Entrepreneurial Politics and Interest Representation in Taiwan
Upload
independentCategory
view
3download
0
Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59
Epidemiologic study of type 2 diabetes in Taiwan
Chih-Jen Chang a, Feng-Hwa Lu a, Yi-Ching Yang a, Jin-Shang Wu a,Ta-Jen Wu b, Muh-Shy Chen c, Lee-Ming Chuang d, Tong-Yuan Tai d,*
a Department of Family Medicine, College of Medicine, National Cheng Kung Uni6ersity, Taipei, Taiwan, ROCb Department of Internal Medicine, College of Medicine, National Cheng Kung Uni6ersity, Taipei, Taiwan, ROC
c Department of Ophthalmology, College of Medicine, National Taiwan Uni6ersity, Taipei, Taiwan, ROCd Department of Internal Medicine, College of Medicine, National Taiwan Uni6ersity, Taipei, Taiwan, ROC
Abstract
Diabetes mellitus (DM) in adults is a global health problem, although its prevalence varies widely betweendifferent populations and the rate has generally increased worldwide. In Taiwan, the mortality rate from DM hasalmost doubled over the past 10 years. The prevalence of DM in Taiwan was established between 1985 and 1996 andthe rates were between 4.9 and 9.2%. The prevalence of impaired glucose tolerance (IGT) was 15.5% (men 15% andwomen 15.9%). The prevalence of DM and IGT increased significantly with age for both genders. The significantfactors associated with newly diagnosed DM were age, BMI, family history of DM, systolic blood pressure(hypertension), physical activity and serum triglyceride levels. The prevalence of large vessel disease (LVD) in DMand non-diabetic subjects were 20.0 and 12.9%, respectively. Among diabetics, 15.8% had ischemic heart disease(IHD), 1.7% leg vessel disease (leg VD), and 2.5% stroke. In non-diabetics, the prevalence of the aforementionedmacroangiopathies were 11.5, 0.2 and 1.2%, respectively. The diabetics had a significantly higher prevalence ofmacrovascular disease than non-diabetic subjects. The most significantly associated with the LVD was serumcholesterol levels. Serum cholesterol and HbA1c were significantly associated with the development of IHD.Cigarette smoking and female gender were significantly associated with the leg VD. The prevalence of diabeticretinopathy (DR) was 35.0%. (background DR 30%, preproliferative DR 2.8% and proliferative DR 2.2%,respectively.) The prevalence of DR for previously and newly diagnosed diabetics were 45.2 and 28.3% (men 42.8 vs.33.3% and women 47.5 vs. 24.8%), respectively. From multiple logistic regression analysis, duration of DM was themost important risk factor related to DR. Diabetic subjects treated with insulin had a higher risk of developingretinopathy than those treated with dietary control. The prevalence of nephropathy and neuropathy were 12.9 and23.5%, respectively. For those patients with and those without nephropathy and neuropathy, the duration of DM,percentage of insulin treatment, percentage of hypertension, and fasting plasma glucose were significantly different.Diabetic duration, hypertension, insulin treatment and glycemic control consistently correlated with nephropathyand neuropathy. In conclusion, the prevalence of DM in Taiwan was between 4.9 and 9.2%, and the prevalence ofIGT was 15.5%. The possible risk factors of newly diagnosed diabetes were age, family history of DM, BMI, SBP(hypertension), physical activity and triglyceride levels. Diabetes in Chinese subjects share many characteristics
www.elsevier.com/locate/diabres
* Corresponding author. Tel.: +886-2-23222169; fax: +886-2-23222169.E-mail address: [email protected] (T.-Y. Tai).
0168-8227/00/$ - see front matter © 2000 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0168 -8227 (00 )00179 -0
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59S50
similar to other Asian populations. The burden imposed by the chronic complications of diabetes is massive. InTaiwan, the mortality rates from DM have increased greatly over the past 10 years. Reduction of the modificable riskfactors such as BMI, hypertenion and dyslipidemia, and increase of physical activity and good glycemic controlthrough public health efforts may help to reduce the risk of DM and its chronic complications. © 2000 ElsevierScience Ireland Ltd. All rights reserved.
Keywords: Epidemiology; Prevalence; Risk factor; Chinese, Type 2 (non-insulin-dependent) diabetes
1. Introduction
Diabetes mellitus (DM) in adults is a globalhealth problem. Although its prevalence varieswidely between different populations from low(B3%), moderate (3–10%), high (11–20%) toextremely high (\20%), the rate has generallyincreased worldwide [1]. The remarkable eco-nomic achievement in the last 30 years has re-sulted in a great improvement in living standardsand prolongation of life expectancy in Taiwan. InTaiwan, the mortality rate from diabetes mellitushas almost doubled over the past 10 years and itsranking in the leading causes of death has in-creased: one twelfth in 1982, one eighth in 1983,one seventh in 1984 and one fifth since 1987 [2]. Ithas become one of the major health problems ofthe country.
2. Material and methods
2.1. Study subjects
2.1.1. Northern Taiwan
2.1.1.1. Taipei Study (1985). This survey was con-ducted from November 1985 to June 1986. Eightof the 78 subdistricts of the Ta-An precinct wererandomly selected. Five villages evenly distributedover the island were also randomly selected. Thetotal number of subjects aged 40 years or olderwho underwent the survey in Taipei City was4272 and that of the five villages was 7206, with aresponse rate of 65.3 and 72.0%, respectively.Among the 715 subjects, 608 subjects, including225 newly diagnosed and 383 previously diag-nosed, participated in a further study.
2.1.1.2. Kin-Hu, Kinmen. The study subjects werethose \30 years of age in Kin-Hu township.According to household registration, 4097 eligibleresidents were invited to the community center toattend the screening test from January to Febru-ary 1991.
