
Statins for early stage chronic kidney disease: an overview of reviews

Introduction
Hypercholesterolemia constitutes oneof the main risk factors of atheroscle-rosis. The atherosclerotic process ispreceded by the endothelial dysfunc-tion and by the thickening of thebasal membrane of the ocular vessels(Trivino et al. 2006; Salazar et al.2007). In the initial phases, VCAM-1and ICAM-1 catch circulating mono-nuclear cells which migrate to thesubendothelial space, where theytransform into macrophages and theninto foam cells (Wu et al. 1995;Vijayagopal & Glancy 1996; Ronget al. 1999). Foam cells underneaththe basal membrane are responsiblefor microatheroma plaque formationon large vessels and, together withcollagen increase, for arteriolar hyali-nosis on medium- and small-vessellayer. In addition, activation ofmacrophages and vascular smooth-muscle cells (VSMC) induces a remod-elling of the extracellular matrix (Ross1993; Matthys et al. 1997; Oorni et al.2000; Salazar et al. 2007). All thesechanges could contribute to a reduc-tion in the vascular tone and lumen.
The factors causing ischaemiadescribed earlier could be related tosome of the mechanisms involved inthe development of age-related macular
Low-dosage statins reducechoroidal damage inhypercholesterolemic rabbits
Blanca Rojas,1 Ana I. Ramırez,1 Juan J. Salazar,1 Rosa de Hoz,1
Alma Redondo,1 Rafaela Raposo,2 Teresa Mendez,3
Teresa Tejerina,4 Alberto Trivino1 and Jose M. Ramırez1
1Institute for Ophthalmic Research, Ramon Castroviejo, Complutense University,Madrid, Spain2Department of Physiology, School of Pharmacy, Complutense University, Madrid,Spain3Department of Biochemistry and Molecular Biology II, School of Pharmacy,
Complutense University, Madrid, Spain4Department of Pharmacology, School of Medicine, Complutense University,Madrid, Spain
ABSTRACT.
Purpose: To describe the ultrastructural changes in the choroid of long-term
hypercholesterolemic rabbits after a low-dosage statin treatment and to evalu-
ate some pleiotropic effects of these drugs on the morphology of endothelial
cells (EC) and vascular smooth-muscle cells (VSMC).
Methods: New Zealand rabbits were divided into three groups: G0, fed a stan-
dard diet; G1, fed a 0.5% cholesterol-enriched diet for 8 months and G2, fed
a 0.5% cholesterol-enriched diet for 8 months plus administration of fluvasta-
tin sodium or pravastatin sodium at a dose of 2 mg ⁄Kg ⁄day each. Eyes were
processed for transmission-electron microscopy.
Results: G1 had a lipid build-up at the suprachoroidea that compressed the
vascular layers with the lumens of the vessels to the point of collapse in some
instances. By contrast, G2 underwent a substantial decrease in suprachoroidal
foam cells and of lipids in the vascular layers while the vascular lumens were
normal. The preservation of cytoplasmic organelles, caveolar system and other
ultrastructural features of EC and VSMC in G2 contrasted with the numerous
signs of necrosis observed in G1. Bruch’s membrane (BM) in G2 contained
fewer lipids and more collagen than in G1.
Conclusion: Treatment with a low dosage of fluvastatin sodium or pravastatin
sodium reduced the lipid build-up as well as the macrophages in the choroid
and restored the vascular lumens of choroidal vessels independently of the cho-
lesterol effect. The normal ultrastructural features of choroidal EC and
VSMC in statin-treated animals suggest that the endothelial function is pre-
served and the ischaemia reduced.
Key words: cholesterol-fed rabbits – choriocapillaris – choroid – electron microscopy – ischaemia –
statins
Acta Ophthalmol.ª 2010 The Authors
Journal compilation ª 2010 Acta Ophthalmol
doi: 10.1111/j.1755-3768.2009.01829.x
Acta Ophthalmologica 2010
1

degeneration (AMD), for which thepathogenesis is still partially unknowntoday.
Among data supporting the impor-tance of cholesterol in the pathogene-sis of AMD are the presence ofcholesterol in drusen (Johnson et al.2001), deposits of lipids in the Bruch’smembrane (BM) and the capacity ofthe retinal pigment epithelium (RPE)to synthesize cholesterol (Malek et al.2003). Current available data areinsufficient to conclude that lipid-low-ering agents, including statins, haveany role in preventing or delaying theonset or progression of AMD (Chuoet al. 2007; Gehlbach et al. 2009). Onthe other hand, clinically significanteffects derived from the use of lipid-lowering drugs cannot be ruled out(Chuo et al. 2007), and whether sub-groups of patients with specific formsof AMD (particularly choroidal neo-vascularization) benefit from statintherapy remains a possibility (Smeethet al. 2005). Epidemiologic, geneticand pathological evidence has showna number of risk factors shared byAMD and atherosclerosis, leading tosuggestions that statins, which areknown to be beneficial in patientswith atherosclerotic disease and hyper-lipidemia, may also exert protectiveeffects in AMD (Guymer et al. 2005;Gehlbach et al. 2009). In addition,some studies have shown the benefitsof using hypolipemic drug therapy todiminish the risk of having AMD(Zambarakji et al. 2006; Tan et al.2006; McGwin et al. 2005).
Statins are selective inhibitors of 3-hydroxy-3-methyl-glutaryl-CoA (HMG-CoA) reductase, which decrease thebiosynthesis of cholesterol and therebyreduce serum cholesterol levels in ani-mals and humans (Kurokawa et al.1995; Song et al. 2005). In fact, theinhibitors of the HMG-CoA reduc-tase, which are responsible for theconversion of HMG-CoA to mevalo-nate a rate-limiting step in cholesterolbiosynthesis, have been demonstratednot only to reduce the morbidity andmortality in human arterial coronarydisease but also to induce atheroscle-rosis regression (Mitani & Kimura2000). It bears noting that statinscould be beneficial not only for theirlipid-lowering properties but for theirother effects referred to as pleiotropic—that is, their capacity to restoreendothelial function, to stabilize ath-
erosclerotic plaque or to diminishoxidative stress and vascular inflam-mation (Mitani & Kimura 2000; Hallet al. 2001; McCarty et al. 2001;McGwin et al. 2003; McGwin & Ows-ley 2007; Yamada et al. 2007). Sucheffects have been demonstrated in rab-bits fed cholesterol at a dose insuffi-cient to reduce plasma-cholesterollevels (Mitani & Kimura 2000; Riki-take et al. 2001).
Previous studies conducted in ourlaboratory have revealed that highcholesterol levels were responsible fora chronic ischaemia in the retina andchoroid of rabbits (Trivino et al. 2006;Salazar et al. 2007). This ischaemiawas secondary to lipid build-up in thesuprachoroidea, changes in the vascu-lar endothelium and the thickening ofthe BM resulting from the deposit oflipids. In these studies, we reportedthat the normalization of plasma-lipidlevels in hypercholesterolemic rabbitsdid not ameliorate the choroidal andretinal changes induced by hyperlipid-emia. As a result of these observa-tions, we studied by considered tostudy the cholesterol-independenteffect of statins, referred to as pleio-tropic effects, on hypercholesterolemicrabbits. The aim of the present workis to demonstrate that in an experi-mental model of long-term hypercho-lesterolemia in rabbits, a dose ofstatins with a minimal lipid-loweringeffect can ameliorate the ultrastructur-al damage of the vascular structuresof the choroid and BM.
