
Early Intervention for Children with Autism Spectrum Disorder UCL talk 27 th June 2014
18
7/2/2014 1 Early Intervention for Children with Autism Spectrum Disorder UCL talk 27 th June 2014 Tony Charman Chair in Clinical Child Psychology Here under false pretences… • Katrina’ s email: –“We are hoping that you might be happy to speak about your work on early interventions for children with ASD, and particularly your thoughts what has led to this work becoming as influential as it is, from the initial idea to its current wide impact”.
-
Upload
leedsbeckett -
Category
Documents
-
view
0 -
download
0
Transcript of Early Intervention for Children with Autism Spectrum Disorder UCL talk 27 th June 2014
7/2/2014
1
Early Intervention for Children
with Autism Spectrum Disorder UCL talk
27th June 2014
Tony Charman Chair in Clinical Child Psychology
Here under false pretences…
• Katrina’s email:
– “We are hoping that you might be happy to speak
about your work on early interventions for children
with ASD, and particularly your thoughts what has led
to this work becoming as influential as it is, from the
initial idea to its current wide impact”.
7/2/2014
2
Here under false pretences…
• Katrina’s email:
– “We are hoping that you might be happy to speak
about your work on early interventions for children
with ASD, and particularly your thoughts what has led
to this work becoming as influential as it is, from the