2.1.1.3. Ann-Lo, Keelung. This survey was per-formed between July 1988 and June 1990 in theAnn-Lo district of Keelung in northern. The re-sponse rate for a total of 9087 eligible subjectswas 67.4%.
2.1.1.4. Taipei Study (1978). A total 217 diabeticpatients (110 men and 107 women) who werediscovered during 1978 survey for adult diabeticsin the Cheng-Chung district of Taipei City. Theywere examined for diabetic retinopathy, neuropa-thy and nephropathy.
2.1.2. Southern TaiwanThe study was performed in Tainan City of
southern Taiwan. The sampling scheme was athree-stage process that generated a stratified sys-temic cluster sample of households throughoutthe city. Of the 2416 eligible people, 1638 (67.8%)participated in the study.
2.2. Methods
With the help of specially trained assistants, allsubjects were interviewed according to a struc-tured questionnaire, while included demographicinformation, past medical history of diabetes andhypertension, current smoking habit, medicationhistory, physical activity, and family history ofDM and hypertension. Obesity was defined as aBMI\27 for men and \25 for women [3] or
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59 S51
BMI\30 for both genders [4]. Overnight fastingserum and plasma samples were kept frozenat −20°C until analysis. Serum total cholesteroland triglyceride were measured enzymatically us-ing automated methods. Diabetes mellitus wasdiagnosed according to the World Health Orga-nization (WHO) criteria [5]. Hypertensionwas deemed present when the systolic pressure\160 mmHg, or when the diastolic pressure \95 mmHg or a history of hypertension and cur-rently receiving treatment [6]. Physical activityand the exercise status as were prescribed previ-ously [4]. Total physical activity assessment wascalculated in MET-hours per week over all activi-ties for the past year [7]. Subjects who smokedless than 100 cigarettes in their lifetime wereclassified as nonsmokers, more than 100cigarettes but had stopped before the examina-tion were classified as ex-smokers, and smoked atthe time of the interview were classified as cur-rent smokers.
According to the protocol of the WHO Multi-national Study on Vascular Disease in Diabetes[8], LVD, including stroke, IHD, and leg VD,were investigated. The ophthalmic examinationswere performed with direct and indirect ophthal-moscopy after dilating the pupils with trop-icamide 1% and phenylepinephrine 10%. Theretinopathy status was divided into normal;background, preproliferative and proliferativeDR. Ophthalmoscopy was performed in 527 ofthe diabetic subjects. Urinalysis for screeningof clinical proteinuria was conducted at leastthree times in a 1-month period. Diabeticnephropathy was defined as a positive result on adipstick test, approximately equivalent to 300–500 mg/l of urine. Neuropathy was confirmed ifthe motor nerves showed abnormal conductionvelocity [9].
The statistical significance was assessed by us-ing the Student’s t-test and the chi-square test.Correlation coefficients were estimated by Spear-man’s method and multiple logistic regressionanalysis was also performed to evaluate multi-variate-adjusted associations between related fac-tors and diabetic macrovascular and micro-vascular diseases.
3. Results
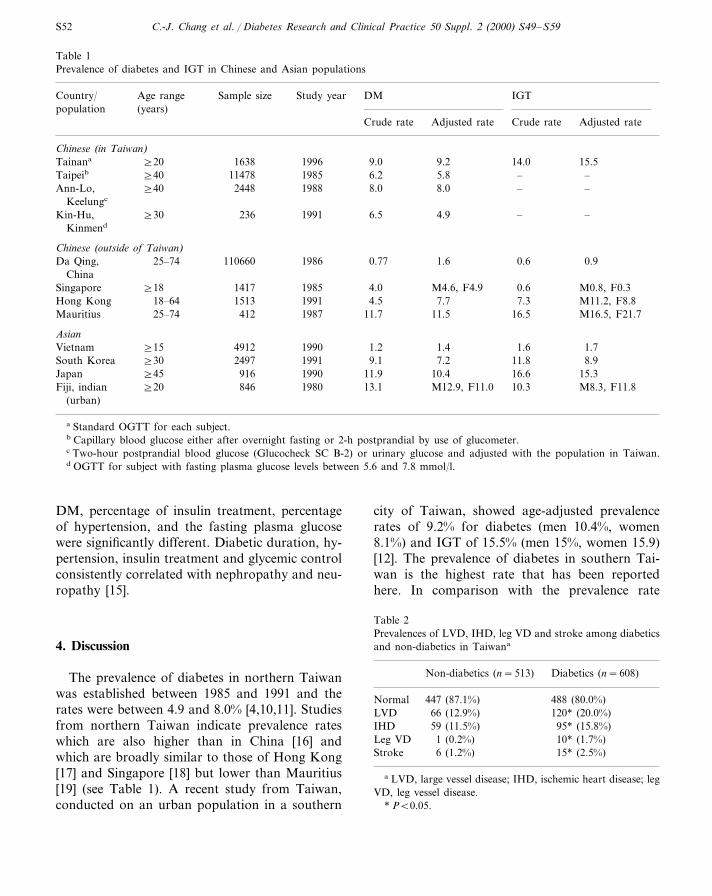
The prevalence of DM in Taiwan was estab-lished between 1985 and 1996 and the rates werebetween 4.9 and 9.2%. The prevalence of IGT was15.5% (men 15% and women 15.9%) (see Table 1).The prevalence of DM and IGT increased signifi-cantly with age for both genders [4,10–12]. Thesignificant factors associated with newly diag-nosed DM were age, BMI (WHR), family historyof DM, systolic blood pressure (hypertension),physical activity and serum triglyceride levels[4,10–12].
