
Intrahepatic Gas at Postmortem Computed Tomography: Forensic Experience as a Potential Guide for In...
10
Intrahepatic Gas at Postmortem Computed Tomography: Forensic Experience as a Potential Guide for In Vivo Trauma Imaging Christian Jackowski, MD, Martin Sonnenschein, MD, Michael J. Thali, MD, Emin Aghayev, MD, Kathrin Yen, MD, Richard Dirnhofer, MD, and Peter Vock, MD Background: Until August 2004 there were 106 forensic cases examined with post- mortem multislice computed tomography (MSCT) and magnetic resonance (MR) im- aging before traditional autopsy within the Virtopsy project. Intrahepatic gas (IHG) was a frequent finding in postmortem MSCT examinations. The aim of this study was to investigate its cause and significance. Methods: There were 84 virtopsy cases retrospectively investigated concern- ing the occurrence, location, and volume of IHG in postmortem MSCT imaging (1.25 mm collimation, 1.25 mm thickness). We assessed and noted the occurrence of intes- tinal distention, putrefaction, and systemic gas embolisms and the cause of death, pos- sible open trauma, possible artificial respi- ration, and the postmortem interval. We investigated the relations between the find- ings using the contingency table ( 2 test) and the comparison of the postmortem in- tervals in both groups was performed using the t test in 79 nonputrefied corpses. Results: IHG was found in 47 cases (59.5%). In five of the cases, the IHG was caused or influenced by putrefaction. Gas distribution within the liver of the remain- ing 42 cases was as follows: hepatic arter- ies in 21 cases, hepatic veins in 35 cases, and portal vein branches in 13 cases; among which combinations also occurred in 20 cases. The presence of IHG was strongly related to open trauma with sys- temic gas. Pulmonary barotrauma as oc- curring under artificial respiration or in drowning also caused IHG. Putrefaction did not seem to influence the occurrence of IHG until macroscopic signs of putre- faction were noticeable. Conclusions: IHG is a frequent finding in traumatic causes of death and requires a systemic gas embolism. Ex- ceptions are putrefied or burned corpses. Common clinical causes such as necrotic bowel diseases appear rarely as a cause of IHG in our forensic case material. Key Words: Forensic radiology, Vir- topsy, Postmortem imaging, Intrahepatic gas, Gas embolism. J Trauma. 2007;62:979 –988. P ostmortem imaging using multislice computed tomog- raphy (MSCT) and magnetic resonance (MR) imaging is being evaluated by several research groups 1–7 as a postmortem investigation technique alternative to traditional destructive autopsy in selected cases. Thereby, intrahepatic gas (IHG) was recognized as a frequent finding in postmor- tem MSCT examinations. It was first described by Yamazaki et al. 8 as hepatic portal venous gas. Shiotani et al. 9 published the first retrospective study in 190 nontraumatic deaths cor- relating the occurrence of intrahepatic portal venous gas with gastrointestinal distention. Traumatic causes of IHG were missing in this study as well as postmortem alterations such as putrefaction; all cases were scanned within 2 hours postmortem. Having data of more than 100 forensic cases with full body MSCT and MR scanning we intended to investigate the occurrence of IHG according to conditions, that are thought to influence the occurrence of IHG such as venous or sys- temic air embolism, 10 artificial respiration, gastrointestinal distention, and putrefaction. 11 MATERIALS AND METHODS From 106 virtopsy cases, 18 cases presenting with direct traumatic injury of the liver (e.g. total destruction of the corpse when run over by train or gun shot wound channels through the liver), 1 case of adipocire, 1 case that was found in a glacier that was scanned before defrosting as well as 1 newborn, and 1 fetus were excluded. The remaining 84 cases were investigated using the scanning procedures correspond- ing to the virtopsy approach as already described in previous publications from 2000 to 2004. 1,12,13 The severity of IHG was semiquantitatively assessed by a subjective observer-dependent grading score from 0 (no gas within the liver), 1 (small amounts of gas within the small peripheral intrahepatic vessels predominantly in anterior parts of the liver), 2 (moderate amounts of IHG within major intrahepatic vessels) to 3 (large amounts of IHG, completely filling the major hepatic vessels), demonstrated in Figure 1. This grading was supported by an objective quantification of the IHG volume. A three-dimensional volume-rendering model of the liver was generated after manual tracing of the liver contours on axial images on a workstation. Volume Submitted for publication September 12, 2005. Accepted for publication November 18, 2005. Copyright © 2007 by Lippincott Williams & Wilkins, Inc. From the Institute of Forensic Medicine (C.J., M.J.T., E.A., K.Y., R.D.) and the Institute of Diagnostic Radiology, Inselspital, (M.S., P.V.), Univer- sity of Bern, Switzerland. Address for reprints: Christian Jackowski, MD, University of Bern, Institute of Forensic Medicine, IRM – Buehlstrasse 20, CH-3012 Bern, Switzerland; email: [email protected]. DOI: 10.1097/01.ta.0000198733.22654.de The Journal of TRAUMA Injury, Infection, and Critical Care Volume 62 • Number 4 979
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Intrahepatic Gas at Postmortem Computed Tomography: Forensic Experience as a Potential Guide for In...

Intrahepatic Gas at Postmortem Computed Tomography:Forensic Experience as a Potential Guide for In Vivo TraumaImagingChristian Jackowski, MD, Martin Sonnenschein, MD, Michael J. Thali, MD, Emin Aghayev, MD,Kathrin Yen, MD, Richard Dirnhofer, MD, and Peter Vock, MD
Background: Until August 2004 therewere 106 forensic cases examined with post-mortem multislice computed tomography(MSCT) and magnetic resonance (MR) im-aging before traditional autopsy within theVirtopsy project. Intrahepatic gas (IHG)was a frequent finding in postmortemMSCT examinations. The aim of this studywas to investigate its cause and significance.
Methods: There were 84 virtopsycases retrospectively investigated concern-ing the occurrence, location, and volume ofIHG in postmortem MSCT imaging (1.25mm collimation, 1.25 mm thickness). Weassessed and noted the occurrence of intes-tinal distention, putrefaction, and systemicgas embolisms and the cause of death, pos-
sible open trauma, possible artificial respi-ration, and the postmortem interval. Weinvestigated the relations between the find-ings using the contingency table (�2 test)and the comparison of the postmortem in-tervals in both groups was performed usingthe t test in 79 nonputrefied corpses.
Results: IHG was found in 47 cases(59.5%). In five of the cases, the IHG wascaused or influenced by putrefaction. Gasdistribution within the liver of the remain-ing 42 cases was as follows: hepatic arter-ies in 21 cases, hepatic veins in 35 cases,and portal vein branches in 13 cases;among which combinations also occurredin 20 cases. The presence of IHG wasstrongly related to open trauma with sys-
temic gas. Pulmonary barotrauma as oc-curring under artificial respiration or indrowning also caused IHG. Putrefactiondid not seem to influence the occurrenceof IHG until macroscopic signs of putre-faction were noticeable.
