The Thai Journal of SURGERY
64
Secretariat Office : Royal Golden Jubilee Building, 2 Soi Soonvijai, New Petchaburi Road, Huaykwang, Bangkok 10310, Thailand Tel. +66 2716 6141-3 Fax +66 2716 6144 E-mail: [email protected] www.tci-thaijo.org/index.php/ThaiJSurg/index Volume 40 October-December 2019 Number 4 ISSN 0125-6068 ORIGINAL ARTICLES Official Publication of The Royal College of Surgeons of Thailand www.tci-thaijo.org/index.php/ThaiJSurg/index The Thai Journal of SURGERY Factors Related to the Quality of Life of Ostomates at Viet Duc Hospital in 2018 Nguyen Duc Chinh, Nguyen Ngoe Thuc, Nguyen Xuan Hung, Truong Viet Dung Prognosis and Clinical Outcome of Papillary Carcinoma of The Breast at A Tertiary Care Hospital Rupporn Sukpanich, Panuwat Lertsithichai, Prakasit Chirappapha, Ronnarat Suvikapakornkul, Yodying Wasuthit, Thongchai Sukornyothin, Sansanee Wongwaisayawan, Monchai Leesombatpaiboon NT-2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in Thailand Buchcha Prammanasudh, Vibul Trakulhoon Vertical Mastopexy Prakasit Chirappapha, Suragit Pornchai SURGICAL TECHNIQUE REVIEW ARTICLE ABSTRACTS 126 Abstracts of the 44 th Annual Scientific Congress of The Royal College of Surgeons of Thailand, 13-16 July 2019, Ambassador City Jomtien Hotel, Jomtien, Pattaya, Cholburi, Thailand (Part II) 97 101 107 117
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The Thai Journal of SURGERY

Secretariat Office :Royal Golden Jubilee Building, 2 Soi Soonvijai, New Petchaburi Road, Huaykwang, Bangkok 10310, ThailandTel. +66 2716 6141-3 Fax +66 2716 6144 E-mail: [email protected] www.tci-thaijo.org/index.php/ThaiJSurg/index
Volume 40 October-December 2019 Number 4
ISSN 0125-6068
ORIGINAL ARTICLES
Official Publication of The Royal College of Surgeons of Thailand www.tci-thaijo.org/index.php/ThaiJSurg/index
The Thai Journal of SURGERY
Factors Related to the Quality of Life of Ostomates at Viet Duc Hospital in 2018Nguyen Duc Chinh, Nguyen Ngoe Thuc, Nguyen Xuan Hung, Truong Viet Dung
Prognosis and Clinical Outcome of Papillary Carcinoma of The Breast atA Tertiary Care HospitalRupporn Sukpanich, Panuwat Lertsithichai, Prakasit Chirappapha,Ronnarat Suvikapakornkul, Yodying Wasuthit, Thongchai Sukornyothin,Sansanee Wongwaisayawan, Monchai Leesombatpaiboon
NT-2013: A Recommended Nutrition Screening and Nutrition Format forPractical Clinical Use in Hospitalized Patients in ThailandBuchcha Prammanasudh, Vibul Trakulhoon
Vertical MastopexyPrakasit Chirappapha, Suragit Pornchai
SURGICAL TECHNIQUE
REVIEW ARTICLE
ABSTRACTS
126 Abstracts of the 44th Annual Scientific Congress of The Royal College of Surgeons ofThailand, 13-16 July 2019, Ambassador City Jomtien Hotel, Jomtien, Pattaya, Cholburi,Thailand (Part II)
97
101
107
117

Royal College of Surgeons of ThailandSecretariat Office :Royal Golden Jubilee Building, 2 Soi Soonvijai, New Petchburi Road,Bangkok 10310, Thailand
OFFICERS 2017 - 2019
President : Tanaphon MaipangPresident-Elect : Paisit SiriwittayakornVice President : Pramook MutiranguraSecretary General : Vitoon ChinswangwatanakulAssistant Scretary : Charnvate SatthaputhTreasurer : Preecha SiritongtawornPast Presidents : Udom Poshakrisna
Sem Pring-Puang-GeoKasarn ChartikavanijCharas SuwanwelaThira LimsilaKijja SindhvanandaArun PausawasdiKitti YensudchaiThongueb UttaravichienChomchark ChuntrasakulPrinya SakiyalakVithya VathanophasNaronk RodwarnaNopadol Wora-UraiSoottiporn ChittmittrapapVajarabhongsa BhudhisawasdiParinya Thavichaigarn
BOARD OF DIRECTORS
Songchai Simaroj Representative of General SurgeonsMonawat Ngerncham Representative of Pediatric SurgeonsSirachai Jindarak Representative of Plastic & Reconstructive SurgeonsSompop Prathanee Representative of Thoracic SurgeonsYodruk Prasert Representative of NeurosurgeonsChaiyong Nualyong Representative of Urological SurgeonsNopdanai Chaisomboon Representative of Colorectal SurgeonsThana Turajane Representative of Orthopedic SurgeonsThanyadej Nimmanwudipong MemberPornchai O-Charoenrat MemberSupakorn Rojananin Member

Editorial Board
First Editor : Thongdee Shaipanich
Emeritus Editor : Soottiporn ChittmittrapapNopadol Wora-UraiPornchai O-charoenrat
Editor-in-Chief : Panuwat Lertsithichai
International Editorial Board :Shuji Shimizu (Japan)Anusak Yiengpruksawan (United States of America)
Editorial Team :Bunpot Sitthinamsuwan Doonyapat Sa-NguanraksaKaweesak Chittawatanarat Pornprom MuangmanPotchavit Aphinives Prakasit ChirappaphaSurasak Sangkhathat Thanyawat SasanakietkulThawatchai Akaraviputh Varut Lohsiriwat
Advisory Board :Paisit SiriwittayakornPramook Mutirangura
Editorial Board:Chairat Supsamutchai Chaiyong NuanyongChaowanun Pornwaragorn Chayanoot RattadilokIttichai Sakarungchai Jule NamchaisiriNarongrit Kantathut Narong RungsakulkijNutsiri Kittitirapong Paisarn VejchapipatPanya Thaweepworadej Phitsanu MahawongPiya Samankatiwat Pornthep PungrasmiSaritphat Orrapin Siripong SirikurnpiboonSompol Permpongkosol Suragit PornchaiSuravej Numhom Teerawut RakchobWiroon Laupattarakasem
ISSN 0125-6068
Published quarterly by : The Royal College of Surgeons of Thailand
Official Publication of The Royal College of Surgeons of Thailand
The THAIJournal of SURGERY

About the JournalThe Thai Journal of Surgery is the official publication of The
Royal College of Surgeons of Thailand issued quarterly.The Thai Journal of Surgery invites concise original articles in
clinical and experimental surgery, surgical education, surgical history,surgical techniques and devices, as well as review articles in surgery andrelated fields. Papers in basic science and translational medicine relatedto surgery are also welcome. The Thai Journal of Surgery is dedicated toserving the needs of the Members of The Royal College of Surgeons ofThailand, specifically the younger researchers and surgeons in trainingwho wish to have an outlet for their research endeavors. The RoyalCollege strives to encourage and help develop Thai Surgeons to becomecompetent researchers in all their given fields. With an internationaloutlook, the Thai Journal of Surgery welcomes submissions from outsideof Thailand as well.
Articles must be contributed solely to The Thai Journal of Surgeryand when published become the property of the Royal College ofSurgeons of Thailand. The Royal College of Surgeons of Thailandreserves copyright on all published materials and such materials may notbe reproduced in any form without the written permission. Manuscriptssubmitted for publication should be sent to our e-Journal system webpage:https://he02.tci-thaijo.org/index.php/ThaiJSurg/about/submissions.
ManuscriptsManuscripts should be typewritten on size A4 paper only with
double spacing and at least one-inch margins. Separate pages: title page,text, acknowledgments, references, individual tables, abstract in Thai,and legends (as the format in this journal). Number pages consecutively,beginning with the title page. Type the page number in the upper right-hand corner of each page. Metric measurements should be used. Genericnames for drugs should be used and if trade name is mentioned, it shouldbe put in parenthesis.
The title page of the manuscript should be typed on a separatesheet and contain the following information:
1. Title of the paper2. Name of Author(s), including first name(s) with academic
degree(s)3. Name of department and institution in which the work was done4. Index word(s)5. Short running title
Illustrations and TablesAll photographs and original drawing should be professionally
made or drawn and uploaded as jpeg, png, tiff files with at least 300 ppi.Typewritten or freehand lettering is not acceptable. Illustration should benumbered along with an appropriate description (legend/caption). Eachtable should be prepared on a separate sheet and should be numberedconsecutively as mentioned in the text and each must have a heading.
ReferencesReferences must be listed on a separate sheet in numeric order as
referred to in the article, not alphabetically. Only references mentionedin the text should be listed and should be selective with not more than 30references except under unusual circumstances. Number references
consecutively in the order in which they are first mentioned in the text.Identify references in text, tables, and legends by Arabic numerals (insuperscript). The references must be verified by the author(s) against theoriginal documents. Example forms of references are given below.Journal
1. Standard Journal Article:List all authors when three or less; when four or more, list only first
three and add et al.Soter NA, Wasserman SI, Austen KF. Cold urticaria: release into thecirculation of histamine and eosinophil chemotatic factor of anaphylaxisduring cold challenge. N Engl J Med 1976; 294:687-90.
2. Corporate Author:The Committee on Enzymes of the Scandinavian Society for
Clinical Chemistry and Clinical Physiology. Recommended method forthe determination of gamma glutamyltransferase in blood. Scand J ClinLab Invest 1976; 36:119-25.Books and Other Monographs
3. Personal Author(s):Osler AG. Complement: mechanisms and functions. Englewood
Cliffs: Prentice - Hall, 1976.4. Corporate Author:American medical Association Department of Drugs. AMA drug
evaluations. 3rd ed. Littleton: Publishing Sciences Group, 1977.5. Editor, Compiler, Chairman as Author:Rhooder AJ. Van Rooyen CE, comps. Textbook of virology: for
students and practitioners of medicine and the other health sciences. 5thed. Baltimore: William & Wilkins, 1968.
6. Chapter in Book:Weinstein L, Swartz. MN. Pathogenic properties of invading
micro-organisms. In: Sodeman WA Jr. Sodeman WA, eds. Pathologicphysiology: mechanisme of disease. Philadelphia: WB Saunders,1974:457-72.
7. Agency Publication:National Center for Health Statistics. Acute conditions: incidence
and associated disability, United States, July1968-June1969. Rockville.Md.: National Center for Health statistics, 1972. Vital and healthstatistics. Series 10: Data from the National health Survey, No. 69:(DHEW publication no. (HSM) 72-1036).Other Articles
8. Newspaper Article:Shaffer RA. Advances in chemistry are starting to unlock mysteries
of the brain: discoveries could help cure alcoholism and insomnia,explain mental illness. How the messengers work. Wall street Journal1977 Aug 12(col. 1), 10(col. 1).
9. Magazine Article:Roueche B. Annals of medicine: the Santa Claus culture. The New
Yorker 1971 Sep 4:66-81.
AbbreviationsUse only standard abbreviations of commonly used approved
abbreviations. Avoid abbreviations in the title. The full term for whichan abbreviation stands should precede its first use in the text unless it isa standard unit of measurement.
The THAIJournal of SURGERY
Official Publication of The Royal College of Surgeons of Thailand
INFORMATION FOR AUTHORS

97
Abstract Objective: The ostoma or artificial anus is a part of life of patients who bear it, which impacts quality of life. There are many ostomates at the Viet Duc Hospital, and thus we conducted a study on the quality of life and related factors to help inform recommendations for improving their quality of life.
Materials and Methods: A descriptive study was conducted on patients 18 years or older having an ostomy from April to June 2018. The tool used was “The City of Hope-Quality of Life-Ostomy Questionnaire (CoH-Qol-OQ)”. Patients were interviewed using the questionnaire. The data was analyzed using SPSS.20.0.
Results: There were a total of 203 patients; 137 were men (68%) and 66 were women (32%). Significant factors related to lower Quality of Life (QoL) included: emergency surgery, primary disease other than cancer, presence of concomitant disease, lack of health insurance, sexual dysfunction, postoperative depression, lack of support groups, difficult ostomy location, change in diet, and longer duration of ostomy care.
Conclusion: The study showed that there were many factors which impact the QoL of ostomates. There-fore, to improve the QoLof ostomates, we need to enhance health education and counseling as well as encourag-ing community integration.
Keywords: Artificial anus, Ostomates, Quality of life of Ostomates.
Correspondence address: Nguyen Duc Chinh, Viet Duc University Hospital, Hanoi; Email: [email protected]
The THAI Journal of SURGERY 2019;40:97-100.Official Publication of The Royal College of Surgeons of Thailand
Factors Related to the Quality of Life of Ostomates at Viet Duc Hospital in 2018Nguyen Duc Chinh, MD*
Nguyen Ngoc Thuc, MD* Nguyen Xuan Hung, MD*
Truong Viet Dung† *Viet Duc University Hospital, Hanoi, Vietnam†Thăng Long University, Hanoi, Vietnam
Original Article
The THAI Journal of SURGERY
Official Publication of The Royal College of Surgeons of Thailand
Vol. 40 October - December 2019 No. 4

Chinh ND, et al. Thai J Surg Oct. - Dec. 201998
IntroductIon
According to the Association of World Council Enterostomal Therapist - WCET1,2,6, estimates the world has nearly 2 million people carrying ostomies, of which about 15% are uretostomies. The largest group includes patients with gastrointestinal stoma, also known as ar-tificial anus or colostomy. Ostomies are distressing to many patients. Numerous studies have shown that the quality of life of these patients is significantly reduced. The ostomy changes psychological status and social activities. Changes include lifestyle changes, reduced ability and the desire to do work, and reduced sexual activities, especially in younger patients. These problems may lead to the self-isolation of patients3,5. There are no official statistics, but it is likely that there are many ostomy patients or ostomates, in Viet-nam2. Large hospitals such as Viet Duc (Hanoi) and Cho Ray (Ho Chi Minh City) hospitals have between 300 to 500 cases of stoma per year. There is little attempt to learn about the quality of life of these patients. Therefore, we conducted the present study aiming to learn about the factors affecting the quality of life of ostomates at Viet Duc Hospital, by which recommendations and advice may be made to improve the quality of care to ostomates.
MaterIals and Methods
All patients who underwent ostomy surgery at the Viet Duc Hospital, who were 18 years or older, regardless of gender, were enrolled into the study. Patients must be least 4 weeks discharged from the hospital and resumed everyday life activities. The present study was a descriptive prospective cross-sectional study. The subjects used the question-naire “The City of Hope Scale-Quality of Life-Ostomy Questionnaire (CoH-Qol-OQ)” by Grant and Davis7. The study was conducted between April and June 2018. Based on the rating scale, the quality of life (QoL) of patients was classified into the following levels: Low QoL if scores ≤ 5 points; Average QoL, if scores are between 5 to 7 points; and High QoL if scores ≥ 7 points. Data were collected and analyzed using SPSS.20 software. Fisher’s exact test was used to determine significant difference beween groups, with significant p-values set at 0.05 or less. Odds Ratios and 95% con-fidence intervals were used to measure associations between risk factors and outcome.
results
There were 203 patients with ostomies, including 137 men (68%) and 66 women (32%). The larget group was aged 60 years and older, constitutng 47% of all patients. Most were farmers (37%), or retired (38%). Most, 92%, have health insurance. In terms of physical QoL, 61% rated their QoL as low, 30% as average, and 9% as good QoL. In terms of welfare, 43% rated low, 40% rated average, and 17% rated good QoL. In terms of psychological impact, 51% rated low, 29% rated average, and 20% rated good QoL. Factors related to low or average QoL are given in Table 1. Table 1 shows that there are 10 factors significantly related to poor (low to average) QoL. These included: emergency surgery, primary disease other than cancer, presence of concomitant disease, lack of health insur-ance, sexual dysfunction, postoperative depression, lack of support groups, difficult ostomy location, change in diet, and longer duration of ostomy care (taking longer than 60 minutes per day).
dIscussIon
According to recent statistics, there are a lot of os-tomates and many involved are concerned. In the present study, we found a few important factors associated with poor QoL. Certain demographic factors are important, but not in the present study. In Naseh’s study (2011)11, age was correlated with the QoL (correlation coefficient, 0.262, p = 0.015). Unmarried men had higher QoL than married men or women6,8,9. In our study, women had lower QoL compared to men, but not by much and was not statisti-cally significant. Similarly, age was not a significant factor. Type of surgery may be related to permanent or temporary ostomy. We found emergency surgery to be significantly related to lower QoL - perhaps due to a ten-dency to permanent ostomy. Some studies show a posi-tive correlation between self-efficiency or confidence and good QoL. Those, who are happy, less anxious, and able to take care of and manage their ostomy better, are confident in their stomy care. Naseh (2011) observed that there is a clear correlation between confidence and physical factors (correlation 0.485; p < 0.001), psycho-logical factors (0.655; p < 0.001), social factors (0.694; p < 0.001), and mental factors (0.393; p < 0.001)6,7,10.

Factors related to the quality of life of ostomates at Viet Duc Hospital in 2018Vol. 40 No. 4 99
Our study similarly shows that patients with depression, as opposed to those with no depression, were 2.83 times as likely (in terms of odds) to have poor QoL. In 81% of patients with postoperative depression, QoL was rated poor (Table 1). Staging and location of colorectal cancer could be important in determining the QoL. In a study of 117 ostomates suffering from colorectal cancer, a positive relationship between the QoL and time since diagnosis was found, meaning that if the disease was diagnosed
at an early stage, the QoL was higher. Chemotherapy or radiotherapy also affected the QoL. Pham Thi Thanh Phuong1 emphasized that the severity of illness, depres-sion, and anxiety; and ability to self-care also affected the QoL of patients, a finding similar to that of some authors3,9,10. Our study showed that chronic concomit-tant diseases were associated with poor QoL, although cancer as a primary reason for ostomy was related to better QoL.
Table 1 Factors related to low or average quality of life of ostomates
Quality of lifeFactor OR p-value Low/Average (%) High (%)
Gender Male 85 (62) 52 (38) 1.22 0.538 Female 44 (67) 22 (33) (0.63 - 2.40)
Age range 18-40 yrs 18 (69) 8 (31) 1.46 0.493 (0.53 - 4.32) 41-60 yrs 51 (61) 33 (39) 1 NA ≥60yrs 60(65) 33(35) 1.24 0.816 (0.45 - 3.65)
Family support Support 7 (58) 5 (42) 1.26 0.761 No support 122 (64) 69 (36) (0.30 - 4.82)
Surgery type Emergency 17 (90) 2 (10) 5.46 0.013 Elective 112 (61) 72 (39) (1.23 - 49.9)
Primary disease Cancers 81 (58) 58 (42) 2.15 0.028 Others 48 (75) 16 (25) (1.07 - 4.45)
Concomittant disease Yes 30 (83) 6 (17) 3.43 0.007 No 99 (59) 68 (41) (1.30 - 10.6)
Health insurance No 120 (67) 60 (33) 3.11 0.020 Yes 9 (39) 14 (61) (1.17 - 8.60)
Sexual issue after surgery No 115 (67) 56 (33) 2.64 0.012 Yes 14 (44) 18 (56) (1.14 - 6.16)
Postoperative depression Yes 33 (81) 8 (19) 2.83 0.011 No 96 (59) 66 (41) (1.18 - 7.53)
Support group No 121 (67) 61 (33) 3.22 0.016 Yes 8 (38) 13 (62) (1.16 - 9.43)
Difficult ostomy location Yes 113 (70) 48 (30) 3.87 < 0.001 No 16 (38) 26 (62) (1.78 - 8.32)
Changing diets Yes 113 (68) 53 (32) 2.80 0.007 No 16 (43) 21 (57) (1.27-6.21)
Duration of ostomy care ≥60minutes 106(74) 37(26) 4.61 < 0.001 < 60 minutes 23 (38) 37 (62) (2.31-9.22)

Chinh ND, et al. Thai J Surg Oct. - Dec. 2019100
Having good knowledge and good self-care skills will make patients have more confidence and improved QoL. Visit costs are quite expensive, and buying ostomy bags for patients with permanent ostomy is a burden due to low incomes or living in disadvantaged areas. In a study by Bich Thuy (2016)2, many patients with ostomy lack both knowledge and practice in taking care of his/her ostomy. Therefore, they need support from health care workers. Other studies also show that not only do patients suffer from their ostomies but other concomit-tant illnesses are of concern and impact QoL3,12,13,14. Though in our study, most patient do not have health insurance, those who do have a significantly bet-ter QoL. Abraham, et al3 in 2014, showed that patients suffering from cancer have bipolar disorder. However, confidence, support from family and society can help improve QoL markedly13,15. In the present study, while family support did not significantly impact QoL, being supported by society seem important for QoL. Ostomy care influences QoL. In our study, difficult ostomy care, requiring longer time for care, were all associated with poor QoL. Finally, having an ostomy requires changes in diet, adversely affecting QoL, at least in the present study.
conclusIon Quality of life of patients having the ostomy is increasing of interest, and is an important part of medi-cal care. Our study clearly showed the impact of certain risk factors on QoL of ostomates. To improve QoL of these patients, issues to consider should include proper management of concomitant diseases, providing health insurance, advising sexual matters, handling postopera-tive depression, encouragement to join support groups, and training to care for difficult ostomies, as well as diet recommendations.
REFERENCES
1. Pham Thi Thanh Phuong. Related factors of self-care for de-pression, anxiety and quality of life among the COPD patients. Mahidol University: Master’s Thesis; 2017.
2. Luu Thi Bich Thuy. Effectiveness of guidance to ostomates in caring her/his ostomy. Hanoi Medical University: Master‘s Thesis; 2017.
3. Abraham KM, Miller CJ, Birgenheir DG, et al. Self-efficacy and quality of life among people with bipolar disorder, J Nervous Mental Dis 2014;202:583.
4. Anaraki F, Vafaie M, Behboo R, et al. Quality of life outcomes in patients living with stoma. Indian J Palliat Care 2012;18:176.
5. Aronovitch SA, Sharp, Harduar ML. Quality of life for patients living with ostomies: Influence of contact with an ostomy nurse. J Wound Ostomy Continence Nursing 2010;37:649-53.
6. Selected abstracts from the 22nd Biennial WCET Congress in Kuala Lumpur. WCET Journal 2018;38:36-43.
7. Institute City of Hope and Beckman Research. Quality of life Questionaire for a Patient with an Ostomy. California (USA): City of Hope National Medical Center; 2013.
8. Jansen L, Koch L, Brenner H, et al. Quality of life among long-term 5 years colorectal cancer survivor: Sytematic review. Eur J Cancer 2010;46:2879-88.
9. Karadag A, Mentes BB, Uner A, et al. Impact of stoma therapy on quality of life in patients with permanent colostomies or ileostomies, Int J Colorect Dis 2003;18:234-8.
10. Liao C, Qin Y. Factors associated with stoma quality of life among stoma patients. Intl J Nursing Sci 2014;1:196-201.
11. Rafii F, Naseh L, Yadegary MA. Relationship between self-efficacy and quality of life in ostomates. Iran J Nursing 2012;25:64-76.
12. Nair CK, George PS, Rethnamma KS, et al. Factors affecting health related quality of life of rectal cancer patients undergoing surgery. Indian J Surg Oncol 2014;5:266-73.
13. Neuman HB, Patil S, Fuzesi S, et al. Impact of a temporary stoma on the quality of life of rectal cancer patients undergoing treatment. Ann Surg Oncol 2011;18:1397-403.
14. Nichols TR. Quality of life in persons living with ostomy as-sessed using the SF36 v2. J Wound Ostomy Continence Nursing 2016;43:616-22.
15. Nugent KP, Daniels P, Stewart B, et al. Quality of Life in stoma patients. Dis Colon Rectum 1999;42:1569-74.

