Derrnatologic Laser Surgery
22
Derrnatologic Laser Surgery Wendy W. Lou, MD, and Roy G. Geronemus, MD A DVANCES IN TECHNOLOGY have made la- sers an important presence in the practice of medicine. Lasers have become a critical part of dermatology providing the treatment of choice for many dermatologic conditions. As a consequence of the therapeutic advances provided by lasers, clinicians today should have an overall under- standing of laser applications and should keep abreast with the advances in this field. After a brief introduction on laser history and physics, clinical applications of lasers will be pre- sented in detail. Four main topics will be the fo- cus: vascular lesions, pigmented lesions, resurfac- ing, and hair removal. LASER HISTORY The concept of light amplification by stimu- lated emission of radiation (LASER) light produc- tion was first proposed by Albert Einstein in 1917 in The Quantum Theory of Radiation. About 40 years later, Townes and Gordon actually built a system producing monochromatic radiation by stimulated emission with microwaves--MASER (microwave amplification by stimulated emission of Radiation). The first LASER was developed by Maiman in 1960 by using ruby crystals and flashlamps. It is no surprise that the field of der- matology leads the advancement of laser technol- ogy because skin is one of the most accessible organs for laser effects. A dermatologist, Goldman, was the first to pub- lish his finding of ruby laser treatment of the hu- man skin in 1963. Subsequently, a number of con- tinuous-wave lasers were developed: argon (488 nm, 514 nm), carbon dioxide (10,600 nm), and neodynium:yttrium-aluminum-garnet (Nd:YAG) (1064 nm). There was initial enthusiasm in the 70s until it became clear that treatments were fre- quently associated with high risk-to-benefit ratio. Because of the nonspecific tissue injury from these continuous-wave lasers, the incidence of scarring was particularly high. Thus, the popularity of this group of lasers declined for those conditions with alternative treatment options or for those that would improve during natural course of disease, such as hemangiomas. In 1983, Anderson and Parrish presented the theory of selective photothermolysis~ which launched a new era in laser technology. With a better understanding of laser-tissue interaction, lasers are developed with specific tissue effects in mind. The first laser developed in accordance with this theory was the flashlamp pumped pulsed dye laser, which has revolutionized the treatment of vascular lesions. Since then, other lasers have been designed and applied in the similar manner. Because of the selective nature of tissue injury, this new generation of lasers has very low inci- dence of long-term side effects if used appropri- ately. Today, lasers often provide a favorable alter- native to traditional nonlaser treatment options for a rapidly expanding list of dermatologic con- ditions. LASER PHYSICS Laser light is a type of electromagnetic radia- tion, which is a form of energy that has properties of both waves and discrete particles of energy called photons. Electromagnetic radiation is often categorized according to wavelengths: gamma rays, x-rays, ultraviolet rays, visible light, infrared radiation, microwaves, and radio waves. The spec- trum of light used in dermatologic lasers is in the visible and infrared wavelength range (400 nm to 10,600 nm). The term LASER is an acronym for light ampli- fication by stimulated emission of radiation, the mechanism by which such light is produced. Elec- trons of an atom or molecules normally orbit in the resting state or the lowest energy state. These electrons may absorb certain set amounts of en- ergy in the form of photons and may be risen to an excited state at a higher energy orbit. Such elec- trons at the excited state are relatively unstable and may spontaneously return to their resting state by discharging photons of light containing the same amount of energy as initially absorbed. Such occurrence is termed spontaneous emission of Reprintedfrom Current Problems in Dermatology 13(1):5-24, 2001 with permission. Copyright 2001, Elsevier Science (USA). All rights reserved. 1085-5629/02/2102-0002535.00/0 doi: l O. 1053/sder.2002.33286 Seminars in Cutaneous Medicine and Surgery, Vol 21, No 2 (June), 2002: pp 107-128 107
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Derrnatologic Laser Surgery

Derrnatologic Laser Surgery Wendy W. Lou, MD, and Roy G. Geronemus, MD
A DVANCES IN TECHNOLOGY have made la- sers an important presence in the practice of
medicine. Lasers have become a critical part of dermatology providing the treatment of choice for many dermatologic conditions. As a consequence of the therapeutic advances provided by lasers, clinicians today should have an overall under- standing of laser applications and should keep abreast with the advances in this field.
After a brief introduction on laser history and physics, clinical applications of lasers will be pre- sented in detail. Four main topics will be the fo- cus: vascular lesions, pigmented lesions, resurfac- ing, and hair removal.
LASER H I S T O R Y
The concept of light amplification by stimu- lated emission of radiation (LASER) light produc- tion was first proposed by Albert Einstein in 1917 in The Quantum Theory of Radiation. About 40 years later, Townes and Gordon actually built a system producing monochromatic radiation by stimulated emission with microwaves--MASER (microwave amplification by stimulated emission of Radiation). The first LASER was developed by Maiman in 1960 by using ruby crystals and flashlamps. It is no surprise that the field of der- matology leads the advancement of laser technol- ogy because skin is one of the most accessible organs for laser effects.
A dermatologist, Goldman, was the first to pub- lish his finding of ruby laser treatment of the hu- man skin in 1963. Subsequently, a number of con- tinuous-wave lasers were developed: argon (488 nm, 514 nm), carbon dioxide (10,600 nm), and neodynium:yttrium-aluminum-garnet (Nd:YAG) (1064 nm). There was initial enthusiasm in the 70s until it became clear that treatments were fre- quently associated with high risk-to-benefit ratio. Because of the nonspecific tissue injury from these continuous-wave lasers, the incidence of scarring was particularly high. Thus, the popularity of this group of lasers declined for those conditions with alternative treatment options or for those that would improve during natural course of disease, such as hemangiomas.
In 1983, Anderson and Parrish presented the
theory of selective photothermolysis~ which launched a new era in laser technology. With a better understanding of laser-tissue interaction, lasers are developed with specific tissue effects in mind. The first laser developed in accordance with this theory was the flashlamp pumped pulsed dye laser, which has revolutionized the treatment of vascular lesions. Since then, other lasers have been designed and applied in the similar manner. Because of the selective nature of tissue injury, this new generation of lasers has very low inci- dence of long-term side effects if used appropri- ately. Today, lasers often provide a favorable alter- native to traditional nonlaser treatment options for a rapidly expanding list of dermatologic con- ditions.
LASER P H Y S I C S
Laser light is a type of electromagnetic radia- tion, which is a form of energy that has properties of both waves and discrete particles of energy called photons. Electromagnetic radiation is often categorized according to wavelengths: gamma rays, x-rays, ultraviolet rays, visible light, infrared radiation, microwaves, and radio waves. The spec- trum of light used in dermatologic lasers is in the visible and infrared wavelength range (400 nm to 10,600 nm).
The term LASER is an acronym for light ampli- fication by stimulated emission of radiation, the mechanism by which such light is produced. Elec- trons of an atom or molecules normally orbit in the resting state or the lowest energy state. These electrons may absorb certain set amounts of en- ergy in the form of photons and may be risen to an excited state at a higher energy orbit. Such elec- trons at the excited state are relatively unstable and may spontaneously return to their resting state by discharging photons of light containing the same amount of energy as initially absorbed. Such occurrence is termed spontaneous emission of
Reprinted from Current Problems in Dermatology 13(1):5-24, 2001 with permission.
Copyright 2001, Elsevier Science (USA). All rights reserved. 1085-5629/02/2102-0002535.00/0 doi: l O. 1053/sder.2002.33286
Seminars in Cutaneous Medicine and Surgery, Vol 21, No 2 (June), 2002: pp 107-128 107

108 LOU AND GERONEMUS
radiation. If an already excited electron absorbs a photon of light, it will emit two photons of light when it falls back to its resting state. These two photons will have the same energy and wave- length and will be spatially and temporally in phase with each other. This is called stimulated emission of radiation. Because most of the elec- trons are normally in the resting state, stimulated emission occurs rarely. However, if external en- ergy is supplied so that most of the electrons in the lasing cavity are in excited states, the chance of stimulated emission is much higher. The state in which most electrons are in the excited state is called population inversion.
The laser apparatus has 3 essential components. The pumping system is the external energy source. The lasing medium (gain medium) sup- plies the electrons necessary for emitting laser ra- diation and determines the wavelength of such radiation. The medium may be a gas, such as ar- gon, carbon dioxide, and copper vapor; a liquid, such as tunable dye; or a solid, such as ruby, alex- andrite, diode, Nd:YAG, and erbium:yttrium-alu- minum-garnet (Er:YAG). The optical resonator (optical cavity, lasing cavity) contains the lasing medium and has two parallel, opposing mirrors, one of which is partially reflective. Photons of light travel back and forth between the mirrors while stimulating emission of more photons of light that are in phase. Finally, some photons of light exit the cavity through the partially reflective mirror and make up the laser beam.
Laser light is generated in a manner that gives it characteristic properties common to all laser beams. Light from a laser is monochromatic, that is, of one wavelength or a very narrow band of wavelengths. The wavelength is characteristic of the particular lasing medium used. This mono- chromacity allows selective absorption by specific chromophores, thus affecting only selective tis- sues. Laser light is also temporally and spatially coherent, meaning that the emitted waves are in phase both in time and space. Such coherence results in a collimated, unidirectional beam of light which is critical to the proper delivery of the laser beam from the optical cavity to the target tissue without much divergence. A collimated beam has the same spot size regardless of how far the tissue is from the handpiece. However, some laser systems are purposely designed with an ad- ditional focusing lens allowing convergence or di-
vergence of the light beam by moving the hand- piece closer to or further from the tissue. Finally, laser light beam is extremely bright containing a large amount of energy in a small area, thus creat- ing a dramatic tissue effect.
In addition to the wavelengths, lasers vary in their pulse durations. Continuous-wave lasers, such as carbon dioxide, argon, and krypton, emit a continuous beam of light at the same energy. Me- chanical shutters may be used with these lasers to allow laser emission for a set time (usually 0.02- 1.00 seconds or more) and similar amount of off or close time. The power is in the 1- to 100-W range. The quasicontinuous-wave lasers, such as the superpulsed carbon dioxide, copper vapor, copper bromide, and potassium-titanyl-phos- phate (KTP) lasers, emit a rapid train of short pulses. These lasers affect the skin in the same manner as the continuous-wave lasers. Pulsed la- sers, such as the flashlamp-pumped pulsed dye laser, emit pulses with peak energy in the kilowatt range and with pulse duration in the 0.5-1.5 ms range. The pause between pulses is long enough for the handpiece to be moved to a new untreated area so that multiple pulsing to the same site does not occur. Q-switched lasers, such as the Q-switched alexandrite, Q-switched Nd:YAG and Q-switched ruby, emit even shorter pulses, in the 5- to 100-ns range. This is achieved with an elec- tro-optic switch turning polarizers 90 degrees to each other blocking light emission from the optic cavity, then turning them parallel to each other allowing the emission of all the stored light. Thus, the emitted beam has very high peak power, in the megawatt to gigawatt range. The combination of high peak power and short pulse duration allows these lasers to effectively target very small parti- cles like tattoo ink and melanosomes.
Laser light incident onto the skin has 4 possible consequences: absorption, reflection, scattering, and transmission. Absorption and scattering ac- counts for most of the incident light, whereas only 4% to 7% of the light is reflected by the stratum corneum. According to the Grotthus-Draper law of photobiology, absorption of light by tissue is necessary for an effect. Chromophores in the tis- sue are particles or molecules that selectively ab- sorb certain wavelengths of light. Thus a given chromophore has a characteristic absorption spectrum. Chromophores present in the skin in-

