Laser doppler flowmetry for bone blood flow measurements: Helium-neon laser light attenuation and...
10
Journal of Orthopaedic Research 4:362-371, Raven Press, New York 0 1986 Orthopaedic Research Society Laser Doppler Flowmetry for Bone Blood Flow Measurement: Correlation with Microsphere Estimates and Evaluation of the Effect of Intracapsular Pressure on Femoral Head Blood Flow Marc F. Swiontkowski, *S. Tepic, *tS. M. Perren, *R. Moor, $R. Ganz, and *B. A. Rahn Department of Orthopaedics and Rehabilitation, Vanderbilt University, Nashville, Tennessee, U.S.A.; *Laboratoryfor Experimental Surgery, Davos, fM. E. Muller Institute for Biomechanics, University of Bern, and $Department of Orthopaedics, University of Bern, Bern, Switzerland Summary: Laser Doppler flowmetry (LDF) was used to measure bone blood flow in the rabbit femoral head and femoral condyles. To correlate the LDF output signal blood cell flux to in vivo blood flow, simultaneous measurements using LDF and 85Sr-labeled microspheres were made in an adult rabbit model. There was no correlation between the two methods for blood flow in the fem- oral condyles and the correlation between the two methods for blood flow in the femoral head does not achieve statistical significance. An LDF signal of 0.4 V was approximately equal to a microsphere measured flow rate of 0.4 ml blood/g bone/min. The strength of the correlation in the latter case may have been affected by (a) large arteriovenous shunts, (b) inadequate mixing of the microspheres with a left ventricular injection, and (c) insufficient numbers of microspheres present in the bone samples with which to satisfy the mathemat- ical requirements of the microsphere method. When LDF was used to evaluate the effect of elevated intracapsular pressure on femoral head blood flow in skeletally mature rabbits, femoral head subchondral bone blood flow declined with increasing intracapsular pressure from a baseline value of 0.343 * 0.036 to a value of 0.127 t 0.27 at 120 cm of water pressure. The decline in femoral head blood flow was statistically significant at pressures of 40 cm of water or higher (p < 0.001), and evaluation of sections of the proximal femora made from preterminal disulphine blue injections confirmed these findings. Intra- capsular tamponade has an adverse effect on femoral head blood flow begin- ning well below central venous pressure and should be considered in the pathophysiology of posttraumatic and nontraumatic necrosis of the femoral head. Laser Doppler flowmetry was easy to use and appears to be a reproduc- ible technique for evaluating femoral head blood flow, offering distinct advan- tages over the microsphere technique for measuring bone blood flow. Further studies of the in vivo calibration of the LDF method for bone blood flow are necessary for the method to have potential for clinical application. Key Words: Laser Doppler flowmetry-Microsphere technique-Bone blood flow-Fem- oral head necrosis- Intracapsular pressure. The direct measurement of cancellous and cor- tical bone blood flow is difficult due to the multi- plicity of arterial inflow and venous outflow channels. Because of this anatomic complexity, di- rect methods of bone blood measurement have not been possible. Most of the methods in experimental use today involve estimation by the Use Of radioac- Address correspondence and reprint requests to Dr. M. F. Swiontkowski at DeDartment of OrthoDaedics and Rehabilita- tion, Vanderbilt University, Nashville, fN 37232, U.S.A. tive tracers. In a comprehensive review of the sub- 362
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Laser doppler flowmetry for bone blood flow measurements: Helium-neon laser light attenuation and...

Journal of Orthopaedic Research 4:362-371, Raven Press, New York 0 1986 Orthopaedic Research Society
Laser Doppler Flowmetry for Bone Blood Flow Measurement: Correlation with Microsphere Estimates and
Evaluation of the Effect of Intracapsular Pressure on Femoral Head Blood Flow
Marc F. Swiontkowski, *S. Tepic, *tS. M. Perren, *R. Moor, $R. Ganz, and *B. A. Rahn
Department of Orthopaedics and Rehabilitation, Vanderbilt University, Nashville, Tennessee, U . S . A . ; *Laboratory for Experimental Surgery, Davos, f M . E. Muller Institute for Biomechanics, University of Bern, and $Department of
Orthopaedics, University of Bern, Bern, Switzerland
Summary: Laser Doppler flowmetry (LDF) was used to measure bone blood flow in the rabbit femoral head and femoral condyles. To correlate the LDF output signal blood cell flux to in vivo blood flow, simultaneous measurements using LDF and 85Sr-labeled microspheres were made in an adult rabbit model. There was no correlation between the two methods for blood flow in the fem- oral condyles and the correlation between the two methods for blood flow in the femoral head does not achieve statistical significance. An LDF signal of 0.4 V was approximately equal to a microsphere measured flow rate of 0.4 ml blood/g bone/min. The strength of the correlation in the latter case may have been affected by (a) large arteriovenous shunts, (b) inadequate mixing of the microspheres with a left ventricular injection, and (c) insufficient numbers of microspheres present in the bone samples with which to satisfy the mathemat- ical requirements of the microsphere method. When LDF was used to evaluate the effect of elevated intracapsular pressure on femoral head blood flow in skeletally mature rabbits, femoral head subchondral bone blood flow declined with increasing intracapsular pressure from a baseline value of 0.343 * 0.036 to a value of 0.127 t 0.27 at 120 cm of water pressure. The decline in femoral head blood flow was statistically significant at pressures of 40 cm of water or higher (p < 0.001), and evaluation of sections of the proximal femora made from preterminal disulphine blue injections confirmed these findings. Intra- capsular tamponade has an adverse effect on femoral head blood flow begin- ning well below central venous pressure and should be considered in the pathophysiology of posttraumatic and nontraumatic necrosis of the femoral head. Laser Doppler flowmetry was easy to use and appears to be a reproduc- ible technique for evaluating femoral head blood flow, offering distinct advan- tages over the microsphere technique for measuring bone blood flow. Further studies of the in vivo calibration of the LDF method for bone blood flow are necessary for the method to have potential for clinical application. Key Words: Laser Doppler flowmetry-Microsphere technique-Bone blood flow-Fem- oral head necrosis- Intracapsular pressure.