Materials and Methods
Twenty-six male adult New Zealandrabbits weighing 2.5 ± 0.5 Kg werehoused separately in cages in an air-conditioned room with a 12-h light ⁄dark cycle. All animals were fed rab-bit-maintenance diet (carbohydrates[N.F.E.] 50%, fibres 15.5%, proteins13.5%, moisture 11%, minerals 7%and lipids 3%; Panlab S.L. Barcelona,Spain) at least 7 days before thebeginning of the experiment andallowed ad libitum access to water.The animals were divided into threegroups: control group (G0; n = 10),fed a rabbit-maintenance diet for 8months; hypercholesterolemic rabbits(G1; n = 8), fed a rabbit-maintenancediet enriched with 0.5% cholesterol(U.A.R., Paris, France) for 8 months;statin group (G2; n = 8), fed a rab-
bit standard diet enriched with 0.5%cholesterol (U.A.R., Paris, France) plusadministration of fluvastatin sodium(Novartis; Farmaceutica, Barcelona,Spain) at a dose of 2 mg ⁄Kg ⁄day(G2A; n = 4) or pravastatin sodium(Bristol-Myers Squibb, Madrid, Spain)at a dose of 2 mg ⁄Kg ⁄day (G2B;n = 4) for 8 months.
Diet consumption was checked daily.Weight was monitored at the beginningof the experiment and monthly there-after. The same schedule was used tomonitor serum values of total choles-terol and triglycerides (Table 1). Forthis purpose, blood samples were takenfrom the marginal vein of the ear andanalysed by a colorimetric reactionwith a commercially available kit(BioMerieux, France). All procedureswere conducted in accordance withAssociation for Research in Vision andOphthalmology Statement for the Useof Animals in Ophthalmic and VisionResearch.
Two rabbits from the hypercholes-terolemic group (G1) and one rabbitfrom the pravastatin group (G2A) diedas a result of a cutaneous infection dur-ing the course of the experiment.
Animals were anaesthetized withsodium thiopentotal intravenouslyinjected and perfused through thecommon left carotid trunk with 2%glutaraldehyde in 0.1 m phosphatebuffer (PB), pH 7.4. For each animal,one of the eyes was used for electronmicroscopy (n = 23). To minimize tis-sue alterations post-mortem, eyes wereenucleated immediately after finishingthe intravenous perfusion and immedi-ately immersed for 5 hr in the samefixative at 4�C. After washing in 0.1 m
PB, the wall of the posterior segment
Table 1. Weights, total cholesterol and tri-
glyceride serum values at the end of the
experiment.
Group Mean ± SEM p*
Weight (Kg) G1 3.920 ± 0.38 NS
G2 3.957 ± 0.28
Cholesterol G1 1061.00 ± 358 NS
G2 968.00 ± 162
Triglycerides G1 296.67 ± 253 NS
G2 264.14 ± 271
* Mann–Whitney test.
NS = Nonsignificant; G1 (n = 6) (0.5%
cholesterol-enriched diet. No treatment); G2
(n = 7) [0.5% cholesterol-enriched diet +
fluvastatin sodium or pravastatin sodium
(2 mg ⁄Kg ⁄ day each)].
Acta Ophthalmologica 2010
2
of the eyes was cut into small piecescomprising all the regions of the eyewall. These fragments were refixed in1% osmium tetroxide in 0.1 m PB for2 hr at 4�C. The tissues were thendehydrated in ascending series of ace-tones and embedded in araldite. Thesemi-thin sections (0.5 lm) werestained with toluidine blue, and afterselection, the blocks were furthertrimmed for ultramicrotomy (ReichertOM-V3 ultramicrotome, Wetzlar,Germany). The thin sections werecontrasted with uranyl acetate andlead citrate, and examined by trans-mission-electron microscopy (TEM;Zeiss 902 electron microscope, Ober-kochen, Germany).
We evaluated the effect of statins onthe choroids by measuring the thick-ness of individual choroidal layers. Thethickness was measured at 10· for thesclera-suprachoroidea complex andvascular layers and 63· for BM. Thequantitative analysis was made in sixanimals from each study group (G0,G1, G2). For each animal, we mea-sured six retinal sections of the medul-lated nerve-fibre region (MNFR) andsix retinal sections of the periphery. Oneach section, three nonadjacent mea-surements were performed.
Data for statistical analysis wereintroduced and processed in aspss 15.0 (comprehensive statisticalsoftware; SPSS Incª, Chicago, IL,USA). The Mann–Whitney U test wasused to analyse the data of weightsand serum-lipids values. For choroi-dal thickness, differences in meanswere analysed using an anova and apost hoc Bonferroni test. A value ofp < 0.05 was considered statisticallysignificant.
Results
Acceptance of the cholesterol-supple-mented diet was rapid, with no majordifferences among the groups regard-ing daily consumption of the diet.Plasma-lipid levels did not statisti-cally differ between statin-treated and-untreated animals. Similarly, no sta-tistical differences were found for theanimal weights (Table 1).
Given that no substantial differ-ences were detected in ultrastructuraland morphological features of thechoroid between the statins analysed,the results of groups G2A and G2Bare described together as G2.
Light microscopy: choroidal thickness
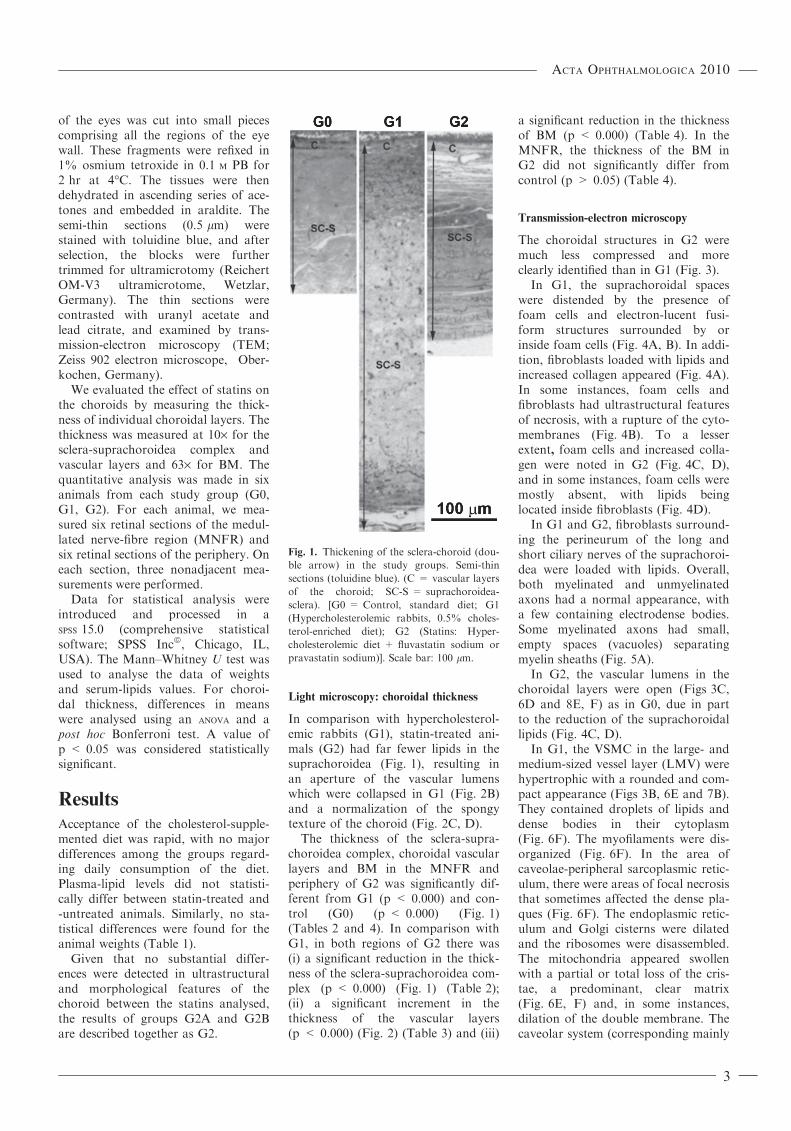
In comparison with hypercholesterol-emic rabbits (G1), statin-treated ani-mals (G2) had far fewer lipids in thesuprachoroidea (Fig. 1), resulting inan aperture of the vascular lumenswhich were collapsed in G1 (Fig. 2B)and a normalization of the spongytexture of the choroid (Fig. 2C, D).