DERMATOLOGIC LASER SURGERY
Table 1. Specifications for 532-nm ms-pulsed Green Lasers
109
Laser Loser Type Maximum Fluence J/cm 2 Spot sizes (mm) Repetition Rate Other Features
Versapulse (Coherent) True pulsed in 1-10 msec domain. 0.26-0.38; upper fluence is 2 10 1-6 Hz Chilled tip Domains above 15 to 50 msec capped by software for consist of 3-msec subpulses safety
Aura KTP (Laserscope) Q-switched domain, pulsed, 1-999; maximum fluence 1, 2, and 4 1-10 Hz Smartscan grouped into millisecond pulses at 4 mm = 14 J/cm 2
CB Diode (Continuum Q-switched domain, pulsed, 0.3-240 0.4, 0.8, and 1.2 1, 5, and 10 Scanner available Biomedical) grouped into millisecond pulses Hz (optional)
Diolite (Iriderm) Q-switched domain, pulsed, 0.1-950 0.2, 0.5, 0.7, 1, Single 0.5, 1, Scanner available grouped into millisecond pulses and 1.4 2, 3, and up (optional)
to 15Hz
NOTE. Reproduced with permission from McGraw-Hill Companies. Copyright @ 2000. Dover J, Arndt K, Geronemus R, et al. Illustrated cutaneous laser surgery. 2nd ed. Norwalk (CT): Appleton & Lange; 2000.
clude water, melanin, nucleic acid, protein, oxy- hemoglobin, and deoxyhemoglobin.
Several measurements of the laser light are commonly encountered in clinical practice. En- ergy (joules) is the amount of work. Power (watts = joules/seconds) is the rate at which the work is done. Fluence (joules/cm 2) is the amount of work applied to a unit area. Fluence is also called energy density. Irradiance (watts/cm 2) is the rate of energy applied to a unit area. Irradiance is also known as power density.
In 1983, Anderson and Parrish presented the theory of selective photothermolysis, which marked a new era in laser applications. The theory predicts selective tissue injury if the following 3 conditions are fulfilled. (1) The wavelength of light is preferentially absorbed by the chro- mophore in the target tissue and not the sur- rounding structures. (2) The pulse duration is less than or equal to the thermal relaxation time (Tr) of the target structure. (3) The fluence is greater than or equal to the threshold fluence for tissue destruction. The thermal relaxation time is de- fined as the time required for an object to cool to 50% of the initial temperature reached. Larger structures usually take longer to cool than smaller ones. The concepts of selective photothermolysis have been applied in the making of numerous new lasers with specific tissue effects in mind.
V A S C U L A R LESIONS
Lasers
Treatment of vascular lesions is one of the first applications of medical laser technology that pro- vides the physician with many unique therapeutic options. Before pulsed lasers, continuous and
quasi-continuous wave lasers, such as the argon, argon pumped tunable dye, copper vapor, and krypton, were used. Because of the nonselective nature of the tissue injury by these lasers, it soon became clear that they were associated with rela- tively high incidences of side effects, in particular, scarring and permanent hypopigmentation. Thus, after initial enthusiasm in treating a variety of vas- cular lesions, their use in the more innocent le- sions such as hemangiomas declined rapidly.
The flashlamp pumped pulsed dye laser for vas- cular lesions was the first laser designed in accor- dance with the principles of selective photother- molysis for the purpose of treating vascular lesions. Its initial wavelength of 577 nm was cho- sen to match an oxyhemoglobin absorption peak, then it was increased to 585 nm for deeper skin penetration. Its 0.45-ms pulse duration is shorter than the thermal relaxation time of the cutaneous vessels. After laser treatment, selective damage of blood vessels with coagulated red blood cells, platelets, and fibrin were noted histologically in the papillary and upper reticular dermis, whereas surrounding structures remain uninjured. Be- cause of the specific nature of vessel destruction, lesions that were not eagerly tackled by laser sur- geons before because of unjustifiably high risk-to- benefit ratios are now amendable to safe and effec- tive treatments. More recently, a wavelength of 595 nm along with a 1.5-ms pulse duration is available for even better tissue penetration and uniform heating of the larger, deeper vessels. The VLS (3, 5, 7, 10 mm, 20 J/cm 2) (Cynosure, Chelmsford, Mass) and Candela ScleroPLUS (Candela Corp, Wayland, Mass) 5, 7, 2 • 7 mm, 30 J/cm 2, Wayland, Mass) both have selectable

110 LOU AND GERONEMUS
Table 2. Pulsed 1064 nm Nd:YAG Lasers
Maximum Fluenee Laser Laser Type J/cm 2 Pulse Width Spat Sizes (ram)
Orion (Laserscope) KTP at 532 nm: quasi-CW with 1-300 J/cm 2 1 1o 500 msec 1, 2, and 4 mm
StarPulse Nd:YAG at 1064 nm:
CW with StarPulse Intense pulsed light at 515-1200
nm Nd:YAG at 1064 nm
Nd:YAG at 532 nm, 1064 nm: quasi-CW, Captured Pulse
VascuLight (ESC) 3-90 J/cm 2 0.5 to 25 msec 8 • 35 ram, 8 • 15 mm
40-150 J/cm 2 1 to 14 msec 6 mm
VeinLase (HGM) 100 J/cm 2 0.5 1o 50 msec captured pulse 0.6, 2, and 4 mm
NOTE. Reproduced with permission from McGraw-Hill Companies. Copyright @ 2000. Dover J, Arndt K, Geronemus R, et al. Illustrated cutaneous laser surgery. 2nd ed. Norwalk (CT): Appleton & Lange; 2000.
wavelengths, 585,590, 595,600 nm, and 1.5 ms- pulse duration. In conjunction with cryogen (tet- rafluoroethane) spray from Dynamic Cooling De- vice (DCD) (Candela Carp), higher fluences may be safely applied with these new modifications for more efficacious treatments. The benefits of these alterations to the laser are already seen in the treatment of a variety of vascular lesions, includ- ing capillary vascular malformations, hemangio- mas, leg telangiectases, and hypertrophic scars. The availability of this modified laser is expected to increase significantly.
Recently, a number of other lasers have been developed to target cutaneous vessels. The Nd: YAG lasers emit at 1064 nm, which should reach 5 to 8 mm into the skin and thus have been used primarily for larger and deeper leg telangiectases, including reticular veins (Table 1). Some have even used these lasers for large deep veins of the lower eyelids with variable success usually with- out purpura. The continuous wave Nd:YAG is rarely used today because of its high risk of scar- ring.
Pulsed alexandrite lasers emit at 755 nm, a wavelength well absorbed by hemoglobin and a wavelength long enough to reach substantial depth into the skin. Thus, there have been studies for low extremity telangiectases, which tend to be larger and deeper compared with other body sites. GentleLASE (755 nm, 8-60J/cm 2, 8-15 mm, 3 ms) (Dynamic Cooling Device, Candela) has been shown to be effective in treatment of leg telangi- ectases. Cynosure TKS (755 nm, 50 J/cm 2, 5, 10, 20 ms, 7, 10 mm) (Cynosure, Inc) is another pulsed alexandrite laser in this class.
Frequency-doubled Q-switched Nd:YAG lasers emit green light at 532 •m by passing a Nd:YAG (1064 nm) laser beam through an optical KTP (potassium-titanyl-phosphate) crystal, which
doubles the frequency and halves the wavelength. The resultant wavelength is 532 nm and is near an oxyhemoglobin absorption peak. A number of such long-pulsed 532-nm lasers are available (Ta- ble 2). VersaPulse (Coherent Laser Carp, Palo Alto, Calif) is a dye-pumped KTP laser that has a water-chilled quartz tip. With the high energy long pulsed green (HELP G) function, the laser is capable of pulse durations of 2 to 50 ins. The Aura (Laserscope-Orion, San Jose, Calif), CB Diode/ 532 (Continuum Biomedical, Dublin, Calif), and Diolite 532 (Iriderm, Mountain View, Calif) are different from the VersaPulse in that they emit a pulsed train of grouped Q-switched pulses, yield- ing a net effect likened to 1 to 100 ms pulse dura- tions. These 3 lasers also have optional scanners. The long pulse widths of these lasers allow slower heating of the vessels without resultant vascular rupture and purpura, unlike the pulsed dye laser treatments. There is notable epidermal melanin absorption at this wavelength, epidermaI injury and the risk of pigmentary alternations is ex- pected to be higher than longer wavelength lasers, especially in skin types III and higher. Also, be- cause skin penetration by light of 532 nm wave- length is limited, only superficial lesions are tar- geted. Currently, facial telangiectases and some fine superficial leg telangiectases are effectively treated.
In addition, intense pulsed light source (Photo- Derm, ESC Medical Systems, Ltd, Haifa, Israel) uses a flashlamp to produce a spectrum of light from 515 nm to 1200 nm and fluences up to 90 J/cm 2. Cutoff filters are place to block light below 515 nm to below 695 nm. The noncoherent light may be delivered in single, double, or triple pulses of 2 to 10 ms each with variable delay between pulses. The 8 • 35 mm spot handpiece allows treatment of large areas with relative ease. An-

DERMATOLOGIC LASER SURGERY 111
other advantage of these systems is the lack of purpura when treating vascular lesions. Although the variability in the treatment parameters of this system theoretically allows them to be adjusted ideally for the characteristics of the target lesion, vast experience is necessary to make such adjust- ments in order to maximize efficacy and minimize side effects. This pulsed light source has been shown to treat portwine stains, hemangiomas, and facial and lower extremity telangiectases. How- ever, the comparison to the pulsed dye laser, more treatments may be necessary for the same degree of lesional clearance.
A number of diode lasers, emitting at 800 nm, 900 nm, or 930 nm, are being studied. The longer wavelengths of light allow deeper skin penetra- tion. They are poorly absorbed by hemoglobin and are minimally absorbed by epidermal mela- nin. This situation actually enables delivery of higher fluences to compensate for the poor ab- sorption by hemoglobin with potentially less epi- dermal side effect. The LightSheer 800 nm diode laser (Coherent Star, Pleasanton, Calif) has a vari- able pulse duration of 5 to 30 ms suitable for those large-caliber vessels situated deeper in the skin.
Cl in ica l A p p l i c a t i o n s
Portwine stains are capillary vascular malfor- mations that appear as dilated vessels in the pap- illary dermis. They are present in 0.3% to 0.5% of neonates as pink patches and gradually darken in color. By the fifth decade of life, approximately two-thirds of the affected individuals will have hypertrophy of the lesion and vascular nodules that might bleed. Much has been studied and writ- ten on the medical necessity and psychological benefit of treating these lesions. However, before the new laser era, management of capillary vascu- lar malformations included excision, dermabra- sion, radiation therapy, and cryotherapy, which often left scarring. Continuous and quasi-contin- uous wave lasers were then used frequently, resulting in scarring and pigmentary changes. Compared with today's laser technology, the risk- benefit ratios of those methods are unacceptable. The laser of choice today for capillary vascular malformations is the pulsed dye laser and its newer modified versions. The cryogen spray used in conjunction with the 595 nm, 1.5 ms laser de- creased the healing period and side effects when patients with portwine stains were treated at 10
Fig 1. Capillary vascular malformation in a 1-month-old boy treated with a modified pulsed dye laster (ScleroPlus laser, Candela, Wayland, Mass) at 595 nm, 11 Jlcm% 7 mm spot, with 30 msec of Dynamic Cooling Device cryogen spray and 30 msec delay. (A) Before. (B) Three weeks after 6 treatments at 3-week intervals.
J/cm 2. Overall, this laser appears to be able to effect better clearance and fewer side effects after comparable number treatments with the original pulsed dye laser. Though multiple treatments are necessary to achieve complete clearance or reach an endpoint of improvement, some trends lie in the characteristics of the lesions. For example, head and neck lesions respond more readily than

