Percutaneous endoscopic gastrostomy—to push or pullA prospective randomized trial
6
0016-5107/86/3204-0253$02.00 GASTROINTESTINAL ENDOSCOPY Copyright © 1986 by the American Society for Gastrointestinal Endoscopy Percutaneous endoscopic gastrostomy-to push or pull A prospective randomized trial Reed B. Hogan, MD, Daniel C. DeMarco, MD J. Kent Hamilton, MD, Charles O. Walker, MD Dan E. Polter, MD Dallas, Texas A prospective randomized study was undertaken to evaluate the Ponsky- Gauderer and Sachs-Vine types of gastrostomy kits. The techniques, complications, morbidity, and mortality with each type of device are compared. Both devices are found to compare favorably to the traditional surgically placed gastrostomy. (Gastrointest Endosc 1986;32:253-258) The feeding gastrostomy is a common operation which can provide a route for nutritional support in a large variety of clinical situations. Since the introduc- tion of percutaneous endoscopic gastrostomy (PEG) in 1980 the procedure has gained acceptance as a safe technique for establishing a tube gastrostomy. There are currently several established techniques for per- cutaneous gastrostomy insertion. The purpose ofthis study was to prospectively eval- uate two methods of PEG, to determine the morbidity and perioperative mortality associated with the pro- cedures, and to compare these results with previously reported surgical and nonsurgical methods. We report our experience in a prospective randomized trial uti- lizing the Ponsky-Gauderer and Sachs-Vine types of gastrostomies. Both gastrostomy devices evaluated were provided in their commercial packages by their manufacturer. Prior to undertaking this prospective study, profi- ciency at percutaneous gastrostomy insertion had been achieved by performing the procedure in over 50 patients. All patients and their families were informed of the nature of the study and risks involved. All were offered the option of a standard surgical gastrostomy. The protocol was approved by the Institutional Re- view Board for Human Protection of Baylor Univer- sity Medical Center. Received June 24, 1985. For revision July 17, 1985. Accepted October 3,1985. From the Department ofGastroenterology, Baylor University Medical Center, Dallas, Texas. Reprint requests: Reed B. Hogan, MD, Gas- trointestinal Associates PA, 500 B East Woodrow Wilson Avenue, Jackson, Mississippi 39216. VOLUME 32, NO.4, 1986 MATERIALS AND METHODS Forty patients were randomized to have percutaneous insertion of a gastrostomy tube under endoscopic control. The underlying disease which necessitated gastrostomy in- sertion most frequently was neurologic dysfunction with impaired deglutition (Table 1). All procedures were per- formed in the endoscopy unit except one which was per- formed in the Intensive Care Unit. There were no outpatient procedures. All procedures were done with sedation using intravenous diazepam or meperidine. The patients were randomized to receive either the Pon- sky-Gauderer or Sachs-Vine type gastrostomy. One patient was randomized to receive a Sachs-Vine type gastrostomy, but due to a tight postirradiation esophageal stricture this could not be placed. In this patient an alternative type gastrostomy was placed. One other patient was not random- ized due to a tight, high esophageal stricture. TECHNIQUE Pull-string Ponsky-Gauderer type gastrostomy (Fig. 1A) This method has been well described. The patient is endoscoped in the supine position. Panendoscopy is rapidly performed, and the appropriate position for the gastrostomy is determined. Using transmitted light with the stomach inflated, the point of maximum intensity on the anterior abdominal wall is palpated with a fingertip or probe and observed through the endoscope. The site is usually superior to the angularis on the anterior wall of the stomach. The site is then infiltrated with 1% lidocaine using a 25-gauge, 11/ 2 -inch needle, which is advanced into the stomach until air can be aspirated. This needle is observed through the endoscope ensuring correct placement. A small %-cm cuta- neous incision is made, and blunt dissection is done through 253
Transcript of Percutaneous endoscopic gastrostomy—to push or pullA prospective randomized trial

0016-5107/86/3204-0253$02.00GASTROINTESTINAL ENDOSCOPYCopyright © 1986 by the American Society for Gastrointestinal Endoscopy
Percutaneous endoscopic gastrostomy-topush or pull
A prospective randomized trial
Reed B. Hogan, MD, Daniel C. DeMarco, MDJ. Kent Hamilton, MD, Charles O. Walker, MD
Dan E. Polter, MD
Dallas, Texas
A prospective randomized study was undertaken to evaluate the PonskyGauderer and Sachs-Vine types of gastrostomy kits. The techniques,complications, morbidity, and mortality with each type of device are compared.Both devices are found to compare favorably to the traditional surgically placedgastrostomy. (Gastrointest Endosc 1986;32:253-258)
The feeding gastrostomy is a common operationwhich can provide a route for nutritional support in alarge variety of clinical situations. Since the introduction of percutaneous endoscopic gastrostomy (PEG)in 1980 the procedure has gained acceptance as a safetechnique for establishing a tube gastrostomy. Thereare currently several established techniques for percutaneous gastrostomy insertion.
