Inflammatory choroidal neovascularization associated with ...

Choroidal Volume Variations with Age,Axial Length, and Sex in Healthy Subjects:A Three-Dimensional Analysis
Giulio Barteselli, MD, Jay Chhablani, MD, Sharif El-Emam, MD, Haiyan Wang, MD, Janne Chuang, BS,Igor Kozak, MD, Lingyun Cheng, MD, Dirk-Uwe Bartsch, PhD, William R. Freeman, MD
Purpose: To demonstrate the 3-dimensional choroidal volume distribution in healthy subjects using en-hanced depth imaging (EDI) spectral-domain optical coherence tomography (SD-OCT) and to evaluate itsassociation with age, sex, and axial length.
Design: Retrospective case series.Participants: A total of 176 eyes from 114 subjects with no retinal or choroidal disease.Methods: The EDI SD-OCT imaging studies of healthy patients who had undergone a 31-raster scanning
protocol on a commercial SD-OCT device were reviewed. Manual segmentation of the choroid was performedby 2 retinal specialists. A macular choroidal volume map and 3-dimensional topography were automaticallycreated by the built-in software of the device. Mean choroidal volume was calculated for each Early TreatmentDiabetic Retinopathy Study (ETDRS) subfield. Regression analyses were used to evaluate the correlationbetween macular choroidal volume and age, sex, and axial length.
Main Outcome Measures: Three-dimensional topography and ETDRS-style volume map of the choroid.Results: Three-dimensional topography of the choroid and volume map was obtained in all cases. The
mean choroidal volume was 0.228�0.077 mm3 for the center ring and 7.374�2.181 mm3 for the total ETDRSgrid. The nasal quadrant showed the lowest choroidal volume, and the superior quadrant showed the highestchoroidal volume. The temporal and inferior quadrants did not show different choroidal volume values.Choroidal volume in all the EDTRS rings was significantly correlated with axial length after adjustment for age(P � 0.0001), age after adjustment for axial length (P � 0.0001), and sex after adjustment for axial length(P � 0.05). Choroidal volume decreases by 0.54 mm3 (7.32%) for every decade and by 0.56 mm3 (7.59%) forevery millimeter of axial length. Male subjects have a 7.37% greater choroidal volume compared with thatof female subjects.
Conclusions: Enhanced depth imaging SD-OCT is a noninvasive and well-tolerated procedure with anexcellent ability to visualize 3-dimensional topography of the choroid and to measure choroidal volume at theposterior pole using manual segmentation. Age and axial length are inversely correlated with choroidal volume,most likely leading to changes in retinal metabolic support in elderly, highly myopic patients. Sexual differencesshould be considered when interpreting an EDI SD-OCT scan of the choroid.
Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussedin this article. Ophthalmology 2012;119:2572–2578 © 2012 by the American Academy of Ophthalmology.
pq
phvmtaEma
The choroid has various valuable functions in the eye,including metabolic support of the retinal pigment epithe-lium (RPE) and the retina1 and blood supply to the outerretinal layers. However, the choroid also is involved in thepathogenesis of several vision-threatening diseases, such asage-related macular degeneration (AMD),2 polypoidal cho-roidal vasculopathy,3 central serous chorioretinopathy,4
Vogt–Koyanagi–Harada disease,5 and high myopia–relatedchorioretinopathy.6
Visualization of the choroid by indirect ophthalmoscopyand fluorescein angiography is difficult because pigment inthe RPE and choroid obstructs the view. Indocyanine green
angiography allows for visualization of choroidal vessel m2572 © 2012 by the American Academy of OphthalmologyPublished by Elsevier Inc.
erfusion but does not provide 3-dimensional anatomic anduantitative evaluations.
By using a spectral-domain optical coherence tomogra-hy (SD-OCT) device, Spaide et al7 developed the en-anced depth imaging (EDI) technique, which enables inivo imaging and measurement of the choroid.7 Since then,any investigators have performed a bi-dimensional de-
ailed analysis of the choroid among healthy patients8–12
nd patients with chorioretinal pathologies,13–27 using theDI technique on various SD-OCT devices. Because auto-ated choroidal segmentation software remains unavail-
ble, choroidal thickness measurements were performed
anually, and choroidal thickness was measured only atISSN 0161-6420/12/$–see front matterhttp://dx.doi.org/10.1016/j.ophtha.2012.06.065

inWcaso
csJdcH
CTticmw3fqT
CTtdmaa3mttqgaocct
sm(�alt
SStasvpa
Barteselli et al � 3D Analysis of the Choroid
selected points along a single horizontal or vertical SD-OCTB-scan passing through the fovea. As a result, exhaustiveinformation about the real volume of the choroid usingSD-OCT is limited.
