
Percutaneous Transluminal Aortic Angioplasty: Techniques and Results
Upload
independentCategory
view
5download
0
logy 130 (2008) 220–226www.elsevier.com/locate/ijcard
International Journal of Cardio
Coronary cyclic flow variations following primary angioplastyis associated with poor short-term prognosis
Mariano Albertal a,⁎, Fernando Cura a, Mitchell W. Krucoff b, Ricardo Baeza d,Alejandro Garcia Escudero c, Lucio T. Padilla a, Jorge Thierer a, Sebastian Fieg a,
Marcelo Trivi a, Jorge A. Belardi a
For the PREMIAR investigatorsa Department of Interventional Cardiology and Endovascular Therapeutics, Instituto Cardiovascular de Buenos Aires, Buenos Aires, Argentina
b Department of Cardiology, Duke University Medical Center, Durham, North Carolina, USAc Department of Interventional Cardiology, Hospital Cosme Argerich, Buenos Aires, Argentina
d Department of Cardiology, Catholic University Hospital, Santiago, Chile
Received 19 December 2006; received in revised form 24 July 2007; accepted 3 August 2007
Available online 4 March 2008
Abstract
Aims: Recent studies have shown that coronary cyclic flow variations (CCFV) is a platelet-related phenomenon that occurred followingreperfusion. Although CCFV predicts acute complications following thrombolytic therapy, its impact following percutaneous coronaryinterventions (PCI) has not been evaluated yet.Methods and results: One hundred and thirty-one patients with ST-segment Elevation Myocardial Infarction (STEMI) who underwent PCI wereincluded in the analysis. All patients have 24-hour ST-segment monitoring. The development of CCFVwas defined as≥ 3 ST-segment transitions(≥150μV).We divided the population in two groups according to the presence (n=14, 10.6%) or absence (n=117) of CCFV. The relation betweenCCFV and 30-day major adverse cardiac events (MACE) was analyzed using a multivariate logistic regression model adjusting for age, sex,diabetes, smoking, anterior infarct, Killip class, and final TIMI flow grade. Clinical and angiographic characteristics were similar between the twogroups. Higher 30-daymortality (21.4 vs. 3.8%, p=0.022) andMACE rates (42.9 vs. 10.7%, p=0.005) were seen in the CCFVgroup.Multivariateregression analysis revealed that patients with CCFV were at increased risk of 30-day MACE (adjusted RR 5.09; 95% CI 1.319.1; p=0.0016).Conclusion: The presence of CCFValtered primary PCI may provide an early indication of insufficient myocardial perfusion and impendingcatastrophic outcome.© 2007 Elsevier Ireland Ltd. All rights reserved.
Keywords: Thrombosis; Infarction; Cyclic flow; ECG monitoring
1. Introduction
Cyclic Coronary Flow Variation (CCFV) was first de-scribed in dogs following coronary arterial Injury [1]. In thiscanine model, the circumflex artery of an anesthetized dogwas dissected out and an electromagnetic flow-meter probe
⁎ Corresponding author. Instituto Cardiovascular de Buenos Aires, BlancoEncalada 1543, Buenos Aires, Argentina.
E-mail address: [email protected] (M. Albertal).
0167-5273/$ - see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2007.08.085
was placed on the artery to continuously measure coronaryblood flow. A plastic encircling cylinder was then placedaround the outside of the coronary artery distal to the flowprobe. The cylinder produced a 70% stenosis and intimaldamage. In this scenario, coronary blood flow periodicallydeclined to zero, producing transient myocardial ischemia.Given time, the blood flow would normalize, leading to theresolution of the ischemia. In the above study, the develop-ment of CCFV was caused by a platelet-mediated thrombus[2–4] gradually forming in the narrowed lumen, till it
221M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
eventually blocked off the blood flow completely. Shortlyafterwards the blood flow was suddenly restored, when thefresh, flimsy thrombus broke up, clearing the lumen andembolizing distally.
The development of CCFVafter an elective procedure [5],though rare, forecast impending acute vessel closure. CCFVhas been reported in 30–50% of patients with acute ST-seg-ment Elevation Myocardial Infarction (STEMI) treated withthrombolytic therapy [6–12], both before and after treatment.To date, the occurrence of this phenomenon after primarypercutaneous interventions (PCI) has not been reported.
