
Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing
7
Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing ROBERTO 0. DANTAS, MARK K. KERN, BENSON T. MASSEY, WYLIE J. DODDS, PETER J. KAHRILAS, JAMES G. BRASSEUR, IAN J. COOK, AND IVAN M. LANG Departments of Medicine, Radiology, and Surgery, Medical College of Wisconsin, Milwaukee, Wisconsin 53226; Department of Medicine, Northwestern University, Chicago, Illinois 60611; and Department of Mechanical Engineering, Pennsylvania State University, University Park, Pennsylvania 16802 DANTAS, ROBERTO O., MARK K. KERN, BENSON T. MASSEY, WYLIE J. DODDS, PETER J. KAHRILAS, JAMES G. BRASSEUR, IAN J. COOK, AND IVAN M. LANG. Effect of swalLowed boZus variables on oral and pharyngeal phases of swallowing. Am. J. Physiol. 258 (Gastrointest. Liver Physiol. 21): G675-G681, 1990.-In this investigation, we studied the effects of bolus volume and viscosity on the quantitative features of the oral and pharyngeal phases of swallowing. Concurrent videofluoros- topic and manometric studies were done in 10 healthy volun- teers who were imaged in lateral projection. Videofluorography was done at 30 frames/s while concurrent manometry was done with 5 intraluminal transducers that straddled the pharynx and upper esophageal sphincter (UES). Submental electromyogra- phy was recorded also. Swallows of 2-20 ml were recorded for low-viscosity liquid barium and high-viscosity paste barium. Analysis indicated that the major effect of increases in bolus volume was an earlier onset of anterior tongue base movement, superior palatal movement, anterior laryngeal movement, and UES opening. These events provide receptive adaptation for receiving a swallowed bolus. Earlier UES opening was associ- ated with an increase in the duration of sphincter opening and sphincter diameter. The major effects of high bolus viscosity, unrelated to bolus volume, were to delay oral and pharyngeal bolus transit, increase the duration of pharyngeal peristaltic waves, and prolong andincrease UES opening. Thus the spe- cific effect of bolus viscosity per se differs substantially from that of bolus volume. We conclude that 1) specific variables of swallowing are affected significantly by the variables of the swallowed bolus, such as volume and viscosity; 2) overall, bolus volume and viscosity affect swallowing in a different manner; and 3) the study findings have implications about the neural control mechanisms that govern swallowing as well as about the diagnosis and treatment of patients with abnormal oral- pharyngeal swallowing. bolus volume; bolus viscosity ALTHOUGH NUMEROUS STUDIES have been directedto- ward quantifying the radiographic and manometric fea- tures of primary esophageal peristalsis (9, 12, 16), little attention has been given to fully characterizing and quantifying the oral and pharyngeal phases of swallowing (7,8). Our aims in this study were to 1) quantify the oral and pharyngeal phases of swallowing in healthy volun- teers and 2) determine the effects of variation in volume and viscosity swallowing. of the swallowed bolus on the variables of METHODS We studied 10 healthy male volunteers who were with- out clinical gastrointestinal symptoms. The subjects ranged in age from 18 to 36 yr with an average age of 26 t 6 (SD) yr. This investigation was approved by the Human Research Review Committee of the Medical Col- lege of Wisconsin and informed obtained from each subject. written consent was For their combined videofluoroscopic-manometric study of swallowing, each subject sat on a stool, turned laterally to the face of the image intensifier. The subjects were instructed to hold their head in a neutral position. Videofluoroscopic recordings were obtained at 90 keV using a g-in. image intensifier mode and appropriate collimation so that a lateral image was obtained of the entire mouth and pharynx. In each subject, we recorded swallows of a low-viscosity liquid barium preparation (Liquid E-Z, E-Z-EM, Westbury, NY) diluted to 40% wt/vol, and a viscous barium paste that was prepared by adding 300 g of Knott’s blueberry syrup to 100 g of barium sulfate so that the mixture had a consistency of thick paste. The density of the liquid barium and barium paste was 1.4 and 2.8 g/cm3, respectively. The viscosity of the liquid barium was 200 cP, whereas that of the paste barium, 60,000 cP, was substantially greater. Dur- ing each study, we recorded swallows of liquid barium and paste barium at the graded volumes of 2, 5, 10, and 20 ml; these were judged to be within the physiological range. Each swallow was initiated with the bolus posi- tioned above the tongue with the tongue tip touching the upper incisors (4), the so-called “tipper’‘-type swallow. Swallows were recorded in duplicate using a Beta video- recorder (Sony SLHF 900) with a O.&in. tape run at 30 frames/s. Desired volumes of barium were delivered to the mouth using a graduated syringe. Each observation was made in duplicate, and subsequent measurements were averaged. Each fluoroscopic sequence was 56 s, and total fluoroscopic time was limited to 52 min. For pharyngeal manometry, we used two strain-gauge manometric probes (Gaeltec, Hackensack, NJ), each with three transducers spaced at 3-cm intervals. The two 0193~1857/90 $1.50 Copyright 0 1990 the American Physiological Society G675
Transcript of Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing

Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing
ROBERTO 0. DANTAS, MARK K. KERN, BENSON T. MASSEY, WYLIE J. DODDS, PETER J. KAHRILAS, JAMES G. BRASSEUR, IAN J. COOK, AND IVAN M. LANG Departments of Medicine, Radiology, and Surgery, Medical College of Wisconsin, Milwaukee, Wisconsin 53226; Department of Medicine, Northwestern University, Chicago, Illinois 60611; and Department of Mechanical Engineering, Pennsylvania State University, University Park, Pennsylvania 16802
DANTAS, ROBERTO O., MARK K. KERN, BENSON T. MASSEY, WYLIE J. DODDS, PETER J. KAHRILAS, JAMES G. BRASSEUR, IAN J. COOK, AND IVAN M. LANG. Effect of swalLowed boZus variables on oral and pharyngeal phases of swallowing. Am. J. Physiol. 258 (Gastrointest. Liver Physiol. 21): G675-G681, 1990.-In this investigation, we studied the effects of bolus volume and viscosity on the quantitative features of the oral and pharyngeal phases of swallowing. Concurrent videofluoros- topic and manometric studies were done in 10 healthy volun- teers who were imaged in lateral projection. Videofluorography was done at 30 frames/s while concurrent manometry was done with 5 intraluminal transducers that straddled the pharynx and upper esophageal sphincter (UES). Submental electromyogra- phy was recorded also. Swallows of 2-20 ml were recorded for low-viscosity liquid barium and high-viscosity paste barium. Analysis indicated that the major effect of increases in bolus volume was an earlier onset of anterior tongue base movement, superior palatal movement, anterior laryngeal movement, and UES opening. These events provide receptive adaptation for receiving a swallowed bolus. Earlier UES opening was associ- ated with an increase in the duration of sphincter opening and sphincter diameter. The major effects of high bolus viscosity, unrelated to bolus volume, were to delay oral and pharyngeal bolus transit, increase the duration of pharyngeal peristaltic waves, and prolong andincrease UES opening. Thus the spe- cific effect of bolus viscosity per se differs substantially from that of bolus volume. We conclude that 1) specific variables of swallowing are affected significantly by the variables of the swallowed bolus, such as volume and viscosity; 2) overall, bolus volume and viscosity affect swallowing in a different manner; and 3) the study findings have implications about the neural control mechanisms that govern swallowing as well as about the diagnosis and treatment of patients with abnormal oral- pharyngeal swallowing.