Previous studies have reported choroidal thickness mea-surements at the fovea and selected points of the choroid inhealthy eyes.8,26,28–30 However, the choroidal thicknessmeasurements in these studies differ from each other, pos-sibly because of limited sample size, different image acqui-sition techniques, and inconsistencies in choosing the loca-tions for repeated measurement. Moreover, the irregularityof the inner chorioscleral border influences the measure-ment at few sampling points.26,27 To overcome this prob-lem, evaluation of the choroid over the entire posterior polewould be a better tool to evaluate chorioretinal diseases.
Choroidal thickness mapping has been reported by Ouy-ang et al,31 who used EDI SD-OCT and manual segmenta-tion. Choroidal volume mapping was introduced by Hirataet al,32 who used an experimental swept-source opticalcoherence tomography at 1050 nm, which is not commer-cially available. Shin et al33 calculated an interpolated cho-roidal volume measurement using a 6-radial scan protocolon a conventional SD-OCT (3D OCT-2000, Topcon Cor-poration, Tokyo, Japan). However, the chorioscleral bound-ary was not detected in all the cases because of scatteringand low penetration of the used wavelength through theRPE. Moreover, inadequate averaging (8 images) and dis-proportionate interpolation due to few (6) scans used mayhave compromised the validity of the measurements.
In a previous report by our group,34 we devised aninnovative method of choroidal volume measurementusing the built-in software for retinal volume measure-ment of an EDI SD-OCT after manual choroidal segmen-tation on a 31-raster scan protocol. Interobserver andintraobserver reproducibility and repeatability of thismethod were excellent.34
The aim of the present study was to perform a 3-dimensional topographic visualization of the choroidal vol-ume of the posterior pole in a large sample of healthysubjects and to assess the correlation of the volume withage, sex, and axial length.
Materials and Methods
Study PopulationStarting in July 2011, all patients undergoing SD-OCT scans at theJacobs Retina Center at Shiley Eye Center, University of Califor-nia San Diego (La Jolla, CA) underwent choroidal imaging as partof their evaluation. A raster scan of the macula using an SD-OCTdevice in EDI mode (Heidelberg Spectralis HRA2; HeidelbergEngineering, Carlsbad, CA) was used to study the choroid. Theraster scan required approximately 30 seconds of additional timeand was therefore incorporated into the standard scanning proto-col. After approval by the institutional review board of the Uni-versity of California at San Diego for chart review and dataanalysis, we retrospectively reviewed charts and images of 176healthy eyes from 114 patients who underwent multimodal exam-ination to rule out retinal pathologies or to document floaters andposterior vitreous detachment over a 3-month period (July 2011
through September 2011). To be considered eligible for data and rmage analysis as part of this study, patients’ eyes must have hado pathology other than floaters and posterior vitreous detachment.e excluded eyes/patients with any systemic or local disease that
ould affect the choroid, including uncontrolled hypertension, di-betes, coagulopathies, AMD, polypoidal choroidal vasculopathy,erous chorioretinopathy, Vogt–Koyanagi–Harada disease, orther conditions that have been shown to affect the choroid.
Patients underwent ophthalmic evaluation, including best-orrected visual acuity, slit-lamp biomicroscopy, axial length mea-urement using ocular biometry (IOLMaster; Carl Zeiss Meditec,ena, Germany), and a raster scan of the macula using the SD-OCTevice in EDI mode without pupillary dilation. The study wasonducted in adherence with the tenets of the Declaration ofelsinki.
horoidal Volume Scanning Protocolhe scanning protocol included 31 high-resolution B-scans cen-
ered at the fovea, associated with a simultaneous near-infraredmage with undilated pupils. An internal fixation light was used toenter the scanning area on the fovea. Each scan was approxi-ately 9.3 mm in length and spaced 240 �m apart. All 31 B-scansere acquired in a continuous, automated sequence and covered a0�25–degree area centered on the fovea. A minimum of 25rames were automatically averaged and used to obtain a good-uality choroidal image using the built-in TruTrack Active Eyeracking software of the device (Heidelberg Engineering).