Continuous high fidelity ECG monitoring of ST-segmentrecovery provides accurate assessment of the timing andquality of myocardial reperfusion during STEMI [13,14] andallows precise detection of CCFV [6–12]. Based on this, acontinuous ST-segment monitoring sub-analysis was per-formed as part of the “Protection of Distal Embolization inHigh-Risk Patients with Acute Myocardial Infarction”(PREMIAR) trial in an attempt to evaluate the incidence of
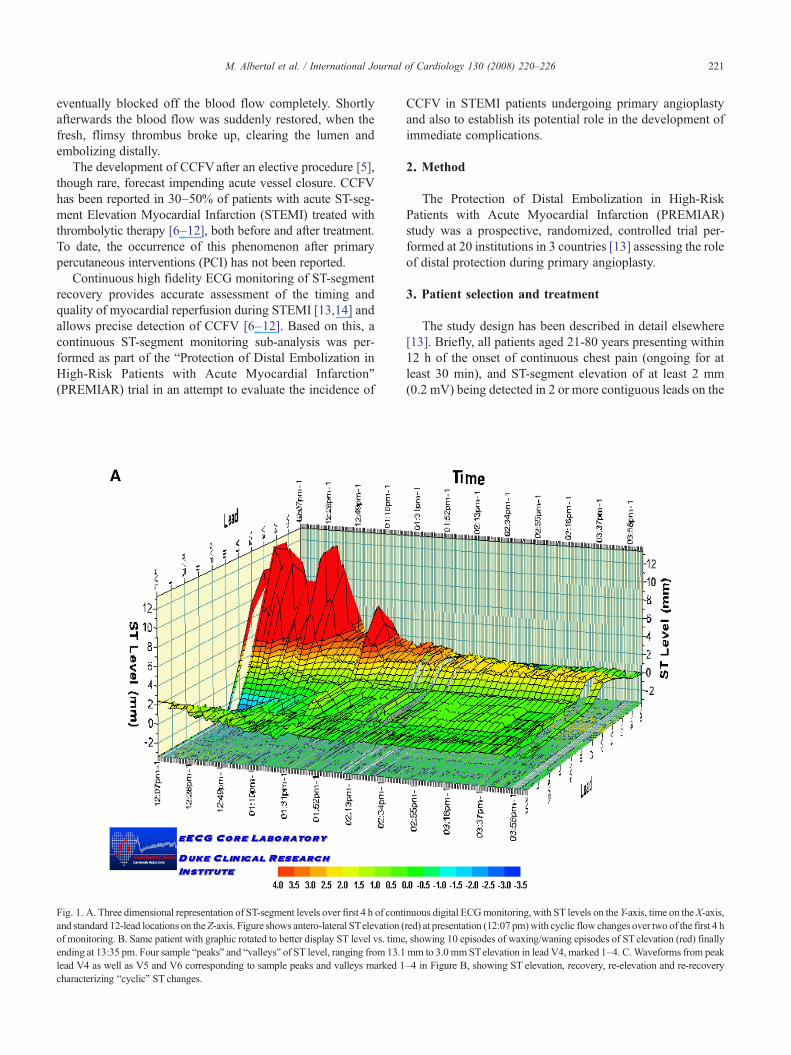
Fig. 1. A. Three dimensional representation of ST-segment levels over first 4 h of contand standard 12-lead locations on theZ-axis. Figure shows antero-lateral STelevation (of monitoring. B. Same patient with graphic rotated to better display ST level vs. timeending at 13:35 pm. Four sample “peaks” and “valleys” of ST level, ranging from 13.1lead V4 as well as V5 and V6 corresponding to sample peaks and valleys marked 1characterizing “cyclic” ST changes.
CCFV in STEMI patients undergoing primary angioplastyand also to establish its potential role in the development ofimmediate complications.
2. Method
The Protection of Distal Embolization in High-RiskPatients with Acute Myocardial Infarction (PREMIAR)study was a prospective, randomized, controlled trial per-formed at 20 institutions in 3 countries [13] assessing the roleof distal protection during primary angioplasty.