bolus volume; bolus viscosity
ALTHOUGH NUMEROUS STUDIES have been directedto- ward quantifying the radiographic and manometric fea- tures of primary esophageal peristalsis (9, 12, 16), little attention has been given to fully characterizing and quantifying the oral and pharyngeal phases of swallowing (7,8). Our aims in this study were to 1) quantify the oral and pharyngeal phases of swallowing in healthy volun- teers and 2) determine the effects of variation in volume
and viscosity swallowing.
of the swallowed bolus on the variables of
METHODS
We studied 10 healthy male volunteers who were with- out clinical gastrointestinal symptoms. The subjects ranged in age from 18 to 36 yr with an average age of 26 t 6 (SD) yr. This investigation was approved by the Human Research Review Committee of the Medical Col- lege of Wisconsin and informed obtained from each subject.
written consent was
For their combined videofluoroscopic-manometric study of swallowing, each subject sat on a stool, turned laterally to the face of the image intensifier. The subjects were instructed to hold their head in a neutral position. Videofluoroscopic recordings were obtained at 90 keV using a g-in. image intensifier mode and appropriate collimation so that a lateral image was obtained of the entire mouth and pharynx. In each subject, we recorded swallows of a low-viscosity liquid barium preparation (Liquid E-Z, E-Z-EM, Westbury, NY) diluted to 40% wt/vol, and a viscous barium paste that was prepared by adding 300 g of Knott’s blueberry syrup to 100 g of barium sulfate so that the mixture had a consistency of thick paste. The density of the liquid barium and barium paste was 1.4 and 2.8 g/cm3, respectively. The viscosity of the liquid barium was 200 cP, whereas that of the paste barium, 60,000 cP, was substantially greater. Dur- ing each study, we recorded swallows of liquid barium and paste barium at the graded volumes of 2, 5, 10, and 20 ml; these were judged to be within the physiological range. Each swallow was initiated with the bolus posi- tioned above the tongue with the tongue tip touching the upper incisors (4), the so-called “tipper’‘-type swallow. Swallows were recorded in duplicate using a Beta video- recorder (Sony SLHF 900) with a O.&in. tape run at 30 frames/s. Desired volumes of barium were delivered to the mouth using a graduated syringe. Each observation was made in duplicate, and subsequent measurements were averaged. Each fluoroscopic sequence was 56 s, and total fluoroscopic time was limited to 52 min.
For pharyngeal manometry, we used two strain-gauge manometric probes (Gaeltec, Hackensack, NJ), each with three transducers spaced at 3-cm intervals. The two
0193~1857/90 $1.50 Copyright 0 1990 the American Physiological Society G675

G676 BOLUS VARIABLES
probes, each 2.5 mm in outer diameter, were taped to- gether so that a total of six transducers were staggered at l&cm intervals. The flat-shaped assembly was 2.5 x 5 mm in diameter. The transducers were standardized and calibrated in a water bath at 37°C. After its passage through the nose, the assembly was positioned so that all its transducers faced posteriorly and the distal trans- ducer (no. 1) was located within the proximal margin of the upper esophageal sphincter (UES) high-pressure zone. Transducer nos. 2-5 were distributed at 1.5-cm intervals through the hypopharynx and oropharynx. Transducer no. 6 was not used. Manometric activity was recorded on an eight-channel Beckman 612 Dynograph recorder run at a paper speed of 100 mm/s. The video and manometric recordings were synchronized by a mod- ified timer (VC 436, Thalner Electronics, Ann Arbor, MI) that provided digital time in milliseconds on the video images and marked the polygraph tracings at l-s intervals.
In each subject, we also recorded submental myoelec- tric activity by bipolar electrodes taped beneath the chin over the mylohyoid-geniohyoid-anterior-digastric muscle complex. Electromyography (EMG) was recorded di- rectly on the polygraph tracing and also on FM tape (Hewlett-Packard 3968A) for subsequent processing via an integrator (4).