The prevalence of LVD in DM and non-dia-betic subjects were 20.0 and 12.9%, respectively.The diabetics had a significantly higher prevalenceof LVD than non-diabetic subjects. Among dia-betics, 15.8% had IHD, 1.7% leg VD and 2.5%stroke. In non-diabetics, the prevalence of theaforementioned macroangiopathies were 11.5, 0.2and 1.2%, respectively. The diabetics had signifi-cantly higher prevalences of IHD, leg VD andstroke than non-diabetics (see Table 2). The mostsignificant risk factor associated with the LVDwas serum cholesterol. No risk factor was signifi-cantly associated with the development of stroke.Cholesterol and HbA1c were significantly associ-ated with development of IHD. Cigarette smokingand female gender were significantly associatedwith leg VD [13].
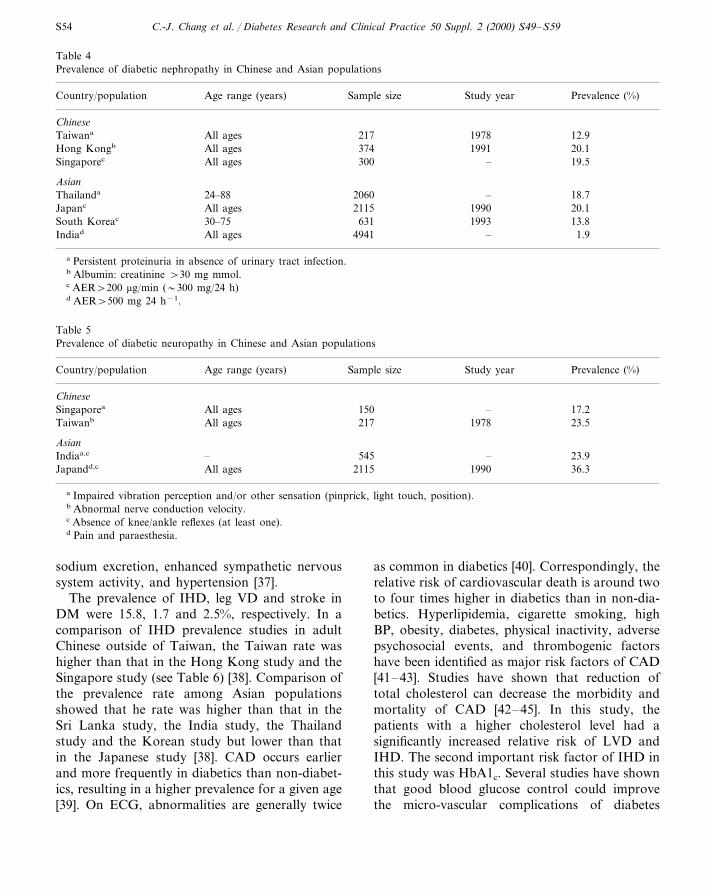
The prevalence of DR was 35.0% (backgroundDR 30%, preproliferative DR 2.8% and prolifera-tive DR 2.2%, respectively) (see Table 3). Theprevalence of DM for previously and newly diag-nosed diabetics were 45.2 and 28.3% (men 42.8 vs.33.3% and women 47.5 vs. 24.8%), respectively.Previously diagnosed diabetics had higher preva-lence of DR than newly diagnosed diabetics, andthese finding were particular prominent in women(Fig. 1). From multiple logistic regression analy-sis, duration of DM was the most important riskfactors related to DR. Diabetic subjects treatedwith insulin had a higher risk of developing DRthan those treated with diet control [14].
The prevalence of nephropathy and neuropathywere 12.9 and 23.5%, respectively (see Tables 4and 5). For those patients with and those withoutnephropathy and neuropathy, the duration of
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59S52
Table 1Prevalence of diabetes and IGT in Chinese and Asian populations
Age range Sample size Study yearCountry/ DM IGTpopulation (years)
Crude rate Adjusted rate Crude rate Adjusted rate
Chinese (in Taiwan)1638 1996 9.0]20 9.2Tainana 14.0 15.5
11478 1985 6.2 5.8Taipeib –]40 –]40 2448 1988 8.0 8.0Ann-Lo, – –
Keelungc
Kin-Hu, ]30 236 1991 6.5 4.9 – –Kinmend
Chinese (outside of Taiwan)25–74Da Qing, 110660 1986 0.77 1.6 0.6 0.9
China1417 1985 4.0Singapore M4.6, F4.9]18 0.6 M0.8, F0.3
Hong Kong 18–64 1513 1991 4.5 7.7 7.3 M11.2, F8.8412Mauritius 198725–74 11.7 11.5 16.5 M16.5, F21.7
Asian4912 1990Vietnam 1.2]15 1.4 1.6 1.72497 1991South Korea 9.1]30 7.2 11.8 8.9
916 1990 11.9]45 10.4Japan 16.6 15.3]20 846 1980 13.1 M12.9, F11.0 10.3 M8.3, F11.8Fiji, indian
(urban)
a Standard OGTT for each subject.b Capillary blood glucose either after overnight fasting or 2-h postprandial by use of glucometer.c Two-hour postprandial blood glucose (Glucocheck SC B-2) or urinary glucose and adjusted with the population in Taiwan.d OGTT for subject with fasting plasma glucose levels between 5.6 and 7.8 mmol/l.
DM, percentage of insulin treatment, percentageof hypertension, and the fasting plasma glucosewere significantly different. Diabetic duration, hy-pertension, insulin treatment and glycemic controlconsistently correlated with nephropathy and neu-ropathy [15].