Conclusions: IHG is a frequentfinding in traumatic causes of death andrequires a systemic gas embolism. Ex-ceptions are putrefied or burned corpses.Common clinical causes such as necroticbowel diseases appear rarely as a cause ofIHG in our forensic case material.
Key Words: Forensic radiology, Vir-topsy, Postmortem imaging, Intrahepaticgas, Gas embolism.
J Trauma. 2007;62:979–988.
Postmortem imaging using multislice computed tomog-raphy (MSCT) and magnetic resonance (MR) imagingis being evaluated by several research groups1–7 as a
postmortem investigation technique alternative to traditionaldestructive autopsy in selected cases. Thereby, intrahepaticgas (IHG) was recognized as a frequent finding in postmor-tem MSCT examinations. It was first described by Yamazakiet al.8 as hepatic portal venous gas. Shiotani et al.9 publishedthe first retrospective study in 190 nontraumatic deaths cor-relating the occurrence of intrahepatic portal venous gas withgastrointestinal distention. Traumatic causes of IHG weremissing in this study as well as postmortem alterationssuch as putrefaction; all cases were scanned within 2 hourspostmortem.
Having data of more than 100 forensic cases with fullbody MSCT and MR scanning we intended to investigate the
occurrence of IHG according to conditions, that are thoughtto influence the occurrence of IHG such as venous or sys-temic air embolism,10 artificial respiration, gastrointestinaldistention, and putrefaction.11
MATERIALS AND METHODSFrom 106 virtopsy cases, 18 cases presenting with direct
traumatic injury of the liver (e.g. total destruction of thecorpse when run over by train or gun shot wound channelsthrough the liver), 1 case of adipocire, 1 case that was foundin a glacier that was scanned before defrosting as well as 1newborn, and 1 fetus were excluded. The remaining 84 caseswere investigated using the scanning procedures correspond-ing to the virtopsy approach as already described in previouspublications from 2000 to 2004.1,12,13
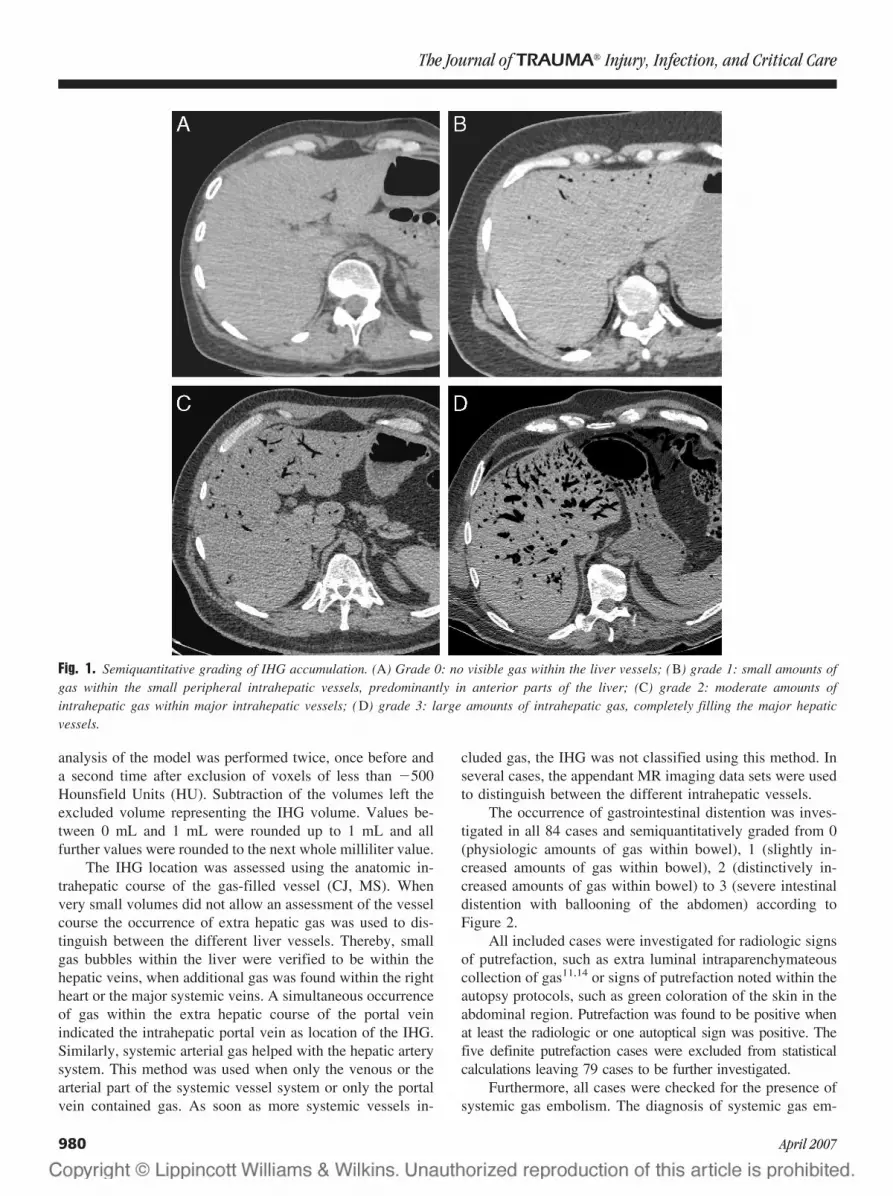
The severity of IHG was semiquantitatively assessed bya subjective observer-dependent grading score from 0 (no gaswithin the liver), 1 (small amounts of gas within the smallperipheral intrahepatic vessels predominantly in anterior partsof the liver), 2 (moderate amounts of IHG within majorintrahepatic vessels) to 3 (large amounts of IHG, completelyfilling the major hepatic vessels), demonstrated in Figure 1.
This grading was supported by an objective quantificationof the IHG volume. A three-dimensional volume-renderingmodel of the liver was generated after manual tracing of theliver contours on axial images on a workstation. Volume
Submitted for publication September 12, 2005.Accepted for publication November 18, 2005.Copyright © 2007 by Lippincott Williams & Wilkins, Inc.From the Institute of Forensic Medicine (C.J., M.J.T., E.A., K.Y., R.D.)
and the Institute of Diagnostic Radiology, Inselspital, (M.S., P.V.), Univer-sity of Bern, Switzerland.
Address for reprints: Christian Jackowski, MD, University of Bern,Institute of Forensic Medicine, IRM – Buehlstrasse 20, CH-3012 Bern,Switzerland; email: [email protected].
DOI: 10.1097/01.ta.0000198733.22654.de
The Journal of TRAUMA� Injury, Infection, and Critical Care
Volume 62 • Number 4 979
analysis of the model was performed twice, once before anda second time after exclusion of voxels of less than �500Hounsfield Units (HU). Subtraction of the volumes left theexcluded volume representing the IHG volume. Values be-tween 0 mL and 1 mL were rounded up to 1 mL and allfurther values were rounded to the next whole milliliter value.
