
De novo partial 2p duplication with postmortem description
10
American Journal of Medical Genetics 10:55-64 (1981) De Novo Partial 2p Duplication With Postmortem Description P. L. Monteleone, J. D. Blair, E. R. Graviss, Su-chiung Chen, A. Salvador, J. A. Grzegocki, and J. A. Monteleone DepartmentofPediatrics(P.L.M.,S.C.,A.S., J.A.G.,J.A.M.), Pathology(J.D.B.),and Radiology (E. R.G.), St. Louis University School of Medicine and Cardinal Glennon Memorial Hospital for Children, St. Louis An unbalanced karyotype most likely consisting of a partial duplication of the short arm of chromosome 2 (pl3+pter) was found in a newborn infant with intrauterine growth retardation, facial, skeletal, and cardiac abnormalities. There was no evidence of a translocation in either parent. At autopsy, striking histopathologic abnormalities were detected in the central nervous system and ovaries. Key words: ovarian dysplasia, partial duplication 2p, fused sternum, hypoplastic pubis INTRODUCTION A syndrome of mental and growth retardation due to duplication of the distal half of 2p was first described by Francke and Jones [1976]. Fourteen cases of this syndrome have been reviewed by Cassidy et a1 [1977]. All 14 cases had a translocation carrier parent [Armendares and Salamanca-Gomez, 1978; Buyse et al, 1977; Bender et al, 1969; Cassidy et al, 1976; Cassidy et al, 1977; Francke and Jones, 1976; Magenis et al, 1975; Neu et al, 1979; Sekhon et al, 1978; Stoll et al, 1974; Yunis, 19781. Only one report [Neu et al, 19791 described autopsy findings in a male with partial 2p duplication. port of autopsy findings in a female patient with this syndrome. In the family described here, no translocation carrier was identified. It is the first re- REPORT OF PATIENT History The patient was a 1,900-g white female born to a 3 1-year-old gravida 1 para 1 aborta 0 white mother and 33-year-old white father at 40 weeks’ gestation by spontaneous vaginal delivery. Pregnancy and labor were unremarkable. The patient had no spontaneous respira- Received for publication November 1, 1980; revision received March 16, 1981. Address all correspondence and reprint requests to P. Monteleone, MD, Cardinal Glennon Memorial Hospital for Children, 1465 South Grand Boulevard, St. Louis, MO 63104. 0148-7299/81/1001-0055$03.00 0 1981 Alan R. Liss, Inc.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of De novo partial 2p duplication with postmortem description
American Journal of Medical Genetics 10:55-64 (1981)
De Novo Partial 2p Duplication With Postmortem Description P. L. Monteleone, J. D. Blair, E. R. Graviss, Su-chiung Chen, A. Salvador, J. A. Grzegocki, and J. A. Monteleone
DepartmentofPediatrics(P.L.M.,S.C., A.S., J.A.G.,J.A.M.), Pathology(J.D.B.),and Radiology (E. R.G.), St. Louis University School of Medicine and Cardinal Glennon Memorial Hospital for Children, St. Louis
An unbalanced karyotype most likely consisting of a partial duplication of the short arm of chromosome 2 (pl3+pter) was found in a newborn infant with intrauterine growth retardation, facial, skeletal, and cardiac abnormalities. There was no evidence of a translocation in either parent. At autopsy, striking histopathologic abnormalities were detected in the central nervous system and ovaries.
Key words: ovarian dysplasia, partial duplication 2p, fused sternum, hypoplastic pubis
INTRODUCTION
A syndrome of mental and growth retardation due to duplication of the distal half of 2p was first described by Francke and Jones [1976]. Fourteen cases of this syndrome have been reviewed by Cassidy et a1 [1977]. All 14 cases had a translocation carrier parent [Armendares and Salamanca-Gomez, 1978; Buyse et al, 1977; Bender et al, 1969; Cassidy et al, 1976; Cassidy et al, 1977; Francke and Jones, 1976; Magenis et al, 1975; Neu et al, 1979; Sekhon et al, 1978; Stoll et al, 1974; Yunis, 19781. Only one report [Neu et al, 19791 described autopsy findings in a male with partial 2p duplication.
port of autopsy findings in a female patient with this syndrome. In the family described here, no translocation carrier was identified. It is the first re-
REPORT OF PATIENT
History
The patient was a 1,900-g white female born to a 3 1 -year-old gravida 1 para 1 aborta 0 white mother and 33-year-old white father at 40 weeks’ gestation by spontaneous vaginal delivery. Pregnancy and labor were unremarkable. The patient had no spontaneous respira-
Received for publication November 1, 1980; revision received March 16, 1981.