4. Discussion
The prevalence of diabetes in northern Taiwanwas established between 1985 and 1991 and therates were between 4.9 and 8.0% [4,10,11]. Studiesfrom northern Taiwan indicate prevalence rateswhich are also higher than in China [16] andwhich are broadly similar to those of Hong Kong[17] and Singapore [18] but lower than Mauritius[19] (see Table 1). A recent study from Taiwan,conducted on an urban population in a southern
city of Taiwan, showed age-adjusted prevalencerates of 9.2% for diabetes (men 10.4%, women8.1%) and IGT of 15.5% (men 15%, women 15.9)[12]. The prevalence of diabetes in southern Tai-wan is the highest rate that has been reportedhere. In comparison with the prevalence rate
Table 2Prevalences of LVD, IHD, leg VD and stroke among diabeticsand non-diabetics in Taiwana
Non-diabetics (n=513) Diabetics (n=608)
447 (87.1%)Normal 488 (80.0%)LVD 66 (12.9%) 120* (20.0%)
95* (15.8%)IHD 59 (11.5%)1 (0.2%) 10* (1.7%)Leg VD
Stroke 6 (1.2%) 15* (2.5%)
a LVD, large vessel disease; IHD, ischemic heart disease; legVD, leg vessel disease.
* PB0.05.
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59 S53
Table 3Prevalence and severity of diabetic retinopathy among newly and previously diagnosed diabetica
Previously diagnosed diabetics TotalRetinopathy Newly diagnosed diabetics
% No.No. % No. %
145Absent 75.9 196 58.4 344 65.023.6 120 35.745 165Background 30.00.5 14 4.2Pre-proliferative 151 2.80 6 1.80 6Proliferative 2.2
a Fisher’s exact test, PB0.005.
among Asian populations (see Table 1), the ratewas higher than that in a Vietnamese study [20],the Korean study [21], close to that of theJapanese study [22], but lower than that in the FijiAsian Indian study [23]. In a comparison withIGT prevalence studies in adult Chinese outsideof Taiwan, the rate was higher than that in the DaQing, China study, [16] the Singapore study, [18]and the Hong Kong study, [17] but close to thatof the Mauritius study [19]. Comparing the preva-lence rate among Asian populations showed thatthe Taiwan rate was higher than that in theVietnamese study, [20] the Korean study, [21] andthe Fiji Asian Indians study, [23] but close to thatof the Japanese study [22].
Studies in different Chinese populations whohave similar genetic characteristics have shownsubstantial variation in the prevalence of diabetesand IGT. This result indicates that environmentalfactors may play an important role, since thelevels of westernization were very different amongthe Chinese in these areas.
From the results of multiple logistic regressionin Taiwan study, the significant risk factors asso-ciated with newly diagnosed diabetes were age,family history of DM, BMI, SBP, physical activ-ity and TG [4,10–12]. Predictive factors forNIDDM in Chinese population are now quitewell described and appear similar to those de-scribed for other populations. These factors havebeen described in studies reported from Taiwan[4,10–12], China [16] and Mauritius [19], as wellas from Hong Kong [17]. Increasing age, obesity,central obesity and a positive family history ofdiabetes are all major factors. Age as an indepen-dent predictor of diabetes has been reported in
many studies [24,25]. Family history of DM as asignificant predictor for diabetes has also beendemonstrated in several studies [26,27]. Physicalinactivity has been less thoroughly examined buthas been shown to be important in Mauritius [19]and Taiwan [12]. Many prospective studies havealso shown that higher physical activity can re-duce the risk of diabetes [28,29]. The mechanismmay be related to increasing insulin sensitivity inskeletal muscle caused by physical activity [30]. Inaddition, BMI [26,27,31], SBP [11,12,31,32] andTG [31,33] have also been associated with theprevalence of diabetes from many studies. It couldbe explained by insulin resistance and hyperinsu-linemia suggested by Reaven in his Banting lec-ture in 1988 [34] and from many other studies[35,36]. The proposed mechanism is that obesesubjects are resistant to insulin-stimulated glucoseuptake, which in turn leads to an increase ininsulin concentration, enhanced hepatic very-low-density lipoprotein triglyceride secretion and hy-pertriglyceridemia and lead to a reduction of
Fig. 1. Comparison of the prevalence of retinopathy betweennewly and previously diagnosed diabetics by gender.
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59S54
Table 4Prevalence of diabetic nephropathy in Chinese and Asian populations
Sample size Study year Prevalence (%)Country/population Age range (years)
Chinese217 1978 12.9Taiwana All ages374 1991All ages 20.1Hong Kongb
300 – 19.5Singaporec All ages
Asian2060 – 18.7Thailanda 24–882115 1990All ages 20.1Japanc
631 1993South Koreac 13.830–754941 – 1.9All agesIndiad
a Persistent proteinuria in absence of urinary tract infection.b Albumin: creatinine \30 mg mmol.c AER\200 mg/min (�300 mg/24 h)d AER\500 mg 24 h−1.
Table 5Prevalence of diabetic neuropathy in Chinese and Asian populations
Country/population Sample sizeAge range (years) Study year Prevalence (%)
ChineseSingaporea 150All ages – 17.2
All agesTaiwanb 217 1978 23.5
Asian–Indiaa,c 545 – 23.9
2115 1990All ages 36.3Japandd,c
a Impaired vibration perception and/or other sensation (pinprick, light touch, position).b Abnormal nerve conduction velocity.c Absence of knee/ankle reflexes (at least one).d Pain and paraesthesia.
sodium excretion, enhanced sympathetic nervoussystem activity, and hypertension [37].
