
Final Thesis for submission
193
UNIVERSITY OF TRINIDAD AND TOBAGO (UTT), 2014 HEALTH SCIENCES Masters in Health Administration (MHA) TITLE: ASSESSMENT OF PATIENTS’ SATISFACTION OF THE MEDICAL SERVICES OFFFERED WITHIN THE TRINIDAD AND TOBAGO DEFENCE FORCE (TTDF) Dexter A Horsford PS57101 2014 University of Trinidad and Tobago | Masters in Health Administration | May 2014
Transcript of Final Thesis for submission

UNIVERSITY OF TRINIDAD AND TOBAGO (UTT), 2014
HEALTH SCIENCES
Masters in Health Administration (MHA)
TITLE: ASSESSMENT OF PATIENTS’ SATISFACTION OF THE MEDICAL
SERVICES OFFFERED WITHIN THE TRINIDAD AND TOBAGO DEFENCE FORCE
(TTDF)
Dexter A Horsford
PS57101
2014
University of Trinidad and Tobago | Masters in Health Administration | May 2014

11565 words
This work is being submitted in partial fulfillment of the
requirements for a Masters in Health Administration (MHA)
ABSTRACT
Objective
To investigate the personnel satisfaction of the medical
services offered within the TTDF develop appropriate
recommendations that can be used to enhance the quality and
accessibility of health care in the TTDF.
Method
The study design used was a survey research design and
conducted using a self-administered questionnaire (see
Appendix A) to determine the level of satisfaction of the
medical services offered in the TTDF. The theoretical
framework, on which this research is based, is the Primary
Provider Theory. Two hundred and fifty of the TTDF personnel
participated in the survey. The analysis was completed using
SPSS. The questionnaire was administered and collected at the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
ii

major camps and bases of the TTDF when it was expected that
the majority of personnel would be on location/
Result
The results for the frequency distribution of the GSAT
Variable indicated an average of 238 personnel responded to
the survey and that there was dissatisfaction. Very satisfied
with the medical services variable had a total of 47.7% that
disagreed. The results showed that the medical care is just
perfect had 58.5% respondent disagreeing whilst 42(17.5%).
The frequency distribution indicated that 88.9% agreed things
about the medical system need to be improved. The variable-
some things about the medical care could be better had 92.9%
of the respondents agreeing. The results for the medical care
is excellent indicated that 60.6% disagree. Finally 79.6%
indicated that they agreed to dissatisfaction with some things
about the medical care. Overall there was a satisfaction rate
of 46.90 percent
Conclusion
The research question “What is the level of patient
satisfaction within the Trinidad and Tobago Defence Force and
University of Trinidad and Tobago | Masters in Health Administration | May 2014
iii

what are the factors that influence it?” was answered in the
study. The study concluded that patients’ satisfaction of the
medical services offered in the TTDF was 46.9percent which was
below the international standards of 95 percent.
Data analysis revealed
A total of 250 personnel participated in the survey with 198
male respondent and 41 female respondents. .The sample
comprised 82.8 percent male and 17.2 percent female conforming
to the general composition of the TTDF male female ratio of
90:10. One hundred and sixty-seven (167) of the respondents
were in the 25-34 age groups representing 69.6 %; with 46 from
the 25-44 age group that represents 18.4%, 26 from the 18-24
age group that represents 10.8% and 1 from the 45 and over
group a percentage of 0.1.
Recommendations
Constructing a process flow of the entire process in medical
inspection room to determine if the time can be reduced to
improve the flow for patients, if time cannot be reduced what
successful and established activities can be introduced that
can occupy the attention of the patient and reduce the
negative impact off waiting for long periods.Reviewing the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
iv

policies, which govern the provision of medical services to
determine adequacy, relevance to personnel medical
needs.Institute a mandatory patients’ satisfaction survey to
help determine the extent of success or failure of the medical
system and services. Take satisfaction scores seriously as in
many jurisdictions this is mandatory
Keywords: Trinidad and Tobago Defence Force (TTDF), personnel
satisfaction, restructuring, opinions, relationship,
association.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
v

ACKNOWLEDGEMENT
The Chief of Defence Staff for approving the study within the
Force
Formation Commanders for their support in conducting the
studies.
Executive Officer of the Trinidad and Tobago Coast Guard-
Lieutenant Commander Archer who’s assistance was timely when I
was faced with the possibility of low response from Coast
Guard also in lieu of the CDS approval.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
vi

Majors KAK Sebastien and AD Williams who approved the study in
lieu of the CDS’s approval.
Major K Francis, Lieutenant N McIntyre and Sub-Lieutenant
Gohnity who assisted me in the gathering of the data.
My family who supported and abided with me along the entire
process.
Dexter A Horsford; R.D.
Mr.
LIST OF ABBREVIATIONS
University of Trinidad and Tobago | Masters in Health Administration | May 2014
vii

AAC Access/Availability/Convenience
AHQR Agency for Healthcare Research
CAHPS Consumer Assessment of Healthcare Providers and Systems
CDS Chief of Defence Staff
CCC Civilian Conservation Corp
CF Canadian Force
CFHS Canadian Force Health Services
CG Coast Guard
COMM Communication
CNCD’s Chronic Non-communicable Diseases
CRDAMC Carl R. Darnall Army Medical Center
DFHQ Defence Force Headquarters
DFR Defence Force Reserves
DFMO Defence Force Medical Officer
DFSI Dental Functional Status Index
DoD Department of Defence
FIN Finance
GSAT General Satisfaction
HEN Health Evidence Network
HLIS Health and Lifestyle Survey
ICE Interactive Customer Evaluation
INTER Interpersonal Aspect
MHA Masters in Health Administration
University of Trinidad and Tobago | Masters in Health Administration | May 2014
viii

MILAT Military Led Academic Training
MIR Medical Inspection Room
MYPARTMilitary Led Youth Programme of Apprenticeship and
Reorientation Training
NCQA National Committee for Quality Assurance
MHS Military Health Services
MHI Rand Mental Health Index
PSS Patient Satisfaction Survey
PSQ Patients’ Satisfaction Questionnaire
R3MMU Role 3 Multinational Medical Unit
SIP Sickness Impact Profile
SSB Support and Services Battalion
SYSP Specialized Youth Service Programme
TTA Trinidad and Tobago Army
TTAG Trinidad and Tobago Air Guard
TTCG Trinidad and Tobago Coast Guard
TTDF Trinidad and Tobago Defence Force
TECH Technical Aspect
TTR Trinidad and Tobago Regiment
UTT University of Trinidad and Tobago
Visitdrho
spVisit to the DFMO Private Office,Hospitalized
WHO World Health Organization
University of Trinidad and Tobago | Masters in Health Administration | May 2014
ix

1st Engr
BnFirst engineering Battalion
1TTR First Infantry Battalion
2TTR Second Infantry Battalion
LIST OF TABLES OR FIGURES
Table Page
Table 1: Showing the Number of Valid Response for the
Demographics Data
Table 2: Showing the Frequency of Sex
Table 3: Showing the Frequency of Age
Table4: Showing the Frequency of Marital Status
Table 5: Showing the Frequency of Education Level
Table 6: Showing the Frequency of Insurance Coverage
Table 7: Showing the Frequency of History of admission to Sick
Bay
Table 8: Showing the Frequency of Years of military service
Table 9: Showing the Frequency of Category of personnel
Table 10: Showing the Frequency of Formations
Table 11: Showing the Number of Valid Response for the General
Satisfaction (GSAT) Variables
Table 12: Frequency Of General Satisfaction (GSAT) Theme
(%)Factors influencing patient satisfaction in the TTDF
29
29
30
31
32
33
34
35
36
37
38
39
41
University of Trinidad and Tobago | Masters in Health Administration | May 2014
x

Tables13: Showing the relationship of significance between each
independent variable and general satisfaction
Tables 14: Showing the relationship of insignificance between
eachindependent variable and general satisfaction
Chart 1: Showing results of Mann-Whitney Test for Sex
Chart 2: Showing results of Kruskal-Wallis Test for History of
Admission to Sick Bay
Chart 3: Showing results of Kruskal-Wallis Test Education Levels
Chart 4: Showing results of Kruskal-Wallis Test for Insurance
Coverage
Chart 5: Showing results of Kruskal-Wallis Test for Marital
Status
Chart 6: Showing results of Kruskal-Wallis Test for Category of
Personnel
Chart 7: Showing results of Kruskal-Wallis Test for Formation
Chart 8: Showing results of Kruskal-Wallis Test for Age
Table 15: Ranks (Mann-Whitney Test) GenSatisfaction History of
admission to Sick Bay
Table 16: Ranks (Mann-Whitney Test) GenSatisfaction and Sex
Chart 1: Frequency Of General Satisfaction(GSAT) Theme
44
46
47
47
48
48
49
49
50
50
51
40
University of Trinidad and Tobago | Masters in Health Administration | May 2014
xi

TABLE OF CONTENT
SUBJECT PAGE
Abstract iiKeywords ivAcknowledgement vList of Abbreviations viList of Tables or Figures viiiIntroduction 1Literature Review 6Research Question 14Objectives 14Study Goal(S) 14Objectives of the Study 14
University of Trinidad and Tobago | Masters in Health Administration | May 2014
xii

Significance or Relevance of Study 15Methodology 16
Data Collection 22Data Analysis 23Limitations 26Strengths 27Ethical Considerations 28
Results 29Discussion 52Conclusion 57
58Recommendations 59References 61Appendices 64
University of Trinidad and Tobago | Masters in Health Administration | May 2014
xiii

INTRODUCTION
The Trinidad and Tobago Defence Force (TTDF) was established
in 1962 under the Defence Force Act 14:01 and was given the
following responsibilities:
To defend the sovereign good of the Republic of Trinidad
and Tobago;
To cooperate with and assist the civil power in
maintaining law and order;
To assist the civil authorities in times of crisis or
disaster;
To perform ceremonial functions on behalf of the State;
To provide Search and Rescue services in keeping with
national requirements and
under international agreements to;
Assist in the prevention of trafficking of narcotics and
other illegal goods;
Monitor the safety of shipping in national waters;
Assist in the development of the national community.
At the time of establishment of TTDF it comprised two
formations, the Trinidad and Tobago Regiment (TTR), comprising
one Battalion and the Trinidad and Tobago and Coast Guard
University of Trinidad and Tobago | Masters in Health Administration | May 2014
(TTCG), consisting of a Naval Arm and Air Wing. Over the past
two decades, the TTDF has been restructured from its original
composition of two formations to four formations. The Regiment
comprising of two Infantry Battalions, one Engineer Battalion
and a Logistic Battalion; an increase in personnel of the
TTCG, the formation of the Trinidad and Tobago Air Guard
(TTAG) and the restructuring of the Trinidad and Tobago
Defence Force Reserves (DFR).
This restructuring of the Force also saw increases in
personnel, equipment and infrastructure. There were also
increases in the military lead exercises locally and regional
deployment (example Haiti-1990, Grenada-2005).This also saw
the military leading the main efforts in various youth
programmes (example Specialized Youth Service Programme
(SYSP), Civilian Conservation Corp (CCC), Military Led
Academic Training (MILAT), Military Led Youth Programme of
Apprenticeship and Reorientation Training (MYPART).
Changes were in the Force were inevitable as it sought to keep
abreast of technology and the mandate of the government.
Before the changes in the Force and by extension the medical
University of Trinidad and Tobago | Masters in Health Administration | May 2014
2

department under-mention is a brief look at the department
before the changes occurred:
The main Medical Inspection Room (MIR) was at Teteron
Barracks, Chaguaramas;
At the time there was two doctors employed (DFMO) and
both operated out of Teteron Barracks;
The First Infantry Battalion situated at Camp Ogden, Long
Circular Road, St. James housed a MIR but was regarded as
all other military outstations and bases inclusive of
Camp Signal Hill, Tobago. These camps and bases were
facilitated by medical orderlies who review the men and
women of the Force with minor cases, and persons who were
classified as major were referred to Teteron Barracks to
be seen by the DFMO;
Patients also went to Teteron for referrals to
specialist, dental or optical treatment;
The MIR at Teteron had two sick-bays (male and female),
where patient confined for review and observation on
recommendation by the DFMO necessary;
University of Trinidad and Tobago | Masters in Health Administration | May 2014
3

At Camp Ogden the DFMO would have visited that location
for the sole purpose of seeing children of DF employees
at the Defence Force Children’s Clinic;
Due to the proximity of the Coast Guard (CG) Headquarters
at Staubles Bay to Teteron, the CG Medics performed most
of their duties at the Teteron Barracks;
The pharmacy is also at Teteron;
Before the expansion, the building housed two doctors’
examination rooms, patient waiting area, two sick-bays,
Medical Services Officer office, general admin office,
treatment room and storage room.
As a result of the restructuring, the medical department
expanded and its services decentralised. Some notable changes
were:
Refurbishment of the MIR at both Teteron Barracks and
Camp Ogden;
Cessation of the Children’s Clinic;
Increase in medical doctors from two to three;
One of the doctors being a serving member of the Force
(Coast Guard);
University of Trinidad and Tobago | Masters in Health Administration | May 2014
4

Utilizing the opportunity to send a serving member to
study medicine;
Expanding the type and levels of training for persons
employed in the medical department, some of the training
includes psychiatric nursing, social sciences, dietetics,
pharmacist, radiology and health administration;
Development of MIR at each of the formations that mirrors
the MIR at Teteron Barracks but at a smaller scale;
Increasing the ambulance fleet; and
Forming greater alliances with external medical service
providers.
In the TTDF, the medical practitioners’ opinions are the
foremost opinions taken into consideration to initiate any
changes of the medical services. The opinions of the
recipients were not garnered, to determine the viability or
extent of their needs. In modern studies, researchers began
considering the viewpoints of patients about health services
as an important gauge of the quality of services that may be
different or in opposition with that of health experts. As a
decisive index for evaluating and improving the quality of
University of Trinidad and Tobago | Masters in Health Administration | May 2014
5

services, consideration is given to patients’ viewpoints
concerning the way of providing health service (Ebrahimniaet
al, 2010).
“A soldier should be fighting fit” is a concept that the
military epitomizes. As serving members of the military
optimum health and physical fitness are fundamental to being
effective military personnel. These essentials ensure that
the individual is alert and able to perform at a high
efficiency level during routine duties, training or
operations. Fit individuals make strong team members and
ensure operational readiness at all times. Additionally, they
are at lower risk of becoming injured during training, or heal
more quickly than someone who is below optimum health and
unfit. Regardless of the appointment or occupational task,
military personnel can be called upon to perform difficult and
dangerous tasks, whether they are combative, peace
enforcement, peacekeeping, or aid to the civil power locally,
regionally or internationally.
Though the operational landscape has changed the need to
adequately provide for military personnel medical needs still
requires the efforts of key stakeholder. Providing for the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
6

increase health care needs saw increases in the cost for
providing the services and Central Government Budgetary annual
allocation towards healthcare for the TTDF personnel.
Healthcare can be considered the provision of all services
that prevents illness and maintains health. It includes the
provision of illness treatment and management and extends to
the maintenance of the mental and physical well-being of a
person. Healthcare is, therefore, more than medical care. It
encompasses more than the availability or affordability of
medical services (Michaelet.al.).
Faced with the challenges to cater for the increased medical
needs and the situations of emerging and re-emerging diseases
the military medical services should be able to adequately
address these situations. Over the years, the standards of
the medical services of the TTDF may not have met these
challenges adequately. Additionally, the medical needs of its
personnel may not have kept abreast with the restructuring of
the Force that over the past two decades saw an increase in
personnel. An increase in personnel suffering from lifestyle
diseases, the number one cause of deaths in the Caribbean, was
noted.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
7

These transformations throughout the Force also executed
changes in the medical services as follows:
An increase in medical staff (example first responders);
An increase in the budgetary allocations for medicines and
equipment;
Increases in the amount of Medical Doctor, Registered Nurses
and employment of a Register Dietitian;
Improvement in the infrastructure;
Increase in outsourcing some medical service (psychological
and psychiatric).
Not all changes were increases there was also the
discontinuation of the family clinic.
Despite the many changes, the medical services department also
had to struggle with the expressed dissatisfactions of the
recipients of the services provided, be it real or perceived.
No formal survey or research was conducted as a result of
these changes in the medical service over the past two
decades, to determine compliance, adequacy, efficiency,
effectiveness, overall confidence and satisfaction of the
system and its providers.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
8

Therefore, the goal of this paper is to examine the patient
satisfaction and how it can be used to enhance the quality and
accessibility of health care in the TTDF.Ascertain what may be
the hindrances and make the appropriate recommendations for
sustainable enhancement in the service base on the findings.
The Primary Provider Theory (Aragon 2006) was the theoretical
framework, used to conduct this research. This Theory
emphasizes the importance of the patient-provider relationship
and the weight of the provider’s patient-centeredness on
outcomes.
LITERATURE REVIEW
The literature review discovered that there were no published
articles on patient satisfaction in the military both locally
and regionally. Carman (2000) pointed out that perception of
service quality is an attitude and that the attitude is a
function of some mixture of features that a patient believes
to be features of quality. Division of these features are in
University of Trinidad and Tobago | Masters in Health Administration | May 2014
9
two sets, such as functional, which include measures such as
ambiance and provider attentiveness; and technical, such as
outcome that describe the service delivery. Consequently,
there exist a relation between perceived service quality and
patient satisfaction. Fordet. al., (1997) noted that a
patient satisfaction has become known over the years as a
significant measure of the quality of care offered by health
care organizations. Donabedian (1998) indicated it was not
only essential for gathering insights into the perspective of
the customers on the delivery of the health care service but
also a key outcome of care. Low patient satisfaction may lead
to poor compliance with the likelihood for waste of resources
and suboptimal clinical outcome. As a result satisfaction of
the genuine demands of the patients should be the outcome of
all medical care (McKinley et. al., 1997).
The literature review also confirmed military forces of other
jurisdictions used satisfaction tools to access their
healthcare systems and with the results implemented desired
changes in their medical services. It also revealed there is
no published work regarding the medical services of the TTDF
or any of its formations. This deficiency highlights the need
University of Trinidad and Tobago | Masters in Health Administration | May 2014
10

to initiate comprehensive studies of the medical services, not
limited to such areas as patients’ satisfaction, compliance,
disease prevalence and immerging trends. Without such
researches suitable programmes cannot be initiated that may
meet the medical needs of the Force. Additionally budgetary
allocation may be underestimated or directed into failing
programmes.
The Canadian Force (CF) completed several researches such as
but not limited to the following:
A survey conducted in 1993 with females to determine the
impact on implant-retained oral prostheses and conventional
complete dentures. This used a completed questionnaire based
on three valid and reliable treatment outcome measures:
Dental Functional Status Index (DFSI),
Rand Mental Health Index (MHI),
Elements of the Sickness Impact Profile (SIP), (Harle and
Anderson. 1993).
In 2000, a pioneering Health and Lifestyle Survey (HLIS) was
completed which provided a baseline census for the entire CF.
The results were used to assist in prioritizing health
resource allocations; developing, assessing the success of
University of Trinidad and Tobago | Masters in Health Administration | May 2014
11

health promotion, illness prevention and intervention
programmes
A follow-up HLIS was completed in 2004 and revealed members
were apprehensive about nutrition, exercise and stress but
commonly satisfied with their profession. Four outcomes were
assessed:
Physical and mental health status of the CF;
Prevalence of behaviours that contribute to health
problems;
Degree of the employment of previous health promotion
programmes;
And the potential, utilization and satisfaction with the
CF health care system. (Kelly 2004).
Whereas, in 2006, a 27-items satisfaction survey was done to
evaluate the introduction of chiropractic services in the
military that were traditionally out-sourced and paid for by
its personnel. Subsequent to this a 3-items survey was used
to review recommendation patterns and satisfaction with the
medical services offered (Boudreau et. al., 2006).
During the period February 2006 to October 2009 the CF Health
Services (CFHS) staffed and led the Role 3 Multinational
University of Trinidad and Tobago | Masters in Health Administration | May 2014
12