Address all correspondence and reprint requests to P. Monteleone, MD, Cardinal Glennon Memorial Hospital for Children, 1465 South Grand Boulevard, St. Louis, MO 63104.
0148-7299/81/1001-0055$03.00 0 1981 Alan R. Liss, Inc.
56 Monteleone et al
tions at birth and was intubated. Both placenta and cord were small. Family history was negative for multiple congenital anomalies and for parental exposure to x-rays or clasto- gens. There was no consanguinity.
Physical Examination
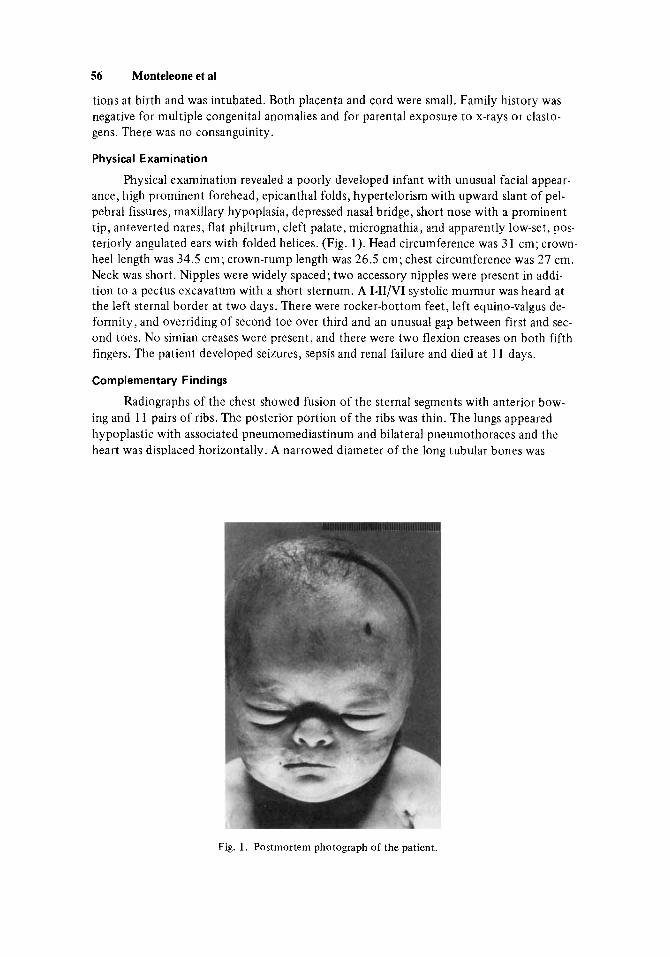
Physical examination revealed a poorly developed infant with unusual facial appear- ance, high prominent forehead, epicanthal folds, hypertelorism with upward slant of pel- pebral fissures, maxillary hypoplasia, depressed nasal bridge, short nose with a prominent tip, anteverted nares, flat philtrum, cleft palate, micrognathia, and apparently low-set, pos- teriorly angulated ears with folded helices. (Fig. 1). Head circumference was 31 cm; crown- heel length was 34.5 cm; crown-rump length was 26.5 cm; chest circumference was 27 cm. Neck was short. Nipples were widely spaced; two accessory nipples were present in addi- tion to a pectus excavatum with a short sternum. A I-II/VI systolic murmur was heard at the left sternal border at two days. There were rocker-bottom feet, left equino-valgus de- formity, and overriding of second toe over third and an unusual gap between first and sec- ond toes. No simian creases were present, and there were two flexion creases on both fifth fingers. The patient developed seizures, sepsis and renal failure and died at 11 days.
Complementary Findings
Radiographs of the chest showed fusion of the sternal segments with anterior bow. ing and 11 pairs of ribs. The posterior portion of the ribs was thin. The lungs appeared hypoplastic with associated pneumomediastinum and bilateral pneumothoraces and the heart was displaced horizontally. A narrowed diameter of the long tubular bones was
Fig. 1. Postmortem photograph of the patient.
De Novo Partial 2p Duplication 57
more apparent distal than proximal. The pubic bones were hypoplastic but the acetabular and iliac angles were normal. Electrocardiogram showed superiorly oriented frontal QRS axis of -90" to -120" and right atrial hypertrophy. On an intravenous urogram, the kid- neys were poorly visualized.
