lung allograft recipientstudied 1 year after transplantation. Higher levels ofaily activity were related to better preserved muscletrength, higher exercise capacity and fewer self-re-orted limitations in physical functioning.
igure 2. Scatterplots of correlations between daily steps and (A)hysical functioning (SF-36: 0 to 100, higher score � fewer limita-ions), (B) 6-minute walk distance (%pred), (C) quadriceps force%pred) and (D) maximum workload (%pred) during an incremental
maximal exercise test on a cycle ergometer.
hysical Activity in Organ Recipients
o our knowledge, no previous studies have assessedaily PA in lung allograft recipients. We found substan-ial (�29% to �66%), statistically significant reductionsompared with healthy controls for all parameters ofaily PA.Objectively measured data on daily PA in other
ransplant populations have been presented in liver andeart allograft recipients.15,16 Evangelista et al15 re-orted very low levels of daily activity in women fromcomparable age cohort after heart transplantation. Ac-
elerometer measures of PA were comparable to thosef cancer patients undergoing radiation therapy.28 Inddition, only 15% of patients reported to engage inctivities of at least moderate intensity. However, PAevels in this study were not compared with a controlroup.In their study, van den Berg-Emons et al16 objectivelyeasured daily PA with accelerometry-based activityonitors after liver transplantation. They found no
tatistically significant reductions in activity levels ofiver recipients in comparison with healthy, age-
atched control subjects (10.2% vs 12.6% dynamicctivities). They concluded that PA is not importantlyeduced in liver recipients. Limitations in exerciseapacity that have been reported in liver recipients arelso less severe than those after lung transplanta-ion.29,30
elation of PA to Physical Fitness and HRQoL
eductions in exercise capacity in lung recipients wereomparable to those noted in earlier studies.6,31 Theresence of muscle weakness in our sample is also inccordance with other data after lung transplanta-ion.9,32,33 Neither in single- nor bilateral lung recipientsas pulmonary function a limitation to maximal exer-
ise capacity. Pulmonary function was therefore mostikely not related to the capacity of performing dailyasks. Our data are in accordance with earlier findingsndicating that, even after single-lung transplantation,xercise capacity is primarily limited by peripheraluscle abnormalities rather than by ventilatory fac-
ors.34 Earlier studies showed that muscle groups wereot uniformly affected with more pronounced leguscle weakness.9,32 This supports the hypothesis thatuscle force is not only affected by anti-inflammatory
nd immunosuppressive drugs, but also by differencesn pre-transplant deconditioning and post-transplant PA.
Because this study was the first to objectively assessA in addition to muscle function, exercise capacity andRQoL, it is for the first time possible to study relation-
hips between these parameters. Higher levels of PAere consistently related to higher (nearly normal) leg
uscle strength, functional exercise capacity and self-
rtcpilbdAbtiroPoaiH
C
Fnbcw
lrlogap
L
Actdntnp
cyearlccta
P
LidH
tiMief
tlcFir
R
1
1
1
1
The Journal of Heart and Lung Transplantation Langer et al. 577Volume 28, Number 6
eported physical functioning (Figure 2). This can beaken as an indication that higher levels of daily PAould contribute to functional recovery after lung trans-lantation. Our cross-sectional data, however, must be
nterpreted with caution. Instead of causing exerciseimitations and impaired quality of life, PA may also onlye an intermediate variable that in turn is largelyetermined by various pre- and post-transplant factors.ssumptions about possible cause–effect relationshipsased on cross-sectional data therefore remain specula-ive. Our findings are in line with those of Painter et al35
n their study of liver transplant recipients. After cor-ection for several post-transplant confounders theybserved a strong relation between (self-reported) dailyA and self-reported physical functioning. The absencef a statistically significant relation between daily PAnd the MCS of the SF-36 is in support of earlier findingsndicating that the physical and mental domains ofRQoL are influenced by different factors.36,37
linical Implications
rom our data it becomes clear that most patients doot return to a normally active lifestyle after LTx. Weelieve that more attention should be paid to thislinically relevant finding in the treatment of patientsho have undergone this procedure.Different strategies could be applied to increase PA in
ung recipients. Several studies already showed positiveesults of structured, supervised exercise training afterung transplantation.38–41 However, the conclusivenessf these studies was limited by the absence of a controlroup. Behavioral lifestyle activity counseling could benother possibility for modifying daily PA after trans-lantation.20
imitations and External Validity
limitation lies within the cross-sectional nature of theollected data. It was not possible to take into accounthe effects of different degrees of pre-transplant PA andeconditioning because PA and physical fitness wereot assessed before transplantation. Although all pa-ients were stable at the time of inclusion we can alsoot exclude the possible negative effects of earlierost-transplant episodes of infection or rejection.The present study has focused particularly on clini-
ally stable older patients (�40 years). Patients �40ears of age (i.e., all patients with cystic fibrosis) werexcluded due to presumably different recovery of dailyctivities (e.g., return to work). It is therefore likely thatecorded activity profiles are only representative forung recipients in this age cohort approximating theseharacteristics. Younger recipients (e.g., patients withystic fibrosis) are probably more active, whereas pa-ients with early development of bronchiolitis obliter-
ns syndrome would be expected to be less active.erspectives
ongitudinal studies or interventional studies (random-zed, controlled trials) are needed to study in greateretail the relationship between PA, physical fitness andRQoL after lung transplantation.Longitudinal studies should assess PA levels of pa-
ients before transplantation to determine how changesn PA after transplantation affect functional recovery.
