
HMGB1 Regulates RANKL-Induced Osteoclastogenesis in a Manner Dependent on RAGE
Upload
karolinskaCategory
view
7download
0
INTRODUCTIONThe primary small-vessel systemic
vasculitic disorders associated with anti-neutrophilic cytoplasmatic antibodies(ANCAs) include Wegener granulomato-sis (WG), microscopic polyangiitis(MPA) and Churg-Strauss syndrome(CSS) and are categorized as ANCA- associated vasculitides (1).
Disease severity and prognosis variesprimarily because of the heterogeneity in
organ involvement. The most commonlyaffected vital organs are the kidneys,characterized by a focal necrotizingand/or crescentic pauci-immuneglomerulonephritis in 70% of ANCA- associated vasculitis (AAV) patients, withimportant implications for therapy andlong-term outcome (2).
A number of cell types have been im-plicated in the development of AAV.These include neutrophils, monocytes
and T and B lymphocytes (3). Animalmodels have confirmed a pathogenic rolefor ANCAs specific for myeloperoxidaseand cytokines, such as tumor necrosisfactor (TNF) and interleukin (IL)-6, areimportant in the disease development inAAV (4–6).
HMGB1, a 30-kDa ubiquitous nuclearprotein, is a DNA-binding proteinknown as a transcription and growth fac-tor (7,8). This protein has also been iden-tified as acting as a proinflammatory me-diator when found extracellularly inanimal models and human disease. Thetranslocation from the nucleus to the ex-tracellular milieu transforms HMGB1into an “alarmin,” a danger signal withthe ability to activate the immune sys-
M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | B R U C H F E L D E T A L . | 2 9
High-Mobility Group Box-1 Protein (HMGB1) Is Increased inAntineutrophilic Cytoplasmatic Antibody (ANCA)-AssociatedVasculitis with Renal Manifestations
Annette Bruchfeld,1 Mårten Wendt,1 Johan Bratt,2 Abdul R Qureshi,1 Sangeeta Chavan,3 Kevin J Tracey,3
Karin Palmblad,4 and Iva Gunnarsson2
1Department of Renal Medicine, CLINTEC, Karolinska Institute, Stockholm, Sweden; 2Unit of Rheumatology, Department ofMedicine, Karolinska University Hospital, Karolinska Institute, Stockholm, Sweden; 3Laboratory of Biomedical Sciences, FeinsteinInstitute for Medical Research, North Shore-LIJ Health System, Manhasset, New York, United States of America; and 4Women’s andChildren’s Health, Astrid Lindgren Children’s Hospital, Karolinska University Hospital, Karolinska Institute, Stockholm, Sweden
High-mobility group box 1 (HMGB1) is a nuclear and cytosolic protein that is increasingly recognized as an important proinflam-matory mediator actively secreted from monocytes and macrophages and passively released from necrotic cells. In antineutrophiliccytoplasmatic antibody (ANCA)-associated vasculitis (AAV), the kidneys are commonly affected vital organs, characterized by focalnecrotizing and/or crescentic pauci-immune glomerulonephritis. The aim of the study was to determine whether HMGB1 serum lev-els are elevated in AAV with renal manifestations. A total of 30 AAV patients (16 female and 14 male; median age 59 years, range17–82) with Wegener granulomatosis, microscopic polyangiitis and Churg-Strauss syndrome with available renal biopsies and serumsamples were included. In seven cases, serum was also obtained at rebiopsy in remission. HMGB1 was analyzed with Western blot.Birmingham Vasculitis Activity Score (BVAS, version 2003), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), urinanaly-sis, creatinine, estimated glomerular filtration rate, sex and age were included in the analysis. Twenty-five episodes of biopsy-provenactive disease with BVAS 17.9 ± 4.6 and 13 cases with inactive biopsies and BVAS 2.3 ± 3.7 (P = 0.0001) were identified. CRP, ESR, hema-turia and proteinuria were significantly higher in active cases. HMGB1 was significantly elevated (P = 0.01) comparing active with in-active cases (120 ± 48 versus 78 ± 46 ng/mL) and significantly lower in the seven control patients (P = 0.03) at rebiopsy in remission.HMGB1 remained higher in inactive cases compared with historic healthy controls (10.9 ± 10.5 ng/mL). HMGB1 levels did not differsignificantly between AAV subgroups. CRP and ESR did not correlate with HMGB1. HMGB1 is significantly increased in AAV with renalinvolvement. Residual HMGB1 elevation in remission could possibly reflect low-grade inflammatory activity or tissue damage. Futurestudies may further reveal whether HMGB1 is useful as a marker of disease activity and a predictor of outcome in AAV.© 2011 The Feinstein Institute for Medical Research, www.feinsteininstitute.orgOnline address: http://www.molmed.orgdoi: 10.2119/molmed.2010.00132
Address correspondence and reprint requests to Annette Bruchfeld, K 56, Karolinska Uni-
versity Hospital at Huddinge, S-141 86 Stockholm, Sweden. Phone: +46-8-58582685; Fax:
+46-8-7114742; E-mail: [email protected].
Submitted July 31, 2010; accepted for publication September 10, 2010; Epub
(www.molmed.org) ahead of print September 10, 2010.