horoidal Volume Image Analysiswo retinal specialists manually performed the choroidal segmen-
ation by applying a previously described method.34 A 6-mm–iameter choroidal volume map, centered on the fovea, was auto-atically generated by the built-in software of the device by
pplying the grid used by the Early Treatment Diabetic Retinop-thy Study (ETDRS).35 The ETDRS grid divides the macula intoconcentric rings (center, inner, and outer), with the inner ringeasuring 1 to 3 mm and the outer ring measuring 3 to 6 mm from
he center (referring to a ring with a diameter of 1 mm centered onhe fovea). The grid further divides inner and outer rings into 4uadrants (superior, inferior, temporal, and nasal); thus, the ETDRSrid divides the macula into 9 subfields. After generating thicknessnd volume maps, 3-dimensional topography of the choroid wasbtained using the same built-in software of the device, and a color-oded thickness map was superimposed on the inner surface of thehoroid in the topographic image using Photoshop CS3 (Adobe Sys-ems Inc., San Jose, CA).
Choroidal volume maps were grouped by axial length, age, andex to facilitate the clinical applications of our findings. To deter-ine the axial length, we judged the eyes’ refraction to be myopic
axial length �24.5 mm), emmetropic (axial length �23.4 mm and24.5 mm), or hyperopic (axial length �23.4 mm) on the basis ofnormal axial length variation with refraction and age found in the
iterature.36,37 Eyes were divided into 3 age groups: eyes of pa-ients aged �40 years, 41 to 60 years, and �61 years.
tatistical Analysistatistical analysis was performed using the Statistical Package for
he Social Sciences version 20 (SPSS Inc., Chicago, IL). All valuesre presented as mean � standard deviation. The Fisher leastignificant difference test was used to compare the choroidalolume at different ETDRS subfields. Pearson’s correlation, inde-endent samples t test, and partial correlation were calculated tossess the relationship of the choroidal volume in the 3 ETDRS
ings of the macula35 with 3 independent factors, including age,2573

crrdit
ccrciqnetD
taa(
Ophthalmology Volume 119, Number 12, December 2012
axial length, and sex. Multiple linear regression analysis was usedto evaluate the correlation between the choroidal volume of eachring and the same grouped factors, dividing eyes by age, axiallength, and sex of the patients. P � 0.05 was considered to bestatistically significant.
Results
A total of 176 eyes of 114 healthy subjects (51 men and 63women), with a mean age of 50 years (range, 14–89 years), wereincluded in the study. Ethnic distribution included 75 Caucasiansubjects, 20 Asian subjects, 18 Hispanic subjects, and 1 blacksubject. A total of 160 eyes were phakic, and 16 eyes werepseudophakic. The best-corrected visual acuity ranged from 20/63to 20/20 (Snellen equivalent). Axial length measurement wasavailable for 146 of 176 eyes (83%). The mean axial length was24.6�1.6 mm (range, 21.03–31.56 mm).
By using high-resolution B-scans and a minimum averaging of25 frames, the choroidal borders were clearly detected in all cases;no eye was excluded because of poor-quality choroidal images.The basement membrane of the RPE appeared as a regular hyper-
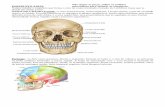
Figure 2. A 3-dimensional topographic visualization of the choroid withan axial length of 23.2 mm (A–D) and an eye with an axial length of 26other quadrants, and the nasal quadrant is the thinnest.
reflective line, with a concave aspect toward the choroid. The c
2574
horioscleral interface (outer border of the choroid) appeared ir-egular and corrugated, following the course of the deepest cho-oidal vessels (Fig 1, available at http://aaojournal.org). Three-imensional choroidal topography and volume map were obtainedn all eyes (Fig 2). In none of the cases did the built-in software failo reconstruct the map or topography.