odifying physical activity as an independent variablen interventional studies would provide the strongestvidence for a causal relationship between PA andunctional recovery after lung transplantation.
In conclusion, this study has shown for the first timehat daily physical activity is substantially reduced afterung transplantation and related to measures of exerciseapacity, muscle force and health-related quality of life.uture studies are needed to determine whether phys-cal activity can be modified to improve functionalecovery after lung transplantation.
EFERENCES
1. Arcasoy SM, Kotloff RM. Lung transplantation. N Engl J Med1999;340:1081–91.
2. Trulock EP, Christie JD, Edwards LB, et al. Registry of theInternational Society for Heart and Lung Transplantation: twenty-fourth official adult lung and heart–lung transplantation report—2007. J Heart Lung Transplant 2007;26:782–95.
3. Myaskovsky L, Dew MA, McNulty ML, et al. Trajectories of changein quality of life in 12-month survivors of lung or heart transplant.Am J Transplant 2006;6:1939–47.
4. Smeritschnig B, Jaksch P, Kocher A, et al. Quality of life after lungtransplantation: a cross-sectional study. J Heart Lung Transplant2005;24:474–80.
5. Lands LC, Smountas AA, Mesiano G, et al. Maximal exercisecapacity and peripheral skeletal muscle function following lungtransplantation. J Heart Lung Transplant 1999;18:113–20.
6. Schwaiblmair M, Reichenspurner H, Muller C, et al. Cardiopul-monary exercise testing before and after lung and heart–lungtransplantation. Am J Respir Crit Care Med 1999;159:1277–83.
7. Ambrosino N, Bruschi C, Callegari G, et al. Time course ofexercise capacity, skeletal and respiratory muscle performanceafter heart–lung transplantation. Eur Respir J 1996;9:1508–14.
8. Krieger AC, Szidon P, Kesten S. Skeletal muscle dysfunction inlung transplantation. J Heart Lung Transplant 2000;19:392–400.
9. Pantoja JG, Andrade FH, Stokic DS, et al. Respiratory and limbmuscle function in lung allograft recipients. Am J Respir Crit CareMed 1999;160:1205–11.
0. Studer SM, Levy RD, McNeil K, et al. Lung transplant outcomes: areview of survival, graft function, physiology, health-related qualityof life and cost-effectiveness. Eur Respir J 2004;24:674–85.
1. Wang XN, Williams TJ, McKenna MJ, et al. Skeletal muscleoxidative capacity, fiber type, and metabolites after lung trans-plantation. Am J Respir Crit Care Med 1999;160:57–63.
2. Pitta F, Troosters T, Spruit MA, et al. Characteristics of physicalactivities in daily life in chronic obstructive pulmonary disease.Am J Respir Crit Care Med 2005;171:972–7.
3. Van der Woude BT, Kropmans TJB, et al. Peripheral muscle forceand exercise capacity in lung transplant candidates. Int J Rehabil
Res 2002;25:351–5.
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
578 Langer et al. The Journal of Heart and Lung TransplantationJune 2009
4. Myers J, Gullestad L, Bellin D, et al. Physical activity patterns andexercise performance in cardiac transplant recipients. J Cardiop-ulm Rehabil 2003;23:100–6.
5. Evangelista LS, Dracup K, Doering LV, et al. Physical activity patternsin heart transplant women. J Cardiovasc Nurs 2004;20:334–9.
6. van den Berg-Emons R, Kazemier G, van Ginneken B, et al.Fatigue, level of everyday physical activity and quality of life afterliver transplantation. J Rehabil Med 2006;38:124–9.
7. Estenne M, Maurer JR, Boehler A, et al. Bronchiolitis obliteranssyndrome 2001: an update of the diagnostic criteria. J Heart LungTransplant 2002;21:297–310.
