Epidemiologic Modeling in the Department of Defense: Capability and Coordination Opportunities
8
COMMENTARIES MILITARY MEDICINE, 179, 6:604, 2014 Epidemiologic Modeling in the Department of Defense: Capability and Coordination Opportunities LCDR Jean-Paul Chretien, MC USN*; COL Joel C. Gaydos, MC USA (Ret.)*; Dylan George, PhD†; COL Jose L. Sanchez, MC USA (Ret.)*; CDR Jeffrey T. McCollum, USPHS*; COL Julie A. Pavlin, MC USA (Ret.)*; CAPT Kevin L. Russell, MC USN* INTRODUCTION Epidemiological models increasingly help to guide preparation for and response to public health emergencies. For example, the Secretary’s Advisory Council on Public Health Prepared- ness, in the U.S. Department of Health and Human Services (HHS), formed a smallpox modeling working group in 2002 to guide national bioterrorism planning. 1 The White House consulted modeling groups supported by the National Insti- tutes of Health to assess pandemic mitigation strategies when the influenza A(H5N1) and influenza A(H1N1)pdm09 strains emerged. In the United Kingdom, authorities used modeling results in establishing control measures during the 2001 foot-and-mouth disease outbreak. 2 Real-time biosurveillance systems model epidemiologic patterns to identify possible disease outbreaks. 3 Epidemiologic models also facilitate evaluation of epidemic control measures once used, such as HIV treatment as a prevention strategy. 4 The U.S. National Strategy for Pandemic Influenza Imple- mentation Plan, issued in 2006, requires the HHS, in coordina- tion with the Department of Defense (DoD) and Department of Homeland Security, to establish a “modeling center with real-time epidemic analysis capabilities” to support policy- and decision-makers. 5 This center is currently under develop- ment in the HHS Office of the Assistant Secretary for Preparedness and Response/Biomedical Advanced Research and Development Authority (ASPR/BARDA). Within the DoD, various organizations support or conduct epidemiologic modeling, and could constitute part of the interagency network centered within HHS. However, in workshops held by the Armed Forces Health Surveillance Center (AFHSC) or the DoD Global Emerging Infections Surveillance and Response System (DoD-GEIS; now part of the AFHSC) in 2005–2010, 6–8 and by U.S. Northern Com- mand (USNORTHCOM) in 2005, participants noted that the DoD lacks formal procedures for coordinating across these programs. As a result, DoD decision-makers sometimes have received conflicting results from different models or model- ing efforts, with no procedures in place to reconcile conflicts or ensure transparency of methods, assumptions, and data across efforts. As a step toward improved epidemiologic modeling capa- bilities and coordination in the DoD, the AFHSC convened the DoD Epidemiologic Modeling Coordination Working Group (WG) in February 2013 in an effort to identify, coor- dinate, and assess current DoD efforts, and provide recom- mendations for improving them. METHODS AFHSC staff partnered with staff at the Office of the Assistant Secretary of Defense for Nuclear, Chemical, and Biological Defense Programs (OASD [NCB]) to identify DoD- and mil- itary Service-level organizations that conduct or support epi- demiologic modeling, and invited these organizations to participate in the WG. All invited organizations participated (Table I).Staff from ASPR/BARDA also participated in the WG because of its evolving role in coordinating epidemio- logic modeling across U.S. Government (USG) agencies. The WG defined “epidemiologic modeling” as using quantitative or qualitative models to make predictions about the current or future state of human population health, includ- ing disease risk and other disease-related variables, in time and space. This definition includes predictions of disease incidence, health impact, intervention effects, epidemiologic spread, agent dispersion, and disease or vector presence, among other possibilities. The specific objectives of the WG were to (1) Identify, describe, and assess the usefulness of current DoD epidemiologic modeling systems *Armed Forces Health Surveillance Center,11800 Tech Road, Suite 220, Silver Spring, MD 20904. †Division of Analytic Decision Support, Biomedical Advanced Research and Development Authority, Department of Health and Human Services, 200 Independence Avenue, S.W. Room 638G, Washington, DC 20201. The views expressed are those of the authors, and do not necessarily represent those of the Department of Defense or Department of Health and Human Services. doi: 10.7205/MILMED-D-13-00406 MILITARY MEDICINE, Vol. 179, June 2014 604 Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014. Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
-
Upload
coruniamericana -
Category
Documents
-
view
3 -
download
0
Transcript of Epidemiologic Modeling in the Department of Defense: Capability and Coordination Opportunities

COMMENTARIES
MILITARY MEDICINE, 179, 6:604, 2014
Epidemiologic Modeling in the Department of Defense:Capability and Coordination Opportunities
LCDR Jean-Paul Chretien, MC USN*; COL Joel C. Gaydos, MC USA (Ret.)*; Dylan George, PhD†;COL Jose L. Sanchez, MC USA (Ret.)*; CDR Jeffrey T. McCollum, USPHS*;
COL Julie A. Pavlin, MC USA (Ret.)*; CAPT Kevin L. Russell, MC USN*
INTRODUCTIONEpidemiological models increasingly help to guide preparation
for and response to public health emergencies. For example,
the Secretary’s Advisory Council on Public Health Prepared-
ness, in the U.S. Department of Health and Human Services
(HHS), formed a smallpox modeling working group in 2002
to guide national bioterrorism planning.1 The White House
consulted modeling groups supported by the National Insti-
tutes of Health to assess pandemic mitigation strategies when
the influenza A(H5N1) and influenza A(H1N1)pdm09 strains
emerged. In the United Kingdom, authorities used modeling
results in establishing control measures during the 2001
foot-and-mouth disease outbreak.2 Real-time biosurveillance
systems model epidemiologic patterns to identify possible
disease outbreaks.3 Epidemiologic models also facilitate
evaluation of epidemic control measures once used, such as
HIV treatment as a prevention strategy.4
The U.S. National Strategy for Pandemic Influenza Imple-
mentation Plan, issued in 2006, requires the HHS, in coordina-
tion with the Department of Defense (DoD) and Department
of Homeland Security, to establish a “modeling center with
real-time epidemic analysis capabilities” to support policy-
and decision-makers.5 This center is currently under develop-
ment in the HHS Office of the Assistant Secretary for
Preparedness and Response/Biomedical Advanced Research
and Development Authority (ASPR/BARDA).