Table 1 (available at http://aaojournal.org) shows the meanhoroidal volume in each area of the ETDRS map. The meanhoroidal volume of the fovea was 0.228�0.077 mm3; the innering choroidal volume was 1.748�0.558 mm3, and the outer ringhoroidal volume was 5.398�1.566 mm3. The choroidal volumen the nasal quadrant was significantly lower than in all the otheruadrants (P � 0.0001), whereas the superior quadrant had a sig-ificantly higher choroidal volume than all the others. No differ-nces were noted in the choroidal volume between the inferior andemporal quadrants. The mean choroidal volume of the total ET-RS map was 7.374�2.181 mm3.
Table 2 (available at http://aaojournal.org) shows a correla-ion analysis between the mean choroidal volume of each ring,ge, axial length, and sex. The mean choroidal volume showed
negative correlation with age (P � 0.01) and axial lengthP � 0.01) in the fovea and inner and outer rings (Pearson’s
rimposed color-coded choroidal thickness map (microns) in an eye with(E–H). The superior quadrant of the macula appears thicker than the
a supe.5 mm
orrelation). For the total macular area, a low-grade correlation

8iatmapa7
(uirlcoc
D
Imutbdtb
rStscr0irm
Barteselli et al � 3D Analysis of the Choroid
was found with age (P � 0.01; r��0.387) and axial length(P � 0.01; r��0.349). No correlation with sex was noted(independent samples t test). After adjustment for axial lengthusing partial correlation analysis, the mean choroidal volumecorrelated significantly with age (P � 0.0001) and sex(P � 0.05) in all the rings. After adjustment for age, the meanchoroidal volume in all the rings was highly correlated withaxial length (P � 0.0001).
Table 3 shows the results of the multiple linear regressionanalysis for mean choroidal volume of the fovea, inner ring, outerring, and total macula. A stepwise method was used to determinethe most unexpected factors. The model determined by age, axiallength, and sex had the best regression. The model showed a goodcoefficient of determination, which was 0.568 (R2�0.323) for thetotal macular choroidal volume.
Table 3. Multiple Linear Regression Analysis for ChoroidalVolume of the Macula by Age, Axial Length, and Sex for Each
Early Treatment Diabetic Retinopathy Study Ring
Factor Coefficient Standard Error R2 P
CenterIntercept 0.861 0.094 0.275 �0.0001Age �0.001 0.000 0.275 �0.0001Axial length �0.021 0.003 0.275 �0.0001Sex �0.025 0.011 0.275 �0.05
Inner circleIntercept 6.346 0.693 0.285 �0.0001Age �0.011 0.002 0.285 �0.0001Axial length �0.153 0.026 0.285 �0.0001Sex �0.180 0.084 0.285 �0.05
Outer circleIntercept 18.300 1.866 0.334 �0.0001Age �0.038 0.006 0.334 �0.0001Axial length �0.405 0.069 0.334 �0.0001Sex �0.664 0.226 0.334 �0.01
Total ETDRS mapIntercept 25.507 2.621 0.323 �0.0001Age �0.051 0.009 0.323 �0.0001Axial length �0.579 0.097 0.323 �0.0001Sex �0.869 0.317 0.323 �0.01
ETDRS � Early Treatment Diabetic Retinopathy Study.
Table 4. Choroidal Volume Measurements for Early Treatmentan
Center Inner Ri
Mean (mm3) SD Mean (mm3)
Age (yrs)�40 (n � 59) 0.255 0.080 1.95041–60 (n � 60) 0.222 0.067 1.714�61 (n � 57) 0.206 0.076 1.576
Axial length*Hyperopic (n � 35) 0.273 0.076 2.052Emmetropic (n � 42) 0.237 0.073 1.810Myopic (n � 69) 0.202 0.068 1.570
SexMale (n � 79) 0.235 0.080 1.802Female (n � 97) 0.222 0.073 1.705
ETDRS � Early Treatment Diabetic Retinopathy Study; SD � standard
*Data are available for 146 eyes.The mean choroidal volume of the total macula (Table 4) was.311�2.199 mm3 in patients aged �40 years, 7.258�1.886 mm3
n patients aged 41 to 60 years, and 6.526�2.108 mm3 in patientsged �61years (Fig 3A–C). By dividing the eyes by axial length,he mean choroidal volume of the total macula was 8.355�2.243m3 in hyperopic eyes, 7.645�2.186 mm3 in emmetropic eyes,
nd 6.761�2.005 mm3 in myopic eyes (Fig 3D–F). Male subjectsresented a mean macular choroidal volume of 7.664�2.283 mm3,nd female subjects presented a mean macular choroidal volume of.138�2.077 mm3.