initial idea to its current wide impact”.
• My response:
Overview • Early social-communication symptoms of ASD
• Theoretical and empirical literature on infant
development of social-communication
• Similar developmental evidence in ASD
• Testing developmental theory
• Towards a social-communication EB (incl. PACT)
• An alternative evidence-base (North American)
– Intensive behavioural intervention
– Poor research, mixed evidence, strong views + strong
disagreement
• NICE guidance
• Glass half-full or half-empty?
4
7/2/2014
3
Autism Spectrum Disorder (DSM-5)
• Deficits in social communication and social
interaction across multiple contexts
– Deficits in social-emotional reciprocity
– Deficits in nonverbal communicative behaviors used for social
interaction
– Deficits in developing, maintaining + understanding relationships
• Restricted, repetitive patterns of behavior, interests,
or activities, as manifested by at least two
– Stereotyped/repetitive motor movements, use of objects, speech
– Insistence on sameness, inflexible adherence to routines, or
ritualized patterns or verbal nonverbal behavior
– Highly restricted, fixated interests that are abnormal in intensity
or focus
– Hyper- or hypo-reactivity to sensory input or unusual interests in
sensory aspects of the environment
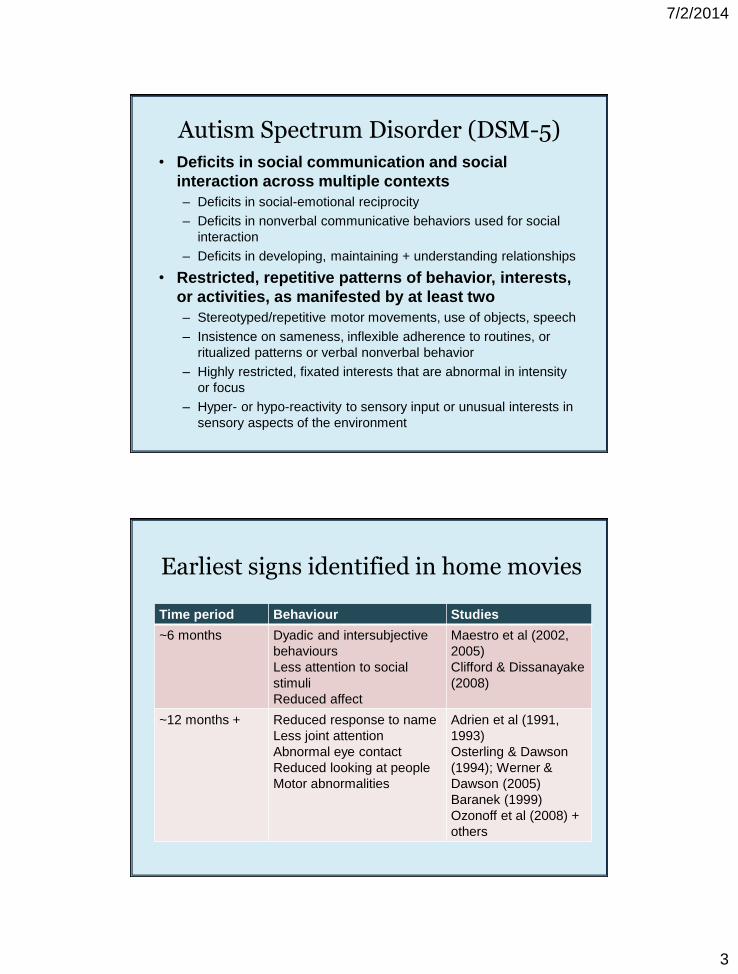
Time period Behaviour Studies
~6 months Dyadic and intersubjective