The IHG location was assessed using the anatomic in-trahepatic course of the gas-filled vessel (CJ, MS). Whenvery small volumes did not allow an assessment of the vesselcourse the occurrence of extra hepatic gas was used to dis-tinguish between the different liver vessels. Thereby, smallgas bubbles within the liver were verified to be within thehepatic veins, when additional gas was found within the rightheart or the major systemic veins. A simultaneous occurrenceof gas within the extra hepatic course of the portal veinindicated the intrahepatic portal vein as location of the IHG.Similarly, systemic arterial gas helped with the hepatic arterysystem. This method was used when only the venous or thearterial part of the systemic vessel system or only the portalvein contained gas. As soon as more systemic vessels in-
cluded gas, the IHG was not classified using this method. Inseveral cases, the appendant MR imaging data sets were usedto distinguish between the different intrahepatic vessels.
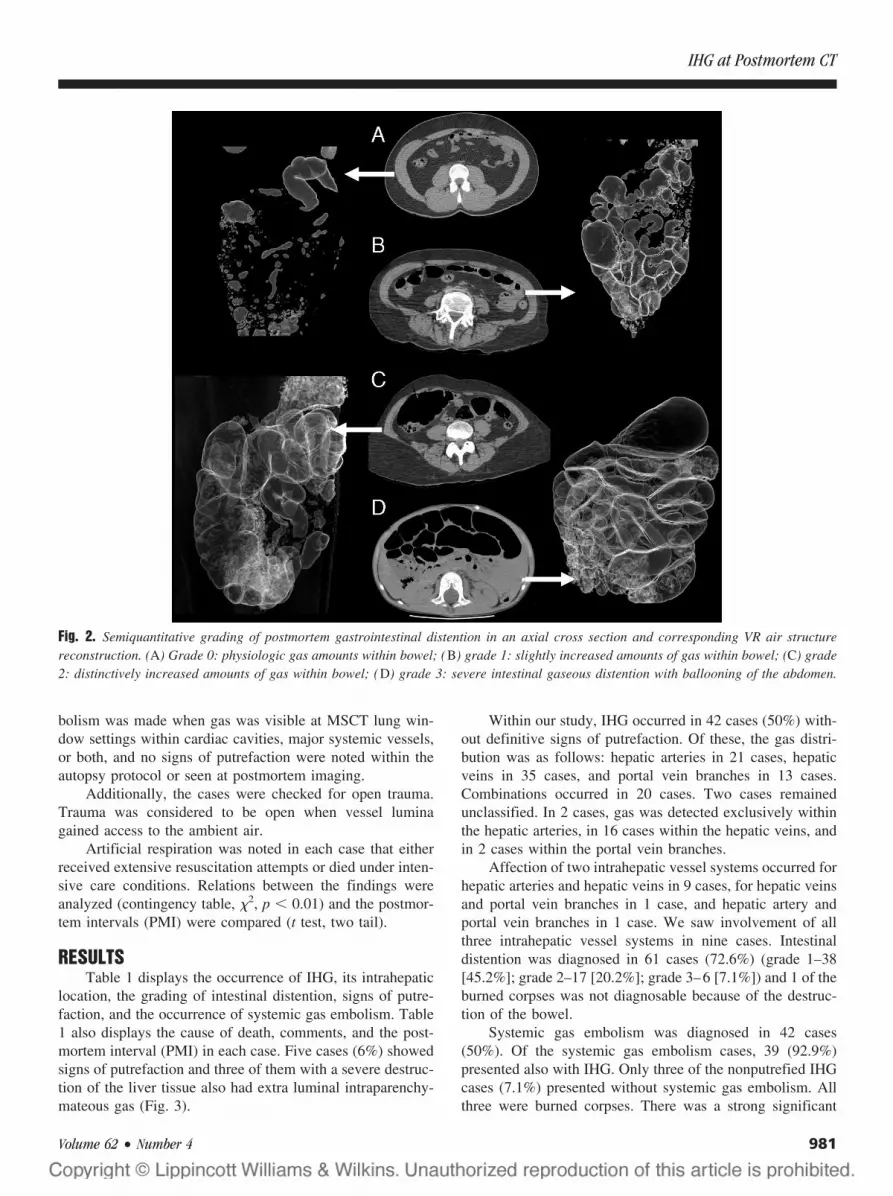
The occurrence of gastrointestinal distention was inves-tigated in all 84 cases and semiquantitatively graded from 0(physiologic amounts of gas within bowel), 1 (slightly in-creased amounts of gas within bowel), 2 (distinctively in-creased amounts of gas within bowel) to 3 (severe intestinaldistention with ballooning of the abdomen) according toFigure 2.
All included cases were investigated for radiologic signsof putrefaction, such as extra luminal intraparenchymateouscollection of gas11,14 or signs of putrefaction noted within theautopsy protocols, such as green coloration of the skin in theabdominal region. Putrefaction was found to be positive whenat least the radiologic or one autoptical sign was positive. Thefive definite putrefaction cases were excluded from statisticalcalculations leaving 79 cases to be further investigated.
Furthermore, all cases were checked for the presence ofsystemic gas embolism. The diagnosis of systemic gas em-
Fig. 1. Semiquantitative grading of IHG accumulation. (A) Grade 0: no visible gas within the liver vessels; (B) grade 1: small amounts ofgas within the small peripheral intrahepatic vessels, predominantly in anterior parts of the liver; (C) grade 2: moderate amounts ofintrahepatic gas within major intrahepatic vessels; (D) grade 3: large amounts of intrahepatic gas, completely filling the major hepaticvessels.
The Journal of TRAUMA� Injury, Infection, and Critical Care
980 April 2007
bolism was made when gas was visible at MSCT lung win-dow settings within cardiac cavities, major systemic vessels,or both, and no signs of putrefaction were noted within theautopsy protocol or seen at postmortem imaging.
Additionally, the cases were checked for open trauma.Trauma was considered to be open when vessel luminagained access to the ambient air.
Artificial respiration was noted in each case that eitherreceived extensive resuscitation attempts or died under inten-sive care conditions. Relations between the findings wereanalyzed (contingency table, �2, p � 0.01) and the postmor-tem intervals (PMI) were compared (t test, two tail).
RESULTSTable 1 displays the occurrence of IHG, its intrahepatic
location, the grading of intestinal distention, signs of putre-faction, and the occurrence of systemic gas embolism. Table1 also displays the cause of death, comments, and the post-mortem interval (PMI) in each case. Five cases (6%) showedsigns of putrefaction and three of them with a severe destruc-tion of the liver tissue also had extra luminal intraparenchy-mateous gas (Fig. 3).
Within our study, IHG occurred in 42 cases (50%) with-out definitive signs of putrefaction. Of these, the gas distri-bution was as follows: hepatic arteries in 21 cases, hepaticveins in 35 cases, and portal vein branches in 13 cases.Combinations occurred in 20 cases. Two cases remainedunclassified. In 2 cases, gas was detected exclusively withinthe hepatic arteries, in 16 cases within the hepatic veins, andin 2 cases within the portal vein branches.
