Groningen Active Living Model (GALM): Stimulating Physical Activity in Sedentary Older Adults
10
Groningen Active Living Model (GALM): stimulating physical activity in sedentary older adults; validation of the behavioral change model Martin Stevens, Ph.D., a, * Koen A.P.M. Lemmink, Ph.D., b Marieke J.G. van Heuvelen, Ph.D., b Johan de Jong, M.Sc., b and Piet Rispens, Ph.D. b a Department of Orthopedics, Groningen University Hospital, Groningen, The Netherlands b Institute of Human Movement Sciences, University of Groningen, Groningen, The Netherlands Abstract Background. A significant proportion of older adults in The Netherlands do not participate regularly in leisure-time physical activity. The Groningen Active Living Model (GALM) was developed to change this situation for the better. Longitudinal results of the validation of the GALM behavioral change model are presented. Methods. We obtained data on potentially mediating variables of physical activity behavior change (self-efficacy, social support, perceived fitness, and enjoyment) from 96 participants in a prospective study during the 18 months the GALM strategy lasted. Results. Prospective analyses revealed significant differences in several potentially mediating variables, although some of these differ- ences were contrary to our hypothesis. Discriminant analysis resulted in canonical correlations of 0.50 after 6 months and 0.66 after 18 months of program participation between adherers and nonadherers, respectively; 73.8 and 80.0% of the subjects were classified correctly. Conclusions. Based on the results, it can be concluded that we partially succeeded in manipulating the potentially mediating variables by means of our GALM strategy. Several mediating variables were identified that reliably discriminated long-term adherers from nonadherers, expanding the generalizability of social cognitive theory-driven variables to a Dutch population. © 2003 American Health Foundation and Elsevier Science (USA). All rights reserved. Keywords: Older adults; Leisure-time physical activity; Behavioral change Introduction As in other Western societies, sedentariness in the Neth- erlands is a potential burden on public health. A sedentary lifestyle is associated with premature death due to coronary heart disease, colon cancer, and non-insulin-dependent dia- betes [1,2]. Regular physical activity has been linked con- sistently and reliably to a reduction in all-cause mortality [3] as well as lower rates of cardiovascular disease and several other debilitating conditions [4 – 6]. In addition to the ben- eficial effects of physical activity on health, regular physical activity also improves older adults’ ability to perform their daily activities, thus enhancing their quality of life [7]. Despite these benefits, a large segment of the Dutch popu- lation of older adults does not participate regularly in lei- sure-time physical activity [8,9]. Sixty-nine percent of the total Dutch adult population are convinced of the impor- tance of sufficient physical activity, but only 40% succeed in being physically active 5 days a week for 30 min at a moderate intensity [10]. Between 40 and 80% of 55- to-65- year-old Dutch adults are physically inactive, depending on the definition and measurement method used [11]. The Groningen Active Living Model (GALM) was de- veloped as a strategy to promote physical activity in seden- tary older adults between the ages of 55 and 65. The GALM stimulation strategy is based on a model of behavioral change (Fig. 1), which was structured with the help of Chen’s program evaluation theory [12], which is compara- ble to the mediation model as proposed by Kraemer et al. This research was made possible by grants from The Netherlands Heart Foundation (Grant 602.314.3), the Praeventiefonds (Grant 27-231), and the Dutch Ministry of Public Health, Welfare and Sports. * Corresponding author. Department of Orthopedics, Groningen Uni- versity Hospital, PO Box 30001, 9700 RB Groningen, The Netherlands. Fax: 31-0-50-3611737 E-mail address: [email protected] (M. Stevens). R Available online at www.sciencedirect.com Preventive Medicine 37 (2003) 561–570 www.elsevier.com/locate/ypmed 0091-7435/$ – see front matter © 2003 American Health Foundation and Elsevier Science (USA). All rights reserved. doi:10.1016/j.ypmed.2003.09.012
Transcript of Groningen Active Living Model (GALM): Stimulating Physical Activity in Sedentary Older Adults
Groningen Active Living Model (GALM): stimulating physical activityin sedentary older adults; validation of the behavioral change model�
Martin Stevens, Ph.D.,a,* Koen A.P.M. Lemmink, Ph.D.,b
Marieke J.G. van Heuvelen, Ph.D.,b Johan de Jong, M.Sc.,b and Piet Rispens, Ph.D.b
a Department of Orthopedics, Groningen University Hospital, Groningen, The Netherlandsb Institute of Human Movement Sciences, University of Groningen, Groningen, The Netherlands
Abstract
Background. A significant proportion of older adults in The Netherlands do not participate regularly in leisure-time physical activity. TheGroningen Active Living Model (GALM) was developed to change this situation for the better. Longitudinal results of the validation of theGALM behavioral change model are presented.
Methods. We obtained data on potentially mediating variables of physical activity behavior change (self-efficacy, social support,perceived fitness, and enjoyment) from 96 participants in a prospective study during the 18 months the GALM strategy lasted.
Results. Prospective analyses revealed significant differences in several potentially mediating variables, although some of these differ-ences were contrary to our hypothesis. Discriminant analysis resulted in canonical correlations of 0.50 after 6 months and 0.66 after 18months of program participation between adherers and nonadherers, respectively; 73.8 and 80.0% of the subjects were classified correctly.
Conclusions. Based on the results, it can be concluded that we partially succeeded in manipulating the potentially mediating variables bymeans of our GALM strategy. Several mediating variables were identified that reliably discriminated long-term adherers from nonadherers,expanding the generalizability of social cognitive theory-driven variables to a Dutch population.© 2003 American Health Foundation and Elsevier Science (USA). All rights reserved.
Keywords: Older adults; Leisure-time physical activity; Behavioral change
Introduction
As in other Western societies, sedentariness in the Neth-erlands is a potential burden on public health. A sedentarylifestyle is associated with premature death due to coronaryheart disease, colon cancer, and non-insulin-dependent dia-betes [1,2]. Regular physical activity has been linked con-sistently and reliably to a reduction in all-cause mortality [3]as well as lower rates of cardiovascular disease and severalother debilitating conditions [4–6]. In addition to the ben-eficial effects of physical activity on health, regular physical
activity also improves older adults’ ability to perform theirdaily activities, thus enhancing their quality of life [7].Despite these benefits, a large segment of the Dutch popu-lation of older adults does not participate regularly in lei-sure-time physical activity [8,9]. Sixty-nine percent of thetotal Dutch adult population are convinced of the impor-tance of sufficient physical activity, but only 40% succeedin being physically active 5 days a week for 30 min at amoderate intensity [10]. Between 40 and 80% of 55- to-65-year-old Dutch adults are physically inactive, depending onthe definition and measurement method used [11].