The video recordings were analyzed in slow motion and by single-frame analysis using the playback capabil- ity of the videorecorder. Timing of events was determined by direct reading of the digital clock recorded on each video frame. Measurements of distance, such as superior or anterior hyoid movement, were made from the tele- vision monitor screen using the anterior margin of the cervical spine as the axis of reference and corrected for magnification (11). Using these methods, we determined the timing of the following: 1) onset and peak submental EMG activity; 2) onset of propulsive tongue tip move- ment at the maxillary incisors; 3) onset tongue base movement; 4) onset of superior and anterior hyoid move- ment; 5) passage of the bolus tail through the fauces and by each manometric recording site; 6) onset of the peri- staltic pressure wave at each transducer; 7) passage of the bolus head through the fauces; 8) peak superior and anterior hyoid movement; 9) onset and offset of UES relaxation; and 10) onset, duration, and offset of UES opening. From these timings, we calculated bolus transit time through the mouth (equivalent oral clearance time), transit time through the pharynx (bolus tail at fauces to closure of UES), and pharyngeal clearance time (entry bolus head into the oropharynx until bolus tail reached the UES segment).
From the pharyngeal manometry tracings, we deter- mined the transit time, amplitude, and duration of the pharyngeal peristaltic pressure complex. During swallow- ing, the UES made an oral excursion of -2-2.5 cm, which brought the central zone of the UES to the level of recording site no. 2. Because UES relaxation occurred while the sphincter was at or near the apogee of its orad excursion (17, 18), we measured UES relaxation from the recording site positioned 1.5 cm proximal to the upper margin of the UES, as described previously (5, 18). We
measured the timing of UES relaxation, onset, moment of complete UES relaxation, and UES relaxation offset, the latter determined by arrival of the pharyngeal con- traction wave at the UES. From these values, we calcu- lated the interval from the onset of manometric UES relaxation to complete relaxation and the duration of complete sphincter relaxation. Last, from the recording site just proximal to the UES, we measured the pressure within the barium bolus immediately before UES open- ing (yield pressure) and during the midpoint of trans- sphincteric barium flow (flow pressure) as well as the pressure from within the open UES during its maximal opening.
Pooled data in the text are given as means t SE unless stated otherwise. In one subject, the manometric data from the pharynx was not analyzed due to a technical failure. Inferences about significant trends related to bolus volume or consistency were based on a two-way analysis of variance for repeated measurements or a paired Student’s t test or correlation analysis where appropriate.
RESULTS
Barium bolus. During the swallow sequence, the swal- lowed barium bolus exhibited a pointed tail that was used as the marker to assess bolus transport (22, 23). Bolus transit times for liquid barium and paste barium are shown in Table 1. For the two different bolus types, an effect was not observed for bolus volume. However, across all volumes, oral and pharyngeal transit time was significantly greater for paste barium than for liquid barium (P < 0.05).
Due to the same method of calculation, the times for oral clearance of the barium boluses are identical to those of oral transit shown in Table 1. Pharyngeal clearance of the bolus, however, differs from pharyngeal transit
TABLE 1. Oral and pharyngeal transit time of swallowed barium boluses in 10 normal subjects
Bolus Oral Transit Pharyngeal Transit
Volume,* ml Liquid Ba Paste Bat Liquid Ba Paste Ba-F
2 0.40t0.04 0.63t0.10 0.43t0.04 0.57t0.11 5 0.39kO.04 0.51~0.06 0.47t0.04 0.56kO.07
10 0.38kO.05 0.52t0.09 0.41t0.04 0.51zk0.05 20 0.36kO.04 0.45t0.07 0.41*0.03 0.50t0.05
Values are means k SE (in s). * No significant effect of bolus volume for any bolus type. -F Across all volumes, values for paste barium > liquid barium (P < 0.05).
TABLE 2. Pharyngeal clearance time of swallowed barium boluses in 10 normal subjects
Bolus Volume,* ml
Clearance Time
Liquid Ba Paste Bat
2 0.59t0.04 0.71kO.12
5 0.64t0.06 0.73kO.07
10 0.65-t-0.04 0.73t0.06
20 0.70t0.03 0.83t0.06
Values are means t SE (in s). * No significant effect of bolus volume for either bolus type. t Across all volumes, values for paste barium > liquid barium (P < 0.05).

BOLUS VARIABLES G677
and is shown in Table 2. For both types of boluses, Peristaltic wave amplitude in the pharynx was not pharyngeal clearance was not volume dependent. Across dependent on either bolus volume or bolus viscosity (Fig. all volumes tested, however, volume clearance for paste 3). Wave duration, however, showed a direct dependence barium was significantly greater than for liquid barium (P < 0.02).
on bolus viscosity (Fig. 4), in that the values for high- viscosity paste barium were longer than for low-viscosity
The duration of UES opening and transsphincteric liquid barium (P < 0.05). Peristaltic wave duration, barium flow during swallowing directly depended on however, was not dependent on bolus volume. bolus volume for both liquid barium and paste barium The duration of swallow-induced manometric UES (Fig. 1). Additionally, the duration of UES opening for relaxation showed a direct dependence on bolus volume paste barium was significantly greater than for liquid barium. Mean flow rate of barium across the UES for
and bolus viscosity. Duration of UES relaxation for paste barium was significantly longer than for liquid barium
liquid barium ranged from 7 t 1 ml/s for 2 ml to 41 t 2 ml/s for 20 ml, whereas that for paste barium was mod-
(Fig. 5). The values of UES relaxation recorded by ma- nometry were comparable to the duration of UES open-
erately slower (P < 0.05). For 2 ml of paste barium, the ing recorded by videofluoroscopy (Fig. I). mean transsphincteric flow rate was 6 t 1 compared with The intrabolus yield pressure that existed immediately 35 t 2 ml/s for 20 ml. before UES opening demonstrated low mean values of
Manometry. Onset of the peristaltic pressure wave ~12 mmHg and was not dependent on either bolus recorded by manometry was essentially coincident with volume or viscosity. In the hypopharynx, upstream in- passage of the barium tail recorded by videofluoroscopy. The maximal difference was to.1 s. The peristaltic
trabolus pressure, for liquid barium during transsphinc- teric barium flow, showed low average values of 5-10
transit times recorded by manometry from the middle mmHg that were not dependent on bolus volume. In oropharynx to the lower hypopharynx (Fig. 2) did not contrast, upstream pressure values for paste barium show any volume dependency, but the transit time for swallows (Fig. 6A) exhibited a pronounced direct de- paste barium was significantly greater than for liquid barium (P c 0.05).
pendence on bolus volume and were substantially greater than those of the liquid barium boluses (P c 0.01). For
Set , example, the mean intrabolus pressure during trans- sphincteric flow of 20 ml of paste barium was 49 mmHg.