112 LOU AND GERONEMUS
Fig 2. Nasal te langiectas ia on a white man treated with pulsed dye laser at 6 .25 J / c m =, 7 mm spot. (A) Before. (B) Two months after 2 treatments.
truncal ones, followed by distal extremity lesions. On the face, centrofacial portions of portwine stains in the trigeminal nerve (V2) distribution are more resistant to treatment than those laterally. Finally, lighter lesions in individuals less than 10 years of age with skin types I-III also tend to re- quire fewer treatments. In fact, there are data in support of treatment during infancy because of the better response and the extremely low risk of side effects with today's technology. Other lasers including VersaPulse (Coherent Laser Corp) and VascuLight (ESC Medical Tech) are being studied for capillary vascular malformations. Despite all that has been written on the medical, social, and psychological detriment on leaving these lesions untreated and despite the relative ease of effective treatment, a surprisingly large portion of today's managed care organizations deny, unethically in our opinion, insurance coverage for treatment.
Hemangiomas are a common vascular lesion in infancy present in 10% of newborns with fre- quency 3 times higher in girls than in boys. After a rapid proliferation period during the first year of life, hemangiomas undergo involution over the next 5 to 10 years. Because an estimated 60% of the lesions occur on the head and neck regions,
there is obvious social and psychological advan- tage in early resolution of these lesions, especially before formal schooling. Although laser therapy is most effective in thin superficial lesions, early treatment of thicker lesions can limit the size of the hemangioma to some extent as well as control ulceration and bleeding. Although monthly to bi- monthly treatment intervals are recommended for regressing hemangiomas, actively proliferating le- sions should be treated every 2 to 3 weeks. The same lasers, the pulsed dye laser and its newer versions, are effective in treating hemangiomas with extremely low risk-to-benefit ratio.
Before the advent of the vascular-specific pulsed dye laser, treatment of facial telangiectases with continuous wave and quasi-continuous wave lasers, even with robotized scanners, had unac- ceptably high risks and thus was rarely used for this purpose. The pulsed dye laser effectively pho- tocoagulated facial telangiectases with the pri- mary side effect of resultant purpura lasting 7 to 10 days after treatment. In one study, good to excellent responses were noted in 97.5% of pa- tients after 1 to 3 treatments with the 585 nm, 450 ms pulsed dye laser at 6-7.75 J/cm 2 and 5 mm spot. Smaller red vessels seemed to have re-

DERMATOLOGIC LASER SURGERY 113
Fig 3. Nevus of Ota on a 6-year-old Asian girl t reated with the Q-switched ruby laser at 4-5 J / c m 2, 6.5 mm spot. (A) Before. (B) Six months after 5 treatments at 8-week intervals.
sponded better than the larger blue ones. The 595 nm, 1.5 ms laser with DCD appears to be more effective on those larger deeper facial vessels. A 2 • 7 m m elliptical spot more closely approxi- mates the configuration of the vessels, and DCD providing cryogen spray offers epidermal protec- tion and decreased patient discomfort. Another group of systems all with millisecond pulse dura- tion can treat facial telangiectases with minimal side effects and without residual purpura: KTP (532 nm) green light lasers, Nd:YAG (1064 nm) laser, and intense pulsed light source as described above. As may be expected from the wavelength, the superficial fine vessels respond well to the 532 nm lasers, whereas the deeper, large-calibered, blue infraorbital vessels are better targeted by the 1064 nm laser.
Regarding the treatment of leg veins, although sclerotherapy has long been the gold standard, its disadvantages include high-technique depen- dence, matting, ulceration, and possible patient allergy to sclerosant. An increasing number of la- sers are being explored and used for the treatment of leg veins. Treatment of leg veins presents a challenge because there is an even wider range of
size and depth of the vessels than on the face. In addition, elevated hydrostatic pressures of the lower extremity and thicker vessel wall often ad- versely affect treatment results. Because of these characteristics, longer wavelength, longer pulse duration, and higher fluence, as well as means of epidermal cooling, are important. Thus, the mod- ifications of longer wavelength (585-600 nm), longer pulse width (i.5 ms), and DCD cryogen spray have advantages over the 585 nm, 450 ms pulsed dye laser. Studies have shown clearance rates as high as 75% at sites treated thrice at 15 to 20 J/cm 2 with a 2 • 7 mm elliptical beam. Post- treatment purpura resolved in 7 to I0 days, and the 20% to 30% incidence of hyperpigmentation all resolved within 3 months. Clearances of 100% after 1 to 2 treatments of vessels <0.5 mm and 80% after up to 4 treatments of vessels 0.5 to 1.0 m m were seen in another study. The 532 nm KTP green light lasers target small superficial vessels. In general, greater than 50% clearance has been reported in 80% to 90% of the sites treated 2 to 4 times at 9.5-16 J/cm 2 and 10 to 20 ms. Transient pigmentary alterations are seen in up to 36% of the sites. Long pulsed alexandrite lasers are being ex-

114 LOU AND GERONEMUS
Table 3. Q-switched Pigment Lasers
Wavelength Pulse Pulse rate Maximum Fluenees Laser Type Manufacturer (rim) Duration (Hz) Spot Sizes (mm) (J/cm 2)
Spectrum RD-1200 QS ruby Spectrum (Palomar) 694.3 28 nsec 0.8 5, 6.5 3-10
Alexlazr QS alexandrite Oandela 758 50 nsec 5 2, 3, 4 3-12 PhotoGeniea-T QS arexandrile Cynosure 752 1 O0 nsec Single-10 2.4 10
Vesapulse VPC FD Nd:YAG Coherent 532 2-50 msec Single-6 2-10 0.26-38 QS FD Nd:YAG 532 4 nsec Single-lO 2-6 0.36-6
QS Nd:YAG 1064 5 nsec Single-lO 2-6 0.75-12
QS alexandrite 755 45 nsec Singled 0 2-6 0.85-12
Medlite IV QS FD, QS Nd:YAG Continuum Biomedical 532, 1064 5-7 nsec 1, 2, 5, 10 532 nm: 2, 3, 4, 6 532 nm: 5 at 3 mm 1064 nm: 3, 4, 6, 8 1064 rim: 6 at 4 mm
NOTE. FD, Frequency-doubled; QS, Q-switched. Reproduced with permission from McGraw-Hill Companies. Copyright @ 2000. Dover J, Arndt K, Geronemus R, el al. Illustrated Cutaneous Laser Surgery.
2rid ed. Norwalk (CT): Appleton & Lange; 2000.
plored for deep large-caliber leg veins. In one study, 20 adult subjects with 54 patches of leg veins up to 2 m m in diameter were treated once at 60 or 80 J/cm 2 with 70-100 ms DCD cryogen (tet- rafluoroethane) spray and 3 ms delay (Gentle- LASE). At 3-month follow-up evaluation, 65% of the sites had greater than 75% clearance and 87% had greater than 50%. Thirty-six percent of the sites had mild or moderate hyperpigmentation at 3 months. Diode lasers emitting at 800 to 810 nm offer good skin penetration and are close to the hemoglobin absorption peak of 915 nm. When an 800 nm pulsed diode laser (LightSheer) was used for leg veins up to 1 mm, 25% cleared after 1 treatment, 50% after 2 treatments, and 75% after 3 treatments. Better clearance was noted with larger vessels. The long pulsed Nd:YAG laser emitting at 1064 nm offers even deeper penetration. With fluences 80-130J/cm 2 at single, double, and triple i0 to 16 ms synchronized pulses, 75% improve- ment was reported 3 months after a single treat- ment of vessels 0.5-3 mm. Lastly, PhotoDerm, an intensed pulsed light source, offers another treat- ment option for leg veins. Wavelength spectrum and pulsed duration may be selected to match the characteristics of the target vessel. In a multi- center trial, 369 sites with up to 3 mm diametered vessels in 159 subjects were treated up to 5 times. Greater than 75% clearance was seen in 79% of the sites, and greater than 50% clearance in 90% of the sites. Unlike treatments with the pulsed dye laser where purpura is a predictable consequence, rup- ture of vessel and purpura is only occasional with these latter systems.
Other common vascular lesions amendable to laser treatment include spider angiomas, rosacea-
associated telangiectases and erythema, and ve- nous lakes. For poikiloderma of Civatte in partic- ular, multiple treatments with the pulsed dye laser at low fluences and large spot size have proved to be optimal. Even hypertrophic scars and psoriatic plaques appear to improve with pulsed dye laser treatments.
The new trends in the treatment of vascular lesions include longer pulse durations, coupled cooling devices, and in some cases, longer wave- lengths. The longer pulse widths in the millisec- ond domain allow more uniform heating of the blood vessels, and thus are less likely to result in vascular rupture and in purpura. Because epider- mal protection has been associated with decreased side effects, a variety of cooling devices are now recommended with the use of the various lasers by either precooling the skin before laser irradiation or simultaneous cooling during the laser proce- dure itself. The Dynamic Cooling Device uses a cryogen (tetrafluoroethane) spray immediately before each laser pulse, as with the GentleLASE long pulsed alexandrite laser and ScleroPLUS la- ser. The laser beam from the VersaPulse (Coher- ent Laser Corp) traverses through a water-cooled quartz plate on the handpiece that comes in con- tact with the epidermis. Cooling gel provides epi- dermal protection and decrease light reflectance from the stratum corneum in the systems such as the Vasculight and Aura. For those deeper, bigger vessels, lasers with longer wavelengths are also being developed for better skin penetration. This category includes the long pulsed alexandrite la- sers, long pulsed Nd:YAG, and modified pulsed dye laser with selectable wavelengths of 585 nm, 590 nm, 595 nm, and 560 nm.

DERMATOLOGIC LASER SURGERY 115
Fig 4. Green and black professional tattoo on a white man treated with Q-switched ruby laser at 8.5 J /cm 2, 5 mm spot. (A) Before. (B) After 3 treatments. (C) After 8 treatments.
REMOVAL OF BENIGN PIGMENTED LESIONS AND TATTOOS
Treatment of benign pigmented lesions and tat- toos depends on melanin and exogenously origi- nated tattoo inks, respectively, as the target chro- mophores. The target structures are melanosome and tattoo pigment containing membrane-bound intracellular granules. Benign pigmented lesions may be a result of increased melanocytes or in- creased melanogenesis in the epidermis, dermis, or both. Examples of increased melanogenesis in- clude ephelides, Becket's nevi, and melasma. Nevi of junctional, intradermal, or compound type, ei- ther congenital or acquired, are lesions with in- creased melanocytes. Tattoos, on the other hand, result from exogenously induced ink, organome- tallic dyes, dirt, or asphalt that are bound in intra- cellular granules of dermal macrophages or fibro- blasts.
Benign P i g m e n t e d Lesions
Traditionally, epidermal pigmented lesions, such as cafe-au-lait macules, ephelides, and len-
tigines, have been tackled by cryotherapy and acid peels such as with trichloracetic acid, alpha-hy- droxy acids, and beta-hydroxy acids with variable success (Table 3). Dermabrasion has been com- monly used for epidermal pigment, and surgical excision commonly for dermal pigment. Resurfac- ing lasers, such as carbon dioxide and erbium: YAG lasers, which are nonselective for melanin have also been used. Dermal pigmented lesions such as nevus of Ota are less responsive to the above treatments and frequently resort to camou- flaging cosmetic tattooing. Lasers that are selec- tive for melanin are the most popular for pig- mented lesions of epidermal, dermal, or combined nature.
In 1963, Goldman et al were the first to exper- iment with 694 nm ruby lasers, both 500/xs nor- mal mode and Q-switched, demonstrated more intense effect on darker-colored skin. Those stud- ies showed melanin as the target chromophore and melanosomes as the target structure. How- ever, it was not until the 1980s that electron mi- croscopy studies confirmed that melanosomes are