The Groningen Active Living Model (GALM) was de-veloped as a strategy to promote physical activity in seden-tary older adults between the ages of 55 and 65. The GALMstimulation strategy is based on a model of behavioralchange (Fig. 1), which was structured with the help ofChen’s program evaluation theory [12], which is compara-ble to the mediation model as proposed by Kraemer et al.
�This research was made possible by grants from The NetherlandsHeart Foundation (Grant 602.314.3), the Praeventiefonds (Grant 27-231),and the Dutch Ministry of Public Health, Welfare and Sports.
* Corresponding author. Department of Orthopedics, Groningen Uni-versity Hospital, PO Box 30001, 9700 RB Groningen, The Netherlands.Fax: �31-0-50-3611737
E-mail address: [email protected] (M. Stevens).
R
Available online at www.sciencedirect.com
Preventive Medicine 37 (2003) 561–570 www.elsevier.com/locate/ypmed
0091-7435/$ – see front matter © 2003 American Health Foundation and Elsevier Science (USA). All rights reserved.doi:10.1016/j.ypmed.2003.09.012

[13]. The GALM behavioral change model distinguishesfour domains within a theoretical framework of action andconceptual domains. The four domains are
1. The treatment domain, in which the changes intendedwith the GALM strategy are effected. The treatmentof GALM consists of three phases: recruitment, in-troductory phase, and follow-up. Together they makeup the GALM strategy and last 1.5 years.
2. The implementation environment domain, in whichthe environment in which the strategy is implementedis described.
3. The outcome domain, in which the intended outcomeof the GALM strategy is described.
4. The intervening mechanism domain, which describesthe underlying mediating variables (self-efficacy, so-cial support, perceived fitness, and enjoyment) linkingtreatment (strategy) to outcome.
The purpose of the strategy is to effect change in thepotentially mediating variables of leisure-time physical ac-tivity [7,14]. The GALM strategy and behavioral changemodel have been described in detail elsewhere [15,16]. Thepurpose of our study is to gain insight into the validity of theGALM behavioral change model. A distinction is made
between the validation of the action and the conceptualdomains. A program’s overall accomplishments requiresuccess in both domains. In validating the action domain weinvestigate whether the treatment effectively manipulatesthe potentially mediating variables. In validating the con-ceptual domain we investigate whether changes in the po-tentially mediating variables influence the outcome vari-ables of program adherence and leisure-time physicalactivity. To be able to analyze the longitudinal influence andthe changes in the potentially mediating variables, we exe-cuted a prospective study in which data were gatheredduring 18 months.
Past research has shown that mediating variables influ-encing behavioral change may not be consistent across thevarious stages of behavioral change. In the GALM behav-ioral change model, social cognitive factors (social support,self-efficacy, and perceived fitness) are considered impor-tant initiators of health behavior and positively influence theearly period of maintenance, but may become less importantover time with repeated performance [17]. McAuley [18]argues that, as individuals adapt physiologically and psy-chologically to the demands placed on them by leisure-timephysical activity participation, and as leisure-time physicalactivity becomes part of their daily schedule and possibly
Fig. 1. The Groningen Active Living Model.
562 M. Stevens et al. / Preventive Medicine 37 (2003) 561–570
becomes less demanding, the role of efficacy cognitions isdiminished. This perspective is in keeping with Bandura’scontention [19] that cognitive control systems play theirmost important role in the acquisition of behavioral profi-ciencies. When behaviors are less demanding and moreeasily engaged in, cognitive control systems such as self-efficacy give way to regulation by lower control systems.Enjoyment can be considered one such system. Severalresearchers suggest that feelings of enjoyment and well-being may play an important role in exercise adherence inthe long term [7,20,21]. Research by Csikszentmihaly [22],Csikszentmihalyi and Rathunde [23], Wankel et al. [21],and Bult and Rispens [24] suggests that social support,self-efficacy, and perceived fitness may be key conditionsfor (re)gaining enjoyment in leisure-time physical activity.
As a first step in evaluating our proposed mediationmodel, we hypothesized that the GALM strategy wouldsucceed in enhancing self-efficacy, social support, and per-ceived fitness, which subsequently would result in the abil-ity of formerly sedentary subjects to experience enjoymentin leisure-time physical activity. Self-efficacy, social sup-port, and perceived fitness are considered conditional to thecentral mediating variable, which is the enjoyment of lei-sure-time physical activity. We also hypothesized that, dur-ing the 18 months the GALM strategy lasted, subjectswould shift from the contemplation/preparation phase to theaction/maintenance phase of the stages of change model[15].
As a second step in evaluating the proposed mediation
model, we hypothesized that the increase in self-efficacy,social support, and perceived fitness would lead to an in-crease in enjoyment experienced in leisure-time physicalactivity, and that this increase in enjoyment experienced[15] would subsequently lead to continuing program adher-ence and an enduring physically active lifestyle.
Method
Subjects
Sedentary older adults between the ages of 55 and 65years formed the target population for the GALM strategy.The GALM physical activity program can be characterizedas a moderately intensive leisure-time physical activity pro-gram with an emphasis on recreational sports activities. The18-month program offers a variety of recreational leisure-time physical activities such as volleyball, basketball, aer-obics, gymnastics, and badminton, and can be adjusted tothe wishes of the participants. Sessions are held once a weekand last 1 h.
