Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) on the Hypercholesterolemic Rabbit Heart
10
Send Orders for Reprints to [email protected] 6896 Current Pharmaceutical Design, 2013, 19, 6896-6905 Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) on the Hypercholes- terolemic Rabbit Heart Bela Juhasz 1, *, Attila Kertész 2 , Jozsef Balla 3,4 , Gyorgy Balla 3,5 , Zoltán Szabo 6 , Mariann Bombicz 1 , Daniel Priksz 1 , Rudolf Gesztelyi 1 , Balazs Varga 1 , David D. Haines 1 and Arpad Tosaki 1 1 Faculty of Pharmacy, Department of Pharmacology, University of Debrecen, Debrecen, Hungary; 2 Faculty of Medicine, Department of Cardiology, University of Debrecen, Debrecen, Hungary; 3 MTA-DE Vascular Biology, Thrombosis and Hemostasis Research Group, Hungarian Academy of Sciences, Debrecen, Hungary; 4 Department of Nephrology, Medical and Health Science Center, Uni- versity of Debrecen, Debrecen, Hungary; 5 Department of Pediatrics, University of Debrecen, Debrecen, Hungary; 6 Institute of Inter- nal Medicine, Medical and Health Science Center, University of Debrecen, Debrecen, Hungary Abstract: Hypothesis. The present study evaluates the hypothesis that sour cherry seed extract (SCSE) protects against cardiovascular disease and inflammation in hypercholesterolemic rabbits, and that this protection correlates with SCSE-induced activity of heme oxy- genase-1 (HO-1), a cytoprotective enzyme contributing to oxidative stress responses. Methods: 18 New Zealand white rabbits were divided into three groups receiving: I. cholesterol-free rabbit chow; II. chow containing 2% cholesterol; or III. 2% cholesterol plus SCSE for 16 weeks. Heart functions were monitored by echocardiography 0, 4, and 16 weeks af- ter the initiation of cholesterol-supplemented feeding. At the 16-week time-point, isolated hearts were subjected to ischemia-reperfusion (I/R), followed by measurement of heart rate (HR), aortic flow (AF), coronary flow (CF), aortic pressure (AoP), and left ventricular de- veloped pressure (LVDP). Myocardial infarct size was determined using triphenyl tetrazolium chloride (TTC). Quantification of fatty streaks was assessed using Sudan-III staining. Western blot analysis was used to determine the content of cytochrome c oxidase III (COX III), vascular endothelial growth factor (VEGF), and HO-1 in the myocardium. Results: Relative to cholesterol-treated animals not receiving SCSE, SCSE-treated animals exhibited significantly improved cardiac func- tion and improved peak early diastolic velocity to peak atrial velocity ratio (E’/A’), along with decreased atherosclerotic plaque formation and infarct size. Increased HO-1 and COX III protein expression and COX activity were also noted in hearts from SCSE-treated rabbits. Conclusions: This study demonstrates SCSE cardioprotective effects on hypercholesterolemic hearts. Correlation of these outcomes with HO-1 expression suggests that the effect may be mediated by activity of this enzyme. However, definitive proof of HO-1 dependence re- quires further investigation. Keywords: Atherosclerosis, isolated rabbit heart, ischaemia/reperfusion, sour cherry seed extract. INTRODUCTION Cardiovascular diseases are the major cause of morbidity and mortality in elderly humans. In these disorders, death most often occurs as a consequence of atherosclerosis, leading to stroke, heart failure, ischemia, and other syndromes characterized by severely dysregulated inflammatory processes and their resulting degradation of tissue function [1]. Microvascular damage associated with a progressive decline in health of cardiovascular tissue typically is accompanied by arterial stiffening and the onset of a diverse range of age-associated pathologies, especially heart, kidney disease, and neurologic disfunction, including dementia [2]. Under physiological conditions, cholesterol and triglycerides are complexed with protein into configurations that allow these non-polar compounds to move freely in the aqueous environment of the bloodstream. These lipoprotein complexes, ranked in order of increasing size, include high density lipoprotein (HDL), low density lipoprotein (LDL), intermediate density lipoprotein (IDL), very low density lipoprotein (VLDL), and chylomicrons [3]. Enterocytes release nascent chylomicrons into lymphatic vessels in the walls of the villi, called lacteals, and transit into the bloodstream via the thoracic duct and left subclavian vein [3]. Lipids are distributed via the bloodstream to different tissues in the body (skeletal muscle, adipose tissue), where triglycerides are extracted by the activity of lipoprotein lipase [3]. *Address correspondence to this author at the Department of Pharmacology, Faculty of Pharmacy, Health and Science Center, University of Debrecen Nagyerdei krt. 98., 4032 Debrecen Hungary; Tel/Fax: 36-52-255586; E-mail: [email protected] HDL particles, which are the smallest (5-15nm) lipoprotein class, have the highest ratio of protein to lipid and are able to sup- press the development of arterial plaques by extracting cholesterol from sites of nascent plaque formation and return it to the liver for recycling [4]. Thus, cholesterol transported in the HDL form pro- motes cardiovascular health, and individuals with high ratios of cholesterol complexed into HDL chylomicrons experience lower rates of cardiovascular disease than those with low HDL/LDL ratios [5]. Individuals may favorably affect their HDL/LDL ratios via certain lifestyle changes, including exercise, weight loss, mild alco- hol usage, increased dietary fiber, and omega-3 fatty acid consump- tion [6-8]. However, other factors related to lifestyle may decrease HDL/LDL, such as smoking [9] and high consumption of saturated fats [10], thereby increasing the risk of developing cardiovascular disorders and exacerbating existing disease. Cholesterol-rich diets have been observed to decrease HDL/LDL ratios in both humans and rabbits, resulting in similar types of deterioration in cardiovas- cular health [11]. Consequently, the outcomes of studies using hy- percholesterolemic rabbit models are expected to have strong rele- vance to human medicine [12, 13]. The present investigation evaluates the effectiveness of upregu- lating the activity of the cytoprotective enzyme heme oxygenase-1 (HO-1) on multiple parameters related to cardiac health in hyper- cholesterolaemic rabbits fed cholesterol-enriched diets during a 16- week timeframe. A hypothesis was tested that sour cherry seed extract (SCSE), a known inducer of heme oxygenase-1 (HO-1), mediates changes in cardiac tissue homeostasis that will make this 18 - 28 /13 $58.00+.00 © 2013 Bentham Science Publishers
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) on the Hypercholesterolemic Rabbit Heart

Send Orders for Reprints to [email protected]
6896 Current Pharmaceutical Design, 2013, 19, 6896-6905
Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) on the Hypercholes-terolemic Rabbit Heart
Bela Juhasz1,*, Attila Kertész2, Jozsef Balla3,4, Gyorgy Balla3,5, Zoltán Szabo6, Mariann Bombicz1, Daniel Priksz1, Rudolf Gesztelyi1, Balazs Varga1, David D. Haines1 and Arpad Tosaki1
1Faculty of Pharmacy, Department of Pharmacology, University of Debrecen, Debrecen, Hungary; 2Faculty of Medicine, Department of Cardiology, University of Debrecen, Debrecen, Hungary; 3MTA-DE Vascular Biology, Thrombosis and Hemostasis Research Group, Hungarian Academy of Sciences, Debrecen, Hungary; 4Department of Nephrology, Medical and Health Science Center, Uni-versity of Debrecen, Debrecen, Hungary; 5Department of Pediatrics, University of Debrecen, Debrecen, Hungary; 6Institute of Inter-nal Medicine, Medical and Health Science Center, University of Debrecen, Debrecen, Hungary
Abstract: Hypothesis. The present study evaluates the hypothesis that sour cherry seed extract (SCSE) protects against cardiovascular disease and inflammation in hypercholesterolemic rabbits, and that this protection correlates with SCSE-induced activity of heme oxy-genase-1 (HO-1), a cytoprotective enzyme contributing to oxidative stress responses. Methods: 18 New Zealand white rabbits were divided into three groups receiving: I. cholesterol-free rabbit chow; II. chow containing 2% cholesterol; or III. 2% cholesterol plus SCSE for 16 weeks. Heart functions were monitored by echocardiography 0, 4, and 16 weeks af-ter the initiation of cholesterol-supplemented feeding. At the 16-week time-point, isolated hearts were subjected to ischemia-reperfusion (I/R), followed by measurement of heart rate (HR), aortic flow (AF), coronary flow (CF), aortic pressure (AoP), and left ventricular de-veloped pressure (LVDP). Myocardial infarct size was determined using triphenyl tetrazolium chloride (TTC). Quantification of fatty streaks was assessed using Sudan-III staining. Western blot analysis was used to determine the content of cytochrome c oxidase III (COX III), vascular endothelial growth factor (VEGF), and HO-1 in the myocardium. Results: Relative to cholesterol-treated animals not receiving SCSE, SCSE-treated animals exhibited significantly improved cardiac func-tion and improved peak early diastolic velocity to peak atrial velocity ratio (E’/A’), along with decreased atherosclerotic plaque formation and infarct size. Increased HO-1 and COX III protein expression and COX activity were also noted in hearts from SCSE-treated rabbits. Conclusions: This study demonstrates SCSE cardioprotective effects on hypercholesterolemic hearts. Correlation of these outcomes with HO-1 expression suggests that the effect may be mediated by activity of this enzyme. However, definitive proof of HO-1 dependence re-quires further investigation.