behaviours
Less attention to social
stimuli
Reduced affect
Maestro et al (2002,
2005)
Clifford & Dissanayake
(2008)
~12 months + Reduced response to name
Less joint attention
Abnormal eye contact
Reduced looking at people
Motor abnormalities
Adrien et al (1991,
1993)
Osterling & Dawson
(1994); Werner &
Dawson (2005)
Baranek (1999)
Ozonoff et al (2008) +
others
Earliest signs identified in home movies
7/2/2014
4
Earliest signs in screening studies
• Lack of joint attention behaviours
– Gaze monitoring, pointing for interest
• Reduced response to name
• Lack of early pretend play
• Reduced range of early play behaviours
• Impoverished range of facial expressiveness
• Reduced interest in people
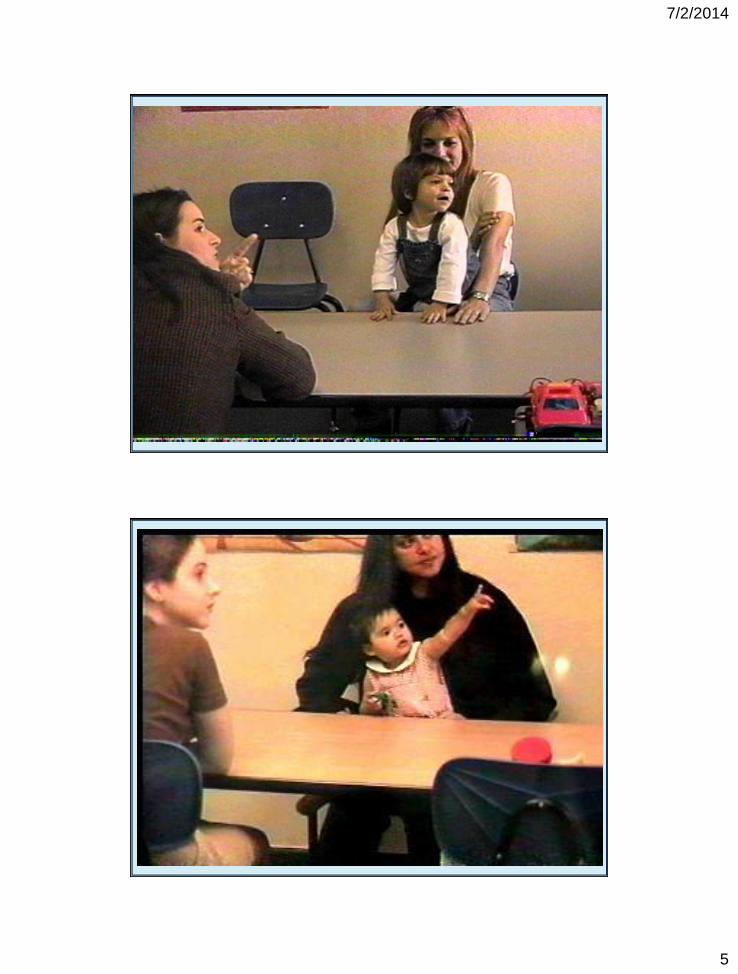
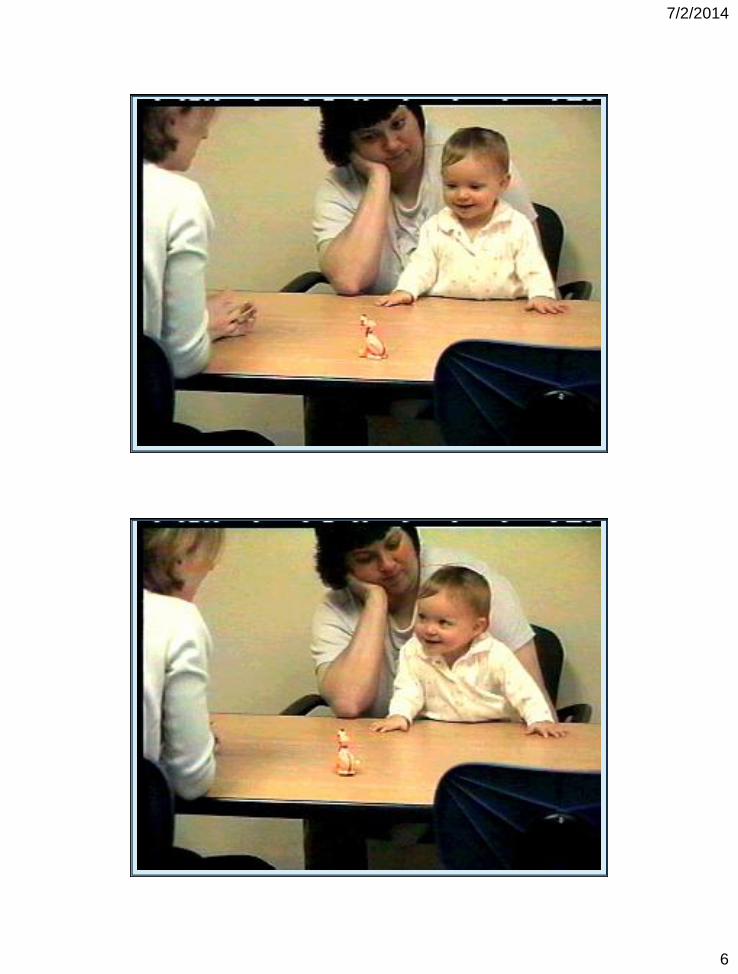
What is joint attention?
7/2/2014
5
7/2/2014
6

7/2/2014
7
Joint attention behaviours are elicited in communicative exchanges
7/2/2014
8
Psycholinguistic theory or ‘How babies learn to talk’
• Synchronous interaction b/t parent + child is
scaffold for emerging communication
─ Referential understanding (what is being said)
─ Intersubjectivity (comprehension that the acts of others
have intent and communicative significance)
• Referential understanding is pivotal for
vocabulary growth and pragmatics
• Behaviour of caregiver influences
development
─ Attending to communication acts increases them
─ Expansion from child’s base (‘semantic contingency’)
