
Early Versus Late Functional Outcome After Successful Percutaneous Pulmonary Valve Implantation
Upload
independentCategory
view
1download
0
Cardiovasc lntervent Radiol ~1993) 16:37-42 CardioVascular and ]nter onal Radio y �9 Springer-Verlag New York Inc. 1993
Percutaneous Transluminal Aortic Angioplasty: Early and Late Results
B e n y a m i n a Morag, ~ Alexander Garn iek , L A,'ie Bass, 2 Jacob Schnciderman,-" Raphael Walden , 2 and Za l lman J. Rubins te in ~
Division of Angiography and [nterventional Radiology. Departments of ~Radiology and :Vascular Surgery, The Chaim Sheba Medical Center. TeI-Hashomer and Sackler School of Medicine, TeI-Aviv University, Israel
Abstract. Percu t aneous t rans lumina l angioplas ty of" the infrarenal abdomina l aorta (13 pat ients) and its bifi.lrcation (15 patients) ,,',as per formed in 28 pa- t ients with a total of 32 di latat ion procedures . The group cons is ted of 16 female and 12 male pat ients and initial successful di la tat ion was achieved in all. Recu r rence within 1 month requir ing bypass surgery occur red in I pat ient . Three pat ients were lost to fol low-up. Long- te rm follow-up in the remaining 24 pat ients ranged from I to 9 years with a mean of 4.5 years. During the fol low-up period, repeat angi- oplas ty of the original s tenosis was performed in 3 pat ients and ano the r pat ient unde rwen t di la tat ion of a new lesion which deve loped in the aorta. Accord- ing to clinical and non invas ive studies, these 4 pa- t ients , as well as the other 20. have main ta ined pa- tency of the treated lesions and arc symp tom free. No immedia te compl ica t ions requir ing surgery oc- curred. We conc lude that angioplas ty is the initial t r ea tmen t of choice in focal lesions of the distal ab- domina l aor ta and its bi furcat ion.
Key words: Aorta , t r ans lumina l a n g i o p l a s t y - - A r t e r - ies, s tenosis
P e r c u t a n e o u s t r ans lumina l angioplas ty (PTA) of pe- ripheral vascu la r disease has been ex tens ive ly re- por ted, with a large series of cases runn ing into the hundreds . In the iliac, femoral , and popli teal areas, long- te rm fol low-up studies have repor ted satisfac- tory overall results [1-6]. However , reports dealing
Address reprint requests to: Benyamina Morag. M.D., Division of Angiography and Interventional Radiology, Department of Radiology. The Chaim Sheba Medical Center, Tel-Hashomer, Israel 52621
specifically with pe rcu taneous t rans lumina l aortic angioplas ty (PTAA) are sporadic and con ta in rela- t ively small n u m b e r s of pat ients [7-13]. Recent ly . reports of larger series have begun to appear , with fol low-up per iods averaging fi-om 25 to 33 months [14-17]. Most series ment ion that the aortic pathol- o,,y~ occurs in relat ively youn~z~ female pat ients , usu- ally heavy smokers , and in whom the aorta is hypo- plastic [12, 13, 18-20].
The age and sex d is t r ibut ion in the present series differs somewha t fl'om those reported by other au- thors. Our initial exper ience with 14 pat ients was p resen ted in 1987 [11]. We now present the results in 28 treated pat ients with special emphas is on the long- term fol low-up which averages 54 months . In- c luding repeat p rocedures , a total of 32 di la tat ions were performed.
Material and Methods
Between 1981 and 1990. 28 patients underwent PTAA. The age and sex distributions of the patients are sho',vn in 'l'akqe I. All the 16 female and 6 of the male patients were heavy smokers. Diabe- tes mellitus was present in I female and 2 mate patients and hypertension 'aas noted in 2 male patients only. All patients had bilateral Iov.,er limb elaudication, with 1 female and 4 males having rest pain.
Diagnostic angiography was performed either via axillarv or the translumbar route. In 13 patients the site of stenosis was in the distal abdominal aorta between the level of the renal arteries and the bifurcation I Fig. I). and in the other 15 the aortic bifurca- tion was involved I Fig. 2). Isolated proximal iliac artery stenoses were not included in this series. There was no male/female differ- ence regarding the site of stenosis. The size of the uninvolved segment of the aorta ranged from II to 18 mm. Although not statistically proven, the female patients tended to have small aortic diameters. Associated distal disease in the iliac, femoral, or popliteal arteries was present in 7 of the 12 male~, and only 3 of the 16 female patients ~Table 2).