The direct measurement of cancellous and cor- tical bone blood flow is difficult due to the multi-
plicity of arterial inflow and venous outflow channels. Because of this anatomic complexity, di- rect methods of bone blood measurement have not been possible. Most of the methods in experimental use today involve estimation by the Use O f radioac-
Address correspondence and reprint requests to Dr. M. F. Swiontkowski at DeDartment of OrthoDaedics and Rehabilita- tion, Vanderbilt University, Nashville, f N 37232, U.S.A. tive tracers. In a comprehensive review of the sub-
362
LASER DOPPLER FLO WMETR YIBONE BLOOD FLOW 363
ject of bone blood flow measurement, Tothill (13) concluded: “There is as yet no really quantitative way of measuring bone blood flow nondestruc- tively.” Furthermore, there is no clinical method for measuring or estimating bone blood flow.
Laser Doppler flowmetry (LDF) is a relatively new method for measuring blood flow within capil- lary beds and has proven useful in measuring bone blood flow both experimentally (S,6) and clinically (R Ganz, MF Swiontkowski, unpublished data). A difficulty with the method is that the output signal, blood cell flux (BCF), is expressed in volts. This is due to the intricate microvascular anatomy and the complexity of the interaction of light with tissue (6,lO). Blood cell flux measured in volts is not a unit of flow and thus is difficult to apply to experi- mental and clinical problems of normal and patho- logic bone perfusion. Estimation of bone blood flow in experimental conditions is considered to be best accomplished by the radioactive-labeled mi- crosphere technique (4,13). The purpose of these studies was to establish the utility of LDF in bone blood flow measurement and to correlate the LDF output signal with a rate for bone blood flow in terms of ml of blood/g of bonelmin by performing simultaneous LDF and microsphere measurements for several sites in a rabbit model.
Femoral head necrosis is an area of particular concern to the orthopaedic surgeon. Elevated in- tracapsular pressure is thought to play a role in the pathophysiology of posttraumatic and nontrau- matic necrosis of the femoral head (3,12,17). In both skeletally mature and immature animals fem- oral head ischemia has been produced by elevation of intracapsular pressure (3,17). In these studies evaluation of femoral head perfusion was per- formed with intravital dyes or oxygen sensors. However, the adverse effect of intracapsular tam- ponade has been difficult to determine because of difficulties in measuring dynamic changes in bone blood flow. Laser Doppler flowmetry selected as the method for evaluating femoral head blood flow under conditions of increasing intracapsular pres- sure in a skeletally mature rabbit model. This study was designed to provide additional information re- garding the utility of LDF in experimental bone blood flow measurement.
MATERIALS AND METHODS
Microsphere Study
The laser Doppler flowmeter (Pfl Periflux; Per-
imed KB, S-1114 86 Stockholm, Sweden) used in this study uses a 2mW He-Ne laser source. The af- ferent fiber within the three-fiber cable conducts the light to the bone. The light within a 1 - 1 .S mm hemisphere under the probe is then reflected by the moving blood cells, producing a Doppler shift. The two efferent fibers conduct the backscattered frac- tion to photodetectors that convert it to electrical energy. The extracted Doppler signal is processed by the two-channel system and transformed into an output signal (BCF). This represents the product of the concentration and mean velocity of the blood cells within the volume of bone under the probe. Further details regarding the principles and engi- neering of the method have been published else- where (9,lO). Due to the intricate anatomy of the microvascular bed and the complexity of the inter- action of light with tissue (5,6,10), the output signal is expressed in volts rather than conventional units of flow (ml/g of bonejmin).
Ten 4 kg adult New Zealand white rabbits were used. The femoral head was selected as one region of interest because of the available data on femoral head blood flow in the rabbit with the microsphere technique. The technique published previously for the rabbit femoral head by Wang et al. (14,15) was carefully followed. Under standard nitrous oxide- halothane anesthesia, an 18-gauge polyethylene catheter with a single port was sutured in place into the left ventricle via the left carotid artery and the position confirmed by the pressure tracings. A 20- gauge catheter was placed into the right brachial ar- tery, advanced 4 cm, and sutured in place. A hepa- rinized saline solution was used to flush this cath- eter and assure patency. This catheter was connected to a roller pump that was adjusted to withdraw at a rate of 2 ml/min when in use (Fig. 1).
