
Plugging the School to Prison Pipeline by Addressing Cultural ...
Upload
khangminh22Category
view
2download
0
Leukocyte Capillary Plugging in Myocardial Ischemiaand Reperfusion in the Dog
ROBERT L. ENGLER, MD,GEERT W. SCHMID-SCHONBEIN, PhD, and
RICHARD S. PAVELEC
After several hours ofischemia an incomplete return ofblood flow has been reported in brain, kidney, skeletalmuscle, and heart. The mechanisms responsible for theno-reflow phenomenon have been unclear, and peri-vascular edema, platelet or red cell plugs, and inter-stitial hemorrhage have been implicated. In the presentstudy evidence is provided that leukocyte entrapmentin capillaries might contribute to no reflow. Leuko-cytes are large and stiff cells, which adhere to vascularendothelium naturally and are known to alter in theiradherence properties under a variety of conditions. Ac-cordingly, 11 open-chest dogs were studied, 1-5 hoursafter left anterior descending coronary artery occlu-sion. Reperfusion (9 dogs) at 75 mm Hg arterial pres-ure was accomplished with Ringer's lactate and carbonsuspension as a marker for capillary patency. In non-ischemic tissue, 98% of the capillaries contained car-
INCOMPLETE RETURN of blood flow, "no re-flow," after periods of ischemia has been reported inbrain, kidney, heart, and skeletal muscle and mayrepresent a single pathophysiologic response.`16 Inheart muscle after interruption of blood flow forabout 90 minutes there is evidence of no reflow. Inthe myocardium histologic signs of myocardial cellinjury precede microvascular injury,7 and the area ofno reflow increases with the duration of the isch-emia.8 It is usually assumed that the no-reflow phe-nomenon is a pathophysiologic disorder at the levelof the capillaries or feeding arterioles. Three mecha-nisms for the no-reflow phenomenon have been sug-gested. Loss of volume regulation in myocardial tis-sue may lead to perivascular swelling, and uponreperfusion this could compress small arterioles orcapillaries.1'3'49 Endothelial cell swelling could causeocclusion of capillaries.9 Interstitial hemorrhage,often observed after reperfusion, could occlude themicrocirculation,10-16 but no general agreement hasbeen reached about the validity of these mechanisms.
From the Research Service and Cardiology Section, Department ofMedicine, Veterans Administration Medical Center, and the Departmentof Medicine, Department of Applied Mechanics and EngineeringSciences-Bioengineering, University of California, La Jolla, Califomia
bon, rare leukocytes, and few erythrocytes, whereastissue from the distribution of the occluded artery washeterogeneous: 60% of the capillaries had no carbon,high hematocrits, and approximately one leukocyteper unbranched capillary; 40% demonstrated reflowand no leukocytes. A significant correlation betweencapillaries without carbon (no reflow) and the frequen-cy of leukocytes remaining in these capillaries in-dicated that leukocytes were present in obstructedcapillaries. Furthermore, the frequency of leukocytesremaining after the washout with lactate was ten timesgreater than in normal arrested heart muscle withoutwashout. Our results suggest that progressive leuko-cyte capillary plugging during myocardial ischemiacontributes to preventing full restoration of capillaryflow upon reperfusion. (Am J Pathol 1983, 111:98-111)
In the present report we present evidence for therole of leukocyte capillary plugging in the no-reflowphenomenon. Several factors make leukocytes morelikely candidates for obstructing capillaries thanother formed elements. Leukocytes are larger andmuch stiffer cells than erythrocytes,17' 18 and leuko-cytes have to deform when entering into capillaries.In addition, they have a natural tendency to adhereto the vascular endothelium.19-21 In certain situa-tions, including arterial hypotension or perivascularswelling, these cells may be unable to traverse a capil-lary. Leukocytes have been directly observed by in-travital microscopy to occlude capillaries during
Supported in part by a grant from the Office of Grad-uate Studies and Research at the University of California,San Diego.
Presented at the Scientific Sessions of the AmericanHeart Association, November 1981 (Circ 64:IV-138, 1981).
Accepted for publication November 12, 1982.Address reprint requests to Robert Engler, MD, Direc-
tor, Intensive Care Unit, VA Medical Center (111-A), 3350La Jolla Village Drive, San Diego, CA 92161.
0002-9440/83/0407-0098
98
LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 99
hypotension in skeletal muscle.6'22 Every obstructedcapillary contained at least one leukocyte. These di-rect observations in skeletal muscle strongly sug-
gested that a similar microvascular obstruction byleukocytes could occur in heart muscle.We therefore studied the role of leukocytes in
plugging capillaries following myocardial ischemia.Our results indicate that the distribution of leuko-cytes in capillaries correlates well with the distribu-tion of no-reflow capillaries and high local hemato-crits. Furthermore, the distribution of leukocytessuggests that leukocytes accumulate in the microcir-culation. Finally, leukocytes are observed occludingcapillaries before the development of interstitialhemorrhage.
Methods
Studies were completed with two groups of dogs.We first carried out studies in two preparations tomeasure the frequency of leukocytes (percent lengthof all capillaries occupied by leukocytes) in normalmyocardial capillaries. In the second series of 9animals the coronary circulation was reperfused after1-5 hours of ischemia. We used Ringer's lactate towash out all formed blood elements from capillariescapable of reflow, and then we used carbon suspen-sion to indicate capillaries capable of reflow. In his-tologic sections from normal and ischemic myocar-dium we determined the frequency of leukocytes incapillaries in both longitudinal sections (parallel tothe fibers) and cross-sections. Capillaries were di-vided in two categories-those with carbon (reflow)and those without carbon (no reflow). The extent ofno reflow was determined as the fraction of capillar-ies in the histologic sections not containing carbon.
Studies Without Reperfusion
Two mongrel dogs were anesthetized with sodiumpentobarbital, 25 mg/kg. Through a left thoracot-omy, the heart was exposed in a pericardial cradle,and a segment of the proximal left anterior descend-ing coronary artery was dissected free. Lidocaine, 2.5mg/kg was given prophylactically to lessen arrhyth-mias, and repeated doses were given as necessary tosuppress premature ventricular depolarizations. Theleft anterior descending coronary artery was ligatednear its origin. Ischemia of the anterior wall was
grossly apparent by discoloration and systolic bulg-ing. After 1 and 3 hours (one animal each) of isch-emia the heart was arrested with a 100 mEq bolus ofKCI injected into the left atrium. The heart was
rapidly excised, and punch biopsies were obtainedfrom normal areas (posterior wall).
Reperfusion Studies
Nine animals were prepared in a fashion similar tothe nonreperfusion protocol. Occlusion of the leftanterior descending coronary artery was maintainedfor 5 hours in 5 animals, 3 hours in 2 animals, and1 hour in 2 animals with a Schwartz clip. Heparin(10,000 units) was given intravenously 3 minutesprior to KCI administration. The heart was rapidlyexcised, and a metal cannula was secured in the leftmain coronary artery, or one cannula in each of theleft anterior descending and circumflex arteries.After removal of the Schwartz clip, the coronary vas-culature was perfused by gravity with Ringer's lactateat 37 C at a pressure of 75 mm Hg for 3 minutes, fol-lowed by carbon black (Pelikan Fount India dryingink, Pelikan AGD-3000, Hanover, Germany) 180 mlmixed with 180 ml of Ringer's lactate for 3 minutes.Biopsy specimens were taken and processed as de-scribed below.