The purpose ofthis study was to prospectively evaluate two methods of PEG, to determine the morbidityand perioperative mortality associated with the procedures, and to compare these results with previouslyreported surgical and nonsurgical methods. We reportour experience in a prospective randomized trial utilizing the Ponsky-Gauderer and Sachs-Vine types ofgastrostomies. Both gastrostomy devices evaluatedwere provided in their commercial packages by theirmanufacturer.
Prior to undertaking this prospective study, proficiency at percutaneous gastrostomy insertion hadbeen achieved by performing the procedure in over 50patients. All patients and their families were informedof the nature of the study and risks involved. All wereoffered the option of a standard surgical gastrostomy.The protocol was approved by the Institutional Review Board for Human Protection of Baylor University Medical Center.
Received June 24, 1985. For revision July 17, 1985. Accepted October3,1985.From the Department ofGastroenterology, Baylor University MedicalCenter, Dallas, Texas. Reprint requests: Reed B. Hogan, MD, Gastrointestinal Associates PA, 500 B East Woodrow Wilson Avenue,Jackson, Mississippi 39216.
VOLUME 32, NO.4, 1986
MATERIALS AND METHODS
Forty patients were randomized to have percutaneousinsertion of a gastrostomy tube under endoscopic control.The underlying disease which necessitated gastrostomy insertion most frequently was neurologic dysfunction withimpaired deglutition (Table 1). All procedures were performed in the endoscopy unit except one which was performed in the Intensive Care Unit. There were no outpatientprocedures. All procedures were done with sedation usingintravenous diazepam or meperidine.
The patients were randomized to receive either the Ponsky-Gauderer or Sachs-Vine type gastrostomy. One patientwas randomized to receive a Sachs-Vine type gastrostomy,but due to a tight postirradiation esophageal stricture thiscould not be placed. In this patient an alternative typegastrostomy was placed. One other patient was not randomized due to a tight, high esophageal stricture.
TECHNIQUE
Pull-string Ponsky-Gauderer type gastrostomy (Fig. 1A)
This method has been well described. The patient isendoscoped in the supine position. Panendoscopy is rapidlyperformed, and the appropriate position for the gastrostomyis determined. Using transmitted light with the stomachinflated, the point of maximum intensity on the anteriorabdominal wall is palpated with a fingertip or probe andobserved through the endoscope. The site is usually superiorto the angularis on the anterior wall of the stomach. Thesite is then infiltrated with 1% lidocaine using a 25-gauge,11/2-inch needle, which is advanced into the stomach untilair can be aspirated. This needle is observed through theendoscope ensuring correct placement. A small %-cm cutaneous incision is made, and blunt dissection is done through
253

Table 1.Indications for gastrostomy in 40 patients
Indication
Cortical or brainstem infarctCancer cachexiaAmyotrophic lateral sclerosisNeurologic traumaParkinsonismRecurrent/aspirationOrganic brain syndromeMeningitisSevere rheumatoid arthritis
Patients
2343222211
changes were done by one of the team members. Tube exitsites were cleaned daily with hydrogen peroxide and dressedwith povidone-iodine ointment. The gastrostomy tubes wereplaced to dependent drainage immediately following theprocedure. Feedings were undertaken the morning followingtube placement if the abdominal examination was normaland bowel sounds were present. All feedings were initiatedwith half-strength Osmolite solution, usually 50 ml followedby 25 ml of water every 4 hours and advanced as rapidly astolerated. In all patients, the external retention device wasslightly loosened at approximately 1 week postinsertion toavoid pressure necrosis.
