
DAVID J. WELLENSTEIN OFFICE-BASED ENDOSCOPIC ...
203
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. https://hdl.handle.net/2066/226629 Please be advised that this information was generated on 2022-02-05 and may be subject to change.
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of DAVID J. WELLENSTEIN OFFICE-BASED ENDOSCOPIC ...
PDF hosted at the Radboud Repository of the Radboud University
Nijmegen
The following full text is a publisher's version.
For additional information about this publication click this link.
https://hdl.handle.net/2066/226629
Please be advised that this information was generated on 2022-02-05 and may be subject to
change.
OFFICE-B
ASED
END
OSCO
PIC SURG
ERY IN LA
RYNG
OLO
GY A
ND
HEA
D A
ND
NECK
ON
COLO
GY
DAV
ID J. W
ELLENSTEIN DAVID J. WELLENSTEIN
OFFICE-BASED ENDOSCOPIC SURGERY IN LARYNGOLOGY AND HEAD AND NECK ONCOLOGY
IMPROVING QUALITY OF CARE AND EFFICIENCY THROUGH INNOVATIVE TECHNIQUES

OFFICE-B
ASED
END
OSCO
PIC SURG
ERY IN LA
RYNG
OLO
GY A
ND
HEA
D A
ND
NECK
ON
COLO
GY
DAV
ID J. W
ELLENSTEIN DAVID J. WELLENSTEIN
OFFICE-BASED ENDOSCOPIC SURGERY IN LARYNGOLOGY AND HEAD AND NECK ONCOLOGY
IMPROVING QUALITY OF CARE AND EFFICIENCY THROUGH INNOVATIVE TECHNIQUES

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 1PDF page: 1PDF page: 1PDF page: 1
OFFICE-BASED ENDOSCOPIC SURGERY IN LARYNGOLOGY AND HEAD AND NECK
ONCOLOGYIMPROVING QUALITY OF CARE AND EFFICIENCY
THROUGH INNOVATIVE TECHNIQUES
David J. Wellenstein
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 2PDF page: 2PDF page: 2PDF page: 2
Design by Bregje Jaspers, ProefschriftOntwerp.nlPrinted by Ipskamp drukkers
Printing of this thesis was financially supported by: Pentax Medical, Soluvos Medical, Lumenis, Medical Disposables Store, Laservision, Mylan, Atos Medical, ALK and Radboud university medical center/Radboud University Nijmegen
Office-based endoscopic surgery in laryngology and head and neck oncologyImproving quality of care and efficiency through innovative techniquesDavid Jonathan WellensteinISBN XXXXCopyright © David J. Wellenstein, 2020

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 3PDF page: 3PDF page: 3PDF page: 3
OFFICE-BASED ENDOSCOPIC SURGERY IN LARYNGOLOGY AND HEAD AND NECK
ONCOLOGYIMPROVING QUALITY OF CARE AND EFFICIENCY
THROUGH INNOVATIVE TECHNIQUES
Proefschrift ter verkrijging van de graad van doctor aan de Radboud Universiteit Nijmegen
op gezag van de rector magnificus prof. dr. J.H.J.M. van Krieken,volgens besluit van het college van decanen
in het openbaar te verdedigen op 11 december 2020om 12:30 uur precies
doorDavid Jonathan Wellenstein
geboren op 26 juni 1988te Leidschendam
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 4PDF page: 4PDF page: 4PDF page: 4
Promoteren:Prof. dr. H.A.M. MarresProf. dr. R.P. Takes
Copromotor:Dr. G.B. van den Broek
ManuscriptcommissieProf. dr. P.D. SiersemaProf. dr. R.J. Baatenburg de Jong (Erasmus MC)Dr. H.F.M. van der Heijden

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 5PDF page: 5PDF page: 5PDF page: 5

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 6PDF page: 6PDF page: 6PDF page: 6
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 7PDF page: 7PDF page: 7PDF page: 7
TABLE OF CONTENTS
Chapter 1 General introduction
Chapter 2 Office-based procedures for the diagnosis and treatment of laryngeal pathology
Chapter 3 Office-based procedures for the diagnosis and treatment of esophageal pathology
Chapter 4 Topical anesthesia for endoscopic office-based procedures of the upper aerodigestive tract
Chapter 5 Safety of flexible endoscopic biopsy of the pharynx and larynx under topical anesthesia
Chapter 6 Office-based CO2 laser surgery for benign and premalignant laryngeal lesions
Chapter 7 Cost analysis of office-based transnasal esophagoscopy
Chapter 8 General discussion
Chapter 9 Appendix 1 and 2
Chapter 10 Summary
Chapter 11 Summary in Dutch
Chapter 12 Acknowledgements
Chapter 13 Curriculum Vitae
Chapter 14 List of publications
9
21
51
75
101
115
129
145
155
167
175
183
189
193
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 8PDF page: 8PDF page: 8PDF page: 8

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 9PDF page: 9PDF page: 9PDF page: 9
CHAPTER 1General introduction

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 10PDF page: 10PDF page: 10PDF page: 10
Chapter 1
10

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 11PDF page: 11PDF page: 11PDF page: 11
General introduction
11
1The fi rst published data about diagnostic and therapeutic offi ce-based procedures in laryngology and head and neck oncology dates back to over more than 120 years(1). During the 20th and 21st century, there have been many changes in health care perspective and necessities. The improvement of endoscopic and digital techniques are in line with these changes, and allow for innovative, less invasive, and cost reducing surgical procedures for patients with laryngeal and head and neck (oncological) lesions. But which of these offi ce-based endoscopic procedures can be useful to incorporate in clinical practice? And how can they contribute to these needed changes in health care?
OFFICE-BASED PROCEDURES
Offi ce-based procedures are diagnostic or therapeutic surgical procedures performed under topical anesthesia, usually in the outpatient clinic, instead of the operating room under general anesthesia. Although the theory of offi ce-based procedures in laryngology and head and neck oncology is known for more than a century, the practice in its current form (i.e. via digital fl exible transnasal endoscopy, usually with working channel) has just been reported on during the last two decades(2, 3).
Before this digital revolution, detection of lesions in the pharynx and larynx was usually performed in the outpatient clinic with a fi beroptic fl exible laryngoscope (see Appendix for a more detailed description). Image quality was poor, and the capacity to store images was lacking. Furthermore, it was not possible to perform endoscopic diagnostic and therapeutic procedures in the outpatient clinic, thus procedures under general anesthesia were the only option.
Figure 1. Transnasal laryngoscope
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 12PDF page: 12PDF page: 12PDF page: 12
Chapter 1
12
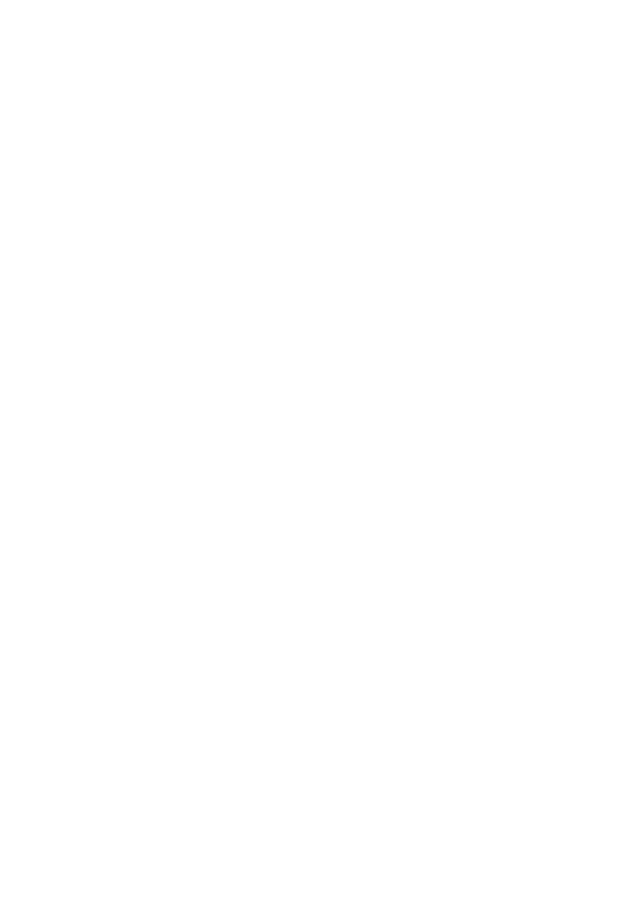
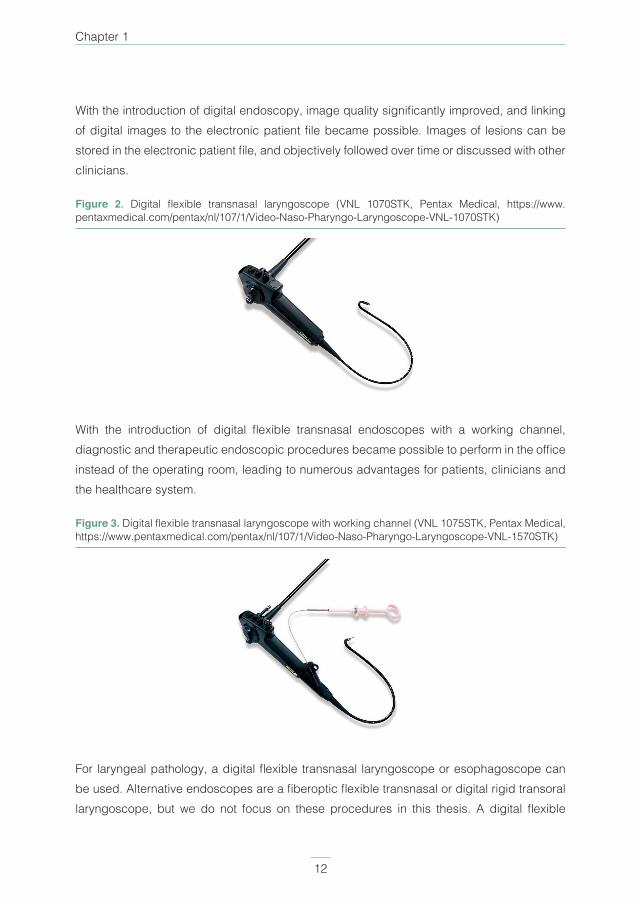
With the introduction of digital endoscopy, image quality significantly improved, and linking of digital images to the electronic patient file became possible. Images of lesions can be stored in the electronic patient file, and objectively followed over time or discussed with other clinicians.
Figure 2. Digital flexible transnasal laryngoscope (VNL 1070STK, Pentax Medical, https://www.pentaxmedical.com/pentax/nl/107/1/Video-Naso-Pharyngo-Laryngoscope-VNL-1070STK)
With the introduction of digital flexible transnasal endoscopes with a working channel, diagnostic and therapeutic endoscopic procedures became possible to perform in the office instead of the operating room, leading to numerous advantages for patients, clinicians and the healthcare system.
Figure 3. Digital flexible transnasal laryngoscope with working channel (VNL 1075STK, Pentax Medical, https://www.pentaxmedical.com/pentax/nl/107/1/Video-Naso-Pharyngo-Laryngoscope-VNL-1570STK)
For laryngeal pathology, a digital flexible transnasal laryngoscope or esophagoscope can be used. Alternative endoscopes are a fiberoptic flexible transnasal or digital rigid transoral laryngoscope, but we do not focus on these procedures in this thesis. A digital flexible

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 13PDF page: 13PDF page: 13PDF page: 13
General introduction
13
1transnasal laryngoscope is available with (distal diameter 4.8 mm) or without (distal diameter 3.0 – 3.5 mm) working channel(4), and both have different advantages and indications. Since a laryngoscope with working channel is shorter (working length 300 vs. 600 mm) and has a less wide diameter (distal diameter 4.9 vs. 5.1 mm) compared to a transnasal esophagoscope(4), this endoscope is easier to handle for clinicians and presumably less uncomfortable for the patient. When a working channel is incorporated in the laryngoscope, it is possible to perform suction in order to increase visualization on a tumor (e.g. in case of abundant saliva or tumor necrosis). Furthermore, diagnostic and therapeutic instrumentation such as flexible biopsy forceps, laser fiber or injection needle can be passed through the working channel. The transnasal esophagoscope is always equipped with a working channel and has the advantage of being able to inflate and perform suction, although not at the same time. The possibility of inflation gives an advantage when inspecting the hypopharynx, and is essential for the esophagus since peristalsis causes the esophagus to collapse.
A VIEW ON THE CURRENT HEALTH CARE SYSTEM Although it is not possible to summarize the developments in health care during the last decades in a single paragraph, some important factors which can be related to office-based procedures are outlined in this paragraph. Historically, (academic) hospitals pursue several goals, such as patient care, education, and research. Recently, improving value for patients is an additional intention in healthcare(5). Value-based healthcare is developed to improve patient centered care, and simultaneously reduce the unsustainable rising costs in healthcare (e.g. due to an aging population and rise in available medical technology). The current vision that health care should be organized around the patient and his or her pathway, and patient related outcomes should be measured instead of former outcome measures, is well adapted(5). With increasing expenses, reaching almost €100 billion in The Netherlands in 2017, the quest for cost saving procedures is ongoing(6). New technologies such as office-based endoscopic procedures have the possibility to considerably change common practice, and can also play a role in patient’s needs. These needs can be different for an individual or patient category, and are usually determined by the patient related variables such as medical condition(5). Anatomical location of a suspected lesion (e.g. anterior commissure of the vocal cord), patient factors (e.g. comorbidity, limited neck extension or dental status) or patient preference may require varying diagnostic or therapeutic approaches. This is where office-based procedures can add to personalized healthcare.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 14PDF page: 14PDF page: 14PDF page: 14
Chapter 1
14
Presumably, patients are worried during the diagnostic tract; they want to know their definitive diagnosis as soon as possible. When the necessary facilities are at hand, office-based procedures can be rapidly performed, leading to decreasing time to diagnosis and treatment(7). Furthermore, in head and neck oncological patients, severe comorbidity could restrict them from general anesthesia. In this patient category, office-based procedures could be their only surgical treatment option.
For clinicians, an important factor when performing new procedures, is feasibility and safety. Thus, studies on feasibility and safety, combined with detailed procedural description, could convince clinicians to start performing office-based endoscopic procedures. With the possibility of performing these procedures, a new set of diagnostic and therapeutic possibilities can be offered to the patient. By performing several procedures in the outpatient clinic, waiting lists for the operating room can be reduced.
This is where office-based procedures become interesting from a healthcare perspective. Since general anesthesia or sedation is redundant in office-based treatments, costs for medication (i.e. general anesthesia), medical staff (e.g. anesthesiologist or operating assistant) and overhead (e.g. the operating room or day admission at the ward) can be reduced.
Although technological innovation starts with investments, in the end value can be increased and costs can be reduced. In healthcare the benefits of technological innovations need to be proven by clinical studies too. Are these procedures feasible? Is the new innovation safe to use in patients? What are the benefits for patients? Will the new technology reduce the overall costs? To answer these questions for office-based endoscopic procedures in laryngology and head and neck oncology, we conducted the literature and clinical studies published in this thesis.
GOALS AND OUTLINE OF THIS THESIS
Several authors have extensively investigated one out of the available office-based procedures, but to our knowledge, an integrated and comprehensive overview on all existing procedures is lacking. The goal of this thesis is to: 1) Identify which office-based procedures, using a digital flexible transnasal endoscope, are available for patients with benign and malignant laryngopharyngeal lesions. By summarizing the current knowledge on office-based procedures in three systematic reviews of literature, missing knowledge on
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 15PDF page: 15PDF page: 15PDF page: 15
General introduction
15
1all available procedures has been identified. 2) To identify the most valuable office-based procedures and factors, for a rapid introduction in daily practice of a large head and neck oncology clinic. Three clinical studies are performed to contribute to improving healthcare for this patient group.
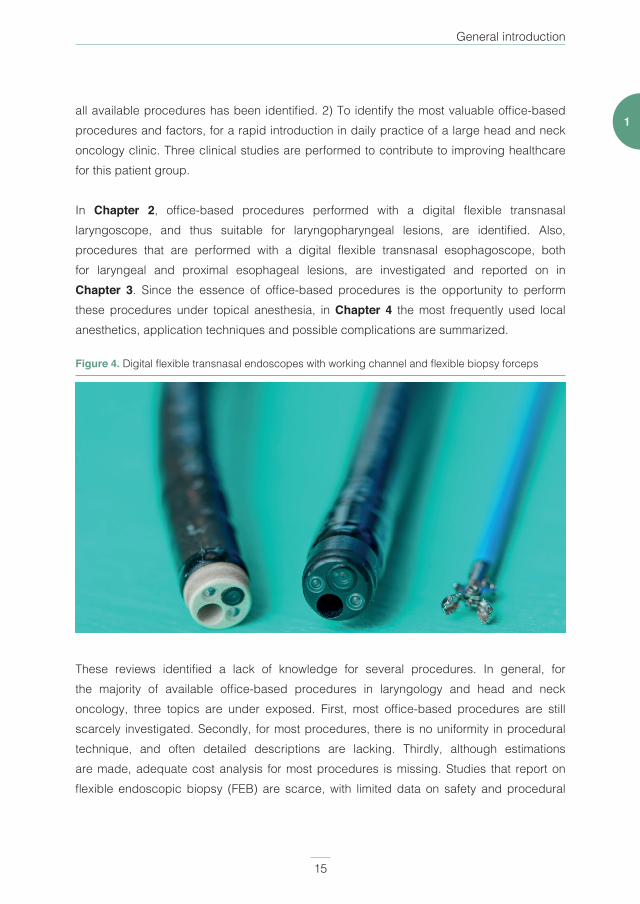
In Chapter 2, office-based procedures performed with a digital flexible transnasal laryngoscope, and thus suitable for laryngopharyngeal lesions, are identified. Also, procedures that are performed with a digital flexible transnasal esophagoscope, both for laryngeal and proximal esophageal lesions, are investigated and reported on in Chapter 3. Since the essence of office-based procedures is the opportunity to perform these procedures under topical anesthesia, in Chapter 4 the most frequently used local anesthetics, application techniques and possible complications are summarized.
Figure 4. Digital flexible transnasal endoscopes with working channel and flexible biopsy forceps
These reviews identified a lack of knowledge for several procedures. In general, for the majority of available office-based procedures in laryngology and head and neck oncology, three topics are under exposed. First, most office-based procedures are still scarcely investigated. Secondly, for most procedures, there is no uniformity in procedural technique, and often detailed descriptions are lacking. Thirdly, although estimations are made, adequate cost analysis for most procedures is missing. Studies that report on flexible endoscopic biopsy (FEB) are scarce, with limited data on safety and procedural
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 16PDF page: 16PDF page: 16PDF page: 16
Chapter 1
16
technique. Thus, a retrospective study which systematically and objectively evaluated complications that occurred during FEB is performed, and can be found in Chapter 5.
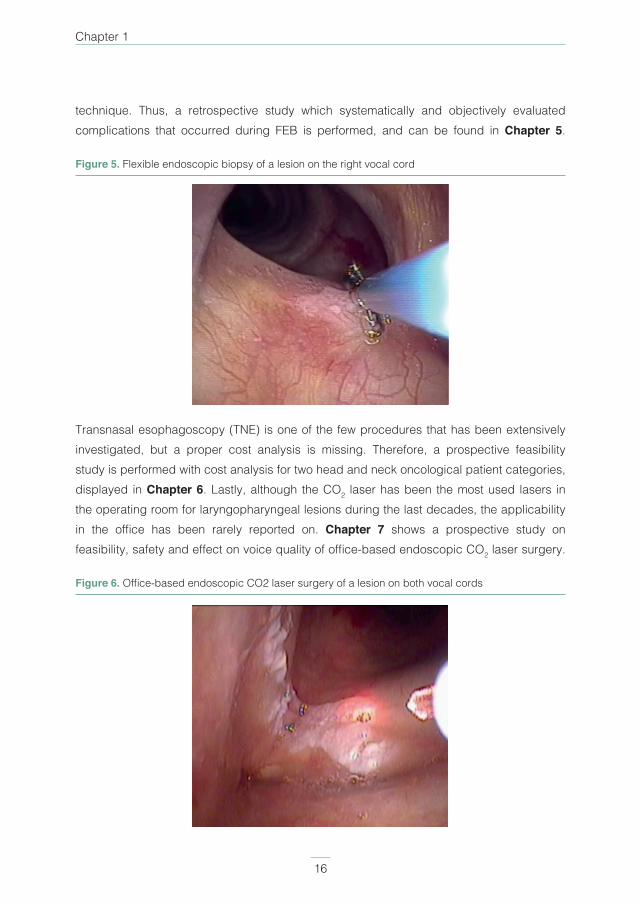
Figure 5. Flexible endoscopic biopsy of a lesion on the right vocal cord
Transnasal esophagoscopy (TNE) is one of the few procedures that has been extensively investigated, but a proper cost analysis is missing. Therefore, a prospective feasibility study is performed with cost analysis for two head and neck oncological patient categories, displayed in Chapter 6. Lastly, although the CO2 laser has been the most used lasers in the operating room for laryngopharyngeal lesions during the last decades, the applicability in the office has been rarely reported on. Chapter 7 shows a prospective study on feasibility, safety and effect on voice quality of office-based endoscopic CO2 laser surgery.
Figure 6. Office-based endoscopic CO2 laser surgery of a lesion on both vocal cords

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 17PDF page: 17PDF page: 17PDF page: 17
General introduction
17
1In Chapter 8, the results of the above mentioned studies are bundled and discussed.
In order to look forward to the future of office-based endoscopic surgery of the pharynx and larynx, we should also get an understanding of its history. Therefore, a summary on the historical development of laryngoscopy and office-based procedures are outlined in Chapter 9 as an appendix. Furthermore, in this chapter several developments in laryngoscopy are explained, to help the reader understand the distinction in terminology.
When reading this thesis, the reader should understand that this is merely the start for office-based procedures in laryngology and head and neck oncology. The goal of this thesis is to provide a solid overview on the current knowledge of office-based procedures, and to give further insight in several procedures that are less studied upon. This work should be interpreted as a guidance for clinicians who are interested in performing office-based procedures, and researchers who want to further investigate the possibilities of these procedures.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 18PDF page: 18PDF page: 18PDF page: 18
Chapter 1
18
REFERENCES
1. Kirstein A. Autoskopie des Larynx und der Trachea (Laryngoscopia directa, Euthyskopie,
Besichtigung ohne Spiegel). Arch Laryngol Rhinol. 1895;3:156-64.
2. Aviv JE, Takoudes TG, Ma G, Close LG. Office-based esophagoscopy: a preliminary report.
Otolaryngol Head Neck Surg. 2001;125(3):170-5.
3. Sato K, Umeno H, Nakashima T. Stroboscopic observation of vocal fold vibration with the
videoendoscope. Ann Otol Rhinol Laryngol. 2003;112(11):965-70.
4. www.pentaxmedical.com.
5. Porter ME. What Is Value in Health Care?. New Engl J Med. 2010;363(26):2477-81.
6. Central Bureau for Statistics (CBS) TN. 2017 [cited 2019 12-04]. Available from: https://opendata.
cbs.nl/statline/#/CBS/nl/dataset/84047NED/table?ts=1556102173859.
7. Schutte HW, Takes RP, Slootweg PJ, Arts M, Honings J, van den Hoogen FJA, et al. Digital
Video Laryngoscopy and Flexible Endoscopic Biopsies as an Alternative Diagnostic Workup
in Laryngopharyngeal Cancer: A Prospective Clinical Study. Ann Otol Rhinol Laryngol.
2018;127(11):770-6.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 19PDF page: 19PDF page: 19PDF page: 19
General introduction
19
1
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 20PDF page: 20PDF page: 20PDF page: 20
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 21PDF page: 21PDF page: 21PDF page: 21
Chapter 2Office-based procedures for the diagnosis
and treatment of laryngeal pathology
David J. Wellenstein, MD1, Henrieke W. Schutte, MD1, Robert P. Takes, MD PhD1, Jimmie Honings, MD PhD1, Henri A.M. Marres, MD PhD1, James A. Burns, MD PhD2,
Guido B. van den Broek, MD PhD1
1. Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands
2. Department of Surgery, Harvard Medical School; Center for Laryngeal Surgery and Voice
Rehabilitation, Massachusetts General Hospital, Boston, Massachusetts, USA
Journal of Voice. 2018 Jul;32(4):502-513.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 22PDF page: 22PDF page: 22PDF page: 22
Chapter 2
22
ABSTRACT
IntroductionSince the development of distal chip endoscopes with a working channel, diagnostic and therapeutic possibilities in the outpatient clinic in the management of laryngeal pathology have increased. Which of these office-based procedures are currently available, and their clinical indications and possible advantages, remains unclear.
Material and MethodsReview of literature on office-based procedures in laryngology and head and neck oncology.
ResultsFlexible endoscopic biopsy, vocal cord injection, and laser surgery are well-established office-based procedures that can be performed under topical anesthesia. These procedures demonstrate good patient tolerability and multiple advantages.
ConclusionOffice-based procedures under topical anesthesia are currently an established method in the management of laryngeal pathology. These procedures offer medical and economic advantages compared with operating room performed procedures. Furthermore, office based procedures enhance the speed and timing of the diagnostic and therapeutic process.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 23PDF page: 23PDF page: 23PDF page: 23
Office-based procedures for laryngeal pathology
23
2
INTRODUCTION
Following the introduction of topical anesthesia in the second half of the 19th century, office-based laryngeal surgery was performed using indirect vision (ie, mirror guided)(1-5). Endoscopic laryngoscopy began its revolution after the first flexible fiberoptic nasolaryngoscope became available in 1975. With a small outer diameter, the endoscope could be passed through the nasal cavity and direct inspection of the larynx through a lens was possible(6, 7). Since then, fiberoptic imaging has evolved to distal chip laryngoscopes with high-resolution image quality in the beginning of the 21st century, which can be monitored and recorded on a video screen. Furthermore, with the inclusion of a working channel in the endoscope, office-based procedures such as laser surgery and vocal cord injection can be performed in an office-based setting(8-12). The recent development of visual enhancement by color filtering, visualizing lesions with different wavelengths of light instead of white light, is another example of the ongoing evolution of laryngoscope techniques(13-19).
This literature review focuses on the current office-based diagnostic and therapeutic procedures available for the management of laryngeal pathology, which can be performed under topical anesthesia. Rosen et al. conducted an extensive review in 2009; since then more experience has been gained and new procedures have been investigated(11). The aim of the current review was to systematically identify the available articles on office-based procedures of the larynx and include them according to proper methodological standards. For each office-based procedure, clinical indications and possible advantages compared with the operative procedure are identified. Our goal is to provide a summary for each procedure, including an extensive procedural description, to use as a guideline when starting with office-based procedures for laryngeal pathology.
MATERIAL AND METHODS
A literature search was performed in the PubMed (MEDLINE), EMBASE and Cochrane Library databases. Keywords and Mesh terms include “ambulatory surgical procedures“, “ambulatory care“, “ambulatory surgery“, “outpatient“, “outpatient department“, “outpatient care“, “transnasal“ and “transoral“. These terms were combined with “pharynx“ and “larynx“. The published studies were included without a date limitation. Figure 1 shows the search strategy in a diagram.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 24PDF page: 24PDF page: 24PDF page: 24
Chapter 2
24
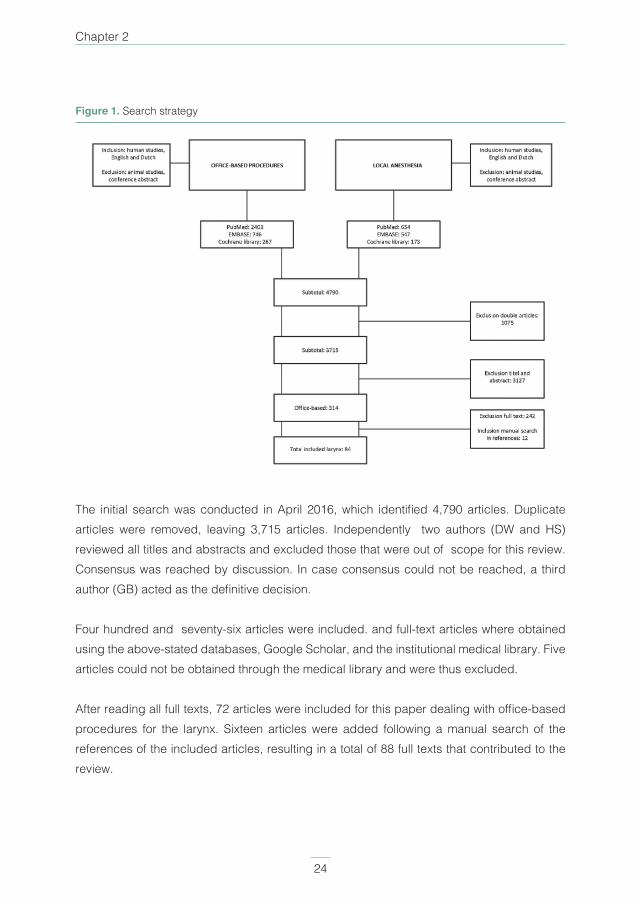
Figure 1. Search strategy
The initial search was conducted in April 2016, which identifi ed 4,790 articles. Duplicate articles were removed, leaving 3,715 articles. Independently two authors (DW and HS) reviewed all titles and abstracts and excluded those that were out of scope for this review. Consensus was reached by discussion. In case consensus could not be reached, a third author (GB) acted as the defi nitive decision.
Four hundred and seventy-six articles were included. and full-text articles where obtained using the above-stated databases, Google Scholar, and the institutional medical library. Five articles could not be obtained through the medical library and were thus excluded.
After reading all full texts, 72 articles were included for this paper dealing with offi ce-based procedures for the larynx. Sixteen articles were added following a manual search of the references of the included articles, resulting in a total of 88 full texts that contributed to the review.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 25PDF page: 25PDF page: 25PDF page: 25
Office-based procedures for laryngeal pathology
25
2
RESULTS
Flexible endoscopic biopsy (FEB)FEB of the larynx can be performed using two different routes. The transoral approach can be done under local anesthesia using an endoscope and curved laryngeal biopsy forceps and has been reported first in the early 1990s. The patient is asked to protrude the tongue, the endoscope is passed transnasally into the laryngopharynx to visualize the biopsy site, and biopsies can be obtained with the forceps through the mouth(9, 10, 20). This procedure can also be used for the removal of laryngeal lesions, such as vocal cord polyps or nodules(21-23). An approach that may be more convenient to reach the biopsy site is the transnasal approach, which became feasible with the development of distal chip laryngoscopes with a working channel. A 1.8-mm flexible biopsy forceps is passed via the working channel of the flexible endoscope, and biopsy or polypectomy can be performed(9, 10, 24, 25).
It has been stated that the use of FEB under local anesthesia should be reserved for patients who are cooperative (eg, minimal gag reflex and ability to sit still) or where general anesthesia poses a substantial health risk(9, 10). On the other hand, when anatomy is distorted due to treatment for head and neck carcinomas or the primary tumor itself, direct suspension microlaryngoscopy biopsies under general anesthesia can be difficult or risky to obtain compared with office-based biopsies(13). Table 1 displays a summary concerning the characteristics of FEB for the larynx.
Lippert et al reported on office-based upper airway biopsies. Twenty-four transoral and 92 transnasal biopsies were performed, and the authors concluded that the success of a biopsy was not significantly related to age, tumor site, tumor stage, or biopsy approach(26). Ninety-seven of the 116 biopsies could be histologically defined, and only nine had to be rebiopsied in the operating room for a definitive diagnosis. This resulted in a difference in time until the start of the treatment, which was 24.2 ± 13.9 days for office-based biopsy and 48.8 ± 49.4 days for operating room biopsy. Walter et al. compared esophagogastroduodenoscopy using a conventional transoral 8.8-mm endoscope (with or without sedation) with transnasal or transoral endoscopy using a 4.9-mm endoscope without sedation(24). Data from 300 procedures incorporating 1,335 biopsies were blindly evaluated by a pathologist; analysis showed no significant difference in the rate of definitive histological diagnose irrespective of the technique used. Cohen et al investigated office-based transnasal biopsies by performing 102 procedures, of which 96 (94.1%) successfully obtained adequate diagnostic tissue(27). Of the 62 patients who had benign pathology or carcinoma in situ, the authors performed
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 26PDF page: 26PDF page: 26PDF page: 26
Chapter 2
26
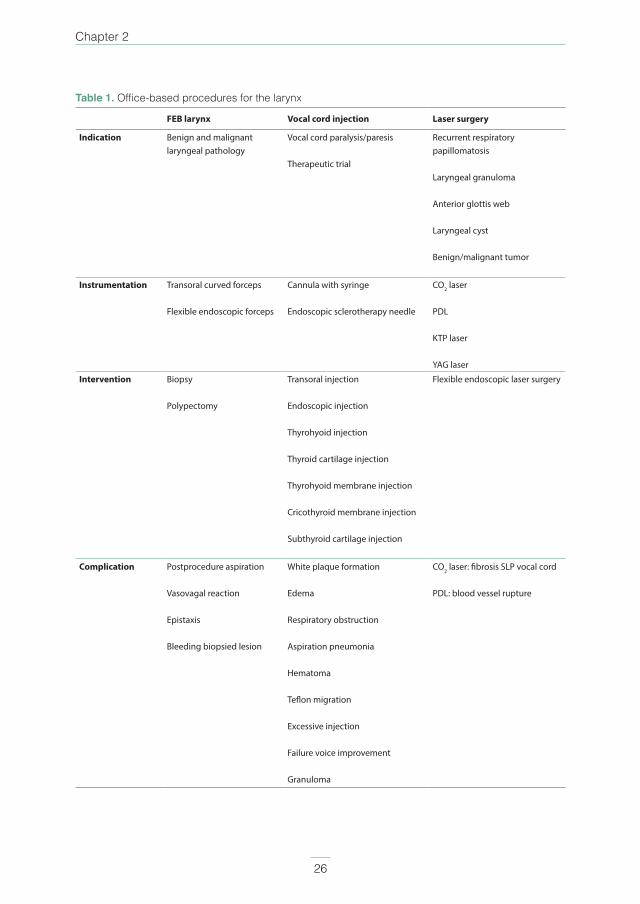
Table 1. Office-based procedures for the larynx
FEB larynx Vocal cord injection Laser surgery
Indication Benign and malignant laryngeal pathology
Vocal cord paralysis/paresis
Therapeutic trial
Recurrent respiratory papillomatosis
Laryngeal granuloma
Anterior glottis web
Laryngeal cyst
Benign/malignant tumor
Instrumentation Transoral curved forceps
Flexible endoscopic forceps
Cannula with syringe
Endoscopic sclerotherapy needle
CO2 laser
PDL
KTP laser
YAG laser
Intervention Biopsy
Polypectomy
Transoral injection
Endoscopic injection
Thyrohyoid injection
Thyroid cartilage injection
Thyrohyoid membrane injection
Cricothyroid membrane injection
Subthyroid cartilage injection
Flexible endoscopic laser surgery
Complication Postprocedure aspiration
Vasovagal reaction
Epistaxis
Bleeding biopsied lesion
White plaque formation
Edema
Respiratory obstruction
Aspiration pneumonia
Hematoma
Teflon migration
Excessive injection
Failure voice improvement
Granuloma
CO2 laser: fibrosis SLP vocal cord
PDL: blood vessel rupture
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 27PDF page: 27PDF page: 27PDF page: 27
Office-based procedures for laryngeal pathology
27
2
57 biopsies using direct microlaryngoscopy under general anesthesia. Using the general anesthetic biopsy results as the gold standard, a transnasal biopsy had a false-negative rate of 33% and a false-positive rate of 1%. The sensitivity of transnasal biopsy was 69.2%, and specificity was 96.1%. Both methods showed a fair agreement (k = 0.38). Zalvan et al performed 26 office-based biopsies and compared these with operating room biopsies in the same patients, demonstrating a concordance of 81%(28). Schindler et al reported on performing anterior glottic polyp removal using a forceps through the working channel of a laryngoscope in two patients with high anesthesia risk or a difficult anatomy(29). Both procedures were successfully executed, and the duration of the procedure, including the administration of the anesthesia, was 20-30 minutes. In 50 patients with vocal cord polyps, Wang et al compared office-based vocal cord polypectomy with the microlaryngoscopic removal of polyps(25). Prior to the in-office removal, a KTP laser was used to coagulate the vocal cord lesion. The only significant difference was a better self-reported VAS score for voice quality after 2 weeks in the in-office polypectomy group, although this significance disappeared after 6 weeks. No complications or significant sequelae occurred.
After a laryngeal FEB, patients should be advised not to eat or drink for 30-45 minutes because of the risk of aspiration due to the topical anesthetic(10). Complications that can occur include vasovagal reaction, postprocedure aspiration, self-limiting epistaxis or bleeding from the biopsied lesion(10, 27). Several studies confirm that patients experience minimal to no complications(13, 24, 26, 27, 30). Furthermore, Naidu et al. concluded that the costs of in-office biopsies are significantly lower compared with biopsies performed in the operating room, which were reported to be $2,053.91 versus $9,024.47 per patient, respectively, in their study(31).
Overall, most patients tolerate FEBs under local anesthesia well(26, 27). Office-based biopsy is equally effective in comparison with biopsies taken in the operating room, although a pitfall of office-based biopsy is that the specimens may be too superficial, and therefore might not be representative of deeper or submucosal tissue(31).
Vocal cord injectionIn 1911, the first unsedated transoral vocal cord injection for paralysis was performed by Brünings using paraffin. Seifert introduced the first percutaneous procedure in 1916 through the cricothyroid ligament. In 1955, Arnold reintroduced the transoral approach using direct laryngoscopy and a syringe with different substances without success but successfully performed the first Teflon (Ethicon Company of Sommerville, New Jersey, USA) injection in 1962. Common adverse effects of Teflon include airway obstruction due to overinjection and particle

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 28PDF page: 28PDF page: 28PDF page: 28
Chapter 2
28
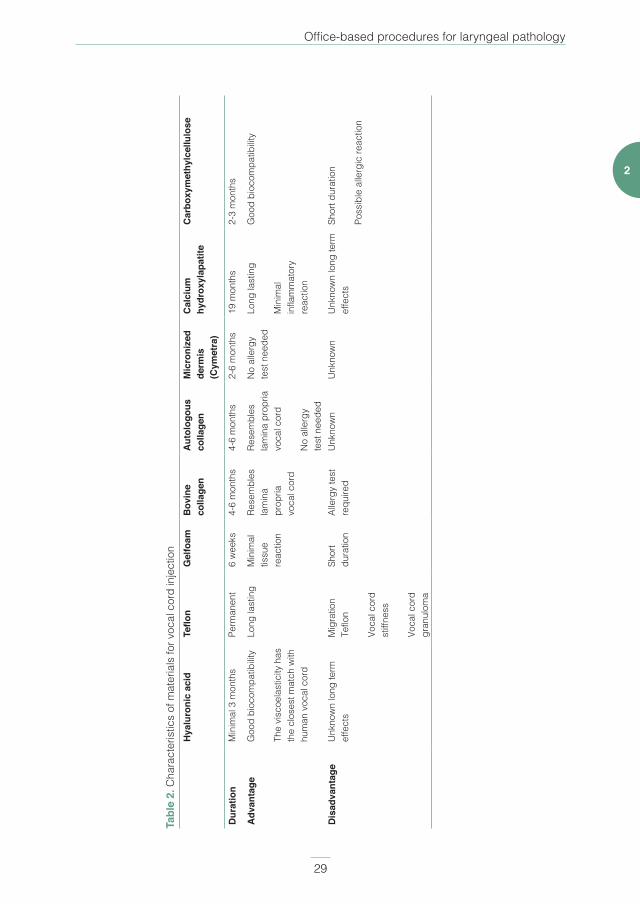
migration and granuloma formation due to foreign body reactions. Therefore, the search for new materials has been extensive, resulting in the reported use of silicone, gelfoam, autologous fat, corticosteroids, collagen, human micronized dermis, autologous fascia, hyaluronic acid, calcium hydroxylapatite, mitomycin C, and botulinum toxin (Botox, Allergan, Inc., Irvine, California, USA). Even the use of stem cells is currently investigated in animal studies(20, 32-47). Indications for vocal cord injection are listed in Table 1(20, 33-35, 37, 39-44, 46-57). The characteristics of most commonly used injectables are displayed in Table 2. Although it is likely that these characteristics are even more extensive, and to prevent loss of information, a detailed summary of these characteristics can be found in other studies(20, 35, 36, 38, 44, 49, 52-54, 56, 58-63). In the following paragraphs there will be a distinction between vocal cord injection as a therapy for vocal cord paresis or paralysis, referred to as augmentation, in contradistinction to vocal cord injection for pharmaceutical administration (ie, drug delivery).
AugmentationSeveral techniques can be used to perform vocal cord injection under topical anesthesia. Several authors described transoral injection needle under indirect vision using a laryngeal mirror(32, 49, 54-56). With the development of the flexible fiberoptic laryngoscope, the transoral injection can be performed under direct vision with the use of a transnasally inserted laryngoscope(33, 35, 40, 45, 57, 64-66). With the advent of flexible digital endoscopes with a working channel, it is now possible to pass a sclerotherapy needle through the working channel to perform vocal cord injection(37, 43, 54, 66-68). An alternative to the transoral or transnasal route is a percutaneous approach, where the thyroarytenoid muscle is injected with or without EMG guidance(54, 57, 60). Variations on the percutaneous approach under the direct vision of a laryngoscope are the thyrohyoid approach(38, 53, 66), through the thyroid cartilage(20, 50, 51, 54, 59, 65,
66), thyroidhyoid membrane (20, 39, 52), cricothyroid membrane(20, 34, 41, 44, 51, 53, 59, 65, 66, 69) or subthyroid cartilage(20, 58). Vocal cord injection can either be superficial (ie, subepithelial) or deep (eg, below the lamina propria). Superficial techniques are used to improve vibratory abnormalities and medial height. Indications for superficial injection include vocal cord scarring and lamina propria deficits(70, 71). Deep injections can be used in dysphonia, dysphagia due to vocal cord paresis or paralysis(50). Deep injections can be temporary using hyaluronic acid, collagen or carboxymethylcellulose. Long-lasting deep injections, in case of longstanding paralysis, may be accomplished with calcium hydroxylapatite(50). For patients with vocal cord paresis, temporary vocal cord augmentation can be used as a therapeutic trial to see whether medialization of the vocal cord results in voice quality improvement(72). Due to the possibility of performing vocal cord augmentation under topical anesthesia, this therapeutic trial can be used as a first step in voice rehabilitation.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 29PDF page: 29PDF page: 29PDF page: 29
Office-based procedures for laryngeal pathology
29
2Ta
ble
2. C
hara
cter
istic
s of
mat
eria
ls fo
r voc
al c
ord
inje
ctio
nH
yalu
roni
c ac
idTe
flon
Gel
foam
Bov
ine
colla
gen
Aut
olog
ous
colla
gen
Mic
roni
zed
derm
is
(Cym
etra
)
Cal
cium
hy
drox
ylap
atite
Car
boxy
met
hylc
ellu
lose
Dur
atio
nM
inim
al 3
mon
ths
Perm
anen
t6
wee
ks4-
6 m
onth
s4-
6 m
onth
s2-
6 m
onth
s19
mon
ths
2-3
mon
ths
Adv
anta
geG
ood
bioc
ompa
tibilit
y
The
visc
oela
stic
ity h
as
the
clos
est m
atch
with
hu
man
voc
al c
ord
Long
last
ing
Min
imal
tis
sue
reac
tion
Rese
mbl
es
lam
ina
prop
ria
voca
l cor
d
Rese
mbl
es
lam
ina
prop
ria
voca
l cor
d
No
alle
rgy
te
st n
eede
d
No
alle
rgy
test
nee
ded
Long
last
ing
Min
imal
in
flam
mat
ory
reac
tion
Goo
d bi
ocom
patib
ility
Dis
adva
ntag
eU
nkno
wn
long
term
ef
fect
sM
igra
tion
Teflo
n
Voca
l cor
d st
iffne
ss
Voca
l cor
d gr
anul
oma
Shor
t du
ratio
nAl
lerg
y te
st
requ
ired
Unk
now
nU
nkno
wn
Unk
now
n lo
ng te
rm
effe
cts
Shor
t dur
atio
n
Poss
ible
alle
rgic
reac
tion

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 30PDF page: 30PDF page: 30PDF page: 30
Chapter 2
30
Remacle et al stated that for collagen injection in glottic insufficiency, two injections should be placed at the posterior aspect and at the mid-vocal cord(47). The vocal cord should be overinjected by approximately 25% due to the soluble vehicle(46). Woo stated that specific materials should be injected into different locations in the vocal cord(20) Relative contraindications are posterior laryngeal gap, large interarytenoid defects, and poor pulmonary status. Small gaps of less than 2 mm have a better chance of success compared with larger glottal gaps. Kwon et al. agreed with this last statement advising the use of injection laryngoplasty only in cases with a mild to moderate laryngeal gap(44). Zeitler and Amin reported the advantages of the thyrohyoid approach compared with other percutaneous approaches(38). In their experience, this technique offers access to all areas of the larynx that are typically not accessible using the transcartilagenous or cricothyroid approaches. Furthermore, the needle enters the laryngeal lumen (versus submucosally in the percutaneous approach), allowing for better visualization and guidance, which ensures a more precise placement of the injectable material. For the cricothyroid and thyrohyoid approach, several authors report that directing the needle at a certain angle will result in a more precise and simpler procedure(39, 58). Kwon et al stated that by using the transcricothyroid approach, the injection material can be placed in the muscle space without violating the vocal ligament-lamina propria-epithelium complex(44). This is in contrast to the transoral or transthyrohyoid approach. Hoffman et al performed an experimental method for needle localization in the larynx in human cadavers by adding a light source to the injection needle(73). The lit tip of the needle can be seen through a flexible videolaryngoscope and thus aid in a more precise procedure.
Objective (videolaryngostroboscopic) and subjective (Voice Handicap Index) voice quality assessments are often improved following vocal cord injection augmentation(35, 39-41, 43-45, 48,
49, 51, 53, 55, 56, 64, 65, 67, 69, 71, 74, 75). Multiple studies reported procedural completion rates of more than 90%(34, 66, 74). Bové et al reported the costs of office-based vocal cord injection to be $500 compared with $2,500 for a performance in the operating room(48). Andrade Filho et al reported office-based costs between $1,200 and $1,386, whereas costs for vocal cord injection in the operating room were between $12,400 and $13,300(64).
Pharmaceutical administrationThis section will address other injection procedures, such as Botox, for spasmodic dysphonia or steroids for vocal cord nodules. For vocal cord nodules, Tateya et al performed steroid injection by injecting directly into the nodule(40). Woo performed office-based steroid injection in patients with recurrent granuloma of the vocal process and injected around
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 31PDF page: 31PDF page: 31PDF page: 31
Office-based procedures for laryngeal pathology
31
2
the lesion(20). A meta-analysis by Wang et al showed an effective improvement range between 82% and 98% for vocal cord injection for benign vocal cord lesions(75). Overall recurrence rates of 4%-31% were observed, and recurrence time ranged between 4 weeks and 9 months. In 12 patients with adductor spasmodic dysphonia, Rhew et al performed a Botox injection into the thyroarytenoid muscle using a flexible needle through the working channel of an endoscope. The site of injection was just lateral of the vocalis muscle(67). Miller et al similarly performed Botox injections into the thyroarytenoid muscle but used EMG guidance. The exact location of the injection is not mentioned(60). Several authors have used either or both medications effectively with no reported complications(40, 55, 60, 67).
Challenges to performing office-based vocal cord injection include the severely anxious patient, vasovagal reactions, an excessive gag reflex, intolerance of the laryngoscope, and anatomical variations(35, 39, 41, 50, 74). Possible short-term complications of vocal cord injection include white plaque formation, edema, respiratory obstruction, aspiration pneumonia, hematoma, Teflon migration and excessive injection(32, 34, 40, 41, 53, 74, 76, 77). Long-term complications include failure of voice improvement, scar formation, and recurrence(32,
36, 40-42, 65, 77-79). Severe acute edema can result in the necessity of a tracheostomy(34, 37). The majority of studies, however, report uneventful office-based vocal cord injections(35, 44, 56, 60, 68). Postprocedural care consists of voice rest for 1 to 3 days, although no uniform consensus exists.
Laser surgeryThere are several lasers available for office-based surgery of the upper aerodigestive tract. Each has advantages and disadvantages given the depth of penetration per unit of power, absorption in water, spectral absorption characteristics, mode of delivery, safety, and cost. It is important to note that while proper selection of a laser wavelength is important, of equal importance is selecting the appropriate power setting, focal length (or spot size), and time of exposure. Failure to consider all of these variables may result in suboptimal overall results including excessive fibrosis of the treated tissue.
Carbon dioxide (CO2) laserThe development of different types of lasers has led to an extensive use in laryngology over the last decade. The most commonly used laser in laryngeal surgery is the CO2 laser. This laser produces light with a wavelength of 10.6 µm and is well absorbed in water(10, 80). When the laser beam is focused, it functions as a hemostatic scalpel, and when it is defocused, it can also be used to ablate tissues. CO2 lasers are optimally used for lesions where the