Blood cell flux of both femoral heads was mea- sured via an anterior capsulotomy. We had earlier observed that the BCF of the subchondral bone could be measured through the articular cartilage. This avoids the production of bleeding which is a potential source of artifact for the LDF method. The probe was placed against the femoral head and held with a clamp that was attached to an external fixator system from a midshaft femoral pin. Fol- lowing the measurements of the femoral heads, both lateral femoral condyles were measured by drilling 2.3 mm holes (for the 2.2 mm probe) 8 mm deep into the midportion of the lateral femoral con- dyles. The probe was again held with the external fixator to minimize motion artifact (Fig. 2 ) .
Data from the LDF and mean arterial pressure
J Orthop Res, Vol. 4, No. 3 , 1986

364
- Difference amplif icr
M . F. SWIONTKOWSKI ETAL.
Signal output processor -signal
I
FIG. 1. Block diagram of the laser Doppler flowmetry differential channel operation setup.
He-Ne - Laser
I \
were sampled every 3 s and stored in a PDP 11/03 computer. Following the series of four measure- ments, one million 15 km 85Sr-labeled microspheres (Nen-Trac, DuPont, Zurich 8050, Switzerland) were injected into the left ventricle over 60 s as the hind limbs were exercised in the supine position. With- drawal via the roller pump was started 30 s before the injection and continued for 2.5 min. The intra- ventricular line was flushed with 1 ml heparinized saline over 30 s following the injection of the mi- crospheres and the animal was killed with a barbi- turate overdose. The femoral heads were removed at the level of the articular cartilage with an osteo- tome and the lateral femoral condyles were re- moved by an oscillating saw and cleaned of all soft tissue. A sample of lung tissue was harvested as a gross indicator of total arteriovenous shunting. The radioactivity of these samples and of two reference blood samples were counted for 5 min in a gamma counter after appropriate adjustment of the so- dium-iodide crystal for *%r. Means and standard deviations were determined for the LDF values and blood pressure during the measurement period for each region of interest. Blood flow estimated from microspheres was calculated using the standard equations (7,s). The LDF versus microsphere-esti- mated blood flow was plotted for the femoral con- dyles and femoral heads.
Photo- Photo-
and filter and filter
- Level indicator - detector __< * detector -
Intracapsular Pressure Study
Eight adult New Zealand white rabbits were
Level indicator
FIG. 2. Schematic of the laser Doppler flowmetry measure- ment sites for microsphere correlation.
J Orthop Res , Vol. 4 , No. 3 , 1986

LASER DOPPLER FLO WMETR YIBONE BLOOD FLOW 365
used. Under standard nitrous oxide-halothane an- esthesia, a superior approach was made to the hip joint with no dissection around the proximal femur. The hip capsule was not opened or exposed. A spe- cially designed 4.0 mm screw was placed into the hip joint from the acetabular side under fluoro- scopic control. The hip joint was distracted during the drilling, tapping, and insertion of the screw in an attempt to prevent injury to the femoral head.
The femoral head in these animals measured 7-8 mm in diameter and this made orientation of the acetabular screw difficult and critical. The angle of inclination was controlled radiographically but was not perfectly reproducible. In animal F11 the angle of orientation of the screw (and therefore the probe) exceeded 60". When the angle of the probe to the tissue to be measured exceeds 45" (6,9,1 l), all the Doppler-shifted light is not received by the efferent bundles, resulting in a falsely low BCF output signal. In each rabbit the hindlimb was left in a neutral rotation, neutral abduction-adduction position so that the probe was resting on the "weight-bearing'' area of the femoral head. Subtle differences in limb positioning as well as in the angle of inclination of the probe may account for some of the variation in baseline LDF. When ro- tating the limb to measure the femoral head blood flow in other regions, the probe was held against the femoral head cartilage by the silastic cuff.
The acetabular screw had a 3.0 mm hole drilled in the central axis and the LDF probe was placed through this hole and against the articular cartilage (Fig. 3 ) . A silastic cuff around the probe provided a water-tight seal for the hip joint. Through a sepa- rate l mm hole in the screw the hip joint was filled with a 6% dextran solution and the pressure main- tained at selected levels using a fluid column and water manometer. The pressure was controlled with a water manometer. Blood pressure was con- tinuously monitored via a catheter in the femoral artery. The LDF and blood pressure data were re- corded at 5 s intervals and stored in a PDP 11/03 computer. The BCF within the subchondral bone of the femoral head was measured under baseline con- ditions and under 20, 40, 80, and 120 cm of water pressure within the joint. Baseline condition was defined as no measurable hydrostatic pressure within the hip joint. Two trials were made at each pressure level, allowing the BCF to return to the baseline for 5 min between the trials. Random ap- plication of the various pressure levels was used to
FIG. 3. Schematic illustration of the acetabular screw with the laser Doppler flowmetry probe and the infusion system for the hip joint.
check the results. After the trials at each pressure level, the pressure within the joint was maintained at either 40 or 80 cm of water for 2 or 6 h (two an- imals for each condition). An injection of disul- phine blue (62.5 mglkg) preceded death from a bar- biturate overdose. Noncalcified sections (1 10 pm thick) of the proximal femora were made to eval- uate perfusion, with the nonoperated side serving as the control. The sections were made of the middle weight-bearing section of the femoral head in the coronal plane and were evaluated using stan- dard light microscopic techniques.