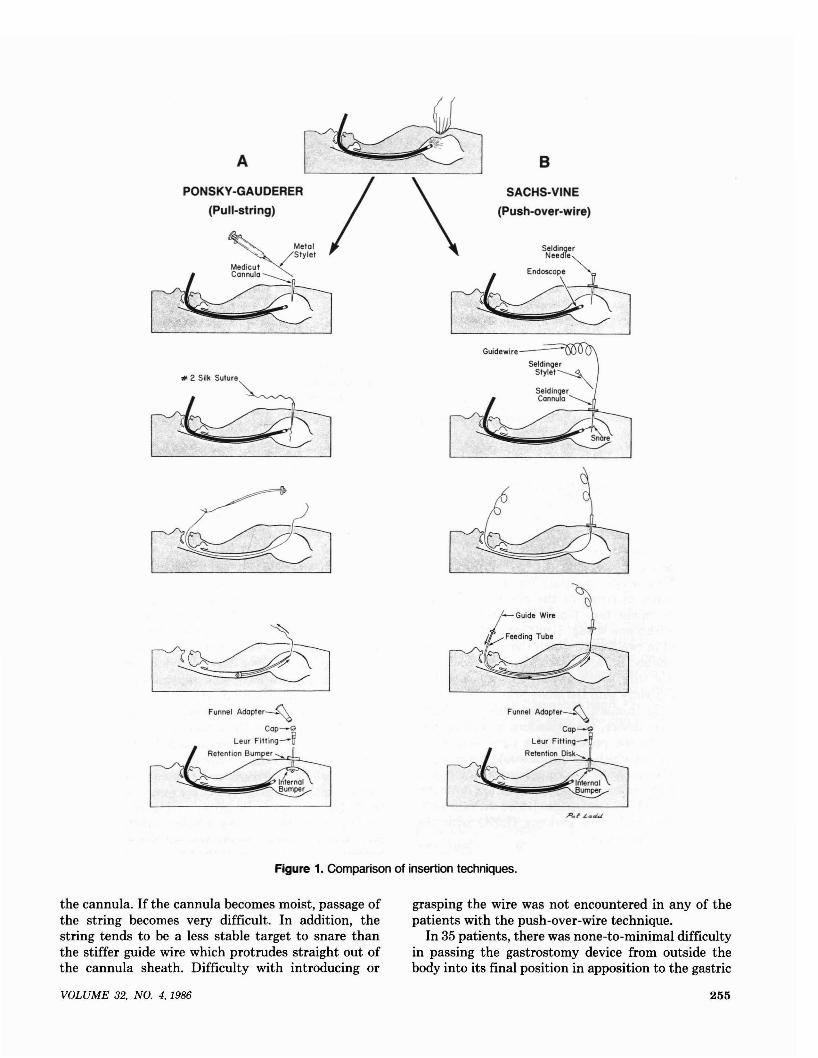
the cutaneous tissue to the fascia. Penetration of the peritoneum is avoided. A 16-gauge Medicut catheter is insertedthrough the incision and into the inflated stomach underdirect vision. The metal stylet is removed and a no. 2, 150cm silk suture is then passed through the catheter sheathinto the stomach. A snare, previously introduced throughthe endoscope and surrounding the catheter, is used to graspthe suture. Both the suture and endoscope are withdrawnthrough the patient's mouth. The 16 F mushroom tip catheter device is then tied to the string exiting the mouth andis generously lubricated. Traction is applied to the silk suturewhich exits the abdomen. The catheter is pulled downwardin a retrograde fashion into the oropharynx, the stomach,and out through the abdominal wall. The endoscope is thenreinserted as the head of the gastrostomy device is pulledfirm against the gastric wall under direct vision. The outerrubber bumper is then positioned externally to hold thestomach in apposition to the abdominal wall.