Medical Unit (R3MMU). The R3MMU experiences were used to
successfully deploy a hospital as part of the earthquake
relief effort in Haiti, in 2010. The training and operating
protocols developed by the R3MMU were applied to disaster
preparedness and trauma care in Canadian civilian hospitals
(Brisebois et. al., 2011).
The US Congress (Senate Committee) in 1993 mandated a survey
under the National Defence Authorization Act for Fiscal Year
of 1993. The survey examined the Military Health Services
(MHS) beneficiaries’ satisfaction with their healthcare
options using questions from the Consumer Assessment of
Healthcare Providers and Systems (CAHPS) Health Plan Survey.
CAHPS was developed by the Agency for Healthcare Research
(AHQR) and the National Committee for Quality Assurance (NCQA)
and is a comprehensive tool for measuring consumer
satisfaction with health plans.
Introduction of TRICARE in the United States (US) occurred to
improve the access to health care system and to take advantage
of the capabilities of the managed-care industry (Schafer
2010). To improve the Department of Defence (DoD) delivery of
health care services, a TRICARE took place in 2011. In this
University of Trinidad and Tobago | Masters in Health Administration | May 2014
13

report a comparison was done between the MHS beneficiaries who
had used TRICARE and the civilian benchmark with respect to
ratings of the health plan, the health care, personal
physician and specialty care. Health plan ratings depend on
access to care and how the plan handles various service
aspects such as claims, referrals, and customer complaints.
(TMA, TMA/HPA&E, 2011).
The US Department of Defense (DoD) introduced the Interactive
Customer Evaluation (ICE) system. This system is a web-based
tool that collects feedback on services provided by various
organizations throughout the DoD. The ICE system allows
customers to submit online comment cards in providing feedback
about the service providers they have encountered at military
installations and related facilities around the world. It is
intended to improve customer service by allowing managers to
monitor the satisfaction levels of services provided through
reports and customer comments. Some benefits of ICE programme
are:
It allows DoD customers to quickly and easily provide
feedback to service provider managers;
Gives leadership timely data on service quality;
University of Trinidad and Tobago | Masters in Health Administration | May 2014
14
Allows managers to benchmark the performance of their
service providers against other DoD organizations;
Encourages communication across organizations by
comparing best practices to increase performance results;
Save money by providing managers a free tool to collect
and organization feedback data used for process
improvement (ICE 2011)
Other benefits of conducting PSS are:
That the responses are reviewed and analysed to determine
what is important to the users of the services.
Returned surveys are tied to funds that can be used to improve
services for the personnel’ improve problem areas, upgrade
amenities and expand services (Darnall Army Medical Center,
2013).
Carl R. Darnall Army Medical Center (CRDAMC, 2013) leadership
indicated that the goal for patient satisfaction was to attain
and sustain 95 percent or higher overall satisfaction rate.
Additionally in Iran there was several patients' satisfaction
studies conducted. The study was also conducted to
investigate the hospitalized patients' satisfaction with
University of Trinidad and Tobago | Masters in Health Administration | May 2014
15

hospital services in six military hospitals located in
different parts of Iran, in 2001 (Ebrahimnia et. al., 2010).
The Jewish General Hospital (2014)indicated that satisfaction
rate of 60percent showed that the hospital was doing a good
job at meeting patients’ needs and expectations. In addition
to continually seek to improve an organization should aim at a
satisfaction rate of 90 percent as attaining 100 percent is
seemingly unrealistic to achieve.
Patient satisfaction has gained significance with health
services and was identified as one of the five service quality
indicators by World Health Organization (WHO). In instances
of research, some researchers considered this as one of the
most important indicators of health services quality. The most
frequent studied groups in this field are the hospitalized
patients. The major fields of studying satisfaction with
health services are consideration of patients’ view on the
quality of hospital services.
WHO identified six main potential sources of information for
addressing quality of primary health care these are:
Household surveys.
Routine reports, from both central and peripheral levels.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
16
Client records.
Direct, structured observation.
Follow-up interview.
Laboratory examinations (Roemer and Montoya-Aguilar,
1988).
Health Evidence Network (HEN) synthesis report on hospital
performance was in response to questions from decision-makers.
It provides a synthesis of the best existing evidence, as well
as a summary of the main findings and policy options related
to the issue. The principal methods of measuring hospital
performance were identified as:
Regulatory inspection,
Public satisfaction surveys,
Third-party assessment,
Statistical indicators.
The majority of which have never been tested rigorously with
evidence of their relative effectiveness mostly from
descriptive studies rather than from controlled trials (Shaw C
2003).
An important factor in the improvement of modern healthcare is
the participation of patients in the management of their
University of Trinidad and Tobago | Masters in Health Administration | May 2014
17

treatment and care. This is recognized in current health
strategies in various jurisdictions. To support this process
it is vital to recognize that the knowledge and experience of
patients receiving health care vary noticeably. A number of
them may have an infrequent or acute medical intervention that
may not develop a customer-service provider relation while
others may have a chronic or more enduring and long-term
relationship with a service provider depending on the nature
and extent of their needs.
People centred health care respects the dignity and value of
each person. It is absolutely desirable and appropriate that
the views of patients should be sought on their experiences
and expectations of health care (Irish Society for Quality and
Safety in Healthcare, 2003)
The literature review identified The Primary Provider Theory
which was developed by Dr. Stephen J. Aragon (Aragon, 2003).
This Theory hierarchically relates its satisfaction constructs
to patients expectations, conceding that the primary provider
has the greatest clinical utility to patients, followed by
time spent waiting for the primary provider, and finally the
provider’s assistant. It is a generalized theory of how the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
18
patient-centeredness of health providers has an effect on the
patient’s care behaviour, during patient encounters and
related outcomes. The Theory holds that outcomes such as
satisfaction, trust, ratings of quality and various clinical
outcomes were fundamentally rooted in the patient’s
relationship with their primary provider. As an evidence-based
outcome measurement paradigm, owing to generalize nature of
the Theory it can accommodate an array of healthcare
practitioners as primary providers, including nurses, nurse
practitioners, dentists, physician assistants, allied health
practitioners, as well as physicians in their respective
settings.
The Theory emphasizes the importance of the patient-provider
relationship and the weight of the provider’s patient-
centeredness on outcomes and was based on the following nine
principles that favour patients in healthcare encounters with
their providers and support the scientific method and
Hippocratic Oath.
Clinical competency is a necessary but insufficient
condition of desired outcomes.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
19

Desired outcomes require more than clinical competency
alone, because the transmission of care and clinical
knowledge require effective communication and interaction
with patients.
Patient-centeredness is an underlying ability that
influences the quality of provider's interaction with and
transmission of care to patients.
Providers' patient-centeredness influences the outcomes
of their patients.
Providers are uniquely responsible for the quality of the
transmission of their care and clinical knowledge to
patients.
Providers who are both clinically competent and patient-
centred are more likely to achieve desired outcomes.
Patients and families value the patient-centeredness of
their providers.
The patient-centeredness of the provider is more
important than the financial objectives of a patient
encounter.
Patients are the best judges of the patient-centeredness
of their providers.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
20

The Primary Provider Theory holds that the patient
satisfaction occurs at the nexus of provider power and patient
expectations. More specifically, patient satisfaction is
principally the function of the underlying network of
interrelated satisfaction constructs, such as satisfaction
with the primary provider, waiting for the provider, and
satisfaction with the provider's assistant(s) or auxiliary
staff. Hierarchically related to patient-centred expectations
of provider value, the Theory specifies that primary providers
offer the greatest clinical value to patients. It is
operationalized by patient-centred measures exclusively, where
only patients judge the quality of service, and all other
judgments are immaterial. The Primary Provider Theory offers
an alternative paradigm for the measurement and realization of
patient satisfaction and it can inform patient-centred
physician practice, medical education, quality improvement,
outcome measurement, and satisfaction survey construction.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
21
RESEARCH QUESTION AND OBJECTIVES:
What is the level of patient satisfaction within the TTDF and
what are the factors that influence it?
HYPOTHESIS
University of Trinidad and Tobago | Masters in Health Administration | May 2014
22

H1: There is an association between patients’ satisfaction and the
medical services offered in the Trinidad and Tobago Defence Force.
H0: There is no association between patients’ satisfaction and the
medical services offered in the Trinidad and Tobago Defence Force.
STUDY GOAL(S):
Improvement of the satisfaction levels within the Force of the
medical services offered.
To establish a bench mark for customer satisfaction of the
medical services.
To make the appropriate recommendations for sustainable
improvement in the services based on the conclusion and result
of the research.
OBJECTIVES OF THE STUDY
The main objective of the study was to determine the level of
patient satisfaction in TTDF,
To determine whether the personnel within the TTDF are
satisfied with the health care services offered.
To identify areas of dissatisfaction that needs to be dealt
with.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
23

To develop recommendations that could be used to enhance the
health care services.
SIGNIFICANCE OR RELEVANCE OF STUDY
The significance of this proposed study is to help set in
place a system or systems of measuring the satisfaction of
deliverables of the medical services within the Force. This
would inform the hierarchy of its medical needs and how the
medical service can be a sustained and viable arm of the Force
in addressing it needs. Having no previous studies completed
on patient satisfaction and outcome of the medical services
within the TTDF the study can be the catalyst for future
studies within the Force on medical outcomes ad patient
satisfaction.
The evaluation system would be used to determine the needs of
the TTDF personnel. Whereby meeting these need may mean
developing new programmes, cessation of some current
programmes or realignment of others. Additionally use to
University of Trinidad and Tobago | Masters in Health Administration | May 2014
24

properly allocated resources for the acquisition of medical
goods and services, and develop a Chronic Non-communicable
Diseases (CNCD’s) Clinics for personnel diagnosed as suffering
from any of these diseases. Further for the future base on
the identified needs the establishment of a military hospital.
METHODOLOGY
The study design used was a survey research design and
conducted using a self-administered questionnaire (see
Appendix A) to determine the level of satisfaction of the
medical services offered in the TTDF. In the study all
variables were group according to the Patients’ Satisfaction
University of Trinidad and Tobago | Masters in Health Administration | May 2014
25

Questionnaire III (PSQ-III) subscales. These variables were
adapted for the study of Patients’ Satisfaction of the medical
services offered in the TTDF. The General Satisfaction (GSAT)
is the dependent variable for patients’ satisfaction and is as
follows:
General Satisfaction (GSAT)
I am very satisfied with the medical services I received
The medical care I have been receiving is just perfect
There are things about the medical system where I receive
my care from that need to be improved.
There are some things about the medical care that I
received that could be better.
All things considered the medical care I received is
excellent.
I am dissatisfied with some things about the medical care
I received.
The independent variables were:
Access/Availability/Convenience (AAC)
Can get care without any trouble in the medical
department
Easy to get medical care in an emergency
University of Trinidad and Tobago | Masters in Health Administration | May 2014
26

Usually kept waiting for a long time at the doctor’s
office
Hard to get medical care on short notice
The office hours are convenient (good).
The office should be open for more hours than it is.
Easy access to the medical specialist needed
Communication (COMM)
Doctors explain the reasons for medical tests
Allowed to say everything that I think is important.
Use of medical terms without explaining meaning.
Sometime ignored what they are told
Listen carefully to what is said
Interpersonal Aspect (INTER)
The doctor who treats me should give me more respect.
The doctors who treat me have a genuine interest in me as
a person.
Sometimes doctors make me feel foolish.
Doctors act too business like and impersonal towards me
My doctor treats me in a very friendly and courteous
manner
University of Trinidad and Tobago | Masters in Health Administration | May 2014
27

When I am receiving medical attention, they should pay
more attention to my privacy.
Doctors always do their best to keep me from worrying
In the case of Finance Aspect (FIN) one variable of the
subscale was used due to the medical services being
provided by the TTDF being free for the military
personnel. The variable used was (I have to pay for more
of my medical care than I can afford)
Time Spent with Doctor (DFMO)
Those who provide my health care sometimes hurry too much
when they treat me
The doctors usually spend plenty of time with me
Crisis in the health care (CRISIS)
There is a crisis in the health care within the Force
today.
Technical Aspect (TECH)
Doctors need to be more thorough
Doctor’s office has everything needed to provide medical
care
Sometimes doctors make me wonder if their diagnosis is
correct
University of Trinidad and Tobago | Masters in Health Administration | May 2014
28

They are careful to check everything when treating and
examining
The medical staff knows about the latest medical
development
Doctors never expose me to unnecessary risks.
The doctor lack experience with my medical problem.
Doctors rarely give advice to avoid illness and staying
healthy.
Some doubts about the ability of the doctor.
Doctors are very competent and well-trained.
The following two sets of variables were included in the
study to assist with improving the illustration of the
study results.
Ratings
Rating the services provided by the female doctor
Rating the services provided by the senior male doctor
Rating the services provided by the enlisted doctor
Rating the services provided by the Pharmacist
Rating the services provided by the Medical Orderlies
Rating the services provided by Other (State the Others)
Rating the medical facilities
University of Trinidad and Tobago | Masters in Health Administration | May 2014
29

Rating the medical services provided
Visit to the DFMO private office, Hospitalized
(Visitdrhosp)
Have you ever been hospitalized?
If ‘Yes’ were you ever visited by the DFMO.
Have you ever visited any other DFMO outside of in their
Private Office?
If ‘Yes’ how were the services provided.
The theoretical framework, on which this research was based,
was the Primary Provider Theory (Aragon, 2003) and will focus
on the following principles:
Clinical competency is a necessary but insufficient
condition of desired outcomes.
Desired outcomes require more than clinical competency
alone, because the transmission of care and clinical
knowledge require effective communication and interaction
with patients.
Patient-centeredness is an underlying ability that
influences the quality of provider's interaction with and
transmission of care to patients.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
30

Providers' patient-centred influences the outcomes of
their patients.
Providers are uniquely responsible for the quality of the
transmission of their care and clinical knowledge to
patients.
Providers who are both clinically competent and patient-
centred are more likely to achieve desired outcomes.
Patients are the best judges of the patient-centeredness of
their providers that are captured in the four constructs to
patients’ expectations. Conceding that the primary provider
has the greatest clinical utility to patients, followed by
time spent waiting for the primary provider, and finally the
provider’s assistant. These principles highlight the need for
a high level of patient centeredness to achieve patient
satisfaction within the TTDF. These principles are:
Patients and families value the patient-centeredness of their
providers.
The patient-centeredness of the provider is more important
than the financial objectives of a patient encounter.
Much focus was not given to the financial aspect of the
provider patient relationship. The reason was that, in the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
31

TTDF there is no cost to the patient for medical services
provided in the TTDF and families are not seen personally in
camps or bases by the TTDF Medical Officer. Additionally
personnel can claim for any monies spent outside of the Force
for medical care sought. Questionnaires were administered and
collected at the major camps and bases of the TTDF. The
researcher and assistants visited the locations when it was
expected that the majority of personnel would be on location
such as:
After Padre Hour; as all Army camps conducts Padre Hour
on Wednesdays where all personnel who are not on leave or
duties are required to attend;
Similar to the Army the Air Guard also conduct Padre Hour
but on Tuesdays;
At Coast Guard during the changing of shift where there
would be maximum personnel on station;
Commanding Officer CG Inaugural Address to the personnel
at Staubles Bay;
For the Reserves during their monthly weekend training;
For Officers and Senior Non-commissioned Officers and
Senior Ratings to be administered at the respective Mess.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
32

The target population for the proposal is the TTDF that
comprises of four formations or units. The male to female
composition or ratio of the TTDF is 9:1 respectively. The
sampling size was selected using the Tables of Random Numbers,
Based on the current strength of the TTDF this figure was
three hundred and fifty-seven (357), of the enlisted personnel
from each formation in relation to the male to female ratio.
The sample size also sought to capture the years in service
and rank structure of the TTDF (see Appendix E).
Personnel excluded were those overseas on military duties or
training, and any recruits in training at the time of
administering the questionnaires. The reasons for these
exclusions were essentially due to accessibility and
availability of personnel overseas on military duties or
training to complete the questionnaire and have it returned in
a timely manner for analysing. The experiences of the recruit
in training are very limited or non-existence, as at the time
of training the only encounter in the medical department would
be that of their initial entry medical exam. Additionally
their responses may contain a high degree of respondent bias,
University of Trinidad and Tobago | Masters in Health Administration | May 2014
33

due to the recruits being instructed to complete the
questionnaire.
To accomplish this task for data collection a questionnaire
for satisfaction was designed and pre-tested before actual
use, using military personnel of the TTDF and non-military
personnel. The researcher reviewed the Defence Act-Chapter 14
of the Laws of Trinidad and Tobago; Standing Orders of the
Regiment; Coast Guard and Air Guard Regulations for documented
reference of standards. The questionnaire included questions
on patient’s satisfaction of the environment where service
provision occurred, the preliminary examinations and the
service offered by the Medical Doctor. Additionally the
questionnaire contained items related to the attitude of all
personnel working in the system.
The researcher and members of staff from the units’ medical
department administered the questionnaires to randomly
selected personnel. Persons were trained to administer the
questionnaire. Due to the uniqueness of the TTDF efforts were
made to capture a close as possible representation of the
composition of the Force, after which collecting the
questionnaires for analysis. The questionnaires after being
University of Trinidad and Tobago | Masters in Health Administration | May 2014
34

collected were secure in a secured draw at the researcher’s
office, which was located outside all military establishments.
Storage of the data was in a password protected file. After
one year, all hard copies of the questionnaires would be
shredded and properly disposed of. Personnel erroneously
placing his or her Regimental Number, Rank or Name on the
questionnaire were invited to complete another questionnaire
and destroy the void copy.
DATA COLLECTION
The questionnaire focused on the participants' level of
satisfaction with the medical services. At least twenty (20)
minutes was ideal for complete the questionnaire. The data
collected was categorized as general Satisfaction, Technical
Quality, Interpersonal Manner, Communication, and Time Spent
University of Trinidad and Tobago | Masters in Health Administration | May 2014
35

with Doctor, Accessibility and Convenience (see Appendix K).
An analysis of the quality of services from the perspective of
the participants happened in six (6) domains. These are
general satisfaction, technical quality, interpersonal
aspects, communication, time spent with the doctor and
personal spending for care or services. The responses were
designed according to Likert Five-point Scale of "strongly
agreed" (five points) to "strongly disagree" (one point).
Testing a similar questionnaire took place in Iran, and in
addition to validity, its reliability has been confirmed with
confidence coefficient of 90 percent (Ebrahimnia M. et. al,
2010).
University of Trinidad and Tobago | Masters in Health Administration | May 2014
36
DATA ANALYSIS
The data was collected using a sample size in Appendix E and
was statistically analysed using SPSS software. Frequency and
relative frequency of different levels of satisfaction were
calculated presented using frequency tables (See AppendixE).
In order to compare the levels of patients’ satisfaction with
different parts of medical services, in each part patients
were divided into two groups (satisfied and dissatisfied).
Dissatisfaction carried scores less than or equal to three,
and scores of four and greater as satisfaction with medical
services in general and in each of the studied parts. to use
the Using tests of significance and inferential statistics
such as Bivariate Correlations (Pearson product-moment
correlation coefficient) was used to test how strong the
relationship, direction of the relationship, measure of
association, and statistical significant of the relationship
(see Appendices F to I)
The Pearson product-moment correlation knew by its shorter
title of the Pearson correlation or Pearson's correlation test
University of Trinidad and Tobago | Masters in Health Administration | May 2014
37

for correlation between variables. This test produces a
coefficient called the Pearson correlation coefficient,
represented as r (that is, the italic lowercase letter r). It
measures the strength and direction of a linear relationship
between two continuous variables. Its values can range from a
positive one (+1) for a perfect positive linear relationship
to a negative one (-1) for a perfect negative linear
relationship. A value of zero (0) signifies no association
between two variables. In choosing Pearson's correlation to
analyse data, part of the process involves scrutinizing the
data to ensure that it can be analysed using Pearson's
correlation. This is accomplished if the data "passes" four
assumptions that are required for Pearson's correlation to
give a valid result, these assumptions are:
Assumption 1: At internal, or ratio level (that is, they
are continuous) the two variables should be measured.
Assumption 2: There needs to be a linear relationship
between the two variables. The best way is to visually
inspect a generated scatterplot.
Assumption 3: There should be no significant outliers as
Pearson's correlation coefficient, r, is sensitive to
University of Trinidad and Tobago | Masters in Health Administration | May 2014
38
outliers. Outliers can have an inflated power on the
value of r as this can lead to Pearson's correlation
efficient not having a value that best represents the
data as a whole.
Assumption 4: This is required for inferential statistics
(null hypothesis significance testing) and is also needed
to satisfy the assumption of bivariate normality.
To satisfy the assumptions before conducting the Pearson
product-moment correlation coefficient various preliminary
test were perform. These teats were Shapiro-Wilk's test (p>.05)
test for normality. A significant value < 0.05 violates the
assumption of normality (i.e., the test is significant at the
p < .05 level). A significant value > 0.05, indicates no
violation of the assumption of normality (i.e., p > .05)
because the Shapiro-Wilk test is testing the null hypothesis
that the data's distribution is equal to a normal
distribution. Rejecting the null hypothesis means that the
data's distribution is not equal to a normal distribution.
Other preliminary tests included visual examination of a
generated scatterplot to test for linearity. Testing and
University of Trinidad and Tobago | Masters in Health Administration | May 2014
39

adjusting for outliers which have the propensity to greatly
alter the results (LAERD 2014).
Interpreting the test of significance the properly stated
result would read: Because (test statistic) had a P-value of
(less than or greater than) 0.05; thus I can (reject or not
reject) the null hypothesis. However significance is not
synonymous with strength. Only a measure of association can
reveal the strength. Significance does not imply that the
relationship is meaningful. Significance does not mean the
relationship is not spurious (both variables are being
affected by a third unidentified variable).
The Mann-Whitney U test (also called the Wilcoxon-Mann-Whitney
test) is a rank-based nonparametric test that was used to
determine if there were differences between two groups on a
continuous or ordinal dependent variable.
In completing Mann-Whitney U test, the following four
assumptions were met. As indicated by LAERD (2013) the first
three relate to the choice of study design, whilst the fourth
reveals the nature of the data:
Assumption 1: There is one dependent variable that is
measured at the continuous or ordinal level.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
40