Figure 4 (available at http://aaojournal.org) shows a significantP � 0.01) negative correlation between the total choroidal vol-me in the ETDRS map and the axial length (R2�0.122). Univar-ate regression analysis showed an approximate decrease in cho-oidal volume of 0.56 mm3 (7.59%) for every millimeter of axialength. Age tended to have a negative correlation of high signifi-ance (P � 0.01; R2�0.150) (Fig 4, available at http://aaojournal.rg). Univariate regression analysis showed an approximate de-rease in choroidal volume of 0.54 mm3 (7.32%) every 10 years.
iscussion
n this study, 3-dimensional visualization of the choroid of theacular area in a large sample of healthy eyes was performed
sing EDI SD-OCT and allowed a comprehensive analysis ofhe choroidal anatomy. Manual segmentation of the choroidalorders was performed following a well-reproducible methodescribed in a previous report by our group.34 The volume ofhe analyzed choroid was automatically calculated by theuilt-in software of the SD-OCT.
So far, no previous report has provided in vivo dataegarding volume of the choroid in normal eyes using EDID-OCT. Hirata et al32 recently reported measurement of
he choroidal volume of the macula using a prototype ofwept-source OCT, which is not yet available commer-ially. In their report, mean choroidal volume of the centering (within the 1.0-mm diameter ETDRS circle) was.159�0.066 mm3, 1.412�0.567 mm3 within the ETDRSnner ring, and 5.411�2.097 mm3 within the ETDRS outering. In our study, results of the choroidal volume measure-ent are higher: The mean choroidal volume of the center
etic Retinopathy Study Rings, Dividing by Age, Axial Length,x
Outer Ring Total ETDRS map
D Mean (mm3) SD Mean (mm3) SD P
76 6.106 1.561 8.311 2.199 �0.00191 5.322 1.346 7.258 1.88650 4.744 1.504 6.526 2.108
64 6.030 1.623 8.355 2.243 �0.0150 5.599 1.593 7.645 2.18610 4.989 1.442 6.761 2.005
87 5.627 1.636 7.664 2.283 �0.0533 5.211 1.489 7.138 2.077
tion.
Diabd Se
ng
S
0.50.40.5
0.50.50.5
0.50.5
devia
2575

ogvs
aU
Ophthalmology Volume 119, Number 12, December 2012
ring was 0.228�0.077 mm3, 1.976�0.634 mm3 within theETDRS inner ring, and 7.374�2.181 mm3 within the ET-DRS outer ring. Explanations for this difference may be thesmaller sample size (31 eyes) or the older mean age (64years) of the population studied by Hirata et al32; moreover,we cannot exclude ethnic variations in the choroidal vol-ume. However, they did not analyze the correlation between
Figure 3. Effect of age (A–C) and axial length (D–F) on the color-codeEarly Treatment Diabetic Retinopathy Study grid. A, Right eye of a 30-yeapatient: Total choroidal volume is 7.39 mm3. C, Right eye of a 70-yealength � 22.5 mm): Total choroidal volume is 8.61 mm3. E, Emmetropiceye (axial length � 26.5 mm): Total choroidal volume is 6.54 mm3.
macular choroidal volume and age, axial length, and sex. In c
2576
ur study, results of multiple regression analysis showed aood coefficient of determination for the macular choroidalolume in the model determined by age, axial length, andex (R2�0.323).
Using stepwise analysis we found that age was highlyssociated with choroidal volume in each ETDRS ring.nivariate regression analysis showed an approximate de-
roidal thickness map and mean choroidal volume of each subfield of thepatient: Total choroidal volume is 8.53 mm3. B, Right eye of a 50-year-oldpatient: Total choroidal volume is 6.36 mm3. D, Hyperopic eye (axialxial length � 24.5 mm): Total choroidal volume is 7.47 mm3. F, Myopic
d chor-oldr-oldeye (a
rease in volume of 0.54 mm3 (7.32%) for every 10 years.

appocapaovp
R
1
1
1
1
1
1
1
Barteselli et al � 3D Analysis of the Choroid
Although the reductions were similar, the R2 value was low(0.150), suggesting great interindividual variations. Withthe increasing age and the regressing choroidal volume, theability of the choroid to supply sufficient levels of oxygenand other metabolites to the RPE and outer retina maydecrease,7 contributing to the onset of AMD in elderlypeople.