116 LOU AND GERONEMUS
actually disrupted after Q-switched laser irradia- tion. These further investigations showed 40 to 750 ns as the necessary pulsed duration for mela- nosome disruption.
The Q-switched ruby laser has as the active medium the ruby crystal made from aluminum oxide and chromium. At the wavelength of 694 nm and pulse duration of 20 to 40 ns, it is capable of high peak powers (10J/cm2). A beam of 694 nm is well absorbed by melanin and by blue-black tattoo ink, and it penetrates approximately 1 mm into the skin permitting effect on both epidermal and dermal pigments. Lentigines, including labial lentigos, usually clear completely after a single treatment. Caf~ au lait macules, Becker's nevi, and nevus spilus usually lighten after a series of treat- ment, but frequently recur in the ensuing months to years. Dermal pigmented lesions such as nevus of Ito and Ota respond well to Q-switched ruby laser treatment, but numerous treatments are nec- essary. Interestingly, minocycline-induced cuta- neous hyperpigmentation, as a result of granules with staining properties similar to melanin and/or hemosiderin, has been successfully treated with Q-switched ruby laser.
The Q-switched alexandrite laser emits 100 ns pulses of 755 nm light, which is close to that of the ruby laser. It has been shown to effectively lighten epidermal and dermal lesions.
The Q-switched Nd:YAG laser emits 10 to 20 ns pulsed either at 1064 nm or at 532 nm when the frequency-doubling KTP crystals are applied. De- spite the relatively poor absorption of 1064 nm light by melanin, its ability to penetrate deeply into the skin offers enough of an advantage for it to be useful. Dermal pigmented lesions, such as nevus of Ito and Ota respond well to this treat- ment. The competitive absorption of the 532 nm light by both melanin and hemoglobin places lim- itations on its use in pigmented lesions and tends to increase its potential risk of side effects. In one study using fluences of 2 to 5 J/cm 2, 84% of len- tigines showed at least 50% lightening after sev- eral treatments. Care au lait macules, Becket's nevi, and nevus spilus tend to recur months after treatment as they do after treatments with other lasers.
The 510 nm flashlamp pumped pulsed-dye la- ser emitting 300 ns pulses was designed for epi- dermal pigments for which considerable success has been shown.
Conditions such as postinflammatory hyper- pigmentation and melasma should be approached with extreme caution as they may worsen. Melasma especially have a high recurrence rate. Minimal intervals between multiple treatments of pigmented lesions are usually 6 to 8 weeks.
Congenital nevi may be lightened with red or infrared light lasers such as the long-pulsed ruby laser used alone or in conjunction with Q-switched lasers. In general, lightening of the lesions is achievable, but recurrences may occur since not all of the melanocytic cells are destroyed. With the long-pulsed red light lasers, fibrosis in the papillary dermis may sometimes obscure the persistent dermal nevus cells providing the clini- cal picture of clearing.
Tattoo Remova l
Before laser, methods of tattoo removal were limited to dermabrasion, salabrasion, and surgical excision, which usually resulted in scarring. Suc- cessful laser tattoo removal was reported as early as 1964 by Goldman et al. However, the technique did not assume popular application until work done by Scottish scientists in the 1980s showing removal of blue-black tattoos without permanent epidermal damage.
Tattoo removal by lasers is probable via a num- ber of mechanisms (Table 3). The high tempera- ture achieved from the laser pulse causes chemical alteration and fragmentation of the tattoo pig- ments. The shattered particles then undergo re- packaging by local macrophages, transportation to regional lymph nodes, and elimination trans- epidermally.
Response of tattoos to laser treatments in gen- eral depends on the particular type and color of the ink and how and when it was placed into the skin. Amateur tattoos, usually containing smaller carbon-based particles, require fewer laser treat- ments for clearance than multicolored profes- sional ones with densely arranged organometallic dyes. Studies with a 25 ns Q-switched ruby laser showed that 85% of amateur tattoos were com- pletely removed in an average of 3 treatments and that 10%, 70%, and 20% of professional tattoos were completely, partially, and minimally cleared, respectively, after an average of 6 treatments.
The Q-switched lasers, ruby (694 nm), alexan- drite (755 nm), and Nd:YAG (1064 nm), are nearly comparable in their abilities to remove
DERMATOLOGIC LASER SURGERY
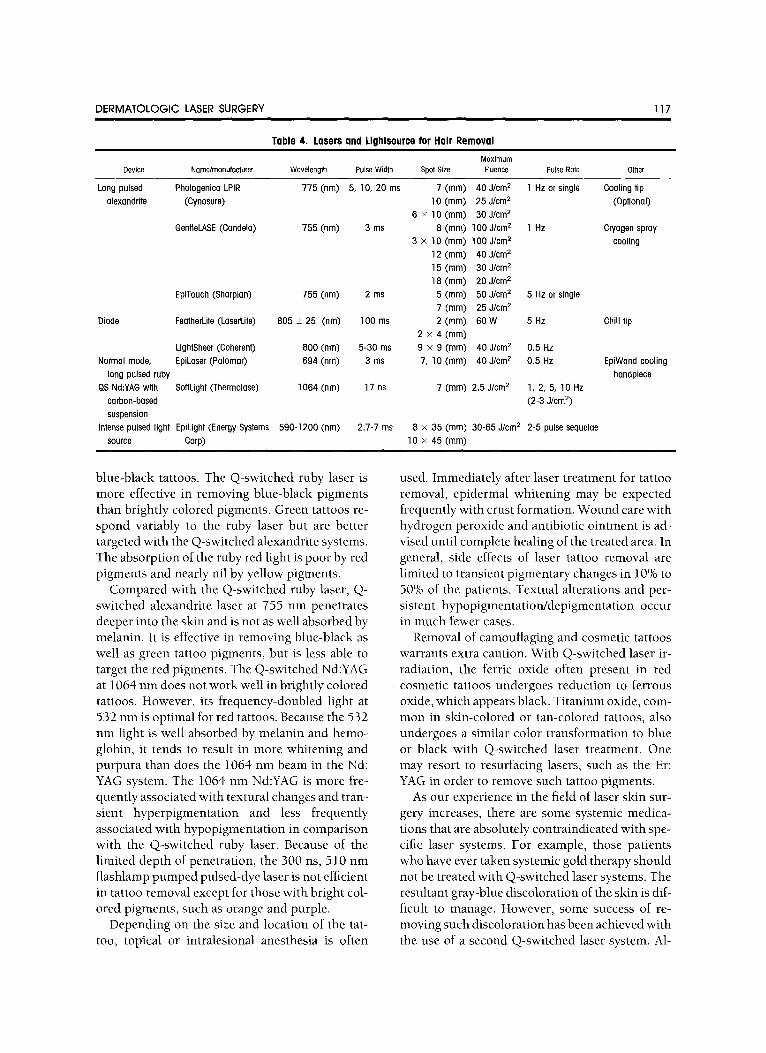
Table 4. Lasers and Lightsource for Hair Removal
117
Maximum Device Name/manufacturer Wavelength Pulse Width Spol Size Fluence Pulse Rate Olher
Long pulsed Photogeniea LPIR 775 (nm) 5, 10, 20 ms 7 (ram) 40 J/crn 2 1 Hz or single Cooling tip alexanddte (Cynosure) 10 (ram) 25 J/cm 2 (Optional)
6 x lO(mm) 30J/cm 2
GentleLASE (Condela) 755 (nm) 3 ms 8 (mm) 100 J/cm 2 1 Hz Cryogen spray 3 X 10 (ram) 100 J/cm 2 cooling
12(ram) 40J/cm 2 15(mm) 30J/cm 2
18 (ram) 20 J/crn 2
EpiTouch (Sharplan) 755 (nm) 2 ms 5 (ram) 50 J/cm 2 5 Hz or single 7 (ram) 25 J/cm 2
Diode FeatherLite (LaserLite) 805 + 25 (nm) 100 ms 2 (ram) 60 W 5 Hz Chill tip 2 x 4 (mm)
LightSheer (Coherent) 600 (nm) 5-30 ms 9 x 9 (mm) 40 J/cm 2 0.5 Hz
Normal mode, EpiLaser (Palomar) 694 (rim) 3 ms 7, 10 (ram) 40 J/cm 2 0.5 Hz EpiWand cooling long pulsed ruby handpiece
QS Nd:YAG with SoflLight (Thermolase) 1064 (nm) 17 ns 7 (mm) 2.5 J/cm 2 1, 2, 5, 10 Hz
carbon-based (2-3 J/cm 2)
suspension Intense pulsed light EpiLight (Energy Systems 590-1200 (rim)
source Carp) 2.7-7 ms 8 • 35 (ram) 30-65 J/cm 2 2-5 pulse sequelae
10 x 45 (ram)
blue-black tattoos. The Q-switched ruby laser is more effective in removing blue-black pigments than brightly colored pigments. Green tattoos re- spond variably to the ruby laser but are better targeted with the Q-switched alexandrite systems. The absorption of the ruby red light is poor by red pigments and nearly nil by yellow pigments.
Compared with the Q-switched ruby laser, Q- switched alexandrite laser at 755 nm penetrates deeper into the skin and is not as well absorbed by melanin. It is effective in removing blue-black as well as green tattoo pigments, but is less able to target the red pigments. The Q-switched Nd:YAG at 1064 nm does not work well in brightly colored tattoos. However, its frequency-doubled light at 532 nm is optimal for red tattoos. Because the 532 nm light is well absorbed by melanin and hemo- globin, it tends to result in more whitening and purpura than does the 1064 nm beam in the Nd: YAG system. The 1064 nm Nd:YAG is more fre- quently associated with textural changes and tran- sient hyperpigmentation and less frequently associated with hypopigmentation in comparison with the Q-switched ruby laser. Because of the limited depth of penetration, the 300 ns, 510 nm flashlamp pumped pulsed-dye laser is not efficient in tattoo removal except for those with bright col- ored pigments, such as orange and purple.
Depending on the size and location of the tat- too, topical or intralesional anesthesia is often
used. Immediately after laser treatment for tattoo removal, epidermal whitening may be expected frequently with crust formation. Wound care with hydrogen peroxide and antibiotic ointment is ad- vised until complete healing of the treated area. In general, side effects of laser tattoo removal are limited to transient pigmentary changes in 10% to 50% of the patients. Textual alterations and per- sistent hypopigmentation/depigmentation occur in much fewer cases.
Removal of camouflaging and cosmetic tattoos warrants extra caution. With Q-switched laser ir- radiation, the ferric oxide often present in red cosmetic tattoos undergoes reduction to ferrous oxide, which appears black. Titanium oxide, com- mon in skin-colored or tan-colored tattoos, also undergoes a similar color transformation to blue or black with Q-switched laser treatment. One may resort to resurfacing lasers, such as the Er: YAG in order to remove such tattoo pigments.
As our experience in the field of laser skin sur- gery increases, there are some systemic medica- tions that are absolutely contraindicated with spe- cific laser systems. For example, those patients who have ever taken systemic gold therapy should n o t be treated with Q-switched laser systems. The resultant gray-blue discoloration of the skin is dif- ficult to manage. However, some success of re- moving such discoloration has been achieved with the use of a second Q-switched laser system. A1-

118 LOU AND GERONEMUS
Fig 5. Unwanted hair in abdominal area treated with a long-pulsed ruby laser (EpiLaser, Palomar, Lexington, Mass) at 694 nm, 3 msec, 7 mm, 35 J l c m =. (A) Before. (B) Three months after 3 treatments at 6-week intervals. Courtesy of Arielle N. B. Kauvar, MD.
though the half-life of isotretinoin and its metab- olites is relatively short, its cutaneous effect, in particular its hinderance to normal wound heal- ing, may last months. Thus it is recommended that laser treatments, especially those that disrupt the epidermal integrity, be postponed for at least 1 year after the last isotretinoin dose.
Tattoo removal continues to be an area yearn- ing for advancement. Tackling some of the more resistant colors, such as yellow, in tattoos and clearing the residual faint pigmentation have al- ways been challenging. Decreasing the number of treatments necessary is also highly desired. These difficulties have in part been overcome by recent work done with carbon-based lotion used in con- junction with Q-switched Nd:YAG at 1064 nm. Normally, the epidermal whitening and crust for- mation prevent tissue effect from a second laser pass immediately after the first. However, if after the traditional first pass of a Q-switched laser, a carbon-based lotion is applied on the treated skin surface followed by Q-switched Nd:YAG (1064 nm) irradiation, an additive photoacoustic effect is believed to take place. Clinically, this protocol
appears to achieve faster clearing than without a traditional second pass or without the carbon- based lotion. Better clearing is also seen with those more resistant bright-colored pigments.
HAIR REMOVAL
Hair reduction is one of the newest areas of laser application. Although it is a valuable tool in the management of various medically related condi- tions of excess hair or hirsutism, the current in- terest in laser hair reduction is also fueled by pub- lic interest. Because of our culture and life style, excess hair, except on the scalp, often seems to be an undesirable trait, as evidenced by the numer- ous methods of hair removal including shaving, waxing, tweezing, and electrolysis. Finally, laser holds the promise of long-term hair reduction with minimal side effects.
Laser hair removal is based on the theory of selective photothermolysis, with follicular mela- nin as the natural target chromophore. Within the hair follicles, melanin is present in the hair shaft, bulb, and follicular epithelium. For individuals with light hairs containing little melanin, exog-