Keywords: Atherosclerosis, isolated rabbit heart, ischaemia/reperfusion, sour cherry seed extract.
INTRODUCTION Cardiovascular diseases are the major cause of morbidity and mortality in elderly humans. In these disorders, death most often occurs as a consequence of atherosclerosis, leading to stroke, heart failure, ischemia, and other syndromes characterized by severely dysregulated inflammatory processes and their resulting degradation of tissue function [1]. Microvascular damage associated with a progressive decline in health of cardiovascular tissue typically is accompanied by arterial stiffening and the onset of a diverse range of age-associated pathologies, especially heart, kidney disease, and neurologic disfunction, including dementia [2]. Under physiological conditions, cholesterol and triglycerides are complexed with protein into configurations that allow these non-polar compounds to move freely in the aqueous environment of the bloodstream. These lipoprotein complexes, ranked in order of increasing size, include high density lipoprotein (HDL), low density lipoprotein (LDL), intermediate density lipoprotein (IDL), very low density lipoprotein (VLDL), and chylomicrons [3]. Enterocytes release nascent chylomicrons into lymphatic vessels in the walls of the villi, called lacteals, and transit into the bloodstream via the thoracic duct and left subclavian vein [3]. Lipids are distributed via the bloodstream to different tissues in the body (skeletal muscle, adipose tissue), where triglycerides are extracted by the activity of lipoprotein lipase [3].
*Address correspondence to this author at the Department of Pharmacology, Faculty of Pharmacy, Health and Science Center, University of Debrecen Nagyerdei krt. 98., 4032 Debrecen Hungary; Tel/Fax: 36-52-255586; E-mail: [email protected]
HDL particles, which are the smallest (5-15nm) lipoprotein class, have the highest ratio of protein to lipid and are able to sup-press the development of arterial plaques by extracting cholesterol from sites of nascent plaque formation and return it to the liver for recycling [4]. Thus, cholesterol transported in the HDL form pro-motes cardiovascular health, and individuals with high ratios of cholesterol complexed into HDL chylomicrons experience lower rates of cardiovascular disease than those with low HDL/LDL ratios [5]. Individuals may favorably affect their HDL/LDL ratios via certain lifestyle changes, including exercise, weight loss, mild alco-hol usage, increased dietary fiber, and omega-3 fatty acid consump-tion [6-8]. However, other factors related to lifestyle may decrease HDL/LDL, such as smoking [9] and high consumption of saturated fats [10], thereby increasing the risk of developing cardiovascular disorders and exacerbating existing disease. Cholesterol-rich diets have been observed to decrease HDL/LDL ratios in both humans and rabbits, resulting in similar types of deterioration in cardiovas-cular health [11]. Consequently, the outcomes of studies using hy-percholesterolemic rabbit models are expected to have strong rele-vance to human medicine [12, 13]. The present investigation evaluates the effectiveness of upregu-lating the activity of the cytoprotective enzyme heme oxygenase-1 (HO-1) on multiple parameters related to cardiac health in hyper-cholesterolaemic rabbits fed cholesterol-enriched diets during a 16-week timeframe. A hypothesis was tested that sour cherry seed extract (SCSE), a known inducer of heme oxygenase-1 (HO-1), mediates changes in cardiac tissue homeostasis that will make this
1873-4286/13 $58.00+.00 © 2013 Bentham Science Publishers

Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) Current Pharmaceutical Design, 2013, Vol. 19, No. 39 6897
plant material an attractive candidate for the prevention and therapy of cardiac disease. The activity of heme oxygenase-1 (HO-1) increases in response to a wide variety of stimuli, including oxidative and inflammatory insults, as well as metabolic and hemodynamic factors such as high glucose, elevated blood pressure, and plasma lipids. Nevertheless, in most cases, the pathophysiological activation of HO-1 results only in a transient or marginal increase of HO-1 activity. It falls below the threshold necessary to activate downstream signaling components of the HO system at levels capable of achieving sig-nificant remission of serious inflammatory pathologies. Thus, strategies for use of HO-1 as a definitive prophylaxis or treatment for type 2 diabetes mellitus (T2DM) and other diseases are ex-pected to make increasing use of pharmacological agents that are capable of increasing the activity of the enzyme. Several well-known plant materials from a broad phylogenetic background contain known inducers of HO-1 activity, including dietary phytochemicals. Examples include epigallocatechin-3-gallate, a polyphenol component of green tea, and curcumin, which is best known as a component of curry. SCSE is a particularly at-tractive candidate for the therapeutic use of HO-1, based on the capacity of this extract at relatively low dosage to increase the ac-tivity of the enzyme to levels that allow protection against ische-mia-reperfusion injury [14-16]. This makes SCSE potentially very valuable in cardiovascular medicine and many other healthcare venues. This advantage is combined with negligible toxicity of the extract at in vivo dosages in excess of 200x the dosage known to be therapeutic [15]. The present report describes preliminary evalua-tion of the capacity of the seed contents to affect the pathogenesis of cardiovascular dysfunction. Three groups of animals were used for these experiments, (i) non-hypercholesterolemic rabbits (control), (ii) hypercholes-terolemic rabbits without SCSE (HC), (iii) hypercholesterolemic rabbits administered SCSE (HC-treated). All animals were provided with cholesterol-supplemented feed for a 16-week period, followed by assessment of selected cardiovascular parameters. These out-come measures included: serum cholesterol levels; atherosclerotic plaque coverage in thoracic arteries; cardiac functions; infarct size in isolated hearts; and expression of COX III, VEGF, and HO-1 protein in tissue taken from I/R-injured isolated hearts. The effect of SCSE on each of the aforementioned outcomes suggests that this material has enormous potential for use in cardiovascular medicine (combination therapy with the conservative drugs), which will be discussed below.