The thickness of the sclera-supra-choroidea complex, choroidal vascularlayers and BM in the MNFR andperiphery of G2 was significantly dif-ferent from G1 (p < 0.000) and con-trol (G0) (p < 0.000) (Fig. 1)(Tables 2 and 4). In comparison withG1, in both regions of G2 there was(i) a significant reduction in the thick-ness of the sclera-suprachoroidea com-plex (p < 0.000) (Fig. 1) (Table 2);(ii) a significant increment in thethickness of the vascular layers(p < 0.000) (Fig. 2) (Table 3) and (iii)
a significant reduction in the thicknessof BM (p < 0.000) (Table 4). In theMNFR, the thickness of the BM inG2 did not significantly differ fromcontrol (p > 0.05) (Table 4).
Transmission-electron microscopy
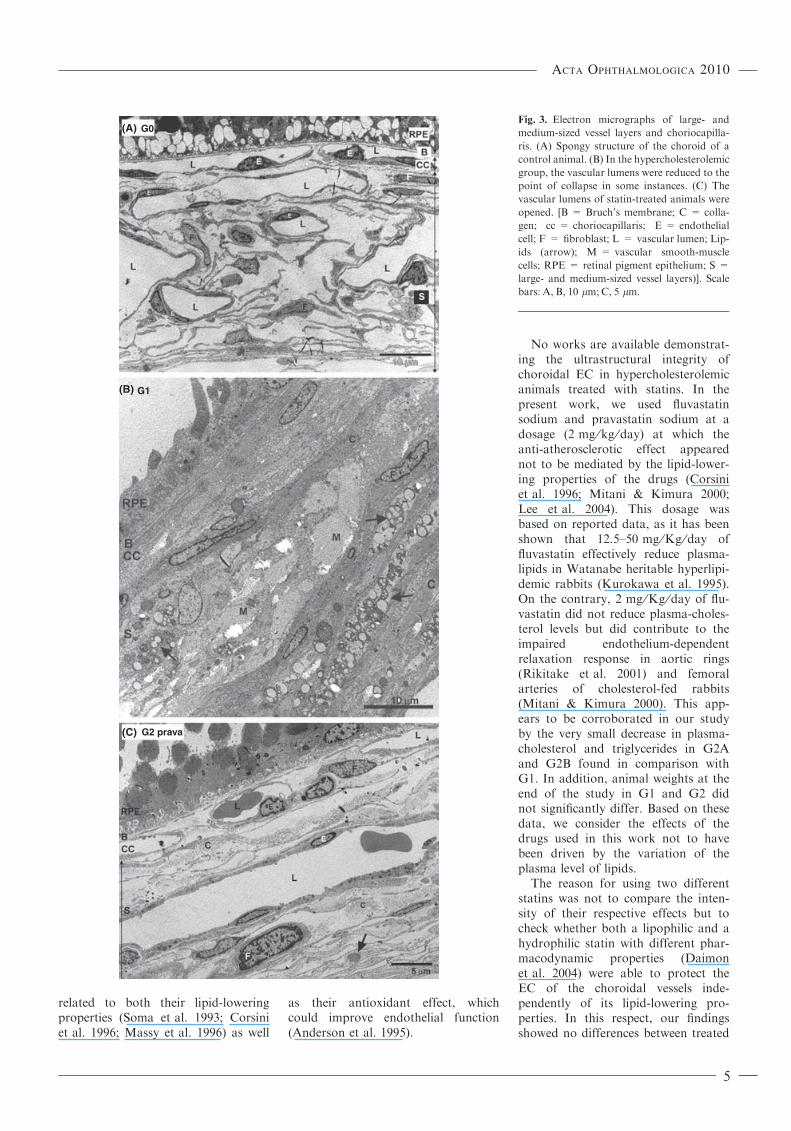
The choroidal structures in G2 weremuch less compressed and moreclearly identified than in G1 (Fig. 3).
In G1, the suprachoroidal spaceswere distended by the presence offoam cells and electron-lucent fusi-form structures surrounded by orinside foam cells (Fig. 4A, B). In addi-tion, fibroblasts loaded with lipids andincreased collagen appeared (Fig. 4A).In some instances, foam cells andfibroblasts had ultrastructural featuresof necrosis, with a rupture of the cyto-membranes (Fig. 4B). To a lesserextent, foam cells and increased colla-gen were noted in G2 (Fig. 4C, D),and in some instances, foam cells weremostly absent, with lipids beinglocated inside fibroblasts (Fig. 4D).
In G1 and G2, fibroblasts surround-ing the perineurum of the long andshort ciliary nerves of the suprachoroi-dea were loaded with lipids. Overall,both myelinated and unmyelinatedaxons had a normal appearance, witha few containing electrodense bodies.Some myelinated axons had small,empty spaces (vacuoles) separatingmyelin sheaths (Fig. 5A).
In G2, the vascular lumens in thechoroidal layers were open (Figs 3C,6D and 8E, F) as in G0, due in partto the reduction of the suprachoroidallipids (Fig. 4C, D).
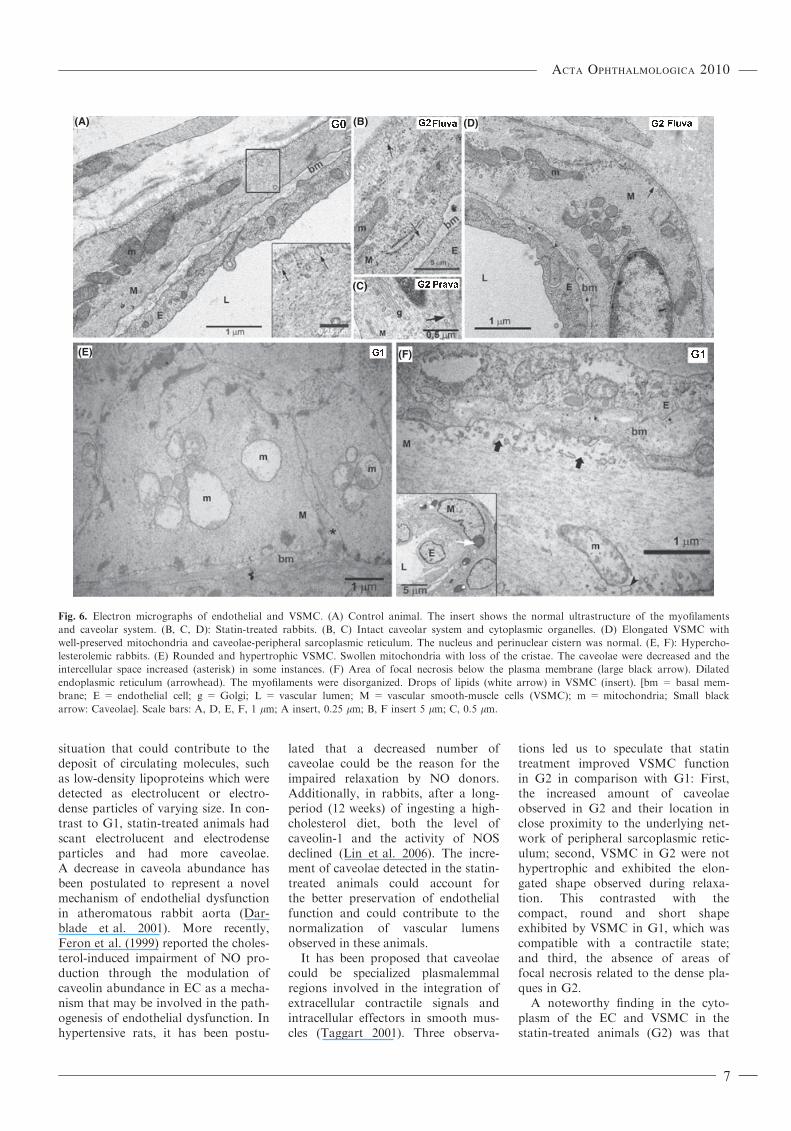
In G1, the VSMC in the large- andmedium-sized vessel layer (LMV) werehypertrophic with a rounded and com-pact appearance (Figs 3B, 6E and 7B).They contained droplets of lipids anddense bodies in their cytoplasm(Fig. 6F). The myofilaments were dis-organized (Fig. 6F). In the area ofcaveolae-peripheral sarcoplasmic retic-ulum, there were areas of focal necrosisthat sometimes affected the dense pla-ques (Fig. 6F). The endoplasmic retic-ulum and Golgi cisterns were dilatedand the ribosomes were disassembled.The mitochondria appeared swollenwith a partial or total loss of the cris-tae, a predominant, clear matrix(Fig. 6E, F) and, in some instances,dilation of the double membrane. Thecaveolar system (corresponding mainly
Fig. 1. Thickening of the sclera-choroid (dou-
ble arrow) in the study groups. Semi-thin
sections (toluidine blue). (C = vascular layers
of the choroid; SC-S = suprachoroidea-
sclera). [G0 = Control, standard diet; G1
(Hypercholesterolemic rabbits, 0.5% choles-
terol-enriched diet); G2 (Statins: Hyper-
cholesterolemic diet + fluvastatin sodium or
pravastatin sodium)]. Scale bar: 100 lm.