RESULTS
Microsphere Study
Two of the 10 injections resulted in acute hypo- tension and the data from these trials were ex-
J Orthop Res. Vol. 4 , No. 3 , I986
366 M . F. SWIONTKOWSKI ET AL.
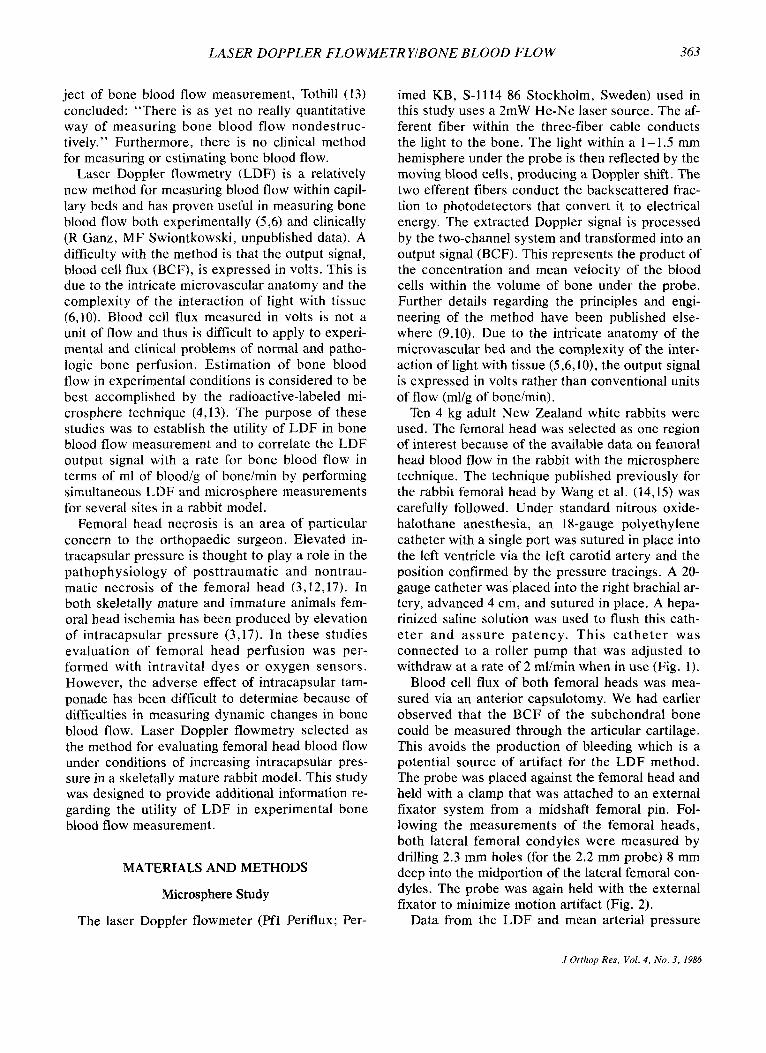
cluded. One femoral head was lost in transfer and was unavailable for counting in the gamma counter and is also excluded. Evaluation of the counts per specimen data and the disintegrations/min/sphere value revealed that there were no specimens that contained >lo0 spheres. The plots correlating the two methods for the femora1 condyles and for the femoral heads are shown in Fig. 4. There was no correlation (r = -0.348) between LDF and the mi- crosphere technique in the femoral condyles, and the correlation for the femoral head (r = 0.490, p < 0.1) approaches but does not achieve statistical sig- nificance.
Large arteriovenous shunt fractions were sus- pected for five of the 10 animals as evidenced by lung counts fivefold higher than the reference tissue (mean flow 2.2 ml blood/g of lung tissue/min versus mean flow 0.42 ml/g of bone/min. This is a crude indicator of left-right (arterial to venous) shunting and reflects spheres that have not been trapped in capillary beds and have returned to the right side of the heart.
I ' I ' I ' I ' I ' I
1 1.01 CONDYLE 0
0.81 & 0
0 - 0 > Y O . t
m 0 00 0 0 i 0 0
. .
FEMORAL HEAD
0
A A
0.5
0.31 0
0.2 0.0 0.2 0.4 0.6 0.8 1.0
BLOOD FLOW (ml/g/min)
FIG. 4. Plot of blood cell flux versus microsphere estima- tions for the femoral condyle (above) and femoral head (below). The linear regression curve for the femoral head is shown (r = 0.490, p < 0.1).
The LDF output signal did not vary >5% over the 100 data points (300 s) for the femoral heads. In five of the femoral condyle measurements brief 10-20 s surges in the output signal to 20-30% higher than the baseline occurred. These corre- spond to the upper group of data points in the aver- aged data plotted in Fig. 4. These surges seemed to correspond to bleeding at the base of the drill holes observed around the LDF probe.