Assumption 2: There is one independent variable that
consists of two categorical, independent groups (i.e., a
dichotomous variable).
Assumption 3: There is independence of observations, that
is, that there is no association between the observations
in each group of the independent variable or between the
groups themselves. If the study fails this assumption,
another statistical test instead of the Mann-Whitney U
test (e.g., a Wilcoxon signed-rank test) must be use
Assumption 4: Make a determination whether the
distribution of scores for both groups of the independent
variable has the similar shape or a different shape.
Since this is a critical assumption of the Mann-Whitney U
test, and will affect interpretation the data generated.
A Kruskal-Wallis test was also performed determine statistical
differences. This test is the non-parametric alternative to
the one way ANOVA and is used to determine whether there are
any statistically significant differences between the
distributions of three or more independent (unrelated) groups.
A Kruskal-Wallis test is most often used for three types of
study design:
University of Trinidad and Tobago | Masters in Health Administration | May 2014
41

Determine if there are differences between three or more
independent groups
Determine if there are differences between conditions
(with no pre-test measurement taken)
Determine if there are differences in change scores
(LAERD, 2013)
LIMITATIONS
The limitations identified would be accessing personnel whom
may be randomly selected and are not available to administer
the questionnaire to them, as a consequence of these personnel
posted on duties or training overseas. A second limitation
would be personnel who may not have access medical care at the
time of administering the survey such as enlisted personnel of
the DFR who are not on the permanent staff or who by virtue of
their status access medical care privately.
A third limitation would be utilizing new recruits who may be
training at the time of administering the questionnaire. This
category of personnel would have had minimal experiences as it
relates to accessing the medical services. Additionally their
encounter would be very limited or non-existence, for, at the
University of Trinidad and Tobago | Masters in Health Administration | May 2014
42

time of training, the only encounter in the medical department
would be that of their initial entry medical exam.
As well as an increase in respondent bias due to the recruit
responding to an instructors command to complete the
questionnaire, where coercion and undue influence or pressure
from the instruction may affect the recruit’s response.
Some limitations to the statistical test are with the Shapiro-
Wilk test larger sample sizes (e.g., above 50 cases) can lead
to a statistically significant result (i.e., data are non-
normal) even when they are normal.
Outliers are a real problem for Pearson's correlation, which
is particularly susceptible to them. The problem results in
the value of Pearson's correlation coefficient being unduly
altered, exerting a negative influence on the value of the
correlation coefficient. As such, it is important to try to
identify outliers in your data.
STRENGTHS
Logistic regression is a very strong tool to control for
confounding in epidemiological research.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
43

ETHICAL CONSIDERATIONS
University of Trinidad and Tobago | Masters in Health Administration | May 2014
44
Approval to conduct the study was sought from The Chief of
Defence Staff (CDS) (see Appendix B). Subsequent to the CDS
approval Formation Commanders were communicated with, for
administering of the questionnaire (see Appendix C). Before
administering the questionnaire, participants were required to
give their written consent, after a full explanation of the
benefits and procedures was given. The Ministries of National
Security and Health was be informed of the CDS approval to
undertake the project.
Although the study undertaken was on patient satisfaction, and
the study tool used was a survey questionnaire, ethical issues
pertaining to the data collection was be addressed.
Consideration was given to confidentiality and anonymity of
patient or respondents (see Appendix D Consent Forms). All
due care was taken to protect the identity of all respondent
by not having any aspect of personnel identification place on
the form (such as personal address, identification number,
addresses – personal and email addresses, regimental number,
rank or name). Before the administering the questionnaire an
explanation on the conducting of and reason for, the process
was given to the respondents.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
45

All documents were secure by the investigator. Utmost
confidentiality was adhered to, for any Regimental Number,
Rank or Name inserted in error on a questionnaire. Whereby
the insertions were blotted off with black markers or given
back to the individual before it is assessed or destroyed in
their presence and then given the opportunity to re-do another
questionnaire. Using the landline the researcher was able to
complete interviews of a sensitive nature to avoid disclosure
of participant numbers. After tabulation of the data and
documented, all responses were disposed of via shredding and
incineration. The researcher stored all tabulated data in
encrypted files that required password access. Accessing
participants’ medical files or record did not occur during
this study.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
46

RESULTS
Characteristics of the Sample Demographic data
Table 1: Showing the Number of Valid Response for the
Demographics Data
Sex Age Marit
al
Statu
s
Educat
ion
Level
Insura
nce
Covera
ge
History
of
admissio
n to
Sick Bay
Years
of
milita
ry
servic
e
Catego
ry of
person
nel
Format
ion
N
Valid 239 240 237 235 235 224 239 240 229
Missi
ng11 10 13 15 15 26 11 10 21
Two hundred and fifty (250) personnel participated in the survey.
Table 2: Showing the Frequency of Sex
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
University of Trinidad and Tobago | Masters in Health Administration| May 2014
47

Valid
Male 198 79.2 82.8 82.8
Female 41 16.4 17.2 100.0
Total 239 95.6 100.0
MissingSystem 11 4.4
Total 250 100.0
A frequency analysis was run and the result indicated that there
was a total of 198 (82.8 %) male and 41 (17.2 %) female
respondents. .The sample conforms to the general composition of
the TTDF male female ratio of 90:10.
Table 3: Showing the Frequency of Age
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid 18-24 26 10.4 10.8 10.8
25-34 167 66.8 69.6 80.4
35-44 46 18.4 19.2 99.6
University of Trinidad and Tobago | Masters in Health Administration| May 2014
48

45 and
over1 .4 .4 100.0
Total 240 96.0 100.0
MissingSystem 10 4.0
Total 250 100.0
Conducting a frequency analysis the results showed that there was
one hundred and sixty-seven (167) respondents in the 25-34 age
groups representing 69.6 %; with 46 from the 25-44 age group that
representing 18.4%, 26 from the 18-24 age group that representing
10.8% and 1 from the 45 and over group representing 0.1%.
Table4: Showing the Frequency of Marital Status
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid Married 82 32.8 34.6 34.6
Single 146 58.4 61.6 96.2
University of Trinidad and Tobago | Masters in Health Administration| May 2014
49
Divorce 7 2.8 3.0 99.2
Separate
d1 .4 .4 99.6
Widowed 1 .4 .4 100.0
Total 237 94.8 100.0
MissingSystem 13 5.2
Total 250 100.0
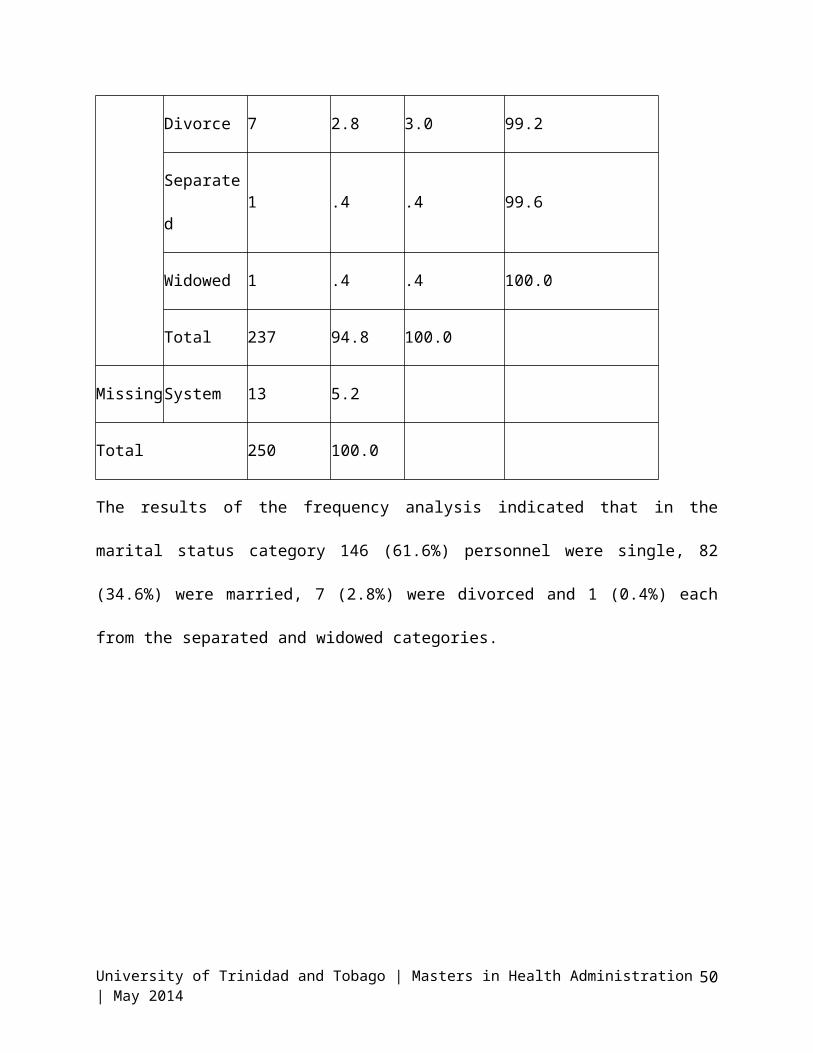
The results of the frequency analysis indicated that in the
marital status category 146 (61.6%) personnel were single, 82
(34.6%) were married, 7 (2.8%) were divorced and 1 (0.4%) each
from the separated and widowed categories.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
50
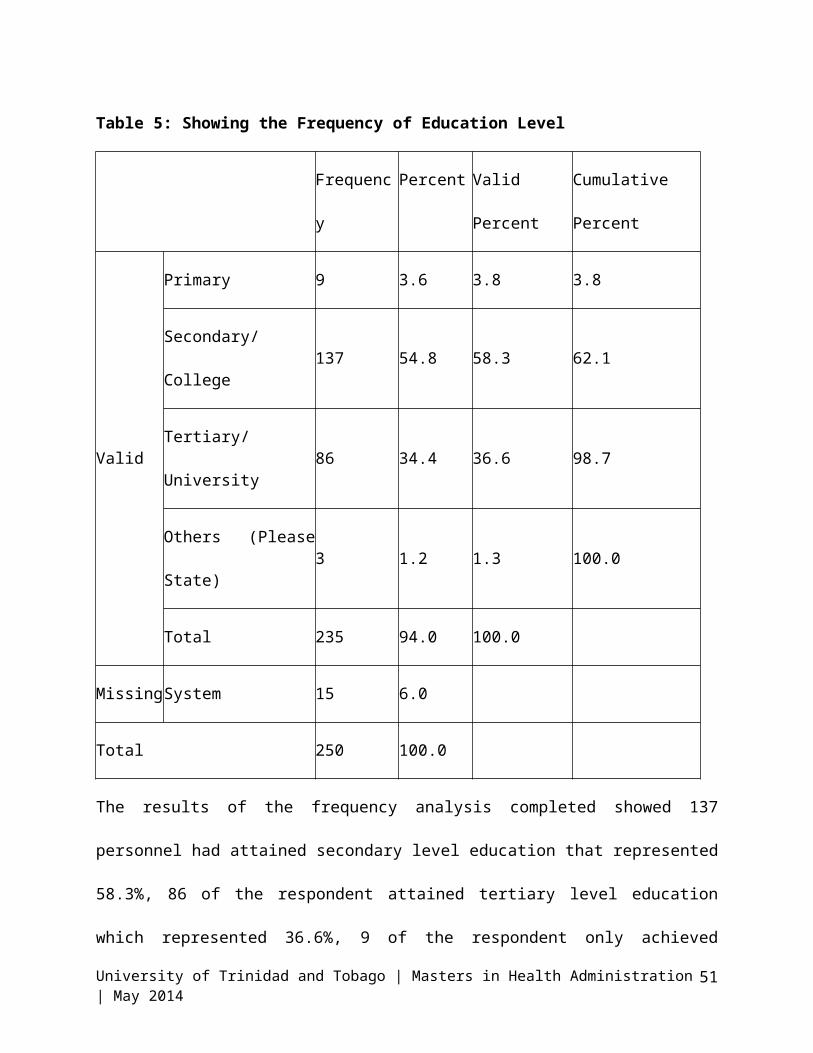
Table 5: Showing the Frequency of Education Level
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid
Primary 9 3.6 3.8 3.8
Secondary/
College137 54.8 58.3 62.1
Tertiary/
University86 34.4 36.6 98.7
Others (Please
State)3 1.2 1.3 100.0
Total 235 94.0 100.0
MissingSystem 15 6.0
Total 250 100.0
The results of the frequency analysis completed showed 137
personnel had attained secondary level education that represented
58.3%, 86 of the respondent attained tertiary level education
which represented 36.6%, 9 of the respondent only achieved
University of Trinidad and Tobago | Masters in Health Administration| May 2014
51

primary level education represented by 3.6% while 3 had achieved
other forms of education represented by 1.3%.
Table 6: Showing the Frequency of Insurance Coverage
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid
Yes 179 71.6 76.2 76.2
No 56 22.4 23.8 100.0
Total 235 94.0 100.0
MissingSystem 15 6.0
Total 250 100.0
The frequency analysis indicated that one hundred and seventy-
nine (179) respondents specified that they had some form of
University of Trinidad and Tobago | Masters in Health Administration| May 2014
52

insurance this represented 71.2%, and 56 specified that they had
no insurance coverage which represented 23.8%.
Table 7: Showing the Frequency of History of admission
to Sick Bay
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid
Yes 94 37.6 42.0 42.0
No 130 52.0 58.0 100.0
Total 224 89.6 100.0
University of Trinidad and Tobago | Masters in Health Administration| May 2014
53
MissingSystem 26 10.4
Total 250 100.0
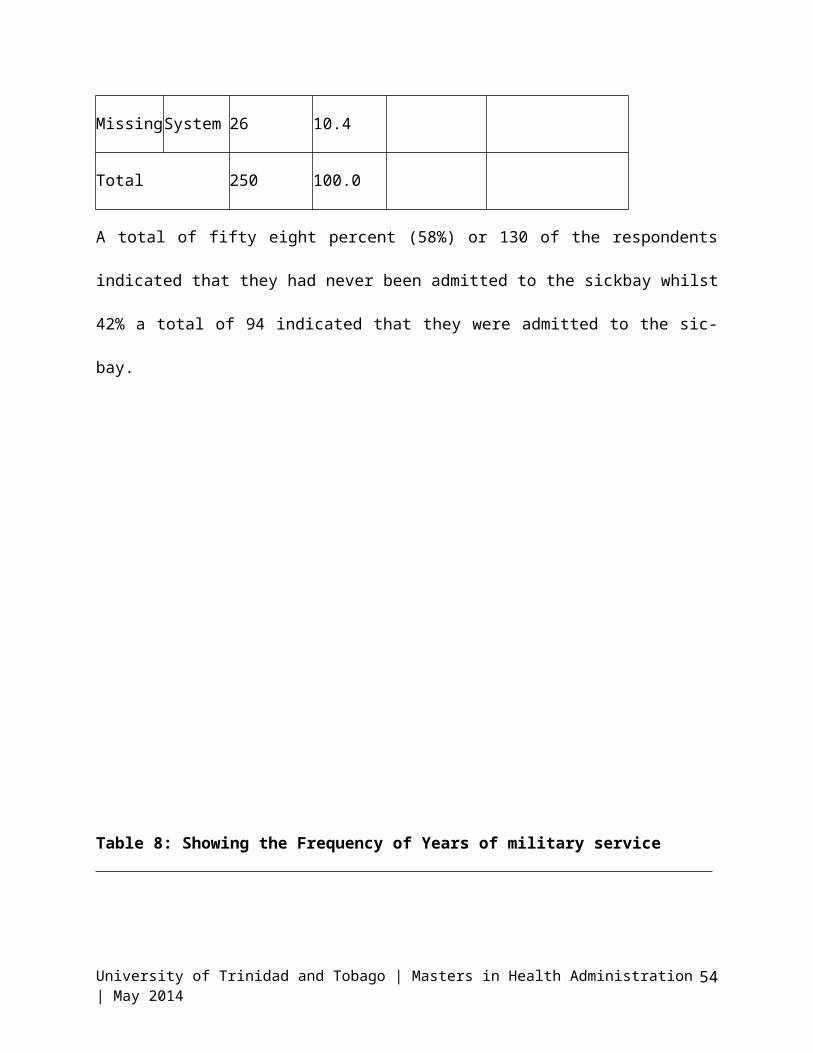
A total of fifty eight percent (58%) or 130 of the respondents
indicated that they had never been admitted to the sickbay whilst
42% a total of 94 indicated that they were admitted to the sic-
bay.
Table 8: Showing the Frequency of Years of military service
University of Trinidad and Tobago | Masters in Health Administration| May 2014
54

Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid
Less than 6
years78 31.2 32.6 32.6
7 to 12 years 118 47.2 49.4 82.0
Over 12 years 42 16.8 17.6 99.6
4.00 1 .4 .4 100.0
Total 239 95.6 100.0
MissingSystem 11 4.4
Total 250 100.0
A frequency analysis was completed on years of military service
the results showed that 118 (49.4%) had served 7 to 12 years, 78
(32.6) less than 6years and 42 (17.6%0 over 12 years.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
55

Table 9: Showing the Frequency of Category of personnel
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid Commissioned
Officer9 3.6 3.8 3.8
Warrant Officer 3 1.2 1.3 5.0
Senior Non-
commissioned
Officer or Senior
Ratings
17 6.8 7.1 12.1
Junior Non-
commissioned
Officer or Junior
Ratings
125 50.0 52.1 64.2
University of Trinidad and Tobago | Masters in Health Administration| May 2014
56

Other Ranks or
Ratings86 34.4 35.8 100.0
Total 240 96.0 100.0
MissingSystem 10 4.0
Total 250 100.0
In the frequency analysis of category of personnel, 9 (3.8%)
respondents were Commissioned Officers, 3 (1.3%) were Warrant
Officer, 17 (7.1%) were Senior Non-commissioned Officer or Senior
Ratings, 125 (52.1%) Junior Non-commissioned Officer or Junior
Ratings and 86 (35.8%) were Other Ranks or Ratings.
Table 10: Showing the Frequency of Formations
Frequenc
y
Percent Valid
Percent
Cumulative
Percent
Valid TTR 166 66.4 72.5 72.5
CG 47 18.8 20.5 93.0
University of Trinidad and Tobago | Masters in Health Administration| May 2014
57

TTAG 13 5.2 5.7 98.7
DFR 3 1.2 1.3 100.0
Total 229 91.6 100.0
MissingSystem 21 8.4
Total 250 100.0
A total of 166 respondent, represent 72.5% were from the Trinidad
and Tobago Regiment, 47 (18.8%) were from the Coast Guard, 13
(5.7%) were from the Air Guard and 3 (1.3%) were from the Defence
Force Reserves.
Levels of Satisfaction
University of Trinidad and Tobago | Masters in Health Administration| May 2014
58

Table 11: Showing the Number of Valid Response for the General
Satisfaction (GSAT) Variables
I am
very
satisfi
ed with
the
medical
service
s I
receive
d
The
medical
care I
have
been
receivi
ng is
just
perfect
There
are
things
about
the
medical
system
where I
receive
my care
from
that
need to
be
improve
d.
There
are
some
things
about
the
medical
care
that I
receive
d that
could
be
better.
All
things
conside
red the
medical
care I
receive
d is
excelle
nt.
I am
dissati
sfied
with
some
things
about
the
medical
care I
receive
d.
N Valid 241 241 242 238 234 235
University of Trinidad and Tobago | Masters in Health Administration| May 2014
59

Missi
ng
9 9 8 12 16 15
Table 12: Frequency Of General Satisfaction (GSAT) Theme (%)
Disagre
e
Uncerta
in
Agree
I am very satisfied with the medical
services I received (GSAT1)
115
(47.7)
48(19.9
)
78
(32.3)
The medical care I have been
receiving is just perfect (GSAT2)
141(58.
5)
58(24.1
)
42(17.5
)
There are things about the medical
system where I receive my care from
that need to be improved. (GSAT3)
9(3.8) 18(7.4) 215(88.
9)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
60