Acta Ophthalmologica 2010
3

to noncoated vesicles) was less numer-ous than in G0 (Fig. 6A, E, F). In gen-eral, the cell junctions were wellpreserved, although, in some instances,the junctions were disrupted and theintercellular space increased (Fig. 6E).In the areas where the tissue was highlydisorganized, other necrotic features(swelling, vacuolization, cytomem-brane necrosis and disappearance ofspecific ultrastructural characteristics)were noted (Fig. 6E, F). In G2, theVSMC looked similar to those in con-trol (Fig. 6A–D) exhibiting an elon-gated shape (Figs 3C and 6D), whilesome contained lipid droplets. Thecaveolar system (Fig. 6B, D) wasgreater than in G1 (Fig. 6E, F), andthe cytoplasmic organelles were normal(Fig. 6B–D). The mitochondria had anormal electrodensity of the matrix,and the cristae and membranes werewell preserved (Fig. 6B, D). Signs ofnecrosis were rare (Fig. 6B–D), withintercellular spaces between VSMCbeing preserved.
In G1, the endothelial cells (EC) ofthe LMV layers and the choriocapilla-ris were altered with respect to G0. In
some instances, they were necrotic(Fig. 8C) while in others they presentedrarefactions in the cytoplasm that con-tributed to lumen reduction. They hadirregular dilation of the perinuclearcistern. The nuclear-pore complex dis-assembly predominated over intactnuclear-pore complexes (Fig. 7A). Thepreservation of the cytoskeleton alter-nated with areas of focal necrosis(Fig. 6F). Electrodense particles andlipid droplets were detected (Fig. 7B).The cytoplasm organelles (endoplasmicreticulum, Golgi cisterns, ribosomes,mitochondria and caveolar system)showed changes similar to those ofVSMC. However, in G2, the EClooked similar to those of control(Fig. 6A–D), the cytoplasmic organ-elles were normal (Fig. 6B, D), and thecaveolar system was greater than in G1(Fig. 6B, D–F). Signs of necrosis wererarely found (Fig. 6B, D).
In G2, the basal membrane of thevessels was thickened, resembling G0more than G1 (Fig. 6A, B, D–F).However, the number of collagenfibres (Fig. 3C) in the adventitia andintervascular spaces was greater thanin control (Fig. 3A) although to a les-ser extent than in G1 (Fig. 3B). Thefoam cells visible in the adventitia ofG1 (Fig. 5B) were not found in G2.In some instances, the fibroblast con-tained lipid droplets (Fig. 3C).
The thickness of BM in statin-trea-ted animals was significantly reduced(Fig. 8E) in comparison with hyper-cholesterolemic rabbits (Fig. 8C, D)because of the disappearance (Fig. 8F)of the electrolucent and electrodenseparticles seen in group G1 (Fig. 8D).In comparison with control (Fig. 8A,B), the thickness of BM in G2 signifi-cantly increased along the periphery,due basically to an enlargement ofcollagen fibres (Fig. 8F).
Discussion
Fluvastatin sodium (a lipophilicentirely synthetic statin metabolised inthe liver) and pravastatin sodium (ahydrophilic statin of fungal origin) are3-hydroxy-3-methyl-glutaryl-coenzymeA (HMG-CoA) reductase inhibitorsthat besides reducing plasma-choles-terol can induce regression of athero-sclerosis (Jukema et al. 1995; Rikitakeet al. 2001). Works undertaken duringthe past 10 years have revealed thatthe benefits of using these drugs are
(A)
(B)
(C)
(D)
Fig. 2. Overall aspect of the vascular layers of the choroid. Semi-thin sections (toluidine blue).
(A) Control animals. The microphotograph illustrates the opened vascular lumens and the
spongy structure of the choroid. (B) Hypercholesterolemic rabbits. The vascular layers had
abundant lipids and some vascular lumens were collapsed. (C, D) Statin-treated animals. Treat-
ment with either statins maintained the vascular lumens opened and the structure of the choroid
resembled control more than G1. (cc = choriocapillaris; v = vascular lumen) [G0 = Control,
standard diet; G1 (Hypercholesterolemic rabbits, 0.5% cholesterol-enriched diet); G2 (sta-
tins = hypercholesterolemic diet + fluvastatin sodium or pravastatin sodium)]. Scale bar:
10 lm.
Table 2. Thickness of the sclera-suprachoroidea complex in the periphery and MNFR.
Group Periphery MNFR
Control 290.045 ± 24.810 306.439 ± 16.124
G1 762.694 ± 251.938 540.487 ± 128.604
G2 548.911 ± 257.799 338.201 ± 66.507
Data are the mean ± SEM. Control (n = 6), standard diet; G1 (n = 6) (Hypercholesterolemic
rabbits, 0.5% cholesterol-enriched diet); G2 (n = 6) (Statins = Hypercholesterolemic
diet + fluvastatin sodium or pravastatin sodium), MNFR = Medullated nerve-fibre region.
Table 3. Thickness of the choroidal vascular
layers in the periphery and MNFR.
Group Periphery MNFR
Control 59.312 ± 12.820 41.635 ± 5.895
G1 86.128 ± 39.711 38.944 ± 13.493
G2 103.879 ± 37.145 54.542 ± 12.596
Data are the mean ± SEM. Control (n = 6),
standard diet; G1 (n = 6). (Hypercholesterol-
emic rabbits, 0.5% cholesterol-enriched diet);
G2 (n = 6) (Statins = Hypercholesterolemic
diet + fluvastatin sodium or pravastatin
sodium); MNFR = Medullated nerve-fibre
region.
Table 4. Thickness of the Bruch’s membrane
in the periphery and MNFR.