8. Pitta F, Troosters T, Probst VS, et al. Quantifying physical activityin daily life with questionnaires and motion sensors in COPD. EurRespir J 2006;27:1040–55.
9. Pitta F, Troosters T, Spruit MA, et al. Activity monitoring forassessment of physical activities in daily life in patients withchronic obstructive pulmonary disease. Arch Phys Med Rehabil2005;86:1979–85.
0. Haskell WL, Lee IM, Pate RR, et al. Physical activity and publichealth: updated recommendation for adults from the AmericanCollege of Sports Medicine and the American Heart Association.Circulation 2007;116:1081–93.
1. Patel SA, Benzo RP, Slivka WA, et al. Activity monitoring andenergy expenditure in COPD patients: a validation study. COPD2007;4:107–12.
2. Ware JE Jr, Sherbourne CD. The MOS 36-item Short-Form HealthSurvey (SF-36). I. Conceptual framework and item selection. MedCare 1992;30:473–83.
3. Ware J, Snow K, Kosinski M. SF-36 Health survey: manual andinterpretation guide. 2000.
4. Aaronson NK, Muller M, Cohen PD, et al. Translation, validation,and norming of the Dutch language version of the SF-36 HealthSurvey in community and chronic disease populations. J ClinEpidemiol 1998;51:1055–68.
5. Mahler DA, Mackowiak JI. Evaluation of the Short-Form 36-itemquestionnaire to measure health-related quality of life in patientswith COPD. Chest 1995;107:1585–9.
6. Limbos MM, Joyce DP, Chan CK, et al. Psychological functioning andquality of life in lung transplant candidates and recipients. Chest2000;118:408–16.
7. Stavem K, Bjortuft O, Lund MB, et al. Health-related quality of life in lungtransplant candidates and recipients. Respiration 2000;67:159–65.
8. Sarna L, Conde F. Physical activity and fatigue during radiationtherapy: a pilot study using actigraph monitors. Oncol Nurs
Forum 2001;28:1043–6.9. Beyer N, Aadahl M, Strange B, et al. Improved physical perfor-mance after orthotopic liver transplantation. Liver TransplantSurg 1999;5:301–9.
0. van Ginneken BT, van den Berg-Emons RJ, Kazemier G, et al.Physical fitness, fatigue, and quality of life after liver transplanta-tion. Eur J Appl Physiol 2007;100:345–53.
1. Williams TJ, Patterson GA, McClean PA, et al. Maximal exercisetesting in single and double lung transplant recipients. Am RevRespir Dis 1992;145:101–5.
2. Pinet C, Scillia P, Cassart M, et al. Preferential reduction ofquadriceps over respiratory muscle strength and bulk afterlung transplantation for cystic fibrosis. Thorax 2004;59:783–9.
3. Reinsma GD, ten Hacken NHT, Grevink RG, et al. Limiting factorsof exercise performance 1 year after lung transplantation. J HeartLung Transplant 2006;25:1310–6.
4. Gibbons WJ, Levine SM, Bryan CL, et al. Cardiopulmonaryexercise responses after single lung transplantation for severeobstructive lung disease. Chest 1991;100:106–11.
5. Painter P, Krasnoff J, Paul SM, et al. Physical activity andhealth-related quality of life in liver transplant recipients. LiverTransplant 2001;7:213–9.
6. Vermeulen KM, van der Bij BW, Erasmus ME, et al. Long-termhealth-related quality of life after lung transplantation: differentpredictors for different dimensions. J Heart Lung Transplant2007;26:188–93.
7. Vasiliadis HM, Collet JP, Poirier C. Health-related quality-of-lifedeterminants in lung transplantation. J Heart Lung Transplant2006;25:226–33.
8. Guerrero K, Wuyam B, Mezin P, et al. Functional coupling ofadenine nucleotide translocase and mitochondrial creatine kinaseis enhanced after exercise training in lung transplant skeletalmuscle. Am J Physiol-Regul Integr Comp Physiol 2005;289:R1144–54.
9. Maury G, Langer D, Verleden G, et al. Skeletal muscle forceand functional exercise tolerance before and after lungtransplantation: a cohort study. Am J Transplant 2008;8:1275– 81.
0. Mitchell MJ, Baz MA, Fulton MN, et al. Resistance trainingprevents vertebral osteoporosis in lung transplant recipients.Transplantation 2003;76:557–62.
1. Stiebellehner L, Quittan M, End A, et al. Aerobic endurancetraining program improves exercise performance in lung trans-
plant recipients. Chest 1998;113:906–12.



