tem. HMGB1 is actively secreted by in-nate immune cells such as macrophagesand monocytes upon endotoxin stimula-tion, is passively released by injured andnecrotic cells, and has been shown tostimulate necrosis- induced inflammation(9–12). Moreover, HMGB1 induces othercytokines such as TNF, IL-1, IL-6 andIL-8 and is also an activator of endothe-lial cells (human umbilical vein endothe-lial cells) leading to the upregulation ofadhesion molecules (13,14). HMGB1 hasbeen shown to interact with toll-like re-ceptor (TLR)-2, TLR-4 and the receptorfor advanced glycation end products(RAGE) in established cell lines and ani-mal models, leading to a downstreamtranslocation of nuclear factor (NF)-κB,inducing immunostimulatory andchemotactic responses (15–17). In animalmodels of arthritis, a strict nuclearHMGB-1 pattern was observed in syn-ovial cells of healthy mice and rats. Incontrast, a distinct pattern of extracellu-lar expression in the cytoplasm ofmacrophages and synoviocytes has beenidentified with immunohistochemicalstaining in animals with arthritis (18,19).Targeting HMGB1 has been demon-strated to confer protection in animalmodels of sepsis, endotoxemia andarthritis (10,20,21). Elevated HMGB1 lev-els in serum have been documented inclinical inflammatory conditions such assepsis and rheumatoid arthritis (RA) aswell as chronic kidney disease (22–25).
The aim of the study was to investi-gate the role of HMGB1 in AAV withrenal involvement and to determinewhether the serum levels may corre-spond to clinical and histopathologicaldisease activity.
MATERIALS AND METHODS
PatientsA total of 30 patients, 16 female and 14
male with a median age of 59 years(range 17–82), with a diagnosis of AAVwere included in the study. They were allinvestigated and treated at the Unit ofRheumatology at Karolinska UniversityHospital between 1998 and 2008. A sum-
mary of patient characteristics includingage, sex, diagnosis, organ involvement,disease activity score, renal biopsy result,renal function and ANCA antibody isshown in Table 1.
Induction therapy for active vasculitisin patients was typically standard induc-tion treatment with corticosteroids andcyclophosphamide either intravenouslyor orally, followed by remission therapywith low-dose corticosteroids and eitherazathioprin or methotrexate. Plasma ex-change was used in one case on renal re-lapse with dialysis dependence 8 yearsafter primary disease (case 4b, see Table 1).During the induction therapy phase(3–6 months), the patients were followedon average six times until remission wasestablished. After that, follow-up wouldbe approximately every third month un-less clinically required.
MethodsAll patients were included in the study
at the time of renal biopsy with simulta-neous collection of serum samples andevaluation of disease activity. Serum wasfrozen within 4 h and stored at –70°C forfuture analysis. In seven of the cases,biopsies were performed during the ac-tive phase of the disease followed by re-peat biopsies in remission 6–9 monthslater. Paired serum samples were avail-able at these two time points. In four pa-tients, biopsy was performed in inactiverenal disease with no samples availableduring active disease. These patients hadhad induction treatment as describedabove, and the remaining two (cases 13and 32) were biopsied and sampled dur-ing workup for suspected AAV withrenal involvement.
HMGB1 was analyzed by Western blotin the sera of patients by a method previ-ously described (24,25). Birmingham Vas-culitis Activity Score (BVAS, version2003) (a clinical evaluation tool standard-ized for the management of patients withsystemic vasculitis where complete re-mission is defined as BVAS = 0), CRP,ESR, urinalysis (dip stick procedure),24-h albumin excretion in urine, creati-nine, estimated glomerular filtration rate
(eGFR) using the modification of diet inrenal disease (MDRD) formula (26), sexand age were included in the analysis.Biochemical analyses and ANCA serol-ogy by enzyme-linked immunosorbentassay (ELISA) were carried out usingroutine methods at the Department ofClinical Chemistry and Department ofClinical Immunology at Karolinska Uni-versity Hospital.
Active kidney disease was defined asongoing focal necrotizing and/or cres-centic pauci-immune glomerulonephritis,whereas renal remission was labeled asthe absence of these lesions. All renalbiopsies were processed for light mi-croscopy, immunofluorescence, and insome cases, electron microscopy accord-ing to standard techniques.
The study protocol was approved bythe local ethics committee, and informedconsent was obtained from each subject.