The prevalence of IHD, leg VD and stroke inDM were 15.8, 1.7 and 2.5%, respectively. In acomparison of IHD prevalence studies in adultChinese outside of Taiwan, the Taiwan rate washigher than that in the Hong Kong study and theSingapore study (see Table 6) [38]. Comparison ofthe prevalence rate among Asian populationsshowed that he rate was higher than that in theSri Lanka study, the India study, the Thailandstudy and the Korean study but lower than thatin the Japanese study [38]. CAD occurs earlierand more frequently in diabetics than non-diabet-ics, resulting in a higher prevalence for a given age[39]. On ECG, abnormalities are generally twice
as common in diabetics [40]. Correspondingly, therelative risk of cardiovascular death is around twoto four times higher in diabetics than in non-dia-betics. Hyperlipidemia, cigarette smoking, highBP, obesity, diabetes, physical inactivity, adversepsychosocial events, and thrombogenic factorshave been identified as major risk factors of CAD[41–43]. Studies have shown that reduction oftotal cholesterol can decrease the morbidity andmortality of CAD [42–45]. In this study, thepatients with a higher cholesterol level had asignificantly increased relative risk of LVD andIHD. The second important risk factor of IHD inthis study was HbA1c. Several studies have shownthat good blood glucose control could improvethe micro-vascular complications of diabetes
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59 S55
[46,47]. Our results also implied that good bloodglucose control is extremely important in decreas-ing IHD in diabetic patients. In a comparison ofleg VD (PVD) prevalence studies among theAsian population, the Taiwan rate was lower thanthat in the India study, the Sri Lanka study andthe Korean study (see Table 7) [38]. PVD isstrongly related to cigarette smoking [48,49]. Wefound that smoking patients had a significantlyincreased relative risk of leg VD compared withnonsmoking patients. Women diabetic subjectsalso had an increased risk of developing leg VDcompared with men in this study. The reason whyneeds further exploration.
Epidemiologic studies of DR have been con-ducted among different populations in many areas
of the world. According to the WHO study [8],the prevalence of retinopathy varies greatly fromone country to another, even when corrected forage and duration of diabetes. A study from north-ern Taiwan showed a prevalence of 35% for DRin NIDDM subjects and was not remarkablydifferent compared with Asian and Western stud-ies (see Table 8) [38]. Despite different studyprocedures and populations, several factors, in-cluding duration of diabetes, age at onset of dia-betes, age at examination, type of diabetestreatment, control of diabetes hypertension,proteinuria, serum creatinine level, serum choles-terol level, and BMI have been found to correlatewith the prevalence of DR. The duration of dia-betes and the prevalence and severity of DR were
Table 6CHD in diabetes in Chinese and Asian populations
Age range (years) Sample sizeCountry/population Study year Prevalence (%)
Chinese1975 24.242235–54Hong Konga,b
]18 117Singaporea,b 1984 2.8]40 21.8479North Taiwana,b 1986
Southern Taiwana,b ]20 1638 1996 20.3
AsianAll ages 18.5Indiaa,c –4941
12.0All age 500 –Sri Lankab
24–88 2060Thailanda,c – 10.5Japanb 1960976All ages 31.6
30–75South Koreab 1993 12.6631
a Past history of angina, myocardial infarction, stroke or bypass surgery.b ECG coronary probable and/or coronary possible (Minnesota Code).c Ischaemic ECG change (further indefined).
Table 7PVD in diabetes in Chinese and Asian populations
Country/population Age range (years) Sample size Study year Prevalence (%)
Chinese]40Northern Taiwana,b 479 1986 1.7
AsianIndiab,c 4941All ages – 3.9
All ages 500 –Sri lankaa,b 5.630–75 631South Koreab 1993 5.9
a Intermittent claudication.b Absent arterial pulses on feet and/or amputation.c Ankle: brachial pressure index B0.9.
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59S56
Table 8Prevalence of diabetic retinopathy in Chinese and Asian populations
Sample size Study year All retinopatyh (%)Country/population Age range (years)
Chinese114 1995 33.0Chinaa All ages422 197535–54 32.5Hong Konga
300 –Singaporea 38.0All ages527 1985]40 34.9Taiwana
Asian6792 –All ages 34.1Indiaa
Pakistana,b 3000All ages – 26.01003 –All ages 31.3Sri Lankaa
24–88Thailandb 2060 – 32.1976 1960Japana 33.0All ages631 199330–75 35.2South Koreaa
a Direct and/or indirect ophthalmoscopy with mydriasis.b Fundus photography.
closely associated in the northern Taiwan study.The longer the duration of diabetes, the higher theprevalence of total DR. The prevalence of totalDR were 29.1% for those subjects who had dia-betes for less than 5 years, and 23.0% for subjectsin whom diabetes was newly diagnosed. Similarresults have also been demonstrated in other stud-ies [50,51]. Some studies found that the durationof diabetes is the most crucial factor for total DR.[52,53].
The prevalence of nephropathy and neuropathyin the northern Taiwan study were 12.9 and23.5%, respectively. For those patients with andthose without nephropathy and neuropathy, theduration of DM, percentage of insulin treatment,percentage of hypertension, and fasting plasmaglucose levels were significantly different. Diabeticduration, hypertension, insulin treatment andglycemic control consistently correlated withnephropathy and neuropathy. In a comparison ofthe nephropathy prevalence studies in the Chineseoutside of Taiwan, the Taiwan rate was lowerthan that in the Singapore study and the HongKong study (see Table 4). Comparing of theprevalence rate among Asian populations (seeTable 4) showed that the rate was higher than theIndia study and close to that of the Korean studybut lower than the Thailand and Japanese studies[38]. Proteinuria was 15 times more prevalent in
diabetics than in non-diabetics [54]. Disease dura-tion was a major determinant of nephropathy[8,54,55] and other factors included cholesterollevels [8], blood pressure [8,56], glycemic control[56] and persistent microalbuminuria [57,58]. Theprevalence of hypertension was higher amongNIDDM patients with proteinuria in the northernTaiwan study. It was well-established that thepresence of hypertension can aggravate diabeticnephropathy and retinopathy [59,60]. However,its role in neuropathy is still ambiguous.