Affection of two intrahepatic vessel systems occurred forhepatic arteries and hepatic veins in 9 cases, for hepatic veinsand portal vein branches in 1 case, and hepatic artery andportal vein branches in 1 case. We saw involvement of allthree intrahepatic vessel systems in nine cases. Intestinaldistention was diagnosed in 61 cases (72.6%) (grade 1–38[45.2%]; grade 2–17 [20.2%]; grade 3–6 [7.1%]) and 1 of theburned corpses was not diagnosable because of the destruc-tion of the bowel.
Systemic gas embolism was diagnosed in 42 cases(50%). Of the systemic gas embolism cases, 39 (92.9%)presented also with IHG. Only three of the nonputrefied IHGcases (7.1%) presented without systemic gas embolism. Allthree were burned corpses. There was a strong significant
Fig. 2. Semiquantitative grading of postmortem gastrointestinal distention in an axial cross section and corresponding VR air structurereconstruction. (A) Grade 0: physiologic gas amounts within bowel; (B) grade 1: slightly increased amounts of gas within bowel; (C) grade2: distinctively increased amounts of gas within bowel; (D) grade 3: severe intestinal gaseous distention with ballooning of the abdomen.
IHG at Postmortem CT
Volume 62 • Number 4 981

Table 1 Results in All 84 Investigated Forensic Cases
CaseGrade
0Grade
1Grade
2Grade
3Gas
VolumeLocation
IntestinalDistension‡
PutrefactionNoted
SystemicGas
EmbolismCause of Death Comments PMI
1 x � x Gunshot to the head* 24 hr2 x � 0 Exsanguination* 24 hr3 x � 0 Exsanguination/fat
embolism*24 hr
4 x 7 mL a. � v. �� x Air embolism* Burned corpse 24 hr5 x 2 mL v. � x Exsanguination/air
embolism*24 hr
6 x � 0 Heart failure† Artificial respiration 72 hr7 x � x Craniocerebral trauma* Artificial respiration 48 hr8 x 1 mL a. � v. �� x Craniocerebral trauma* 24 hr9 x 1 mL v. ��� x Exsanguination* Artificial respiration 24 hr
10 x ��� 0 Strangulation† 24 hr11 x 8 mL v. x Gunshot to the head* 24 hr12 x 3 mL v. � x Gunshot to the head* 12 hr15 x 1 mL v. � x Craniocerebral trauma* 24 hr16 x �� 0 Gunshot to the head* 24 hr18 x � 0 Craniocerebral trauma* Artificial respiration 5 hr19 x � 0 Cerebral edema† Artificial respiration 24 hr21 x 1 mL v. � x Gunshot to the head* 96 hr22 x 9 mL a. � v. � p. �� x Gunshot to the head* 48 hr23 x 4 mL a. � v. � x Craniocerebral trauma/air
embolism*24 hr
24 x �� 0 SIDS† Artificial respiration 36 hr25 x � 0 Heart failure† Artificial respiration 24 hr27 x 81 mL tis. des. ��� x 0 Craniocerebral trauma* 2–4 wk28 x 19 mL a. � v. � p. ��� x Craniocerebral trauma* Artificial respiration 24 hr30 x � 0 Exsanguination* Artificial respiration 12 hr31 x � x Air embolism* 24 hr32 x � 0 Strangulation† 24 hr33 x 3 mL a. � v. �� x Exsanguination* 24 hr34 x � 0 Drowning† 12 hr35 x � 0 Fat embolism* Artificial respiration 36 hr36 x 71 mL a. � v. � p. �� x Exsanguination* 60 hr37 x � 0 Fat embolism* Artificial respiration 24 hr40 x � 0 Craniocerebral trauma* Artificial respiration 48 hr43 x � 0 Septicemia/heart failure† Artificial respiration 48 hr46 x � 0 Cerebral edema* Artificial respiration 48 hr47 x 1 mL ? � x Exsanguination* 12 hr50 x � 0 Manual strangulation† 36 hr51 x � 0 Manual strangulation† 36 hr53 x �� 0 Hypothermia† Artificial respiration 48 hr54 x 3 mL a. � v. � p. � x Exsanguination* Artificial respiration 12 hr55 x 1 mL a. � x Multiple organ failure* Artificial respiration 72 hr56 x 1 mL v. � 0 Carbon monoxide
poisoning†Burned corpse 24 hr
58 x 1 mL v. � p. no bowel 0 Burn shock† Burned corpse 24 hr61 x 13 mL a. � v. � p. ��� x Exsanguination/fat
embolism*48 hr
62 x 123 mL tis. des. ��� x 0 Pneumonia† 3–4 wk63 x 18 mL a. � v. � p. ��� x Exsanguination* 12 hr65 x 1 mL a. � v. � x Fat embolism/positional
asphyxia*24 hr
66 x 6 mL a. � v. � p. � x Exsanguination* 24 hr67 x 16 mL a. � v. � x Craniocerebral trauma* 24 hr68 x � 0 Cerebral edema* Artificial respiration 6 hr69 x 21 mL p. � x Cerebral edema* Artificial respiration 24 hr70 x 189 mL tis. des. ��� x 0 Drowning 144 hr72 x 2 mL v. � x Air embolism* 24 hr73 x 2 mL v. � x Gunshot to the head* 12 hr74 x 3 mL v. � x Craniocerebral trauma* 12 hr75 x 2 mL p. �� x 0 Strangulation 48 hr76 x 3 mL a. � v. � x Drowning Artificial respiration 48 hr77 x 6 mL a. � v. � x Drowning Artificial respiration 24 hr78 x 32 mL v. � x 0 Exsanguination/drowning* 120 hr79 x 2 mL a. � v. � p. � 0 Blood aspiration* Burned corpse 48 hr80 x � 0 Craniocerebral trauma* Burned corpse 48 hr81 x 4 mL a. � v. � p. � x pneumothorax* 12 hr83 x � 0 Strangulation† Artificial respiration 12 hr84 x �� 0 Craniocerebral trauma* Artificial respiration 24 hr85 x 1 mL a. � v. � x Heart failure† Artificial respiration 12 hr
The Journal of TRAUMA� Injury, Infection, and Critical Care
982 April 2007

relation of the finding of IHG and systemic gas as well as astrong significant relation between systemic gas and trau-matic cause of death.
The intrahepatic measured gas volumes varied from 1mL to 189 mL. The three highest volumes measured were 81mL, 123 mL, and 189 mL and occurred in putrefaction cases.The range in all 79 nonputrefaction cases was 1 to 71 mL.
Intestinal gas amounts in nonputrefied cases did notdiffer from normal physiologic vital dimensions (grade 0) in17 cases (21.5%). Intestinal distention of grade 1 occurred in38 cases (48.1%), of grade 2 in 17 cases (21.5%), and ofgrade 3 in 6 cases (7.7%). One case showed a destruction ofthe intestine because of burning.