ImmunhistochemistryImmunohistochemical stainings were
performed on cryosectioned 4-μm formaldehyde-fixed sections of renalbiopsies. For detection of HMGB1 ex-pression, sections were stained accord-ing to protocols previously described(27). Briefly, to reduce background stain-ing due to unspecific binding, sectionswere incubated with 2% normal goatsera for 30 min. Thereafter, the slideswere incubated overnight with an affinity-purified monoclonal mouseIgG2b anti-HMGB1 antibody (concentra-tion 2 μg/mL, 2G7, received as a hy-bridoma from Critical Therapeutics, Lex-ington, KY, USA). Cells were thereafterincubated with Alexa Fluor© 488 conju-gated goat antimouse IgG2b antibody(Molecular Probes, Invitrogen, Eugene,OR, USA) for 30 min, and nuclei werecounterstained with Hoechst 33342.Phosphate-buffered saline supplementedwith 0.1% saponin was used in all subse-quent washes and incubation steps topermeabilize the cells. In each assay,controls for staining specificity were included, based on parallel stainingstudies omitting the primary antibodyand using a primary isotype-matched
3 0 | B R U C H F E L D E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1
H M G B 1 I N A N C A - A S S O C I A T E D R E N A L V A S C U L I T I S
R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | B R U C H F E L D E T A L . | 3 1
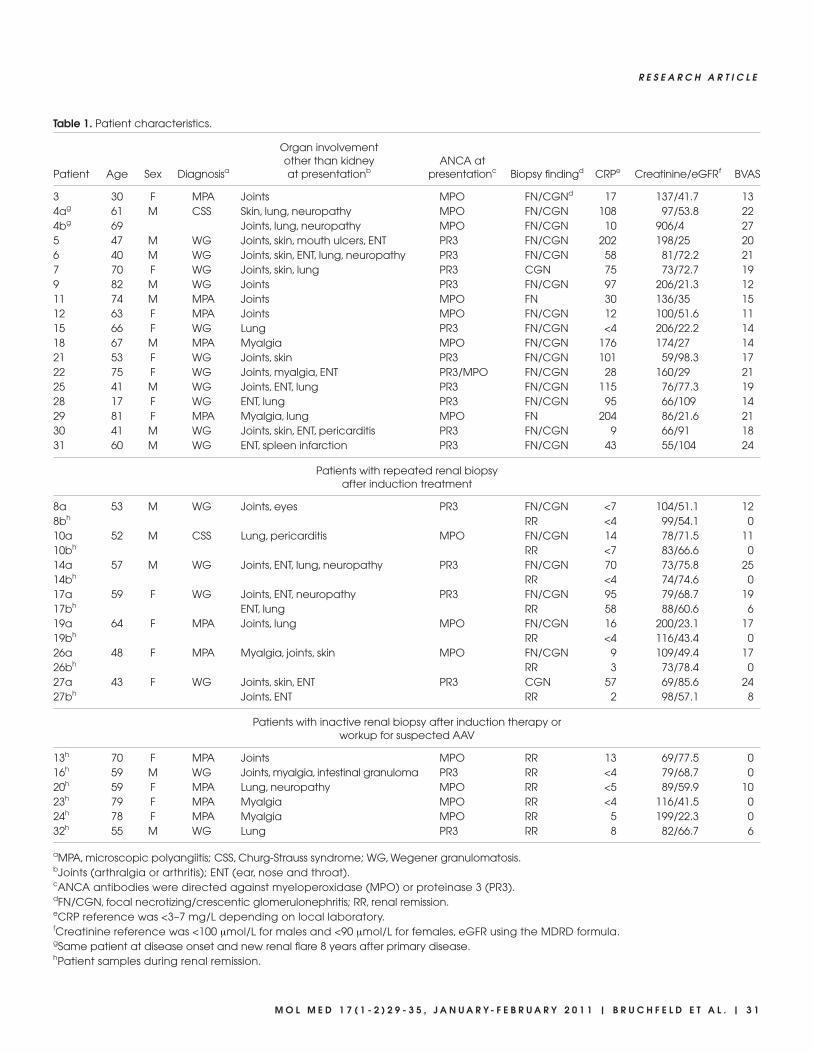
Table 1. Patient characteristics.
Organ involvement other than kidney ANCA at
Patient Age Sex Diagnosisa at presentationb presentationc Biopsy findingd CRPe Creatinine/eGFRf BVAS
3 30 F MPA Joints MPO FN/CGNd 17 137/41.7 134ag 61 M CSS Skin, lung, neuropathy MPO FN/CGN 108 97/53.8 224bg 69 Joints, lung, neuropathy MPO FN/CGN 10 906/4 275 47 M WG Joints, skin, mouth ulcers, ENT PR3 FN/CGN 202 198/25 206 40 M WG Joints, skin, ENT, lung, neuropathy PR3 FN/CGN 58 81/72.2 217 70 F WG Joints, skin, lung PR3 CGN 75 73/72.7 199 82 M WG Joints PR3 FN/CGN 97 206/21.3 1211 74 M MPA Joints MPO FN 30 136/35 1512 63 F MPA Joints MPO FN/CGN 12 100/51.6 1115 66 F WG Lung PR3 FN/CGN <4 206/22.2 1418 67 M MPA Myalgia MPO FN/CGN 176 174/27 1421 53 F WG Joints, skin PR3 FN/CGN 101 59/98.3 1722 75 F WG Joints, myalgia, ENT PR3/MPO FN/CGN 28 160/29 2125 41 M WG Joints, ENT, lung PR3 FN/CGN 115 76/77.3 1928 17 F WG ENT, lung PR3 FN/CGN 95 66/109 1429 81 F MPA Myalgia, lung MPO FN 204 86/21.6 2130 41 M WG Joints, skin, ENT, pericarditis PR3 FN/CGN 9 66/91 1831 60 M WG ENT, spleen infarction PR3 FN/CGN 43 55/104 24
Patients with repeated renal biopsyafter induction treatment
8a 53 M WG Joints, eyes PR3 FN/CGN <7 104/51.1 128bh RR <4 99/54.1 010a 52 M CSS Lung, pericarditis MPO FN/CGN 14 78/71.5 1110bh RR <7 83/66.6 014a 57 M WG Joints, ENT, lung, neuropathy PR3 FN/CGN 70 73/75.8 2514bh RR <4 74/74.6 017a 59 F WG Joints, ENT, neuropathy PR3 FN/CGN 95 79/68.7 1917bh ENT, lung RR 58 88/60.6 619a 64 F MPA Joints, lung MPO FN/CGN 16 200/23.1 1719bh RR <4 116/43.4 026a 48 F MPA Myalgia, joints, skin MPO FN/CGN 9 109/49.4 1726bh RR 3 73/78.4 027a 43 F WG Joints, skin, ENT PR3 CGN 57 69/85.6 2427bh Joints, ENT RR 2 98/57.1 8
Patients with inactive renal biopsy after induction therapy or workup for suspected AAV
13h 70 F MPA Joints MPO RR 13 69/77.5 016h 59 M WG Joints, myalgia, intestinal granuloma PR3 RR <4 79/68.7 020h 59 F MPA Lung, neuropathy MPO RR <5 89/59.9 1023h 79 F MPA Myalgia MPO RR <4 116/41.5 024h 78 F MPA Myalgia MPO RR 5 199/22.3 032h 55 M WG Lung PR3 RR 8 82/66.7 6
aMPA, microscopic polyangiitis; CSS, Churg-Strauss syndrome; WG, Wegener granulomatosis.bJoints (arthralgia or arthritis); ENT (ear, nose and throat).cANCA antibodies were directed against myeloperoxidase (MPO) or proteinase 3 (PR3). dFN/CGN, focal necrotizing/crescentic glomerulonephritis; RR, renal remission.eCRP reference was <3–7 mg/L depending on local laboratory. fCreatinine reference was <100 μmol/L for males and <90 μmol/L for females, eGFR using the MDRD formula.gSame patient at disease onset and new renal flare 8 years after primary disease.hPatient samples during renal remission.