IntroductIon
Breast cancer is a heterogenous disease with vary-ing morphology, behavior, and response to therapy. In 2003, the WHO defined invasive papillary carcinoma of breast as a type of invasive mammary carcinoma1. Papillary carcinoma of breast represents 0.5% of
newly diagnosed of breast cancers2,3,4. The term papil-lary carcinoma encompasses a morphologically hetero-geneous group of lesions which share growth pattern characterized by the presence of fibrovascular stalks lined by epithelial cells4. Malignant papillary neoplasm of the breast includes DCIS which arises in intraductal
The THAI Journal of SURGERY 2019;40:101-106.Official Publication of the Royal College of Surgeons of Thailand
101
Prognosis and Clinical Outcome of PapillaryCarcinoma of The Breast at A Tertiary CareHospitalRupporn Sukpanich, MD*
Panuwat Lertsithichai, MD*
Prakasit Chirappapha, MD*
Ronnarat Suvikapakornkul, MD*
Yodying Wasuthit, MD*
Thongchai Sukornyothin, MD*
Sansanee Wongwaisayawan, MD†
Monchai Leesombatpaiboon, MD*
*Breast and Endocrine Surgery Unit, Department of Surgery, Ramathibodi Hospital†Department of Pathology, Ramathibodi Hospital
Abstract Objective: To determine the clinical, pathologic and prognostic features of papillary breast cancer seen at a tertiary care hospital.
Materials and Methods: A retrospective review of medical charts of patients seen during the period between January 2010 to December 2013 was performed.
Results: There were 86 patients with papillary breast cancer who underwent surgery during the period. This constituted 3% of all breast cancer patients who underwent surgery during the same period. The majority (74%) were invasive papillary cancers. Most patients were menopausal with an average age of 61 years. Most cancers were hormone-receptor positive, and HER2 negative. The average tumor size was 2 cm and only 10% had axillary node metastasis. The majority (69%) underwent mastectomy and most (60%) had hormonal therapy as the only systemic adjuvant. Under a median follow-up of 22 months (range; 1 to 53 months), there were no recurrences or deaths observed in the series.
Conclusion: Papillary breast cancer has a very good prognosis and treatment should be minimized in a similar way as a mucinous carcinoma.
Keywords: Papillary breast cancer, Papillary lesions, Prognosis
Original Article
Correspondence address: Monchai Leesombatpaiboon, Breast and Endocrine Surgery Unit, Department of Surgery, Ramathibodi Hospital; Email:

Sukpanich R, et al. Thai J Surg Oct. - Dec. 2019102
papilloma, papillary DCIS, intracystic (encapsulated) papillary carcinoma, solid papillary carcinoma and invasive papillary carcinoma4-7. All malignant papillary neoplasms of the breast lack an intact myoepithelial cell layer within the papillae, which differentiates them from intraductal papilloma. Proposed criteria for DCIS arising in a papillary lesion include the presence of DCIS greater than 3mm in size8, and DCIS comprising at least a third but less than 90% of the papillary lesion7. The area of DCIS usually composes of uniform appearing cells with low or intermediate nuclear atypia. Papillary DCIS is characterized by the presence of fibrovascular fronds lined by neoplastic epithelium with no pre-existing benign papilloma. The lining epithelium is typically monomorphic, stratified columnar cells. Nuclei are usually of low or intermediate grade. There are no myoepithelial cells in the papillae, but this layer is retained at periphery of the involved duct. Intracystic (encapsulated) papillary carcinoma is a solitary, centrally located malignant papillary pro-liferation involving a dilated duct. The duct is filled with slender fibrovascular stalks lacking myoepithelial cells. The involved duct is surrounded by a thick fibrous capsule, also without a myoepithelial cell layer, leading some investigators to propose that this lesion should be considered invasive rather than in situ. On the other hand, some consider the lesion in situ based on the presence of basement membrane (collagen type IV) and the indolent behavior of the lesion9. Some intracystic papillary car-cinoma may be associated with an invasive component characterized by an infiltrative appearance with exten-sion beyond the fibrous capsules and associated stromal reaction. In these cases, it is recommended that the stag-ing should be determined based on the size of invasive component only, in order to prevent overtreatment4-6. Solid papillary carcinoma appears as a well cir-cumscribed, densely cellular, expansile nodules of epi-thelial cells. Extra and intracellular mucin production are common, and there is an underlying fibrovascular core. Solid papillary carcinoma is often accompanied by an area of invasive carcinoma (usually mucinous or neuroendocrine-like carcinoma)4,10,11. The diagnosis of Invasive papillary carcinoma is extremely rare and should be reserved for infiltrating breast carcinoma exhibiting papillary morphology. This invasive lesion tends to be found in older women, typi-cally aged 70 years or more12. These patients are older
than those with the more common breast cancer and papillomas. Clinically apparent papillary lesions will present with a breast lump or bloody nipple discharge. These lesions may also be asymptomatic, but detectable on screening mammography or ultrasonography. Differen-tiating between benign and malignant lesions via core biopsies may be difficult because the invasive part is seen at the periphery, while biopsies are targeted at the center. On breast imaging findings, there are three basic ultrasonographic profiles: intraductal mass with or without duct dilatation; intracystic mass; and, solid pattern with an intraductal mass completely filling the duct. Papillary carcinomas are noted to have a larger solid component and spontaneous intracystic bleeding. In both benign and malignant lesions, the shape of the lesion is often round or oval, and with circumscribed margins. However, nonparallel orientation, an echogenic halo, posterior acoustic enhancement and associated microcalcification are more frequently found in malig-nant lesions4. Mammographic findings usually show a well circumscribed and homogenous mass, although sometimes the border may be obscured. Malignant and benign lesions often cannot be distinguished by the mammography. The prevalence of malignancy on surgical excision for papillary lesions found on core needle biopsy ranges from 17 to 34%13. Excisional biopsy should be done for all papillary lesions diagnosed on needle biopsy due to a high upgrade rate to malignancy. Available data suggests better outcome for papil-lary carcinoma compared to non-specific invasive ductal carcinoma, but treatment related information is limited. The lack of information underscores the need for treat-ment and outcome related studies in papillary carcinoma of the breast. Because of its relative rarity, there is a paucity of information regarding this type of tumor. Most previous studies are based on small case series. In the present study, we reviewed 86 patients with papillary carcinoma, including both invasive and noninvasive types, in terms of clinicopathologic findings, molecular immunohis-tochemistry, and overall disease-related outcomes at a single institute.
MaterIals and Methods
Medical charts of patients diagnosed with malig-

Prognosis and Clinical Outcome of Papillary Carcinoma of The Breast at A Tertiary Care HospitalVol. 40 No. 4 103
Table 1 Summary of patient and pathological characteristics
Characteristics Summary (n = 86 unless stated otherwise)
Age (years): mean (SD) [range]Core Needle Biopsy diagnosis (n = 62) (%) Papillary cancer Invasive mammary cancer Ductal carcinoma in situ Papillary lesion with atypia Papillary lesion InflammationandfibrocysticchangeInitialexcisionalbiopsyNumberofoperations(%) One Multiple (re-excision or mastectomy)Definitivebreastsurgery(%) Mastectomy Breast conserving surgeryInvasive papillary cancer (%) Microinvasive papillary cancer Mixed papillary cancer (%) With ductal carcinoma, NOS With mucinous carcinomaSize of primary tumor (cm); n = 78 Mean (SD) Median (range)Axillary nodes evaluated (%) Positive axillary nodes (%)Estrogen receptor expression (%) Mean (SD) Median (range)Progesterone receptor expression (%) Mean (SD) Median (range) Ki 67 (%); n = 80 Mean (SD) Median (range)HER2/neu expression; n = 84 (%) 0 1+ 2+ 3+Triple negative cancer
nant papillary carcinoma of breast treated at Ramathibodi Hospital from January 2010 to December 2013 were reviewed. Patients with the diagnosis of micropapillary carcinoma or those with incomplete clinicopathologic information were excluded. All patients underwent clinical examination and mammographic and ultrasound evaluation before
the surgery. Preliminary tissue diagnosis was usually done with core needle biopsy (Ramathibodi Hospital), although a few was done via excisional biopsy (from outside institutions). All patients received standard surgical management either with mastectomy or breast conserving surgery, and axillary management depending on nodal status.
61.7 (13.9) [31 to 90]
25/62 (40)11/62 (18)6/62 (10)11/62 (18)5/62 (8)4/62 (6)24 (28)
54 (63)32 (37)
59 (69)27 (31)64 (74)
8/64 (13)28 (33)
21/28 (75)10/28 (36)
2.2 (1.4)2.0 (0.2 to 7.0)
71 (83)7/71 (10)
84.2 (21.8)90 (0 to 100)
52.2 (36.5)60 (0 to 100)
18.8 (15.1)15 (2 to 80)
43/84 (51)20/84 (24)19/84 (23)
2/84 (2)2 (2)

Sukpanich R, et al. Thai J Surg Oct. - Dec. 2019104
Table 2 Adjuvant treatment, follow-up and outcomes of patients with papillary cancer
Treatment and outcomes Summary (n = 85 unless stated otherwise) *
Chemotherapy; n = 84 (%) None 4AC 4AC+12P 6FAC 6CMF 4TCRadiation therapy; n = 84 (%)Hormonal treatment; n = 84 (%)Hormonal treatment only; n = 84 (%)Follow-up time (months) Mean (SD) Median (range)Recurrent cancerCancer-related deaths
* One patient was lost to follow-up
Adjuvant treatment was given based on prognostic and predictive factors such as tumor size, estrogen receptor status, HER2 status and nodal status. Information retrieved from medical records in-cluded patient-related data (age at diagnosis, menopausal status), tumor characteristics (size, grade, ER, PR and HER2 status with associated percentages), surgical treat-ment, nodal status, type of adjuvant systemic treatment, radiation therapy, date of last follow-up, and disease status or survival at last follow-up. The study protocol was approved by the Ethics Committee of Ramathibodi Hospital. Statistical comparison between independent groups or categories was done using t-test, rank test, chi-square test, or Fisher’s exact test as appropriate. The statistical software Stata v. 12 (Stata Corp., College Station, USA) was used for all analyses.
results Most of the patients were postmenopausal, with a median age of 61 years (range, 31 to 90 years; see Table 1). No male papillary breast cancer was seen in the pe-riod under study. The majority of papillary breast cancer was invasive (74%). There were 28 patients (33%) with mixed type carcinoma. These were either with invasive ductal (74%) or mucinous carcinoma (36%). In the present study, no co-existence between the papillary carcinoma and neuroendocrine tumor was found.
The average tumor size was 2.2 cm. The Estro-gen Receptor (ER) was positive in 97% of papillary carcinomas, with an average ER expression of 84.2%. Expression of Ki67 was low, with an average of 18.8%. HER2 expression was negative (IHC 0 or 1+) in 75 % of patients, with the rest being mostly equivocal (IHC 2+; 23%). Confirmatory tests such as FISH was not done in most of these latter cases because of the small size of the tumor and treatment with Trastuzumab was not con-sidered necessary. Only 2 invasive papillary carcinomas were found to be HER2 positive (IHC 3+) in the present study. However, these two patients had mixed invasive papillary and ductal carcinoma, so HER2 positivity could be from the invasive ductal part. Among the 86 patients in the present study, 27 (31%) underwent breast conserving therapy (BCT), and 59 (69%) underwent mastectomy. Some patients (37%) underwent secondary surgeries because their first op-erations were not able to completely remove the tumor. Sentinel lymph nodes biopsy (SLNB) was performed for clinically node negative breast cancer. In 71 patients, a dual technique consisting of a blue dye and radioisotope injection was used to identify the SLN’s. There were 7 patients (10%) with positive SLNB. Patients who had macrometastasis in the sentinel nodes underwent axillary node dissection, but no additional positive nodes were found in all cases. In 3 patients with micrometastasis on SLNB, axillary dissection was omitted.
63/84 (75)11/84 (13)1/84 (1)6/84 (7)2/84 (2)1/84 (1)
19/84 (23)79/84 (94)50/84 (60)
24.1 (12.7)22.2 (1.0 to 52.7)
00

Prognosis and Clinical Outcome of Papillary Carcinoma of The Breast at A Tertiary Care HospitalVol. 40 No. 4 105
Adjuvant treatment was given based on tumor bi-ology, staging, and surgery performed. Only 4 patients received no adjuvant treatment after surgery. Of these, 2 were lost to follow up, and the remaining 2 refused any adjuvant treatment. Chemotherapy was given based on tumor staging and biology. Anthracycline-based regimen was the main regimen in the study (as shown in the Table 2). Hormonal treatment, either with tamoxifen or an aromatase inhibitor, was prescribed for most patients (94%) due to the vast majority having ER-positive tumor. Over half (60%) of patients received hormonal treatment as their only adjuvant treatment. Radiation therapy (RT) was provided for 19 (23%) patients, 15 of whom had undergone BCT. Patients who underwent BCT with and without whole breast RT were compared (Table 3). RT was omitted in patients who were older and frail, some with smaller tumors, such that axillary surgery was usually omitted as well and hormonal therapy was likely given as the only adjuvant treatment. Patients were followed every 3 to 6 months in the first 5 years. The median follow-up time was 22 months (range, 1 to 53 months). No recurrences, both local and distant, were found in any patient in the study, and no cancer related deaths were observed.
dIscussIon
In the present study, the proportion of papillary carcinoma was approximately 3% of all breast cancers undergoing surgery, a relatively high proportion. Simi-larly, although the published literature suggests true in-vasive papillary carcinoma to be rare (e.g., 1 to 2%), the present study found a much higher proportion of invasive papillary carcinoma. There is no clear explanation as to
why this was the case, although the overdiagnosis of invasiveness is one explanation. Nonetheless, most of the patients in the present study were predominantly post-menopausal, which was consistent with previous studies. Papillary carcinomas in the present study were found to be mostly ER positive and HER2 negative, also consistent with previous reports. A novel finding was that IHC HER2 equivocal or positive papillary cancers were often in association or mixed with invasive ductal carcinoma. Previous reports suggest that invasive papillary carcinomas are less aggressive, with better prognosis compared to invasive ductal carcinoma of no special type. But due to the relative rarity of this type of cancer, no clear conclusions could be found in the literature. The present study seems to show that all papillary cancers, including invasive types, have very good prognosis under the current standard treatment regimen, with no cancer recurrence or cancer-related deaths observed in all patients, although the follow-up period was rather short. A significant proportion of patients underwent BCT without whole breast irradiation, and no recur-rences were detected within the follow-up period. Other studies concluded that solid papillary carci-noma was closely related to mucinous carcinoma14. In the present study, the coexistence with mucinous carci-noma, for both in situ and invasive papillary cancers, was also seen. This evidence, along with the estimated low incidence of cancer recurrence and mortality, and the fact that most of the tumors were ER positive and HER2 negative, suggests that invasive papillary carcinoma of the breast has a very good to excellent prognosis, similar to that of mucinous carcinoma. This leads to the recommendation that the treatment of most papil-
Table 3Comparingpatientswithbreastconservingsurgerywhodidordidnotundergowholebreastirradiation
Characteristic and Treatment RT (n = 15) No RT (n = 11) p-valuea
Age (years): mean (SD) 54.6 (11.1) 72.0 (16.1) < 0.001Size (cm): median (range) 1.9 (0.4 to 6.0) 0.8 (0.2 to 4.7) 0.312ER expression (%): median (range) 95 (80 to 100) 90 (0 to 100) 0.133PR expression (%): median (range) 80 (5 to 95) 30 (0 to 100) 0.215Ki67: median (range) 20 (2 to 40) 15 (5 to 60) 0.916HER2/neu expression: median (range) 0 (0 to 2+) 1+ (0 to 2+) 0.692Axillary nodes evaluated (%) 13 (87) 1 (9) < 0.001Hormonal treatment only (%) 0 10 (91) < 0.001
a: p-valueaccordingtot-test,ranktest,chi-squaretest,orFisher’sexacttestasappropriate;RT:wholebreastradiationtherapy

Sukpanich R, et al. Thai J Surg Oct. - Dec. 2019106
lary carcinomas of the breast could be limited to local and hormonal treatment. However, these observations require further confirmation. Major limitations of the present study included the possibility of overdiagnosis of the invasiveness of papillary carcinoma, and the short period of follow-up. Also, treatment recommendations made have never been tested. But the present results strongly suggest very good prognosis for this type of cancer, and the idea of mini-mizing the use of chemotherapy or other toxic systemic treatment should be carefully considered.
conclusIon
The present study found a higher proportion of invasive papillary carcinoma of the breast compared to other studies. The prognosis of this type of breast cancer was found to be very good to excellent. It is suggested that invasive papillary carcinoma should be considered a good prognosis subtype and treatment could be mini-mized accordingly.
REFERENCES
1. Liu ZY, Liu N, Wang YH, et al. Clinicopathologic character-istics and molecular subtypes of invasive papillary carcinoma of the breast: a large case study. J Cancer Res Clin Oncol 2013;139:77-84.
2. Fisher ER, Palekar AS, Redmond C, et al. Pathologic findings from the National Surgical Adjuvant Breast Project (proto-col no. 4) VI. Invasive papillary cancer. Am J Clin Pathol 1980;73:313-22.
3. Gentile A, Becette V. Invasive papillary and pseudopapillary (micropapillary) carcinoma of the breast. Arch Anat Cytol Patho 1996;44:225-30.
4. Pal SK, Lau SK, Kruper L, et al. Papillary carcinoma of the breast: an overview. Breast Cancer Res Treat 2010;122:637-45.
5. Mulligan AM, O’Malley FP. Papillary lesions of the breast: a review. Adv Anat Pathol 2007;14:108-19.
6. Collins LC, Schnitt SJ. Papillary lesions of the breast: selected diagnostic and management issues. Histopathology 2008;52: 20-9.
7. Ueng SH, Mezzetti T, Tavassoli FA. Papillary neoplasms of the breast: a review. Arch Pathol Lab Med 2009;133:893-907.
8. Page DL, Salhany KE, Jensen RA, Dupont WD. Subsequent breast carcinoma risk after biopsy with atypia in a breast papil-loma. Cancer 1996;78:258-66.
9. Esposito NN, Dabbs DJ, Bhargava R. Are encapsulated papil-lary carcinomas of the breast in situ or invasive? A basement membrane study of 27 cases. Am J Clin Pathol 2009;131:228-42.
10. Maluf HM, Koerner FC. Solid papillary carcinoma of the breast. A form of intraductal carcinoma with endocrine differentiation frequently associated with mucinous carcinoma. Am J Surg Pathol 1995;19:1237-44.
11. Nassar H, Qureshi H, Volkanadsay N, Visscher D. Clinicopatho-logic analysis of solid papillary carcinoma of the breast and as-sociated invasive carcinomas. Am J Surg Pathol 2006;30:501-7.
12. Koerner F. Papilloma and papillary carcinoma. Semin Diag Pathol 2010;27:13-30.
13. Jakate K, De Brot M, Goldberg F, et al. Papillary lesions of the breast: impact of breast pathology subspecialization on core bi-opsy and excision diagnoses. Am J Surg Pathol 2012;36:544-51.
14. Oh EJ, Koo JS, Kim JY, Jung WH. Correlation between solid papillary carcinoma and associated invasive carcinoma accord-ing to expression of WT1 and several MUCs. Pathol Res Pract 2014;210:953-8.

IntroductIon Nutrition Screening (NS) and Nutrition Assessment (NA) are the initial steps in the Nutrition Care Process (NCP). In the past, these procedures were seldom per-formed for hospitalized patients due to lack of interest and knowledge. In 2000, the BNT format (Bhumibol Adulyadej Hospital Nutrition Triage) was developed and proposed for NA and was widely adopted in many hospitals in Thailand1-6. Later, BNT was replaced by the NT 2013 format, to conform with the Consensus State-ment 2012 of A.S.P.E.N., ESPEN, and the Academy of Nutrition and Dietetics on Identification of Adult Malnutrition7-10.
Recently, the Society of Parenteral and Enteral Nutrition of Thailand (SPENT) has obtained the support from the Ministry of Public Health (MOPH) to set up “A Qualified Nutrition Support Hospital” and establishing Nutrition Support Teams in hospitals. Simultaneously the National Health Security Office (NHSO) also sup-ports the adoption of NT 2013 format and allows for cost reimbursement relating to the malnutrition diagnosis based on NT 2013 format11. These two activities have built up the interest and growth in NCP among medical personnel nation-wide. A study by a group of investigators, reported by Health Intervention and Technology Assessment Program - HI-
The THAI Journal of SURGERY 2019;40:107-116.Official Publication of the Royal College of Surgeons of Thailand
107
NT 2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in ThailandBuchcha Prammanasudh, RNVibul Trakulhoon, MDDepartment of Surgery, Bhumibol Adulyadej Hospital, Bangkok
Abstract Nutrition Screening (NS) and Nutrition Assessment (NA) are the initial steps in Nutrition Care Process (NCP). In 2000, the BNT format (Bhumibol Adulyadej Hospital Nutrition Triage) was proposed and was widely used in many hospitals for NS and NA in Thailand. Later, the BNT was updated and became the NT 2013 format in conformance with the Consensus Statement 2012 of A.S.P.E.N., ESPEN, and the Academy of Nutrition and Dietetics on Identification of Adult Malnutrition. Recently, the Society of Parenteral and Enteral Nutrition Sup-port of Thailand (SPENT) was supported by the Ministry of Public Health (MOPH) to initiate “The Qualified Nutrition Support Hospital” project, to encourage the establishment of Nutrition Support Teams at various hospi-tals. Subsequently the National Health Security Organization (NHSO) began allowing hospitals to file claims for reimbursement for the cost of implementing the new Nutrition Care Process within the NT 2013 format. Also, as an endorsement of the NT 2013, a study by a group of investigators, reported by HITAP has recommended the NT format to be used for NS and NA in Thailand.
Keywords: Nutrition screening, Nutrition assessment, BNT-NT 2013 nutrition assessment form
Review Article
Correspondence address: Vibul Trakulhoon, MD, Department of Surgery, Bhumibol Adulyadej Hospital, Bangkok; Email: trakulhoonvbt@gmail.
com

Prammanasudh B, Trakulhoon V Thai J Surg Oct. - Dec. 2019108
TAP12 has recommended the NT 2013 format to be used for NS and NA in Thailand.
The Consensus Statement 2012 Of A.S.P.E.N., ESPEN, and The Academy of Nutrition and Dietetics On Identification of Adult Malnutrition7-10
The Consensus Statement had divided the etiology of malnutrition into three categories: starvation-related malnutrition; chronic disease or inflammation related malnutrition; and, acute illness or acute injury related malnutrition (hypermetabolism and hypercatabolism). The authors also proposed six criteria to identify adult malnutrition: 1) History of inadequate diet or nutrient intake 2) Decrease body weight 3) Accumulation of fluid or edema 4) Loss of body fat 5) Loss of body muscle 6) Loss of muscle strength Thus, all of these criteria are modified to be used by the NT 2013 format.
Suggestion of The Consensus Statement7
The authors placed emphasis on patient-specific definitions, the effect of inflammation, and also the three related etiologies of malnutrition. The following points were suggested for consideration. 1. The meaning of adult malnutrition and under-nutrition is the same. 2. History of illness and Diagnosis are useful for identification of a patient’s status. 3. Physical examination can reveal the func-tional and nutritional status. 4. Malnutrition is not correlated with BMI; both too low and too high BMI may increase risk. 5. The amount of caloric intake should be monitored. 6. Inflammatory conditions increase the risk of malnutrition. 7. No definite inflammatory indicator is pro-posed for diagnosis. 8. Serum albumin/prealbumin are not related to malnutrition, but inflammation. 9. Follow up and appropriate reassessment is better than any single measure. 10. Chronic illness is one lasting at least three months (National Center for Health Statistics). 11. Nutritional assessment in certain conditions
should be done carefully. For example, an 80 to 90-year-old patient who looks healthy and can take an optimal amount of diet (i.e., less than generally recommended) may weigh less than the ideal body weight but is optimally active. Thus, to diagnose the patient as malnourished is not appropriate.
NT 2013: A Nutrition Screening and Nutrition Assessment Format NT 2013 is a scored nutrition evaluation tool con-sisting of two parts: Nutrition Screening and Nutrition Assessment. The parameters correspond to those of the Consensus Statement of 2012. We also include ECOG (Eastern Cooperative Oncology Group) and Karnofsky Performance Status scoring system which are widely used for evaluation of performance status among can-cer patients. The ECOG scale, now part of the ECOG-ACRIN Cancer Research Group, was published in 1982. It is in the public domain and is therefore available freely for public use. It is displayed below both for future refer-ence and to spur further standardization among research-ers who design and evaluate cancer clinical research13.
Figure 1 ECOG Performance Status and grading
Nutrition Screening There are four yes/no questions to be answered during screening. These are: 1. Decreasing diet or nutrient intake during the past seven days or more?

NT 2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in ThailandVol. 40 No. 4 109
2. Decreasing body weight during the past six months? 3. BMI less than 18.5 or more than 24.9? 4. Presently having critical illness or serious injury? Answering yes to any of the above questions sug-gests that there are abnormalities. Two or more yes’s require that the patient proceeds to Nutrition Assessment to obtain additional detailed information. Generally, the concept of screening parameters should be simple, use little time, and sufficiently informative to determine whether a patient requires further assessment. Para- meters most frequently used are BW or BMI. We may also add one or two more questions, and the more ques-tions the more reliable the result, although possibly unnecessarily time consuming. However, from our study, four questions give sufficient reliability to screen for patients at risk, especially in the context where there may not be sufficient time to apply NA.
Nutrition Assessment The concepts of NA are: 1. The inclusion of various relevant causes. 2. Each cause should be classified along with a degree of adverse effect on the patient, combined into a scoring system. 3. The severity scores of the diseases or harmful conditions should not be constant or a fixed number, but should correlate with disease status. The NT format follows the above concepts carefully to prevent oversensitivity and low specificity in detecting malnutrition risk. The format includes nine items used to assess patient conditions and evaluations for the purpose of weighing and scoring the risk of malnutrition effect on the patient. The severity of related causes can be scored in the following way: 1) a score of 0 means no disease or not at risk 2) a score of 1 means little or mild adverse effect 3) a score of 2 means moderately harmful 4) a score of 3 means severely affected The final score is the sum of scores from item 1 to item 8 below and can then be classified into four levels of nutrition status, in item 9. These are: NT-1 (score 0-4) means no malnutrition or at risk NT-2 (score 5-7) means mild malnutrition NT-3 (score 8-10) means moderate malnutrition
NT-4 (score > 11) means severe malnutrition
Item 1: History of Diet or Other Nutrients Intake We have to find out the patient’s real intake and not only rely on the physician’s prescription. To assess the abnormality of nutrient intake, four aspects should be integrated, these are: the type, the amount, the quality, and the duration of related inappropriate dietary intake. The type of food is different in nutritional value, for example: regular diet, soft diet, liquid diet or only some snack, fruits or juice. The amount of intake should not be subjective such as: can take some food, just a small amount, but should be an objective view such as: 75-100 %, 25-50 %, less than 10 % of usual, or just only 3-4 spoons of a meal or the patient is on NPO (nothing per oral) and on IV fluid. The quality of food should be considered: low in calorie and/or protein or inappropriate compositions of nutrients. The duration of inappropriate diet intake, in days, weeks or months; the longer the time, the more the ad-verse effect. These four pieces of information are integrated to form a score for severity of the patient’s status. Extra care should be taken when assessing the following patients. Patients who are on NG tube feeding with adequate quantity of blenderized diet (BD), are usually not abnormal. Patients who are on liquid diet may be misinterpreted for taking low quality meal. Also make sure before scoring the abnormality whether the patient is having the medical food formula. Patients who are on parenteral nutrition may receive adequate energy, protein, and other nutrients.
Item 2: Unintentional Loss of Body Weight (BW) There are generally three aspects of BW (kg). The usual BW is the BW when the patient is in a good health or normal health or at the early beginning of illness. The current BW is the BW when the patient is seen or recent BW (not excluding the edema or ascites status or tumor mass). The ideal BW is the calculated BW obtained from the patient’s height in centimeter minus 100 in men or 105 -110 in women. IBW can be calculate from the equation. For men: IBW (kg) = 50.0 + [0.91 x [height (cm) -152.4]] For women: IBW (kg) = 45.5 + [0.91 x [height

Prammanasudh B, Trakulhoon V Thai J Surg Oct. - Dec. 2019110
(cm) - 152.4]]14
To assess the amount and degree of BW change we should consider: 1. The Amount of weight loss can be calculated by UBW minus CBW. 2. The Weight loss as a percentage can be cal-culated by {(UBW-CBW) / UBW} x 100. 3. The Duration of weight loss in terms of weeks or months. Sometimes when the BW cannot be obtained due to non-weighing for a long time. We can consider whether the CBW is less than IBW by at least 20% or CBW is less than previous year’s BW of about 20% or more. These two aspects can be considered to be severe changes in BW. BMI, like a BW measurement is a simple and use-ful parameter but with several limitations. High BMI represents excess amount of fatty tissue but not the muscular component of the body. Normal BMI does not exclude malnutrition. BMI less or greater than normal range may both indicate malnourished risk. However low BMI should be interpreted carefully in conjunction with performance status, occupation, and race; for example, marathon runners, ballet dancers, jockeys (horse racing), and Asians may have low BMI without malnutrition.
Item 3: Edema or Accumulation of Fluid There are two types of edema of the body. The localized form is usually related to local causes, and in general the adverse effect is less than that of the general form. Examples of localized edema include a right lower leg edema from deep vein thrombosis, or a left arm edema postmastectomy with axillary lymph node dissection. The generalized form is usually more important as it is related to systemic causes. Examples include pitting edema over both lower legs and arms or facial edema. The cause may be from heart failure, liver dis-ease, chronic kidney disease or malnutrition. Physical examination can differentiate the degree of edema. By applying finger pressure on the affected part for about 5 seconds, and assessing the depth of the cutaneous pitting, 2, 4, 6, or 8 mm depth corresponds to 1+, 2+, 3+, or 4+ degree of edema, respectively. The assessment of severity of edema by a more common scoring system uses scores 0, 1, 2, and 3, where a score of 0 refers to no edema, a score of 1 or 2 means mild or moderate edema, and a score of 3 means severe edema.
Figure 2 Degree of edematous skin = 3+ (abdominal wall & both lower legs); severity score = 3
Figure 3 Evaluation of the subcutaneous fat of the body