Histologic Analysis
Biopsies from the subendocardium were trimmedto about 2 x 2 x 4 mm and were fixed in 2.5% glu-taraldehyde (pH 7.4, 350 mOsm) overnight andwashed with cacodylate buffer adjusted to pH 7.4and 350 mOsm. The biopsy specimens were postfixedin 1%7o osmium tetraoxide and dehydrated in gradedsteps of ethanol from 30% to 1007o and embeddedin Araldite resin. The tissue was oriented with thefiber direction parallel to the edge of the tissue block.Thin sections (0.5-2,) were stained with 1% tolui-dine blue. An average of 25 biopsies from each area(anterior and posterior wall) of each heart were ob-tained, and one random section of each biopsy speci-men was used for analysis (to avoid biasing the databy using multiple sections of the same capillary). Sec-tions were studied by a "blinded" observer with alight microscope with oil-immersion objectives ( x 50,NA 1.30; x 100, NA 1.32) and x 12.5 eyepieces.The microscope was mounted on an air-suspendedtable, and a television camera and video monitorwere used for measurements. All cells were identifiedby direct visualization, and the television monitorwas used for measurements. All length measurementswere calibrated with a 2-mm micrometer scale with0.010-mm divisions. Many sections contained bothlongitudinal and cross-sectional fiber orientation.Areas with long segments of capillaries (at least 50,)
Vol. Ill - No. 1

100 ENGLER ET AL
were used for longitudinal analysis, and areas wherecapillary and muscle fibers appeared to be perpen-dicular to the section were used for cross-sectionalanalysis. Areas where fibers and capillaries were cutobliquely were excluded from the analysis.The objective of the measurements was to obtain
the average frequency of leukocytes in capillaries andthe average fraction of capillaries that were plugged(no reflow) in each biopsy specimen. If the leukocyteswere selectively plugging capillaries, then the fre-quency of leukocytes should correspond to the frac-tion of capillaries without reflow.The section was scanned and counted in a system-
atic pattern similar to the roster lines in television sothat all capillaries in the 2 x 4 mm section werecounted. In longitudinal areas, the length of eachcapillary segment visible on the section was mea-sured, the length occupied by each leukocyte wasmeasured, and the presence of erythrocytes or carbonwas recorded. If carbon was seen anywhere in thecapillary, the entire capillary was considered reper-fused. These measurements were summed for the en-
tire section (see below). In the cross-sectional areasthe number of capillaries, the number of capillarieswithout carbon, and the number of capillaries con-taining a leukocyte was recorded. For each biopsysite section the total of the longitudinal measure-ments and cross-sectional counts for the entire 2 x4 mm section was considered one "sample." A totalof 91 samples or biopsy sites from the reperfusionstudies were of good quality and contained adequatenumbers of longitudinal or cross-sectional capillariesfor analysis. Only biopsy sites with more than 1 mmtotal length of capillary measured or more than 100capillary cross-sections were included in the analysis.Some biopsy sites were not used because tissue orien-tation in the Araldite block was not optimal for lon-gitudinal measurements or cross-sectional counting.The criteria for identification of leukocytes were as
follows: the leukocyte nucleus and/or cytoplasm hadto be recognizable, together with the surrounding en-dothelial cell. In a few sections the identification ofleukocytes by light microscopy was confirmed byelectron microscopy (Figures 1 and 2).
Figure 1 - Electron micrograph of a longitudinal section of a no-reflow capillary. A leukocyte is seen on the left, and tightly packed erythro-cytes fill the capillary.
AJP * April 1983
LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 101
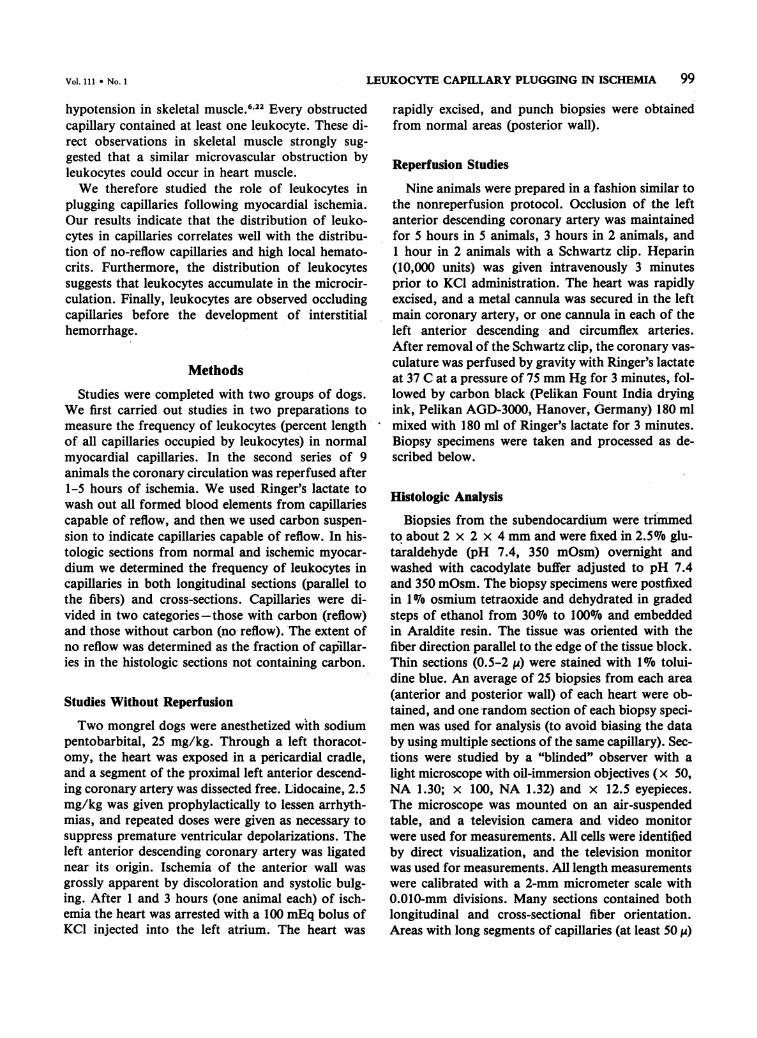
Figure 2-Electron micrograph of a capillary cross-section containing a leukocyte in dog myocardium after 5 hours of ischemia. Note theclose attachment between the leukocyte and the endothelium.