leads to more vocabulary
Early social communication in ASD
• Although deficits in JA are amongst the earliest
signs of ASD…
– Early JA abilities related to later language (Charman et
al., 2003; Mundy et al., 1990)
– Early JA related to later symptom severity (Charman,
2003)
– In TD early JA related to later theory of mind skills
(Charman et al., 2000)
– JA skills at 2 years predict outcomes at 7 years
(Charman et al., 2005; Veness et al., 2014)
• Whilst an early impairment; developmental
continuity with that seen in typical
development

7/2/2014
9
Testing developmental theory
7/2/2014
10
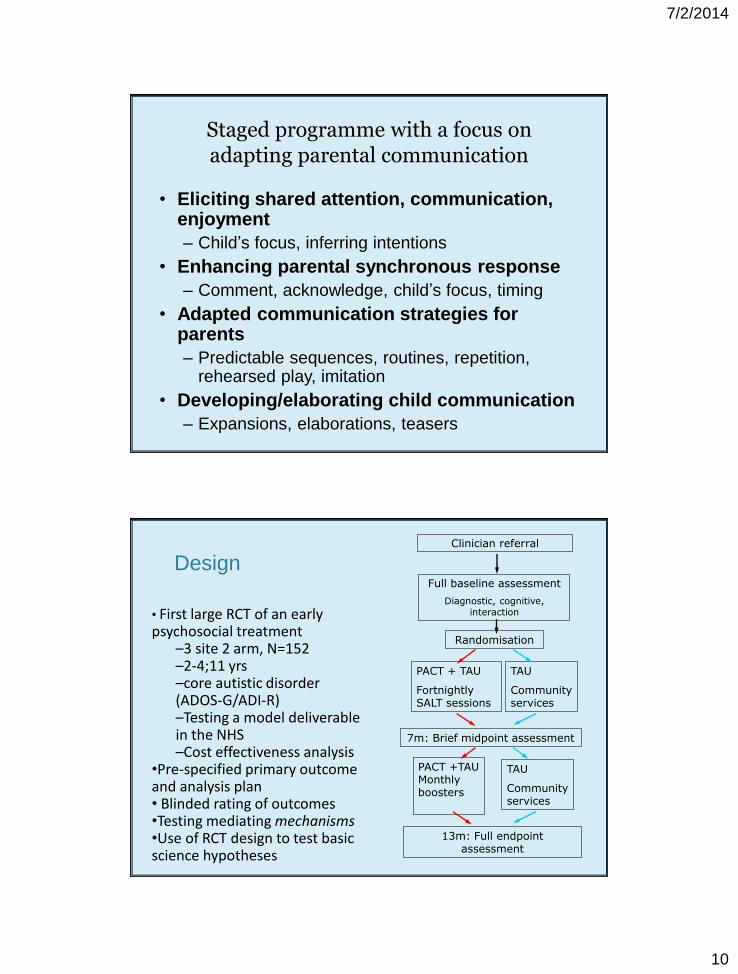
Staged programme with a focus on adapting parental communication
• Eliciting shared attention, communication, enjoyment
– Child’s focus, inferring intentions
• Enhancing parental synchronous response
– Comment, acknowledge, child’s focus, timing
• Adapted communication strategies for parents
– Predictable sequences, routines, repetition, rehearsed play, imitation
• Developing/elaborating child communication
– Expansions, elaborations, teasers
Clinician referral
Full baseline assessment
Diagnostic, cognitive, interaction
PACT + TAU
Fortnightly SALT sessions
7m: Brief midpoint assessment
TAU
Community services
13m: Full endpoint assessment
PACT +TAU Monthly boosters
TAU
Community services
Randomisation
Design
• First large RCT of an early psychosocial treatment