There was no significant relation between the occurrenceof gastrointestinal distention (all gradings) and IHG in ourdata although in grade 3 gastrointestinal distention five of sixcases showed IHG. All of the IHG cases involving the intra-hepatic branches of the portal vein showed at least grade 1distention. Artificial respiration was noticed in 31 (39.2%) ofthe nonputrefied cases and showed no significant relation tothe occurrence of IHG.
After exclusion of the five putrefaction cases the meanpostmortem interval (PMI) in 42 cases showing IHG was29.1 hours (standard deviation 14.3 hours) and in 37 cases
without IHG 29.3 hours (s 15.8 hours). There was no signif-icant difference in PMIs of both groups.
Of the 79 nonputrefied cases, 48 (60.8%) presented withan open trauma as cause of death (Table 1). Of these, 32(66.7%) also showed IHG. There was a significant relationbetween open trauma and the occurrence of IHG in ourpopulation.
DISCUSSIONThis study investigated the occurrence and cause of IHG
detected in postmortem MSCT investigations. Yamazaki etal.8 and Shiotani et al.9 first described hepatic portal venousgas as a frequent finding in postmortem computed tomogra-phy and correlated it to the occurrence of intestinal distention.Their 190 cases were of nontraumatic nature and scannedwithin 2 hours postmortem. Thereby, the traumatic causes ofIHG as well as postmortem alterations such as putrefactionleading to IHG were missing.
We noticed within our first 100 virtopsy cases morelocations of IHG, such as the hepatic venous system, thehepatic arterial system, and within the tissue. Biliary tractgas, a frequent clinical finding,15 did not occur in our 79investigated cases.
Table 1 Results in All 84 Investigated Forensic Cases (continued)
CaseGrade
0Grade
1Grade
2Grade
3Gas
VolumeLocation
IntestinalDistension‡
PutrefactionNoted
SystemicGas
EmbolismCause of Death Comments PMI
86 x 3 mL p. �� x Intoxication† Artificial respiration 24 hr87 x 37 mL a. � p. � x Strangulation† 48 hr88 x 3 mL v. � x Pneumothorax* Artificial respiration 60 hr89 x �� 0 Exsanguination/fat
embolism*48 hr
90 x 1 mL v. � x Heart failure† Artificial respiration 48 hr91 x �� 0 Manual strangulation† 24 hr92 x �� 0 Intoxication† 24 hr93 x � 0 Heart failure† 24 hr94 x � 0 Strangulation† 24 hr96 x �� 0 Pneumonia/necrotizing
laryngitis†Artificial respiration 24 hr
97 x � 0 Strangulation† 6 hr98 x � 0 Immaturity (fetus 22
weeks)†24 hr
99 x �� 0 Heart failure† 24 hr100 x � 0 Hypothermia† 24 hr101 x 2 mL v. � x Heart failure† Artificial respiration 24 hr102 x 1 mL ? �� x Craniocerebral trauma* 24 hr103 x 1 mL v. � x Cerebral edema* Artificial respiration 48 hr104 x 1 mL v. ��� x Exsanguination/fat
embolism*24 hr
105 x 1 mL v. � x Exsanguination/fatembolism*
48 hr
106 x 3 mL a. �� x Heart failure† Artificial respiration 24 hr
Semiquantitative subjective grading of the quantity of the intrahepatic gas from 0 to 3 (according to Fig. 1) and the result of the volumetriccomputed tomography assessment are seen. The intrahepatic location is noted. When it could not be assessed a question mark was set. Theoccurrence of intestinal distention is noted (according to Fig. 2). Putrefaction signs as well as the occurrence of systemic gas embolism aredisplayed. Comments show whether the case underwent artificial respiration or was burned. PMI indicates the time between death and scanning.
* Traumatic cause of death.† Nontraumatic cause of death.‡ �, grade 0; �, grade 1; ��, grade 2; ���, grade 3.a, hepatic artery; v, hepatic veins; p, portal vein branches; PMI, postmortem interval; tis. des.; tissue destruction.
IHG at Postmortem CT
Volume 62 • Number 4 983

Wolfel and Brogdon16 comprehensibly considered thegas within the liver seen on plain radiographs to be driveninto the biliary tree from the upper gastrointestinal tract at thetime of a blunt abdominal injury. Our findings do not supportthis possible explanation for IHG in cases of abdominaltrauma. We did not detect relevant volumes of gas within thebiliary tract although biliary gas could not be completelyexcluded because two cases of IHG could not be classified.
Intrahepatic Venous GasThe most frequent location of IHG in this study was the
hepatic venous system. Having abundant traumatic caseswithin our population and noticing the strong relation ofsystemic gas embolism and intrahepatic venous gas, we as-sume trauma with gas embolism to be the commonest cause.Mainly craniocerebral trauma and head shot wounds wereassociated with IHG. Both conditions range among the maincauses for venous air embolism according to the literature andour own experiences.10,17–20 We also hypothesize this to bethe mechanism for intrahepatic venous gas accumulation.Other traumatic injuries might also cause gas to enter thehepatic venous system such as blunt or open abdominaltrauma.21
Thereby, it remains arguable whether a retrograde gastransport into the liver veins occurs passively postmortemwhen the corpse is stored in supine position because of theascending force. Alternatively, it might occur vitally in ret-rograde direction via an increased right ventricular pressureand an insufficiency of the tricuspid valve after gaseousocclusion of the pulmonary artery even against the buoyancyof gas bubbles in fluids (Fig. 4). The second explanationmight be supported by the finding of gas within the vessels ofdorsal liver parts, which are below the level of the vena cavain supine position.
Intrahepatic Arterial GasIn 21 cases, gas was shown within the arterial system.
Gas can enter the arterial system via a patent foramen ovalecombined with an increasing right atrial pressure in gaseouspulmonary artery embolism. It may even pass the pulmonarycapillary bed22–25 or in direct pulmonary trauma (contusion,laceration) with damage to the alveolar-capillary barrier itmay reach the pulmonary veins.26 We also assume alveolar
Fig. 3. Putrefaction gas. Axial MSCT image of the liver in putre-faction case 70 and corresponding air structure reconstruction in ananteroposterior view. Note the diffuse and more bubble-like distri-bution of the putrefaction gas within the decomposed dorsal livertissue in addition to the predominantly anterior intravascular gas.
Fig. 4. Intrahepatic venous gas in upright corpse position. Gas within hepatic veins (arrows) and hepatic arteries (doubled arrow) in a caseof a gunshot wound to the head and remaining in upright position. Either an active and vital retrograde gas transportation downwards intothe hepatic veins resulting from an increased right ventricular pressure after total gaseous occlusion of the right ventricular outflow tractand pulmonary artery, or a passive gas transport caused by buoyancy from right atrium into the liver veins, when the corpse was stored andscanned in supine position, might have been responsible.