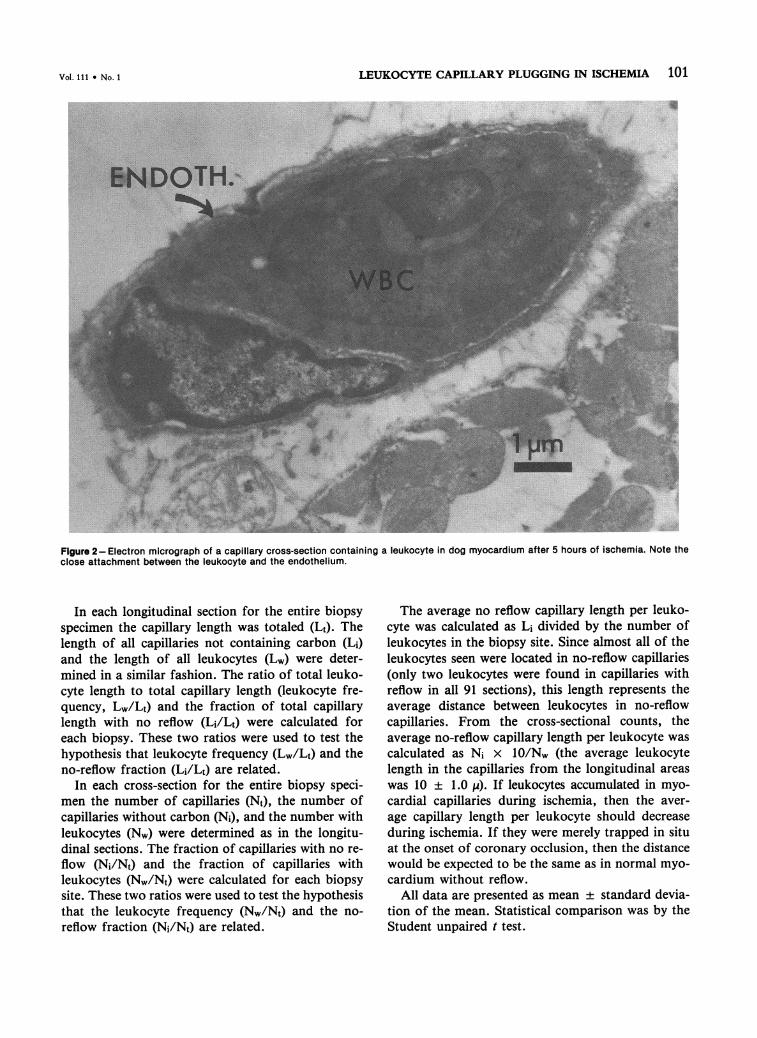
In each longitudinal section for the entire biopsyspecimen the capillary length was totaled (Lt). Thelength of all capillaries not containing carbon (Li)and the length of all leukocytes (Lw) were deter-mined in a similar fashion. The ratio of total leuko-cyte length to total capillary length (leukocyte fre-quency, Lw/Lt) and the fraction of total capillarylength with no reflow (Li/Lt) were calculated foreach biopsy. These two ratios were used to test thehypothesis that leukocyte frequency (Lw/Lt) and theno-reflow fraction (Li/Lt) are related.
In each cross-section for the entire biopsy speci-men the number of capillaries (Nt), the number ofcapillaries without carbon (Ni), and the number withleukocytes (Nw) were determined as in the longitu-dinal sections. The fraction of capillaries with no re-flow (Ni/Nt) and the fraction of capillaries withleukocytes (Nw/Nt) were calculated for each biopsysite. These two ratios were used to test the hypothesisthat the leukocyte frequency (Nw/Nt) and the no-reflow fraction (Ni/Nt) are related.
The average no reflow capillary length per leuko-cyte was calculated as Li divided by the number ofleukocytes in the biopsy site. Since almost all of theleukocytes seen were located in no-reflow capillaries(only two leukocytes were found in capillaries withreflow in all 91 sections), this length represents theaverage distance between leukocytes in no-reflowcapillaries. From the cross-sectional counts, theaverage no-reflow capillary length per leukocyte wascalculated as Ni x 10/Nw (the average leukocytelength in the capillaries from the longitudinal areaswas 10 ± 1.0 4). If leukocytes accumulated in myo-cardial capillaries during ischemia, then the aver-age capillary length per leukocyte should decreaseduring ischemia. If they were merely trapped in situat the onset of coronary occlusion, then the distancewould be expected to be the same as in normal myo-cardium without reflow.
All data are presented as mean ± standard devia-tion of the mean. Statistical comparison was by theStudent unpaired t test.
Vol. 111 * No. 1

102 ENGLER ET AL
Results
Studies Without Reperfusion
In longitudinal sections from areas of normal myo-cardium the average length of capillary per leukocytewas 2433 ,I. In cross-sections from normal myocar-
dium the average length per leukocyte was 3621 I.These lengths indicate the average distance betweenleukocytes in the normal microcirculation at any one
time.
Reperfusion Studies
Adequate reperfusion of the large epicardial coro-
nary arteries was confirmed by direct visualization ofthe washout of blood by the clear Ringer's lactate sol-ution and by the black carbon suspension.
Normal Myocardium (Posterior Wall)
Almost every capillary contained carbon and, atmost, a few erythrocytes (hematocrit less than 3%).In a total of 91690 y of longitudinal capillary 98.2%of the length was filled with carbon (Figure 3, Table
1). In 5223 cross-sections 96.9% contained carbon(Figure 4). No extravasation of carbon was seen. Thepicture was quite homogeneous in all 9 dogs, and inall but two biopsy specimens from the normal areamore than 98% of the vessels contained carbon. Thefew capillaries without carbon in the longitudinal sec-tions did not demonstrate high hematocrits (less than20%); when erythrocytes were present, they wereseparated by plasma gaps without carbon. Only twoleukocytes in vessels containing carbon were iden-tified.
Ischemic Myocardium (Anterior Wall)The microscopic appearance in biopsies from isch-
emic areas was heterogeneous (Figure 5). In somesections only occasional capillaries contained carbon,longitudinally sectioned capillaries showed highhematocrits with tightly packed erythrocytes (hema-tocrit >75%7o). In other sections there was a seeminglyrandom mixture of capillaries with no carbon andhigh hematocrit and capillaries with carbon and fewor no erythrocytes (Figures 6-8).
Figure 3-Longitudinal section of normal myocardium showing carbon particles in every capillary.
AJP * April 1983
-.1C
LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 103
(C\l)O00 (00CII) 10N
0 0 ,t 0oL C 00cn CD CY) r- a o. CD CDt
c; ci _; u ci _: c ci c;
0) r-cc - 0 0oC00 UJ) _ o - _ci .- .l .- .~ .- V-
o CV CD CY V. _ CO
0 l;rCII) 0) 0)0a)00o
o- C O 0)_.11 CM 0
O o CD 00 00 0
0 .C.-)
_'00o o oo o
.O' C 00 0)
66 0 0
o o o 6 o0 o _- CM CM4 Cfo C4 Coo Co
100o oC C -t_ U)C111-o U) 11 Ch _- CM IT O000 CM C4 CCM t ) CM
."it C 04 o 0 0)0t C
v- r-YU CW) CM LO CD- YU) r
'- D 0C0) LO00-o CD0.)0 0 0C CC) L . -0) CM00 _OcOcO_00
0) 01 0 0) C 00 coCo 10U) 0 N 00 C f- C) (DCD00 it )0 0 'IO CV C01 cM CII _- ' _- CM _- _- c
LOr- o cmo 001 0 (
C(0 0D - 00C '0 _--. 0000_.-_ o _ c ci_C
0 0) T'- q,C")CCe)00001(00-0.