For PTAA. the double balloon technique was used in all the

38 B. blorag et al.: Percutaneous Trans lumina l Aortic Angioplas ty
Fig. 1. A 40-year-old female pauent with severe bilateral claudication at 100 m. A Severe aortic s tenos is at the L,4 level imme~ diately proximal to the bifurcation with a sy~,tolic p ressure gradient of 90 mm Hg. B Double balloon dilatation. C Po,~tdilatation aortogram. No residual pressure gradient. D Second aortic stenotic lesion appearing 3 years htter at the L3 levet with a pressure gradient of 70 m m Hg. The original angi- oplasty site remains well patent. E After dilatation of the second stenotic lesion. No residual p res su re gradient. Patient had re- mained a symptomat i c for the 5 years since follow-up angioplas ty .
Table 1. Patient statistics
Age Male Female
30-50 2 l0 51-60 6 4 61-80 4 2 Total 12 1"-6
Table 2. Incidence oF distal disease
Age Male Female
30-50 1 1 51-60 3 I 61-80 :~ I Total 7 3
bifurcation lesions and in 7 of the aortic s tenoses ~,Fig. 3~, before the introduction of large balloons [9, 1 I 1. Since then. the remain- ing 6 patients with aortic lesions have been treated with a single balloon (Fig. I). The balloon size was calculated according to the vessel diameter measured on the diagnostic angiogram, with 12-ram balloons being the largest used in the aorta. In order to avoid overst re tching, the chosen balloon diameter was I-2 mm less than the width of the aorta above and below the stenosis.
Ba!loon inflation was discont inued wheneve r the patient noted abdominal or back pain. The length of the balloons used depended on the length of the stenotic segment (Fig. 2). Angioplasty was performed via the transfemoral app roach in all patients.
Systolic, diastolic, and mean arterial pressures were recorded proximal and dista! to the tesions before and after the dilatat ions, with post -PTAA angiography being per formed at the end of the procedure. The main parameter in a s se s s ing the result of dilata-
B. Morag et al.: Pereutaneous Transluminal Aortic Angioplasty 39
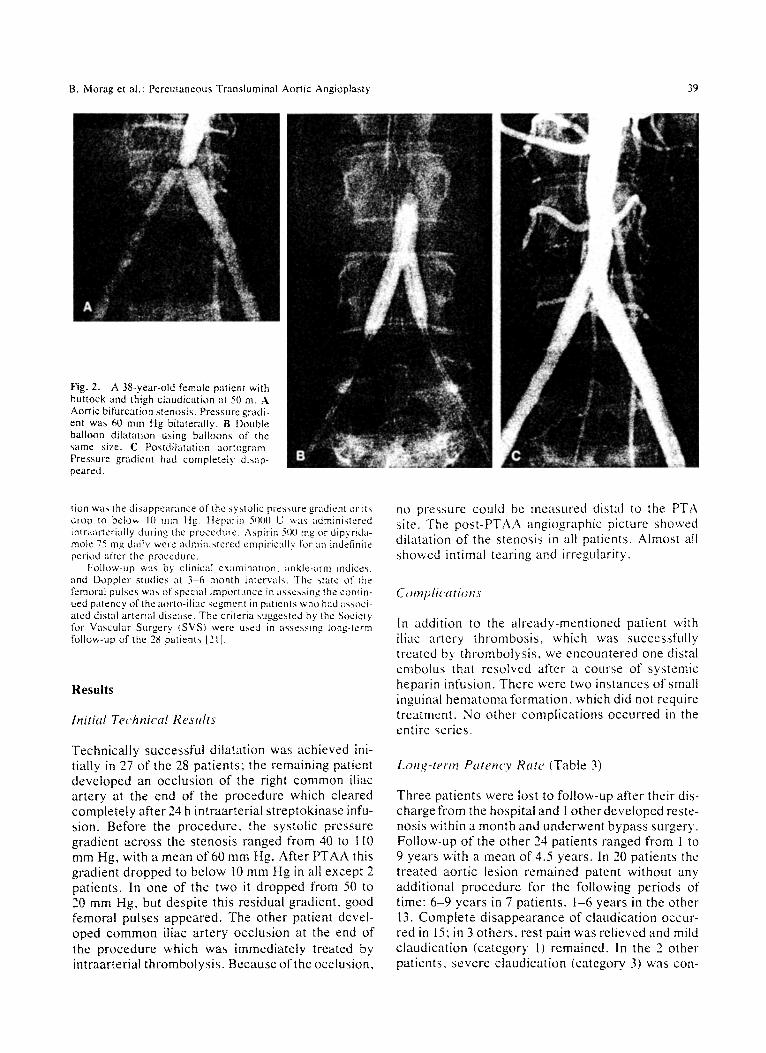
Fig. 2. A 38-year-old female patient with buttock and thigh claudication at 50 m. A Aortic bifurcation stenosis . Pressure gradi- ent was 60 mm Hg bilaterally. B Double balloon dilatation using balloons of the same size. C Postdilatation a o r t o g r a m Pressure gradient had completely db, ap- peared.