immunoglobulin of irrelevant antigenspecificity (negative mouse IgG2b con-trol, DAKO Cytomation, Glostrup, Denmark).
StatisticsContinuous variables are presented as
the median (10th to 90th percentile).Group differences were determined bynonparametric Wilcoxon two-samplerank sum test and χ2 test for nominalvariables, and univariate correlations be-tween variables were assessed usingSpearman rank correlation (ρ). Statisticalsignificance was set at the level of P <0.05. A multivariate general linear modelwas used to assess the relationship be-tween HMGB1 and various subgroups ofvasculitis adjusting for eGFR (MDRDformula). Statistical computations werecarried out using SAS 9.2 (SAS CampusDrive, Cary, NC, USA).
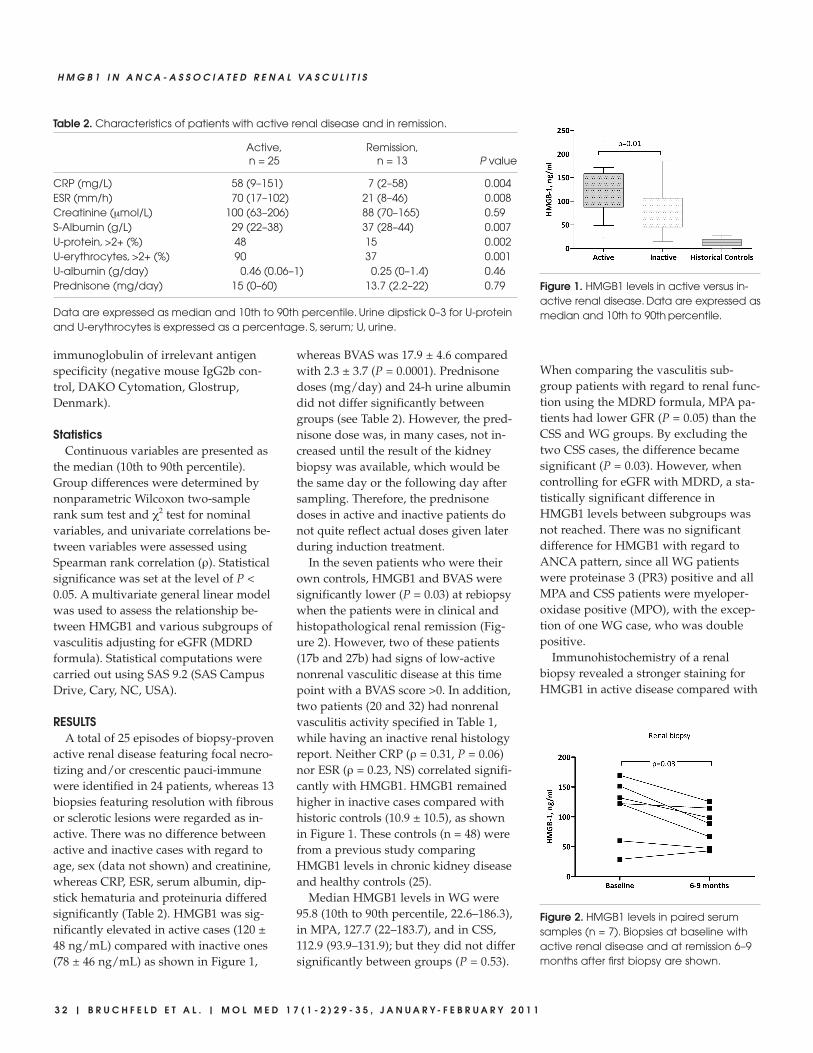
RESULTSA total of 25 episodes of biopsy-proven
active renal disease featuring focal necro-tizing and/or crescentic pauci-immunewere identified in 24 patients, whereas 13biopsies featuring resolution with fibrousor sclerotic lesions were regarded as in-active. There was no difference betweenactive and inactive cases with regard toage, sex (data not shown) and creatinine,whereas CRP, ESR, serum albumin, dip-stick hematuria and proteinuria differedsignificantly (Table 2). HMGB1 was sig-nificantly elevated in active cases (120 ±48 ng/mL) compared with inactive ones(78 ± 46 ng/mL) as shown in Figure 1,
whereas BVAS was 17.9 ± 4.6 comparedwith 2.3 ± 3.7 (P = 0.0001). Prednisonedoses (mg/day) and 24-h urine albumindid not differ significantly betweengroups (see Table 2). However, the pred-nisone dose was, in many cases, not in-creased until the result of the kidneybiopsy was available, which would bethe same day or the following day aftersampling. Therefore, the prednisonedoses in active and inactive patients donot quite reflect actual doses given laterduring induction treatment.