3. Patient selection and treatment
The study design has been described in detail elsewhere[13]. Briefly, all patients aged 21-80 years presenting within12 h of the onset of continuous chest pain (ongoing for atleast 30 min), and ST-segment elevation of at least 2 mm(0.2 mV) being detected in 2 or more contiguous leads on the
inuous digital ECGmonitoring, with ST levels on the Y-axis, time on theX-axis,red) at presentation (12:07 pm)with cyclic flow changes over two of the first 4 h, showing 10 episodes of waxing/waning episodes of STelevation (red) finallymm to 3.0 mmSTelevation in lead V4, marked 1–4. C.Waveforms from peak–4 in Figure B, showing ST elevation, recovery, re-elevation and re-recovery
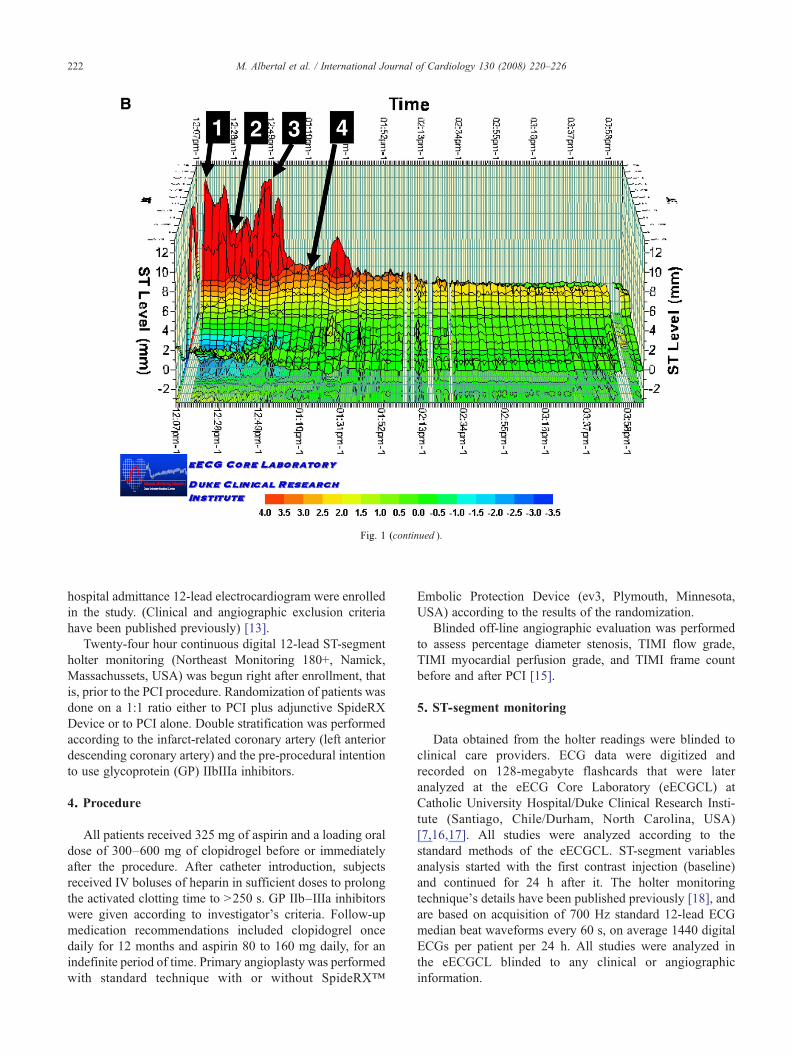
Fig. 1 (continued ).
222 M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
hospital admittance 12-lead electrocardiogram were enrolledin the study. (Clinical and angiographic exclusion criteriahave been published previously) [13].
Twenty-four hour continuous digital 12-lead ST-segmentholter monitoring (Northeast Monitoring 180+, Namick,Massachussets, USA) was begun right after enrollment, thatis, prior to the PCI procedure. Randomization of patients wasdone on a 1:1 ratio either to PCI plus adjunctive SpideRXDevice or to PCI alone. Double stratification was performedaccording to the infarct-related coronary artery (left anteriordescending coronary artery) and the pre-procedural intentionto use glycoprotein (GP) IIbIIIa inhibitors.
4. Procedure
All patients received 325 mg of aspirin and a loading oraldose of 300–600 mg of clopidrogel before or immediatelyafter the procedure. After catheter introduction, subjectsreceived IV boluses of heparin in sufficient doses to prolongthe activated clotting time to N250 s. GP IIb–IIIa inhibitorswere given according to investigator's criteria. Follow-upmedication recommendations included clopidogrel oncedaily for 12 months and aspirin 80 to 160 mg daily, for anindefinite period of time. Primary angioplasty was performedwith standard technique with or without SpideRX™
Embolic Protection Device (ev3, Plymouth, Minnesota,USA) according to the results of the randomization.
Blinded off-line angiographic evaluation was performedto assess percentage diameter stenosis, TIMI flow grade,TIMI myocardial perfusion grade, and TIMI frame countbefore and after PCI [15].