tion was the disappearance of the systolic pressure gradient or its drop to below 10 mm Hg. Heparin 5000 U was administered intraarteriaily dr, ring the procedure. Aspirin 500 mg or dip.vrMa- mole 75 mg daily were adminislered empirically for an indefinite period after the procedure.
Folk>w-up was by clinical examinat ion, ankle-arm indices. and Doppler studies at 3 -6 month intervals. The state o r t h e femoral pulses was of special importance in assess ing the contin- ued patency of the aorto-il[ac segment in patients who had asst;,ci- ated distal arterial disease. The criteria .suggested by the Society for Vascular Surgery {SVS) were u~,ed in assess ing long-term follow-up of the 28 patients [21].
Results
Initial Technical ResMts
Technically successful dilatation was achieved ini- tially in 27 of the 28 patients; the remaining patient developed an occlusion of the right common iliac artery at the end of the procedure which cleared completely after 24 h intraarterial streptokinase infu- sion. Before the procedure, the systolic pressure gradient across the stenosis ranged from 40 to 1 I0 mm Hg, with a mean of 60 mm Hg. After PTAA this gradient dropped to below l0 mm Hg in all except 2 patients. In one of the two it dropped from 50 to 20 mm Hg, but despite this residual gradient, good femoral pulses appeared. The other patient devel- oped common iliac artery occlusion at the end of the procedure which was immediately treated by intraarterial thrombolysis. Because of the occlusion,
no pressure could be measured distal to the PFA site. The post-PTAA angiographic picture showed dilatation of the stenosis in all patients. Almost all showed intimal tearing and irregularity.
C~mplk'atiop~s
In addition to the already-mentioned patient with iliac artery thrombosis, which was successfully treated by thrombolysis, we encountered one distal embolus that resolved after a course of systemic heparin infusion. There were two instances of small inguinal hematoma formation, which did not require treatment. No other complications occurred in the entire se,-ies.
Long-term Paten('y Rate (Table 3)
Three patients were lost to follow-up after their dis- charge from the hospital and 1 other developed reste- nosis within a month and underwent bypass surgery. Follow-up of the other 24 patients ranged from 1 to 9 years with a mean of 4.5 years. In 20 patients the treated aortic lesion remained patent without any additional procedure for the following periods of time: 6-9 years in 7 patients, t -6 years in the other 13. Complete disappearance of claudication occur- red in 15; in 3 others, rest pain was relieved and mild claudication (category 1) remained. In the 2 other patients, severe claudication (category 3) was con-

40 B. Morag et al.: Percutaneous Transluminal Aortic Angioplasty
Fig. 3. A 62-year-old male patient with rest pain. A Eccentric distal aortic stenosis with additiona} left common iliac artery stenosis. The pressure gradient v, as 100 mm Hg bilaterally. B Double balloon dilatations with a longer 10-cm balloon w:,s used on the left side. C Postdilatation angiogram. Pressure gradient was reduced to 5 mm Hg alter peripheral vasodilatation.
verted to mild (category 1). All 5 patients who re- tained mild claudication had associated peripheral disease. In the 15 totally asymptomat ie patients, ankle-arm indices rose by an average of 0.30 to above 1.00. In the 5 patients with associated distal disease, normal femoral pulses were present in all, but their ankle-arm indices averaged 0.8 as com- pared with 0.6 before the procedure.
Repeat angioplasty was performed in 4 patients during the follow-up period. One developed a second site of stenosis in the aorta 3 years after the initial dilatation and the original treated stenosis remained dilated (Fig. 1). Since the second PTAA 5 years ago the patient has remained symptom free. Restenosis at the site of the original dilatation occurred in the other 3 patients 2 years after the original angioplasty. These 3 patients had all undergone dilatation of aor- tic bifurcation lesions and the restenosis occurred on one side of the bifurcation in each of them. They were all redilated and have since remained patent and symp tom free with good femoral pulses for 2, 4, and 6 years, respectively.