We also found a significant negative correlation withaxial length in all ETDRS rings. Univariate regression anal-ysis showed an approximate decrease in volume of 0.56mm3 (7.59%) for every millimeter of axial length. Similar tothe regression of age, the R2 was low (0.122), suggestinggreat interindividual variations. Choroidal thinning seems tobe prominent in highly myopic eyes; this may play a role inthe pathophysiologic features of vision loss in high myopia,such as a relative ischemia of the outer retina, RPE, and thechoroid itself.13
Moreover, our study is the first to report intersexualdifferences in choroidal volume in healthy subjects: Menhave a significantly greater choroidal volume than women(7.37% greater than in women). The influence of sex inchoroidal thickness and volume was not assessed in previ-ous reports.7,9,13,29,31–33 Clinic-based studies have previ-ously documented that the retina is thicker in men than inwomen38–41; thus, we can speculate a similar finding for thechoroid. However, a longitudinal follow-up study is neededto address the clinical significance of this finding.
The present study also showed that nasal choroid volumein the inner ring was significantly lower than the superiorchoroid; likewise, nasal choroidal volume of the outer ringwas significantly lower than of all the other outer-ringquadrants. This loss of choroidal tissue in the nasal quadrantcould be a contributing cause for the development of peri-papillary atrophy and may play a role in glaucoma, aspreviously speculated by Spaide et al.7
Study Limitations
Our study has some limitations. First, it is retrospective innature; however, we carefully excluded eyes/patients withconditions that have been suggested to affect the choroid,and we included only normal eyes and eyes with onlyfloaters and posterior vitreous detachment in this study.Second, we performed manual segmentation of choroidalborders on SD-OCT B-scans because reliable software toperform automated choroidal segmentation is not available.Although manual segmentation may at first seem to be lessreliable, we did show in a previous report that our manualtechnique is highly reproducible.34 In the future, automatedchoroidal segmentation software may reduce the risk oferrors of manual segmentation still further. Third, we didnot study the potential effect of ethnicity, diurnal variation,blood pressure, hydration status, and other systemic orgenetic factors on macular choroidal volume; further studiesare warranted to evaluate those factors.
In conclusion, our study shows that EDI SD-OCT is anoninvasive and well-tolerated procedure with an excellentability to visualize choroidal anatomy and to measure cho-roidal volume at the posterior pole using manual segmen-
tation without pupillary dilation. Age, axial length, and sexre highly associated with choroidal volume in normalatients, most likely leading to insufficient metabolic sup-lements for the macula, especially in elderly, highly my-pic patients. Our study provides a normative database forhoroidal volume, which may be useful for future choroidalnalysis studies in various chorioretinal diseases. A larger,rospective, multicenter study would help to evaluate vari-tions of macular choroidal volume related to ethnicity andther systemic or genetic factors. Assessment of choroidalolume may provide an innovative way to understand theathophysiology and evaluate the clinical course.
eferences
1. Linsenmeier RA, Padnick-Silver L. Metabolic dependence ofphotoreceptors on the choroid in the normal and detachedretina. Invest Ophthalmol Vis Sci 2000;41:3117–23.
2. Grossniklaus HE, Green WR. Choroidal neovascularization.Am J Ophthalmol 2004;137:496–503.
3. Gomi F, Tano Y. Polypoidal choroidal vasculopathy and treat-ments. Curr Opin Ophthalmol 2008;19:208–12.
4. Gupta B, Mohamed MD. Photodynamic therapy for variantcentral serous chorioretinopathy: efficacy and side effects.Ophthalmologica 2011;225:207–10.
5. Rajendram R, Evans M, Rao NA. Vogt-Koyanagi-Haradadisease. Int Ophthalmol Clin 2005;45:115–34.
6. Fitzgerald ME, Wildsoet CF, Reiner A. Temporal relationshipof choroidal blood flow and thickness changes during recoveryfrom form deprivation myopia in chicks. Exp Eye Res 2002;74:561–70.
7. Spaide RF, Koizumi H, Pozzoni MC. Enhanced depth imagingspectral-domain optical coherence tomography. Am J Oph-thalmol 2008;146:496–500.