MATERIALS AND METHODS Animals and Induction of Hypercholesterolemia. The experi-ments were carried out with adult male New Zealand rabbits with a body weight range of 2.0-2.5 kg. Animals received humane care in compliance with the “Principles of Laboratory Animal Care” for-mulated by the National Society for Medical Research, prepared by the National Academy of Sciences (publication No. 86 23, revised 1985). The rabbits were provided with laboratory rodent chow, or chow enriched with 2.0 % cholesterol (Godollo LTD, Budapest, Hungary), or cholesterol-supplemented chow containing 30 mg/kg sour cherry seed extract (SCSE) daily for 16 weeks ad libitum. Serum Cholesterol Measurement. Serum cholesterol levels in the venous blood of each animal were measured using a Cardio-Check serum cholesterol analyzer (Point Of Care Diagnostics, Ltd., Artarmon, New South Wales, Australia) at time-points 0 (baseline), 2, 4, 8, and 16 weeks following initiation of feeding. Echocardiography. Echocardiography was conducted under light anesthesia (ketamine 15 mg/kg, xylazine 3 mg/kg, i.m). The chest of each rabbit was shaved and the animal was positioned in a dorsal decubitus position. Imaging of each heart was accomplished using a 7 MHz ultrasound probe and a Sequoia 512 echograph
(Siemens/Acuson, Tarrytown, New York, U.S.A.) with fundamen-tal imaging modality. Images were stored on magneto-optical disks for off-line analysis. Parasternal long axis views were obtained and recorded to ensure that the mitral and aortic valves as well as the apex were visualized. The exact position of the transducer was ad-justed as necessary to acquire standard images. The parasternal short axis views were recorded at the mid-papillary muscle level. M-mode tracings were performed at the mid-papillary muscle level, either in parasternal long or short axis views with a sweep speed of 150 mm/second, and measurements were taken using the leading edge to leading edge method with 0.1 mm accuracy. All measure-ments were made by a single observer who was blind to the identity of the tracings. All measurements were averaged over three to five consecutive cardiac cycles. Echocardiographic measurements included septal (IVSTD) and posterior (PWTD) left ventricular (LV) wall thickness in diastole, LV cavity size (end-diastolic (LVEDD) and end-systolic (LVESD) dimensions, aortic root, and left atrial antero-posterior diameter. Fractional shortening was computed as follows: (LVEDD-LVESD)/LVEDD, and as global systolic function was balanced, the ejection fraction (EF) was derived as EF = (LVEDD2-LVESD2)/ LVIDD2. Left ventricular myocardial mass was calculated using LVMass (Troy) = 1.05 ([LVEDD + PWTD + IVSTD]3- [LVEDD]3). Left ventricular outflow tract flow velocity-time integral, peak aortic flow velocity, mitral inflow early (E) and late (A) velocities, deceleration time (DT), and tissue Doppler velocities of the lateral mitral anulus (systolic S', early E' and late A' diastolic) were recorded. All the measurements were obtained at the time of examination by the echosonographer, and subsequently read by two separate physicians who were blinded to the groups; the average of the measurements was used for subsequent analysis. Rabbit Heart Isolation. Following a 16-week period, during which the animals were administered 2% cholesterol-enriched chow, heparin (1000 IU/kg) and ketamine/xylazine (40/5 mg/kg) were injected intravenously. Next, thoracotomies were performed on each animal; the hearts were excised and placed into ice-cold perfusion buffer. The aortas were then cannulated, and hearts were perfused according to Langendorff method for a 5-minute washout period at a constant perfusion pressure equivalent to 100 cm of water (10 kPa). The perfusion medium consisted of a modified Krebs-Henseleit bicarbonate buffer: 118 mM NaCl, 4.7 mM KCl, 1.7 mM CaCl2, 25 mM NaHCO3, 0.36 mM KH2PO4, 1.2 mM MgSO4, and 10 mM glucose[17]. The left atrium was cannulated and the Langendorff system was adapted and switched to isolated working hearts, as previously described in a rat model [18], adapted for rabbit heart experiments [19]. The revised procedure used a left atrial filling pressure of 17 cm (1.7 kPa) and aortic afterload pres-sure of 90 cm (9.0 kPa) of buffer. Aortic flow was measured by a calibrated flow meter (Gilmont Instruments, Barrington, Illinois, USA), and coronary flow rate was measured by a timed collection of the coronary perfusate that dripped from the heart. Induction of Global Ischemia and Reperfusion in Isolated Hearts. Following a 10-minute aerobic perfusion of the heart, the atrial inflow and aortic outflow lines were clamped at a point close to the origin of the aortic cannula, and the peristaltic pump (MAS-TERFLEX, Vernon Hills, Illinois, USA) was stopped. Reperfusion was initiated by unclamping the atrial inflow and aortic outflow lines. In order to eliminate the incidence of arrhythmias, the initial 10 minutes of reperfusion was carried out in Langendorff mode. To prevent the myocardium from drying out during normothermic global ischemia, the thermostated glassware (in which hearts were suspended) was covered and the vapor content was kept at a con-stant level. Pre-selected exclusion criteria for our studies demanded that isolated working hearts were excluded if: I. Ventricular ar-rhythmias occurred before the induction of ischemia; and II. Coro-nary flow and aortic flow rates were less than 45 ml/min and 50 ml/minute, respectively, prior to the initiation of global ischemia.

6898 Current Pharmaceutical Design, 2013, Vol. 19, No. 39 Juhasz et al.
Cardiac Functional Indices. Cardiac function was recorded and monitored throughout the experimental period by a computer sys-tem that monitored silver electrodes and pressure transducers con-nected directly to the isolated hearts (ADInstruments, PowerLab, Castle Hill, Australia) in the control, hypercholesterolemic, and SCSE-treated hypercholesterolemic groups. Before ischemia, and during reperfusion, heart rate (HR), coronary flow (CF), and aortic flow (AF) rates were registered. Left ventricular developed pressure (LVDP) was also recorded by the insertion of a catheter into the left ventricle via the left atrium and mitral valve [17]. The hemody-namic parameters were registered by a computer acquisition system (ADInstruments, PowerLab, Castle Hill, Australia). The isolation of hearts, ischemia/reperfusion, and the measure-ments of cardiac function, were conducted following 16 weeks of cholesterol-supplemented diet, and comparisons were made be-tween the age-matched noncholesterolemic, hypercholesterolemic, and SCSE-fed hypercholesterolemic groups. Cardiac function was registered before the induction of normothermic global ischemia, and during reperfusion. Infarct Size Determination. 100 ml of 1 % triphenyl tetrazolium chloride (TTC) solution in phosphate buffer (Na2HPO4 88 mM, NaH2PO4 1.8 mM) was administered via the side arm of the aortic cannula, and then stored at -70˚C for later analysis. Hearts were sliced transversely [20] in a plane perpendicular to the apico-basal axis into 2-3 mm thick sections, weighted, blotted dry, placed in between microscope slides, and scanned on a Hewlett-Packard Scanjet 5p single pass flat bed scanner (Hewlett-Packard, Palo Alto, California, USA). Using NIH 1.61 image processing software, each image was subjected to equivalent degrees of background subtrac-tion, brightness, and contrast enhancement for improved clarity and distinctness. Infarct area of each slice were traced and the respec-tive areas were calculated by pixel density analysis [21]. Infarcted areas was measured by computerized planometry software and multiplied by the weight of each slice, followed by summing the results to obtain the weight of the risk zone (total weight of the left ventricle in grams) and the infarct zone (grams). Infarct size was expressed as a percentage ratio of the infarct zone to the risk zone (weight of the left ventricle). Here, triphenyltetrazolium, (TTC) staining, a direct, post-sacrifice approach to imaging the infracted areas, is used to avoid problems in clearly demonstrating infracted zones, along with high cost intrinsic to recently-developed non-invasive imaging methodology used with live animals [22, 23]. Analysis of Atherosclerotic Lesions. Quantification of fatty streaks was performed with Sudan III stain. Thoracic arteries were harvested, dissected free of excess connective tissue and fat, rinsed with modified Krebs-Henseleit buffer, and fixed in 10 % (vol/vol) buffered formalin. Carotid arteries were then opened longitudinally, and exposed to 5 mg/mL Sudan III in 70 % (vol/vol) isopropanol for 15 minutes in a water bath at 37 °C, and the stain was differen-tiated with several rinses of 70 % isopropanol. The arteries were then scanned, and the atherosclerotic plaque was determined [17, 21]. Cytochrome c Oxidase (COX) Activity. The activity of cyto-chrome c oxidase in rabbit myocardium was measured using a col-orimetric assay kit for oxidation of cytochrome c by this enzyme (Sigma-Aldrich, St. Louis, Missouri, U.S.A.). Briefly, mitochondria isolated from freshly harvested heart muscle using the MITOISO1 kit (Sigma-Aldrich, St. Louis) were treated with dithiothreitol to reduce cytochrome c, followed by COX-mediated reoxidation of the molecule. COX activity at room temperature (~22 °C) in each sample was measured as a decrease in absorbance of ferrocyto-chrome c, at an absorbance wavelength of 550 nm (UV Helios Al-pha S2 spectrophotometer) in its conversion from a reduced to oxi-dized state. The COX activity in any particular sample was reported as (-�A550/min)