Within the DoD, various organizations support or conduct
epidemiologic modeling, and could constitute part of the
interagency network centered within HHS. However, in
workshops held by the Armed Forces Health Surveillance
Center (AFHSC) or the DoD Global Emerging Infections
Surveillance and Response System (DoD-GEIS; now part of
the AFHSC) in 2005–2010,6–8 and by U.S. Northern Com-
mand (USNORTHCOM) in 2005, participants noted that the
DoD lacks formal procedures for coordinating across these
programs. As a result, DoD decision-makers sometimes have
received conflicting results from different models or model-
ing efforts, with no procedures in place to reconcile conflicts
or ensure transparency of methods, assumptions, and data
across efforts.
As a step toward improved epidemiologic modeling capa-
bilities and coordination in the DoD, the AFHSC convened
the DoD Epidemiologic Modeling Coordination Working
Group (WG) in February 2013 in an effort to identify, coor-
dinate, and assess current DoD efforts, and provide recom-
mendations for improving them.
METHODSAFHSC staff partnered with staff at the Office of the Assistant
Secretary of Defense for Nuclear, Chemical, and Biological
Defense Programs (OASD [NCB]) to identify DoD- and mil-
itary Service-level organizations that conduct or support epi-
demiologic modeling, and invited these organizations to
participate in the WG. All invited organizations participated
(Table I).Staff from ASPR/BARDA also participated in the
WG because of its evolving role in coordinating epidemio-
logic modeling across U.S. Government (USG) agencies.
The WG defined “epidemiologic modeling” as using
quantitative or qualitative models to make predictions about
the current or future state of human population health, includ-
ing disease risk and other disease-related variables, in time
and space. This definition includes predictions of disease
incidence, health impact, intervention effects, epidemiologic
spread, agent dispersion, and disease or vector presence,
among other possibilities.
The specific objectives of the WG were to
(1) Identify, describe, and assess the usefulness of current
DoD epidemiologic modeling systems
*Armed Forces Health Surveillance Center,11800 Tech Road, Suite 220,
Silver Spring, MD 20904.
†Division of Analytic Decision Support, Biomedical Advanced Research
and Development Authority, Department of Health and Human Services,
200 Independence Avenue, S.W. Room 638G, Washington, DC 20201.
The views expressed are those of the authors, and do not necessarily
represent those of the Department of Defense or Department of Health
and Human Services.
doi: 10.7205/MILMED-D-13-00406
MILITARY MEDICINE, Vol. 179, June 2014604
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

(2) Assess coordination across DoD epidemiological model-
ing programs
(3) Provide recommendations to advance DoD epidemiologic
modeling (i.e., to improve the utility of DoD epidemio-
logic modeling activities in supporting decision-making
among DoD users of modeling results).
WG members identified relevant DoD epidemiologic
modeling systems based on their knowledge, review of pro-
gramming within their components or offices, and queries to
DoD- and Service-level research and public health organiza-
tions about activities they support or participate in which may
meet the WG definition of epidemiologic modeling. The WG
described systems based on the following characteristics:
— Purpose
— Sponsor
— Modeling Approach
— Operational Status (mutually exclusive levels)
— Operational: The system or its results currently are
available for routine use in operations by planners or
medical personnel.
— Preoperational: The system is in development and
not yet operational.
— Operational Application (nonmutually exclusive levels):
— Planning: The system is designed for use in pre-
event planning.
— Response: The system is designed for use during
events to support response.
— Military Specificity (mutually exclusive levels)
— Military: The system currently incorporates data on
specific or generic military populations to provide
results for those populations.
— Nonmilitary: The system does not currently provide
results for military populations.
— Intervention Assessment (mutually exclusive levels)
— Intervention assessment capability: The system
allows evaluations of prevention or mitigation
actions (e.g., mitigation measures against a public
health emergency).
— No intervention assessment capability: The system
does not allow assessment of interventions.
To make a preliminary assessment of the usefulness of
modeling systems, the WG determined whether the system
is used routinely in military operations, and reviewed assess-
ments of its performance characteristics in real-world or
simulated environments in sponsor evaluations, project
reports, and published manuscripts. The WG made these sub-
jective judgments based on their knowledge of the systems
and consultation with others external to the WG who were
familiar with the systems and their applications.
The WG developed recommendations for epidemiologic
modeling during teleconferences and through e-mail commu-
nication. It reviewed previous assessments of DoD epidemi-
ologic modeling and consulted external experts involved in
those previous assessments as needed to clarify their methods
and results.