Autopsy Findings
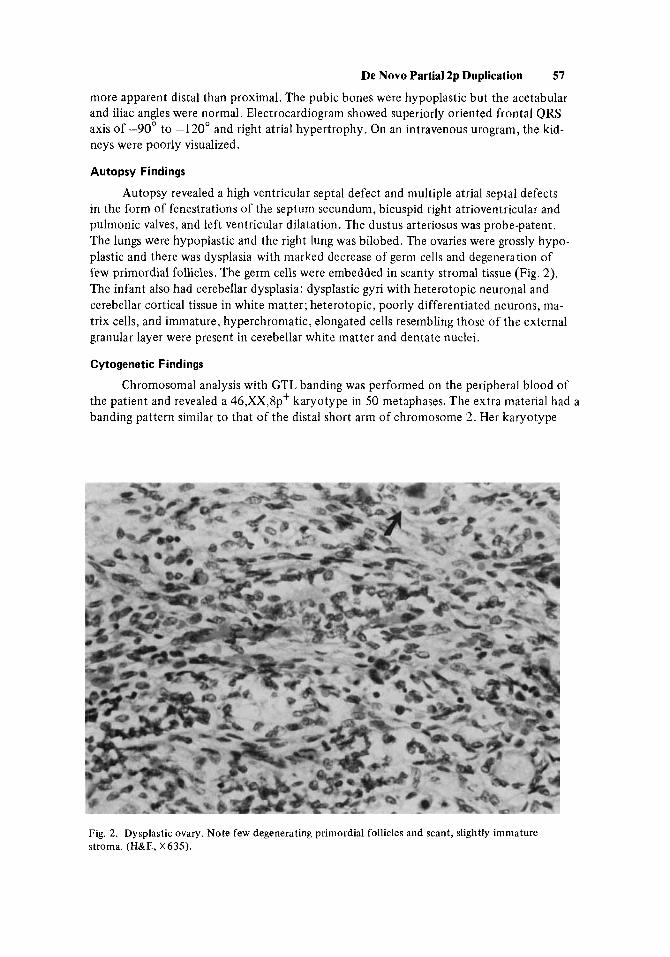
Autopsy revealed a high ventricular septal defect and multiple atrial septal defects in the form of fenestrations of the septum secundum, bicuspid right atrioventricular and pulmonic valves, and left ventricular dilatation. The dustus arteriosus was probe-patent. The lungs were hypoplastic and the right lung was bilobed. The ovaries were grossly hypo- plastic and there was dysplasia with marked decrease of germ cells and degeneration of few primordial follicles. The germ cells were embedded in scanty stromal tissue (Fig. 2). The infant also had cerebellar dysplasia: dysplastic gyri with heterotopic neuronal and cerebellar cortical tissue in white matter; heterotopic, poorly differentiated neurons, ma- trix cells, and immature, hyperchromatic, elongated cells resembling those of the external granular layer were present in cerebellar white matter and dentate nuclei.
Cytogenetic Findings
the patient and revealed a 46,XX,8pt karyotype in 50 metaphases. The extra material had a banding pattern similar to that of the distal short arm of chromosome 2. Her karyotype
Chromosomal analysis with GTL banding was performed on the peripheral blood of
Fig. 2. Dysplastic ovary. Note few degenerating primordial follicles and scant, slightly immature stroma. (H&E, X635).
TAB
LE I.
Dup
licat
ion
(2p)
Syn
drom
e
1 2
3 4
5 6
7 8
Ref
eren
ce
[I01
[7
1 16
1 15
1
-
Ban
ding
met
hod
Pare
ntal
tran
sloc
atio
n
Patie
nt
Sex
Ges
tatio
n B
irth
wei
ght
(gm
) B
irth
leng
th (
cm)
Age
at r
epor
t G
row
th r
etar
datio
n Ps
ycho
mot
or r
etar
datio
n C
rani
ofac
ial a
rea
Hig
h pr
omin
ent
fore
head
Fr
onta
l ups
wee
p of
hai
r H
y per
telo
rism
Ep
ican
thal
fol
ds
Max
illar
y hy
popl
asia
Sh
ort n
ose
with
pro
min
ent
Bro
ad a
lveo
lar
ridge
s/na
r-
Smal
l man
dibl
e/po
inte
d ch
in
Ptos
is
Stra
bism
us
Myo
pia
Dac
ryos
teno
sis
Hyd
roce
phal
us
Web
bing
of
neck
tip (
“pug
nos
e”)
row
pal
ate
R Q
G
G
t(2;
I 4)(
p22;
pll)
mat
t(
2;18
)(p2
3;pl
l)pa
t t(
2;7)
(p23
;q36
)mat
t(
2;3)
(p23
;p27
)mat
1 M
term
3,
200
50
7 Yr
<
3rd%
pr
ofou
nd
+ + + + + + + + + + + -
-
-
2 M
term
3,
450
52
3 m
o ..