There are some things about the
medical care that I received that
could be better. (GSAT4)
5(2.1) 12 (5) 221
(92.9)
All things considered the medical
care I received is excellent.
(GSAT5)
142(60.
6)
53
(22.6)
39
(16.6)
I am dissatisfied with some things
about the medical care I received.
(GSAT6)
23(9.8) 25
(10.6)
187
(79.6)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
61

0.00%
20.00%
40.00%
60.00%
80.00%
100.00%Chart 1: Frequency Of General Satisfaction(GSAT) Theme
Disagree
Total number of respondents who agree = 585
Total number of respondent who strongly agree = 435
Total of respondents = 585 + 435 = 1020
Average percentage of respondents that agree = (1020/585) x 20 =
34.87 percent
Average percentage of respondents that disagree = (1020/435) x 20
= 46.90 percent
University of Trinidad and Tobago | Masters in Health Administration| May 2014
62
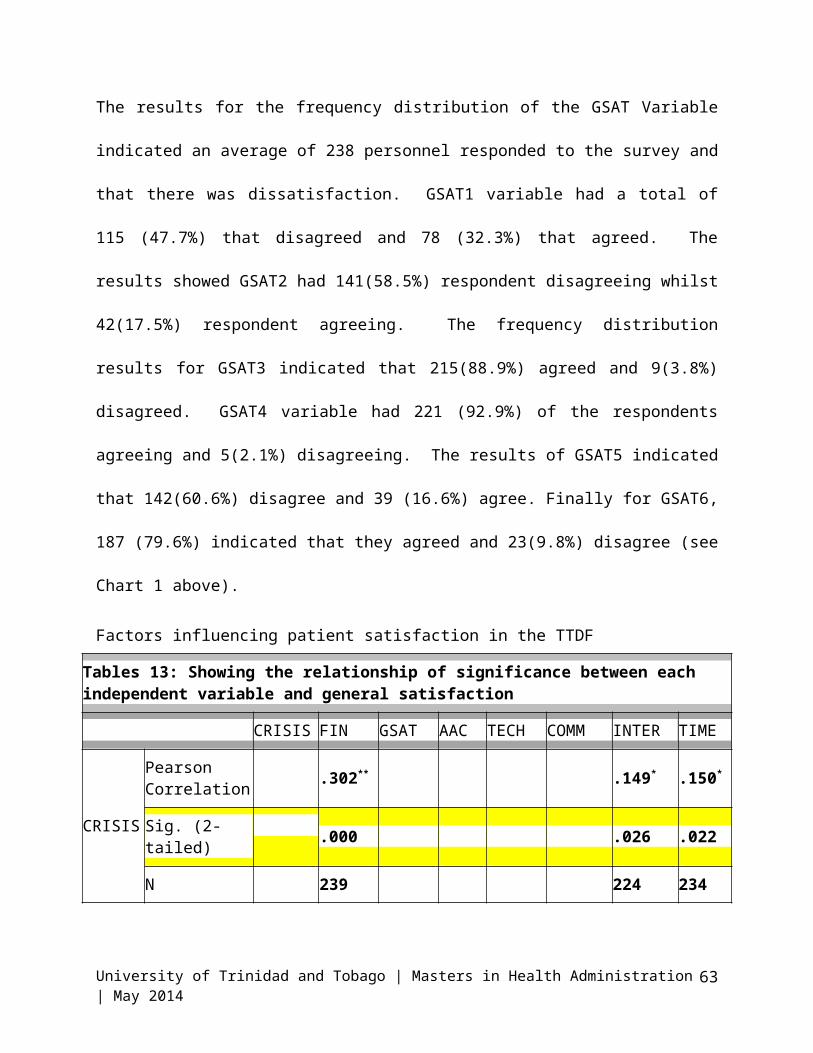
The results for the frequency distribution of the GSAT Variable
indicated an average of 238 personnel responded to the survey and
that there was dissatisfaction. GSAT1 variable had a total of
115 (47.7%) that disagreed and 78 (32.3%) that agreed. The
results showed GSAT2 had 141(58.5%) respondent disagreeing whilst
42(17.5%) respondent agreeing. The frequency distribution
results for GSAT3 indicated that 215(88.9%) agreed and 9(3.8%)
disagreed. GSAT4 variable had 221 (92.9%) of the respondents
agreeing and 5(2.1%) disagreeing. The results of GSAT5 indicated
that 142(60.6%) disagree and 39 (16.6%) agree. Finally for GSAT6,
187 (79.6%) indicated that they agreed and 23(9.8%) disagree (see
Chart 1 above).
Factors influencing patient satisfaction in the TTDF
Tables 13: Showing the relationship of significance between each independent variable and general satisfaction
CRISIS FIN GSAT AAC TECH COMM INTER TIME
CRISIS
Pearson Correlation .302** .149* .150*
Sig. (2-tailed) .000 .026 .022
N 239 224 234
University of Trinidad and Tobago | Masters in Health Administration| May 2014
63

FIN
Pearson Correlation .302
** .134* .274** .184**
Sig. (2-tailed) .000 .043 .000 .005
N 239 228 224 233
GSAT
Pearson Correlation
.426*
* .207** .294** .180** .191**
Sig. (2-tailed) .000 .002 .000 .008 .004
N 216 222 221 216 225
AAC
Pearson Correlation .426** .305** .235** .229** .211**
Sig. (2-tailed) .000 .000 .000 .001 .002
N 216 220 220 215 224
TECH
Pearson Correlation .134* .207** .305*
* .205** .332** .207**
Sig. (2-tailed) .043 .002 .000 .002 .000 .002
N 228 222 220 225 220 229
COMM
Pearson Correlation .294** .235*
* .205** .188** .268**
Sig. (2-tailed) .000 .000 .002 .005 .000
N 221 220 225 221 230
INTER Pearson Correlation
.149* .274** .180** .229*
*.332** .188** .219**
University of Trinidad and Tobago | Masters in Health Administration| May 2014
64

Sig. (2-tailed) .026 .000 .008 .001 .000 .005 .001
N 224 224 216 215 220 221 224
TIME
Pearson Correlation .150
* .184** .191** .211*
* .207** .268** .219**
Sig. (2-tailed) .022 .005 .004 .002 .002 .000 .001
N 234 233 225 224 229 230 224
A Pearson product-moment correlation coefficient was computed to
assess the relationship between General Satisfaction, the
(Dependent Variables) and Timing (Independent Variables) of
personnel of the Trinidad and Tobago Defence Force (TTDF).
Preliminary analyses showed the relationship to be linear with
both variables normally distributed, as assessed by Shaprio-
Wilktest (p> .05). There was a positive correlation between the
two variables, r = .191, n = 225, p < 0.004, with general
satisfaction explaining 3.65% (r2 = .0365) variation in the
timing. Overall, there was a correlation between General
Satisfaction and Timing. Increases in the general satisfaction
were correlated with increases in timing. We reject the null
hypothesis but fail to reject the alternative hypothesis.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
65
A Pearson product-moment correlation coefficient was run to
assess the relationship between General Satisfaction and
Communication of personnel of the TTDF. Preliminary results
showed the relationship to be linear with both variables normally
distributed, as assessed by Shaprio-Wilk test (p> .05). There
was a positive correlation between the two variables, r = .294, n
= 221, p < 0.000, with Communication explaining 8.64% (r2 =
0.0864) of the variation in general satisfaction. Overall, there
was a positive correlation between General Satisfaction composite
Variable (Dependent Variables) and Timing Composite Variable.
Increases in the General Satisfaction were correlated with
increases in Communication. Thus we can reject the null
hypothesis and fail to reject the alternative hypothesis.
A Pearson product-moment correlation coefficient was computed to
assess the relationship between General Satisfaction and
Technical Ability of personnel of the TTDF. Preliminary analyses
showed the relationship to be linear with both variables normally
distributed, as assessed by Shaprio-Wilk test (p> .05). There
was a positive correlation between the two variables, r = .207, n
University of Trinidad and Tobago | Masters in Health Administration| May 2014
66
= 222, p = 0.002, with Technical Ability explaining 4.28% (r2 =
0.0428) of the variation in General Satisfaction. We can reject
the null hypothesis and accept the alternative hypothesis
A Pearson product-moment correlation coefficient was computed to
assess the relationship between General Satisfaction and
Access/Availability/Convenience (AAC). There was a moderate
positive correlation between the two variables, r = .426, n =
216, p < 0.000, with AAC Variables explaining 18.15% (r2 =
0.1815). We can reject the null hypothesis and accept the
alternative hypothesis.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
67

Tables 14: Showing the relationship of insignificance between each independent variableand general satisfaction
CRISIS
DEMO FIN GSAT AAC TECH COMM INTER TIME Visitdrhos
p
Ratings
CRISIS
Pearson Correlation 1 -.124 .053 -.00
5 .066 .014
Sig. (2-tailed) .086 .432 .935 .319 .832
N 240 191 225 224 229 232
DEMO
Pearson Correlation -.124 1 .041 .068 -.04
5 .006 -.017 -.044 -.051
Sig. (2-tailed) .086 .573 .366 .545 .937 .813 .557 .489
N 191 193 191 181 181 183 186 181 188
FIN
Pearson Correlation .041 1 .111 .071 .090
Sig. (2-tailed) .573 .098 .288 .174
N 191 239 224 224 231
GSAT
Pearson Correlation .053 .068 .111 1
Sig. (2-tailed) .432 .366 .098
N 225 181 224 225AAC Pearson
Correlation-.005 -.045 .071
University of Trinidad and Tobago | Masters in Health Administration | May 2014 68

Sig. (2-tailed) .935 .545 .288
N 224 181 224
TECH
Pearson Correlation .066 .006
Sig. (2-tailed) .319 .937
N 229 183
COMM
Pearson Correlation .014 -.017 .090
Sig. (2-tailed) .832 .813 .174
N 232 186 231
INTER
Pearson Correlation -.044
Sig. (2-tailed) .557
N 181
TIME
Pearson Correlation -.051
Sig. (2-tailed) .489 .005 .004 .002 .002 .000 .001
N 188 233 225 224 229 230 224 234
Visitdrhosp
Pearson Correlation -.227 -.262 -.208 -.074 .004 -.055 .065 .141 .324 1 -.660
Sig. (2-tailed) .189 .227 .232 .682 .984 .754 .715 .434 .058 .154
N 35 23 35 33 33 35 34 33 35 35 6
University of Trinidad and Tobago | Masters in Health Administration | May 2014 69

Ratings
Pearson Correlation -.094 .156 -.043 .211 .235 -.095 .135 -.076 -.00
4 -.660 1
Sig. (2-tailed) .620 .489 .822 .273 .212 .622 .477 .689 .983 .154
N 30 22 30 29 30 29 30 30 30 6 30**. Correlation is significant at the 0.01 level (2-tailed).*. Correlation is significant at the 0.05 level (2-tailed).
University of Trinidad and Tobago | Masters in Health Administration | May 2014 70

A Pearson product-moment correlation coefficient was run to
assess the relationship between General Satisfaction composite
variable and Independent composite variables (Hospitalization
and Visit to the DFMO private office) of personnel of TTDF.
Preliminary analyses showed the relationship to be linear with
both variables normally distributed, as assessed by Shaprio-
Wilk test (p = .05). However there was no correlation between
the two variables, r = -.660, n = 6, p =0.154. There was no
statistically significant relationship between General
Satisfaction composite variables (Dependent Variable) and
Hospitalization and Visit to the DFMO private office variables
(Independent Variable), so we cannot reject the null
hypothesis.
A Pearson product-moment correlation coefficient was run to
assess the relationship between General Satisfaction and
Demographic Variable of personnel of TTDF. Preliminary
analyses showed the relationship to be linear with both
variables normally distributed, as assessed by Shaprio-Wilk
test (p = .05). However there was no significant correlation
between the two variables, r = .068, n = 181, p = 0.366.

Chart 1: Showing results of Mann-Whitney Test of Sex
A Mann-Whitney Test was run for Sex and the results showed
that p=.004 which is below the significance level of .05,
indicating that the Null Hypothesis should be rejected.
Chart 2: Showing results of Kruskall Wallis Test of History of
admission to Sick
University of Trinidad and Tobago | Masters in Health Administration | May 2014
72

A Kruskal-Wallis Test was run for the Demographic variable
(Age) and the results showed that p=.000 which is below the
significance level of .05, indicating that the Null Hypothesis
should be rejected.
Chart 3: Showing results of Kruskall Wallis Test of Education
Levels
A Kruskal-Wallis Test was run for the Demographic variable
(Education Level) and the results showed that p=.000 which is
below the significance level of .05, indicating that the Null
Hypothesis should be rejected.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
73

Chart 4: Showing results of Kruskall Wallis Test for Insurance
Coverage
A Kruskal-Wallis Test was completed for the Demographic
variable (Insurance Coverage) and the results showed that
p=.000 which is below the significance level of .05,
indicating that the Null Hypothesis should be rejected.
Chart 5: Showing results of Kruskall Wallis Test of Marital
Status
University of Trinidad and Tobago | Masters in Health Administration | May 2014
74

A Kruskal-Wallis Test was run for the Demographic variable
(Marital Status) and the results showed that p=.001 which is
below the significance level of .05, indicating that the Null
Hypothesis should be rejected.
Chart 6: Showing results of Kruskall Wallis Test of Categoryof Personnel
A Kruskal-Wallis Test was completed for the Demographic
variable (Category of Personnel) and the results showed that
p=.000 which is below the significance level of .05,
indicating that the Null Hypothesis should be rejected.
Chart 7: Showing results of Kruskall Wallis Test of Formation
University of Trinidad and Tobago | Masters in Health Administration | May 2014
75

A Kruskal-Wallis Test was completed for the Demographic
variable (Formation) and the results showed that p=.027 which
is below the significance level of .05, indicating that the
Null Hypothesis should be rejected.
Chart 8: Showing results of Kruskall Wallis Test of Age
University of Trinidad and Tobago | Masters in Health Administration | May 2014
76

A Kruskal-Wallis Test was completed for the Demographic
variable (Age) and the results showed that p=.000 which is
below the significance level of .05, indicating that the Null
Hypothesis should be rejected.
Table 15: Ranks (Mann-Whitney Test) between GAST and History
of admission to the sick bay
History of admission to Sick Bay N
Mean
Rank
Sum of
Ranks
GenSatisfac
tion
Yes 87 107.11 9319.00
No 121 102.62 12417.00
Total 208
Test Statisticsa
GenSatisfaction
Mann-
Whitney U
5036.000
Wilcoxon W 12417.000
Z -.537
Asymp. Sig.
(2-tailed)
.591
a. Grouping Variable: History of University of Trinidad and Tobago | Masters in Health Administration | May 2014
77
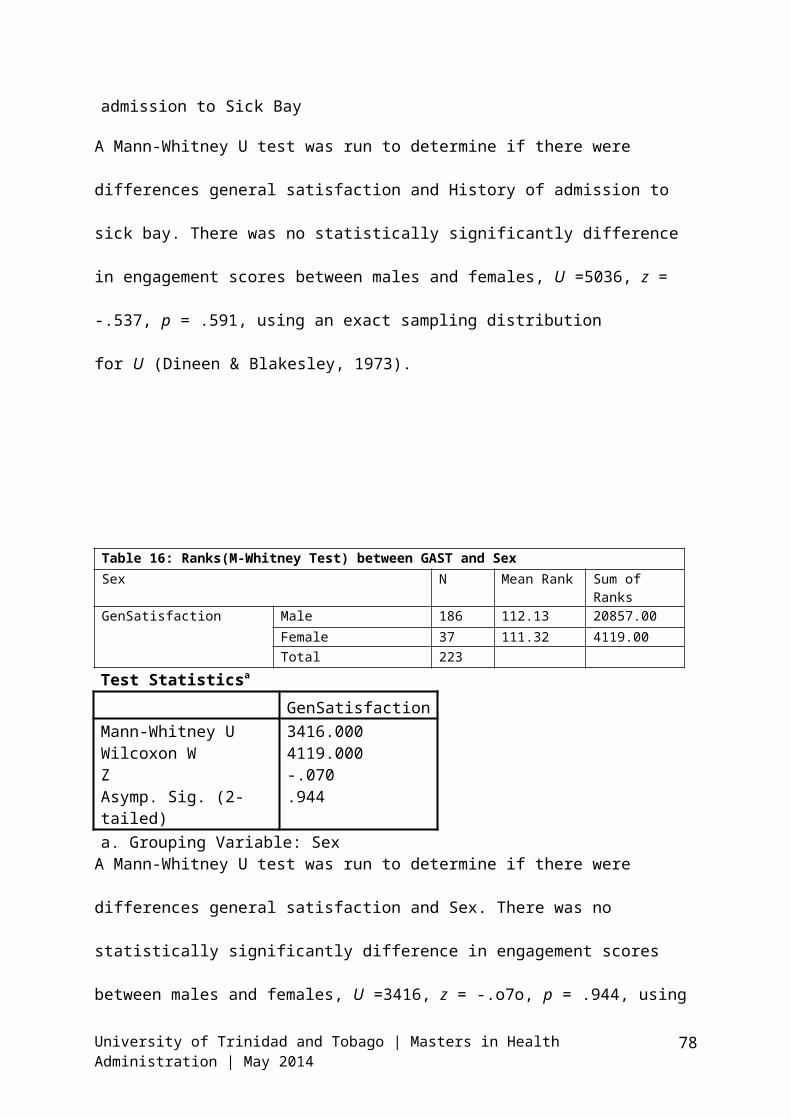
admission to Sick Bay
A Mann-Whitney U test was run to determine if there were
differences general satisfaction and History of admission to
sick bay. There was no statistically significantly difference
in engagement scores between males and females, U =5036, z =
-.537, p = .591, using an exact sampling distribution
for U (Dineen & Blakesley, 1973).
Table 16: Ranks(M-Whitney Test) between GAST and SexSex N Mean Rank Sum of
RanksGenSatisfaction Male 186 112.13 20857.00
Female 37 111.32 4119.00Total 223
Test Statisticsa
GenSatisfactionMann-Whitney U 3416.000Wilcoxon W 4119.000Z -.070Asymp. Sig. (2-tailed)
.944
a. Grouping Variable: SexA Mann-Whitney U test was run to determine if there were
differences general satisfaction and Sex. There was no
statistically significantly difference in engagement scores
between males and females, U =3416, z = -.o7o, p = .944, using
University of Trinidad and Tobago | Masters in Health Administration | May 2014
78
an exact sampling distribution for U (Dineen & Blakesley,
1973).
DISCUSSION
A total of 250 personnel participated in the survey with 198
male respondent and 41 female respondents. .The sample
comprised 82.8 percent male and 17.2 percent female conforming
to the general composition of the TTDF male female ratio of
90:10. One hundred and sixty-seven (167) of the respondents
were in the 25-34 age groups representing 69.6 %; with 46 from
the 25-44 age group that represents 18.4%, 26 from the 18-24
age group that represents 10.8% and 1 from the 45 and over
group a percentage of 0.1.
In the marital status category 146 (61.6%) personnel were
single, 82 (34.6%) were married, 7 (2.8%) were divorced and 1
(0.4%) each from the separated and widowed categories. A
total of 137 personnel had attained secondary level education
that represented 58.3%, 86 of the respondent attained tertiary
level education which represented 36.6%, 9 of the respondent
only achieved primary level education a3.6% while 3 had
University of Trinidad and Tobago | Masters in Health Administration | May 2014
79

achieved other forms of education represented by 1.3%. One
hundred and seventy-nine (179) respondents indicated that they
had some form of insurance this represented 71.2%, and 56
indicated that they had no insurance coverage which
represented 23.8%.
Fifty eight percent (58%) or 130 of the respondents indicated
that they had never been admitted to the sickbay and 42% a
total of 94 indicated that they were admitted to the sic-bay.
On the subject of the years of military service the results
showed that 118 (49.4%) had served7 to 12 years, 78 (32.6)
less than 6years and 42 (17.6%0 over 12 years. In the
category of personnel 9 respondents that represented 3.8% were
Commissioned Officers, 3 (1.3%) were Warrant Officer, 17
(7.1%) were Senior Non-commissioned Officer or Senior Ratings,
125 (52.1%)Junior Non-commissioned Officer or Junior Ratings
and 86 (35.8%)Other Ranks or Ratings. A total of 166
respondent, represent 72.5% were from the Trinidad and Tobago
Regiment, 47 (18.8%) from the Coast Guard, 13 (5.7%) from the
Air Guard and 3 (1.3%) from the Defence Force Reserves.
The results for the frequency distribution of the General
Satifaction (GSAT) Variable indicated an average of 238
University of Trinidad and Tobago | Masters in Health Administration | May 2014
80

personnel responded to the survey and showed a level
dissatisfaction. A total of 47.7% indicateddissatisfied with
the medical services I received. The results showed 58.5%
respondent disagreeing with the medical care is just perfect.
The frequency distribution results for GSAT3 (There are things
about the medical system that need to be improved) indicated
that 88.9% agreed. There are some things about the medical
care that could be better variable had 92.9% of the
respondents agreeing. The results indicated that 60.6%
disagree that the medical was excellent. Finally 79.6%
indicated dissatisfaction with some things about the medical
care.
This result was validated by the level of satisfaction of
46.90 percent. Further investigation would be necessary to
determine what are the root causeds for these results.
A Pearson product-moment correlation coefficient was computed
to assess the relationship between General Satisfaction, the
(Dependent Variables) and the Independent Variables of
personnel of the Trinidad and Tobago Defence Force (TTDF).
Preliminary analyses showed the relationship to be linear with
both variables normally distributed, as assessed by Shaprio-
University of Trinidad and Tobago | Masters in Health Administration | May 2014
81