0 00 0000.c-
_ ._- CD o o Co CD Co o CD _
101 10010 00o0coCD01 0't0 -r000 0co(D 0 0Ot 0) - 00 C C 00 00 C -,,t 0 - C0 0 C) 04 _- C' _-
0~6 ,"Oi
CV0 *
6
r.- 0000 0 C 0O000
6 6
0 00o 0 N oC 0) o00 0 _ CO J)101CU0)101L 10 0 0 "it0o. C00 CM O0 C\ mt _ _-- C_- _- I_- _- _
0 0oc o
CV) U')
LOa a
00-o
.00)Ca
o
J 0(c
0C
0 0C C
00
00
En 0
2 .00 E
C
2o
0(
0.00-
C.)0w z
Cd
0)O-
CD
0)0
0 )0O
U) 0
0 CJ
) .0co
_ -
CO*
c)oE a
0 0.0
0)
E~ 0
coC
0.)co0 0
CD~ 0
C
(DZ0) 0
3 >'
0-
Longitudinal Sections
In the longitudinal sections 79158 ,. of capillarieswere measured; 60Vo of the total length in the po-tentially ischemic region (all anterior wall biopsies)did not contain carbon. The correlation between thefraction of capillary length without reflow and theleukocyte frequency (all longitudinal sections, an-terior and posterior wall) was 0.57 (P < 0.0001; n =48) (Figure 9). The average distance between leuko-cytes in no-reflow capillaries was 292 ± 208 , after5 hours of ischemia (Table 2). This distance is dra-matically less than the average distance between leu-kocytes in normal myocardial capillaries without lac-tate washout (2433 4A).
Cross-Sections
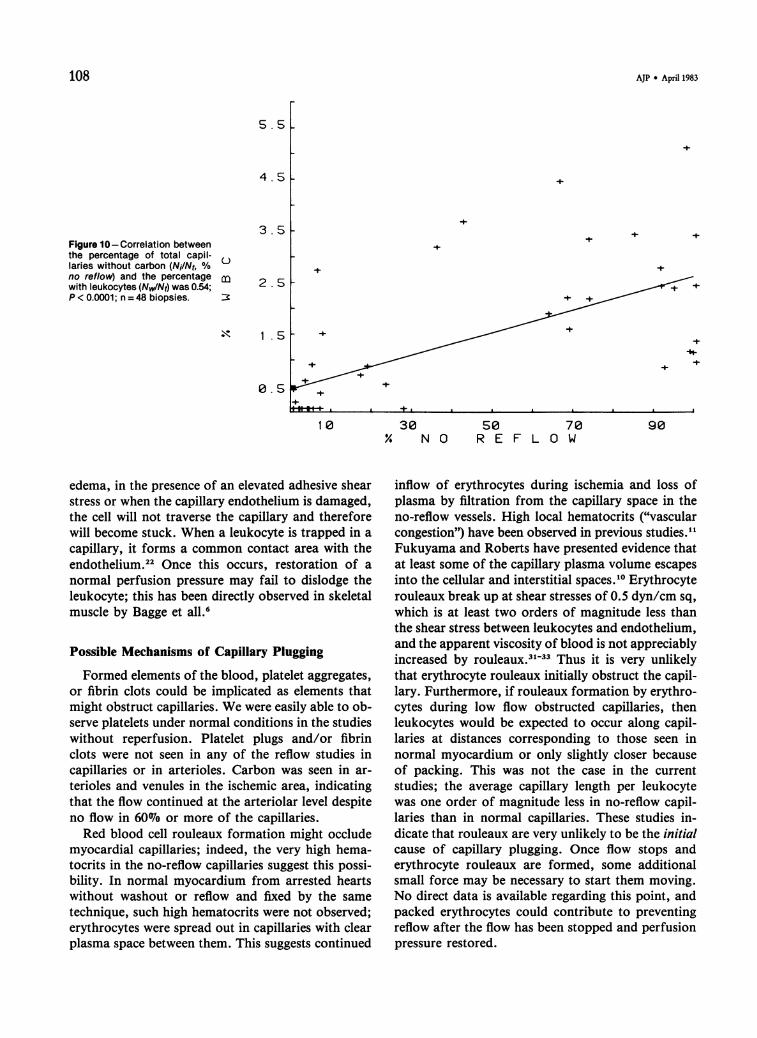
In the cross-sections a total of 7041 capillaries werecounted; 68% of cross-sections in the ischemic area(all anterior wall biopsies) did not contain carbon.The correlation between the fraction of capillarieswithout reflow and the fraction of total capillarieswith leukocytes (all cross-sections, anterior and pos-terior wall) was 0.54 (P < 0.0001; n = 43) (Figure 10).In cross-sections from the ischemic area (anteriorwall) the average distance between leukocytes in theno-reflow capillaries was 327 ± 278 1A (Table 2). Theaverage capillary distance between leukocytes incross-sections of normal myocardium without reper-fusion was much larger (3621 IA; P < 0.0001).
In all studies no emigration of leukocytes acrossthe vascular endothelium was observed. The arte-rioles and venules always contained carbon particlesat various densities, indicating some flow in these ves-sels during reperfusion.The length of the contact area between leukocyte
and capillary endothelium varied from 7 to 15 jA; themean was 10 ± 1.0 M.
Discussion
In examining the possible role of leukocytes in theno-reflow phenomenon following ischemia, we willproceed from consideration of the rheologic proper-ties of leukocytes, the anatomy of the coronary mi-crocirculation, the balance between forces pushingleukocytes through capillaries, and opposing adher-ence forces to the endothelium, to the evidence forleukocyte involvement derived from the currentstudies. We will also consider how our findings relateto previous descriptions of the no-reflow phenomenon.
.lt CV7 cs
0)0o
00
(0c00
0)(cCncn0
4-.)
._
CN
c
Jo
0)
0)-J
z
0)_ DZ E
C
Z~
Z ECz
0)
Z-EC
-3
C_
-J
-i
-
-J-j
0
E0).-C
E0Z
0E0
(0
E0Z
U00)
cnV
0j)0.c)
a:0)-C
C(0)c
01)
.0ct
co
ILE0
C-
0
0.
0
CD
E
0
(0co0.
0
a)
.00a
C 0c0 E.0
cco .,cn
0
Vol.111I * No. 1
-z^"3.1'od-l
_- a
J- la
J- la

104 ENGLER ET AL
Figure 4-Cross-section of capillaries in normal myocardium. All vessels (several are indicated by the arrows) are filled with carbon particles.Black and white photograph does not distinguish carbon particles from other darkly stained cell structures, but carbon particles are readilyrecognized by their brown color in light microscopy.