5. ST-segment monitoring
Data obtained from the holter readings were blinded toclinical care providers. ECG data were digitized andrecorded on 128-megabyte flashcards that were lateranalyzed at the eECG Core Laboratory (eECGCL) atCatholic University Hospital/Duke Clinical Research Insti-tute (Santiago, Chile/Durham, North Carolina, USA)[7,16,17]. All studies were analyzed according to thestandard methods of the eECGCL. ST-segment variablesanalysis started with the first contrast injection (baseline)and continued for 24 h after it. The holter monitoringtechnique's details have been published previously [18], andare based on acquisition of 700 Hz standard 12-lead ECGmedian beat waveforms every 60 s, on average 1440 digitalECGs per patient per 24 h. All studies were analyzed inthe eECGCL blinded to any clinical or angiographicinformation.
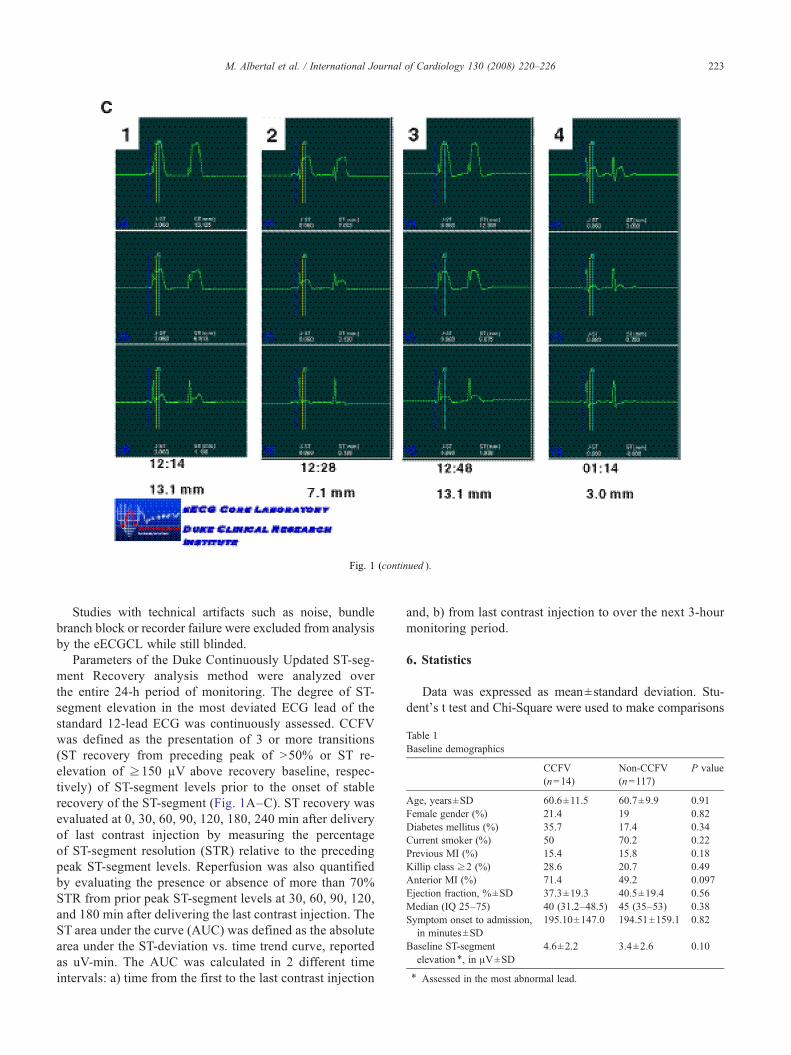
Fig. 1 (continued ).
Table 1Baseline demographics
CCFV(n=14)
Non-CCFV(n=117)
P value
Age, years±SD 60.6±11.5 60.7±9.9 0.91Female gender (%) 21.4 19 0.82Diabetes mellitus (%) 35.7 17.4 0.34Current smoker (%) 50 70.2 0.22Previous MI (%) 15.4 15.8 0.18Killip class ≥2 (%) 28.6 20.7 0.49Anterior MI (%) 71.4 49.2 0.097Ejection fraction, %±SD 37.3±19.3 40.5±19.4 0.56Median (IQ 25–75) 40 (31.2–48.5) 45 (35–53) 0.38Symptom onset to admission,
in minutes±SD195.10±147.0 194.51±159.1 0.82
Baseline ST-segmentelevation ⁎, in μV±SD
4.6±2.2 3.4±2.6 0.10
⁎ Assessed in the most abnormal lead.
223M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
Studies with technical artifacts such as noise, bundlebranch block or recorder failure were excluded from analysisby the eECGCL while still blinded.