Group Periphery MNFR
Control 1.691 ± 0.304 1.573 ± 0.270
G1 2.946 ± 1.269 3.112 ± 0.884
G2 2.065 ± 1.007 1.552 ± 0.244
Data are the mean ± SEM. Control (n = 6),
standard diet; G1 (n = 6) (Hypercholesterol-
emic rabbits, 0.5% cholesterol-enriched diet);
G2 (n = 6) (Statins = Hypercholesterolemic
diet + fluvastatin sodium or pravastatin
sodium); MNFR = Medullated nerve-fibre
region.
Acta Ophthalmologica 2010
4
related to both their lipid-loweringproperties (Soma et al. 1993; Corsiniet al. 1996; Massy et al. 1996) as well
as their antioxidant effect, whichcould improve endothelial function(Anderson et al. 1995).
No works are available demonstrat-ing the ultrastructural integrity ofchoroidal EC in hypercholesterolemicanimals treated with statins. In thepresent work, we used fluvastatinsodium and pravastatin sodium at adosage (2 mg ⁄kg ⁄day) at which theanti-atherosclerotic effect appearednot to be mediated by the lipid-lower-ing properties of the drugs (Corsiniet al. 1996; Mitani & Kimura 2000;Lee et al. 2004). This dosage wasbased on reported data, as it has beenshown that 12.5–50 mg ⁄Kg ⁄day offluvastatin effectively reduce plasma-lipids in Watanabe heritable hyperlipi-demic rabbits (Kurokawa et al. 1995).On the contrary, 2 mg ⁄Kg ⁄day of flu-vastatin did not reduce plasma-choles-terol levels but did contribute to theimpaired endothelium-dependentrelaxation response in aortic rings(Rikitake et al. 2001) and femoralarteries of cholesterol-fed rabbits(Mitani & Kimura 2000). This app-ears to be corroborated in our studyby the very small decrease in plasma-cholesterol and triglycerides in G2Aand G2B found in comparison withG1. In addition, animal weights at theend of the study in G1 and G2 didnot significantly differ. Based on thesedata, we consider the effects of thedrugs used in this work not to havebeen driven by the variation of theplasma level of lipids.
The reason for using two differentstatins was not to compare the inten-sity of their respective effects but tocheck whether both a lipophilic and ahydrophilic statin with different phar-macodynamic properties (Daimonet al. 2004) were able to protect theEC of the choroidal vessels inde-pendently of its lipid-lowering pro-perties. In this respect, our findingsshowed no differences between treated
(A)
(B)
(C)
G0
G1
G2 prava
Fig. 3. Electron micrographs of large- and
medium-sized vessel layers and choriocapilla-
ris. (A) Spongy structure of the choroid of a
control animal. (B) In the hypercholesterolemic
group, the vascular lumens were reduced to the
point of collapse in some instances. (C) The
vascular lumens of statin-treated animals were
opened. [B = Bruch’s membrane; C = colla-
gen; cc = choriocapillaris; E = endothelial
cell; F = fibroblast; L = vascular lumen; Lip-
ids (arrow); M = vascular smooth-muscle
cells; RPE = retinal pigment epithelium; S =
large- and medium-sized vessel layers)]. Scale
bars: A, B, 10 lm; C, 5 lm.
Acta Ophthalmologica 2010
5

animals. For this reason, data fromstatin-treated animals were groupedfor the purposes of results descriptionand discussion.
In G2, we found some alterationsthat were not present in G0, such asclumps of electrodense particles, somefoam cells and fibroblast-containinglipids. However, the lipid build-up inthe suprachoroidea and the subse-quent thickening of this ocular layer,among the most striking findings inG1 that have also been reported byothers (Francois & Neetens 1966; Vin-ger & Sachs 1970; Salazar et al. 2007),were significantly reduced in G2, thestatin-treated group. The suprachoroi-dal thickening in G1 caused astraightening of the vessels passingthrough it and a reduction of theirlumens. The reduction of the supra-choroidal lipids in G2 suggests nomechanical compression of the vascu-lar layers of the choroid, and there-fore, because no lumen reduction wasfound, we deduced that the choroidalblood flow had not been compro-mised. On the other hand, the mainte-nance of the choroidal vascular
lumens in G2 could account for lesserstress on EC by means of a decreasein the local tangential forces exertedon the vessel walls when the insidevascular radius decreased. Accord-ingly, endothelial dysfunction wouldnot result.
The lumen reduction in the choroi-dal vessels of G1 was thus because ofcompression caused by the lipid build-up in the suprachoroidea and vessellayers as well as by hypertrophy ofVSMC and the rarefactions of EC. Incontrast to G1, LMV in G2 had openlumens similar to those of G0, due inpart to the reduction of the supracho-roidal lipids. In addition, the EC hadnormal features, maintaining theirarrangement as a monolayer intercon-nected by cell junctions (Dejana1996).
The traffic of molecules between theblood and the cell wall can be identi-fied by a microvesicular system com-posed of caveolae and a glycocalix ofthe apical surface (Badimon & Martı-nez-Gonzalez 2006). There is anemerging role of caveolins, a family ofproteins critical to caveolar function,
in organizing and modulating thebasic functions of smooth muscles(Hardin & Vallejo 2006) and vascularfunctions dependent on NO and Ca2+
signalling (Drab et al. 2001; Hardin &Vallejo 2006).
It has been postulated that a changein caveolae abundance could havedirect impact on vascular function (Linet al. 2006). Caveolin-1 is involved inthe regulation of cellular cholesterolhomoeostasis and promotes cellularcholesterol efflux (Lin et al. 2006). Ithas been reported that in the earlystages of hypercholesterolemia, caveo-lin-1 synthesis increases to remove theexcess cholesterol from the cells. How-ever, in our experiment, after long peri-ods of feeding, caveolin-1 synthesiswas repressed. EC and VSMC in G1(32 weeks of hypercholesterolemia)exhibited less caveolae than G0, a
(A) (B)
(C) (D)
Fig. 4. Electron micrographs of the suprachoroidea. (A, B) Suprachoroidal build-up of lipids
(*) and rupture of the cytomembranes of foam cells in hypercholesterolemic rabbits. (C, D) In
statin-treated animals, the collagen increased and the lipids were located mainly inside the fibro-
blast. [FC = Foam cells; cholesterol clefts (arrow); C = collagen; F = fibroblast; M = macro-
phage]. Scale bars: A, C, 5 lm; B, 2 lm; D, 10 lm.
(A)
(B)
Fig. 5. Electron micrographs of hypercholes-
terolemic rabbits. (A) Large- and medium-
sized vessel layers: Foam cells in the adventitia.
Most myelinated and unmyelinated axons of
the ciliary nerves had a normal appearance. In
some instances, small vacuoles separating mye-
lin sheaths (arrowhead) were observed. (B) A
macrophage (M) in the outer collagen layer of
Bruch’s membrane (BM). [Ad = adventitia;
CN = ciliary nerve; E = endothelial cell;
e = elastic layer of BM; F = fibroblast;
FC = foam cells; L = vascular lumen; Lipids
(arrow); ic = inner collagen layer of BM;
oc = outer collagen layer of BM; RPE = reti-
nal pigment epithelium]. Scale bars: 5 lm.