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 32PDF page: 32PDF page: 32PDF page: 32
Chapter 2
32
superficial lamina propria (SLP) does not have to be spared because the heat produced can cause fibrosis. This is especially true for lesions located on the vocal cords. Zeitels and Burns stated that indications for office-based CO2 laser are treatment of most supraglottic lesions and in cases where the SLP has already been damaged by prior surgery or local invasion(81). Besides malignant tumors, the CO2 laser can be used for recurrent respiratory papillomatosis, granulomas, anterior glottic web, laryngeal cysts and amyloidosis(82). Possible complications include thermal damage, tissue necrosis, SLP scarring and anterior commissure web formation(83).
In the past, a significant limitation of the CO2 laser was the lack of a flexible delivery system and passage through the working channel of an endoscope. Since the development of photonic bandgap fibers, it is possible to deliver the CO2 energy through thin fibers and therefore through the working channel of a flexible laryngoscope or bronchoscope(10, 84, 85). Currently, there are several types of flexible CO2 laser fibers commercially available.
In two patients with recurrent respiratory papillomatosis, Koufman et al performed 10 procedures of in-office flexible CO2 laser with a laser setting between 8 and 17 W. No complications were reported about the safety of the technique(82).
Pulsed dye laser (PDL)The photoangiolytic lasers target hemoglobin and were originally used to treat dermatologic vascular lesions before being adapted for use in the larynx(86, 87). Photoangiolytic lasers can be used to treat recurrent respiratory papillomatosis, mucosal dysplasia, laryngeal keratosis, leukoplakia, early stage glottic carcinoma, ectasias, and hemorrhagic polyps (82,
88-93). An example of this type of laser is the 585-nm PDL, which has a wavelength close to an absorbance peak of oxyhemoglobin, namely 571-nm. The energy is delivered in pulses of 0.5 ms and reaches approximately 2 mm in depth(89, 91, 92). When used for angiolytic properties, the PDL causes no vaporizing of the SLP, and bilateral vocal cord disease can be treated with reduced risk of anterior glottic web formation. When used for vaporizing keratotic lesions, the penetration depth is deeper and possibly causes scarring of the SLP. The disadvantages of the PDL include the high cost, difficulty in excising exophytic lesions because of the lack of superficial penetration, and heating of extravasated blood during surgery and thus decreasing selectivity of laser energy delivery(81, 92). When a vessel ruptures, the laser cannot function due to difficulty in penetrating the excessive blood. Furthermore, in PDLs used in an office-based setting, the distance from the laser tip to the lesion cannot be calibrated which results in less precise surgery compared with laser surgery performed
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 33PDF page: 33PDF page: 33PDF page: 33
Office-based procedures for laryngeal pathology
33
2
in the operating room under general anesthesia(83, 92). To our knowledge, the PDL is currently not commercially available anymore.
Power settings for the PDL can vary, and no uniform protocol is agreed. Zeitels and Burns used 0.6 to 0.8 J per pulse(92). Koufman et al used different settings per lesion, which primarily differed in the given pulse rate(82). The median energy delivered for all lesions is 1.0 J, although the median number of pulses vary with 161 for papillomatosis, 113 for glottal leukoplakia or dysplasia, 119 for granuloma, and 94.5 for Reinke’s edema.
Zeitels et al performed an office-based PDL treatment of laryngeal dysplasia and papillomas under local anesthesia on 51 patients (82 procedures), of which 77 were completed and five aborted due to patient intolerance or inability to visualize the lesion(92). Sixty-eight cases were judged to have more than 50% regression on postoperative videolaryngoscopy. The remaining nine showed 25%-50% regression. Rees et al performed 328 PDL procedures in 131 unsedated patients using a TNE with a working channel(89). A total of 68% of the patients completed the questionnaire about discomfort with an average VAS score for discomfort of 2.6, which was more significant in the throat than the nose (VAS 2.4 versus 0.6, respectively). Seventy-five patients did not use any pain medication after the procedure. Of the 131 patients, 54 had undergone previous treatment in the operating room and 83% of them were more comfortable with an in-office PDL treatment because of time, cost, and comfort difference. The authors stated that the complication rate of the PDL is the same as for TNE, although specific results are lacking. Koufman et al performed 406 PDL procedures in 151 patients and had four complications, of which one was a vasovagal reaction and two were vocal cord hematomas, and in one patient the PDL fiber tip broke off, which was retrieved with cupped forceps(82). Koszewski et al performed 13 in-office laser treatments for Reinke’s edema with the PDL(94). Average energy delivered is 128 ± 75 J (range, 23-268 J), and no complications occurred. Voice quality significantly improved after laser surgery, phonatory frequency range increased, percent jitter decreased, and phonation threshold pressure decreased. Franco performed 28 PDL laser surgery treatments in eight patients with laryngeal keratosis with atypia, and in 16 used 20% aminolevulinic acid in the larynx as a photodynamic therapy(91). Eighteen of the 28 procedures were performed under local anesthesia using the transnasal route, and all patients showed regression between 10% and 100%, with six patients having more than 85% regression. No significant differences were seen for laser pulses, energy per pulse, and interval between procedures for the office-based procedure compared with the operating room procedure.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 34PDF page: 34PDF page: 34PDF page: 34
Chapter 2
34
Potassium-titanyl-phosphate (KTP) laserAnother type of photoangiolytic laser is the KTP laser, which operates on a wavelength of 532 nm, which lies closely to another absorbance peak of oxyhemoglobin (approximately 541 nm). The KTP laser offers pulsed energy through thin glass fibers (0.2-0.6 mm), therefore potentially making it suited to pass the work channel of the laryngoscope, and for a continuous wave mode for hemostatic cutting(83, 90, 95, 96). The diameter of the fiber is smaller than that required for the PDL, therefore causing potentially less damage to the working channel of the laryngoscope. For maximum protection of the working channel of the laryngoscope, a protective endosheath is available to cover the laser fiber. Furthermore, slower intravascular heating causes less vessel wall rupture and extravasation that is commonly observed in the use of the PDL(83, 90). The KTP laser is also less expensive than the PDL(83, 90). In contrary to the PDL, Mallur et al proposed a classification system to define the effect of KTP laser surgery on laryngeal tissues by varying in fiber to tissue distance(97).
As seen with the PDL, settings for the KTP laser also vary among authors. Zeitels et al performed 72 procedures of office-based KTP laser surgery in 48 patients with recurrent papillomatosis or keratosis with dysplasia(90). Laser parameters were set to a 15-ms pulse width and a 5.25-J per pulse maximum output. For the papillomatosis group(20 patients, 36 procedures), all procedures were completed. For the keratosis group (28 patients, 36 procedures), one lesion could not be visualized and one patient had glottic stenosis. In the keratosis group, 29 patients had information available for follow-up. Eighteen patients had 75%-100% disease regression, seven patients had 50%-75% regression, and four patients had 25%-50% regression. Mallur et al investigated the ideal KTP laser parameters for in-office benign vocal cord lesion resections in 47 patients(98). Mean energy delivered was 27.7 W and the pulse width was 27.5 ms. In all cases, a setting of two pulses per second was used. For each benign lesion the authors used different parameters, with vocal cord granulomas requiring the highest wattage and Reinke’s edema the lowest. In all lesions except polyps, a significant decrease in size was seen when pretreatment images were compared with 1-month posttreatment images. After 2 months all lesions were still smaller compared with preprocedural measurements. Sheu et al investigated the effect of the KTP laser on benign vocal cord lesions in 102 patients(99). Treatment had a significant effect on reducing the size of vocal cord lesions for all diagnoses at both initial and long-term follow-up. Furthermore, there was a statistically significant reduction in lesion size from short- to long-term follow-up for all lesions, although only in 33% of the cases were long-term follow-up data available. Wang et al performed vocal cord polypectomy by combining the KTP laser surgery with endoscopic removal of the polyp using forceps and compared this with the KTP laser only for treatment
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 35PDF page: 35PDF page: 35PDF page: 35
Office-based procedures for laryngeal pathology
35
2
outcomes and complications(100). Laser parameters were 6 -8 W and pulse width was 15-25 ms. The average duration was 15 minutes per procedure. Twenty patients with unilateral hemorrhagic vocal polyps underwent a KTP laser with polyp removal, and 16 only had KTP laser surgery. Mean phonation time in the KTP laser-assisted polypectomy group showed significant improvement after 2 and 6 weeks compared with no significant improvement in the KTP group after 2 weeks, but again significant improvement after 6 weeks. A similar pattern was seen in VHI scores. One case of vocal cord hematoma occurred. In 31 patients with vocal cord polyps, Sridharan et al performed KTP laser surgery(101). Laser settings ranged from 15-35 W with a pulse length of 20-30 ms, and the total energy delivered varied between 13 and 272 J (mean 88.3 J). The VHI significantly decreased after laser treatment, but acoustic analysis did not significantly improve. Koszewski et al performed 12 in-office laser treatments for Reinke’s edema with the KTP laser(94). Average energy delivered was 126 ± 63 J (range, 47-246 J). There were no complications reported. Voice quality significantly improved after laser surgery, phonatory frequency range increased, percent jitter decreased, and phonation threshold pressure decreased. Hirano et al. performed KTP laser surgery in patients with vocal cord granulomas and reported a 40% recurrence rate after laser surgery(102).
Xie et al conducted a systematic review on KTP laser use for office-based laryngeal surgery under topical anesthesia(103). No systematic reviews on this topic were available, and only eight case series were found with a total of 243 KTP procedures. No studies compared the KTP laser with other lasers for efficacy. There is no evidence that KTP laser surgery is less safe compared with other modalities.
Yttrium-aluminum-garnet (YAG) laserThe YAG laser is a diode laser that operates with a continuous wave beam, which is mostly absorbed by melanin and hemoglobin. Different diodes can be used on the laser, such as thulium (1930-2040 nm), neodymium (1064 nm), and erbium (2940 nm). The YAG laser has the same cutting properties as the CO2 laser, and functions when bleeding occurs(80). Furthermore, because of the solid laser fibers, the YAG laser can be used for endoscopic dissection, which can be a disadvantage of the CO2 laser given the hollow nature of CO2 fiber(83). As a result, some feel that the utility for the YAG laser lies between that of the CO2 laser and the PDL(104). The YAG laser can be used for laryngeal cysts, amyloidosis, recurrent respiratory papillomatosis, granulomas and anterior web(82). The Neodymium : YAG laser has a wavelength exactly twice that of the KTP laser, and both lasers behave similarly and have similar indications.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 36PDF page: 36PDF page: 36PDF page: 36
Chapter 2
36
Zeitels et al performed 32 procedures of 2013 nm Thulium : YAG laser excisions under local anesthesia, of which 20 were for papillomatosis, six were for microinvasive carcinoma, three were for benign supraglottic lesions, two were for edema, and one was for granuloma(104). A glass fiber of 0.365 mm was used with power settings between 4 and 7 W and in a continuous mode. No complications were reported. At power settings below 4 W, the laser is far less effective. Tissue easily adheres to the fiber tip which requires cleaning. This effect is less often seen at power settings of 4 W and above. Tissue healing does not appear to be adversely affected when power levels are increased. Koufman et al performed 27 Thulium : YAG laser treatments in 17 patients with recurrent respiratory papilloma, granuloma, amyloid, vocal cord lesion, dystonia, and glottal web(82). One self-limiting vocal cord hematoma occurred.
DISCUSSION
In the last two decades, office-based procedures under topical anesthesia in laryngology have made tremendous progress. With the development of distal chip laryngoscopes and the inclusion of a working channel, more diagnostic and therapeutic procedures can be performed in the outpatient clinic instead of the operating room, resulting in multiple advantages(31, 48, 64, 105-108). Laryngeal surgery under general anesthesia has the disadvantage of delaying time to diagnosis and or therapy because of scheduling, dental damage due to rigid endoscopy, and the previously mentioned health risk associated with anesthesia(10). In patients at high risk of undergoing sedation or general anesthesia, or in those patients with a difficult head and neck anatomy, office-based surgery may be a solution(9, 10, 13). Although careful preprocedural planning should always be performed and if indicated, periprocedural monitoring should be used. All these issues are particularly important in head and neck oncological patients who often present with significant comorbidities. The success of the procedure depends, in part, on the patients’ cooperation, which is determined by multiple factors(9, 10, 35, 39, 50, 65, 67, 74). Most problems can be minimized by adequate topical anesthesia and a clear explanation of the procedure, which helps ease the patient. Which anesthetic to use, the method of application, and possible complications have all yet to be determined. In comparison with endoscopy under general anesthesia, it is possible to ask patients to perform different throat movements to improve access to the lesion, such as the valsalva maneuver to increase the visualization of the piriform sinus and the postcricoid region. This has led to a broad spectrum of office-based procedures that are currently being performed in the outpatient clinic by laryngologists and head and neck surgeons. Each procedure will initially have challenges, which can be overcome with proper training. Adequately acquiring the skill to perform office-based diagnostics (such as TNE) is easier than tackling therapeutic
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 37PDF page: 37PDF page: 37PDF page: 37
Office-based procedures for laryngeal pathology
37
2
procedures. The authors of this review recommend starting with these diagnostic types of office-based procedures to develop a skill set that will be transferable to more advanced therapeutic techniques. The procedure should be short and painless. Furthermore, the patient’s tolerability of the procedure should be monitored and when needed, the patient should be given adequate instructions. These instructions are essential when performing more challenging procedures such as biopsy or laser surgery, as the patient has to position the head for adequate lesion exposure or controlling vocal cord movement. The outcome of office-based procedures depends on the practitioners’ experience and the patients’ cooperation.
The effectiveness of biopsies taken under topical anesthesia can be limited by an excessive gag reflex(27). With adequate topical anesthesia, in the form of spraying the oropharynx and hypopharynx and a transcricothyroid membrane injection or administration through the working channel with lidocaine, this problem can be minimized. However, superficial biopsies can result in an inconclusive pathological diagnosis(31). If a superficial biopsy is suspected by the clinician, more biopsies can then be obtained during the procedure. A negative office-based biopsy should only be accepted when the clinical suspicion matches the result(26). In case of doubt, the office-based procedure can be repeated, or biopsies can be obtained by a rigid endoscopy under general anesthesia.
A negative pathological diagnosis can undo the initial advantages of the procedure, namely being rapid and less expensive, if the procedure has to be repeated or eventually performed in the operating room. Digital chromoendoscopy could be a promising technique in decreasing this possible inaccuracy. By using different light filters in the endoscope or in a postprocessing method, broader tumor margins can be detected that are normally not seen with white light. This may be beneficial in case of second primary tumor or recurrence, where tumor margins are more difficult to objectively assess(13). Biopsies can be obtained from these margins, which could improve diagnostic accuracy.
Biopsy forceps can also be used to remove polyps, nodules or granulomas through either the working channel of the endoscope or transorally(21, 23, 25, 29, 45, 102). The surgical manipulation in office-based polypectomy is limited, and therefore not all laryngeal pathology can be adequately removed using this approach. Tai et al stated that wide-based submucosal lesions, delicate vocal cord lesions and lesions with high vascularity should be avoided(45). Laryngeal granulomas have a high tendency for recurrence(102). This could be an argument in favor of in-office removal, as it can safely be repeated with minimal health risk. Some
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 38PDF page: 38PDF page: 38PDF page: 38
Chapter 2
38
patients have no other option than office-based procedures in case of a high risk of general anesthesia(29). The only absolute contra-indication for office-based procedures, which includes office-based biopsies, is a compromised airway. Relative contraindications are intolerance to a prior office-based biopsy and the use of anticoagulants(28).
A large prospective comparative study between office-based and operating room biopsies was not found in the current search strategy for this review. Therefore, higher-level evidence concerning the accuracy of laryngeal FEB under local anesthesia is still awaited. However, as is demonstrated in the previous sections, many groups have now reported significant experience with office-based techniques, suggesting that these are increasingly common.
Although vocal cord injections have been performed for more than a century, the procedure in an office-based setting has gained popularity since the development of flexible laryngoscopes. Each of the several techniques has its own challenges. Using a sclerotherapy needle through the working channel of the endoscope requires additional injection fluid, as the fluid has to pass through the entire length of the endoscope(67). Furthermore, an extra assistant is needed to perform the injection(43, 52, 67). Jin et al found it difficult to predict injection depth in the cricothyroid approach, which could be remedied by bending the needle tip(58). The percutaneous thyrohyoid approach has to be done at a specific angle, which due to anatomical variety, is not possible in all patients. This can also be overcome by bending the needle to a specific degree(39, 52). Amin described the reach of the injection in the true and false vocal cords for percutaneous methods(71).
Which injection approach produces better results in objective and subjective voice quality measures has not yet been studied in a randomized controlled trial. Although not randomized, Woo et al compared the thyrohyoid with the cricrothyroid approach and found a more objective voice improvement for the thyrohyoid procedure(53). In this approach, more calcium hydroxylapatite was used compared with the cricothyroid approach. Almost all studies reported improvement of voice quality, which also applies when compared with operating room-performed vocal cord augmentation(35, 39-41, 43, 48, 49, 51, 53, 55, 56, 64, 65, 67, 69, 71, 74, 75). In a retrospective case-control review, more minor complications were seen in office-based injections compared with operating room-performed injections(74). Bové et al described the indications for operating room injections if patients require direct microlaryngoscopic removal, patients having a pathological process of the SLP that requires microlaryngoscopy, patients have a concomitant operative procedure, and in patients having low thresholds for tolerating office-based injections(48).
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 39PDF page: 39PDF page: 39PDF page: 39
Office-based procedures for laryngeal pathology
39
2
For some of the mentioned materials, the amount of the substance, location, and depth that can be injected in the true and false vocal cords are reported(9). Mallur and Rosen reported on the use of different materials for temporary or permanent vocal cord pathologies and described the technique for each different injection approach(65). The more soft tissue stays between the injected substance and membranous vocal cord, the less chance of local inflammatory reaction(20, 109). Almost all substances require overinjection as injected volumes decrease in the days after injection. Although no uniform percentage is mentioned in the literature, estimates vary between 10% and 50%(20, 46, 55, 69). This has to be kept in mind when performing vocal cord injections, as gaining good speech function during the procedure may only mimic a good long-term result. No uniform consensus is known on the amount of voice rest after the procedure, varying from 1 to 7 days(41, 43, 65).
Although voice rest can often help in reducing benign vocal cord lesions, office-based injections under topical anesthesia appear to be an effective therapy with good patient tolerance. The injection approach used depends on the preference of the clinician, as no proper investigation has been conducted to determine the most successful approach. The most appropriate injectable is dependent on the vocal cord pathology, as each substance has its own qualities, although again, clinician preference is often the determining factor.
For a wide variety of benign laryngeal pathologies, laser surgery under topical anesthesia has proven to be another promising therapeutic endoscopic treatment modality. Especially in patients with frequent recurrences, the burden of general anesthesia for each laser treatment is not to be underestimated, and office-based laser surgery offers a less burdensome alternative. The possible downside is that this could lead to more procedures as the threshold to perform laser surgery becomes lowe(81-83, 90, 92). The high recurrence rate of papillomas could be another explanation for this increase of in-office-performed laser surgery, as it is much more convenient to repeat than a procedure in general anesthesia. With the development of the PDL and the KTP and YAG lasers in addition to the flexible fiber delivery of the CO2 laser, specific benign lesions can be targeted with the appropriate laser(81, 82). The current review only found one study that used the CO2 laser in an in-office setting and two where a thulium-based YAG laser was used (82, 104). Each laser operates on a different wave length and has therefore specific advantages, which are stated above, although no studies were found to compare the effectiveness of different lasers for specific laryngeal lesions(103). Rosen et al therefore stated that the choice of laser is purely theoretical(11). Which laser settings are ideal to use for different pathological lesions are not mentioned in the current included studies, as all authors use different laser parameters. Mallur et al reported on the used wattage and pulse width of the KTP laser for different benign pathologies
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 40PDF page: 40PDF page: 40PDF page: 40
Chapter 2
40
but could not accurately conclude which parameters were best to use(98). Shue et al even stated that it is unreliable to depend on the data of the laser settings, as the actual energy delivered and the uptake by the tissue are uncertain(99). In multiple study populations, different lasers show promising results with a large reported degree of regression for the treated pathology and improvement of voice quality(82, 83, 92, 95, 98, 101, 110).
Of 54 patients who have undergone operating room and office-based laser surgery, the majority preferred the office-based procedure(89). Laser surgery requires extra attention to safety procedures for the patient and staff(10, 83). The working channel of the endoscope has to be protected against damage caused by heat from the laser, which used to be a problem with the CO2 laser but has recently been overcome(82, 84, 85). Xie et al conducted a systematic review and found no evidence to indicate that office-based laser surgery is less safe compared with operating room-performed laser surgery(103). The same was seen in large fiber KTP lasers, which resulted in the preference of 0.4-mm laser fibers(90).Postprocedural care is in line with other office-based procedures. Furthermore, voice rest is recommended, although again the amount of days is not uniform and varies between 5 and 7 days(10, 110).
There is a need for more clinical studies to establish the selection criteria for the treatment of benign and malignant lesions by office-based laser surgery. There are no studies that investigate the use of office-based laser surgery for early glottic carcinoma. The oncological effectiveness of in-office laser surgery remains unknown. The effectiveness of most of the procedures for benign lesions is determined by the percentage of regression of the lesion (90-92, 102, 110).
This review has systematically searched for the current literature on office-based procedures in laryngology and head and neck oncology. By not limiting the date in the search strategy, the content of the screened articles became extensive. Because most office-based procedures were performed in the last two decades, it could be possible to limit the date to 20 years. Although extensive, there are articles missing that could be in the scope of this review. Furthermore, to accurately assess the quality of each article and thus the assumed conclusions of that article, a methodological assessment has to be performed. The main goal of the study is to present an overview of current literature.
With the ongoing development of new techniques for office-based procedures, the future has much to offer. The improvement in image quality, as seen after the introduction of distal chip endoscopes, is ever ongoing. Current endoscopes offer high resolution images with the option of a working channel. Furthermore, color filters offer better visual enhancement for

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 41PDF page: 41PDF page: 41PDF page: 41
Office-based procedures for laryngeal pathology
41
2
proper inspection of mucosa surface changes, which could facilitate earlier tumor detection. The next step is 4K and high- definition (HD) endoscopes, which are already available. Compared with the high-resolution endoscopes, the image quality is even more detailed. HD image quality with thinner diameter endoscopes with working channels will be of great value in the future.
The current endoscopes operate with one arm, which means there is a single tube that can move in different directions and contains the camera and working channel, through which instruments may be passed. Although many office-based procedures can be performed with this endoscope, there remain anatomical sites that are difficult to properly treat, such as the posterior pharyngeal wall. This problem can be overcome by developing an endoscope containing multiple arms. When inserted transnasally, the endoscope should resemble the current endoscopes. When the designated anatomical site is reached, the distal part of the endoscope should possess the quality of unfolding in multiple arms. The camera should be a separate arm to adequately overview the site and the other endoscope arms. These arms can contain working channels, so multiple instruments can be passed through at the same time. Another possibility is to incorporate several instruments, such as biopsy forceps, an injection needle, or a surgical knife, in the endoscope arms. This will save time to pass instruments through the working channel and be applicable in different medical specialties.
The authors of this review believe that office-based procedures are the future for a rapid medical diagnosis and treatment, with minimal health risks for the patient. As described above, the last two decades has led to a wide variety of procedures that are performed under local anesthesia. The rapid rise in technological knowledge will benefit this ongoing evolution for the next 20 years.
CONCLUSION
The development of distal chip endoscopes with a working channel has led to an increase in office-based procedures performed for laryngeal pathology. Laryngeal FEB, vocal cord injection, and laser surgery have been widely investigated and demonstrate good patient tolerability and both diagnostic and therapeutic accuracy comparable with that achieved with operating room-based procedures. Overall, office-based procedures result in a shorter procedural duration, a more rapid diagnostic process, reduced costs, and reduced health risks largely due to avoiding sedation or general anesthesia. Data on complications are available only from prospective observational series, and higher-level evidence is awaited.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 42PDF page: 42PDF page: 42PDF page: 42
Chapter 2
42
REFERENCES
1. Lewin, G., Allgemeine Medizinische Central-Zeitung. Vol. 30:654. 1861.
2. Mackenzie, M., The extirpation of growths. In: The use of the laryngoscope in diseases of the
throat with an appendix on rhinoscopy. 1865, Churchill, London: J & A.
3. Elsberg, L., Laryngoscopal surgery illustrated in the treatment of morbid growths within the
larynx. 1866, Philadelphia, Pa: Collins.
4. Solis-Cohen, J., Removal of a fibrous polyp from the inferior surface of the right vocal fold with the
aid of the laryngoscope. Am J Med Sci, 1867. April: p. 404-7.
5. Koller, K., Ueber die Verwendung des Cocain zur Anasthesirung am Aug. Wien Med Wochenschr,
1884. 34: p. 1276.
6. Williams, G.T., I.M. Farquharson, and J. Anthony, Fibreoptic laryngoscopy in the assessment of
laryngeal disorders. J Laryngol Otol, 1975. 89(3): p. 299-316.
7. Silberman, H.D., H. Wilf, and J.A. Tucker, Flexible fiberoptic nasopharyngolaryngoscope. Ann
Otol Rhinol Laryngol, 1976. 85(5 Pt.1): p. 640-5.
8. Koufman, J.A., Introduction to office-based surgery in laryngology. Curr Opin Otolaryngol Head
Neck Surg, 2007. 15(6): p. 383-6.
9. Simpson, C.B. and M.R. Amin, Office-based procedures for the voice. Ear Nose Throat J, 2004.
83(7 Suppl 2): p. 6-9.
10. Shah, M.D. and M.M. Johns, 3rd, Office-based laryngeal procedures. Otolaryngol Clin North Am,
2013. 46(1): p. 75-84.
11. Rosen, C.A., et al., Advances in office-based diagnosis and treatment in laryngology.
Laryngoscope, 2009. 119(SUPPL. 2): p. S185-S212.
12. Zeitels, S.M., et al., Foresight in laryngology and laryngeal surgery: a 2020 vision. Ann Otol Rhinol
Laryngol Suppl, 2007. 198: p. 2-16.
13. Pan, C.T., et al., NBI flexible laryngoscopy targeted tissue sampling in head and neck cancer
patients with difficult airways. European Archives of Oto-Rhino-Laryngology, 2013. 270(1): p.
263-269.
14. Arantes, V., et al., Effectiveness of unsedated transnasal endoscopy with white-light, flexible
spectral imaging color enhancement, and lugol staining for esophageal cancer screening in
high-risk patients. J Clin Gastroenterol, 2013. 47(4): p. 314-21.
15. O’Brien, T.J. and K. Parham, Transnasal esophagoscopy: white-light versus narrowband imaging.
Ann Otol Rhinol Laryngol, 2008. 117(12): p. 886-90.
16. Wang, C.H., et al., Use of transnasal endoscopy for screening of esophageal squamous cell
carcinoma in high-risk patients: yield rate, completion rate, and safety. Dig Endosc, 2014. 26(1):
p. 24-31.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 43PDF page: 43PDF page: 43PDF page: 43
Office-based procedures for laryngeal pathology
43
2
17. Wang, W.H. and K.Y. Tsai, Narrow-band imaging of laryngeal images and endoscopically proven
reflux esophagitis. Otolaryngol Head Neck Surg, 2015. 152(5): p. 874-80.
18. Masaki, T., et al., Narrow band imaging in the diagnosis of intra-epithelial and invasive laryngeal
squamous cell carcinoma: a preliminary report of two cases. Auris Nasus Larynx, 2009. 36(6): p.
712-6.
19. Ho, C.Y., K.T. Chan, and P.Y. Chu, Comparison of narrow-band imaging and conventional
nasopharyngoscopy for the screening of unaffected members of families with nasopharyngeal
carcinoma. Eur Arch Otorhinolaryngol, 2013. 270(9): p. 2515-20.
20. Woo, P., Office-based laryngeal procedures. Otolaryngol Clin North Am, 2006. 39(1): p. 111-33.
21. Omori, K., et al., Videoendoscopic laryngeal surgery. Ann Otol Rhinol Laryngol, 2000. 109(2): p.
149-55.
22. Mahieu, H.F. and F.G. Dikkers, Indirect microlaryngostroboscopic surgery. Arch Otolaryngol
Head Neck Surg, 1992. 118(1): p. 21-4.
23. Lan, M.C., et al., Office-based treatment of vocal fold polyp with flexible laryngosvideostroboscopic
surgery. J Otolaryngol Head Neck Surg, 2010. 39(1): p. 90-5.
24. Walter, T., et al., Biopsy specimens obtained with small-caliber endoscopes have comparable
diagnostic performances than those obtained with conventional endoscopes: a prospective
study on 1335 specimens. J Clin Gastroenterol, 2010. 44(1): p. 12-7.
25. Wang, C.T., et al., Comparison of treatment outcomes of transnasal vocal fold polypectomy
versus microlaryngoscopic surgery. Laryngoscope, 2015. 125(5): p. 1155-60.
26. Lippert, D., et al., In-office biopsy of upper airway lesions: Safety, tolerance, and effect on time to
treatment. Laryngoscope, 2015. 125(4): p. 919-923.
27. Cohen, J.T., et al., Reliability of a transnasal flexible fiberoptic in-office laryngeal biopsy. JAMA
Otolaryngol Head Neck Surg, 2013. 139(4): p. 341-5.
28. Zalvan, C.H., et al., Comparison of trans-nasal laryngoscopic office based biopsy of
laryngopharyngeal lesions with traditional operative biopsy. Eur Arch Otorhinolaryngol, 2013.
270(9): p. 2509-13.
29. Schindler, A., P. Capaccio, and F. Ottaviani, Videoendoscopic surgery for inaccessible glottic
lesions. J Laryngol Otol, 2005. 119(11): p. 899-902.
30. Wellenstein, D.J., et al., Safety of flexible endoscopic biopsy of the pharynx and larynx under
topical anesthesia. Eur Arch Otorhinolaryngol, 2017.
31. Naidu, H., et al., Comparison of efficacy, safety, and cost-effectiveness of in-office cup forcep
biopsies versus operating room biopsies for laryngopharyngeal tumors. J Voice, 2012. 26(5): p.
604-6.
32. Lewy, R.B., Experience with vocal cord injection. Ann Otol Rhinol Laryngol, 1976. 85(4 Pt 1): p.
440-50.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 44PDF page: 44PDF page: 44PDF page: 44
Chapter 2
44
33. Benjamin, B., Vocal cord injection using local anaesthesia. Journal of the Otolaryngological
Society of Australia, 1983. 5(2): p. 27-30.
34. Ward, P.H., D.G. Hanson, and E. Abemayor, Transcutaneous Teflon injection of the paralyzed
vocal cord: a new technique. Laryngoscope, 1985. 95(6): p. 644-9.
35. Ford, C.N., P.A. Staskowski, and D.M. Bless, Autologous collagen vocal fold injection: a
preliminary clinical study. Laryngoscope, 1995. 105(9 Pt 1): p. 944-8.
36. Netterville, J.L., et al., Lateral laryngotomy for the removal of Teflon granuloma. Ann Otol Rhinol
Laryngol, 1998. 107(9 Pt 1): p. 735-44.
37. Trask, D.K., D.L. Shellenberger, and H.T. Hoffman, Transnasal, endoscopic vocal fold
augmentation. Laryngoscope, 2005. 115(12): p. 2262-5.
38. Zeitler, D.M. and M.R. Amin, The thyrohyoid approach to in-office injection augmentation of the
vocal fold. Curr Opin Otolaryngol Head Neck Surg, 2007. 15(6): p. 412-6.
39. Rees, C.J., D.A. Mouadeb, and P.C. Belafsky, Thyrohyoid vocal fold augmentation with calcium
hydroxyapatite. Otolaryngol Head Neck Surg, 2008. 138(6): p. 743-6.
40. Tateya, I., et al., Steroid injection to vocal nodules using fiberoptic laryngeal surgery under topical
anesthesia. Eur Arch Otorhinolaryngol, 2004. 261(9): p. 489-92.
41. Hsu, Y.B., M.C. Lan, and S.Y. Chang, Percutaneous corticosteroid injection for vocal fold polyp.
Arch Otolaryngol Head Neck Surg, 2009. 135(8): p. 776-80.
42. Lee, S.H., et al., Local steroid injection via the cricothyroid membrane in patients with a vocal
nodule. Arch Otolaryngol Head Neck Surg, 2011. 137(10): p. 1011-6.
43. Wang, C.T., et al., Transnasal endoscopic steroid injection: a practical and effective alternative
treatment for benign vocal fold disorders. Laryngoscope, 2013. 123(6): p. 1464-8.
44. Kwon, T.K., et al., Calcium hydroxylapatite injection laryngoplasty for the treatment of
presbylaryngis: long-term results. Laryngoscope, 2010. 120(2): p. 326-9.
45. Tai, S.K., P.Y. Chu, and S.Y. Chang, Transoral laryngeal surgery under flexible
laryngovideostroboscopy. J Voice, 1998. 12(2): p. 233-8.
46. Ford, C.N. and D.M. Bless, Clinical experience with injectable collagen for vocal fold augmentation.
Laryngoscope, 1986. 96(8): p. 863-9.
47. Remacle, M., et al., Correction of glottic insufficiency by collagen injection. Ann Otol Rhinol
Laryngol, 1990. 99(6 Pt 1): p. 438-44.
48. Bove, M.J., et al., Operating room versus office-based injection laryngoplasty: a comparative
analysis of reimbursement. Laryngoscope, 2007. 117(2): p. 226-30.
49. Kimura, M., et al., Clinical experience with collagen injection of the vocal fold: a study of 155
patients. Auris Nasus Larynx, 2008. 35(1): p. 67-75.
50. Sulica, L., et al., Current practice in injection augmentation of the vocal folds: indications,
treatment principles, techniques, and complications. Laryngoscope, 2010. 120(2): p. 319-25.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 45PDF page: 45PDF page: 45PDF page: 45
Office-based procedures for laryngeal pathology
45
2
51. Lee, S.W., et al., Utility of injection laryngoplasty in the management of post-thyroidectomy vocal
cord paralysis. Thyroid, 2010. 20(5): p. 513-7.
52. Sung, C.K. and G.J. Tsao, Single-operator flexible nasolaryngoscopy-guided transthyrohyoid
vocal fold injections. Ann Otol Rhinol Laryngol, 2013. 122(1): p. 9-14.
53. Woo, S.H., et al., Comparative analysis on the efficiency of the injection laryngoplasty technique
using calcium hydroxyapatite (CaHA): the thyrohyoid approach versus the cricothyroid approach.
J Voice, 2013. 27(2): p. 236-41.
54. Truong, D.D. and R. Bhidayasiri, Botulinum toxin therapy of laryngeal muscle hyperactivity
syndromes: comparing different botulinum toxin preparations. Eur J Neurol, 2006. 13 Suppl 1: p.
36-41.
55. Hoffman, H., et al., Laryngeal collagen injection as an adjunct to medialization laryngoplasty.
Laryngoscope, 2002. 112(8 Pt 1): p. 1407-13.
56. Kimura, M., et al., Collagen injection as a supplement to arytenoid adduction for vocal fold
paralysis. Ann Otol Rhinol Laryngol, 2008. 117(6): p. 430-6.
57. Bastian, R.W. and K.G. Delsupehe, Indirect larynx and pharynx surgery: a replacement for direct
laryngoscopy. Laryngoscope, 1996. 106(10): p. 1280-6.
58. Jin, S.M., et al., Transcutaneous injection laryngoplasty through the cricothyroid space in the
sitting position: anatomical information and technique. Eur Arch Otorhinolaryngol, 2008. 265(3):
p. 313-9.
59. Chhetri, D.K. and N. Jamal, Percutaneous injection laryngoplasty. Laryngoscope, 2014. 124(3):
p. 742-5.
60. Miller, R.H., G.E. Woodson, and J. Jankovic, Botulinum toxin injection of the vocal fold for
spasmodic dysphonia. A preliminary report. Arch Otolaryngol Head Neck Surg, 1987. 113(6): p.
603-5.
61. Carroll, T.L. and C.A. Rosen, Long-term results of calcium hydroxylapatite for vocal fold
augmentation. Laryngoscope, 2011. 121(2): p. 313-9.
62. Kwon, T.K., et al., Serial computed tomographic and positron emission tomographic properties
of injection material used for vocal fold augmentation. Laryngoscope, 2013. 123(10): p. 2491-6.
63. Kwon, T.K., C.A. Rosen, and J. Gartner-Schmidt, Preliminary results of a new temporary vocal
fold injection material. J Voice, 2005. 19(4): p. 668-73.
64. Andrade Filho, P.A., R.L. Carrau, and R.A. Buckmire, Safety and cost-effectiveness of intra-
office flexible videolaryngoscopy with transoral vocal fold injection in dysphagic patients. Am J
Otolaryngol, 2006. 27(5): p. 319-22.
65. Mallur, P.S. and C.A. Rosen, Office-based laryngeal injections. Otolaryngol Clin North Am, 2013.
46(1): p. 85-100.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 46PDF page: 46PDF page: 46PDF page: 46
Chapter 2
46
66. Young, V.N., et al., Patient tolerance of awake, in-office laryngeal procedures: A Multi-Institutional
Perspective. Laryngoscope, 2012. 122(2): p. 315-321.
67. Rhew, K., D.A. Fiedler, and C.L. Ludlow, Technique for injection of botulinum toxin through the
flexible nasolaryngoscope. Otolaryngol Head Neck Surg, 1994. 111(6): p. 787-94.
68. Hussain, A., G. Thiel, and M. Shakeel, Trans-nasal injection of botulinum toxin. J Laryngol Otol,
2009. 123(7): p. 783-5.
69. Tirado, Y., et al., Office-based injection laryngoplasty in the irradiated larynx. Laryngoscope,
2010. 120(4): p. 703-6.
70. Mortensen, M. and P. Woo, Office steroid injections of the larynx. Laryngoscope, 2006. 116(10):
p. 1735-9.
71. Amin, M.R., Thyrohyoid approach for vocal fold augmentation. Ann Otol Rhinol Laryngol, 2006.
115(9): p. 699-702.
72. Carroll, T.L. and C.A. Rosen, Trial vocal fold injection. J Voice, 2010. 24(4): p. 494-8.
73. Hoffman, H.T., et al., Transillumination for needle localization in the larynx. Laryngoscope, 2015.
125(10): p. 2341-2348.
74. Mathison, C.C., et al., Comparison of outcomes and complications between awake and asleep
injection laryngoplasty: a case-control study. Laryngoscope, 2009. 119(7): p. 1417-23.
75. Wang, C.T., et al., Intralesional steroid injection for benign vocal fold disorders: a systematic
review and meta-analysis. Laryngoscope, 2013. 123(1): p. 197-203.
76. Nakamura, M., et al., Over-injection of autologous fat in the vocal fold: how to remove the excess?
Eur Arch Otorhinolaryngol, 2009. 266(10): p. 1589-93.
77. Woo, J.H., et al., Efficacy of percutaneous vocal fold injections for benign laryngeal lesions:
Prospective multicenter study. Acta Otolaryngol, 2011. 131(12): p. 1326-32.
78. Coleman, J.R., Jr., et al., Histomorphometric and laryngeal videostroboscopic analysis of the
effects of corticosteroids on microflap healing in the dog larynx. Ann Otol Rhinol Laryngol, 1999.
108(2): p. 119-27.
79. Tateya, I., et al., Steroid Injection for Reinke’s Edema Using Fiberoptic Laryngeal Surgery. Acta
Oto-Laryngologica, 2003. 123(3): p. 417-420.
80. Rathfoot, C.J. and J.A. Coleman, Laser utilization in the oral pharynx. Otolaryngol Clin North Am,
1996. 29(6): p. 963-72.
81. Zeitels, S.M. and J.A. Burns, Laser applications in laryngology: past, present, and future.
Otolaryngol Clin North Am, 2006. 39(1): p. 159-72.
82. Koufman, J.A., et al., Office-based laryngeal laser surgery: a review of 443 cases using three
wavelengths. Otolaryngol Head Neck Surg, 2007. 137(1): p. 146-51.
83. Zeitels, S.M. and J.A. Burns, Office-based laryngeal laser surgery with local anesthesia. Curr
Opin Otolaryngol Head Neck Surg, 2007. 15(3): p. 141-7.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 47PDF page: 47PDF page: 47PDF page: 47
Office-based procedures for laryngeal pathology
47
2
84. Devaiah, A.K., et al., Surgical utility of a new carbon dioxide laser fiber: functional and histological
study. Laryngoscope, 2005. 115(8): p. 1463-8.
85. Zeitels, S.M., et al., Carbon dioxide laser fiber for laryngeal cancer surgery. Ann Otol Rhinol
Laryngol, 2006. 115(7): p. 535-41.
86. Anderson, R.R. and J.A. Parrish, Selective photothermolysis: precise microsurgery by selective
absorption of pulsed radiation. Science, 1983. 220(4596): p. 524-7.
87. Gange, R.W., R.R. Anderson, and E. Gonzalez, Laser treatment of port-wine stains. Br J Dermatol,
1988. 119(1): p. 131-2.
88. Cohen, J.T., J.A. Koufman, and G.N. Postma, Pulsed-dye laser in the treatment of recurrent
respiratory papillomatosis of the larynx. Ear, Nose and Throat Journal, 2003. 82(8): p. 558.
89. Rees, C.J., et al., Patient tolerance of in-office pulsed dye laser treatments to the upper
aerodigestive tract. Otolaryngol Head Neck Surg, 2006. 134(6): p. 1023-7.
90. Zeitels, S.M., et al., Office-based 532-nm pulsed KTP laser treatment of glottal papillomatosis and
dysplasia. Ann Otol Rhinol Laryngol, 2006. 115(9): p. 679-85.
91. Franco, R.A., Jr., Aminolevulinic acid 585 nm pulsed dye laser photodynamic treatment of
laryngeal keratosis with atypia. Otolaryngol Head Neck Surg, 2007. 136(6): p. 882-7.
92. Zeitels, S.M., et al., Office-based treatment of glottal dysplasia and papillomatosis with the 585-
nm pulsed dye laser and local anesthesia. Ann Otol Rhinol Laryngol, 2004. 113(4): p. 265-76.
93. Franco, R.A., Jr., et al., 585-nm pulsed dye laser treatment of glottal papillomatosis. Ann Otol
Rhinol Laryngol, 2002. 111(6): p. 486-92.
94. Koszewski, I.J., et al., Office-Based Photoangiolytic Laser Treatment of Reinke’s Edema: Safety
and Voice Outcomes. Otolaryngol Head Neck Surg, 2015. 152(6): p. 1075-81.
95. Zeitels, S.M. and J.A. Burns, Office-based laryngeal laser surgery with the 532-nm pulsed-potassium-
titanyl-phosphate laser. Curr Opin Otolaryngol Head Neck Surg, 2007. 15(6): p. 394-400.
96. Levine, H.L., Endoscopy and the KTP/532 laser for nasal sinus disease. Ann Otol Rhinol Laryngol,
1989. 98(1 Pt 1): p. 46-51.
97. Mallur, P.S., et al., Proposed classification system for reporting 532-nm pulsed potassium titanyl
phosphate laser treatment effects on vocal fold lesions. Laryngoscope, 2014. 124(5): p. 1170-5.
98. Mallur, P.S., et al., Quantification of benign lesion regression as a function of 532-nm pulsed
potassium titanyl phosphate laser parameter selection. The Laryngoscope, 2011. 121(3): p. 590-
595.
99. Sheu, M., et al., Multi-institutional experience with the in-office potassium titanyl phosphate laser
for laryngeal lesions. J Voice, 2012. 26(6): p. 806-10.
100. Wang, C.T., et al., Office-based potassium titanyl phosphate laser-assisted endoscopic vocal
polypectomy. JAMA Otolaryngol Head Neck Surg, 2013. 139(6): p. 610-6.
101. Sridharan, S., et al., Patient-based outcomes of in-office KTP ablation of vocal fold polyps.
Laryngoscope, 2014. 124(5): p. 1176-9.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 48PDF page: 48PDF page: 48PDF page: 48
Chapter 2
48
102. Hirano, S., et al., Fiberoptic laryngeal surgery for vocal process granuloma. Ann Otol Rhinol
Laryngol, 2002. 111(9): p. 789-93.
103. Xie, X., et al., KTP 532 nm Laser for Laryngeal Lesions. A Systematic Review. Journal of Voice,
2013. 27(2): p. 245-249.
104. Zeitels, S.M., et al., Office-based and microlaryngeal applications of a fiber-based thulium laser.
Ann Otol Rhinol Laryngol, 2006. 115(12): p. 891-6.
105. Bush, C.M. and G.N. Postma, Transnasal esophagoscopy. Otolaryngol Clin North Am, 2013.
46(1): p. 41-52.
106. Sabirin, J., M. Abd Rahman, and P. Rajan, Changing trends in oesophageal endoscopy: a
systematic review of transnasal oesophagoscopy. ISRN Otolaryngol, 2013. 2013: p. 586973.
107. McPartlin, D.W., et al., How we do it: transnasal fibreoptic oesophagoscopy. Clin Otolaryngol,
2005. 30(6): p. 547-50.
108. Frieling, T., et al., Krefeld CONTRA study: Conventional peroral esophago-gastro-duodenoscopy
(EGD) vs. Transnasal EGD a prospective and randomised study with independent evaluation of
conscious sedation, endoscope diameter, and access path. Zeitschrift fur Gastroenterologie,
2010. 48(8): p. 818-824.
109. Chheda, N.N., et al., Revision laryngeal surgery for the suboptimal injection of calcium
hydroxylapatite. Laryngoscope, 2008. 118(12): p. 2260-3.
110. Franco, R.A., Jr., In-office laryngeal surgery with the 585-nm pulsed dye laser. Curr Opin
Otolaryngol Head Neck Surg, 2007. 15(6): p. 387-93.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 49PDF page: 49PDF page: 49PDF page: 49
Office-based procedures for laryngeal pathology
49
2
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 50PDF page: 50PDF page: 50PDF page: 50
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 51PDF page: 51PDF page: 51PDF page: 51
Chapter 3Office-based procedures for diagnosis
and treatment of esophageal pathology
David J. Wellenstein, MD1, Henrieke W. Schutte, MD1, Henri A.M. Marres, MD PhD1, Jimmie Honings, MD PhD1, Peter C. Belafsky, MD PhD2, Gregory N. Postma, MD3,
Robert P. Takes MD, PhD1, Guido B. van den Broek, MD PhD1
1. Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands
2. Professor and Director, Center for Voice and Swallowing, Department of Otolaryngology and Head
and Neck Surgery, University of California, Davis School of Medicine, Sacramento, California
3. Professor and Vice Chairman, Department of Otolaryngology,
Medical College of Georgia at Augusta University, Augusta, Georgia
Head & Neck. 2017 Sep;39(9):1910-1919.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 52PDF page: 52PDF page: 52PDF page: 52
Chapter 3
52
ABSTRACT
IntroductionDiagnostic and therapeutic office-based procedures under topical anesthesia are emerging in the daily practice of laryngologists and head and neck surgeons. Since the introduction of the transnasal esophagoscope, office-based procedures for the esophagus are increasingly performed.
MethodsA systematic review of literature on office-based procedures under topical anesthesia for the esophagus.
ResultsTransnasal esophagoscopy is an extensively investigated office-based procedure. This procedure shows better patient tolerability and equivalent accuracy compared to conventional transoral esophagoscopy, as well as time and cost savings. Secondary tracheo-esophageal puncture, esophageal dilatation, esophageal sphincter injection, and foreign body removal are less investigated, but show promising results.
DiscussionWith the introduction of the transnasal esophagoscope, an increasing number of diagnostic and therapeutic office-based procedures for the esophagus are possible, with multiple advantages. Further investigation must prove the clinical feasibility and effectiveness of the therapeutic office-based procedures.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 53PDF page: 53PDF page: 53PDF page: 53
Office-based procedures for esophageal pathology
53
3
INTRODUCTION
The emergence of digital endoscopes with a working channel has transformed the daily practice of diagnostic and therapeutic procedures in laryngology and head and neck oncology(1). During the last two decades, extensive research has led to a revolution in which an increasing number of procedures have gone from being performed in the operating room under general anesthesia to being performed in the outpatient clinic under topical anesthesia(1-3). This has led to faster diagnostic and therapeutic procedures with proper diagnostic accuracy, time and cost savings, and possible health benefits due to eliminating the risk of sedation or general anesthesia(1).
Several office-based procedures that are performed for the larynx have proven their advantages over the years. With the introduction of the transnasal esophagoscope by Shaker in 1994, the possibility of performing in-office procedures under topical anesthesia for the esophagus has also increased(4). Although laryngologists were the first to perform an esophagoscopy, investigation of the esophagus is currently the expertise of many disciplines including gastroenterology, thoracic surgery and otolaryngology(5, 6). Since the first studies emerged with laryngologists using the transnasal esophagoscopy (TNE), esophageal diagnostics and therapeutic procedures has increasingly been performed by laryngologists and head and neck surgeons(6, 7).
This review of the literature focuses on the available diagnostic and therapeutic office-based procedures for the esophagus, performed under topical anesthesia. This review is an extension of our other work concerning office-based procedures for the larynx.
METHODS
A literature search was performed in the PubMed (MEDLINE), EMBASE and Cochrane Library databases. Keywords and Mesh terms include ‘ambulatory surgical procedures’, ‘ambulatory care’, ‘ambulatory surgery’, ‘outpatient’, ‘outpatient department’, ‘outpatient care’, ‘transnasal’ and ‘transoral’. These terms were combined with ‘esophagus’. The published studies were included without a date limitation. Figure 1 shows the search strategy in a diagram.
The initial search was conducted in April 2016, which identified 4790 articles. Duplicate articles were removed, leaving 3715 articles. Four hundred and seventy-six articles were included; full text articles were obtained using the stated databases, Google Scholar, and
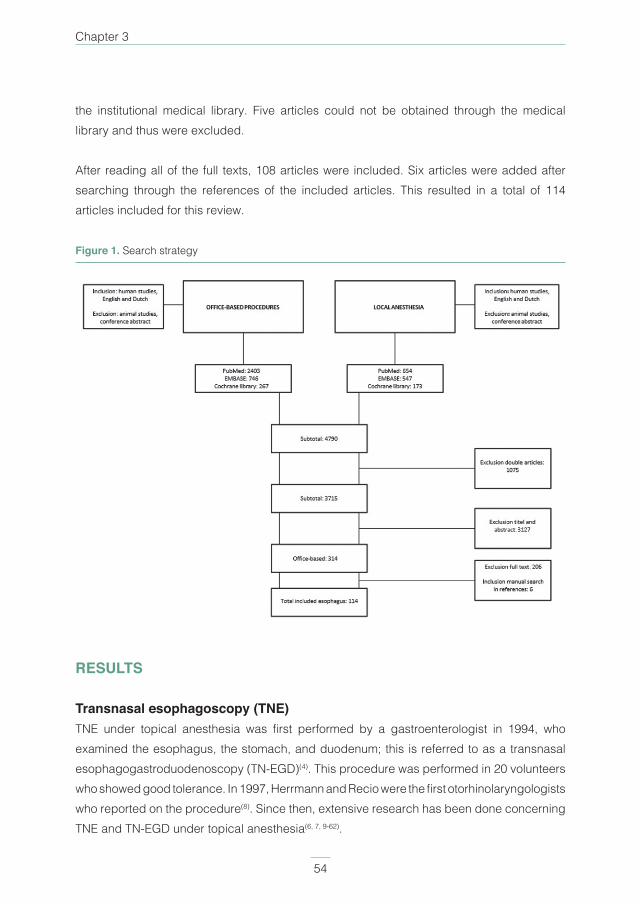
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 54PDF page: 54PDF page: 54PDF page: 54
Chapter 3
54
the institutional medical library. Five articles could not be obtained through the medical library and thus were excluded.
After reading all of the full texts, 108 articles were included. Six articles were added after searching through the references of the included articles. This resulted in a total of 114 articles included for this review.
Figure 1. Search strategy
RESULTS
Transnasal esophagoscopy (TNE)TNE under topical anesthesia was first performed by a gastroenterologist in 1994, who examined the esophagus, the stomach, and duodenum; this is referred to as a transnasal esophagogastroduodenoscopy (TN-EGD)(4). This procedure was performed in 20 volunteers who showed good tolerance. In 1997, Herrmann and Recio were the first otorhinolaryngologists who reported on the procedure(8). Since then, extensive research has been done concerning TNE and TN-EGD under topical anesthesia(6, 7, 9-62).