Push-over-wire Sachs-Vine gastrostomy (Fig. 18)
The initial portion of this technique is identical to theabove technique. Once the endoscope is in position and theappropriate site has been determined, a small incision ismade in the abdominal wall and dissection is performeddown to the fascia. A Seldinger needle is directed throughthe incision into the stomach under direct vision. The innerstylet is removed, and a 300-cm flexible tipped guide wire isinserted through the needle into the stomach. The guidewire is grasped with a snare device and pulled through themouth while removing the endoscope. The guide wire extends from the mouth, as shown in the diagram. It is important to have the wire taut. The feeding tube is pushed overthe guide wire into the stomach and out the puncture site.The advancing tapered portion of the feeding tube dilatesthe puncture site while pushing the stylet from the tract,allowing the tip to exit through the abdominal wall. Whenthe tip of the dilating device is exposed, it can be graspedand pulled until the catheter head is secure against thegastric wall. The guide wire is removed, and the endoscopeis reinserted to assure proper positioning of the innerbumper against the stomach wall. The feeding tube is secured with an external retention disk, which is sutured ortaped in place.
Postoperative management
After insertion of the percutaneous gastrostomy all patients were managed in an identical manner. The patientsreceived daily follow-up with wound checks. Dressing
254
Comparison of techniques
Several aspects of the procedure were evaluated with eachplacement. The overall duration of the procedure was recorded from the start of the initial endoscopy until the tubewas secured in place and reinsertion of the endoscope forvisualization had been completed. The insertion was evaluated on five major points: introducing the stylet into thestomach, grasping and withdrawing the string/wire, traversing the oropharynx to the stomach with the gastrostomydevice, pulling the gastrostomy head flush against the stomach wall, and overall difficulty with insertion. These fiveparameters were given a grade on a scale of 0 to 3 with 0being no difficulty, 1 = minimal difficulty, 2 = difficult, and3 = impossible. A grade of 3 in any of these categories meantthat the procedure could not be performed.
In the postinsertion period, the tubes were evaluated forany evidence of inflammation around the tube exit site. Thepatients were examined on a daily basis with the maximalamount of inflammation being graded on a scale of 0 to 5.The following scale was used: 0 = no inflammation, 1 = 1cm or less erythema, 2 = purulent drainage expressed fromexit site, 3 = spontaneous drainage, 4 = incision and debridement required, and 5 = incision and debridement requiredalong with tube removaL The patients were evaluated forclinical evidence of reflux or aspiration, and treatment wasinitiated when needed. The time required from insertionuntil the initial feeding and the time required to reachmaintenance feeding were also evaluated. The period of timein the hospital and prior to and after the percutaneousgastrostomy was recorded. Other complications were recorded, and patients who had their tubes removed were alsonoted. Thirty-day follow-up was obtained on all survivingpatients. Follow-up weights were not always obtainable.