Leukocyte Rheology
Recent findings regarding the properties of leuko-cytes suggest that they are the most likely of all theformed elements of blood to be associated with capil-lary plugging. The non-Newtonian properties ofblood have been attributed to the erythrocytes, anda rather detailed model of the erythrocyte has beendeveloped.23 The erythrocyte consists of a thin bicon-cave membrane filled with a Newtonian fluid with acoefficient of viscosity about 0.06 poise. The averageerythrocyte volume is about 90 cu 1., and its majordiameter is about 8 MA.24 In contrast, the leukocytesare larger spherical cells (182 cu,) with an averagediameter of 7.5 ,u for neutrophils.17 The mechanicalproperties of the leukocyte protoplasm have recentlybeen investigated."8 These cells show a relatively stiffviscoelastic response and have a significantly highercoefficient of viscosity (130 poise, about 2100 times)than erythrocytes. Thus, leukocytes are larger, muchstiffer cells.
Coronary Microcirculation
The coronary capillary bed consists of a networkof relatively long (up to 1-2 mm) capillaries with across-sectional density of 2000-3200/sq mm, depend-ing upon species.25'26 These capillary networks inter-connect through extensive anastomoses, but capillaryloops from different large epicardial coronary ar-teries do not interconnect.27 The average unbranchedepicardial capillary length in the dog is 102,.25 Func-tional intercapillary distances (the average distancebetween perfused capillaries) during closure of afeeding arteriole or capillary is maintained by inter-capillary anastomoses and is of critical importance inmaintaining a uniformly short diffusion path, be-cause 02 gradients in cardiac muscle are extremelysensitive to the length of the diffusion path.26'28'29Thus, an increase in the functional intercapillary dis-tance of 30% can lead to a partial pressure of oxygenof 0 mm Hg at some tissue locations.29 Our datademonstrating 60-68% of capillaries blocked sug-
AJP * April 1983
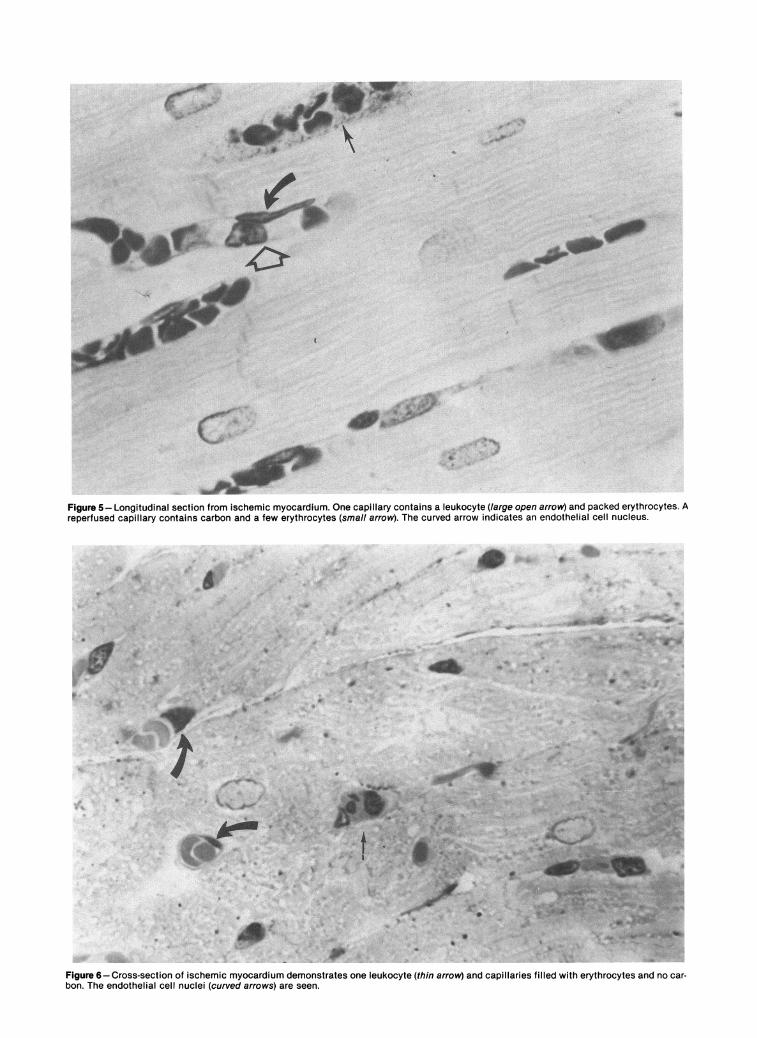
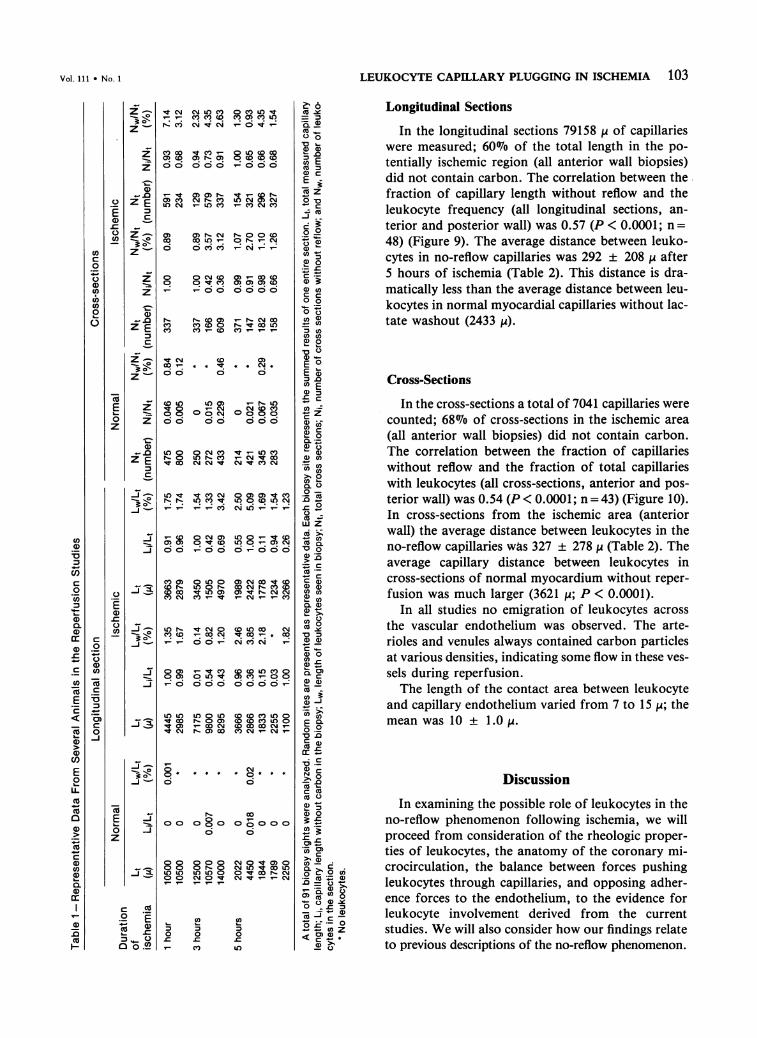
Figure 5-Longitudinal section from ischemic myocardium. One capillary contains a leukocyte (large open arrow) and packed erythrocytes. Areperfused capillary contains carbon and a few erythrocytes (small arrow). The curved arrow indicates an endothelial cell nucleus.