DERMATOLOGIC LASER SURGERY 119
Fig 6. Facial rhytides in a 70-year-old woman treated with a carbon dioxide laser (Ultrapulse, Coherent, Santa Clara, Cali f ) at 300 m J, 60 watts, and density of 6. (A) Before. (B) Six months after treatment.
enously applied carbon is used as the chro- mophore with a certain laser system. Red and infrared lights (600-1100 nm) are the best wave- lengths to provide the desired combination of se- lective absorption by melanin and deep penetra- tion into the dermis. Another parameter of critical concern in selective follicular injury is the pulse duration. For hair follicles with average diameters of 200 to 300/xm, the thermal relaxation time is estimated to be 40 to 100 ms. Thus, to minimize epidermal injury, the optimal pulse duration of a hair removal laser should be less than 40 to 100 ms and greater than the thermal relaxation time of the epidermis, which is about 3 ms.
Several systems are available today for hair re- moval (Table 4). The long-pulsed ruby, long- pulsed alexandrite, and the diode lasers all use melanin within the hair follicle as the chro- mophore for selective thermal injury. Different Q-switched Nd:YAG lasers have been used for hair reduction with or without an application of exog- enous carbon. Non-laser intense pulsed light sources can also target melanin and are used for the same purpose. Many of these systems incorpo- rate a cooling handpiece, cooling gel, or cryogen spray in an attempt to protect the epidermis from
thermal injury, thus allowing higher fluences to be applied safely.
The long-pulse ruby lasers emit at a wavelength of 694 nm and include EpiLaser (Palomar, Lex- ington, Mass) and EpiTouch Ruby (ESC/Sharplan Medical Systems, Needham, Mass). After a single treatment of 13 fair-skinned, dark-haired subjects in one study using a long-pulsed ruby laser (694 nm, 3 ms, 7, 10 mm, 10-40 J/cm 2, EpiLaser), all had hair-growth delays lasting 3 to 6 months com- pared with wax epilated or shaved control sites. The amount of hair reduction appeared to be en- ergy-dependent. In only 4 of these 13 subjects, less than 50% regrowth of terminal hairs were observed at 2-year follow-up. Hair counts in these 4 are similar at 6-month, 1-year, and 2-year fol- low-ups, implying the persistence of these changes in some individuals. Histologic examina- tion revealed a decrease in large terminal hairs and a reciprocal increase in miniaturized, vellus-like hair follicles in these subjects. One study that used a different ruby laser (694 nm, 800/xs, 4-5 mm, 10-40 J/cm 2, EpiTouch) reported 40% to 80% re- growth of arm hair 12 weeks after a single treat- ment. Further studies have shown improved effi- cacy with larger spot size, 10 mm, compared with

120 LOU AND GERONEMUS
7 mm. In addition, cooling of the epidermis de- creases incidence of side effects.
The long-pulse alexandrite lasers emitting at 755 nm have similar mechanisms of action as the long-pulsed ruby laser. EpiTouch Alex (ESC/ Sharplan Medical Systems), GentleLASE (Candela Laser Corp), and Photogenica LPIR (Cynosure, Inc) are currently available. In 1 study of 126 patients treated up to 5 times with a long-pulsed alexandrite laser (755 nm, 2 ms, 5-7 mm, up to 50 J/cm 2, EpiTouch), 90% hair reduction was found at 3 months after the last treatment. A comparison study of the long-pulse alexandrite and long-pulse ruby laser showed similar efficacy and side effect profiles. Similar to the ruby laser, larger spot size, 10 mm, appears to be more effective than 7 mm spot size, and higher fluences resulted in greater hair reduction. An analysis of 392 patients treated with a long-pulsed alexandrite laser (755 nm, 5, 10, 20 ms, 7, 10, 6 • 10 mm, up to 40 J/cm 2, Photogenica LPIR) showed a higher incidence of erosions in the 62 patients with darker or black skin. A study of 14 subjects of skin type IV and V was conducted by using a long-pulsed alexandrite laser (GentleLASE) at 8-20 J/cm 2, 3 ms, 15 mm, 100 ms DCD with 3 ms delay. After a short period of hair growth delay after a single treatment ses- sion, regrowths at the treatment sites were com- parable with the control sites by 3-month fol- low-up evaluation.
Diode lasers emitting at 800 nm include Feath- erLite (LaserLite, Boston, Mass) and LightSheer (Coherent-Star, Pleasanton, Calif). When 58 sub- jects of skin types II and lli were treated with a diode laser (800 nm, 5-30 ms, 9 • 9 mm, up to 40 J/cm 2, LightSheer) once or twice at l -month inter- vals, approximately 90% of the dark-haired sub- jects and 30% of the blonde-haired subjects showed hair growth delays. Higher fluences and multiple treatments were associated with greater amount of hair loss. Both the reduction in hair diameters and lightening of hair color reached statistical significance. Long-term hair regrowth data at an average follow-up of 20 months after treatment are available from a prospective fol- low-up of 20 out of 50 original subjects treated with a diode laser (LightSheer). Regrowth was 22% to 31% at 1 month after a single treatment and stabilized between 65% to 75% at 3 months to 20 months. Longer growth delays were seen after 2 treatments at a 1-month interval, with regrowth
plateau starting at 6 months and ranging 47% to 66%. Transient pigmentary changes were limited in those with skin types II and III.
Q-switched Nd:YAG lasers emitting at 1064 nm have been used with (SoftLight, Thermolase Corp, Carrollton, Tex) and without (MedLite IV, Con- tinuum Biomedical) exogenous carbon. In the SoftLight system, carbon is physically introduced into the hair follicles by rubbing a carbon-based lotion onto the skin and wiping it off the skin surface immediately before laser irradiation. The microparticulate carbon is propelled down the hair shaft and generates photoacoustic waves when low-energy laser light is absorbed. This re- suits in a photomechanical disruption of the hair follicle. Because follicular melanin is not the target chromophore, blonde and red-haired patients may be effectively treated by this method. In ad- dition, because the absorption of 1064 nm light by epidermal melanin is minimal, this system may be used more safely in darker skin-typed patients. Growth delays have been reported for up to 3 months after a single treatment. However, al- though better than wax-epilation, which yield hair regrowth at 1-month follow-up, hair re- growth is seen at 6 month after a single SoftLight treatment. Permanent hair loss has not been ob- tained even with multiple treatments. The Q-switched Nd:YAG laser in the nanosecond pulse range appears to cause reversible photome- chanical disruption of the follicle, but not photo- thermal injup/seen with millisecond-range lasers.
Intense pulsed light source, such as the Epi- Light (ESC Medical Systems) is a non-laser system also used for hair removal. Rather than emitting a specific wavelength of light as by a laser, it emits light with wavelengths ranging from 540 to 1200 nm. The characteristics of the emitted energy can be tailored to patients with different hair and skin color combinations by means of different cut-off filters adjusting the quality of light and variable pulse widths. In one study, 60% hair reduction was reported 12 weeks after a single treatment with various cut-off filters (34-44 J/cm 2, 2-5 pulses, 1.5-3.5 ms, 20-50 ms delays). Adverse ef- fects included posttreatment erythema in 7%, hy- perpigmentation in 3%, and blistering in 11%. Other investigators have reported similar data.
Most of the laser and light source systems today use some form of epidermal cooling technique for epidermal protection and patient comfort. The

D E R M A T O L O G I C LASER SURGERY
Table 5. High Peak Power C02 Lasers, Flashsconners, and Er:YAG Lasers
121
Er:YAG Laser Coherent UltroPulse Tissue Technology TruPulse Sharplan SilkLaser (various manufacturers)
Laser lype 100 watt C02 6 W C02 20-150 W C02 Wavelength 10.6 tLm 10.6 t~m 10.6 >m Delivery Method Individual Gaussian Individual square pulses Spiral (SilkTouch, FeatherTouch) or
pulses rasterized (SureTouch) scan with focused beam
Power 500 W peak power, 10,0O0 W peak power, 7-]00 W average power, CW beam pulsed pulsed
Pulse duration 650-950 tLS 60-100 tLS 0.03-0.52 S scan duration; 300- 1000 ,u,s tissue dwell time
Energy N/A CW laser
Er:YAG 2.94 t~m Individual pulses
Effect of increasing Increases rate of pulsing Increases rate of pulsing power
10-20 W average power
250-350/~s
O. 1-3 J/pulse Adjustable 50-500 m J/pulse 10-500 m J/pulse Adjustable by adjustable by changing pulse width changing peak power
Energy fluence 5-7 J/cm 2 5-7 J/cm 2 5-15 Jlam 2 or more 1-60 J/era 2 Spot size 3 mm collimated; 2.25- 1 and 3 mm 6.9 mm 0.6-15-mm scan size with 0.1-0.25- 2-8 mm collimated or focused;
mm spot CPG spatula mm focused beam paltern generator Spot Shape Round spot; various Square spot Round, square, elliptical, or doughnut Round; various with CPG
with CPG scan (SilkTouch, FeatherTouch); various (SureTouch)
Increases thickness of tissue removed with each scan
Increases rate of pulsing (1-20 Hz)
NOTE. CPG, Computer paltern generator. Reproduced with permission from: Dover J, Arndt K, Geronemus R, et al. Illustrated Cutaneous Laser Surgery, 2nd ed. Norwalk (CT): Appleton & Lange; 2000.
various methods of epidermal cooling include ap- plication of ice or cooling gel, glass chamber, dy- namic cooling device with cryogen spray (tetraflu- oroethane [HFC 134-], boiling point = -26.2~ and contact cooling via a chilled sapphire and quartz tip. Because the epidermis contains mela- nin, the target chromophore, epidermal injury may occur with treatments. Cooling of the epider- mis will minimize this risk and also allow the use of fluences higher than would be safe without epidermal cooling. This concept is especially im- portant in the treatment of individuals with darker skin types or with a tan because the com- peting epidermal melanin is the main reason for the higher incidence of side effects in this popula- tion.
Most of the hair reduction treatments have been in individuals of skin types I-Ill. Thus, the side effects are minimal and largely transient. Mild er- ythema and perifollicular edema are expected and desired immediately after laser treatment for hair removal, although erythema and crusting may be present for a few days. Pigmentary changes may be seen and usually resolve in several months. Blis- tering is uncommon and normally heals without any lasting sequelae. In the hands of the experi- enced physicians or with conservative treatment
parameters, scarring is an extremely rare occur- rence.
Treatment of individuals with tanned skin or with skin types IV-VI is complicated by the abun- dance of competing epidermal melanin leading to a much higher risk of pigmentary alterations and epidermal damage. Although the incidences of pigmentary changes may be decreased by the pre- treatment and posttreatment use of bleaching agents and strict sun avoidance, it is still a signif- icant problem. Because of the side effect profile, these individuals are often treated at low fluences, thus resulting in less hair reduction for a shorter period of time compared with the non-tanned, skin types I-III counterparts. Nevertheless, laser treatments at the restricted parameters have been shown to dramatically improve conditions such as pseudo folliculitis, highly prevalent in this popu- lation. Thus, despite the challenges, researchers are actively attempting to develop systems and define parameters for safer and more effective long-term hair reduction for darker skin typed individuals.
Traditionally, it was believed that the matrix area of the hair bulb is solely responsible for fol- licular regeneration. It followed that there must be irreversible destruction of those stem cells for per-