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 55PDF page: 55PDF page: 55PDF page: 55
Office-based procedures for esophageal pathology
55
3
The most frequently described technique for unsedated TNE is with the patient in an upright seated ‘sniffing’ position. After topical anesthesia and decongestion of the nasal cavity and topical anesthesia of the oropharynx, the endoscope is inserted through the most patent side of the nose. Although, Herrmann and Recio argued against using pharyngeal topical anesthesia, due to decreased pharyngeal sensibility, hypersalivation, and possible aspiration(8). For an easier passage through the nasal cavity, a lubricant can be used. Rosen et al. stated that patients should fast prior to the examination, although no consensus is found on duration and clinical relevance(1). The endoscope is directed into the piriform sinus, after which the patient is asked to burp or swallow. The upper esophageal sphincter opens and the endoscope is passed into the esophagus, the stomach, and in case of a TN-EGD, into the duodenum. Inspection of the mucosa is performed by pulling the endoscope slowly upwards in a circumferential manner. For inspection of the esophagus, air is blown through the working channel to open the esophagus(4, 6, 7, 15-18, 20, 21, 24, 25, 29, 31-33, 37-39, 42, 43, 47-50, 52, 57, 63-66). The gastrointestinal junction is difficult to inspect and requires more time. The caudal portion of the gastrointestinal junction can be visualized by passing the endoscope in the gastric cardia and by performing a retroflexion of the tip of the endoscope up to 210ᵒ, although not all endoscopes possess this feature(40, 42, 54, 64, 67).
The normal diameter of a transnasal esophagoscope is between 4.7 and 6.0 millimeter (mm) and contains a working channel, although there are studies in which an ultrathin endoscope is used with a diameter between 3.1 and 4.0 mm(13, 22, 68). Catanzaro et al. compared the image quality of a 3.1-mm TN-EGD to a conventional TN-EGD and found less accuracy in the ultrathin endoscope in diagnosing Barrett’s esophagus and esophageal varices(13). However, Mokhashi et al. found contradicting results(68).
Indications and interventions for which TNE are used are displayed in Table 1(6, 7, 9, 10, 13-
25, 27-30, 32-34, 37, 38, 40-44, 46, 49, 50, 52, 53, 56-60, 62, 64, 68-81). Overall, patients reported good tolerability of TNE under topical anesthesia, and some studies even found better tolerability compared to transoral esophagoscopy under topical anesthesia or sedation(11, 20, 27, 33, 35, 37, 39, 46, 52, 53, 56, 70, 82). Of the patients who underwent TNE under topical anesthesia, who in some cases also had undergone transoral esophagoscopy, 71% to 100% stated that they would prefer to undergo the unsedated transnasal procedure in the future(22, 24, 28, 33, 46, 70, 71, 82). Studies compared the diagnostic accuracy of TNE to transoral esophagoscopy and found similar results in detecting gastrointestinal pathology(13-15, 22, 24, 41, 47, 50, 62).
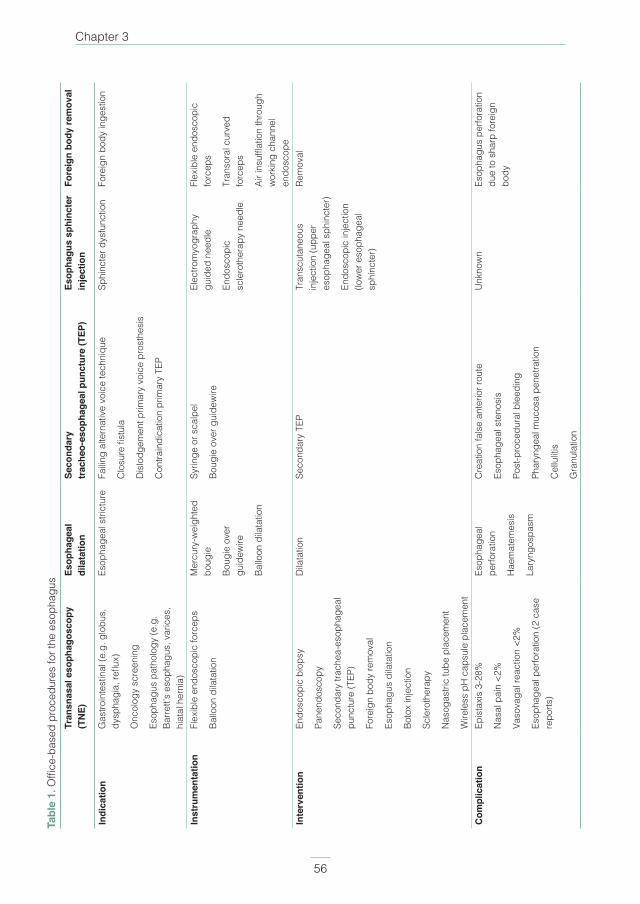
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 56PDF page: 56PDF page: 56PDF page: 56
Chapter 3
56
Tabl
e 1.
Offi
ce-b
ased
pro
cedu
res
for t
he e
soph
agus
Tran
snas
al e
soph
agos
copy
(T
NE)
Esop
hage
al
dila
tatio
nSe
cond
ary
tr
ache
o-es
opha
geal
pun
ctur
e (T
EP)
Esop
hagu
s sp
hinc
ter
inje
ctio
nFo
reig
n bo
dy re
mov
al
Indi
catio
nG
astro
inte
stin
al (e
.g. g
lobu
s,
dysp
hagi
a, re
flux)
Onc
olog
y sc
reen
ing
Esop
hagu
s pa
thol
ogy
(e.g
. Ba
rrett’
s es
opha
gus,
var
ices
, hi
atal
her
nia)
Esop
hage
al s
trict
ure
Failin
g al
tern
ativ
e vo
ice
tech
niqu
e
Clo
sure
fist
ula
Dis
lodg
emen
t prim
ary
voic
e pr
osth
esis
Con
train
dica
tion
prim
ary
TEP
Sphi
ncte
r dys
func
tion
Fore
ign
body
inge
stio
n
Inst
rum
enta
tion
Flex
ible
end
osco
pic
forc
eps
Ballo
on d
ilata
tion
Mer
cury
-wei
ghte
d bo
ugie
Boug
ie o
ver
guid
ewire
Ballo
on d
ilata
tion
Syrin
ge o
r sca
lpel
Boug
ie o
ver g
uide
wire
Elec
trom
yogr
aphy
gu
ided
nee
dle
Endo
scop
ic
scle
roth
erap
y ne
edle
Flex
ible
end
osco
pic
forc
eps
Tran
sora
l cur
ved
forc
eps
Air i
nsuf
flatio
n th
roug
h w
orki
ng c
hann
el
endo
scop
eIn
terv
entio
nEn
dosc
opic
bio
psy
Pane
ndos
copy
Seco
ndar
y tra
chea
-eso
phag
eal
punc
ture
(TEP
)
Fore
ign
body
rem
oval
Esop
hagu
s di
lata
tion
Boto
x in
ject
ion
Scle
roth
erap
y
Nas
ogas
tric
tube
pla
cem
ent
Wire
less
pH
cap
sule
pla
cem
ent
Dila
tatio
nSe
cond
ary
TEP
Tran
scut
aneo
us
inje
ctio
n (u
pper
es
opha
geal
sph
inct
er)
Endo
scop
ic in
ject
ion
(low
er e
soph
agea
l sp
hinc
ter)
Rem
oval
Com
plic
atio
nEp
ista
xis
3-28
%
Nas
al p
ain
<2%
Vaso
vaga
l rea
ctio
n <2
%
Esop
hage
al p
erfo
ratio
n (2
cas
e re
ports
)
Esop
hage
al
perfo
ratio
n
Hae
mat
emes
is
Lary
ngos
pasm
Cre
atio
n fa
lse
ante
rior r
oute
Esop
hage
al s
teno
sis
Post
-pro
cedu
ral b
leed
ing
Phar
ynge
al m
ucos
a pe
netra
tion
Cel
lulit
is
Gra
nula
tion
Unk
now
nEs
opha
gus
perfo
ratio
n du
e to
sha
rp fo
reig
n bo
dy

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 57PDF page: 57PDF page: 57PDF page: 57
Office-based procedures for esophageal pathology
57
3
The most common complication during TNE under topical anesthesia is self-limited epistaxis, which occurs in less than 3% of the procedures among otolaryngologists(6, 21, 28, 82). Other possible complications are nasal pain during endoscope intubation and vasovagal reaction, both of which occur in less than 2% of the procedures(7, 21, 40, 41, 52, 82). The most feared complication during esophagoscopy is esophageal perforation. Although it is more frequently caused during rigid esophagoscopy, two cases of proximal esophageal perforation have occurred during TNE(36, 83). The performance of unsedated TNE causes less increase in blood pressure and heart rate compared to the transoral method(4, 35, 37, 47).
The costs of unsedated TNE are reported to be much lower compared to sedated transoral esophagoscopy, although Sabirin et al. stated that a robust cost-effectiveness analysis is still awaited(84). McPartlin et al. performed a cost analysis for TNE compared to the barium swallow examination(20). The authors concluded that after one year, the initial costs of purchasing the esophagoscope were fully met and from there on, £230 (82%) per patient is saved. Frieling et al. found pharmaceutical cost reduction of €18.489 per year for unsedated TN-EGD compared to sedated TN-EGD(31). Potential cost savings could come from reduction in radiology (barium swallow ± £150), follow-up (± £80) and esophagoscopy in general anesthesia (± £450)(76). When also considering indirect costs such as hours absent from work, an unsedated TNE could save up to $2000 per procedure(65).
Esophageal dilatationA benign esophageal stricture is a possible complication of, among others, gastro-esophageal reflux disease, ingestion of caustic agents, chemo-radiation therapy, or esophagitis(77, 78). For dilatations of these strictures, different techniques have been used, such as bougienage through a rigid endoscope by using Chevalier Jackson’s gum elastic bougies or Teflon bougies(77). Another method is dilating over a guidewire or with mercury weighted dilators, which do not need a wire(64, 77, 78). Since the introduction of balloon dilatation in 1981, this procedure has become an alternative method of esophageal dilatation(79-81). Rees described her technique for balloon dilatation, under topical anesthesia, by inserting the endoscope and guidewire transnasally and positioning them so the transparent dilating balloon could be visualized(79).
Stoddard and Simms performed 524 unsedated dilatations by using mercury weighted dilators in 109 patients with benign esophageal strictures(77). Patients tolerated the procedure well and only two patients could not swallow the dilators. Orenstein and Whitington performed 211 unsedated dilatations on 13 children using mercury dilators(78). All children showed

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 58PDF page: 58PDF page: 58PDF page: 58
Chapter 3
58
improved intake of solid foods after dilatation and parents reported a greater preference for dilatation without general anesthesia or sedation. In 40 patients with esophageal cancer, Lin et al. placed nasogastric feeding tubes with TNE guidance(26). In 12 patients (23 procedures) the tube placement failed, after which the authors performed esophageal dilatation by using Savary dilators. Rees reported on her experiences with transnasal balloon dilatation(80). Thirty-eight patients underwent 54 procedures, of which 20 were performed under topical anesthesia. Advantages of balloon dilatation are direct visualization of the dilated area, less gagging because of transnasal passage, and for a decreased need for sedation because of good patient tolerance under topical anesthesia.
The articles above mention no occurrence of esophageal perforation(77, 78, 80). Two patients had self-limiting hematemesis during mercury weighted dilators(77), one patient had self-limiting laryngospasm, and one patient experienced excessive gagging during balloon dilatation(80). Rees et al. reported no minor or major complications in the 40 performed balloon dilatations(79).
Secondary tracheo-esophageal puncture (TEP)In patients who underwent a laryngectomy, the formation of a tracheo-esophageal fistula sometimes resulted in intelligible speech. Although initially aspiration was a problem, Blom and Singer overcame this by developing a speech prosthesis with a one-way valve to place in the fistula. This prevented aspiration and resulted in proper air flow from the trachea to the pharynx(85). The formation of this fistula is often performed during the laryngectomy and is therefore called a primary tracheo-esophageal puncture (TEP).
In some cases, direct formation of the fistula is difficult and thus needs to be performed in a later stage. Indications are displayed in Table 1(86-89). This procedure is called a secondary TEP and used to be performed by using a rigid endoscope during general anesthesia(64, 89-91). With the development of adequate topical anesthesia techniques and minimal invasive instruments, this procedure can now be performed in an office-based setting.
Although there are several techniques described in the literature, all show similarity. A patient is seated and topically anesthetized in the nasal cavity, pharynx, and around the TEP site. In the past, a balloon catheter was transnasally introduced into the esophagus which produced a bulging in the posterior tracheal wall to mark the puncture(85). The puncture can be created using a syringe, after which a guidewire is placed into the puncture site. A dilator is placed over the guidewire to create a proper fistula(64, 85, 91-96). Some authors left the catheter in place within the fistula to mature, ranging from 1 to 14 days(85, 86, 90, 93, 96-99). Although, there are

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 59PDF page: 59PDF page: 59PDF page: 59
Office-based procedures for esophageal pathology
59
3
authors who placed the voice prosthesis directly after the fistula was created(64, 87, 89, 91, 100-
102). Hong described a technique were the patient lies down and an endoscope is inserted in the esophagus. The illumination of the tip of the endoscope marked the puncture site, after which air was blown into the esophagus to protect the posterior esophageal wall(90). A combination of the above described procedures can also be done by introducing the endoscope transorally over an intubation tube with a balloon. The light of the endoscope functions as a marker for the puncture site, and the balloon as protection of the posterior esophageal wall. A voice prosthesis is retrogradely placed, which means that the prosthesis is placed on the guidewire and pulled back through the mouth and esophagus and into the fistula(100). Iwai et al. used a perpendicular incision in the anterior esophageal wall to create a puncture under the direct vision of a transnasally inserted endoscope. The authors then used the endoscope with working channel to grasp a small catheter through the stoma by using biopsy forceps, and the catheter was pulled out of the mouth(101). More authors have since used a scalpel or curved hemostat to create the puncture site(64, 86, 89, 99, 102). Furthermore, with the recent development of flexible TNE with a working channel, air insufflation into the esophagus is possible; this results in minimal risk of posterior esophageal wall damage(86, 87,
89, 93, 95, 97-99). Fukuhara et al. described a method in which they created the TEP by passing a long needle through the working channel of the TNE and created the puncture(88).
Overall, the success percentages for in-office secondary TEP is high(86, 89, 97, 99-101). Several studies mention good patient tolerability under topical anesthesia(85, 88, 90, 100, 101) and find intelligible speech after voice prosthesis placement(85, 87, 91, 93, 94). The average duration of in-office secondary TEP is between 10 and 30 minutes(85, 88-90, 101, 102).
Although several studies reported no complications during the procedure(85, 87, 93, 101), the possible complications which can occur are not uniformly reported and are mentioned in Table 1(86, 89, 91, 94, 99, 100). The advantages of secondary TEP using flexible endoscopy are that the risks of general anesthesia are avoided, there is minimal stress to the patient, good visualization, short procedural duration with quick recovery, and the possibility of direct voice prosthesis placement(89, 92, 93, 98, 101, 103); although, the latter is also possible during primary TEP. By using a TNE, additional advantages include the ability to bypass esophageal strictures and screen for recurrent pathology(88, 102, 103).

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 60PDF page: 60PDF page: 60PDF page: 60
Chapter 3
60
Esophagus sphincter injectionAlthough not as routinely performed as an injection into the vocal cords, injection of the esophageal sphincter is possible. A transcutaneous method for the upper esophageal sphincter and a TNE-guided method for the lower esophageal sphincter have been described(104, 105).
Murry et al. performed transcutaneous botulinium toxin (Botox) injection into the cricopharyngeal muscle in 13 patients with upper esophageal sphincter dysfunction who did not respond to conventional swallowing therapy(104). A needle was inserted, under electromyography (EMG) guidance, percutaneously near the inferior border of the cricoid cartilage and was then advanced posteromedially following the contour of the cricoid cartilage. The patient was asked to vocalize, to rule out placement of the needle into the intrinsic laryngeal musculature, and was asked to tense the neck and tilt the head to rule out placement into the strap or paraspinal muscles. Eleven patients showed swallowing improvement within four weeks after the injection and two patients did not. Pre-procedural, six patients could not eat orally and were fed using percutaneous endoscopic gastrostomy feedings, five could eat orally, and two used both methods. Post-procedural, one patient could still not eat orally and nine could, whereas three were mixed. After a long term follow-up (mean, 26.5 weeks), all patients showed significant decrease in penetration and aspiration during swallowing examinations. Furthermore, the authors showed an overview of 8 articles which performed upper esophageal sphincter injections; 3 were under topical anesthesia using EMG or CT guidance(104). In those 3 articles, only 12 patients were treated and all showed functional improvement.
Rees described the technique of Botox injection in the lower esophageal sphincter through the working channel of a transnasal esophagoscope in patients with achalasia(105). Only topical anesthesia in the nasal cavity was necessary, although in patients with strong gag reflexes, viscous lidocaine, it was administered to the oropharynx. An endoscopic needle was passed through the working channel and Botox was injected, under direct vision, into the lower esophageal sphincter. Rees reviewed the literature on lower esophageal sphincter injection with Botox and reported the following predictors for success, age (older than 50 years), vigorous achalasia, initial clinical response, and manometric decrease in lower esophageal sphincter pressure after injection(105). Different outcomes were mentioned, such as success rates up to 70% after a mean 49-month follow-up; although, another study found 34% symptom free after 2 years. A Cochrane review compared pneumatic dilatation to Botox injection and found similar initial responses, but longer functional improvement following the dilation.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 61PDF page: 61PDF page: 61PDF page: 61
Office-based procedures for esophageal pathology
61
3
Foreign body removalAs described above, with the development of TNE with a working channel, more procedures are performed in an office-based setting under topical anesthesia. By using a 1.8-mm flexible forceps through the working channel, foreign bodies in the esophagus can be removed through either the nose or mouth(106-108). Abou-Nader et al. performed five foreign body removals using TNE(69). Sharp foreign bodies were difficult to remove due to the possibility of perforating the esophagus or upper respiratory tract. Bennett et al. performed five foreign body removals using TNE with forceps through the working channel and had 100% success in the removals(106).
Under direct vision through a laryngoscope, foreign bodies in the larynx or hypopharynx can also be removed using transorally inserted curved forceps(16, 109-112). Tai et al. removed foreign bodies in the larynx with transoral curved forceps in four patients and did not report any complications(109). In 117 patients with proven fish bone ingestion, Ngan et al. reported 21 directly removed foreign bodies and 82 using endoscopy(112). The mean hospital stay was 7 hours. Three patients showed morbidity on removal, one patient had a mucosal tear of the proximal esophagus, and two required more than 40 minutes to retrieve the foreign body. Kaygusuz et al. reported two patients with leeches in the larynx, which were removed with forceps and direct laryngoscopy under topical anesthesia(111). Van Hasselt et al. performed 78 foreign body removals using a flexible esophagoscope under topical anesthesia(113). The authors mentioned that 41% were retrieved and 33 complications occurred, of which 10 were major (i.e., esophageal perforation, neck abscess) and 23 minor (i.e., post-operative pyrexia, pharyngeal or esophageal ulcer). There was no mentioning in which group the complications occurred and how the foreign bodies were removed. In 138 children with coins ingested, Qayyum et al. performed 94 removals using a laryngoscope and crocodile forceps; no complications occurred(110).
Another method of foreign body removal is by blowing air through the working channel and passing the foreign body into the stomach(21, 107, 108, 114). This procedure should be avoided in case of sharp foreign bodies. Specific inspection of the mucosa after removal is critical, because of possible esophageal perforation and the subsequent possibility of developing mediastinitis(107). Among 302 patients with suspected foreign bodies, all underwent TNE because the lateral neck X-ray and laryngoscopy showed no foreign bodies(107). Fifty-two patients had a proven foreign body ingested; 36 were directly removed using forceps or advancement in the stomach. No major complications occurred. Woo and Kim performed 55 fish bone removals with TNE and flexible forceps and 10 by blowing air through the working channel of the endoscope(108).

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 62PDF page: 62PDF page: 62PDF page: 62
Chapter 3
62
Two studies mention the use of a balloon attached to a flexible endoscope to perform foreign body removals, therefore protecting the esophageal mucosa(114, 115). Jeen et al. reported on their experience with sharp foreign body removal in 22 patients, using a flexible endoscope with an oral side balloon attached to the end(114). By inflating the balloon just above the foreign body, the authors were able to push the foreign body into the stomach. The foreign body was then removed by using an endoscopic protector hood. In one patient, the procedure failed and in two cases, mild hemorrhage occurred. Sato and Nakashima reported on their use of three different video endoscopes (flexible video endoscopes equipped with and without a hood at their tips, and a rigid video endoscope) for foreign body removal(115). The forceps to obtain the foreign body was built in the endoscope. The flexible endoscope without a hood was inserted transnasally and the other transorally. Seventeen patients were examined. In the larynx, the endoscope without a hood should be used either transnasally or transorally. For foreign bodies in the upper portion of the hypopharynx, the video endoscope without a hood could be used either transnasally or transorally. In the lower portion of the hypopharynx, a video endoscope with a hood should be used with the oral approach.
DISCUSSION
The introduction of flexible distal chip laryngoscopes in combination with proper topical anesthesia has expanded the possibilities of transnasal office-based procedures in laryngology and head and neck oncology. Since the introduction of flexible esophagoscopes with a small diameter, transnasal examination of the esophagus under topical anesthesia is possible. This has led to an increase in the exploration of the diagnostic and therapeutic possibilities for the esophagus, as happened for the larynx when transnasal distal chip laryngoscopes became available. The most important factor for success in performing office-based procedures for the esophagus is patient acceptability. Adequate topical anesthesia and good patient instructions are vital to successful procedures.
With extensive knowledge of the nasal anatomy, laryngologists and head and neck surgeons are familiar with passing an endoscope through the nose. This has led to the emerging of TNE in laryngology and head and neck oncology(61). The procedure has considerable advantages compared to flexible transoral esophagoscopy, which are summarized above.
Dysphagia, globus, and screening for esophageal carcinoma are frequent indications in the outpatient clinic, for which diagnostic imaging such as barium swallow examination or a panendoscopy under general anesthesia is performed. Adequate biopsies of a suspected

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 63PDF page: 63PDF page: 63PDF page: 63
Office-based procedures for esophageal pathology
63
3
lesion are the key to a reliable histological diagnosis. In patients with diagnosed head and neck squamous cell carcinoma, incidence of esophageal carcinoma ranges between 0.8% and 15.9%, although the incidence may even be higher(21, 32, 43, 116). Whether or not patients with head and neck cancer should be screened for esophagus cancer is an ongoing matter of discussion(117). However, with the ease and short duration of TNE, one can state that it is less burdensome to perform this procedure. Furthermore, if TNE is performed instead of barium swallow examination to exclude esophageal pathology, this reduces an extra procedure, thus resulting in decreased diagnostic delay, cost savings, and avoiding the risk of radiation exposure(7, 56, 76). Standard screening can also be applied to specific types of head and neck cancer, such as hypopharyngeal carcinoma, where patients show a higher incidence of esophageal carcinoma compared to other upper respiratory anatomical sites(116, 118).
With the emergence of TNE, esophageal dilatation in outpatient clinics under topical anesthesia is another possible office-based procedure. Several authors concluded that balloon dilatation is more effective and feasible compared to the use of bougies in the office-based setting, with better visualization of the esophageal stricture and causing less trauma(79-81).
In the current literature search, we only found one study in which 20 unsedated balloon dilatations were performed in an office-based setting(80). Although it is possible that studies were missed in the search, based on the current information, balloon dilatation under topical anesthesia has not been adequately investigated.
Secondary TEP may be indicated in specific laryngectomy patients(86-89, 100). Different techniques have been described and no uniform protocols are mentioned. As seen in the literature, variations on techniques of long existing procedures are still being invented(95). There were no studies found in this literature search that investigate the effectiveness of different secondary TEP techniques. Also, randomized studies that compare direct voice prosthesis placement versus waiting on fistula maturation, were not found. Bergeron et al. mentioned the advantage of direct prosthesis placement; patients had less outpatient clinic visits to the speech-language pathologist compared to primary TEP(89). Damrose stated that by delaying voice prosthesis placement after secondary TEP, post-procedural edema could resolve(95). However, with the use of the more recent dilatational kits (e.g. Provox Vega® puncture set), direct placement of the prosthesis is possible with minimal edema. Patient motivation remains an important factor when performing secondary TEP under topical anesthesia, as seen by the possible complications(91).

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 64PDF page: 64PDF page: 64PDF page: 64
Chapter 3
64
All the different secondary TEP procedures have shown to be safe and effective, although they have not been investigated in large randomized study populations. In the designated patient population, this procedure could restore speech function.
Esophagus sphincter injection is a procedure which is infrequently performed. The authors of this review found only two studies which described different techniques for upper and lower esophagus sphincter injection. Botox injection in the esophageal sphincter may be an effective procedure for patients who do not respond to traditional therapy, such as medication or surgery(104, 105). Whether or not this procedure is more effective compared to standard therapies has not been investigated. For upper esophageal sphincter injection, one should have experience with EMG-guided procedures. Endoscopic upper sphincter injection has not yet been found in literature. For lower esophageal sphincter injection, again TNE is a useful tool in guiding the needle under direct vision. It remains to be seen whether or not this procedure will routinely be performed in the future.
The use of TNE provides a wide view of the larynx and esophagus and can therefore be efficient in rapid diagnosis and removal, when suspecting foreign body ingestion(107, 115). Foreign body removal using TNE should be used for selected foreign bodies(106). Which foreign bodies are safe to remove using TNE has not been defined; although one can imagine that sharp foreign bodies need extra care. Rapid diagnosis is sometimes lifesaving, as airway obstruction or esophageal perforation could have a high mortality risk(113, 114). Esophageal perforation because of a sharp foreign body is estimated to occur in 15% to 30% of cases(114). To protect the esophageal mucosa, several methods which use an inflated balloon for protection have been described(114, 115).
In most studies concerning foreign body removal, independent of the approach, is a small amount of patients being treated and incomplete documentation of the removal method. A large study comparing office-based foreign body removal to operation room performed removal is still awaited. One can imagine that foreign bodies located in the hypopharynx, larynx, and proximal esophagus can be easily removed using TNE.
This review of literature on office-based procedures for the esophagus is in extent to our previous work on office-based procedures for the larynx. Both reviews provide a detailed summary on the available office-based procedures in laryngology and head and neck oncology, and should be considered as a unity. This review has systematically searched and included all available articles on this subject. The possibility exists that articles that are

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 65PDF page: 65PDF page: 65PDF page: 65
Office-based procedures for esophageal pathology
65
3
in the scope for this review were missed in the literature search. Furthermore, we focused on procedures that were most reported on, or that are frequently performed by head and neck surgeons. Therefore, it is possible that not all available office-based procedures are reported in the current review. A methodological analysis was not performed due to the descriptive nature of this review, which could have resulted in more thorough conclusions.
The introduction of distal chip endoscopes has led to an increase in the use of office-based procedures of the esophagus. Transnasal esophagoscopy has been extensively investigated and shows better patient tolerability and equal diagnostic accuracy compared to flexible transoral esophagoscopy, as well as time and cost savings. Procedures such as secondary tracheo-esophageal puncture, esophageal dilatation, esophagus sphincter injection, and foreign body removal are less frequently investigated, but show promising results. These procedures should be performed in specific cases and by a clinician with proper experience in performing these procedures. Further studies need to be executed to investigate their feasibility, and diagnostic and therapeutic accuracy in the outpatient clinic. As in all office-based procedures, success depends upon adequate patient selection, clinician education and training, topical anesthesia, and patient instruction. With the ongoing refinement of procedural techniques and anesthesia, office-based procedures will continue to evolve into standard practice for laryngologists and head and neck surgeons.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 66PDF page: 66PDF page: 66PDF page: 66
Chapter 3
66
REFERENCES
1. Rosen CA, Amin MR, Sulica L, et al. Advances in office-based diagnosis and treatment in
laryngology. Laryngoscope 2009;119(SUPPL. 2):S185-S212.
2. Zeitels SM, Blitzer A, Hillman RE, Anderson RR. Foresight in laryngology and laryngeal surgery:
a 2020 vision. Ann Otol Rhinol Laryngol Supplement 2007;198:2-16.
3. Koufman JA. Introduction to office-based surgery in laryngology. Curr Opin Otolaryngol Head
Neck 2007;15(6):383-6.
4. Shaker R. Unsedated trans-nasal pharyngoesophagogastroduodenoscopy (T-EGD): technique.
Gastrointest Endosc 1994;40(3):346-8.
5. Marshall RE, Anggiansah A. Ambulatory oesophageal bile reflux monitoring in Barrett’s
oesophagus. Br J Surg 1996;83(3):425-6.
6. Aviv JE, Takoudes TG, Ma G, Close LG. Office-based esophagoscopy: a preliminary report.
Otolaryngol Head Neck Surg 2001;125(3):170-5.
7. Belafsky PC, Postma GN, Daniel E, Koufman JA. Transnasal esophagoscopy. Otolaryngol Head
Neck Surg 2001;125(6):588-9.
8. Herrmann IF, Recio SA. Laryngeal and Tracheal SurgeryFunctional pharyngoesophagoscopy:
A new technique for diagnostics and analyzing deglutition. Opere Tech Otolaryngo-Head Neck
Surg 1997;8(3):163-167.
9. Dua KS, Ruan E, Shaker R. Transnasal pharyngoesophagogastroduodenoscopy (T-PEGD) in a
patient with acute upper gastrointestinal bleeding. Endoscopy 1996;28(6):530.
10. Campo R, Brullet E, Montserrat A, et al. Identification of factors that influence tolerance of upper
gastrointestinal endoscopy. Eur J Gastroenterol Hepatol 1999;11(2):201-4.
11. Campo R, Montserrat A, Brullet E. Transnasal gastroscopy compared to conventional gastroscopy:
a randomized study of feasibility, safety, and tolerance. Endoscopy 1998;30(5):448-52.
12. Craig A, Hanlon J, Dent J, Schoeman M. A comparison of transnasal and transoral endoscopy
with small-diameter endoscopes in unsedated patients. Gastrointest Endosc 1999;49(3 Pt 1):292-
6.
13. Catanzaro A, Faulx A, Pfau PR, et al. Accuracy of a narrow-diameter battery-powered endoscope
in sedated and unsedated patients. Gastrointest Endosc 2002;55(4):484-7.
14. Saeian K, Staff D, Knox J, et al. Unsedated transnasal endoscopy: a new technique for
accurately detecting and grading esophageal varices in cirrhotic patients. Am J Gastroenterol
2002;97(9):2246-9.
15. Saeian K, Staff DM, Vasilopoulos S, et al. Unsedated transnasal endoscopy accurately detects
Barrett’s metaplasia and dysplasia. Gastrointest Endosc 2002;56(4):472-8.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 67PDF page: 67PDF page: 67PDF page: 67
Office-based procedures for esophageal pathology
67
3
16. Chu PY, Guo YC, Tai SK, Hwang JL, Tsai TL, Chang SY. Videofiberoptic examination of the
pharyngoesophageal segment and esophagus in patients after total laryngectomy. Head Neck
2003;25(10):858-863.
17. Ramadass T, Ayyaswamy G. Office based trans nasal esophagoscopy, and its role. Indian J
Otolaryngol Head Neck Surg 2003;55(4):238-41.
18. Andrus JG, Dolan RW, Anderson TD. Transnasal esophagoscopy: a high-yield diagnostic tool.
Laryngoscope 2005;115(6):993-6.
19. Kumar VV, Amin MR. Evaluation of middle and distal esophageal diverticuli with transnasal
esophagoscopy. Ann Otol Rhinol Laryngol 2005;114(4):276-8.
20. McPartlin DW, Nouraei SA, Tatla T, Howard DJ, Sandhu GS. How we do it: transnasal fibreoptic
oesophagoscopy. Clin Otolaryngol 2005;30(6):547-50.
21. Postma GN, Cohen JT, Belafsky PC, et al. Transnasal esophagoscopy: revisited (over 700
consecutive cases). Laryngoscope 2005;115(2):321-3.
22. Thota PN, Zuccaro G, Vargo JJ, Conwell DL, Dumot JA, Xu M. A randomized prospective trial
comparing unsedated esophagoscopy via transnasal and transoral routes using a 4-mm video
endoscope with conventional endoscopy with sedation. In: Endoscopy; 2005. p. 559-65.
23. Halum SL, Postma GN, Bates DD, Koufman JA. Incongruence between histologic and
endoscopic diagnoses of Barrett’s esophagus using transnasal esophagoscopy. Laryngoscope
2006;116(2):303-6.
24. Jobe BA, Hunter JG, Chang EY, et al. Office-based unsedated small-caliber endoscopy is
equivalent to conventional sedated endoscopy in screening and surveillance for Barrett’s
esophagus: a randomized and blinded comparison. Am J Gastroenterol 2006;101(12):2693-703.
25. Kim CY, O’Rourke RW, Chang EY, Jobe BA. Unsedated small-caliber upper endoscopy: an
emerging diagnostic and therapeutic technology. Surg Innov 2006;13(1):31-9.
26. Lin CH, Liu NJ, Lee CS, et al. Nasogastric feeding tube placement in patients with esophageal
cancer: application of ultrathin transnasal endoscopy. Gastrointest Endosc 2006;64(1):104-7.
27. Sharma A, Price T, Mierzwa K, Montgomery P, Qayyum A, Bradnam T. Transnasal flexible laryngo-
oesophagoscopy: an evaluation of the patient’s experience. J Laryngol Otol 2006;120(1):24-31.
28. Cho S, Arya N, Swan K, et al. Unsedated transnasal endoscopy: a Canadian experience in daily
practice. Can J Gastroenterol 2008;22(3):243-6.
29. O’Brien TJ, Parham K. Transnasal esophagoscopy: white-light versus narrowband imaging. Ann
Otol Rhinol Laryngol 2008;117(12):886-90.
30. Atkinson M, Chak A. Screening for Barrett’s Esophagus. Tech Gastrointest Endosc 2010;12(2):62-
66.
31. Frieling T, Schindler P, Kuhlbusch-Zicklam R, Heise J, Hulsdonk A, Kreysel C. Krefeld CONTRA
study: Conventional peroral esophago-gastro-duodenoscopy (EGD) vs. Transnasal EGD
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 68PDF page: 68PDF page: 68PDF page: 68
Chapter 3
68
a prospective and randomised study with independent evaluation of conscious sedation,
endoscope diameter, and access path. Z Gastroenterol 2010;48(8):818-824.
32. Su YY, Fang FM, Chuang HC, Luo SD, Chien CY. Detection of metachronous esophageal squamous
carcinoma in patients with head and neck cancer with use of transnasal esophagoscopy. Head
Neck 2010;32(6):780-5.
33. Chang JY, Talley NJ, Locke GR, 3rd, et al. Population screening for barrett esophagus: a
prospective randomized pilot study. Mayo Clin Proc 2011;86(12):1174-80.
34. Karkos PD, Thorley D, Kaptanis S, Issing WJ. Transnasal oesophagoscopy, laryngopharyngeal
reflux (LPR) and oesophageal pathology: the vocal fold granuloma example and ‘the granulomas,
LPR and Barrett’s triad’. Clin Otolaryngol 2011;36(5):516-7.
35. Kataoka H, Hayano J, Mizushima T, et al. Cardiovascular tolerance and autonomic nervous
responses in unsedated upper gastrointestinal small-caliber endoscopy: a comparison between
transnasal and peroral procedures with newly developed mouthpiece. Dig Endosc 2011;23(1):78-
85.
36. Moriwaki Y, Arata S, Iwashita M, Toyoda H, Kosuge T, Suzuki N. A case of cervical esophageal
perforation after transnasal gastrointestinal fibroscopy using a small-caliber fiber. Endoscopy
2011;43 Suppl 2 UCTN:E147-8.
37. Ai ZL, Lan CH, Fan LL, et al. Unsedated transnasal upper gastrointestinal endoscopy has
favorable diagnostic effectiveness, cardiopulmonary safety, and patient satisfaction compared
with conventional or sedated endoscopy. Surg Endosc 2012;26(12):3565-72.
38. Cheng CC, Fang TJ, Lee TJ, et al. Role of flexible transnasal esophagoscopy and patient
education in the management of globus pharyngeus. J Formos Med Assoc 2012;111(3):171-5.
39. Chung JW, Park S, Chung MJ, et al. A novel disposable, transnasal esophagoscope: a pilot trial
of feasibility, safety, and tolerance. Endoscopy 2012;44(2):206-9.
40. Peery AF, Hoppo T, Garman KS, et al. Feasibility, safety, acceptability, and yield of office-based,
screening transnasal esophagoscopy (with video). Gastrointest Endosc 2012;75(5):945-953.e2.
41. Shariff MK, Bird-Lieberman EL, O’Donovan M, et al. Randomized crossover study comparing
efficacy of transnasal endoscopy with that of standard endoscopy to detect Barrett’s esophagus.
Gastrointest Endosc 2012;75(5):954-61.
42. Siwiec RM, Dua K, Surapaneni SN, Hafeezullah M, Massey B, Shaker R. Unsedated transnasal
endoscopy with ultrathin endoscope as a screening tool for research studies. Laryngoscope
2012;122(8):1719-23.
43. Arantes V, Albuquerque W, Salles JM, et al. Effectiveness of unsedated transnasal endoscopy
with white-light, flexible spectral imaging color enhancement, and lugol staining for esophageal
cancer screening in high-risk patients. J Clin Gastroenterol 2013;47(4):314-21.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 69PDF page: 69PDF page: 69PDF page: 69
Office-based procedures for esophageal pathology
69
3
44. Dolan RW, Anderson TD. Practical applications of in-office fiberoptic transnasal esophagoscopy
in the initial evaluation of patients with squamous cell cancer of the head and neck. Ear Nose
Throat J 2013;92(9):450-5.
45. Gill AS, Long JL. Transnasal esophagoscopy and the diagnosis of a mediastinal foregut
duplication cyst. Ear Nose Throat Jl 2013;92(8):332-334.
46. Knuth J, Kunze DE, Benz C, et al. Is the transnasal access for esophagogastroduodenoscopy
in routine use equal to the transoral route? A prospective, randomized trial. Z Gastroenterol
2013;51(12):1369-1376.
47. Tsuboi M, Arai M, Maruoka D, et al. Utility and stability of transnasal endoscopy for examination
of the pharynx - a prospective study and comparison with transoral endoscopy. Int J Med Sci
2013;10(9):1085-91.
48. Tsuboi M, Arai M, Maruoka D, et al. Utility of unsedated transnasal endoscopy for pharyngeal
observation during esophagogastroduodenoscopy. A prospective study to assess
cardiopulmonary function. Scand J Gastroenterol 2013;48(7):884-9.
49. Wang CP, Tseng PH, Chen TC, et al. Transnasal esophagogastroduodenoscopy for evaluation
of upper gastrointestinal non-neoplastic disorders in patients with fresh hypopharyngeal cancer.
Laryngoscope 2013;123(4):975-979.
50. Aedo MR, Zavala-Gonzalez MA, Meixueiro-Daza A, Remes-Troche JM. Accuracy of transnasal
endoscopy with a disposable esophagoscope compared to conventional endoscopy. World J
Gastrointest Endosc 2014;6(4):128-36.
51. Alashkar B, Faulx AL, Hepner A, et al. Development of a program to train physician extenders
to perform transnasal esophagoscopy and screen for Barrett’s esophagus. Clin Gastroenterol
Hepatol 2014;12(5):785-92.
52. Chung EJ, Rho YS, Jung KY, Kim JW, Lee SW. The Role of Transnasal Esophagoscopy in ENT
Office: A Prospective, Multicenter Study in Korea. Clin Exp Otorhinolaryngol 2014;7(2):123-5.
53. Kadayifci A, Atar M, Parlar S, Balkan A, Koruk I, Koruk M. Transnasal endoscopy is preferred by
transoral endoscopy experienced patients. In: J Gastrointestin Liver Dis; 2014. p. 27-31.
54. Kawada K, Okada T, Sugimoto T, Kishimoto S, Kawano T. Intraoropharyngeal U-turn method
using transnasal esophagogastroduodenoscopy. Endoscopy 2014;46 Suppl 1 UCTN:E137-8.
55. Lin LF, Ma KZ, Tu HL. A prospective randomized study comparing transnasal and peroral 5-mm
ultrathin endoscopy. J Formos Med Assoc 2014;113(6):371-376.
56. Streckfuss A, Bosch N, Plinkert PK, Baumann I. Transnasal flexible esophagoscopy (TNE):
an evaluation of the patient’s experience and time management. Eur Arch Otorhinolaryngol
2014;271(2):323-8.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 70PDF page: 70PDF page: 70PDF page: 70
Chapter 3
70
57. Wang CH, Lee YC, Wang CP, et al. Use of transnasal endoscopy for screening of esophageal
squamous cell carcinoma in high-risk patients: yield rate, completion rate, and safety. Dig Endosc
2014;26(1):24-31.
58. Sami SS, Dunagan KT, Johnson ML, et al. A randomized comparative effectiveness trial of novel
endoscopic techniques and approaches for Barrett’s esophagus screening in the community.
Am J Gastroenterol 2015;110(1):148-58.
59. Sugimoto H, Kawai T, Naito S, et al. Surveillance of short-segment Barrett’s esophagus using
ultrathin transnasal endoscopy. J Gastroenterol Hepatol 2015;30 Suppl 1:41-5.
60. Wang WH, Tsai KY. Narrow-band imaging of laryngeal images and endoscopically proven reflux
esophagitis. Otolaryngol Head Neck Surg 2015;152(5):874-80.
61. Gooi Z, Ishman SL, Bock JM, Blumin JH, Akst LM. Changing Patterns in Reflux Care: 10-Year
Comparison of ABEA Members. Ann Otol Rhinol Laryngol 2015.
62. Shariff MK, Varghese S, O’Donovan M, et al. Pilot randomized crossover study comparing the
efficacy of transnasal disposable endosheath with standard endoscopy to detect Barrett’s
esophagus. Endoscopy 2016;48(2):110-6.
63. Belafsky PC. Office endoscopy for the laryngologist/bronchoesophagologist. Curr Opin
Otolaryngol Head Neck 2002;10(6):467-471.
64. Postma GN, Amin MR, Simpson CB, Belafsky PC. Office procedures for the esophagus. Ear Nose
Throat J 2004;83(7 Suppl 2):17-21.
65. Bush CM, Postma GN. Transnasal esophagoscopy. Otolaryngol Clin North Am 2013;46(1):41-
52.
66. Wang CT, Huang TW, Liao LJ, Lo WC, Lai MS, Cheng PW. Office-based potassium titanyl
phosphate laser-assisted endoscopic vocal polypectomy. JAMA Otolaryngol Head Neck Surg
2013;139(6):610-6.
67. Postma GN. Transnasal esophagoscopy. Curr Opin Otolaryngol Head Neck 2006;14(3):156-158.
68. Mokhashi MS, Wildi SM, Glenn TF, et al. A prospective, blinded study of diagnostic
esophagoscopy with a superthin, stand-alone, battery-powered esophagoscope. Am J
Gastroenterol 2003;98(11):2383-9.
69. Abou-Nader L, Wilson JA, Paleri V. Transnasal oesophagoscopy: diagnostic and management
outcomes in a prospective cohort of 257 consecutive cases and practice implications. Clin
Otolaryngol 2014;39(2):108-13.
70. Young VN, Smith LJ, Sulica L, Krishna P, Rosen CA. Patient tolerance of awake, in-office laryngeal
procedures: A Multi-Institutional Perspective. Laryngoscope 2012;122(2):315-321.
71. O’Connor JJ. Office esophagogastroduodenoscopy. Int Surg 2007;92(1):32-3.
72. Adler DG. Ultrathin transnasal endoscopy without sedation: The straight skinny. Gastrointest
Endosc 2012;75(5):962-964.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 71PDF page: 71PDF page: 71PDF page: 71
Office-based procedures for esophageal pathology
71
3
73. Mori A, Ohashi N, Yoshida A, et al. Unsedated transnasal ultrathin esophagogastroduodenoscopy
may provide betterdiagnostic performance in gastroesophageal reflux disease. Dis Esophagus
2011;24(2):92-98.
74. Friedman M, Schalch P, Vidyasagar R, Kakodkar KA, Mazloom N, Joseph NJ. Wireless upper
esophageal monitoring for laryngopharyngeal reflux (LPR). Otolaryngol Head Neck Surg
2007;137(3):471-6.
75. Zaman A, Hapke R, Sahagun G, Katon RM. Unsedated peroral endoscopy with a video ultrathin
endoscope: patient acceptance, tolerance, and diagnostic accuracy. Am J Gastroenterol
1998;93(8):1260-3.
76. Price T, Sharma A, Snelling J, et al. How we do it: The role of trans-nasal flexible laryngo-
oesophagoscopy (TNFLO) in ENT: one year’s experience in a head and neck orientated practice
in the UK. Clin Otolaryngol 2005;30(6):551-6.
77. Stoddard CJ, Simms JM. Dilatation of benign oesophageal strictures in the outpatient department.
Br J Surg 1984;71(10):752-753.
78. Orenstein SR, Whitington PF. Esophageal stricture dilatation in awake children. J Pediatr
Gastroenterol Nutr 1985;4(4):557-562.
79. Rees CJ. In-office unsedated transnasal balloon dilation of the esophagus and trachea. Curr
Opin Otolaryngol Head Neck 2007;15(6):401-4.
80. Rees CJ, Fordham T, Belafsky PC. Transnasal balloon dilation of the esophagus. Arch Otolaryngol
Head Neck Surg 2009;135(8):781-3.
81. Vaghela HM, Moir AA. Hydrostatic balloon dilatation of pharyngeal stricture under local
anaesthetic. J Laryngol Otol 2006;120(1):56-8.
82. Dumortier J, Napoleon B, Hedelius F, et al. Unsedated transnasal EGD in daily practice: results
with 1100 consecutive patients. Gastrointest Endosc 2003;57(2):198-204.
83. Zaman A. A randomized trial of peroral versus transnasal unsedated endoscopy using an ultrathin
videoendoscope. Gastrointest Endosc 1999;49(3):279.
84. Sabirin J, Abd Rahman M, Rajan P. Changing trends in oesophageal endoscopy: a systematic
review of transnasal oesophagoscopy. ISRN Otolaryngol 2013;2013:586973.
85. Bath AP, Toynton SC, Innes AJ. Technique of tracheo-oesophageal puncture under local
anaesthesia. J Laryngol Otol 1994;108(11):980-2.
86. Doctor VS, Enepekides DJ, Farwell DG, Belafsky PC. Transnasal oesophagoscopy-guided in-
office secondary tracheoesophageal puncture. J Laryngol Otol 2008;122(3):303-306.
87. Snelling JD, Price T, Montgomery PQ, Blagnys BL. How we do it: secondary tracheoesophageal
puncture under local anaesthetic, using a trans-nasal flexible laryngo-oesophagoscope (TNFLO).
Logoped Phoniatr Vocol 2007;32(2):80-2.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 72PDF page: 72PDF page: 72PDF page: 72
Chapter 3
72
88. Fukuhara T, Fujiwara K, Nomura K, Miyake N, Kitano H. New method for in-office secondary voice
prosthesis insertion under local anesthesia by reverse puncture from esophageal lumen. Ann
Otol Rhinol Laryngol 2013;122(3):163-8.
89. Bergeron JL, Jamal N, Erman A, Chhetri DK. Office-based tracheoesophageal puncture: updates
in techniques and outcomes. Am J Otolaryngol 2014;35(5):549-53.
90. Hong GS, John AB, Theobald D, Soo KC. Flexible endoscopic tracheo-oesophageal puncture
under local anaesthetic. J Laryngol Otol 1995;109(11):1077-9.
91. Desyatnikova S, Caro JJ, Andersen PE, Cohen JI, Wax MK. Tracheoesophageal puncture in the
office setting with local anesthesia. Ann Otol Rhinol Laryngol 2001;110(7 Pt 1):613-6.
92. Sidell D, Shamouelian D, Erman A, Gerratt BR, Chhetri D. Improved tracheoesophageal prosthesis
sizing in office-based tracheoesophageal puncture. Ann Otol Rhinol Laryngol 2010;119(1):37-41.
93. Sidell D, Ghadiali M, Chhetri DK. Unsedated office-based tracheoesophageal puncture using a
novel guidewire technique. Otolaryngol Head Neck Surg 2010;142(2):284-5.
94. Duvdevani SI, Talmi YP, Horowitz Z, Wolf M, Bedrin L. Secondary tracheoesophageal puncture
and myotomy--A novel outpatient technique. Head Neck 2012;34(5):717-20.
95. Damrose EJ, Cho DY, Goode RL. The hybrid tracheoesophageal puncture procedure: indications
and outcomes. Ann Otol Rhinol Laryngol 2014;123(8):584-90.
96. Spofford B, Jafek B, Barcz D. An improved method for creating tracheoesophageal fistulas from
Blom-Singer or Panje voice prostheses. Laryngoscope 1984;94(2 I):257-258.
97. LeBert B, McWhorter AJ, Kunduk M, et al. Secondary tracheoesophageal puncture with in-office
transnasal esophagoscopy. Arch Otolaryngol Head Neck Surg 2009;135(12):1190-4.
98. Allen J, Belafsky PC. Seldinger technique for in-office tracheoesophageal puncture. Ear Nose
Throat J l 2010;89(8):355-6.
99. Morrison MP, Chheda NN, Postma GN. The tough tracheoesophageal puncture. Am J Otolaryngol
2012;33(1):113-5.
100. Eerenstein SE, Schouwenburg PF. Secondary tracheoesophageal puncture with local anesthesia.
Laryngoscope 2002;112(4):634-7.
101. Iwai H, Yukawa H, Yamamoto T, et al. Secondary shunt procedure for alaryngeal patients in an
outpatient clinic. Acta Otolaryngol 2002;122(6):661-4.
102. Bach KK, Postma GN, Koufman JA. In-Office Tracheoesophageal Puncture Using Transnasal
Esophagoscopy.Laryngoscope 2003;113(1):173-176.
103. Doctor VS. In-office unsedated tracheoesophageal puncture. Curr Opin Otolaryngol Head Neck
2007;15(6):405-8.
104. Murry T, Wasserman T, Carrau RL, Castillo B. Injection of botulinum toxin A for the treatment of
dysfunction of the upper esophageal sphincter. Am J Otolaryngol2005;26(3):157-62.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 73PDF page: 73PDF page: 73PDF page: 73
Office-based procedures for esophageal pathology
73
3
105. Rees CJ. In-office transnasal esophagoscope-guided botulinum toxin injection of the lower
esophageal sphincter. Curr Opin Otolaryngol Head Neck 2007;15(6):409-11.
106. Bennett AM, Sharma A, Price T, Montgomery PQ. The management of foreign bodies in the
pharynx and oesophagus using transnasal flexible laryngo-oesophagoscopy (TNFLO). Ann R
Coll Surg Engl 2008;90(1):13-6.
107. Shih CW, Hao CY, Wang YJ, Hao SP. A New Trend in the Management of Esophageal Foreign
Body: Transnasal Esophagoscopy. Otolaryngol Head Neck Surg 2015;153(2):189-92.
108. Woo SH, Kim KH. Proposal for methods of diagnosis of fish bone foreign body in the Esophagus.
Laryngoscope 2015;125(11):2472-5.
109. Tai SK, Chu PY, Chang SY. Transoral laryngeal surgery under flexible laryngovideostroboscopy.
J Voice 1998;12(2):233-8.
110. Qayyum MK, Farzooq A, Munir A, Sajid M. Removal of foreign body coin from upper end of
oesophagus: Is general anaesthesia always needed? Pak J Med Health Sci 2014;8(2):440-441.
111. Kaygusuz I, Yalcin S, Keles E. Leeches in the larynx. Eur Arch Otorhinolaryngol 2001;258(9):455-
457.
112. Ngan JH, Fok PJ, Lai EC, Branicki FJ, Wong J. A prospective study on fish bone ingestion.
Experience of 358 patients. Ann Surg 1990;211(4):459-62.
113. Van Hasselt CA. Management of ingested foreign bodies: A retrospective review of 5240 patients.
J Laryngol Otol 2001;115(12):954-957.
114. Jeen YT, Chun HJ, Song CW, et al. Endoscopic removal of sharp foreign bodies impacted in the
esophagus. Endoscopy 2001;33(6):518-22.
115. Sato K, Nakashima T. Office-based foreign-body management using videoendoscope. Am J
Otolaryngol 2004;25(3):167-72.
116. Su YY, Chen WC, Chuang HC, et al. Effect of routine esophageal screening in patients with head
and neck cancer. JAMA Otolaryngol Head Neck Surg 2013;139(4):350-4.
117. Roof SA, Amin MR. Transnasal esophagoscopy in modern head and neck surgery. Curr Opin
Otolaryngol Head Neck 2015;23(2):171-5.
118. Bradley PJ, Bradley PT. Searching for metachronous tumours in patients with head and neck
cancer: the ideal protocol! Curr Opin Otolaryngol Head Neck 2010;18(2):124-33.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 74PDF page: 74PDF page: 74PDF page: 74
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 75PDF page: 75PDF page: 75PDF page: 75
Chapter 4Topical anesthesia for endoscopic office-based procedures
of the upper aerodigestive tract
David J. Wellenstein MD1 , Raymond A.B. van der Wal MD2, Henrieke W. Schutte MD1, Jimmie Honings MD PhD1, Frank J.A. van den Hoogen MD PhD1, Henri A.M. Marres MD
PhD1, Robert P. Takes MD PhD1, Guido B. van den Broek MD PhD1
1 Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands2 Department of Anesthesiology, Radboud university medical center, Nijmegen, The Netherlands
Journal of Voice. 2019 Sep;33(5):732-746.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 76PDF page: 76PDF page: 76PDF page: 76
Chapter 4
76
ABSTRACT
ObjectiveOver the last two decades, an increase in office-based procedures under topical anesthesia in laryngology and head and neck oncology has occurred. Adequate anesthesia in the nasal cavity, pharynx, and larynx is essential for successful performance of these procedures. Our goal is to provide an objective summary on the available local anesthetics, methods of application, local secondary effects, efficacy, and complications.
Material and MethodsA descriptive review of literature on topical anesthesia for office-based procedures in laryngology and head and neck oncology was performed.
ResultsLidocaine is the most applied and investigated topical anesthetic. Topical anesthesia results in decreased sensory function without impairing motor function of the pharynx and larynx. For the nasal cavity, cotton pledgets soaked in anesthetic spray and decongestant, or anesthetic gel, are effective. For the pharynx, anesthetic spray is the most frequently used and effective method. For the larynx, applying local anesthesia through a catheter through the working channel of the endoscope or anesthetic injection through the cricothyroid membrane is effective. Studies comparing the most effective application methods for each anatomical site are lacking. Complications of topical lidocaine administration are rare.
ConclusionsBy properly applying topical anesthesia to the upper aerodigestive tract, several surgical procedures in laryngology and head and neck oncology can be performed in the outpatient clinic under topical anesthesia instead of the operating room under general anesthesia. Lidocaine is the most investigated anesthetic, with adequate efficacy and few complications. Studies that determine the most effective application methods are still wanting.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 77PDF page: 77PDF page: 77PDF page: 77
Topical anesthesia for office-based procedures
77
4
INTRODUCTION
The use of topical anesthesia, in combination with the more recent development of flexible transnasal laryngoscopes with a working channel, has led to an increase in performance of so-called office-based procedures in laryngology and head and neck oncology over the past 2 decades(1, 2). Currently, a wide variety of procedures are performed under topical anesthesia, such as flexible endoscopic biopsy, transnasal esophagoscopy, and endoscopic laser surgery(3, 4). To successfully perform office-based procedures, patient cooperation and adequate topical anesthesia are essential(5).
Cocaine was the first agent used to provide local anesthesia for the upper aerodigestive tract in the late 19th century. The method of action of local anesthetics is based on the blocking of voltage-gated sodium channels that are present on the cell membranes of nerves and muscles. Blocking of these channels prevents initiation or propagation of action potentials thereby achieving local anesthesia(6). Since the introduction of cocaine as a local anesthetic, a spectrum of new synthetic topical anesthetics have been developed, which are summarized for the upper aerodigestive tract in Table 1.
With the wide variety of local anesthetics available, it remains unclear which local anesthetics and which methods of application are available and provide the best conditions for office-based procedures of the upper aerodigestive tract. Therefore, we conducted a systematic literature search to try to answer these questions in a descriptive review, for office-based procedures of the pharynx and larynx. For each anatomical site, the most frequently used anesthetics, the available methods of application, and local secondary effects are highlighted. Furthermore, efficacy and safety of topical anesthesia of the upper aerodigestive tract are outlined. Our purpose is to provide an objective summary of the available literature, to be used for guidance of physicians who are interested in performing office-based procedures for the pharynx and larynx.
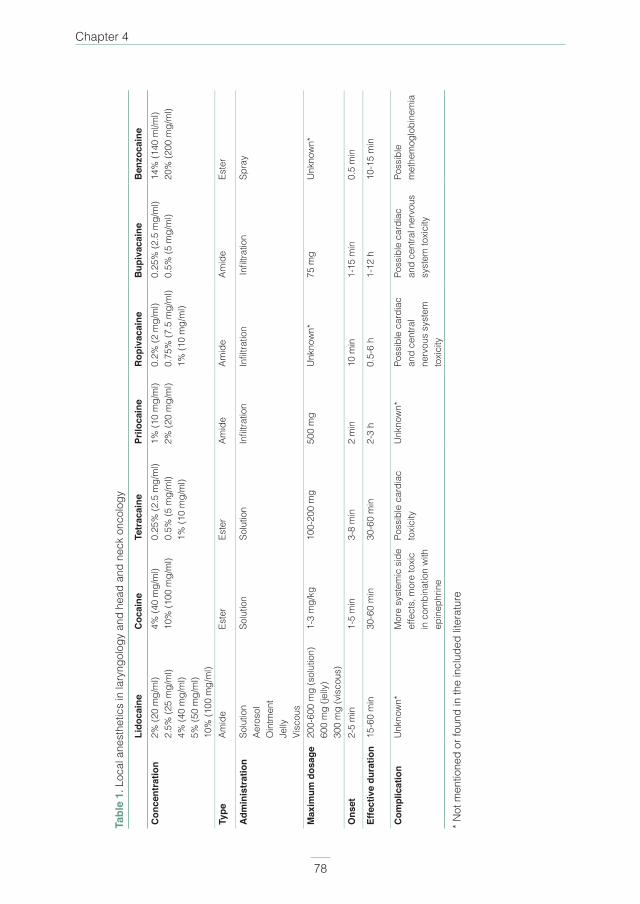
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 78PDF page: 78PDF page: 78PDF page: 78
Chapter 4
78
Tabl
e 1.
Loc
al a
nest
hetic
s in
lary
ngol
ogy
and
head
and
nec
k on
colo
gy
Li
doca
ine
Coc
aine
Tetr
acai
ne
Prilo
cain
e R
opiv
acai
ne
Bup
ivac
aine
B
enzo
cain
eC
once
ntra
tion
2% (2
0 m
g/m
l) 2.
5% (2
5 m
g/m
l)4%
(40
mg/
ml)
5% (5
0 m
g/m
l)10
% (1
00 m
g/m
l)
4% (4
0 m
g/m
l)10
% (1
00 m
g/m
l)0.
25%
(2.5
mg/
ml)
0.5%
(5 m
g/m
l)1%
(10
mg/
ml)
1% (1
0 m
g/m
l)2%
(20
mg/
ml)
0.2%
(2 m
g/m
l)0.
75%
(7.5
mg/
ml)
1% (1
0 m
g/m
l)
0.25
% (2
.5 m
g/m
l)0.
5% (5
mg/
ml)
14%
(140
ml/m
l)20
% (2
00 m
g/m
l)
Type
Am
ide
Este
rEs
ter
Amid
eAm
ide
Amid
eEs
ter
Adm
inis
trat
ion
Solu
tion
Aero
sol
Oin
tmen
tJe
llyVi
scou
s
Solu
tion
Solu
tion
Infil
tratio
nIn
filtra
tion
Infil
tratio
nSp
ray
Max
imum
dos
age
200-
600
mg
(sol
utio
n)60
0 m
g (je
lly)
300
mg
(vis
cous
)
1-3
mg/
kg10
0-20
0 m
g50
0 m
gU
nkno
wn*
75 m
gU
nkno
wn*
Ons
et2-
5 m
in1-
5 m
in3-
8 m
in2
min
10 m
in1-
15 m
in0.
5 m
in
Effe
ctiv
e du
ratio
n15
-60
min
30-6
0 m
in30
-60
min
2-3
h0.
5-6
h1-
12 h
10-1
5 m
in
Com
plic
atio
nU
nkno
wn*
Mor
e sy
stem
ic s
ide
effe
cts,
mor
e to
xic
in c
ombi
natio
n w
ith
epin
ephr
ine
Poss
ible
car
diac
to
xici
tyU
nkno
wn*
Poss
ible
car
diac
an
d ce
ntra
l ne
rvou
s sy
stem
to
xici
ty
Poss
ible
car
diac
an
d ce
ntra
l ner
vous
sy
stem
toxi
city
Poss
ible
m
ethe
mog
lobi
nem
ia
* Not
men
tione
d or
foun
d in
the
incl
uded
lite
ratu
re
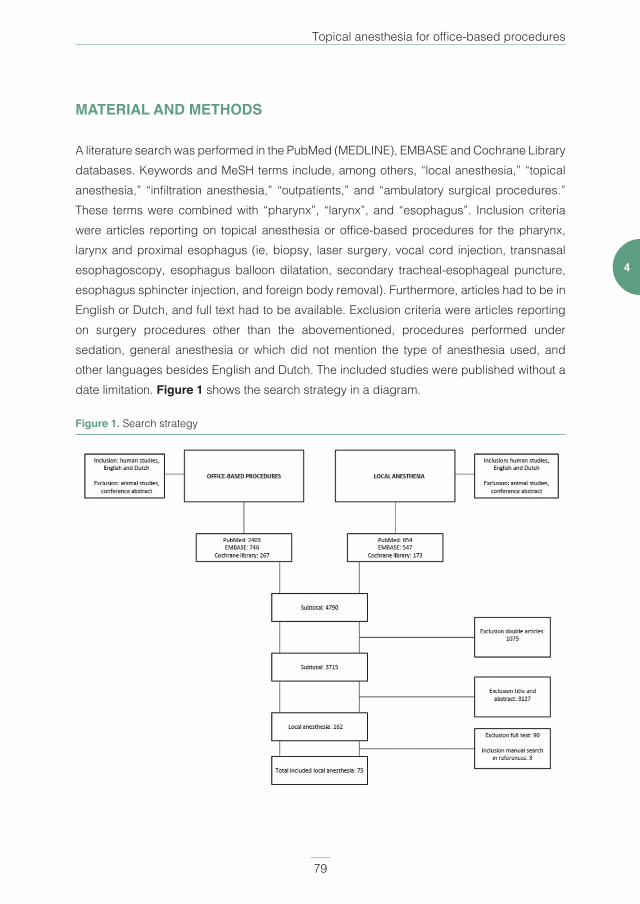
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 79PDF page: 79PDF page: 79PDF page: 79
Topical anesthesia for office-based procedures
79
4
MATERIAL AND METHODS
A literature search was performed in the PubMed (MEDLINE), EMBASE and Cochrane Library databases. Keywords and MeSH terms include, among others, “local anesthesia,” “topical anesthesia,” “infiltration anesthesia,” “outpatients,” and “ambulatory surgical procedures.” These terms were combined with “pharynx”, “larynx”, and “esophagus”. Inclusion criteria were articles reporting on topical anesthesia or office-based procedures for the pharynx, larynx and proximal esophagus (ie, biopsy, laser surgery, vocal cord injection, transnasal esophagoscopy, esophagus balloon dilatation, secondary tracheal-esophageal puncture, esophagus sphincter injection, and foreign body removal). Furthermore, articles had to be in English or Dutch, and full text had to be available. Exclusion criteria were articles reporting on surgery procedures other than the abovementioned, procedures performed under sedation, general anesthesia or which did not mention the type of anesthesia used, and other languages besides English and Dutch. The included studies were published without a date limitation. Figure 1 shows the search strategy in a diagram.
Figure 1. Search strategy