NT 2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in ThailandVol. 40 No. 4 111
Item 4: Assessment of Body Fat Loss Physical examination should be done carefully to assess the subcutaneous fat; at the temporalis area, eye-lids, cheeks, chest wall, prominent clavicle, subclavicu-lar skin fold and ribs, abdominal wall, arms especially biceps and triceps skin folds, hands, pelvis, and lower extremities. Skin calipers are infrequently used for this examination. Other related factors or information to be included when determining the severity of body fat loss are the loss of BW, thin appearance, decrease in size of the body and extremities, looseness of clothing, watch and ring etc. Then the appropriate severity score of edema will be selected as 0, 1, 2, 3.
Item 5: Assessment of Muscle Loss The assessment process consists of visual inspec-tion, manual palpation, and estimating the size and contour of individual muscles. The procedure can be done simultaneously with and is similar to assessment of body fat loss. The overall status of body muscle loss is assessed similarly with a severity score of 0, 1, 2, or 3; as in Figure 4.
Item 6: Assessment of Muscle Strength Practically, we can assess the overall muscle strength by patient’s general appearance and activity as defined by ECOG or Karnofsky scores. Physical examination can obtain more information from his or her self-movement and the ability to resist active force. Spontaneous movements of extremities, hands, and neck should be noted, for example. The active parts should be evaluated but not the diseased component. Some authors suggest testing muscle strength by hand-grip dynamometer (HGD). However, there are some disad-vantages of using such devices, such as requiring the patient’s cooperation, limited application to a few parts of the body, the lack of standardization, inconvenience, and the high cost of the device. The muscle strength may be classified into six grades of 0, 1, 2, 3, 4, 515 as shown in the chart below.
Item 7: Assessment of the Chronic Diseases and Severity This item consists of various chronic diseases of medical and surgical conditions. The Consensus State-ment suggests that a chronic disease should be at least of six months’ duration. We propose some criteria to be considered before scoring each condition.
Figure 4 Evaluation of subcutaneous fat and muscle mass and the degree of muscle mass deficit
Figure 5 Physical examination to assess muscle strength
Evaluation of Subcutaneous Fat Evaluation of Muscle Mass 0 = no deficit, 1+ = mild deficit, 2+ = moderate deficit, 3+ = severe deficit

Prammanasudh B, Trakulhoon V Thai J Surg Oct. - Dec. 2019112
1. The harmful effect of the diseases to the body on nutrition status, the hypermetabolism or hypercatabolism effects are not constant but vary with the stage of disease and the treatment process. 2. The severity scores of the chronic disease are 0 for no disease or no risk; 1 and 2 for mild and moderate risk respectively, and 3 for high risk. 3. When scoring for multiple diseases or condi-tions, the final sum of score should not be higher than three to prevent over-sensitivity and low specificity. The following are examples for consideration. 1) Solid cancer. The harmful effects are related to stage 1, 2, 3, 4 of disease so the severity score is not constant or fixed. The scores 0, 1, 2, 3 should be care-fully selected to match the disease status.
2) Pulmonary diseases. For example, COPD16,
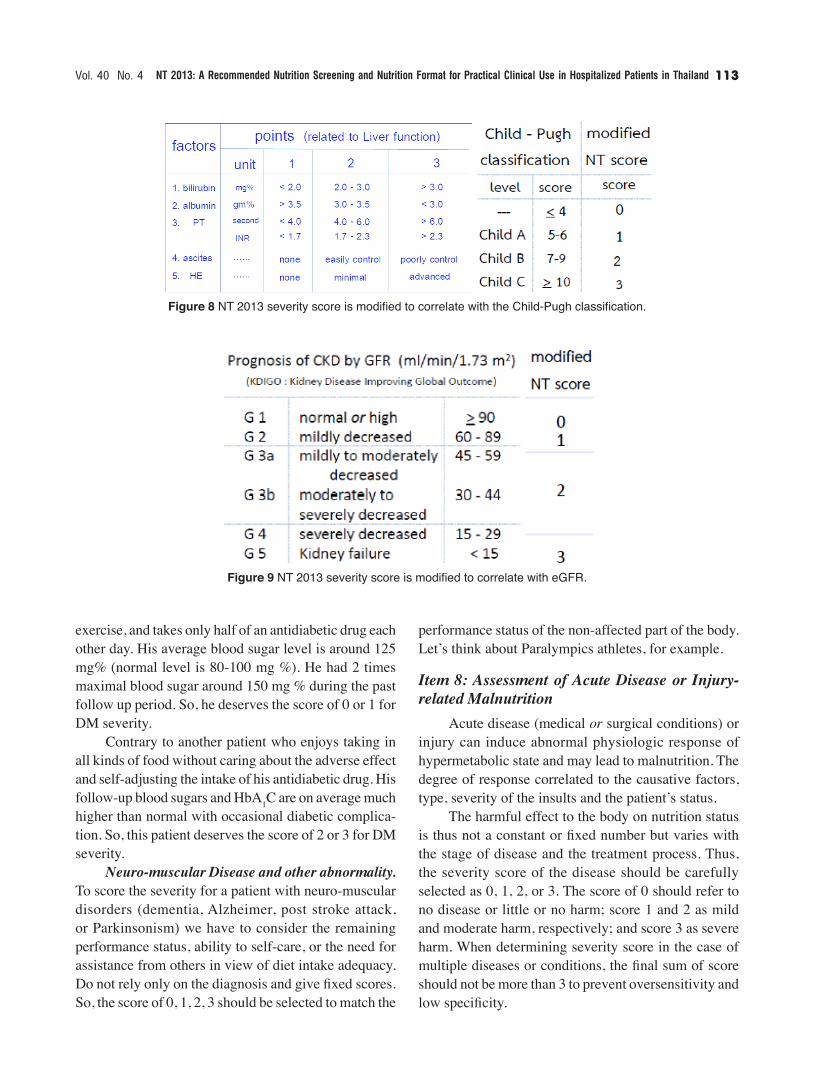
TB, chronic bronchitis will affect the lung tissue and decrease the efficiency of lung function, which is related to stage of disease and result of treatment. To score the severity of pulmonary function status, we modified the CAT (COPD-severity-assessment test) based on the mMRC (modified Medical Research Council) Dyspnea scale, which provides a single number for the degree of breathlessness. The severity score in NT format is modified to incorporate mMRC scale as in Figure 7. 3) Liver disease17. To score the severity of liver function status, we modified the NT score to correspond to the Child - Pugh classification as shown in Figure 8. 4) Kidney Disease18. A patient with chronic kidney disease should have a deterioration of glomerular filtra-tion rate. The severity score in NT 2013 is modified to correspond to the various abnormal levels of eGFR, as in Figure 9. 5) Diabetes Mellitus. A diabetic patient who regu-larly keeps a good control of blood sugar or hemoglobin A1C level will have a reduced diabetic-related complica-tion. So, the scoring of disease severity should not be a constant or fixed number or just due to the diagnosis of DM, but instead it should be adjusted to blood sugar level and clinical manifestations. For example, a university teacher has been diag-nosed with DM for about five years. He always keeps a good diabetic care with regular diet control, frequent
Figure 6 NT 2013 severity score is modified to correlate with muscle strength
Figure 7 NT 2013 severity score is modified to correlate with mMRC Dyspnea scale.
NT 2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in ThailandVol. 40 No. 4 113
exercise, and takes only half of an antidiabetic drug each other day. His average blood sugar level is around 125 mg% (normal level is 80-100 mg %). He had 2 times maximal blood sugar around 150 mg % during the past follow up period. So, he deserves the score of 0 or 1 for DM severity. Contrary to another patient who enjoys taking in all kinds of food without caring about the adverse effect and self-adjusting the intake of his antidiabetic drug. His follow-up blood sugars and HbA1C are on average much higher than normal with occasional diabetic complica-tion. So, this patient deserves the score of 2 or 3 for DM severity. Neuro-muscular Disease and other abnormality. To score the severity for a patient with neuro-muscular disorders (dementia, Alzheimer, post stroke attack, or Parkinsonism) we have to consider the remaining performance status, ability to self-care, or the need for assistance from others in view of diet intake adequacy. Do not rely only on the diagnosis and give fixed scores. So, the score of 0, 1, 2, 3 should be selected to match the
performance status of the non-affected part of the body. Let’s think about Paralympics athletes, for example.
Item 8: Assessment of Acute Disease or Injury-related Malnutrition Acute disease (medical or surgical conditions) or injury can induce abnormal physiologic response of hypermetabolic state and may lead to malnutrition. The degree of response correlated to the causative factors, type, severity of the insults and the patient’s status. The harmful effect to the body on nutrition status is thus not a constant or fixed number but varies with the stage of disease and the treatment process. Thus, the severity score of the disease should be carefully selected as 0, 1, 2, or 3. The score of 0 should refer to no disease or little or no harm; score 1 and 2 as mild and moderate harm, respectively; and score 3 as severe harm. When determining severity score in the case of multiple diseases or conditions, the final sum of score should not be more than 3 to prevent oversensitivity and low specificity.
Figure 8 NT 2013 severity score is modified to correlate with the Child-Pugh classification.
Figure 9 NT 2013 severity score is modified to correlate with eGFR.

Prammanasudh B, Trakulhoon V Thai J Surg Oct. - Dec. 2019114
The following are examples for consideration. 1) Critically Ill Patients19. There are multiple scoring systems for assessment of severity of Illness, such as SOFA, APACHE, and SAPS. The SOFA score is used to evaluate six organ dysfunctions, graded from 0 to 4 and recently adapted to quickSOFA (qSOFA score) which is intended to screen patients for ICU admission. The higher the score the higher mortality rate. So, NT 2013 is modified to correlated with the qSOFA score (bedside score) to assess the severity of patient’s dys-functional status (Figure 10). 2) Sepsis20,21,22. In 2016 the Third International Consensus Definitions defined sepsis as a dysregulated host response to infection that leads to organ dysfunction and should be distinguished from uncomplicated infec-tion. Septic shock is a subset of sepsis with circulatory and metabolic abnormalities. New sepsis-3 clinical crite-ria are suspected infection with acute organ dysfunction: defined as an increase by 2 or more points from baseline SOFA score. The criteria for septic shock include sepsis plus vasopressor resuscitation to increase MAP to > 65 mmHg with serum lactate > 2.0 mmol/L despite adequate fluid
resuscitation. The SOFA score has been simplified to qSOFA score. There are various studies in sepsis patients showing that the increase in scores correlated with the higher risk of in-hospital mortality. The qSOFA score may be used as screening criteria for transferring the patient to ICU. 3) Pneumonia23. The CURB-65 criteria (a sever-ity of illness score) include 5 variables: C=confusion; U = urea >7 mmol/L; R =respiratory rate > 30/min; B = SBP < 90 or DBP< 60; 65 = age > 65 years. The study found the relationship between total score and outcome as shown in Figure 11.
Figure 10 NT 2013 severity score is modified to correlate with qSOFA score.
Figure 12 NT 2013 severity score is modified to correlate with severity of Burn injury.
Figure 11 NT 2013 severity score is modified to correlate with CURB-65 score.

NT 2013: A Recommended Nutrition Screening and Nutrition Format for Practical Clinical Use in Hospitalized Patients in ThailandVol. 40 No. 4 115
Figure 13 NT 2013 severity score is modified to correlate with the extent of operations.
4) Burns 24,25 (Second degree or more severe burn). The pathophysiologic metabolic response varies with the degree of burns. The hypermetabolic and hyper-catabolic state increases with the extent of burn surface area. Generally, adult patients with BSA less than 15 % can be managed with oral hydration and intravenous fluid resuscitation is not necessary (Figure 12). 5) Recent Major Operation. Surgery can induce physiological and metabolic alteration in patients. The greater the extent of operation and complications, the greater the hypermetabolic - hypercatabolic response. Starvation-related conditions due to NPO may worsen the case. For patients who undergo a major operation without any adverse effect and not requiring ICU care, the severity score should be 1 or 2. But for a patient who had complications affecting the vital signs, the severity score should be 2 or 3 as correlated to the patient’s condi-tion. Figure 13, provides examples of various operations to be considered.
Item 9: Summation of total score and classification level of NT 2013 This last item is the summation of total score from item-1 to item-8. The final number of score will be used to indicate the level of nutrition status by NT 2013 which have been classified into 4 levels: NT-1 (score 0-4) = normal nutrition or just at risk; NT-2 (score 5-7) = mild malnutrition; NT-3 (score 8-10) = moderate; NT- 4 (score > 11) = severe malnutrition.
conclusIon
We present a review of the nutritional screening and assessment process as codified by the NT 2013 format. We hope that the underlying principles and logic can be widely applied in all clinical situations and help optimize the care of moderate to severely ill patients who are often significantly malnourished.
REFERENCES
1. Jitapunkul J, Sarasin K. Comparative study: BNT vs SGA on nutrition screening & assessment in surgical patients. In-training research of General Surgical Residency Training Program pre-sentation. Bhumibol Adulyadej Hospital, 2002.
2. Jarayapun R, Gate C. The prevalence of malnutrition in surgical patients in Bhumibol Adulyadej Hospital. In-training research of General Surgical Residency Training Program presentation. Bhumibol Adulyadej Hospital, 2006.
3. Sirigunya S. The prevalence of malnutrition in gynaeco-oncologic inpatients in Bhumibol Adulyadej Hospital. In-training research of Obstretic and Gynaecological Residency Training Program presentation. Bhumibol Adulyadej Hospital, 2010.
4. Pibul K, Techapongsatorn S, Thiengthiantham R, Manomaip-iboon A, Trakulhoon V. Nutrition assessment for 200 surgical patients by BNT and SGA. Thai J Surg 2011;32:45-8.
5. Identification of Malnutrition. In: Guideline for Medical Docu-ment Audit. National Health Security Organization (NHSO). 2010;1:191-217.
6. Chittawatanarat K, Chaiwat O, Morakul S, Kongsayreepong S. Outcomes of nutrition status assessment by Bhumibol Nutrition Triage/Nutrition Triage (BNT/NT) in multicenter THAI-SICU study. J Med Assoc Thai 2016;99:S184-92.
7. White JV, Guenter P, Jensen GL, et al, Academy Malnutrition Work Group et al. Consensus statement: Academy of Nutrition and Dietetics and the American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J Parenter Enteral Nutr 2012;36:275-83.
8. Malone A, Hamilton C. The Academy of Nutrition and Dietet-ics /The American Society for Parenteral and Enteral Nutrition Consensus Malnutrition Characteristics: application in practice. Nutr Clin Pract 2013;28:639-50.
9. Jensen GL, Mirtallo J, Compher C, et al. Adult starvation and disease related malnutrition: a rational approach for etiology-based diagnosis in the clinical practice setting from the Inter-national Consensus Guideline Committee. JPEN J Parenter Enteral Nutr 2010;34:156-9.
10. Mueller C, Compher C, Druyan ME. The American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors. A.S.P.E.N. clinical guidelines: nutrition screening, assessment, and intervention. JPEN J Parent Ent Nutr 2011;35:16-24.
11. Charoensilp B. Updated Diagnosis Related Groups [DRGs]

Prammanasudh B, Trakulhoon V Thai J Surg Oct. - Dec. 2019116
and Reimbursement of Malnutrition Diagnoses. Presentation in Annual Meeting of Society of Parenteral and Enteral Nutrition of Thailand - SPENT. 29 November 2018.
12. Chittawatanarat K, Tekarnjanavanich S, Premayothin P. Devel-opment of Nutrition Screening and Assessment Tool to identify hospitalized patient at risk which is appropriate to use in Thailand. Policy Brief, issue 39, November 2016. Health Intervention and Technology Assessment Program- HITAP. http://www.hitap.net/research/165294.
13. Oken M, Creech R, Tormey D, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5:649-55.
14. ARDS Network. IBW Formula. N Engl J Med 2000;342:1301-8.15. Lowenstein DH, Joseph BM, Stephen LH. Approach to the
Patient with Neurologic Disease. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 3028.
16. Silverman EK, Crapo JD, Make BJ. Chronic obstructive pul-monary disease. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 1996.
17. Garney MG, Hoofnagle JH. Approach to the patient with liver disease. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20th ed, New York: McGraw-Hill Education; 2018. p. 2337.
18. Bargman JM, Skoreki KL. Chronic Kidney Disease. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison ‘s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 2112.
19. Kress JP, Hall JB. Approach to the patient with critical illness. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20th ed. NewYork: McGraw-Hill Education; 2018. p. 2023.
20. Raith EP, Udy AA, Bailey M, McGloughlin S, et al. Prognostic accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for in hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 2017;317:290-300.
21. Seymoore CW, Derek CA. Sepsis and septic shock. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 2044.
22. Gyawali B, Ramakrishna K, Dhamoon AS. Sepsis: The evolution in definition, pathophysiology, and management. SAGE Open Med 2019;7:2050312119835043.
23. Mandell LA, WunderinkR. Pneumonia. In: Jameson JL, Kasper DL, Longo DL, Fauci AS, Hauser SL, Loscalzo J, editors. Har-rison ‘s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill Education; 2018. p. 908.
24. Friedstat J, Fred WE, Gibran. Burns. In: Brunicardi FC, Dana KA, Billiar TR, et al. Schwartz’s Principle of Surgery; 10th ed. New York: McGraw-Hill Education; 2015. p. 227.
25. Berger MM. Nutrition support in burns patients. In: Sobotka L, Allison PS, Meire RF, et al, editors. Basic in Clinical Nutrition. ESPEN 4th edition; 2011. p. 563.

IntroductIon
Mastopexy is surgery to correct breast ptosis. Mastopexy focuses on raising the breast mound and leaving the scar as planned initially. In 1925 Dartigues was the first person to describe a vertical mastopexy technique, but it did not become popular. In 1969, Lassus resurrected this technique and popularized it1,2. In 1990, Lejour modified Lassus’s technique, which became the most wide-spread to date3.In this article we will mainly describe a modification of Lassus’ vertical mastopexy technique.
defInItIon of ptosIs
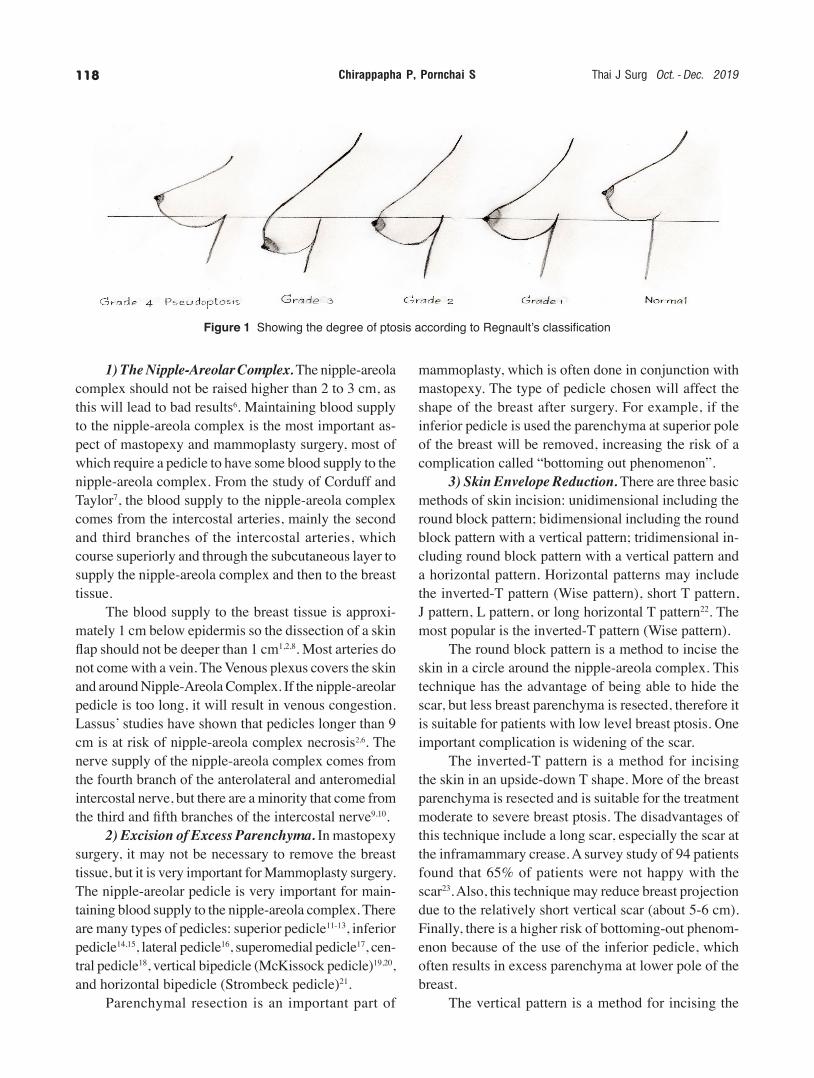
The word “ptosis” comes from the Greek meaning “Falling”4. “Falling of the breast” means the nipple’s position is lowered compared to the inframammary crease. In normal breasts, the nipple position should be above the inframammary crease. The degree to which nipple falls below the level of the inframammary crease determines the severity of ptosis. The oldest and most recognized classification of ptosis is Regnault’s classification5. Regnault’s classification is divided into 3 degrees or grades as follows (Figure 1):
Grade 1: The position of nipple is less than 1 cm above the inframammary crease. Grade 2: The position of nipple is 1-3 cm below the inframammary crease, but the upper contour of the breast still above the inframammary crease. Grade 3: the position of nipple is more than 3 cm below the inframammary crease and the upper contour of the breast is below the inframammary crease.Pseudoptosis is a condition in which the lower pole of the breast is below the inframammary crease but the nipple is still above than the inframammary crease (Figure 1).
Mastopexy and MaMMoplasty
Both operations are to correct ptosis by raising the nipple and areola complex, cutting off excess skin and correct contour of the breast. The only difference is that mammoplasty surgery mainly focuses on breast resection to reduce breast size, while mastopexy surgery focuses on raising the nipples and areola complex to a higher level up and correct contour of the breast. Principles of mastopexy and mammoplasty surgery include: Nipple-Areola Complex elevation and without compromising vascularity; Excision of excess paren-chyma; Skin envelope reduction; and Breast shaping.
The THAI Journal of SURGERY 2019;40:117-125.Official Publication of the Royal College of Surgeons of Thailand
117
Vertical MastopexyPrakasit Chirappapham, MD*
Suragit Pornchai, MD†
*Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University Bangkok, Thailand †Department of Surgery, Saraburi Hospital, Thailand
Abstract Mastopexy is surgery to correct breast ptosis. In this article we present our technique of vertical scar mas-topexy relevant to breast conserving surgery for breast cancer. We also review common indications, techniques, pitfalls and complications of mastopexy that general surgeons should know.
Keywords: Vertical mastopexy
Surgical Technique
Correspondence address: Prakasit Chirappapha, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University Bang-
kok, Thailand; Email: [email protected]
Chirappapha P, Pornchai S Thai J Surg Oct. - Dec. 2019118
1) The Nipple-Areolar Complex. The nipple-areola complex should not be raised higher than 2 to 3 cm, as this will lead to bad results6. Maintaining blood supply to the nipple-areola complex is the most important as-pect of mastopexy and mammoplasty surgery, most of which require a pedicle to have some blood supply to the nipple-areola complex. From the study of Corduff and Taylor7, the blood supply to the nipple-areola complex comes from the intercostal arteries, mainly the second and third branches of the intercostal arteries, which course superiorly and through the subcutaneous layer to supply the nipple-areola complex and then to the breast tissue. The blood supply to the breast tissue is approxi-mately 1 cm below epidermis so the dissection of a skin flap should not be deeper than 1 cm1,2,8. Most arteries do not come with a vein. The Venous plexus covers the skin and around Nipple-Areola Complex. If the nipple-areolar pedicle is too long, it will result in venous congestion. Lassus’ studies have shown that pedicles longer than 9 cm is at risk of nipple-areola complex necrosis2,6. The nerve supply of the nipple-areola complex comes from the fourth branch of the anterolateral and anteromedial intercostal nerve, but there are a minority that come from the third and fifth branches of the intercostal nerve9,10. 2) Excision of Excess Parenchyma. In mastopexy surgery, it may not be necessary to remove the breast tissue, but it is very important for Mammoplasty surgery. The nipple-areolar pedicle is very important for main-taining blood supply to the nipple-areola complex. There are many types of pedicles: superior pedicle11-13, inferior pedicle14,15, lateral pedicle16, superomedial pedicle17, cen-tral pedicle18, vertical bipedicle (McKissock pedicle)19,20, and horizontal bipedicle (Strombeck pedicle)21. Parenchymal resection is an important part of
mammoplasty, which is often done in conjunction with mastopexy. The type of pedicle chosen will affect the shape of the breast after surgery. For example, if the inferior pedicle is used the parenchyma at superior pole of the breast will be removed, increasing the risk of a complication called “bottoming out phenomenon”. 3) Skin Envelope Reduction. There are three basic methods of skin incision: unidimensional including the round block pattern; bidimensional including the round block pattern with a vertical pattern; tridimensional in-cluding round block pattern with a vertical pattern and a horizontal pattern. Horizontal patterns may include the inverted-T pattern (Wise pattern), short T pattern, J pattern, L pattern, or long horizontal T pattern22. The most popular is the inverted-T pattern (Wise pattern). The round block pattern is a method to incise the skin in a circle around the nipple-areola complex. This technique has the advantage of being able to hide the scar, but less breast parenchyma is resected, therefore it is suitable for patients with low level breast ptosis. One important complication is widening of the scar. The inverted-T pattern is a method for incising the skin in an upside-down T shape. More of the breast parenchyma is resected and is suitable for the treatment moderate to severe breast ptosis. The disadvantages of this technique include a long scar, especially the scar at the inframammary crease. A survey study of 94 patients found that 65% of patients were not happy with the scar23. Also, this technique may reduce breast projection due to the relatively short vertical scar (about 5-6 cm). Finally, there is a higher risk of bottoming-out phenom-enon because of the use of the inferior pedicle, which often results in excess parenchyma at lower pole of the breast. The vertical pattern is a method for incising the
Figure 1 Showing the degree of ptosis according to Regnault’s classification