122
manent hair reduction. Along this logic, laser sci- entists believe that follicles are most vulnerable to injury by various lasers or light sources during the anagen phase when melanin chromophore is more abundant near those stem cells in the deep dermis. Because the duration of the hair cycle dif- fers for different body sites, repeat treatments are usually done when there is a wave of rapid hair regrowth or between 4 and 8 weeks. However, according to the recent bulge-activation hypothe- sis, the bulge area of the outer root sheath near the arrector pili muscle insertion contains pluripoten- tial cells, which contributes to the new hair matrix when induced by the dermal papillae during late telogen. Thus, injury to stem cells in the bulge area would lead to follicular destruction. Because the location of the bulge does not change during the follicular cycle, perhaps the anagen phase would not be a prerequisite for laser effect on hair growth. Although some recent clinical data show additive hair reduction from repeat treatments within several days to a couple of weeks of the previous treatment session, the mechanism re- mains to be elucidated. Perhaps nonanagen hairs were affected. Or alternatively, telogen hairs were induced to start anagen by the first treatment, and the subsequent treatment session affected these hairs that newly began anagen.
As we better understand laser and follicular in- teraction, a true optimal treatment interval, if there is such, will be derived. In addition, faster treatments with larger spot sizes and/or rapid rep- etition rate may be anticipated in the coming years. With the refinement of epidermal cooling systems, perhaps treatment of darker and tanned skin will become safer with improved efficacy. Our data on laser hair reduction are limited by the short duration for which this technology has been available. Currently, permanent hair reduction is defined as a significant reduction in the number of terminal hairs that remain stable for a period longer than the complete growth cycle of follicles at a given anatomic site. More long-term results after multiple treatments will truly define the phrase permanent hair reduction.
RESURFACING
The main goal of facial rejuvenation is to even the skin texture and pigmentation. Since the dawn of time, mud packs, fruit extracts, and mechanical exfoliants have been used for these purposes.
LOU A N D GERONEMUS
Table 6. Indications tar Carbon Dioxide Lasers
Aclnic cheilitis Actinic keratoses Adenoma sebaceum DermatosJs papulosa nigra Epidermal nevi Er,/throplasia at Quyerat Facial rhytides Facial scars, including acne, traumatic, varicella Rhinophyma Sebaceous hyperplasia
More recent procedures and better-refined prod- ucts include creams and peels with hydroxy acids and vitamin A derivatives. These remain relatively limited in their ability to provide dramatic im- provements. Even though phenol peels and dermabrasions are more effective in improving rhytides, they have largely been replaced by re- surfacing lasers.
Laser application in dermatology has been based on the theory of selective photothermolysis. For the 10,600 nm light emitted by a carbon diox- ide laser, water is the chromophore in skin. Un- fortunately, the continuous-wave carbon dioxide lasers used for skin resurfacing in the 1980s and early 1990s carried a relatively high risk of scar- ring because of significant thermal diffusion. Al- though laser light penetrates only about 30/xm, its thermal effect reaches about 1 mm because of heat diffusion. The thermal relaxation time of the 30 /xm layer is less than 1 ms. The new short-pulsed, high peak power, rapidly scanned, focused-beam CO 2 lasers with less than 1 ms pulse width are able to provide precise control over the amount of tis- sue ablation and thermal damage. The high-en- ergy pulsed carbon dioxide and scanned carbon dioxide lasers along with the new Er:YAG lasers will be discussed (Table 5).
A high-energy pulsed carbon dioxide laser is Ultra-Pulse laser (Coherent Laser Carp). It has been shown that about 5 J/cm 2 is needed of the pulsed fluence to ablate skin tissue. With a beam diameter of 2.5 mm, 5 Hz of 30 to 50 millijoules is considered optimal when using the UltraPulse la- ser. This set of parameters gives 20 to 30 /,m of tissue vaporization and 40 to 120/xm of residual thermal damage. A single pass is expected to result in partial or complete epidermal loss with mini- mal dermal effect. Dermal vaporization will ensue with additional passes and will be proportional to the pulse energy and total number of passes. In the

DERMATOLOGIC LASER SURGERY 123
human skin, UltraPulse laser will result in 20/xm, 40/xm, and 70/xm of thermal damage after 1, 2, and 3 passes, respectively.
Compared with the UltraPulse laser, the Tru- Pulse (Tissue Technologies, Albuquerque, NM) carbon dioxide laser has higher peak power pulses, but lower average power and shorter pulse durations (30/xs-1000/xs). It is capable of reach- ing fluences over 5 J/cm 2, which is necessary to ablate human skin. Within the 60-100 /xs pulse duration, which is shorter than that which would be capable from the UltraPulse, TruPulse's result- ant zone of vaporization with each pass and zone of residual thermal damage are also smaller, about 30/xm and 15 to 30/xm, respectively. Thus, more passes are required for a given depth of ablation, but a thinner layer of residual thermal damage is left behind. Early observations are that there are less oozing, crusting, and erythema with TruPulse laser compared with other carbon dioxide lasers.
A flashscanner using rapidly oscillating mirrors in the handpiece scans a focused continuous-wave laser beam in a spiral pattern across the tissue, thus keeping the laser beam at a given spot for less than 1 ms. With this feature, vaporization is achieved whereas thermal damage is limited to a 40 to 50 /xm radius. SilkTouch (ESC/Sharplan Medical Systems) is equipped with such a scanner that may be programmed to scan 1 to 16 mm diameter and various shapes (circles, ellipses, squares). Depending on the scan size, a cycle of skin resurfacing scan takes 0.2 to 0.45 seconds.
The Er:YAG laser is a relatively new player in skin resurfacing. Its water absorption coefficient is 10 times that of the carbon dioxide laser. It is able to ablate thin layer of tissue with minimal thermal injury as compared with the carbon diox- ide laser. Because there is less residual thermal injury compared with carbon dioxide, healing af- ter Er:YAG resurfacing is much faster. Also, there does not appear to be the hypopigmentation seen years after carbon dioxide laser resurfacing. Be- cause of this, resurfacing of isolated cosmetic units should be done with Er:YAG lasers only to avoid a pigment discrepancy and line of demarca- tion.
Facial rejuvenation of photodamaged skin manifesting in rhytides and actinic keratoses is one of the original and still the primary applica- tions of laser resurfacing technology. However, a long list of other indications exists including a
multitude of benign lesions (Table 6). It is impor- tant to note that carbon dioxide resurfacing of anatomic sites other than the face for the purposes of rejuvenation is contraindicated due to the high risk of scarring. Er:YAG laser, however, appears to be safer in non-facial sites when used cautiously.
The two main contraindications of facial resur- facing in a patient who is otherwise medically healthy enough to undergo the procedure are re- cent systemic isotretinoin use or recent facial sur- gery or tissue augmentation. Because of the poten- tial adverse effects of isotretinoin on wound healing, it is traditionally recommended to post- pone resurfacing for at least 1 year after dis- continuing the medication. Concomitant facial surgery, such as facelift, or facial tissue augmen- tation, such as lipotransfer, is not recommended because the incidence of scarring is much higher. A waiting period of at least 6 months is recom- mended between facial resurfacing and these other procedures.
Patient selection, patient compliance, pretreat- ment and posttreatment skin care, treatment techniques, and close clinical follow-up are all especially critical in optimizing results and mini- mizing side effects of facial resurfacing. Psycho- logical preparation of the period immediately after treatment and patient expectation of long-term outcome cannot be overemphasized. Fitzpatrick skin types I and II are ideal, with skin types III and IV carrying higher risk of pigmentary alterations. Those undergoing carbon dioxide laser resurfac- ing should also be warned of the frequent occur- rence of mild hypopigmentation of the treated skin years after the procedure. The line a color demarcation is usually more apparent in darker- skinned (skin type III and IV) patients. Prelaser topical tretinoin cream nightly is usually recom- mended, as such application seems to help mini- mize milia formation after the procedure. Bleach- ing agents are often recommended for 4 to 6 weeks before surgery for those in the higher risk category for hyperpigmentation. Anti-viral and anti-bacte- rial prophylaxis should always be used starting the day before the procedure and during the entire healing phase until complete re-epithelialization. An intravenous dose of antibiotics is also fre- quently given intraoperatively. Some laser sur- geons routinely use anti-fungal prophylaxis, but most only administer anti-fungal agents in high-

124 LOU AND GERONEMUS
risk patients or the patients demonstrate fungal overgrowth or infection during the healing phase.
Treatments of cosmetic units are generally per- formed with local anesthesia or nerve blocks. Al- though nerve blocks may be used for full-face procedures, twilight sedation by means of intrave- nous propafol with the concomitant used of fent- anyl and ketorolac tromethamine (Toradol, Roche Laboratories, Nutley, NJ) administered by an an- esthesiologist offers much greater patient com- fort. Supplemental oxygen is not recommended for safety concerns.
Postoperative care ranges from open to closed technique and a combination of both. In the open technique, gauze soaked with water, acetic acid, or hydrogen peroxide are used to soak the treated area followed by an application of a thick layer of ointment such as Aquaphor healing ointment (Beiersdorf-Jobst, Inc, Norwalk, Conn). This pro- cess is repeated several times a day initially but the frequency is decreased rapidly and is stopped after re-epithelialization. This open technique, al- though labor intensive, has the advantage of al- lowing potentially earlier detection of infection or other problems than the close technique. The open technique leaves the skin more susceptible to injury such as from scratching. If insufficient ointment is applied, re-epithelialization may be delayed. In the closed technique, a semi-occlusive dressing is secured to the face for up to a week. Advocate of this method claim greater patient comfort and faster healing. However, problems such as potential delayed detection of infection and feeling of claustrophobia by some patients. Some use the occlusive dressing for 1 to a few days followed by the open technique. A new class of dressing in the category of skin substitutes, cul- tured skin fibroblasts, biologic response modifiers such as growth factors and the likes have been used on burn wound and are currently being mar- keted for post-resurfacing use. Because of the high cost of these products, no adequately controlled studies have been done to support any claims of advantage over current methods.
Antiviral, antibacterial, and if desired antifun- gal agents should be continued during the postop- erative period until re-epithelialization is com- plete. Oral analgesics such as Tylenol with codeine (McNeil Pharmaceutical, Rariton, NJ), Vicodin (Knoll Laboratories, Mount Olive, NJ), or Percocet (DuPont Pharma, Wilmington, Del) are
taken on an as needed basis as the pain tolerance ranges widely among patients. Oral steroids, ei- ther prednisone 60-100 mg for 3-4 days or a Medrol Dosepak (UpJohn, Kalamazoo, Mich) may be used, but the threshold of administering it should be much higher for patients with a history of oral herpes simplex infections.
The potential complications of facial resurfac- ing include acute viral/herpetic infection, bacte- rial infection, and yeast overgrowth. Possible long-term side effects include scarring, prolonged erythema, and burning sensation. These may all be minimized by antimicrobial prophylaxis, close clinical observation, and avoiding the above-men- tioned contraindications of resurfacing.
Recently, carbon dioxide followed by 1 to 2 passes of Er:YAG to remove the ablated debris has been studied. This combination results in a thick zone of residual thermal injury which seems to correlate with collagen shrinkage and less healing time than without the Er:YAG passes. Faster re- epithelialization and less thermal injury are seen when the Er:YAG is used to resurface carbon di- oxide vaporized skin. In light of the potential ben- efits of combining the techniques, efforts have been made to design one system that offers both. Derma K (ESC Medical Systems, Needham, Mass) possesses the 250 to 350 microsec Er:YAG and a continuous-wave carbon dioxide lasers. Contour (Sciton, Palo Alto, Calif) is a 2940 nm Er:YAG laser with variable repetition rate and pulse energy combinations to effect thermal damage. How these systems actually fair with the traditional car- bon dioxide and Er:YAG lasers in terms of clinical results remains to be seen.
Other new trends in skin rejuvenation include non-laser techniques and non-ablative methods. A radio frequency device (Visage, Palo Alto, Calif) can remove the epidermis leaving a thin zone of dermal thermal damage by a method termed cold ablation. Ultrasound has also been used in skin resurfacing. Nonablative laser treatments of rhyt- ides, also termed subsurfacing, are a promising concept emerging in application. Attempts are be- ing made to heat the dermis to cause fibroplasia and collagen remodeling without epidermal in- jury. Studies are being done with numerous lasers emitting in the red to infrared ranging up to 1320 nm usually with epidermal cooling systems. Most of these systems target specific dermal chro- mophores, which in turn act as heat sources stim-