–3 site 2 arm, N=152 –2-4;11 yrs –core autistic disorder (ADOS-G/ADI-R) –Testing a model deliverable in the NHS –Cost effectiveness analysis
•Pre-specified primary outcome and analysis plan • Blinded rating of outcomes •Testing mediating mechanisms •Use of RCT design to test basic science hypotheses
7/2/2014
11
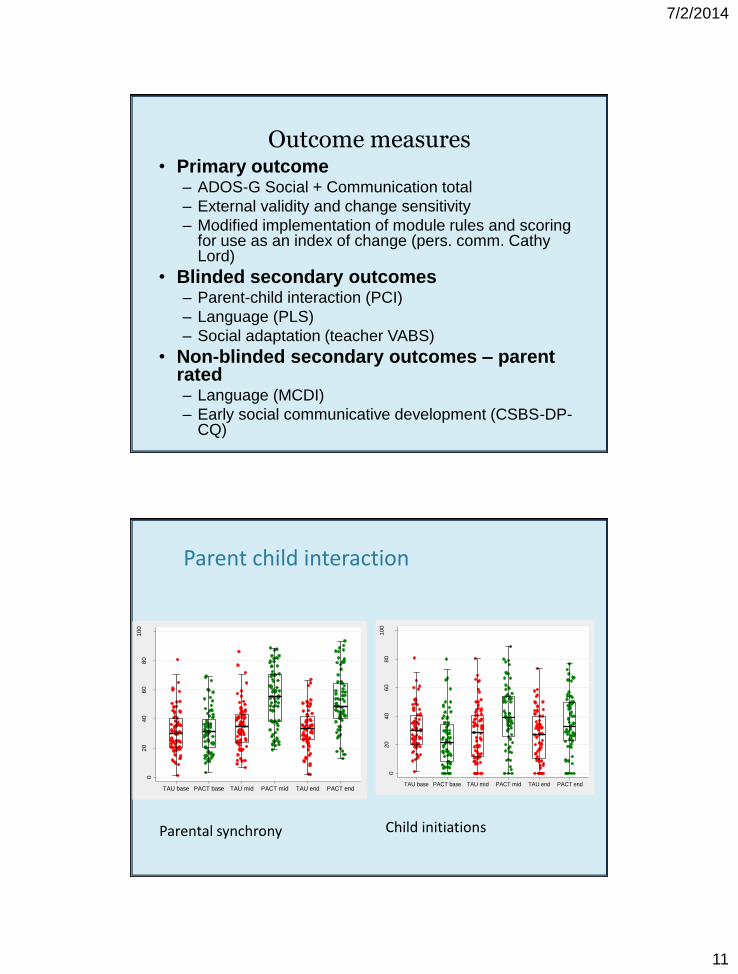
Outcome measures • Primary outcome
– ADOS-G Social + Communication total
– External validity and change sensitivity
– Modified implementation of module rules and scoring for use as an index of change (pers. comm. Cathy Lord)
• Blinded secondary outcomes – Parent-child interaction (PCI)
– Language (PLS)
– Social adaptation (teacher VABS)
• Non-blinded secondary outcomes – parent rated – Language (MCDI)
– Early social communicative development (CSBS-DP-CQ)
020
40
60
80
100
PC
I: p
erc
ent
of
child
acts
initia
tion
TAU base PACT base TAU mid PACT mid TAU end PACT end
020
40
60
80
100
PC
I: p
erc
ent
of
pare
nt
acts
in s
ynchro
ny
TAU base PACT base TAU mid PACT mid TAU end PACT end
Parent child interaction
Parental synchrony Child initiations
7/2/2014
12
01
02
03
0
Mo
difie
d A
DO
S-G
socia
l-co
mm
un
ica
tio
n to
tal
TAU baseline PACT baseline TAU endpoint PACT endpoint
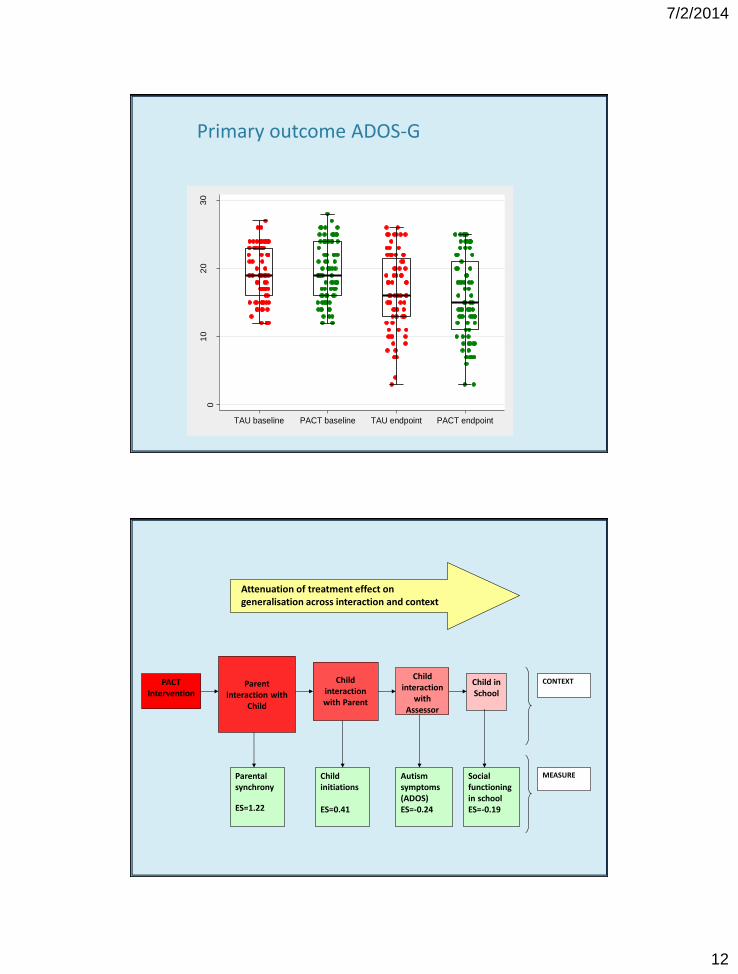
Primary outcome ADOS-G
PACT Intervention
Attenuation of treatment effect on generalisation across interaction and context