8. Margolis R, Spaide RF. A pilot study of enhanced depthimaging optical coherence tomography of the choroid in nor-mal eyes. Am J Ophthalmol 2009;147:811–5.
9. McCourt EA, Cadena BC, Barnett CJ, et al. Measurement ofsubfoveal choroidal thickness using spectral domain opticalcoherence tomography. Ophthalmic Surg Lasers Imaging2010;41(Suppl):S28–33.
0. Manjunath V, Taha M, Fujimoto JG, Duker JS. Choroidalthickness in normal eyes measured using Cirrus HD opticalcoherence tomography. Am J Ophthalmol 2010;150:325–9.
1. Ding X, Li J, Zeng J, et al. Choroidal thickness in healthyChinese subjects. Invest Ophthalmol Vis Sci 2011;52:9555– 60.
2. Rahman W, Chen FK, Yeoh J, et al. Repeatability of manualsubfoveal choroidal thickness measurements in healthy sub-jects using the technique of enhanced depth imaging opticalcoherence tomography. Invest Ophthalmol Vis Sci 2011;52:2267–71.
3. Spaide RF. Enhanced depth imaging optical coherence tomog-raphy of retinal pigment epithelial detachment in age-relatedmacular degeneration. Am J Ophthalmol 2009;147:644–52.
4. Fujiwara T, Imamura Y, Margolis R, et al. Enhanced depthimaging optical coherence tomography of the choroid inhighly myopic eyes. Am J Ophthalmol 2009;148:445–50.
5. Yasuno Y, Okamoto F, Kawana K, et al. Investigation ofmultifocal choroiditis with panuveitis by three-dimensionalhigh-penetration optical coherence tomography. J Biophoton-ics 2009;2:435–41.
6. Imamura Y, Fujiwara T, Margolis R, Spaide RF. Enhanceddepth imaging optical coherence tomography of the choroid in
central serous chorioretinopathy. Retina 2009;29:1469–73.2577

3
3
3
3
3
3
3
3
3
3
4
4
Ophthalmology Volume 119, Number 12, December 2012
17. Maruko I, Iida T, Sugano Y, et al. Subfoveal choroidal thick-ness after treatment of central serous chorioretinopathy. Oph-thalmology 2010;117:1792–9.
18. Yeoh J, Rahman W, Chen F, et al. Choroidal imaging ininherited retinal disease using the technique of enhanced depthimaging optical coherence tomography. Graefes Arch ClinExp Ophthalmol 2010;248:1719–28.
19. Reibaldi M, Boscia F, Avitabile T, et al. Enhanced depthimaging optical coherence tomography of the choroid in id-iopathic macular hole: a cross-sectional prospective study.Am J Ophthalmol 2011;151:112–7.
20. Maruko I, Iida T, Sugano Y, et al. Subfoveal choroidal thick-ness after treatment of Vogt-Koyanagi-Harada disease. Retina2011;31:510–7.
21. Imamura Y, Iida T, Maruko I, et al. Enhanced depth imagingoptical coherence tomography of the sclera in dome-shapedmacula. Am J Ophthalmol 2011;151:297–302.
22. Fong AH, Li KK, Wong D. Choroidal evaluation using en-hanced depth imaging spectral-domain optical coherence to-mography in Vogt-Koyanagi-Harada disease. Retina 2011;31:502–9.
23. Vance SK, Imamura Y, Freund KB. The effects of sildenafilcitrate on choroidal thickness as determined by enhanceddepth imaging optical coherence tomography. Retina 2011;31:332–5.
24. Mwanza JC, Hochberg JT, Banitt MR, et al. Lack of associ-ation between glaucoma and macular choroidal thickness mea-sured with enhanced depth imaging optical coherence tomog-raphy. Invest Ophthalmol Vis Sci 2011;52:3430–5.
25. Maruko I, Iida T, Sugano Y, et al. Subfoveal retinal andchoroidal thickness after verteporfin photodynamic therapy forpolypoidal choroidal vasculopathy. Am J Ophthalmol 2011;151:594–603.
26. Chung SE, Kang SW, Lee JH, Kim YT. Choroidal thicknessin polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology 2011;118:840–5.