DERMATOLOGIC LASER SURGERY 125
ulating fibroplasia and collagen remodeling. One minor disadvantage exists for those patients with significant sun damage manifesting in lentigines
and solar keratoses as well as rhytides. These nonablative techniques would not be able to treat those epidermal lesions adequately.
RECOMMENDED READING
General Anderson RR, ParrishJA. The optics of human skin. J Invest
Dermatol 1981;77:13-9. Anderson RR, Parrish JA. Selective photothermolysis: pre-
cise microsurgery by selective absorption of pulsed radiation. Science 1983;220:524-7.
Einstein A. Zur Quantentheorie der Strahlung. Physik Z 1917;18:121. (English translation in: van der Waerden BL, editor. Sources of quantum mechanics. Amsterdam, North Holland; 1967. p. 63-77.)
Goldman L, Rockwell JR Jr. Laser reaction in living tissue. In: Lasers in medicine. New York: Gordon and Breach; 1971. p. 163-85.
Maiman TH. Stimulated optical radiation in ruby. Nature 1960;187:493.
Polla BS, Anderson RR. Thermal injury by laser pulses: pro- tection by heat shock despite failure to induce heat-shock response. Lasers Surg Med 1987;7:398-404.
Vascular lesions Adrian RM. Treatment of leg telangiectasia using a long
pulse frequency-doubled neodymium: YAG laser in 532 nm. Dermatol Surg 1998;24:22i-6.
Apfelberg DB, Kosek J, Maser MR, et al. Histology of port- wine stains after argon laser treatment. Br J Plast Surg 1979; 32:232-7.
Ashinoff R, Geronemus RG. Capillary Hemangiomas and treatment with flash lamp-pumped pulsed dye laser. Arch Der- matol 1991;127:202-5.
Ashinoff R, Geronemus RG. Failure of the flashlamp- pumped dye laser to prevent progression of the deeper com- ponent of hemangiomas. Pediatr Dermatol 1993;10:77-88.
Ashinoff R, Geronemus RG. Flashlamp-pnmped pulsed dye laser for port-wine stains in infancy: earlier versus later treat- ment. J Am Acad Dermatol 1991;24:467-72.
Augustin M, Zschocke I, Wick K, et al. Psychosocial stress of patients with port wine stains and expectations of dye laser treatment. Dermatology 1998;197:353-60.
Bernstein EF, Lee J, LoweryJ, et al. Treatment of spider veins with the 595 nm pulsed dye laser. J Am Acad Dermatol 1998; 24:737-40.
Bernstein LJ, Grossman MC, Kauvar ANB, et al. Effect of 7 mm versus 5 mm spot size on pulsed dye laser treatment of port wine stains and hemangiomas. Laser Surg Med 1996; (suppl 8):32.
Chess C, Chess Q. Cool laser optics treatment of large tel- angiectasia of the lower extremities. J Derm Surg Oncol 1993; 19:74-80.
Clodius I. Surgery for the extensive facial port-wine stain? Aesthetic Plast Surg 1985;9:61-8.
Conway H, Montroy RE. Permanent camouflage of capillary hemangiomas of the face by interdermal injection of insoluble pigments (tattooing): indications for surgery. NY State J Med 1965;65:876.
Dierickx CC, Casparian JM, Venugopalan V, et al. Thermal relaxation of port wine stain vessels probed in vivo. The need for 1-10 millisecond laser pulse treatment. J Invest Dermatol 1995;105:709-14.
Dixon JA, Heuther SE, Rotering SH. Hypertrophic scarring in argon laser treatment of port-wine stains. Plast Reconstru Surg Med 1987;7:495-8.
Dover JS, Geronemus G, Stern RS. Dye laser treatment of port-wine stains: comparison of continuous wave dye laser with a robotized scanning device and the pulsed dye laser. J Am Acad Dermatol 1995;32:237-40.
Enjolras O, Riche MC, Merland JJ, et al. Management of alarming hemangiomas in infancy: a review of 25 cases. Pedi- atrics 1990;85:491-8.
Finn MC, Glowachi J, Mulliken JB. Congenital vascular le- sions: clinical application of a new classification. J Pediatr Surg 1983;18:894-900.
Fitzpatrick RE, Lowe NJ, Goldman MP, et al. Flashlamp- pumped pulsed dye laser treatment of port-wine stains. J Der- matol Surg Oncol 1994;20:743-8.
Frieden 1J, Eichenfield LF, Esterly NB, et al. Guidelines of care for hamangiomas of infancy. J Am Acad Dermatol 1997; 37:631-7.
Frieden IJ. Management of hemangiomas. Pediatr Dermatol 1997;14:757-83.
Garden JM, Polla LL, Tan OT. The treatment of port-wine stains by the pulsed dye laser. Arch Dermatol 1988;124:889- 96.
Garden JM, Tan OT, Kerschmann R, et al. Effect of dye laser pulse duration on selective cutaneous vascular injury. J Invest Dermatol 1986;87:653-7.
Geronemus RG, Ashinoff R. The medical necessity of eval- uation and treatment of port-wine stains. J Dermatol 5urg Oncol 1991;17:76-9.
Geronemus RG. Pulsed dye treatment of vascular lesions in children. J Dermatol Surg Oncol 1993;19:303-10.
Glassberg E, Lask GP, Tan EML, et al. The flashlamp- pumped 577 nm pulsed tunable dye laser: clinical efficacy and in vitro studies. J Dermatol Surg Oncol 1988; 14:1200-8.
Goldberg DJ, Meine JG. Treatment of facial telangiectases with the diode-pumped frequency-doubled Q-switched Nd: YAG laser. Dermatol Surg 1998;24:828-32.
Goldman MP, Eckhouse S. Photothermal sclerosis of leg veins. Dermatol Surg 1996;22:323-30.
Goldman MP, Fitzpatrick RE. Pulsed dye laser treatment of leg telangiectasia: with and without simultaneous sclerother- apy. J Dermatol Oncol 1990;16:338-44.
Goldman MP, Kaplan RP, Dully DM. Postsclerotherapy hy- perpigmentation: a histologic evaluation. J Dermatol Surg On- col 1987;13:547-50.
Gonzalez E, Gange RW, Momtaz KT. Treatment of telangi- ectasia and other benign vascular lesions with the 577 nm pulsed dye laser. J Am Acad Dermatol 1992;27:220-6.

126 LOU AND GERONEMUS
Hidano A, Ogihara Y. Cryotherapy with solid carbon diox- ide in the treatment of nevus flammeus. J Dermatol Surg Oncol 1977;3:213-6.
Hsia J, Lowery JA, Zelickson B. Treatment of leg telangiec- tasia using long pulse dye at 595 nm. Laser Surg Med 1997; 220:1-5.
Jacob AH, Walton RG. The incidence of birthmarks in the neonate. Pediatrics 1976;58:212-22.
Kauvar ANB, Geronemus RG. Repetitive pulsed dye laser treatments improve persistent port-wine stains. Dermatol Surg 1995;21:515-21.
Kauvar ANB, Lou WW, Quintana AT. Effect of cryogen spray cooling on treatment of leg telangiectasia with 595 nm, 1.5 msec and 755 nm, 3 msec lasers. Laser Surg Med 1999; 19(suppl 11):19.
Kauvar ANB, Waldorf HA, Geronemus RG. Effect of 7 mm versus 5 mm spot size on pulsed dye laser treatment of port wine stains and hemangiomas. Laser Surg Med 1995;56(suppl 7):56.
Landthaler M, Haina D, Waidelich W, et al. Laser therapy of venous lakes and telangiectasia. Plast Reconstr Surg 1984;73: 78-83.
Lanigan SW, CotterillJA. Psychological disabilities amongst patients with port wine stains. BrJ Dermato11989;121:209-15.
Lanigan SW. Acquired port wine stains: clinical and psycho- logical assessment and response to pulsed dye laser therapy. BrJ Dermatol 1997;137:86-90.
McClean K, Hanke CW. The medical necessity for treatment of port-wine stains. Dermatol Surg 1997;23:663-7.
McDaniel DH, Ash K, Loral J, et al. Laser therapy of spider leg veins: clinical evaluation of a new long pulsed alexandrite laser. Dermatol Surg 1999;25:52-8.
Miliora MT. Facial disfigurement: a self-psychological per- spective on the hide-and-seek fantasy of an avoidant personal- ity. Bulletin of the Menninger Clinic 1998;62:378-94.
MorelliJG, Tan OT, Garden J, et al. Tunable dye Iaser (577 nm) treatment of port-wine stains. Lasers Surg Med 1986;6: 94-9.
Mulliken JB, Glowacki J. Hemangiomas and vascular mal- formations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 1982;69:412- 22.
Mulliken JB. Capillary (port-wine) and other telangiectatic stains. In: Mulliken JB, Young AE, editors. Vascular birth- marks, hemangiomas, and malformations. Philadelphia: Saun- ders; 1988.
Nelson JS, Milner TE, Anvari B, et al. Dynamic epidermal coiling in conjunction with laser-induced photothermolyses of port wine stain blood vessels. Lasers Surg Med 1996; 19:224-9.
Nguyen CM, YohnJJ, Huff C, et al. Facial port wine stains in childhood: prediction of the rate of improvement as a function of the age of the patient, size and location of the port wine stain and the number of treatments with the pulsed dye (585 nm) laser. BrJ Dermatol 1998;138:821-5.
Polla LL, Tan TO, Garden JM, Parrish JA. Tunable pulsed dye laser for the treatment of benign cutaneous vascular ecta- sia. Dermatologia 1987;174:11-7.
Quintana AT, Grossman MC, Kauvar ANB, et al. Removal of leg veins with Laserscope potassium titanyl phosphate-532 nm laser. Laser Surg Med 1998;41(suppl 10):41.
Renfro L, Geronemus RG. Anatomical differences of port-
wine stains in response to treatment with the pulsed dye laser. Arch Dermatol 1993;129:182-8.
Ruiz-Esparza J, Goldman MP, Fitzpatrick RE, et al. Flashlamp-pumped dye laser treatment of telangiectasia. J Der- matol Surg Oncol 1993;19:1000-3.
Schroeter CA, Neuman HAM. An intense light source. The photodenn VL-flashlamp as a new treatment possibility for vascular skin lesions. Dermatol Surg 1998;24:743-8.
Tan TO, Carney M, Margolis R, et al. Histologic response of port-wine stains treated argon, carbon dioxide and tunable dye lasers. Arch Dermatol 1986;122:1016-22.
Troilius A, Wrangsjo B, Ljunggren B. Potential psychologi- cal benefits from early treatment of port-wine stains in chil- dren. BrJ Dermatol 1998;139:59-65.
Van Gemert MJC, Welch AJ, Picketing JW, et al. Wave- lengths for laser treatment of port wine stains and telangiecta- sia. Lasers Surg Med 1995;16:147-55.
Waldorf H, Alster T, Kauvar ANB, et al. Effect of dynamic cooling on 585 nm pulsed dye laser treatment of port-wine stain birthmark. Dermatol Surg 1997;23:519-25.
Waner M, Suen JY, Dinehart S, et al. Laser photocoagulation of superficial proliferating hemangiomas. J Dermatol Surg On- col 1994;20:43-6.
Pigmented lesions Ashinoff R, Geronemus RG. Q-switched ruby laser treat-
ment of labial lentigos. J Am Acad Dermatol 1992;27:809-11. DePadova-Elder SM, Milgraum S. Q-switched ruby laser
treatment of labial lentigines in Peutz-Jeghers syndrome. J Dermatol Surg Oncol 1994;20:830-2.
Dover J, Polla L, Margolis R, et al. Pulse width dependence of pigment cell damage at 694 nm in guinea pig skin. Proc SPIE 1987;712:200-5.
Fitzpatrick RE, Goldman MP, Ruiz-Esparza J. Laser treat- ment of benign pigmented epidermal lesion using a 300 nsec- ond pulse and a 510 nm wavelength. J Dermatol Surg Oncol 1993;18:341-7.
Geronemus RG. Q-switched ruby laser therapy of nevus of Ota. Arch Dermatol 1992;128:1618-22.
Goldberg DJ. Benign pigmented lesions: treatment with the Q-switched ruby laser. J Dermatol Surg Oncol 1993; 19:376-9.
Goldberg DJ, Stampien T. Q-switched ruby laser treatment of congenital nevi. Arch Dermatol 1995;131:621-3.
Goldman L, Blaney DJ, Kindel DJ, et al. Pathology of the effect of the laser beam on the skin. Nature 1963;197:912-4.
Goldman L, IgelmanJM, Richfield DF. Impact of the laser on nevi and melanomas. Arch Dermatol 1964;90:71-5.
Goldman, Wilson RG, Hornby P, et al. Radiation from a Q-switched ruby laser. J Invest Dermatol 1965;44:69-71.
Goyal S, Arndt KA, Stern RS, et al. Laser treatment of tattoos: a prospective, pared, comparison study of the Q-switched Nd: YAG (1064 nm), frequency-doubled Q-switched Nd:YAG (532 nm), and Q-switched ruby lasers. J Am Acad Dermatol 1997; 36:122-5.
GrevelinkJM, van Leeuwen RL, Anderson RR, et al. Clinical and histological responses of congenital melanocytic nevi after single treatment with Qswitched lasers. Arch Dermatol 1997; 133:349-53.
Kilmer S, Anderson R. Clinical use of the Q-switched ruby and the Q-switched Nd:YAG (1064 nm and 532 nm) lasers for treatment of tattoos. J Dermatol Surg Oncol 1993;19:330-8.