Western Blot Analysis: Total protein (100 g) in the Clontech Extraction buffer was added to an equal volume of sodium dodecyl sulfate (SDS) buffer and boiled for 10 minutes before being sepa-rated on 12 % SDS polyacrylamide gels in a running buffer (25 mM Tris 192 mM glycine, 0.1 % (wt/vol) SDS, pH 8.3) at 120 V. The Precision plus Protein Kaleidoscope standards (10 l) (Bio-Rad Laboratories, California, U.S.A.) were used as molecular-weight standards. The gel was transferred onto a nitrocellulose membrane (Bio-Rad Laboratories, Hercules, California, U.S.A.) at 100 V and left for 1 hour in a transfer buffer (25 mM Tris base 192 mM gly-cine 20 % (vol/vol) methanol, pH 8.3). After blocking the mem-branes for 1 hour in a Tris-buffered saline (TBS-T) (50 mM Tris, pH 7.5, 150 mM NaCl) containing 0.1 % (vol/vol) Tween-20 and 5 % (wt/vol) nonfat dry milk, blots were incubated overnight at 4°C with the primary antibody (HO-1, VEGF, COX III, COX IV, GAPDH). Membranes were washed 3 times in TBS-T before being incubated for 1 hour with horseradish peroxide (HRP)-conjugated secondary antibody diluted 1:2,000 in TBS-T and 1 % (wt/vol) nonfat dry milk. Detection was made by autoradiography for vari-able lengths of time with Medical X-Ray Film (Agfa-Gevaert N.V., Belgium). GAPDH (cytoplasm), COX IV (mitochondrial) was used as the loading control (Sigma-Aldrich, St. Louis, Missouri, U.S.A.). Quantitative analysis of scanned Western blots to estimate levels of HO-1, VEGF, COX III, COX IV and GAPDH protein in each sam-ple were calculated using the Scion for Windows Densitometry Image program version Alpha 4.0.3.2 (Scion Corporation, Mary-land, USA). Signal intensity for bands corresponding to each pro-tein of interest was estimated and reported in arbitrary units ± SEM. For these experiments, the Scion Densitometry Image program was selected as most cost-effective for evaluation of selected proteins. The product is public domain software derived from an imaging program used routinely by the United States National Institutes of Health (NIH). It was selected for the present study based on its diverse range of application and reliability. Also, it is available free of charge at www.scioncorp.com and is thus widely used. Statistics: Results are expressed as mean ± SEM (n=6 in each group). One-way analysis of variance was first carried out to test any differences between the mean values of different groups. If differences were established, the results between two groups were compared by Tukey test. Results were considered to be significant if p<0.05.
RESULTS Serum cholesterol levels in hypercholesterolemic animals ad-ministered cholesterol-supplemented feed were evaluated during the study period. As shown in (Fig. 1), total serum cholesterol in hypercholesterolemic animals provided with feed containing 2 % cholesterol became significantly increased during the 16-week time-course of the study relative to levels observed in hypercholes-terolemic rabbits receiving cholesterol-supplemented feed contain-ing 30 mg/kg SCSE (p<0.05). Non-hypercholesterolemic rabbits receiving cholesterol-free feed (normal chew) maintained stable serum cholesterol during the entire course of the study at levels significantly lower than cholesterol-treated hypercholesterolemic rabbits (p<0.05). Plaque coverage in thoracic arteries is shown in (Fig. 2). The extent of plaque coverage in hypercholesterolemic rabbits receiving 30 mg/kg SCSE daily in addition to feed supplemented with 2 % cholesterol was significantly less than the coverage observed in cholesterol-fed animals without SCSE (p<0.05). Moreover, both the SCSE-treated and untreated hypercholesterolemic groups exhibited significantly elevated plaque coverage relative to the nonhypercho-lesterolemic rabbits (p<0.05). Fig. (3) shows the effect on cardiac functional parameters of hypercholesterolemia, elevated dietary cholesterol, SCSE treatment, and the length of post ischemic reperfusion in isolated working

Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) Current Pharmaceutical Design, 2013, Vol. 19, No. 39 6899
Fig. (1). Serum Cholesterol: Time Course Measurements. Average total serum cholesterol levels (mmol/l ± SEM) in 3 groups of rab-bits (n = 6 per group), each administered feed containing 2 % cholesterol, were measured using the CardioCheck serum cholesterol analyzer during a 16-week time-course in non hypercholesterolemic (open circle), hypercho-lesterolemic rabbits (filled squares); hypercholesterolemic animals treated daily with 30 mg/kg SCSE (filled triangles).* p<0.05 for comparison of serum cholesterol in hypercholesterolemic, SCSE-treated rabbits versus HC treated group (HC).
Fig. (2). Arterial Plaque Coverage. Atherosclerotic plaque coverage in Sudan III-stained luminal sections of thoracic arteries harvested from 3 groups of rabbits (n = 4 per group), ad-ministered feed containing 2 % cholesterol during a 16-week time-course for a nonhypercholesterolemic group (control); a hypercholesterolemic group (HC); and a group of hypercholesterolemic animals treated daily with 30 mg/kg SCSE (HC-treated). Results are shown as the average percentage of plaque coverage in arteries from each group of animals ± SEM. * p<0.05 for comparison of percentage atherosclerotic plaque coverage in arteries of hypercholesterolemic, SCSE-treated (HC treated) rabbits versus hypercholesterolemic (HC) rabbits given no SCSE. # p<0.05 for comparison of percentage atherosclerotic plaque coverage in arteries of hypercholesterolemic, SCSE-treated rabbits versus nonhypercho-lesterolemic rabbits (control).
hearts taken from animals in each of the test groups. The cardiac functions evaluated included: heart rate (HR, 3A); aortic flow (AF, 3B); coronary flow (CF, 3C).and left ventricular developed pressure (LVDP, 3D). The effect of I/R injury included a trend toward lower values for each of the functional parameters as a result of occur- rence of the injury and increasing reperfusion time. Significantly better aortic flow was observed at 60 and 120 min of reperfusion in SCSE-treated hypercholesterolemic animals versus those not re-ceiving the extract (p<0.05), whereas a comparison of these groups
revealed coronary flow to be significantly improved only in hearts subjected to a 120-min reperfusion period (p<0.05). The average extent of infarct zones in isolated working hearts subjected to I/R hearts is represented by histograms in (Fig. 4).These outcomes reveal that relative to non-hypercholesterolemic rabbits, hearts from hypercholesterolemic animals manifested larger infarct zones. Moreover, the average extent of infarcted areas was observed to be significantly lower in hearts from SCSE-treated hypercholesterolemic animals (p<0.05). The outcome of experiments conducted to assess the ratio of peak early diastolic velocity to peak atrial velocity (E’/A’ ratio) are shown in (Fig. 5). E’/A’ ratios were calculated from echocardio-graphic measurements conducted on each test group of rabbits. It was observed that hypercholesterolemic rabbits fed 30 mg/kg SCSE daily in addition to 2 % cholesterol (HC-Treated) during a 16-week period exhibited significantly higher E’/A’ ratios than hypercholes-terolemic animals not administered the extract (HC) (p<0.05) (5A). Tissue Doppler images produced by echocardiographic evaluation of hearts from each group of animals were used as the basis for E’/A’ determination are shown for control (5B), HC (5C) and HC-treated (5D) rabbits. Cytochrome c oxydase (COX) activity in cardiac tissue was measured in myocardium extracted from hearts of hypercholes-terolemic animals administered 2 % cholesterol-enriched feed with-out SCSE treatment (HC), or feed supplemented with 30 mg/kg SCSE (HC-treated). Each I/R heart was subjected to 30 minutes of global ischemia followed by 120 min of reperfusion, followed by evaluation of homogenized tissue samples for total COX activity using colorimetric assay for oxidation of mitochondrial ferrocyto-chrome c. The outcomes of these experiments, shown in (Fig. 6),reveal that SCSE-treated hypercholesterolemic animals exhibited significantly lower COX activity in cardiac tissue compared with rabbits in the untreated group (p<0.05). Myocardial tissue levels of three major mediators of cardiac homeostasis were determined by Western blot analysis. As shown in (Fig. 7), the presence of COX III (7A), HO-1 (7B), and VEGF (7C) was evaluated in tissue extracted from both I/R-injured and uninjured hearts of rabbits with or without hypercholesterolemia and fed either normal or cholesterol-rich diets. I/R-injured heart tissue from hypercholesterolemic rabbits administered SCSE was observed to contain significantly greater quantities of COX III and HO-1 protein (p<0.05), but not VEGF.