Potential participants were recruited in five local GALMprojects by means of a special recruitment strategy whichconsisted of a population strategy and a network strategy. Inthe population strategy, older adults in a selected municipalarea received a written invitation and were visited at homeby a member of the local GALM team. As attending byoneself is often a barrier, potential participants were invited
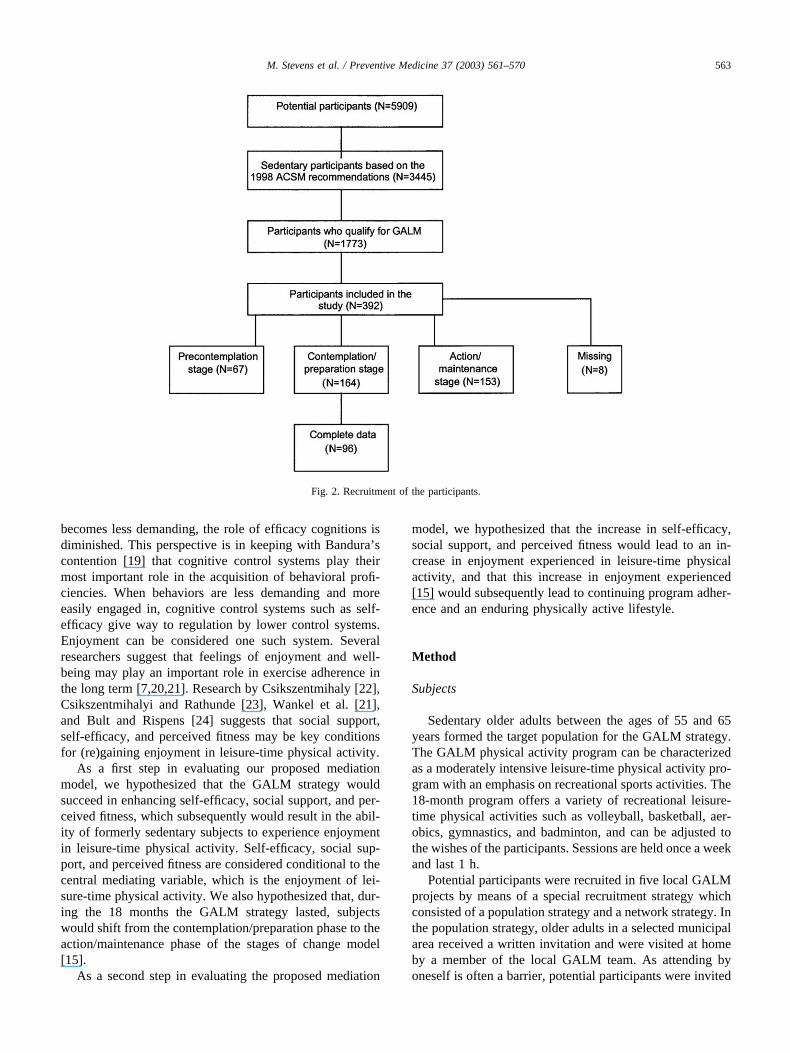
Fig. 2. Recruitment of the participants.
563M. Stevens et al. / Preventive Medicine 37 (2003) 561–570

to bring someone along, even if that person were not sed-entary or did not fit in the age category; this is called thenetwork strategy [15].
Five levels of urbanization can be applied to municipal-ities in The Netherlands. We selected five municipalities torepresent each level of urbanization, in order for the overallsample to be an illustrative cross section of the Dutchpopulation. A total of 5,909 potential participants wererecruited. Based on estimates of available data [15], about60% (N � 3,545) of those who received the invitation couldbe considered sedentary based on the 1998 ACSM recom-mendations on exercise and physical activity for olderadults [25], and, in turn, half (N � 1773) of these qualifiedfor GALM. The other half was not interested in leisure-timephysical activity or was unable to participate due to illness,personal circumstances, or other reasons. By means of thisrecruitment strategy, 392 subjects in five local GALMprojects in The Netherlands were included in the overallstudy (Fig. 2). Each participant had to read and sign awritten informed consent approved by the medical ethicalboard of the Groningen University Hospital.
At the start of the study, 17% (N � 67) of the subjectscould be classified in the precontemplation stage, 42% (N �164) in the contemplation/preparation stage, and 39% (N �153) in the action/maintenance phase. Stages of change datawere missing for 2% (N � 8) of the subjects. In this study,participants in the contemplation/preparation phase wereconsidered relevant to study the dynamics of behavioralchange and were included in the current analyses (Fig. 2).
To be able to validate the dynamic nature of the model,three measurements were planned: a measurement at thestart of the project (T0); a second measurement after com-pleting the introductory program, which ended 6 monthsafter the start of the GALM project (T1); and a final mea-surement after completing the follow-up program, 18months after the start of the GALM project (T2).
Measures
The questionnaire used contained items related to demo-graphic factors (sex, age, and educational level as a reflec-tion of socioeconomic status) and potentially mediatingvariables of leisure-time physical activity participation.
In this study we distinguished three dimensions of self-efficacy: self-efficacy with respect to physical ability, self-efficacy for overcoming barriers, and task self-efficacy, de-fined as participants’ belief that they can continue leisure-time physical activities at a certain frequency and duration,at a specified level of intensity, and over a certain period[26]. We measured these dimensions using three subscales:a Dutch version (LIVAS) [27] of the Perceived PhysicalAbility subscale of the Physical Self-Efficacy scale devel-oped by Ryckman et al. [28] to measure self-efficacy withrespect to physical ability, and a Dutch translation of McAu-ley’s self-efficacy questionnaire containing two subscales tomeasure self-efficacy for overcoming barriers and task self-
efficacy [18]. Cronbach’s �’s for the Dutch versions of thethree scales were 0.80, 0.84, and 0.90 [29]. A Dutch versionof the scales for measuring Social Support for Diet andExercise Behaviors by Sallis et al. [30] was used to measuresocial support for leisure-time physical activity participa-tion. This scale is made up of three subscales: the exercisingtogether subscale from the Friend Support for ExerciseHabits Scale, and the participation and involvement sub-scale and the rewards and punishment subscale, both fromthe Family Support for Exercise Habits Scale. Only the firsttwo subscales were used in this study. Respective �’s for thetwo subscales of the Dutch version were 0.69 and 0.71 [31].For this longitudinal study the Dutch version of the scaleswas extended with social support from group members,since this can be considered important to the process ofbehavioral change. The extended measure was collected atT1 and T2; the Cronbach � for this scale at T1 was 0.83.Lemmink’s perceived fitness questionnaire [32] with aCronbach � of 0.94 was used to measure perceived fitness.The Groningen Enjoyment Questionnaire (GEQ) was usedto measure subjects’ enjoyment in leisure-time physicalactivity. The Cronbach � of this scale was 0.88 [33]. ADutch translation of the stages of change questionnaire byMarcus and Owen [34] was used to obtain informationabout the process of behavioral change during the 18months the GALM program lasted, as well as to obtaininformation about adherence to the program, as one of theoutcome variables.
Statistical analysis
The data were analyzed with SPSS 10.0. When missingvalues frustrated the calculation of sum scores, we workedto replace missing values with the mean score of all otheritems of that scale so that sum scores could be calculated.Missing values were highest for the LIVAS scale (8.3%).The size of Cronbach’s � combined with the total number ofitems of the scale limits the number of items that can bereplaced by this method.