Intracapsular Pressure Study
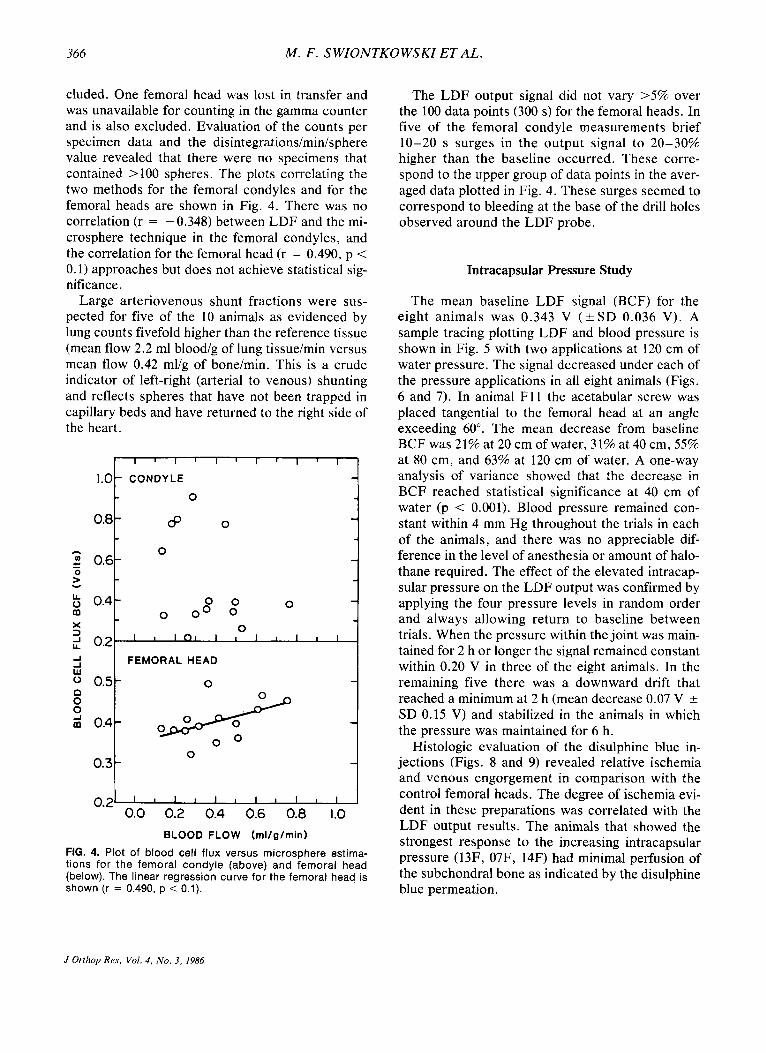
The mean baseline LDF signal (BCF) for the eight animals was 0.343 V ( k S D 0.036 V). A sample tracing plotting LDF and blood pressure is shown in Fig. 5 with two applications at 120 cm of water pressure. The signal decreased under each of the pressure applications in all eight animals (Figs. 6 and 7). In animal F11 the acetabular screw was placed tangential to the femoral head at an angle exceeding 60". The mean decrease from baseline BCF was 21% at 20 cm of water, 31% at 40 cm, 55% at 80 cm, and 63% at 120 cm of water. A one-way analysis of variance showed that the decrease in BCF reached statistical significance at 40 cm of water (p < 0.001). Blood pressure remained con- stant within 4 mm Hg throughout the trials in each of the animals, and there was no appreciable dif- ference in the level of anesthesia or amount of halo- thane required. The effect of the elevated intracap- sular pressure on the LDF output was confirmed by applying the four pressure levels in random order and always allowing return to baseline between trials. When the pressure within the joint was main- tained for 2 h or longer the signal remained constant within 0.20 V in three of the eight animals. In the remaining five there was a downward drift that reached a minimum at 2 h (mean decrease 0.07 V 2 SD 0.15 V) and stabilized in the animals in which the pressure was maintained for 6 h.