A.
mmHg
zoo{ aa >
g g 150- 0= .I -- r = loo- t;s .- & e 50-
Bolus Volume [ml)
FIG. 1. Duration of upper esophageal sphincter (UES) opening and transsphincteric flow of barium. Values are means t SE for 10 normal subjects. For swallowed bolus volume of 2-20 ml, significant bolus dependence existed for low-viscosity liquid barium and high-viscosity paste barium (P < 0.01). For each volume, paste barium was associated with longer UES opening than liquid barium.
- --
Bob Volume (ml] Cl Liquid Ba El Paste Ba
FIG. 3. Manometric values of peristaltic wave amplitude in the pharynx. Values averaged for 3 recording sites. Values are means t SE for 9 normal subjects. Amplitude of pharyngeal peristaltic pressure complex was not affected by bolus volume or bolus type.
Set I
g 0.6- .- I- - .- ii 0.4- + z a3 E 0.2- k E
1 T T/-~---- --- ----------
k-----7-
o Liquid Ba A Paste Ba
i .. 4 lb .. 2b
Bolus Volume [ml]
FIG. 2. Pharyngeal transit time for swallowed barium boluses meas- ured from manometry. Values are means t SE for 9 normal subjects. Transit time measured by manometry corresponded to passage time of the tail of the barium bolus from the level of the fauces to the upper esophageal sphincter (UES). A rrival of bolus tail at UES corresponded to closure of the sphincter.
Set 0.5 -j
5 10
Bolus Volume [ml] Cl Liquid Ba El Paste Ba
FIG. 4. Manometric values of peristaltic wave duration in the phar- ynx. Values averaged for 3 recording sites in 9 normal subjects. Values are means of: SE. Wave duration was not dependent on bolus volume. However, for each value shown, wave duration for paste barium was significantly longer (P < 0.01) than for liquid barium.

G678 BOLUS VARIABLES
o Liquid Ba
A Paste Ba
= OLll , 1 ‘1 I 2 5 10 20
Bolus Volume [ml]
FIG. 5. Duration of manometric upper esophageal sphincter (UES) relaxation induced by barium swallows. Averaged values, means t SE, shown for 10 normal subjects. For both thin liquid barium and viscous barium paste, a significant direct relationship existed between the duration of manometric UES relaxation and bolus volume (P < 0.05). For each volume, the value for paste was significantly longer than for that of liquid barium (P < 0.01).
A
Bolus Volume [ml)
mmHg
50 e z z 40 CL g 30 0 g 20 - 2 10 =>
0 5 10
Bolus Volume [ml\ Cl Liquid Ba tZJ Paste Ba
FIG. 6. Intrabolus pressure during transsphincteric flow of swal- lowed barium. A: values are means I~I SE for 10 normal subjects. A strong direct correlation existed between bolus volume and intrabolus pressure for paste barium (r = 0.64, P c 0.01). Although a trend existed for liquid barium, it was not significant. For each volume, the intrabolus pressure for paste was significantly greater than for liquid barium (P 2 0.05). B: pressures recorded within the open UES during transsphinc- teric flow.
Intrabolus pressures at the level of the UES transsphincteric flow of barium are shown in Fig.
during 6B .
Timings. Shown in Table 3 are the timings of swallow- related events for liquid barium and paste barium in- dexed to propulsive ton .gue tip movement at the maxil- lary in .cisors as the zero referen ce. Inspection of the data
indicates that the leading complex of the onset of sub- mental EMG, superior hyoid movement, and tongue base movement all occurred in a close temporal relationship of -0.1-02 s with the onset of propulsive tongue tip movement at the maxillary incisors. The latter is taken as the zero temporal reference. Tongue base movement, palatal movement, and UES opening all had a direct temporal dependence on bolus volume for both liquid barium and paste barium (P c 0.05). A direct dependence on bolus viscosity existed for the onset and peak of anterior hyoid movement, onset of UES opening, and UES closure.