Vertical MastopexyVol. 40 No. 4 119
skin leaving mainly a vertical scar. This technique is often used for correcting mild to moderate breast ptosis and results in a better breast contour than the inverted T pattern. Some advantages of vertical patterns compared to inverted-T patterns include less scarring, with no or only a small scar at the inframammary fold, the scar is positioned where the patient cannot see, and a lower risk of hypertrophic scar. According to Lassus, in a study of 1,350 patients treated with the vertical pattern during a 40-year period (439 mastopexies and 911 mammoplas-ties), only 4 patients had hypertrophic scars2. The vertical pattern usually increases the breast projection more than inverted T pattern, as mentioned previously, as the vertical pattern favors forward breast projection. A part of the reason is that the breast paren-chyma is sutured together vertically, not suture horizon-tally. This will also result in better breast contour. There is also less chance of “bottoming-out phenomenon”. According to Lassus, the contour of the breast was still well maintained 20 years after vertical mastopexy sur-gery1. Vertical mammaplasty with a short scar is a modi-fied technique that shortens the vertical scar, causing increase in the breast projection and decrease the width of the breast, allowing it to maintain the breast contour for longer24,25. 4) Breast Shaping. Breast shaping can be done in several ways, such as resection of the skin, resection and suturing of the breast parenchyma, fixing it to fascia or the use of artificial materials such as synthetic mesh or acellular dermal matrix to bind the parenchyma into certain shapes26-28.
Indications And Assessment For Vertical Mas-topexy Optimum results for vertical mastopexy require careful patient selection. Suitable patients include young patients with small or medium-sized breast, with mild to moderate breast ptosis, and with normal skin elastic-ity1,2,29,30. Patients with large breasts or severe breast pto-sis are not suitable for vertical mastopexy, due to reports of higher incidence of complications31. Immediately after surgery, the shape of the breast and the scar are usually not being as good as they should be. Final results can be predicted after 3 months1,3,31-34. Preoperative assessment includes the degree of breast ptosis, breast size, and skin elasticity.
1) The degree of breast ptosis. Evaluation of breast ptosis must assess the relationship between the nipple and the inframammary crease by measuring the distance between suprasternal notch to the nipple, which averages 18 to 22 cm. Knowing this distance will allow the assessment of how much to lift the nipples and also determines the techniques for mastopexy surgery. Ptosis may also be measured from the inframammary crease or mid shaft of humerus to the nipple. 2) The degree of breast size. Assessing the pa-tient’s breast size and shape requirements is an important step in surgical planning. However, if after the surgery the patient is not satisfied with the size and shape of the breast, further corrective procedures can be performed. For example, if the breast size is too small, corrections to increase the volume, such as using breast implants or lipofilling, can be done. On the other hand, if the breast is still too large after the surgery, it can be corrected by reducing body weight or further resections of breast parenchyma. 3) The degree of skin elasticity. Normal skin elasticity will help maintain the shape of the breast in the long term, compared to high skin elasticity. Skin puckering or wrinkle wounds on the underside of the breast will subside spontaneously, usually within 2 months, with normal skin elasticity, but it might take more than 5 to 6 months if the skin is highly elastic3. In addition, patients with high skin elasticity are at a higher risk of bottoming-out. It should also be explained to patients that after the surgery, the results may not be satisfactory at first. The upper pole fullness might initially seem greater than normal, and the lower pole might look flat early after surgery. It takes a period of 2 to 3 months before the shape of the breast settles2,35. It must be explained to the patients that complications after surgery may may occur, such as breast asymmetry, changes in nipple sensation, nipple and breast necrosis, and possible scarring.
Preoperative Drawing And Marking Drawing and markings on the patient should be done in a standing position. There are measurements and distance records of various lines. The following should be drawn or marked: a line from suprasternal notch to nipple; a line from suprasternal notch to the umbilicus to mark the midline; a line representing the inframam-mary crease on both sides; the breast meridian on both sides (drawn from the side of the clavicle 7 cm from
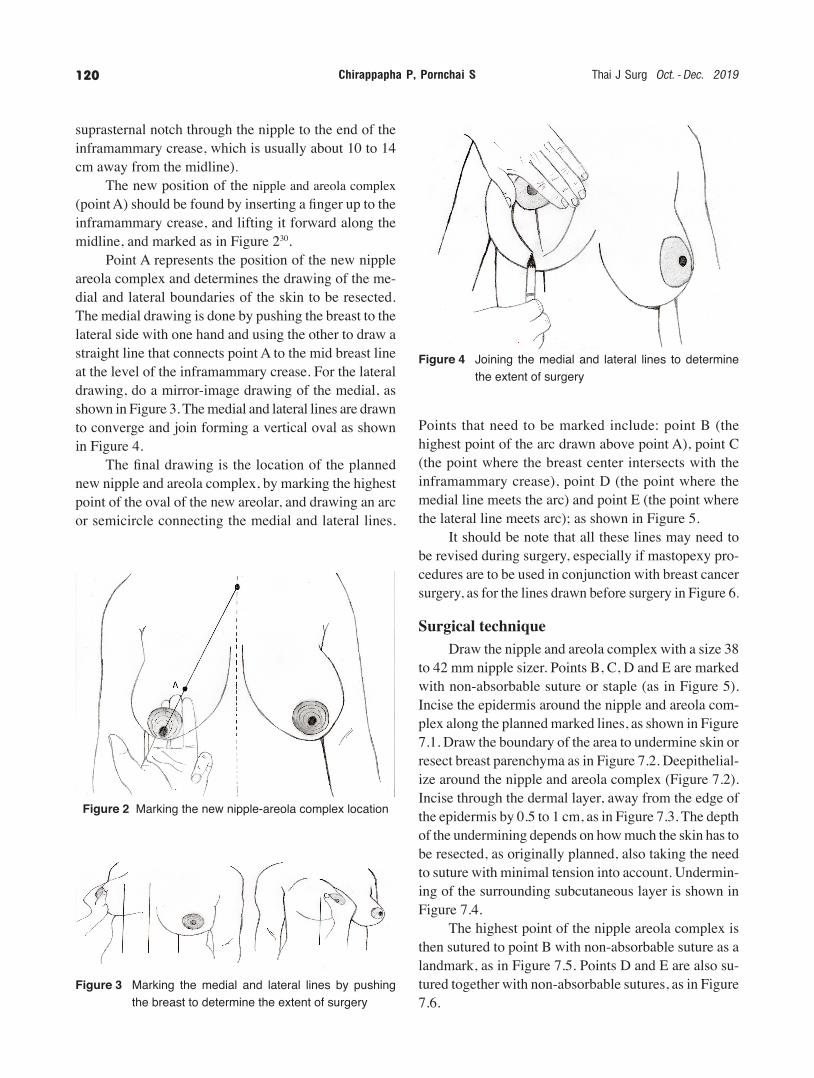
Chirappapha P, Pornchai S Thai J Surg Oct. - Dec. 2019120
suprasternal notch through the nipple to the end of the inframammary crease, which is usually about 10 to 14 cm away from the midline). The new position of the nipple and areola complex (point A) should be found by inserting a finger up to the inframammary crease, and lifting it forward along the midline, and marked as in Figure 230. Point A represents the position of the new nipple areola complex and determines the drawing of the me-dial and lateral boundaries of the skin to be resected. The medial drawing is done by pushing the breast to the lateral side with one hand and using the other to draw a straight line that connects point A to the mid breast line at the level of the inframammary crease. For the lateral drawing, do a mirror-image drawing of the medial, as shown in Figure 3. The medial and lateral lines are drawn to converge and join forming a vertical oval as shown in Figure 4. The final drawing is the location of the planned new nipple and areola complex, by marking the highest point of the oval of the new areolar, and drawing an arc or semicircle connecting the medial and lateral lines.
Points that need to be marked include: point B (the highest point of the arc drawn above point A), point C (the point where the breast center intersects with the inframammary crease), point D (the point where the medial line meets the arc) and point E (the point where the lateral line meets arc); as shown in Figure 5. It should be note that all these lines may need to be revised during surgery, especially if mastopexy pro-cedures are to be used in conjunction with breast cancer surgery, as for the lines drawn before surgery in Figure 6.
Surgical technique Draw the nipple and areola complex with a size 38 to 42 mm nipple sizer. Points B, C, D and E are marked with non-absorbable suture or staple (as in Figure 5). Incise the epidermis around the nipple and areola com-plex along the planned marked lines, as shown in Figure 7.1. Draw the boundary of the area to undermine skin or resect breast parenchyma as in Figure 7.2. Deepithelial-ize around the nipple and areola complex (Figure 7.2). Incise through the dermal layer, away from the edge of the epidermis by 0.5 to 1 cm, as in Figure 7.3. The depth of the undermining depends on how much the skin has to be resected, as originally planned, also taking the need to suture with minimal tension into account. Undermin-ing of the surrounding subcutaneous layer is shown in Figure 7.4. The highest point of the nipple areola complex is then sutured to point B with non-absorbable suture as a landmark, as in Figure 7.5. Points D and E are also su-tured together with non-absorbable sutures, as in Figure 7.6.
Figure 2 Marking the new nipple-areola complex location
Figure 3 Marking the medial and lateral lines by pushing the breast to determine the extent of surgery
Figure 4 Joining the medial and lateral lines to determine the extent of surgery

Vertical MastopexyVol. 40 No. 4 121
After surgery on both sides, try the patient is in a sitting position to assess the shape of the breast, whether further adjustment is needed. If the breast shape is satisfactory, then suture the wound with absorbable suture. In this patient was used Monocryl 4-0, then all non-absorbable suture was removed, shown in Figure 8. After the operation, the lower pole of breast should be flat and the upper pole of the breast will often project. The breast regains shape due to gravity and skin elasticity, which takes approximately 2-3 months after surgery3,33 as Figure 9. The above picture shows the patient before the surgery. The below picture shows the same patient three months after the surgery.
Post-Operative Care Within 24 hours, it is important to look at the color of the nipple and areola complex for necrosis or not. Postoperative pain is usually mild to moderate and can be treated with NSAID. May be consider using opioid drugs in some patients. If the patient is awake, can eat and ambulation. In the early postoperative period, the scar may be below the inframammary crease but this will be hide by the downward movement of the breast, taking about 2-3 months. If after 3 months the scars or breast shape are still not satisfactory, surgery may be considered for this period of time3,33.
Complication after surgery Several studies show that vertical mastopexy sur-gery has very few complications1,3,30,31,36-39. Risk factors will increase, corresponding to the larger breast size. Lejour reported having performed vertical mastopexy surgery in 476 patients. The most common complica-tions are seroma, which is about 5%, Nipple and Areolar necrosis is 0.4%, infection is 0.4% and Hematomas are 1.2% which can be found after a few hours of surgery. If the breast is cut less or less under the skin, the condi-tion can be reduced34. The recurrence was approximately 0.016% at 1 year after surgery3. According to Lassus reports, after vertical masto-pexy surgery, even after 20 years, still able to maintain the contour of the breast shape1. Distortion areolas (teardrop-shaped areolas) are a common complication. This can be prevented by fixing suture to the vertical line of areola 2 points40.
Figure 6 Showing a patient with breast ptosis and com-pleted drawings for vertical mastopexy surgery
Figure 5 Showing lines around the nipple and areola com-plex and other important points (A, B, C, D, and E)

Chirappapha P, Pornchai S Thai J Surg Oct. - Dec. 2019122
Figure 7 The details of Vertical mastopexy surgery 7.1 Showing the epidermal incision 7.2 Showing the deepithelialization skin around the nipple and areola complex and drawing of boundaries to under-
mine the subcutaneous layer 7.3 Showing the cutting through the dermis 7.4 Showing the undermine of the surrounding subcutaneous layer 7.5 Showing the suture of the highest point of the nipple and areola complex to the B point 7.6 Showing the suture of the skin together

Vertical MastopexyVol. 40 No. 4 123
Figure 8 Showing the patient after Vertical mastopexy surgery
Figure 9 Showing a female patient with moderate breast ptosis with vertical mastopexy surgery

Chirappapha P, Pornchai S Thai J Surg Oct. - Dec. 2019124
13. Arufe HN, Erenfryd A, Saubidet M. Mammaplasty with a single, vertical, superiorly-based pedicle to support the nipple-areola. Plast Reconstr Surg 1977;60(2):221-7.
14. Courtiss EH, Goldwyn RM. Reduction mammaplasty by the inferior pedicle technique. An alternative to free nipple and areola grafting for severe macromastia or extreme ptosis. Plast Reconstr Surg 1977;59(4):500-7.
15. Robbins TH. A reduction mammaplasty with the areola-nipple based on an inferior dermal pedicle. Plast Reconstr Surg 1977;59(1):64-7.
16. Skoog TD. A technique of breast reduction: transposition of the nipple on a cutaneous vascular pedicle. Acta Chir Scand 1963;126:453-65.
17. Orlando JC, Guthrie RH. The superomedial dermal pedicle for nipple transposition. Br J Plast Surg 1975;28(1):42-5.
18. Hester TR, Bostwick J, Miller L. Breast reduction utilizing the maximally vascularized central breast pedicle. Plast Reconstr Surg 1985;76(6):890-900.
19. McKissock PK. Reduction mammaplasty with a vertical dermal flap. Plast Reconstr Surg 1972;49(3):245-52.
20. McKissock PK. Reduction mammaplasty by the vertical bi-pedicle flap technique. Rationale and results. Clin Plast Surg 1976;3(2):309-20.
21. Strombeck JO. Mammaplasty: report of a new technique based on the two pedicle procedure. Br J Plast Surg. 1960;13:79.
22. Nahai F. Clinical decision-making in breast surgery. The Art of Aesthetic Surgery. 2005:1817-58.
23. Sprole AM, Adepoju I, Ascherman J. Horizontal or vertical? An evaluation of patient preferences for reduction mammaplasty scars. Aesthetic Surg J 2007;27(3):257-62.
24. Marchac D. Reduction mammaplasty with a short horizontal scar. Reduction Mammaplasty Boston: Little, Brown; 1990. p. 317-36.
25. Marchac D, Olarte GD. Reduction mammaplasty and correction of ptosis with a short inframammary scar. Plast Reconstr Surg 1982;69(45).
26. Benelli L. A new periareolar mammaplasty: the “round block” technique. Aesthetic Plast Surg 1990;14(2):93-100.
27. Graf R, Biggs TM. In search of better shape in mastopexy and reduction mammoplasty. Plast Reconstr Surg 2002;100(1):321-2.
28. Góes JC. Periareolar mammaplasty: double skin technique with application of polyglactin or mixed mesh. Plast Reconstr Surg 1996;97(5):959-68.
29. Hoffman A, Wuestner-Hofmann M, Basseto F. Breast reduction: modified “Lejour technique” in 500 large breasts. Plast Reconstr Surg 2007;120:1095-104.
30. Hidalgo DA. Vertical mammaplasty. Plast Reconstr Surg 2005;115(4):1179-97.
31. Lejour M. Vertical mammaplasty: early complications after 250 personal consecutive cases. Plast Reconstr Surg 1999;104(3):764-70.
32. Graf RM, Tolazzi ARD, Ono MC. Vertical mammaplasty. Techno Aesthetic Plast Surg 2009:217-27.
33. Hall-Findlay EJ. A simplified vertical reduction mamma-plasty: shortening the learning curve. Plast Reconstr Surg 1999;104(3):748-59.
In nipple sensation, Lejour reported 170 patients following the surgery for 6 months. They found that 7 patients had reduced nipple sensation and 1 lost nipple sensation completely31. Lactation after vertical mastopexy surgery is dif-ficult to predict because it depends on many factors, especially breast parenchyma resection. If resecting a large amount of breast parenchyma, there is little to have a chance of lactation.
conclusIon
Mastopexy surgery and Mammoplasty surgery are both methods for collected breast ptosis. Mastopexy surgery focuses on raising the nipple and areola complex and creating a good breast contour. Vertical mastopexy surgery will leave the scar vertical, Suitable for young patients and mild to moderate breast ptosis. It also helps to reduce scarring, increase breast projection, reduce width of breast, make good breast contour in the long time and have few complications.
REFERENCES
1. Lassus C. Update on vertical mammaplasty. Plast Reconstr Surg 1999;104(7):2289-98.
2. Lassus C. Vertical scar breast reduction and mastopexy without undermining. Surgery of the Breast: Principles and Art. 3rd ed. 2011. p. 990-1006.
3. Lejour M. Vertical mammaplasty: update and appraisal of late results. Plast Reconstr Surg 1999;104(3):771-81.
4. Michelow B, Nahai F. Mastopexy. Plastic Surgery: Indications, Operations and Outcomes. 2000:2769-81.
5. Regnault P. Breast ptosis. Definition and treatment. Clin Plast Surg 1976;3(2):193-203.
6. Grotting JC, Chen SM. Control and precision in mastopexy. Art Aesthetic Surg 2005:1907-50.
7. Corduff N, Taylor GI. Subglandular breast reduction: the evolution of a minimal scar approach to breast reduction. Plast Reconstr Surg. 2004;113:175-84.
8. Hall-Findlay EJ. Vertical breast reduction. Semin Plast Surg 2004;18(3):211-24.
9. Hanna MK, Nahai F. Applied anatomy of the breast. Art Aes-thetic Surg 2005:1790-815.
10. Greuse M, Hamdi M, DeMey A. Breast sensitivity after vertical mammaplasty. Plast Reconstr Surg 2001;107(4):970-6.
11. Weiner L, Aiache A, Silver L. A single dermal pedicle for nipple transposition in subcutaneous mastectomy, reduction mamma-plasty, or mastopexy. Plast Reconstr Surg 1973;51(2):115-20.
12. Weiner D. Breast reduction: the superior pedicle technique (dermal and composite). Reduction Mammaplasty Philadelphia: Lippincott Williams & Wilkins; 1990. p. 233-8.

Vertical MastopexyVol. 40 No. 4 125
34. Nahai F, Boehm K. Mastopexy. Cosmetic and reconstructive Breast Surgery. 2009. p. 109-18.
35. Spear SL, Howard MA. Evolution of the vertical reduction mammaplasty. Plast Reconstr Surg 2003;112:855-68.
36. Berthe J, Massaut J, Greuse M. The vertical mammaplasty: a reappraisal of the technique and its complications. Plast Reconstr Surg 2003;111(7):2192-9.
37. Lista F, Ahmad J. Vertical scar reduction mammaplasty: a 15-year experience including a review of 250 consecutive cases. Plast Reconstr Surg 2006;117(7):2152-65.
38. Spector JA, Kleinerman R, Culliford AT. The vertical reduction mammaplasty: a prospective analysis of patient outcomes. Plast Reconstr Surg 2006;117(2):374-81.
39. Thienen CE. Areolar vertical approach (AVA) mammaplasty: Lejour’s technique evolution. Clin Plast Surg 2002;29:365-77.
40. Wallach SG. Avoiding the teardrop-shaped nipple-areola complex in vertical mammaplasty. Plast Reconstr Surg 2000;106(5):1217-8.

The THAI Journal of SURGERY 2019;40:126-149.Official Publication of the Royal College of Surgeons of Thailand
126
Abstracts of the 44th Annual Scientific Congressof The Royal College of Surgeons of Thailand,13-16 July 2019, Ambassador City JomtienHotel, Pattaya, Cholburi, Thailand (Part II)
ACS Basic Science
CHANGE OF BASAL METABOLIC RATE IN SUPER-OBESE PATIENTS WITH VERY LOW-CALORIE DIET BEFORE BARIATRIC SURGERY
Komol Chaivanijchaya1, Fon Pakul1, Sikarin Sornphiphatphong1, Suthikiat Joradol1, Satkunan Mark2, Suthep Udomsawaengsup1
1 Department of Surgery, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand2 Department of Surgery, Hospital Raja Permaisuri Bainun Ipoh, Malaysia
Background: The principles of weight loss is based on the imbalance between energy intake and expenditure; where energy intake should be less than utilized. It is desirable to know the energy expenditure of individuals to design and monitor effective planning or maintenance weight loss. Energy requirements can be estimated or measured using variety of methods. This study is designed to measure the daily changes of basal metabolic rate (BMR) in super morbid obese patients with limited calorie intake 2 weeks before operation. Materials and Methods: We included super-obese patients (BMI > 50 kg/m2) that were admitted for preoperative acute weight loss program 2 weeks prior to surgery in Chulalongkorn Hospital. All patients received diet of 800 kcal/day with protein 1.5 g/kg/day. Energy assessment was done using indirect calorimetry of each subject in the morning on day 1, 7, 14 after admission and post-operative day 7. We used a portable indirect
calorimeter (Fitmate GS) and Haris-benedict formula to calculated BMR at the same day. Results: Seven patients were recruited in this study. The calculated BMR was steadily decreasing but there was statistically significant difference in BMR that obtained from indirect calorimetry that was less than the calculated BMR at day 14 and postop day 7 (p = 0.025 and 0.010 respectively). Patients loss more of their body weight in first week than 2nd week (4.53% vs. 1.29%, respectively) Conclusions: BMR was decrease with limited calorie intake. Measured BMR was significantly lower after 14 days of low calorie diet related with weight loss was more in the first week compared to the second week so that Haris-Benedict formula significantly overesti-mated BMR during this period.
CLINICAL SAFETY TEST OF POLYESTER CON-TAINING HERBAL EXTRACT AND AG+ DRESS-ING IN HEALTHY VOLUNTEER
Wongsakorn Veerakarnjana1, Kusuma Chinaroon-chai1, Natthida Owattanapanich1, Pornprom Muang-man1, Nantaporn Namviriyachote1Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Background: The polyester containing herbal extract (aloe vera and centella asiatica) (SIHERB) has

AbstractsVol. 40 No. 4 127
been proved that this dressing can reduce cost of treat-ment, improve regeneration of tissue and decrease pain sensation during wound care without any complication or irritating reaction. The dressing containing of Ag+ have been used for reducing rate of infection in burn and trauma and our research team was interested to develop the new polyester containing herbal extract and Ag+ (SIHERBplus) and would like to study the clinical safety test of this dressing. Objectives: To study the clinical safety test and compare the skin irritating reaction between polyester containing herbal extract and polyester containing herbal extract plus silver in healthy volunteer. Materials and Methods: Two part of the study was done. The first part of study was done in laboratory to study the discharge absorption, moist evaporation, Ag distribution and efficacy for inhibit bacterial growth between dressing material with other dressing material including Aquacel, Urgotul SSD, Bactigras and Allevyn. The second part of study was done in a group of 60 healthy volunteer who were included for the study that attached 2x2 cm of SIHERB and SIHERBplus on each side of both shoulders. Skin allergic reaction was ob-served and evaluated by the skin irritating score system at day 0, 3 and 7. Results: The result was shown that SIHERB and SIHERBplus had no significant difference of water absorption compare with Urgotul SSD and Bactigras but less absorption compare with other. Aquacel was the material that most change in weight and structure after moist evaporation. There was no significant difference for Ag distribution and efficacy for inhibit bacterial growth between SIHERBplus with other antibiotic containing dressing. There was no significant difference of skin allergic reaction between SIHERBplus and SIHERB at day 0 (p = 0.108), day 3 (p = 0.102), and day 7 (p = 0.705) by Wilcoxon Sigged Rank test. Conclusions: SIHERBplus is a safety dressing with no significant difference in skin allergic reaction when compare with routinely used SIHERB. The result of this study can be used further in phase II study to measure the efficacy of this dressing material. Keywords: Herbal extraction, Skin allergy, Aloe vera, Centella, Wound dressing
HIGH EXPRESSION OF PROLACTIN RECEP-TOR IN BREAST CANCER TISSUE WAS COR-RELATED WITH LOWER OVERALL SURVIVAL
Doonyapat Sa-nguanraksa1, Cholladda Thasripoo1, Norasate Samarnthai2, Tanawan Kummalue3, Pornchai O-charoenrat1
1 Division of Head Neck and Breast Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand2 Department of Pathology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand3 Department of Clinicalpathology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Background: Prolactin (PRL) is a polypeptide hormone secreted by the anterior pituitary responsible for the growth and differentiation of the normal mam-mary gland and plays a role in breast cancer. Objectives: To evaluate the roles of prolactin (PRL) and prolactin receptor (PRLR) polymorphisms as well as PRLR expression in breast cancer risk and clinical outcomes in Thai breast cancer patients. Patients and Methods: PRL (rs3756824 C/G and rs2244502 T/A) and PRLR (rs37364 G/T and rs249537 A/G) polymorphisms were genotyped by real-time PCR. Immunohistochemistry (IHC) was performed to assess PRLR expression in breast cancer tissue. The correla-tions between PRL and PRLR polymorphisms and breast cancer susceptibility/aggressiveness as well as the asso-ciations between PRLR expression and clinicopathologi-cal parameters were determined by Chi-square statistics. The survival outcomes were assessed by Kaplan Meier analysis and Cox proportional hazard model. P-values of < 0.05 were considered as statistically significant. Results: A total of 237 breast cancer patients and 119 controls were examined. PRL and PRLR polymor-phisms were not correlated with breast cancer suscep-tibility. PRL rs2244502 TA and AA genotypes were more frequent in progesterone receptor (PgR) positive breast cancer patients (p = 0.029). PRLR rs3756824 CC genotype was associated with PgR negative and HER2 positive (p = 0.010 and p = 0.011, respectively). IHC was performed in 107 breast cancer tissues. There was no association between PRLR polymorphisms and PRLR expression. High expression of PRLR was significantly associated with presence of lymphovascular invasion (p =