In the seven patients who were theirown controls, HMGB1 and BVAS weresignificantly lower (P = 0.03) at rebiopsywhen the patients were in clinical andhistopathological renal remission (Fig-ure 2). However, two of these patients(17b and 27b) had signs of low-activenonrenal vasculitic disease at this timepoint with a BVAS score >0. In addition,two patients (20 and 32) had nonrenalvasculitis activity specified in Table 1,while having an inactive renal histologyreport. Neither CRP (ρ = 0.31, P = 0.06)nor ESR (ρ = 0.23, NS) correlated signifi-cantly with HMGB1. HMGB1 remainedhigher in inactive cases compared withhistoric controls (10.9 ± 10.5), as shownin Figure 1. These controls (n = 48) werefrom a previous study comparingHMGB1 levels in chronic kidney diseaseand healthy controls (25).
Median HMGB1 levels in WG were95.8 (10th to 90th percentile, 22.6–186.3),in MPA, 127.7 (22–183.7), and in CSS,112.9 (93.9–131.9); but they did not differsignificantly between groups (P = 0.53).
When comparing the vasculitis sub-group patients with regard to renal func-tion using the MDRD formula, MPA pa-tients had lower GFR (P = 0.05) than theCSS and WG groups. By excluding thetwo CSS cases, the difference becamesignificant (P = 0.03). However, whencontrolling for eGFR with MDRD, a sta-tistically significant difference inHMGB1 levels between subgroups wasnot reached. There was no significantdifference for HMGB1 with regard toANCA pattern, since all WG patientswere proteinase 3 (PR3) positive and allMPA and CSS patients were myeloper-oxidase positive (MPO), with the excep-tion of one WG case, who was doublepositive.
Immunohistochemistry of a renalbiopsy revealed a stronger staining forHMGB1 in active disease compared with
3 2 | B R U C H F E L D E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1
H M G B 1 I N A N C A - A S S O C I A T E D R E N A L V A S C U L I T I S
Figure 2. HMGB1 levels in paired serumsamples (n = 7). Biopsies at baseline withactive renal disease and at remission 6–9months after first biopsy are shown.
Figure 1. HMGB1 levels in active versus in-active renal disease. Data are expressed asmedian and 10th to 90th percentile.
Table 2. Characteristics of patients with active renal disease and in remission.
Active, Remission,n = 25 n = 13 P value
CRP (mg/L) 58 (9–151) 7 (2–58) 0.004ESR (mm/h) 70 (17–102) 21 (8–46) 0.008Creatinine (μmol/L) 100 (63–206) 88 (70–165) 0.59S-Albumin (g/L) 29 (22–38) 37 (28–44) 0.007U-protein, >2+ (%) 48 15 0.002U-erythrocytes, >2+ (%) 90 37 0.001U-albumin (g/day) 0.46 (0.06–1) 0.25 (0–1.4) 0.46Prednisone (mg/day) 15 (0–60) 13.7 (2.2–22) 0.79
Data are expressed as median and 10th to 90th percentile. Urine dipstick 0–3 for U-proteinand U-erythrocytes is expressed as a percentage. S, serum; U, urine.
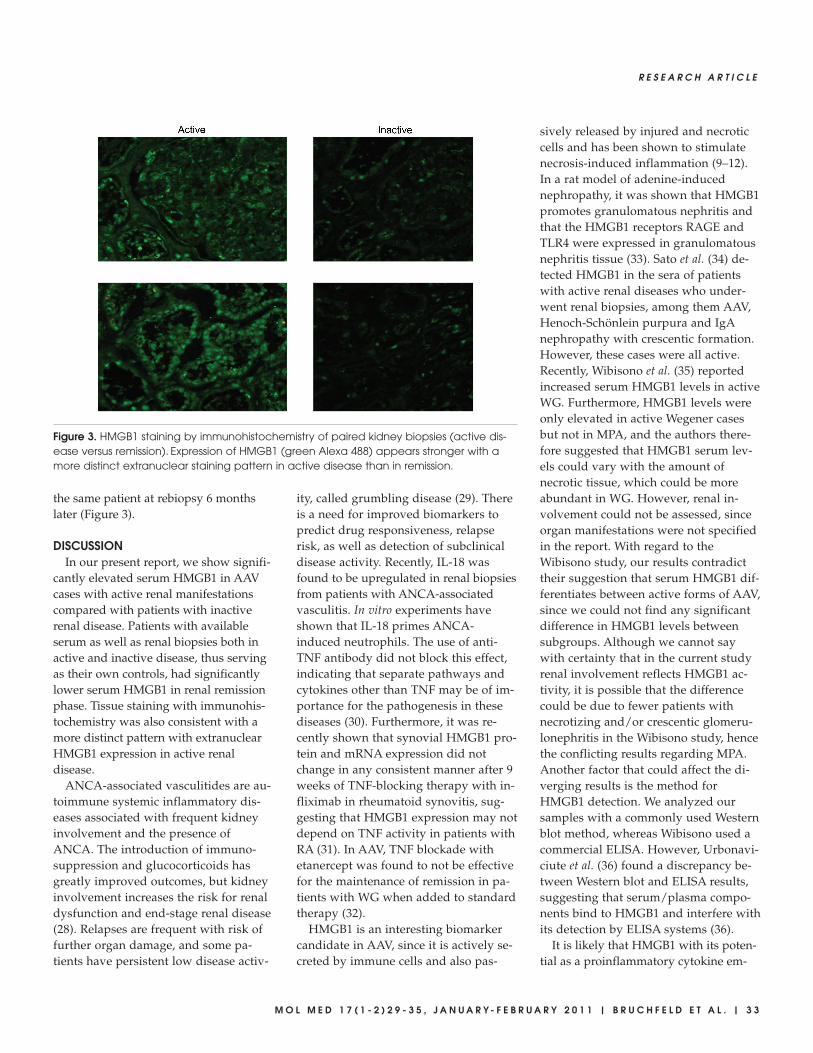
the same patient at rebiopsy 6 monthslater (Figure 3).