To validate the first part of the proposed mediationmodel, descriptive statistics were used first to determine ifparticipants shifted through the stages of change. Then arepeated measurement analysis of variance was conductedover the three data points with the potentially mediatingvariables as dependent variables, time of measurement asthe within-subject factor, and group (adherence/non-adher-ence) as the between-subject factor. Main effect of time anddifferences between adjacent points of measurement (T0 vsT1, T1 vs T2) give information about the validation of theaction domain. Time � group interaction effects providedinformation on the validity of both parts of the proposedmediation model. Main effects of group and differencesbetween the groups on the three points of measurement giveinformation separately on the validation of the second por-tion of the model. P values lower than 0.05 were consideredto indicate statistical significance. Additionally, discrimi-
564 M. Stevens et al. / Preventive Medicine 37 (2003) 561–570
nant analysis was used to validate the second portion of themodel. By means of this analysis, information was obtainedabout the predictive value of the potentially mediating vari-ables independently of each other. Canonical correlationwas used to measure the degree of association between thediscriminant scores and nonadherers versus adherers.
Results
At T0, 164 participants were identified in the contem-plation/preparation stage. At T1, 125 and at T2, 103 of thoseparticipants returned the questionnaire, response rates of 82and 67%, respectively. Data from all three measurementswere available for 96 subjects. Age of the subjects rangedfrom 49 to 79 years, with a mean of 60. Women made up62.5% and men 37.5% of the sample. With respect toeducation, 42.7% of the subjects had achieved elementaryeducation level, 35.4% had a secondary education level, and21.9% had followed higher education. Subjects werescreened for chronic diseases: 22.3% reported no chronicdisease, 45.7% had one or two chronic diseases, and 32.0%had three or more. At T1 and T2, no significant differenceswere found for sex, age, education, and chronic diseases be-tween subjects who appeared to be adherers and nonadherers.
All subjects were categorized according to their score onthe stages of change questionnaire [34] during the threemeasurements. Table 1 lists the number of subjects in eachstage of change for the three points of measurement. Addi-tionally the data on the stages of change questionnaire wereused to categorize subjects as either adherers or nonadherersafter the 18-month GALM program. Subjects still in theprecontemplation, contemplation, and preparation phasesafter 18 months were considered nonadherers. Subjects inthe action or maintenance phases were considered adherers.
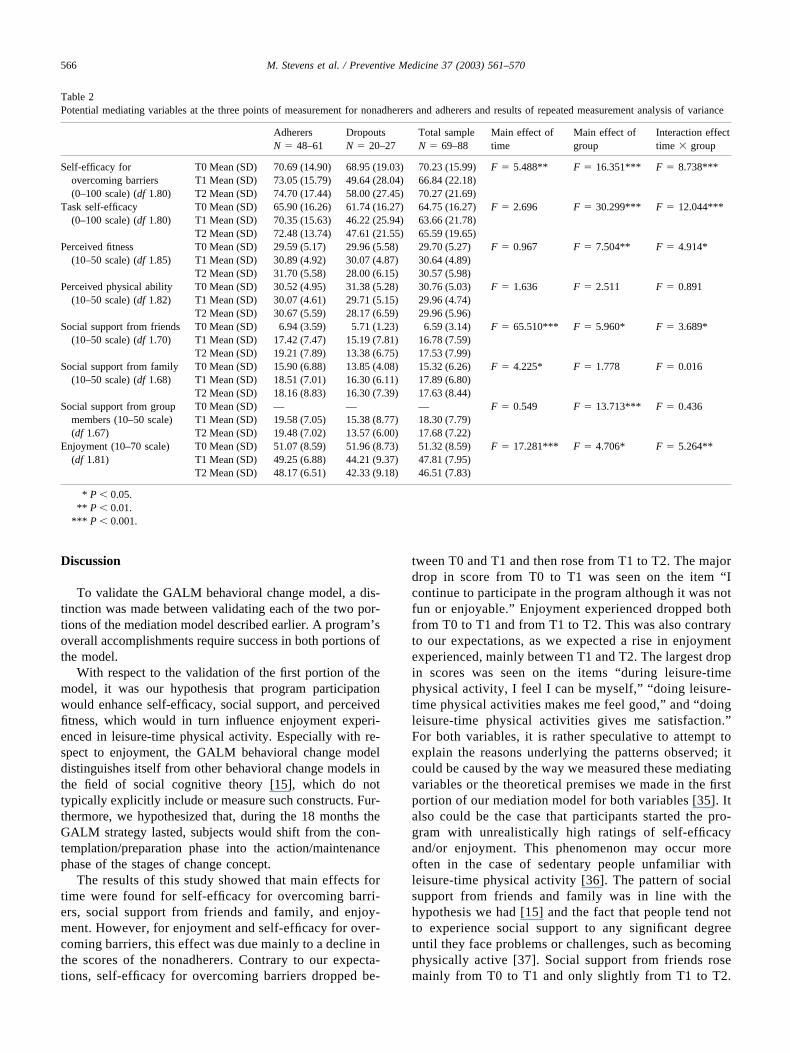
We hypothesized that, during the 18 months the GALMstrategy lasted, subjects would shift from the contemplation/preparation phase into the action/maintenance phase of thestages of change. From T0 through T2 indeed a shift wasseen from the contemplation/preparation to the action/main-tenance stage. Table 2 lists means and standard deviationsof the potentially mediating variables at the three points of
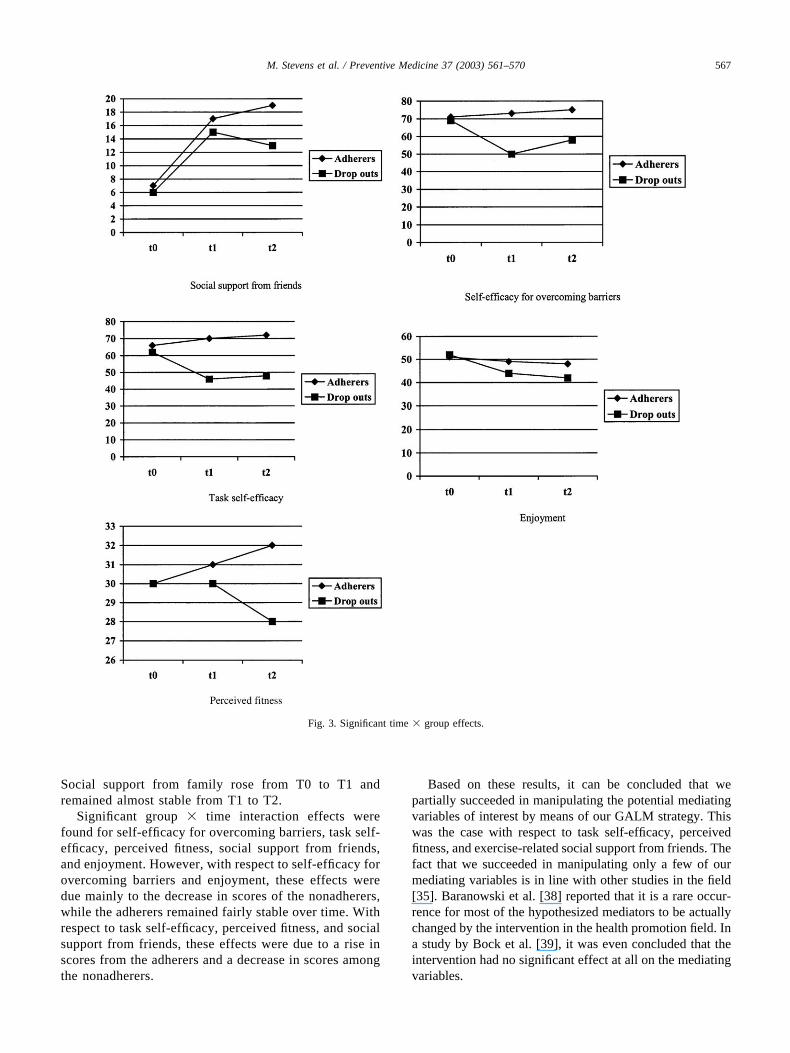
measurements for nonadherers and adherers separately, aswell as the results of the repeated measures analyses ofvariance. In Fig. 3, significant interaction effects are shown.
For self-efficacy for overcoming barriers and task self-efficacy, we observed at T0 few differences between adher-ers and nonadherers, with a slight increase in self-efficacyfor the adherers during the whole program and a strongdecrease in self-efficacy for the nonadherers between T0and T1. For both self-efficacy measures, the time � groupinteraction effect and the main effect of group were signif-icant. For the total sample, self-efficacy was lowest on T1,with a significant main effect of time in self-efficacy forovercoming barriers. Perceived physical ability showed nosignificant effects, although the nonadherers decreased onthis variable while the adherers remained fairly stable (seeTable 2).