Abstracts Thai J Surg Oct. - Dec. 2019128
0.011). Patients with PRLR rs249537 AA genotype had significantly poorer overall survival than other geno-types (p = 0.012). In addition, patients with high PRLR expression had lower overall survival (p = 0.025). Conclusions: High PRLR expression was cor-related with aggressiveness of breast cancer. PRLR
expression might be used as a prognostic factor. Further study regarding the role of PRLR as a target for breast cancer therapy should be conducted. Keywords: Breast cancer, Prolactin, Prolactin receptor, Polymorphisms, Immunohistochemistry
ICS Inventor Award
Pisith Viseshakul Award
ROBOT-ASSISTED ENDONASAL ENDOSCOPIC TRANS-SPHENOIDAL SURGERY
Sorayouth Chumnanvej1, Suwiphat Chalongwongse2, Branesh M. Pillai2, Jackrit Suthakorn2
1 Neurosurgery Division, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok,10400 Thailand2 Center for Biomedical and Robotics Technology (BART LAB), Department of Biomedical Engineering, Faculty of Engineering, Mahidol University, Salaya, 73170 Thailand
Background: Endonasal Endoscopic Trans-sphenoidal Surgery (EETS) is a minimally invasive procedure to approach and remove pituitary tumors and other sellar lesions. The procedure causes less pain, allows faster recovery, and provides further minimally invasive access for other critical cases. However, a slight deviation of direction from the target area can be fatal to patients. The aim of present study was to design and develop a prototype robot to demonstrate a more accurate neurosurgical robot-assisted EET approach. Materials and Methods: The effectiveness of a prototype robot in executing a minimally invasive EET surgery was studied on 6 cadavers. The robot was
equipped with a multi-information integrated technique for surgery including QR code tracking. The robot was controlled and driven by the neurosurgeon. A standard procedure of EET was followed and the robot carried out the first stage of EET under the supervision of neu-rosurgeon. The tumor or lesion was removed by the neurosurgeon. Results: The prototype robot was observed to reach the target area, the sphenoid sinus, accurately and precisely in all 6 cadavers. The result was determined by qualitative analysis and was confirmed by the neuro-surgeon. The time for the entire EET surgical procedure showed marked reduction compared to the traditional EET approach. Conclusion: A new neurosurgical approach using a robot prototype has been described in this study. The prototype robot had successfully achieved the goal to guide the neurosurgeon to reach the sphenoid sinus ac-curately. The robot design was found to be technically feasible and can be used for assisting the EET procedure. Keywords: Endonasal Endoscopic Trans-sphenoidal Surgery (EETS), Pituitary tumors, Robot-assisted EET approach.
CORRELATION BETWEEN MAXIMUM CLOT FIRMNESS IN FIBTEM AND SERUM FIBRINO-GEN IN CRITICAL TRAUMA PATIENTS
Supamongkol Khunakeanan1, Osaree Akaraborworn2, Burapat Sangthong2, Komet Thongkhao2
1 Department of Surgery, Faculty of medicine, Prince of Songkla University, Hat Yai, Songkhla 90110, Thailand 2 Division of Trauma and Critical Care, Department of Surgery, Faculty of Medicine, Prince of Songkla University, Hat Yai, Song-khla, Thailand
Background: The serum Fibrinogen and Rotational Thromboelastometry (FIBTEM and ROTEM) can provide information on the coagulation status of patients, which is useful in the decision to transfuse blood components. FIBTEM, which is one of the studies in ROTEM, is considered a test for fibrinogen level. However, the cor-relation between FIBTEM and actual fibrinogen has not been clearly demonstrated. Objective: To determine the relationship between serum fibrinogen level and FIBTEM. Materials and Methods: This is a retrospective

AbstractsVol. 40 No. 4 129
cohort study of all trauma patients who met the trauma activation criteria during May 2017 to January 2019 at Songklanagarind Hospital. Patients who had serum fibrinogen level and ROTEM results were eligible for the study. The relationship between maximal clot firm-ness (MCF) measured in FIBTEM and serum fibrinogen level was determined using a linear regression model. The Area under a Receiver Operating Characteristic curve (AuROC) was used to measure the performance of FIBTEM MCF in predicting hypofibrinogenemia, which was defined as serum fibrinogen < 200 mg/dL. Results: Eighty-seven patients were included in the study. Seventy-three patients were men (84%), and the
median age was 40 years. The linear regression equation relating FIBTEM MCF to serum fibrinogen was demon-strated to be: Serum Fibrinogen (mg/dL) = 138+15.2x (FIBTEM MCF) (p < 0.01; R2 = 0.35) FIBTEM MCF could predict hypofibrinogenemia with an AuROC of 0.81. Conclusion: FIBTEM MCF may not be a good predictor of actual level of serum fibrinogen. However, FIBTEM MCF could be useful in predicting pofibrino-genemia in trauma patients. Keywords: Rotational thromboelastometry, Fi-brinogen, Multiple trauma
Poster Competition
A MULTICENTRE COMPARISON BETWEEN INPATIENT AND OUTPATIENT PREOPERATIVE ACUTE WEIGHT LOSS IN SUPEROBESE PA-TIENTS UNDERGOING BARIATRIC SURGERY
Satkunan Mark2, Komol Chaivanijchaya1, Fon Pakul1, Sikarin Sornphiphatphong1, Suthikiat Joradol1, Siva-nesan Ramasamy1, Kirubakaran Malapan2, Suthep Udomsawaengsup1
1 Department of Surgery, Faculty of Medicine, King Chulalongkorn Memorial Hospital Bangkok, Thailand2 Department of Surgery, Hospital Raja Permaisuri Bainun Ipoh Jalan Raja Ashman 30450 Ipoh Perak, Malaysia
Background: Preoperative preparation is impor-tant in patients undergoing bariatric surgery. One of the key components is preoperative acute weight loss (AWL) whereby patients are given very low-calorie diet to achieve approximately 10% weight loss. It reduces the liver size to facilitate the procedure, reduces risk of perioperative complications and achieves desirable postoperative weight loss. Objectives: To show that preoperative inpatient AWL produces better preoperative weight loss when compared to outpatient. Materials and Methods: This is a multicentre retrospective analysis comparing the outcomes between inpatient and outpatient preoperative AWL for patients
with > BMI 50 undergoing bariatric surgery. All patients were prescribed with very low-calorie diet (800/kcal/day) preoperatively. Results: There were 71 patients in the inpatient group and 37 patients in the outpatient group. The mean BMI in the inpatient and outpatient group was 61.3 and 58.2 respectively. The mean weight prior to AWL was 173 kg in the inpatient group and 151.6 kg in the outpatient. Following AWL, the average weight loss in the inpatient group was 12 kg (7%) and 3.7 kg (4.5%) in the outpatient group. The comparison is statistically significant (p < 0.001). There was one cancellation in the outpatient group due to large left lobe of liver while there were none in the patient group and no adverse complications in both groups. However, the postopera-tive weight loss was comparable in both groups. Conclusions: Inpatient AWL produces significant preoperative weight loss compared to outpatients. The desired weight loss in inpatient group is comparable to other studies worldwide. Though it is significant in pre-operative weight loss, the post-operative weight loss is comparable in both study groups. While inpatient group allows better monitoring; the outpatient group creates a positive impact on overall healthcare cost and hospital bed occupancy rates. Keywords: Acute weight loss, Very low-calorie diet, Bariatric Surgery, Obesity

Abstracts Thai J Surg Oct. - Dec. 2019130
ADEQUATE ENOXAPARIN DOSAGE FOR VE-NOUS THROMBOEMBOLISM PROPHYLAXIS IN BARIATRIC SURGERY
Sikarin Sornphiphatphong, Komol Chaivanijchaya, Fon Pakul, Suthikiat Joradol, Krit Kitisin, Suppa-ut Pungpapong, Chadin Tharavej, Patpong Navicharern, Suthep UdomsawaengsupDepartment of Surgery, Faculty of Medicine, Chulalongkorn Uni-versity, Bangkok, Thailand
Background: Venous thromboembolism (VTE) is a relatively common postoperative complication that may lead to multiple serious problems including death. Morbidly obese is an independent risk factor for VTE with an increased risk greater than 2-3 folds. Proper dosing regimen of enoxaparin for VTE prophylaxis in morbidly obese is not clearly defined in available guidelines and there are no reported studies pertaining to the adequacy of prophylactic dosage used in Thai population. Objectives: To assess the achievement of desired target anti-factor Xa level after the administration of enoxaparin for VTE prophylaxis in patients planned for bariatric procedure. Materials & Methods: An observational des-criptive study carried out on morbidly obese patients scheduled for bariatric procedure in King Chulalongkorn Memorial Hospital since January 2019. All recruited patients received either 40 mg or 60 mg of enoxaparin subcutaneously 12 hours before the scheduled operative time. Blood specimens for peak 4-hour anti-factor Xa level were collected at 4 hours after the administration of enoxaparin. The target range of anti-factor Xa level was defined between 0.2-0.5 IU/ml. Results: There were 12 patients that underwent bariatric procedure during our study period. Eight pa-tients received 40 mg of enoxaparin while 4 patients received 60 mg. The mean anti-factor Xa levels were 0.20 IU/ml in the 40 mg group and 0.38 IU/ml in the 60 mg group. The percentage of target level achievement in both groups were 62.5% and 100% respectively. There were no patients that obtained levels exceeding 0.5 IU/ml of anti-factor Xa. There was no significant perioperative bleeding complication in both the 2 groups. Conclusions: For VTE prophylaxis in bariatric procedure, enoxaparin dosage at 60 mg subcutaneously
achieved the desired target levels of anti-factor Xa when compared to 40 mg without any unwanted complications. The trend of anti-factor Xa level is inversely proportion-ate to increasing body weight. Keywords: Venous thromboembolism, Prophylaxis, Bariatric surgery, Morbid obesity, Enoxaparin
LAPAROSCOPIC INGUINAL HERNIA REPAIR: THE IDEAL DAY CARE LAPAROSCOPIC SUR-GERY: HOSPITAL RAJA PERMAISURI BAINUN IPOH, EXPERIENCE
Satkunan Mark, Kah Ling Loh, Hisyam Sidik, Yang Wai YanDepartment of Surgery, Hospital Raja Permaisuri Bainun Ipoh Jalan Raja Ashman, 30450 Ipoh Perak, Malaysia
Background: Day care surgery is an emerging and promising surgical concept benefiting patients and healthcare system. At present, laparoscopic cholecys-tectomy and laparoscopic inguinal hernia repairs are the two commonest laparoscopic procedures performed as day care. Objective: To present our experience and outcome that day care laparoscopic inguinal hernia repairs is safe, advantageous and ideal as day case surgery. Materials and Methods: This is a retrospective outcome analysis of all-day care laparoscopic inguinal hernia repairs performed between January 2013 and December 2018 in Hospital Raja Permaisuri Bainun Ipoh Malaysia. Results: A total of 354 cases of laparoscopic in-guinal hernia repair performed between January 2013 and December 2018. All cases were planned as day care. There were 54 cases done using the transabdominal pre-peritoneal repair technique (TAPP) and 300 cases using the totally extraperitoneal repair technique (TEP). Mean operating time was 67 minutes. There was a total of 20 cases of unplanned admissions. The causes for these admissions were difficult extubation, high post-operative blood pressure and intra-op atrial fibrillation requiring post-operative monitoring. Nine cases were converted to open hernia repair and recurrence rate in our series was 4.8%. Our series shows a success day care discharge rate of 94.4%. Conclusion: Laparoscopy in general produces little post-operative pain and faster recovery. When it

AbstractsVol. 40 No. 4 131
is coupled with day care anaesthetic protocol, it makes laparoscopic inguinal hernia repair an ideal procedure for day care surgery. Our analysis therefore shows that both techniques of laparoscopic hernia repair can be performed safely as day care surgeries. Keywords: Day care surgery, Laparoscopic ingui-nal hernia repair
PREDICTIVE FACTORS OF CHRONIC KIDNEY DISEASE IN KIDNEY DONORS AFTER LIVING-DONOR NEPHRECTOMY
Pokket Sirisreetreerux1, Malik Hajidae1, Charoen Leenanupunth1, Sith Phongkitkarun2
1 Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, 104002 Department of Radiology, Faculty of Medicine Ramathibodi Hos-pital, Mahidol University, Bangkok, Thailand, 10400
Background: Kidney transplantation (KT) is the ideal option for renal replacement therapy. Living-donor KT gained more popularity worldwide. However, from previous studies the incidence of chronic kidney disease (CKD) may occur in 1% of living donors, with a mor-tality rate of 4%. Appropriate selection of the donor is therefore an important concern. Objective: To determine the risk factors associated with post-donation CKD. Materials and Methods: We retrospectively review medical records of the patients who underwent donor nephrectomy between January 2011 to November 2017. Information on gender, age, BMI, preoperative creatinine with estimated glomerular filtration rate (GFR) using CKD-EPI formula, surgical approach and side of nephrectomy were collected. The kidney volume was calculated from computerized tomography (CT) scan using the Extended Brilliance Workspace system software. Postoperative GFR measurements within 18 months after nephrectomy were recorded. CKD was defined as GFR < 60 ml/min/1.73 m2. Risk factors as-sociated with CKD were determined using multivariable logistic regression models. Results: Among 452 patients, 36% were men. Mean age and BMI were 40 years old and 24.3 kg/m2, respectively. Mean ± SD preoperative GFR was 104.8 ± 15.3 ml/min/1.73m2. Mean ± SD of remaining kid-
ney volume was 124.7 ± 24.1 ml. Male gender and age over 40 years old were significantly associated with an increased risk of CKD, with OR’s of 3.6 (95% CI 2.0 to 6.6) and 5.6 (95% CI 3.2 to 9.7), respectively. Preopera-tive GFR of more than 100 ml/min/1.73 m2 and remain-ing kidney volume of more than 120 mL significantly decreased the risk of CKD, with OR’s of 0.09 (95% CI 0.06 to 0.16) and 0.5 (95% CI 0.3 to 0.8), respectively. Conclusion: Gender, age, preoperative GFR and remaining kidney volume were associated with post-donation CKD. Proper evaluation and selection of donors along with side of the kidney to be removed are key to preserve kidney function after donor nephrectomy. Keywords: Living-donor nephrectomy, Kidney donor, Predictive factor, Chronic kidney disease
URETEROSCOPIC LASER LITHOTRIPSY IN THE TREATMENT OF URETERIC STONES
Min Thway1, Sai Ngin2, La Win3, Myo Than4, Kyaw Hlaing5
1 Specialist Registrar (General Surgery) at Surgical Ward 2, Depart-ment of Surgery, Yangon General Hospital, University of Medicine 1, Yangon, Myanmar2 Consultant Urologist, Department of Urology, Yangon Speciality Hospital, University of Medicine 1, Yangon, Myanmar3 Associate Professor, Department of Urology, Yangon Speciality Hospital, University of Medicine 1, Yangon, Myanmar4 Professor, Department of Urology, San Pya General Hospital, University of Medicine 2, Yangon, Myanmar5 Former Professor and Head of Department of Urology, Yangon Speciality Hospital, University of Medicine 1, Yangon, Myanmar
Background: Laser technologies are established standard modalities for application on lithotripsy. The introduction of the Ho: YAG laser have broadened the indications for ureteroscopic stone management (URS) to include larger stone size throughout the whole up-per urinary tract. Ureteroscopy has evolved the most minimally invasive approach to the ureter and kidney. Furthermore, recent development in the design of ure-teroscopic and endoscopic instruments has enabled the URS to replace the open surgery treatments for urinary calculi over the last decade as a minimally invasive modality Ho: YAG. Objectives: 1. To describe the demographic factors of patients with ureteric stones. 2. To identify the intra- and post-procedural com-

Abstracts Thai J Surg Oct. - Dec. 2019132
plications within one month. 3. To determine the requirement for auxiliary pro-cedure and re-treatment after the procedure. 4. To find out the stone free rate after ureteroscopic laser lithotripsy. Materials and Methods: The study was hospital based prospective study which was carried out in De-partment of Urology, Yangon Speciality Hospital dur-ing one-year period from 1st January to 31st December, 2016. Total 45 patients were treated with semi-rigid Ho: YAG laser lithotripsy. URS was done with Karl Storz laser machine and Karl Storz semi-rigid ureteroscope. Demographic factor of the patients with ureteric stones, complications of URS laser lithotripsy within one month,
the requirement for the auxillary procedure, retreatment after the procedure and stone clearance rate were evalu-ated. Results: Overall stone clearance rate was 95.56%, no retreatment rate, requirement for auxillary procedure (ESWL as alternative) was 4.4%. Mean procedural dura-tion was 27.64 minutes and mean post-op hospital stay was 3.8 days. Effectiveness Quotient was 91.49%. Conclusions: Semi-rigid ureteroscopy using holmium laser is safe and effective option for treatment of ureteric stones. The results demonstrated that the holmium YAG laser has high overall stone clearance rate and low morbidity. Keywords: Holmium Laser, Ureteric Stones
Poster Non-Competition
COMPARISON OF COMPLICATION IN EX-TENDED LATISSIMUS DORSI FLAP VERSUS LATISSIMUS DORSI FLAP WITH IMPLANT IN TOTAL BREAST RECONSTRUCTION
Prakasit Chirappapha, Panya Thaweepworadej, Kasamar Chitmetha, Chayanoot Rattadilok, Thitipat Wattanakul, Sivaporn Pondeenana, Sermsri Pongratanakul, Tanet Chatmongkonwat,Songpol Phosuwan, Jirat TeerapradithBreast and Endocrine Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok
Background: Latissimus Dorsi (LD) myocutane-ous flap is one of the most popular and feasible technique for breast reconstruction after mastectomy. Breast pros-thesis can be used to decreased volume of the harvested myocutaneous flap and might be reduced functional deficit after reconstruction. Objective: We conducted the study to evaluated functional deficit and shoulder movement after extended LD flap compared with LD flap and prosthesis. Materials and Methods: Between December 2015 and May 2018, 31 patients performing LD flap in our institute were enrolled in the study. Patient demograph-ics, operative details, post-operative morbidities and shoulder movement were collected. Shoulder movement were evaluated pre- and post-operatively with range of motion (ROM) limitation and American Shoulder and
Elbow Surgeons Shoulder Score (ASES). Outcomes were compared between Extended LD flap and LD flap with prosthesis. Results: Twenty-one women were performed an immediate breast reconstruction with LD flap and prosthesis, and the rest of them were performed an extended LD flap. Seventy-four percent of the patients were performed an operation on the dominant side. Seroma (90.5% in LD flap with prosthesis group, and 90% in extended LD group). Four patients in LD flap with prothesis group and 1 patient in extended LD group had decreasing of shoulder ROM after 6 months of operation. Flexion was the most common direction that impaired after operation followed by extension and external rotation. But when evaluated with ASES score, only one patient in LD flap with prosthesis group had decreasing in only 1 point. The results were not statistically significant different between groups. When comparing by each question in ASES score, extended LD flap group had significant more time-to-recovery in the question of “wash your back/do up bra” and “throw a ball overhand”. Conclusion: Latissimus dorsi myocutaneous flap can be performed with a very low impact on shoulder function. In our study, slightly decreased in range of mo-tion was observed on both LD flap techniques, but there was no impact on functional outcome in ASES score. LD flap with prosthesis had shown faster functional recovery when compared with extended LD flap technique.

AbstractsVol. 40 No. 4 133
EFFECTIVENESS OF TRANSCATHETER ARTE-RIAL EMBOLIZATION FOR PATIENTS WITH SHOCK FROM ABDOMINOPELVIC TRAUMA
Thana Boonsinsukh1, Panitpong Maroongroge2
1 Department of Surgery, Faculty of Medicine, Srinakharinwirot University, Ongkharak, Nakhon Nayok, 26120, Thailand2 Department of Radiology, Faculty of Medicine, Srinakharinwirot University, Ongkharak, Nakhon Nayok, 26120, Thailand
Background: Transcatheter arterial embolization (TAE) is a useful endovascular technique for control hemorrhage in blunt abdominopelvic trauma without shock. In hypovolemic shock, open surgery is still con-sidered the gold standard treatment. However, several studies reported that TAE is safe and effective for control hemorrhage in these settings. Objective: To evaluate the effectiveness of TAE for patients with shock from abdominopelvic trauma. Materials and Methods: The medical records with abdominopelvic trauma at Her Royal Highness Princess Maha Chakri Sirindhorn Medical Center, Srinakharin-wirot University from January 2014 to January 2019 were retrospectively reviewed. We enrolled patients with shock underwent angiography suite. The exclusion criteria were patients who underwent transcatheter an-giogram but did not need to embolization. Shock status was defined as a systolic blood pressure of 90 mmHg or lower and a shock index 1.0 or greater. Results: Of the 319 patients, 13 patients with shock underwent TAE. 77% were male. The mean age was 38.6 years. The average injury severity score was 30.5. The most common mechanism of injury was traf-fic accident (84.6%). The embolization performed in 7 liver injuries, 5 pelvic fractures and 1 splenic injury. None of the patients had TAE failure. The treatment time for TAE was approximately 40 + 15.9 minutes. Mean length of hospital stay was 20.8 + 16.4 days. Two pa-tients died (15.4%). There was no embolization-related complication and repeat angiography was not required in all patients. A significant improvement in systolic blood pressure (p = 0.042) and decrease in heart rate (p = 0.003), lactate concentration (p = 0.027), crystalloid fluid (p = 0.002) and blood transfusion requirement (p = 0.003) were observed after TAE. Conclusions: TAE is a safe and effective method for treating shock patients with rapid response or
transient response in resuscitation. For non-response resuscitation, TAE is addition useful option for arterial hemorrhage control in abdominopelvic trauma. Keywords: Transcatheter arterial embolization, Abdominopelvic trauma, Hypovolemic shock
HEPATICODUODENOSTOMY AS AN ALTERNA-TIVE ENTEROBILIARY RECONSTRUCTION FOR HEPATECTOMY IN HILAR CHOLANGIO-CARCINOMA: SAKON NAKHON HOSPITAL EXPERIENCE
Nisit Tongsiri1, Witchuda Kittiwararit2, Tippawan Boonprom2, Hathaithip Boonporm2
1 Department of Surgery, Sakon Nakhon Hospital, Sakon Nakhon, Thailand2 Department of Nursing, Sakon Nakhon Hospital, Sakon Nakhon, Thailand
Background: The Curative treatment for hilar cholangiocarcinoma is hepatic resection with enterobili-ary reconstruction, and the reconstruction of choice is hepaticojejunostomy (HJ). However, some of HCCA patients in our case series could not be securely per-formed enterobiliary reconstruction with HJ as they had shortened mesentery or severe edematous small bowel; therefore, enterobiliary reconstruction with hepatico-duodenostomy (HD) was established. There were some reports showed favourable outcomes of HD as biliary reconstruction in liver transplantation, major post-operative bile duct injury, and choledochal cyst surgery; therefore, HD might be an alternative for enterobiliary reconstruction in resectable HCCA patients. Objective: To gather information of early outcomes of HD as enterobiliary reconstruction for hepatic resec-tion in HCCA. Materials and Methods: Data was retrospective collected from 26 patient records of hepatic resections in HCCA which were performed from May 2017 to April 2019 at Sakon Nakhon Hospital. Outcomes measure included total operative time, intra-operative blood loss, and morbidities were collected. Results: HJ was established in 23 patients. There were 3 hepatic resections had HD as enterobiliary recon-struction. The average total operative time in HJ group was 601 minutes and the average estimated blood loss was 1,886 ml. In HD group, the average total operative

Abstracts Thai J Surg Oct. - Dec. 2019134
time was 427 minutes and the average estimated blood loss was 1733 ml. In HJ group, there were post-operative liver (POLF) failure grade I in 3 patients (13%), POLF grade III in 1 patient (4.3%), post-operative bile leakage in 3 patients (13%), acute kidney injury (AKI) grade I in 4 patients (17.4%), AKI grade III in 2 patients (8.7%), su-perficial surgical site infection (SSI) in 2 patients (8.7%), deep SSI in 1 patients (4.3%), and portal vein thrombosis in 3 patients (13%). There was 1 peri-operative mortality in HJ group due to POLF. In HD group, there was only one complication which was POLF grade I. Conclusions: HD is a feasible alternative entero-biliary reconstruction for hepatic resection in HCCA when HJ cannot be performed.
IDIOPATHIC GRANULOMATOUS MASTITIS: A COMPARATIVE OUTCOME BETWEEN 44 PATIENTS WITH DIFFERENT TREATMENT MODALITIES
Prakasit Chirappapha, Panya Thaweepworadej,Chairat Supsamutchai, Namsiri Biadul, Panuwat Lertsithichai, Tanet Chatmongkonwat, Sermsri Pongrattanakul, Sivaporn Pondeenana, Songpol Phosuwan, Jirat TeerapradithBreast and Endocrine Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok
Background: Idiopathic granulomatous mastitis (IGM) is an uncommon benign chronic inflammatory which can clinically and radiographically mimic abscess or breast cancer. Definitive diagnosis was made by histo-pathology and the exclusion other identifiable etiology. An Optimal treatment strategy has yet to be established. Objective: The aim of the present study was to report and describe the clinical signs, radiological find-ings, management, clinical course, and clinical outcome after treatment of IGM. Materials and Methods: We retrospectively reviewed medical records of our institute from March 1990 to October 2016. A Total 44 patients were identified as having pathologically confirmed IGM. Patient cha-racteristics, clinical presentation, radiological findings, microbiological work-up, tissue pathology, treatment modalities, outcomes, and follow-up data were reviewed. Results: Forty-four women and one man were diagnosed as having IGM. The median follow-up time
was 21 months (range, 1 to 120 months). The mean age was 38 years (range, 20 to 81 years). The median time to diagnosis was 21 days (range, 2 to 246 days). Thirty patients were treated by surgery, 6 patients with steroid, and 3 patients with other modalities in the first setting. Multimodal treatment was required in one-third of patients. Only 25 of 39 patients (64%) were cured in the first setting. The median time-to-healing was 84 days (75, 115 and 238 days in surgery, steroid, and other modalities group, respectively). The surgical group had the shortest time-to-healing, but not significantly so (p = 0.23). In 25 patients who underwent surgical excision, 13 patients (52%) had wound complications. 5 of 39 patients (13%) had recurrence. Conclusion: IGM is not an uncommon benign condition which is sometimes difficult distinguish from malignancy. Surgery is associated with a shorter healing time, but has a high risk of wound complications. There was no significant difference between each treatment modality in terms of disease recurrence. Multimodal treatment was required in one-third of patients.
ISOLATED COLONIC METASTASIS FROM BREAST CANCER: THE FIRST CASE REPORT FROM THAILAND
Tanakorn Tarapongpun, Dunyapat Sa-nguanraksa,Pornchai O-charoenratDivision of Head Neck and Breast Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Objective: To report the unusual presentation of breast cancer patient with isolated colonic metastasis and treatment recommendation. Case presentation: A 62-year-old Thai female presented with abdominal pain for 4 months and signifi-cant weight loss since December 2017. Computerized tomography (CT) of whole abdomen revealed segmental wall thickening at transverse colon with two areas of hyper-enhancing mucosa. Colonoscopic examination demonstrated two lesions of short segment indurated submucosal infiltration at transverse colon. The biopsy was performed and revealed poorly differentiated ad-enocarcinoma. Further immunohistochemical study was consistent with lobular breast carcinoma in origin (CK7+/CK20-, CDX2-, GCDFP15-, TTF-1-, Napsin A-,