. ..
.
+ + + - + + + + -
-
-
-
-
-
-
F 41 w
k 3,
700
53
9 m
o (4
yr)
< 3
rd%
pr
ofou
nd
+ + - + + + + + - + + + -
-
1 M
40 w
k 2,
350
46
< 3r
d%
prof
ound
8 yr
+ + + + + + + + + + + + -
-
2 F 42 w
k 2,
260
53
12 y
r < 3
rd%
pr
ofou
nd
+ + + - + + + + + - + + -
-
1 M
term
3,
525
5 Yr
<5
th%
m
arke
d
...
+ - + + + + + + + + ...
-
-
-
2 M
term
3,
465
1 Yr
<
5th%
de
laye
d
...
+ - + + + + + + + + ...
+ -
-
3 M
term
3,
125
18 y
r <5
th%
pr
ofou
nd
...
+ + + - + + + + - + ...
-
-
-
c
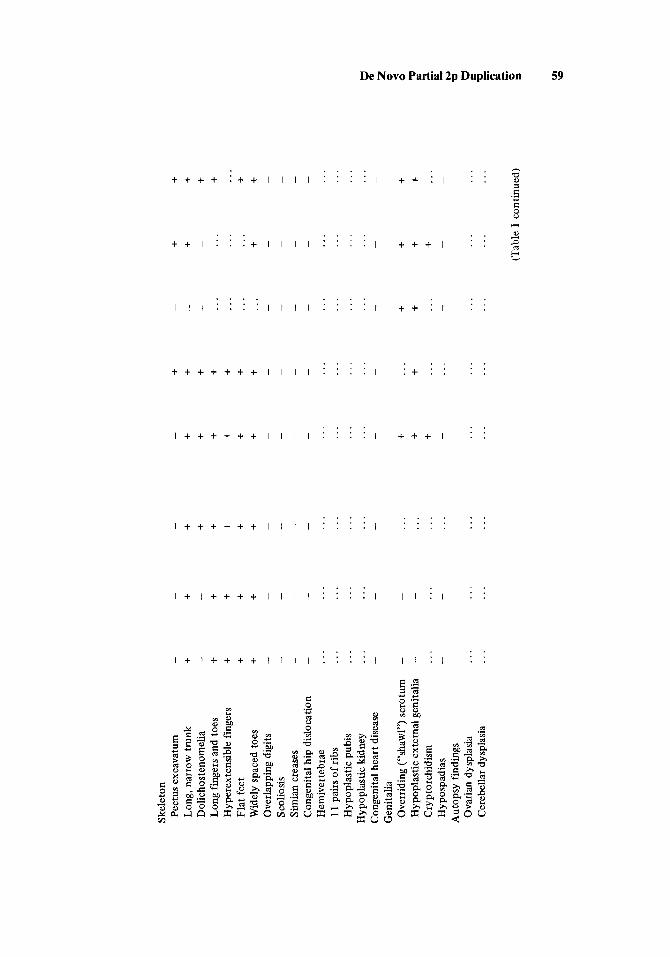
Skel
eton
Pe
ctus
exc
avat
um
Long
, nar
row
tru
nk
Dol
icho
sten
omel
ia
Long
fing
ers
and
toes
H
yper
exte
nsib
le f
inge
rs
Flat
fee
t W
idel
y sp
aced
toes
O
verla
ppin
g di
gits
S c
olio
sis
Sim
ian
crea
ses
Con
geni
tal h
ip d
islo
catio
n H
emiv
erte
brae
11
pai
rs o
f ri
bs
Hyp
opla
stic
pub
is
Hyp
opla
stic
kid
ney
Con
geni
tal h
eart
dis
ease
G
enita
lia
Ove
rrid
ing
(“sh
awl”
) sc
rotu
m
Hyp
opla
stic
ext
erna
l gen
italia
C
rypt
orch
idis
m
H yp
ospa
dias
A
utop
sy f
indi
ngs
Ova
rian
dysp
lasi
a C
ereb
ella
r dy
spla
sia
...
...
...
...
...
...
...
...
-
-
...
...
-
-
...
...
...
...
...
-
- ... ...
...
...
- + + + - ...
...
-
- ...
...
...
...
- ... + ..
.. ...
...
-
-
- ...
...