Acta Ophthalmologica 2010
6
situation that could contribute to thedeposit of circulating molecules, suchas low-density lipoproteins which weredetected as electrolucent or electro-dense particles of varying size. In con-trast to G1, statin-treated animals hadscant electrolucent and electrodenseparticles and had more caveolae.A decrease in caveola abundance hasbeen postulated to represent a novelmechanism of endothelial dysfunctionin atheromatous rabbit aorta (Dar-blade et al. 2001). More recently,Feron et al. (1999) reported the choles-terol-induced impairment of NO pro-duction through the modulation ofcaveolin abundance in EC as a mecha-nism that may be involved in the path-ogenesis of endothelial dysfunction. Inhypertensive rats, it has been postu-
lated that a decreased number ofcaveolae could be the reason for theimpaired relaxation by NO donors.Additionally, in rabbits, after a long-period (12 weeks) of ingesting a high-cholesterol diet, both the level ofcaveolin-1 and the activity of NOSdeclined (Lin et al. 2006). The incre-ment of caveolae detected in the statin-treated animals could account forthe better preservation of endothelialfunction and could contribute to thenormalization of vascular lumensobserved in these animals.
It has been proposed that caveolaecould be specialized plasmalemmalregions involved in the integration ofextracellular contractile signals andintracellular effectors in smooth mus-cles (Taggart 2001). Three observa-
tions led us to speculate that statintreatment improved VSMC functionin G2 in comparison with G1: First,the increased amount of caveolaeobserved in G2 and their location inclose proximity to the underlying net-work of peripheral sarcoplasmic retic-ulum; second, VSMC in G2 were nothypertrophic and exhibited the elon-gated shape observed during relaxa-tion. This contrasted with thecompact, round and short shapeexhibited by VSMC in G1, which wascompatible with a contractile state;and third, the absence of areas offocal necrosis related to the dense pla-ques in G2.
A noteworthy finding in the cyto-plasm of the EC and VSMC in thestatin-treated animals (G2) was that
(A)
(E) (F)
(C)
(B) (D)
Fig. 6. Electron micrographs of endothelial and VSMC. (A) Control animal. The insert shows the normal ultrastructure of the myofilaments
and caveolar system. (B, C, D): Statin-treated rabbits. (B, C) Intact caveolar system and cytoplasmic organelles. (D) Elongated VSMC with
well-preserved mitochondria and caveolae-peripheral sarcoplasmic reticulum. The nucleus and perinuclear cistern was normal. (E, F): Hypercho-
lesterolemic rabbits. (E) Rounded and hypertrophic VSMC. Swollen mitochondria with loss of the cristae. The caveolae were decreased and the
intercellular space increased (asterisk) in some instances. (F) Area of focal necrosis below the plasma membrane (large black arrow). Dilated
endoplasmic reticulum (arrowhead). The myofilaments were disorganized. Drops of lipids (white arrow) in VSMC (insert). [bm = basal mem-
brane; E = endothelial cell; g = Golgi; L = vascular lumen; M = vascular smooth-muscle cells (VSMC); m = mitochondria; Small black
arrow: Caveolae]. Scale bars: A, D, E, F, 1 lm; A insert, 0.25 lm; B, F insert 5 lm; C, 0.5 lm.
Acta Ophthalmologica 2010
7

mitochondria maintained a normalultrastructure. This is of outstandingimportance, taking into account thatthese organelles represent a funda-mental structure in the aerobic metab-olism (Poche et al. 1968) and thatthey are extremely sensitive tohypoxia. The importance of mito-chondria is well known in oxidativephosphorylation to generate ATP.Mitochondrial phosphorylation isimpaired in ischaemic situations and,as a consequence of oxidative stress,DNA, proteins and lipids are dam-aged by a surge in free radicals(Simon & Johns 1999). From themitochondrial integrity observed inG2, good functioning of EC andVSMC could be deduced.
In G1, the basal membranes con-tained foam cells forming microath-eromas (Salazar et al. 2007), and therewas an increase in the collagen fromthe adventitia. These collagen fibrescan be synthesized by VSMC (Ara-goncillo et al. 2000), which, as aconsequence of the hyperlipidemia,gradually modify their phenotype. In
statin-treated animals (G2A, G2B),the basal membranes resembled G0more than G1. However, an increasein collagen fibres in the vascularadventitia and in the intervascularspaces and even fibroblast containingclumps of lipids could still bedetected. These features could beexplained first by the low lipid-decreasing capability of statins at thedosage employed in this work and,second, to macrophage activity andtheir ability to produce matrix metal-loproteinases (Henney et al. 1991;Galis et al. 1994) in the areas ofhigher concentration of foam cells,
where esterified and free-cholesterolreabsorption is followed by sclerogen-ic activity (Abdulla et al. 1967).
In G2, fluvastatin sodium and pra-vastatin sodium prevented atheroscle-rotic damage at the choriocapillarylevel, because, as opposed to whathappened in G1, scant rarefactions,hypertrophy or necrosis of EC wereobserved. In addition, the vascularlumen remained open, most probablyas a consequence of the maintenanceof the endothelial-depending relaxa-tion, similar to what has beenreported by other authors in thecoronary vessels (Corsini et al. 1996).
(A)
(B)
Fig. 7. Electron micrographs of hypercholes-
terolemic rabbits. (A) Irregular dilation of the
perinuclear cistern and nuclear-pore complex
disassembly (arrow). (B) The endothelium
contained drops of lipids (arrowhead) and
the basal membrane (bm) electrodense inclu-
sions. The vascular lumens (L) were filiform.
(E = endothelial cell; M = vascular smooth-
muscle cells; m = mitochondria). Scale bars:
A, 0.5 lm; B, 2 lm.
(A) (B)
(C)
(E) (F)
(D)
Fig. 8. Electron micrographs of the choriocapillaris and Bruch’s membrane (BM). (A, B): Con-
trol animals. (A) Normal endothelial cell. (B) Normal BM and choriocapillaris lumen. (C, D):
Hypercholesterolemic rabbits. (C) Necrotic endothelial cell. (D) Electrolucent particles (arrow)
at the collagenous layers of BM. Hypertrophic endothelial cell of the choriocapillaris and lumen
reduction. (E, F): statin-treated animals. (E) Endothelial cell of the choriocapillaris without
necrotic features. Normal vascular lumen. (F) No electrolucent particles were observed in the
BM. Enlarged collagen fibres (arrowhead). (cc = choriocapillaris; E = endothelial cell;
e = elastic layer; ic = inner collagenous layer; oc = outer collagenous layer; L = lumen;
RPE, retinal pigment epithelium). Scale bars: A, E, 2 lm; B, C, D, F, 1 lm.
Acta Ophthalmologica 2010
8

This fact together with the relief ofthe mechanical compression becauseof the reduction in the lipid build-upin the suprachoroidea could explainthe significantly increased thickeningof the vascular layers of statin-treatedanimals.
Similar to G1, thickening and lipidaccumulation in BM has beendescribed in human AMD (Curcioet al. 2001, 2005). These deposits oflipids or lipid-rich material could addresistance to the flow of solutes andwater through the Bruch-retinal pig-ment epithelium, as demonstrated bythe studies that have measured thehydraulic conductivity of isolated BM(Moore et al. 1995; Starita et al. 1996).BM in G2 was significantly thinnerthan in G1 because of the absence ofelectrodense and electrolucent particlesobserved in G1. In comparison to G0,the thickness of the BM in G2 wassignificantly greater in the peripherybecause of an increase in the size ofcollagen fibres, most probably second-ary to the sclerogenic activity thatfollows lipid reabsorption. This featurewas detected mainly in the outer colla-gen layer with no appreciable ultra-structural alterations in the elastic one.Findings in G2 could represent animprovement in the semi-permeablefiltration-barrier function of BM, thusallowing the diffusion of nutrientsfrom the choriocapillaris and removalof cell debris from RPE.