Parameters of the Duke Continuously Updated ST-seg-ment Recovery analysis method were analyzed overthe entire 24-h period of monitoring. The degree of ST-segment elevation in the most deviated ECG lead of thestandard 12-lead ECG was continuously assessed. CCFVwas defined as the presentation of 3 or more transitions(ST recovery from preceding peak of N50% or ST re-elevation of ≥150 μV above recovery baseline, respec-tively) of ST-segment levels prior to the onset of stablerecovery of the ST-segment (Fig. 1A–C). ST recovery wasevaluated at 0, 30, 60, 90, 120, 180, 240 min after deliveryof last contrast injection by measuring the percentageof ST-segment resolution (STR) relative to the precedingpeak ST-segment levels. Reperfusion was also quantifiedby evaluating the presence or absence of more than 70%STR from prior peak ST-segment levels at 30, 60, 90, 120,and 180 min after delivering the last contrast injection. TheST area under the curve (AUC) was defined as the absolutearea under the ST-deviation vs. time trend curve, reportedas uV-min. The AUC was calculated in 2 different timeintervals: a) time from the first to the last contrast injection
and, b) from last contrast injection to over the next 3-hourmonitoring period.
6. Statistics
Data was expressed as mean±standard deviation. Stu-dent's t test and Chi-Square were used to make comparisons
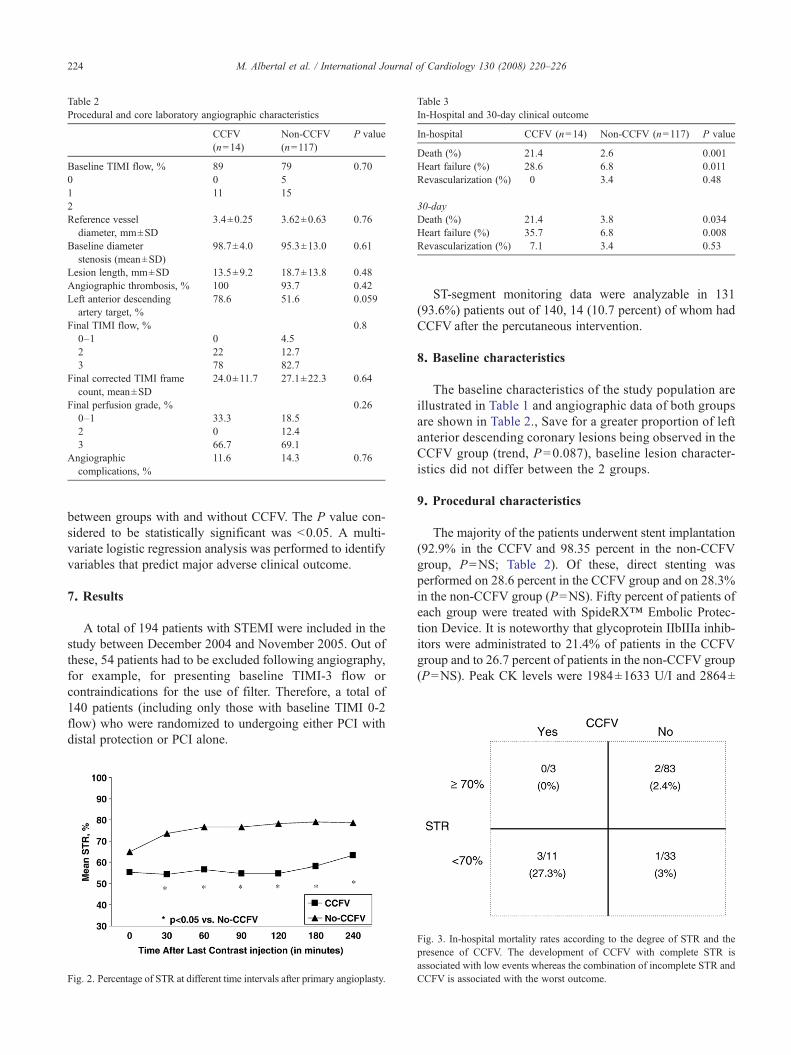
Table 2Procedural and core laboratory angiographic characteristics
CCFV(n=14)
Non-CCFV(n=117)
P value
Baseline TIMI flow, % 89 79 0.700 0 51 11 152Reference vessel
diameter, mm±SD3.4±0.25 3.62±0.63 0.76
Baseline diameterstenosis (mean±SD)
98.7±4.0 95.3±13.0 0.61
Lesion length, mm±SD 13.5±9.2 18.7±13.8 0.48Angiographic thrombosis, % 100 93.7 0.42Left anterior descending
artery target, %78.6 51.6 0.059
Final TIMI flow, % 0.80–1 0 4.52 22 12.73 78 82.7
Final corrected TIMI framecount, mean±SD
24.0±11.7 27.1±22.3 0.64
Final perfusion grade, % 0.260–1 33.3 18.52 0 12.43 66.7 69.1
Angiographiccomplications, %
11.6 14.3 0.76
Table 3In-Hospital and 30-day clinical outcome
In-hospital CCFV (n=14) Non-CCFV (n=117) P value
Death (%) 21.4 2.6 0.001Heart failure (%) 28.6 6.8 0.011Revascularization (%) 0 3.4 0.48
30-dayDeath (%) 21.4 3.8 0.034Heart failure (%) 35.7 6.8 0.008Revascularization (%) 7.1 3.4 0.53
224 M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
between groups with and without CCFV. The P value con-sidered to be statistically significant was b0.05. A multi-variate logistic regression analysis was performed to identifyvariables that predict major adverse clinical outcome.