DISCUSSION Elevated levels of serum cholesterol correlate strongly with the occurrence and severity of cardiovascular disease, particularly athe-rosclerosis [24]. Cholesterol is a member of a class of compounds called sterols, which in vertebrates and a wide range of other organ-isms, are formed in the liver via the HMG-CoA reductase pathway from acetyl-coenzyme A [25]. Cholesterol is the major sterol pro-duced by animals and is a primary precursor for vitamin D, bile acids, and steroid hormones [26]. Its basic structure consists of an aliphatic chain linked to a planar segment of 4 aromatic rings and a hydroxyl (-OH) group, giving it both polar and non-polar regions that allow its incorporation into cell membranes in a configuration that confers membrane fluidity and permeability [25]. During the lifetime of an individual afflicted with hypercholes-terolemia, sustained high levels of serum cholesterol result in arte-rial stiffening and an accumulation of atheromatous plaques, caus-ing stenosis (narrowing) of the involved blood vessels. Rupture of plaques may cause clots and thrombus formations, resulting in ob-struction of blood vessels, heart attack, and stroke [27]. These proc-esses reduce tissue oxygenation, leading to ischemic injury to many organs, most notably tissues of the heart, kidneys, lungs, and brain [2]. In addition, the presence of a large number of macrophages in plaque matrices results in plaque material becoming a potent source
0 2 4 8 160
10
20
30controlHCtreated
*
week
Tota
l ser
um c
hole
ster
ol (m
mol
/l)
Control
HC
HC-Treated
0
20
40
60
80
100
*#
Athe
rosc
lero
tic c
over
age
(%)

6900 Current Pharmaceutical Design, 2013, Vol. 19, No. 39 Juhasz et al.
Fig. (4). Infarct Size in Isolated Working Heart. Hearts were isolated from 3 groups of rabbits (n = 6 per group), adminis-tered feed containing 2 % cholesterol during a 16-week time-course for a nonhypercholesterolemic group (control); a hypercholesterolemic group (HC); and a group of hypercholesterolemic animals treated daily with 30 mg/kg SCSE (HC-treated). Isolated working hearts were subjected to ischemia and reperfusion in modified Krebs-Henseleit bicarbonate buffer
using working heart apparatus. Infarct size was measured in hearts follow-ing reperfusion by perfusion with TTC solution, followed by microscopic analysis of transverse sections of each heart. Average sizes of infarct zone for hearts in each group ± SEM are shown for each treatment group. * p<0.05 for comparison of average % infarct size in hypercholesterolemic, SCSE-treated rabbits (HC-treated) versus hypercholesterolemic rabbits given no SCSE (HC).
of inflammatory cytokines and other mediators of inflammation [2], which lead to hyperstimulation of the primary immune response and a diverse range of pathologies [2]. HDL/LDL levels are significantly decreased in individuals af-flicted with hypercholesterolaemia [28, 29], a condition with both genetic and dietary/environmental contributors, in which excessive levels of cholesterol are present in the serum, predominantly in the LDL form [28, 30]. Chronic elevation of LDL cholesterol that oc-curs with hypercholesterolemia eventually develops into atheroscle-rosis, which is the leading cause of death in elderly humans [24, 31]. Hence, a major research imperative currently being pursued in cardiovascular medicine is the development of low-cost dietary countermeasures to the effects of hypercholesterolemia. The present investigation evaluated the effect of enhanced cho-lesterol intake on multiple parameters known to correlate with the pathogenesis of hypercholesterolemia, and examined the effect on
Fig. (3). Cardiac Function in Isolated Working Hearts. Hearts were isolated from 3 groups of rabbits (n = 6 per group), administered feed containing 2 % cholesterol during a 16-week time-course for a nonhyper-cholesterolemic group (control); a hypercholesterolemic group (HC); and a group of hypercholesterolemic animals treated daily with 30 mg/kg SCSE (HC-treated). Isolated working hearts harvested from animals in each group were subjected to global ischemia followed by either 60 or 120 min of reperfusion (I/R). Results are shown as average values from each group of animals ± SEM of heart rate (HR, beats/minute, 3A); aortic flow (AF, ml/minute, 3B); coronary flow (CF, ml/min, 3C); and left ventricular developed pressure (LVDP, mmHg, 3D). * p<0.05 for comparison of the magnitude of each cardiac function measured in hypercholesterolemic, SCSE-treated rabbits versus hypercholesterolemic rabbits given no SCSE. # p<0.05 for comparison of the magnitude of each cardiac function measured in hypercholesterolemic, hypercholesterolemic rabbits versus non-hyper-cholesterolaemic (control) group.
0
50
100
150
200
250
300
Preischemic 60 min ofReperfusion
120 min ofReperfusion
Hear
t Rat
e (b
eat/
min
)
Control
HC
HC-Treated
0
20
40
60
80
100
120
Preischemic 60 min ofReperfusion
120 min ofReperfusion
Aort
ic fl
ow (m
l/m
in)
Control
HC
HC-Treated
*
0
10
20
30
40
50
60
70
Preischemic 60 min ofReperfusion
120 min ofReperfusion
Coro
nary
flow
(ml/
min
)
Control
HC
HC-Treated
0
20
40
60
80
100
120
140
160
Preischemic 60 min ofReperfusion
120 min ofReperfusion
LVDP
(mm
Hg)
Control
HC
HC-Treated
A B
C D
#
#
#
#
#
#
Control
HC
HC-Treated
0
20
40
60
*#
Infa
rct S
ize
(%)

Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) Current Pharmaceutical Design, 2013, Vol. 19, No. 39 6901
Fig. (5A). E’/A’ ratios for rabbits fed 2 % cholesterol for 16 weeks, including nonhypercholesterolemic (control) rabbits, hypercholesterolemic ani-mals (HC) and hypercholesterolemic rabbits fed 30 mg/kg SCSE daily in addition to cholesterol (HC-treated). * p<0.05 for comparison of average E`/A` ratio in hypercholesterolemic, SCSE-treated rabbits (HC-treated) versus hypercholesterolemic rabbits given no SCSE (HC).
Fig. (5B). Nonhypercholesterolemic rabbits fed with normal chew for 16 weeks (control).