...
...
-
-
-
- ...
...
...
...
- + + ..
-
+ +
+ +
-
+ ..
. +
...
...
...
+ +
+
-
-
-
-
...
...
...
...
...
...
...
...
-
-
+ +
+ +
+ ..
. -
-
...
...
...
...
z s ii
(Tab
le I
con
tinue
d)
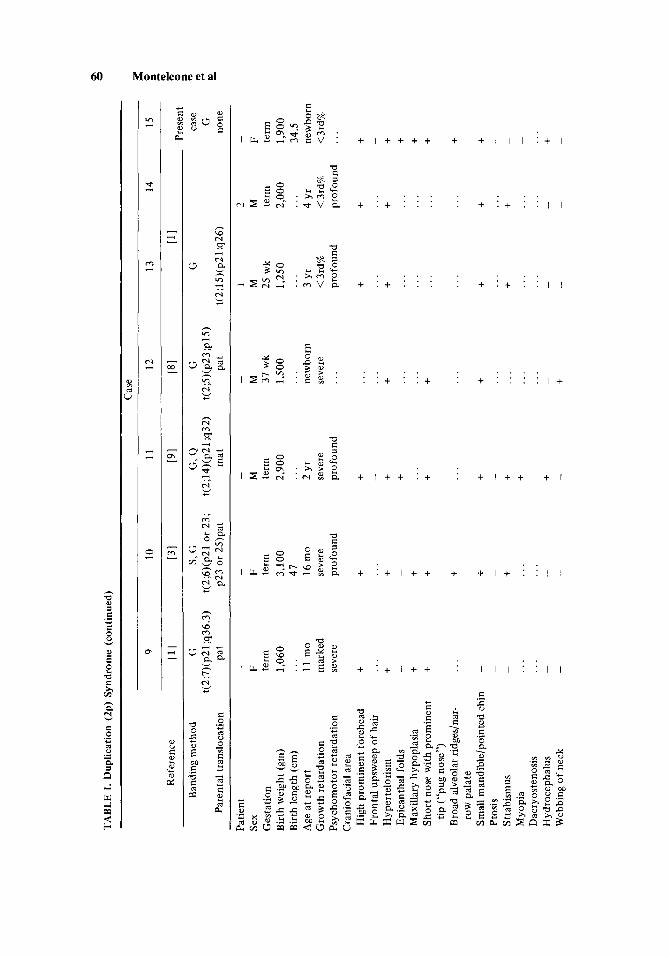
TAB
LE I
. Dup
licat
ion
(2p)
Syn
drom
e (c
ontin
ued)
Cas
e
9 10
11
12
13
14
15
Pres
ent
Ref
eren
ce
Ill
[31
191
PI
111
Ban
ding
met
hod
G
s, G
G, Q
G
G
ca
se
Pare
ntal
tran
sloc
atio
n Pa
t p2
3 or
25)
pat
mat
Pa
t t(
2;15
)(p2
1 :q2
6)
none
t(
2;7)
(p21
;q36
.3)
t(2;
6)(p
21 o
r 23
; t(
2;14
)(p2
1;q3
2)
t(2;
5)(p
23;p
W
G
Patie
nt
Sex
Ges
tatio
n B
irth
wei
ght
(gm
) B
irth
leng
th (
cm)
Age
at r
epor
t G
row
th re
tard
atio
n Ps
ycho
mot
or r
etar
datio
n C
rani
ofac
ial a
rea
Hig
h pr
omin
ent f
oreh
ead
Fron
tal u
psw
eep
of h
air
Hyp
erte
lori
sm
Epic
anth
al f
olds
M
axill
ary
hypo
plas
ia
Shor
t now
with
pro
min
ent
Bro
ad a
lveo
lar r
idge
s/na
r-
Smal
l man
dibl
e/po
inte
d ch
in
Ptos
is
Stra
bism
us
Myo
pia
Dac
ryos
teno
sis
Hyd
roce
phal
us
Web
bing
of
neck
tip (
“pug
nos
e”)
row
pal
ate
-
F term
1,
060
11 m
o m
arke
d se
vere
...
+ ...
+ - + + ...
-
-
- ...
...
-
-
-
F term
3,
100
41
16
mo
seve
re
prof
ound
-
M
term
2,
900
...
2 Yr
se
vere
pr
ofou
nd
-
M
31 w
k 1,
500
new
born
se
vere
...
...
1 M
25 w
k 1,
250
2 M
term
2,
000
4 yr
<
3rd%
pr
ofou
nd
...