RESULTS
Insertion techniques
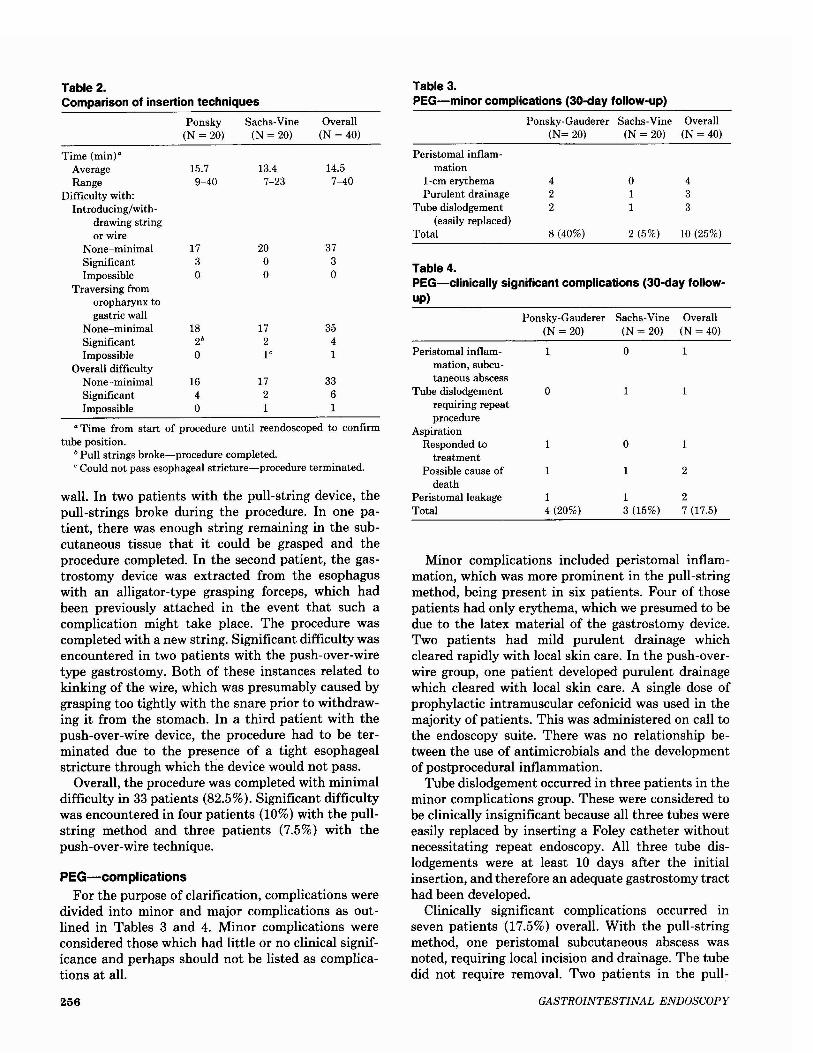
The comparison of insertion techniques is outlinedin Table 2. Forty patients were randomized-20 toeach group. The average time required was 14.5 min(range, 7 to 40 min). The pull-string method averaged15.7 min compared to the 13.4 min with the over-thewire methods. The difference was not significant. Nodifficulty was encountered with introducing or withdrawing the string or wire in 37 patients. In threepatients involving the pull-string method, significantdifficulty was encountered passing the suture through
GASTROINTESTINAL ENDOSCOPY
B
SACHS-VINE
(Push-over-wire)
A ~PONSKY-GAUDERER / \
(Pull-string)
Metal Seldinger/StYlet Needle""
~~
Funnel AdaPter_~
Cop-Q
Leur Fifting-W
Retention B./um....:..p_er~t;;::>.._
Funnel AdoPter_~
Cop-Q
Leur Fifting-W
Retention Disk......
Figure 1. Comparison of insertion techniques.
the cannula. If the cannula becomes moist, passage ofthe string becomes very difficult. In addition, thestring tends to be a less stable target to snare thanthe stiffer guide wire which protrudes straight out ofthe cannula sheath. Difficulty with introducing or
grasping the wire was not encountered in any of thepatients with the push-over-wire technique.
In 35 patients, there was none-to-minimal difficultyin passing the gastrostomy device from outside thebody into its final position in apposition to the gastric
VOLUME 32. NO.4, 1986 255
a Time from start of procedure until reendoscoped to confirmtube position.
b Pull strings broke-procedure completed., Could not pass esophageal stricture-procedure terminated.
PEG-complicationsFor the purpose of clarification, complications were
divided into minor and major complications as outlined in Tables 3 and 4. Minor complications wereconsidered those which had little or no clinical significance and perhaps should not be listed as complications at all.
wall. In two patients with the pull-string device, thepull-strings broke during the procedure. In one patient, there was enough string remaining in the subcutaneous tissue that it could be grasped and theprocedure completed. In the second patient, the gastrostomy device was extracted from the esophaguswith an alligator-type grasping forceps, which hadbeen previously attached in the event that such acomplication might take place. The procedure wascompleted with a new string. Significant difficulty wasencountered in two patients with the push-over-wiretype gastrostomy. Both of these instances related tokinking of the wire, which was presumably caused bygrasping too tightly with the snare prior to withdrawing it from the stomach. In a third patient with thepush-over-wire device, the procedure had to be terminated due to the presence of a tight esophagealstricture through which the device would not pass.