Fig. (5C). Hypercholesterolemic rabbits fed 2 % cholesterol for 16 weeks (HC). Treated
0
1
2
E'/A
' rat
io
Control
HC
HC-Treated*
E’ A’
E’ A’
6902 Current Pharmaceutical Design, 2013, Vol. 19, No. 39 Juhasz et al.
Fig. (5D). Hypercholesterolemic rabbits fed 2 % cholesterol and 30 mg/kg SCSE daily for 16 weeks (HC-treated). Tissue Doppler evaluations were conducted on 3 groups of rabbits (n = 4 per group), administered feed containing 2 % cholesterol during a 16-week time-course for a nonhypercholesterolemic group (Control); a hypercholesterolemic group (HC); and a group of hypercholesterolemic animals treated daily with 30 mg/kg SCSE (HC-treated). Echocardiographic measurements on anesthetized animals used a 7 MHz ultrasound probe and a Sequoia 512 echograph. Images obtained from ventricular septal walls of rabbit hearts were used to estimate the ratio of peak early diastolic velocity to peak atrial velocity (E’/A’ ratio) repre-sented as histograms in figure 5A as averages for each treatment group ± SEM. The relative magnitude of E’ and A’ were obtained by measurement of the extent to which mitral annular systolic tissue Doppler velocities (S’) and longitudinal contractile function of the left ventricular myocardium correlate with relaxing function of the left ventricular myocardium, and late diastolic annular velocities (A’); and how these variables relate to pumping function of the left atrium. These outcomes for any particular heart may be readily visualized in the Doppler image and are shown for hearts of representative animals in the non-hypercholesterolemic control group (5B); hypercholesterolemic animals (5C); and a group of SCSE-treated hypercholesterolemic rabbits (5D). The tissue Doppler images which are shown in figures 5B, 5C and 5D demonstrate the lateral and septal mitral annular velocities.
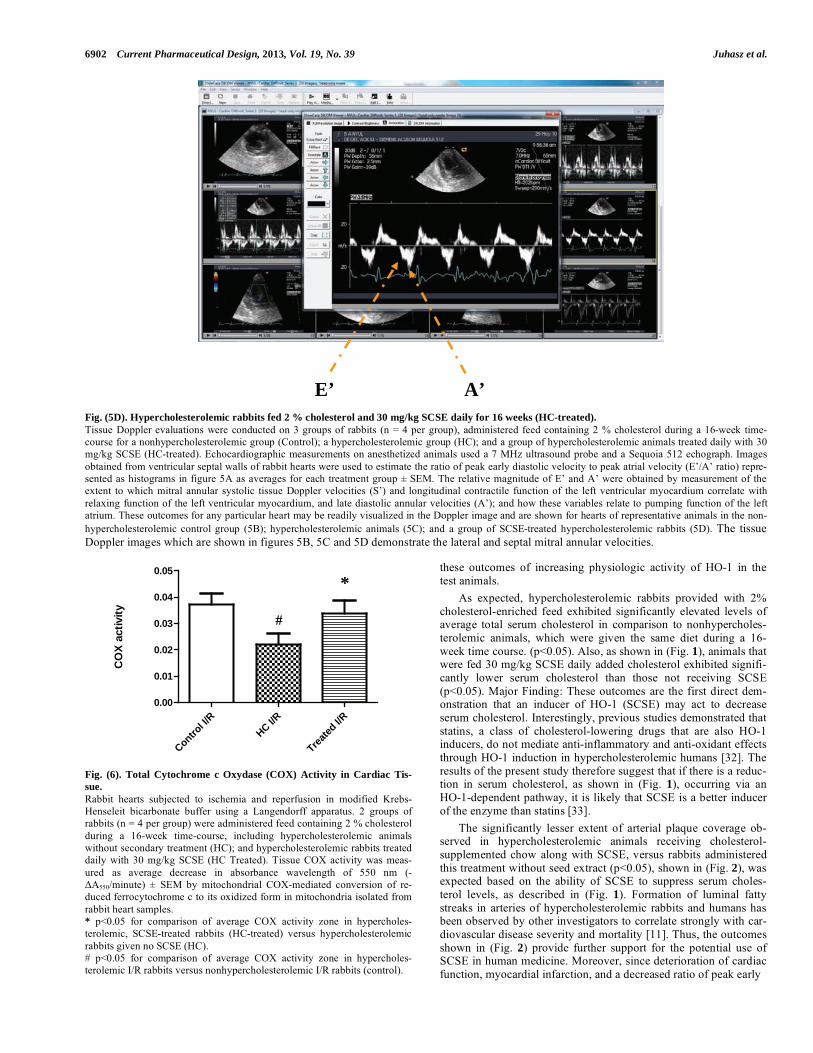
Fig. (6). Total Cytochrome c Oxydase (COX) Activity in Cardiac Tis-sue. Rabbit hearts subjected to ischemia and reperfusion in modified Krebs-Henseleit bicarbonate buffer using a Langendorff apparatus. 2 groups of rabbits (n = 4 per group) were administered feed containing 2 % cholesterol during a 16-week time-course, including hypercholesterolemic animals without secondary treatment (HC); and hypercholesterolemic rabbits treated daily with 30 mg/kg SCSE (HC Treated). Tissue COX activity was meas-ured as average decrease in absorbance wavelength of 550 nm (-�A550/minute) ± SEM by mitochondrial COX-mediated conversion of re-duced ferrocytochrome c to its oxidized form in mitochondria isolated from rabbit heart samples. * p<0.05 for comparison of average COX activity zone in hypercholes-terolemic, SCSE-treated rabbits (HC-treated) versus hypercholesterolemic rabbits given no SCSE (HC). # p<0.05 for comparison of average COX activity zone in hypercholes-terolemic I/R rabbits versus nonhypercholesterolemic I/R rabbits (control).
these outcomes of increasing physiologic activity of HO-1 in the test animals. As expected, hypercholesterolemic rabbits provided with 2% cholesterol-enriched feed exhibited significantly elevated levels of average total serum cholesterol in comparison to nonhypercholes-terolemic animals, which were given the same diet during a 16-week time course. (p<0.05). Also, as shown in (Fig. 1), animals that were fed 30 mg/kg SCSE daily added cholesterol exhibited signifi-cantly lower serum cholesterol than those not receiving SCSE (p<0.05). Major Finding: These outcomes are the first direct dem-onstration that an inducer of HO-1 (SCSE) may act to decrease serum cholesterol. Interestingly, previous studies demonstrated that statins, a class of cholesterol-lowering drugs that are also HO-1 inducers, do not mediate anti-inflammatory and anti-oxidant effects through HO-1 induction in hypercholesterolemic humans [32]. The results of the present study therefore suggest that if there is a reduc-tion in serum cholesterol, as shown in (Fig. 1), occurring via an HO-1-dependent pathway, it is likely that SCSE is a better inducer of the enzyme than statins [33]. The significantly lesser extent of arterial plaque coverage ob-served in hypercholesterolemic animals receiving cholesterol-supplemented chow along with SCSE, versus rabbits administered this treatment without seed extract (p<0.05), shown in (Fig. 2), was expected based on the ability of SCSE to suppress serum choles-terol levels, as described in (Fig. 1). Formation of luminal fatty streaks in arteries of hypercholesterolemic rabbits and humans has been observed by other investigators to correlate strongly with car-diovascular disease severity and mortality [11]. Thus, the outcomes shown in (Fig. 2) provide further support for the potential use of SCSE in human medicine. Moreover, since deterioration of cardiac function, myocardial infarction, and a decreased ratio of peak early
E’ A’
Control I/
RHC I/R
Treated
I/R0.00
0.01
0.02
0.03
0.04
0.05*
CO
X ac
tivity #

Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) Current Pharmaceutical Design, 2013, Vol. 19, No. 39 6903
Fig. (7). Western Blot Analysis for Biomarkers of Cardiac Tissue Func-tion. Expression of COX III (7A), VEGF (7B), and HO-1 (7C) protein in rabbit myocardium was measured in homogenized cardiac tissue samples drawn from 4 test groups (n = 6 per group), defined as follows: 1. I/R-injured hearts from non-hypercholesterolemic animals fed with normal, non-cholesterol-supplemented chow (Control); 2. Non-I/R-injured hearts from nonhypercholesterolemic animals fed with 2 % cholesterol-supplemented chow (HC baseline); 3. I/R-injured hearts from hypercholesterolemic ani-mals fed with 2 % cholesterol-supplemented chow. (HC I/R); 4. I/R-injured hearts from hypercholesterolemic animals fed with 2 % cholesterol-supplemented chow treated with 30 mg/kg SCSE (HC I/R treated). GAPDH, and COX IV expression level was measured as a reference protein. Western blot analyses were conducted on each tissue homogenate in triplicate and the signal intensity of resulting bands corresponding to proteins of interest was measured using the Scion for Windows Densitometry Image program, Alpha 4.0.3.2. Tissue content of each protein is shown in arbitrary units as the mean for each group of rabbits ±SEM. * p<0.05 for comparison of average levels of COX III, HO-1 and VEGF in myocardium of hypercholesterolemic, SCSE-treated rabbits (HC-treated) versus hypercholesterolemic rabbits given no SCSE (HC).