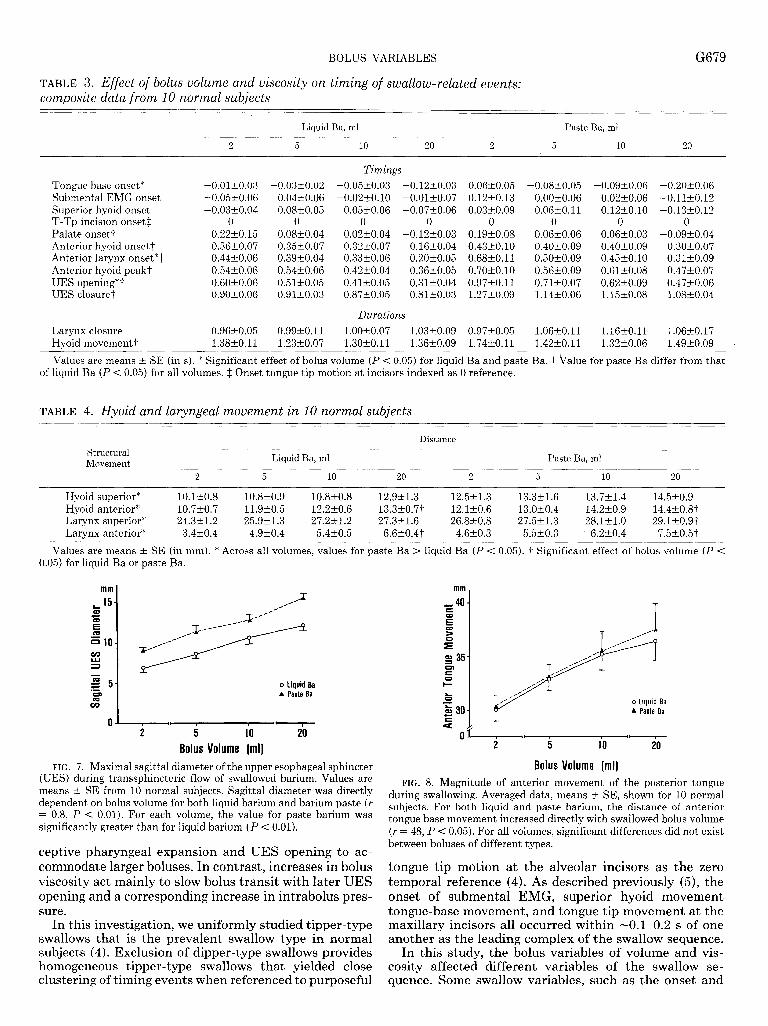
Distance measurements. The maximal distances of su- perior and anterior hyoid movement for the hyoid and larynx during swallowing are shown in Table 4. A signif- icant bolus effect (P < 0.05) occurred for the magnitude of anterior hyoid movement, superior laryngeal move- ment (paste only), and anterior laryngeal movement. The magnitude of each movement was significantly different for paste than for liquid barium. Maximum sagittal di- mension of the UES directly depended on bolus volume for both liquid barium and paste barium (Fig. 7). For each volume, the maximal sagittal U ‘ES diameter was significantly greater for barium paste than liquid ( PC 0.01).
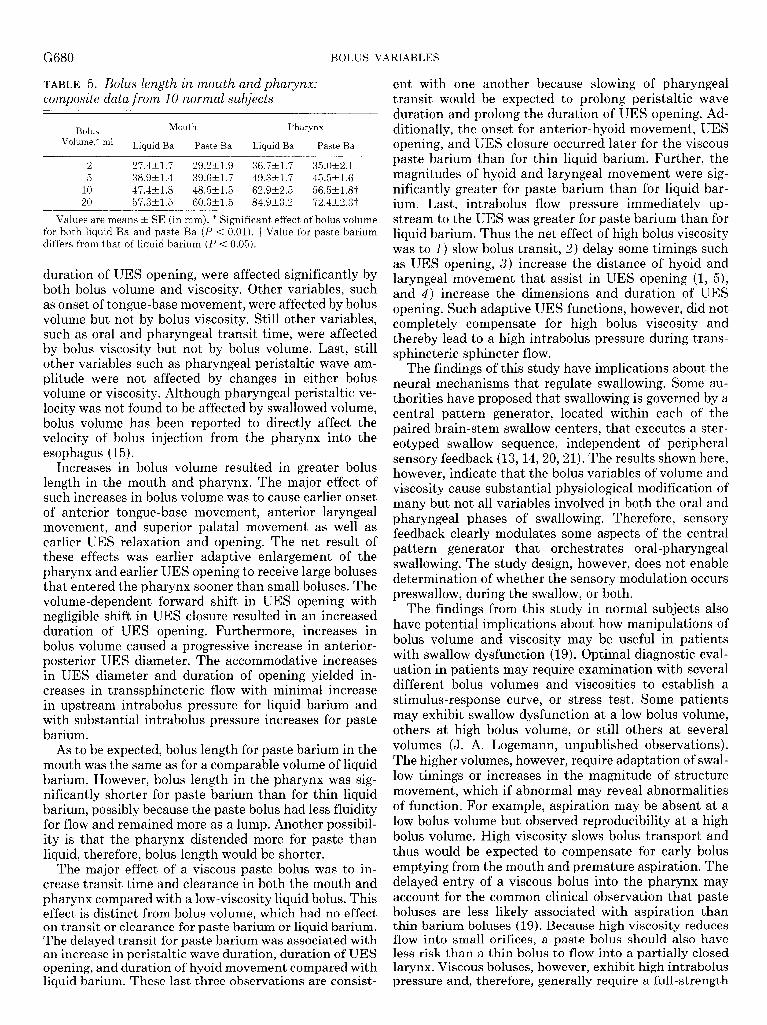
Analysis of tongue base movement indicated that the magnitude of anterior movement of the tongue base during swallowing increased directly with bolus volume both for liquid barium and paste barium (P < 0.05). However, there was no difference between the two types of barium boluses (Fig. 8).
Table 5 lists the measurements of bolus length in the mouth and pharynx. In both areas, a significant direct relationship existed for bolus volume for both liquid barium and paste barium. Additionally, bolus length was significantly shorter for paste barium than liquid barium for the 10 and 20 ml volumes.