The Journal of TRAUMA� Injury, Infection, and Critical Care
984 April 2007

rupture because of emphysema aquosum in cases of drowning orbecause of pulmonary barotrauma caused by high-inspiratorypressures during artificial respiration to cause systemic arte-rial gas emboli.27–30 This might explain the 10 cases whichshowed gas within the liver vessels, but died because of anontraumatic manner of death. Four of them died of heartfailure (cases 85, 90, 101, and 106) under artificial respira-tion. Because the PMI in these four cases (12–48 hours) didnot increase as compared with the entire population studied,we assume an agonal barotrauma because of artificial respi-ration as the most likely cause for the intravascular gas.Additionally, the two drowning cases (cases 76 and 77) hadalveolar ruptures because of a typical drowning process31 thatfacilitated the entrance of gas into the vascular system. Instrangulation (case 87) the pulmonary trauma caused by thestrong breathing attempts against narrowed or occluded air-ways also facilitated ruptures of the alveolar wall and gascould enter the mediastinum32 or the pulmonary vascularsystem.
The 31 artificial respiration cases included only 14 caseswith IHG and thereby had a lower percentage of IHG(45.2%), as compared with the entire population studied(53.2%). In some cases of natural death (cases 85, 90, 101,and 106), resuscitation seems to be the only obvious mech-anism allowing gas to enter the vascular system. Other caseswith IHG and a traumatic manner of death might have beeninfluenced in their occurrence of intravascular gas by artifi-cial respiration.
Intrahepatic Portal Venous GasPortal venous gas occurred in 13 cases and exclusively in
2 of them. In clinical radiology portal venous gas is indicativeof necrotic bowel disease, e.g. after mesenteric arteryocclusion33–40 or in Crohn disease.41,42 Blunt traumatic in-jury is rarely considered to cause portal venous gas but anincreasing number of case reports describe the finding ofportal venous gas without necrotic bowel diseases.21,43–46
Portal venous gas was also described in child abuse.47
The two cases with exclusively portal venous gas (cases69 and 86) need a more detailed discussion. Case 69 wasbased on a person who was hit by a motorcycle and sufferedfatal abdominal blunt trauma indicating traumatic damage ofthe mucosa allowing intestinal gas to enter the portal venoussystem. Case 86 was based on a person who succumbed tolethal oral intoxication with severe necrosis of the intestinalmucosa and grade 2 distention. In these two cases, we assumea damage to the barrier between the intestinal lumen and thecapillary bed of the mesentery to be responsible for the portalvenous gas, comparable to the clinical experience in necroticbowel disease.
All additional cases with portal venous gas either alreadyshowed putrefaction signs or also presented with gas in fur-ther hepatic vessels. Because most of them also had sufferedtrauma, we assume the mechanism of the gas entry to theportal vein was through the capillary bed of the intestine after
arterial gas embolism. This may be supported by the 10 casesthat showed a combination of hepatic artery gas embolismand portal venous gas as the mesenterial arteries are branch-ing in anatomic correlation to the celiac trunk.
Massive amounts of portal venous gas were also presentin strangulation (case 87). Knowing the severe barotraumacaused arterial gas embolism including the mesenterial arter-ies in this case we postulate a passage of the arterial gas viathe mesenteric capillary bed into the portal vein as cause forthe massive portal venous gas (Fig. 5). Systemic arterial gasthat does not enter the supra-aortic arteries will predomi-nantly accumulate within the celiac trunk and the mesentericarteries as these are the nondependent branches of the ab-dominal aorta when death occurs in supine position, such asunder intensive care or resuscitation.
Burned CorpsesIn burned corpses (cases 56, 58, and 79), the gas distri-
bution did not follow the above-mentioned rules. The devel-opment of intravascular gas was assumed to be caused byheat in all vessels. Remarkable is the fact that burned corpseswere the only exception that showed IHG without systemicgas embolism. The heat affected predominantly the surface ofthe trunk and the IHG was found in the periphery of the liver.
PutrefactionPutrefaction was only found to be a cause of relevant
volumes of IHG in cases that showed radiologic signs ofputrefaction or when signs of putrefaction were noticed dur-ing autopsy. This was based on the results of Pedal et al.48
who investigated intracardiac gas in 111 autopsy cases chro-matographically. They found putrefaction gas in 64 cases, ofwhich only 6 had no note of putrefaction within the autopsyprotocol. The lack of chromatographic confirmation of pu-trefaction gas is a limitation of our retrospective study.
The earliest time that putrefaction gas starts developingis considered to be 148 to 2 days49,50 postmortem. Thus, insome cases with a PMI of more than 1 day, the measured gasvolumes might have been influenced by beginning putrefac-tion. However, we assume that this is not a relevant influenceon the volume of gas until secure signs of putrefaction arenoticed either at autopsy or in postmortem imaging. This canbe supported by the mean PMI in the group of cases with IHG(after exclusion of the five secure putrefaction cases) and thegroup without IHG. The mean PMI did not significantlydiffer between both groups; therefore, a relevant influence ofputrefaction is also statistically improbable. In our study, thecases of IHG even showed a slightly shorter mean PMI.
This does not exclude the possibility that particular caseswith an increased PMI and probably warm postmortem con-ditions might have already developed putrefaction gas beforeany macroscopic or radiologic signs. However, our results donot support the assumption of Oliver et al.,51 who presentedfour cases of diving fatalities and ascribed small amounts ofgas within the intrahepatic circulation as a postmortem alter-
IHG at Postmortem CT
Volume 62 • Number 4 985

ation because of putrefaction. They supported their explana-tion by the presentation of a control scan of a head shotwound case with a PMI of 27 hours, which also showed gaswithin the liver vessels. As shown in our results, IHG is avery frequent finding in craniocerebral trauma and it ismostly because of venous air embolism. In our opinion,Oliver’s case was not a proof of early postmortem putrefac-tion gas formation in postmortem imaging. However, decom-pression in scuba diving accidents has also to be consideredas a potential cause of IHG in postmortem computed tomog-raphy examination, although the circumstances should nor-mally give enough clues to the cause. Impressive amounts ofgas within the liver vessels in scuba diving accidents wereshown in postmortem computed tomography by severalauthors.51,52
Besides putrefaction gas and decompression, an earlypostmortem nonbacterial CO2 formation50,53 has to be dis-cussed as a possible source of gas bubbles in postmortemMSCT examinations. Within the supravital period, the pro-
duction of CO2 via the aerobic metabolism can last up to 10to 15 hours postmortem. Additionally, the increase in lactatelevels54 because of the supravital glycolysis will cause anincreased release of CO2 from the bicarbonate of the blood.50
The protein decomposition furthermore leads to increasingCO2 within the blood.55 In particular cases, the gas volumemight be slightly influenced by these reactions but the 37cases without IHG argue against a relevant systematic post-mortem CO2 formation.
Intestinal DistentionInvestigation of intestinal distention did not reveal any
obvious relation to the occurrence of IHG except for grade 3distention. Intestinal distention of grades 0 to 2 seemed not tohave an effect on the finding of IHG because the occurrenceof IHG was not increased compared with the cases withoutdistention. In 5 of 6 cases (83.3%) with grade 3 intestinaldistention IHG occurred. The small number of cases does notallow for any conclusion.