A previous review summarized several olderclinic-based studies with prevalence of variousneuropathies ranging from 20 to 100% [61]. Aconsensus conference, convened in 1988 in SanAntonio, Texas [62] made recommendations forthe standardization of neuropathy endpoints. Sev-eral population-based studies with the prevalenceof neuropathy ranged from 10.5 to 32.1% [63–66].The prevalence of neuropathy was 17.2% in thenorthern Taiwan study. In comparing the neu-ropathy prevalence studies in Chinese outside ofTaiwan and Asian populations, the Taiwan ratewas higher than that in the Singapore study andclose to that of the India study but lower thanthat of the Japanese study (see Table 5). Theprevalence of diabetic neuropathy was examinedin a recent multicenter study in the UK involving3949 hospital-treated patients with NIDDM.
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59 S57
Neuropathy was present in 32.1% in NIDDMpatients and was positively correlated with ageand duration of diabetes [67]. There is very littleinformation using the current batteries of teststhat can be used to estimate the risk of neuropa-thy in unselected populations of diabetic patients,whether neuropathy risk increases like that ofretinopathy, or plateaus like nephropathy, is animportant but unanswered question.
References
[1] WHO Ad Hoc Diabetes Reporting Group, H. King, M.Rewers, Global estimates for prevalence of diabetes melli-tus and impaired glucose tolerance in adults, Diabetes.Care. 16 (1993) 157–177.
[2] Department of Health, Health and Vital Statistics. I.General Health Statistics, Taipei, Republic of China,Department of Health, Executive Yuan, 1996.
[3] National Diabetes Data Group, Classification and diag-nosis of diabetes mellitus and other categories of glucoseintolerance, Diabetes 28 (1979) 1039–1057.
[4] T.Y. Tai, C.L. Yang, C.J. Chang, et al., Epidemiology ofdiabetes mellitus among adults in Taiwan, ROC, J. Med.Assoc. Thailand 70 (Suppl. 2) (1987) 42–48.
[5] WHO Study Group on Diabetes Mellitus, Diabetes melli-tus, WHO Technical Report Series 727, Geneva, 1985, pp.9–12.
[6] World Health Organization, Hypertension and coronaryheart disease: classification and criteria for epidemiologi-cal study, WHO Technical Report Series 168, Geneva,1959.
[7] R.S. Paffenbarger, S.N. Blair, I.M. Lee, R.T. Hyde, Mea-surement of physical activity to assess health effects infree-living populations, Med. Sci. Sport Exerc. 25 (1993)60–70.
[8] World Health Organization, Multinational study of vas-cular disease in diabetes: prevalence of small vessel andlarge vessel disease in diabetic patients from 14 centers,Diabetologia 28 (1985) 615–640.
[9] R.C. Chen, S.M. Sung, C.F. Chen, C.J. Tzeng, I.N. Lien,T.P. Hung, Normal motor nerve conduction velocityamongst Chinese in Taiwan, J. Formos. Med. Assoc. 77(1978) 394–401.
[10] J.D. Lin, W.B. Shieh, M.J. Hung, H.S. Hung, Diabetesmellitus and hypertension based on the family history and2-h postprandial blood sugar in the Ann-Lo district(Northern Taiwan), Diabetes Res. Clin. Pract. 20 (1993)75–85.
[11] P. Chou, M.J. Liao, H.S. Kuo, K.H. Hsiao, S.T. Tsai, Apopulation survey on the prevalence of diabetes in Kin-Hu, Kinmen, Diabetes Care 17 (1994) 1055–1058.
[12] F.H. Lu, Y.C. Yang, J.S. Wu, C.H. Wu, C.J. Chang, Apopulation-based study of the prevalence and associated
factors of diabetes in southern Taiwan, Diabet. Med. 15(1998) 564–572.
[13] C.C. Fu, C.J. Chang, C.H. Tseng, et al., Development ofmacrovascular diseases in NIDDM patients in northernTaiwan, Diabetes Care 16 (1993) 137–143.
[14] M.S. Chen, C.J. Kao, C.J. Chang, T.J. Wu, C.C. Fu, C.J.Chen, T.Y. Tai, Prevalence and risk factors of diabeticretinopathy among non-insulin-dependent diabetic sub-jects, Am. J. Ophthalmol. 114 (1992) 723–731.
[15] T.Y. Tai, C.H. Tsneg, S.M. Sung, R.F. Huang, C.J.Chen, S.H. Tsai, Retinopathy, neuropathy and nephropa-thy in non-insulin-dependent diabetic patients, J. Formos.Med. Assoc. 90 (1991) 936–940.
[16] S.R. Pan, Y.H. Hu, G.W. Li, P.A. Liu, P.H. Bennett,B.V. Howard, Impaired glucose tolerance and its relation-ship to ECG-indicated coronary heart disease and riskfactors among Chinese-Da Qing IGT and diabetes study,Diabetes Care 16 (1993) 150–156.
[17] C.S. Cockram, J. Woo, E. Lau, et al., The prevalence ofdiabetes mellitus and impaired glucose tolerance amongHong Kong Chinese adults of working age, Diabetes Res.Clin. Pract. 21 (1993) 67–73.
[18] A.C. Thai, P.P.B. Yeo, K.C. Ln, K. Hung, W.Y. Ng,K.F. Lui, J.S. Cheas, Diabetes mellits and its chroniccomplications in Singapore: an increasing healthcareproblem, Ann. Acad. Med. Singapore 19 (1990) 517–523.