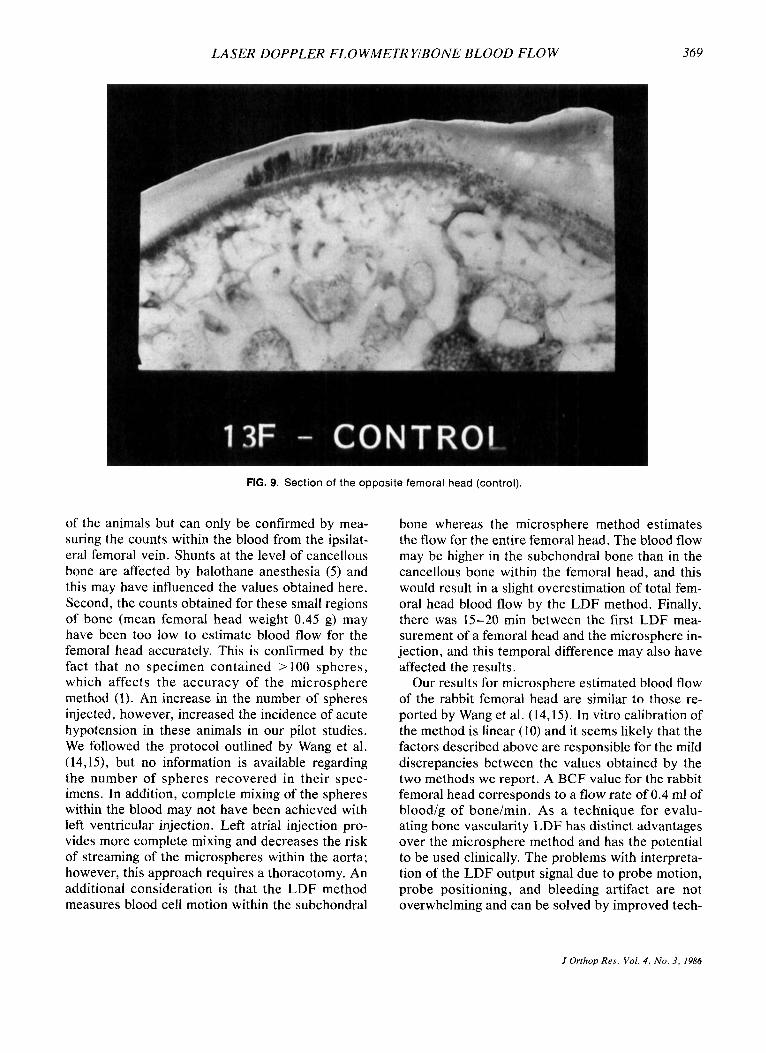
Histologic evaluation of the disulphine blue in- jections (Figs. 8 and 9) revealed relative ischemia and venous engorgement in comparison with the control femoral heads. The degree of ischemia evi- dent in these preparations was correlated with the LDF output results. The animals that showed the strongest response to the increasing intracapsular pressure (13F, 07F, 14F) had minimal perfusion of the subchondral bone as indicated by the disulphine blue permeation.
J Orthop Res, Vol. 4 , No. 3 , 1986
LASER DOPPLER FLO WMETR YIBONE BLOOD FLOW 367
70FRO3
BC F .5- . . .... , . . . I . . , - ' . . - I 1. .Ir- 1'. .3- .2- . I- . . . . . ..... 120CM H20 t . . . . , ..... . . . . . . .
c t c 4 PRESSURE ON
4 PRESSURE OFF
DISCUSSION
LDF Method and Microsphere Correlation
The LDF method was quick, easy, and gave re- producible data over the measurement periods. On multiple measurements at the same site, LDF proved to be reproducible within 5% for the femoral heads which is similar to the experience of Hellem et al. (6) in comparing LDF with 133Xe washout for bone blood flow measurement. Motion artifact was avoided by using the external fixator unit to hold the probe. Bleeding artifact was avoided for the femoral heads by measuring through the femoral head articular cartilage but was evident for the fem-
LDF Volts 1
I 0-I 0 20 LO 80 120 cm H,O
lntracapsular Pressure
FIG. 6. Plot of the individual animal responses to each of the four intracapsular pressure conditions.
FIG. 5. Copy of the PDP 11/03 output showing blood pressure above and blood cell flux below. There IS a 5 s interval be- tween data points. The intracapsular pres- sure (120 cm water) was applied at points 10 and 50 and released at points 30 and 75 as
I I
I I indicated by the arrows.
oral condyles as a result of drilling holes into the cancellous bone. The microsphere technique was more time-consuming and technically difficult. Acute hypotension following injection of the spheres into the left ventricle was also a problem.
We hypothesize that the lack of correlation be- tween the two methods for the femoral condyles is due to bleeding artifact. The drilling of 2.3 mm holes was accompanied by brisk bleeding from the holes as expected. The LDF method cannot distin- guish blood flow within sinusoids, capillaries, or terminal arterioles from bleeding due to disruption
0 20 40 60 80 100 120 INTRACAPSULAR PRESSURE ICP (cm &O)
u .w
FIG. 7. Graph of the composite data for all eight animals under the five pressure conditions. Standard error of the mean is represented by the bars.
J Orrhop Res, Vol. 4 , NO. 3 , 1986

368 M . F . SWIONTKOWSKI ET AL.
FIG. 8. Section of femoral head following disulphine blue injection. For 2 h prior to the preterminal injection 80 cm of water pressure was applied within the hip joint. The sections reveal relative ischemia as evidenced by narrowing of vascular channels and decreased dye uptake.
of these structures. This was evidenced by strong surges in the LDF signal at irregular time intervals. Eventually it should be possible to get an accurate reading from the base of a drill hole after the bleeding ceases. The flow within the trabecular bone would, however, be influenced by the trauma of drilling for a minimum of 4 to 6 weeks. This is also a problem for the hydrogen and 133Xe washout methods of estimating bone blood flow (6,11,13,16) since they also require drilling and insertion of an electrode or injection of gas. Measurements with the LDF method can be made at the surface of cor- tical or cancellous bone. When measuring more deeply in the bone, an implant to hold the probe should be used and a period of time allowed for the bone at the base of the implant to stabilize.