Overall, the procedure was completed with minimaldifficulty in 33 patients (82.5%). Significant difficultywas encountered in four patients (10%) with the pullstring method and three patients (7.5%) with thepush-over-wire technique.
18 17 352b 2 40 l' 1
16 17 334 2 60 1 1
2
27 (17.5)
1
1
1
Overall(N = 40)
o
o
1
1
13 (15%)
1
1
o
1
14 (20%)
Ponsky-Gauderer Sachs-Vine(N = 20) (N = 20)
Table 3.PEG-minor complications (30-day follow-up)
Ponsky-Gauderer Sachs-Vine Overall(N= 20) (N= 20) (N = 40)
Peristomal inflam-mation
l-cm erythema 4 0 4Purulent drainage 2 1 3
Tube dislodgement 2 1 3(easily replaced)
Total 8 (40%) 2 (5%) 10 (25%)
Peristomal inflammation, subcutaneous abscess
Tube dislodgementrequiring repeatprocedure
AspirationResponded to
treatmentPossible cause of
deathPeristomalleakageTotal
Table 4.PEG-clinically significant complications (30-day followup)
Minor complications included peristomal inflammation, which was more prominent in the pull-stringmethod, being present in six patients. Four of thosepatients had only erythema, which we presumed to bedue to the latex material of the gastrostomy device.Two patients had mild purulent drainage whichcleared rapidly with local skin care. In the push-overwire group, one patient developed purulent drainagewhich cleared with local skin care. A single dose ofprophylactic intramuscular cefonicid was used in themajority of patients. This was administered on call tothe endoscopy suite. There was no relationship between the use of antimicrobials and the developmentof postprocedural inflammation.
Tube dislodgement occurred in three patients in theminor complications group. These were considered tobe clinically insignificant because all three tubes wereeasily replaced by inserting a Foley catheter withoutnecessitating repeat endoscopy. All three tube dislodgements were at least 10 days after the initialinsertion, and therefore an adequate gastrostomy tracthad been developed.
Clinically significant complications occurred inseven patients (17.5%) overall. With the pull-stringmethod, one peristomal subcutaneous abscess wasnoted, requiring local incision and drainage. The tubedid not require removal. Two patients in the pull-
373o
14.57-40
Overall(N = 40)
20oo
13.47-23
Sachs-Vine(N = 20)
173o
15.79-40
Ponsky(N = 20)
Table 2.Comparison of insertion techniques
Time (min)"AverageRange
Difficulty with:Introducing/with
drawing stringor wire
None-minimalSignificantImpossible
Traversing fromoropharynx togastric wall
None-minimalSignificantImpossible
Overall difficultyNone-minimalSignificantImpossible
256 GASTROINTESTINAL ENDOSCOPY

string group had documented aspiration. One of theseresponded to conservative treatment. The second patient aspirated during the procedure and subsequentlyexpired 25 days postprocedure. The aspiration wasconsidered to be one of many factors that led to hisultimate demise. The fourth patient in the pull-stringgroup to have a clinically significant complicationdeveloped peristomal leakage approximately 1 weekafter insertion. This necessitated a larger tube placement.
In the push-over-wire technique group, three clinically significant complications were noted. One patient had tube dislodgement within 48 hours followingplacement. This did not result in clinically apparentperitonitis but did require a second procedure to replace the tube. An episode of aspiration occurred onthe fifth day postprocedure as an outpatient. Thepatient died the following day. The third patient inthis group developed peristomal leakage around thetube 1 week postinsertion which was managed withlocal wound care and insertion of a larger tube.
30-day mortality
Table 5 shows the overall 30-day mortality for the40 patients to be 15% (six patients). There were threedeaths in each group. Only one death was consideredto be procedure related, that being the aspirationwhich occurred at the time of tube placement in apatient undergoing a pull-string type of gastrostomy.The other aspiration-related death did not occur during the procedure but, as previously mentioned, 5 dayslater as an outpatient. The other deaths were notrelated to the gastrostomy and included progressionof underlying neoplasm, myocardial infarction, andsudden death for undocumented reason.