Wilktest (p> .05). Overall, there was a correlation between
General Satisfaction (Dependant Variable) and the Independent
Variables - AAC, TECH, COMM, INTER and TIME.
Increases in the general satisfaction were correlated with
increases AAC, TECH, COMM, INTER and TIME variables. We reject
the null hypothesis but fail to reject the alternative
hypothesis for these variables.
A Pearson product-moment correlation coefficient was run to
assess the relationship between General Satisfaction composite
variable and Independent composite variables (Hospitalization
and Visit to the DFMO private office) of personnel of
TTDF,Demographic Variable of personnel of TTDF,Interpersonal
relationships,Ratings in the health care in TTDF of personnel
of TTDF0. Preliminary analyses showed the relationship to be
linear with both variables normally distributed, as assessed
by Shaprio-Wilk test (p = .05). However there was no
correlation between the Dependent variables and Independent
variables of: Hospitalization and Visit to the DFMO private
office) of personnel of TTDF,Demographic Variable of personnel
of TTDF,Interpersonal relationships, andRatings in the health
care in TTDF. There was no statistically significant
University of Trinidad and Tobago | Masters in Health Administration | May 2014
82

relationship between General Satisfaction composite variables
(Dependent Variable) and these Independentvariables, so we
cannot reject the null hypothesis.
Analysis of variance (ANOVA) is a statistical analysis tool
used to analyse the differences between group means and their
associated procedures (such as-variation among and between
groups. The results of the Anova test run between General
Satisfaction and the following Demographic Variables
(Formation, Category of personnel, Years of military service,
History of admission to sick bay, Education, Age and Sex)
indicated that there was no significance difference between
these Demographic Variables and general satisfaction with p-
values higher than the acceptance level of .05. This is an
indication that these variables does not make a difference in
the level of patients’ satisfaction of the medical services
offered in the TTDF.
However, the results of the Anova tests indicated that there
was significance difference between Demographic Variables
(Insurance coverage and Marital Status) and General
Satisfaction with p-values lower than the acceptance level
of .05 (.038 and .047 respectively) This is an indication that
University of Trinidad and Tobago | Masters in Health Administration | May 2014
83

these may make a difference in the level of patients’
satisfaction of the medical services offered in the TTDF.
The Jewish General Hospital (2014) asserted that a patients’
satisfaction rate of 80% indicates that the intuition did a
good job. Though achieving 100% may not be practical however
intuition should endeavour to reach a satisfaction level of
95%. Carl R. Darnall Army Medical Center (CRDAMC, 2013)
administration point out that the object for patient
satisfaction was to achieve and maintain 95 percent or greater
overall satisfaction rate. In this research, the results
showed that the average rate of satisfaction by respondents
equalled 46.90% in contrast to international standards of 95%.
The reasons for the level of dissatisfaction can be attributed
to the services provided as indicated by the result. One area
that the respondents indicated that needed to be address is
the waiting time, as 25% indicated that the waiting time to
see the DFMO was too long. A frequency analysis was run and
the results indicated for that those who provide health care
sometimes hurry too much when they treat shown by a 70.7%
result. The time taken for medical assessment by DFMO was too
University of Trinidad and Tobago | Masters in Health Administration | May 2014
84

short as indicated by 74%. Additionally 80.4% indicated that
heir was a crisis in the medical services in the TTDF.
Other factors that can contribute to the low rate ofsatisfactions are:
The interpersonal aspect of care received a poor rating
by the personnel.
A total of 56.8% of respondents indicated that they were
ignored by the DFMO during their medical assessment.
It is difficult to get medical care at short notice.
Seventy seven percent indicated that more attention
should be paid to the personnel’s privacy.
Sixty six percent indicated that waiting time was too
long.
A total of 56.8% indicated that the DFMO does not explain
medical terms when they are used.
Sixty three percent indicated that the DFMO should give
personnel more respect.
Doctors act too business like and impersonal towards
personnel had a score of 46.4%.
A total of 90% of persons who were hospitalized indicated
that they were not visited by the DFMO who is required to
University of Trinidad and Tobago | Masters in Health Administration | May 2014
85

visit personnel at the hospital when they are
hospitalized.
The results showed that 70.7% indicated that providers
hurry too much in their treatment processes. While 73.9%
indicated that the DFMO does not spent sufficient time in
the assessment of personnel. Sixty seven percent
indicated that they have to spend more on medical care,
even though all services should be provided directly by
the DFMO or via referrals.
The Primary Provider Theory was supported by the results in
conducting of this research. This Theory hierarchically
relates its satisfaction constructs to patients expectations,
conceding that the primary provider has the greatest clinical
utility to patients, followed by time spent waiting for the
primary provider, and finally the provider’s assistant. As
the expectations were not greatly met the provider who has
the greatest clinical utility to the patients negatively
affected as patients were ignored by the DFMO the
interpersonal aspect were poorly rated and the time spent in
assessment was low including a long waiting time to see the
DFMO.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
86
The Primary Provider Theory is a generalized theory of how the
patient-centeredness of health providers has an effect on the
patient’s care behaviour, during patient encounters and
related outcomes. The Theory holds that outcomes such as
satisfaction, trust, ratings of quality and various clinical
outcomes were fundamentally rooted in the patient’s
relationship with their primary provider. The results of the
study showed that the personnel did not have sound
relationship with the primary provider.
The usefulness of the theory and its relevance in the study
was critical as it directed the researcher to focus on the
factors that influences patient’s satisfaction. Additionally
to help determine what measures can be instituted to assist
with improvement to the health care system. It also
highlighted the fact that patients’ views can and should be
taken into consideration, to be used as drivers to better and
more effective and efficient service provision.
The greatest challenge encountered throughout the research was
ethical approval, and subsequent dissemination of the approval
to Formation Commanders. The processes used to overcome this
challenge were to constantly enquire and follow-up the stages
University of Trinidad and Tobago | Masters in Health Administration | May 2014
87

of approval. Additionally liaising with and seeking the
approval of Unit Commanders in lieu of the CDS’s approval to
administer the questionnaire. Determining the ideal time when
maximum amount of personnel were in the camps or on bases.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
88

CONCLUSION AND RECOMMENDATIONS
The research question “What is the level of patient
satisfaction within the TTDF and what are the factors that
influence it?” was answered in the study. The study concluded
that patients’ satisfaction of the medical services offered in
the TTDF was 46.9percent which was below the international
standards of 95 percent. The theory coincided with the
methodology of using a PSQ and having a predominantly
quantitative method. Even though a principally qualitative
approach could have also suited the research and focus group
discussion and interviews may well have been utilized.
The results showed that personnel indicated that there was a
crisis in the medical services new questions that can be
researched are:
What is the root cause/s of the crisis and the
implication/s if not adequately addressed?
To what extent are the current policies for medical
service provision meeting for the current needs of the
TTDF?
University of Trinidad and Tobago | Masters in Health Administration | May 2014
89

To what extent are the providers not meeting the
expectation of the recipients of the medical services
provided?
What are best practices for medical innovation in the MIR
that creates higher patient satisfaction?
The extent of the objectives was met as the main objective of
the study to determine the level of patient satisfaction in
TTDF was determined by the satisfaction rate of 46.8%.
Personnel were not satisfied overall with the health care
services offered. Additionally identifying some critical
areas of dissatisfaction, which need to be dealt with over
time to improve the satisfaction levels.
RECOMMENDATIONS
Recommendations were developed that could be used to enhance
the health care services.Further to the results recommendation
that can be used to improve the overall satisfaction level
are:
Construct a process flow the medical inspection room to
determine where the time waiting can be identified. Once
completed determine if the time can be reduced to improve
the flow for patients, if time cannot be reduced what
University of Trinidad and Tobago | Masters in Health Administration | May 2014
90
successful and established activities can be introduced
that can occupy the attention of the patient and reduce
the negative impact off waiting for long
periods.Reviewing of the policies which govern the
provision of medical services to determine adequacy,
relevance and currency to personnel medical needs.
Institute a mandatory patients’ satisfaction survey to
help determine the extent of success or failure of the
medical system and services. Take satisfaction scores
seriously as in many jurisdictions this is mandatory
Institute a monitoring and evaluation mechanism to assist
with the on-going evaluation of the medical services,
providers and facilities using key performance
indicators.
Establish a sense of trust between provider and patient.
Make sure that patient feels respected, comfortable and
valued. This may require some form of training in
customer relationship and medical skills via continuous
professional development.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
91

Ensure that staff is motivated to provide quality care
service, while embracing changes that may occur over
time.
Key to patient satisfaction is checking out the patients’
complaints to determine validity and help drive the
process for quality care. Additionally uncovering
patients’ actual needs.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
92

REFERENCES:
Aragon, S, .J. (2003). A Patient Satisfaction Theory and its
Robustness Across Gender in Emergency Department: A
Multigroup Structural Equation Modelling Investigation.
American Journal of Medical Quality, vol 18 No 16, Nov/Dec 2003.
Boudreau L. A., Busse J. W. & McBride G., (2006) Chiropractic
Services in the Canadian Armed Forces: A Pilot Project, Military Medicine
2006 (Jun); 171 (6): 572–576.
Campbell, S. M.; Braspenning, J.; Hutchinson, A. & Marshall,
M. (2002) Quality indicators in primary care Research methods used in
developing and applying.Qual. Saf. Health Care 2002; 11;358-364
University of Trinidad and Tobago | Masters in Health Administration | May 2014
93

Carman, J.M. (2000), “Patient perceptions of service quality:
Combining the dimensions”, Journal of Services Marketing, vol.14,
no. 4, pp. 337-352.
Col Brisebois, R., MajHennecke, P., Capt(Naval) Kao, R., Maj
McAlister, V., Lt Col Po, J., Lt Col Stiegelmar, R., & Col
Tien, H. - For the Canadian Forces Health Services Research
Consortium, (2011) The Role 3 Multinational Medical Unit at
Kandahar Airfield 2005–2010: Canadian Journal of Surgery 2011;
54(6S):S124-S129 and J Can Chir, Vol. 54, Suppl.
Donabedian, A. (1998), “The quality of care. How can it be
assessed?”, Journal of American Medical Association, vol. 260, no.
12, pp. 1743-1748.
Ebrahimnia, M.,Ameriyoon, A., NaziabadFareham, M.,
&HaddamVista, H. R., (2010) Satisfaction rate of hospitalized patients in
military hospitals with presented services: Iranian Journal of
Military Medicine Summer 2010, Volume 12, Issue 2; 101-105.
Correspondence; Email: [email protected] Received
2009/07/05; Accepted 2010/03/14
Ford, R.C., Bach, S.A and Fettler, M.D. (1997), “Methods of
measuring patient satisfaction in health care
University of Trinidad and Tobago | Masters in Health Administration | May 2014
94

organizations”, Health Care Management Review, vol. 22, no. 2,
pp. 74-89.
Jewish General Hospital, (2014). Overall Patient
Satisfaction. [Online] Available:
http://www.jgh.ca/en/qisatisfactionrates [Accessed: 1st
April, 2014]
Harle, T. J. &Anderson, J. D. (1993) Patient satisfaction with implant-
supported prostheses 1993. Int J Prosthodont. 1993 Mar-Apr;
6(2):153-62.
Kelly., G. (2004) Health and Lifestyle Information Survey 2004
LAERD (2013). Statistical Analysis. [Online] Available:
https://statistics.laerd.com/premium/account.php [Accessed:
1st April, 2014]
McKinley, R. K., Manku-Scott, T., Hastings, A.M., French, D.P.
and Baker, R. (1997), “Reliability and validity of a new
measure of patient satisfaction without-of-hours primary
medical care in the United Kingdom: Development of a
patient questionnaire”, British Medical Journal, vol. 314, pp.193-
198.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
95

Marshall, G N & Hays., R. D. (1994) The Patient Satisfaction
Questionnaire Short-Form (PSG-18), RAND
Roemer, M. I. & Montoya-Aguuilar, C. (1988) Quality assessment and
assurance in Primary Health care: WHO Geneva 1988
Roller, M.R. (2011) Qualitative Research Design: Selective
articles from research designs review. Roller Marketing
Research, October, 2011
Schafer, J. J. (2008) Reaching a Better Management Model for Military
Medicine. Fall 2008, Vol. 86 Issue 4, p18-32, 15p, Washington
(D.C.) United States . Database: Business Source Complete
Shaw, C. (2003) How can hospital performance be measured and monitored?
Copenhagen, WHO Regional Office for Europe (Health Evidence
Network Report);
http://www.euro.who.int/document/e82975.pdf, accessed 29
August 2003).
TRICARE Management Activity (TMA), Health Program Analysis &
Evaluation Directorate (TMA/HPA&ED), in the Office of the
Assistant Secretary of Defence (Health Affairs) (OASD/HA),
(2011) The Evaluation of the TRICARE Program: Fiscal Year 2011 Report to
Congress
University of Trinidad and Tobago | Masters in Health Administration | May 2014
96

APPENDICESAppendix A
Sample Questionnaire
Adapted from the Long-Form Patient Satisfaction Questionnaire
(PSG III) (Grant 1998- RAND)
INSTRUCTIONSOn the following pages are some things personnel say abouthealthcare. Please read each one carefully before you answer,keeping in mind the medical care you are receiving now or havereceived. (If you have not received care recently, think about
University of Trinidad and Tobago | Masters in Health Administration | May 2014
97

what you would expect if you received care today.)We areinterested in your honest opinion, your feelings, GOOD andBAD, about the medical services you have received and howstrongly do you AGREE or DISAGREE with each of the followingstatements?Please tick your responses where applicable for each question,one response only per question.You are not required to place any identification marks on theform(I.E. YOUR REGIMENTAL NUMBER, RANK, AND NAME OR ANY OTHERDISTINGUISHING FEATURES THAT ARE UNIQUE TO YOU AND CANIDENTIFY YOU).
Sex: [] Male [] Female
Age: [] 18-24 [] 25-35 [] 36-45 [] 46 and over
Marital status: [] Married [] Single [] Divorce
[] Separated [] Widowed
Education: [] Primary School [] Secondary or College []
Tertiary[] Others (State)
Insurance coverage: [] Yes [] No
History of admission to Sick Bay: [] Yes [] No
Years of military service: [] Less than 6 years [] 7 to
12 years [] Over 12 years
Category of personnel: [] Commissioned Officer
[] Warrant Officer, Fleet Chief Petty
Officer, Chief Petty Officer
[] Senior Non-commissioned Officer or
Senior Ratings
University of Trinidad and Tobago | Masters in Health Administration | May 2014
98

[] Junior Non-commissioned Officer or
Junior Ratings
[] Other Ranks or Ratings
Strong
ly
Agree
Agree Uncerta
in
Disagr
ee
Strong
ly
Disagr
ee
1. If I need medicalcare, I can get carewithout any trouble inthe medicaldepartment.
[] [] [] [] []
2. Doctors need to bemore thorough intreating and examiningme.
[] [] [] [] []
3. I am very satisfied with the medical services I received.
[] [] [] [] []
4. It is easy for me to get medical care in anemergency.
[] [] [] [] []
5. Doctors are good aboutexplaining the reasonsfor medical tests.
[] [] [] [] []
6. I am usually keptwaiting for a longtime when I am at thedoctor’s office.
[] [] [] [] []
7. I think my doctor’soffice has everythingneeded to provide
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
99

medical care.
8. The doctor who treatsme should give me morerespect.
[] [] [] [] []
9. The medical care Ihave been receiving isjust perfect.
[] [] [] [] []
10. Sometimes doctorsmake me wonder iftheir diagnosis iscorrect.
[] [] [] [] []
11. During my medicalvisit, I am alwaysallowed to sayeverything that Ithink is important.
[] [] [] [] []
12. When I go formedical care, they arecareful to checkeverything whentreating and examiningme.
[] [] [] [] []
13. It is .hard for meto get medical care onshort notice
[] [] [] [] []
Strong
ly
Agree
Agree Uncerta
in
Disagr
ee
Strong
ly
Disagr
ee
14. The doctors whotreat me have agenuine interest in meas a person.
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
100

15. Sometimes doctorsuse medical termswithout explainingwhat they mean.
[] [] [] [] []
16. For me the officehours when I can getmedical care areconvenient (good) forme.
[] [] [] [] []
17. There are thingsabout the medicalsystem where I receivemy care from that needto be improved.
[] [] [] [] []
18. The office I receivemy medical care shouldbe open for more hoursthan it is.
[] [] [] [] []
19. The medical staffthat treats me knowsabout the latestmedical development
[] [] [] [] []
20. I have to pay formore of my medicalcare than I canafford.
[] [] [] [] []
21. I have easy accessto the medicalspecialist I need.
[] [] [] [] []
22. Sometimes doctorsmake me feel foolish.
[] [] [] [] []
23. Where I get medicalcare, I have to waittoo long for emergency
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
101

treatment.
24. Doctors act toobusiness like andimpersonal towards me
[] [] [] [] []
25. There is a crisis inthe health care in theDefence Force today.
[] [] [] [] []
26. Doctors never exposeme to unnecessaryrisks.
[] [] [] [] []
Agree Uncer
tain
Disagre
e
Strong
ly
Disagr
ee
Strong
ly
Agree
27. There are somethings about themedical care that Ireceived that could bebetter.
[] [] [] [] []
28. My doctor treats mein a very friendly andcourteous manner.
[] [] [] [] []
29. Those who provide myhealth care sometimeshurry too much whenthey treat me.
[] [] [] [] []
30. The doctor I haveseen lack experiencewith my medicalproblem.
[] [] [] [] []
31. Places where I canaccess medical care in
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
102

the Defence Force areconveniently located.
32. Doctors sometimeignore what I tellthem.
[] [] [] [] []
33. When I am receivingmedical attention,they should pay moreattention to myprivacy.
[] [] [] [] []
34. If I have a medicalquestion, I can reacha doctor without anyproblem.
[] [] [] [] []
35. Doctors rarely giveme advice on ways toavoid illness andstaying healthy.
[] [] [] [] []
36. All thingsconsidered the medicalcare I received isexcellent.
[] [] [] [] []
37. Doctors listencarefully to what Ihave to say.
[] [] [] [] []
38. I have some doubtsabout the ability ofthe doctors who treatme.
[] [] [] [] []
39. The doctors usuallyspend plenty of timewith me.
[] [] [] [] []
40. Doctors always dotheir best to keep me
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
103

from worrying.Strong
ly
Agree
Agree Uncerta
in
Disagr
ee
Strong
ly
Disagr
ee
41. I find it hard toget an appointment formedical care rightaway
[] [] [] [] []
42. I am dissatisfiedwith some things aboutthe medical care Ireceived.
[] [] [] [] []
43. My doctors are verycompetent and well-trained.
[] [] [] [] []
44. I am able to getmedical care wheneverI need it.
[] [] [] [] []
45. Have you ever beenhospitalized?
Yes [] No []
46. If “Yes” were youever visited by theDFMO?
Yes [] No []
47. Have you evervisited any other DFMOoutside of in theirPrivate Office?
Yes [] No []
Excelle
ntGood Fair Poor Very
Poor
48. If “Yes “how werethe services provided?
[] [] [] [] []
Completely
Somewhat
NeitherSatisfi
Somewhat
Completely
University of Trinidad and Tobago | Masters in Health Administration | May 2014
104
Satisfied
Satisfied
ed norDissatisfied
Dissatisfied
Dissatisfied
49. How would you ratethe services providedby following:
Female Doctor [] [] [] [] []
Senior Male Doctor [] [] [] [] []
Enlisted Male Doctor [] [] [] [] []
Pharmacist [] [] [] [] []
Medical Orderlies [] [] [] [] []
Others (State) [] [] [] [] []
Completely
Satisfied
SomewhatSatisfied
NeitherSatisfied norDissatisfied
Somewhat
Dissatisfied
Completely
Dissatisfied
50. How would you ratethe medicalfacilities?
[] [] [] [] []
51. Overall how wouldyou rate the medicalservices provided?
[] [] [] [] []
52. During your MilitaryService have you seenany changes in theservices provided?
Yes[] No[]
53. If “Yes”, how do yourate the changes inthe Medical Services
[] [] [] [] []
University of Trinidad and Tobago | Masters in Health Administration | May 2014
105

you have seenimplemented?
54.State possible recommendations to improve quality of service you can rate them in order of importance:
55.If “YES” to Question 52: State the changes in the Medical Services that you have seen implemented during your career.
56.State possible areas that you think should be eliminated toimprove service quality you can rate them in order or priority:
THANK YOU VERY MUCH FOR YOURHONEST ANDVALUED OPINION.
Appendix B
Letter of request to Chief of Defence Staff
Chief of Defence StaffTrinidad and Tobago Defence ForceDefence Force Headquarters
University of Trinidad and Tobago | Masters in Health Administration | May 2014
106