Discussion
Prior to the introduction of percutaneous angi- oplasty, the only t reatment available to patients with abdominal aortic stenoses wets surgical bypass graft- ing or endar te rec tomy. PTAA now offers a safe and effective alternative to surgery. For angioplasty to be acceptable , its results should be at least as good as surgery and its morbidity and mortality lower.
According to many repor ted series, the initial patency rate after aor to-femoral bypass surgery ranges from 90 to 100% [22-26]. Long-term follow- up shows patency rates of 80-90% at 5 years and 65-80% after 10 years [22-26]. The perioperat ive mortality of surgery ranges f rom I to 5%, with mor- bidity reaching 27% in some series [24-26]. Late complications related to these grafts (except occlu- sion) have been reported in 2 .4-6 .8% of patients [26-29]. Patients requiring repeat surgery have even higher morbidity and mortal i ty rates [30].
Angioplasty as an al ternat ive or complement to surgery is ah'eady a well-established procedure in treating peripheral vascular disease [31]. PTAA of the infrarenal aorta has only recent ly been reported in significant numbers [13-17]. The fear of aortic rupture has not been substant ia ted, and initial suc- cess rates of about 95% have been reported in most series [7-17, 32]. The morbidi ty and mortality have been low, with most compl ica t ions being treatable by conservat ive means only. Aort ic rupture has been

B. Morag et al.: Percutaneous Transluminal Aortic Angioplasty
"Fable 3. Long-term results by life ruble analysis of 32 angioplasty procedures in 28 patients
4t
Interval No. End of No. Interval (months} patients follow-up tailed patency rate
Cumulative Standard patency rate error (%1
0-1 32 3 I 0.96 96.88 3.08 1 - 12 28 5 1 I).96 93.42 4,51
1 "~_-~.'4 ""~_ 4 1 0.95 89.17 5.98 24-36 17 2 2 0.88 78.68 8.74 36-48 13 3 -- 1 78.68 8.74 48-60 l0 2 -- 1 78.68 8.74 6(I-72 8 3 -- I 78.68 8.74 72-84 5 2 -- I 78.68 8.74 84-96 3 2 -- I 78.68 8.74 96-108 1 I -- 1 78.68 8.74
reported in only I patient in whom a calcified plaque causing stenosis was dilated using 2 x 8-ram bal- loons simultaneously [32]. The present series, which encountered no serious complications requiring sur- gery, confirms the low complication rate. Only 1 patient needed bypass surgery due to early recur- rence and the operation was not compromised by the previous PTAA.
Our series differs slightly from many others irt that we had a higher proportion of male patients. The clinical features of the female patients were in keeping with other reported series in that they were young, all were heavy smokers, and their aortic di- ameters tended to be smaller [12, 13, 16, 18-20]. The male patients were older and more prone to associated distal arterial disease. The results of the aortic dilatation were equally good in both male and female patients, with those who had localized aortic lesions becoming completely asymptomatic. Some of those with peripheral disease became asymptom- atic and the others improved significantly. Addi- tional treatment for distal disease was instituted when necessary, but details of these treatments have not been included in this report.
In our institution, all patients with suspected aor- tic or lilac disease have initial diagnostic arteriogra- phy performed via the translumbar or occasionally by the axillary route. This allows clear and unim- peded visualization of the aortic bifurcation, and the best approach to the angioplasty procedure is planned on the basis of the angiographic findings. This method did not raise our complication rate and we still prefer translumbar aortography as the initial diagnostic procedure of choice in elective peripheral vascular assessment.
All patients with bifurcation lesions were treated by the double balloon technique via bilateral femoral punctures. This allowed for various combinations of balloon sizes, and the simultaneous inflation pre- vented inadvertent compromise of the contralateral
side, In aortic lesions either a single large balloon or double "kiss ing" balloons were used. The size of the balloon selected was always 1 or 2 mm less than the aortic diameter above and below the lesion in order to avoid overstretching of the wall.
In assessing the efficacy of dilatation during the procedure, we relied mainly on the pressure gradient measurements. Ideally, complete disappearance of" the gradient should be achieved, but a residual gradi- ent of up to 10 mm Hg in the presence of good femoral pulses was regarded as acceptable.