DISCUSSION
Although bolus volume and consistency are known to affect the quantitative features of primary esophageal peristalsis (9, 12, 16), the effect of swallowed bolus vol- ume and viscosity on the oral and pharyngeal phases of swallowing have not been thoroughly quantitated (3, 6, 10). In this study, we recorded preesophageal swallow events by concurrent videofluoroscopy and manometry as well as submental EMG and determined the effects of differences in barium volume and viscosity on the quan- titative features of the oral and pharyngeal phase of swallowing. The results indicated the following: 1) deglu- titive oral and pharyngeal transit is directly related to bolus viscosity and unaffected by bolus volume, 2) nei- ther bolus volume nor viscosity affect the amplitude of pharyngeal peristalsis, 3) the distance of anterior hyoid and laryngeal movement increased with increases in bolus volume, 4) bolus volume and viscosity had a direct effect on the timing and duration of UES relaxation, and 5) the magnitude of anterior movement of the tongue base correlated directly with bolus volume but not bolus type. These findings suggest that bolus volume modulates the central swallowing program by inducing earlier re-
BOLUS VARIABLES G679
TABLE 3. Effect of bolus volume and viscosity on timing of swallow-related events: composite data from 10 normal subjects
2
Liquid Ba, ml Paste Ba, ml
5 10 20 2 5 10 20
Tongue base onset* Submental EMG onset Superior hyoid onset T-Tp incision onset* Palate onset? Anterior hyoid onset? Anterior larynx onset”? Anterior hyoid peak? UES opening”7 UES closure?
Larynx closure Hyoid movement?
-0.01rt0.03 - -0.05t0.06 -0.03t0.04
0 0.22t0.15 0.36t0.07 0.44-r-0.06 0.54t0.06 0.60t0.06 0.90t0.06
.0.03-+0.02 0.04t0.06 0.08t0.05
0 0.08rtO.04 0.35t0.07 0.39Iko.04 0.54t0.06 0.51t0.05 0.91zk0.03
0.96t0.05 0.99t0.11 1.38kO.11 1.23t0.07
Timings
-0.05riro.03 -0.12t0.03 -0.02t0.10 -0.01t0.07
0.05t0.06 -0.07t0.06 0 0
0.02t0.04 -0.12t0.03 0.32t0.07 0.16kO.04 0.33t0.06 0.20t0.05 0.42t0.04 0.36t0.05 0.41t0.05 0.31-r-0.04 0.87t0.05 0.81t0.03
Durations
1.00t0.07 1.03t0.09 1.3ot,o.11 1.36kO.09
0.06t0.05 0.12t0.13 0.03t0.09
0 0.19t0.08 0.43t0.10 0.68t0.11 0.70t0.10 0.97zko.11 1.27t0.09
0.97_to.o5 1.74t_o.11
-0.08t0.05 O.OOt0.06 0.06t0.11
0 0.06~0.06 0.40t0.09 0.50*0.09 0.56t0.09 0.7lzkO.07 1.14t0.06
1.06_tO.11 1.42+_0,.11
-0.09kO.06
0.02t0.06 0.12t0.10
0 0.06_tO.O3 0.40~0.09 0.45*0.10 0.61~0.08 0.62_tO,O9 1.15t0.08
1.16kO.11 1.32kO.06
-0.20t0.06 -0.110.12 -0.13t0.12
0 -0.09~0.04
0.3o-eo.07 0.3kko.09 0.47kO.07 0.47kO.06 1.08kO.04
1.06t0.17 1.49t0.09
Values are means k SE (in s). * Significant effect of bolus volume (P < 0.05) for liquid Ba and paste Ba. t Value for paste Ba differ from that of liquid Ba (P < 0.05) for all volumes. $ Onset tongue tip motion at incisors indexed as 0 reference.
TABLE 4. Hyoid and laryngeal movement in 10 normal subjects
Structural Movement
2
Distance
Liquid Ba, ml Paste Ba, ml
5 10 20 2 5 10 20
Hyoid superior* 10.13-0.8 10.8kO.9 10.8t0.8 12.9kl.3 12.521.3 13.3H.6 13.7t1.4 14.5kO.9 Hyoid anterior* 10.7kO.7 11.9t0.5 12.2t0.6 13.3+0.7? 12.lkO.6 13.0t0.4 14.2t0.9 14.4+0.83 Larynx superior* 24.3k1.2 25.9t1.3 27.2t1.2 27.3kl.6 26.8t0.8 27.5t1.3 28.l:l.O 29.1+0.9t Larynx anterior* 3.4kO.4 4.9kO.4 5.4kO.5 6.6+0.4? 4.6t0.3 5.5kO.3 6.2~0.4 7.5+0.5-t
Values are means t_ SE (in mm). * Across all volumes, values for paste Ba > liquid Ba (P < 0.05). 7 Significant effect of bolus volume (P < 0.05) for liquid Ba or paste Ba.
o Liquid Ba A Paste Ba
,I., I I I 2 5 10 20
Bolus Volume [ml) FIG. 7. Maximal sagittal diameter of the upper esophageal sphincter
(UES) during transsphincteric flow of swallowed barium. Values are means -t SE from 10 normal subjects. Sagittal diameter was directly dependent on bolus volume for both liquid barium and barium paste (r = 0.8, P < 0.01). For each volume, the value for paste barium was significantly greater than for liquid barium (P < 0.01).
ceptive pharyngeal expansion and UES opening to ac- commodate larger boluses. In contrast, increases in bolus viscosity act mainly to slow bolus transit with later UES opening and a corresponding increase in intrabolus pres- sure.
In this investigation, we uniformly studied tipper-type swallows that is the prevalent swallow type in normal subjects (4). Exclusion of dipper-type swallows provides homogeneous tipper-type swallows that yielded close clustering of timing events when referenced to purposeful
mm
-40
o Liquid Ba A Paste Ba
---T-
I I I I
5 10 -T
Bobs Volume [ml)
FIG. 8. Magnitude of anterior movement of the posterior tongue during swallowing. Averaged data, means t SE, shown for 10 normal subjects. For both liquid and paste barium, the distance of anterior tongue base movement increased directly with swallowed bolus volume (r = 48, P < 0.05). For all volumes, significant differences did not exist between boluses of different types.
tongue tip motion at the alveolar incisors as the zero temporal reference (4). As described previously (5), the onset of submental EMG, superior hyoid movement tongue-base movement, and tongue tip movement at the maxillary incisors all occurred within -0.1-0.2 s of one another as the leading complex of the swallow sequence.