diastolic velocity to peak atrial velocity (E’/A’ ratio) are major indicators of hypercholesterolemia-associated heart disease [34-36], the ability of SCSE to significantly improve each of these measures relative to rabbits receiving no SCSE extract (p<0.05, (Figs. 3, 4,and 5)) is additional evidence for the preventive and therapeutic value of this extract. As shown in (Figs. 6 and 7A), relative to I/R-injured heart tis-sue from untreated hypercholesterolemic animals, hearts taken from SCSE-treated animals exhibited significantly elevated activity of cytochrome c oxidase (COX) and expression of COX protein (p<0.05). The role of COX in regulating ATP synthesis and me-tabolism [37] offers novel strategies by which agents such as SCSE that modulate COX to potentially exert highly beneficial effects on general health – with particular relevance in cardiovascular medi-cine. The lack of significant differences in VEGF content of I/R-injured heart tissue of cholesterol-fed, SCSE-treated rabbits versus animals not fed the extract (7B) is difficult to comprehensively interpret based on the current data. This signaling molecule is angi-ogenic and stimulates vascularization in response to injury as well as during embryonic development, but it may also contribute to tumor survival through neovascularization [38, 39]. Tissue damage in coronary artery disease due to a depletion of regenerative endo-thelial progenitor cells may be counteracted with statins, and also with VEGF [40]. The authors of the present study therefore evalu-ated the capacity of SCSE, which like statins is an HO-1 inducer, to stimulate VEGF expression. The failure of SCSE to induce signifi-cantly higher VEGF levels in heart tissue suggests that statin-mediated VEGF induction is not an event downstream of HO-1 production. The clinical significance of these observations remains to be determined. The data in (Fig. 7C) shows that HO-1 protein expression in I/R-injured hearts of SCSE-treated hypercholesterolemic animals is significantly higher than rabbits not receiving the extract (p<0.05). This outcome is expected based on the known properties of SCSE [2]. In recent years, HO-1 has emerged as a particularly attractive tool for the prevention and management of a broad range of human and animal diseases characterized by elevated levels of reactive oxygen-containing molecules[2]. A major mechanism by which the
Figure 7A
Figure 7B
Control
HC baseli
neHC I/R
HC I/R Trea
ted0
5000
10000
15000
20000
25000C
OX
III-p
rote
in le
vel
Control
HC baseli
neHC I/R
HC I/R Trea
ted0
10000
20000
30000
HO
-1 p
rote
in le
vel
*
*
32kD
Figure 7C
Control
HC baseli
neHC I/R
HC I/R Trea
ted0
10000
20000
30000
VEG
F pr
otei
n le
vel
GAPDH�protein�level�
COX�IV�protein�level��(mitochondrial�housekeeping�protein)�

6904 Current Pharmaceutical Design, 2013, Vol. 19, No. 39 Juhasz et al.
enzyme contributes to antioxidant defense is through suppression by bilirubin (a heme degradation metabolite) of NADPH oxidase, a major physiologic source of reactive oxygen. This inhibition has been shown to be a potent contributor to protection against oxida-tive tissue damage in cardiovascular disease and many other serious chronic diseases [2, 41-44]. Animals in all studies except for those producing data shown in (Fig. 7) were fed chow containing 2% cholesterol for 16-weeks. This condition was included as an experimental constant, expected to result in significant upregulation of each of the selected patho-logical features with particularly high values expected in hypercho-lesterimic animals. These outcomes were further expected to enable clear demonstration of the effect of treatment with SCSE and it was not deemed necessary to evaluate the effect of normal, versus cho-lesterol-enhanced chow. The authors departed from this basic strat-egy in design of the experiments shown in (Fig. 7). Here, the authors reasoned that the contrast in tissue content of COX, VEGF and HO-1 between SCSE-treated, versus untreated might be illus-trated more clearly if shown in comparison with samples from ani-mals in which the basic, cholesterol amplifying condition was omit-ted. Results shown in (Fig. 7) suggest that although inclusion of groups not receiving cholesterol-supplemented feed was not strictly necessary to demonstrate effect of SCSE, inclusion of this group provided additional clarity as to the result of 2% cholesterol on each parameter measured. SCSE has potential to emerge as a major contributor to preven-tion and management of cardiovascular disease, and many other disorders characterized by disregulated inflammation. Other than low cost and broad availability, the benefit to patients of using SCSE-based therapies is the negligible toxicity of this plant mate-rial [15]. This is contrasted with the risk posed to patients by the anti-hypercholesterolemic drugs that are currently in use. Examples include simvastatin, lovastatin, atorvastatin, rosuvastatin, and others which may have adverse side effects, such as rhabdomyolysis. Therefore, SCSE is potentially a very valuable adjuvant to statins. Many other healthcare applications are possible for this fascinating and valuable plant material.
CONFLICT OF INTEREST The authors confirm that this article content has no conflicts of interest.
ACKNOWLEDGEMENTS This study was supported by grants from OTKA (78223, 104017), OTKA-K 83478, and in part by the project of New Hun-gary Development Plan, co-financed by the European Union and the European Social Fund of TAMOP-4.2.1/B-09/1/KONV-2010-0007, TAMOP-4.2.2./B-10/1-2010-0024, and TAMOP-4.2.2.A-11/1/KONV-2012-0045. MTA-DE Vascular Biology, Thrombosis and Hemostasis Research Group are supported by the Hungarian Academy of Sciences (MTA-DE Vasc. Biol. 11003). The research took place under the project with identification number of TÁMOP 4.2.4.A/2-11-1-2012-0001 entitled “National Excellence Program – Convergence program for elaboration and operation of support-system sponsoring Hungarian students and researchers”, funded by the European Union, co-financed by the European Social Fund. The authors are sincerely grateful to Stephanie C. Fox, J.D. of QueenBeeEdit of Bloomfield Connecticut, U.S.A. ([email protected]) for her hard work in organizing, formatting, and editing this article.
REFERENCES[1] McClintock D, Gordon LB, Djabali K. Hutchinson-Gilford
progeria mutant lamin A primarily targets human vascular cells as detected by an anti-Lamin A G608G antibody. Proc Natl Acad Sci USA 2006; 103: 2154-9.
[2] Haines DD, Lekli I, Teissier P, Bak I, Tosaki A. Role of haeme oxygenase-1 in resolution of oxidative stress-related pathologies: focus on cardiovascular, lung, neurological and kidney disorders. Acta Physiol (Oxf) 2012; 204: 487-501.
[3] Hussain MM. A proposed model for the assembly of chylomicrons. Atherosclerosis 2000; 148: 1-15.
[4] Nakano T, Nakajima K, Niimi M, et al. Detection of apolipoproteins B-48 and B-100 carrying particles in lipoprotein fractions extracted from human aortic atherosclerotic plaques in sudden cardiac death cases. Clin Chim Acta 2008; 390: 38-43.
[5] Toth PP. Cardiology patient page. The "good cholesterol": high-density lipoprotein. Circulation 2005; 111: e89-91.
[6] Israili ZH, Lyoussi B, Hernandez-Hernandez R, Velasco M. Metabolic syndrome: treatment of hypertensive patients. Am J Ther 2007; 14: 386-402.
[7] Liebson PR, Amsterdam EA. Prevention of coronary heart disease. Part I. Primary prevention. Dis Mon 1999; 45: 497-571.
[8] Safeer RS, Cornell MO. The emerging role of HDL cholesterol. Is it time to focus more energy on raising high-density lipoprotein levels? Postgrad Med 2000; 108: 87-90, 93-8.