-
F term
1,
900
34.5
ne
wbo
rn
<3rd
%
...
3 yr
<
3rd%
pr
ofou
nd
t ...
+ - + +
+ - + +
t ...
+
t ...
+
+ ..
. ..
. + ..
. ..
. +
...
...
...
+ ..
.
t
...
+ - +
+ ...
...
...
...
+ ...
+
+ ...
+ ..
. ..
. -
-
t
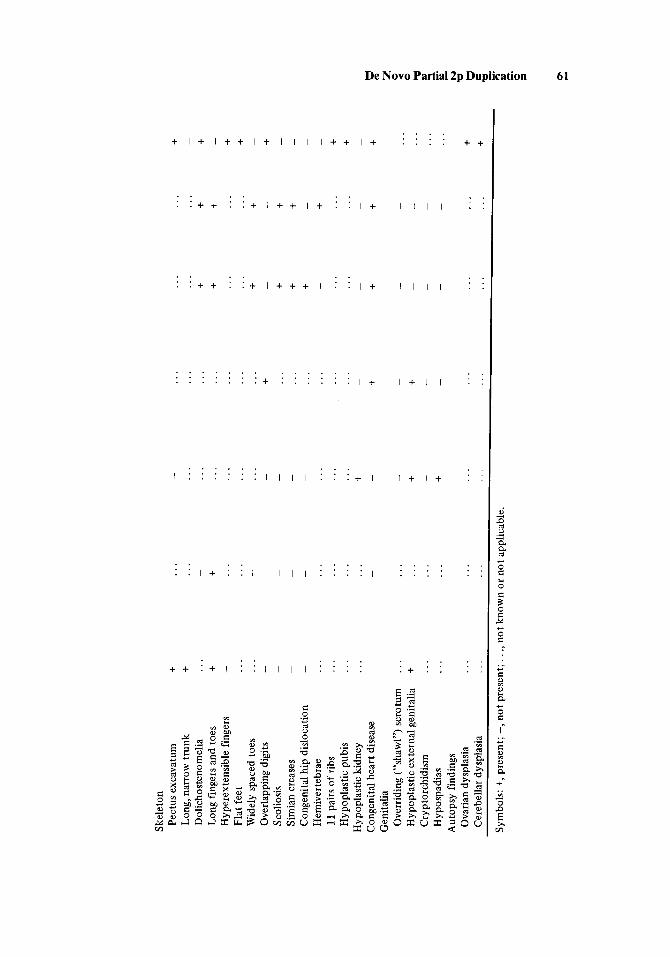
Skel
eton
Pe
ctus
exc
avat
um
Long
, nar
row
tru
nk
Dol
icho
sten
omel
ia
Long
fin
gers
and
toes
H
yper
exte
nsib
le f
inge
rs
Flat
feet
W
idel
y sp
aced
toes
O
verla
ppin
g di
gits
Sc
olio
sis
Sim
ian
crea
ses
Con
geni
tal h
ip d
islo
catio
n H
emiv
erte
brae
11
pai
rs o
f ri
bs
Hyp
opla
stic
pub
is
Hyp
opla
stic
kid
ney
Con
geni
tal h
eart
dis
ease
G
enita
lia
Ove
rrid
ing
(“sh
awl”
) sc
rotu
m
Hyp
opla
stic
ext
erna
l gen
italia
C
rypt
orch
idis
m
H yp
ospa
dias
A
utop
sy f
indi
ngs
Ova
rian
dysp
lasi
a C
ereb
ella
r dys
plas
ia
+ + ...
+ - ...
...
-
-
-
- ...
...
...
...
- ...
+ ...
...
...
...
- + ...
...
-
-
-
-
- ...
...
...
...
- ...
...
...
...
...
...
+
...
...
...
...
...
...
+ ...
...
...
...
...
...
- + - + -
-
...
...
+ + ...
...
+ - + + + - ...
...
- + -
-
-
-
...
...
+ -k ...
...
+ - + + - + ...
...
- + -
-
-
-
+ - + - + + - + -
-
-
- + + - + ...
...
...
...
...
...
...
...
...
...
a +
...
...
...
...
+ 5
’E
! i;’
...
...
Sym
bols
: +, p
rese
nt; -, n
ot p
rese
nt;.