: I.e
' * '!
'$wit''<s~~~~~I
Figure 6-Cross-section of ischemic myocardium demonstrates one leukocyte (thin arrow) and capillaries filled with erythrocytes and no car-bon. The endothelial cell nuclei (curved arrows) are seen.
-

Figure 7-One leukocyte plugging a single capillary in the schemic area. A high hematocrit and a deformed elongated leukocyte (arrow) areseen. Red blood cells are stained with nonuniform intensity.
Figure 8-Two adjacent capillaries show reflow and no reflow, which is typical of the heterogeneous pattern in the ischemic area.
;'.....

LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 107
1-
+
Figure 9-Correlation betweenthe percentage of total capillary
+ length without carbon (Ni/Nt, %no reflow) and the percentage oftotal capillary length with leuko-cytes (Lw/Lt, % WBC) was 0.57; P< 0.0001; n = 43 biopsies.
± +
+ + + +
+++F++
+ + +I
30 so 70% N O R E F L O W
gests the possibility of local ischemia despite ade-quate coronary arteriolar pressures upon reperfu-sion. In normal myocardium multiple intercapillaryanastomoses minimize the effect of blockage of a
single feeding arteriole or capillary, result in a func-tional capillary length equivalent to the unbranchedlength, and help maintain a uniform short diffusionpath.
Leukocyte Adherence and Plugging
Leukocytes have a natural tendency to adhere tothe vascular endothelium, primarily in postcapillaryvessels under normal circumstances. The strength ofthe adhesive shear stress between the leukocyte and
endothelium membrane has been estimated in therabbit omentum and was found to range between 500and 1000 dyn/sq cm.2" This value may change sig-nificantly during an inflammatory reaction, in thepresence of agents that modify leukocyte adhesion,or in the presence of damaged capillary endothelium.When leukocytes enter into capillaries of the myo-
cardium, they have to be deformed.22 During thisprocess the leukocyte membrane is brought into closeproximity to the capillary endothelium. In an unin-flamed microcirculation under normal arterial pres-
sure the deformed leukocyte is pushed along the ca-
pillary and adheres to the endothelium in postcapillaryvenules.20 However, under a reduced arterial pres-
sure, when capillaries are narrowed by perivascular
Table 2-Leukocytes in Ischemic Region Capillaries
Duration Longitudinal Cross-sectionofischemia Li Li Nix10 NixlO(hours) Li/Lt (ZA#WBC) Li/Lt (M/#WBC) Ni/Nt (p/#WBC) Ni/Nt (A/#WBC)
1 0.91 476 1.00 741 1.00 4201 0.96 553 0.99 590 0.73 350 1.00 11203 0.42 315 0.43 360 0.95 410 0.42 1203 0.63 130 1.00 581 0.91 380 0.36 1105 0.62 389 0.96 390 0.92 116 0.99 9205 1.00 110 0.36 95 0.65 690 0.91 3305 0.94 61 0.03 0.66 150 0.98 8905 0.21 172 0.15 67 1.00 300 0.98 380
Sample biopsy sights: Li, length of capillary without carbon from entire biopsy site; Lt, total length of capillary from biopsy site; Lu/Lt, frac-tion of length without reflow from biopsy site; #WBC, number of leukocytes seen in capillaries in biopsy site; Ni, number of cross sectionswithout carbon; Nt, total number of cross sections counted; and N /Nt, fraction of cross section without carbon (no reflow).
* No leukocytes.The average length of capillary without reflow per leukocyte was calculated by dividing the total no-reflow capillary length by the number of
leukocytes. This was multiplied by 10 for the cross-sections because the average leukocyte length was 10 p.
1 8
1 4
CD 10
6
2
+
1 0 90
Vol. 111 * No. 1
108 AJP * April 1983
Figure 10-Correlation betweenthe percentage of total capil-laries without carbon (Ni/Nt, %no reflow) and the percentagewith leukocytes (Nw/Nt) was 0.54;P < 0.0001; n = 48 biopsies.
9030 50 70% N O R E F L O W
edema, in the presence of an elevated adhesive shearstress or when the capillary endothelium is damaged,the cell will not traverse the capillary and thereforewill become stuck. When a leukocyte is trapped in a
capillary, it forms a common contact area with theendothelium.22 Once this occurs, restoration of a
normal perfusion pressure may fail to dislodge theleukocyte; this has been directly observed in skeletalmuscle by Bagge et all.6
Possible Mechanisms of Capillary Plugging
Formed elements of the blood, platelet aggregates,or fibrin clots could be implicated as elements thatmight obstruct capillaries. We were easily able to ob-serve platelets under normal conditions in the studieswithout reperfusion. Platelet plugs and/or fibrinclots were not seen in any of the reflow studies incapillaries or in arterioles. Carbon was seen in ar-
terioles and venules in the ischemic area, indicatingthat the flow continued at the arteriolar level despiteno flow in 60% or more of the capillaries.Red blood cell rouleaux formation might occlude
myocardial capillaries; indeed, the very high hema-tocrits in the no-reflow capillaries suggest this possi-bility. In normal myocardium from arrested heartswithout washout or reflow and fixed by the same
technique, such high hematocrits were not observed;erythrocytes were spread out in capillaries with clearplasma space between them. This suggests continued
inflow of erythrocytes during ischemia and loss ofplasma by filtration from the capillary space in theno-reflow vessels. High local hematocrits ("vascularcongestion") have been observed in previous studies."1Fukuyama and Roberts have presented evidence thatat least some of the capillary plasma volume escapesinto the cellular and interstitial spaces.'0 Erythrocyterouleaux break up at shear stresses of 0.5 dyn/cm sq,
which is at least two orders of magnitude less thanthe shear stress between leukocytes and endothelium,and the apparent viscosity of blood is not appreciablyincreased by rouleaux.3133 Thus it is very unlikelythat erythrocyte rouleaux initially obstruct the capil-lary. Furthermore, if rouleaux formation by erythro-cytes during low flow obstructed capillaries, thenleukocytes would be expected to occur along capil-laries at distances corresponding to those seen innormal myocardium or only slightly closer becauseof packing. This was not the case in the currentstudies; the average capillary length per leukocytewas one order of magnitude less in no-reflow capil-laries than in normal capillaries. These studies in-dicate that rouleaux are very unlikely to be the initialcause of capillary plugging. Once flow stops anderythrocyte rouleaux are formed, some additionalsmall force may be necessary to start them moving.No direct data is available regarding this point, andpacked erythrocytes could contribute to preventingreflow after the flow has been stopped and perfusionpressure restored.
_5. 5
4. 5
3. 5
K
+
+
C-)
+t
+*
+
11 1 .5
+
+
a al + I I a I a A
+
1 0

LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 109
Interstitial hemorrhage after reflow has been de-scribed.10'13'14"6 Our data suggest that the no-reflowphenomenon precedes hemorrhage, as suggested byprevious studies,3"5'34 because extensive no reflowwas observed in 9 dogs without loss of vascular in-tegrity to erythrocytes or carbon.