Perceived fitness was similar for adherers and nonadher-ers at T0, but increased for the adherers and decreased forthe nonadherers, as demonstrated by the significant time �group and group effects.
For both groups, social support from friends increasedstrongly between T0 and T1, with a significant main effectof time. At all three measurement points, the adherers per-ceived more social support from friends than the nonadher-ers, with a significant main effect of group. For adherers,social support from friends continued to increase betweenT1 and T2, but decreased for nonadherers, as demonstratedby a significant time � group interaction effect. For bothgroups, social support from family increased between T0and T1 and remained stable between T1 and T2, with onlya significant main effect of time. Social support from groupmembers was measured only at T1 and T2. At these mea-surement points, adherers perceived more support fromgroup members than the nonadherers, as shown by a sig-nificant main effect of group. Social support of group mem-bers remained stable between T1 and T2 for both groups.
Finally, enjoyment was comparable at T0 for adherersand nonadherers. Both groups reported some decrease intheir enjoyment levels during the program, with a smallerdecrease for the adherers, resulting in significant main ef-fects of time and group and a significant time � groupinteraction effect.
To gain insight into the relative importance of the po-tential mediating variables in discriminating between adher-ers and nonadherers, a multivariate discriminant analysiswas used. Table 3 shows that task self-efficacy, self-efficacyfor overcoming barriers, and enjoyment played the greatestrole in explaining the difference in scores between theadherers and nonadherers at T1. We computed a canonicalcorrelation of 0.50 and found that 73.8% of the subjectswere classified correctly. The analysis at T2 revealed thattask self-efficacy, social support from group members, andenjoyment explained most of the difference between adher-ers and nonadherers. A canonical correlation of 0.66 wascomputed, and 80.0% of the subjects were classified cor-rectly.
Table 1Stage of change at the three points of measurementa
Stage T0(N � 96)
T1(N � 96)
T2(N � 96)
Precontemplation — 2 (2.1%) 8 (8.3%)Contemplation 94 10 (10.4%) 19 (19.8%) 1Preparation 2 38 (39.6%) 3 (3.1%)Action/maintenance — 39 (40.6%) 66 (68.8%) 2Missing — 7 (7.3%) —
a T0, baseline measurement; T1, measurement after the introductoryprogram; T2, measurement after the follow-up program; 1 dropouts; 2adherers.
}}
565M. Stevens et al. / Preventive Medicine 37 (2003) 561–570
Discussion
To validate the GALM behavioral change model, a dis-tinction was made between validating each of the two por-tions of the mediation model described earlier. A program’soverall accomplishments require success in both portions ofthe model.
With respect to the validation of the first portion of themodel, it was our hypothesis that program participationwould enhance self-efficacy, social support, and perceivedfitness, which would in turn influence enjoyment experi-enced in leisure-time physical activity. Especially with re-spect to enjoyment, the GALM behavioral change modeldistinguishes itself from other behavioral change models inthe field of social cognitive theory [15], which do nottypically explicitly include or measure such constructs. Fur-thermore, we hypothesized that, during the 18 months theGALM strategy lasted, subjects would shift from the con-templation/preparation phase into the action/maintenancephase of the stages of change concept.