In this study, the bolus variables of volume and vis- cosity affected different variables of the swallow se- quence. Some swallow variables, such as the onset and
G680 BOLUS VARIABLES
TABLE 5. Bolus length in mouth and pharynx: composite data from 10 normal subjects
Bolus Mouth Pharynx
Volume,* ml Liquid Ba Paste Ba Liquid Ba Paste Ba
2 27.4tl.7 29.2kl.9 36.7t1.7 35.0t2.1 5 38.9t1.4 39.6t1.7 49.3t1.7 45.5k1.6
10 47.4k1.8 48.5t1.5 62.9t2.5 56.5kl.W 20 57.3t1.5 60.3t1.5 84.923.2 72.4&2.3-f-
Values are means -+ SE (in mm). * Significant effect of bolus volume for both liquid Ba and paste Ba (P < 0.01). -i- Value for paste barium differs from that of liquid barium (P < 0.05).
duration of UES opening, were affected significantly by both bolus volume and viscosity. Other variables, such as onset of tongue-base movement, were affected by bolus volume but not by bolus viscosity. Still other variables, such as oral and pharyngeal transit time, were affected by bolus viscosity but not by bolus volume. Last, still other variables such as pharyngeal peristaltic wave am- plitude were not affected by changes in either bolus volume or viscosity. Although pharyngeal peristaltic ve- locity was not found to be affected by swallowed volume, bolus volume has been reported to directly affect the velocity of bolus injection from the pharynx into the esophagus (15).
Increases in bolus volume resulted in greater bolus length in the mouth and pharynx. The major effect of such increases in bolus volume was to cause earlier onset of anterior tongue-base movement, anterior laryngeal movement, and superior palatal movement as well as earlier UES relaxation and opening. The net result of these effects was earlier adaptive enlargement of the pharynx and earlier UES opening to receive large boluses that entered the pharynx sooner than small boluses. The volume-dependent forward shift in UES opening with negligible shift in UES closure resulted in an increased duration of UES opening. Furthermore, increases in bolus volume caused a progressive increase in anterior- posterior UES diameter. The accommodative increases in UES diameter and duration of opening yielded in- creases in transsphincteric flow with minimal increase in upstream intrabolus pressure for liquid barium and with substantial intrabolus pressure increases for paste barium.
As to be expected, bolus length for paste barium in the mouth was the same as for a comparable volume of liquid barium. However, bolus length in the pharynx was sig- nificantly shorter for paste barium than for thin liquid barium, possibly because the paste bolus had less fluidity for flow and remained more as a lump. Another possibil- ity is that the pharynx distended more for paste than liquid, therefore, bolus length would be shorter.
The major effect of a viscous paste bolus was to in- crease transit time and clearance in both the mouth and pharynx compared with a low-viscosity liquid bolus. This effect is distinct from bolus volume, which had no effect on transit or clearance for paste barium or liquid barium. The delayed transit for paste barium was associated with an increase in peristaltic wave duration, duration of UES opening, and duration of hyoid movement compared with liquid barium. These last three observations are consist-
ent with one another because slowing of pharyngeal transit would be expected to prolong peristaltic wave duration and prolong the duration of UES opening. Ad- ditionally, the onset for anterior-hyoid movement, UES opening, and UES closure occurred later for the viscous paste barium than for thin liquid barium. Further, the magnitudes of hyoid and laryngeal movement were sig- nificantly greater for paste barium than for liquid bar- ium. Last, intrabolus flow pressure immediately up- stream to the UES was greater for paste barium than for liquid barium. Thus the net effect of high bolus viscosity was to 1) slow bolus transit, 2) delay some timings such as UES opening, 3) increase the distance of hyoid and laryngeal movement that assist in UES opening (1, 5), and 4) increase the dimensions and duration of UES opening. Such adaptive UES functions, however, did not completely compensate for high bolus viscosity and thereby lead to a high intrabolus pressure during trans- sphincteric sphincter flow.
The findings of this study have implications about the neural mechanisms that regulate swallowing. Some au- thorities have proposed that swallowing is governed by a central pattern generator, located within each of the paired brain-stem swallow centers, that executes a ster- eotyped swallow sequence, independent of peripheral sensory feedback (13,14,20,21). The results shown here, however, indicate that the bolus variables of volume and viscosity cause substantial physiological modification of many but not all variables involved in both the oral and pharyngeal phases of swallowing. Therefore, sensory feedback clearly modulates some aspects of the central pattern generator that orchestrates oral-pharyngeal swallowing. The study design, however, does not enable determination of whether the sensory modulation occurs preswallow, during the swallow, or both.
The findings from this study in normal subjects also have potential implications about how manipulations of bolus volume and viscosity may be useful in patients with swallow dysfunction (19). Optimal diagnostic eval- uation in patients may require examination with several different bolus volumes and viscosities to establish a stimulus-response curve, or stress test. Some patients may exhibit swallow dysfunction at a low bolus volume, others at high bolus volume, or still others at several volumes (J. A. Logemann, unpublished observations). The higher volumes, however, require adaptation of swal- low timings or increases in the magnitude of structure movement, which if abnormal may reveal abnormalities of function. For example, aspiration may be absent at a low bolus volume but observed reproducibility at a high bolus volume. High viscosity slows bolus transport and thus would be expected to compensate for early bolus emptying from the mouth and premature aspiration. The delayed entry of a viscous bolus into the pharynx may account for the common clinical observation that paste boluses are less likely associated with aspiration than thin barium boluses (19). Because high viscosity reduces flow into small orifices, a paste bolus should also have less risk than a thin bolus to flow into a partially closed larynx. Viscous boluses, however, exhibit high intrabolus pressure and, therefore, generally require a full-strength

BOLUS VARIABLES G681
peristaltic wave (8) and forceful posterior tongue thrust (2) for their transport, whereas transport for a thin bolus may remain relatively normal with mild weakness of the
9 ’
normal mechanisms of pharyngeal bolus transport, e.g., posterior tongue thrust and pharyngeal peristalsis.