AbstractsVol. 40 No. 4 135
mammaglobulin+, GATA3+, ER+, PR-, HER-2-). Mam-mogram and breast ultrasonography showed 7.5x5.2 mm irregular indistinct hypoechoic mass at right upper quadrant. Excisional biopsy of right breast mass revealed invasive lobular carcinoma, moderately differentiated carcinoma (ER > 90%, Negative for PR and HER-2, Ki-67 6%). Additional metastatic work up including CT chest and bone scan showed no metastasis. Results: Final diagnosis was made as invasive lobular carcinoma with isolated colonic metastasis (cT1N0M1). She received treatment with letrozole 2.5 mg once daily since March 2018. At 6-month follow-up, her abdominal symptom and imaging were improved. Follow-up serum tumor markers were gradually decreased (CEA: 4.75 ± 3.62 ± 2.67; CA 15-3: 61.25 ± 47.69 ± 40.66). Conclusion: We reported the first case in Thailand of isolated colonic metastasis of non-palpable breast cancer. Colonic involvement by metastatic invasive lobular breast carcinoma suggests an advanced disease. Systemic hormonal or chemotherapy produces a favor-able response. Awareness of this condition may lead to proper investigations including colonic biopsy, thus avoiding unnecessary surgery.
LOCO-REGIONAL RECURRENCE AFTER NIPPLE-SPARING MASTECTOMY IN BREAST CANCER PATIENTS
Prakasit Chirappapha, Panya Thaweepworadej,Panuwat Lertsithichai, Thongchai Sukarayothin,Monchai Leesombatpaiboon, Sermsri Pongratanakul,Sivaporn Pondeenana, Tanet Chatmongkonwat, Songpol Phosuwan, Jirat TeerapraditDepartment of Surgery, Breast and Endocrine Surgery Unit, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Background: Although Breast Conserving Surgery (BCS) is the most commonly performed for early breast cancers, mastectomy still plays an important role, espe-cially for cancers with multicentricity and for prophy-lactic purposes. Previous studies reported locoregional recurrence (LRR) after nipple-sparing mastectomy (NSM) to be comparable to that of BCS. Objective: To determine oncologic safety and risk factors of LRR after NSM at our institute. Materials and Methods: We prospectively in-
cluded 65 NSM’s performed on 63 patients for both therapeutic and prophylactic indications from January 2007 to June 2017. Information on demographics, op-erative details, oncologic outcome, and post-operative complications was collected. Factors associated with LRR were also determined. Results: The mean age of patients was 43 years (30 to 61 years). Fifty-eight (89%) NSM’s were for therapeutic and 7 (11%) were for prophylactic indica-tions. Forty of 51 patients (78%) underwent NSM for invasive breast cancer, and the rest were for in-situ breast cancer. Necrosis of the nipple was the most common complication (19%), but most were successfully ma-naged conservatively. After an average follow-up of 40.4 months (8 to 128 months), no deaths were observed, but three patients (6%) developed locoregional recurrence, giving a three-year disease-free survival of 89.7%. One patient developed Paget’s disease of nipple, and required subsequent NAC excision, while the rest had regional lymph node recurrence. In a subgroup analysis, only triple-negative subtype showed an association with locoregional recurrence (p = 0.048). Conclusion : NSM is feasible and oncologically safe in selected patients. Nipple necrosis was the most common complication. A low rate of early locoregional recurrence was observed. The triple negative breast cancer subtype may be associated with LRR. Long-term follow-up is still required. Keywords: Nipple Sparing Mastectomy (NSM), Nipple-Areolar-Complex Sparing Mastectomy (NAC), Mastectomy, Breast reconstruction, Breast cancer, Lo-coregional recurrence (LRR)
PORTAL VEIN RESECTION IN HEPATECTOMY FOR HILAR CHOLANGIOCARCINOMA: A CASE SERIES FROM SAKON NAKHON HOSPITAL
Nisit Tongsiri1, Witchuda Kittiwararit2, Tippawan Boonprom2, Hathaithip Boonporm2
1 Department of Surgery, Sakon Nakhon Hospital, Sakon Nakhon, Thailand2 Department of Nursing, Sakon Nakhon Hospital, Sakon Nakhon, Thailand
Background: Aggressive en bloc liver resection with vascular resection is necessary for curative treat-ment of hilar cholangiocarcinoma (HCCA) with portal

Abstracts Thai J Surg Oct. - Dec. 2019136
vein invasion (PVI), the safety of portal vein resection (PVR) has been demonstrated by many leading hepato-biliary centers. However, for novice hepatobiliary center, PVR is challenging procedure, and the early outcomes of PVR in HCCA should be monitored. Objective: To gather information regarding early outcomes of PVR in hepatectomy for HCCA in Sakon Nakhon Hospital. Materials and Methods: Data was retrospectively collected from 26 resectable HCCA patients from May 2017 to April 2019 at Sakon Nakhon Hospital. Outcomes measure include total operative time (TOT), estimated blood loss (EBL), blood transfusion (BT), Pringle's ma-neuver duration (PMD) and peri-operative morbidities were collected. Results: There were 6 PVR (23.1%) from total 26 hepatic resection for HCCA in this series. There was no statistical significant in average TOT (547 mins vs 638 mins, p = 0.273), EBL (1,972 ml vs 1,373 ml, p = 0.41), BT (653 ml vs 593 ml, p = 0.83), and PMD (42 mins vs 46 mins, p = 0.98) between no PVR group and PVR group. The complications between no PVR group and PVR group had no statistical significant; these compli-cations were post-operative biliary fistula (3 cases vs 1 case, p = 1), post-operative liver failure (4 cases vs 1 case, p = 1), acute kidney injury (5 cases vs 1 case, p = 1), surgical site infection (4 cases vs 0 case, p = 0.54), Portal vein thrombosis (1 case vs 2 cases, p = 0.123), chylous ascites (1 case vs 1 case, p = 0.42), intercostal drainage for post-operative pleural effusion (2 cases vs 0 case, p = 1), and peri-operative death (1 case vs 0 case, p = 1). Conclusion: PVR can be performed to increase R0 resection in resectable HCCA with PVI without significant increase in TOT, EBL, BT, PMD, and com-plications.
SHORT-TERM OUTCOMES OF SUTURE VERSUS RING ANNULOPLASTY FOR FUNC- TIONAL TRICUSPID REGURGITATION CON-COMITANT WITH MITRAL VALUE REPAIR IN CENTRAL CHEST INSTITUTE OF THAILAND (CCIT)
Thanit Kunanusont, MD, Sahapom Wathanawani-chchakun, MD, Suthon Narongchaikul, MD, Chakkraphun Jampates, MD, Piyawat Lerdsomboon, MD, Pramote Porapakkham, MD,
Chaiwut Yottasurodom, MD, Choosak Kasemsarn, MD, Taweesak Chotivatanapong, MDDepartment of Cardiothoracic Surgery, Central Chest Institute of Thailand, Nonthaburi, Thailand
Background: Prophylactic tricuspid annuloplasty is currently issued worldwide. Surgical techniques of tricuspid annuloplasty have been being debated. Objective: To compare short-term outcomes between suture and ring annuloplasty for correcting functional tricuspid regurgitation in patients underwent mitral value repair at CCIT. Materials and Methods: A respective review of 133 patients underwent tricuspid annuloplasty con-comitant with mitral value repair (MVr) from 2011 to 2015. Suture and Ring annuloplasty were performed in 45 patients (Bicuspidization; 100%) and 88 patients, respectively. Postoperative echocardiographic moderate or greater TR was compared between groups and factors for improving post-operative TR were identified. Results: Patient characteristics intraoperative data were comparable except pre-operative AF that was higher in ring group (p < 0.001) and AOX time that was higher fin suture group (p = 0.008). pre=operative echocardiographic values were significantly worse in ring group including LVEF (60.2212 vs. 65.6f 7.5%; p = 0.002), LVEDD (56.8k 11.8 vs. 51.6 ± 8.0 mm; p = 0.003) and RVDd (23.1f 7.7 vs. 17.3 + 8.1 mm; p = 0.002). Mean follow-up time was 182 days (p = 0.90). Post-operative moderate or greater TR was higher in suture group but no statistically significant difference (15.6% vs. 9.1%; p = 0.265). Post-operative moderate or greater TR in ring group was significantly lower than suture group in degenerative MVr (0% vs. 17.6%; p = 0.019). There were no significant differences of moder-ate or greater TR between groups in any MVr results. Multivariate analysis showed no pre-operative atrial fibrillation and ring annuloplasty as significant factors for improving post-operative TR in severe mitral regur-gitation patients. Conclusion: Suture and ring annuloplasty are ac-ceptable for correcting functional tricuspid regurgitation. However, ring annuloplasty is better for controlling post-operative tricuspid regurgitation in severe mitral regurgitation patients during short-term follow-up. Keywords: Functional tricuspid regurgitation, Tri-cuspid value repair, Annuloplasty, Mitral value repair, Bicuspidization

AbstractsVol. 40 No. 4 137
VALIDATION OF CANCERMATH MODEL AS PROGNOSTIC TOOL FOR THAI BREAST CAN-CER PATIENTS
Nuanphan Polchai1, Warapan Numprasit1, Doonyapat Sa-nguanraksa1, Suthipol Udompunthurak2, Pornchai O-charoenrat1
1 Division of Head Neck and Breast Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand2 Division of clinical epidemiology, Department of Health Research and Development, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Background: Web-based prognostic programs have been developed to aid decision making for adjuvant systemic treatment in breast cancer. CancerMath model is one of the web-based prognostic tools which predict survival up to 15 years after diagnosis of breast cancer. Objective: To validate the CancerMath model in Thai breast cancer patients. Materials and Methods: A total of 655 patients who underwent surgical treatment for stage I to III breast cancer from 2003 to 2011 at the Division of Head Neck and Breast Surgery, Department of Surgery, Siriraj Hospital, Mahidol University, Thailand were recruited. Model-predicted overall survival (OS) with patient’s actual OS were compared. The ability of the model was evaluated by using receiver-operating characteristic (ROC) analysis. Analyses were performed using SPSS for Window version 22.0 (SPSS Inc., Chicago, IL, USA). Results: The median age at diagnosis was 50 years (27-86 years). Median tumor size was 2.4 cm (0.1-17.5 cm) and 40.46 % of the patients had lymph node metasta-sis; 61.53% of them had estrogen-receptor positive breast cancer. Most of the patients received systemic therapy (94.35%). CancerMath-predicted and observed 5-year OS were 88.6% and 91.8%, respectively. CancerMath-predicted and observed 10-year OS were 77.3% and 87.4%, respectively. The area under ROC curve for 5-year and 10-year OS was 0.73 (95% CI = 0.67-0.80) and 0.75 (95% CI = 0.68-0.81), respectively. Conclusions: CancerMath model slightly under-estimated OS, however, this model might be used as a prognostic tool in Thai breast cancer patients. Keywords: Breast cancer, Predictive model, Cancer Math, Survival
VALIDATION OF MAGEE EQUATION IN PRE-DICTING RESPONSE TO NEOADJUVANT CHE-MOTHERAPY IN HORMONE RECEPTOR POSI-TIVE AND HER2 NEGATIVE BREAST CANCER PATIENTS
Napat Saigosoom1, Eng O-charoenrat2, Doonyapat Saguanraksa1, Suthipol Udompunturak3, Pornchai O-charoenrat1
1 Division of Head and Neck Surgery, Department of Surgery, Siriraj Hospital, Mahidol University, Bangkok, Thailand 107002 Faculty of Medical Sciences, University College London, London, United Kingdom WC1E 6BT3 Department of Research Development, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand 10700
Background: Magee Equations have been de-veloped as accurate tools for predicting complete pathological response and clinical outcomes in breast cancer patients treated with neoadjuvant chemotherapy. Therefore, they have been used effectively in routine clinical practice. Objective: To assess for complete pathological response rates (pCR) after neoadjuvant chemotherapy (NAC) in hormonal receptor (HR) positive, HER2 nega-tive breast cancer using Magee Equation 2 scores in Thai patients. Materials and Methods: Patients with HR posi-tive, HER2 negative breast cancer who received NAC from January 2010 to May 2018 at Siriraj Hospital, Mahidol University, Thailand were retrospectively re-viewed. The pCR was defined as the absence of invasive tumor in the breast resection specimens; residual in situ carcinoma was allowed. Pre-treatment status of HR and HER2 were used to calculate the Magee Equation 2 Scores using the equation: “18.8042 + Nottingham score x 2.34123 + ER H-score (-0.03749) + PR H-score (-0.03065) + (0 for HER2 negative, 1.82921 for equivocal, 11.51378 for HER2 positive) + tumor size x 0.04267” The Magee Equation scores were divided into 3 categories to match the Oncotype Dx: 0 to <18 (low), 18 to <31 (intermediate), and 31 or higher scores (high). The pCR rate with respect to Magee Equation categories was analyzed. Kaplan-Meier survivals curved for disease free survival and overall survival were analyzed with respect to Magee Equation categories. P-values were obtained using log rank tests.

Abstracts Thai J Surg Oct. - Dec. 2019138
Results: A total of 757 women were identified within the designated time window, of whom 215 were eligible for participation. The pCR rate for low, intermediate, and high Magee Equation 2 scores was 4.8%, 3.6%, and 23.8%, respectively. Patients with high Magee Equation 2 scores were more likely to achieve pCR compared with those with intermediate or low scores (OR = 7.41, 95% CI 2.63-20.91, p < 0.001). Those with high Magee Equation 2 Scores had higher locoregional recurrence (OR = 2.47, 95% CI 1.05- 5.78, p = 0.045). The 5-year disease-free and overall survival rates were
69.7%, 50.8%, 54.9%, and 80.2%, 81.0%, 61.8% for low, intermediate, and high scores, respectively. The patients with high score had significantly lower overall survival (p = 0.034). Conclusion: Among patients with HR positive and HER2 negative/equivocal breast cancer treated with NAC, Magee Equation is a highly effective tool for predicting the pCR and clinical outcome. Keywords: Breast cancer, Magee Equation, Neo-adjuvant chemotherapy, Pathologic complete response, Survival
Resident Contest Award
A COMPARATIVE STUDY OF DIFFERENT PRE- SERVATION METHODS FOR DICED CARTILAGE GRAFT VIABILITY: A RANDOMIZED DOUBLE-BLIND CONTROLLED TRIAL
Niti Chuysakul, MD1, Sarayuth Dumrongwongsiri, MD1,Artit Jinawath, MD2, Surawej Numhom, MD1
1 Division of Plastic and Reconstructive surgery, Department of Surgery, Ramathibodi Hospital2 Department of Pathology, Ramathibodi Hospital
Background: Diced costal cartilage graft has recently widespread use for primary and secondary rhi-noplasty. Preserved autologous costal cartilage has been use in patient who had undergone primary rhinoplasty and required revision procedure. The viability of costal cartilage grafts, in many forms, has been researched since the using of costal cartilage grafts in surgical pro-cedures but preservation period and viability of costal cartilage grafts have not been described. This study was performed to compare the viability of diced costal cartilage grafts when preserved in different media and temperature. Materials and Methods: Costal cartilage graft was obtained from ten patients. Each cartilage was diced into 1-mm pieces and preserved in 3 groups. From each group were sampling at immediate, 4 weeks, 12 weeks and 24 weeks after harvested; processed by thin-section histo-logy; stained with hematoxylin and eosin; and evaluated to determine costal cartilage viability and architectural characteristics. Results: Diced costal cartilage grafts preserved in NSS at -20 °C had the highest viability and also de-
monstrated the strongest staining with the hematoxylin and eosin stains. Diced costal cartilage preserved in UW solution yielded the lowest viability and minimal stain-ing with hematoxylin and eosin. Furthermore, absolute numbers of nucleated lacunae and basophilic lacunae were significantly higher for grafts preserved in NSS at -20°C at 24 weeks compare to other groups. Conclusions: Diced costal cartilage graft is be-coming widespread use in primary and secondary rhi-noplasty. There are many ways to preserved cartilage grafts. This study demonstrates that preservation of diced costal cartilage grafts in NSS at -20°C is the best way to preserve diced costal cartilage graft among 3 groups and can be preserved up to 24 weeks after harvested. Keywords: Diced costal cartilage graft, Rhino-plasty, Hematoxylin, Eosin
A RANDOMIZED CONTROLLED STUDY COM-PARING CLINICAL OUTCOMES BETWEEN NON-INVASIVE CONTINUOUS POSITIVE AIR-WAY PRESSURE VENTILATION (NIV-CPAP) AND CONVENTIONAL OXYGEN THERAPY IN SEVERE TRAUMATIC BLUNT CHEST INJURY PATIENTS
Jatuporn Sirikun, Natthida Owattanapanich, Sumawadee BoonyasurakDepartment of Surgery, Faculty of Medicine, Siriraj hospital, Bang-kok 10700, Thailand
Background: Several studies have suggested that non-invasive ventilator reduced mortality and intuba-

AbstractsVol. 40 No. 4 139
tion rate in respiratory failure. However, the benefits of NIV-CPAP for the management of blunt chest trauma are still controversial. Objective: To compare the clinical outcome be-tween NIV-CPAP and conventional oxygen therapy. Materials and Methods: A randomized control trial was conducted in level I trauma center hospital. The inclusion criteria were adult patients who had blunt chest injury with trauma thoracic severity score between 5-15 points or chest AIS ≥ 3 points. Patients were randomly assigned between receiving conventional oxygen therapy providing by mask with bag > 10 LPM and NIV- CPAP. All parameters were monitored, including vital signs, clinical respiratory failure and artery blood gas at before and after the receiving oxygen therapy. The primary outcome was the intubation rate and secondary outcomes were length of hospital stay and ICU stay, mortality rate and complications. Results: We included total 28 patients, 12 patients in NIV-CPAP group and 15 patients in conventional oxygen therapy group. A patient was excluded from this trial. The baseline characteristics of patients in each group were no differences. This study was prematurely stopped due to significant higher rate of intubation in the control group (33.33%). Moreover, the infection rate in control group was higher than experimental group but no significant differences were observed in LOS, ICU stay and other secondary outcomes. Conclusion: The results of this study suggested that NIV-CPAP was potential to be useful in the management of severe traumatic blunt chest injury patients. Keywords: Noninvasive ventilator continuous positive airway pressure, Blunt chest injury, Thoracic trauma severity score
ASSOCIATION BETWEEN SERUM BETA 2 MICROGLOBULIN LEVELS AND CLINICO-PATHOLOGIC MOLECULAR SUBTYPES OF BREAST CANCER
Sorrasit Jongvilaikasem, Somrit Mahattanobon, Srila Samphao, Surasak SangkhathatDepartment of Surgery, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla 90110, Thailand
Background: β2-microglobulin (β2-M) is a low molecular weight protein which is a part of the invariant
light chain of the HLA antigen molecule. An immunohis-tochemical study reported that serum β2-microglobulin in breast cancers was significantly higher than that of benign breast tumors. In addition, expression levels of β2-M protein in breast cancer significantly differ among the 4 molecular subtypes. Objective: To determine the association between serum β2-M level and clinico-pathologic molecular characteristics of breast cancer, including the molecular subtype and clinical stages. The results of this study may support the use of serum β2-M level as a prognostic marker in breast cancer. Materials and Methods: A prospective cohort study was conducted, obtaining serum samples from fe-male patients who had histologically confirmed invasive breast cancer and who were treated at Songklanagarind Hospital during the years 2017-2018. Results: A total of 160 patients were included in the present study. The most common histological type was invasive ductal carcinoma (152 cases; 95%) the most frequent tumor grade was grade II (72 cases; 45%), and 58 cases (45%) had lymphovascular invasion. Most patients had T2 staging (84 cases; 53%), Most metastasis (7 cases, 4%). The most common molecular subtype was luminal A, followed by luminal B and the others. Serum β2-M level was found to be significantly associated with age and metastatic. Conclusion: Serum β2-M was significantly higher in women with metastatic breast cancer when compared to those with no metastasis. The marker may have a role in the prediction of metastatic status and prognostication of breast cancer.
CHEST RADIOGRAPHY AND CLINICAL OUT-COME OF CONGENITAL DIAPHRAGMATIC HERNIA IN SONGKLANAGARIND HOSPITAL
Napasorn Phutong, Piyawan Chiengkriwate, Surasak Sangkhathat, Kaimook BoonsanitDivision of Pediatric Surgery, Songklanagarind Hospital, Faculty of Medicine, Prince of Songkla University, Hatyai, Songkla, 90110, Thailand
Background: Chest x-ray radiography (CXR) re-sults were evaluated for clinical outcomes of persistent pulmonary hypertension (PPH) and pulmonary hypo-plasia (PH) in congenital diaphragmatic hernia (CDH).

Abstracts Thai J Surg Oct. - Dec. 2019140
Materials and Methods: Twenty-two neonates with CDH were retrospectively reviewed for patient demography, clinical data, initial arterial blood gas, CXR and PPH to assess operative findings, treatment outcome and survival. Results: An intrathoracic stomach (ITS) was found in 6/22 CXR examinations with statistically significant differences in Apgar score at 1 minute and 5 minutes (1-min; ITS 7 (6,8) versus non-ITS 8 (8,9) p = 0.018, 5-min; ITS 7.8 (1.8) versus non-ITS 9.2 (0.7) p = 0.035), initial arterial blood gas bicarbonate level (ITS 15.5 (14.7, 19.2) versus non-ITS 21.2 (20.2, 23.4) p = 0.007), and PPH (50% ITS versus 6.2% non-ITS, p = 0.046). Pulmonary hypoplasia (PH) shape was recorded by CXR as apex 14/22 and hilar 8/22 with no statistically significant differences in clinical outcomes and PPH. Regarding the severity of mediastinal shift on chest x-ray results, 17/22 CXR examinations showed medi-astinal shift displaced more than the mid-clavicular line with no statistically significant differences in clinical outcome, hernia content, PPH, length of hospital stay (LOS), complication, and survival. Conclusion: Intrathoracic stomach findings in-vestigated by CXR were demonstrated as markers of possible PPH. Furthermore, pulmonary hypoplasia shape and severity of mediastinal shift did not correlate with any clinical outcome, hernia content, PPH, LOS, complication and survival. Keywords: Congenital Diaphragmatic Hernia, Pulmonary hypoplasia, Persistent pulmonary hyperten-sion of the newborn, Intrathoracic stomach, Lung-thorax ratio
COMPARATIVE STUDY OF THREE FAT GRAFT FILTRATION TECHNIQUES ON THE VOLUME EFFICACY AND THE ADIPOCYTE VIABILITY: AN EXPERIMENTAL STUDY
Sirada Suttiwattana, Surawej Numhom, Ajchariya Sarovath, Thiti TantithamDivision of Plastic and Reconstructive Surgery, Department of Sur-gery, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Background: Fat grafting has been widely used in plastic surgery operations in both aesthetic and recon-structive surgery. Centrifugation is a common method for fat preparation. However, a centrifuge machine may not be available, and there are also many specific steps to be followed in order to obtain the condensed fat. An alternate method for the fat preparation is the
filtration technique. Various materials have been tested as a filter, and currently there has been no research which investigated the filter performances in comparison. Objectives: To evaluate the volume and concen-trating efficacy of three different filtration materials, i.e. nylon cloth, Telfa and metal sieve. Also the adipocyte viability of fat obtained by both centrifugation and filtra-tion techniques would be compared. Materials and Methods: Lipoaspirate was ob-tained from nine female patients undergoing cosmetic liposuction. To determine the volume efficacy, lipoaspi-rate was divided into four specimens equally for one centrifugation and three filtration techniques with nylon cloth, Telfa and metal sieve. Each processed fat was then spun further to assess the separation of its compo-nents and the volume of fat loss. Results: Nylon cloth, Telfa and metal sieve filters were as effective as the centrifugation technique in re-moving oil and aqueous components. The filtration group showed significant decrease in the fat volume compared to the centrifugation. The nylon cloth and the metal sieve filters yielded more fat losses of 29 ± 11% and 32 ± 9% respectively. Nonetheless, the fat loss measured from Telfa was only 16 ± 8 %. Conclusions: As far as this study was concerned, Telfa was the most effective filtration material compared to nylon cloth or metal sieve. Despite some fat loss in the process, the filtration technique is a simpler and economical method for fat grafting preparation in the case which the centrifugation method is not available. Keywords: Lipoaspirate, Nylon cloth, Telfa, Metal sieve
CORRELATION OF TRANSIENT ELASTOGRA-PHY AND PROGRESSION OF CIRRHOSIS IN LONGTERM SURVIVORS OF BILIARY ATRESIA
Witsanee Srisuwan1, Surasak Sangkhathat1, Piyawan Chiengkriwate1, Panu Wetwittayakhlang2,Supika Kritsaneepaiboon3
1 Department of Surgery, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla 90110, Thailand 2 Department of Internal Medicine and NKC Institute of Gastroen-terology and Hepatology, Faculty of Medicine, Hat Yai, Songkhla 90110, Thailand 3 Department of Radiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla 90110, Thailand
Background: A recent developed non-invasive tool, transient elastrography (TE), has been reported to