Leukocyte Capillary Plugging
Our experiments were designed to test the hypo-thesis that leukocytes adhering to capillary endothe-lium could prevent reperfusion of capillaries follow-ing 1, 3, or 5 hours of ischemia. The lactate solutionwas used to clear all capillaries that could be perfusedby 75 mm Hg arterial pressure. The heparin adminis-tration and lactate flush were needed to prevent coag-ulation in the presence of the -carbon suspension andto clear all formed blood elements from capillariescapable of reflow. Carbon particles then filled thosecapillaries capable of reflow. The high percentage ofcarbon-filled capillaries in the normal area indicatesthat the carbon infusion is a good marker for capil-lary flow. The direct correlation between the fractionof capillaries without carbon (no reflow) and theaverage leukocyte frequency in both longitudinal andcross-sectional biopsies supports our hypothesis. If asingle leukocyte entering a capillary in the ischemicarea totally blocks flow, then only one leukocyte perunbranched capillary would be expected. We rarelyobserved more than one leukocyte per capillary evenin sections where long segments of capillaries (100 p)were visible. The average capillary length per leuko-cyte without reflow was found to be 292 1i from thelongitudinal sections in the ischemic area after 5hours. This value is of the same magnitude as the un-branched capillary length of 102 ,i in the dog epicar-dium measured by Bassingthwaighte and co-workers25and much less than the average distance betweenleukocytes in normal, perfused myocardial capil-laries. Unbranched capillary lengths in the endo-cardium of the dog have been reported. The strictcriteria used for identification of leukocytes suggeststhe likelihood that we have underestimated the fre-quency of leukocytes in the light-microscopic analy-sis of our biopsy specimens. The present findings thussupport the concept that there is about one leukocyteper "no reflow" capillary.We cannot draw conclusions from the comparison
of the fraction of no-reflow capillaries at 1, 3, and 5hours of ischemia because of the marked variabilityin the degree of ischemia between animals in the dogmodel of ischemia. Our data do indicate that whenno reflow occurs as early as 1 hour after ischemia,
leukocytes are present at a frequency compatible withobstruction of a single capillary by a single leukocyte.
Leukocyte Accumulation During Ischemia
If the 2433 ,u to 3621 IA capillary length per leuko-cyte observed in the normal nonreperfused myo-cardium is an indication of the normal incidence ofleukocytes in the microcirculation, then the 10-foldincrease in incidence of leukocytes suggests con-tinued "wash-in" of leukocytes during ischemia bycollateral flow and progressive entrapment. Thismechanism would lead to a continuing increase incoronary vascular resistance as more capillaries be-came plugged during ischemia. Leukocytes are ableto reach the central ischemic area because the areacontinues to be perfused immediately after coronaryocclusion at approximately 200/ of normal flow.35The previously described progressive increase incoronary vascular resistance, decrease in coronaryflow, and decrease in peak reactive hyperemia duringmyocardial ischemia may be explained by progressivecapillary obstruction." 35'36
Relation of Leukocyte Plugging toMyocardial Ischemia
Recent studies have shown that the no-reflow phe-nomenon occurs only within areas of myocardiumthat demonstrate histologic evidence of extensivenecrosis." Prevention of reflow by leukocyte pluggingtherefore does not appear to prevent large-scale my-ocardial salvage: However, it is still possible that themechanism of action of nonsteroidal antiinflamma-tory agents, steroids, and hyaluronidase in salvagingsmall amounts of myocardium is prevention of pro-gressive leukocyte plugging." 36-43 Direct endothelialdamage from ischemia seems to occur after extensivemyocyte damage, indicating that endothelial changesare less likely to be involved in no-reflow or progres-sive increases in vascular resistance in the first fewhours of ischemia.7The mechanism of leukocyte capillary plugging has
been seen recently in skeletal muscle capillaries inhemorrhagic shock with the use of intravital micros-copy, where inflow and plugging of capillaries byleukocytes can be observed directly.6 Our findingsparallel these direct observations of Bagge et a16 in anumber of ways. All arterioles and venules were per-fused during ischemia. Only a fraction of capillarieswere occluded. Bagge et al observed a leukocyte inevery capillary without flow. We observed leukocytesonly in capillaries without flow at an average length
Vol. 111 * No. 1
110 ENGLER ET AL AJP * April 1983
compatible with one leukocyte per unbranched capil-lary length. Direct observations of this kind duringhypotension suggest that the mechanism of leukocytecapillary plugging may play an important role in theno-reflow phenomenon of shock and perhaps leads toprogressive ischemia in brain, kidney, and heart2-4' 93'
and other organs.
ConclusionsLeukocytes were seen in no-reflow myocardial cap-
illaries at a frequency 10 times that found in normalperfused myocardium, suggesting that leukocytesaccumulate in ischemic myocardial capillaries. Leu-kocyte frequency correlated with the fraction of no-reflow capillaries in 91 areas of reperfused myocardi-um, suggesting a relationship between no reflow andleukocyte capillary plugging. The average capillarydistance per leukocyte was compatible with obstruc-tion of a single unbranched capillary by a single leu-kocyte. The results of the present study suggest a keyrole of progressive leukocyte capillary plugging inmyocardial ischemia and the no-reflow phenomenon.