RESULTS
Description of DoD EpidemiologicModeling Systems
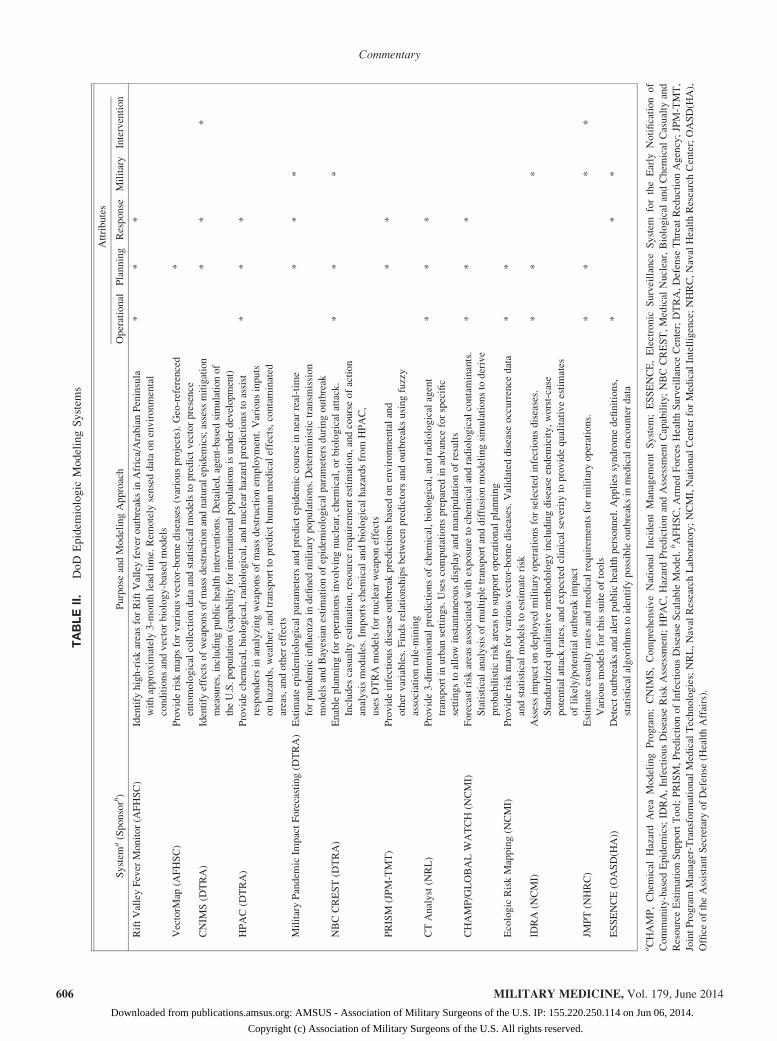
The WG identified 13 modeling systems (Table II). Four of
these focus specifically on vector-borne diseases, one focuses
on influenza-like illness, and each of the other eight includes
infectious diseases with various transmission mechanisms or
chemical or radiological agents. DoD sponsors of the systems
include health surveillance or research organizations (AFHSC,
TABLE I. Organizations Participating in the DoD Epidemiologic Modeling Capabilities Working Group
Organizationa Mission
AFHSC/Division of Integrated Biosurveillance Evaluate and identify DoD biosurveillance needs; synchronize DoD biosurveillance efforts;
and support DoD decision-makers through provision of information products, regular
communication, and as-needed consultation based on relevant biosurveillance data and information
AFHSC/GEIS Contribute to the protection of all DoD health care beneficiaries and the global community through
an integrated worldwide emerging infectious disease surveillance system
BARDA Develop and procure medical countermeasures that address the public health and medical
consequences of chemical, biological, radiological, and nuclear (CBRN) accidents, incidents
and attacks, pandemic influenza, and emerging infectious diseases
DTRA Safeguard the United States and its allies from global weapons of mass destruction threats
by integrating, synchronizing, and providing expertise, technologies, and capabilities across
all operating environments
DTRA Technical Reachback Provide WMD analysis and technical assistance 24/7 to warfighters, U.S. Government, and first
responders. Serve as a hub for pandemic modeling by interagency agreement with HHS
JPM-TMT Provide the warfighter and the Nation with innovative medical solutions to protect against and treat
emerging, genetically engineered, or unknown biothreats
OASD(NCB) Drive the capability to prevent, protect against, and respond to weapons of mass destruction threats
aAFHSC, Armed Forces Health Surveillance Center; BARDA, Biomedical Advanced Research and Development Authority; GEIS, Global Emerging
Infections Surveillance and Response System; HHS, Department of Health and Human Services; DTRA, Defense Threat Reduction Agency; JPM-TMT,
Joint Project Manager-Transformational Medical Technologies; OASD(NCB), Office of the Assistant Secretary of Defense for Nuclear, Chemical, and
Biological Defense Programs.
MILITARY MEDICINE, Vol. 179, June 2014 605
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.
TABLEII.
DoD
Epidem
iologic
ModelingSystem
s
System
a(Sponsorb)
Purpose
andModelingApproach
Attributes
Operational
Planning
Response
Military
Intervention
RiftValleyFever
Monitor(A
FHSC)
Identify
high-riskareasforRiftValleyfever
outbreaksin
Africa/ArabianPeninsula
withapproxim
ately3-m
onth
lead
time.Rem
otely
senseddataonenvironmental
conditionsandvectorbiology-based
models
**
*
VectorM
ap(A
FHSC)
Providerisk
mapsforvariousvector-bornediseases(variousprojects).Geo-referenced
entomologicalcollectiondataandstatisticalmodelsto
predictvectorpresence
*
CNIM
S(D
TRA)
Identify
effectsofweaponsofmassdestructionandnaturalepidem
ics;assess
mitigation
measures,includingpublichealthinterventions.Detailed,agent-based
simulationof
theU.S.population(capabilityforinternationalpopulationsisunder
development)
**
*
HPAC(D
TRA)
Providechem
ical,biological,radiological,andnuclearhazardpredictionsto
assist
respondersin
analyzingweaponsofmassdestructionem
ployment.Variousinputs
onhazards,weather,andtransportto
predicthuman
medicaleffects,contaminated
areas,andother
effects
**
*
MilitaryPandem
icIm
pactForecasting(D
TRA)
Estim
ateepidem
iologicalparam
etersandpredictepidem
iccoursein
nearreal-tim
e
forpandem
icinfluenza
indefined
militarypopulations.Deterministictransm
ission
modelsandBayesianestimationofepidem
iologicalparam
etersduringoutbreak
**
*
NBCCREST(D
TRA)
Enableplanningforoperationsinvolvingnuclear,chem
ical,orbiologicalattack.