Airways RoadCHAGUARAMAS November2012
REQUEST FOR APPROVAL COMPLETE A SURVEY OF PERSONNELSATIFACTION OF THE MEDICAL SERVICES OFFERED IN THE DEFENCEFORCE
1. Approval is hereby requested by Lieutenant (Ret) Dexter
A Horsford to conduct a survey of the personnel satisfaction
of the medical services offered within the Trinidad and Tobago
Defence Force (TTDF or Force).This is in partial fulfilment of
the Masters of Health Administration being read for under the
University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance,
adequacy, efficiency, effectiveness and overall confidence in
the system and its providers is being met while providing
service to its serving members and their dependants. To
determine what may be the hindrances, and to make possible
recommendations for sustainable improvement in the services
base on the findings.
3. The significance of this proposed study is to help set
in place a system or systems of measuring the satisfaction of
deliverables of the medical services within the Force that
would inform the hierarchy of its medical needs and how the
medical service can be a sustained and viable arm of the TTDF
in addressing it needs
University of Trinidad and Tobago | Masters in Health Administration | May 2014
107
4. Submitted for your consideration.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosures:1. Copy of questionnaire to be administered.2. Copy of the proposal
Appendix C
Letter of request to Formation Commanders, Permanent Secretary
Ministry of National Security and Ethics Committee Ministry of
Health
Commanding OfficerTrinidad and Tobago ArmyArmy HeadquartersCorner of Knox and Abercrombie StreetsPORT OF SPAIN November 2012
APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTION OF THEMEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a survey of
the personnel satisfaction of the medical services offered within
the Trinidad and Tobago Defence Force (TTDF or Force).This is in
partial fulfilment of the Masters of Health Administration being
read for under the University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance, adequacy,
efficiency, effectiveness and overall confidence in the system and
it providers is being met while providing service to its serving
University of Trinidad and Tobago | Masters in Health Administration | May 2014
108

members and their dependants. To determine what may be the
hindrances, and to make possible recommendations for sustainable
improvement in the services base on the findings.
3. The significance of this proposed study is to help set in
place a system or systems of measuring the satisfaction of
deliverables of the medical services within the Force that would
inform the hierarchy of its medical needs and how the medical
service can be a sustained and viable arm of the TTDF in addressing
it needs.
4. Further approval is being sought to conduct the survey
within your formation.
5. Submitted for your consideration.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
Commanding OfficerTrinidad and Tobago Coast GuardCoast Guard HeadquartersStaubles BayCHAGUARAMAS November 2012
REQUEST FOR APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTIONOF THE MEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a survey of
University of Trinidad and Tobago | Masters in Health Administration | May 2014
109

the personnel satisfaction of the medical services offered within
the Trinidad and Tobago Defence Force (TTDF or Force).This is in
partial fulfilment of the Masters of Health Administration being
read for under the University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance, adequacy,
efficiency, effectiveness and overall confidence in the system and
it providers is being met while providing service to its serving
members and their dependants. To determine what may be the
hindrances, and to make possible recommendations for sustainable
improvement in the services base on the findings.
3. The significance of this proposed study is to help set in
place a system or systems of measuring the satisfaction of
deliverables of the medical services within the Force that would
inform the hierarchy of its medical needs and how the medical
service can be a sustained and viable arm of the TTDF in addressing
it needs.
4. Further approval is being sought to conduct the survey
within your formation.
5. Submitted for your consideration.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
University of Trinidad and Tobago | Masters in Health Administration | May 2014
110

Commanding OfficerTrinidad and Tobago Air GuardAir Guard HeadquartersPiarco Air StationNorthbank RoadPIARCO November 2012
REQUEST FOR APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTIONOF THE MEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a survey of
the personnel satisfaction of the medical services offered within
the Trinidad and Tobago Defence Force (TTDF or Force).This is in
partial fulfilment of the Masters of Health Administration being
read for under the University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance, adequacy,
efficiency, effectiveness and overall confidence in the system and
it providers is being met while providing service to its serving
members and their dependants. To determine what may be the
hindrances, and to make possible recommendations for sustainable
improvement in the services base on the findings.
3. The significance of this proposed study is to help set in place
a system or systems of measuring the satisfaction of deliverables of
the medical services within the Force that would inform the
hierarchy of its medical needs and how the medical service can be a
University of Trinidad and Tobago | Masters in Health Administration | May 2014
111

sustained and viable arm of the TTDF in addressing it needs.
4. Further approval is being sought to conduct the survey within
your formation.
5. Submitted for your consideration.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
Commanding OfficerTrinidad and Tobago Defence Force ReservesDefence Force Reserve HeadquartersMacaqueripeCHAGUARAMAS November 2012
REQUEST FOR APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTIONOF THE MEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a survey of
the personnel satisfaction of the medical services offered within
the Trinidad and Tobago Defence Force (TTDF or Force).This is in
partial fulfilment of the Masters of Health Administration being
read for under the University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
University of Trinidad and Tobago | Masters in Health Administration | May 2014
112

services offered in the TTDF. To determine if compliance, adequacy,
efficiency, effectiveness and overall confidence in the system and
it providers is being met while providing service to its serving
members and their dependants. To determine what may be the
hindrances, and to make possible recommendations for sustainable
improvement in the services base on the findings.
3. The significance of this proposed study is to help set in place
a system or systems of measuring the satisfaction of deliverables of
the medical services within the Force that would inform the
hierarchy of its medical needs and how the medical service can be a
sustained and viable arm of the TTDF in addressing it needs.
4. Further approval is being sought to conduct the survey within
your formation.
5. Submitted for your consideration.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
Ethical CommitteeMinistry of HealthPark and Edward Streets
University of Trinidad and Tobago | Masters in Health Administration | May 2014
113

PORT OF SPAIN November 2012
APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTION OF THEMEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a survey of
the personnel satisfaction of the medical services offered within
the Trinidad and Tobago Defence Force (TTDF or Force).This is in
partial fulfilment of the Masters of Health Administration being
read for under the University Of Trinidad and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance, adequacy,
efficiency, effectiveness and overall confidence in the system and
it providers is being met while providing service to its serving
members and their dependants. To determine what may be the
hindrances, and to make possible recommendations for sustainable
improvement in the services base on the findings.
3. The significance of this proposed study is to help set in place
a system or systems of measuring the satisfaction of deliverables of
the medical services within the Force that would inform the
hierarchy of its medical needs and how the medical service can be a
sustained and viable arm of the TTDF in addressing it needs.
4. Further approval is being sought to conduct the survey within
your formation.
DA Horsford
University of Trinidad and Tobago | Masters in Health Administration | May 2014
114

Lieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
Permanent SecretaryMinistry of National SecurityTemple Court 1Abercrombie StreetsPORT OF SPAIN November 2012
APPROVAL TO COMPLETE A SURVEY OF PERSONNEL SATIFACTION OF THEMEDICAL SERVICES OFFERED IN THE DEFENCE FORCE
1. Approval was sought and acceded to by the Chief Of Defence
Staff, by Lieutenant (Ret) Dexter A Horsford to conduct a
survey of the personnel satisfaction of the medical services
offered within the Trinidad and Tobago Defence Force (TTDF or
Force).This is in partial fulfilment of the Masters of Health
Administration being read for under the University Of Trinidad
and Tobago.
2. The aim of this thesis is to review the current medical
services offered in the TTDF. To determine if compliance,
adequacy, efficiency, effectiveness and overall confidence in
the system and it providers is being met while providing
service to its serving members and their dependants. To
determine what may be the hindrances, and to make possible
recommendations for sustainable improvement in the services
University of Trinidad and Tobago | Masters in Health Administration | May 2014
115
base on the findings.
3. The significance of this proposed study is to help set in place
a system or systems of measuring the satisfaction of
deliverables of the medical services within the Force that
would inform the hierarchy of its medical needs and how the
medical service can be a sustained and viable arm of the TTDF
in addressing it needs.
4. Further approval is being sought to conduct the survey within
your formation.
DA HorsfordLieutenant (Retired)Registered Dietitian
Enclosure:1. Copy of Questionnaire to be administered.2. Copy of the proposal3. Chief of Defence Staff approval
Appendix D
Interviewer Initials: Questionnaire Number:
TO BE KEPT BY THE PARTICIPANT
University of Trinidad and Tobago
University of Trinidad and Tobago | Masters in Health Administration | May 2014
116

Centre for Health Sciences - Masters in Health
Administration
To determine quality satisfaction of the medical services
in Trinidad and Tobago Defence Force.
Questionnaire to determine satisfaction of the medical
services within the
Defence Force
Introduction:
My name is Dexter A Horsford and I am a Postgraduate student
at the University of Trinidad and Tobago. I am currently doing
a project in fulfillment of my Master's Degree in Health
Administration in the area of medical services quality
satisfaction. My project title is ‘To determine quality
satisfaction of the medical services in Trinidad And Tobago
Defence Force.’The purpose of this project is determine the
quality and standard of the medical services within the
Defence Force and if the personnel are satisfied with it.
Interviews are being carried out with medical practitioners,
pharmacist, dietitian, patients, nurses, technicians and
medical orderlies who will be asked about the quality of the
medical services if they are meeting the needs of the patients
and with the patients to determine their satisfaction. The
interview will take approximately 10 to 15 minutes of your time
University of Trinidad and Tobago | Masters in Health Administration | May 2014
117

and will be tape recorded. I am the only person who has
access to the tapes, which will be kept electronically on a
password protected computer and destroyed by me once I have
completed transcription.
Participation is voluntary and you may withdraw at any timewithout penalty. You may also refuse to answer any questionwhich makes you uncomfortable. All information provided willbe treated in a confidential manner and no names will appearon the transcribed interview, only Questionnaire Numbers.The list linking the names and questionnaire numbers will bekept in a locked drawer in a secured office, to which only Iwill have access. Once the data has been entered into acomputer and verified, the list and any identifyinginformation will be shredded.
Extracts of the interview may be used in the report, but youwill not be identified in any way. There are no risks areassociated with your participation.
This project has been approved by the MHA Postgraduate ThesisCommittee of the University of Trinidad and Tobago as well asthe Ministry of National Security, Chief of Defence Staff andFormation Commanders.
If there are any questions or concerns you have concerning
this project, please do not hesitate to contact either myself
or my supervisor:
STUDENT CONTACT INFORMATION: Dexter A Horsford
email: [email protected]
Phone: 868-626-1410 (H); 868-
726-3748 (C)
SUPERVISOR CONTACT INFORMATION:
University of Trinidad and Tobago | Masters in Health Administration | May 2014
118

If you have any questions or concerns about your rights as a research subject you may contact, anonymously if you wish, theMHA Postgraduate Thesis Committee Chair (Dr. Bennie Berkeley) at the University of Trinidad and Tobago at 868-642-8888, ext21468 or by email:[email protected] .
Interviewer Initials: Questionnaire
Number:
THIS COPY TO BE KEPT BY THE INTERVIEWER
Informed Consent Form:
I,________________________(print full name), hereby agree to
participate in the project outlined above. I give my permission to
be interviewed and for the interview to be tape recorded. I
understand the nature and intent of the research and have been
University of Trinidad and Tobago | Masters in Health Administration | May 2014
119

given the opportunity to ask questions. I understand where to
direct any future questions that I may have. I have received a copy
of the consent form.
PARTICIPANT'S STATEMENT
Participant Name: Signature:
Interviewer Name: Signature:
Date:
Interviewer Initials: Questionnaire
Number:
University of Trinidad and Tobago | Masters in Health Administration | May 2014
120

THIS COPY TO BE KEPT BY THE PARTICIPANT
Informed Consent Form:
I,________________________(print full name), hereby agree to
participate in the project outlined above. I give my permission to
be interviewed and for the interview to be tape recorded. I
understand the nature and intent of the research and have been
given the opportunity to ask questions. I understand where to
direct any future questions that I may have. I have received a copy
of the consent form.
PARTICIPANT'S STATEMENT
Participant Name: Signature:
Interviewer Name: Signature:
Date:
University of Trinidad and Tobago | Masters in Health Administration | May 2014
121

Appendix E
Thesis Sampling Size Matrix-Lt (Ret) DA Horsford
TTDF Population (N)=5040 Sample Size (S)=357
TTA=2921
57.956%
S=207
Off SNCO Cpl/LCpl Pte
3.0% 12.5% 45.5% 38.5%
6 26 95(39/56) 80
1Bn
2Bn
SSB
Eng
DFHQ
1Bn
2Bn
SSB
Eng
DFHQ
1Bn
2Bn
SSB
Eng
DFHQ
1Bn
2Bn
SSB
Eng
DFHQ
2 1 1 1 1 7 4 5 5 5 30 16 16 16 17 18 17 17 17 11
1TTR/RHQ==57 2TTR=38 SSB=38 1st Engr=38 DFHQ=34
LegendOfficer (Off)Senior Non Commissioned Officer (SNCO)Senior Rates (SR)Corporal/Leading Seaman (Cpl/LS)Able Seaman, Ordinary Seaman; Senior Aircraft Crewman, Junior Air Crewman; Private (OR)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
122
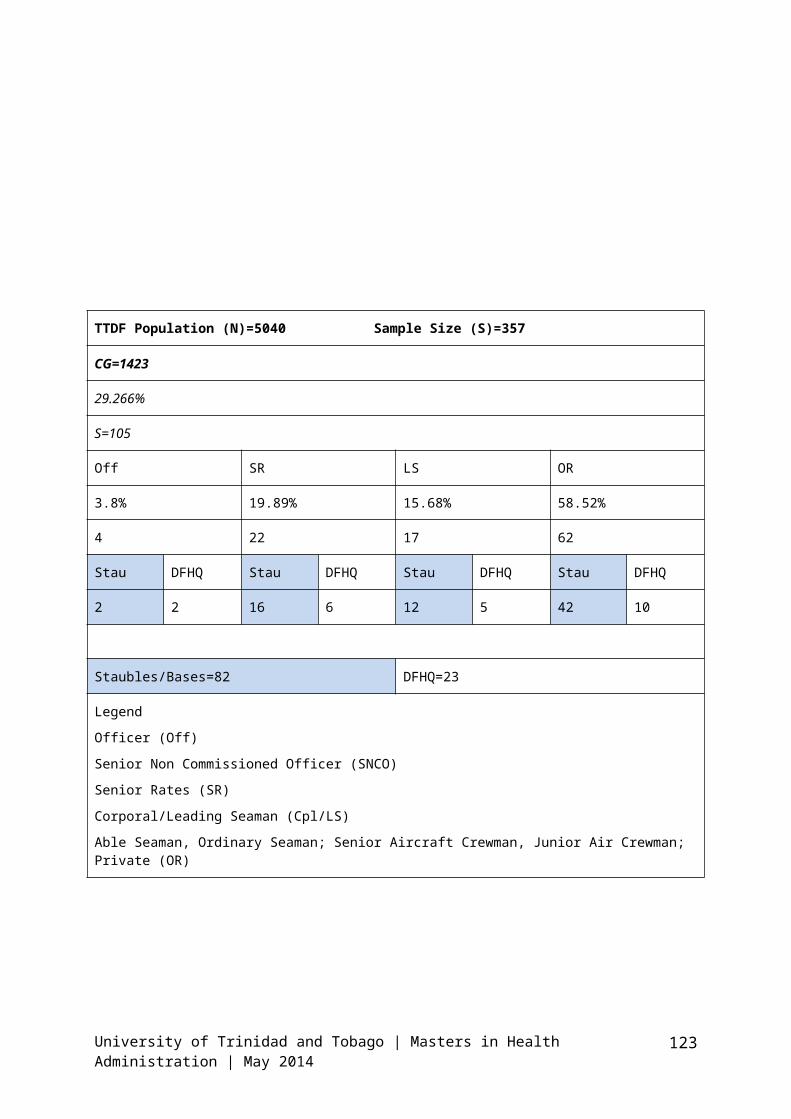
TTDF Population (N)=5040 Sample Size (S)=357
CG=1423
29.266%
S=105
Off SR LS OR
3.8% 19.89% 15.68% 58.52%
4 22 17 62
Stau DFHQ Stau DFHQ Stau DFHQ Stau DFHQ
2 2 16 6 12 5 42 10
Staubles/Bases=82 DFHQ=23
LegendOfficer (Off)Senior Non Commissioned Officer (SNCO)Senior Rates (SR)Corporal/Leading Seaman (Cpl/LS)Able Seaman, Ordinary Seaman; Senior Aircraft Crewman, Junior Air Crewman; Private (OR)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
123

TTDF Population (N)=5040 Sample Size (S)=357
TTAG=434
8.611%
S=31
Off WO Sgt Cpl OR
12.21% 2.30% 9.21% 16.12% 57.14%
4 1 3 5 18
AG DFHQ AG DFHQ AG DFHQ AG DFHQ AG DFHQ
3 1 1 0 2 1 3 2 12 6
TTAG=21 DFHQ=10
LegendOfficer (Off)Senior Non Commissioned Officer (SNCO)Senior Rates (SR)Corporal/Leading Seaman (Cpl/LS)Able Seaman, Ordinary Seaman; Senior Aircraft Crewman, Junior Air Crewman; Private (OR)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
124

TTDF Population (N)=5040 Sample Size (S)=357
DFR (Perm Staff)=212
4.206%
15
Off WO/FCPO/CPO SSgt/PO/Sgt Cpl/LS/LCpl OR
4.72% 5.19% 13.21% 28.77% 48.11%
1 1 2 4 7
DFR DFHQ DFR DFHQ DFR DFHQ DFR DFHQ DFR DFHQ
1 0 1 0 1 1 2 2 5 2
DFR=10 DFHQ=5
LegendOfficer (Off)Senior Non Commissioned Officer (SNCO)Senior Rates (SR)Corporal/Leading Seaman (Cpl/LS)Able Seaman, Ordinary Seaman; Senior Aircraft Crewman, Junior Air Crewman; Private (OR)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
125

Appendix F
Table 2 - Demographic characteristics, insurance coverage and the history of hospitalization or admitted to Sick-bay in the studied population
Variable Number PercentSex Male
Female
Age
18-2425-3536-4546 and over
EducationPrimary schoolSecondary or CollegeTertiary
Marital status
MarriedSingleDivorceSeparatedWidowed
Insurance coverage
YesNo
University of Trinidad and Tobago | Masters in Health Administration | May 2014
126

History ofadmission to Sick Bay
YesNo
Appendix G
Table 3 - The frequency of different levels of satisfaction inseven domains under studySatisfactionlevel↓Domain→
Completelysatisfied
Satisfied
Neithersatisfiednordissatisfied
Dissatisfied
Completelydissatisfied
General satisfactionItems: 3, 9, 14, 42Technical quality
University of Trinidad and Tobago | Masters in Health Administration | May 2014
127

Items: 2, 5, 7, 10, 12, 38Interpersonal mannerItems: 9, 24, 28CommunicationItems: 1, 3, 5, 28Time spent with DoctorItems: 10, 12, 29, 39Accessibility and convenienceItems: 7, 8, 13, 15, 21, 23, 41, 44(Values that would be in parentheses would be percentage and
values outside the parentheses
Would be the numbers)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
128
Appendix H
Table 4 - The overall level of satisfaction or dissatisfactionof patients with the servicesOverall level↓Area→
Satisfied Satisfied Dissatisfied Level ofSignificance
General satisfactionTechnical qualityInterpersonal mannerCommunication
Time spent with DoctorAccessibility and convenience(Values that would be in parentheses would be percentage and
values outside the parentheses
Would be the numbers)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
129