The results of this study showed that main effects fortime were found for self-efficacy for overcoming barri-ers, social support from friends and family, and enjoy-ment. However, for enjoyment and self-efficacy for over-coming barriers, this effect was due mainly to a decline inthe scores of the nonadherers. Contrary to our expecta-tions, self-efficacy for overcoming barriers dropped be-
tween T0 and T1 and then rose from T1 to T2. The majordrop in score from T0 to T1 was seen on the item “Icontinue to participate in the program although it was notfun or enjoyable.” Enjoyment experienced dropped bothfrom T0 to T1 and from T1 to T2. This was also contraryto our expectations, as we expected a rise in enjoymentexperienced, mainly between T1 and T2. The largest dropin scores was seen on the items “during leisure-timephysical activity, I feel I can be myself,” “doing leisure-time physical activities makes me feel good,” and “doingleisure-time physical activities gives me satisfaction.”For both variables, it is rather speculative to attempt toexplain the reasons underlying the patterns observed; itcould be caused by the way we measured these mediatingvariables or the theoretical premises we made in the firstportion of our mediation model for both variables [35]. Italso could be the case that participants started the pro-gram with unrealistically high ratings of self-efficacyand/or enjoyment. This phenomenon may occur moreoften in the case of sedentary people unfamiliar withleisure-time physical activity [36]. The pattern of socialsupport from friends and family was in line with thehypothesis we had [15] and the fact that people tend notto experience social support to any significant degreeuntil they face problems or challenges, such as becomingphysically active [37]. Social support from friends rosemainly from T0 to T1 and only slightly from T1 to T2.
Table 2Potential mediating variables at the three points of measurement for nonadherers and adherers and results of repeated measurement analysis of variance
AdherersN � 48–61
DropoutsN � 20–27
Total sampleN � 69–88
Main effect oftime
Main effect ofgroup
Interaction effecttime � group
Self-efficacy forovercoming barriers(0–100 scale) (df 1.80)
T0 Mean (SD) 70.69 (14.90) 68.95 (19.03) 70.23 (15.99) F � 5.488** F � 16.351*** F � 8.738***T1 Mean (SD) 73.05 (15.79) 49.64 (28.04) 66.84 (22.18)T2 Mean (SD) 74.70 (17.44) 58.00 (27.45) 70.27 (21.69)
Task self-efficacy(0–100 scale) (df 1.80)
T0 Mean (SD) 65.90 (16.26) 61.74 (16.27) 64.75 (16.27) F � 2.696 F � 30.299*** F � 12.044***T1 Mean (SD) 70.35 (15.63) 46.22 (25.94) 63.66 (21.78)T2 Mean (SD) 72.48 (13.74) 47.61 (21.55) 65.59 (19.65)
Perceived fitness(10–50 scale) (df 1.85)
T0 Mean (SD) 29.59 (5.17) 29.96 (5.58) 29.70 (5.27) F � 0.967 F � 7.504** F � 4.914*T1 Mean (SD) 30.89 (4.92) 30.07 (4.87) 30.64 (4.89)T2 Mean (SD) 31.70 (5.58) 28.00 (6.15) 30.57 (5.98)
Perceived physical ability(10–50 scale) (df 1.82)
T0 Mean (SD) 30.52 (4.95) 31.38 (5.28) 30.76 (5.03) F � 1.636 F � 2.511 F � 0.891T1 Mean (SD) 30.07 (4.61) 29.71 (5.15) 29.96 (4.74)T2 Mean (SD) 30.67 (5.59) 28.17 (6.59) 29.96 (5.96)
Social support from friends(10–50 scale) (df 1.70)
T0 Mean (SD) 6.94 (3.59) 5.71 (1.23) 6.59 (3.14) F � 65.510*** F � 5.960* F � 3.689*T1 Mean (SD) 17.42 (7.47) 15.19 (7.81) 16.78 (7.59)T2 Mean (SD) 19.21 (7.89) 13.38 (6.75) 17.53 (7.99)
Social support from family(10–50 scale) (df 1.68)
T0 Mean (SD) 15.90 (6.88) 13.85 (4.08) 15.32 (6.26) F � 4.225* F � 1.778 F � 0.016T1 Mean (SD) 18.51 (7.01) 16.30 (6.11) 17.89 (6.80)T2 Mean (SD) 18.16 (8.83) 16.30 (7.39) 17.63 (8.44)
Social support from groupmembers (10–50 scale)(df 1.67)
T0 Mean (SD) — — — F � 0.549 F � 13.713*** F � 0.436T1 Mean (SD) 19.58 (7.05) 15.38 (8.77) 18.30 (7.79)T2 Mean (SD) 19.48 (7.02) 13.57 (6.00) 17.68 (7.22)
Enjoyment (10–70 scale)(df 1.81)
T0 Mean (SD) 51.07 (8.59) 51.96 (8.73) 51.32 (8.59) F � 17.281*** F � 4.706* F � 5.264**T1 Mean (SD) 49.25 (6.88) 44.21 (9.37) 47.81 (7.95)T2 Mean (SD) 48.17 (6.51) 42.33 (9.18) 46.51 (7.83)
* P � 0.05.** P � 0.01.
*** P � 0.001.
566 M. Stevens et al. / Preventive Medicine 37 (2003) 561–570
Social support from family rose from T0 to T1 andremained almost stable from T1 to T2.
Significant group � time interaction effects werefound for self-efficacy for overcoming barriers, task self-efficacy, perceived fitness, social support from friends,and enjoyment. However, with respect to self-efficacy forovercoming barriers and enjoyment, these effects weredue mainly to the decrease in scores of the nonadherers,while the adherers remained fairly stable over time. Withrespect to task self-efficacy, perceived fitness, and socialsupport from friends, these effects were due to a rise inscores from the adherers and a decrease in scores amongthe nonadherers.
Based on these results, it can be concluded that wepartially succeeded in manipulating the potential mediatingvariables of interest by means of our GALM strategy. Thiswas the case with respect to task self-efficacy, perceivedfitness, and exercise-related social support from friends. Thefact that we succeeded in manipulating only a few of ourmediating variables is in line with other studies in the field[35]. Baranowski et al. [38] reported that it is a rare occur-rence for most of the hypothesized mediators to be actuallychanged by the intervention in the health promotion field. Ina study by Bock et al. [39], it was even concluded that theintervention had no significant effect at all on the mediatingvariables.
Fig. 3. Significant time � group effects.
567M. Stevens et al. / Preventive Medicine 37 (2003) 561–570

With respect to the stages of change variable, it can beconcluded that subjects shifted from the contemplation/preparation phase to the action/maintenance phase, confirm-ing that participants indeed move through these stages ofchange during the 18-month period. This result is an indi-cation that the formerly sedentary participants did generallychange their lifestyle into a physically active one. In thisrespect, this study is one of the few that has been specifi-cally designed to change the lifestyle of older adults [40].The effect of this lifestyle change on health and fitness is theobjective of a parallel study that is being currently carriedout.