Fig. 5. Intrahepatic gas without putrefaction. Axial MSCT images (small figures in the middle) and corresponding air structure reconstruc-tions of the abdomen in an anteroposterior view. (A) Case 78: only the hepatic vein system (arrow) is involved in the gas embolism; (B) case69: the intrahepatic gas is located exclusively in the portal vein system (dashed arrow); (C) case 87: intrahepatic gas is located predominantlyin the intrahepatic portal vein system (dashed arrow) in combination with small amounts within hepatic artery branches (note the doubledcourse, doubled arrows); (D) case 36: the intrahepatic gas because of venous and arterial air embolism within hepatic vein/inferior vena cava(arrow), hepatic artery/celiac trunk (doubled arrows), and intrahepatic portal branches (dashed arrow).
The Journal of TRAUMA� Injury, Infection, and Critical Care
986 April 2007

As seen in Table 1, similar gas volumes were not alwayssubjectively graded within the same group. Especially smallvolumes (1–4 mL) were variably graded between grade 1 and2. We assume this to be caused by a different gas distributionwithin the liver. The volume distributed within many smallvessels may lead to an underestimation and the same volumeseen within fewer but major vessels may act conversely. Weappraise the objectively measured gas volumes as more valuablewhen compared with the subjective observer dependant grading.
When putrefaction and other processes contributing topostmortem gas development, such as burning or local mi-crobiologic infections (clostridia), can be excluded, distinctvolumes of IHG represent a so-called vital sign.1 Althoughthe transport into the liver vessels may also occur passivelypostmortem, its entrance into the systemic circulation and itsdistribution within the body needs an ongoing circulation.Especially hepatic arterial gas embolism depends on an an-tegrade blood flow.
Besides all forensic causes of IHG, nonforensic clinicalentities have to be taken into consideration, such as gasgangrene within the intestine and abdomen,56 enteritis andcolitis,35,57 cholangitis,35 seizure,58 or idiopathic gas.59,60
CONCLUSIONIHG is a frequent finding in postmortem imaging in
forensic medicine. The most common cause is of a traumaticnature because of craniocerebral trauma or blunt forces. It isstrongly related to the occurrence of systemic gas embolism.
ACKNOWLEDGMENTSWe would like to thank the team of MTRA’s (Karin Zwygart, Verena
Beutler, Elke Spielvogel, Christoph Laeser, and Carolina Dobrowolska) fortheir excellent help in acquiring the scans within the virtopsy project as wellas Urs Konigsdorfer and Roland Dorn for their experienced assistance atautopsy and Therese Perinat for the histologic preparations as well asNaseem J. Malik for the support in article preparation.
REFERENCES1. Thali MJ, Yen K, Schweitzer W, et al. Virtopsy, a new imaging
horizon in forensic pathology: virtual autopsy by postmortemmultislice computed tomography (MSCT) and magnetic resonanceimaging (MRI)—a feasibility study. J Forensic Sci. 2003;48:386–403.
2. Ezawa H, Yoneyama R, Kandatsu S, et al. Introduction of autopsyimaging redefines the concept of autopsy: 37 cases of clinicalexperience. Pathol Int. 2003;53:865–873.
3. Shiotani S, Kohno M, Ohashi N, et al. Non-traumatic postmortemcomputed tomographic (PMCT) findings of the lung. Forensic SciInt. 2004;139:39–48.
4. Rutty GN, Swift B. Accuracy of magnetic resonance imaging indetermining cause of sudden death in adults: comparison withconventional autopsy. Histopathology. 2004;44:187–189.
5. Roberts IS, Benbow EW, Bisset R, et al. Accuracy of magneticresonance imaging in determining cause of sudden death in adults:comparison with conventional autopsy. Histopathology. 2003;42:424–430.
6. Patriquin L, Kassarjian A, Barish M, et al. Postmortem whole-bodymagnetic resonance imaging as an adjunct to autopsy: preliminaryclinical experience. J Magn Reson Imaging. 2001;13:277–287.
7. Bisset RA, Thomas NB, Turnbull IW, Lee S. Postmortemexaminations using magnetic resonance imaging: four year review ofa working service. BMJ. 2002;324:1423–1424.
8. Yamazaki K, Shiotani S, Ohashi N, Doi M, Honda K. Hepatic portalvenous gas and hyper-dense aortic wall as postmortem computedtomography finding. Leg Med (Tokyo). 2003;5(suppl 1):S338–S341.
9. Shiotani S, Kohno M, Ohashi N, et al. Postmortem computedtomographic (PMCT) demonstration of the relation betweengastrointestinal (GI) distension and hepatic portal venous gas(HPVG). Radiat Med. 2004;22:25–29.
10. Jackowski C, Thali M, Sonnenschein M, et al. Visualization andquantification of air embolism structure by processing postmortemMSCT data. J Forensic Sci. 2004;49:1339–1342.
11. Thali MJ, Yen K, Schweitzer W, et al. Into the decomposed body-forensic digital autopsy using multislice-computed tomography.Forensic Sci Int. 2003;134:109–114.
12. Aghayev E, Yen K, Sonnenschein M, et al. Virtopsy post-mortemmulti-slice computed tomography (MSCT) and magnetic resonanceimaging (MRI) demonstrating descending tonsillar herniation:comparison to clinical studies. Neuroradiology. 2004;46:559–564.
13. Jackowski C, Schweitzer W, Thali M, et al. Virtopsy: postmortemimaging of the human heart in situ using MSCT and MRI. ForensicSci Int. 2005;149:11–23.
14. Jachau K, Heinrichs T, Kuchheuser W, et al. Computed tomographyand magnetic resonance imaging compared to pathoanatomicfindings in isolated human autopsy hearts. Rechtsmedizin. 2004;14:109–116.
15. Hoddick W, Jeffrey RB, Federle MP. CT differentiation of portalvenous air from biliary tract air. J Comput Assist Tomogr. 1982;6:633–634.
16. Wolfel DA, Brogdon BG. Intrahepatic air: a sign of trauma.Radiology. 1968;91:952–953.
17. Adams V, Guidi C. Venous air embolism in homicidal blunt impacthead trauma. Case reports. Am J Forensic Med Pathol. 2001;22:322–326.
18. Adams VI, Hirsch CS. Venous air embolism from head and neckwounds. Arch Pathol Lab Med. 1989;113:498–502.
19. Kerner T, Fritz G, Unterberg A, Falke KJ. Pulmonary air embolismin severe head injury. Resuscitation. 2003;56:111–115.
20. Messmer JM. Massive head trauma as a cause of intravascular air.J Forensic Sci. 1984;29:418–424.
21. Brown MA, Hauschildt JP, Casola G, Gosink BB, Hoyt DB.Intravascular gas as an incidental finding at US after bluntabdominal trauma. Radiology. 1999;210:405–408.
22. Black M, Calvin J, Chan KL, Walley VM. Paradoxic air embolismin the absence of an intracardiac defect. Chest. 1991;99:754–755.