AbstractsVol. 40 No. 4 141
provide good correlation between liver stiffness mea-surement (LSM) and liver fibrosis in various chronic liver diseases in adults and children. Objective: To use transient elastography (TE) to evaluate the correlation between liver stiffness measure (LSM) and functional status of native liver in longterm follow up of pediatric patients with biliary atresia (BA). Materials and Methods: Twenty cases of BA who had undergone hepatic portoenterostomy and had good initial outcome (total bilirubin < 2 mg/dL) were enrolled for a transient elastography. The LSMs derived from the study were analyzed with clinical and radiological pa-rameters and endoscopic findings of esophageal varices. Results: The median age at enrollment of the 20 cases was 8.4 years. Of the 20 cases, 15 were diagnosed as cirrhosis by ultrasonography and 9 had esophageal varices detected by an endoscopy. Parameters that were significantly associated with LSM were history of cholangitis, splenomegaly, cirrhosis and esophageal varices. Significantly higher LSM was found to be cor-related with hyperbilirubinemia, transaminitis, alkaline phosphatasemia, thrombocytopenia and prolonged INR. On linear regression, LSM was significantly correlated with pediatric end-stage liver disease score at the r
2of
0.32 and correlated with the aspartate transaminase to platelet ratio index at the r
2 of 0.70. The area under the receiver operating characteristic curve that reflected the performance of LSM in predicting esophageal varices was 0.97. At the cut-off value of 10.2 kPa, the sensitivity and specificity of LSM in predicting esophageal varices were 100% and 72.7%, respectively. Conclusion: TE can be useful as a non-invasive, point-of-care evaluation of liver fibrosis in long term follow-up of BA. A high LSM indicates surveillance for esophageal varices in these patients. Keywords: Transient elastrography, Biliary atresia, Liver stiffness measurement
DOES STEPPED GRAFTS DECREASE THE HE-MODYNAMIC CHANGE AFTER HEMODIALY-SIS ACCESS CREATION? THE FINGER-BRA-CHIAL INDEX EVALUATION: RANDOMIZED CONTROLLED TRIAL
Patompong Akkarapattanakool, MD, Piyanut Pootracool, MD, Wiwat Tirapanich, MD, Sopon Jirasiritum MD, Surasak Leela-Udomlipi, MD, Suthas Horsirimanont, MD,
Nutsiri Kittitirapong, MD, Chaowanan Pornwarakorn, MDDivision of Vascular Surgery, Department of Surgery, Faculty of Medicine Ramathibodi hospital, Mahidol University, Bangkok, Thailand
Background: Stepped graft is commonly used in hemodialysis patients to prevent ischemia steal syn-drome; however, its efficacy remains uncertain. Objective: To compare hemodynamic change in microvascular perfusion in the hemodialysis patients who used standard 6 mm diameter polytetrafluoroethy-lene (PTFE) graft to the patients who utilized 4-7 mm stepped PTFE graft and access potential risk factors lead-ing to development of steal syndrome after hemodialysis access creations. Materials and Methods: A total of 60 patients who were underwent brachial artery-based hemodialysis ac-cess during June, 2018 to January, 2019 were identified in a randomized double-blinded clinical trial. All patients were divided equally into 2 groups. A control group of 30 patients were received forearm dialysis access using the standard 6 mm PTFE grafts while another group of 30 patients were received 4-7 mm stepped grafts. All patients were assessed pre- and postoperative finger pressures and finger brachial index (FBI). In addition, univariate analysis and multivariate analysis were per-formed to analyze primary and assisted primary patency rate, time to develop the ischemic steal and reinterven-tion rate. Results: Of the 60 patients with hemodialysis access grafts, median age of patients who received the standard 6 mm grafts (n=30) and the 4-7 mm stepped grafts (n=30) and were 62.5 years and 67.5 years, respectively. There was no significant in median operation times between the 6 mm grafts group and the 4-7 mm stepped grafts group (117.5 minutes vs 119 minutes; p = 0.50). Mean arterial pressure and mean finger pressure were not significant different (148.72 mmHg vs 151.48 mmHg; p = 0.70 and 141 mmHg vs 128.5 mmHg; p = 0.62). The outcome from the univariate analysis found out that 3 risk factors significantly related to ischemic steal which are FBI postop day 1 (OR = 0.01, 95% (CI), 0-0.63; p = 0.028), FBI 2 weeks (OR = 0.92, 95% (CI), 0.86-0.98; p = 0.017) and Female gender (OR = 8.55, 95% (CI), 1.02-71.63; p = 0.048). Kaplan Meier survival analysis showed that the FBI results of the patients receiving stepped grafts were improved after 3 months

Abstracts Thai J Surg Oct. - Dec. 2019142
post operation, however, there is no significant different in complications compared to the patients receiving the 6 mm grafts. Conclusions: 4-7 mm stepped grafts can improve hemodynamic change in hemodialysis access patients after 3 months post operation with no difference in pri-mary patency rate and complications compared to the standard 6 mm grafts. Keywords: Dialysis Grafts, Stepped grafts, Steal syndrome, Finger brachial index
EFFECT OF PUBOPROSTATIC LIGAMENT PRESERVATION DURING ROBOTIC-ASSISTED LAPAROSCOPIC RADICAL PROSTATECTOMY ON EARLY CONTINENCE: RANDOMIZED CON-TROLLED TRIAL
Wattanachai Ratanapornsompong1, Suthep Pachara-takul2, Premsant Sangkum1, Chareon Leenanupan1, Wisoot Kongcharoensombat1
1 Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand2 Division of Urology, Department of Surgery, Police Hospital, Bangkok, Thailand
Background: Prostate cancer is the eighth most common cancer in Thailand. Post-radical prostatectomy incontinence is common. Continence is an important factor in improving patient quality of life. Most patients will regain continence in the first year after surgery, but enhancing continence recovery is still attractive due to better quality of life. Objective: To prove the effectiveness of pubo-prostatic ligament-preserving RARP on enhancing early continence compared with the standard technique RARP. Moreover, the margin status is also compared between the two groups. Materials and Methods: Ninety-two patients with localized adenocarcinoma of the prostate scheduled for RARP from August 2017 to January 2019 were prospec-tively single-blinded and randomized into two groups: group A included patients for whom a standard RARP was performed (n = 46), and group B included patients for whom a puboprostatic ligament-sparing RARP was performed (n = 46). The primary outcome was conti-nent status at Foley catheter removal day and 3 months after surgery using the score from the International
Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form (ICIQ-UI SF) and pad usage. The secondary outcomes were the pathological margin status, blood loss, operative time, and complications. Results: Ninety-six patients were enrolled in this trial, with a mean age of 67.3 (6 years and median Prostate-Specific Antigen (PSA) of 9.77 ng/ml (range: 0.92–64). There were no significant differences in baseline characteristics. Continence status at 3 months postoperative was evaluated by the ICIQ-UI SF. The mean score was 8.74 (4.28 for group A and 6.93 (3.96 for group B. The score was better for group B (p = 0.038). There was one case in group A of complete or severe incontinence (more than 5 pads/day) at 3 months after surgery. Groups A and B did not exhibit significant differ-ences regarding their margin status (p = 0.828). Positive margins were detected in 34.78% of patients in group A and 36.96% in group B. There was also no difference in perioperative parameters: blood loss, operative time, and perioperative complications. Conclusion: We propose the use of puboprostatic ligament-sparing RARP as a method to accelerate early continence without affecting the final oncological out-come.
FACTOR INFLUENCING VENOUS LEG ULCER HEALING AND RECURRENCE RATE AFTER ENDOVENOUS RADIOFREQUENCY ABLATION OF INCOMPETENT SAPHENOUS VEIN
Jarunee Jieamprasertbun, MD1, Nuttawut Sermsatha-nasawadi, MD, PhD1, Sasima Tongsai, PhD2
1 Division of Vascular Surgery, Department of Surgery, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand2 Division of Clinical Epidemiology, Department of Research and Development, Faculty of Medicine, Siriraj Hospital, Mahidol Uni-versity, Bangkok, Thailand
Objective: While compression bandaging is the mainstay of leg ulcer treatment. Recently, the EVRA trial, reveals early endovenous saphenous ablation ac-celerates VLU healing. Our study was performed to evaluate the rate of VLU healing and recurrence after saphenous ablation by radiofrequency ablation (RFA). Materials and Methods: We retrospectively re-viewed all CEAP C5 or C6 patients treated with RFA to define the incidence of ulcer healing and recurrence

AbstractsVol. 40 No. 4 143
in Siriraj Hospital, Bangkok, Thailand between January 2011 and December 2017. Time to healing, time to ulcer recurrence and factors associated with ulcer healing and ulcer recurrence were evaluated by Kaplan-Meier survival analysis. Results: Sixty-two limbs including C6 32 limbs and C5 30 limbs were included. RFA was performed in 58 great saphenous veins (GSV) and 2 anterior accessory saphenous veins (AASV). Concomitant RFA of GSV and AASV were performed in 2 limbs. Deep venous insufficiency was present in 10 limbs (16%). Median follow-up time was 753 days after RFA. VLU healed 31% at 3 months, 47% at 6 months, and 66% at 1 year after RFA. Concomitant ultrasound-guided foam sclero-therapy (UGFS) of the pathologic perforating vein was the improving factor for ulcer healing [HR 2.83 (95% CI: 1.07-7.55); p = 0.03]. VLU recurrence was found 8% at 1 year, 14% at 2 years, and 23% at 3 years after RFA. VLU recurred significantly more often in patients with deep venous insufficiency [HR 3.722 (95% CI 1.049-13.207); p = 0.029]. Conclusions: UGFS of the pathologic perforating vein at the time of RFA of saphenous vein improved VLU healing. VLU recurrence was more frequent in patients with concomitant deep venous reflux. We suggest per-forming UGFS of the pathologic perforating vein at the time of RFA of incompetence saphenous vein to improve VLU healing. Patients with associated deep vein reflux should be monitored for ulcer recurrence.
ILIOCAVAL VENOUS OBSTRUCTION IN THAI PATIENTS WITH ADVANCED CHRONIC VENOUS INSUFFICIENCY
Parichat Tanmit, Nuttawut Sermsathanasawadi, Kanin PruekprasertDivision of Vascular Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Background: Patients with advanced chronic venous insufficiency (CVI) have a high incidence of iliocaval venous obstruction (ICVO). Although direct Duplex Ultrasound Scanning (DUS) of the inferior vena cava and iliac veins may not provide sufficient diagnosis detail due to the presence of bowel gas and body fat, indirect evidence from DUS could be helpful. Objective: To determine the prevalence and
clinical predictors and accuracy of > 50% ICVO in Thai patients with advanced CVI, as well as the accuracy of indirect DUS for the diagnosis of ICVO. Materials and Methods: Patients with lipoder-matosclerosis, healed or active venous leg ulceration (C4b-C6) were prospectively enrolled into the study. Patients were evaluated by DUS and Computed Tomo-graphic Venography (CTV). DUS was used to determine the presence of loss of respiratory variation in common femoral vein (CFV) and reversed flow in superficial epigastric vein (SEV). Percentage of venous obstruction was measured using the observed cross-sectional area of luminal stenosis on CTV. The prevalence and clinical predictors of > 50% ICVO were determined, and the accuracy of DUS for the diagnosis of > 50% ICVO was compared with CTV. Results: A total of 106 patients (135 limbs) were enrolled. The mean age was 58 ± 12 years, and 57 (54%) of patients were women. Greater than 50% ICVO by CTV was found in 37 (27%) limbs. Independent pre-dictors of > 50% ICVO included the left-side (OR: 4.1; 95% CI 1.8 to 9.7) and previous history of DVT in the affected leg (OR = 5.2; 95% CI 1.9 to 14.2). The sensi-tivity and specificity of loss of respiratory variation in CFV, for the diagnosis of > 50% ICVO, were 24 % and 100%, respectively; the sensitivity and specificity of the reversed flow in SEV were 20% and 100%, respectively. Conclusion: Limbs with C4b-C6, especially in the left side or with a history of DVT in that limb, had a high prevalence of ICVO and may usually undergo DUS. Limbs with positive DUS results, including loss of respiratory variation in CFV or reversed flow in SEV, should be considered for venous intervention, but those with negative DUS findings may require CTV.
OUTCOME OF THE LIFT PROCEDURE FOR COMPLEX ANAL FISTULA AT A TERTIARY CARE HOSPITAL IN SOUTHERN THAILAND
Supakool Jearanai, MD, Worrawit Wanitsuwan, MDDepartment of Surgery, Faculty of Medicine, Prince of Songkhla University, Hat Yai, Songkhla 90110, Thailand
Background: Complex anal fistula is commonly encountered disease, which requires careful evaluation before a definitive repair.At Songklanagarind Hospital, ligation of the intersphincteric fistula tract (LIFT), with

Abstracts Thai J Surg Oct. - Dec. 2019144
or without combination with electrocautery under direct vision (video-assisted anal fistula treatment, VAAFT), also called VA-LIFT is used for fistula treatment. Objective: To evaluate the effectiveness of the LIFT procedure for the treatment of complex anal fistula, in terms of healing and the recurrent rates and fecal incontinence at 1 year after the procedure, as well to identify associated risk factors. Materials and Methods: A retrospective study of 229 complex anal fistula patients who underwent the LIFT procedure at Songklanagarind Hospital from January 2012 to December 2017 was performed. Infor-mation on age, sex, comorbidity, history of previous anal surgery, prolonged sitting time on toilet seat, smoking, alcohol drinking, spicy food consumption, fistula char-acteristics, fistula recurrences and fecal incontinence was collected. Result: Of the 229 patients, 167 (73%) healed completely at the end of follow-up. There were 63 (27%) recurrences, but none had post procedure fecal incontinence. Electrocautery via the VAAFT technique was protective factor for recurrent fistula (p < 0.001). Factors associated with recurrence included a history of anal surgery (p < 0.001) and spicy food consumption (p = 0.002). Conclusion: The LIFT technique is effective for the treatment of complex anal fistula, which clinicians should consider combining with VAAFT to reduce recur-rence, since VA-LIFT seems more effective compared with conventional curettage technique. Keywords: Fistula in ano, Ligation of intersphinc-teric fistula tract (LIFT), VAAFT
RANDOMIZED CONTROLLED TRIAL OF GENOTYPE-GUIDED VERSUS CONVENTIONAL WARFARIN INITIAL DOSING IN HEART VALVE REPLACEMENT: AN INTERIM ANALYSIS
Sukrita Samphao1, Voravit Chittithavorn1, Pongsanae Duangpakdee1, Phuripong Rodneum1,Surasak Sangkhathat1, Laorrat Lertlam2
1 Department of Surgery, Faculty of Medicine, Prince of Songkla University, Songkhla 90110, Thailand2 Warfarin Clinic, Department of Pharmacy, Songklanagarind Hospi-tal, Prince of Songkla University, Songkhla 90110, Thailand
Background: Warfarin is an anticoagulant widely used to prevent thromboembolic events in the patients requiring heart value replacement. Using an optimal
warfarin starting dose may reduce the time taken to reach stable INR level. Currently, studies show that there are two genes, VKORC1 and CYP2C9, which are strongly associated with warfarin initial dosing requirement. Objective: To compare the proportion of the pa-tients who can reach two consecutive warfarin therapeu-tic levels by using the same dose of warfarin (defined as the warfarin stable dose) between two groups. Materials and Methods: This is an interim analy-sis of randomized trial conducted at one medical center, which included 30 patients who underwent heart valve replacement and required warfarin anticoagulation. Patients were randomized, using blocks of four, into conventional warfarin initial dosing group and genotype-guided warfarin initial dose group. Clinical follow-up time was 90 days. Results: There were 15 patients in each group. Most of the patients underwent single heart valve replacement. The ratio of tissue valve to metallic valve replacement was 2:1 in both groups. The genotype distribution of CYP2C9 and VKORC1 was well-balanced. The pro-portion of the patients who could reach warfarin stable dose was the same in each group (53%). Time taken to achieved warfarin stable dose was longer on average in the genotype-guided warfarin initial dose group (33 days vs. 13 days, p = 0.09). However, the duration of a stable dose was also longer in the genotype-guided warfarin group (48 days vs. 33 days, p = 0.34). No patient had major hemorrhagic or thrombotic complications. Conclusion: The proportion of patients who could reach warfarin stable dose was not significantly different between groups using conventional vs. genotype-guided warfarin initial dosing. However, this is an interim analy-sis, and the study showed no major adverse events, so the trial should be continued until completion, to include 80 patients overall. Keywords: Pharmacogenetics, CYP2C9, VKORC1, Warfarin, Heart valve replacement
SURFACE ANATOMY FOR SURGERY AROUND TRANSVERSE SINUS RELATION TO LAMB-DOID SUTURE, INION AND SUPERIOR NUCHAL LINE
Panit Satapornteera, MD, Atthaporn Boongird MDDivision of Neurosurgery, Department of Surgery, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Background: Dural venous sinuses in occipital

AbstractsVol. 40 No. 4 145
and suboccipital region are preserved and prevent from injury when creating a craniotomy. Localization these venous sinuses direction usually uses the inion, superior nuchal line, muscle insertion, or other surface landmarks. This study is aimed to interpret the accuracy of the sur-face landmarks in estimating the exact location of the dural venous structures. Materials and Methods: We dissected 51 forma-lin-fixed skulls and studied the superficial landmarks in the occipital and suboccipital areas which were lambdoid sutures, inion, and superior nuchal lines within 4 cm lateral to the inion on both sides. The distance between them and the transverse sinuses and torcular were mea-sured using Venier caliper. Results: Inion located at the torcular herophili in 68.6%, but inferior to the torcular 19.61%. The right superior nuchal line located at the transverse sinus 68.6%, inferior to the sinus 13.7%, and superior to the sinus 17.7%. The left superior nuchal line located at the transverse sinus 66.7%, inferior to the sinus 9.8%, and superior to the sinus 23.5%. Lambdoid sutures located superior to the sinuses 3.5 cm on the right and 3.8 cm on the left. The right transverse sinus was greater than the left sinus significantly. Conclusion: The findings showed that inion and superior nuchal lines were relatively related to the trans-verse sinuses and torcular herophili and can be used to predict their locations in order to prevent injuries. The lambdoid was not a good landmark because its variability related to the sinuses. Keywords: Lambdoid, Inion, Superior nuchal lines, Torcular
THE OUTCOME OF SACUBITRIL/VALSARTAN VERSUS ENALAPRIL FOR EJECTION FRAC-TION IMPROVEMENT IN PATIENTS WITH OP-ERATIVE CORONARY ARTERY BYPASS GRAFT
Warach Taksinachanekij, MD, Kriengchai Prasongsukarn, MDDivision of Cardiothoracic Surgery, Department of Surgery, Phra-mongkutklao Hospital and College of Medicine, Bangkok, 10400, Thailand
Background: From the PARADIGM-HF trial, the combination of sacubitril/valsartan has significant
mortality benefit, reducing the risk for cardiovascular (CV) death and hospitalizations in patients with heart failure and reduced ejection fraction when compare with enalapril. With those underwent coronary artery bypass graft (CABG), there is no study comparing the benefit of those receiving these two drugs. Objective: To study the outcome of ejection frac-tion improvement in patients who underwent CABG and receiving sacubitril/valsartan compare to those with CABG and receiving enalapril. Materials and Methods: Randomized control trial study, from June 2018 to February 2019 at department of surgery, Phramongkutklao hospital, total 28 patients, with low ejection fraction (EF < 40%) were underwent CABG in elective situation. After conducting a sample selection according to the criteria of the study, the sample consisted of 16 patients (8 patients in control group, 8 patients in experimental group). Experimental group received sacubitril/valsartan while control group received enalapril. Echocardiography was performed before operation and 3 months post operatively. Results: Average age of patients is 62.5 years (male 4/ female 4) in control group versus 61.5 years (male 5/ female 3) in experimental group. In control group, EF improvement changed from average 35% to 49% post-operatively while the experimental group EF improvement changed from average 29% to 47% post-operatively. When compare EF post-operative between control group and experimental group is 49% versus 47%, respectively. Conclusions: Patients with left ventricular dys-function, CABG can significantly improve post-oper-atively (Paired t-test: significant different, p-value = 0.0031; 95% CI 0.06-0.22; control group, = 0.0005; 95% CI 0.11-0.24, experimental group). When compare EF post-operative between control group and experimental group is non-significant different (Independent t-test: p-value = 0.752; 95% CI -0.12-0.16). The result from this study can make surgeons have alternative treatment in patients with low EF coronary artery disease. Keywords: Sacubitril/valsartan, Low ejection frac-tion, Coronary artery bypass graft

Abstracts Thai J Surg Oct. - Dec. 2019146
VDO Award
A SAFE TECHNIQUE FOR PNEUMATIC REDUC-TION OF INTUSSUSCEPTION IN CHILDREN
Kwanhathai Sakulsansern1, Kotchakorn Verasmith2, Kesorn Boonkum2, Panthira Odthon2, Sani Molagool3, Nopporn Sritippho4
1 Division of Pediatric Surgery, Department of Surgery, Sawan Pra-charak Hospital, Nakhon Sawan, 60000, Thailand2 Department of Diagnostic and Therapeutic Radiology, Sawan Pra-charak Hospital, Nakhon Sawan, 60000, Thailand3 Division of Pediatric Surgery, Department of Surgery, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand4 Division of Pediatric Surgery, Department of Surgery, Sawan Pra-charak Hospital, Nakhon Sawan, 60000, Thailand
Background: Intussusception is the most common cause of intestinal obstruction in early childhood. Pneu-matic reduction has a higher success rate and few com-plications compared to barium enema and hydrostatic reductions, especially if performed under intravenous (IV) sedation. Objective: The purpose of this video is to de-monstrate our technique of pneumatic reduction under fluoroscopic guidance with IV sedation. Materials and Methods: A sedated child was given air enema under fluoroscopic guidance using locally assembled equipment. The intraluminal pres-sure was monitored with a pressure gauge, which was maintained between 80 to 110 mmHg. Fentanyl and Midazolam were used for IV sedation. Results: The case was reduced successfully. No bowel perforation occurred. There was no complication to associated with IV sedation, which also did not add any difficulty to the pneumatic reduction. The fluoro-scopic time and time needed for reduction was noticeably short. Conclusions: The technique described was easy, safe, fast, effective and the equipment involved easy to assemble. We recommend it for regular use in the pneumatic reduction of intussusception.
NO-SCALPEL VASECTOMY: LEARNING MATE-RIAL FOR MEDICAL STUDENTS
Pokket Sirisreetreerux1, Wit Viseshsindh1, Kittinut Kijvikai1, Wachira Kochakarn1
1 Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi hospital, Bangkok, Thailand
Vasectomy is a method of male contraception. This procedure is considered the irreversible or permanent sterilization procedures because vasectomy reversal procedures has still remained technically demanding, expensive and may not restore the pre-vasectomy condition. No-scalpel vasectomy (also called keyhole vasectomy or NSV) is a modern method of delivery, ligation and excision of vas deferens instead of giving a long incision as in conventional vasectomy. NSV does not need surgical sutures to close the skin. Compared with conventional vasectomy technique, the benefits of no-scalpel vasectomy include a shorter operating time, less pain and swelling, and faster recovery with similar success rates. In the aspect of medical education, vasec-tomy is considered the mandatory procedure (surgical skill level 4) which the medical students have to know how to give the advice regarding the indication, the contraindication, the steps of the operation and the com-plication after the procedure. Unfortunately, nowadays the vasectomy gains less popularity because there are many reversible and effective methods of contraception. As the result, the number of vasectomy patients has been significantly decreased all over the country. Therefore, Division of Urology, Department of Surgery, Faculty of Medicine Ramathibodi Hospital, Mahidol University developed a VDO of NSV which included history and benefit, instruments and supplies, anesthesia, surgical ap-proach and technique, complications and post-operative care. The author believes that this education VDO will be benefit to medical students and the surgeons to make them more confident to perform NSV and could be ad-ditionally used for the patients’ counselling. Keywords: Birth control, No-scalpel vasectomy, Vasectomy technique
ROBOT-ASSISTED LAPAROSCOPIC BOARI FLAP REIMPLANTAION IN BENIGN URETERAL STRICTURE FROM TUBERCULOSIS: A CASE REPORT
Keeree Komvuttikarn 1, Premsant Sangkum1, Suthep
Pacharatakul2, Wisoot Kongchareonsombat1
1 Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand2 Division of Urology, Department of Surgery, Police Hospital, Bangkok, Thailand

AbstractsVol. 40 No. 4 147
Background: A Boari flap reimplantation can be used to bridge defects in the long ureteral strictures. Multiple methods have been described for the creation of Boari flaps. With the benefits of robot-assisted surgery, it aids in visualization and suturing. We adopted the same open technique for the robot-assisted Boari flap reimplantation with the aims of equivalent efficiency. Case presentation: We reported a 35-year-old male patient with long ureteral stricture from tubercu-losis whom had undergone robot-assisted laparoscopic Boari flap reimplantaion. The patient recovered well post-operatively. Conclusion: Robot-assisted Boari flap ureteral reimplantation can be performed with technical preci-sion.
SURGICAL FACTORS IMPROVING CONTI-NENCE IN ROBOTIC ASSISTED LAPARO-SCOPIC RADICAL PROSTATECTOMY, REAL SURGICAL EXPERIENCE IN RAMATHIBODI HOSPITAL, A CASE REPORT
Wattanachai Ratanapornsompong1, Suthep Pachara-takul2, Premsant Sangkum1, Chareon Leenanupan1, Wisoot Kongcharoensombat1
1 Division of Urology, Department of Surgery, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand2 Division of Urology, Department of Surgery, Police Hospital, Bangkok, Thailand
Background: Continence is the second most im-portant outcome after Robotic Assisted Laparoscopic Radical Prostatectomy (RARP). The incontinence after prostatectomy is mostly from intrinsic sphincter deficien-cy. The factors affected continence are age, continence status before surgery, length of remaining urethra and striated sphincter, etc. There are multiple procedures to enhance continent recovery. Objective: To share the real surgical aspect of continent enhancing procedures in Robotic Assisted Laparoscopic Radical Prostatectomy. Patient data: A Thai 71 years old male patient had prostate specific antigen (PSA) 13 ng/ml. Trans-rectal ultrasound guided prostatic biopsy showed prostatic adenocarcinoma gleason 4+4=8 left lobe of prostate gland. Patient was undergone RARP. Procedure: We performed the continent enhancing
procedures. First, we preserved bladder neck by per-formed postero-lateral approach when separate bladder and prostate. Puboprostatic ligament was claimed to be one of continent complexes and we performed pubo-prostatic ligament preservation before control dorsal vein complex. Additional hanging stiches were done using V-lok No.0 to hang up urethra with pubic bone. The bladder neck was preserved. Then, we preserve right carvernous nerve using interfascial technique. Finally, urethra length was preserved as much as possible. Results: The surgical procedure was finished in 110 minutes and estimated blood loss was 240 ml. Patient was doing well after procedure and discharge to home in 3 days. Foley catheter was removed in post-operative day 7 and patient has only mild symptom of stress urinary incontinence. Conclusion: The continent enhancing procedures were technically feasible and help patient to early gain of continence. The technique has to adapt individually and need randomized control trial to statistical prove.
THE ROLE OF MINIMALLY INVASIVE SUR-GERY FOR MANAGEMENT OF SMALL BOWEL OBSTRUCTION
Fon Pakul1, Komol Chaivanijchaya1, Sikarin Sorn-phiphatphong1, Suthikiat Joradol1, Satkunan Mark2, Suthep Udomsawaengsup1
1 Department of Surgery, Faculty of Medicine, King Chulalongkorn memorial hospital, Bangkok, Thailand2 Department of Surgery, Hospital Raja Permaisuri Bainun Ipoh, Malaysia
Background: Small bowel obstruction (SBO) is one of the common surgical emergencies encountered. Up to 60% of patients requires surgical treatment. Ex-plore laparotomy is the standard approach to treat SBO. However, laparoscopic approach is gaining popularity. Objective: To demonstrate the feasibility and safety of laparoscopic approach for the treatment of SBO and outcomes after surgery. Materials and Methods: We report series of 4 cases. The first case was an 87-year-old male presented with abdominal pain. CT scan showed dilatation of je-junum with abrupt change in caliber at proximal ileum. The second case was a 63-year-old female presented with abdominal distension and vomiting. She has a past

Abstracts Thai J Surg Oct. - Dec. 2019148
history total abdominal hysterectomy 10 years ago. CT scan showed dilatation of small bowel with transition point in the terminal ileum. The third case was 26-year-old female presented with abdominal pain and could not pass gas. CT scan showed the intussusception at ileum. The fourth case was 35-year-old presented with severe abdominal cramping. CT scan showed distal small bowel obstruction. The operative steps include safe access to the abdomen, diagnostic laparoscopy, adhesiolysis and inspecting the entire intestine. Results: There was no intra-operative complica-tion such as bowel injury or bleeding. There were no conversions to open surgery in our series. Laparoscopic approach is associated with minimal post-operative pain, shorter hospital stay and lower risk of post-operative morbidity. Conclusion: Laparoscopic approach for SBO is safe, feasible and effective. The careful preoperative evaluation and safe surgical technique play a role to improve the treatment outcomes.
TOTAL LAPAROSCOPIC PANCREATICODUO-DENECTOMY: HOW I DO IT
Pornraksa Ovartchaiyapong1, Pongsatorn Tangtawee1*, Paramin Muangkaew1, Watoo Vassanasiri1
1 Department of surgery, Faculty of Medicine Ramathibodi hospital, Mahidol university, Bangkok 10400, Thailand
This video demonstrates the surgical procedure of total laparoscopic pancreaticoduodenectomy. The video begins with the profile of the patient who has ampulla carcinoma. The procedure is divided into 8 major steps to help understand the whole operation easily. Step-by-step of the procedure are demonstrated. Diagrams with the label of the important landmark anatomy are inserted to facilitate comprehension of the procedure. English narration is provided along the length of video to emphasize the important points and to communicate some messages to the audience. Keywords: Laparoscopic, Pancreaticoduodenec-tomy
Young Investigator Award
ASSESSMENT OF LIVER VOLUME REDUC-TION AFTER PREOPERATIVE ACUTE WEIGHT LOSS FOR BARIATRIC SURGERY AT KING CHULALONGKORN MEMORIAL HOSPITAL: A COMPUTED TOMOGRAPHY-BASED ANALYSIS
Suthikiat Joradol1, Sikarin Sornphiphatphong1, Komol Chaivanijchaya1, Fon Pakul1, Satkunan Mark3,
Natthaporn Tanpowpong2, Nisanard Pisuchpen2, Wipusit Taesombat1, Suthep Udomsawaengsup1
1 Department of Surgery, Faculty of Medicine, King Chu-lalongkorn Memorial hospital, Chulalongkorn University, Bangkok, Thailand2 Department of Radiology, Faculty of Medicine, King Chulalongkorn Memorial hospital, Chulalongkorn University, Bangkok, Thailand3 Department of Surgery, Hospital Raja Permaisuri Bainun Ipoh, Malaysia
Background: Super-obese patients (BMI ≥ 50 kg/m2) have a higher perioperative risk undergoing surgery due to hepatomegaly, massive adiposity, and severe
co-morbidities. Most of the guidelines recommended performing the laparoscopic Roux-en-Y gastric bypass (LRYGB) in this patient group as staged operation to lower the risk by reducing the liver size and volume, as well as improving co-morbidities conditions. Our center used to offer laparoscopic sleeve gastrectomy (LSG) as the staged operation for LRYGB in super-obese patients. The main disadvantage of staged operation is the patients need to undergo the re-operation. To overcome this dis-advantage, we use the 2 weeks preoperative acute weight loss (AWL) follow by LRYGB to facilitate LRYGB as the single operation. Objectives: Our study aimed to evaluate the effi-cacy of preoperative AWL in reducing the liver volume assessed by computed tomography (CT) as well as evaluated the reduction of co-morbidities’ severity. Materials and Methods: All super-obese patients were admitted with a diet of 800 kcal/day for 2 weeks prior to LRYGB. The co-morbidities were monitored and recorded. The liver volume was measured from CT before and after AWL.