[9] Hausenloy DJ, Yellon DM. Targeting residual cardiovascular risk: raising high-density lipoprotein cholesterol levels. Heart 2008; 94: 706-14.
[10] Thijssen MA, Mensink RP. Fatty acids and atherosclerotic risk. Handb Exp Pharmacol 2005: 165-94.
[11] Masson D, Deckert V, Gautier T, et al. Worsening of diet-induced atherosclerosis in a new model of transgenic rabbit expressing the human plasma phospholipid transfer protein. Arterioscler Thromb Vasc Biol 2011; 31: 766-74.
[12] Gysembergh A, Kloner RA, Przyklenk K. Pretreatment with the gap junction uncoupler heptanol does not limit infarct size in rabbit heart. Cardiovasc Pathol 2001; 10: 13-7.
[13] Przyklenk K, Li G, Simkhovich BZ, Kloner RA. Mechanisms of myocardial ischemic preconditioning are age related: PKC-epsilon does not play a requisite role in old rabbits. J Appl Physiol 2003; 95: 2563-9.
[14] Szabo ME, Gallyas E, Bak I, et al. Heme oxygenase-1-related carbon monoxide and flavonoids in ischemic/reperfused rat retina. Invest Ophthalmol Vis Sci 2004; 45: 3727-32.
[15] Bak I, Czompa A, Csepanyi E, et al. Evaluation of systemic and dermal toxicity and dermal photoprotection by sour cherry kernels. Phytother Res 2011; 25: 1714-20.
[16] Bartekova M, Carnicka S, Pancza D, Ondrejcakova M, Breier A, Ravingerova T. Acute treatment with polyphenol quercetin improves postischemic recovery of isolated perfused rat hearts after global ischemia. Can J Physiol Pharmacol 2010; 88: 465-71.
[17] Das S, Mukherjee S, Lekli I, et al. Tocotrienols confer resistance to ischemia in hypercholesterolemic hearts: insight with genomics. Mol Cell Biochem 2012; 360: 35-45.
[18] Neely JR, Liebermeister H, Battersby EJ, Morgan HE. Effect of pressure development on oxygen consumption by isolated rat heart. Am J Physiol 1967; 212: 804-14.
[19] Juhasz B, Der P, Turoczi T, Bacskay I, Varga E, Tosaki A. Preconditioning in intact and previously diseased myocardium: laboratory or clinical dilemma? Antioxid Redox Signal 2004; 6: 325-33.
[20] Schultz JE, Yao Z, Cavero I, Gross GJ. Glibenclamide-induced blockade of ischemic preconditioning is time dependent in intact rat heart. Am J Physiol 1997; 272: H2607-15.
[21] Dickson EW, Blehar DJ, Carraway RE, Heard SO, Steinberg G, Przyklenk K. Naloxone blocks transferred preconditioning in isolated rabbit hearts. J Mol Cell Cardiol 2001; 33: 1751-6.
[22] Csonka C, Kupai K, Kocsis GF, et al. Measurement of myocardial infarct size in preclinical studies. J Pharmacol Toxicol Methods 2010; 61: 163-70.
[23] Salloum FN, Takenoshita Y, Ockaili RA, et al. Sildenafil and vardenafil but not nitroglycerin limit myocardial infarction through opening of mitochondrial K(ATP) channels when administered at reperfusion following ischemia in rabbits. J Mol Cell Cardiol 2007; 42: 453-8.
[24] Libby P. Managing the risk of atherosclerosis: the role of high-density lipoprotein. Am J Cardiol 2001; 88: 3N-8N.
[25] Fahy E, Subramaniam S, Brown HA, et al. A comprehensive classification system for lipids. J Lipid Res 2005; 46: 839-61.

Cardioprotective Effects of Sour Cherry Seed Extract (SCSE) Current Pharmaceutical Design, 2013, Vol. 19, No. 39 6905
[26] Hanukoglu I. Steroidogenic enzymes: structure, function, and role in regulation of steroid hormone biosynthesis. J Steroid Biochem Mol Biol 1992; 43: 779-804.
[27] Finn AV, Nakano M, Narula J, Kolodgie FD, Virmani R. Concept of vulnerable/unstable plaque. Arterioscler Thromb Vasc Biol 2010; 30: 1282-92.
[28] Guerin M. Reverse cholesterol transport in familial hypercholesterolemia. Curr Opin Lipidol 2012; 23: 377-85.
[29] Rana JS, Boekholdt SM, Kastelein JJ, Shah PK. The role of non-HDL cholesterol in risk stratification for coronary artery disease. Curr Atheroscler Rep 2012; 14: 130-4.
[30] Durrington P. Dyslipidaemia. Lancet 2003; 362: 717-31. [31] Bhatnagar D, Soran H, Durrington PN. Hypercholesterolaemia and
its management. BMJ 2008; 337: a993. [32] Ong WY, Tan B, Pan N, et al. Increased iron staining in the
cerebral cortex of cholesterol fed rabbits. Mech Ageing Dev 2004; 125: 305-13.
[33] Ravingerova T, Adameova A, Kelly T, et al. Changes in PPAR gene expression and myocardial tolerance to ischaemia: relevance to pleiotropic effects of statins. Can J Physiol Pharmacol 2009; 87: 1028-36.
[34] Benn M, Watts GF, Tybjaerg-Hansen A, Nordestgaard BG. Familial Hypercholesterolemia in the Danish General Population: Prevalence, Coronary Artery Disease, and Cholesterol-Lowering Medication. J Clin Endocrinol Metab 2012.
[35] Le Grand B, Vie B, Faure P, Degryse AD, Mouillard P, John GW. Increased resistance to ischaemic injury in the isolated perfused atherosclerotic heart of the cholesterol-fed rabbit. Cardiovasc Res 1995; 30: 689-96.
[36] Rubinstein J, Pelosi A, Vedre A, Kotaru P, Abela GS. Hypercholesterolemia and myocardial function evaluated via tissue doppler imaging. Cardiovasc Ultrasound 2009; 7: 56.
[37] Li T, Matozel M, Boehme S, et al. Overexpression of cholesterol 7alpha-hydroxylase promotes hepatic bile acid synthesis and secretion and maintains cholesterol homeostasis. Hepatology 2011; 53: 996-1006.
[38] Amo Y, Masuzawa M, Hamada Y, Katsuoka K. Expression of vascular endothelial growth factor in a human hemangiosarcoma cell line (ISO-HAS). Arch Dermatol Res 2001; 293: 296-301.
[39] Holmes K, Roberts OL, Thomas AM, Cross MJ. Vascular endothelial growth factor receptor-2: structure, function, intracellular signalling and therapeutic inhibition. Cell Signal 2007; 19: 2003-12.
[40] Urbich C, Dimmeler S. Risk factors for coronary artery disease, circulating endothelial progenitor cells, and the role of HMG-CoA reductase inhibitors. Kidney Int 2005; 67: 1672-6.
[41] Csont T, Bereczki E, Bencsik P, et al. Hypercholesterolemia increases myocardial oxidative and nitrosative stress thereby leading to cardiac dysfunction in apoB-100 transgenic mice. Cardiovasc Res 2007; 76: 100-9.
[42] Kocsis GF, Csont T, Varga-Orvos Z, Puskas LG, Murlasits Z, Ferdinandy P. Expression of genes related to oxidative/nitrosative stress in mouse hearts: effect of preconditioning and cholesterol diet. Med Sci Monit 2010; 16: BR32-9.
[43] Datla SR, Dusting GJ, Mori TA, Taylor CJ, Croft KD, Jiang F. Induction of heme oxygenase-1 in vivo suppresses NADPH oxidase derived oxidative stress. Hypertension 2007; 50: 636-42.
[44] Schulz R, Wambolt R. Inhibition of nitric oxide synthesis protects the isolated working rabbit heart from ischaemia-reperfusion injury. Cardiovasc Res 1995; 30: 432-9.
Received: March 6, 2013 Accepted: April 9, 2013