7. Results
A total of 194 patients with STEMI were included in thestudy between December 2004 and November 2005. Out ofthese, 54 patients had to be excluded following angiography,for example, for presenting baseline TIMI-3 flow orcontraindications for the use of filter. Therefore, a total of140 patients (including only those with baseline TIMI 0-2flow) who were randomized to undergoing either PCI withdistal protection or PCI alone.
Fig. 2. Percentage of STR at different time intervals after primary angioplasty.
ST-segment monitoring data were analyzable in 131(93.6%) patients out of 140, 14 (10.7 percent) of whom hadCCFV after the percutaneous intervention.
8. Baseline characteristics
The baseline characteristics of the study population areillustrated in Table 1 and angiographic data of both groupsare shown in Table 2., Save for a greater proportion of leftanterior descending coronary lesions being observed in theCCFV group (trend, P=0.087), baseline lesion character-istics did not differ between the 2 groups.
9. Procedural characteristics
The majority of the patients underwent stent implantation(92.9% in the CCFV and 98.35 percent in the non-CCFVgroup, P=NS; Table 2). Of these, direct stenting wasperformed on 28.6 percent in the CCFV group and on 28.3%in the non-CCFV group (P=NS). Fifty percent of patients ofeach group were treated with SpideRX™ Embolic Protec-tion Device. It is noteworthy that glycoprotein IIbIIIa inhib-itors were administrated to 21.4% of patients in the CCFVgroup and to 26.7 percent of patients in the non-CCFV group(P=NS). Peak CK levels were 1984±1633 U/I and 2864±
Fig. 3. In-hospital mortality rates according to the degree of STR and thepresence of CCFV. The development of CCFV with complete STR isassociated with low events whereas the combination of incomplete STR andCCFV is associated with the worst outcome.

225M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
1849 U/I for the CCFV and non-CCFV groups (P=NS),respectively. Post-procedural angiographic flow parame-ters such as TIMI flow grade, TIMI frame count and TIMIperfusion grade did not differ between the groups (Table 2).
10. ST-segment recovery analysis
The quality of reperfusion according to ECG analysis ofpercentage STR is shown in Figs. 1 and 2. The degree ofSTR did not differ between the groups at 0 min (that is pointof delivery of last contrast injection), whereas values at 30,60, 90, 120, 180 and 240 min remained lower in the CCFVcompared to those in the non-CCFV group (Figs. 1 and 2).
During the percutaneous procedure, the median AUCwas comparable between groups (4107 in CCFV group vs.3778 μV-minutes in the non-CCFV group, P=0.58), where-as a significantly higher median AUC was observed afterthe procedure in patients with CCFV (7076 vs. 5500 μV-minutes, P=0.023).
11. Clinical outcome
In-hospital and 30-day clinical outcome are depicted inTable 3. Death and congestive heart failure were morecommon in the CCFV group than in the non-CCFV group(Table 3). Major adverse cardiac events rates (death, re-infarction, congestive heart failure and urgent revasculariza-tion) were higher in the CCFV group during hospitalization(28.6 vs. 9.5%, P=0.058) and at 30 days (42.9 vs. 10.7percent, P=0.005).
The combination of CCFV and presence of incompleteSTR (b70%) at 90 min showed the worst clinical outcome,whereas no deaths were observed in patients with CCFVwho achieved complete STR (Fig. 3). Patients withoutCCFV had low death rates, regardless of the degree of STR(Fig. 3).
Stepwise multivariate logistic regression analysis identi-fied the following predictors of 30-day major adverse cardiacevents: increasing heart rate (1.04; 95% CI 1.0 to 1.08,P=0.021), high Killip class (3.65; 95% CI 1.17 to 11.3,P=0.025) and the presence of CCFV (5.09, 95% CI 1.35to 19.14, P=0.016). Age, STEMI location and presence ofdiabetes did not emerge as significant predictors of majoradverse cardiac events.