In hypercholesterolemic New Zea-land rabbits, treatment with fluva-statin sodium and pravastatin sodiumat a dose insufficient to normalizeplasma-lipid levels (2 mg ⁄Kg ⁄day)prevents the progression of atheroscle-rosis in the different vascular layers ofthe choroid. The significant reductionof the lipid build-up at the supra-choroidea relieves the mechanicalcompression of choroidal vessels. Thenormal ultrastructure of EC andVSMC suggests that the endothelium-depending relaxation is maintained,thus reducing the ischaemia. The dis-appearance of lipids in BM presum-ably improves oxygen and nutrienttransport (Ramırez et al. 2006; Tri-vino et al. 2006; Salazar et al. 2007).
The ultrastructural observations inthe choroidal vascular tissue of thepresent work moved us to hypothesizethat the effects of the statins used hereare probably mediated by an overre-gulation of the endothelial nitric oxide
and a downregulation of endothelin-1,similar to what has been reported instudies on the direct consequences ofthe endothelial dysfunction in extraoc-ular tissues (Corsini et al. 1996). Thishypothesis should be confirmed by theperformance of functional studies onocular vascular reactivity. In addition,the findings of this study lead us topropose a possible role of statins inthose ocular diseases having endothe-lial dysfunction in their physiopathol-ogy such as AMD, glaucoma ordiabetic retinopathy among others.
Acknowledgments
Supported by RETICs Patologıa Ocu-lar del Envejecimiento, Calidad Visualy Calidad de Vida (Grant RD07 ⁄0062, Instituto de Salud Carlos III,Ministerio de Sanidad y Consumo);RETICs RECAVA (Grant RD06 ⁄0014 ⁄ 0007, Instituto de Salud CarlosIII, Ministerio de Sanidad y Con-sumo); Fundacion Mutua Madrilena(Grant 4131173); and FISS (GrantPI080920).
The authors thank Agustın Fernan-dez, Marıa Luisa Garcıa Gil and theCentro de Microscopia Electronica‘Luis Bru’ (Universidad Complutensede Madrid) for technical assistance inelectron microscopy. Desiree Con-treras and Francisca Vargas for tissueprocessing. David Nesbitt and AlistairRoss for correcting the English ver-sion of this work.
ReferencesAbdulla YH, Adams CWM & Morgan RS
(1967): Connective tissue reactions to
implantation of purified sterol, sterol esters,
phosphoglycerides and free fatty acids.
J Pathol Bacteriol 94: 63–71.
Anderson TJ, Meredith IT, Yeung AC, Frei B,
Selwyn AP & Ganz P (1995): The effect of
cholesterol-lowering and antioxidant ther-
apy on endothelium-dependent coronary
vasomotion. N Engl J Med 332: 488–493.
Aragoncillo P, Maeso R, Vazquez-Perez S
et al. (2000): The protective role of ator-
vastatin on function, structure and ultra-
structure in the aorta of dyslipidemic
rabbits. Virchows Arch 437: 545–554.
Badimon L & Martınez-Gonzalez J (2006):
Disfuncion endotelial. Rev Esp Cardiol
6(Supl): 21A–30A.
Chuo JY, Wiens M, Etminan M & Maberley
DA (2007): Use of lipid-lowering agents
for the prevention of age-related macular
degeneration: a meta-analysis of observa-
tional studies. Ophthalmic Epidemiol 14:
367–374.
Corsini A, Pazzucconi F, Pfister P, Paoletti R
& Sirtori CR (1996): Inhibitor of prolifera-
tion of arterial smooth-muscle cells by flu-
vastatin. Lancet 348: 1584.
Curcio CA, Millican CL, Bailey T & Kruth
HS (2001): Accumulation of cholesterol
with age in human Bruch’s membrane.
Invest Opthalmol Vis Sci 42: 265–274.
Curcio CA, Presley JB, Malek G, Medeiros
NE, Avery DV & Kruth HS (2005): Esteri-
fied and unesterified cholesterol in drusen
and basal deposits of eyes with age-related
maculopathy. Exp Eye Res 81: 731–741.
Daimon M, Aomi S, Kawamata T & Kuro-
sawa H (2004): Pravastatin, a 3-hydroxy-
3-methylglutaryl coenzyme A reductase
inhibitor, reduces delayed neuronal death
following transient forebrain ischemia in
the adult rat hypocampus. Neurosci Lett
362: 122–126.
Darblade B, Caillaud D, Poirot M, Fouque
M, Thiers JC, Rami J, Bayard F & Arnal
JF (2001): Alteration of plasmalemmal
caveolae mimics endothelial dysfunction
observed in atheromatous rabbit aorta.
Cardiovas Res 50: 566–576.
Dejana E (1996): Endothelial adherens junc-
tions: implications in the control of vascu-
lar permeability and angiogenesis. J Clin
Invest 98: 1949–1953.
Drab M, Verkade P, Elger M et al. (2001):
Loss of cavoelae, vascular dysfunction, and
pulmonary defects in caveolin-1 disrupted
mice. Science 293: 2449–2452.
Feron O, Chantal D, Moniotte S, Desager JP
& Balligand JL (1999): Hypercholesterol-
emia decreases nitric oxide production by
promoting the interaction of caveolin and
endothelial nitric oxide synthase. J Clin
Invest 103: 897–905.
Francois J & Neetens A (1966): Vascular
manifestations of experimental hypercho-
lesteraemia in rabbits. Angiologica 3: 1–20.
Galis ZS, Sukhova GK, Lark MW & Libby
P (1994): Increased expression of matrix
metalloproteinases and matrix degrading
activity in vulnerable regions of human
atherosclerotic plaques. J Clin Invest 94:
2493–2503.
Gehlbach P, Li T & Hatef E (2009): Statins
for age-related macular degeneration.
Cochrane Database Syst Rev 3: CD006927.
DOI: 10.1002/14651858.CD006927.pub2.
Guymer RH, Chiu AW, Lim L & Baird PN
(2005): HMG CoA reductase inhibitors
(statins): do they have a role in age-related
macular degeneration? Surv Ophthalmol
50: 194–206.
Hall NF, Gale CR, Syddall H, Phillips DI &
Martyn CN (2001): Risk of macular degen-
eration in users of statins: cross sectional
study. BMJ 323: 375–376.
Hardin CD & Vallejo J (2006): Caveolins in
smooth muscle: form organizing function.
Cardiovas Res 69: 808–815.
Henney AM, Wakeley PR, Davies MJ, Fos-
ter K, Hembry R, Murphy G & Humph-
ries S (1991): Localization of stromelysin
Acta Ophthalmologica 2010
9

gene expression in atherosclerotic plaques
by in situ hybridization. Proc Natl Acad
Sci USA 88: 8154–8158.
Johnson LV, Leitner WP, Staples MK &
Anderson DH (2001): Complement activa-
tion and inflammatory processes in drusen
formation and age related macular degen-
eration. Exp Eye Res 73: 887–896.
Jukema JW, Bruschke AV, van Boven AJ
et al. (1995): Effects of lipid lowering by
pravastatin on progression and regression
of coronary artery disease in symptomatic
men with normal to moderately elevated
serum cholesterol levels. The Regression
Growth Evaluation Statin Study
(REGRESS). Circulation 91: 2528–2540.
Kurokawa J, Hayashi K, Toyota Y, Shingu
T, Shiomi M & Kajiyama G (1995): High
dose of fluvastatin sodium (XU62-320), a
new inhibitor of 3-hydroxy-3-methylgluta-
ryl coenzyme A reductase, lowers plasma
cholesterol levels in homozygous Watana-
be-heritable hyperlipidemic rabbits. Bio-
chim Biophys Acta 1259: 99–104.
Lee TM, Lin MS, Chou TF, Tsai CH &
Chang NC (2004): Effect of pravastatin on
left ventricular mass by activation of
myocardial K ATP channels in hypercho-
lesterolemic rabbits. Atherosclerosis 176:
273–278.