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 80PDF page: 80PDF page: 80PDF page: 80
Chapter 4
80
The initial search was conducted in April 2016, which identified 4790 articles. Duplicate articles were removed, leaving 3715 articles. Four hundred and seventy-six articles were included; full text articles were obtained using the stated databases, Google Scholar, and the institutional medical library. Five articles could not be obtained through the medical library and thus were excluded.
After reading all of the full texts, 72 articles were included. Three articles were added after searching through the references of the included articles. This resulted in a total of 75 articles included for this review.
RESULTS
Topical anesthesia of the nasal cavityFor the nose, a combination of a local anesthetic with a vasoconstricting and decongesting component (eg, oxymetazoline or epinephrine) can be used in spray or drained in cotton pledgets(7-12). Although no studies were found that investigated the most effective duration of leaving cotton pledgets in the nasal cavity, up to 15 minutes has been reported(10). The included studies did not mention the maximum dosage of topical anesthesia that can be safely applied in the nasal cavity. Anesthetic gel is an alternative to spray or gauze pledgets(13). Table 2 provides an overview of included studies that investigated topical anesthesia for the nasal cavity(12-15).
Gauze pledgets soaked in local anesthesia or anesthetic gel seem to provide more adequate nasal anesthesia compared with anesthetic spray, when a wide diameter transnasal endoscope (eg, transnasal laryngoscope with working channel or esophagoscope) is used(12, 13). Although transnasal laryngoscopes usually have a smaller outer diameter compared with transnasal laryngoscopes with working channel or transnasal esophagoscopes, Özkiriş et al still found that topical nasal anesthesia with gauze pledgets resulted in less nasal pain (measured with visual analogue score) during endoscope insertion compared with a saline solution, for a transnasal laryngoscope with a 4.2-mm diameter. The authors did not investigate the effect of topical anesthesia for the pharynx or larynx. The results of the study by Frosh et al showed, that when an even smaller transnasal laryngoscope (ie, 3.7-mm diameter) is used, topical anesthetic spray is no longer beneficial for nasal pain reduction upon endoscope insertion(15).
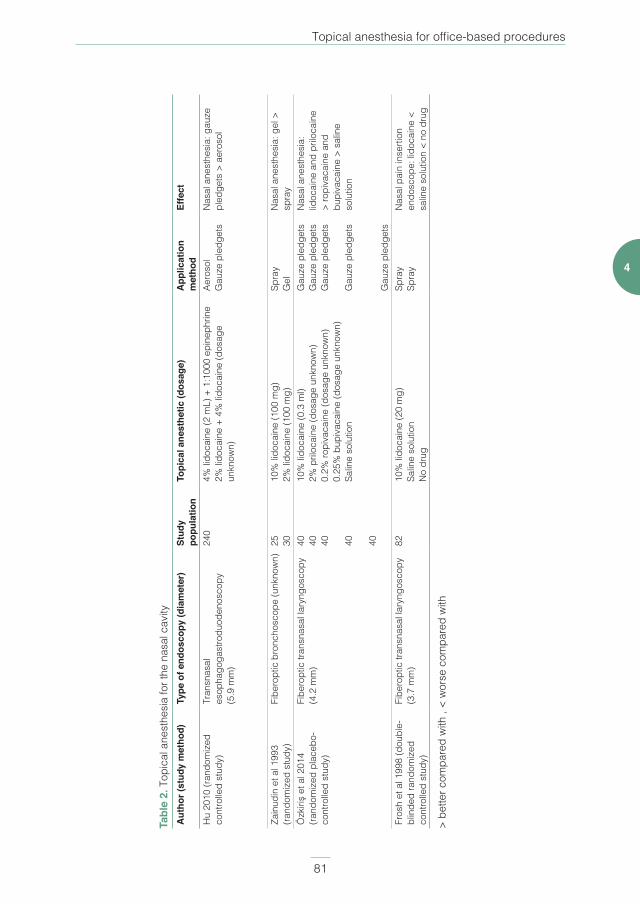
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 81PDF page: 81PDF page: 81PDF page: 81
Topical anesthesia for office-based procedures
81
4
Tabl
e 2.
Top
ical
ane
sthe
sia
for t
he n
asal
cav
ityA
utho
r (st
udy
met
hod)
Type
of e
ndos
copy
(dia
met
er)
Stud
y po
pula
tion
Topi
cal a
nest
hetic
(dos
age)
App
licat
ion
met
hod
Effe
ct
Hu
2010
(ran
dom
ized
co
ntro
lled
stud
y)Tr
ansn
asal
es
opha
goga
stro
duod
enos
copy
(5
.9 m
m)
240
4% li
doca
ine
(2 m
L) +
1:1
000
epin
ephr
ine
2% li
doca
ine
+ 4%
lido
cain
e (d
osag
e un
know
n)
Aero
sol
Gau
ze p
ledg
ets
Nas
al a
nest
hesi
a: g
auze
pl
edge
ts >
aer
osol
Zain
udin
et a
l 199
3 (ra
ndom
ized
stu
dy)
Fibe
ropt
ic b
ronc
hosc
ope
(unk
now
n)25 30
10%
lido
cain
e (1
00 m
g)2%
lido
cain
e (1
00 m
g)Sp
ray
Gel
Nas
al a
nest
hesi
a: g
el >
sp
ray
Özk
iriş
et a
l 201
4 (ra
ndom
ized
pla
cebo
-co
ntro
lled
stud
y)
Fibe
ropt
ic tr
ansn
asal
lary
ngos
copy
(4
.2 m
m)
40 40 40 40 40
10%
lido
cain
e (0
.3 m
l)2%
pril
ocai
ne (d
osag
e un
know
n)0.
2% ro
piva
cain
e (d
osag
e un
know
n)0.
25%
bup
ivac
aine
(dos
age
unkn
own)
Salin
e so
lutio
n
Gau
ze p
ledg
ets
Gau
ze p
ledg
ets
Gau
ze p
ledg
ets
Gau
ze p
ledg
ets
Gau
ze p
ledg
ets
Nas
al a
nest
hesi
a:
lidoc
aine
and
pril
ocai
ne
> ro
piva
cain
e an
d bu
piva
cain
e >
salin
e so
lutio
n
Fros
h et
al 1
998
(dou
ble-
blin
ded
rand
omiz
ed
cont
rolle
d st
udy)
Fibe
ropt
ic tr
ansn
asal
lary
ngos
copy
(3
.7 m
m)
8210
% li
doca
ine
(20
mg)
Salin
e so
lutio
nN
o dr
ug
Spra
ySp
ray
Nas
al p
ain
inse
rtion
en
dosc
ope:
lido
cain
e <
salin
e so
lutio
n <
no d
rug
> be
tter c
ompa
red
with
, <
wor
se c
ompa
red
with
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 82PDF page: 82PDF page: 82PDF page: 82
Chapter 4
82
Topical anesthesia of the pharynxStudies investigating the anesthetic effect of topical anesthesia on the pharynx during transoral endoscopy are summarized in Table 3(16-27). Spraying of the pharynx is one of the oldest and most used methods of topical anesthesia. By spraying the oral cavity first, the patient gets acquired to the bitter taste and effect of the anesthetic(9, 11). Afterward, spraying in the oropharynx while letting the patient inhale deeply often results in coughing and thus spreading of the anesthetic in the pharynx and larynx(9). Alternative methods for topical anesthesia of the pharynx are anesthetic lozenges(26) or gargling of a viscous anesthetic solution, which should not be swallowed for at least 5 minutes(8, 25, 27). After all pharyngeal and laryngeal anesthesia administration, patients should be advised to remain nil per os for 60 minutes after application to prevent aspiration(5, 7). Studies that compared different application methods found anesthetic spray to result in more adequate pharyngeal anesthesia, compared with alternative application methods.
Different types of topical anesthetics used and compared with sedation, placebo or a control group and are summarized in Table 3. Overall, lidocaine was the most investigated topical anesthetic. Lidocaine resulted in less discomfort for patients during endoscopy, and endoscopists found the procedure easier to perform, compared with placebo or no anesthesia. When sedation was used, patients experienced less discomfort compared with topical anesthesia, although again endoscopists found the procedure better to perform under topical anesthesia.
Several studies investigated the effect of topical anesthesia on sensory and motor function of the pharynx. Ertekin et al investigated the effect of 220-240 mg lidocaine spray on swallowing function in 12 healthy volunteers(28). The participants received sips of water ranging from 3 to 20 ml. Laryngeal movements were measured using a piezoelectric (ie, electricity resulting from pressure) device. Five volunteers showed early-stage aspiration and only one volunteer swallowed 20 ml of water, after which dysphagia occurred. The effect of anesthesia lasted 3-6 minutes. Chee et al investigated the effect of topical anesthesia on pharyngeal swallowing and sensation(29). Twenty participants randomly received placebo, 10 mg, 20 mg, and 40 mg of lidocaine spray once, each on different days. Afterward they underwent swallowing and sensation tests. Sensation was significantly affected for the 20-mg, and 40-mg doses, but not for the 10-mg dose. The 40-mg dose lasted for 60 minutes, whereas the 20 mg dose lasted 30 minutes, which significantly differed. Although swallowing capacity was not significantly affected, the swallowing speed was significantly reduced in all groups and mostly with 40 mg of lidocaine. Mansson and Sandberg compared topical anesthesia
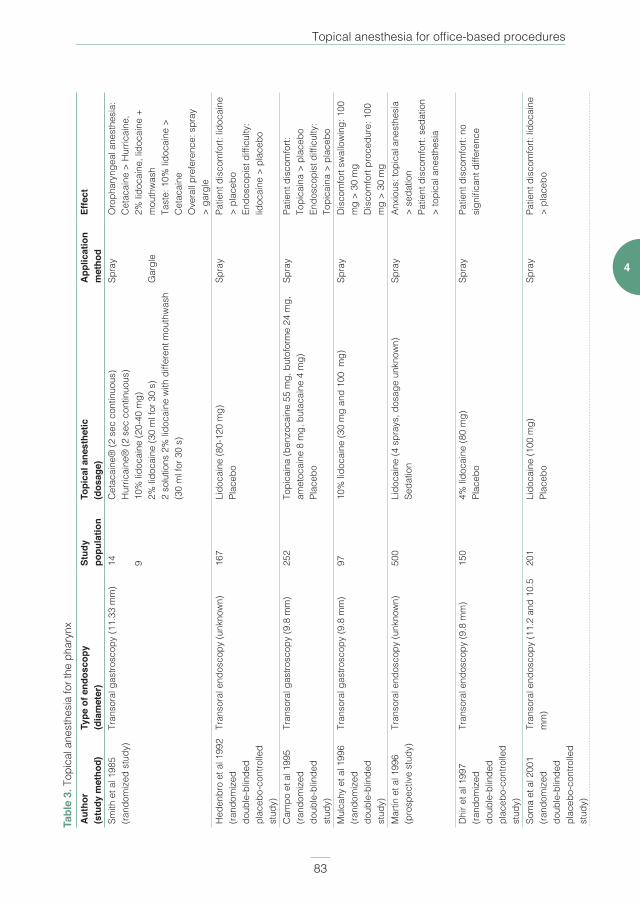
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 83PDF page: 83PDF page: 83PDF page: 83
Topical anesthesia for office-based procedures
83
4
Tabl
e 3.
Top
ical
ane
sthe
sia
for t
he p
hary
nxA
utho
r (s
tudy
met
hod)
Type
of e
ndos
copy
(d
iam
eter
)St
udy
popu
latio
nTo
pica
l ane
sthe
tic
(dos
age)
App
licat
ion
met
hod
Effe
ct
Smith
et a
l 198
5 (ra
ndom
ized
stu
dy)
Tran
sora
l gas
trosc
opy
(11.
33 m
m)
14 9
Cet
acai
ne®
(2 s
ec c
ontin
uous
) H
urric
aine
® (2
sec
con
tinuo
us)
10%
lido
cain
e (2
0-40
mg)
2% li
doca
ine
(30
ml f
or 3
0 s)
2 so
lutio
ns 2
% li
doca
ine
with
diff
eren
t mou
thw
ash
(30
ml f
or 3
0 s)
Spra
y G
argl
e
Oro
phar
ynge
al a
nest
hesi
a:
Cet
acai
ne >
Hur
ricai
ne,
2% li
doca
ine,
lido
cain
e +
mou
thw
ash
Tast
e: 1
0% li
doca
ine
>
Cet
acai
neO
vera
ll pr
efer
ence
: spr
ay
> ga
rgle
Hed
enbr
o et
al 1
992
(rand
omiz
ed
doub
le-b
linde
d pl
aceb
o-co
ntro
lled
stud
y)
Tran
sora
l end
osco
py (u
nkno
wn)
167
Lido
cain
e (8
0-12
0 m
g)Pl
aceb
oSp
ray
Patie
nt d
isco
mfo
rt: li
doca
ine
> pl
aceb
oEn
dosc
opis
t diffi
culty
: lid
ocai
ne >
pla
cebo
Cam
po e
t al 1
995
(rand
omiz
ed
doub
le-b
linde
d st
udy)
Tran
sora
l gas
trosc
opy
(9.8
mm
)25
2To
pica
ina
(ben
zoca
ine
55 m
g, b
utof
orm
e 24
mg,
am
etoc
aine
8 m
g, b
utac
aine
4 m
g)Pl
aceb
o
Spra
yPa
tient
dis
com
fort:
To
pica
ina
> pl
aceb
oEn
dosc
opis
t diffi
culty
: To
pica
ina
> pl
aceb
oM
ulca
hy e
t al 1
996
(rand
omiz
ed
doub
le-b
linde
d st
udy)
Tran
sora
l gas
trosc
opy
(9.8
mm
)97
10%
lido
cain
e (3
0 m
g an
d 10
0 m
g)Sp
ray
Dis
com
fort
swal
low
ing:
100
m
g >
30 m
gD
isco
mfo
rt pr
oced
ure:
100
m
g >
30 m
gM
artin
et a
l 199
6(p
rosp
ectiv
e st
udy)
Tran
sora
l end
osco
py (u
nkno
wn)
500
Lido
cain
e (4
spr
ays,
dos
age
unkn
own)
Seda
tion
Spra
yAn
xiou
s: to
pica
l ane
sthe
sia
> se
datio
nPa
tient
dis
com
fort:
sed
atio
n >
topi
cal a
nest
hesi
a
Dhi
r et a
l 199
7(ra
ndom
ized
do
uble
-blin
ded
plac
ebo-
cont
rolle
d st
udy)
Tran
sora
l end
osco
py (9
.8 m
m)
150
4% li
doca
ine
(80
mg)
Pl
aceb
oSp
ray
Patie
nt d
isco
mfo
rt: n
o si
gnifi
cant
diff
eren
ce
Som
a et
al 2
001
(rand
omiz
ed
doub
le-b
linde
d pl
aceb
o-co
ntro
lled
stud
y)
Tran
sora
l end
osco
py (1
1.2
and
10.5
m
m)
201
Lido
cain
e (1
00 m
g)Pl
aceb
oSp
ray
Patie
nt d
isco
mfo
rt: li
doca
ine
> pl
aceb
o
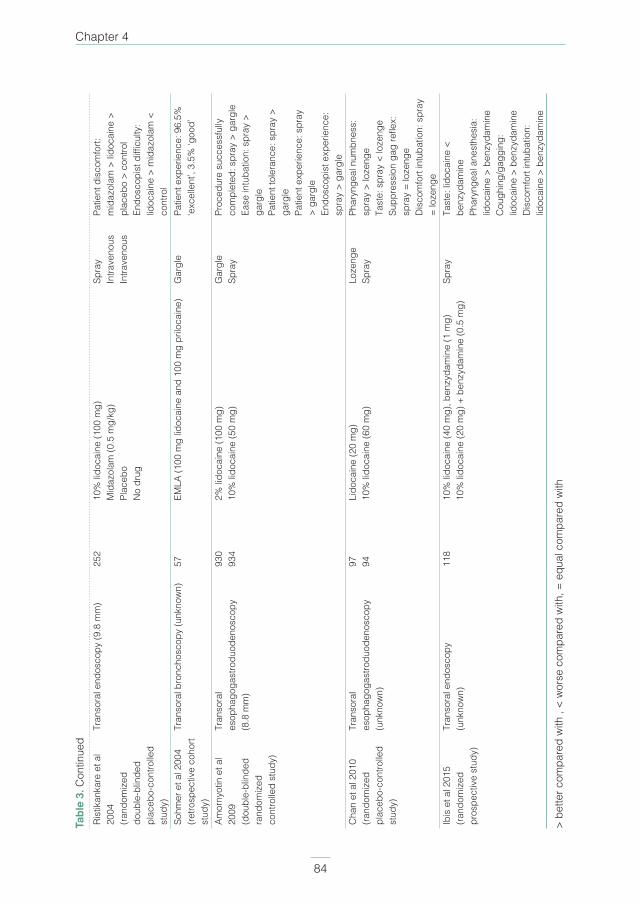
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 84PDF page: 84PDF page: 84PDF page: 84
Chapter 4
84
Rist
ikan
kare
et a
l 20
04(ra
ndom
ized
do
uble
-blin
ded
plac
ebo-
cont
rolle
d st
udy)
Tran
sora
l end
osco
py (9
.8 m
m)
252
10%
lido
cain
e (1
00 m
g)M
idaz
olam
(0.5
mg/
kg)
Plac
ebo
No
drug
Spra
yIn
trave
nous
Intra
veno
us
Patie
nt d
isco
mfo
rt:
mid
azol
am >
lido
cain
e >
plac
ebo
> co
ntro
lEn
dosc
opis
t diffi
culty
: lid
ocai
ne >
mid
azol
am <
co
ntro
lSo
hmer
et a
l 200
4(re
trosp
ectiv
e co
hort
stud
y)
Tran
sora
l bro
ncho
scop
y (u
nkno
wn)
57EM
LA (1
00 m
g lid
ocai
ne a
nd 1
00 m
g pr
iloca
ine)
Gar
gle
Patie
nt e
xper
ienc
e: 9
6.5%
‘e
xcel
lent
’, 3.
5% ‘g
ood’
Amor
nyot
in e
t al
2009
(dou
ble-
blin
ded
rand
omiz
ed
cont
rolle
d st
udy)
Tran
sora
l es
opha
goga
stro
duod
enos
copy
(8
.8 m
m)
930
934
2% li
doca
ine
(100
mg)
10%
lido
cain
e (5
0 m
g)G
argl
eSp
ray
Proc
edur
e su
cces
sful
ly
com
plet
ed: s
pray
> g
argl
eEa
se in
tuba
tion:
spr
ay >
ga
rgle
Patie
nt to
lera
nce:
spr
ay >
ga
rgle
Patie
nt e
xper
ienc
e: s
pray
>
garg
leEn
dosc
opis
t exp
erie
nce:
sp
ray
> ga
rgle
Cha
n et
al 2
010
(rand
omiz
ed
plac
ebo-
cont
rolle
d st
udy)
Tran
sora
l
esop
hago
gast
rodu
oden
osco
py
(unk
now
n)
97 94Li
doca
ine
(20
mg)
10%
lido
cain
e (6
0 m
g)Lo
zeng
eSp
ray
Phar
ynge
al n
umbn
ess:
sp
ray
> lo
zeng
eTa
ste:
spr
ay <
loze
nge
Supp
ress
ion
gag
refle
x:
spra
y =
loze
nge
Dis
com
fort
intu
batio
n: s
pray
=
loze
nge
Ibis
et a
l 201
5(ra
ndom
ized
pr
ospe
ctiv
e st
udy)
Tran
sora
l end
osco
py
(unk
now
n)11
810
% li
doca
ine
(40
mg)
, ben
zyda
min
e (1
mg)
10
% li
doca
ine
(20
mg)
+ b
enzy
dam
ine
(0.5
mg)
Spra
yTa
ste:
lido
cain
e <
benz
ydam
ine
Phar
ynge
al a
nest
hesi
a:
lidoc
aine
> b
enzy
dam
ine
Cou
ghin
g/ga
ggin
g:
lidoc
aine
> b
enzy
dam
ine
Dis
com
fort
intu
batio
n:
lidoc
aine
> b
enzy
dam
ine
> be
tter c
ompa
red
with
, <
wor
se c
ompa
red
with
, = e
qual
com
pare
d w
ith
Tabl
e 3.
Con
tinue
d

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 85PDF page: 85PDF page: 85PDF page: 85
Topical anesthesia for office-based procedures
85
4
with placebo for oropharyngeal sensitivity and oropharyngeal dry swallowing (ie, saliva)(30). Participants who received topical anesthesia had significant increase in swallowing time, with an average increase of 67%. Additionally, the same authors found unchanged proximal esophageal swallowing function after topical anesthesia with lidocaine(31). However, when higher doses of lidocaine were administered, contraction of the pharynx was significantly prolonged and relaxation of the proximal esophageal sphincter was significantly shortened.
Topical anesthesia of the larynxThe results of studies investigating the anesthetic effect of topical anesthesia on the larynx are summarized in Table 4(32-40). No studies were found comparing different application methods for topical anesthesia to the larynx. In this paragraph, we therefore summarize the most applied methods. An effective method of anesthetizing the larynx is inserting the anesthetic through the working channel of the endoscope(8, 41-43). The endoscope is inserted transnasally and positioned above the vocal cords. The local anesthetic, in a syringe, is released in the working channel of the endoscope and thus directly applied into the larynx and on the vocal cords. Alternatively, the syringe is placed on a small diameter catheter (eg, epidural catheter), which is directed through the working channel of the endoscope and placed above the vocal cords. Another widely used application method for the larynx and upper trachea is performed with an injection through the cricothyroid membrane. After inserting the needle through the membrane, the syringe is drawn back to check if air bubbles arise, which confirms adequate localization in the larynx and safe injection of the anesthetic solution. After injection, the syringe should be removed quickly, as the patient vigorously coughs because of irritation of the larynx(5, 7, 9, 41, 44). If a patient has a tracheostoma, the cannula can be removed and the anesthetic can be applied through the tracheostoma(5, 44). Some authors used a syringe with curved cannula to transorally apply the anesthetic to the larynx and upper trachea under direct vision of an endoscope(5, 7, 42, 44). A superior laryngeal nerve block is another possible method of locally anesthetizing the larynx for office-based procedures. The location of the injection is where the internal branch of the superior laryngeal nerve crosses the thyrohyoid membrane. This is in the thyrohyoid space, halfway between the hyoid bone and the superior border of the thyroid cartilage and halfway between the anterior midline and the superior cornu of the thyroid cartilage(7, 41). Again, when inserting the needle, the syringe is drawn back to confirm that the tip is not inserted in an artery or the larynx. Local anesthesia, with or without a vasoconstricting agent, can be used. This procedure is repeated at the opposite side. It is essential not to penetrate the thyrohyoid membrane, in contrast to the cricothyroid membrane approach, to prevent endangering the airway. Sensation returns after approximately 3 hours, although the effective time to perform
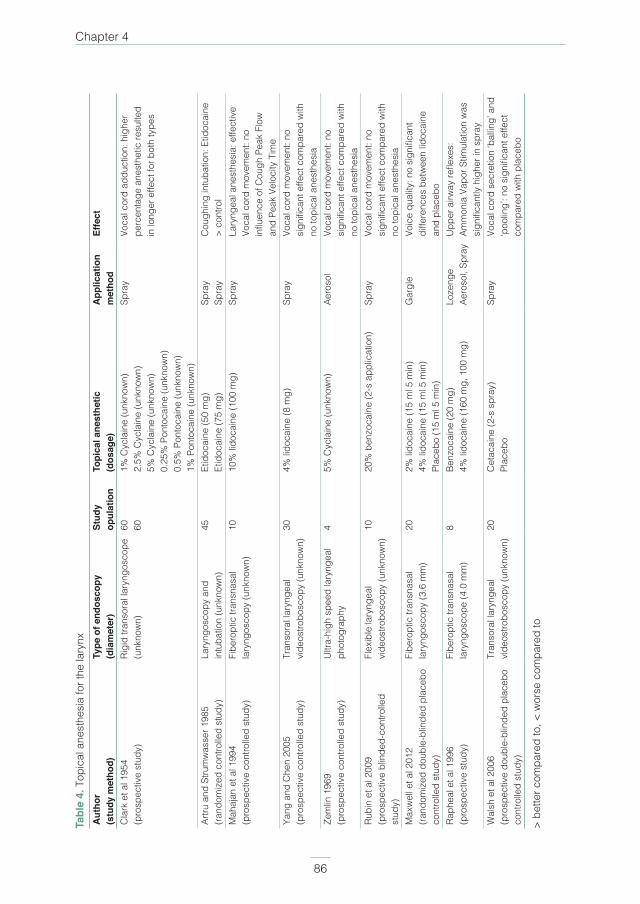
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 86PDF page: 86PDF page: 86PDF page: 86
Chapter 4
86
Tabl
e 4.
Top
ical
ane
sthe
sia
for t
he la
rynx
Aut
hor
(stu
dy m
etho
d)Ty
pe o
f end
osco
py
(dia
met
er)
Stud
y op
ulat
ion
Topi
cal a
nest
hetic
(d
osag
e)A
pplic
atio
n m
etho
dEf
fect
Cla
rk e
t al 1
954
(pro
spec
tive
stud
y)Ri
gid
trans
oral
lary
ngos
cope
(u
nkno
wn)
60 601%
Cyc
lain
e (u
nkno
wn)
2.5%
Cyc
lain
e (u
nkno
wn)
5%
Cyc
lain
e (u
nkno
wn)
0.25
% P
onto
cain
e (u
nkno
wn)
0.5%
Pon
toca
ine
(unk
now
n)1%
Pon
toca
ine
(unk
now
n)
Spra
yVo
cal c
ord
addu
ctio
n: h
ighe
r pe
rcen
tage
ane
sthe
tic re
sulte
d in
long
er e
ffect
for b
oth
type
s
Artru
and
Stru
mw
asse
r 198
5 (ra
ndom
ized
con
trolle
d st
udy)
Lary
ngos
copy
and
in
tuba
tion
(unk
now
n)45
Etid
ocai
ne (5
0 m
g)Et
idoc
aine
(75
mg)
Spra
ySp
ray
Cou
ghin
g in
tuba
tion:
Etid
ocai
ne
> co
ntro
lM
ahaj
an e
t al 1
994
(pro
spec
tive
cont
rolle
d st
udy)
Fibe
ropt
ic tr
ansn
asal
la
ryng
osco
py (u
nkno
wn)
1010
% li
doca
ine
(100
mg)
Spra
yLa
ryng
eal a
nest
hesi
a: e
ffect
ive
Voca
l cor
d m
ovem
ent:
no
influ
ence
of C
ough
Pea
k Fl
ow
and
Peak
Vel
ocity
Tim
e Ya
ng a
nd C
hen
2005
(pro
spec
tive
cont
rolle
d st
udy)
Tran
sora
l lar
ynge
al
vide
ostro
bosc
opy
(unk
now
n)30
4% li
doca
ine
(8 m
g)Sp
ray
Voca
l cor
d m
ovem
ent:
no
sign
ifica
nt e
ffect
com
pare
d w
ith
no to
pica
l ane
sthe
sia
Zem
lin 1
969
(pro
spec
tive
cont
rolle
d st
udy)
Ultr
a-hi
gh s
peed
lary
ngea
l ph
otog
raph
y4
5% C
ycla
ine
(unk
now
n)Ae
roso
lVo
cal c
ord
mov
emen
t: no
si
gnifi
cant
effe
ct c
ompa
red
with
no
topi
cal a
nest
hesi
aRu
bin
et a
l 200
9 (p
rosp
ectiv
e bl
inde
d-co
ntro
lled
stud
y)
Flex
ible
lary
ngea
l vi
deos
trobo
scop
y (u
nkno
wn)
1020
% b
enzo
cain
e (2
-s a
pplic
atio
n)Sp
ray
Voca
l cor
d m
ovem
ent:
no
sign
ifica
nt e
ffect
com
pare
d w
ith
no to
pica
l ane
sthe
sia
Max
wel
l et a
l 201
2(ra
ndom
ized
dou
ble-
blin
ded
plac
ebo
cont
rolle
d st
udy)
Fibe
ropt
ic tr
ansn
asal
la
ryng
osco
py (3
.6 m
m)
202%
lido
cain
e (1
5 m
l 5 m
in)
4% li
doca
ine
(15
ml 5
min
)Pl
aceb
o (1
5 m
l 5 m
in)
Gar
gle
Voic
e qu
ality
: no
sign
ifica
nt
diffe
renc
es b
etw
een
lidoc
aine
an
d pl
aceb
o Ra
phea
l et a
l 199
6(p
rosp
ectiv
e st
udy)
Fibe
ropt
ic tr
ansn
asal
la
ryng
osco
pe (4
.0 m
m)
8Be
nzoc
aine
(20
mg)
4% li
doca
ine
(160
mg,
100
mg)
Loze
nge
Aero
sol,
Spra
yU
pper
airw
ay re
flexe
s:
Amm
onia
Vap
or S
timul
atio
n w
as
sign
ifica
ntly
hig
her i
n sp
ray
Wal
sh e
t al 2
006
(pro
spec
tive
doub
le-b
linde
d pl
aceb
o co
ntro
lled
stud
y)
Tran
sora
l lar
ynge
al
vide
ostro
bosc
opy
(unk
now
n)20
Cet
acai
ne (2
-s s
pray
)Pl
aceb
oSp
ray
Voca
l cor
d se
cret
ion
‘bal
ling’
and
‘p
oolin
g’: n
o si
gnifi
cant
effe
ct
com
pare
d w
ith p
lace
bo
> be
tter c
ompa
red
to, <
wor
se c
ompa
red
to
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 87PDF page: 87PDF page: 87PDF page: 87
Topical anesthesia for office-based procedures
87
4
the procedure is shorter(41). As seen for pharyngeal anesthesia, less frequently described topical anesthesia methods for the larynx are also available. Several authors soaked cotton pledgets in local anesthesia and used a sponge holder to apply this directly to the larynx(11, 45). Erickson described the use of nebulizing the local anesthetic, which requires the nebulizer to produce droplets of the same size that the upper respiratory mucosa can uptake(9). In practice, this was found to be more difficult as it resulted in inadequate dosage to the specific anatomical site. A squeeze bulb nebulizer is often used for this purpose(46). Christoforidis et al described the use of an ultrasonic nebulizer, which offers the advantages of self-administration by patients, even distribution of the anesthetic, and control of particle size(47). The authors noticed no complications in 273 patients. Thawley et al used a face mask covering the nose and mouth to apply topical anesthesia via a nebulizer(48). For the abovementioned alternative anesthesia methods for the larynx, no information regarding efficacy was mentioned.
Topical anesthesia applied on the upper airway was found to have minimal impact on breathing pattern(32). Furthermore, minimal effect is seen on bronchus dilatation and constriction. The cough reflex is suppressed because the anesthetic blocks the afferent nerve endings. Other motor functions, such as vocal cord adduction or capability of coughing, are also not influenced after topical anesthesia administration to the larynx(33-40).
Efficacy of topical anesthesiaSufficient topical anesthesia will blunt autonomic reflexes such as hypertension, tachycardia, and coughing. Blunting of these reflexes can therefore be used to assess efficacy of the achieved topical anesthesia. Studies investigating the efficacy of topical anesthesia to the upper aerodigestive tract are summarized in Table 5(25, 33, 49-53).
Most studies investigated the effect of topical anesthesia to the upper aerodigestive tract during transoral endoscopy or surgery under general anesthesia. When topical anesthesia was used during manipulation in the upper aerodigestive tract (eg, laryngoscopy, intubation, or extubation), blood pressure and heart rate were usually less increased, compared with a control group(33, 50, 51). However, Ristikankare et al found contradicting results in a randomized study comparing sedation, topical anesthesia, placebo and no drug, which showed no significant changes between all groups(53). When two different topical anesthetics were used, no significant changes in cardiovascular parameters were found during extubation(49).
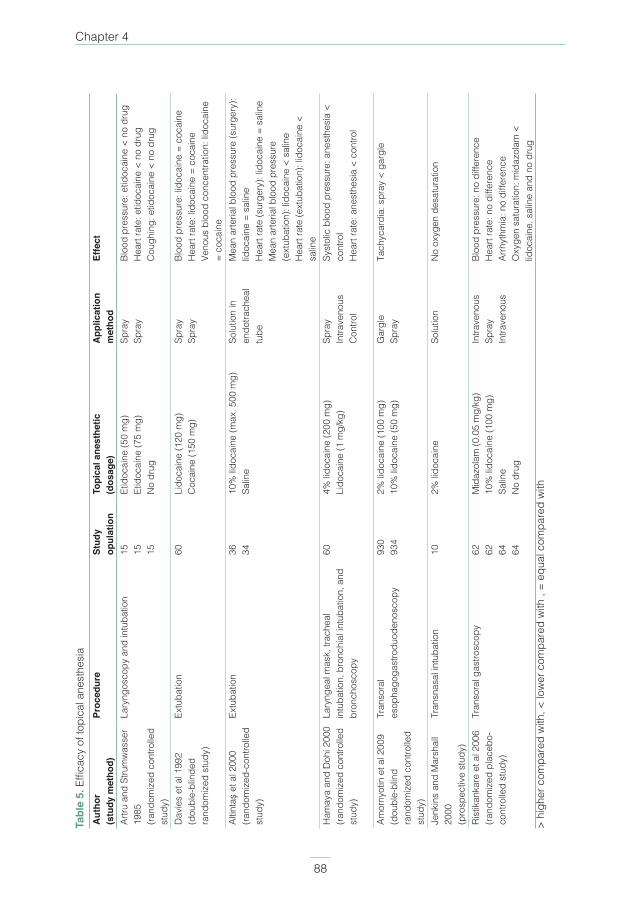
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 88PDF page: 88PDF page: 88PDF page: 88
Chapter 4
88
Tabl
e 5.
Effi
cacy
of t
opic
al a
nest
hesi
aA
utho
r (s
tudy
met
hod)
Proc
edur
e St
udy
opul
atio
nTo
pica
l ane
sthe
tic
(dos
age)
App
licat
ion
met
hod
Effe
ct
Artru
and
Stru
mw
asse
r 19
85(ra
ndom
ized
con
trolle
d st
udy)
Lary
ngos
copy
and
intu
batio
n15 15 15
Etid
ocai
ne (5
0 m
g)Et
idoc
aine
(75
mg)
No
drug
Spra
ySp
ray
Bloo
d pr
essu
re: e
tidoc
aine
< n
o dr
ugH
eart
rate
: etid
ocai
ne <
no
drug
Cou
ghin
g: e
tidoc
aine
< n
o dr
ug
Dav
ies
et a
l 199
2(d
oubl
e-bl
inde
d ra
ndom
ized
stu
dy)
Extu
batio
n60
Lido
cain
e (1
20 m
g)C
ocai
ne (1
50 m
g)Sp
ray
Spra
yBl
ood
pres
sure
: lid
ocai
ne =
coc
aine
Hea
rt ra
te: l
idoc
aine
= c
ocai
neVe
nous
blo
od c
once
ntra
tion:
lido
cain
e =
coca
ine
Altin
taş
et a
l 200
0(ra
ndom
ized
-con
trolle
d st
udy)
Extu
batio
n36 34
10%
lido
cain
e (m
ax. 5
00 m
g)Sa
line
Solu
tion
in
endo
trach
eal
tube
Mea
n ar
teria
l blo
od p
ress
ure
(sur
gery
): lid
ocai
ne =
sal
ine
Hea
rt ra
te (s
urge
ry):
lidoc
aine
= s
alin
eM
ean
arte
rial b
lood
pre
ssur
e (e
xtub
atio
n): l
idoc
aine
< s
alin
eH
eart
rate
(ext
ubat
ion)
: lid
ocai
ne <
sa
line
Ham
aya
and
Doh
i 200
0(ra
ndom
ized
con
trolle
d st
udy)
Lary
ngea
l mas
k, tr
ache
al
intu
batio
n, b
ronc
hial
intu
batio
n, a
nd
bron
chos
copy
604%
lido
cain
e (2
00 m
g)Li
doca
ine
(1 m
g/kg
)Sp
ray
Intra
veno
usC
ontro
l
Syst
olic
blo
od p
ress
ure:
ane
sthe
sia
< co
ntro
lH
eart
rate
: ane
sthe
sia
< co
ntro
l
Amor
nyot
in e
t al 2
009
(dou
ble-
blin
d ra
ndom
ized
con
trolle
d st
udy)
Tran
sora
l es
opha
goga
stro
duod
enos
copy
930
934
2% li
doca
ine
(100
mg)
10%
lido
cain
e (5
0 m
g)G
argl
eSp
ray
Tach
ycar
dia:
spr
ay <
gar
gle
Jenk
ins
and
Mar
shal
l 20
00(p
rosp
ectiv
e st
udy)
Tran
snas
al in
tuba
tion
102%
lido
cain
eSo
lutio
nN
o ox
ygen
des
atur
atio
n
Rist
ikan
kare
et a
l 200
6(ra
ndom
ized
pla
cebo
-co
ntro
lled
stud
y)
Tran
sora
l gas
trosc
opy
62 62 64 64
Mid
azol
am (0
.05
mg/
kg)
10%
lido
cain
e (1
00 m
g)
Salin
eN
o dr
ug
Intra
veno
usSp
ray
Intra
veno
us
Bloo
d pr
essu
re: n
o di
ffere
nce
Hea
rt ra
te: n
o di
ffere
nce
Arrh
ythm
ia: n
o di
ffere
nce
O
xyge
n sa
tura
tion:
mid
azol
am <
lid
ocai
ne, s
alin
e an
d no
dru
g>
high
er c
ompa
red
with
, < lo
wer
com
pare
d w
ith ,
= eq
ual c
ompa
red
with