The long-term follow-up oF out" series of patients is highly encouraging. Even those patients who re- turned with restenoses were successfully treated by repeat angioplasty. The high patency rate of the whole group averaging 4.5 years, with the longest of 9 years, suggests that the results of PTAA will equal or surpass those achieved for lilac artery dilatation. Restenosis developing after PTAA can be treated by repeat dilatation without adding to the complication rate such as occurs in repeat surgery. Another ad- vantage of PTAA over surgery in males is the avoid- ante of neurogenic impotence that may result after surgical dissection in the region of the distal aorta and its bifurcation [33-35].
In conclusion, we believe that because of the good short- and long-term results as well as its safety, availability, and cost-effectiveness, PTAA should be the initial procedure of choice in all in- stances of distal aortic stenoses. The role ofintravas- cular stents in these patients is still to be assessed. In view of the good results with PTAA, including repeat procedures, stents may be reserved for se- lected, complicated procedures.
R e f e r e n c e s
1. Kadir S. White R1, Kaufman SL, Barth KIt, Williams GM. Burdick JF. O'Maru CS. Smith GW, Stonesifer GL. Ernst CB, Minkin SL cl983) l,ong-term results of aorto lilac angi- oplasty. Surgery 94: 10-14

42 B. Morag et al.: Percutaneous Translumimfl Aortic Angioplasty
2. Gallino A. MaMer F. Probst P, Nachbur B (1984) Percutane- pus transluminal angioplasty of the arteries of the lower limbs: A 5 year follow-up. Circulation 70:619-623
3. Borozan PG, Schuler JJ, Spigos DG, Hanigan DP ~1985~ Long-term hemodynamic evaluation of lower extremity per- cutaneous transluminal angioplasty. J Vasc Surg 2:785-793
4, Johnston KW, Rae M. Hogg-Joahnston SA, Colapinto RF. Walker PM, Baird RJ, Sniderman KW, Kalman P(1987i Five- year results of a prospective study of percutaneous translumi- nal angioplasty. Ann Surg 206:403-413
5. Heuriksen LO. Jorgensen BO. Holstein PE. Karle A. Sager P (1988) Percutaneous transluminal angioplasty of infrarenal arteries in intermittent claudication. Acta Chir Scand 154:573-576
6. Stokes KR, Strunk HM. Campbell DR, Gibbons GW. Wheeler HG. Clouse ME I1990) Five-year restdts of lilac femoropopliteal diabetic patients. Radiology 174:977-982
7. Grollman JH. Del Vicario M. Mittal AK (1980) Percutaneous transluminal abdominal aortic angioplasty. A JR 134: 1053-1054
8. Velasques G. Castaneda-Zuniga W, Formanek A. Zollikofer C, Barreto A. Nicoloff D, Amplatz K. Sullivan A 1t980) Nonsurgical aortoplasty in Leriche syndrome. Radiology 134:359-360
9. Teglmeyer C, Keltum C. Kron IL. Memzer RM Jr ~1985) Percutaneous transluminal angioplasty in the region of the aorlic bitkncation. Radiology 157:661-665
10. Charlebois N, Saint-Georges G, Hudon G (1986) Percuhme- ous transhuninal :mgiopla'q:v c,f the lower abdonlina] ;~ortzl. A JR 1,16:369-37t
I 1. Morag g. Rubins;.ein Z, Kessler A, Schneidcrman J. l,evink- kopt M, Bass A (1987) Percutuneous tran,,luminal angioplasly of the distal abdominal aorta and it,; bifurcation. Cardio,-asc lntervent Radiol 10:I"9-133
t2. Heeney D. Books';ein J. Daniel,, E. \Varmalh M. Horn J. Ro'a Icy W 119831 Transtuminal angioplast,,, ot" the abdominal aorta. Report of 6 women. Radiology 148:81-83
13. Belli AM, Hemingway AP. Curnberland DC, Welsh CL! 1989) Percutaneous transluminal angioplast_v of the diMal abdomi hal aorta, Eur J Vase Surg 3:..I'49-453