Includes
casualty
estimation,resourcerequirem
entestimation,andcourseofaction
analysismodules.Im
portschem
icalandbiologicalhazardsfrom
HPAC,
usesDTRAmodelsfornuclearweaponeffects
**
*
PRISM
(JPM-TMT)
Provideinfectiousdisease
outbreak
predictionsbased
onenvironmentaland
other
variables.Findsrelationshipsbetweenpredictorsandoutbreaksusingfuzzy
associationrule-m
ining
**
CTAnalyst(N
RL)
Provide3-dim
ensionalpredictionsofchem
ical,biological,andradiologicalagent
transportin
urban
settings.Usescomputationsprepared
inadvance
forspecific
settingsto
allowinstantaneousdisplayandmanipulationofresults
**
*
CHAMP/GLOBALWATCH(N
CMI)
Forecastrisk
areasassociated
withexposure
tochem
icalandradiologicalcontaminants.
Statisticalanalysisofmultipletransportanddiffusionmodelingsimulationsto
derive
probabilisticrisk
areasto
supportoperationalplanning
**
*
EcologicRiskMapping(N
CMI)
Providerisk
mapsforvariousvector-bornediseases.Validated
disease
occurrence
data
andstatisticalmodelsto
estimaterisk
**
IDRA(N
CMI)
Assessim
pactondeployed
militaryoperationsforselected
infectiousdiseases.
Standardized
qualitativemethodologyincludingdisease
endem
icity,worst-case
potentialattack
rates,andexpectedclinicalseverityto
providequalitativeestimates
oflikely/potentialoutbreak
impact
**
*
JMPT(N
HRC)
Estim
atecasualty
ratesandmedicalrequirem
entsformilitaryoperations.
Variousmodelsforthissuiteoftools
**
**
ESSENCE(O
ASD(H
A))
Detectoutbreaksandalertpublichealthpersonnel.Applies
syndromedefinitions,
statisticalalgorithmsto
identify
possibleoutbreaksin
medicalencounterdata
**
*
aCHAMP,Chem
ical
HazardAreaModelingProgram;CNIM
S,ComprehensiveNational
IncidentManagem
entSystem
;ESSENCE,Electronic
Surveillance
System
fortheEarly
Notificationof
Community-based
Epidem
ics;ID
RA,InfectiousDisease
RiskAssessm
ent;HPAC,HazardPredictionandAssessm
entCapability;NBCCREST,Medical
Nuclear,Biological
andChem
ical
Casualty
and
ResourceEstim
ationSupportTool;PRISM,PredictionofInfectiousDisease
Scalable
Model.bAFHSC,Arm
edForces
HealthSurveillance
Center;DTRA,Defense
Threat
ReductionAgency;JPM-TMT,
JointProgram
Manager-Transform
ational
MedicalTechnologies;NRL,NavalResearchLaboratory;NCMI,NationalCenterforMedicalIntelligence;NHRC,NavalHealthResearchCenter;OASD(H
A),
Office
oftheAssistantSecretary
ofDefense
(HealthAffairs).
MILITARY MEDICINE, Vol. 179, June 2014606
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

Naval Health Research Center, Naval Research Laboratory,
Office of the Assistant Secretary of Defense for Health
Affairs [OASD (HA)]), organizations with a mission to coun-
ter weapons of mass destruction (Defense Threat Reduction
Agency [DTRA], Joint Program Manager-Transformational
Medical Technologies [JPM-TMT]), and the National Center
for Medical Intelligence (NCMI).Technical approaches also
vary widely; for example, the systems use individual-based
models (Comprehensive National Incident Management Sys-
tem [CNIMS]), deterministic transmission models (Military
Pandemic Influenza Impact Forecasting project), association
rule-mining (Prediction of Infectious Disease Scalable Model
[PRISM]), and qualitative methodologies (Infectious Disease
Risk Assessment [IDRA]), among other approaches. Nine of
the systems are operational.
Analysis of other system attributes identified multiple
capabilities for similar applications and lack of capabilities
for other applications. For example, five of the systems pro-
vide predictions for vector-borne diseases (four focusing spe-
cifically on vector-borne diseases—ecologic risk mapping
systems sponsored by NCMI and AFHSC, PRISM, and the
Rift Valley fever [RVF] Monitor; and IDRA, which includes
vector-borne and other diseases), whereas no operational sys-
tems designed for use in a response scenario currently allow
for assessment of intervention strategies specifically in mili-
tary populations, though CNIMS is developing this capability.
(The WG did identify two DoD systems designed for use in
military populations that are no longer funded or available:
the Pandemic Influenza Policy Model9 and Gryphon10).
Usefulness of DoD Epidemiologic ModelingSystems: Operational Systems
The WG found some evidence of usefulness for all of the
operational systems. For some, published evaluations are not
available, but routine use in military operations may provide
indirect evidence of their usefulness:
— The Joint Medical Planning Tool (JMPT), which began
development in 1998, was accredited in 2012 as a DoD
medical planning and programming tool after progressing
through a rigorous verification and validation process.
The DoD authorizes the JMPT for use in medical
systems analysis, logistics analysis, operational risk
assessments, and theater medical course of action
assessments. Military medical planners routinely use
the JMPT to predict the burden and types of combat
and noncombat casualties in preparing for operations.