27. Koizumi H, Yamagishi T, Yamazaki T, et al. Subfoveal cho-roidal thickness in typical age-related macular degenerationand polypoidal choroidal vasculopathy. Graefes Arch ClinExp Ophthalmol 2011;249:1123–8.
28. Ikuno Y, Maruko I, Yasuno Y, et al. Reproducibility of retinaland choroidal thickness measurements in enhanced depth im-aging and high-penetration optical coherence tomography.Invest Ophthalmol 2011;52:5536–40.
29. Ikuno Y, Kawaguchi K, Nouchi T, Yasuno Y. Choroidalthickness in healthy Japanese subjects. Invest Ophthalmol Vis
Sci 2010;51:2173–6.Footnotes and Financial Disclosures
discussed in this article.
SR(tr
CWEf
2578
0. Esmaeelpour M, Povazay B, Hermann B, et al. Three-dimen-sional 1060-nm OCT: choroidal thickness maps in normal sub-jects and improved posterior segment visualization in cataractpatients. Invest Ophthalmol Vis Sci 2010;51:5260–6.
1. Ouyang Y, Heussen FM, Mokwa N, et al. Spatial distributionof posterior pole choroidal thickness by spectral domain op-tical coherence tomography. Invest Ophthalmol Vis Sci 2011;52:7019–26.
2. Hirata M, Tsujikawa A, Matsumoto A, et al. Macular choroi-dal thickness and volume in normal subjects measured byswept-source optical coherence tomography. Invest Ophthal-mol Vis Sci 2011;52:4971–8.
3. Shin JW, Shin YU, Lee BR. Choroidal thickness and volumemapping by a six radial scan protocol on spectral-domainoptical coherence tomography. Ophthalmology 2012;119:1017–23.
4. Chhablani J, Barteselli G, Wang H, et al. Repeatability andreproducibility of manual choroidal volume measurementsusing enhanced depth imaging optical coherence tomography.Invest Ophthalmol Vis Sci 2012;53:2274–80.
5. Early Treatment Diabetic Retinopathy Study Research Group.Photocoagulation for diabetic macular edema: Early Treat-ment Diabetic Retinopathy Study report number 1. Arch Oph-thalmol 1985;103:1796–806.
6. Strang NC, Schmid KL, Carney LG. Hyperopia is predomi-nantly axial in nature. Curr Eye Res 1998;17:380–3.
7. Llorente L, Barbero S, Cano D, et al. Myopic versus hyperopiceyes: axial length, corneal shape and optical aberrations. J Vis[serial online] 2004;4:288–98. Available at: http://www.journalofvision.org/content/4/4/5.long. Accessed June 6,2012.
8. Kelty PJ, Payne JF, Trivedi RH, et al. Macular thicknessassessment in healthy eyes based on ethnicity using StratusOCT optical coherence tomography. Invest Ophthalmol VisSci 2008;49:2668–72.
9. Wong AC, Chan CW, Hui SP. Relationship of gender, bodymass index, and axial length with central retinal thicknessusing optical coherence tomography. Eye (Lond) 2005;19:292–7.
0. Duan XR, Liang YB, Friedman DS, et al. Normal macularthickness measurements using optical coherence tomographyin healthy eyes of adult Chinese persons: the Handan EyeStudy. Ophthalmology 2010;117:1585–94.
1. Song WK, Lee SC, Lee ES, et al. Macular thickness variationswith sex, age, and axial length in healthy subjects: a spectraldomain-optical coherence tomography study. Invest Ophthal-
mol Vis Sci 2010;51:3913–8.Originally received: March 14, 2012.Final revision: June 23, 2012.Accepted: June 28, 2012.Available online: August 24, 2012. Manuscript no. 2012-378.
Department of Ophthalmology, Jacobs Retina Center at Shiley Eye Center,University of California San Diego, La Jolla, California.
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materials
upported by National Institutes of Health Grants R01EY007366 and01EY018589 (W.R.F.), R01EY016323 (D.U.B.), and R01EY020617
L.C.). RPB Incorporated and unrestricted funds from Jacobs Retina Cen-er. The funding organizations had no role in the design or conduct of thisesearch.
orrespondence:illiam R. Freeman, MD, University of California at San Diego, Shiley
ye Center, 0946, 9415 Campus Point Drive, La Jolla, CA 92037. E-mail:
[email protected].Copyright © 2022 FDOKUMEN