[19] G.K. Dowse, P.Z. Zimmet, H. Gareeboo, et al., Abdomi-nal obesity and physical inactivity as risk factors forNIDDM and impaired glucose tolerance in Indian, Gre-ole and Chinese Mauritians, Diabetes Care 14 (1991)271–282.
[20] P.S. Quoc, M.A. Charles, N.H. Cuong, et al., Bloodglucose distribution and prevalence of diabetes in Hanoi,Am. J. Epidemiol. 139 (1994) 713–722.
[21] Y. Park, H. Lee, C.S. Koh, H. Min, K. Yoo, Y. Kim, Y.Shin, Prevalence of diabetes and IGT in YonchonCounty, South Korea, Diabetes Care 48 (1995) 545–548.
[22] A. Sekikawa, M. Tominaga, K. Takahashi, et al., Preva-lence of diabetes and impaired glucose tolerance in Funa-gata area, Japan, Diabetes Care 16 (1993) 570–574.
[23] P. Zimmet, R. Taylor, P. Ram, H. King, G. Sloman, L.R.Raper, D. Hunt, Prevalence of diabetes and impairedglucose tolerance in the biracial (Melanesian and Indian)population of Fiji: a rural–urban comparison, Am. J.Epidemiol. 118 (1983) 673–688.
[24] R.B. Lipton, Y. Liao, R.S. Cooper, D. McGee, Determi-nants of incident non-insulin-dependent diabetes mellitusamong blacks and whites in a national sample: theNHANES I epidemiologic follow-up study, Am. J. Epi-demiol. 138 (1993) 826–839.
[25] P.W. Wilson, K.M. Anderson, W.B. Kannel, Epidemiol-ogy of diabetes mellitus in the elderly: The FraminghanStudy, Am. J. Med. 80 (Suppl. 5A) (1986) 3–9.
[26] W.J. Butler, L.D. Ostrander, W.J. Carman, D.E. Lam-phier, Diabetes mellitus in Techmseh, Michigan: preva-lence, incidence, and associated conditions, Am. J.Epidemiol. 116 (1982) 971–980.
C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59S58
[27] W.C. Knowler, P.H. Bennett, R.F. Hamman, M. Miller,Diabetes incidence and prevalence in Pima Indians: a19-fold greater incidence than in Rochester, Minnesota,Am. J. Epideniol. 108 (1978) 497–505.
[28] S.P. Helmrich, D.R. Ragland, R.W. Leng, R.S. Paffen-barger, Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus, N. Engl. J. Med. 325(1991) 147–152.
[29] J.E. Manson, E.B. Rimm, M.J. Stampfer, et al., Physicalactivity and incidence of non-insulin-dependent diabetesmellitus in women, Lancet 338 (1991) 774–778.
[30] J.T. Devlin, Effects of exercise on insulin sensitivity inhumans, Diabetes Care 15 (1992) 1690–1693.
[31] J.H. Medalie, C.M. Papier, M.A. Gloodbourt, J.B. Her-man, Major factors in the development of diabetes melli-tus in 10 000 men, Arch. Intern. Med. 135 (1975)811–817.
[32] P.A. Morales, B.D. Mitchell, R.A. Valdez, H.P. Hazuda,M.P. Stern, S.M. Haffner, Incidence of NIDDM andimpaired glucose tolerance in hypertensive subjects: TheSan Antonio Heart Study, Diabetes 42 (1993) 154–161.
[33] E. Barrett-Connor, S.M. Grndy, M.J. Holdbrook, Plasmalipids and diabetes mellitus in an adults community, Am.J. Epidemiol. 115 (1982) 657–663.
[34] G.M. Reaven, Banting lecture : role of insulin resistancein human disease, Diabetes 37 (1988) 1595–1607.
[35] R.A. DeFronzo, E. Ferrannini, Insulin resistance: a mul-tifaceted syndrome responsible for NIDDM, obesity, hy-pertension, dyslipidemia, and atherosclerotic cardio-vascular disease, Diabetes Care 14 (1991) 173–194.
[36] G.M. Reaven, H. Lithell, L. Landsberg, Hypertensionand associated metabolic abnormalities: the role of insulinresistance and the sympathoadrenal system, N. Engl. J.Med. 334 (1996) 374–381.
[37] J.M. Flback, J.R. Sowers, Epidemiologic and clinicalaspects of insulin resistance and hyperinsulinemia, Am. J.Med. 91 (Suppl. 1A) (1991) 115–215.
[38] A.F. Amos, D.J. McCarty, P. Zimmet, The rising globalburden of diabetes and its complications: estimate andprojection to the year 2010, Diabet. Med. 14 (1997)S7–S85.
[39] W.B. Kannel, D.L. MecGee, Diabetes and glucose toler-ance as risk factors for cardiovascular disease, the Fram-ingham Study, Diabetes Care 2 (1979) 920–926.
[40] E. Barrett-Connor, T. Orchard, Diabetes and heart dis-ease, in: M.I. Harris, R.F. Hmmah (Eds.), Diabetes inAmerica. NIH Publication XVI, 1985, pp. 1–41.
[41] The Lipid Research Clinics Coronary Primary PreventionTrial Results 1. Reduction in incidence of coronary heartdisease, J. Am. Med. Assoc. 251 (1984) 351–364.
[42] M.H. Frick, O. Elo, K. Haapa, et al., Helsinki HeartStudy — primary prevention trial with gemfibrozil inmiddle-aged men with dyslipidemia, N. Engl. J. Med. 317(1987) 1237–1245.
[43] D.H. Blankenhom, S.A. Nessim, R.L. Johnson, M.E.Sanmacro, S.P. Azen, L. Cashin-Hemphill, Beneficial ef-fects of combined colestipol-niacin therapy on coronary
atherosclerosis and coronary venous bypass grafts, J. Am.Med. Assoc. 257 (1987) 3233–3240.