Parent interaction with
Child
Parental synchrony
ES=1.22
Child interaction with Parent
Child interaction
with Assessor
Child in School
Child initiations ES=0.41
Autism symptoms (ADOS) ES=-0.24
Social functioning in school ES=-0.19
CONTEXT
MEASURE
7/2/2014
13
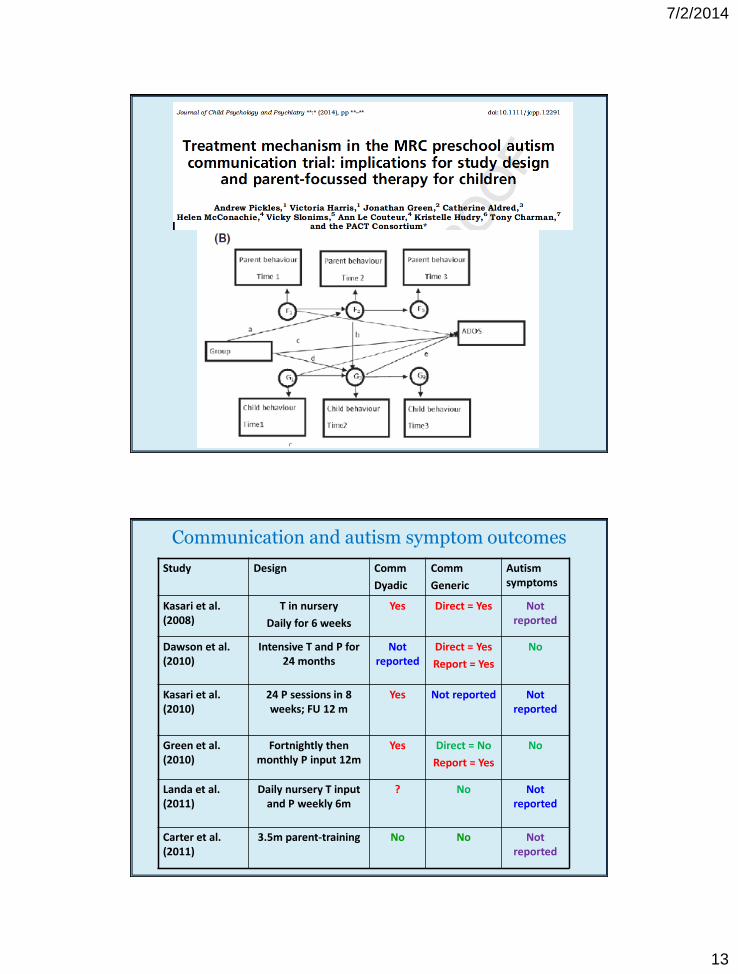
Communication and autism symptom outcomes
Study Design Comm
Dyadic
Comm
Generic
Autism symptoms
Kasari et al. (2008)
T in nursery
Daily for 6 weeks
Yes Direct = Yes
Not reported
Dawson et al. (2010)
Intensive T and P for 24 months
Not reported
Direct = Yes
Report = Yes
No
Kasari et al. (2010)
24 P sessions in 8 weeks; FU 12 m
Yes Not reported Not reported
Green et al. (2010)
Fortnightly then monthly P input 12m
Yes
Direct = No
Report = Yes
No
Landa et al. (2011)
Daily nursery T input and P weekly 6m
? No Not reported
Carter et al. (2011)
3.5m parent-training No No Not reported
7/2/2014
14
(Some) agreement on shared targets, content
• Targeting early social communication skills
• Within the context of dyadic relational
interaction
• Core curriculum includes:
– Promoting joint attention and joint engagement,
imitation and pretend play
– Emphasise reciprocity, emotional attunement,
following child initiated exchanges
• Differences in structure, delivery + intensity
– Degree of directiveness and behavioural techniques
– Parent- or therapist-mediated, intensity and length
Why was the work liked (by some)?