Hellem et al. (6) reported no correlation between the LDF method and the 133Xe washout technique for measuring bone blood flow in the cancellous bone of the pig mandible. The LDF measurements proved to be far more reproducible than the 133Xe estimates for blood flow. The 133Xe method is in- fluenced by injection depth and tissue diffusion
rate. The LDF indicates the product of the mean velocity and concentration of the blood cells within the volume of bone under the probe. Blood cells within any type of vascular channel will influence the signal. Because of tissue diffusion parameters, the 133Xe method estimates only capillary blood flow within an undefined volume of bone in the re- gion of the injection. The hydrogen washout tech- nique has been used to monitor the effects of im- mobilization on femoral head blood flow in puppies (1 1). The method was shown to be reproducible but does require drilling for insertion of the platinum electrode which may alter local blood flow as it did during the femoral condyle measurements in this study.
The correlation between the LDF measurements and the microsphere estimates for femoral head blood flow approaches but does not achieve statis- tical significance (r = 0.490, p < 0.1). There are several factors that may influence this correlation. First, there may be large arteriovenous shunts functional at the level of the proximal femur. This is suggested by the high lung counts observed in 50%
.I Orthop Res, Vol. 4, No. 3, 1986
LASER DOPPLER FLO WMETR YIBONE BLOOD FLOW 369
FIG. 9. Section of the opposite femoral head (control)
of the animals but can only be confirmed by mea- suring the counts within the blood from the ipsilat- era1 femoral vein. Shunts at the level of cancellous bone are affected by halothane anesthesia (5 ) and this may have influenced the values obtained here. Second, the counts obtained for these small regions of bone (mean femoral head weight 0.45 g) may have been too low to estimate blood flow for the femoral head accurately. This is confirmed by the fact that no specimen contained >lo0 spheres, which affects the accuracy of the microsphere method (1). An increase in the number of spheres injected, however, increased the incidence of acute hypotension in these animals in our pilot studies. We followed the protocol outlined by Wang et al. (14,15), but no information is available regarding the number of spheres recovered in their spec- imens. In addition, complete mixing of the spheres within the blood may not have been achieved with left ventricular injection. Left atrial injection pro- vides more complete mixing and decreases the risk of streaming of the microspheres within the aorta; however, this approach requires a thoracotomy. An additional consideration is that the LDF method measures blood cell motion within the subchondral
bone whereas the microsphere method estimates the flow for the entire femoral head. The blood flow may be higher in the subchondral bone than in the cancellous bone within the femoral head, and this would result in a slight overestimation of total fem- oral head blood flow by the LDF method. Finally, there was 15-20 min between the first LDF mea- surement of a femoral head and the microsphere in- jection, and this temporal difference may also have affected the results.
Our results for microsphere estimated blood flow of the rabbit femoral head are similar to those re- ported by Wang et al. (14,15). In vitro calibration of the method is linear (10) and it seems likely that the factors described above are responsible for the mild discrepancies between the values obtained by the two methods we report. A BCF value for the rabbit femoral head corresponds to a flow rate of 0.4 ml of bloodlg of bonelmin. As a technique for evalu- ating bone vascularity LDF has distinct advantages over the microsphere method and has the potential to be used clinically. The problems with interpreta- tion of the LDF output signal due to probe motion, probe positioning, and bleeding artifact are not overwhelming and can be solved by improved tech-
J Orthov Res, Vol. 4, No. 3, 1986

3 70 M . F . SWIONTKOWSKI ET AL.
niques for probe holding and avoidance of bleeding in the region of the probe tip. Further correlative studies including repeat microsphere trials in other animal models are necessary to clarify these pre- liminary results.
Intracapsular Pressure Study
Since the LDF probe is motion sensitive, we used an acetabular screw as a probe holder. The potential problem of bleeding in the region of the probe producing an artifact was avoided by placing the probe against the femoral head articular carti- lage. The acetabular approach to the femoral head with no dissection around the hip capsule also al- lowed for a more accurate evaluation of femoral head blood flow. The surgical manipulation and hal- othane anesthesia may have influenced the femoral head perfusion to some degree but are necessary for the LDF technique.
Accuracy in blood flow measurement was im- proved by the 5 s sampling interval and a minimum of two trials at each pressure level. Random appli- cation of the sequence of pressures confirmed the effect of elevated intracapsular pressure on femoral head blood flow. The histologic sections of the di- sulphine blue preterminal injections also confirmed the effect of the intracapsular pressure but serve as only a gross estimation of bone perfusion and do not represent true bone blood flow.