With respect to the second portion of the proposedmediation model, we hypothesized that the changes in thepotential mediating variables (self-efficacy, social sup-port, perceived fitness, and enjoyment) would eventuallylead to an enduring physically active lifestyle [15]. As aconsequence of this hypothesis, it should have been pos-sible to detect differences between people with less thanadequate adherence to the GALM physical activity pro-gram and those who adequately adhered. In this study,main group effects for adherers and nonadherers werefound for self-efficacy for overcoming barriers, task self-efficacy, perceived fitness, social support from friendsand group members, and enjoyment. For self-efficacy forovercoming barriers, task self-efficacy, and perceivedfitness, an increase was seen in the scores for adhererswhile a decrease was observed for nonadherers. For thesocial support from friends variable, an increase was seenin scores for both the adherers and nonadherers, althoughthe largest increase was seen in the adherers. With re-spect to both social support from group members andenjoyment, a decrease was seen in the scores of bothgroups, although the scores among the nonadherers de-creased the most.
From the results of the discriminant analysis, it can beconcluded that enjoyment plays a relatively importantrole in explaining the difference between adherers andnonadherers, at both T1 and T2. Besides the role ofenjoyment, the dominant role of task self-efficacy andself-efficacy for overcoming barriers at T1 and T2 is in
line with earlier research with respect to the role ofself-efficacy and behavioral change [41]. At T2, besidestask self-efficacy and enjoyment, social support fromgroup members played an important role in this sample.The relative importance of social support from groupmembers found in the discriminant analyses at T2 justi-fies this extension of the original social support scale bySallis et al. [30] with an additional subscale for groupmembers to cover the full range of social support thatsubjects can receive during the process of behavioralchange. Especially for older adults, social support fromgroup members can be important, given that with increas-ing age loved ones (mainly spouses) pass away.
The GALM behavioral change model was especiallydesigned to provide a theoretical framework for the GALMstrategy. In this longitudinal study, only participants fittingin the contemplation/preparation phase were included. Withrespect to behavioral change, this group was considered ofprimary interest. Subjects in the maintenance/action phaseare already active, while subjects in the precontemplationphase report little intention or motivation to become moreactive currently. In terms of stimulation of a physicallyactive lifestyle, this latter group is likely to be the mostrelevant but also the most difficult to reach. In that sense, itremains a challenging and laborious task to develop effec-tive strategies by which subjects in the precontemplationphase can also be effectively persuaded to become physi-cally active. A promising step in this direction is the factthat our recruitment strategies yielded a reasonably largepercentage of precontemplators (17%) who signed up forthe GALM program.
In general, it is assumed that physical activity behav-ior models and theories of behavioral change account forsomewhere between 20 and 40% of the explained vari-ance in physical activity participation. Some researchersare more conservative and give percentages of between20 and 30%, but they argue that with the development ofmodels specifically designed for physical activity behav-ior it should be possible to reach explanations of highervariance percentages [42]. For the time being, it looks asif we succeeded in this respect with the GALM behav-
Table 3Discriminant analysis using potentially mediating variables to explain adherers from dropouts after 6 months (T1) and 18 months (T2)(standardized coefficients)
T1a T2b
Task self-efficacy 0.84 Task self-efficacy 0.85Self-efficacy for overcoming barriers 0.72 Social support from group members 0.52Enjoyment 0.47 Enjoyment 0.49Social support from group members 0.39 Self-efficacy for overcoming barriers 0.43Social support from family 0.29 Social support from friends 0.39Social support from friends 0.15 Perceived fitness 0.39Perceived physical ability 0.74 Perceived physical ability 0.31Perceived physical fitness 0.30 Social support from family 0.17
a Wilks � 0.75; canonical r � 0.50; classified correctly 73.8%.b Wilks � 0.56; canonical r � 0.66; classified correctly 80.0%.
568 M. Stevens et al. / Preventive Medicine 37 (2003) 561–570

ioral change model with canonical correlations of 0.50and 0.66 (percentages of explained variances of 25 and44%, respectively). On the other hand, we did not suc-ceed in manipulating all of the potential mediating vari-ables being targeted, and we have only some indicationsabout the relative importance of the different mediatingvariables during the process of behavioral change. Fol-low-up research is needed to make definitively clear if thehypothesis as formulated in the conceptual domain is avalid one, and whether, ultimately, enjoyment is the mainmediating variable for a lasting physically active lifestyleor whether self-efficacy, social support, and perceivedfitness also remain important. Especially with respect toenjoyment, the GALM behavioral change model distin-guishes itself from other behavioral change models in thefield of social cognitive theory [15].
Acknowledgment
For critical suggestions during preparation of the articlethe authors thank Dr. A.C. King of Stanford MedicalSchool, Palo Alto, CA, USA.
References
[1] Powell KE, Blair SN. The public health burdens of sedentary livinghabits: theoretical but realistic estimates. Med Sci Sports Exerc 1994;26:851–6.
[2] Bijnen FCH, Mosterd WL, Caspersen CJ. Physical inactivity: a riskfactor for coronary heart disease; a position statement for the WorldHealth Organization, governments, heart foundations, societies ofcardiology and other health professionals. Geneva: International So-ciety for the World Health Organization; 1992.
[3] Blair SN, Kohl HW, Paffenbarger RS, Clark DG, Cooper KH, Gib-bons LW. Physical fitness and all-cause mortality: a prospective studyof healthy men and women. JAMA 1989;262:2395–401.
[4] Bouchard C, Shephard RJ, Stephens TS 1994. Physical activity,fitness, and health. International proceedings and consensus state-ment. Champaign, IL: Human Kinetics.
[5] Bijnen FCH, Feskens EJM, Caspersen CJ, Giampaoli S, NissinenAM, Menotti A, et al. Physical activity and cardiovascular risk factorsamong elderly men in Finland, Italy, and The Netherlands. Am JEpidemiol 1996;143:553–61.
[6] Schuit AJ. Regular physical activity in old age. Effect on coronaryheart disease risk factors and well-being. Thesis, Wageningen Agri-cultural University; 1997.
[7] Physical activity and health: a report of the Surgeon General. Atlanta,GA: Department of Health and Human Services, Centers for DiseaseControl and Prevention, National Center for Chronic Disease Preven-tion and Health Promotion; 1996.
[8] Persbericht PB98-139. Voorburg: Centraal Bureau voor de Statistiek(CBS); 1998.
[9] Backx FJG, Swinkels H, Bol E. Hoe lichamelijk (in)actief zijn Ned-erlandse volwassenen in hun vrije tijd. CBS Maandschrift 1994;3:4–11.