— Like the JMPT, the Hazard Prediction and Assessment
Capability (HPAC) underwent extensive verification
and validation testing before achieving DoD accredita-
tion for modeling chemical, biological, radiological,
and nuclear (CBRN) hazardous dispersion. DTRA
Technical Reachback uses HPAC to provide hazard
analysis and technical support 24 hours per day, 7 days
per week to warfighters, government officials, and first
responders to CBRN incidents. As an example, during
July 2011 through June 2013, DTRA Reachback
responded to over 2,000 requests for information using
HPAC. A complementary system, the Nuclear Biologi-
cal Chemical Casualty and Resource Estimation Support
Tool, uses HPAC outputs to estimate casualties and med-
ical requirements. (DTRA Technical Reachback also
uses CNIMS for infectious disease modeling, though
this capability is not yet fully operational; see below.)
— CT Analyst, like HPAC, models dispersion of chemical,
biological, and radiological agents. CT Analyst focuses
on urban settings, with detailed representations of
urban geometry and fluid dynamic models. A key fea-
ture of the system is performance and storage of
modeling computations for a specific geographic set-
ting in a database before an event occurs. When an
event occurs, users can employ a lookup function to
retrieve predictions instantly (instead of performing
the modeling at that time, which would take longer).
These immediate results could prove crucial to first
responders, and the system has been used in emergency
preparations for many high-profile events and munici-
palities to enable an immediate response.
— Military planners and medical personnel routinely use
NCMI’s country- and region-specific IDRAs and eco-
logical risk maps in preparing for and conducting oper-
ations. For example, DoD policy requires medical
officers to prescribe antimalarial chemoprophylaxis
based on NCMI risk assessments,11 and force health
protection officers typically use NCMI risk assess-
ments to develop predeployment or deployed force
health protection briefings.
Military planners also use NCMI’s Chemical Hazard Area
Modeling Program (CHAMP) and GLOBAL WATCH sys-
tems to forecast chemical or radiological hazards in opera-
tional environments. Like HPAC, CHAMP forecasts hazards
based on environmental conditions. Although HPAC, as
implemented in DTRA Reachback, provides decision support
during response to an event, CHAMP provides forecasts that
consider a wide range of possible environmental conditions to
guide planning before an event occurs (e.g., where to locate a
military camp). GLOBAL WATCH provides near-term fore-
casts for hazards that would result from release of chemical
or radiological agents from facilities in areas of concern
worldwide, using daily atmospheric forecasts.
Published evaluations are available for two of the opera-
tional systems: the Rift Valley fever (RVF) Monitor and the
Electronic Surveillance System for the Early Notification of
Community-based Epidemics (ESSENCE); a summary of
these systems are given below.
RVF Monitor
RVF is a mosquito-borne viral disease of humans and animals,
which occurs throughout sub-Saharan Africa, Egypt, and the
MILITARY MEDICINE, Vol. 179, June 2014 607
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

Arabian Peninsula; outbreaks are linked to elevated rainfall
and other climatic conditions that favor emergence and trans-
mission by mosquito vectors. The RVF Monitor uses satellite
measurements of sea surface temperature, outgoing longwave
radiation, rainfall, and normalized difference vegetation index
to identify conditions favorable for relevant vector activity
months before outbreaks, and communicates warnings to host
country health authorities, international organizations, and
USG agencies and field offices. Updates are available on a
U.S. Department of Agriculture (USDA) Website (http://
www.ars.usda.gov/Business/docs.htm?docid=23464).
DoD-GEIS, the National Aeronautics and Space Adminis-
tration’s Goddard Space Flight Center, and USDA partnered
to initiate this program in 1999, following the largest
documented RVF epidemic/epizootic in the Horn of African
1997–1998. (Besides human morbidity and mortality, the
outbreak caused significant economic loss because of a ban
on livestock exports from the region.) The system predicted
conditions likely to lead to an RVF outbreak in September
2006, 3 months before a large outbreak in East Africa.12 The
prediction enabled host countries to initiate preparedness,
surveillance, and response activities approximately 2 months
earlier than during the 1997–1998 outbreak, likely reducing
the human, animal, and economic impacts.13
Early Notification of Community-based Epidemics
Researchers at the Walter Reed Army Institute of Research
(WRAIR), with support from the Johns Hopkins University
Applied Physics Laboratory, developed the initial ESSENCE
system in 1999 to improve detection of bioterrorist attack.14
The system received data daily from ambulatory encounters
in military medical treatment facilities (MTFs) in the National
Capital Area, and automatically mapped ICD-9 diagnoses to
syndrome groups and generated alerts based on statistical
algorithms comparing observed to expected syndrome counts.
Today, ESSENCE is a web-based application operated by
OASD(HA) covering all nondeployed MTFs globally
(approximately 500 facilities), and the DoD requires these
MTFs to ensure that at least two trained ESSENCE users
monitor the system.15 Though designed initially to detect
biologic agent attacks, medical personnel across the DoD use
ESSENCE daily to detect naturally occurring outbreaks and
assess trends. Facility-level users and others with enhanced
access can view identifying information on patients and pro-
viders to support epidemiologic investigation and outbreak
control, as well as clinical management of cases.
ESSENCE validation studies have reported favorable sensi-
tivity and specificity of the syndrome groupings compared to
clinical records16 or laboratory results.17 Anecdotally, ESSENCE
has facilitated detection and monitoring of numerous out-
breaks and other public health events. However, an assessment
of its usefulness during an influenza A(H1N1)pdm09 outbreak
at the U.S. Air Force Academy, conducted by the Centers for
Disease Control and Prevention (CDC), found its timeliness
and sensitivity inadequate to support effective response.18
Usefulness of DoD Epidemiologic ModelingSystems: Preoperational Systems
For some of the preoperational systems, publications have
reported favorable performance in testing or pilot applications:
— PRISM predicted dengue outbreaks 4 weeks in advance
in Peru using clinical, meteorologic, climatic, and social–
political data with positive predictive value = 0.69,
negative predictive value = 0.98, sensitivity = 0.62,
and specificity = 0.98 against previously unused inci-
dence data.19
— A preliminary version of the Military Pandemic Influ-
enza Forecasting system included epidemiologic models
using influenza-like illness (ILI) data from the influenza
A(H1N1)pdm09 pandemic for the 50 largest U.S. mili-
tary bases and surrounding civilian populations.20 The
analysis showed synchronization of epidemics between
military and local civilian populations, with an approxi-
mately 1-week lag, in most cases, from civilian to mili-
tary population peaks. An extension of this effort is
developing capabilities for epidemic curve prediction in
specific military populations.