Appendix I
Table 5 – Univariate Statistics for subscales and constituent
items
Subscale and items Mean SD
General satisfactionItems: 3, 9, 14, 42Technical qualityItems: 2, 5, 7, 10, 12, 38Interpersonal mannerItems: 9, 24, 28CommunicationItems: 1, 3, 5, 28Time spent with DoctorItems: 10, 12, 29, 39Accessibility and convenienceItems: 7, 8, 13, 15, 21, 23, 41, 44
University of Trinidad and Tobago | Masters in Health Administration | May 2014
130

Appendix J
Table 6 -Budget (Proposed)
Expendables 500.00
Capital Expenditure 2,000.00
Total Expenditure 2,500.00
Funding would be covered by Grant and employer support.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
131

Appendix K
Table 1: Abbreviated Item Content and Scale Groupings,
Questionnaire
Item Abbreviated Item Content Direction of
Variable
Placement[a] by Scale Wording Label
General Satisfaction (GSAT)
3 Very satisfied with care +
PSQ01
27 Some things could be better –
PSQ02
University of Trinidad and Tobago | Masters in Health Administration | May 2014
132

36 Medical care is excellent +
PSQ03
17 Things need to be improved –
PSQ04
9 Care just about perfect + PSQ05
42 Dissatisfied with some things –
PSQ06
Technical Quality (TECH)
12 Careful to check everything +
PSQ07
2 Doctors need to be more thorough –
PSQ08
7 Office has everything needed +
PSQ09
10 Wonder if diagnosis is correct –
PSQ10
19 Know latest medical developments +
PSQ11
30 Lack experience with my problems –
PSQ12
43 Doctors competent, well-trained +
PSQ13
38 Doubt about ability of doctors –
PSQ14
26 Never expose me to risk + PSQ15
35 Doctors rarely give advice –
PSQ16
Interpersonal Aspects (INTER)
University of Trinidad and Tobago | Masters in Health Administration | May 2014
133

24 Too business-like, impersonal –
PSQ17
40 Do best to keep me from worrying +
PSQ18
33 Should pay attention to privacy –
PSQ19
14 Genuine interest in me + PSQ20
22 Make me feel foolish –
PSQ21
28 Very friendly and courteous +
PSQ22
8 Should give me more respect –
PSQ23
Communication (COMM)
5 Explain the reason for tests +
PSQ24
15 Use terms without explaining – PSQ25
11 Say everything that’s important +
PSQ26
32 Ignore what I tell them – PSQ27
37 Doctors listen carefully +
PSQ28
Time Spent with Doctor (TIME)
39 Doctors spend plenty of time +
PSQ29
29 Hurry too much when treat me – PSQ30
Access/Availability/Convenience
University of Trinidad and Tobago | Masters in Health Administration | May 2014
134

1 Get hospital care without trouble +
PSQ31
13 Hard to get care on short notice –
PSQ32
4 Easy to get care in an emergency +
PSQ33
18 Office should be open more hours –
PSQ34
31 Care conveniently located +
PSQ35
23 Wait too long for emergency treatment –
PSQ36
34 Can reach doctor for help with medical
Question + PSQ37
41 Hard to get appointment right away –
PSQ38
16 Office hours are convenient +
PSQ39
6 Kept waiting at doctor’s office –
PSQ40
21 Easy access to specialists +
PSQ41
44 Get medical care whenever need it +
PSQ42
[a]Order of item in PSQ-III is administered in the Medical
Outcomes Study (MOS). This section of the MOS questionnaire
included 51 items; item 30 refers to beliefs about a crisis in
University of Trinidad and Tobago | Masters in Health Administration | May 2014
135

health care and is not used in scoring the satisfaction
subscales.
University of Trinidad and Tobago | Masters in Health Administration | May 2014
136

Appendix L
GANTT Chart of time line for Project
University of Trinidad and Tobago | Masters in Health Administration | May 2014
ID Task Name Duration Start Finish
12 First drraft of proposal 90 days Tue 03/04/12 M on 06/08/123 Biostatistics and Epidemiology input to develop a proposal – Year 1 (Sept 2011 – July 2012) 230 days Thu 01/09/11 W ed 18/07/124 Submission of proposal to PG Project Committee – by July 2011 30 days Fri 01/07/11 Thu 11/08/115 Proposal Grade from BS lecturer – by August 2012 30 days M on 03/09/12 Fri 12/10/126 First submission of proposal to M HA Postgraduate Thesis Committee – by beginning of Year 2 (September 2012) 30 days M on 02/09/13 Fri 11/10/137 Resubmission of proposal, with revisions (if needed) - for grading – November 2012 60 days M on 01/10/12 Fri 21/12/128 Assignment of supervisor – by January 2013 60 days Thu 29/11/12 W ed 20/02/139 Protocol completed and submitted to relevant ministry or committee – by February 2013 30 days Tue 29/01/13 M on 11/03/1310 Continue literature review, make necessary contacts at institution, desk work – by November 2012 to M arch 2013 150 days Thu 01/11/12 W ed 29/05/1311 Permission and ethical approval granted – by M arch 2013 30 days Fri 01/03/13 Thu 11/04/1312 Begin data collection – by April 2013 152 days M on 01/04/13 Tue 29/10/1313 Begin data analysis – by September 2013 30 days M on 02/09/13 Fri 11/10/1314 Begin write-up of thesis – by October 2013 30 days Tue 01/10/13 M on 11/11/1315 First draft of thesis submitted to supervisor (copy all members of M HA Postgraduate Thesis Committee) – by November 2013 28 days Fri 01/11/13 Tue 10/12/1316 Poster Presentation of project in UTT Atrium with internal and external audience – by December 2013 1 day Tue 31/12/13 Tue 31/12/1317 Final draft of thesis submitted to supervisor – by early January 2014 45 days M on 02/12/13 Fri 31/01/1418 Final thesis submitted for grading – February 2014 87 days Thu 31/10/13 Fri 28/02/14
JunJulAugSepOctNovDecJanFebM arAprM ayJunJulAugSepOctNovDecJanFebM arAprM ayJunJulAugSepOctNovDecJanFebM arQtr 2, 2011Qtr 3, 2011Qtr 4, 2011Qtr 1, 2012Qtr 2, 2012Qtr 3, 2012Qtr 4, 2012Qtr 1, 2013Qtr 2, 2013Qtr 3, 2013Qtr 4, 2013Qtr 1, 2014
2011 2012 2013 2014
137

University of Trinidad and Tobago | Masters in Health Administration | May 2014 138

Appendix L: Responses to questions 54, 55 and 561. 54. State possible
recommendations to improve quality of service you can rate them in order of importance:
55. If ‘YES’ to Question 52: State the changes in the Medical Services that you have seen implemented during your career.
56. State possible areas that you thinkshould be eliminatedto improve service quality you can ratethem in order of priority:
2. Access to specialists;Additional staff.
Acquisition of ambulance;Visits to bases by medical department.
3. The inclusion of a serving member as a DFMO since employed his service has beenexceptional, he ensures that you arewell informed and under stands and also carries out thorough checks whenadministering medical attention toindividuals.
4. More instructors to help out the patients till the doctor reaches;Equipment’s that are working properly.
5. Medic staff be sent for more or advance training;Bigger facility to accommodate more patients;Treat and deal with persons with ‘genuine’
Using Divon CR to treat all forms of pain only (TTCG);For smooth operations to administration process, administer cases at high
University of Trinidad and Tobago | Masters in Health Administration| May 2014
139

cases and not fake cases (put them on charge);Have a Duty NCO/SeniorRate instead of Duty Medic only;Have better drugs available (Divon CR and Panadol cannot heal all patients problem in the TTDF)
priority eliminate all ungenuine cases;Absence of a driver for the ambulance.
6. Quick service;Care of patients;Confidentiality of patients’ sickness.
7. More doctors at disposal to deal with number of patients coming to facilities.
8. Medical Orderlies needmore training;Need proper equipment;Need a doctor 24/7;Need a dentist 24/7;Need a Military Hospital or a proper health plan paid for by the government. TheMIR is a Doctor officeand nothing else.
9. Time waiting to see doctor;Manner in which some orderlies operate.
Renovation was done making more room forpatients, and air-condition placed forcomfort.
10.Medic be send to the hospital for OJT;
The sick-bay was improved and better,
University of Trinidad and Tobago | Masters in Health Administration| May 2014
140

so to deal with persons going sick, Camp Ogden and Teteron.
11.There should be more than one doctor attending to patients;Doctor hours should belonger.
12.Equality across the board.
People majority.
13.More welcoming and order in the staff;More waiting accommodations.
More medical assistance in the staff.
14.Proper respect and care from doctors whentreating patients;Medical in-confidence practice should be enforced;Correct dosage and supply with reference to quantity when issuing medicine to patient by doctors andmedics alike.The immediate dismissal and transferof medics or doctors who abuse or don’t enforce the medical in-confidence procedure;Less military approachand more medical approach from a humaneand professional stand
Proper seating and space accommodation for patients;A more sanitized environment;A faster reaction with reference to screening of patients by medics.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
141

point with reference to (doctor patient/medic patient relationship).
15.Need a doctor who could be there longer;Need more medics so the screening process will be faster.
16.Have a Commissioned Doctor with better customer service for soldiers;Improve on the medics so we won’t have to pay for or look for itelsewhere;The doctor must stay alittle longer and not 1 or 2 hours.Working ambulance at each camp;Doctor at each camp location;Increase medicine for soldiers who are having babies and soldiers who have civilian wives having babies.
17.Assist soldiers in andout of uniform with extreme urgency, and also there family;Make sure machine to test be always working;Limit time frame for
Get rid of those don’t care;Place people who know what they are doing;Update machinery;Hold those accountable for
University of Trinidad and Tobago | Masters in Health Administration| May 2014
142

test and results. delinquency.18.Employing more
doctors, have them work a shift system just in case of any emergency.Equipment for saving lives must be bought and put to use (eg x-ray machine, CT Scan machines and ultra sound machines) for soldiers that need this type of services and cannot afford;Improve the transport system in the medical field also ambulance drivers should not have to look for an Orderly Officer to sign Work Ticket in emergency.
CO FundTTR Sport FundMilart/Mypart
19.The current Female DFMO should be fired because she does not pay attention to the need of sick personnel;Better screening;Upgrade of facilities;More time with the Dr;Lecture on how to stayhealthy in this stressful organization.
20.Faster service;Better facilities;
Nothing should be eliminated just improved.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
143

Better quality medication.
21.The medical departmentstaff needs to change often.
22.Better trained staff;Improved and more modern equipment;Better facilities;Improved administrative procedures;Increase in medical staff;Provide the military with its own hospital and medical practitioners.
Slightly improved facilities;Increase in staff;Slightly, but not modern, better equipment.
23.More doctors;More medication.
24.Fire doctors if they do not want to work;Visit their private place.Enlist more doctors
25.Have proper medical facilities and qualified doctor.
26.Better equipment;Improved facilities.
27.Doctor at MIR every day;Medication more available.Better disposals
Medic are more able;Better service from orderlies;Better brand name medication that
Longer process to see DFMO then after you wait hours no doctor and you have to come again and again;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
144

suited towards orthopaedics injuries;More vitamins.
work.
28.Doctor every day;More medics;More equipment for medics to work with;Blood test available.
Waiting long periodsto see a doctor.
29.The MI Room should operate by a first come first serve basisand not by seniority or who is your medic friend;More responsibility should be performed bythe medical staff whenhandling patients’ files to avoid misplacement.
30. Improve the space inthe waiting area;Attendance has improved a little.
31.Have a private doctor for TTDF 24 hrs and not only on a morning.They should not be a member of the service.
32.A bigger facility;More medical staff;More equipment upgraded;More access to medication.
Having to wait on a doctor to get dentalof optical device.
33.All medical personnel
University of Trinidad and Tobago | Masters in Health Administration| May 2014
145
consistently trained and kept up to date onequipment;New and functioning ambulances are needed;New equipment.
34. Drugs, the MIR and equipment
35.The TTDF have its own medical facility.
36.More staff;Update machines. Think we should have more than one doctor
37.Certified medics;Updated machine and equipment.
38.Well trained doctors;More mature staff;Better equipment.
More structure equipment
39.New doctor;Better train staff;Better equipment;Proper medication;Better facility. More doctors
Communication;The waiting period
The waiting period
40.Better MI Rooms;More qualified medics;Doctors who don’t feellike screening you or vex you came.
41.Better equipment;Better training for
University of Trinidad and Tobago | Masters in Health Administration| May 2014
146

medical orderlies.42.Let the medical staff
have lectures to TTDF of STD’s and proper hygiene.Increase the medical staff
43.Be more professional;Be more understanding.
New facilities;New equipment;More staff.
Long waiting to see doctor
44.Improvement in the procurement process toaid in medical invoices and medication.
45.More doctors;Bigger staff;Bigger facilities;Random check-up;Treating all ranks fair;Better medical attention.
46.Antibiotics should be available in the MI Room;Doctors should be accessible in the TTDF;Doctors should stop act business like whenproviding advice.
47.We should be able to get prescription medication at our medical institutions.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
147

48.Medics need to be morepolite;Medics need to be further trained;MI Room needs to be more stocked with medical equipment and supplies;There need to be more than 1 doctor visitingpersonnel;Doctors need to be able to provide their services from Monday –Friday at least.
49.Doctors to be more polite and concerned about patients;Medical facilities to be improved;Doctors to listen carefully to what I have to say;Doctor to explain medical terms and things to patients.
Nothing should be eliminated just quality should be improved.
50.Need to have more staff;Need to report the doctor;Need to have a place soldiers can go and get more service.
51.More doctors trained in different fields; Get person from the outside to help
University of Trinidad and Tobago | Masters in Health Administration| May 2014
148
trained and educate person in the TTDF.
52.A doctor in camp for 24hrs;Much more Drs as well as pharmacists assigned to serve the TTDF;No more second class drugs (genuine drugs for faster wellness and relief).
53.Having the addition of2 more doctors and round the clock rotation of these doctors who should be certified;Other staff should be sent on courses so that they can be better medical officers.
54.The faster screening of patients so they can see the doctor.
The lengthy wait to see the doctor.
55.Increase size of facility;Increase staffing;More persons should beexposed to training atexternal agencies bothlocal and foreign;Improved relations with external agenciesto ensure speedy and priority treatment of military personnel.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
149

56.Having more time spentwith the patients;Give proper drugsProper screen process.More medics for screening process;Attending to more ill patient first;
Long hours of waiting;No more first come first serve.
57.More doctors58.Have doctors at the
facility medical unit from 8:00 – 4:00 daily;Get doctor who are commit to serving the members of the military.
59.Better privacy, accommodation.
60.Employed more doctors and personal assistance;Improve more better machines;Must more medical insurance and cheaper;Better medicine.
61.Change female doctor. Change the female doctor her manners is not good.
62.Transport can be improved;Doctors could be more professional.
63.Let the OC mind their own business
Stop the fraternization.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
150

64.Give patient more attention.
65.Training course;Confidentiality of patient.
66.Need more staff so we can see more patients on a daily basis and faster.
The facilities has been extended;New machines and things have been brought in to help the patients (beds, mattresses, etc.)
67.Need more qualified doctors;More professional training of the medical staff;Increase staff;Bigger facilities.
68.More up to date medical equipment and facilities;Faster medical treatments for emergencies.
69.Relieve the female doctor of her contract;Properly train the medical orderlies in CSR;Properly train the Orderlies in dispensing pharmaceuticals;Have more civilians towork in the medical
No area should be eliminated, but mostif not all should beimproved so as to gain better quality for soldiers.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
151

room.70.MI Room to small;
Little to no emergencyprotocol;Each unit should have emergency life precaution protocol.Empathetic personnel with advanced trained skills required
The physical infrastructure and seating arrangement are much better but the medical officers’ attitude needs major adjustment.
Change the female doctor and get a more professional DFMO;Basic inefficiencies;Pharmacy lacks a lotof basic medicine.
71.Better equipment;Better seating arrangement;(If possible) separatebuilding.
72.We need to build a military hospital to eliminate this ongoingproblem;Proper training needs to be done.
73.Professionalism;Care;Love for what you do and know as a doctor;Regards and respect.
74.The doctor needs to doa physical assessment of patients and not read new medical report and judge the patient;More medics are neededin all military establishments;More equipment is
University of Trinidad and Tobago | Masters in Health Administration| May 2014
152

needed mainly defibrillators;The attitude of the doctors to wards patients should be a lot more caring. It appears that they treat us all as if we are trying to use the medical system to get free time.
75.More medical machines to conduct medical test etc.;Send members of medical staff to further their skill inthe medical field.The working area should be a bit cleaner and more organized;The doctor should havea more professional office area.
The response on carefor soldiers have improve by 50%;The quantity of medication has improved by 50%;The facility has been upgraded.
76.More training and patience.
77.More medical courses Because of the medical courses
78.Remove the female existing DFMO;Replace the female existing DFMO with a doctor that actually works to help/assist the TTDF.Recommend the AdMed card for all TTDF
Remove the waiting time mandatory;Clico Health Plan that is use by existing TTDF personnel;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
153

personnel. It’s the only pre-paid insurance policy in T&T.
79.More care and attention needed.
80.More doctors;Better doctors;Doctors who care aboutthe people that they see on a day to day.
81.A doctor on call at least until 1200hrs.The sick-bay could be improved as for comfort of patient admitted.
82.People skills;Professional ethics and training;Proper facilities;Relocation and additional installations throughout the Force.
The facility should not be in any camp;Currently the femaledoctor directs soldiers to go only to West Shore Medical and states she only recognizes reports and results from that institution. This isbias and improper practice and should be reported to the NWRHA head.
83.Better equipment for the medical staff to do their jobs;Working ambulances;More effort and time spent do their jobs by
University of Trinidad and Tobago | Masters in Health Administration| May 2014
154

the doctor.84.More ambulances;
ECG equipment;More medical staff.
85.More enlisted medical staff
86.Give more training;Give more incentive.
More medication;Better and more equipment.
87.More ambulance service;Need more medical equipment.
Facility service.
88.Better CSR service;More listening by doctors of patients’ illness before diagnosis.
89.Medics take your situation for granted and more on personality than professional;Need more qualified nurses rather than medics who just have the first aid certificate;Need who is punctual and consistent not to mention efficient;The pharmacist does a great job but she needs to be provided with a wider range of drugs so she doesn’t have to substitute
Stop let officers sign your sick-leavebecause they aren’t in the medical fieldto determine whetheror not you are or aren’t really sick. In other words what the doctor says doesn’t really matter than;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
155

drugs which are recommended;TTDF needs to put proper service in place when referred tospecialist whereas bills are subsidized and the best care is provided in the interest of the soldier and establishment;In the service at the public hospital.
90.More doctors;Longer hours;Doctor frequently visiting the MI Room.
91.More doctors that are willing to listen to your problems and givespecifics like the enlisted doctor.
92.Better infrastructure;Doctor should be available more;More ambulance;More qualified staff.
93.Need a doctor who is more professional whencoming to dealing withpersonnel of the Force.
We have the quantityand personnel to do the job but in a "don’t care" attitude towards individuals. People personalize things too much.
94.More doctors;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
156
Doctors available every day;Doctors to physically check patients;Doctors who care aboutpatients’ well-being.
95.Be more efficient;More doctors needed inthe TTDF MI Room.
96.Expand the medical department with more equipment
Training in the medical staff;Facility upgrade wasdone.
Stop admitting patient to sick-bay.
97.Expansion Some minor small equipment
Requiring personnel abroad
98.Distribution of knowledge to those on off station
Courteous staff
99. Short waiting period100.Increase capacity101.More training for
medical staff; more modern equipment;Improved facilities.
102.Round the clock serviceable ambulance;More modernize equipment/machinery;Easy access to doctor on station;More personnel medically trained withminimum of basic firstaid.
Just improvement no areas to be eliminated.
103.Enlist additional
University of Trinidad and Tobago | Masters in Health Administration| May 2014
157

medical officers;Establish medical policy to set standards and execute medical boarding of chronically ill/injured personnel.
104.Pay closer attention to problems of ratings.
105.More doctors should beemployed;Higher skill is required;More caring doctors should be employed.
Less unskilled doctors.
106.A working ambulance;More upgrade medical equipment needed;Bigger and more spacious medical room.
TTDF stop accept sick leave from private organization.
107.Overall general facelift of the medical department.
Hostility.
108.Expansion in facilities.
Stereo types.
109.A little more understanding.
110.A proper MI Room, always have to stand around to be attended too;Proper equipment;Enough medication;Another doctor or 2 should be enlisted;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
158