12. Discussion
Approximately 10 percent of patients in the study dem-onstrated CCFV, which was associated with an adverseshort-term clinical outcome. Interestingly, although bothexperimental and human reports have suggested platelets ashaving a key role in this phenomenon, intense plateletinhibition induced by the administration of IV heparin bolusand clopidrogel loading did not prevent the development ofCCFV in the present study. Moreover, stent implantation thatwas also expected to contribute to plaque stabilization, by
sealing intimal tears didn't seem to prevent CCFV either,suggesting that this phenomenon may be more related tomicrovascular changes than epicardial mechanics.
To date, scant data have been reported regarding CCFVfollowing balloon angioplasty [19,20], and there are no reportsavailable evaluating its development after stent implantation.Our study is the first published experience investigating CCFVin patients undergoing stent implantation during primaryangioplasty. One may infer, from our findings, that it may notbe possible to predict the development of CCFV during and/orimmediately after the percutaneous intervention, using moreroutinely available static methods such as post-proceduralangiographic and/or serial static electrocardiographic resultsAlmost by definition, CCFV requires continuous methodolo-gies such as ECG monitoring, and continuously updatedanalysis techniques, to define its presence whether in real time,for clinical use, or retrospectively in research, such as is pre-sented in this report.
Since ST-segment monitoring started during first contrastinjection, it is possible that some transient ST re-elevationscould result from the mechanical PCI coronary occlusionsthemselves.With the average duration of balloon inflations forstenting at 30 s or less, and the resolution of the continuousECGs at 60 s, the influence of the PCI procedure in differ-entiating these groups is unlikely. Furthermore, the similarnumber of balloon inflations across the two groups and thesimilar median AUC during the procedure and STR im-mediately after the procedure suggests the CCFV phenomenareported here are not simply a reflection of the PCI inflations.
Importantly in our observations, CCFV had strong pre-dictive information related to short-term outcome. Based onthe importance of this feature in predictive regressionmodels,it should be noted for future studies that use of static markerssuch as angiographic blush, serial static ECGs or enzymecurves couldn't identify the presence of CCFV events.Interestingly, and consistent with findings in recent rando-mized studies, the use of distal protection devices in our studydid not seem to affect the development of CCFV, showing nosubstantial benefits as an adjunctive tool during primaryangioplasty [14,21].
13. Study limitations
Though most of the important clinical characteristicspreviously known to influence AMI outcomes were similarbetween the two groups, it is also true that the retrospectivedesign of this study and the size of the study population raisethe potential for confounding. In the PREMIAR trial, patientswith basal TIMI III flow or with unsuitable coronary anatomyfor distal filter placement were excluded. These exclusioncriteria may have altered the actual incidence of CCFV. In ourstudy, the putative mechanisms involved in the developmentof CCFV were not explored. Post-procedural intra-coronaryultrasound evaluation or translesional gradient assessmentmay have contributed to further understanding of this phe-nomenon. Despite these limitations, the strong difference

226 M. Albertal et al. / International Journal of Cardiology 130 (2008) 220–226
found in death rate appears intriguing and warrants furtherinvestigation in larger studies.
14. Conclusion
The presence of CCFV, although infrequent after primaryangioplasty, may provide an early indication of insufficientmyocardial perfusion and impending catastrophic outcome.Detection and quantification of this phenomenon in humanpatients presenting with STEMI requires a continuous mon-itoring technique, for which non-invasive, high fidelitydigital ECG recording appears well suited.
References
[1] Folts JD, Crowell Jr EB, Rowe GG. Platelet aggregation in partiallyobstructed vessels and its elimination with aspirin. Circulation1976;54:365–70.
[2] Apprill P, Schmitz JM, Campbell WB, et al. Cyclic blood flow variationsinduced by platelet-activating factor in stenosed canine coronary arteriesdespite inhibition of thromboxane synthetase, serotonin receptors, andalpha-adrenergic receptors. Circulation 1985;72:397–405.
[3] Bush LR, Campbell WB, Buja LM, Tilton GD,Willerson JT. Effects ofthe selective thromboxane synthetase inhibitor dazoxiben on variationsin cyclic blood flow in stenosed canine coronary arteries. Circulation1984;69:1161–70.
[4] Ashton JH, Schmitz JM, Campbell WB, et al. Inhibition of cyclic flowvariations in stenosed canine coronary arteries by thromboxane A2/prostaglandin H2 receptor antagonists. Circ Res 1986;59:568–78.