Lin WW, Lin YC, Chang TY, Tsai SH, Ho
HC, Chen YT & Yang VC (2006): Caveo-
lin-1 expression is associated with plaque
formation in hypercholesterolemic rabbits.
J Histochem Cytochem 54: 897–904.
Malek G, Li CM, Guidry C, Medeiros NE
& Curcio CA (2003): Apolipoprotein B
in cholesterol-containing drusen and
basal deposits of human eyes with age-
related maculopathy. Am J Pathol 162:
413–425.
Massy ZA, Keane WF & Kasiske BL (1996):
Inhibition of the mevalonate pathway: ben-
efits beyond cholesterol reduction? Lancet
347: 102–103.
Matthys KE, Van Hove CE, Kockx MM,
Andries LJ, Van Osselaer N, Herman AG
& Bult H (1997): Local application of LDL
promotes intimal thickening in the collared
carotid artery of the rabbit. Arterioscler
Thromb Vasc Biol 17: 2423–2429.
McCarty CA, Mukesh BN, Guymmer RH,
Baird PN & Taylor HR (2001): Cholesterol
lowering medications reduce the risk of
age-related maculopathy progression. Med
J Aust 175: 340.
McGwin G & Owsley C (2007): Statins and
age-related macular maculopathy. In: Tom-
bran-Tink J & Barnstable CJ (ed.). Retinal
degenerations: biology, diagnostics, and
therapeutics. Tortowa, New Jersey: Human
Press 185–196.
McGwin G, Owsley C, Curcio CA & Crain
RJ (2003): The association between statin
use and age-related maculopathy. Br J
Ophthalmol 87: 1121–1125.
McGwin G, Xie A & Owsley C (2005): The
use of cholesterol-lowering medications and
age-related macular degeneration. Ophthal-
mology 112: 488–494.
Mitani H & Kimura M (2000): Fluvastatin,
HMG-CoA reductase inhibitor: antiathero-
genic profiles through its lipid-lowering-
dependent and –independent actions.
Cardiovasc Drug Rev 18: 284–303.
Moore DJ, Hussain AA & Marshall J (1995):
Age-related variation in the hydraulic con-
ductivity of Bruchs’s membrane. Invest
Ophthalmol Vis Sci 36: 1290–1297.
Oorni K, Pentikainen MO, Ala-Korpela M &
Kovanen PT (2000): Aggregation, fusion,
and vesicle formation of modified low den-
sity lipoprotein particles: molecular mecha-
nisms and effects on matrix interactions.
J Lipid Res 41: 1703–1714.
Poche R, de Mello Mattos CM, Rembarz HW
& Stoepel K (1968): Uber das mitochond-
rien: myofibrillen in den Herznuskelzellen
der ratte bvei druckhypertrophie des her-
zens. Virchows Arch Pathol Anat 344: 100–
110.
Ramırez AI, Salazar JJ, De Hoz R, Rojas B,
Ruiz E, Tejerina T, Ramırez JM & Trivino
A (2006): Macroglial and retinal changes in
hypercholesterolemic rabbits after normali-
zation of cholesterol levels. Exp Eye Res
83: 1423–1438.
Rikitake Y, Kawashima S, Takeshita S et al.
(2001): Anti-oxidative properties of fluvast-
atin, an HMG-CoA reductase inhibitor,
contribute to prevention of atherosclerosis
in cholesterol-fed rabbits. Atherosclerosis
154: 87–96.
Rong JX, Shen L, Chang YH, Richters A,
Hodis HN & Sevanian A (1999): Choles-
terol oxidation products induce vascular
foam cell lesion formation in hypercholes-
terolemic New Zealand white rabbits. Arte-
rioscler Thromb Vasc Biol 19: 2179–2187.
Ross R (1993): The pathogenesis of athero-
sclerosis: a perspective for the 1990s. Nat-
ure 362: 801–809.
Salazar JJ, Ramırez AI, De Hoz R, Ruiz E,
Tejerina T, Trivino A & Ramırez JM
(2007): Alterations in the choroid in hyper-
cholesterolemic rabbits: reversibility after
normalization of cholesterol levels. Exp
Eye Res 84: 412–422.
Simon DK & Johns DR (1999): Mitochon-
drial disorders: clinical and genetic fea-
tures. Annu Rev Med 50: 111–127.
Smeeth L, Cook C, Chakravarthy U, Hub-
bard R & Fletcher AE (2005): A case
control study of age related macular degen-
eration and use of statins. Br J Ophthalmol
89: 1171–1175.
Soma MR, Donetti E, Parolini C, Mazzini
G, Ferrari C, Fumagalli R & Paoletti R
(1993): HMG CoA reductase inhibitors. In
vivo effects on carotid intimal thickening in
normocholesterolemic rabbits. Arterioscler
Thromb 13: 571–578.
Song J, Deng P, Stinnett SS, Epstein DL &
Rao PV (2005): Effects of Cholesterol-
Lowering Statins on the Aqueous Humor
Outflow Pathway. Invest Ophthalmol Vis
Sci 46: 2424–2432.
Starita C, Hussain AA, Pagliarini S & Mar-
shal J (1996): Hydrodynamics of ageing
Bruch’s membrane: implication for macular
disease. Exp Eye Res 26: 565–572.
Taggart MJ (2001): Smooth muscle excita-
tion-contraction coupling: a role for caveo-
lae and caveolins? News Physiol Sci 16:
61–65.
Tan JS, Mitchell P, Rochtchina E & Wang JJ
(2007): Statins and the long-term risk of
incident age-related macular degeneration:
the Blue Mountains Eye Study. Am J
Ophthalmol 143: 685–687.
Trivino A, Ramırez AI, Salazar JJ, De Hoz
R, Rojas B, Padilla E, Tejerina T & Ram-
ırez JM (2006): A cholesterol-enriched diet
induces ultrastructural changes in retinal
and macroglial rabbit cells. Exp Eye Res
83: 357–366.
Vijayagopal P & Glancy L (1996): Macro-
phages stimulate cholesteryl ester accumu-
lation in cocultured smooth muscle cells
incubated with lipoprotein-proteoglycan
complex. Arterioscler Thromb Vasc Biol
16: 1112–1121.
Vinger PF & Sachs BA (1970): Ocular mani-
festation of hyperlipoproteinemia. Am J
Ophthalmol 70: 563–573.
Wu Ch, Chang S, Chen M & Lee I (1995):
Early change of vascular permeability in
hypercholesterolemic rabbits. Arterioscler
Thromb Vasc Biol 15: 529–533.
Yamada K, Sakurai E, Itaya M, Yamasaki S
& Ogura Y (2007): Inhibition of laser-
induced choroidal neovascularization by
atorvastatin by downregulation of monocyte
chemotactic protein-1 synthesis in mice.
Invest Ophthalmol Vis Sci 48: 1839–1843.
Zambarakji HJ, Nakazawa T, Connolly E
et al. (2006): Dose-dependent effect of pita-
vastatin on VEGF and angiogenesis in a
mouse model of choroidal neovasculariza-
tion. Invest Ophthalmol Vis Sci 47: 2623–
2631.
Received on July 2nd 2009.
Accepted on November 11th, 2009.
Correspondence:
Jose Manuel Ramırez
Instituto de Investigaciones Oftalmologicas
Ramon Castroviejo
School of Medicine
Complutense University
28040 Madrid
Spain
Tel: + 34 91 3941358
Fax: +34 91 3941359
Email: [email protected]
Acta Ophthalmologica 2010
10
Copyright © 2022 FDOKUMEN




