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 89PDF page: 89PDF page: 89PDF page: 89
Topical anesthesia for office-based procedures
89
4
Complications of local anestheticsSystemic toxicitySystemic toxicity of local anesthetics is caused by the alteration of the functioning of the cardiac conductivity system and the functioning of the central nervous system. Toxicity of the latter usually begins with lightheadedness, dizziness, visual and auditory impairment, and disorientation. Twitching, tremors, and convulsions can follow. With increasing systemic concentrations, central nervous system depression will progress resulting in respiratory depression or arrest. For the cardiovascular system, direct cardiac effects of toxicity can result in blocking of the cardiac contractibility (ie, cardiac depression) and conduction (eg, bradycardia). Direct vascular effects are either vasodilatation, possible in high doses of synthetic anesthetics, or vasoconstriction, which can be seen in low concentrations of synthetic anesthetics and cocaine(6).
Several studies investigated the systemic concentrations of local anesthetics after topical administration to the pharynx and larynx. Dosages of topical anesthesia administered ranged from 100 to 800 mg, using spray, gel, or solution(49, 50, 52, 54-61). Although most studies investigated the effect of lidocaine, some authors studied cocaine(49) or prilocaine(60). Almost all studies showed venous blood concentrations that were below the maximum dosage of lidocaine and thus did not exceed a plasma concentration of 5 µg/ml. Reasoner et al compared topical lidocaine spray with laryngeal nerve block and found, shortly after administration, significantly higher venous blood concentrations in the laryngeal nerve block group(61). After 10 minutes, this difference disappeared. Applying topical anesthesia to the trachea resulted in higher blood concentration compared with the application of the same amount of anesthesia in the larynx and thus has greater chance of exceeding the maximum dosage(54, 55). The duration of reaching peak plasma concentrations for lidocaine varied from 5 to 60 minutes(49, 52, 54, 55, 57, 58, 60), although Altintas et al showed highest concentrations 90 minutes after they administered lidocaine solution in the cuff of the endotracheal tube in order to diffuse to the trachea(50). For cocaine, the peak plasma concentration was reached after 12 minutes and for prilocaine between 10 and 60 minutes(49, 60). Viegas and Stoelting investigated the arterial plasma concentration after topical anesthesia with lidocaine(62). Ten patients received lidocaine spray to the larynx and trachea and of these 10 patients, 4 additionally received viscous lidocaine on the intubation tube. After 9-15 minutes, mean lidocaine concentration was lower in the nonviscous group compared with the viscous group. Hamaya and Dohi also compared lidocaine spray and intravenous lidocaine on arterial blood concentrations(51). Serum concentration of lidocaine was significantly higher in the bronchial spray group compared with the trachea and larynx groups.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 90PDF page: 90PDF page: 90PDF page: 90
Chapter 4
90
Complications after topical anesthesia administration to the upper aerodigestive tract are usually caused by overdosage. In Table 6, cases of overdosage due to topical anesthesia administration are summarized(9, 41, 59, 63, 64).
Anaphylactic reactionAnaphylactic reactions to local anesthetics are rare and account for less than 1% of local anesthetic complications(1). Daily mentioned that most reactions are responses to ester-type local anesthetics, because breakdown of this type of anesthetic produces para-aminobenzoic acid, which often results in cross-reactions(1). Several case reports have been published that concern patients who developed a systemic overreaction after topical anesthesia to the larynx, which are summarized in Table 6(65-67).
MethemoglobinemiaMethemoglobinemia is a disorder in which high levels of methemoglobin are present in blood plasma concentration, which is normally below 1% - 3%(68-73). Methemoglobinemia is known to be frequently caused by benzocaine, an ester-type anesthetic. A 10-year retrospective case-control study showed a prevalence of 0.035%(73). Although less frequently reported, lidocaine, prilocaine, and tetracaine are also capable of causing methemoglobinemia(69, 72, 74). Benzocaine is 3.7 times more likely to cause methemoglobinemia, compared with anesthetics not containing benzocaine(73). Methemoglobin is a form of hemoglobin that contains ferric iron (Fe3+), which has less potential of binding oxygen compared with ferrous iron (Fe2+), and could lead to hypoxia(69-77). Amounts varying from 15 to 25 mg/kg of benzocaine can induce methemoglobinemia(75). Clinical signs are dyspnea, cyanosis, changing of mental status, headache, and fatigue(68). A diagnosis is made by obtaining an arterial blood gas sample, which reveals a brown color and an elevated methemoglobin level. Furthermore, persisting cyanosis unresponsive to 100% oxygen administration can confirm the diagnosis(68, 70, 74, 77, 78). Methemoglobin concentrations between 10% and 25% often result in cyanosis, as levels of 35%-40% cause the abovementioned clinical signs. When 60% of methemoglobin is found, lethargy can occur and concentrations above 70% probably result in death(7, 68, 69, 71, 77, 78), although some authors reported lethality above 50%(73). Several studies mentioned signs of methemoglobinemia using 20% benzocaine doses varying from 20 to 80 mg, or from 1 to 5 seconds of spraying(68, 69, 71, 74, 78). The dosage used for cetacaine was not mentioned(75). Treatment options are administration of oral ascorbic acid in case of less severe complaints or intravenous administration of methylene blue in case of severe complaints(7, 68-70, 72-78). In case of no response to methylene blue, blood transfusion or hyperbaric oxygen therapy are alternative therapies(72, 77).
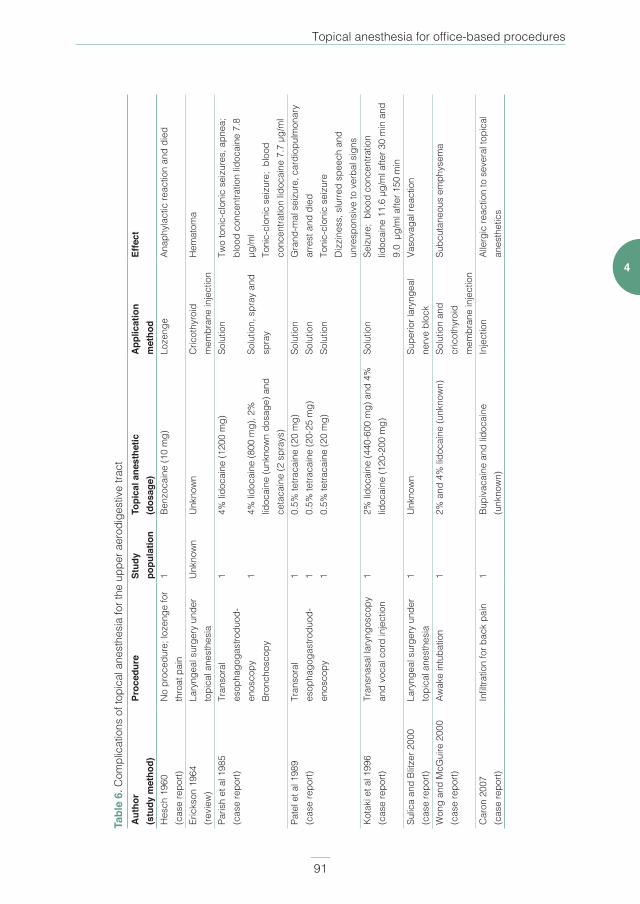
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 91PDF page: 91PDF page: 91PDF page: 91
Topical anesthesia for office-based procedures
91
4
Tabl
e 6.
Com
plic
atio
ns o
f top
ical
ane
sthe
sia
for t
he u
pper
aer
odig
estiv
e tra
ctA
utho
r (s
tudy
met
hod)
Proc
edur
e St
udy
popu
latio
nTo
pica
l ane
sthe
tic
(dos
age)
App
licat
ion
m
etho
dEf
fect
Hes
ch 1
960
(cas
e re
port)
No
proc
edur
e; lo
zeng
e fo
r th
roat
pai
n1
Benz
ocai
ne (1
0 m
g)Lo
zeng
eAn
aphy
lact
ic re
actio
n an
d di
ed
Eric
kson
196
4 (re
view
)La
ryng
eal s
urge
ry u
nder
to
pica
l ane
sthe
sia
Unk
now
nU
nkno
wn
Cric
othy
roid
m
embr
ane
inje
ctio
nH
emat
oma
Paris
h et
al 1
985
(cas
e re
port)
Tran
sora
l es
opha
goga
stro
duod
-en
osco
pyBr
onch
osco
py
1 1
4% li
doca
ine
(120
0 m
g)
4% li
doca
ine
(800
mg)
, 2%
lid
ocai
ne (u
nkno
wn
dosa
ge) a
nd
ceta
cain
e (2
spr
ays)
Solu
tion
Solu
tion,
spr
ay a
nd
spra
y
Two
toni
c-cl
onic
sei
zure
s, a
pnea
; bl
ood
conc
entra
tion
lidoc
aine
7.8
µg
/ml
Toni
c-cl
onic
sei
zure
; bl
ood
conc
entra
tion
lidoc
aine
7.7
µg/
ml
Pate
l et a
l 198
9 (c
ase
repo
rt)Tr
anso
ral
esop
hago
gast
rodu
od-
enos
copy
1 1 1
0.5%
tetra
cain
e (2
0 m
g)0.
5% te
traca
ine
(20-
25 m
g)0.
5% te
traca
ine
(20
mg)
Solu
tion
Solu
tion
Solu
tion
Gra
nd-m
al s
eizu
re, c
ardi
opul
mon
ary
arre
st a
nd d
ied
Toni
c-cl
onic
sei
zure
Diz
zine
ss, s
lurre
d sp
eech
and
un
resp
onsi
ve to
ver
bal s
igns
Kota
ki e
t al 1
996
(cas
e re
port)
Tran
snas
al la
ryng
osco
py
and
voca
l cor
d in
ject
ion
12%
lido
cain
e (4
40-6
00 m
g) a
nd 4
%
lidoc
aine
(120
-200
mg)
So
lutio
nSe
izur
e; b
lood
con
cent
ratio
n lid
ocai
ne 1
1.6
µg/m
l afte
r 30
min
and
9.
0 µ
g/m
l afte
r 150
min
Sulic
a an
d Bl
itzer
200
0 (c
ase
repo
rt)La
ryng
eal s
urge
ry u
nder
to
pica
l ane
sthe
sia
1U
nkno
wn
Supe
rior l
aryn
geal
ne
rve
bloc
kVa
sova
gal r
eact
ion
Won
g an
d M
cGui
re 2
000
(cas
e re
port)
Awak
e in
tuba
tion
12%
and
4%
lido
cain
e (u
nkno
wn)
Solu
tion
and
cric
othy
roid
m
embr
ane
inje
ctio
n
Subc
utan
eous
em
phys
ema
Car
on 2
007
(cas
e re
port)
Infil
tratio
n fo
r bac
k pa
in1
Bupi
vaca
ine
and
lidoc
aine
(u
nkno
wn)
Inje
ctio
nAl
lerg
ic re
actio
n to
sev
eral
topi
cal
anes
thet
ics

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 92PDF page: 92PDF page: 92PDF page: 92
Chapter 4
92
DISCUSSION
Lidocaine is the most investigated local anesthetic for office-based procedures for the upper aerodigestive tract. For nasal anesthesia, all included studies investigated the effectiveness of lidocaine, with one study comparing lidocaine with several alternatives, and all studies concluded that lidocaine is an effective topical anesthetic for the nasal cavity(14). The most effective method of application is not extensively compared and investigated, but cotton pledgets soaked in a local anesthetic and decongestant seems most effective(12). No information was available on the ideal duration upon which the cotton pledgets should be left in the nasal cavity. Anesthetic gel applied in the nasal cavity is an alternative(13). Studies comparing lidocaine with cocaine or tetracaine were not found, although specific qualities are reported. Cocaine has a stronger anesthetic effect and causes vasoconstriction, compared with lidocaine, but is also more toxic with more systemic side effects(10). Tetracaine has a longer anesthetic effect compared with lidocaine, although the side effects are also reported to be more severe(14).
Anesthetizing the pharynx is possible in several ways, with spraying as the most investigated method. Again, lidocaine was the most used anesthetic that showed good sensory suppression(16-24). By administrating topical anesthesia to the pharynx, pharyngeal swallowing is temporarily changed(28, 29). For the larynx, no studies were found that compared topical anesthesia administration techniques for effectiveness during endoscopy. Administration of local anesthesia through the working channel of the endoscope was used in several studies and resulted in adequate anesthesia, although a cricothyroid membrane injection or a laryngeal nerve block showed comparable results(7-9, 41-44). Administrating topical anesthesia to the larynx also showed adequate sensory suppression without impairing motor function(32-40). Increasing concentrations of anesthesia resulted in longer duration of the anesthetic effect(29,
79).
Secondary effects of topical anesthesia administration on the pharynx and larynx are usually decreased rise in blood pressure and heart rate, compared with administrating placebo or nothing(33, 50). These secondary effects of topical anesthesia might indicate that appliance of a local anesthetic results in less stress to the body when a patients is intubated or examined with an endoscope.
For the pharynx and larynx, lidocaine is the most used and investigated topical anesthetic. Although the maximum amount of lidocaine that can be safely administered varies
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 93PDF page: 93PDF page: 93PDF page: 93
Topical anesthesia for office-based procedures
93
4
in literature from 200 to 600 mg, the toxic blood concentration of 5 µg/ml was never exceeded(61). A systemic overreaction due to lidocaine administration to the pharynx and larynx is rare(16), although administration to the trachea and bronchus should be performed with caution, as more rapid and higher systemic uptake is seen for these anatomical sites(54,
55). Several alternative topical anesthetics are available, each with different qualities, but large randomized studies that compare these with lidocaine for effectiveness and possible complications during endoscopy or office-based procedures are still wanting. We did not find any studies reporting on the incidence and treatment of laryngospasm.
Our goal was to provide an objective summary on topical anesthesia for endoscopic office-based procedures for the pharynx and larynx, and thus guidance for physicians who are interested in starting with these procedures. The current literature search lacked adequate studies comparing different application methods for topical anesthesia, and thus, this descriptive review is the only information at hand. Based on these studies, and our experience in office-based procedures under topical anesthesia(3, 4, 80), we offer our current expert opinion on topical anesthesia use for office-based procedures. Adequate patient instruction is essential for a successful procedure, and beforehand we explain the procedure and anesthesia techniques. Applying cotton pledgets in the nose is sensitive upon insertion and could lead to sneezing and excessive watering of the eyes. For the nose, we insert two to three cotton pledgets soaked in 10% lidocaine and 0.1% xylometazoline in each nasal cavity, and leave these in situ for a minimum of 10 minutes. Although the exact amount of both solutions varies, around four sprays of 10% lidocaine and 1 ml of 0.1% xylometazoline is used for each cotton pledget. For the pharynx, between 8 and 14 sprays of 10% lidocaine are used. We explain to the patient that spraying results in coughing, numbness of the tongue and throat, the formation of excessive saliva, and difficulty in swallowing. First, several sprays are applied to the oral cavity and thereafter to the pharynx, while letting the patient deeply inhale. For laryngeal anesthesia, patients are informed on similar effects to pharyngeal anesthesia, plus the short feeling of dyspnea when topical anesthesia is applied on the vocal cords. A small epidural catheter is passed through the working channel of the laryngoscope and positioned above the vocal cords. Thereafter, the patient is asked to perform a persisting “I” tone, and 2.5 ml of 4.3% lidocaine is applied on the vocal cords in several stages. Lidocaine with a lower percentage is used, because of less viscosity compared with 10% lidocaine, which cannot pass through the catheter. When both percentages of lidocaine were directly inserted through the working channel of the laryngoscope, we experienced blurring of the camera and therefore reduced vision. In the past, we have extensively performed laryngeal anesthesia with an injection through the cricothyroid membrane using 1.0 ml of
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 94PDF page: 94PDF page: 94PDF page: 94
Chapter 4
94
10% lidocaine, but experienced less laryngeal anesthesia and a more traumatic patient experience. All patients are advised not to eat or drink for 60 minutes after laryngopharyngeal anesthesia is performed.
This descriptive review has systematically searched and included all available articles on this subject. The possibility exists that articles that are in the scope of this review were missed in the literature search. Furthermore, a methodological analysis was not performed because of the descriptive nature of this review, which could have resulted in more thorough conclusions.
In conclusion, by applying adequate topical anesthesia to the upper aerodigestive tract, several surgical procedures in laryngology and head and neck oncology can be performed in the outpatient clinical instead of the operating room under general anesthesia. Lidocaine is the most investigated anesthetic, with adequate efficacy and few complications.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 95PDF page: 95PDF page: 95PDF page: 95
Topical anesthesia for office-based procedures
95
4
REFERENCES
1. Daily, W.W., Local anesthesia of the head and neck. Ear Nose Throat J, 1981. 60(1): p. 19-24.
2. Zeitels, S.M., et al., Foresight in laryngology and laryngeal surgery: a 2020 vision. Ann Otol Rhinol
Laryngol Suppl, 2007. 198: p. 2-16.
3. Wellenstein, D.J., et al., Office-based procedures for diagnosis and treatment of esophageal
pathology. Head Neck, 2017.
4. Wellenstein, D.J., et al., Safety of flexible endoscopic biopsy of the pharynx and larynx under
topical anesthesia. Eur Arch Otorhinolaryngol, 2017.
5. Rosen, C.A., et al., Advances in office-based diagnosis and treatment in laryngology.
Laryngoscope, 2009. 119(SUPPL. 2): p. S185-S212.
6. Miller, R.D., Miller’s anesthesia. 7th ed. 2010, Philadelphia, PA: Churchill Livingstone/Elsevier.
7. Simpson, C.B., M.R. Amin, and G.N. Postma, Topical anesthesia of the airway and esophagus.
Ear Nose Throat J, 2004. 83(7 Suppl 2): p. 2-5.
8. Jourdy, D.N. and A. Kacker, Regional anesthesia for office-based procedures in
otorhinolaryngology. Anesthesiol Clin, 2010. 28(3): p. 457-68.
9. Erickson, J.C., 3rd, SURFACE ANESTHESIA OF THE AIRWAY AND LARYNX. Int Anesthesiol Clin,
1964. 2: p. 709-24.
10. Bernal-Sprekelsen, M. and A. Schmelzer, Local anesthesia of the head and neck. Anesth Pain
Control Dent, 1992. 1(2): p. 81-4.
11. Woo, P., Office-based laryngeal procedures. Otolaryngol Clin North Am, 2006. 39(1): p. 111-33.
12. Hu, C.T., Gauze pledgetting versus endoscopic-guided aerosolized spray for nasal anesthesia
before transnasal EGD: a prospective, randomized study. Gastrointest Endosc, 2010. 71(1): p.
11-20.
13. Zainudin, B.M., M.H. Rafia, and A.W. Sufarlan, Topical nasal anaesthesia for fibreoptic
bronchoscopy: lignocaine spray or gel? Singapore Med J, 1993. 34(2): p. 148-9.
14. Ozkiris, M., et al., Comparison of topical anesthetic effects of lidocaine, prilocaine, ropivacaine,
and bupivacaine in transnasal fiberoptic nasopharyngolaryngoscopy. Am J Rhinol Allergy, 2014.
28(3): p. e141-3.
15. Frosh, A.C., et al., Is local anaesthesia actually beneficial in flexible fibreoptic nasendoscopy?
Clin Otolaryngol Allied Sci, 1998. 23(3): p. 259-62.
16. Smith, J.L., A. Opekun, and D.Y. Graham, Controlled comparison of topical anesthetic agents in
flexible upper gastrointestinal endoscopy. Gastrointestinal Endoscopy, 1985. 31(4): p. 255-258.
17. Mulcahy, H.E., et al., A double-blind randomized trial of low-dose versus high-dose topical
anaesthesia in unsedated upper gastrointestinal endoscopy. Alimentary Pharmacology and
Therapeutics, 1996. 10(6): p. 975-979.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 96PDF page: 96PDF page: 96PDF page: 96
Chapter 4
96
18. Martin, J.P., P.A. Arlett, and G. Holdstock, Development of a sedation policy for upper GI
endoscopy based on an audit of patients’ perception of the procedure. Eur J Gastroenterol
Hepatol, 1996. 8(4): p. 355-7.
19. Dhir, V., et al., Topical pharyngeal anesthesia without intravenous sedation during upper
gastrointestinal endoscopy. Indian J Gastroenterol, 1997. 16(1): p. 10-1.
20. Ristikankare, M., et al., Is routine sedation or topical pharyngeal anesthesia beneficial during
upper endoscopy? Gastrointestinal Endoscopy, 2004. 60(5): p. 686-694.
21. Ibis, M., et al., Lidocaine versus lidocaine plus benzydamine as a topical anesthesia regimen for
unsedated upper gastrointestinal endoscopy: A comparison study. Turk J Gastroenterol, 2015.
26(3): p. 224-7.
22. Hedenbro, J.L., et al., A randomized, double-blind, placebo-controlled study to evaluate topical
anaesthesia of the pharynx in upper gastrointestinal endoscopy. Endoscopy, 1992. 24(6): p. 585-
7.
23. Campo, R., et al., Topical pharyngeal anesthesia improves tolerance of upper gastrointestinal
endoscopy: a randomized double-blind study. Endoscopy, 1995. 27(9): p. 659-64.
24. Soma, Y., et al., Evaluation of topical pharyngeal anesthesia for upper endoscopy including
factors associated with patient tolerance. Gastrointest Endosc, 2001. 53(1): p. 14-8.
25. Amornyotin, S., et al., Topical viscous lidocaine solution versus lidocaine spray for pharyngeal
anesthesia in unsedated esophagogastroduodenoscopy. Endoscopy, 2009. 41(7): p. 581-6.
26. Chan, C.K.O., K.L. Fok, and C.M. Poon Flavored anesthetic lozenge versus Xylocaine spray used
as topical pharyngeal anesthesia for unsedated esophagogastroduodenoscopy: A randomized
placebo-controlled trial. Surgical Endoscopy and Other Interventional Techniques, 2010. 24,
897-901 DOI: 10.1007/s00464-009-0687-9.
27. Sohmer, B., et al., EMLA cream is an effective topical anesthetic for bronchoscopy. Canadian
Respiratory Journal, 2004. 11(8): p. 587-588.
28. Ertekin, C., et al., Effect of mucosal anaesthesia on oropharyngeal swallowing. Neurogastroenterol
Motil, 2000. 12(6): p. 567-72.
29. Chee, C., et al., The influence of chemical gustatory stimuli and oral anaesthesia on healthy
human pharyngeal swallowing. Chem Senses, 2005. 30(5): p. 393-400.
30. Mansson, I. and N. Sandberg, Oro-pharyngeal sensitivity and elicitation of swallowing in man.
Acta Otolaryngol, 1975. 79(1-2): p. 140-5.
31. Mansson, I. and N. Sandberg, Effects of surface anesthesia on deglutition in man. Laryngoscope,
1974. 84(3): p. 427-37.
32. Karlsson, J.A., Airway anaesthesia and the cough reflex. Bull Eur Physiopathol Respir, 1987. 23
Suppl 10: p. 29s-36s.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 97PDF page: 97PDF page: 97PDF page: 97
Topical anesthesia for office-based procedures
97
4
33. Artru, A.A. and T.A. Strumwasser, Intratracheal aerosolized etidocaine to attenuate cardiovascular
and cough responses to laryngoscopy and intubation. Annals of Emergency Medicine, 1985.
14(11): p. 1069-1073.
34. Mahajan, R.P., et al., Effect of topical anaesthesia on the motor performance of vocal cords as
assessed by tussometry. Anaesthesia, 1994. 49(12): p. 1028-30.
35. Yang, C.C. and S.H. Chen, Impact of topical anesthesia on acoustic characteristics of voice
during laryngeal telescopic examination. Otolaryngol Head Neck Surg, 2005. 132(1): p. 110-4.
36. Zemlin, W.R., The effect of topical anesthesia on internal laryngeal behavior. Acta Otolaryngol,
1969. 68(1): p. 168-76.
37. Rubin, A.D., et al., The effect of topical anesthesia on vocal fold motion. J Voice, 2009. 23(1): p.
128-31.
38. Maxwell, M.J., et al., Vocalization assessed by electrolaryngography is unaffected by topical
lidocaine anesthesia: a prospective, crossover, randomized, double-blind placebo-controlled
study. Anesth Analg, 2012. 114(4): p. 785-90.
39. Raphael, J.H., G.D. Stanley, and J.A. Langton, Effects of topical benzocaine and lignocaine on
upper airway reflex sensitivity. Anaesthesia, 1996. 51(2): p. 114-8.
40. Walsh, J., R.C. Branski, and K. Verdolini, Double-blind study on the effects of topical anesthesia
on laryngeal secretions. J Voice, 2006. 20(2): p. 282-90.
41. Sulica, L. and A. Blitzer, Anesthesia for laryngeal surgery in the office. Laryngoscope, 2000.
110(10 Pt 1): p. 1777-9.
42. Zeitels, S.M., et al., Office-based treatment of glottal dysplasia and papillomatosis with the 585-
nm pulsed dye laser and local anesthesia. Ann Otol Rhinol Laryngol, 2004. 113(4): p. 265-76.
43. Zeitels, S.M., et al., Office-based 532-nm pulsed KTP laser treatment of glottal papillomatosis and
dysplasia. Ann Otol Rhinol Laryngol, 2006. 115(9): p. 679-85.
44. Hogikyan, N.D., Transnasal endoscopic examination of the subglottis and trachea using topical
anesthesia in the otolaryngology clinic. Laryngoscope, 1999. 109(7 Pt 1): p. 1170-3.
45. Colman, M.F. and R. Reynolds, The use of topical cocaine to prevent laryngospasm after general
anesthesia on endoscopy procedures. Laryngoscope, 1985. 95(4): p. 474.
46. Vale, R., A laryngeal spray. Anaesthesia, 1967. 22(2): p. 314-5.
47. Christoforidis, A.J., J.F. Tomashefski, and R.I. Mitchell, Use of an ultrasonic nebulizer for the
application of oropharyngeal, laryngeal and tracheobronchial anesthesia. Chest, 1971. 59(6): p.
629-33.
48. Thawley, S.E., Head and neck and plastic surgery: Nebulized anesthesia for the nose, pharynx,
larynx, and trachea. Laryngoscope, 1987. 97(4): p. 499-500.
49. Davies, D.W., S.L. Moylan, and G. O’Sullivan, Topical anaesthesia of the larynx: cocaine or
lignocaine? Eur J Anaesthesiol, 1992. 9(5): p. 393-7.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 98PDF page: 98PDF page: 98PDF page: 98
Chapter 4
98
50. Altintas, F., et al., Lidocaine 10% in the endotracheal tube cuff: blood concentrations,
haemodynamic and clinical effects. Eur J Anaesthesiol, 2000. 17(7): p. 436-42.
51. Hamaya, Y. and S. Dohi, Differences in cardiovascular response to airway stimulation at different
sites and blockade of the responses by lidocaine. Anesthesiology, 2000. 93(1): p. 95-103.
52. Jenkins, S.A. and C.F. Marshall, Awake intubation made easy and acceptable. Anaesthesia and
Intensive Care, 2000. 28(5): p. 556-561.
53. Ristikankare, M., et al., Sedation, topical pharyngeal anesthesia and cardiorespiratory safety
during gastroscopy. J Clin Gastroenterol, 2006. 40(10): p. 899-905.
54. Curran, J., C. Hamilton, and T. Taylor, Topical analgesia before tracheal intubation. Anaesthesia,
1975. 30(6): p. 765-8.
55. Rosenberg, P.H., J. Heinonen, and M. Takasaki, Lidocaine concentration in blood after topical
anaesthesia of the upper respiratory tract. Acta Anaesthesiologica Scandinavica, 1980. 24(2): p.
125-128.
56. Nydahl, P.A. and K. Axelsson, Venous blood concentration of lidocaine after nasopharyngeal
application of 2% lidocaine gel. Acta Anaesthesiol Scand, 1988. 32(2): p. 135-9.
57. Soda, K., et al., Serum lidocaine and MEGX concentrations after pharyngeal anesthesia for
gastroscopy. Endoscopy, 1994. 26(4): p. 347-51.
58. Scott, D.B., et al., Plasma lignocaine concentrations following endotracheal spraying with an
aerosol. Br J Anaesth, 1976. 48(9): p. 899-902.
59. Kotaki, H., et al., Safe and effective topical application dose of lidocaine for surgery with
laryngomicroscopy. Clin Pharmacol Ther, 1996. 60(2): p. 229-35.
60. Larijani, G.E., et al., The efficacy and safety of EMLA cream for awake fiberoptic endotracheal
intubation. Anesth Analg, 2000. 91(4): p. 1024-6.
61. Reasoner, D.K., et al., A comparison of anesthetic techniques for awake intubation in neurosurgical
patients. J Neurosurg Anesthesiol, 1995. 7(2): p. 94-9.
62. Viegas, O. and R.K. Stoelting, Lidocaine in arterial blood after laryngotracheal administration.
Anesthesiology, 1975. 43(4): p. 491-3.
63. Parish, R.C., R.T. Moore, and V.P. Gotz, Seizures following oral lidocaine for esophageal
anesthesia. Drug Intell Clin Pharm, 1985. 19(3): p. 199-201.
64. Wong, D.T. and G.P. McGuire, Subcutaneous emphysema following trans-cricothyroid membrane
injection of local anesthetic. Can J Anaesth, 2000. 47(2): p. 165-8.
65. Hesch, D.J., Anaphylactic death from use of a throat lozenge. J Am Med Assoc, 1960. 172: p.
12-5.
66. Patel, D., S. Chopra, and M.D. Berman, Serious systemic toxicity resulting from use of tetracaine
for pharyngeal anesthesia in upper endoscopic procedures. Dig Dis Sci, 1989. 34(6): p. 882-4.
67. Caron, A.B., Allergy to multiple local anesthetics. Allergy Asthma Proc, 2007. 28(5): p. 600-1.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 99PDF page: 99PDF page: 99PDF page: 99
Topical anesthesia for office-based procedures
99
4
68. Linares, L.A., T.Y. Peretz, and J. Chin, Methemoglobinemia induced by topical anesthetic
(benzocaine). Radiother Oncol, 1990. 18(3): p. 267-9.
69. Cooper, H.A., Methemoglobinemia caused by benzocaine topical spray. South Med J, 1997.
90(9): p. 946-8.
70. Haynes, J.M., Acquired methemoglobinemia following benzocaine anesthesia of the pharynx.
Am J Crit Care, 2000. 9(3): p. 199-201.
71. Kuschner, W.G., et al., Benzocaine-associated methemoglobinemia following bronchoscopy in a
healthy research participant. Respir Care, 2000. 45(8): p. 953-6.
72. Lavergne, S., et al., Methemoglobinemia and acute hemolysis after tetracaine lozenge use. J Crit
Care, 2006. 21(1): p. 112-4.
73. Chowdhary, S., et al., Risk of topical anesthetic-induced methemoglobinemia: a 10-year
retrospective case-control study. JAMA Intern Med, 2013. 173(9): p. 771-6.
74. Marinella, M.A., When brown and blue make red: A case of acquired methemoglobinemia. Heart
and Lung: Journal of Acute and Critical Care, 2006. 35(3): p. 205-206.
75. Seibert, R.W. and J.J. Seibert, Infantile methemoglobinemia induced by a topical anesthetic,
cetacaine. Laryngoscope, 1984. 94(6): p. 816-817.
76. Aepfelbacher, F.C., P. Breen, and W.J. Manning, Methemoglobinemia and topical pharyngeal
anesthesia. N Engl J Med, 2003. 348(1): p. 85-6.
77. Moos, D.D. and J.D. Cuddeford, Methemoglobinemia and benzocaine. Gastroenterol Nurs,
2007. 30(5): p. 342-5; quiz 346-7.
78. Malhotra, S., M. Kolda, and N.C. Nanda, Local Anesthetic-Induced Methemoglobinemia During
Transesophageal Echocardiography. Echocardiography, 1998. 15(2): p. 165-168.
79. Clark, R.E., L.R. Orkin, and E.A. Rovenstine, An objective method of evaluating topical anesthesia
in man utilizing the laryngeal reflex; the effect of methylcellulose, triton A-20, and hyaluronidase
as determined thereby. Anesthesiology, 1954. 15(2): p. 161-73.
80. Wellenstein, D.J., et al., Office-Based Procedures for the Diagnosis and Treatment of Laryngeal
Pathology. J Voice, 2017.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 100PDF page: 100PDF page: 100PDF page: 100
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 101PDF page: 101PDF page: 101PDF page: 101
Chapter 5Safety of flexible endoscopic biopsy of the pharynx and
larynx under topical anesthesia
David J. Wellenstein, MD1,2, Joey K. de Witt, MD1,3, Henrieke W. Schutte MD2, Jimmie Honings MD PhD2, Frank J.A. van den Hoogen MD PhD2, Henri A.M. Marres MD PhD2,
Robert P. Takes MD PhD2, Guido B. van den Broek, MD PhD2
1 These authors contributed equally to this work2 Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands3 Department of Surgery, The Netherlands Cancer Institute,
Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands
European Archives of Otorhinolaryngology. 2017 Sep;274(9):3471-3476.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 102PDF page: 102PDF page: 102PDF page: 102
Chapter 5
102
ABSTRACT
IntroductionRecent advancements in transnasal endoscopy enable a shift in diagnostic workup of lesions in the pharynx and larynx, from an examination with biopsy under general anesthesia to an office-based examination with flexible endoscopic biopsy under topical anesthesia. Procedural complications were evaluated to assess the safety of office-based flexible endoscopic biopsy in patients with benign and malignant laryngopharyngeal lesions.
MethodsPatients who underwent flexible endoscopic biopsy from 2012 to 2016 were evaluated retrospectively. Complications were classified using the Clavien–Dindo classification of surgical complications.
ResultsA total of 201 flexible endoscopic biopsies were performed in 187 patients. Two Clavien–Dindo grade I (laryngospasm and anterior epistaxis), one grade II (laryngeal bleeding), and one grade IIIb (laryngeal edema) complication were observed. The first complication was self-limiting and the other three required an intervention. All patients fully recovered without sequelae.
ConclusionFlexible endoscopic biopsy appears to be a safe office-based procedure for the diagnosis of benign and malignant laryngopharyngeal lesion.
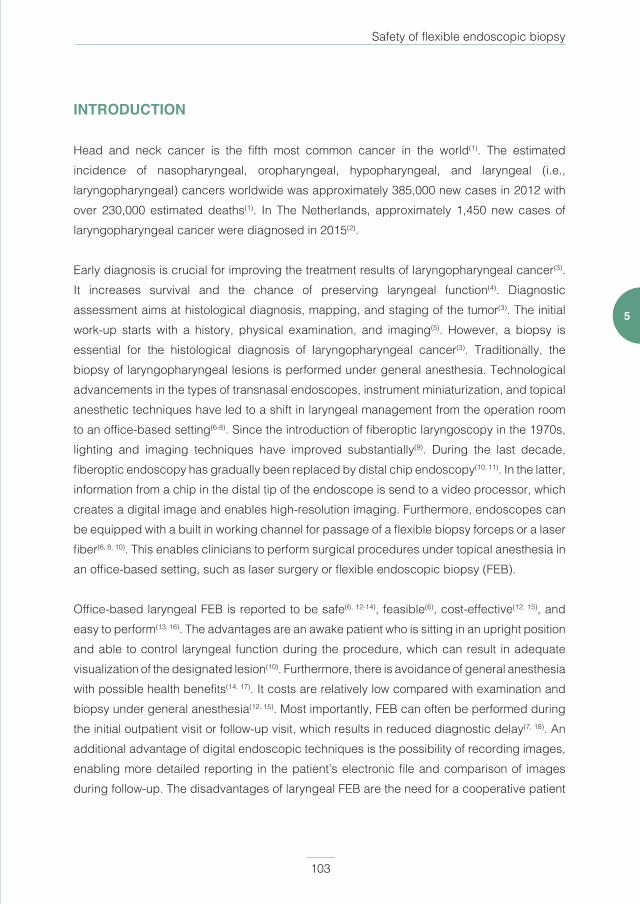
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 103PDF page: 103PDF page: 103PDF page: 103
Safety of flexible endoscopic biopsy
103
5
INTRODUCTION
Head and neck cancer is the fifth most common cancer in the world(1). The estimated incidence of nasopharyngeal, oropharyngeal, hypopharyngeal, and laryngeal (i.e., laryngopharyngeal) cancers worldwide was approximately 385,000 new cases in 2012 with over 230,000 estimated deaths(1). In The Netherlands, approximately 1,450 new cases of laryngopharyngeal cancer were diagnosed in 2015(2).
Early diagnosis is crucial for improving the treatment results of laryngopharyngeal cancer(3). It increases survival and the chance of preserving laryngeal function(4). Diagnostic assessment aims at histological diagnosis, mapping, and staging of the tumor(3). The initial work-up starts with a history, physical examination, and imaging(5). However, a biopsy is essential for the histological diagnosis of laryngopharyngeal cancer(3). Traditionally, the biopsy of laryngopharyngeal lesions is performed under general anesthesia. Technological advancements in the types of transnasal endoscopes, instrument miniaturization, and topical anesthetic techniques have led to a shift in laryngeal management from the operation room to an office-based setting(6-8). Since the introduction of fiberoptic laryngoscopy in the 1970s, lighting and imaging techniques have improved substantially(9). During the last decade, fiberoptic endoscopy has gradually been replaced by distal chip endoscopy(10, 11). In the latter, information from a chip in the distal tip of the endoscope is send to a video processor, which creates a digital image and enables high-resolution imaging. Furthermore, endoscopes can be equipped with a built in working channel for passage of a flexible biopsy forceps or a laser fiber(6, 8, 10). This enables clinicians to perform surgical procedures under topical anesthesia in an office-based setting, such as laser surgery or flexible endoscopic biopsy (FEB).
Office-based laryngeal FEB is reported to be safe(6, 12-14), feasible(6), cost-effective(12, 15), and easy to perform(13, 16). The advantages are an awake patient who is sitting in an upright position and able to control laryngeal function during the procedure, which can result in adequate visualization of the designated lesion(10). Furthermore, there is avoidance of general anesthesia with possible health benefits(14, 17). It costs are relatively low compared with examination and biopsy under general anesthesia(12, 15). Most importantly, FEB can often be performed during the initial outpatient visit or follow-up visit, which results in reduced diagnostic delay(7, 18). An additional advantage of digital endoscopic techniques is the possibility of recording images, enabling more detailed reporting in the patient’s electronic file and comparison of images during follow-up. The disadvantages of laryngeal FEB are the need for a cooperative patient
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 104PDF page: 104PDF page: 104PDF page: 104
Chapter 5
104
(e.g., able to sit still, minimal gag reflex)(8) and the inability to perform deep biopsies of submucosal tumors(12).
Due to the relative novelty of this office-based procedure, few studies are available and complication rates have been assessed in small sample sizes(6, 7, 12-14, 19). Therefore, the aim of this study was to investigate the complications of transnasal FEB under topical anesthesia in patients with benign and malignant laryngopharyngeal lesions. This study provides a more detailed insight into the safety of the procedure. To assess safety, complications were evaluated using the Clavien–Dindo classification, which is an objective scoring system for classifying complications and is also reproducible(20). To our knowledge, the investigated study population is the largest in the literature.
MATERIALS AND METHODS
Patient selectionThis retrospective cohort study was conducted from April 2012 to April 2016 at the Department of Otorhinolaryngology and Head and Neck Surgery of the Radboud University Medical Center in Nijmegen, The Netherlands. Eligible study participants were patients aged 18 years or older who underwent transnasal FEB under topical anesthesia for benign or malignant laryngopharyngeal lesions. Anticoagulant (i.e., thrombocyte aggregation inhibitors, adenosine diphosphate receptor inhibitors, and vitamin K antagonists) use was not considered a contraindication. Submucosal lesions or lesions with undefined tumor margins visualized during diagnostic flexible laryngoscopy were excluded. These patients were excluded because the FEB procedure was performed not only to obtain a histological diagnosis, but also to provide information on tumor size and stage. Patients who underwent multiple biopsies for recurrent lesions or for two separate suspected laryngopharyngeal lesions were included twice.
Diagnostic work-upIn this study, FEB was the first choice for diagnostic work-up of benign and malignant laryngopharyngeal lesions, as shown in figure 1. Patients visiting the outpatient clinic of our department usually receive FEB the same day. As all other diagnostic (imaging) procedures are performed within two days and the results of histological and cytological examination are available within one day, each case can be discussed in the multidisciplinary head and neck oncology tumor board meeting after two days. The histology result of laryngeal FEB was positive for malignancy (i.e., malignant result), negative for malignancy (i.e., nonmalignant
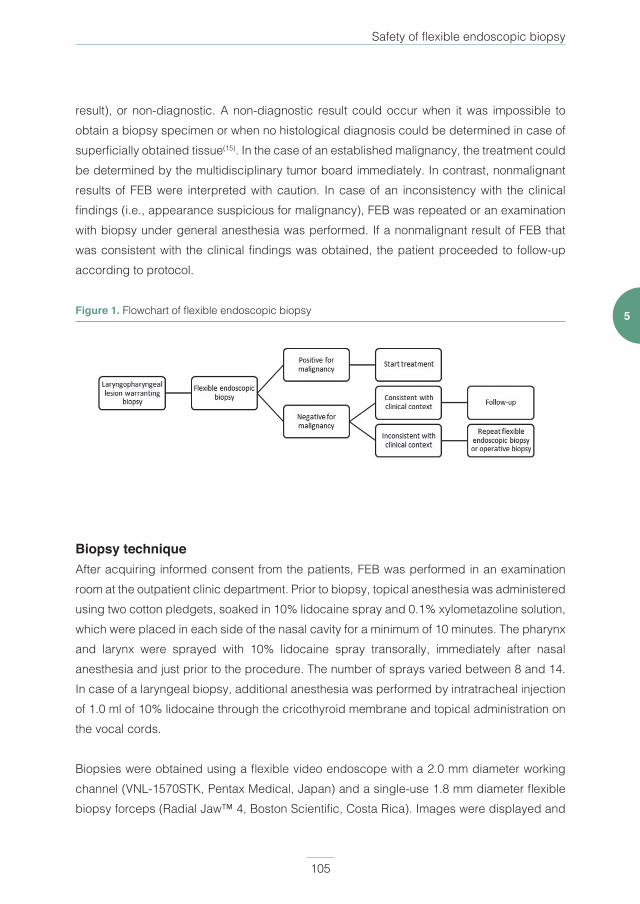
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 105PDF page: 105PDF page: 105PDF page: 105
Safety of flexible endoscopic biopsy
105
5
result), or non-diagnostic. A non-diagnostic result could occur when it was impossible to obtain a biopsy specimen or when no histological diagnosis could be determined in case of superficially obtained tissue(15). In the case of an established malignancy, the treatment could be determined by the multidisciplinary tumor board immediately. In contrast, nonmalignant results of FEB were interpreted with caution. In case of an inconsistency with the clinical findings (i.e., appearance suspicious for malignancy), FEB was repeated or an examination with biopsy under general anesthesia was performed. If a nonmalignant result of FEB that was consistent with the clinical findings was obtained, the patient proceeded to follow-up according to protocol.
Figure 1. Flowchart of flexible endoscopic biopsy
Biopsy techniqueAfter acquiring informed consent from the patients, FEB was performed in an examination room at the outpatient clinic department. Prior to biopsy, topical anesthesia was administered using two cotton pledgets, soaked in 10% lidocaine spray and 0.1% xylometazoline solution, which were placed in each side of the nasal cavity for a minimum of 10 minutes. The pharynx and larynx were sprayed with 10% lidocaine spray transorally, immediately after nasal anesthesia and just prior to the procedure. The number of sprays varied between 8 and 14. In case of a laryngeal biopsy, additional anesthesia was performed by intratracheal injection of 1.0 ml of 10% lidocaine through the cricothyroid membrane and topical administration on the vocal cords.
Biopsies were obtained using a flexible video endoscope with a 2.0 mm diameter working channel (VNL-1570STK, Pentax Medical, Japan) and a single-use 1.8 mm diameter flexible biopsy forceps (Radial Jaw™ 4, Boston Scientific, Costa Rica). Images were displayed and