10.
This work was supported, in part, by National Institute of Diabetes and Digestive and Kidney Diseases Grant DK-25731. R. 0. Dantas was 11. supported by a grant from the Conselho National de Desenvolvimento Cientifico e Tecnologico (CNPq), Brazil.
This work was presented, in part, at the Meeting of the American Motility Society, October 1988, Asilomar, CA, and has appeared in 12. abstract form (Gastroenterology 95: 861, 1988).
Address for reprint requests: W. J. Dodds, Medical College of Wis- consin, Froedtert Memorial Lutheran Hospital, Dept. of Radiology, 9200 W. Wisconsin Ave., Milwaukee, WI 53226. 13.
Received 15 May 1989; accepted in final form 7 December 1989. 14.
REFERENCES 15.
1.
2.
3.
4.
5.
6.
7.
8.
ASOH, R., AND R. K. GOYAL. Manometry and electromyography of the upper esophageal sphincter in the opossum. Gastroenterology 74: 514-520, 1978. CERENKO, D., F. M. S. MCCONNEL, AND R. T. JACKSON. Quanti-
16.
tative assessment of pharyngeal bolus driving forces. OtoZaryngoZ. Head Neck Surg. 100: 57-63, 1989. CHRISTRUP JORGEN. Normal swallowing of foodstuffs of pasty
17.
consistence. Danish Med. Bull. 2: 79-91, 1964. COOK, I. J., W. J. DODDS, R. 0. DANTAS, M. K. KERN, B. T. MASSEY, R. SHAKER, AND W. J. HOGAN. Timing of videofluoros-
18 *
topic, manometric events, and bolus transit during the oral and pharyngeal phases of swallowing. Dysphagia. 4: 8-15, 1989. 19. COOK, I. J., W. J. DODDS, R. 0. DANTAS, B. T. MASSEY, M. K. KERN, I. M. LANG, J. G. BRASSEUR, AND W. J. HOGAN. Opening 20. mechanism of the human upper esophageal sphincter. Am. J. 21, Physiol. 257 (Gastrointest. Liver Physiol. 20): G748-G759, 1989. COSTER, S. T., AND W. J. SCHWARZ. Rheology and the swallow- 22. safe bolus. Dysphagia 1: 113-118, 1987. CURTIS, D. J., D. F. CRUESS, A. H. DACHMAN, AND E. MASO. Timing in the normal pharyngeal swallow. Inuest. Radial. 19: 523- 23. 529, 1984. DODDS, W. J., W. J. HOGAN, S. B. LYDON, E. T. STEWART, J. J. STEFF, AND R. C. ARNDORFER. Quantitation of pharyngeal motor
function in normal human subjects. J. Appl. Physiol. 39: 692-696, 1975. DODDS, W. J., W. J. HOGAN, D. P. REID, E. T. STEWART, AND R. C. ARNDORFER. A comparison between primary esophageal peri- stalsis following wet and dry swallows. J. AppZ. Physiol. 35: 851- 857, 1973. DODDS, W. J., P. J. KAHRILAS, J. DENT, AND W. J. HOGAN. Considerations about pharyngeal manometry. Dysphagia 1: 209- 214, 1987. DODDS, W. J., K. M. MAN, I. J. COOK, P. J. KAHRILAS, E. T. STEWART, M. K. KERN. Influence of bolus volume on swallow- induced hyoid movement in normal subjects. AJR 150: 1307-1309, 1988. DOOLEY, C. P., B. SCHLOSSMACHER, AND J. E. VALENZUELA. Effects of alterations in bolus viscosity on esophageal peristalsis in humans. Am. J. Physiol. 254 (Gastrointest. Liver Physiol. 17): Gl-G4,1988. DOTY, R. W. Neural organization of deglutition. Handbook of Physiology. Alimentary Canal. Washington, DC: Am. Physiol. Sot., 1968, sect. 6, vol. 4, p. 1861-1902. DOTY, R. W., AND J. D. BOSMA. An electromyographic analysis of reflex deglutition. J. Neurophysiol. 19: 44-60, 1956. FISHER, M. A., T. R. HENDRIX, J.,N. HUNT, AND A. J. MURRILLS. Relation between volume swallowed and velocity of the bolus ejected from the pharynx into the esophagus. Gastroenterology 74: 1238-1240, 1978. HOLLIS, J. B., AND D. 0. CASTELL. Effect of dry swallows and wet swallows of different volumes on esophageal peristalsis. J. Appl. Physiol. 38: 1161-l 164, 1975. ISBERG, A., M. E. NILSSON, AND H. SCHIRATZKI. The upper esophageal sphincter during normal deglutition. Acta Radial. Diagn. 23: 563-568, 1985. KAHRILAS, P. J., W. J. DODDS, J. DENT, J. A. LOGEMANN, AND R. SHAKER. Upper esophageal sphincter function during degluti- tion. Gastroenterology 95: 52-62, 1988. LOGEMANN, J. A. Manual for the Videofluorographic Study of SwaZZowing. San Diego, CA: College-Hill, 1986. MILLER, A. J. Deglutition. Physiol. Rev. 62: 129-184, 1982. MILLER, A. J. Neurophysiological basis of swallowing. Dysphagia 1: 91-100, 1986. SHAKER, R., I. J. S. COOK, W. J. DODDS, AND W. J. HOGAN. Pressure-flow dynamics of the oral phase of swallowing. Dysphagia 3: 79-84,1988. SOKOL, E. M., P. HEITMANN, B. S. WOLF, AND B. R. COHEN. Simultaneous cineradiographic and manometric study of the phar- ynx, hypopharynx and cervical esophagus. Gastroenterology 51: 960-974, 1966.



