DISCUSSION
The feeding gastrostomy is a common operationwhich can provide a route for nutritional support in alarge variety of clinical situations. A number of studieshave confirmed substantial morbidity and mortalityrates which accompany the placement of a gastrostomy by traditional surgical methods. As outlined inTable 6 the operative gastrostomy has an overall
Table 5.3D-day mortality
Ponsky-Gauderer Sachs-Vine Overall(N = 20) (N = 20) (N= 40)
Procedure related I" 1b 2(aspiration)
Nonrelated 2 2 4Total 3 3 6 (15%)
" Aspiration at time of procedure in intensive care setting; deathon day 25 postprocedure.
b Aspiration 5 days postprocedure; death on day 6.
VOLUME 32, NO.4, 1986
morbidity in the range of 6% to 75%.1-6 In severalseries the combined 30-day operative and hospitalmortality associated with the operative gastrostomyranges from 5% to 37% (Table 6).1-5
Since the introduction in 1980 of the PEG, theprocedure has gained acceptance as a safe techniquefor establishing a tube gastrostomy. The medical literature currently contains over 450 case reports documenting the successful placement of the tube gastrostomies in this manner (Table 7). Complicationsfrom the procedure have been in the range of 9% to15% and include localized infections, gastric leakage,aspiration, bowel perforation, local tissue necrosis,and peritonitis. The 30-day mortality is not well reported, but when given it has been 9% to 24%.7-12
Analysis of our data indicates little difference in theoverall ease of insertion with the two techniques.Problems occur mainly with the device which deliversthe gastrostomy tube through the upper gastrointestinal tract, i.e., the string or wire. The breaking of twostrings with the Ponsky-Gauderer type device madethese two procedures difficult. The routine use of aretrieval device, an alligator toothed forceps attachedto the oral end of the tube, makes retrieval easy ifstring breakage occurs. Difficulties encountered withthe Sachs-Vine tubes other than the esophageal stricture were due to a kinking of the snared guide wire,which made advancement of the device over the wiredifficult to initiate and added significant time to twoprocedures.
The complications noted in this study were followedin a prospective manner with careful follow-up. Forthis reason, minor complications were recorded in alarge number of patients (25%). We did not considerthese to be significant since they had no bearing onthe clinical outcome. It is interesting to note that thelatex tube with the pull-string device more frequentlywas involved in peristomal inflammation compared tothe Silastic tube, which is known to cause less localinflammation. On the other hand, the Silastic tube ismuch stiffer than the latex tube and is therefore more
Table 6.Complications of surgical gastrostomy
Total Perioperative 30-daypatients morbidity mortality
Heimbach la 1970b 83 60 (72%) 52 (37%)Mequidand 1979 46 3 (6%) 17 (37%)
Williams2
Pomerantz et al.3 1980 106 9 (9%) 5 (5%)Swartzendruber 1982 121 55 (45%) 13 (11 %)
and Laws·Wasiljew et al.5 1982 147 23 (16%) 9 (6%)Wilkinson and 1982 67 31 (46%) 20 (30%)
Pickelman6
" Superior numbers refer to references.b Includes jejunostomy procedures.
257

Table 7.Complications of PEG
Total Perioperative 30-daypatients morbidity mortality
Strodel et al.7a 1983 43 5 (12%) 4 (9%)Ponsky et al.B 1983 150 15 (10%) b
Larson et al.9 1983 23 2 (10%) - b
Deutsch lO 1984 23 2 (10%) 2 (10%)Russell et al. ll 1984 28 3 (9%) 4 (14%)Cohen et al. 12 1984 207 33 (15%) b
Baylor 1985< 40 7 (17.5%) 6 (15%)
a Superior numbers refer to references.b No procedure-related mortality; 30-day mortality not given.<Present study-clinically significant complications.
difficult to bandage and slightly less comfortable forthe patient. Although both the manufacturers andphysicians will argue in favor of their favorite type ofmaterial, we could find no clinically significant advantage to either tube.