— The developers of CNIMS have used detailed represen-
tations of parts of the United States to evaluate outbreak
detection and response measures. For example, they
assessed the performance of several ILI surveillance
strategies in Boston,21 influenza epidemic mitigation
strategies in Miami,22 and household isolation strate-
gies for influenza in Miami and Seattle.23 The CNIMS
team also provided analyses to USNORTHCOM
to support USNORTHCOM response to the influenza
A(H1N1)pdm09 pandemic; and to the U.S. Army
Surgeon General, Alabama National Guard, and
USNORTHCOM for pandemic planning.
— VectorMap, developed by WRAIR with AFHSC sup-
port, is a mapping tool that facilitates determination of
vector location and disease transmission risks through an
intuitive graphical interface. It integrates entomologic
surveillance through incorporation of global vector col-
lections data and ecologic niche modeling to determine
suitable habitats for vector presence as a proxy for
vector-borne disease risk. Several initiatives to identify
potential disease vector habitats have achieved promis-
ing results in validation studies against entomologic
collection data.24 VectorMap is web based (http://www
.vectormap.org/) and readily accessible to the general
public and military personnel to support ongoing opera-
tional risk assessments for vector-borne diseases.
Coordination across DoD EpidemiologicModeling Efforts
The WG found that the DoD does not have an established
process for coordinating the planning, development, fielding,
and evaluation of epidemiologic modeling systems, as
reported by previous U.S. military conferences.6–8 However,
MILITARY MEDICINE, Vol. 179, June 2014608
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

the WG noted that an informal professional network of pro-
gram officers and modelers spans many of the programs.
They share information on current and planned activities,
providing some coordination that could provide a foundation
for more formal coordination procedures.
Recommendations
To advance DoD epidemiologic modeling capabilities and
coordination, the WG developed four recommendations:
Recommendation 1:The DoD or DoD organizations should
establish policy and procedures to coordinate epidemiologic
modeling. The recommended relationship structure to per-
form this coordination is a network of DoD organizations
that perform or support epidemiologic modeling, including
a coordination hub. The network would serve as the DoD
focus for epidemiologic modeling-related issues, including
requests for modeling results from DoD, interagency, and
other customers, and would conduct and coordinate research
and assessment to guide the development of DoD epidemio-
logic modeling capabilities.
DoD policy establishing the network would provide the
necessary authority to carry out its mission, but the network
could form initially using more expedient means, for example,
memoranda of understanding among participating organizations
and a mutually agreed charter consistent with the missions of
participating organizations. The coordination hub could be
based at an existing DoD organization with operational epide-
miologic modeling capabilities or other useful assets. DTRA
Reachback, which already serves as the operational hub for the
Department of Homeland Security Interagency Modeling and
Atmospheric Assessment Center, and has an interagency
agreement with BARDA to support epidemiologic modeling,
might best fill this role. The WG should continue, and shift to
an active role in advancing this coordination agenda.
Recommendation 2: The nascent DoD epidemiologic
modeling network should systematically identify epidemio-
logic modeling efforts and opportunities across the DoD, and
capabilities beyond the DoD. Although several DoDWGs have
considered DoD epidemiologic modeling capabilities, there has
not been a systematic assessment of efforts and opportunities
across the DoD. Such an assessment would include representa-
tive tactical and strategic potential users of epidemiologic
modeling systems and results,25 and would identify key oppor-
tunities for epidemiologic modeling capability development
within the DoD. Paired with that study, systematic identifica-
tion and assessment of epidemiologic modeling systems,
methods, and networks beyond the DoD would highlight
potential resources for DoD epidemiologic modeling efforts,
and areas where the DoD could initiate new efforts. The WG
could undertake these tasks immediately, and transition them
to the DoD epidemiologic modeling network when it forms.
Recommendation 3: The nascent DoD epidemiologic
modeling network should address key opportunities for improv-
ing DoD epidemiologic modeling capabilities that already are
evident. The WG identified several opportunities that DoD
organizations could begin to address immediately, possibly
within their existing epidemiologic modeling programs.
These include opportunities for
— An operational modeling system for assessment of
interventions and forecasting in military populations.
AFHSC could help establish this capability in
CNIMS, which has performed several ad hoc modeling
analyses in military populations, by sharing Defense
Medical Surveillance System data and military
epidemiologic expertise.
— Common standards for verification and validation of
DoD epidemiologic modeling systems. The experience
of the JMPT and other systems that underwent a rigor-
ous DoD verification and validation process might pro-
vide lessons here.
— Common standards defining the operational readiness
of DoD epidemiologic modeling systems or the
underlying models (akin to the Technology Readiness
Level system used in DoD and other agencies and
industry sectors).
— Improved mutual understanding of capabilities among
DoD decision-makers and epidemiologic modelers. DoD
modelers could provide coordinated capabilities brief-
ings to selected decision-makers to begin the dialogue.
Recommendation 4: The AFHSC should continue to lead the
DoD Epidemiologic Modeling Coordination WG to advance
and monitor the agenda specified in Recommendations 1–3.
TheWG should develop operational plans for implementing
the recommendations and tracking and reporting progress;
and should also continue to identify, coordinate, and assess
DoD epidemiologic modeling efforts and provide recommen-
dations for improving them.