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 106PDF page: 106PDF page: 106PDF page: 106
Chapter 5
106
recorded using a video processor (EPK-i5000, Pentax Medical, Japan). During biopsy, the flexible video endoscope was inserted transnasally in patients in a sitting position. After visualization of the laryngopharyngeal lesion, a biopsy forceps was passed through the working channel. The lesion was approached with an open jaw biopsy forceps, pushed deep into the lesion, and closed. The biopsy forceps was pulled back swiftly, while feeling for resistance when removing the tissue from the suspected lesion, which indicates a deeply taken biopsy. If possible, 3 deep biopsies were taken from each suspected lesion. All biopsies were performed by two physicians, either head and neck surgeons or senior residents under direct supervision.
Data collection and analysisData were collected on patient characteristics (i.e., sex, age, anticoagulation use, biopsy site, and definitive histological diagnosis) and complications. A complication was defined as any deviation from the normal course after the performance of a FEB procedure(20). To minimize subjectivity in the reporting of complications, terms such as ‘minor’, ‘major’, ‘mild’, or ‘severe’ were avoided. Instead, the Clavien–Dindo classification of surgical complications was used(20). Statistical analysis was performed using IBM Statistical Package for Social Sciences Statistics 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp).
RESULTS
Two hundred and one transnasal FEB procedures in 187 patients were included with 561 obtained biopsies, resulting in an average of 2.8 biopsies per procedure. There were 14 double inclusions, of which 13 were due to suspected recurrent lesions and one patient had two separate tumors that required FEB.
Patient characteristics are shown in table 1. The study population consisted mostly of men (78.6%) of older age (mean 66.8 years). Almost one third of patients used anticoagulants (29.9%). The most common biopsy site was the larynx with 138 biopsies (68.7%). Definitive histology results were squamous cell carcinoma in over half of the cases (57.2%) and severe dysplasia or carcinoma in situ in over one fifth of the cases (21.4%). One histology result showed a lymphoma. In 5 out of 201 procedures, it was impossible to obtain a biopsy specimen. In one patient, the flexible endoscope could not be passed through the nose due to the small nasal anatomy of the patient; in two patients, a complication occurred during biopsy and the procedure, therefore, had to be aborted (i.e., laryngeal bleeding and supraglottic
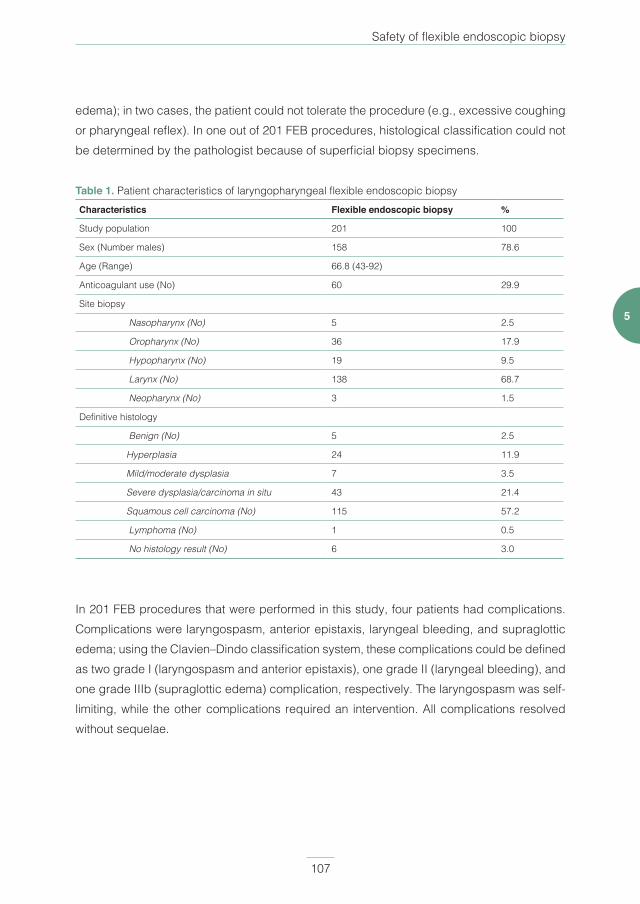
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 107PDF page: 107PDF page: 107PDF page: 107
Safety of flexible endoscopic biopsy
107
5
edema); in two cases, the patient could not tolerate the procedure (e.g., excessive coughing or pharyngeal reflex). In one out of 201 FEB procedures, histological classification could not be determined by the pathologist because of superficial biopsy specimens.
Table 1. Patient characteristics of laryngopharyngeal flexible endoscopic biopsyCharacteristics Flexible endoscopic biopsy %
Study population 201 100
Sex (Number males) 158 78.6
Age (Range) 66.8 (43-92)
Anticoagulant use (No) 60 29.9
Site biopsy
Nasopharynx (No) 5 2.5
Oropharynx (No) 36 17.9
Hypopharynx (No) 19 9.5
Larynx (No) 138 68.7
Neopharynx (No) 3 1.5
Definitive histology
Benign (No) 5 2.5
Hyperplasia 24 11.9
Mild/moderate dysplasia 7 3.5
Severe dysplasia/carcinoma in situ 43 21.4
Squamous cell carcinoma (No) 115 57.2
Lymphoma (No) 1 0.5
No histology result (No) 6 3.0
In 201 FEB procedures that were performed in this study, four patients had complications. Complications were laryngospasm, anterior epistaxis, laryngeal bleeding, and supraglottic edema; using the Clavien–Dindo classification system, these complications could be defined as two grade I (laryngospasm and anterior epistaxis), one grade II (laryngeal bleeding), and one grade IIIb (supraglottic edema) complication, respectively. The laryngospasm was self-limiting, while the other complications required an intervention. All complications resolved without sequelae.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 108PDF page: 108PDF page: 108PDF page: 108
Chapter 5
108
Case 1: LaryngospasmA 61-year-old man was referred to us with a neck metastasis from an unknown primary tumor. During diagnostic flexible laryngoscopy, a small ulcerative lesion was observed on the laryngeal side of the epiglottis. The patient underwent a FEB and after the first biopsy, laryngospasm with stridor occurred. The patient was attended in the outpatient clinic and the symptoms were self-limiting. No further biopsies were performed. The patient underwent an examination under general anesthesia that did not reveal a malignancy. The tumor was defined as an unknown primary and the patient underwent treatment according to protocol.
Case 2: Anterior epistaxisA 63-year-old woman had a FEB for a suspicious lesion in the vallecula with extension up to the epiglottis. After the first biopsy, the patient developed anterior epistaxis. Intranasal cotton pledgets soaked in 0.1% xylometazoline were placed in the right nostril. The anterior epistaxis stopped and 3 more biopsies were performed.
Case 3: Laryngeal bleedingA 73-year-old woman was diagnosed with an intubation granuloma, which she developed after surgery two months earlier. During examination under general anesthesia, adequate visualization of the intubation granuloma was not possible because of the small mandibular space and limited retroflexion of the neck. Therefore, a FEB was scheduled. After injecting topical anesthesia through the cricothyroid membrane of the glottic region, hemoptysis occurred. There were no symptoms of dyspnea or stridor. Nebulized adrenalin and xylometazoline were ineffective, but the laryngeal bleeding stopped after subcutaneous injection of 0.5 mg of adrenalin around the cricothyroid membrane. The patient had an overnight observation in the hospital. On follow-up four weeks later, spontaneous regression of the intubation granuloma was observed during flexible laryngoscopy.
Case 4: Subglottic edemaA 83-year-old man with a medical history of chronic obstructive pulmonary disease and Alzheimer’s disease was referred by the general practitioner to our hospital because of with hoarseness and increasing dyspnea. Treatment with inhalation corticosteroids was started because of suspicion of an exacerbation of the chronic obstructive pulmonary disease. At flexible laryngoscopy, a large bilateral glottic tumor was observed. After taking the first biopsy, the patient experienced a strong pharyngeal reflex and started coughing vigorously. Additional topical anesthesia was administered and the procedure was temporarily paused.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 109PDF page: 109PDF page: 109PDF page: 109
Safety of flexible endoscopic biopsy
109
5
It was not possible to proceed with the FEB because of coughing, and the patient was dismissed from the hospital without additional complaints.
The same evening, the patient was admitted to the emergency department with increasing dyspnea and laryngeal edema was seen during flexible laryngoscopy. He was repeatedly nebulized with 30 ml of salbutamol/ipratropium at 0.1/1.0 mg and administered 0.5 mg adrenalin intravenously. The effect was insufficient, and the patient underwent a tracheotomy in the operation room with biopsies the next day, which histologically showed squamous cell carcinoma of the vocal cords.
DISCUSSION
In the last decade, technological advancements have caused a shift in the evaluation of most laryngopharyngeal lesions from the operating room to an office-based setting(6, 8). However, before a diagnostic method is implemented in clinical practice, several factors need to be considered(14). First, the safety of office-based FEB for laryngopharyngeal lesions has to be determined. The current study showed that 4 complications occurred out of 201 FEB procedures, and each complication did not occur twice. Thus, the incidence was 0.5% for each complication. A few studies reported on the safety of FEB for laryngopharyngeal lesions, showing low complication rates(6, 7, 12-14). Cohen et al. reported 3 complications in 112 patients, including “a post-procedure aspiration in one patient (without serious consequences) and a self-limited epistaxis in two patients”(13). Further description, for example, on the intervention or outcome of these complications, was not provided by the authors. Lippert et al. assessed the safety of FEB in 24 transoral and 76 transnasal procedures(14). No complications were reported and no association was observed with procedure tolerance or biopsy approach. Three other articles, with patient numbers varying from 12 to 76 patients, reported no complications during FEB(6, 7, 12).
To our knowledge, this is currently the largest study cohort for FEB reported in the literature. Furthermore, complications were systematically identified and classified according to a validated protocol. The results of the current study are in line with those of previous studies regarding the complications of FEB for laryngopharyngeal lesions, and showed 4 complications in a total of 201 procedures. Grade I and II complications, anterior epistaxis and laryngeal bleeding, demanded intervention as well as the grade IIIb complication of supraglottic edema. The grade I complication of laryngospasm was self-limiting. It is

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 110PDF page: 110PDF page: 110PDF page: 110
Chapter 5
110
important to note that all complications recovered without sequelae. The case of supraglottic edema resulted in a tracheostomy, which was reversed approximately 2 weeks later.
Contraindications are an important consideration in any surgical procedure. In this study, a patient with a compromised airway was considered an absolute contraindication, which is in agreement with the reported literature(7). In retrospect, the fourth case may not have had a compromised airway during biopsy, but he did have a compromised airway, which required a tracheotomy, when he was admitted to the emergency department. In some studies, anticoagulant use was considered a relative contraindication; patients were advised to stop anticoagulation use, defer the procedure, or they were excluded from further analysis(6, 7,
14, 15). In the current study, anticoagulant use was not considered a contraindication and it was reported in 29.9% of the patients who underwent FEB. One of four patients (25%) with a complication in this cohort used anticoagulants but did not develop bleeding. Although care should be taken in patients who use anticoagulants, we believe that this should not be a factor that prevents an FEB under topical anesthesia.
A limitation of this study was the retrospective study design. Furthermore, there was a possibility of selection bias, and some complications may have developed after the outpatient clinic visit, which might not be included in this study. Also, the physician judged whether a patient could cooperate in FEB under topical anesthesia. This is a subjective measure and it therefore might differ between physicians. It is important to note that this would occur less often with more experience gained with a number of laryngeal FEB procedures and local anesthetic techniques.
CONCLUSION
In this study, FEB for laryngopharyngeal lesions showed low complication rates and we thus conclude that the performance of FEB under topical anesthesia is safe for the histological diagnosis of benign and malignant laryngopharyngeal lesions. These results can contribute to a wider understanding of the possible complications that can occur during FEB and help guide physicians when FEB is first performed in the outpatient clinic.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 111PDF page: 111PDF page: 111PDF page: 111
Safety of flexible endoscopic biopsy
111
5
REFERENCES
1. Ferlay, J., I. Soerjomataram, and M. Ervik. GLOBOCAN 2012 v1.0, Cancer Incidence and
Mortality Worldwide: IARC CencerBase No.11 [Internet]. Lyon, France: International Agency for
Research on Cancer; 2013. Available from: http://globocan.iarc.fr, accessed on 27/05/2016. .
2. Dutch Cancer Registration, managed by Netherlands Comprehensive Cancer Organisation ©
May 2016. Available from: http://cijfersoverkanker.nl/, accessed on 27/05/2016.
3. Chu, E.A. and Y.J. Kim, Laryngeal Cancer: Diagnosis and Preoperative Work-up. Otolaryngologic
Clinics of North America, 2008. 41(4): p. 673-695.
4. Agrawal, N. and P.K. Ha, Management of Early-Stage Laryngeal Cancer. Otolaryngologic Clinics
of North America, 2008. 41(4): p. 757-769.
5. Thekdi, A.A. and R.L. Ferris, Diagnostic assessment of laryngeal cancer. Otolaryngologic Clinics
of North America, 2002. 35(5): p. 953-969.
6. Richards, A.L., et al., The utility of office-based biopsy for laryngopharyngeal lesions: comparison
with surgical evaluation. Laryngoscope, 2015. 125(4): p. 909-12.
7. Zalvan, C.H., et al., Comparison of trans-nasal laryngoscopic office based biopsy of
laryngopharyngeal lesions with traditional operative biopsy. Eur Arch Otorhinolaryngol, 2013.
270(9): p. 2509-13.
8. Wellenstein, D.J., et al., Office-based procedures for diagnosis and treatment of esophageal
pathology. Head Neck, 2017.
9. Williams, G.T., I.M. Farquharson, and J. Anthony, Fibreoptic laryngoscopy in the assessment of
laryngeal disorders. Journal of Laryngology and Otology, 1975. 89(3): p. 299-316.
10. Rosen, C.A., et al., Advances in office-based diagnosis and treatment in laryngology.
Laryngoscope, 2009. 119 Suppl 2: p. S185-212.
11. Eller, R., et al., Flexible Laryngoscopy: A Comparison of Fiber Optic and Distal Chip Technologies.
Part 1: Vocal Fold Masses. Journal of Voice, 2008. 22(6): p. 746-750.
12. Naidu, H., et al., Comparison of efficacy, safety, and cost-effectiveness of in-office cup forcep
biopsies versus operating room biopsies for laryngopharyngeal tumors. J Voice, 2012. 26(5): p.
604-6.
13. Cohen, J.T. and L. Benyamini, Transnasal Flexible Fiberoptic in-office Laryngeal Biopsies-Our
Experience with 117 Patients with Suspicious Lesions. Rambam Maimonides Med J, 2014. 5(2):
p. e0011.
14. Lippert, D., et al., In-office biopsy of upper airway lesions: safety, tolerance, and effect on time to
treatment. Laryngoscope, 2015. 125(4): p. 919-23.
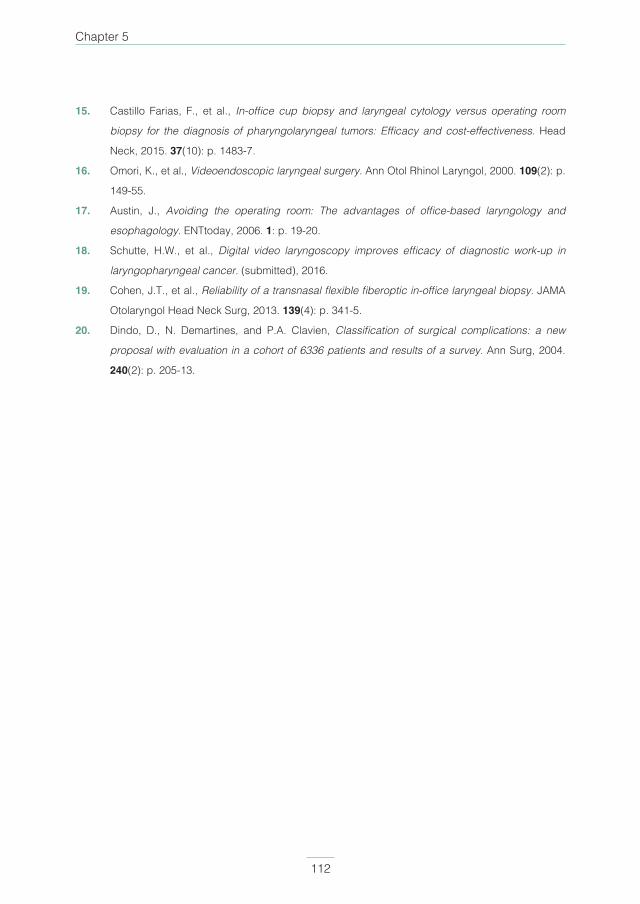
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 112PDF page: 112PDF page: 112PDF page: 112
Chapter 5
112
15. Castillo Farias, F., et al., In-office cup biopsy and laryngeal cytology versus operating room
biopsy for the diagnosis of pharyngolaryngeal tumors: Efficacy and cost-effectiveness. Head
Neck, 2015. 37(10): p. 1483-7.
16. Omori, K., et al., Videoendoscopic laryngeal surgery. Ann Otol Rhinol Laryngol, 2000. 109(2): p.
149-55.
17. Austin, J., Avoiding the operating room: The advantages of office-based laryngology and
esophagology. ENTtoday, 2006. 1: p. 19-20.
18. Schutte, H.W., et al., Digital video laryngoscopy improves efficacy of diagnostic work-up in
laryngopharyngeal cancer. (submitted), 2016.
19. Cohen, J.T., et al., Reliability of a transnasal flexible fiberoptic in-office laryngeal biopsy. JAMA
Otolaryngol Head Neck Surg, 2013. 139(4): p. 341-5.
20. Dindo, D., N. Demartines, and P.A. Clavien, Classification of surgical complications: a new
proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg, 2004.
240(2): p. 205-13.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 113PDF page: 113PDF page: 113PDF page: 113
Safety of flexible endoscopic biopsy
113
5
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 114PDF page: 114PDF page: 114PDF page: 114
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 115PDF page: 115PDF page: 115PDF page: 115
Chapter 6Office-based CO2 laser surgery for benign and
premalignant laryngeal lesions
David J. Wellenstein MD 1, Jimmie Honings MD PhD1, Anouk S. Schimberg MD1, Henrieke W. Schutte MD1, Jasmijn M. Herruer MD PhD1, Frank J.A. van den Hoogen MD PhD1,
Robert P. Takes MD PhD1, Guido B. van den Broek MD PhD1
1 Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands
The Laryngoscope. 2019 Sep 9. doi: 10.1002/lary.28278.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 116PDF page: 116PDF page: 116PDF page: 116
Chapter 6
116
ABSTRACT
ObjectivePatients with laryngeal pathology are often treated with CO2 laser surgery, usually in the operating room under general anesthesia. Although office-based laser surgery using several other laser types has been investigated, prospective studies on office-based CO2 laser surgery are scarce. Our goal was to investigate the feasibility of office-based CO2 laser surgery for benign and premalignant laryngeal pathology by analyzing completion rate, safety, effect on voice quality and success rate (i.e., no residual or recurrent disease).
MethodsA prospective cohort study was performed of 30 consecutive procedures. Inclusion started in June 2016 and was completed in August 2018. Adult patients with clinically benign or premalignant laryngeal lesions who could not undergo transoral laser microsurgery in the operating room under general anesthesia were included. Reasons were either contra-indications for general anesthesia, previously failed therapeutic laryngoscopy under general anesthesia, and preference of a procedure under topical anesthesia by the patient. The mean follow-up was 9 months.
ResultsThirty procedures were performed in 27 patients (24 males) with an average age of 62 years. Twenty-nine (97%) procedures were fully completed without complications. The mean preoperative Voice Handicap Index (VHI) score (VHI 44) significantly decreased 2 months (VHI 28, p = 0.032) and 6 months (VHI 14, p < 0.001) after the procedure. Almost two-thirds of patients showed no residual or recurrent disease at their follow-up visits.
ConclusionOffice-based CO2 laser surgery is a feasible and safe procedure which results in significant voice quality improvement. Almost two-thirds of patients did not require further treatment.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 117PDF page: 117PDF page: 117PDF page: 117
Feasibility of office-based CO2 laser surgery
117
6
INTRODUCTION
For decades, the CO2 laser has been the most frequently used laser in the operating room for removal of laryngeal lesions under general anesthesia(1). After the introduction of digital flexible laryngoscopes with a working channel, a shift has been made in performing surgical procedures on the larynx in an office-based setting under topical anesthesia instead of in the operating room under general anesthesia(2, 3). This evolvement has already led to an extensive practice of office-based laser surgery using the pulsed dye laser and potassium-titanyl-phosphate (KTP) laser(3). Although these studies demonstrated office-based laser surgery to be feasible, effectiveness was variably reported and often only as partial removal of disease(3).
In the past, office-based CO2 laser surgery was impossible to perform due to the absence of a flexible laser fiber that could be passed through the working channel of a flexible laryngoscope. Since this problem has been overcome, flexible fibers for office-based CO2 laser surgery are now commercially available(4, 5). Currently, few studies have reported on the feasibility of office-based CO2 laser surgery for laryngeal pathology, and most are retrospective case series(6-9). Our goal was to prospectively investigate the feasibility of office-based CO2 laser surgery on patients with benign and premalignant laryngeal lesions. Safety, effect on voice quality and effectiveness (i.e. no residual or recurrent disease) of office-based CO2 laser surgery were evaluated.
MATERIALS AND METHODS
Patient inclusionThis prospective study was conducted in accordance with the guidelines established in the Declaration of Helsinki, and was approved by the local medical ethical committee of our institution (file number 2015-2045). The study was conducted in our tertiary referral center. Thirty consecutive procedures were included. Inclusion criteria were adult patients with a clinically benign or premalignant laryngeal lesion. Reasons for undergoing an office-based procedure were either contra-indications for general anesthesia, previously failed therapeutic laryngoscopy under general anesthesia, or a strong preference for a procedure under topical anesthesia by the patient. Patients underwent flexible endoscopic biopsy (FEB) under topical anesthesia to obtain histology prior to office-based laser surgery, according to our department’s protocol(10). An exception was, if patients with a medical history of a benign laryngeal tumor (e.g., laryngeal papilloma) were seen with suspicion of recurrent disease

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 118PDF page: 118PDF page: 118PDF page: 118
Chapter 6
118
during flexible laryngoscopy. In these patients, new biopsies were only obtained in case of doubt on pathology. All patients with malignant pathology found after FEB were excluded. In the early phase of the study, patients underwent FEB just prior to laser treatment in the same session. In a later phase, FEB was performed several days in advance of laser surgery, to prevent bleeding which may interferes with the effectiveness of the CO2 laser. A procedure was considered successful (i.e. success rate) when no residual or recurrent disease was detected after a minimal follow-up of 6 months.
ProcedurePatients were treated in our outpatient clinic surgical procedure room. Patients were instructed and anesthetized (nasal cavity and oropharynx) according to our department’s protocol(10). At the beginning of the study, laryngeal anesthesia was provided by injection through the cricothyroid membrane with 1.0 ml 10% lidocaine. Later on, we used an alternative method for laryngeal anesthesia; 2.5 ml of 4.3% lidocaine was dripped on the larynx through an epidural catheter (Perifix®, B. Braun Medical Inc., Bethlehem, Pennsylvania, USA) that was passed through the working channel of the flexible laryngoscope (VNL-1570STK or VNL-J10, Pentax Medical, Uithoorn, The Netherlands).
A CO2 laser (AcuPulse™ DUO, Lumenis, Yokneam, Israel) with flexible laser fiber (FiberLase ENDURE™, Lumenis, Yokneam, Israel) and matching protection cover were used to perform all office-based procedures. Prior to the start of the procedure, a laser safety check was performed (i.e., no reflecting objects in the room, windows blinded, doors closed, laser fiber and settings checked, proper smoke evacuation of CO2 fumes, patient, surgeons and nurses wearing laser safety glasses, and surgeons and nurses wearing laser masks). Patients were treated while sitting in an upright position. While one clinician performed laryngoscopy and controlled the laser, the other controlled the laser fiber. The laser settings were superpulse, continuous wave mode and 6 Watt energy delivery. Pathology on the right true vocal cord was preferably accessed through the left nasal cavity and on the left vocal cord through the right, in order to guarantee maximum visibility of the laryngeal lesion.
After the procedure, surgeons kept on their masks for ten minutes in order to clear the fumes from the surgical room. Patients were advised no oral intake for one hour and obtain voice rest for three days. Furthermore, patients were asked to complete the Voice Handicap Index (VHI) prior to the procedure, and two and six months after the procedure during outpatient clinic visits(11). This validated questionnaire contains 30 items which score the patients’ voice quality on an emotional, functional and physical level. A VHI
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 119PDF page: 119PDF page: 119PDF page: 119
Feasibility of office-based CO2 laser surgery
119
6
score below 20 corresponds with a normal voice, whereas a score above 60 means that patients experience their decreased voice quality as a handicap(11). Standard follow-up after office-based laser surgery was performed with a consultation by telephone two weeks after the procedure, and outpatient clinic visits 2 and 6 months after the procedure. In some cases, patients were also examined 1 year after the procedure.
AnalysisStatistical analysis was performed using IBM Statistical Package for Social Sciences Statistics 25 (released 2017; IBM, Corp., Armonk, NY) and IBM Statistical Package for Social Sciences Statistics 25.0 (IBM Corp.). A paired t test was used to calculate the statistical significance for VHI scores. A P value of < 0.05 was considered statistical significant.
RESULTS
Since the start of inclusion in June 2016, the target of 30 procedures for benign and premalignant laryngeal pathology was reached in August 2018. Patient characteristics are displayed in Table 1. Leukoplakia and vocal cord polyp were the main clinical indications to perform office-based CO2 laser surgery. Histology revealed vocal cord polyp and hyperplasia in most cases. In four procedures, no histology was obtained (three patients with suspicion of recurrent leukoplakia and one patient with suspicion of recurrent laryngeal papilloma). Twenty-nine (97%) procedures were fully completed. One male patient with suspicion of a polyp on the left true vocal cord developed a severe gag reflex after FEB. Even after additional laryngeal topical anesthesia, laser surgery could not be performed. Histology revealed a polyp. This patient was contacted 2 months after FEB and had an improved voice quality. Although suggested, the patient declined follow-up with flexible laryngoscopy in the outpatient clinic.
In 29 procedures, no complications occurred. The VHI scores prior to the procedures were available in 23 of 29 patients, and revealed a mean score of 44. Two months after the procedure, the mean VHI decreased to 28, which was statistically significant (p = 0.032). After 6-month follow-up, the mean VHI decreased to 14, which was also statistically significant compared to the VHI prior to office-based CO2 laser surgery (p < 0.001). The difference in mean VHI score between two and six months post procedural was not statistically significant (p = 0.091).
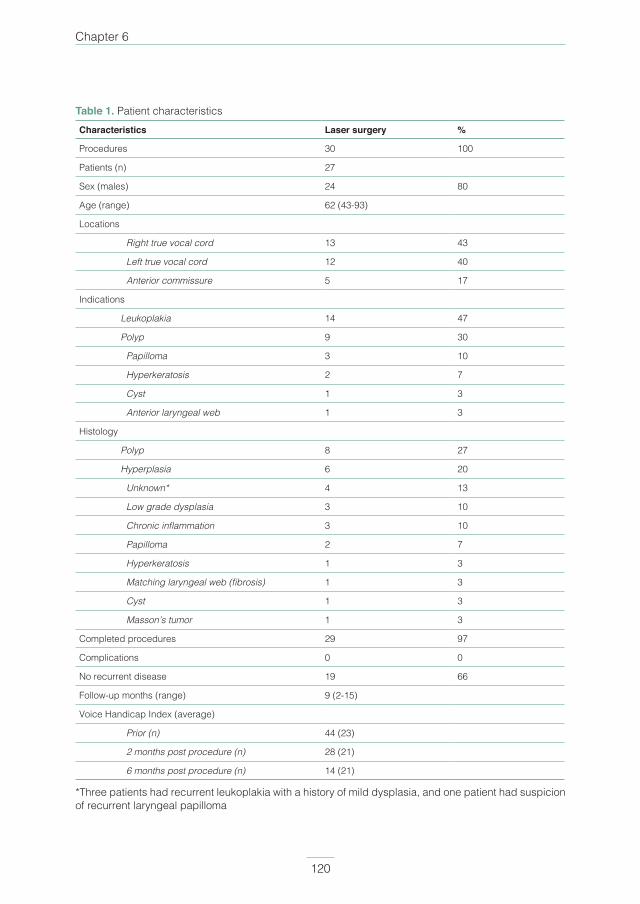
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 120PDF page: 120PDF page: 120PDF page: 120
Chapter 6
120
Table 1. Patient characteristicsCharacteristics Laser surgery %
Procedures 30 100
Patients (n) 27
Sex (males) 24 80
Age (range) 62 (43-93)
Locations
Right true vocal cord 13 43
Left true vocal cord 12 40
Anterior commissure 5 17
Indications
Leukoplakia 14 47
Polyp 9 30
Papilloma 3 10
Hyperkeratosis 2 7
Cyst 1 3
Anterior laryngeal web 1 3
Histology
Polyp 8 27
Hyperplasia 6 20
Unknown* 4 13
Low grade dysplasia 3 10
Chronic inflammation 3 10
Papilloma 2 7
Hyperkeratosis 1 3
Matching laryngeal web (fibrosis) 1 3
Cyst 1 3
Masson’s tumor 1 3
Completed procedures 29 97
Complications 0 0
No recurrent disease 19 66
Follow-up months (range) 9 (2-15)
Voice Handicap Index (average)
Prior (n) 44 (23)
2 months post procedure (n) 28 (21)
6 months post procedure (n) 14 (21)
*Three patients had recurrent leukoplakia with a history of mild dysplasia, and one patient had suspicion of recurrent laryngeal papilloma
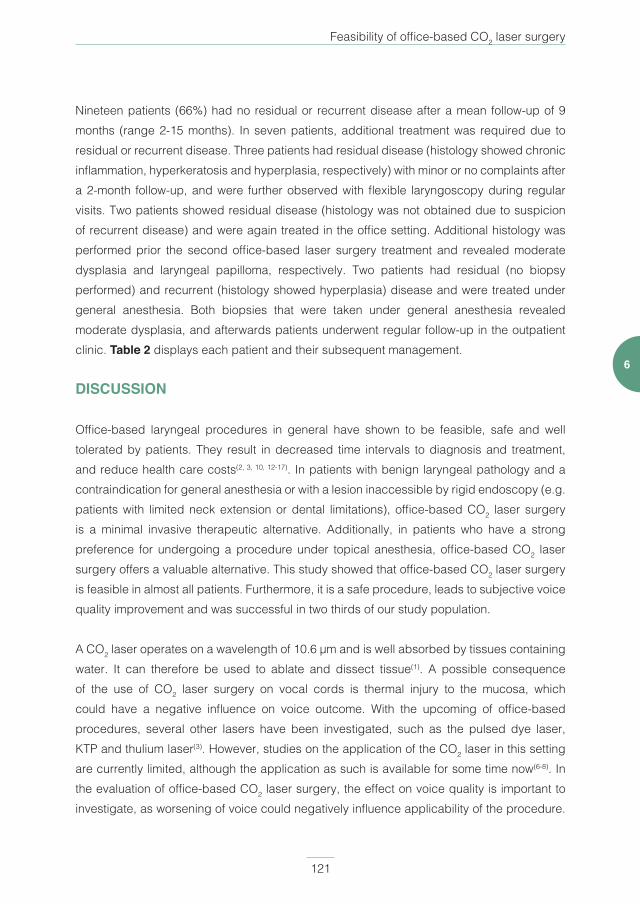
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 121PDF page: 121PDF page: 121PDF page: 121
Feasibility of office-based CO2 laser surgery
121
6
Nineteen patients (66%) had no residual or recurrent disease after a mean follow-up of 9 months (range 2-15 months). In seven patients, additional treatment was required due to residual or recurrent disease. Three patients had residual disease (histology showed chronic inflammation, hyperkeratosis and hyperplasia, respectively) with minor or no complaints after a 2-month follow-up, and were further observed with flexible laryngoscopy during regular visits. Two patients showed residual disease (histology was not obtained due to suspicion of recurrent disease) and were again treated in the office setting. Additional histology was performed prior the second office-based laser surgery treatment and revealed moderate dysplasia and laryngeal papilloma, respectively. Two patients had residual (no biopsy performed) and recurrent (histology showed hyperplasia) disease and were treated under general anesthesia. Both biopsies that were taken under general anesthesia revealed moderate dysplasia, and afterwards patients underwent regular follow-up in the outpatient clinic. Table 2 displays each patient and their subsequent management.
DISCUSSION
Office-based laryngeal procedures in general have shown to be feasible, safe and well tolerated by patients. They result in decreased time intervals to diagnosis and treatment, and reduce health care costs(2, 3, 10, 12-17). In patients with benign laryngeal pathology and a contraindication for general anesthesia or with a lesion inaccessible by rigid endoscopy (e.g. patients with limited neck extension or dental limitations), office-based CO2 laser surgery is a minimal invasive therapeutic alternative. Additionally, in patients who have a strong preference for undergoing a procedure under topical anesthesia, office-based CO2 laser surgery offers a valuable alternative. This study showed that office-based CO2 laser surgery is feasible in almost all patients. Furthermore, it is a safe procedure, leads to subjective voice quality improvement and was successful in two thirds of our study population.
A CO2 laser operates on a wavelength of 10.6 µm and is well absorbed by tissues containing water. It can therefore be used to ablate and dissect tissue(1). A possible consequence of the use of CO2 laser surgery on vocal cords is thermal injury to the mucosa, which could have a negative influence on voice outcome. With the upcoming of office-based procedures, several other lasers have been investigated, such as the pulsed dye laser, KTP and thulium laser(3). However, studies on the application of the CO2 laser in this setting are currently limited, although the application as such is available for some time now(6-8). In the evaluation of office-based CO2 laser surgery, the effect on voice quality is important to investigate, as worsening of voice could negatively influence applicability of the procedure.
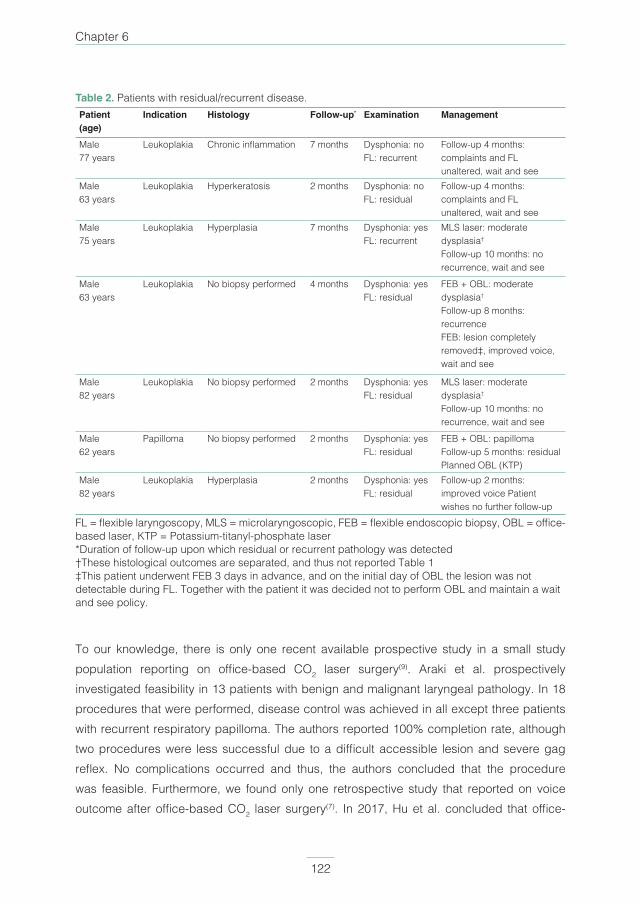
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 122PDF page: 122PDF page: 122PDF page: 122
Chapter 6
122
Table 2. Patients with residual/recurrent disease.Patient(age)
Indication Histology Follow-up* Examination Management
Male 77 years
Leukoplakia Chronic inflammation 7 months Dysphonia: noFL: recurrent
Follow-up 4 months: complaints and FL unaltered, wait and see
Male63 years
Leukoplakia Hyperkeratosis 2 months Dysphonia: noFL: residual
Follow-up 4 months: complaints and FL unaltered, wait and see
Male75 years
Leukoplakia Hyperplasia 7 months Dysphonia: yesFL: recurrent
MLS laser: moderate dysplasia†
Follow-up 10 months: no recurrence, wait and see
Male63 years
Leukoplakia No biopsy performed 4 months Dysphonia: yesFL: residual
FEB + OBL: moderate dysplasia†
Follow-up 8 months: recurrenceFEB: lesion completely removed‡, improved voice, wait and see
Male82 years
Leukoplakia No biopsy performed 2 months Dysphonia: yesFL: residual
MLS laser: moderate dysplasia†
Follow-up 10 months: no recurrence, wait and see
Male62 years
Papilloma No biopsy performed 2 months Dysphonia: yesFL: residual
FEB + OBL: papillomaFollow-up 5 months: residualPlanned OBL (KTP)
Male82 years
Leukoplakia Hyperplasia 2 months Dysphonia: yesFL: residual
Follow-up 2 months: improved voice Patient wishes no further follow-up
FL = flexible laryngoscopy, MLS = microlaryngoscopic, FEB = flexible endoscopic biopsy, OBL = office-based laser, KTP = Potassium-titanyl-phosphate laser*Duration of follow-up upon which residual or recurrent pathology was detected†These histological outcomes are separated, and thus not reported Table 1‡This patient underwent FEB 3 days in advance, and on the initial day of OBL the lesion was not detectable during FL. Together with the patient it was decided not to perform OBL and maintain a wait and see policy.
To our knowledge, there is only one recent available prospective study in a small study population reporting on office-based CO2 laser surgery(9). Araki et al. prospectively investigated feasibility in 13 patients with benign and malignant laryngeal pathology. In 18 procedures that were performed, disease control was achieved in all except three patients with recurrent respiratory papilloma. The authors reported 100% completion rate, although two procedures were less successful due to a difficult accessible lesion and severe gag reflex. No complications occurred and thus, the authors concluded that the procedure was feasible. Furthermore, we found only one retrospective study that reported on voice outcome after office-based CO2 laser surgery(7). In 2017, Hu et al. concluded that office-
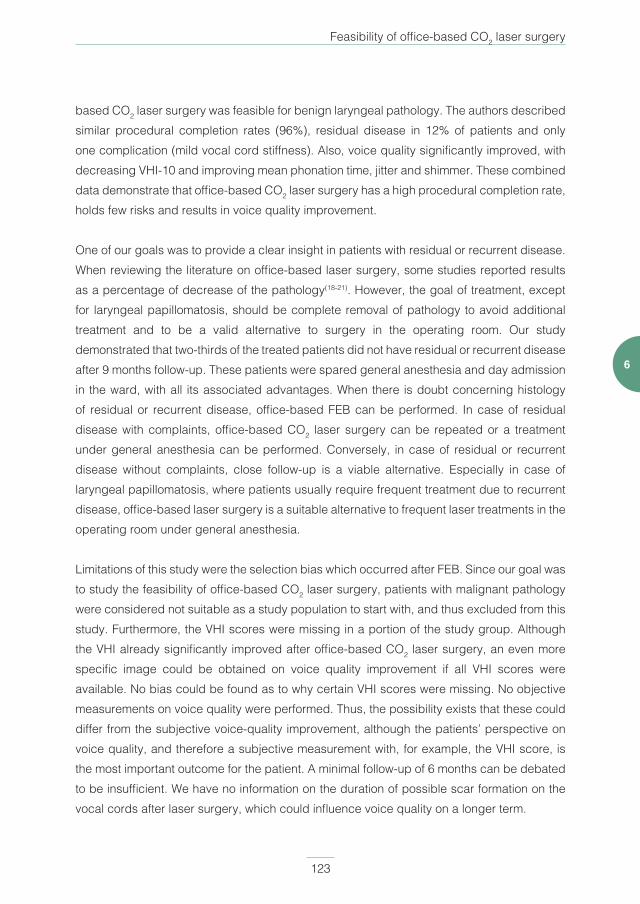
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 123PDF page: 123PDF page: 123PDF page: 123
Feasibility of office-based CO2 laser surgery
123
6
based CO2 laser surgery was feasible for benign laryngeal pathology. The authors described similar procedural completion rates (96%), residual disease in 12% of patients and only one complication (mild vocal cord stiffness). Also, voice quality significantly improved, with decreasing VHI-10 and improving mean phonation time, jitter and shimmer. These combined data demonstrate that office-based CO2 laser surgery has a high procedural completion rate, holds few risks and results in voice quality improvement.
One of our goals was to provide a clear insight in patients with residual or recurrent disease. When reviewing the literature on office-based laser surgery, some studies reported results as a percentage of decrease of the pathology(18-21). However, the goal of treatment, except for laryngeal papillomatosis, should be complete removal of pathology to avoid additional treatment and to be a valid alternative to surgery in the operating room. Our study demonstrated that two-thirds of the treated patients did not have residual or recurrent disease after 9 months follow-up. These patients were spared general anesthesia and day admission in the ward, with all its associated advantages. When there is doubt concerning histology of residual or recurrent disease, office-based FEB can be performed. In case of residual disease with complaints, office-based CO2 laser surgery can be repeated or a treatment under general anesthesia can be performed. Conversely, in case of residual or recurrent disease without complaints, close follow-up is a viable alternative. Especially in case of laryngeal papillomatosis, where patients usually require frequent treatment due to recurrent disease, office-based laser surgery is a suitable alternative to frequent laser treatments in the operating room under general anesthesia.
Limitations of this study were the selection bias which occurred after FEB. Since our goal was to study the feasibility of office-based CO2 laser surgery, patients with malignant pathology were considered not suitable as a study population to start with, and thus excluded from this study. Furthermore, the VHI scores were missing in a portion of the study group. Although the VHI already significantly improved after office-based CO2 laser surgery, an even more specific image could be obtained on voice quality improvement if all VHI scores were available. No bias could be found as to why certain VHI scores were missing. No objective measurements on voice quality were performed. Thus, the possibility exists that these could differ from the subjective voice-quality improvement, although the patients’ perspective on voice quality, and therefore a subjective measurement with, for example, the VHI score, is the most important outcome for the patient. A minimal follow-up of 6 months can be debated to be insufficient. We have no information on the duration of possible scar formation on the vocal cords after laser surgery, which could influence voice quality on a longer term.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 124PDF page: 124PDF page: 124PDF page: 124
Chapter 6
124
Flaws in our study were a change of policy for topical anesthesia administration and timing of biopsy. In the first phase of the study, we used the injection technique through the cricothyroid membrane. Patients reported that this technique was uncomfortable, especially the brief feeling of severe dyspnea that occurs directly after injection of the local anesthetic, while the needle is being retracted from the larynx. Therefore, we chose a less invasive technique during the course of the study which is described above. Our experience was that this technique is less uncomfortable for the patient and resulted in a more properly anesthetized larynx, and is therefore currently our standard method of laryngeal anesthesia for office-based procedures. The procedure is usually well tolerated. In this study, there was one procedure that failed due to extensive coughing, which occurred in a patient anesthetized with the newer technique. Another change in policy during the study was the timing of performing FEB. During the starting phase of the study, FEB was performed just prior to CO2 laser surgery in the same session. After FEB, minor bleeding occurs, which results in less optimal tissue penetration of the CO2 laser. Therefore, during the course of the study, patients underwent FEB 3 days in advance. Although this resulted in more patient inconvenience, since they required an extra outpatient clinic visit, CO2 laser surgery was easier to perform and histology was known prior to treatment.
To our knowledge, this is the largest prospective study, and the only one prospectively investigating voice quality, on office-based CO2 laser surgery for benign and premalignant laryngeal lesions. Our findings are comparable to the results of other authors, and together, these studies offer significant insight in how to perform office-based CO2 laser surgery and hopefully motivate other clinicians to start performing this procedure. In the nearby future, comparison between microlaryngoscopic and office-based CO2 laser surgery with regards to effectiveness, costs and patient experience should be investigated. Furthermore, in patients with small malignant glottic laryngeal carcinoma (i.e. T1a) with severe comorbidity or an inaccessible lesion during rigid microlaryngoscopy, office-based CO2 laser surgery could be an alternative. Although this is a delicate study population, the usual alternative treatment modality is radiotherapy. Future studies should evaluate the value of office based CO2 laser surgery in this group of patients.
CONCLUSION
In conclusion, office-based CO2 laser surgery for benign and premalignant laryngeal lesions is a feasible and safe procedure, which leads to significant voice quality improvement. This procedure is an effective alternative treatment method, especially for patients in whom general

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 125PDF page: 125PDF page: 125PDF page: 125
Feasibility of office-based CO2 laser surgery
125
6
anesthesia is contraindicated, who have an inaccessible lesion during microlaryngoscopy or a strong preference for a procedure under topical anesthesia. Two-thirds of the patients did not require further treatment.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 126PDF page: 126PDF page: 126PDF page: 126
Chapter 6
126
REFERENCES
1. Zeitels SM, JA Burns. Laser applications in laryngology: past, present, and future. Otolaryngol
Clin North Am, 2006. 39(1): p. 159-72.
2. Wellenstein DJ, Schutte HW, Marres HAM, et al. Office-based procedures for diagnosis and
treatment of esophageal pathology. Head Neck, 2017. 39(9): p. 1910-1919.
3. Wellenstein DJ, Schutte HW, Takes RP, etal. Office-Based Procedures for the Diagnosis and
Treatment of Laryngeal Pathology. J Voice, 2018. 32(4): p. 502-513.
4. Devaiah AK, Shapshay SM, Desai U, et al. Surgical utility of a new carbon dioxide laser fiber:
functional and histological study. Laryngoscope 2005. 115(8): p. 1463-8.
5. Zeitels SM, Kobler JB, Heaton JT, Faquin W. Carbon dioxide laser fiber for laryngeal cancer
surgery. Ann Otol Rhinol Laryngol 2006. 115(7): p. 535-41.
6. Koufman JA, Rees CJ, Frazier WD, et al. Office-based laryngeal laser surgery: a review of 443
cases using three wavelengths. Otolaryngol Head Neck Surg 2007. 137(1): p. 146-51.
7. Hu HC, Lin SY, Hung YT, Chang SY. Feasibility and associated limitations of office-based
laryngeal surgery using carbon dioxide lasers. JAMA Otolaryngol Head Neck Surg 2017. 143(5):
p. 485-491.
8. Halum SL, Moberly AC. Patient tolerance of the flexible CO2 laser for office-based laryngeal
surgery. J Voice, 2010. 24(6): p. 750-4.
9. Araki K, Tomifuji M, Uno K, et al. Feasibility of transnasal flexible carbon dioxide laser surgery for
laryngopharyngeal lesions. Auris Nasus Larynx 2019; 46:772–778.<<
10. Wellenstein DJ, de Witt JK, Schutte HW, et al. Safety of flexible endoscopic biopsy of the pharynx
and larynx under topical anesthesia. Eur Arch Otorhinolaryngol 2017. 274(9): p. 3471-3476.
11. Jacobson BH, Johnson A, Grywalski, et al., The Voice Handicap Index (VHI). Am J Speech Lang
Pathol 1997. 6(3): p. 66-70.
12. Naidu H, Noordzij JP, Samim A, Jalisi S, Grillone GA. Comparison of efficacy, safety, and
cost effectiveness of in-office cup forcep biopsies versus operating room biopsies for
laryngopharyngeal tumors. J Voice 2012. 26(5): p. 604-6.
13. Schutte HW, Takes RP, Slootweg PJ, et al. Digital video laryngoscopy and flexible endoscopic
biopsies as an alternative diagnostic workup in laryngopharyngeal cancer: a prospective clinical
study. Ann Otol Rhinol Laryngol, 2018. 127(11): p. 770-776.
14. Lippert D, Hoffman MR, Dang P, McCulloch TM, Hartig GK, Dailey SH. In-office biopsy of upper
airway lesions: safety, tolerance, and effect on time to treatment. Laryngoscope 2015. 125(4): p.
919-23.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 127PDF page: 127PDF page: 127PDF page: 127
Feasibility of office-based CO2 laser surgery
127
6
15. Castillo Farias F, Cobeta I, Souviron R, et al. In-office cup biopsy and laryngeal cytology versus
operating room biopsy for the diagnosis of pharyngolaryngeal tumors: efficacy and cost-
effectiveness. Head Neck, 2015. 37(10): p. 1483-7.
16. Andrade Filho PA, Carrau RL, Buckmire RA. Safety and cost-effectiveness of intra-office flexible
videolaryngoscopy with transoral vocal fold injection in dysphagic patients. Am J Otolaryngol,
2006. 27(5): p. 319-22.
17. Wellenstein DJ, Honings J, Schutte HW, et al. Cost analysis of office-based transnasal
esophagoscopy. Eur Arch Otorhinolaryngol 2019; 276:1457–1463.<<
18. Zeitels SM, Akst LM, Burns JA, Hillman RE, Broadhurst MS, Anderson RR. Office-based 532-nm
pulsed KTP laser treatment of glottal papillomatosis and dysplasia. Ann Otol Rhinol Laryngol
2006; 115:679–685.
19. Zeitels SM, Franco RA Jr, Dailey SH, Burns JA, Hillman RE, Anderson RR. Office-based treatment
of glottal dysplasia and papillomatosis with the 585-nm pulsed dye laser and local anesthesia.
Ann Otol Rhinol Laryngol 2004; 113:265–276.
20. Franco RA Jr. Aminolevulinic acid 585 nm pulsed dye laser photodynamic treatment of laryngeal
keratosis with atypia. Otolaryngol Head Neck Surg 2007; 136:882–887.
21. Sheu M, Sridharan S, Kuhn M, et al. Multi-institutional experience with the in-office potassium
titanyl phosphate laser for laryngeal lesions. J Voice, 2012. 26(6): p. 806-10.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 128PDF page: 128PDF page: 128PDF page: 128
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 129PDF page: 129PDF page: 129PDF page: 129
Chapter 7Cost analysis of office-based transnasal esophagoscopy
David J. Wellenstein MD 1, Jimmie Honings MD PhD1, Henrieke W. Schutte MD1, Jasmijn M. Herruer MD1, Frank J.A. van den Hoogen MD PhD1, Henri A.M. Marres MD PhD1, Robert P.
Takes MD PhD1, Guido B. van den Broek MD PhD1
1 Department of Otorhinolaryngology and Head and Neck Surgery,
Radboud university medical center, Nijmegen, The Netherlands
European Archives of Otorhinolaryngology. 2019 May;276(5):1457-1463.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 130PDF page: 130PDF page: 130PDF page: 130
Chapter 7
130
ABSTRACT
PurposeAlthough office-based transnasal esophagoscopy has been investigated extensively, a cost analysis is still lacking. We performed a cost analysis combined with feasibility study for two diagnostic processes: patients with globus pharyngeus and/or dysphagia, and hypopharyngeal carcinoma.
MethodsProspective cohort study.
ResultsForty-one procedures were performed, of which 35 were fully completed. The procedure was well tolerated with mild complaints such as nasal or pharyngeal pain and burping. Four complications occurred: 2 minor epistaxis and 2 vasovagal reactions. In patients with globus pharyngeus and/or dysphagia, transnasal esophagoscopy resulted in a cost saving of €94.43 (p 0.026) per procedure, compared to our regular diagnostic process. In patients with suspicion of hypopharyngeal carcinoma, cost savings were € 831.41 (p 0.000) per case.
ConclusionsCost analysis showed that office-based transnasal esophagoscopy can provide significant cost savings for the current standard of care. Furthermore, this procedure resulted in good patient acceptability and few complications.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 131PDF page: 131PDF page: 131PDF page: 131
Cost analysis of office-based TNE
131
7
INTRODUCTION
Inspection of the gastrointestinal tract with a flexible fiberoptic transoral endoscope became available in the late 1950s(1). Shortly thereafter, Hirschowitz reported on a flexible fiberoptic esophagoscope with two working channels, enabling suction or obtaining biopsies(2). Since the 1980s, fiberoptic endoscopy has slowly been replaced by distal chip endoscopy. In these endoscopes, a charge-coupled device (CCD) chip is located in the tip of the endoscope and images are seen on a video screen(3). Since then, addition of a working channel in the digital endoscope and enhancement of image quality has transformed the field of diagnostic and therapeutic endoscopy. Through this ongoing development, endoscopes with smaller diameters became available, and thus the first studies were published on transnasal esophagoscopy (TNE) in the 1990s(4, 5).
Since then, TNE has been extensively reported on, and has proved to accurately diagnose esophageal pathology(6-16). Several studies showed better patient acceptability and less cardiopulmonary stress (i.e. rise in blood pressure and heart rate) during TNE, compared to transoral esophagoscopy(4, 15, 17-29). Furthermore, TNE can be used for therapeutic office-based procedures under topical anesthesia, such as foreign body removal or esophageal balloon dilatation(30).
For otorhinolaryngologists and head and neck surgeons, inspection of the esophagus can be useful, in patients suffering from globus pharyngeus or dysphagia, to directly exclude mucosal esophageal pathology. Traditional diagnostics for these patients are limited to flexible pharyngolaryngoscopy, video fluoroscopy, rigid esophagoscopy under general anesthesia, and referral to a gastroenterologist in cases requiring flexible esophageal inspection. Furthermore, in the diagnostic workup of hypopharyngeal carcinoma, inspection of the proximal esophagus is usually performed under general anesthesia to determine the distal border of the tumor. With the introduction of TNE, examination of the esophagus for these indications can be performed in the outpatient clinic under topical anesthesia and additional indications are likely to be developed and established in the future(30, 31).
Although TNE has been extensively investigated in the last two decades, a cost analysis is still awaited(32). There are several articles that reported on cost savings of TNE under topical anesthesia, but most were estimated cost savings(11, 18, 33). Therefore, the goal of this study is to determine the actual cost difference for office-based TNE compared to two regular diagnostic processes. In patients with globus pharyngeus and/or dysphagia, the costs of