• Based on well-established psychological
theory (developmental not autism)
• The fact that similar associations were found
in typical and atypical development
strengthened confidence in the finding
• Combination of longitudinal and intervention
effects further strengthened confidence
• Focused on (putative) ‘core’ or ‘primary’
symptoms
• Developmental cascade model is inherently
attractive (if you are an optimist)…
7/2/2014
15
An alternative evidence-base?
• 40 year story going back to 1970s
• Intensive behavioural intervention
– Lovaas/ABA/Early Intensive Behavioural Intervention
– Originally ‘discrete trial training’ (DTT), now includes
‘pivotal response training’ (PRT)
– Strongly held views (primarily in North America)
regarding the evidence-base for EIBI
• Against NICE/Cochrane evidence weak
– Very few RCTs, mostly case/control studies
– No primary outcome, unclear re. blinding, small Ns
• Claims of positive outcome and ‘cure’
– In mainstream class and ‘Indistinguishable from peers’
For some consensus has been reached
• Promising Early Start Denver Model (ESDM)
– Dawson et al (2010) Pediatrics
– 2 years, 25 hours per week, combined behavioural
and developmental/dyadic
• Many reviews and states now mandate EIBI
as the best-evidenced intervention for ASD
– View that 15-25 hours is required
– Main technique (and theory) is behavioural/ABA
– Focus is on skills acquisition
– Vary in social-communication/developmental focus
• RCTs not possible
– Beyond equipoise; very intensive treatment; ethics
7/2/2014
16
NICE systematic review process • NCCMH team agreed with GDG early on
– At least 2 RCTs allowing some meta-analysis
– Many/most trials low quality criterion
• Paucity of trials and those with similar
outcomes prevented much meta-analysis
• Some aspects of social-communication
interventions just ‘missed the cut’
• More cautious (on the basis of evidence)
than some other (child) MH NICE guidance
• Recent Cochrane reviews more positive
– Parent-mediated, JA-theory of mind, social skills…
7/2/2014
17
NICE – Children and Young People
• ‘Consider’ a social-communication
intervention
– To increase joint attention, engagement, reciprocal
communication
– Mediated by parent, teacher or (school-age) peers
• Support in developing life skills
• Adapted CBT for anxiety
• Interventions for challenging behaviour and
co-existing mental health problems
7/2/2014
18
Glass half full or half empty?
• At last autism field conducting RCTs!
• Standards of reporting improving
– Primary outcomes; blinding; ITT analyses
• Many of the programmes have overlapping
theoretical basis, aims and techniques
– Target social communication and social interaction
– Often combine (in different proportions) behavioural
and developmental theory
• How to compare and integrate ‘best practice’
from the accumulating evidence?
• What are the appropriate goals/outcomes?
– And how do we measure them?
Ways forward…? • Clearly need to conduct more trials
– iBASIS
– Group parent training in NIHR PG
– Current applications (EME, H2020)
• How to square the circle between NICE and
‘received wisdom’ poorer quality studies…?
• How to square with current highly variable
(and often low) post-diagnostic provision?
– What treatment is provided (in health, in education)..?
– How well evidence-based it is..?
– What should the model of treatment be for ‘chronic’
neurodevelopmental disorders…as opposed to
episodic psychiatric disorders?




