DISCUSSIONIn our present report, we show signifi-
cantly elevated serum HMGB1 in AAVcases with active renal manifestationscompared with patients with inactiverenal disease. Patients with availableserum as well as renal biopsies both inactive and inactive disease, thus servingas their own controls, had significantlylower serum HMGB1 in renal remissionphase. Tissue staining with immunohis-tochemistry was also consistent with amore distinct pattern with extranuclearHMGB1 expression in active renal disease.
ANCA-associated vasculitides are au-toimmune systemic inflammatory dis-eases associated with frequent kidneyinvolvement and the presence ofANCA. The introduction of immuno-suppression and glucocorticoids hasgreatly improved outcomes, but kidneyinvolvement increases the risk for renaldysfunction and end-stage renal disease(28). Relapses are frequent with risk offurther organ damage, and some pa-tients have persistent low disease activ-
ity, called grumbling disease (29). Thereis a need for improved biomarkers topredict drug responsiveness, relapserisk, as well as detection of subclinicaldisease activity. Recently, IL-18 wasfound to be upregulated in renal biopsiesfrom patients with ANCA-associatedvasculitis. In vitro experiments haveshown that IL-18 primes ANCA- induced neutrophils. The use of anti-TNF antibody did not block this effect,indicating that separate pathways andcytokines other than TNF may be of im-portance for the pathogenesis in thesediseases (30). Furthermore, it was re-cently shown that synovial HMGB1 pro-tein and mRNA expression did notchange in any consistent manner after 9weeks of TNF-blocking therapy with in-fliximab in rheumatoid synovitis, sug-gesting that HMGB1 expression may notdepend on TNF activity in patients withRA (31). In AAV, TNF blockade withetanercept was found to not be effectivefor the maintenance of remission in pa-tients with WG when added to standardtherapy (32).
HMGB1 is an interesting biomarkercandidate in AAV, since it is actively se-creted by immune cells and also pas-
sively released by injured and necroticcells and has been shown to stimulatenecrosis-induced inflammation (9–12).In a rat model of adenine-inducednephropathy, it was shown that HMGB1promotes granulomatous nephritis andthat the HMGB1 receptors RAGE andTLR4 were expressed in granulomatousnephritis tissue (33). Sato et al. (34) de-tected HMGB1 in the sera of patientswith active renal diseases who under-went renal biopsies, among them AAV,Henoch-Schönlein purpura and IgAnephropathy with crescentic formation.However, these cases were all active.Recently, Wibisono et al. (35) reportedincreased serum HMGB1 levels in activeWG. Furthermore, HMGB1 levels wereonly elevated in active Wegener casesbut not in MPA, and the authors there-fore suggested that HMGB1 serum lev-els could vary with the amount ofnecrotic tissue, which could be moreabundant in WG. However, renal in-volvement could not be assessed, sinceorgan manifestations were not specifiedin the report. With regard to theWibisono study, our results contradicttheir suggestion that serum HMGB1 dif-ferentiates between active forms of AAV,since we could not find any significantdifference in HMGB1 levels betweensubgroups. Although we cannot saywith certainty that in the current studyrenal involvement reflects HMGB1 ac-tivity, it is possible that the differencecould be due to fewer patients withnecrotizing and/or crescentic glomeru-lonephritis in the Wibisono study, hencethe conflicting results regarding MPA.Another factor that could affect the di-verging results is the method forHMGB1 detection. We analyzed oursamples with a commonly used Westernblot method, whereas Wibisono used acommercial ELISA. However, Urbonavi-ciute et al. (36) found a discrepancy be-tween Western blot and ELISA results,suggesting that serum/plasma compo-nents bind to HMGB1 and interfere withits detection by ELISA systems (36).
It is likely that HMGB1 with its poten-tial as a proinflammatory cytokine em-
R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | B R U C H F E L D E T A L . | 3 3
Figure 3. HMGB1 staining by immunohistochemistry of paired kidney biopsies (active dis-ease versus remission). Expression of HMGB1 (green Alexa 488) appears stronger with amore distinct extranuclear staining pattern in active disease than in remission.

anates from systemic inflammation inAAV in addition to local necrotizing orgranulomatous processes. Our study, toour knowledge the largest one inHMGB1 and vasculitis with renal mani-festations, includes both active cases andcases without active renal lesions andmay thus add more insight into the roleof HMGB1 regulation during differentdisease stages. However, it would be im-portant to study AAV patients with dif-ferent disease manifestations to clarifythe difference between localized diseaseand systemic disease, as well as the im-portance of kidney disease for HMGB1expression.