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 132PDF page: 132PDF page: 132PDF page: 132
Chapter 7
132
TNE under topical anesthesia are compared with traditional flexible laryngoscopy and video fluoroscopy. In patients suspected of hypopharyngeal carcinoma, costs of TNE under topical anesthesia including taking biopsies are compared to the common practice of inspection under general anesthesia including biopsies. Furthermore, patient experiences and safety were evaluated.
MATERIALS AND METHODS
Patient inclusionThis prospective study was conducted in accordance with the guidelines established in the Declaration of Helsinki and was approved by the local medical ethical committee of our center (2015-2156). We estimated that 35 completed procedures would be sufficient to perform a cost analysis and investigate feasibility of office-based TNE. The first included patient category were adult patients with globus pharyngeus and/or dysphagia. All patients underwent a complete examination, including laryngoscopy, in our hospital or in the hospital from which they were referred. This patient category usually already underwent regular diagnostics (e.g. video fluroscopy) and therapy (e.g. proton pump inhibitor or consultation of a speech language pathologist). Thus, they were examined to exclude a laryngopharyngeal or esophageal malignancy as the cause for their complaints. The second included patient category were patients with suspicion of hypopharyngeal carcinoma. These patients were referred from other (i.e. secondary) hospitals, were a suspicious tumor was seen during flexible laryngoscopy. Other hospitals refer patients immediately in order to reduce diagnostic delay. These patients were examined to identify the tumor, determine the distal extension in relation to the esophagus, and obtain biopsies under topical anesthesia the same day. Furthermore, they also underwent imaging diagnostics according to the national guidelines. There were no exclusion criteria.
SettingThis study was conducted in our tertiary referral center. Patients indicated for one of the two categories where included from January to September 2016. All patients were consecutively included, until 35 completed procedures were performed. This resulted in 41 attempted procedures.
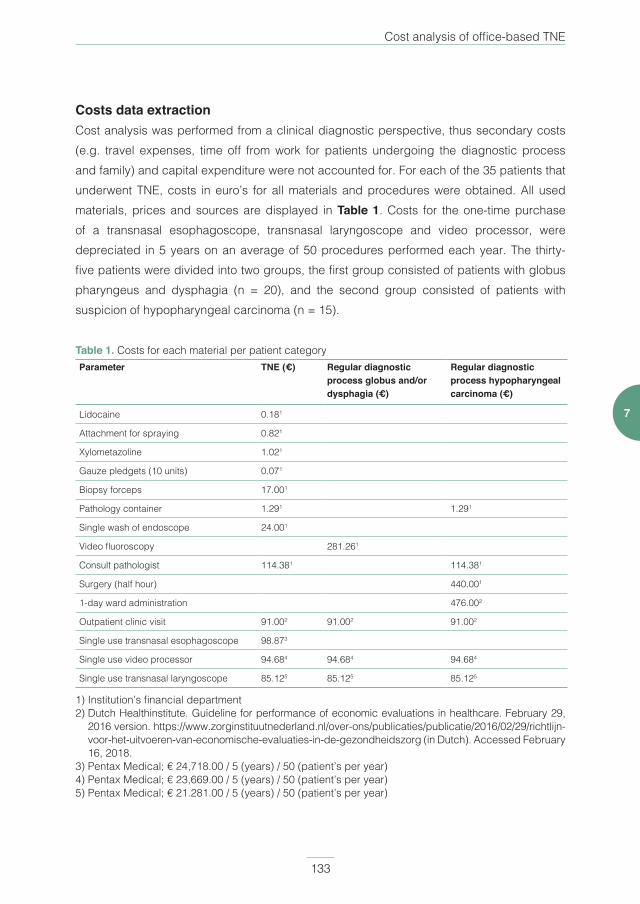
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 133PDF page: 133PDF page: 133PDF page: 133
Cost analysis of office-based TNE
133
7
Costs data extractionCost analysis was performed from a clinical diagnostic perspective, thus secondary costs (e.g. travel expenses, time off from work for patients undergoing the diagnostic process and family) and capital expenditure were not accounted for. For each of the 35 patients that underwent TNE, costs in euro’s for all materials and procedures were obtained. All used materials, prices and sources are displayed in Table 1. Costs for the one-time purchase of a transnasal esophagoscope, transnasal laryngoscope and video processor, were depreciated in 5 years on an average of 50 procedures performed each year. The thirty-five patients were divided into two groups, the first group consisted of patients with globus pharyngeus and dysphagia (n = 20), and the second group consisted of patients with suspicion of hypopharyngeal carcinoma (n = 15).
Table 1. Costs for each material per patient categoryParameter TNE (€) Regular diagnostic
process globus and/or dysphagia (€)
Regular diagnostic process hypopharyngeal carcinoma (€)
Lidocaine 0.181
Attachment for spraying 0.821
Xylometazoline 1.021
Gauze pledgets (10 units) 0.071
Biopsy forceps 17.001
Pathology container 1.291 1.291
Single wash of endoscope 24.001
Video fluoroscopy 281.261
Consult pathologist 114.381 114.381
Surgery (half hour) 440.001
1-day ward administration 476.002
Outpatient clinic visit 91.002 91.002 91.002
Single use transnasal esophagoscope 98.873
Single use video processor 94.684 94.684 94.684
Single use transnasal laryngoscope 85.125 85.125 85.125
1) Institution’s financial department2) Dutch Healthinstitute. Guideline for performance of economic evaluations in healthcare. February 29,
2016 version. https://www.zorginstituutnederland.nl/over-ons/publicaties/publicatie/2016/02/29/richtlijn-voor-het-uitvoeren-van-economische-evaluaties-in-de-gezondheidszorg (in Dutch). Accessed February 16, 2018.
3) Pentax Medical; € 24,718.00 / 5 (years) / 50 (patient’s per year)4) Pentax Medical; € 23,669.00 / 5 (years) / 50 (patient’s per year)5) Pentax Medical; € 21.281.00 / 5 (years) / 50 (patient’s per year)
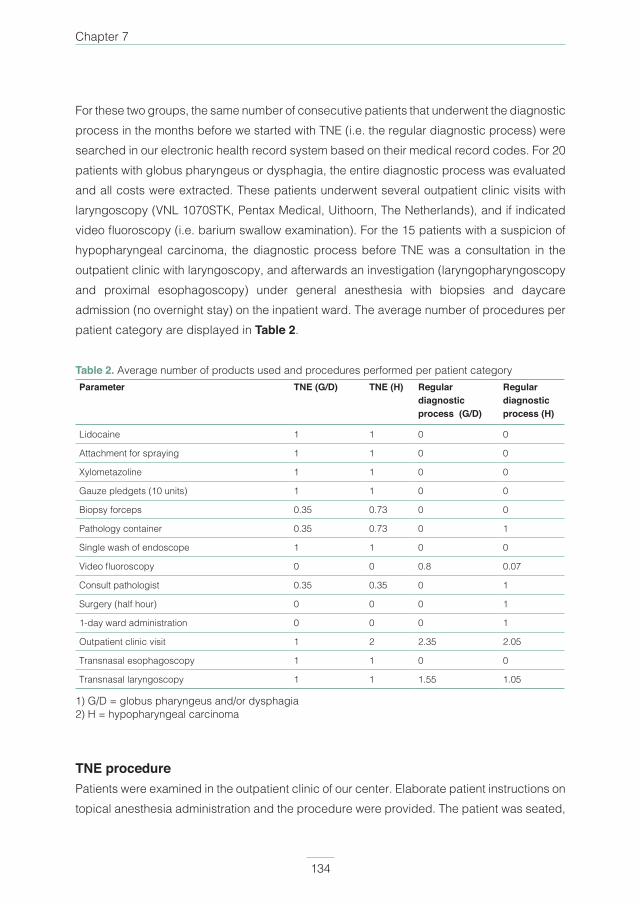
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 134PDF page: 134PDF page: 134PDF page: 134
Chapter 7
134
For these two groups, the same number of consecutive patients that underwent the diagnostic process in the months before we started with TNE (i.e. the regular diagnostic process) were searched in our electronic health record system based on their medical record codes. For 20 patients with globus pharyngeus or dysphagia, the entire diagnostic process was evaluated and all costs were extracted. These patients underwent several outpatient clinic visits with laryngoscopy (VNL 1070STK, Pentax Medical, Uithoorn, The Netherlands), and if indicated video fluoroscopy (i.e. barium swallow examination). For the 15 patients with a suspicion of hypopharyngeal carcinoma, the diagnostic process before TNE was a consultation in the outpatient clinic with laryngoscopy, and afterwards an investigation (laryngopharyngoscopy and proximal esophagoscopy) under general anesthesia with biopsies and daycare admission (no overnight stay) on the inpatient ward. The average number of procedures per patient category are displayed in Table 2.
Table 2. Average number of products used and procedures performed per patient categoryParameter TNE (G/D) TNE (H) Regular
diagnostic process (G/D)
Regular diagnostic process (H)
Lidocaine 1 1 0 0
Attachment for spraying 1 1 0 0
Xylometazoline 1 1 0 0
Gauze pledgets (10 units) 1 1 0 0
Biopsy forceps 0.35 0.73 0 0
Pathology container 0.35 0.73 0 1
Single wash of endoscope 1 1 0 0
Video fluoroscopy 0 0 0.8 0.07
Consult pathologist 0.35 0.35 0 1
Surgery (half hour) 0 0 0 1
1-day ward administration 0 0 0 1
Outpatient clinic visit 1 2 2.35 2.05
Transnasal esophagoscopy 1 1 0 0
Transnasal laryngoscopy 1 1 1.55 1.05
1) G/D = globus pharyngeus and/or dysphagia2) H = hypopharyngeal carcinoma
TNE procedurePatients were examined in the outpatient clinic of our center. Elaborate patient instructions on topical anesthesia administration and the procedure were provided. The patient was seated,
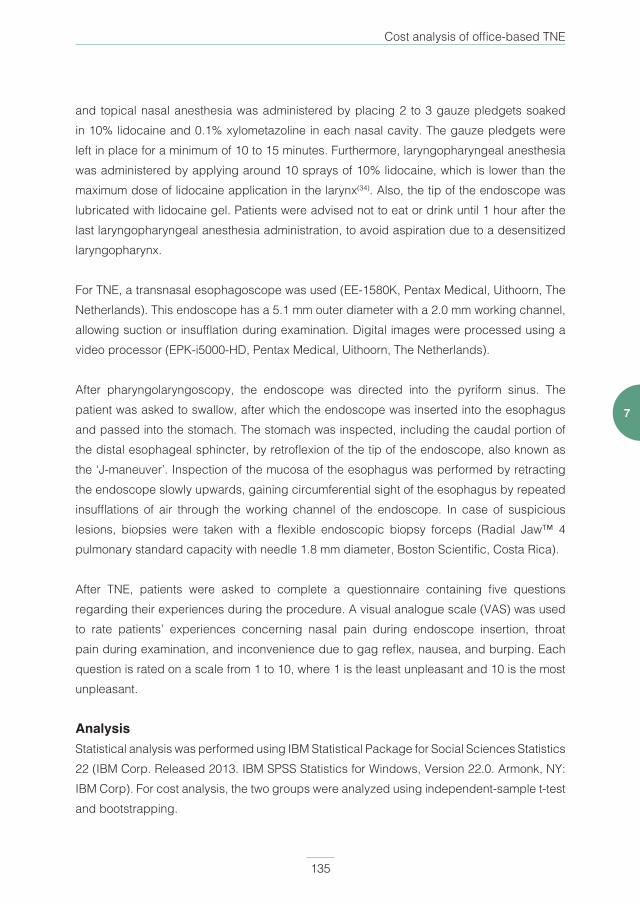
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 135PDF page: 135PDF page: 135PDF page: 135
Cost analysis of office-based TNE
135
7
and topical nasal anesthesia was administered by placing 2 to 3 gauze pledgets soaked in 10% lidocaine and 0.1% xylometazoline in each nasal cavity. The gauze pledgets were left in place for a minimum of 10 to 15 minutes. Furthermore, laryngopharyngeal anesthesia was administered by applying around 10 sprays of 10% lidocaine, which is lower than the maximum dose of lidocaine application in the larynx(34). Also, the tip of the endoscope was lubricated with lidocaine gel. Patients were advised not to eat or drink until 1 hour after the last laryngopharyngeal anesthesia administration, to avoid aspiration due to a desensitized laryngopharynx.
For TNE, a transnasal esophagoscope was used (EE-1580K, Pentax Medical, Uithoorn, The Netherlands). This endoscope has a 5.1 mm outer diameter with a 2.0 mm working channel, allowing suction or insufflation during examination. Digital images were processed using a video processor (EPK-i5000-HD, Pentax Medical, Uithoorn, The Netherlands).
After pharyngolaryngoscopy, the endoscope was directed into the pyriform sinus. The patient was asked to swallow, after which the endoscope was inserted into the esophagus and passed into the stomach. The stomach was inspected, including the caudal portion of the distal esophageal sphincter, by retroflexion of the tip of the endoscope, also known as the ‘J-maneuver’. Inspection of the mucosa of the esophagus was performed by retracting the endoscope slowly upwards, gaining circumferential sight of the esophagus by repeated insufflations of air through the working channel of the endoscope. In case of suspicious lesions, biopsies were taken with a flexible endoscopic biopsy forceps (Radial Jaw™ 4 pulmonary standard capacity with needle 1.8 mm diameter, Boston Scientific, Costa Rica).
After TNE, patients were asked to complete a questionnaire containing five questions regarding their experiences during the procedure. A visual analogue scale (VAS) was used to rate patients’ experiences concerning nasal pain during endoscope insertion, throat pain during examination, and inconvenience due to gag reflex, nausea, and burping. Each question is rated on a scale from 1 to 10, where 1 is the least unpleasant and 10 is the most unpleasant.
AnalysisStatistical analysis was performed using IBM Statistical Package for Social Sciences Statistics 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). For cost analysis, the two groups were analyzed using independent-sample t-test and bootstrapping.
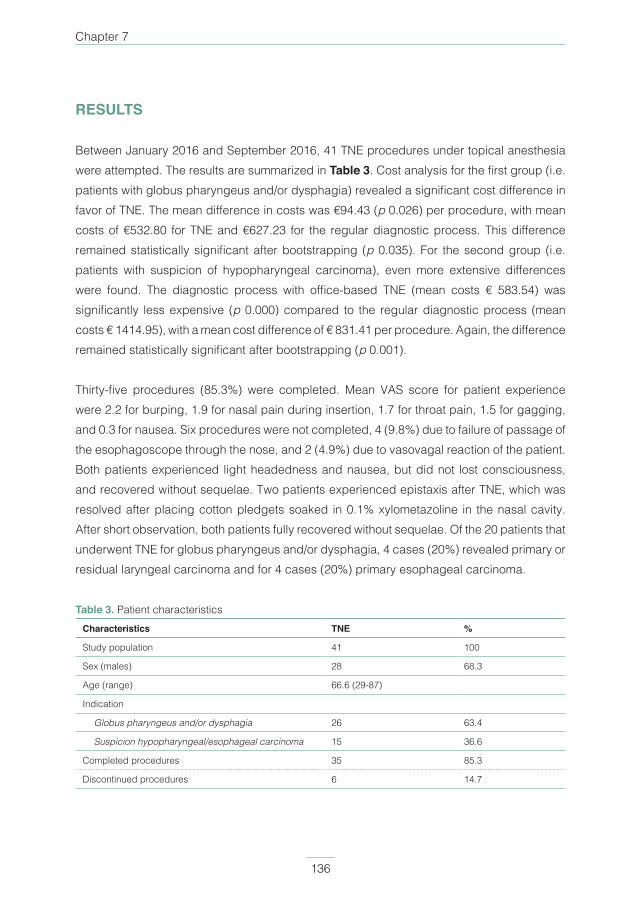
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 136PDF page: 136PDF page: 136PDF page: 136
Chapter 7
136
RESULTS
Between January 2016 and September 2016, 41 TNE procedures under topical anesthesia were attempted. The results are summarized in Table 3. Cost analysis for the first group (i.e. patients with globus pharyngeus and/or dysphagia) revealed a significant cost difference in favor of TNE. The mean difference in costs was €94.43 (p 0.026) per procedure, with mean costs of €532.80 for TNE and €627.23 for the regular diagnostic process. This difference remained statistically significant after bootstrapping (p 0.035). For the second group (i.e. patients with suspicion of hypopharyngeal carcinoma), even more extensive differences were found. The diagnostic process with office-based TNE (mean costs € 583.54) was significantly less expensive (p 0.000) compared to the regular diagnostic process (mean costs € 1414.95), with a mean cost difference of € 831.41 per procedure. Again, the difference remained statistically significant after bootstrapping (p 0.001).
Thirty-five procedures (85.3%) were completed. Mean VAS score for patient experience were 2.2 for burping, 1.9 for nasal pain during insertion, 1.7 for throat pain, 1.5 for gagging, and 0.3 for nausea. Six procedures were not completed, 4 (9.8%) due to failure of passage of the esophagoscope through the nose, and 2 (4.9%) due to vasovagal reaction of the patient. Both patients experienced light headedness and nausea, but did not lost consciousness, and recovered without sequelae. Two patients experienced epistaxis after TNE, which was resolved after placing cotton pledgets soaked in 0.1% xylometazoline in the nasal cavity. After short observation, both patients fully recovered without sequelae. Of the 20 patients that underwent TNE for globus pharyngeus and/or dysphagia, 4 cases (20%) revealed primary or residual laryngeal carcinoma and for 4 cases (20%) primary esophageal carcinoma.
Table 3. Patient characteristicsCharacteristics TNE %
Study population 41 100
Sex (males) 28 68.3
Age (range) 66.6 (29-87)
Indication
Globus pharyngeus and/or dysphagia 26 63.4
Suspicion hypopharyngeal/esophageal carcinoma 15 36.6
Completed procedures 35 85.3
Discontinued procedures 6 14.7
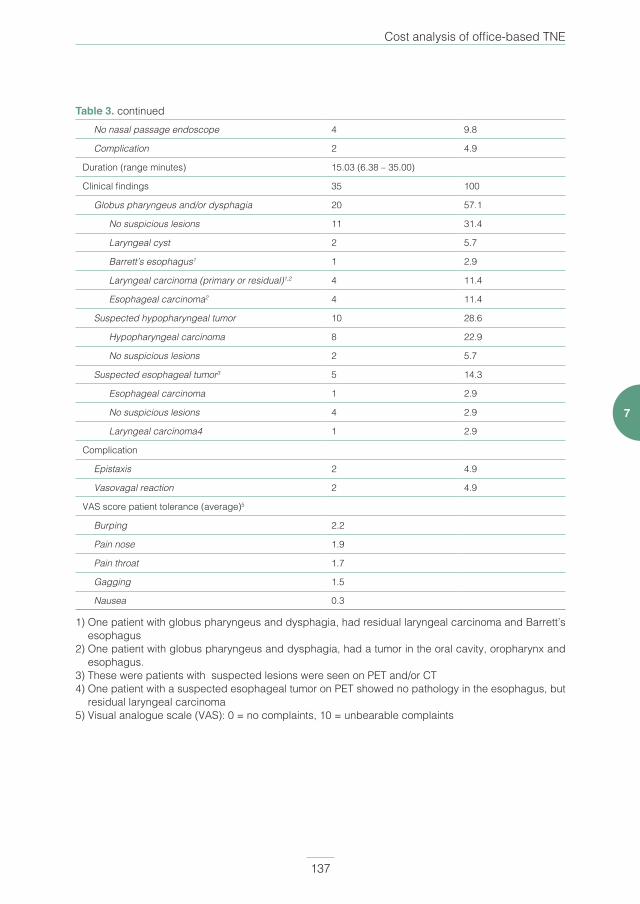
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 137PDF page: 137PDF page: 137PDF page: 137
Cost analysis of office-based TNE
137
7
No nasal passage endoscope 4 9.8
Complication 2 4.9
Duration (range minutes) 15.03 (6.38 – 35.00)
Clinical findings 35 100
Globus pharyngeus and/or dysphagia 20 57.1
No suspicious lesions 11 31.4
Laryngeal cyst 2 5.7
Barrett’s esophagus1 1 2.9
Laryngeal carcinoma (primary or residual)1,2 4 11.4
Esophageal carcinoma2 4 11.4
Suspected hypopharyngeal tumor 10 28.6
Hypopharyngeal carcinoma 8 22.9
No suspicious lesions 2 5.7
Suspected esophageal tumor3 5 14.3
Esophageal carcinoma 1 2.9
No suspicious lesions 4 2.9
Laryngeal carcinoma4 1 2.9
Complication
Epistaxis 2 4.9
Vasovagal reaction 2 4.9
VAS score patient tolerance (average)5
Burping 2.2
Pain nose 1.9
Pain throat 1.7
Gagging 1.5
Nausea 0.3
1) One patient with globus pharyngeus and dysphagia, had residual laryngeal carcinoma and Barrett’s esophagus
2) One patient with globus pharyngeus and dysphagia, had a tumor in the oral cavity, oropharynx and esophagus.
3) These were patients with suspected lesions were seen on PET and/or CT4) One patient with a suspected esophageal tumor on PET showed no pathology in the esophagus, but
residual laryngeal carcinoma5) Visual analogue scale (VAS): 0 = no complaints, 10 = unbearable complaints
Table 3. continued

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 138PDF page: 138PDF page: 138PDF page: 138
Chapter 7
138
DISCUSSION
Although office-based TNE has been extensively investigated in the last decades and several studies mentioned the estimated cost savings for office-based TNE, a cost analysis was never performed(11, 18). Therefore, we conducted this prospective clinical study to analyze the cost savings of TNE for two diagnostic indications, and investigate the feasibility at our tertiary referral center. We demonstrated that office-based TNE provides significant cost savings in patients suffering from globus pharyngeus and/or dysphagia, in whom the primary goal was to exclude an esophageal tumor as the cause of their complaints. Even more significant cost reduction was found in patients with (suspicion of) hypopharyngeal carcinoma that underwent office-based TNE with biopsies. In these patients, examination under general anesthesia with biopsies can be omitted. As was expected, cost savings were even greater compared to cost savings for patients with globus pharyngeus and dysphagia.
An overall advantage of TNE is the favorable patient acceptance, as our own experience and several other studies have shown(30). Only few minor complications occurred, with no long lasting consequences for the patient. When reviewing our complications compared to the literature, we noticed higher rates of epistaxis and vasovagal reaction(30). In patients with globus pharyngeus and/or dysphagia, 20% of the patients had esophageal carcinoma found during TNE. Although this rate was surprisingly high, similar rates have been reported in the literature(30). Patients with globus pharyngeus and/or dysphagia that are referred to our tertiary hospital, are probably a selected group of patients and different, compared to the category of patients that are seen in a non-academic secondary referral clinic. Most esophageal pathology was found in patients suffering from both globus pharyngeus and dysphagia, thus this combination might be a strong indication to perform TNE. An ongoing point of discussion is the screening for second primary tumors in the esophagus by esophagoscopy in patients with hypopharyngeal carcinoma, given the relatively higher incidence of esophageal carcinoma in these patients(30). The short duration of a TNE, with few complications and good patient acceptance, could favor performing TNE, especially if the incidence rates of esophageal carcinoma are as high as found in our study.
Although we did not investigate this in our current study, our experience is that office-based TNE results in a faster diagnostic process(35). In patients with globus pharyngeus and/or dysphagia, office-based TNE gives less burden for the patient. When no pathology is found,
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 139PDF page: 139PDF page: 139PDF page: 139
Cost analysis of office-based TNE
139
7
patients can be reassured immediately and secondary diagnostics (e.g. video fluoroscopy or referral to a gastroenterologist) can be avoided. Furthermore, TNE might replace video fluoroscopy, as it is a faster procedure, with significant cost savings and no radiation exposure. Due to this study, a significant decrease in video fluoroscopy has occurred in our center for patients with globus pharyngeus and/or dysphagia. If esophageal pathology is encountered during endoscopy, histology can also be obtained. All patients referred to us with suspicion of a head and neck malignancy are seen weekly in our multidisciplinary head and neck oncological center. With the introduction of TNE in the diagnostic process, patients with suspected hypopharyngeal carcinoma undergo TNE the same day to identify the distal border of the tumor, and biopsies are obtained. By arranging a fast diagnostic track, biopsies during TNE (instead of endoscopy under general anesthesia) are evaluated within two days by the pathologist and our diagnostic process has shortened from two and a half weeks, to two days.
Potential limitations of this study are the limited number of patients included and the lack of a power analysis, which could result in less reliable data. We chose the number of 35 participants in the context of evaluation of feasibility for TNE at our department. We performed a post hoc power analysis, that showed high power (1 – β 0.91) for the chosen sample size. Furthermore, indirect costs (i.e. secondary costs and capital expenditure) were not evaluated in this study, because our goal was to evaluate the cost savings from a medical perspective. By including these costs, such as travel time and time absence from work of patients and their family, a more robust cost analysis could be performed.
In conclusion, office-based TNE resulted in significant cost savings, for patients with globus pharyngeus and/or dysphagia, and suspicion of hypopharyngeal carcinoma. Furthermore, this procedure resulted in good patient acceptance and had few complications.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 140PDF page: 140PDF page: 140PDF page: 140
Chapter 7
140
REFERENCES
1. Hirschowitz BI, Peters CW, Curtiss LE. Preliminary report on a long fiberscope for examination of
stomach and duodenum. Med Bull (Ann Arbor). 1957;23(5):178-80.
2. Hirschowitz BI. A Fibre Optic Flexible Cesophagoscope. Lancet. 1963;2(7304):388.
3. Marsh BR. Historic development of bronchoesophagology. Otolaryngol Head Neck Surg.
1996;114(6):689-716.
4. Shaker R. Unsedated trans-nasal pharyngoesophagogastroduodenoscopy (T-EGD): technique.
Gastrointest Endosc. 1994;40(3):346-8.
5. Herrmann IF, Recio SA. Laryngeal and Tracheal SurgeryFunctional pharyngoesophagoscopy: A
new technique for diagnostics and analyzing deglutition. Operative Techniques in Otolaryngology-
Head and Neck Surgery. 1997;8(3):163-7.
6. Aviv JE, Takoudes TG, Ma G, Close LG. Office-based esophagoscopy: a preliminary report.
Otolaryngol Head Neck Surg. 2001;125(3):170-5.
7. Belafsky PC, Postma GN, Daniel E, Koufman JA. Transnasal esophagoscopy. Otolaryngol Head
Neck Surg. 2001;125(6):588-9.
8. Postma GN, Bach KK, Belafsky PC, Koufman JA. The role of transnasal esophagoscopy in head
and neck oncology. Laryngoscope. 2002;112(12):2242-3.
9. Andrus JG, Dolan RW, Anderson TD. Transnasal esophagoscopy: a high-yield diagnostic tool.
Laryngoscope. 2005;115(6):993-6.
10. Postma GN, Cohen JT, Belafsky PC, et al. Transnasal esophagoscopy: revisited (over 700
consecutive cases). Laryngoscope. 2005;115(2):321-3.
11. Price T, Sharma A, Snelling J, et al. How we do it: The role of trans-nasal flexible laryngo-
oesophagoscopy (TNFLO) in ENT: one year’s experience in a head and neck orientated practice
in the UK. Clin Otolaryngol. 2005;30(6):551-6.
12. Bennett AM, Sharma A, Price T, Montgomery PQ. The management of foreign bodies in the
pharynx and oesophagus using transnasal flexible laryngo-oesophagoscopy (TNFLO). Ann R
Coll Surg Engl. 2008;90(1):13-6.
13. Cheng CC, Fang TJ, Lee TJ, et al. Role of flexible transnasal esophagoscopy and patient
education in the management of globus pharyngeus. J Formos Med Assoc. 2012;111(3):171-5.
14. Dolan RW, Anderson TD. Practical applications of in-office fiberoptic transnasal esophagoscopy
in the initial evaluation of patients with squamous cell cancer of the head and neck. Ear Nose
Throat J. 2013;92(9):450-5.
15. Chung EJ, Rho YS, Jung KY, Kim JW, Lee SW. The Role of Transnasal Esophagoscopy in ENT
Office: A Prospective, Multicenter Study in Korea. Clin Exp Otorhinolaryngol. 2014;7(2):123-5.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 141PDF page: 141PDF page: 141PDF page: 141
Cost analysis of office-based TNE
141
7
16. Abou-Nader L, Wilson JA, Paleri V. Transnasal oesophagoscopy: diagnostic and management
outcomes in a prospective cohort of 257 consecutive cases and practice implications. Clin
Otolaryngol. 2014;39(2):108-13.
17. Campo R, Montserrat A, Brullet E. Transnasal gastroscopy compared to conventional gastroscopy:
a randomized study of feasibility, safety, and tolerance. Endoscopy. 1998;30(5):448-52.
18. McPartlin DW, Nouraei SA, Tatla T, Howard DJ, Sandhu GS. How we do it: transnasal fibreoptic
oesophagoscopy. Clin Otolaryngol. 2005;30(6):547-50.
19. Sharma A, Price T, Mierzwa K, Montgomery P, Qayyum A, Bradnam T. Transnasal flexible laryngo-
oesophagoscopy: an evaluation of the patient’s experience. J Laryngol Otol. 2006;120(1):24-31.
20. Chang JY, Talley NJ, Locke GR 3rd, et al. Population screening for barrett esophagus: a
prospective randomized pilot study. Mayo Clin Proc. 2011;86(12):1174-80.
21. Kataoka H, Hayano J, Mizushima T, et al. Cardiovascular tolerance and autonomic nervous
responses in unsedated upper gastrointestinal small-caliber endoscopy: a comparison
between transnasal and peroral procedures with newly developed mouthpiece. Dig Endosc.
2011;23(1):78-85.
22. Ai ZL, Lan CH, Fan LL, et al. Unsedated transnasal upper gastrointestinal endoscopy has
favorable diagnostic effectiveness, cardiopulmonary safety, and patient satisfaction compared
with conventional or sedated endoscopy. Surg Endosc. 2012;26(12):3565-72.
23. Chung JW, Park S, Chung MJ, et al. A novel disposable, transnasal esophagoscope: a pilot trial
of feasibility, safety, and tolerance. Endoscopy. 2012;44(2):206-9.
24. Knuth J, Kunze DE, Benz C, et al. Is the transnasal access for esophagogastroduodenoscopy
in routine use equal to the transoral route? A prospective, randomized trial. Z Gastroenterol.
2013;51(12):1369-76.
25. Kadayifci A, Atar M, Parlar S, Balkan A, Koruk I, Koruk M. Transnasal endoscopy is preferred by
transoral endoscopy experienced patients. J Gastrointestin Liver Dis. 2014;23(1):27-31.
26. Streckfuss A, Bosch N, Plinkert PK, Baumann I. Transnasal flexible esophagoscopy (TNE):
an evaluation of the patient’s experience and time management. Eur Arch Otorhinolaryngol.
2014;271(2):323-8.
27. Young VN, Smith LJ, Sulica L, Krishna P, Rosen CA. Patient tolerance of awake, in-office laryngeal
procedures: a multi-institutional perspective. Laryngoscope. 2012;122(2):315-21.
28. Dumortier J, Napoleon B, Hedelius F, et al. Unsedated transnasal EGD in daily practice: results
with 1100 consecutive patients. Gastrointest Endosc. 2003;57(2):198-204.
29. Tsuboi M, Arai M, Maruoka D, et al. Utility and stability of transnasal endoscopy for examination
of the pharynx - a prospective study and comparison with transoral endoscopy. Int J Med Sci.
2013;10(9):1085-91.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 142PDF page: 142PDF page: 142PDF page: 142
Chapter 7
142
30. Wellenstein DJ, Schutte HW, Marres HAM, et al. Office-based procedures for diagnosis and
treatment of esophageal pathology. Head Neck. 2017;Sep;39(9):1910-1919
31. Howell RJ, Pate MB, Ishman SL, Isseroff TF, Rubin AD, Soliman AM, et al. Prospective multi-
institutional transnasal esophagoscopy: Predictors of a change in management. Laryngoscope.
2016;126(12):2667-71.
32. Sabirin J, Abd Rahman M, Rajan P. Changing trends in oesophageal endoscopy: a systematic
review of transnasal oesophagoscopy. ISRN Otolaryngol. 2013;2013:586973.
33. Bush CM, Postma GN. Transnasal esophagoscopy. Otolaryngol Clin North Am. 2013;46(1):41-
52.
34. Wellenstein DJ, van der Wal RAB, Schutte HW, et al. Topical Anesthesia for Endoscopic Office-
based Procedures of the Upper Aerodigestive Tract. J Voice. 2018 Jul 13
35. Schutte HW, Slootweg PJ, Takes RP, et al. Digital video laryngoscopy and flexible endoscopic
biopsies as an alternative diagnostic work-up in laryngopharyngeal cancer; a prospective clinical
study. Ann Otol Rhinol Laryngol. 2018 Nov;127(11):770-776.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 143PDF page: 143PDF page: 143PDF page: 143
Cost analysis of office-based TNE
143
7

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 144PDF page: 144PDF page: 144PDF page: 144

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 145PDF page: 145PDF page: 145PDF page: 145
Chapter 8General discussion

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 146PDF page: 146PDF page: 146PDF page: 146
Chapter 8
146
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 147PDF page: 147PDF page: 147PDF page: 147
General discussion
147
8
Studies on office-based endoscopic surgery in laryngology and head and neck oncology have been slowly emerging over the last decade. This thesis provides a synthesized view on these diagnostic and therapeutic procedures. By identifying differences in technique, and the subsequent advantages and limitations, the reader is provided with more understanding on feasibility of each available procedure. Based on the systematic reviews of literature displayed in Chapter 2, 3 and 4, we further investigated three office-based procedures. In Chapter 5, 6 and 7 clinical studies on FEB, CO2 laser surgery and TNE are found, respectively.
Laryngeal office-based endoscopic proceduresFEB became available when the transnasal esophagoscope with working channel was introduced in the beginning of the 21st century(1). Ten years later, the first clinical studies which used a digital flexible transnasal laryngoscope were published(2, 3). Since then, the number of publications on FEB has been slowly increasing. The available literature has shown that FEB is feasible, safe, and frequently results in a definitive pathologic diagnosis. This, in turn, decreases diagnostic and therapeutic waiting times, and reduces costs. Some studies also compared FEB with biopsies taken under general anesthesia, and found promising results in favor of FEB. When analyzing the literature in our review in Chapter 2, we experienced that reporting on procedural technique was limited and safety was scarcely investigated. Most studies reported on small study populations and not in a systematic manner. We conducted a retrospective cohort study in which we investigated safety of FEB in the largest patient population known to date, and objectively classified and analyzed each complication. Displayed in Chapter 5, this study shows that FEB is a safe procedure with only four independent complications in 201 procedures, in which all patients recovered without sequelae. The primary lessons learned from the outcome of the study were to not perform FEB in patients with a suspected compromised airway (e.g. large bilateral vocal cord tumor) and that anticoagulant use appeared not to be a contra-indication.
In several ways, FEB has significantly changed the diagnostic tract for patients with suspected head and neck malignancy. More recently, other benefits from FEB have been published: 1) The majority of patients are spared from general anesthesia, with assumed health benefits. 2) Significant reduction in time to diagnosis (2 versus 16 days) and treatment (27 versus 41.5) is realized(4). 3) Costs are significantly reduced (€108.64 versus €821.58), since use of the operating room and day admission in the ward became redundant(4). Information on patient experience (patient reported experience measures) was not found in the literature and is an important factor to investigate in future research. Because there are many advantages for
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 148PDF page: 148PDF page: 148PDF page: 148
Chapter 8
148
taking a biopsy in an office-based setting instead of a procedure under general anesthesia, we believe that this should be the standard of care.
Vocal cord injection is the most historically used office-based procedure, and has been extensively investigated. As can be read in Chapter 2, several procedural techniques have been investigated, but comparative data on the most effective approach is still awaited. Over the course of more than a century, many materials for injection have been used and deserted, since each has its own advantages and limitations. Again, studies that compare different materials for effectiveness are lacking. Most studies show that office-based vocal cord injection is feasible and results in voice quality improvement, and several studies reported significant cost savings in favor of the in-office setting.
Office-based laser surgery became possible with the availability of a flexible laser fiber, which can be passed through the working channel of an endoscope(5). The first studies that reported on office-based laser surgery used a pulsed dye laser (PDL) and potassium-titanyl-phosphate (KTP) laser. Later the yttrium-aluminium-garnet (YAG) and carbon dioxide (CO2) laser were introduced. Each laser operates on a different wave length, and thus have their own clinical indications, advantages and limitations. Comparative studies between different lasers are lacking. Office-based PDL and KTP laser surgery are the most investigated procedures, and have shown to be feasible, well tolerated by patients, and resulted in decreased or eradicated vocal cord pathology. There is no uniformity, however, in laser settings which are used for office-based laser surgery. YAG and CO2 lasers are scarcely investigated in an office-based setting. Since the CO2 laser is the most widely used laser in the operating room for laryngeal lesions, we conducted a prospective feasibility study on office-based CO2 laser surgery for benign and premalignant vocal cord lesions. Displayed in Chapter 6, this study shows that CO2 laser surgery is feasible in the majority of patients with benign and premalignant vocal cord lesions and safe in an office-based setting. Furthermore, voice quality significantly improves after six months follow up compared to the pre-procedural voice. Two thirds of the study population show no residual or recurrent disease after follow-up. When critically evaluating our study, patient experience is missing and this should be investigated too, since this an important part of feasibility. Only one prospective and one retrospective study were found that investigated office-based CO2 laser surgery, and these studies showed similar results(6, 7). Since feasibility seems properly investigated, the next step will be to widen the clinical indications for performing office-based CO2 laser surgery. In our prospective study, we included patients with benign and premalignant laryngeal pathology, who either had a contra-indication for general anesthesia, previously failed therapeutic

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 149PDF page: 149PDF page: 149PDF page: 149
General discussion
149
8
laryngoscopy under general anesthesia, or a strong preference for a procedure under topical anesthesia. With our gained experience and results, we now offer this procedure to all patients with benign or premalignant laryngeal pathology. A follow-up study will investigate feasibility of office-based laser surgery in patients with small residual or recurrent vocal cord carcinoma. Different lasers have various treatment characteristics, future research should focus on comparison of lasers for treatment in patients with laryngeal disease. Esophageal office-based endoscopic proceduresFor the esophagus, a similar systematic review of the literature as for the larynx was conducted. In Chapter 3, this review shows that there are five procedures identified on office-based procedures for the proximal esophagus.
Diagnostic TNE is the most investigated office-based procedure, with over 50 studies published. This procedure can be used for pathology concerning the pharynx, larynx and esophagus. Furthermore, a transnasal esophagoscope can be used for the four remaining office-based procedures for the proximal esophagus (i.e. secondary tracheo-esophageal puncture (TEP), foreign body removal, esophageal balloon dilation, and esophageal sphincter injection). TNE shows to be feasible, well tolerated by the patient and has low complication rates. When TNE is compared to transoral esophagoscopy, patients experience similar or better procedural tolerance and authors found comparable accuracy in detecting esophageal pathology. Few studies report on costs for office-based TNE, and all studies estimated the cost difference. Therefore, we conducted a prospective feasibility study on office-based TNE in two head and neck oncological patient categories, and performed a cost analysis compared to our past diagnostic tracts for these patient categories. As can be read in Chapter 7, office-based TNE is feasible, safe and well tolerated by patients with globus pharyngeus and/or dysphagia, or suspicion of hypopharyngeal carcinoma. Furthermore, in both patient categories significant cost reduction was realized. All patients with suspicion of hypopharyngeal carcinoma should undergo a TNE with biopsy and to determine all borders the extension of the tumor. If the distal border can be adequately visualized, these patients are spared from a procedure under general anesthesia. With gained experience, in our opinion TNE should be standardized in the diagnostic track of a head and neck oncological department.
Furthermore, one can consider changing the diagnostic in patients with globus pharyngeus and/or dysphagia. Patients with combined complaints of globus pharyngeus and dysphagia, with suspicion of esophageal lesions, can undergo a TNE instead of video fluoroscopy (i.e.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 150PDF page: 150PDF page: 150PDF page: 150
Chapter 8
150
barium swallow examination). If pathology is found, direct biopsy taking during endoscopic investigation is possible. By gaining more experience with TNE, several new procedures that were identified after writing the review in Chapter 3 are currently studied.
Four other office-based procedures for the proximal esophagus have been identified. Secondary TEP, foreign body removal, esophageal balloon dilation, and esophageal sphincter injection are available office-based procedures. For all procedures, especially in the latter two, available literature is scarce and investigated study populations are small. The studies that were available, showed similarity in results as for all office-based procedures, namely high feasibility, good patient tolerability and few complications. Prospective studies, ideally with larger study populations, are desired for these procedures.
Topical anesthesia for office-based endoscopic surgeryIn order to successfully perform an office-based procedure for laryngeal or esophageal pathology, adequate topical anesthesia is fundamental. In the same manner as both above mentioned systematic reviews of literature, a third review was conducted on topical anesthesia for office-based procedures of the upper aerodigestive tract, presented in Chapter 4. Lidocaine is the most used local anesthetic for office-based procedures of the pharynx and larynx, and results in decreased sensation without interfering with motor functions. For the nasal cavity, topical anesthesia combined with a decongesting agent on cotton pledgets, is effective. For the pharynx, topical anesthesia spray is the most effective method. For the larynx, a small catheter passed through the working channel of the endoscope or an injection through the cricothyroid membrane can be performed to supply topical anesthesia. Complications of lidocaine appliance in the pharynx and larynx are rare. However, comparative studies about the most effective local anesthetic and application method are lacking.
Lessons learnedFor decades, otorhinolaryngologists have used the flexible transnasal laryngoscope on a daily basis to investigate the pharynx and larynx of a patient. Previously, flexible laryngoscopes with working channel were not available. The consequence is, that many otorhinolaryngologists still perform rigid endoscopic procedures in the operating room under general anesthesia. However, because otorhinolaryngologists are familiar with working with an (flexible) endoscope to examine the pharynx and larynx, handling a transnasal flexible endoscope with working channel should be quick to learn. In unpublished data, our research group found no significant difference in procedural success if a first-year resident

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 151PDF page: 151PDF page: 151PDF page: 151
General discussion
151
8
or experienced head and neck surgeon performed FEB. After gaining experience and confidence in diagnostic endoscopic procedures, we recommend starting with therapeutic office-based procedures such as laser surgery.
The success of an office-based procedure is largely dependent on the combination of a cooperative patient and adequate topical anesthesia. By taking time to explain the procedure to a patient, expectations can be managed and the patient is aware of what to expect during the procedure. Furthermore, by talking to a patient during a procedure, and reporting on the process or asking for the patients’ help (e.g. movement of the head in order to create more visibility on an anatomical site), patients are distracted. As a result, cooperation of a patient can be increased. In the discussion in Chapter 4, an elaborate summary on the topical anesthesia techniques we use is given. Independent from local anesthetics or techniques used, it is essential to take the time for the anesthetic to become effective. Especially in laryngeal pathology, where excessive vocal cord movement leads to a difficult procedure, it is advised to test the sensitivity after topical anesthesia by touching the larynx with the endoscope. If movement is still seen, extra topical anesthesia should be applied. We experienced a difficult, or even unsuccessful procedure, if an office-based procedure was started when the larynx was not optimally desensitized. Although better to establish prior to the start of a procedure, applying extra topical anesthesia during a procedure can occasionally still result in completion of a procedure. In case of an uncomfortable patient after applying extra topical anesthesia, one should stop the procedure and plan a procedure in general anesthesia. Continuing the procedure in these patients results mostly in a traumatic experience and an unsuccessful procedure.
It is a challenge, and important aspect, to properly arrange the (technological) infrastructure around office-based procedures. Digital photos and videos, taken during a procedure, have to be coupled to the electronic patient file. Ideally, this has to be programmed automatically, as this will result in less administrative burden for clinicians and a faster consult for clinician and patient. Since systems are constantly being updated, this is a continuous process which needs frequently monitoring, guidance and patience.
Future researchAlthough suggestions have been made for future studies, a major pillar for research in the nearby future is to compare office-based endoscopic procedures with the current golden standard of care (i.e. a procedure under general anesthesia). Although most procedures have already shown to be feasible and safe to perform, we still notice hesitation by clinicians to
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 152PDF page: 152PDF page: 152PDF page: 152
Chapter 8
152
start performing office-based procedures. Although the general opinion is that a randomized controlled trial is the highest form of scientific evidence, we doubt if this is the most suitable study setup for office-based procedures. This will result in a group of patients that will be subjected to general anesthesia and thus associated potential health risks, and diagnostic or therapeutic delay. Alternatives, such as a cohort study with a matched control group, should be considered.
Furthermore, there are a lack of studies on cost differences between office-based procedures and procedures in general anesthesia. The major issue at hand is that each country has its own financial system, and therefore comparing cost-effectiveness is a challenge. There is great variability in hospital costs, hospital charges and physician fees(8).
Since value-based health care has made its introduction in current day medicine, patient reported outcome measures (PROM’s) and patient reported experience measures (PREM’s) have to be part of an adequate cost-effectiveness analysis.
In conclusion, this thesis shows that many office-based procedures are feasible, safe and in line with the current developments in health care, where personalized health care, minimal invasive surgery, innovation, and cost reduction can be realized.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 153PDF page: 153PDF page: 153PDF page: 153
General discussion
153
8
REFERENCES
1. Aviv JE, Takoudes TG, Ma G, Close LG. Office-based esophagoscopy: a preliminary report.
Otolaryngol Head Neck Surg. 2001;125(3):170-5.
2. Postma GN, Bach KK, Belafsky PC, Koufman JA. The role of transnasal esophagoscopy in head
and neck oncology. Laryngoscope. 2002;112(12):2242-3.
3. Naidu H, Noordzij JP, Samim A, Jalisi S, Grillone GA. Comparison of efficacy, safety, and
cost-effectiveness of in-office cup forcep biopsies versus operating room biopsies for
laryngopharyngeal tumors. J Voice. 2012;26(5):604-6.
4. Schutte HW, Takes RP, Slootweg PJ, Arts M, Honings J, van den Hoogen FJA, et al. Digital
Video Laryngoscopy and Flexible Endoscopic Biopsies as an Alternative Diagnostic Workup
in Laryngopharyngeal Cancer: A Prospective Clinical Study. Ann Otol Rhinol Laryngol.
2018;127(11):770-6.
5. Zeitels SM, Burns JA. Laser applications in laryngology: past, present, and future. Otolaryngol
Clin North Am. 2006;39(1):159-72.
6. Hu HC, Lin SY, Hung YT, Chang SY. Feasibility and Associated Limitations of Office-Based
Laryngeal Surgery Using Carbon Dioxide Lasers. JAMA Otolaryngol Head Neck Surg.
2017;143(5):485-91.
7. Araki K, Tomifuji M, Uno K, Suzuki H, Tanaka Y, Tanaka S, et al. Feasibility of transnasal flexible
carbon dioxide laser surgery for laryngopharyngeal lesions. Auris Nasus Larynx. 2019;46(5):772-
8.
8. Schimberg AS, Wellenstein DJ, van den Broek EM, Honings J, van den Hoogen FJA, Marres
HAM, et al. Office-based vs. operating room-performed laryngopharyngeal surgery: a review of
cost differences. Eur Arch Otorhinolaryngol. 2019.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 154PDF page: 154PDF page: 154PDF page: 154
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 155PDF page: 155PDF page: 155PDF page: 155
Chapter 9Appendix 1Appendix 2

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 156PDF page: 156PDF page: 156PDF page: 156
Chapter 9
156
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 157PDF page: 157PDF page: 157PDF page: 157
Appendix
157
9
APPENDIX 1
HISTORY OF LARYNGOSCOPY AND OFFICE-BASED PROCEDURES
There is uncertainty about by whom, and thus when, the first article was published which reported on visualization of the larynx by means of indirect laryngoscopy. Some say that Babington was the first in 1829, although others proclaim that Garcia was the first in 1855(1, 2). In the following years after Garcia’s article, indirect laryngoscopy was further studied and clinically applied by Turck and Czermak(1, 3, 4).
In 1852, Green published the first known article that reported on direct laryngoscopy and treatment of vocal cord pathology(1, 5). When laryngeal topical anesthesia was invented by Jellinek in 1884, the performance of procedures in the larynx under topical anesthesia was made possible(6). Over 10 years later, Kirstein published on direct laryngoscopy and direct endolaryngeal surgery by using topical laryngeal anesthesia(7). This work was extensively proceeded by Chevalier Jackson in the beginning of the 20th century(8).
The endoscopic revolution, which can be considered the basis for allowing the performance of office-based procedures in its current state, was the invention of the flexible fiberoptic laryngoscope. Sawashima and Hirose were the first to publish on the technique in 1968, and it was later extensively clinically investigated in the mid-1970s(9, 10). Already back then, Williams et al. predicted that the implementation of flexible fiberoptic laryngoscopy in daily practice would drastically decrease the number of hospital admissions for direct laryngoscopy under general anesthesia(10). This statement, made over 40 years ago is currently applicable for the performance of office-based procedures, where patients do not have to undergo procedures such as microlaryngoscopy with biopsies, laser surgery or inspection of the proximal esophagus under general anesthesia. In the decades following, and currently still the most used laryngoscope in the office setting, the flexible fiberoptic laryngoscope would become the primary diagnostic tool for laryngopharyngeal pathology. Furthermore, in the 1980s the first articles reporting on the use of flexible fiberoptic laryngoscopy for vocal cord augmentation in an office-based setting were published(11). By visualizing the pharynx and larynx through the nasal cavity, instruments could be passed transorally or percutaneously.
In 1994, Shaker was the first gastroenterologist to report on the use of a fiberoptic transnasal esophagoscope in patients under topical anesthesia(12). The introduction of transnasal esophagoscopy (TNE) under topical anesthesia widened the field of endoscopy in the office