DISCUSSIONThis report validates the need for epidemiologic modeling
coordination in the DoD identified in previous meetings,6–8 and
offers new recommendations for improving coordination. It
also provides, to our knowledge, a first attempt to identify
and characterize epidemiologic modeling activities across the
DoD, and recommendations for addressing apparent needs
for DoD epidemiologic modeling capabilities. Of note, the
WG found that an important opportunity is to develop model-
ing capabilities for interventions against public health events
in military populations.
A strength of the WG effort that produced this report is
partnership between the public health and nuclear, chemical,
and biological defense communities of the DoD, represented
by WG members from OASD(HA) and OASD(NCB), respec-
tively, and their component organizations. This brings together
varied perspectives on needs for modeling coordination and
capabilities in the DoD, and may facilitate efforts to coordinate
MILITARY MEDICINE, Vol. 179, June 2014 609
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

funding and operation of epidemiologic modeling systems that
grow from the WG’s efforts.
This report is a preliminary attempt to identify and char-
acterize DoD epidemiologic modeling activities. WG mem-
bers represented offices and organizations most likely to
sponsor or conduct epidemiologic modeling, and their pro-
fessional networks extend to other DoD entities that sponsor
such efforts. The WG, however, may have failed to identify
some relevant activities. WG members believe, though, that
even if they did not identify all activities that met inclusion
criteria, the key needs identified by the WG—for improved
coordination and for some specific capabilities—likely would
remain valid. The WG also did not attempt a systematic
assessment of the usefulness of DoD epidemiologic modeling
systems, but did conduct a largely informal and expedient,
preliminary assessment to identify key needs and motivate a
more comprehensive analysis. The proxies of system useful-
ness (e.g., routine use of operational systems, or reported
performance metrics for preoperational systems) cannot sub-
stitute for impact measures. As noted in Recommendation 2,
the need for a more thorough evaluation remains, and could
identify important opportunities for advancing epidemiologic
modeling not captured in the present report.
One recommendation of the WG that warrants special
attention is the need for improved mutual understanding
among epidemiologic modelers and DoD decision-makers
who might use the results of such modeling efforts. Improv-
ing coordination and technical modeling capabilities cannot
achieve improvements in the ultimate outcomes of interest
for the DoD—such as public health, security, or financial
costs—if decision-makers do not use the results, whether
because they lack awareness of DoD modeling capabilities
or confidence in them as decision-support tools. Proponents
of epidemiologic modeling must take care to identify, to
those who may use the results for decision-making, the key
assumptions and limitations of their approaches, a recognized
good practice in epidemiologic modeling.26 Although
modelers may fear that pointing out possible weaknesses in
their methods may undermine confidence in their results,
decision-makers likely will prefer to incorporate these con-
siderations into their analysis. Decisions based on modeling
where limitations are hidden and key assumptions not made
explicit may not only fail to achieve the desired outcomes but
could cause deep distrust of epidemiological modeling as a
guide to decision-making if perceived as misinforming the
decision-making process.
The WG calls on those who support or conduct epidemio-
logic modeling in the DoD to take the first step in building
partnerships with DoD decision-makers. The effort to collab-
orate more closely must be mutual, but for decision-makers
to reciprocate, the DoD epidemiologic modeling community
must convince them of the relevance of these efforts to the
problems that decision-makers confront, and of the modeling
community’s commitment to educating decision-makers on
the capabilities and limitations of their methods.
ACKNOWLEDGMENT
We thank representatives of epidemiologic modeling programs for sharing
information on their efforts, and Dr. Rohit Chitale for encouraging the
working group.
REFERENCES
1. McKenzie FE: Smallpox models as policy tools. Emerg Infect Dis 2004;
10: 2044–7. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC2483404/; accessed July 8, 2013.
2. Kitching RP, Thursfield MV, Taylor NM: Use and abuse of mathematical
models: an illustration from the 2001 foot and mouth disease epidemic in
the United Kingdom. Rev Sci Tech 2006; 25: 293–331.
3. Fricker RD: Some methodological issues in biosurveillance. Stat Med
2011; 30: 403–15.
4. Boily MC, Masse B, Alsallaq R, et al: HIV treatment as prevention:
considerations in the design, conduct, and analysis of cluster random-
ized controlled trials of combination HIV prevention. PLoS Med 2012;
9:e1001250. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC3393676/; accessed July 8, 2013.
5. Homeland Security Council: National Strategy for Pandemic Influenza.
Implementation Plan. The White House, May 2006. Available at: http://
www.flu.gov/planning-preparedness/federal/pandemic-influenza-imple
mentation.pdf; accessed July 8, 2013.
6. Chretien JP, Linthicum KJ, Pavlin JA, Gaydos JC, Malone JL: Epidemi-
ologic applications of emerging infectious disease modeling to support
US military readiness and national security. Emerg Infect Dis 2006.
Available at: http://wwwnc.cdc.gov/eid/article/12/1/05-1214_article.htm;
accessed July 8, 2013.
7. Feighner BH, Eubank S, Glass RJ, Davey VJ, Chretien JP, Gaydos JC:
Infectious disease modeling and military readiness. Emerg Infect Dis
2009; 15: e1. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/
PMC2819869/; accessed July 8, 2013.
8. Feighner BH, Kircher A, Davey VJ, Burke RL, Gaydos JC: 2010 con-
ference on infectious disease modeling sponsored by the U.S. Depart-
ment of Defense. Mil Med 2010; 175: 388–9.
9. Feighner BH, Chretien JP, Murphy SP, et al: The pandemic influenza
policy model: a planning tool for military public health officials. Mil
Med 2009; 174: 557–65.