DERMATOLOGIC LASER SURGERY 127
Knoell KA, Milgraum SS, Kutenplon M. Q-switched ruby laser treatment of minocycline-induced cutaneous hyperpig- mentation. Arch Dermatol 1996;132:1251-2.
Milgraum S, Cohen M, Aauletta M. Treatment of blue nevi with the Q-switched ruby laser. J Am Acad Dermato11995;32: 307-10.
Polla L, Margolis R, Dover J, et al. Melauosomes are a pri- mary target of Q-switched ruby laser-irradiation in guinea pig skin. J Invest Dermatol 1987;89:281-6.
Taylor CR, Anderson RR. Treatment of benign pigmented epidermal lesions by Q-switched ruby laser. J Invest Dermatol 1993;32:908-12.
Ueda S, Imayama S. Normal-mode ruby laser for treating congenital nevi. Arch Dermatol 1997;133:355-9.
Waldorf HA, Kauvar ANB, Geronemus RG. Treatment of small and medium congenital nevi with the Q-switched ruby laser. Arch Dermatol 1996;132:301-4.
Watanabe S, Takahashi H. Treatment of nevus of Ota with the Q-switched ruby laser. N EnglJ Med 1994;331:1745-50.
Hair reduction Cotsarelis G, Sun TT, Lavker RM. Label-retaining cells re-
side in the bulge area of the pilosebaceous unit: implications for follicular stein ceils, hair cycles, and skin carcinogenesis. Cell 1990;61:1329-7.
Dierickx CC, Campos VB, Lin D, et al. Influence of hair growth cycle on efficacy of laser hair removal. Laser Surg Med 1999;884:2l.
Dierickx CC, Grossman MC, Farinelli WA, et al. Hair re- moval by a pulsed infrared laser system [abstract]. Lasers Surg Med 1998;$10:42.
Dierickx CC, Melanie MC, Farinelli WA, et al. Permanent hair removal by normal-mode ruby Iaser. Arch Dermato11998; 134:837-42.
Duque V, Dierickx CC, Lin D, et al. Long pulsed ruby laser for hair removal: comparison between different spot sizes, temperatures and interval between first and second treatment [abstract[. Lasers Surg Med 1998;$10:39.
Finkel B, Eliezri YD, Waldman A, et al. Pulsed alexandrite lasers technology for norl-invasive hair removal. J Clin Laser Med Surg 1997;15:225-9.
Gold MH, Bell MW, Foster TD, et al. Long-term epilation using the EpiLight broad band, intense pulsed light hair re- moval system. 1997;23:909-13.
Goldberg DJ, Littler CM, Wheeland RG. Topical suspen- sion-assisted Q-switched Nd:YAG laser hair removal. Derma- tol Surg 1997;23:741-5.
Grossman MC, Dierickx C, Farinalli W, et al. Damage to hair follicles by normal-mode ruby laser pulses. J Am Acad Derma- tol 1996;35:889-94.
Kilmer SL, Chotzen VA. Q-switched Nd:YAG hair removal without adjuvant topical preparation. Laser Surg Med 1997;$9: 31.
Lask G, Elman M, Slatkine M, et al. Laser-assisted hair re- moval by selective photothermolysis. Dermatol Surg 1997;23: 737-9.
Lou WW, Quintana AT, Geronemus RG, et al. Prospective study of hair reduction by diode laser (800 nm) with long-term follow-up. Dermatol Surg 2000;26:428-32.
Lou WW, Geronemus RG, Grossman MC. Hair removal
with long pulsed alexandrite laser for patients with skin types III-V. Laser Surg Med 1999;89(suppl 11):23.
Nanni CA, Alster TA. Complications of laser assisted hair removal using the Q-switched Nd:YAG, long-pulsed ruby, and long-pulsed alexandrite lasers. Lasers Surg Med 1998;(suppl 10):67.
Nanni CA, Alster TS. Optimizing treatment parameters for hair removal using a topical carbon-based solution and 1064-nm Q-switched Neodymium:YAG laser energy. Arch Dermatol 1997;133:1546-9.
Narurkar V, Miller HM, Seltzer R. The safety and efficacy of the long pulsed alexandrite laser for hair removal in various skin types [abstract]. Lasers Surg Med 1998;189:39.
Sun TT, Cotsarelis G, Lavker RM. Hair follicular stem cells: the bulge-activation hypothesis. J Invest DermatoI 1991;96: 775-85.
Woo TY, Molnar G. Laser assisted hair removal using the Cynosure long pulsed alexandrite laser [abstract]. Lasers Surg Med 1998;186:39.
Resurfacing Apfelberg DB. A critical appraisal of high-energy pulsed
carbon dioxide laser facial resurfacing for acne scars. Ann Plast Surg 1997;38:95-100.
Bernstein LJ, Kauvar ANB, Grossman MC, et al. The short- and long-term side effects of carbon dioxide laser resurfacing. Dermatol Surg 1997;23:519-25.
Bernstein LJ, Kauvar ANB, Grossman MC, et al. Scar resur- facing with high-energy, short-pulsed and flashscanning car- bon dioxide lasers. Dermatol Surg 1998;24:101-7.
Brugmans MJP, KemperJ, Gijsbers GHM, et al. Temperature response of biological materials to pulsed non-ablative CO2 laser irradiation. Lasers Surg Med 1991;11:587-94.
Chernoff G~ Slatkine M, Zair E, et al. SilkTouch: a new technology for skin resurfacing in aesthetic surgery. J Clin Laser Med Surg 1995;13:97-100.
Chernoff WG, Schoenrock LD, Cramer H, et al. Cutaneous laser resurfacing. Int J Aesth Restor Surg 1995;3:57-68.
Cotton J, Hood HF, Gonin R, et al. Histologic evaluation of pre-auricular and post-auricular human skin after high-en- ergy, short-pulse carbon dioxide laser. Arch Dermatol 1996; 132:425-8.
Drnovsek-Olup B, Vedlin B. Use of Er:YAG laser for benign skin disorders. Lasers Surg Med 1997;21:13-9.
Fulton JE. Complications of laser resurfacing. Dermatol Surg 1997;24:91-9.
Green HA, Burd E, Nishioka NS, et aI. Middermal wound healing. A comparison between dermatomal excision and pulsed carbon dioxide laser ablation. Arch Dermato11992;128: 639-45.
Green HA, Domankevitz Y, Nishioka NS. Pulsed carbon dioxide laser ablation of burned skin: in vitro and in vivo analysis. Lasers Surg Med 1998;10:476-84.
Hobbs ER, Bailin PL, Wheeland RG, et al. Superpulsed la- sers: minimizing thermal damage with short duration, high irradiance pulses. J Dermatol Surg Oncol 1987;13:955-64.
Hohenleutner U, Hohenleutener S, Baumler W, et al. Fast and effective skin ablation with an Er:YAG laser: determina- tion of ablation rates and thermal damage zones. Lasers Surg Med 1997;20:242-7.
Johnson TM, Sebastien TS, Lowe L, et al. Carbon dioxide

128 LOU AND GERONEMUS
laser treatment of actinic cheilitis. J Am Acad Dermatol 1988; 19:876-8.
Kauvar ANB, Geronenms RG, Waldorf HA. Char-free tissue ablation: a comparative histopathological analysis of new car- bon dioxide (CO 2) laser systems. Lasers Surg Med 1995; 16(suppl 7):50.
Khatri KA, Ross V, Grevelink JM. Comparison of erbium: YAG and carbon dioxide lasers in resurfacing of facial rhytides. Arch Dermatol 1999;135:391-7.
Lawes K, Thomsen S, Nolan K, et al. Skin resurfacing using an ultrasonic aspirator. Proceedings of SPIE. 1998;3245:374- 81.
Lowe NJ, Lask G, Griffin ME. Laser skin resurfacing: pre- and posttreatment guidelines. Dermatol Surg 1995;21:1017-9.
Manuskiatti W, Fitzpatrick RE, Goldman MP, et al. Prophy- lactic antibiotics in patients undergoing laser resurfacing of the skin. J Am Acad Dermatol 1999;40:77-84.
Ratner D, Viron A, Puvion-Dutilleul F, et al. Pilot uhrastruc- ture evaluation of human preauricular skin before and after high-energy pulsed carbon dioxide laser treatment. Arch Der- matol 1998;134:582-7.
Rubenstein R, Roenigk HH Jr, 8tegman SJ, et al. Atypical
keloids after dermabrasion in patients taking isotretinoin. J Am Acad Dermatol 1986;15:280-5.
Ross EV, McKinlay JR, Anderson RR. Why does carbon dioxide resurfacing work? Arch Derm 1999;135:444-54.
Sriprachya-Anunt S, Fitzpatrick RE, Goldman MP, et al. Infections complicating pulsed carbon dioxide laser resurfac- ing for photoaged facial skin. Dermatol Surg 1887;23:527-36.
Waldorf HA, Kauvar ANB, Geronemus RG. Skin resurfacing of fine to deep rhytides using a char-free carbon dioxide laser in 47 patients. Dermatol Surg 1995;2l:940-6.
Walsh JJ, Deutsch TF. Pulsed CO2 laser tissue ablation: measurement of the ablation rate. Lasers Surg Med 1988;8: 264-75.
Weinstein C, Ramirez OM, Pozner JN. Postoperative care following CO 2 laser resurfacing: avoiding pitfall. Plast Recontr Surg 1997;100:1855.
Yang CC, Chai CY. Animal study of skin resurfacing using the UltraPulse carbon dioxide laser. Ann Plast Surg 1955;35: 154-8.
Young CK. Resurfacing of pitted facial scars with a pulsed Er:YAG laser. Dermatol Surg 1997;23:880-3.