Significant complications were seen in seven patients (18%) overall. There was no significant difference in the two techniques. The most worrisome complication was aspiration which contributed to thecause of death in two patients. No relationship couldbe found between the patient's clinical condition andthe risk for aspiration in our study. Routinely we takemeasures to prevent this occurrence by initiating ourfeedings with small boluses which are gradually increased over several days. We also elevate the head ofthe bed and diligently check for gastric residuals priorto each feeding. If there are more than lOD ml presentin the stomach, that feeding is held.
As outlined in Table 6, the previously reportedsurgical gastrostomy literature has a complication rateof 6% to 72% and a 3D-day mortality rate of 5% to37%. It is hard to draw a true comparison from thesestudies to our patient population since they are doneat different institutions, involve different patient populations, and presumably have differing criteria forsignificant (i.e., recordable) complications. The 3Dday mortality of 15% in our study compares favorablywith the surgical literature; however, patient selectioncould presumably alter these figures. We tend to havepatients referred who are poor surgical risks and therefore would be expected to have a high morbidity andmortality.
As shown in Table 7, the recent literature on percutaneous endoscopic gastrostomy placement by various authors shows a complication rate of 9% to 15%which is slightly lower than the 17.5% significantcomplication rate seen in our study. This likely is areflection of the prospective nature of our study andthe care taken to record all complications. The 3D-day
258
mortality is given in only three of the summarizedstudies. The other three studies state no procedurerelated mortality, but the 3D-day mortality is notgiven. Our 15% mortality is similar to that recordedin prior reports. It is of interest that many of thesereports suggest that the 3D-day mortality rate is lowerwith PEG than with the surgically placed gastrostomy.This could imply a reduction in procedure-relatedmortality associated with surgically placed gastrostomies or be due to the performance of endoscopicgastrostomies on a less severely ill patient population.The nonprocedure-related mortality rate should beapproximately the same if the patient populations aresimilar.
In summary, in our patient population no significant difference could be found between the push-overwire versus the pull-string methods of percutaneousgastrostomy placement. Significant difficulty is frequently encountered (17.5%) in these procedures.Rarely does this result in a procedure failure. Theperioperative complication rates and 3D-day mortalityrates compare favorably with those reported in thesurgical literature.
ACKNOWLEDGMENTS
The authors wish to thank Janie Francis and LoriMorrow for their help in preparing the manuscript.
REFERENCES
1. Heimbach DM. Surgical feeding procedures in patients withneurological disorders. Ann Surg 1970;172:311.
2. Mequid MM, Williams LF. The use of gastrostomy to correctmalnutrition. Surg Gynecol Obstet 1979;149:27-32.
3. Pomerantz MA, Salomon J, Dunn R. Permanent gastrostomyas a solution to some nutritional problems in the elderly. JAmGeriatric Soc 1980;28:104-7.
4. Swartzendruber FD, Laws HL. The superior feeding gastrostomy. Am Surg 1982;48:276-8.
5. Wasiljew BK, Ujiki GT, Beal JM. Feeding gastrostomy: complications and mortality. Am J Surg 1982;143:194-5.
6. Wilkinson WA, Pickelman J. Feeding gastrostomy: a reappraisal. Am Surg 1982;48:273-5.
7. Strodel WE, Eckhauser FE, Lemmer JH, Knol JA, Dent TL.Endoscopic percutaneous gastrostomy. Contemp Surg1983;23:17-23.
8. Ponsky JL, Gauderer MWL, Stellato TA. Percutaneous endoscopic gastrostomy. Arch Surg 1983;118:913-4.
9. Larson DE, Fleming CR, Ott BJ, Schroeder KW. Percutaneousendoscopic gastrostomy, simplified access for enteral nutrition.Mayo Clin Proc 1983;58:103-7.
10. Deutsch SF. Surgical and endoscopic percutaneous gastrostomyfeeding tubes. Clin Consult Nutr Support 1984;4:1-7.
11. Russell TR, Brotman M, Norris F. Percutaneous gastrostomy,a new simplified and cost effective technique. Am J Surg1984;148:132-7.
12. Cohen NN, Plumer PA, Ockrymiek SB, Shah N. Percutaneousendoscopic gastrostomy: a pragmatic approach to nutrition inpatients unable to swallow (abstract). Gastrointest Endosc1983;29:181.
GASTROINTESTINAL ENDOSCOPY