The definition of renal involvement inthis report was based on the histologicalreport. Because a kidney biopsy is a snap-shot, it is possible that some minor activ-ity was missed even though the qualityof the biopsy and the expertise of thepathologist was excellent. Persistence oflow-grade hematuria and/or proteinuriacould also correlate to some remainingactivity. However, the four patients witha BVAS >0 and renal remission accordingto the pathology report presented mainlywith other disease manifestations such asjoints; ear, nose and throat; lung; andneuropathy either as grumbling diseaseor new-onset symptoms.
Nevertheless, our results indicate thatpatients with biopsy-proven renal remis-sion, albeit not always in complete dis-ease remission according to BVAS, hadlower circulating HMGB1 levels than pa-tients with active renal vasculitis, sug-gesting a role for HMGB1 in kidney dis-ease associated with AAV.
Interestingly, HMGB1 remained ele-vated in remission when compared withhistorical controls, which may reflect re-maining low-grade inflammatory activityor tissue damage. Considering the lack ofcorrelation with common inflammatorymarkers such as CRP and ESR in the cur-rent study, HMGB1 merits further re-search as a marker for both active diseaseand possible subclinical activity in AAV.
We have previously shown thatHMGB1 correlates with renal function inchronic kidney disease (25). In the cur-
rent study, we could not find such a cor-relation. One possible explanation is thelimited patient number; another explana-tion is that the renal function was signifi-cantly higher and the range smaller com-pared with the previous study, whichincluded patients with a wide range ofglomerular filtration rates. When com-paring the vasculitis subgroups, MPA pa-tients had significantly lower GFR thanWG patients, which is a common findingand has implications for worse outcomein AAV (37). Again, although HMGB1levels did not differ significantly be-tween AAV groups in the current study,HMGB1 seems to be a relevant factorwith regard to renal function and wouldbe worthwhile to follow over time inAAV with renal involvement.
Therapeutic targeting of HMGB1 usingantagonistic, truncated HMGB1 A boxprotein or neutralizing HMGB1-specificantibodies has been demonstrated toconfer protection in animal models ofsepsis, endotoxemia and collagen- induced arthritis (10,20,21). If HMGB1 isproven to be an important inflammatorymediator in vasculitis (in particular, ifanti-HMGB1 antibodies will diminishdisease activity in AAV models), reduc-ing HMGB1 expression may be an inter-esting new drug target in AAV.
In summary, we have demonstrated in-creased serum HMGB1 levels in activeAAV with renal involvement with signifi-cantly lower levels in the remissionphase. However, serum levels of HMGB1in the remission phase still remained ele-vated compared with healthy controls.These findings may reflect a persistentlow-grade inflammatory activity or tissuedamage despite an appearance of clinicaland histopathological renal remission.Further studies may reveal whetherHMGB1 is a predictor of disease activityand outcome in AAV and a possible tar-get for pharmacological modulation.
ACKNOWLEDGMENTSWe thank Westman Research Fund,
Karolinska Institutet Funds, TheSwedish League Against Rheumatism,King Gustav V:S Memorial Fund, the
Swedish Research Council, The SwedishSociety of Medicine and the Fund forRenal Research.
DISCLOSUREThe authors declare that they have no
competing interests as defined by Molec-ular Medicine, or other interests thatmight be perceived to influence the re-sults and discussion reported in thispaper.
REFERENCES1. Jennette JC, et al. (1994) Nomenclature of sys-
temic vasculitides: proposal of an internationalconsensus conference. Arthritis Rheum. 37:187–92.
2. Jayne D. (2009) Progress of treatment in ANCA-associated vasculitis (Review). Nephrology (Carl-ton) 14:42–8.
3. Voswinkel J, Muller A, Lamprecht P. (2005) IsPR3-ANCA formation initiated in Wegener’sgranulomatosis lesions? Granulomas as potentiallymphoid tissue maintaining autoantibody pro-duction. Ann. N. Y. Acad. Sci. 1051:12–9.
4. Xiao H, et al. (2002) Antineutrophil cytoplasmicautoantibodies specific for myeloperoxidasecause glomerulonephritis and vasculitis in mice.J. Clin. Invest. 110:955–63.
5. Little MA, et al. (2005) Antineutrophil cytoplasmantibodies directed against myeloperoxidaseaugment leukocyte-microvascular interactions invivo. Blood 15:2050–8.
6. Hattar K, et al. (2002) Wegener’s granulomatosis:antiproteinase 3 antibodies induce monocyte cy-tokine and prostanoid release-role of autocrinecell activation. J. Leukoc. Biol. 71:996–1004.
7. Bianchi ME, Beltrame M, Paonessa G. (1989) Spe-cific recognition of cruciform DNA by nuclearprotein HMG1. Science 243:1056–9.
8. Bianchi ME, Beltrame M. (2000) Upwardly mo-bile proteins. Workshop: the role of HMG pro-teins in chromatin structure, gene expression andneoplasia. EMBO Rep. 1:109–14.
9. Lotze MT, Tracey KJ. (2005) High-mobility groupbox 1 protein (HMGB1): nuclear weapon in theimmune arsenal. Nat. Rev. Immunol. 5:331–42.
10. Wang H, et al. (1999) HMG-1 as a late mediatorof endotoxin lethality in mice. Science 285:248–51.
11. Wang H, Yang H, Tracey KJ. (2004) Extra cellularrole of HMGB1 in inflammation and sepsis. J. In-tern. Med. 255:320–31.
12. Scaffidi P, Misteli T, Bianchi ME. (2002) Releaseof chromatin protein HMGB1 by necrotic cellstriggers inflammation. Nature 418:191–5.