. ., no
t kno
wn
or n
ot a
pplic
able
. $. 3
ch 3
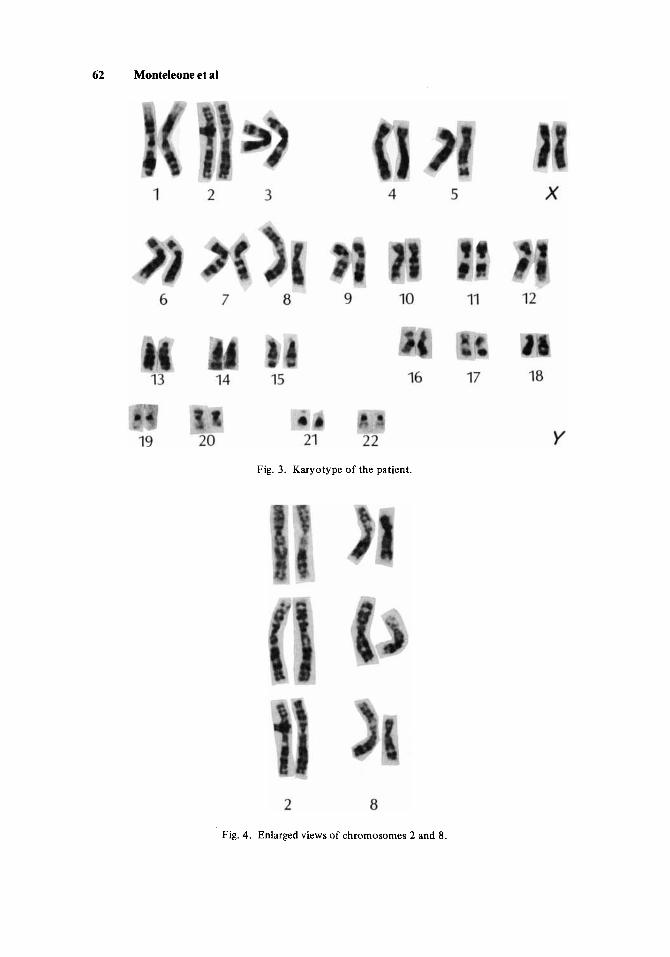
62 Monteleone et al
Fig. 3. Karyotype of the patient.
Fig. 4. Enlarged views of chromosomes 2 and 8.

De Novo Partial 2p Duplication 63
has been interpreted as 46,XX,-8,+der(8),t(2;8)(p13 ;p23), indicating duplication of re- gion 2p13-+2pter (Figs. 3,4). Chromosomes of both parents were normal. The possibility of non-paternity was looked for and ruled out with major blood groups and chromosome heteromorphisms.
DISCUSSION
Partial duplication of the distal short arm of chromosome 2 has been reported in 14 cases. The characteristic clinical features are physical and mental retardation, unusual facial appearance with microcephaly, frontal bossing, hypertelorism, antimongoloid slant, flat nasal bridge, epicanthal folds, strabismus, myopia, ptosis, broad gums, anteverted nares, highly arched palate, long philtrum, and malformed ears. Several cases have had heart murmurs, abnormal sternal segmentation, pectus excavatum, thin posterior ribs and nar- rowed diaphyses of the long tubular bones. Several males have had a small penis and cryptorchidism. Our patient showed most of the described clinical findings. In addition, she had a cleft soft palate and hypoplastic pubic bones that have not been previously re- ported in this entity.
Neu [ 19791 reported autopsy findings on one patient who had a “double-outlet right ventricle and transposition of the great arteries, hypoplastic right ventricle, atrial septal defect, ventricular septal defect and patent ductus arteriosus.” Microscopic examina- tion of frontal lobe sections revealed heterotopias of undifferentiated neurons and stream- ing groups of matrix cells within the white matter between the floor of the ventricle and cortex of the frontal lobe. Very similar brain lesions were found in our patient. The central nervous system findings are similar to those described by Terplan [ 19661 in the cerebellum of patients with trisomy 13 and in the frontal lobe of the patient described in Neu et a1 [1979]. Thus, these dysplastic lesions are not specific for either trisomy 13 or partial du- plication of 2p. Small penis and cryptorchism have been found in male patients. There has been no previous autopsy report on female patients. The autopsy of our case demonstrated ovarian dysplasia.