Better trained staff who knows how to deal with private information.
111.Better equipment. Stop victimizing juniors.
112.Ambulance;More improved medical supplies.
113.A (DFMO) on the Station
114.EquipmentStaff
115.Larger variety of medicationMore medical staff
116.More staff (well trained)More doctors on duty (more experience)
117.The medical orderlies training can be improved in such ways,where their ways of dealing with patients and the matter.Their work experience should come hand in hand with such field being trained in, for
The level/rank in which persons classed a medic.
118.Bring back a doctor atAir Guard;Ensure PT becomes a must so persons can befit and healthy.
119.The advance training The Upgrade of the
University of Trinidad and Tobago | Masters in Health Administration| May 2014
159
required and the recent training required needs to be of first priority, themedical orderly need to be properly certified for the job.More specialization interms of medical orderly.
ambulance equipment and medical room equipment.
120.Military hospital (North, Central, South, East locations);The above manned by civil doctors and nurses;Doctors on duty 24hrs at the hospital, not “on call”.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
160

Table Showing Coded Responses for Question 54 (State possible
recommendations to improve quality of service you can rate them
in order of importance)
ITEMS TOTAL PERCENTAGE (%)Equipment (improved,
increase)27 22
More Staff 26 21.1Training 23 18.7More Doctors 20 16.2Ambulance (increase,
operational)10 8.1
Medication (access,
better, increase)8 6.5
Bigger facility 5 4.1Military Hospital 5 4.1
University of Trinidad and Tobago | Masters in Health Administration| May 2014
161

Table Showing Responses for Questions 55 and 56
55. If ‘YES’ to Question 52:
State the changes in the
Medical Services that you
have seen implemented during
your career.
56. State possible areas that
you think should be eliminated
to improve service quality you
can rate them in order of
priority:
1. Acquisition of ambulance;
Visits to bases by medical
department.
Using Divon CR to treat all
forms of pain only (TTCG);
For smooth operations to
University of Trinidad and Tobago | Masters in Health Administration| May 2014
162

administration process,
administer cases at high
priority eliminate all
ungenuine cases;
Absence of a driver for the
ambulance.
2. The inclusion of a serving
member as a DFMO since
employed his service has been
exceptional, he ensures that
you are well informed and
under stands and also carries
out thorough checks when
administering medical
attention to individuals.
Get rid of those don’t care;
Place people who know what they
are doing;
Update machinery;
Hold those accountable for
delinquency.
3. Renovation was done making
more room for patients, and
air-condition placed for
comfort.
People majority.
4. The sick-bay was improved and
better, so to deal with
persons going sick, Camp
Ogden and Teteron.
CO Fund
TTR Sport Fund
Milart/Mypart
5. More medical assistance in
the staff.
Nothing should be eliminated
just improved.
6. Proper seating and space
accommodation for patients;
Longer process to see DFMO then
after you wait hours no doctor
University of Trinidad and Tobago | Masters in Health Administration| May 2014
163
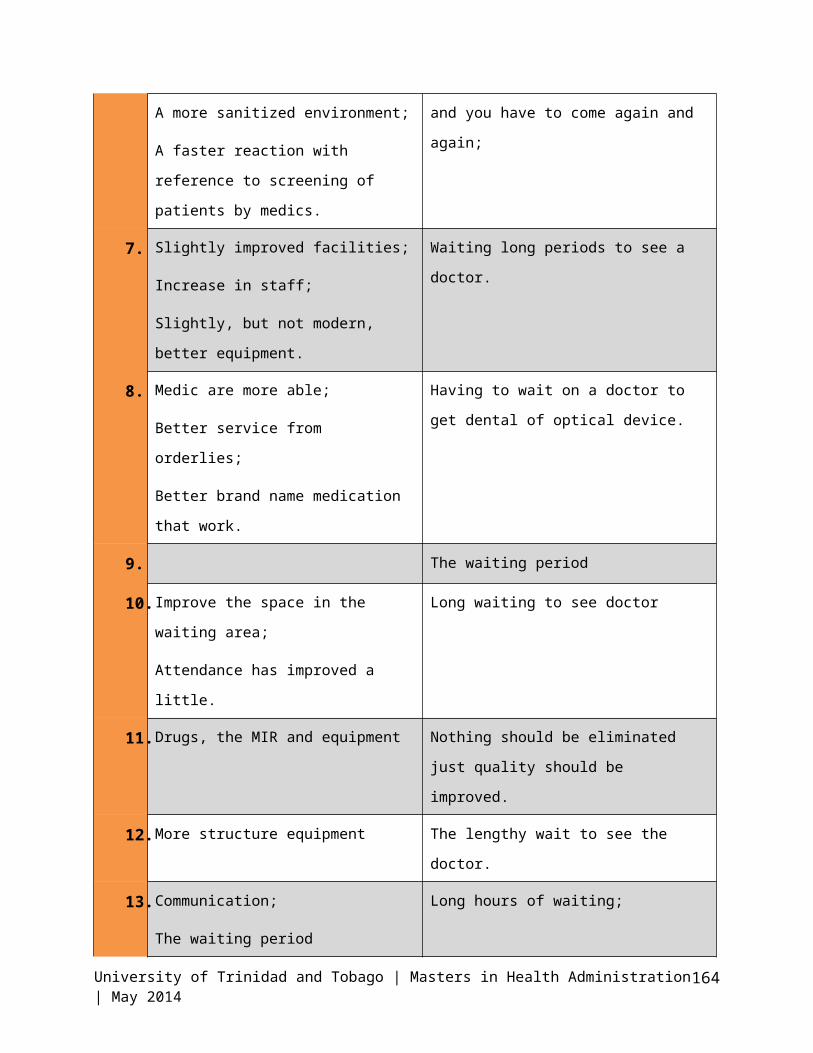
A more sanitized environment;
A faster reaction with
reference to screening of
patients by medics.
and you have to come again and
again;
7. Slightly improved facilities;
Increase in staff;
Slightly, but not modern,
better equipment.
Waiting long periods to see a
doctor.
8. Medic are more able;
Better service from
orderlies;
Better brand name medication
that work.
Having to wait on a doctor to
get dental of optical device.
9. The waiting period
10.Improve the space in the waiting area;
Attendance has improved a
little.
Long waiting to see doctor
11.Drugs, the MIR and equipment Nothing should be eliminated
just quality should be
improved.
12.More structure equipment The lengthy wait to see the
doctor.
13.Communication;
The waiting period
Long hours of waiting;
University of Trinidad and Tobago | Masters in Health Administration| May 2014
164
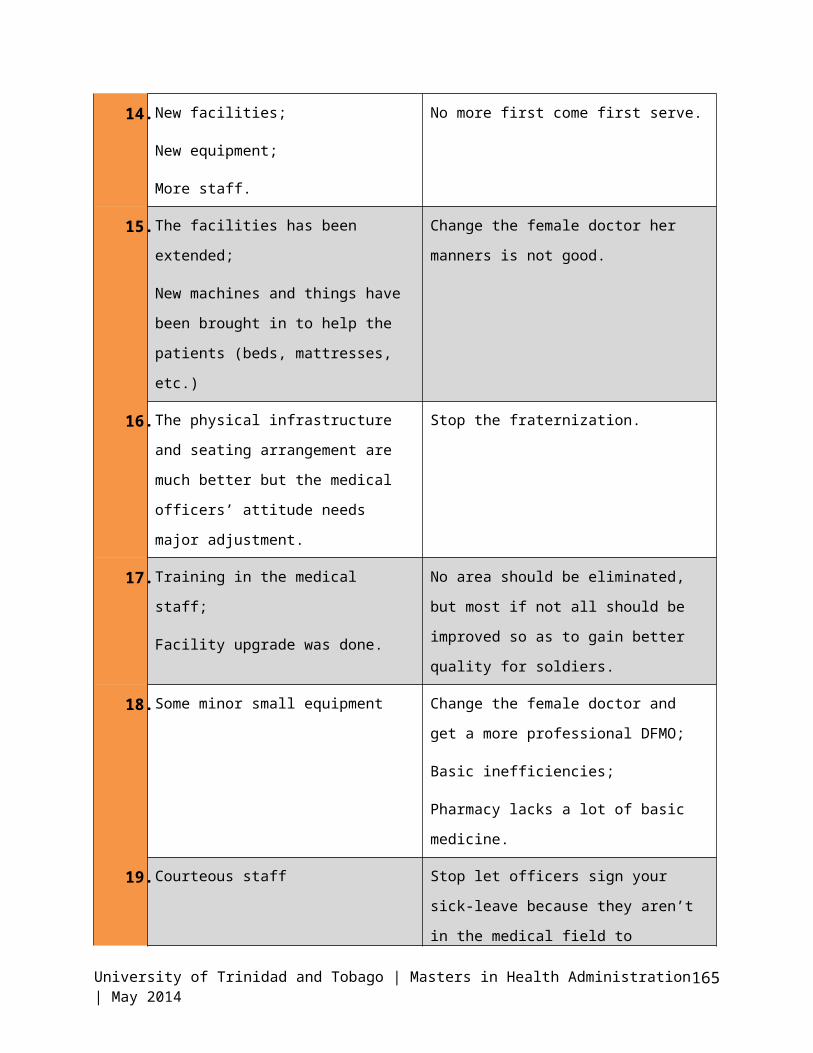
14.New facilities;
New equipment;
More staff.
No more first come first serve.
15.The facilities has been extended;
New machines and things have
been brought in to help the
patients (beds, mattresses,
etc.)
Change the female doctor her
manners is not good.
16.The physical infrastructure and seating arrangement are
much better but the medical
officers’ attitude needs
major adjustment.
Stop the fraternization.
17.Training in the medical staff;
Facility upgrade was done.
No area should be eliminated,
but most if not all should be
improved so as to gain better
quality for soldiers.
18.Some minor small equipment Change the female doctor and
get a more professional DFMO;
Basic inefficiencies;
Pharmacy lacks a lot of basic
medicine.
19.Courteous staff Stop let officers sign your
sick-leave because they aren’t
in the medical field to
University of Trinidad and Tobago | Masters in Health Administration| May 2014
165

determine whether or not you
are or aren’t really sick. In
other words what the doctor
says doesn’t really matter
than;
20.Short waiting period We have the quantity and
personnel to do the job but in
a "don’t care" attitude towards
individuals. People personalize
things too much.
21.TTDF stop accept sick leave from private organization.
Stop admitting patient to sick-
bay.
22.The Upgrade of the ambulance equipment and medical room
equipment
Requiring personnel abroad
23. Just improvement no areas to be
eliminated
24. Less unskilled doctors.
25. Hostility.
26. Stereo types.
27. Stop victimizing juniors.
28. The level/rank in which persons
classed a medic.
University of Trinidad and Tobago | Masters in Health Administration| May 2014
166

University of Trinidad and Tobago | Masters in Health Administration| May 2014
167

Appendix M: Frequency distribution Tables and Related Charts
Table of Frequency Distribution of
Access/Availability/Convenience (AAC) Subscale (%)
Disagre
e
Uncerta
in Agree
Can get care without any trouble in
the medical department (AAC1)
54
(22.6)
83
(34.9)
101
(42.5)
Easy to get medical care in an
emergency(AAC2)
80
(33.2)
83
(34.4)
78
(32.4)
Usually kept waiting for a long time
at the doctor’s office (AAC3)
52
(23.6)
30
(12.4)
159
(66.0)
Hard to get medical care on short
notice(AAC4)
49
(20.3)
46
(19.0)
147
(60.8)
The office hours are convenient
(good) (AAC5)
119
(49.2)
39
(16.1)
84
(34.7)
The office should be open for more 35 30 177
University of Trinidad and Tobago | Masters in Health Administration| May 2014
168

hours than it is (AAC6) (14.4) (12.4) (73.1)
Easy access to the medical
specialist needed (AAC7)
144
(60.3)
50
(20.9)
45
(18.8)
01020304050607080
22.6
33.223.6 20.3
49.2
14.4
60.3
34.9 34.4
12.419 16.1
12.420.9
42.532.4
6660.8
34.7
73.1
18.8
Chart represening AAC Frquency
DisagreeUncertain
Table representing frequency distribution ofCommunication Theme
Frequency distribution (%)
Disagree
Uncerta
in Agree
Doctors explain the reasons for 73 65(26.9 104(43)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
169

medical tests (COMM1) (30.1) )
Allowed to say everything that I
think is important (COMM2)
64
(26.7)
37
(15.5)
139
(57.9)
Use of medical terms without
explaining meaning (COMM3)
75
(31.1) 29 (12)
137
(56.8)
Sometime ignored what they are
told (COMM4)
76
(32.2)
38
(16.1)
122(51.
7)
Listen carefully to what is said
(COMM5)
88
(37.2)
59
(24.9)
89
(37.5)
30.1 26.7 31.1 32.2 32.726.915.5 12 16.1
24.943
57.9 56.8 51.737.5
Chart showing Communication Theme Frequency distribution (%)
Disagree Uncertain Agree
Table showing frequency distribution of Interpersonal Care
University of Trinidad and Tobago | Masters in Health Administration| May 2014
170

Theme Frequency Distribution (%)
DisagreeUncertai
nAgree
The doctor who treats me should
give me more respect (INTER1)
65
(26.8)24 (9.9)
154
(63.4)
The doctors who treat me have a
genuine interest in me as a
person (INTER2)
108
(44.8)
79
(32.8)
54
(22.4)
Sometimes doctors make me feel
foolish (INTER3)
100
(42.4)
36
(15.3)
100
(42.4)
Doctors act too business like and
impersonal towards me (INTER4)
80
(33.5)
48
(20.1)
111
(46.4)
My doctor treats me in a very
friendly and courteous manner
(INTER5)
72
(30.1)43 (18)
124
(51.9)
When I am receiving medical
attention, they should pay more
attention to my privacy (INTER6)
32
(13.6)22 (9.3)
182
(77.1)
Doctors always do their best to
keep me from worrying (INTER7)
102
(44.3)
66
(28.7)62 (27)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
171
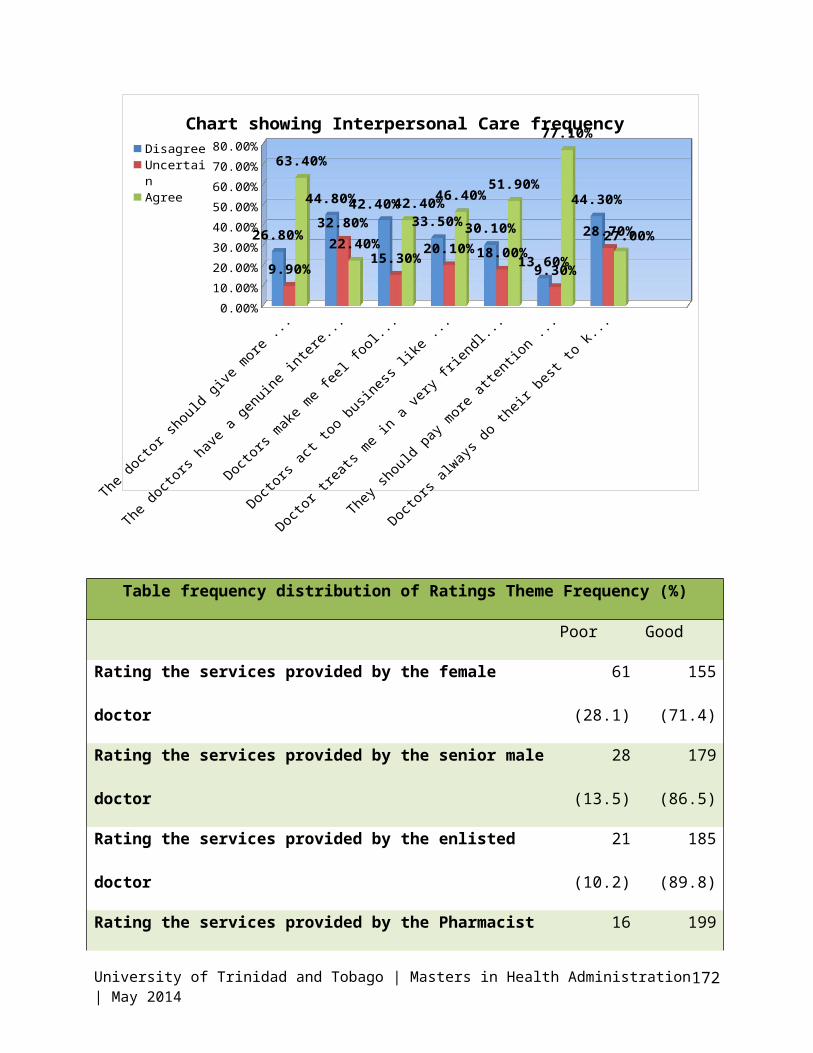
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%
26.80%
44.80%42.40%33.50%30.10%
13.60%
44.30%
9.90%
32.80%
15.30%20.10%18.00%9.30%
28.70%
63.40%
22.40%
42.40%46.40%51.90%
77.10%
27.00%
Chart showing Interpersonal Care frequency DisagreeUncertainAgree
Table frequency distribution of Ratings Theme Frequency (%)
Poor Good
Rating the services provided by the female
doctor
61
(28.1)
155
(71.4)
Rating the services provided by the senior male
doctor
28
(13.5)
179
(86.5)
Rating the services provided by the enlisted
doctor
21
(10.2)
185
(89.8)
Rating the services provided by the Pharmacist 16 199
University of Trinidad and Tobago | Masters in Health Administration| May 2014
172

(7.5) (92.5)
Rating the services provided by the Medical
Orderlies
38
(17.6)
178
(82.5)
Rating the services provided by Other (State
the Others)
26
(22.1)
92 (78)
Rating the medical facilities 89
(39.1)
139
(60.9)
Rating the medical services provided 76
(33.3)
152
(66.7)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
173

0102030405060708090
100
28.1
13.5 10.2 7.517.6 22.1
39.133.3
71.4
86.5 89.8 92.582.5 78
60.9 66.7
Chart showing Ratings Theme Frequency Poor
University of Trinidad and Tobago | Masters in Health Administration| May 2014
Table showing Frequency Statistics for personnel
hospitalized and visited by the DFMO
Frequen
cy
Percen
t
Valid
Percent
Cumulative
Percent
Valid
Yes 110 44.0 47.00 47.0
No 124 49.6 53.0 100.0
Total 234 93.6 100.0
Missin
g
Syste
m16 6.4
Total 250 100.0
174

Yes No
47
53
Chart showing Have you ever been hospitalized
University of Trinidad and Tobago | Masters in Health Administration| May 2014
175

University of Trinidad and Tobago | Masters in Health Administration| May 2014
Table showing frequency of- If ‘Yes’ were you ever
visited by the DFMO
Frequen
cy
Percen
t
Valid
Percent
Cumulative
Percent
Valid
Yes 11 4.4 9.9
No 99 39.6 89.2 99.1
3.00 1 .4 .9 100.0
Total 111 44.4 100.0
Missin
g
Syste
m139 55.6
Total 250 100.0
176

10%
90%
Chart showing frequency of Visited by the DFMO
at hospital
YesNo
University of Trinidad and Tobago | Masters in Health Administration| May 2014
Table showing Frequency of ‘Have you ever visit
any other DFMO outside of in their Private Office’
Frequen
cy
Percen
t
Valid
Percent
Cumulative
Percent
Valid
Yes 61 24.0 27.0 27.0
No 161 64.4 72.5 99.5
4.00 1 .4 .5 100.0
Total 222 88.8 100.0
Missing
System
28 11.2
Total 250 100.0
177

University of Trinidad and Tobago | Masters in Health Administration| May 2014
Table for Frequency of If ‘Yes’ how were the
services provided
Frequenc
y Percent
Valid
Percen
t
Cumulat
ive
Percent
Poor 4 1.6 6.8 6.8
Good 55 22 93.2 100
Valid Total 59 23.6 100
Missing
Syste
m 191 76.4
Total 250 100
178

Poor7%
Good93%
Chart showing frequency of-How was the Doctor service
at the private office
Table showing Frequency Distribution (%) of Time variables.
Finance and Crisis Variables
DisagreeUncerta
inAgree
Those who provide my health care
sometimes hurry too much when they
treat me. (Time1)
46 (19.5
%)
23
(9.7%)
167
(70.7%)
The doctors usually spend plenty of
time with me (Time2)
175
(73.9%)
27
(11.4%)
35
(14.8%)
I have to pay for more of my medical
care than I can afford (FIN)
47
(19.6%)
32
(13.4%)
160
(67%)
There is a crisis in the health care 16 31 193
University of Trinidad and Tobago | Masters in Health Administration| May 2014
179

within the Force today. (Crisis) (6.6%) (12.9%) (80.4%)
University of Trinidad and Tobago | Masters in Health Administration| May 2014
180




