14 "fakes WF. Kumpe DA, Brown SB. Parker SH. Lattes RG, Cook PS. Haas DK.Gibson MD. Hopper KD. Reed MD.Cox iq E, Bourne EE. Stiffen DJ (1989) Percutaneous translumimd aortic angioplasty: Techniques and results. Radiology 172:965-970
15. Tadavarthy AK. Sullivan WA Jr. Nicoloff D. Castaneda- Zuniga WR, Hunter DW, Amplatz K (1989) Aorta balloon angioplasty: 9-year ft.'allow-up. Radiology 170: 1039-1041
16. Odurny A, Colapinto RF, Sniderman KW. Johnston W (1989) Percutaneous transluminal angioplasty of abdominal aortic stenoses. Cardiovasc lntervent Radiol 12:I-6
17. Ravimandulam K, Rap VRK, Kumar S. Supra AK. Joseph S. L nni M, Rap AS (I 9901 Obstruction of the infraremtl portion of the abdominal aorta: Results of lreatment with butloon angioplasty. A JR 156:1257-1260
18. Constantino M J. Smith RB I l l . Perdue GD (1979) Segmental aortic occlusion. Arch Surg 114:317-318
19. Delaurentis DA. Friedmann P, Nolt'erth CC Jr. Wilson A. Naide D (1978) Atheroscle,osis and the hypoplastic aortic system. Surgery 83:27-37
20. Cronenwett JL, GareR ME (1983) Arteriographic measure- ment of the abdominal aorta, iliac and fen(oral arteries in women with atherosclerotic occlusive disease. Radiology 148:389-392
21. Rutherford RB, Flanigan DP. Gupta SK. Johnston KW. Kar- mody A. Whittemore AD. Baker JD, Ernst CB (1986) Sug- gested standards for reports dealing with lower extremity ischemia. J Vasc Surg 4:80-94
22. SzHagyi DE. Elliot JP, Smith RF. Rcddy D, McPharlin M I1986) A thirty-year survey of the reconstructive surgical treatment of aortoitiac occlusive disease. J Vasc Surg 3:421-436
23. Crawt\'~rd ES. Bomberger RA. Gtaeser DH. Saleh SA, Rus- sell WL (19811 Aorto-iliac occlusive disease: Factors influ- encing survival and function follovr reconstructive opera- tion over a 25-year period. Surgery 90:t055-1067
24. Nevelsteen ,'\, Say R. Daenen W. Boel A. Stalpaert G (1980) Aortofemoral grafting: Factors influencing late results. Sur- gery 88:642-653
25. Brev. ster DC. Darling RC (197,'4/Optimal methods of aorto- iltac reconstruction. Surgery 84:739-748
26. Poulias GE, Polemis L. Skoutas B {1985} Bilateral aorto- femoral bypass in the presence of aorto-iliac occlusive dis- ease :rod Iaclors determining results. J Curdiovusc Surg 26:527-538
27. Champion MC, Sul!ivan SN, Coles 1C, Ooldbach M, Watson WC 11982! Aortoenteric fistuh,,: Incidence. presentation, rec- ognition and management. Ann Surg 195:31.1-317
2H. Levy MJ. Todd DE. Liilehci CW. Varco P,L 11965) Aortico- inte,,lin,d fistulas fol lowing surgery of the aorla. Stug Oynecol Ohstet [ 20:992-996
29. Yaeger RA. McConnell DB, Sa~,aki TM, Vetto RM (1985) Aortic and peripheral pro,,'hctic graft infection: Dift)rential management and causes of mortality. Am J Surg 150:36-43
30. Bre,a ster DC. MeierGH. Darling RC'. Moncure AC. l,aMura- gtia GM, Abbott WM 1t9871 Reoperation for aortofemoral graft limb occlusion: Optimal methods and long-term result:,. J Var, c Surg 5:363-374
31. Tegtmeyer CJ. Hartwell GD. Selby JB, Robertson R. Kron IJ. Tribble C(i !1991~ Results and complications of angi- oplasty in aortoiliac disease. Circulation 83 (suppl 1): 1-53-60
32. Bcrger T. Sorensen R. Konrad J (1986) Aortic rupture: A complication of transluminal angioplasty. A JR 146:373-374
33. Sabri S. Cotton LT ( 1971 ) Sexual function following aortoiliac reconstruction. Lancet 2:1218-1219
34. DePalma RG, Levin SB. Fe/dman S t1978~ Preserwuion of erectile function after aortoiliac recon,,,truction. Arch Surg 113:958-962
35. Miles JR. Miles DG. Johnson G 11982~ Aottoiliac operations and sexual dysfunction. Arch Surg 117:1177-1181
Copyright © 2022 FDOKUMEN




