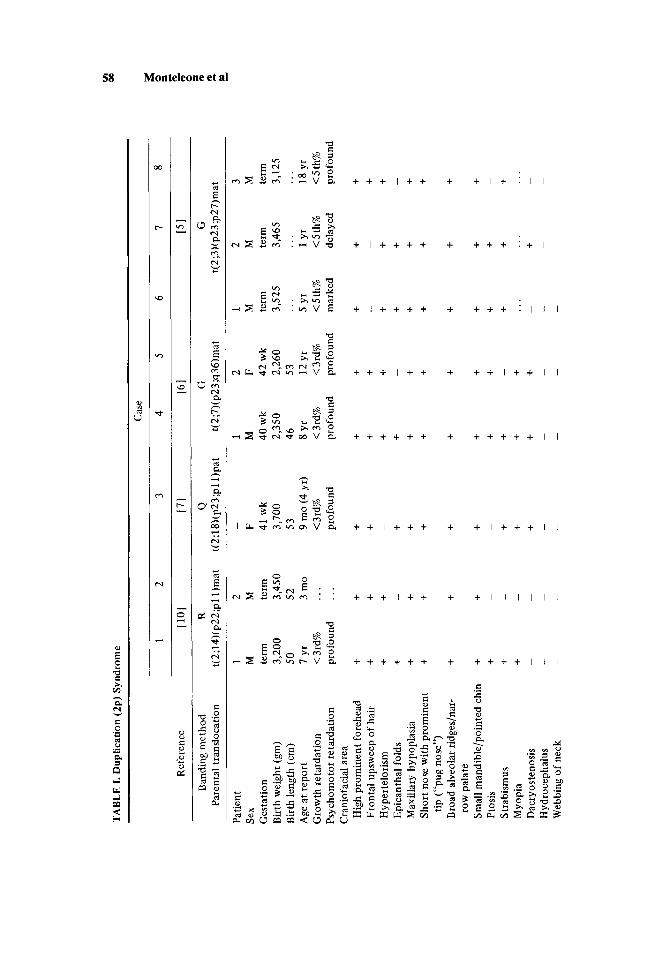
The clinical findings in all patients including the present case are very similar in spite of the fact that different amounts of 2p were duplicated (Table I). The 14 previously re- ported cases had a carrier parent with translocations between 2p and chromosomes 3 , 5 , 7, 14, 15 or 18. Our patient did not have a carrier parent and thus her translocation is sporadic. The risk of recurrence is unknown, but presumed to be low.
ACKNOWLEDGMENTS
We wish to acknowledge the help of Dr. H. Chung for his review of the neuropathol- ogy findings and Dr. Rathaya Vongsnichakul for the initial postmortem report. We thank Michael Tietjens and Tanvagarn Satayaviboon for their invaluable assistance.
REFERENCES
Armendares S, Salamanca-Gomez F (1978): Partial 2p trisomy (p2l jp te r ) in two siblings of a family
Buyse M, Bull MJ, Atkins L (1977): Prenatal diagnosis of partial trisomy 2p. Am J Hum Genet 29:26A. Bender K, Reinwein H, Gorman LZ et a1 (1969): Familiare 2/C-translocation: 46,XY,t(2p-*;Cp+) und
with a 2p-*:15q+ translocation. Clin Genet 13:17-24.
46,XX,Cpf. Humangenetik 8:94-104.
64 Monteleone et al
Cassidy SB, McGee BJ, Heller RM et a1 (1976): Distal 2p trisomy (2) (p23-tter) in three members of a family with a balanced 2p-;3p' translocation. Abstracts V International Congress of Human Genetics. Mexico City, October.
J Pediatr 91(6):934-938. Cassidy SB, Heller RM, Chazen EM et a1 (1977): The chromosome 2 distal short-arm trisomy syndrome.
Francke U, Jones KL (1976): The 2p partial trisomy syndrome. Am J Dis Child 130:1244-1249. Magenis RE, Koler RD, Lovrien E et a1 (1975): Gene dosage: Evidence for assignment of erythrocyte
acid phosphatase locus to chromosome 2. Proc Natl Acad Sci USA 72:4526-4530. Neu RL, Dennis NR, Fisher JE (1979): Partial 2p trisomy in a 46,XY,der(5),t(2;5)(p23;plS)pat infant;
autopsy findings. Anna1 Gbnbt 22(1):33-34. Sekhon GS, Taysi K, Rath R (1978): Partial trisomy for the short arm of chromosome 2 due to familial
balanced translocation. Hum Genet 44:99-103. Stoll C, Messer J, Vors J (1974): Translocation t(2;14) equilibrbe chez une mere et trisomie partielle
d'une partie du bras court d'un chromosome No. 2 chez deux de ses enfants. Ann G h b t (Paris) 17: 193-196.
Terplan KL, Sandberg AA, Aceto T Jr (1966): Structural anomalies in the cerebellum in association with trisomy. JAMA 197(7):557-568.
Edited by Uta Francke




