[44] Multiple Risk Factor Intervention Trial Research Group,Multiple risk factor intervention trial. Risk factor changesand mortality results, J. Am. Med. Assoc. 248 (1982)1465–1477.
[45] W.D. Stamler, J.D. Neaton, Prevalence and prognosticsignificance of hypercholesterolemia in men with hyper-tension: prospective data on the primary screenees of themultiple risk factor intervention trial, Am. J. Med. 80(Suppl. 2A) (1986) 33–36.
[46] R. Engerman, J.J. Bloodworth, S. Nelson, Relationshipof microvascular disease in diabetes to metabolic control,Diabetes 26 (1977) 760–769.
[47] P. Raskin, J. Rosenstock, Blood glucose control anddiabetic complications, Ann. Intern. Med. 105 (1986)254–263.
[48] R.B. Paisey, G. Arredondo, A. Villalobos, O. Lozaano,L. Guevara, S. Kelly, Association of differing dietary,metabolic, and clinical risk factors with macrovascularcomplications of diabetes: a prevalence study of 503Mexican type II diabetic subjects I, Diabetes Care 7(1984) 421–427.
[49] UK Prospective Diabetes Study: 6, Complications innewly diagnosed type 2 diabetic patients and their associ-ation with different clinical and biochemical risk factors,Diabetes Res. 13 (1990) 1–11.
[50] The Wisconsin Epidemiologic Study of DiabeticRetinopathy, III. Prevalence and risk of diabetic retinopa-thy when age at diagnosis is 30 or more years, Arch,Ophthalmol, 102 (1984) 527–532.
[51] L.M. Aiello, L.I. Rand, J.C. Briones, M.Z. Wafai, J.G.Sebestyen, Diabetic retinopathy in Joslin clinic patientswith adult-onset diabetes, Ophthalmology 88 (1981) 619–623.
[52] I.J. Constable, M.W. Knuiman, T.A. Welborn, R.L.Cooper, K.M. Stantion, V.J. McCann, G.C. Grose, As-sessing the risk of diabetic retinopathy, Am. J. Ophthal-mol. 97 (1984) 53–61.
[53] B. Jerneld, P. Algvere, Relationship of duration and onsetof diabetes to prevalence of diabetic retinopathy, Am. J.Ophthalmol. 102 (1986) 431–437.
[54] S.A. Kamenetsky, P.H. Bannett, S. Dippe, M. Miller,P.M. Le Compte, A clinical and histologic study ofdiabetic nephropathy in the Pimas Indians, Diabetes 23(1974) 61–64.
[55] W.H. Hemman, S.M. Teutsch, Kidney diseases associatedwith diabetes, in: M.I. Harrris, R.F. Hammah (Eds.),Diabetes in America. NIH Publlication XIV, 1985, pp.1–31.
[56] C.E. Mogensen, C.K. Christensen, Predicting diabeticnephropathy in insulin-dependent diabetes, N. Engl. J.Med. 321 (1982) 1430–1432.
[57] R.J. Jarrett, G.C. Viberti, A. Argyropoulos, et al., Mi-croalbuminuria predicts mortality in non-insulin-depen-dent diabetics, Diabet. Med. 1 (1984) 17–19.

C.-J. Chang et al. / Diabetes Research and Clinical Practice 50 Suppl. 2 (2000) S49–S59 S59
[58] C.E. Mogensen, R.W. Bilous, D. Mackintosch, J.J. Bend-ing, H. Keen, Long term correction of hyperglycemia andprogression of renal failure in insulin-dependent diabetes,Br. Med. J. 286 (1983) 598–621.
[59] J.M. Sprafke, A.P.M. Bender, H.G. Jagger, Prevalence ofhypertension and associated risk factors among diabeticindividuals: the three-city study, Diabetes Care 11 (1982)685–688.
[60] C.E. Mogensen, Long-term antihypertensive treatmentinhibiting progression of diabetic nephropathy, Br. Med.J. 285 (1982) 685–688.
[61] D.A. Greene, A.A.F. Sima, M.A. Pfeifer, Neuropathy, in:C.E. Mogensen, E. Standl (Eds.), Prevention and Treat-ment of Diabetic Late Complications, Wlater de Gruyter,Berlin, 1989, pp. 93–150.
[62] Consensus Statement, Report and recommendations ofthe San Antonio conference on diabetic neuropathy, Dia-betes 37 (1988) 1000–1004.
[63] D.P. Walters, W. Gatling, M.A. Muullee, R.D. Hill,The prevalence of diabetic distal sensory neuropathy
in an English community, Diabet. Med. 9 (1992) 349–353.
[64] J.M. Lethtinen, M. Uusitupa, O. Sitonen, K. Pyorala,Prevalence of neuropathy in newly diagnosed NIDDMand non-diabetic control subjects, Diabetes 38 (1989)1307–1313.
[65] M.W. Knuiman, T.A. Welborn, V.J. McCann, K.G.Stanton, I.J. Constable, Prevalence of diabetic complica-tions in relation to risk factors, Diabetes 35 (1986) 1332–1339.
[66] P.J. Palumbo, L.R. Elveback, J.P. Whisnant, Neurologiccomplications of diabetes mellitus: transient ischemic at-tack, stroke, and peripheral neuropathy, Adv. Neurol. 19(1978) 593–601.
[67] M.J. Young, A.J.M. Boulton, A.F. Macleod, D.R.R.Williams, P.H. Sonsken, A multicentre study of theprevalence of diabetic peripheral neuropathy in theUnited Kingdom hospital clinic population, Diabetologia36 (1993) 150–154.
.
Copyright © 2022 FDOKUMEN