13. Andersson U, et al. (2000) High mobility group 1protein (HMG-1) stimulates proinflammatory cy-tokine synthesis in human monocytes. J. Exp.Med. 192:565–70.
14. Treutiger CJ, et al. (2003) High mobility group 1B-box mediates activation of human endothe-lium. J. Intern. Med. 254:375–85.
3 4 | B R U C H F E L D E T A L . | M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1
H M G B 1 I N A N C A - A S S O C I A T E D R E N A L V A S C U L I T I S
15. Kokkola R, et al. (2005) RAGE is the major recep-tor for the proinflammatory activity of HMGB1in rodent macrophages. Scand. J. Immunol. 61:1–9.
16. Park JS, et al. (2006) High mobility group box 1protein interacts with multiple Toll-like recep-tors. Am. J. Physiol. Cell Physiol. 290:C917–24.
17. Yu M, et al. (2006) HMGB1 signals through toll-like receptor (TLR) 4 and TLR2. Shock 26:174–9.
18. Kokkola R, et al. (2002) High mobility group boxchromosomal protein 1: a novel proinflammatorymediator in synovitis. Arthritis Rheum. 46:2598–603.
19. Pullerits R, et al. (2003) High mobility group boxchromosomal protein 1, a DNA binding cytokine,induces arthritis. Arthritis Rheum. 48:1693–700.
20. Yang H, et al. (2004) Reversing established sepsiswith antagonists of endogenous high-mobilitygroup box 1. Proc. Natl. Acad. Sci. U. S. A.101:296–301.
21. Kokkola R, et al. (2003) Successful treatment ofcollagen-induced arthritis in mice and rats bytargeting extracellular high mobility group boxchromosomal protein 1 activity. Arthritis Rheum.48:2052–8.
22. Sunden-Cullberg J, et al. (2005) Persistent eleva-tion of high mobility group box-1 protein(HMGB1) in patients with severe sepsis and sep-tic shock. Crit. Care Med. 33:564–73.
23. Hatada T, et al. (2005) Plasma concentrations andimportance of high mobility group box protein inthe prognosis of organ failure in patients withdisseminated intravascular coagulation. Thromb.Haemost. 94:975–9.
24. Goldstein RS, et al. (2007) Cholinergic anti- inflammatory pathway activity and high mobilitygroup box-1 (HMGB1) serum levels in patientswith rheumatoid arthritis. Mol. Med. 13:210–5.
25. Bruchfeld A, et al. (2008) High mobility group boxprotein-1 correlates with renal function in chronickidney disease (CKD). Mol. Med. 14:109–15.
26. Levey AS, Bosch JP, Lewis JB, Greene T, RogersN, Roth D. (1999) A more accurate method to es-timate glomerular filtration rate from serum cre-atinine: a new prediction equation: Modificationof Diet in Renal Disease Study Group. Ann. In-tern. Med. 130:461–70.
27. Ostberg T, et al. (2010) Protective targeting ofHMGB1 in a spontaneous arthritis model. Arthri-tis Rheum. 62:2963–72.
28. Booth AD, et al. (2003) Outcome of ANCA- associated renal vasculitis: a 5-year retrospectivestudy. Am. J. Kidney Dis. 41:776–84.
29. Hogan SL, et al. (2005) Predictors of relapse andtreatment resistance in antineutrophil cytoplas-mic antibody-associated small-vessel vasculitis.Ann. Intern. Med. 143:621–31.
30. Hewins P, et al. (2006) IL-18 is upregulated in thekidney and primes neutrophil responsiveness inANCA-associated vasculitis. Kidney Int. 69:605–15.
31. Sundberg E, et al. (2008) Systemic TNF blockadedoes not modulate synovial expression of thepro-inflammatory mediator HMGB1 in rheuma-toid arthritis patients: a prospective clinicalstudy. Arthritis Res. Ther. 10:R33.
32. Wegener’s Granulomatosis Etanercept Trial(WGET) Research Group. (2005) Etanercept plusstandard therapy for Wegener’s granulomatosis.N. Engl. J. Med. 352:351–61.
33. Oyama Y, et al. (2010) High-mobility group box-1protein promotes granulomatous nephritis inadenine-induced nephropathy. Lab. Invest.90:853–66.
34. Sato F, et al. (2008) High mobility group boxchromosomal protein 1 in patients with renal dis-eases. Nephron. Clin. Pract. 108:c194–201.
35. Wibisono D, et al. (2010) Serum HMGB1 levelsare increased in active Wegener’s granulomatosisand differentiate between active forms of ANCA-associated vasculitis. Ann. Rheum. Dis. 69:1888–9.
36. Urbonaviciute V, Fürnrohr BG, Weber C,Haslbeck M, Wilhelm S, Herrmann M, Voll RE.(2007) Factors masking HMGB1 in human serumand plasma. J. Leukoc. Biol. 81:67–74.
37. Mukhtyar C, et al. (2008) Outcomes from studiesof antineutrophil cytoplasm antibody associatedvasculitis: a systematic review by the EuropeanLeague Against Rheumatism systemic vasculitistask force. Ann. Rheum. Dis. 67:1004–10.
R E S E A R C H A R T I C L E
M O L M E D 1 7 ( 1 - 2 ) 2 9 - 3 5 , J A N U A R Y - F E B R U A R Y 2 0 1 1 | B R U C H F E L D E T A L . | 3 5
Copyright © 2022 FDOKUMEN




