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 158PDF page: 158PDF page: 158PDF page: 158
Chapter 9
158
for otorhinolaryngologists and head and neck surgeons(13). In the beginning of the 21st century, the first reports on digital TNE, and shortly thereafter digital flexible laryngoscopy, became available(14, 15). In 2001, Aviv et al. reported on the integration of a working channel in the digital transnasal esophagoscope, which enabled to perform office-based procedures through the endoscope(14). This was later integrated in the digital flexible laryngoscope, which is shorter in length and smaller in diameter compared to the digital transnasal esophagoscope, thus making it presumably less uncomfortable for the patient and easier to handle for the clinician. With the development of instrumentation that could be passed through the working channel of the endoscope, such as flexible biopsy forceps and laser fibers, we entered a new phase for office-based procedures.
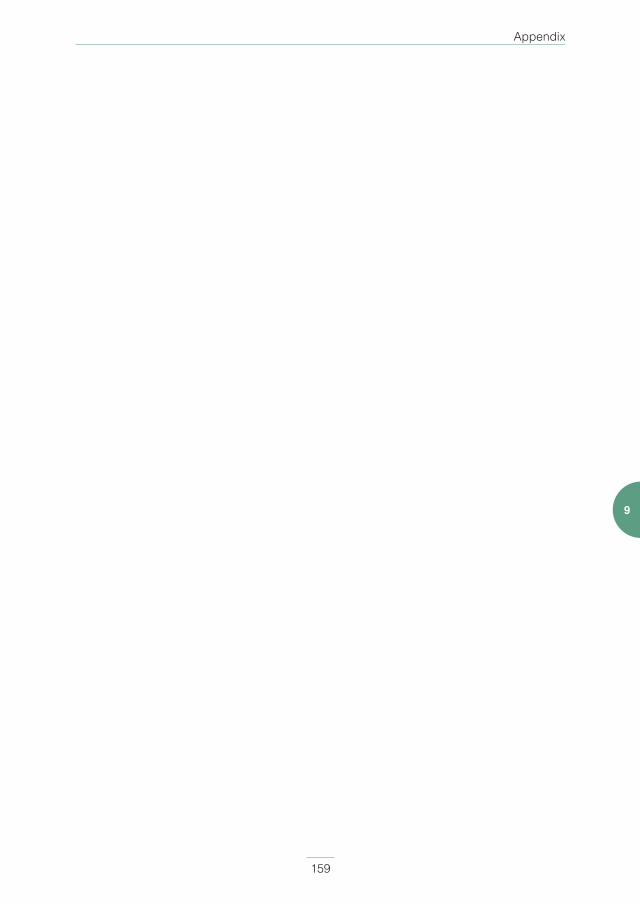
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 159PDF page: 159PDF page: 159PDF page: 159
Appendix
159
9

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 160PDF page: 160PDF page: 160PDF page: 160
Chapter 9
160
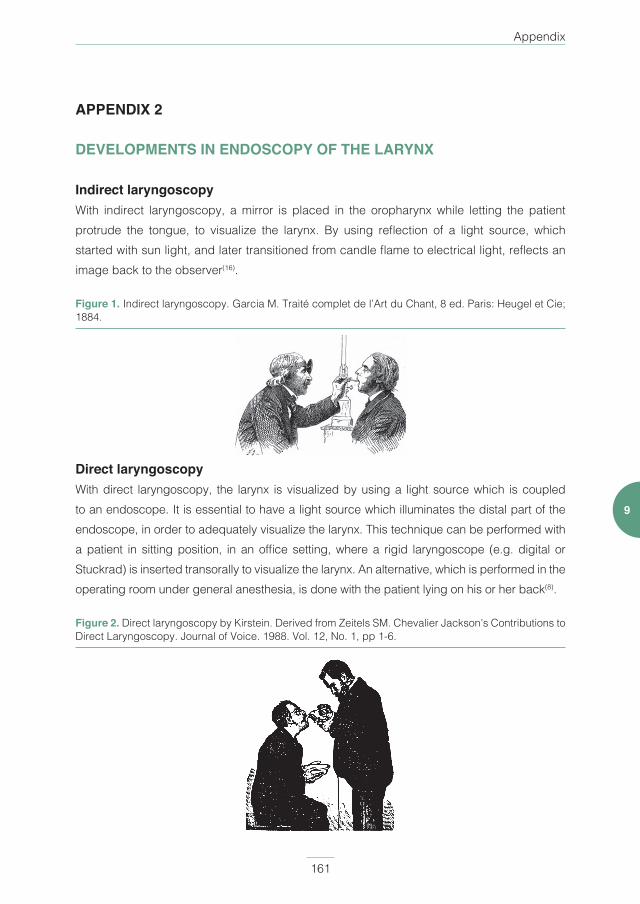
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 161PDF page: 161PDF page: 161PDF page: 161
Appendix
161
9
APPENDIX 2
DEVELOPMENTS IN ENDOSCOPY OF THE LARYNX
Indirect laryngoscopyWith indirect laryngoscopy, a mirror is placed in the oropharynx while letting the patient protrude the tongue, to visualize the larynx. By using reflection of a light source, which started with sun light, and later transitioned from candle flame to electrical light, reflects an image back to the observer(16).
Figure 1. Indirect laryngoscopy. Garcia M. Traité complet de l’Art du Chant, 8 ed. Paris: Heugel et Cie; 1884.
Direct laryngoscopyWith direct laryngoscopy, the larynx is visualized by using a light source which is coupled to an endoscope. It is essential to have a light source which illuminates the distal part of the endoscope, in order to adequately visualize the larynx. This technique can be performed with a patient in sitting position, in an office setting, where a rigid laryngoscope (e.g. digital or Stuckrad) is inserted transorally to visualize the larynx. An alternative, which is performed in the operating room under general anesthesia, is done with the patient lying on his or her back(8).
Figure 2. Direct laryngoscopy by Kirstein. Derived from Zeitels SM. Chevalier Jackson’s Contributions to Direct Laryngoscopy. Journal of Voice. 1988. Vol. 12, No. 1, pp 1-6.
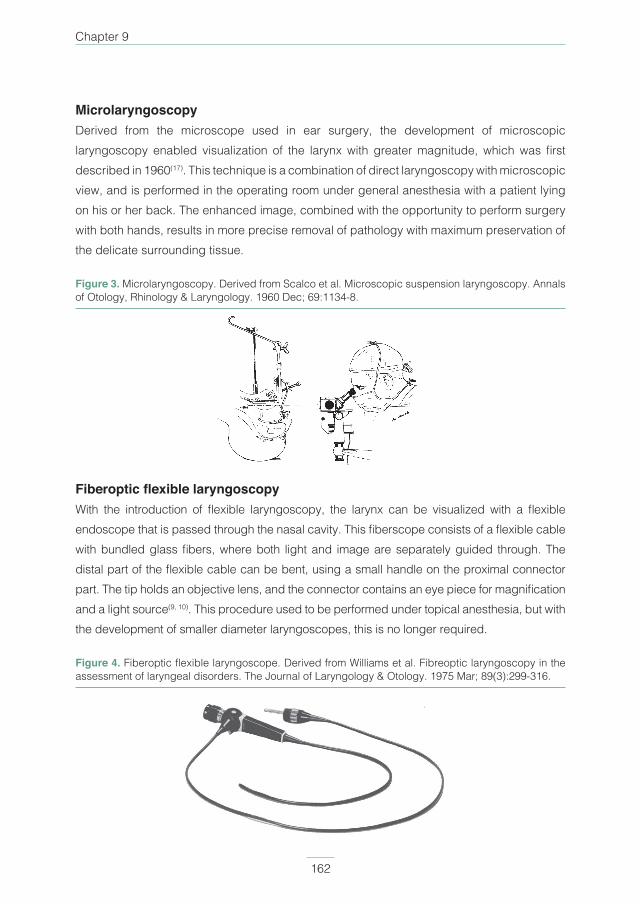
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 162PDF page: 162PDF page: 162PDF page: 162
Chapter 9
162
MicrolaryngoscopyDerived from the microscope used in ear surgery, the development of microscopic laryngoscopy enabled visualization of the larynx with greater magnitude, which was fi rst described in 1960(17). This technique is a combination of direct laryngoscopy with microscopic view, and is performed in the operating room under general anesthesia with a patient lying on his or her back. The enhanced image, combined with the opportunity to perform surgery with both hands, results in more precise removal of pathology with maximum preservation of the delicate surrounding tissue.
Figure 3. Microlaryngoscopy. Derived from Scalco et al. Microscopic suspension laryngoscopy. Annals of Otology, Rhinology & Laryngology. 1960 Dec; 69:1134-8.
Fiberoptic fl exible laryngoscopyWith the introduction of fl exible laryngoscopy, the larynx can be visualized with a fl exible endoscope that is passed through the nasal cavity. This fi berscope consists of a fl exible cable with bundled glass fi bers, where both light and image are separately guided through. The distal part of the fl exible cable can be bent, using a small handle on the proximal connector part. The tip holds an objective lens, and the connector contains an eye piece for magnifi cation and a light source(9, 10). This procedure used to be performed under topical anesthesia, but with the development of smaller diameter laryngoscopes, this is no longer required.
Figure 4. Fiberoptic fl exible laryngoscope. Derived from Williams et al. Fibreoptic laryngoscopy in the assessment of laryngeal disorders. The Journal of Laryngology & Otology. 1975 Mar; 89(3):299-316.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 163PDF page: 163PDF page: 163PDF page: 163
Appendix
163
9
Digital fl exible laryngoscopyWith the development of charged coupled devices (CCDs), the fi rst digital laryngoscopes became available(15). By introducing a chip in the tip of the endoscope (i.e. distal-chip or chip-on-tip endoscopy), the captured light in the distal lens of the endoscope could be transferred to an electrical signal, and converted to a digital image on a computer. As with fl exible fi beroptic laryngoscopy, the procedure is performed in the outpatient clinic and through the nasal cavity. With the current small sized chips, and thus small laryngoscope diameter, topical anesthesia is generally not necessary. Topical anesthesia becomes necessary when a working channel is integrated in the laryngoscope to perform offi ce-based procedures.
Figure 5. Digital fl exible laryngoscope. Derived from Sato et al. Stroboscopic observation of vocal cord fi bration with the videoendoscope. Annals of Otology, Rhinology & Laryngology. 2003 Nov; 112(11):965-70.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 164PDF page: 164PDF page: 164PDF page: 164
Chapter 9
164
REFERENCES
1. Pieters BM, Eindhoven GB, Acott C, van Zundert AA. Pioneers of laryngoscopy: indirect, direct
and video laryngoscopy. Anaesth Intensive Care. 2015;43 Suppl:4-11.
2. Garcia M. Observations on the Human Voice. Proceedings of the Royal Society, London.
1855;3:399-408.
3. Turck L. On the laryngeal mirror and its mode of employment, with engravings on wood. Zeitschrifi
der Gesellschaft der Aertze ze Wein. 1858;26:401-09.
4. Czermak JN. Uber den Kehlkopfspiegel. Wiener MedWochenschrift. 1858;7(13):196-98.
5. Green H. On the surgical treatment of polypi of the larynx, and œdema of the glottis. New York,:
G.P. Putnam; 1852. xi, 9 -124 p. p.
6. Jelinek E. Das Cocain als anastheticum und analgeticum fur den pharynx und larynx. Wien Med
Wochenschr. 1884;45:1334-7, 64-7.
7. Kirstein A. Autoskopie des Larynx und der Trachea (Laryngoscopia directa, Euthyskopie,
Besichtigung ohne Spiegel). Arch Laryngol Rhinol. 1895;3:156-64.
8. Zeitels SM. Chevalier Jackson’s contributions to direct laryngoscopy. J Voice. 1998;12(1):1-6.
9. Sawashima M, Hirose H. New laryngoscopic technique by use of fiber optics. J Acoust Soc Am.
1968;43(1):168-9.
10. Williams GT, Farquharson IM, Anthony J. Fibreoptic laryngoscopy in the assessment of laryngeal
disorders. J Laryngol Otol. 1975;89(3):299-316.
11. Ward PH, Hanson DG, Abemayor E. Transcutaneous Teflon injection of the paralyzed vocal cord:
a new technique. Laryngoscope. 1985;95(6):644-9.
12. Shaker R. Unsedated trans-nasal pharyngoesophagogastroduodenoscopy (T-EGD): technique.
Gastrointest Endosc. 1994;40(3):346-8.
13. Herrmann IF, Recio SA. Functional pharyngoesophagoscopy: a new technique for diagnostics
and analyzing deglutition. Oper Tech Otolaryngol Head Neck Surg. 1997;8(3):163-7.
14. Aviv JE, Takoudes TG, Ma G, Close LG. Office-based esophagoscopy: a preliminary report.
Otolaryngol Head Neck Surg. 2001;125(3):170-5.
15. Sato K, Umeno H, Nakashima T. Stroboscopic observation of vocal fold vibration with the
videoendoscope. Ann Otol Rhinol Laryngol. 2003;112(11):965-70.
16. Rosen CA, Amin MR, Sulica L, Simpson CB, Merati AL, Courey MS, et al. Advances in office-
based diagnosis and treatment in laryngology. Laryngoscope. 2009;119 Suppl 2:S185-212.
17. Scalco AN, Shipman WF, Tabb HG. Microscopic suspension laryngoscopy. Ann Otol Rhinol
Laryngol. 1960;69:1134-8.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 165PDF page: 165PDF page: 165PDF page: 165
Appendix
165
9

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 166PDF page: 166PDF page: 166PDF page: 166
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 167PDF page: 167PDF page: 167PDF page: 167
Chapter 10Summary

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 168PDF page: 168PDF page: 168PDF page: 168
Chapter 10
168
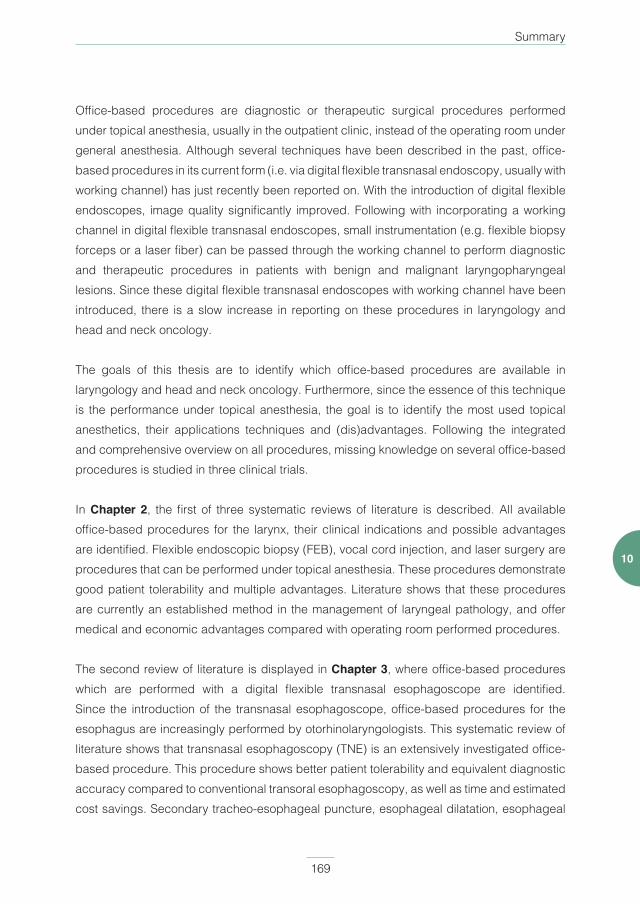
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 169PDF page: 169PDF page: 169PDF page: 169
Summary
169
10
Office-based procedures are diagnostic or therapeutic surgical procedures performed under topical anesthesia, usually in the outpatient clinic, instead of the operating room under general anesthesia. Although several techniques have been described in the past, office-based procedures in its current form (i.e. via digital flexible transnasal endoscopy, usually with working channel) has just recently been reported on. With the introduction of digital flexible endoscopes, image quality significantly improved. Following with incorporating a working channel in digital flexible transnasal endoscopes, small instrumentation (e.g. flexible biopsy forceps or a laser fiber) can be passed through the working channel to perform diagnostic and therapeutic procedures in patients with benign and malignant laryngopharyngeal lesions. Since these digital flexible transnasal endoscopes with working channel have been introduced, there is a slow increase in reporting on these procedures in laryngology and head and neck oncology.
The goals of this thesis are to identify which office-based procedures are available in laryngology and head and neck oncology. Furthermore, since the essence of this technique is the performance under topical anesthesia, the goal is to identify the most used topical anesthetics, their applications techniques and (dis)advantages. Following the integrated and comprehensive overview on all procedures, missing knowledge on several office-based procedures is studied in three clinical trials.
In Chapter 2, the first of three systematic reviews of literature is described. All available office-based procedures for the larynx, their clinical indications and possible advantages are identified. Flexible endoscopic biopsy (FEB), vocal cord injection, and laser surgery are procedures that can be performed under topical anesthesia. These procedures demonstrate good patient tolerability and multiple advantages. Literature shows that these procedures are currently an established method in the management of laryngeal pathology, and offer medical and economic advantages compared with operating room performed procedures.
The second review of literature is displayed in Chapter 3, where office-based procedures which are performed with a digital flexible transnasal esophagoscope are identified. Since the introduction of the transnasal esophagoscope, office-based procedures for the esophagus are increasingly performed by otorhinolaryngologists. This systematic review of literature shows that transnasal esophagoscopy (TNE) is an extensively investigated office-based procedure. This procedure shows better patient tolerability and equivalent diagnostic accuracy compared to conventional transoral esophagoscopy, as well as time and estimated cost savings. Secondary tracheo-esophageal puncture, esophageal dilatation, esophageal
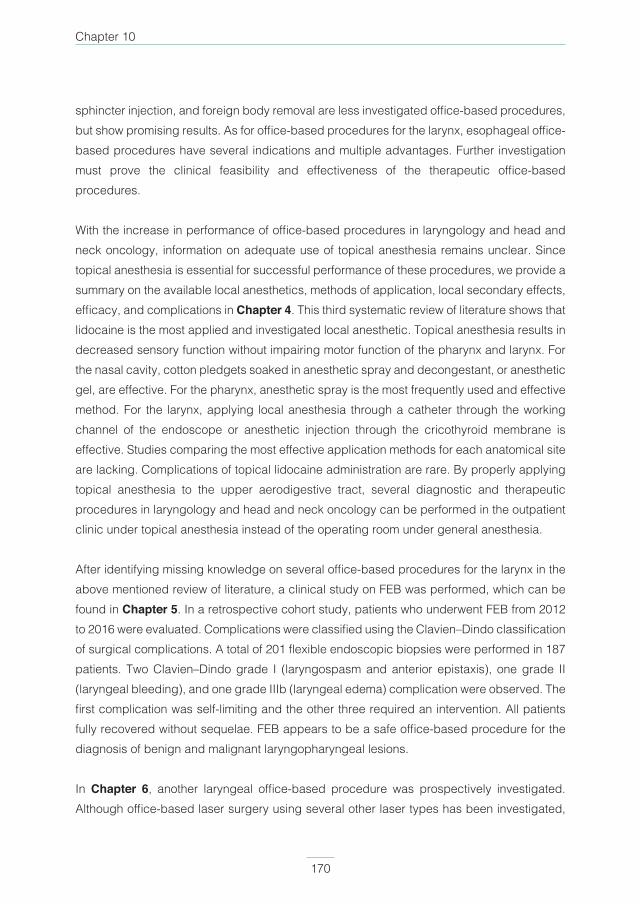
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 170PDF page: 170PDF page: 170PDF page: 170
Chapter 10
170
sphincter injection, and foreign body removal are less investigated office-based procedures, but show promising results. As for office-based procedures for the larynx, esophageal office-based procedures have several indications and multiple advantages. Further investigation must prove the clinical feasibility and effectiveness of the therapeutic office-based procedures.
With the increase in performance of office-based procedures in laryngology and head and neck oncology, information on adequate use of topical anesthesia remains unclear. Since topical anesthesia is essential for successful performance of these procedures, we provide a summary on the available local anesthetics, methods of application, local secondary effects, efficacy, and complications in Chapter 4. This third systematic review of literature shows that lidocaine is the most applied and investigated local anesthetic. Topical anesthesia results in decreased sensory function without impairing motor function of the pharynx and larynx. For the nasal cavity, cotton pledgets soaked in anesthetic spray and decongestant, or anesthetic gel, are effective. For the pharynx, anesthetic spray is the most frequently used and effective method. For the larynx, applying local anesthesia through a catheter through the working channel of the endoscope or anesthetic injection through the cricothyroid membrane is effective. Studies comparing the most effective application methods for each anatomical site are lacking. Complications of topical lidocaine administration are rare. By properly applying topical anesthesia to the upper aerodigestive tract, several diagnostic and therapeutic procedures in laryngology and head and neck oncology can be performed in the outpatient clinic under topical anesthesia instead of the operating room under general anesthesia.
After identifying missing knowledge on several office-based procedures for the larynx in the above mentioned review of literature, a clinical study on FEB was performed, which can be found in Chapter 5. In a retrospective cohort study, patients who underwent FEB from 2012 to 2016 were evaluated. Complications were classified using the Clavien–Dindo classification of surgical complications. A total of 201 flexible endoscopic biopsies were performed in 187 patients. Two Clavien–Dindo grade I (laryngospasm and anterior epistaxis), one grade II (laryngeal bleeding), and one grade IIIb (laryngeal edema) complication were observed. The first complication was self-limiting and the other three required an intervention. All patients fully recovered without sequelae. FEB appears to be a safe office-based procedure for the diagnosis of benign and malignant laryngopharyngeal lesions.
In Chapter 6, another laryngeal office-based procedure was prospectively investigated. Although office-based laser surgery using several other laser types has been investigated,

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 171PDF page: 171PDF page: 171PDF page: 171
Summary
171
10
prospective studies on office-based CO2 laser surgery are scarce. Since the CO2 laser is the most used laser for the treatment of laryngeal pathology in the operating room, our goal was to investigate the feasibility of office-based CO2 laser surgery for benign and premalignant laryngeal lesions by analyzing completion rate, safety, effect on voice quality and success rate (i.e., no residual or recurrent disease). In a prospective cohort study, 30 consecutive procedures were performed and evaluated in adult patients with clinically benign or premalignant laryngeal lesions who could not undergo transoral laser microsurgery in the operating room under general anesthesia. Reasons were either contra-indications for general anesthesia, previously failed therapeutic laryngoscopy under general anesthesia, or preference of a procedure under topical anesthesia by the patient. Twenty-nine (97%) procedures were fully completed without complications. The mean preoperative Voice Handicap Index (VHI) score (VHI 44) significantly decreased 2 months (VHI 28, p = 0.032) and 6 months (VHI 14, p < 0.001) after the procedure. Almost two-thirds of patients showed no residual or recurrent disease at their follow-up visits, and thus did not require further treatment. Thus, office-based CO2 laser surgery is a feasible and safe procedure which results in significant voice quality improvement.
Lastly, although office-based TNE has been investigated extensively, a cost analysis is still lacking. Therefore, found in Chapter 7, we performed a cost analysis combined with a prospective feasibility study for two diagnostic processes: patients with globus pharyngeus and/or dysphagia, and patients with a suspected hypopharyngeal carcinoma. Forty-one procedures were performed, of which 35 (85%) were fully completed. The procedure was well tolerated with mild complaints such as nasal or pharyngeal pain, and burping. Four complications occurred: two minor epistaxis and two vasovagal reactions. In patients with globus pharyngeus and/or dysphagia, TNE resulted in a cost saving of €94.43 (p 0.026) per procedure, compared to our regular diagnostic process. In patients with a suspected hypopharyngeal carcinoma, cost savings were €831.41 (p 0.000) per case. In conclusion, office-based TNE is a feasible procedure with good patient acceptability and few complications. Furthermore, cost analysis showed that office-based TNE can provide significant cost savings for the current standard of care.
This thesis shows that, with the introduction of digital flexible transnasal endoscopes, either with or without a working channel, there has been an increase in the performance of office-based procedures in laryngology and head and neck oncology. Several office-based procedures are extensively investigated and have shown to be feasible, safe and well tolerated by the patient. While for other procedures, more studies are still awaited. Overall,

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 172PDF page: 172PDF page: 172PDF page: 172
Chapter 10
172
these procedures are in line with the current development in health care where personalized health care, minimal invasive surgery, innovation, and cost reduction can be realized.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 173PDF page: 173PDF page: 173PDF page: 173
Summary
173
10
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 174PDF page: 174PDF page: 174PDF page: 174

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 175PDF page: 175PDF page: 175PDF page: 175
Chapter 11Summary in Dutch

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 176PDF page: 176PDF page: 176PDF page: 176
Chapter 11
176
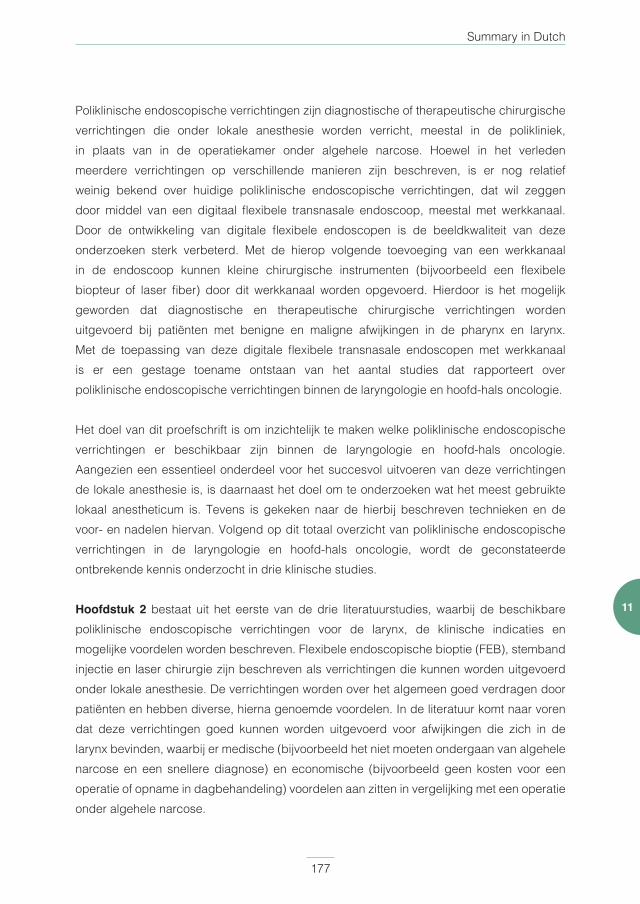
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 177PDF page: 177PDF page: 177PDF page: 177
Summary in Dutch
177
11
Poliklinische endoscopische verrichtingen zijn diagnostische of therapeutische chirurgische verrichtingen die onder lokale anesthesie worden verricht, meestal in de polikliniek, in plaats van in de operatiekamer onder algehele narcose. Hoewel in het verleden meerdere verrichtingen op verschillende manieren zijn beschreven, is er nog relatief weinig bekend over huidige poliklinische endoscopische verrichtingen, dat wil zeggen door middel van een digitaal flexibele transnasale endoscoop, meestal met werkkanaal. Door de ontwikkeling van digitale flexibele endoscopen is de beeldkwaliteit van deze onderzoeken sterk verbeterd. Met de hierop volgende toevoeging van een werkkanaal in de endoscoop kunnen kleine chirurgische instrumenten (bijvoorbeeld een flexibele biopteur of laser fiber) door dit werkkanaal worden opgevoerd. Hierdoor is het mogelijk geworden dat diagnostische en therapeutische chirurgische verrichtingen worden uitgevoerd bij patiënten met benigne en maligne afwijkingen in de pharynx en larynx. Met de toepassing van deze digitale flexibele transnasale endoscopen met werkkanaal is er een gestage toename ontstaan van het aantal studies dat rapporteert over poliklinische endoscopische verrichtingen binnen de laryngologie en hoofd-hals oncologie.
Het doel van dit proefschrift is om inzichtelijk te maken welke poliklinische endoscopische verrichtingen er beschikbaar zijn binnen de laryngologie en hoofd-hals oncologie. Aangezien een essentieel onderdeel voor het succesvol uitvoeren van deze verrichtingen de lokale anesthesie is, is daarnaast het doel om te onderzoeken wat het meest gebruikte lokaal anestheticum is. Tevens is gekeken naar de hierbij beschreven technieken en de voor- en nadelen hiervan. Volgend op dit totaal overzicht van poliklinische endoscopische verrichtingen in de laryngologie en hoofd-hals oncologie, wordt de geconstateerde ontbrekende kennis onderzocht in drie klinische studies.
Hoofdstuk 2 bestaat uit het eerste van de drie literatuurstudies, waarbij de beschikbare poliklinische endoscopische verrichtingen voor de larynx, de klinische indicaties en mogelijke voordelen worden beschreven. Flexibele endoscopische bioptie (FEB), stemband injectie en laser chirurgie zijn beschreven als verrichtingen die kunnen worden uitgevoerd onder lokale anesthesie. De verrichtingen worden over het algemeen goed verdragen door patiënten en hebben diverse, hierna genoemde voordelen. In de literatuur komt naar voren dat deze verrichtingen goed kunnen worden uitgevoerd voor afwijkingen die zich in de larynx bevinden, waarbij er medische (bijvoorbeeld het niet moeten ondergaan van algehele narcose en een snellere diagnose) en economische (bijvoorbeeld geen kosten voor een operatie of opname in dagbehandeling) voordelen aan zitten in vergelijking met een operatie onder algehele narcose.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 178PDF page: 178PDF page: 178PDF page: 178
Chapter 11
178
Het tweede literatuuronderzoek, dat is terug te vinden in Hoofdstuk 3, gaat over de toepasbaarheid van poliklinische endoscopische verrichtingen voor de oesofagus. Met de ontwikkeling van de flexibele transnasale oesofagoscoop worden poliklinische endoscopische verrichtingen onder lokale anesthesie voor de oesofagus in toenemende mate door KNO-artsen en hoofd-hals chirurgen uitgevoerd. Dit literatuuronderzoek heeft op dezelfde systematische manier als het onderzoek in Hoofdstuk 2 onderzocht welke diagnostische en therapeutische mogelijkheden er zijn. Het diagnostisch onderzoek van de oesofagus door middel van transnasale oesofagoscopie (TNE) is uitvoerig onderzocht in de literatuur. Deze verrichting wordt beter verdragen door de patiënt en laat een even grote nauwkeurigheid zien in vergelijking met de conventionele transorale oesofagoscopie, die wordt uitgevoerd door Maag-, Darm- en Lever (MDL)-artsen. Daarnaast is deze verrichting sneller en wordt er in een aantal studies geschat, en door ons onderzoek bevestigd (zie Hoofdstuk 7), dat de kosten lager zijn. Mogelijke therapeutische poliklinische behandelingen onder lokale anesthesie in de oesofagus zijn de secundaire tracheo-oesofageale punctie, dilatatie van de oesofagus, oesofageale sfincter injectie en corpus alienum verwijdering. Hoewel er minder wetenschappelijke literatuur beschikbaar is voor deze therapeutische verrichtingen, laten ze veelbelovende uitkomsten zien. De klinische haalbaarheid en effectiviteit moet nog verder worden onderzocht. De voordelen van deze verrichtingen zijn conform Hoofdstuk 2.
De hierboven beschreven toename van poliklinische endoscopische verrichtingen onder l okale anesthesie binnen de laryngologie en hoofd-hals oncologie bieden nog geen duidelijkheid over de lokale anesthesie technieken, die essentieel zijn voor het succesvol kunnen uitvoeren van de verrichting. Daarom hebben wij in Hoofdstuk 4 op dezelfde systematische wijze als de eerdere twee studies, een derde literatuurstudie uitgevoerd naar de beschikbare lokale anesthetica, de methodes van toediening, de lokale secundaire effecten, alsmede de effectiviteit en eventuele complicaties. Lidocaine is het meest gebruikte lokaal anestheticum. Lokale anesthesie resulteert in verminderde sensorische functie (verdoofd gevoel) zonder de motorische functie (spreken en ademen) aan te tasten. Voor de neusholte worden watten met lokale anesthesie en een ontzwellend middel (bijvoorbeeld xylometazoline) of een lokaal verdovende gel toegepast, en beide blijken effectief. Voor de pharynx is spray het meest gebruikte middel. Voor de larynx kan lokale anesthetica door het werkkanaal van de flexibele endoscoop worden gedruppeld, of kan een injectie worden gegeven door het membrana cricothyroidea. Het ontbreekt aan studies die de verschillende lokale anesthesie technieken met elkaar vergelijken op effectiviteit. Systemische complicaties door het aanbrengen van oppervlakkige anesthesie met lidocaine zijn zeldzaam. Door het adequaat toedienen van lokale anesthesie in de bovenste luchtweg
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 179PDF page: 179PDF page: 179PDF page: 179
Summary in Dutch
179
11
is het mogelijk om verschillende diagnostische en therapeutische verrichtingen uit te voeren in de polikliniek in plaats van in de operatiekamer onder algehele narcose bij patiënten met afwijkingen in de pharynx en larynx.
Door het uitvoeren van bovenstaande drie literatuurstudies is alle huidige kennis over poliklinische endoscopische verrichtingen binnen de laryngologie en hoofd-hals oncologie zo volledig mogelijk beschreven. Hierop volgend hebben wij een retrospectieve studie verricht naar de complicaties die kunnen ontstaan na het verrichten van FEB, die is weergegeven in Hoofdstuk 5. Patiënten die tussen 2012 en 2016 deze verrichting hebben ondergaan, zijn retrospectief geanalyseerd. Complicaties zijn geclassificeerd volgens de Clavien-Dindo classificatie voor chirurgische complicaties. In totaal zijn er 201 verrichtingen uitgevoerd bij 187 patiënten. Twee Clavien-Dindo graad I (laryngospasme en anterieure epistaxis), één graad II (laryngeale bloeding na lokale anesthesie) en één graad IIIb (laryngeaal oedeem) complicaties werden gevonden. De eerste complicatie was “self-limiting” en voor de andere drie complicaties was een interventie noodzakelijk. Alle patiënten genazen zonder nevenschade. Hieruit kunnen we concluderen dat FEB een veilige poliklinische endoscopische ingreep is voor de diagnose van benigne en maligne afwijkingen in de pharynx en larynx.
In Hoofdstuk 6 is een volgende endoscopische behandeling klinisch onderzocht. Hoewel poliklinische endoscopische laserchirurgie voor verschillende andere soorten lasers al uitgebreid is onderzocht, is dit voor de CO2 laser maar beperkt gerapporteerd. Aangezien de CO2 laser de meest gebruikte laser is in de operatiekamer voor de behandeling van laryngeale afwijkingen, is ons doel om prospectief te onderzoeken of het haalbaar is om in de polikliniek de CO2 laser te gebruiken voor de behandeling van benigne en premaligne afwijkingen van de stemband. We hebben onderzocht hoeveel verrichtingen volledig konden worden uitgevoerd. Daarnaast is gekeken naar het aantal opgetreden complicaties, het effect op de subjectieve stemkwaliteit en het succes van de behandelingen (dat wil zeggen geen residu of recidief van de aandoening). In een prospectieve studie zijn 30 opeenvolgende verrichtingen uitgevoerd en geanalyseerd bij volwassen patiënten met klinisch benigne of premaligne afwijkingen op de stembanden. Deze patiënten konden een transorale chirurgische behandeling in de operatiekamer onder algehele narcose niet ondergaan. Inclusiecriteria waren contra-indicatie voor algehele narcose, een eerder gefaalde behandeling op de operatiekamer, of een sterke voorkeur voor een verrichting onder lokale anesthesie. Negenentwintig (97%) verrichtingen konden volledig worden afgerond zonder complicaties. De gemiddelde preoperatieve Voice Handicap Index (VHI)
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 180PDF page: 180PDF page: 180PDF page: 180
Chapter 11
180
score (VHI 44) verbeterde significant 2 maanden (VHI 28, p = 0.032) en 6 maanden (VHI 14, p < 0.001) na de behandeling. Bijna twee derde (66%) van de patiënten had geen residu of recidief afwijking op de stembanden tijdens de follow-up controles, wat vervolgbehandeling overbodig maakte. Hieruit kunnen we concluderen dat poliklinische endoscopische CO2 laser chirurgie een haalbare en veilige behandelmethode is, waarbij ook de subjectieve stemkwaliteit significant is verbeterd na de verrichting.
Tenslotte hebben we een prospectieve haalbaarheidsstudie verricht naar TNE, gecombineerd met een kostenanalyse. In Hoofdstuk 7 is de weergave van het onderzoek naar twee patiëntencategorieën, te weten patiënten met globus pharyngeus met/zonder dysfagie en patiënten met de verdenking op een hypopharynxcarcinoom. Tweeënveertig opeenvolgende TNE verrichtingen zijn uitgevoerd, waarvan er 35 (85%) volledig konden worden afgerond. De verrichting werd over het algemeen goed verdragen met slechts milde klachten van nasale of pharyngeale pijn, en boeren. Er was sprake van vier complicaties: twee milde anterieure epistaxis en twee vasovagale reacties. In de groep van patiënten met globus pharyngeus met/zonder dysfagie resulteerde TNE in een kostenbesparing van gemiddeld €94.43 (p 0.026) per verrichting, vergeleken met de regulier geleverde zorg. In de groep van patiënten met de verdenking op een hypopharynxcarcinoom, was de gemiddelde kostenbesparing €831.41 (p 0.000) per verrichting. Concluderend laat deze studie zien dat poliklinische TNE een haalbare en veilige diagnostische verrichting is, die goed wordt verdragen door patiënten. Daarnaast laat deze studie zien dat de verrichting een significante kostenbesparing oplevert in vergelijking met de huidige geleverde zorg in de boven beschreven patiëntencategorieën.
Dit proefschrift stelt, dat met de ontwikkeling van digitale flexibele endoscopen met of zonder werkkanaal, er in toenemende mate en met succes poliklinische endoscopische chirurgie wordt uitgevoerd bij patiënten met laryngologische en hoofd-hals oncologische afwijkingen. Verschillende poliklinische endoscopische verrichtingen zijn uitgebreid onderzocht en laten zien dat ze haalbaar en veilig zijn, en goed worden verdragen door patiënten. Daarnaast zijn er overigens ook verrichtingen die minder goed zijn onderzocht, en die vervolgonderzoek behoeven. In het algemeen zijn poliklinische endoscopische verrichtingen in lijn met de huidige ontwikkelingen in de zorg, waarbij er meer nadruk ligt op gepersonaliseerde gezondheidszorg, minimaal invasieve chirurgie, innovatie en kostenbesparing.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 181PDF page: 181PDF page: 181PDF page: 181
Summary in Dutch
181
11

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 182PDF page: 182PDF page: 182PDF page: 182
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 183PDF page: 183PDF page: 183PDF page: 183
Chapter 12Acknowledgements

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 184PDF page: 184PDF page: 184PDF page: 184
Chapter 12
184
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 185PDF page: 185PDF page: 185PDF page: 185
Acknowledgements
185
12
Het is niet mogelijk mijn dankbaarheid volledig op papier te zetten, maar hieronder volgt een deel ervan. Dit proefschrift was nooit gelukt zonder de (in)directe hulp van iedereen in mijn omgeving.
Prof. dr. Marres, beste Henri, dank voor je heldere overziende blik. Vooral in de eindfase van dit proefschrift kwam jouw onuitputtelijke brede kennis naar voren en heb je ervoor gezorgd dat dit proefschrift een passend begin en einde heeft gekregen.
Prof. dr. Takes, beste Robert, dank voor je eindeloze geduld en kennis. Vanaf het begin tot het eind wist jij met jouw snelle reacties en scherpe analyses ervoor te zorgen dat er vaart bleef in de voortgang van mijn proefschrift. Jouw wetenschappelijke en grammaticale kennis is van een ander niveau, waarbij je in elke fase scherp had waar we stonden en hoe we verder moesten. Daarnaast kan je moeilijke discussies altijd verlichten met één van je legendarische uitspraken of anekdotes.
Dr. van den Broek, beste Guido, dank voor je visie, gedrevenheid, collegialiteit en inmiddels vriendschap. Jij bent de bedenker van dit project. Je hebt een bewonderingswaardige gedrevenheid naar het verbeteren van de zorg en bent een pionier op dit gebied. Doordat jij buiten de vertrouwde kaders durft te treden, zorg je daadwerkelijk voor verandering. Daarnaast stimuleer je mij om een betere KNO-arts te worden. Onze eindeloze gesprekken over nieuwe ideeën, toekomstige projecten en het leven eromheen gaan nooit vervelen.
Beste leden van de manuscriptcommissie, dank voor de tijd en moeite die jullie hebben gestoken in het lezen en beoordelen van mijn proefschrift.
Collega’s van de KNO, wat een geweldige omgeving om in te werken. Stafleden, jullie zorgen voor een inspirerend opleidingsklimaat, waarbij hard werken in een veilige omgeving wordt afgewisseld met jullie waardevolle aanwezigheid bij de wekelijkse sociale activiteiten. Henri en Frank, bedankt voor de kans die jullie me hebben geboden. Verpleegkundigen, polikliniek assistenten, secretaresses en alle andere medewerkers, zonder jullie is het niet mogelijk om in zo’n omgeving te werken. Marlou, bedankt voor je tomeloze inzet en hulp bij alles wat we rondom dit project samen hebben gedaan. Collega AIOS, PA en onderzoekers, het is een feest om met jullie samen te werken. Ondanks de hoge werkdruk blijven we in staat om met én voor elkaar te werken. De ontelbare en legendarische vrijdagmiddag borrels, (sport)activiteiten en weekenden zijn en blijven hier een belangrijke factor in. Stafleden van mijn twee perifere ziekenhuizen, het Jeroen Bosch Ziekenhuis

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 186PDF page: 186PDF page: 186PDF page: 186
Chapter 12
186
en het Canisius Wilhelmina Ziekenhuis, bedankt voor jullie belangrijke bijdrage aan mijn ontwikkeling. Ik heb ongelooflijk veel geleerd en gelachen in de tijd dat ik bij jullie werk(te).
Vrienden uit Voorburg, wat uniek dat wij na 20 jaar nog steeds bij elkaar zijn. Ondanks dat we elkaar minder zien, blijven de avonden en weekenden als vanouds. We hebben weinig nodig om oude tijden te doen herleven. Olivier, ik mis je. Vrienden uit Amsterdam, met jullie heb ik mijn studentenleven vorm gegeven. In een geweldige en belangrijke periode in mijn leven hebben we zoveel meegemaakt waardoor we unieke vriendschappen voor het leven hebben gesloten. Peter, geweldig dat je als jaargenoot en collega mijn paranimf bent. Ondanks dat we elkaar minder vaak zien, hebben we elkaar meegemaakt in de bieb, aan de lamp en nu achter de katheder. Vrienden uit Nijmegen, ik had niet durven hopen dat ik in deze fase van mijn leven nog zoveel nieuwe vrienden zou maken. Wat wij meemaken in de opleiding en daarbuiten zorgt voor een bijzondere band.
Lieve Edmund, Marius en Max. De band die wij als broers hebben is uniek. Ondanks zulke verschillende karakters zijn we de afgelopen tien jaar alleen maar meer naar elkaar toe gegroeid. Ik mis de tijd dat we met z’n vieren in Amsterdam woonde, en wekelijks bij elkaar over de vloer kwamen. In deze roerige tijden is het fijn om jullie te hebben. Lieve Max, al van jongs af aan waren we altijd samen. Ondanks dat we verschillende paden bewandelen, weten we elkaar altijd weer te vinden. Geweldig dat jij mijn paranimf bent. Lieve Sarah, Tessa 1 en 2, Noah, Jake en Ella, jullie zorgen ervoor dat onze familie compleet is.
Liever ouders, jullie onvoorwaardelijke liefde, steun en doorzettingsvermogen om het maximale uit mij te halen heeft z’n vruchten afgeworpen. Jullie zijn mijn voorbeeld wat betreft het creëren van een warm gezin én beide nog het maximale uit een carrière te halen. Jullie onuitputbare energie om in elke levensfase van ons wat bij te dragen is bewonderingswaardig.
Lieve Jobine, mijn liefde. Je bent mijn tegenpool die mij compleet maakt. Jouw wilskracht inspireert me. Je zorgt ervoor dat ik anders tegen zaken aankijk, waardoor ik een completer beeld krijg. Je hebt me ontdooid. En met Maxime en onze zoon op komst, wordt mijn leven nog completer.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 187PDF page: 187PDF page: 187PDF page: 187
Acknowledgements
187
12

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 188PDF page: 188PDF page: 188PDF page: 188
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 189PDF page: 189PDF page: 189PDF page: 189
Chapter 13Curriculum Vitae

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 190PDF page: 190PDF page: 190PDF page: 190
Chapter 13
190
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 191PDF page: 191PDF page: 191PDF page: 191
Curriculum Vitae
191
13
David Wellenstein was born on the 26th of June 1988 in Leidschendam, The Netherlands. He finished his high school (VWO, Scholengemeenschap Dalton, Voorburg) in 2006, and afterward travelled through Australia and started a college education in physiotherapy. In 2008, he started medical school at the Free University (VU) in Amsterdam, which he finished in 2015. After graduating medical school, he started as a house officer at the Department of Otorhinolaryngology and Head and Neck Surgery of the Radboud university medical center (Radboudumc). In Augustus 2015 he started with his PhD on office-based procedures in laryngology and head and neck oncology. In December 2016 he started his residency at the Department of Otorhinolaryngology and Head and Neck Surgery of the Radboudumc, with two internships at the Department of Otorhinolaryngology of the Jeroen Bosch Hospital in Den Bosch and the Canisius Wilhelmina Hospital in Nijmegen.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 192PDF page: 192PDF page: 192PDF page: 192
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 193PDF page: 193PDF page: 193PDF page: 193
Chapter 14List of publications

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 194PDF page: 194PDF page: 194PDF page: 194
Chapter 14
194
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 195PDF page: 195PDF page: 195PDF page: 195
List of publications
195
14
Kappert KDR, van Dijk S, Wellenstein D, van Alphen MJA, van Son RJJH, Smeele LE, Balm AJM. Five Specific Tongue Movements in a Healthy Population. Dysphagia. 2020 Oct 11. doi: 10.1007/s00455-020-10195-y. Online ahead of print.
Schimberg AS, Wellenstein DJ, Schutte HW, Honings J, van den Hoogen FJA, Marres HAM, Takes RP, van den Broek GB. Flexible Endoscopic Biopsy: Identifying Factors to Increase Accuracy in Diagnosing Benign and Malignant Laryngopharyngeal Pathology. J Voice. 2020 May 17:S0892-1997(20)30130-2. doi: 10.1016/j.jvoice.2020.04.015.
Schutte HW, Heutink F, Wellenstein DJ, van den Broek GB, van den Hoogen FJA, Marres HAM, van Herpen CML, Kaanders JHAM, Merkx TMAW, Takes RP. Impact of Time to Diagnosis and Treatment in Head and Neck Cancer: A Systematic Review. Otolaryngol Head Neck Surg. 2020 Feb 25:194599820906387.
Schimberg AS, Klabbers TM, Wellenstein DJ, Heutink F, Honings J, van Engen-Van Grunsven I, Verdaasdonk RM, Takes RP, van den Broek GB. Optimizing Settings for Office-Based Endoscopic CO2 Laser Surgery Using an Experimental Vocal Cord Model. Laryngoscope. 2020 Feb 5. doi: 10.1002/lary.28518.
Wellenstein DJ, Honings J, Schimberg AS, Schutte HW, Herruer JM, van den Hoogen FJA, Takes RP, van den Broek GB. Office-based CO2 laser surgery for benign and premalignant laryngeal lesions. Laryngoscope. 2019 Sep 9. doi: 10.1002/lary.28278.
Schimberg AS, Wellenstein DJ, van den Broek EM, Honings J, van den Hoogen FJA, Marres HAM, Takes RP, van den Broek GB. Office-based vs. operating room-performed laryngopharyngeal surgery: a review of cost differences. Eur Arch Otorhinolaryngol. 2019 Nov;276(11):2963-2973.
Wellenstein DJ, Honings J, Schutte HW, Herruer JM, van den Hoogen FJA, Marres HAM, Takes RP, van den Broek GB. Cost analysis of office-based transnasal esophagoscopy. Eur Arch Otorhinolaryngol. 2019 May;276(5):1457-1463.
Wellenstein DJ, van der Wal RAB, Schutte HW, Honings J, van den Hoogen FJA, Marres HAM, Takes RP, van den Broek GB. Topical Anesthesia for Endoscopic Office-based Procedures of the Upper Aerodigestive Tract. J Voice. 2019 Sep;33(5):732-746.
549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 196PDF page: 196PDF page: 196PDF page: 196
Chapter 14
196
Van den Broek GB, Wellenstein DJ. Ontwikkelingen in de flexibele bovensteluchtweg endoscopie. Nederlands Tijdschrift voor Keel-Neus-Oorheelkunde. Issue: November 2018, Volume: 24, Number: 4
Wellenstein DJ, Schutte HW, Takes RP, Honings J, Marres HAM, Burns JA, van den Broek GB. Office-Based Procedures for the Diagnosis and Treatment of Laryngeal Pathology. J Voice. 2018 Jul;32(4):502-513.
Wellenstein DJ, de Witt JK, Schutte HW, Honings J, van den Hoogen FJA, Marres HAM, Takes RP, van den Broek GB. Safety of flexible endoscopic biopsy of the pharynx and larynx under topical anesthesia. Eur Arch Otorhinolaryngol. 2017 Sep;274(9):3471-3476.
Wellenstein DJ, Schutte HW, Marres HAM, Honings J, Belafsky PC, Postma GN, Takes RP, van den Broek GB. Office-based procedures for diagnosis and treatment of esophageal pathology. Head Neck. 2017 Sep;39(9):1910-1919.

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 197PDF page: 197PDF page: 197PDF page: 197
List of publications
197
14

549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-Wellenstein549724-L-sub01-bw-WellensteinProcessed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020Processed on: 21-10-2020 PDF page: 198PDF page: 198PDF page: 198PDF page: 198






