Intracapsular pressures in the range used in this study have been measured in patients with femoral neck fractures (2,12). Drake and Meyers (2) have suggested that unless the pressure within the hip capsule is greater than central venous pressure it plays no role in the pathophysiology of posttrau- matic necrosis of the femoral head. Our data sug- gest that pressures lower than central venous pres- sure have a negative effect on femoral head blood flow in an intact femur. The intraarticular pressure at which the effect became statistically significant (40 cm H,O) probably represents the local venous pressure within the capsular veins draining the fem- oral head. These pressures would probably have a much greater effect with a disrupted femoral neck. Intracapsular pressures in this range have also been shown by Ganz et al. (3) and Woodhouse (17) to produce femoral head ischemia in animal models with an open physis. The effect we have docu- mented here in skeletally mature rabbits may in- deed be more dramatic in juvenile rabbits. In evalu- ating the histologic preparations it seemed apparent
that the effect on total blood flow (LDF) occurred on the venous side as we frequently observed di- lated subchondral sinuoids compared with the con- trol side.
From these studies we conclude that LDF pro- vides advantages over other methods used to esti- mate bone blood flow and it has the potential for clinical application. The technique has been used clinically in measuring femoral head blood flow in- traosseously as well as across the articular cartilage (R Ganz, MF Swiontkowski, unpublished data). Application for cancellous bone blood flow in the distal femur has also proven possible across the ar- ticular cartilage and within the cancellous bone. In this respect, LDF measurement through articular cartilage seems possible up to a 2 mm thickness. The method has also been used in measuring blood flow within intact and reconstructed cruciate liga- ments.
Acknowledgment: This study was supported by the Swiss National Science Foundation (Grant No. 88.235.0.84) and by a grant from A 0 International. Spe- cial thanks to Tony Keller, M.S.E. , for reviewing the manuscript, and to Holly Quick for preparing the rnanu- script.
1.
2.
3.
4.
5.
6.
7.
8.
9.
REFERENCES
Buckberg GD, Luck JL, Payne P, Hoffman JI, Archie JP, Fixler DE: Some sources of error in measuring regional blood flow with radioactive microspheres. J Appl Physiol
Drake JK, Meyers MH: Intracapsular pressure and he- moarthrosis following femoral neck fracture. Clin Ortlzop
Ganz R, Luthi U , Rahn BA, Perren SM: Intraartikulare druckerhohung und epiphysare durchblutungsstorung. Orth- opade 10:6-8, 1981 Gross PM, Marcus ML, Heistad DD: Measurement of blood flow to bone and marrow in experimental animals by means of the microsphere technique. J Bone Joint Surg [Am]
Hellem S, Jacobsson LS, Nilsson GE: Microvascular re- sponse in cancellous bone to experimental halothane in- duced hypotension in pigs. Int J OralSurg 12:178-185, 1983 Hellem S, Jacobsson LS, Nilsson GE, Lewis DH: Measure- ment of microvascular blood flow in cancellous bone using laser Doppler flowmetry and 133Xe clearance. Int J Oral
Heyman MA, Payne BD, Hoffman JI, Rudolph AM: Blood flow measurements with radionuclide labeled particles. Prog Cardiovasc Dis 20:55-79, 1977 Lunde PKM, Michelson K: Determination of cortical blood flow in rabbit femur by radioactive microspheres. Acta Physiol Scand 80:39-44, 1970 Nilsson GE, Salerud EG, Tenland T, Oberg PA: Laser Doppler tissue blood flow measurements. In: Biomedical Applicutions of Laser Light Scattering, ed by DB Satelle,
31~598-604, 1971
182:172-176, 1984
63: 1028- 103 1, 198 1
Surg 12:165-177, 1983
J Orthop Rrs , Vol. 4, No. 3, I986

LASER DOPPLER FLO WMETR YIBONE BLOOD FLOW
WI Lee, BR Ware, Amsterdam, ElsevieriNorth Holland Biomedical Press, 1982, pp 335-348
10. Nilsson GE, Tenland T, Oberg PA: Evaluation of a laser Doppler flowmeter for measurement of tissue blood flow. IEEE Trans Biomed Eng BME-27: No. 10, 1980
1 1 . Schoenecker PL, Bitz DM, Whiteside LA: The acute effect of position of immobilization on capital femoral epiphyseal blood flow. J Bone Joint Surg [Am] 60:899-904, 1978
12. Soto-Hall R, Johnson LH, Johnson R: Alterations in the in- traarticular pressures in transcervical fractures. J Bone Joint Surg [Am] 45:662, 1963
13. Tothill P: Bone blood flow measurement. J Biomed Eng 6:251-256, 1984
14. Wang GJ, Dughman SS, Reger SI, Stamp WJ: The effect of
3 71
core decompression on femoral head blood flow in steroid- induced avascular necrosis of the femoral head. f Bone Joint Surg [Am] 67:121-124, 1985
15. Wang GJ, Hubbard SL, Reger SI, Miller ED, Stamp WJ: Femoral head blood flow in long-term steroid therapy: Study of a rabbit model. South Med J 76:1530-1532, 1983
16. Whiteside LA, Lesker PA, Simmons DJ: The measurement of regional bone and bone marrow blood flow in the rabbit using the hydrogen washout technique. Clin Orrhop
17. Woodhouse CF: Dynamic influences of vascular occlusion affecting the development of avascular necrosis of the fem- oral head. Clin Orthop 32:119-128, 1962
122:340-346, 1977
J Orthop ReJ. Vol . 4, No. 3 , 1986