10. Yu B, Wang J, McGowan M, Vaidyanathan G, Younger K: Gryphon: a
hybrid agent-based modeling and simulation platform for infectious
diseases. In: Advances in Social Computing: Proceedings of Third Inter-
national Conference on Social Computing, Behavioral Modeling, and
Prediction, SBP 2010, Bethesda, MD, March 30–31, 2010, pp 199–207.
Edited by Chai S-K, Salerno JJ, Mabry PL, Berlin, Germany, Springer-
Verlag, 2010. Available at: http://link.springer.com/chapter/10.1007/
978-3-642-12079-4_26; accessed July 8, 2013.
11. Assistant Secretary of Defense (Health Affairs): Guidance on medications
for prophylaxis of malaria, Department of Defense, April 15, 2013. Avail-
able at http://www.health.mil/libraries/HA_Policies_and_Guidelines/
13-002.pdf; accessed November 19, 2013.
12. Anyamba A, Chretien JP, Small J, et al: Prediction of a Rift Valley
fever outbreak. Proc Natl Acad Sci USA 2009; 106: 955–9.
Available at: http://www.ncbi.nlm/nih.gov/pmc/articles/PMC2626607/;
accessed July 8, 2013.
13. Anyamba A, Linthicum KJ, Small J, et al: Prediction, assessment of
the Rift Valley fever activity in East and Southern Africa 2006–2008
and possible vector control strategies. Am J Trop Med Hyg 2010;
83(2 Suppl): 43–51. Available at http://www.ncbi.nlm/nih.gov/pmc/
articles/PMC2913499/; accessed July 8, 2013.
14. Lewis MD, Pavlin JA, Mansfield JL, et al: Disease outbreak detection
system using syndromic data in the greater Washington DC area. Am J
Prev Med 2002; 23: 180.
15. Department of Defense Instruction 6200.03: Public health emer-
gency management within the Department of Defense, Department
MILITARY MEDICINE, Vol. 179, June 2014610
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.

of Defense, March 5, 2010. Available at: http://www.afhsc.mil/
viewDocument?file=DoD_PDFs/DoDI_6200.03_5_Mar_2010.pdf; accessed
July 8, 2013.
16. Betancourt JA, Hakre S, Polyak CS, Pavlin JA: Evaluation of ICD-9
codes for syndromic surveillance in the electronic surveillance system
for the early notification of community-based epidemics. Mil Med 2007;
172: 346–52.
17. Marsden-Haug N, Foster VB, Gould PL, et al: Code-based syndromic
surveillance for influenza like illness by International Classification of
Diseases, Ninth Revision. Emerg Infect Dis 2007; 13: 207–16.
Available at: http://www.ncbi.nlm/nih.gov/pmc/articles/PMC2725845/;
accessed July 8, 2013.
18. Centers for Disease Control and Prevention: Assessment of ESSENCE
performance for influenza-like illness surveillance after an influenza
outbreak—U.S. Air Force Academy, Colorado, 2009. MMWR Morb
Mortal Wkly Rep 2011; 60: 406–9. Available at: http://www.cdc.gov/
mmwr/preview/mmwrhtml/mm6013a3.htm; accessed July 8, 2013.
19. Buczak AL, Koshute PT, Babin SM, Feighner BH, Lewis SH: A data-
driven epidemiological prediction method for dengue outbreaks using
local and remote sensing data. BMCMed Inform Decis Mak 2012; 12: 124.
Available at: http://www.ncbi.nlm/nih.gov/pmc/articles/PMC3534444/;
accessed July 8, 2013.
20. Riley P, Ben-Nun M, Armenta R, et al: Multiple estimates of transmis-
sibility for the 2009 influenza pandemic based on influenza-like-illness
data from small US military populations. PLoS Comput Biol 2013;
9: e1003064. Available at: http://www.ncbi.nlm/nih.gov/pmc/articles/
PMC3656103/; accessed July 8, 2013.
21. Lewis B, Eubank S, Abrams AM, Kleinman K: In silico surveillance:
evaluating outbreak detection with simulation models. BMC Med Inform
Decis Mak 2013; 13: 12. Available at: http://www.biomedcentral.com/
1472-6947/13/12/abstract; accessed July 8, 2013.
22. Marathe A, Lewis B, Barrett C, et al: Comparing effectiveness of top-
down and bottom-up strategies in containing influenza. PLoS One
2011; 6: e25149. Available at: http://www.ncbi.nlm/nih.gov/pmc/articles/
PMC3178616/; accessed July 8, 2013.
23. Marathe A, Lewis B, Chen J, Eubank S: Sensitivity of household transmis-
sion to household contact structure and size. PLoS One 2011; 6: e22461.
Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3148222/;
accessed July 8, 2013.
24. Witt CJ, Richards AL, Masuoka PM, et al: The AFHSC-Division
of GEIS Operations Predictive Surveillance Program: a multidisciplinary
approach for the early detection and response to disease outbreaks. BMC
Public Health 2011; 11 Suppl 2: S10. Available at: http://www.ncbi.nlm/
nih.gov/pmc/articles/PMC3092411/; accessed July 8, 2013.
25. Schlegelmich S, Lenart B, King LB, et al: Summary of the current
operational epidemiological modeling landscape. J Bus Contin Emer
Plan 2012; 5: 338–51.
26. Woolhouse M, Fevre E, Handel I, et al: A guide to good practice for
quantitative veterinary epidemiology. 2011. Available at http://www
.qve-goodpracticeguide.org.uk/guide; accessed November 19, 2013.
MILITARY MEDICINE, Vol. 179, June 2014 611
Commentary
Downloaded from publications.amsus.org: AMSUS - Association of Military Surgeons of the U.S. IP: 155.220.250.114 on Jun 06, 2014.
Copyright (c) Association of Military Surgeons of the U.S. All rights reserved.