[5] Eichhorn EJ, Grayburn PA, Willard JE, et al. Spontaneous alterationsin coronary blood flow velocity before and after coronary angioplastyin patients with severe angina. J Am Coll Cardiol 1991;17:43–52.
[6] Veldkamp RF, Green CL,Wilkins ML, et al. Comparison of continuousST-segment recovery analysis with methods using static electrocardio-grams for noninvasive patency assessment during acute myocardialinfarction. Thrombolysis and Angioplasty in Myocardial Infarction(TAMI) 7 Study Group. Am J Cardiol 1994;73:1069–74.
[7] Krucoff MW. Cyclic coronary flow: defining preinfarction angina atthe crossroads of unstable angina and myocardial infarction. Md Med2001:60–4 Suppl.
[8] Dellborg M, Riha M, Swedberg K. Dynamic QRS-complex and ST-segment monitoring in acute myocardial infarction during recombinanttissue-type plasminogen activator therapy. The TEAHAT Study Group.Am J Cardiol 1991;67:343–9.
[9] Dellborg M, Topol EJ, Swedberg K. Dynamic QRS complex and STsegment vectorcardiographic monitoring can identify vessel patency in
patients with acute myocardial infarction treated with reperfusiontherapy. Am Heart J 1991;122:943–8.
[10] Johanson P, Svensson AM, Dellborg M. Clinical implications of earlyST-segment variability. A report from the ASSENT 2 ST-monitoringsub-study. Coron Artery Dis 2001;12:277–83.
[11] Johanson P, Swedberg K, Dellborg M. ST variability during the first4 hours of acute myocardial infarction predicts 1-year mortality. AnnNoninvasive Electrocardiol 2001;6:198–202.
[12] Johanson P, Wallentin L, Nilsson T, Bergstrand L, Lindahl B, DellborgM. ST-segment analyses and residual thrombi in the infarct-relatedartery: a report from the ASSENT PLUS ST-monitoring substudy. AmHeart J 2004;147:853–8.
[13] Cura F, Garcia Escudero A, Berrocal D, et al. Protection of DistalEmbolization in High-Risk Patients with Acute ST-Segment ElevationMyocardial Infarction Randomized Controlled Trial. AJC J Feb 12006;99(3):357–63.
[14] Stone GW, Webb J, Cox DA, et al. Distal microcirculatory protectionduring percutaneous coronary intervention in acute ST-segmentelevation myocardial infarction: a randomized controlled trial. JAMA2005;293:1063–72.
[15] Henriques JP, Zijlstra F, van 't Hof AW, et al. Angiographic assessmentof reperfusion in acute myocardial infarction by myocardial blushgrade. Circulation 2003;107:2115–9.
[16] Ohman EM, Kleiman NS, Gacioch G, et al. Combined acceleratedtissue-plasminogen activator and platelet glycoprotein IIb/IIIa integrinreceptor blockade with integrilin in acute myocardial infarction.Results of a randomized, placebo-controlled, dose-ranging trial.IMPACT-AMI investigators. Circulation 1997;95:846–54.
[17] Moliterno DJ, Topol EJ. Conjunctive use of platelet glycoprotein IIb/IIIa antagonists and thrombolytic therapy for acute myocardialinfarction. Thromb Haemost 1997;78:214–9.
[18] Roe MT, Green CL, Giugliano RP, et al. Improved speed and stabilityof ST-segment recovery with reduced-dose tenecteplase and eptifiba-tide compared with full-dose tenecteplase for acute ST-segmentelevation myocardial infarction. J Am Coll Cardiol 2004;43:549–56.
[19] Sunamura M, di Mario C, Piek JJ, et al. Cyclic flow variations afterangioplasty: a rare phenomenon predictive of immediate complica-tions. DEBATE Investigator's Group. Am Heart J 1996;131:843–8.
[20] Anderson HV, McNatt J, Clubb FJ, et al. Platelet inhibition reducescyclic flow variations and neointimal proliferation in normal andhypercholesterolemic–atherosclerotic canine coronary arteries. Circu-lation 2001;104:2331–7.
[21] Gick M, Jander N, Bestehorn HP, et al. Randomized evaluation of theeffects of filter-based distal protection on myocardial perfusion andinfarct size after primary percutaneous catheter intervention inmyocardial infarction with and without ST-segment elevation.Circulation 2005;112:1462–9.
Copyright © 2022 FDOKUMEN




