AbstractsVol. 40 No. 4 149
Results: Our study recruited 6 patients (2 male and 4 female) with a mean age of 38. The mean BMI reduced from 55.6 kg/m2 (baseline) to 51.8 kg/m2. The mean left lobe liver volume reduced from 718.94 ml. (baseline) to 568.24 ml. (22%), which is statistically significant. The co-morbidities’ parameters also demonstrated the improvement after the AWL. Conclusions: The preoperative AWL is effective method to reduce the liver volume prior to LRYGB in super-obese patients. We demonstrated the effectiveness of volume reduction by using CT as objective assess-ment. Preoperative AWL may potentially play a role to decrease the severity of patients’ co-morbidities in a short period before surgery. Keywords: Bariatric surgery, Morbid obesity, Laparoscopic Roux-en-Y gastric bypass, Acute weight loss, Liver volume
DYNAMIC REANIMATION OF SMILE IN FA-CIAL PARALYSIS: GRACILIS FUNCTIONING FREE MUSCLE FLAP INNERVATED BY MAS-SETERIC NERVE: THE FIRST VIETNAMESE SERIES
Mai-Anh Bui, Trung-Truc VuDepartment of Plastic -Maxillofacial Surgery, Viet-Duc University Hospital, 40 Trang Thi, Hanoi, Vietnam
Background: Facial palsy affects both the func-tional and aesthetic aspects of the face. Many techniques
for both static and dynamic facial reanimation have been described. Here, we present our series of facial reanimation using the functioning free gracilis muscle flap innervated by the masseteric nerve. Materials and Methods: In the period of 2012 and 2018, facial reanimation in patients with facial palsy us-ing the functioning free gracilis muscle flap innervated with the ipsilateral masseteric nerve was performed in 33 patients. The extent of oral commissure movement was determined by the measurements and comparison on both sides of the face from the auricular tragion to the oral commissure, both at rest and with forced smile. Results: All patients followed up for at least 9 months. 31 out of 33 patients (94%) were either satisfied or very satisfied with their outcome. The measurements for oral commissure movement on the side of facial paralysis were found to be similar to that of the normal side in all 18 cases. Very good result for 7/33 patients (21.21%); good result for 18/33 patients (54.54%); Moderate result of 5/33 patients (15.25%), 3/33 patients (9%) fair result. Conclusion: Although it is not the first choice of facial reanimation in the current management of unilate-ral facial paralysis since it doesn’t provide spontaneity, the masseteric nerve is a powerful and reliable facial reanimation donor nerve to innervate the functioning free gracilis muscle flap, which can restore the dynamic smile with minimal donor morbidity. Keywords: Facial paralysis, Facial reanimation, Masseteric nerve, Functioning free gracilis muscle transplantation

Thai J Surg Oct. - Dec. 2019150
An Open Letter from the Editor of the Thai Journal of Surgery
Dear Colleagues and Members of The Royal College of Surgeons of Thailand, and our valued Contributors and Readers,
We are thrilled to inform you of our full transition to the e-Journal format. This means that we will no longer send print versions of the Journal to our Members or Subscribers. However, we will continue to pro-vide Contact Libraries and Contributors with a limited number of print copies of the Journal and individual journal articles (reprints), for archival or academic purposes. We may, in the future, provide print copies of the Journal for those individuals who wish to receive the print copies, but at cost. We think you will agree that the e-Journal format will make access to the Journal much easier and to a broader audience, as well as help reduce unnecessary waste. And the electronic access will be free to all. Our Journal can be accessed via: https://he02.tci-thaijo.org/index.php/ThaiJSurg.
We will begin the transition in the year 2020, starting with volume 41 of the Journal. Therefore, the issue you are holding in your hands is the last print version. We hope you will understand and support our decision in this regard. If you have any queries or comments, please do not hesitate to contact us through the links and email provided below. Thank you for your kind support of the Thai Journal of Surgery over the years, and for your continuing support in the future.
Sincerely,
Panuwat Lertisithichai, MD. Editor-in-Chief of the Thai Journal of Surgery
Secretariat Office: The Thai Journal of Surgery – The Royal of College of Surgeons of ThailandRoyal Golden Jubilee Building, 2 Soi Soonvijai, New Petchburi Road, Huay Kwang, Bangkok 10310, ThailandURL: www.rcst.or.th
AndMs.Pakjira ManeewongJournal Manager of The Thai Journal of SurgeryEmail: [email protected]

151
AA 5-year retrospective review of acute complications and associated
factors of those complications of central vein catheterization in the department of surgery, Siriraj Hospital, 77*
A comparative study of different preservation methods for diced cartilage graft viability: a randomized doubleblind controlled trial, 138*
A comparison between sodium phosphate and polyethylene glycol for bowel preparation for colonoscopy at Vajira Hospital, 77*
A comparison of length of hospital stay between open and laparo-scopic ventral hernia repair, 78*
A little thing that is important in wound care: a periwound, 94*A multicenter comparison between inpatient and outpatient pre-
operative acute weight loss in superobese patients undergoing bariatric surgery, 129*
A randomized controlled study comparing clinical outcomes between non-invasive continuous positive air-way pressure ventilation (NIV-CPAP) and conventional oxygen therapy in severe trau-matic blunt chest injury patients, 138*
A safe technique for pneumatic reduction of intussusception in children, 146*
Accuracy for diagnosis of acute appendicitis by Ripasa score and Alvarado score, 78*
Adequate enoxaparin dosage for venous thromboembolism prophy-laxis in bariatric surgery, 130*
Aneurysmal change in arteriovenous fistulas: retrospective analysis from single institute in Thailand, 79*
Arteriovenous of the head and neck: treatment and outcome, 94*Assessment of liver volume reduction after preoperative acute weight
loss for bariatric surgery at King Chulalongkorn Memorial Hos-pital: a computed tomography-based analysis, 148*
Association between serum beta 2 microglobulin levels and clinico-pathologic molecular subtypes of breast cancer, 139*
BBreast conserving surgery with random rotation flap, 71
CChange of basal metabolic rate in super-obese patients with very
low-calorie diet before bariatric surgery, 126*Chest radiography and clinical outcome of congenital diaphragmatic
hernia in Songklanagarind Hospital, 139*Clinical safety test of polyester containing herbal extract and Ag+
dressing in healthy volunteer, 126*
Comparative study of three fat graft filtration techniques on the volume efficacy and the adipocyte viability: an experimental study, 140*
Comparison of complication in extended latissimus dorsi flap versus latissimus dorsi flap with implant in total breast reconstruction, 132*
Correlation between maximum clot firmness in fibtem and serum fibrinogen in critical trauma patients, 128*
Correlation of transient elastography and progression of cirrhosis in longterm survivors of biliary atresia, 140*
DDoes stepped grafts decrease the hemodynamic change after hemo-
dialysis access creation? The finger-brachial index evaluation: randomized controlled trial, 141*
Durability of RV-PA homograft at pulmonic position in congenital heart procedures at Rajavithi Hospital, 95*
Dynamic reanimation of smile in facial paralysis: gracilis function-ing free muscle flap innervated by masseteric nerve: the first Vietnamese series, 149*
EEarly outcome and feasibility of ambulatory groin herniorrhaphy in
single institute, 79*Effect of puboprostatic ligament preservation during robotic-assisted
laparoscopic radical prostatectomy on early continence: random-ized controlled trial, 142*
Effectiveness of transcatheter arterial embolization for patients with shock from abdominopelvic trauma, 133*
Efficacy of silk sutures compared with non-absorbable polymer clips for cystic duct ligation in laparoscopic cholecystectomy: a prospective randomized controlled study, 80*
Evaluation of initial results of laparosopic inguinal hernia repair in children at Viet Duc University Hospital, 91*
Experience in obturator hernia at Chiangrai Prachanukroh Hospital, 17
FFactor influencing venous leg ulcer healing and recurrence rate after
endovenous radiofrequency ablation of incompetent saphenous vein, 142*
Factors affecting short life expectancy of untreated hepatocellular carcinoma patients after diagnosis, 35
Factors influencing the early and late overall survival after endo-vascular aneurysm repair for ruptured abdominal aortic-iliac
Subjects Index to Volume 40(January to December 2019)
*Abstract (Supplement)

Thai J Surg Oct. - Dec. 2019152
aneurysm, 80*Factors related to the quality of life of ostomates at Viet Duc Hospital
in 2018, 97
GGroin hernia repair under local anesthesia in one day surgery-8-year
experience, 27
HHepaticoduodenostomy as an alternative enterobiliary reconstruction
for hepatectomy in hilar cholangiocarcinoma: Sakon Nakhon Hospital experience, 133*
High expression of prolactin receptor in breast cancer tissue was correlated with lower overall survival, 127*
IIdiopathic granulomatous mastitis: a comparative outcome between
44 patients with different treatment modalities, 134*Iliocaval venous obstruction in Thai patients with advanced chronic
venous insufficiency, 143*Incidence and risk factors associated with intraabdominal hyperten-
sion and primary abdominal compartment syndrome in abdomi-nopelvic injury, 81*
Incidence of treatment failure in esophageal perforation: a retrospec-tive study, 81*
Isolated colonic metastasis from breast cancer: the first case report from Thailand, 134*
LLaparoscopic inguinal hernia repair: the ideal day care laparoscopic
surgery: Hospital Raja Permaisuri Bainun Ipoh, experience, 130*Laparoscopic low anterior resection for obstructing rectal cancer
without bowel preparation, 82*Laparoscopic treatment of cholecystoduodenal fistula: a case report,
22Loco-regional recurrence after nipple-sparing mastectomy in breast
cancer patients, 135*
MMammographic microcalcification and breast cancer: a radio-
pathologic correlation, 82*Management of peritoneal dialysis catheter malfunction: opened or
laparoscopic technique?, 83*Meckel’s diverticulum tip attaches to posterior umbilicus caused
umbilical pain in 11-year-old-boy: a case report, 49Mortality rate and associated factor of necrotizing fasciitis, 83*
NNon-hodgkin lymphoma initially presenting as acute appendicitis:
a case report, 44No-scalpel vasectomy: learning material for medical students, 146*Novel mutation of NR5A1 in a case of 46,XY disorder of sexual
development: a case report, 65NT-2013: a recommended nutrition screening and nutrition format
for practical clinical use in hospitalized patients in Thailand, 107
OOutcome and prognostic factors for periampullary carcinoma after
pancreaticoduodenectomy: a single tertiary center experience, 84*
Outcome of the lift procedure for complex anal fistula at a tertiary
care hospital in southern Thailand, 143*Outcomes and satisfaction of esophageal replacement in children
at Queen Sirikit National Institute of Child Health: a 10-year review, 9
Outcomes comparison between basilic vein transposition and arm straight graft for hemodialysis in end stage renal disease, 84*
Outcomes of sacrococcygeal teratoma: 18-year experience at a tertiary care hospital, 92*
Ovarian tumors in children: an 11-year review, 1
PPenile replantation: the first three successful cases in Vietnam, 95*Portal vein resection in hepatectomy for hilar cholangiocarcinoma:
a case series from Sakon Nakhon Hospital, 135*Predictive factors of chronic kidney disease in kidney donors after
living-donor nephrectomy, 131*Prevalence and clinical application to liver surgery of the portal
vein variation, 85*Prognosis and clinical outcome of papillary carcinoma of the beast
at a tertiary care hospital, 101
RRadiologic patterns associated with surgical necrotizing enterocolitis
and diagnostic indexes among departments, 92*Randomized controlled trial comparing between outpatient bowel
preparation versus bowel preparation in hospital for colonos-copy, 85*
Randomized controlled trial of genotype-guided versus conventional warfarin initial dosing in heart valve replacement: an interim analysis, 144*
Retrospectives study of different management for elderly patients with cancer of stomach and esophagogastric junction, 86*
Risk factors associated with biliary complications after deceased donor liver transplantation, 86*
Risk factors for pleural effusion following pediatrics liver transplan-tations in Ramathibodi Hospital, 93*
Risk factors of duodenal perforation post-endoscopic retrograde cholangiopancreatography, 87*
Risk factors of in-hospital mortality after surgery for acute aortic dissection Stanford type a in Songklanagarind Hospital, 87*
Robot-assisted endonasal endoscopic trans-sphenoidal surgery, 128*Robot-assisted laparoscopic boari flap reimplantation in benign
ureteral stricture from tuberculosis: a case report, 146*
SShort-term outcomes of suture versus ring annuloplasty for functional
tricuspid regurgitation concomitant with mitral value repair in Central Chest Institute of Thailand (CCIT), 136*
Superior epigastric artery: safety zones for pedicle TRAM flap reconstruction: a case series, 53
Surface anatomy for surgery around transverse sinus relation to lambdoid suture, inion and superior nuchal line, 144*
Surgery for disorder of sexual development: a retrospective descrip-tive study, 93*
Surgical factors improving continence in robotic assisted laparoscop-ic radical prostatectomy, real surgical experience in Ramathibodi Hospital, a case report, 147*
Surgical resection versus radiofrequency ablation for small hepato-cellular carcinoma, 88*
T

Vol. 40 No. 4 153
The accuracy of prognostic scoring systems for post-operative morbidity and mortality in patient with perforated peptic ulcer in Buddhachinaraj Phitsanulok Hospital, 88*
The association between somatotype and outcomes in critically Ill surgical patients, 58
The comparison of time barium esophagography to Eckardt’s score for accessing response to perioral endoscopic myotomy in achalasia patient, 89*
The outcome of sacubitril/valsartan versus enalapril for ejection fraction improvement in patients with operative coronary artery bypass graft, 145*
The relationship between intraincisional analgesic infiltration and opioid prescription after open inguinal hernia repair, 89*
The role of minimally invasive surgery for management of small bowel obstruction, 147*
Total laparoscopic pancreaticoduodenectomy: how I do it, 148*
UUreteroscopic laser lithotripsy in the treatment of ureteric stones,
131*
VValidation of cancermath model as prognostic tool for Thai breast
cancer patients, 137*Validation of magee equation in predicting response to neoadjuvant
chemotherapy in hormone receptor positive and HER2 negative breast cancer patients, 137*
Varicose veins: risk factors and patterns of venous reflux in Thai patients, 90*
Venous thromboembolism in trauma patients, the first report from a private tertiary care hospital, 90*
Vertical mastopexy, 117

Thai J Surg Oct. - Dec. 2019154
AAchavanuntakul C, 82*Ajjimarangsi S, 85*Akaraborworn O, 128*Akkarapattanakool P, 141*Anuponganant W, 82*Attawettayanon W, 65
BBiadul N, 134*Boongird A, 144*Boonkum K, 146*Boonpipattanapong K, 87*Boonporm H, 133*, 135*Boonprachern K, 81*Boonprom T, 133*, 135*Boonsanit K, 139*Boonsayompu T, 44Boonsinsukh T, 133*Boonthai A, 93*Boonyasurak S, 138*Branesh PM, 128*Bui MA, 95*, 149*Bunyayothin W, 49
CChainapapong K, 27Chaivanijchaya K, 126*, 129*, 130*, 147*, 148*Chalongwongse S, 128*Changsiriwattanathamrong J, 85*Chantakhow S, 92*Chantip A, 35Chatmongkonwat T, 132*, 134*, 135*Chennavasin P, 89*Chiengkriwate P, 139*, 140*Chinaroonchai K, 126*Chinsakchai K, 80*Chinswangwatanakul V, 77*Chirappapha P, 53, 71, 101, 117, 132*, 134*, 135*Chitmetha K, 132*Chittawatanarat K, 58Chittithavorn V, 87*, 144*Chotsamitkul W, 87*Chtmongkonwat T, 132*Chu MP, 91*Chumnanvej S, 128*Chuysakul N, 138*
DDang THT, 91*Daowan C, 95*Deeprasertvit A, 80*Do TNL, 94*Duangpakdee P, 87*, 144*Dumronggittigule W, 84*Dumrongwongsiri S, 138*
FFoofuengmonkolkit K, 95*Fuengfoo P, 79*
HHahtapornsawan S, 80*Hajidae M, 131*Hlaing K, 131*Hong QQ, 91*Hongjinda S, 79*Hongku K, 80*Horsirimanont S, 141*
IInsiripong S, 44
JJampates C, 136*Janpatompong T, 78*Jansiriyotin P, 35Jaruratanasirikul S, 65Jearanai S, 143*Jieamprasertbun J, 142*Jinawath A, 138*Jirasiritum S, 141*Jirathammaopas J, 85*Jongvilaikasem S, 139*Joradol S, 126*, 129*, 130*, 147*, 148*
KKachornvitaya P, 90*Kanlerd A, 81*Khiewcharoen N, 17Khorana J, 92*Khunakeanan S, 128*Khunpugdee S, 82*Kijvikai K, 146*Kitisin K, 130*
Authors Index to Volume 40(January to December 2019)
*Abstract (Supplement)

Vol. 40 No. 4 155
Kittitirapong N, 141*Kittivarakul E, 87*Kittiwararit W, 133*, 135*Kitudomrat S, 71Kochakarn W, 146*Komvuttikarn K, 146*Kongcharoensombat W, 142*, 146*, 147*Kongsayreepong S, 80*Kosarat S, 92*Kositamongkol P, 84*Kraikhong C, 1Kritayakirana K, 79*, 90*Kritsaneepaiboon S, 140*Kumjornkijbovorn T, 84*Kummalue T, 127*Kunanusont T, 136*
LLaochareonsuk W, 65Laohapensang M, 92*Laohavichitra K, 78*Laorwong S, 1Leela-Udomlipi S, 141*Leenanupan C, 131*, 142*, 147*Leesombatpaiboon M, 53, 101, 135*Lerdsomboon P, 136*Lertlam L, 144*Lertsithichai P, 101, 134*, 135*Limsrichamrern S, 84*Litdang B, 77*Loh KL, 130*Lohitvisate W, 82*Luvira V, 81*
MMahattanobon S, 139*Mahawithitwong P, 84*Malapan K, 129*Manakijsirisuthi W, 22Manasnayakorn S, 83*Maneechay W, 65Manomayangoon C, 83*Mark S, 126*, 129*, 130*, 147*, 148*Maroongroge P, 133*Methasate A, 86*Mokarapong P, 95*Molagool S, 93*, 146*Moungthard H, 82*Muangkaew P, 148*Muangman P, 126*Mutirangura P, 80*
NNa Nan R, 80*Nakornchai K, 81*Nampoolsuksan C, 86*Namviriyachote N, 126*Narongchaikul S, 136*Narueponjirakul N, 90*Navicharern P, 130*Ngerncham M, 92*
Ngin S, 131*Nguyen DC, 97Nguyen DG, 91*Nguyen HH, 94*, 95*Nguyen NT, 97Nguyen Q, 95*Nguyen VH, 91*Nguyen XH, 97Niramis R, 9Nongnuang K, 79*Nonthasoot B, 86*Numhom S, 138*, 140*Numprasit W, 137*
OO-charoenrat E, 137*O-charoenrat P, 127*, 134*, 137*Odthon P, 146*Orrapin S, 84*Ovartchaiyapong P, 148*Owattanapanich N, 126*, 138*
PPacharatakul S, 142*, 146*, 147*Pakul F, 126*, 129*, 130*, 147*, 148*Parakonthun T, 86*Pattom J, 88*Phalanusitthepha C, 77*, 89*Phongkitkarun S, 131*Phosuwan S, 132*, 134*, 135*Phutong N, 139*Pisuchpen N, 148*Polchai N, 137*Pondeenana S, 132*, 134*, 135*Pongratanakul S, 132*, 134*, 135*Poocharoen W, 8Poonyasanthan P, 83*Pootracool P, 141*Porapakkham P, 136*Pornchai S, 53, 117Pornwarakorn C, 141*Prajumsukh K, 84*Prammanasudh B, 107Prapassaro T, 80*Prasert W, 82*Prasongsukarn K, 145*Prichayudh S, 89*Promyarat C, 86*Pruekprasert K, 143*Puangpunngam N, 80*Pungpapong S, 78*, 130*Puthakunraksa D, 49
RRamasamy S, 129*Ratanapornsompong W, 142*, 147*Rattadilok C, 132*Rodneum P, 144*Rodsakan T, 88*Roekwibunsi S, 93*Rojanaratanangoon S, 93*

Thai J Surg Oct. - Dec. 2019156
Ruangsetakit C, 80*
SSaigosoom N, 137*Sakulsansern K, 146*Samarnthai N, 127*Samphao S, 139*, 144*Sangkhathat S, 65, 87, 139*, 140*, 144*Sangkum P, 142*, 146*, 147*Sangthong B, 128*Sanguanlosit S, 88*Sa-nguanraksa D, 127*, 134*, 137*Sanserestid P, 84*Santrakul N, 77*Sarovath A, 140*Satapornteera P, 144*Satitkanmanee E, 81*Sermsathanasawadi N, 80*, 142*, 143*Setthalikhit T, 83*Sidik H, 130*Siewseng T, 79*Simarangsan P, 79*Siribumrungwong B, 84*Sirikun J, 138*Sirisai C, 82*Sirisreetreerux P, 131*, 146*Sirivatanauksorn Y, 84*Siriwanitchaphan W, 90*Sornphiphatphong S, 126*, 129*, 130*, 147*, 148*Srikuea K, 84*Srina P, 93*Sriprayoon W, 90*Srisuwan W, 140*Sritippho N, 146*Sukarayothin T, 53, 101, 135*Sukpanich R, 101Suksamanapan N, 92*Supsamutchai C, 53, 134*Surakarn E, 90*Surakunprapha P, 94*Suthakorn J, 128*Suttiwattana S, 140*Suvikapakornkul R, 101Swangsri J, 86*
TTaesombat W, 88*, 148*Taksinachanekij W, 145*Tangtawee P, 148*Tanmit P, 143*Tanpowpong N, 148*Tantitham T, 140*Tarapongpun T, 134*Teerapradith J, 132*, 134*, 135*Than M, 131*Thanachatchairattana P, 93*Thapananon T, 77*Tharavej C, 130*
Thasripoo C, 127*Thawatchaimangmee P, 78*Thaweepworadej P, 53, 132*, 134*, 135*Thiengthiantham R, 77*Thienhiran A, 79*Thirapattaraphan C, 93*Thongkan T, 85*Thongkhao K, 128*Thongpisitsombut B, 89*Thway M, 131*Tirapanich W, 141*Titapun A, 94*Tongsai S, 77*, 142*Tongsin A, 1Tongsiri N, 133*, 135*Tovikkai C, 84*Trakulhoon V, 107Tran TS, 94*Truong VD, 97
UUdompunthurak S, 137*Udomsawaengsup S, 126*, 129*, 130*, 147*, 148*Uthaipaisanwong A, 90*Uthedphonrattanagul P, 92*
VVassanasiri W, 53, 148*Veerakarnjana W, 126*Verasmith K, 146*Viseshsindh W, 146*Visrutaratna P, 92*Vo TC, 91*Vongwattanakit P, 83*Vu TT, 95*, 149*Vu HT, 91*Vuthivanich C, 80*
WWanitsuwan W, 143*Wasuthit Y, 101Wathanawanichchakun S, 136*Wattanakul T, 132*Weerachareonkul D, 89*Wetwittayakhlang P, 140*Wiboonkwan N, 85*Win L, 131*Witoopinyoparb K, 44Wongkiethachorn N, 94*Wongkiethachorn S, 94*Wongkietkachorn A, 94*Wongwaisayawan S, 101Wongwanit C, 80*
YYan YW, 130*Yingruxpund T, 58Yutthapong K, 9