References1. Jarmakani JMM, Cox JL, Graham TC, Hackel DB:
Coronary hemodynamics and myocardial perfusionafter reestablishing coronary flow in experimental my-ocardial infarction. Am J Cardiol 1974, 33:146A
2. Ames A, Wright RL, Kowada M, Thurston JM,Majno G: Cerebral ischemia: II. The no reflow phe-nomenon. Am J Pathol 1968, 52:437-453
3. Kloner RA, Ganote CE, Jennings RB: The "no reflow"phenomenon after temporary coronary occlusion inthe dog. J Clin Invest 1974a, 54:1496-1508
4. Flores J, DiBona DR, Beck CH, Leaf A: The role ofcell swelling in ischemic renal damage and the protec-tive effect of hypertonic solute. J Clin Invest 1972, 51:118-126
5. Krug A, deRochemont WM, Korb G: Blood supply ofthe myocardium after temporary coronary occlusion.Circ Res 1966, 19:57-62
6. Bagge U, Ammundson B, Lauritzen C: White bloodcell deformability and plugging of skeletal muscle cap-illaries in hemorrhagic shock. Acta Physiol Scand1980, 108:159-163
7. Kloner RA, Rude RE, Carlson N, Maroko PR,DeBoer LWV, Braunwald E: Ultrastructural evidenceof microvascular damage and myocardial cell injuryafter coronary artery occlusion: Which comes first?Circulation 1980, 62:945-952
8. Darsee JR, Kloner RA: The no reflow phenomenon: Atime limiting factor for reperfusion after coronary oc-clusion? Am J Cardiol 1980, 46:800-806
9. Kloner RA, Ganote CE, Whalen DA, Jennings RB:Effect of a transient period of ischemia on myocardialcells: II. Fine structure during the first few minutes ofreflow. Am J Pathol 1974b, 74:399-422
10. Fukuyama T, Roberts R: Reperfusion induced hemor-rhage-a factor in the development of "no reflow."Circulation (Suppl III) 1980, 62:145
11. Lang T-W, Corday E, Gold H, Meerbaum S, RubinsS, Costantini C, Hirose S, Osher J, Rosen V: Conse-quences of reperfusion after coronary occlusion:Effects on hemodynamics and regional myocardialmetabolic function. Am J Cardiol 1974, 33:69-81
12. Mathur VS, GA Guinn, WH Burris: Maximal revas-cularization (reperfusion) in intact conscious dogs after2 to 5 hours of coronary occlusion. Am J Cardiol 1975,36:252-261
13. Bresnahan GF, Roberts R, Shell WE, Ross J Jr, SobelBE: Deleterious effects due to hemorrhage after myo-cardial reperfusion. Am J Cardiol 1974, 33:82-86
14. Capone RJ, Most AS: Myocardial hemorrhage aftercoronary reperfusion in pigs. Am J Cardiol 1978, 41:259-266
15. Fishbein MC, Y-Rit J, Lando U, Kanmatsuse K,Mercier JC, Ganz W: The relationship of vascular in-jury and myocardial hemorrhage to necrosis afterreperfusion. Circulation 1980, 62:1274-1279
16. Higginson LAJ, F White, HA Heggtveit, TM Sanders,CM Bloor, JW Covell: Determinants of myocardialhemorrhage after coronary reperfusion in the anesthe-tized dog. Circulation 1982, 65:62-69
17. Schmid-Schonbein GW, Shih YY, Chien S: Morphom-etry of human leukocytes. Blood 1980a, 56:866-876
18. Schmid-Schonbein GW, Sung KPL, Tozeren H,Skalak R, Chien S: Passive mechanical properties ofhuman leukocytes. Biophys J 1981, 35:243-256
19. Atherton A, Born GVR: Quantitative investigations ofthe adhesiveness of circulating polymorphonuclearleukocytes to blood vessel walls. J Physiol (Lond)1972, 222:447-474
20. Schmid-Schonbein GW, Usami S, Skalak R, Chien S:The interaction of leukocytes and erythrocytes in capil-lary and post capillary vessels. Microvasc Res 1980b,19:45-70
21. Schmid-Schonbein GW, Fung Y-C, Zweifach BW:Vascular endothelium-leukocyte interaction: Stickingshear force in venules. Circ Res 1975, 36:173-184
22. Bagge U, Johansson BR, Olofsson J: Deformation ofwhite blood cells in capillaries. Adv Microcirc 1977, 7:18-28
23. Chien S: The Red Blood Cells. 2nd edition, Vol 2, Bio-physical behavior of red cells in suspension, AcademicPress, 1975
24. Evan E, Fung YC: Improved measurement of theerythrocyte geometry. Mirovasc Res 1972, 4:335-347
25. Bassingthwaighte JB, Yipintsoi T, Harvey RB: Micro-vasculature of the dog left ventricular myocardium.Microvasc Res 1974, 7:229-249
26. Feldstein ML, Henquell L, Honig CR: Frequency anal-ysis of coronary intercapillary distances: Site of capil-lary control. Am J Physiol 1978, 4:H321-H325
27. Okun EM, SM Factor, ES Kirk: End capillary loops inthe heart: An explanation for discrete myocardial in-farctions without border zones. Science 1979, 206:565-569
28. Henquell L, LaCelle PL, Honig CR: Capillary dia-meter in rat heart in situ: Relation to erythrocyte de-formability, 02 transport, and transmural 02 gradi-ents. Microvasc Res 1976, 12:259-274
29. Henquell L, Odoroff CL, Honig CR: Coronary inter-capillary distance during growth: Relation to PO2 andaerobic capacity. Am J Physiol 1976, 231:1852-1859
30. Haack DW, Bush LR, Shalfer M, Lucchesi BR: Lan-thanium staining of coronary microvascular endothe-lium: Effects of ischemia reperfusion, propranolol, andatenolol. Microvasc Res 1981, 21:362-376
31. Chien S, Sung LA, Kim S, Burke AM, Usami S: Deter-mination of aggregation force in rouleaux fluid me-chanical technique. Microvasc Res 1977, 13:327-333
Vol. 111 * No. 1 LEUKOCYTE CAPILLARY PLUGGING IN ISCHEMIA 111
32. Chien S, King RG, Schuessler GB, Skalak R, TozerenA, Usami S, Copley L: Roles of red cell deformabilityand aggregation in blood viscosity. AICHE Symp Ser1978, 74:56-60
33. Wells R, Schmid-Schonbein H: Red cell deformationand fluidity of concentrated cell suspensions. J ApplPhysiol 1969, 27:213-217
34. Parker PE, Bashour FA, Downey HF, Boutros IS:Coronary reperfusion effects of vasodilation (papav-erine and adenosine). Am Heart J 1977, 93:66-72
35. Guyton RA, McClenathan JH, Michaelis LL: Evolu-tion of regional ischemia distal to a proximal coronarystenosis: Self propagation of ischemia. Am J Cardiol1977, 40:381-392
36. Askenazi J, Hillis LD, Diaz PE, Davis MA, Braun-wald E, Maroko PR: The effects of hyaluronidase incoronary blood flow following coronary artery occlu-sion in the dog. Circ Res 1977, 40:566-571
37. Maroko PR, Libby P, Ginks WR, Bloor CM, ShellWE, Sobel BE, Ross J Jr: Coronary artery reper-fusion: I. Early effects on local myocardial functionand the extent of myocardial necrosis. J Clin Invest1972, 51:2710-2716
38. Powell WJ Jr, Dibona DR, Flores J, Leaf A: The pro-tective effect of hyperosmotic mannitol in myocardialischemia and necrosis. Circulation 1976, 54:603-615
39. DaLuz PL, Forrester JS, Wyatt HL, Diamond GA,
Chag M, Swan HJC: Myocardial reperfusion in acuteexperimental ischemia: Beneficial effects of prior treat-ment with steroids. Circulation 1976, 53:847-852
40. Hill JH, Ward PA: The phlogistic role of C3 leukotac-tic fragments in myocardial infarcts of rats. J Exp Med1972, 133:885-900
41. Willerson JT, Powell WJ Jr, Guiney TE, Stark JJ,Sanders CA, Leaf A: Improvement in myocardialfunction and coronary blood flow in ischemic myo-cardium after mannitol. J Clin Invest 1972, 51:2989-2998
42. Maclean D, Fishbein MC, Braunwald E, Maroko P:Long-term preservation of ischemic myocardium afterexperimental coronary artery occlusion. J Clin Invest1978, 61:541-551
43. Jugdutt BI, Hutchius GM, Bulkley BH, Pitt B, BecherLC: Effect of Indomethacin on collateral blood flowand infarct size in the conscious dog. Circulation 1979,59:734-743
AcknowledgmentThe authors acknowledge the encouragement and sup-
port of J. W. Covell, MD, Colin Bloor, MD, and the ad-vice from B. W. Zweifach, PhD.
Copyright © 2022 FDOKUMEN




