23. Ho AM, Ling E. Systemic air embolism after lung trauma.Anesthesiology. 1999;90:564–575.
24. Muth CM, Shank ES. Gas embolism. N Engl J Med. 2000;342:476–482.
25. Butler BD, Hills BA. Transpulmonary passage of venous air emboli.J Appl Physiol. 1985;59:543–547.
26. Saada M, Goarin JP, Riou B, et al. Systemic gas embolismcomplicating pulmonary contusion. Diagnosis and management usingtransesophageal echocardiography. Am J Respir Crit Care Med.1995;152:812–815.
27. Morris WP, Butler BD, Tonnesen AS, Allen SJ. Continuous venousair embolism in patients receiving positive end-expiratory pressure.Am Rev Respir Dis. 1993;147:1034–1037.
28. Bricker MB, Morris WP, Allen SJ, Tonnesen AS, Butler BD.Venous air embolism in patients with pulmonary barotrauma. CritCare Med. 1994;22:1692–1698.
29. Marini JJ, Culver BH. Systemic gas embolism complicatingmechanical ventilation in the adult respiratory distress syndrome.Ann Intern Med. 1989;110:699–703.
IHG at Postmortem CT
Volume 62 • Number 4 987

30. Cavadore P, Brunat G, Perrigault PF, Colson P. [Cerebral arterial airembolism associated with pneumothorax in a patient with pressuresupport ventilation.] Ann Fr Anesth Reanim. 2000;19:249–252.
31. Brinkmann B, Fechner G, Puschel K. [Lung histology inexperimental drowning.] Z Rechtsmed. 1983;89:267–277.
32. Aghayev E, Yen K, Sonnenschein M, et al. Pneumomediastinum andsoft tissue emphysema of the neck in postmortem CT and MRI: anew vital sign in hanging? Forensic Sci Int. 2005;153:181–188.
33. Torzilli G, Cattaneo S, Lumachi V, et al. Ultrasonographic detectionof portal branches and hepatic vein gas associated with mesentericartery occlusion: a new finding correlated with patient prognosis?Chir Ital. 2000;52:295–298.
34. Kriegshauser JS, Reading CC, King BF, Welch TJ. Combinedsystemic and portal venous gas: sonographic and CT detection intwo cases. AJR Am J Roentgenol. 1990;154:1219–1221.
35. Hou SK, Chern CH, How CK, et al. Hepatic portal venous gas:clinical significance of computed tomography findings. Am J EmergMed. 2004;22:214–218.
36. Chou CK, Mak CW, Tzeng WS, Chang JM. CT of small bowelischemia. Abdom Imaging. 2004;29:18–22.
37. Merritt CR, Goldsmith JP, Sharp MJ. Sonographic detection ofportal venous gas in infants with necrotizing enterocolitis. AJR Am JRoentgenol. 1984;143:1059–1062.
38. Thomachot L, Arnal JM, Vialet R, Albanese J, Martin C. [Lethalportal venous gas after cardiopulmonary arrest.] Ann Fr AnesthReanim. 1998;17:369–371.
39. Peh WC, Muttarak M. Clinics in diagnostic imaging (53). Hepaticportal venous gas due to mesenteric infarction. Singapore Med J.2000;41:471–473.
40. Monneuse O, Gruner L, Henry L, et al. [Hepatic portal venous gas.]Ann Chir. 2000;125:435–438.
41. Gosink BB. Intrahepatic gas: differential diagnosis. AJR Am JRoentgenol. 1981;137:763–767.
42. Peloponissios N, Halkic N, Pugnale M, et al. Hepatic portal gas inadults: review of the literature and presentation of a consecutiveseries of 11 cases. Arch Surg. 2003;138:1367–1370.
43. Furuya Y, Yasuhara H, Ariki K, et al. Hepatic portal venous gascaused by blunt abdominal trauma: is it a true ominous sign ofbowel necrosis? Report of a case. Surg Today. 2002;32:655–658.
44. Nesher E, Aizner A, Kashtan H, et al. Portal vein air embolizationafter blunt abdominal trauma: a case report and review of theliterature. Eur J Emerg Med. 2002;9:163–165.
45. Vauthey JN, Matthews CC. Portal vein air embolization after bluntabdominal trauma. Am Surg. 1988;54:586–588.
46. Friedman D, Flancbaum L, Ritter E, Trooskin SZ. Hepatic portalvenous gas identified by computed tomography in a patient withblunt abdominal trauma: a case report. J Trauma. 1991;31:290–292.
47. Wu JW, Chen MY, Auringer ST. Portal venous gas: an unusualfinding in child abuse. J Emerg Med. 2000;18:105–107.
48. Pedal I, Moosmayer A, Mallach HJ, Oehmichen M. [Air embolismor putrefaction? Gas analysis findings and their interpretation.]Z Rechtsmed. 1987;99:151–167.
49. Patzelt D, Lignitz E, Keil W, Takatsu A. [Diagnostic problem of airembolism in a corpse.] Beitr Gerichtl Med. 1979;37:401–405.
50. Keil W, Bretschneider K, Patzelt D, et al. [Air embolism orputrefaction gas? The diagnosis of cardiac air embolism in thecadaver.] Beitr Gerichtl Med. 1980;38:395–408.
51. Oliver J, Lyons TJ, Harle R. The role of computed tomography inthe diagnosis of arterial gas embolism in fatal diving accidents inTasmania. Australas Radiol. 1999;43:37–40.
52. Plattner T, Thali MJ, Yen K, et al. Virtopsy-postmortem multislicecomputed tomography (MSCT) and magnetic resonance imaging(MRI) in a fatal scuba diving incident. J Forensic Sci. 2003;48:1347–1355.
53. Froboese C. Uber die Luftembolie der Milz. Ferner kurze Mitteilunguber ein ungeklartes Pneumopericard. Virchows Arch Path Anat.1947;314:39.
54. Jetter WW. Post-mortem biochemical changes. J Forensic Sci. 1959;4:330–341.
55. Daldrup T. Postmortaler Eiweisszerfall in menschlichen Organen:Reaktionen und zeitliche Zusammenhange. Thesis, Aachen; 1978.
56. Sasaki T, Nanjo H, Takahashi M, et al. Non-traumatic gas gangrenein the abdomen: report of six autopsy cases. J Gastroenterol. 2000;35:382–390.
57. Liebman PR, Patten MT, Manny J, Benfield JR, Hechtman HB.Hepatic–portal venous gas in adults: etiology, pathophysiology andclinical significance. Ann Surg. 1978;187:281–287.
58. Chen KW, Shin JS, Chi CH, Cheng L. Seizure: a rare and transientcause of portal venous gas. Am J Gastroenterol. 1997;92:351–352.
59. Sebastia C, Quiroga S, Espin E, et al. Portomesenteric vein gas:pathologic mechanisms, CT findings, and prognosis. Radiographics.2000;20:1213–1224.
60. Niki M, Shimizu I, Horie T, et al. Hepatic portal venous gasdisappearing within 24 hours. Intern Med. 2002;41:950–952.
The Journal of TRAUMA� Injury, Infection, and Critical Care
988 April 2007




