[10] Urlings IJM, Douwes M, Hildebrandt VH, Stiggelbout M, OoijendijkWTM. Relatieve validiteit van een vragenlijst naar lichamelijke ac-tiviteit volgens de ’beweegnorm’. Geneeskunde Sport 2000;33:17–22.
[11] Greef de MHG, Stevens M, Bult P, Lemmink KAPM, Rispens P.Groningen Active Living Model: manual. Haarlem: De Vrieseborch,1997.
[12] Chen HT. Theory driven evaluations. Newbury Park, CA: Sage, 1990.[13] Kraemer HC, Stice E, Kazdin A, Offord D, Kupfer D. How do risk
factors work together? Mediators, moderators, and independent, over-lapping, and proxy risk factors. Am J Psychiatry 2001;158:848–56.
[14] Dishman RK, Sallis JF. Determinants and interventions for physicalactivity and exercise. In: Bouchard C, Shephard RJ, Stephens TS,editors. Physical activity, fitness, and health. International proceed-ings and consensus statement. Champaign, IL: Human Kinetics,1994. p. 214–38.
[15] Stevens M, Bult P, Greef de MHG, Lemmink KAPM, Rispens P.Groningen Active Living Model (GALM): stimulating physical ac-tivity in sedentary older adults. Prev Med 1999;29:267–76.
[16] Stevens M, Lemmink KAPM, Greef de MHG, Rispens P. GroningenActive Living Model (GALM): stimulating physical activity in sed-entary older adults; first results. Prev Med 2000;31:547–53.
[17] Maddux JE, Brawley L, Boykin A. Self-efficacy and health behavior:prevention, promotion and detection. In: Maddux JE, editor. Self-efficacy, adaptation, and adjustment: theory, research, and applica-tion. New York: Plenum; 1995, p. 173–96.
[18] McAuley E. Self-efficacy and the maintenance of exercise participa-tion in older adults. J Behav Med 1993;16:103–13.
[19] Bandura A. Human agency in social cognitive theory. Am Psychol1989;44:1175–84.
[20] King AC, Blair SN, Bild DE, Dishman RK, Dubbert PM, Marcus BH,et al. Determinants of physical activity and interventions in adults.Med Sci Sports Exerc 1992;24(Suppl):221–36.
[21] Wankel LM, Yardley JK, Graham J. The effects of motivationalinterventions upon the exercise adherence of high and low self-motivated adults. Can J Appl Sport Sci 1985;10:147–56.
[22] Csikzentmihaly M. Beyond boredom and anxiety. London: Jossey–Bass, 1975.
[23] Csikzentmihaly M, Rathunde K. The measurement of flow in everyday life: toward a theory of emergent motivation. In: Jacobs JE,editor. Nebraska Symposium on Motivation, 1992: developmentalperspectives on motivation. Lincoln, NE: Univ. of Nebraska; 1993, p.229.
[24] Bult P, Rispens P. Learning to move, acquiring versatility in move-ment through upbringing and education. Maastricht: Shaker, 1999.
[25] American College of Sports Medicine Position Stand. exercise andphysical activity for older adults. Med Sci Sports Exerc 1998;30:992–1008.
[26] McAuley E, Mihalko SL. Measuring exercise related self-efficacy. In:Duda JL, editor. Advances in sport and exercise psychology mea-surement. Fitness Technol 1998:371–90.
[27] Bosscher RJ, Laurijssen L, Boer de E. Measuring physical self-efficacy in old age. Percept Mot Skills 1993;77:470.
[28] Ryckman RM, Robbins MA, Thornton B, Contrell P. Developmentand validation of a physical self-efficacy scale. J Personal Soc Psy-chol 1982;42:891–900.
[29] Stevens M, Bakker-van Dijk A, Greef de MHG, Lemmink KAPM,Rispens P. A Dutch questionnaire for self-efficacy in leisure-timephysical activity. J Aging Physical Activity 2001;9:223–32.
[30] Sallis JF, Grossman RM, Pinski RB, Patterson TL, Nader PR. Thedevelopment of scales to measure social support for diet and exercisebehaviors. Prev Med 1987;16:825–36.
[31] Stevens M, Bakker-van Dijk A, Greef de MHG, Lemmink KAPM,Rispens P. A Dutch version of the social support for exercise behav-iors scale. Percept Mot Skills 2000;90:771–4.
[32] Lemmink KAPM. The Groningen fitness test for the elderly [thesis].Groningen: Groningen Univ, 1996.
[33] Stevens M, Moget P, Greef de MHG, Lemmink KAPM, Rispens P. TheGroningen enjoyment Questionnaire (GEQ): a measure of enjoyment inleisure-time physical activity. Percept Mot Skills 2000;90:601–4.
569M. Stevens et al. / Preventive Medicine 37 (2003) 561–570

[34] Marcus BH, Owen N. Motivational readiness, self-efficacy and deci-sion-making for exercise. J Appl Soc Psychol 1992;22:3–16.
[35] Sallis JF. Progress in behavioral research on physical activity. AnnBehav Med 2001;23:77–8.
[36] Oman RF, King AC. Predicting the adoption and maintenance ofexercise participation using self-efficacy and previous exercise par-ticipation rates. Am J Health Promot 1998;12:154–61.
[37] Heuvelen van MJG. Physical activity, physical fitness and disabilityin older persons (thesis). Groningen: Univ. of Groningen, 1999.
[38] Baranowski T, Anderson C, Carmack C. Mediating variable frame-work in physical activity interventions: how are we doing? Howmight we do better? Am J Prev Med 1998;15:266–97.
[39] Bock BC, Marcus BH, Pinto BM, Forsyth LH. Maintenance ofphysical activity following an individualized motivationally tailoredintervention. Ann Behav Med 2001;23:79–87.
[40] King AC, Rejeski WJ, Buchner DM. Physical activity interventionstargeting older adults: a critical review and recommendations. Am JPrev Med 1998;15:316–33.
[41] McAuley E, Lox C, Duncan TE. Long-term maintenance of exercise,self-efficacy, and physiological change in older adults. J Gerontol1993;48:218–24.
[42] Baranowski T, Lin LS, Wetter DW, Resnicow K, Hearn MD. Theoryas mediating variables: why aren’t community interventions workingas desired? Ann Epidemiol 1997;7(No. 57):589–95.
570 M. Stevens et al. / Preventive Medicine 37 (2003) 561–570