association between upper limb global strength and - Redalyc
Upload
mumbaiunivercityCategory
view
2download
0
SIR Reporting Standards for the Treatment ofAcute Limb Ischemia with Use of TransluminalRemoval of Arterial ThrombusNilesh Patel, MD, Subcommittee Chair, David Sacks, MD, Committee Chair, Rajesh I. Patel, MD,
Kenneth P. Moresco, MD, Kenneth Ouriel, MD, Richard Gray, MD, Walter T. Ambrosius, PhD,Curtis A. Lewis, MD, MBA, and the members of the Society of Interventional Radiology TechnologyAssessment Committee
J Vasc Interv Radiol 2003; 14:S453–S465
Abbreviations: PAD � peripheral arterial disease, PAT � percutaneous aspiration thrombectomy, PMT � percutaneous mechanical thrombectomy, SVS/ISCVS � Society of Vascular Surgery/International Society of Cardiovascular Surgery, TRT � transluminal removal of thrombus
ACUTE limb ischemia is any suddendecrease or worsening in limb perfu-sion that causes a potential threat tolimb viability (1). Acute peripheral ar-terial occlusion may be caused by insitu thrombosis or embolus. In this ar-ticle, the term “thrombus” will be usedto describe arterial occlusion causedby in situ thrombosis or embolus. Per-cutaneous or “open” surgical tech-niques can be used to remove thethrombus. Current percutaneousmethods for transluminal removal ofthrombus (TRT) include thrombolytictherapy (ie, catheter-directed, pharma-comechanic), percutaneous aspirationthrombectomy (PAT), and percutane-ous mechanical thrombectomy (PMT).These methods may be used in combi-nation. Surgical techniques entail an
“open” procedure that necessitates anarteriotomy for the removal of throm-bus.
Of the various TRT methods usedto treat acute limb ischemia, catheter-directed thrombolytic therapy withurokinase has been the most widelystudied. Catheter-directed thrombo-lytic therapy has at least three theoret-ical and practical advantages over sur-gical thromboembolectomy: lessendothelial trauma, angiographic vi-sualization of the underlying lesion(s)and runoff vessels, and, in many cases,ready access for definitive translumi-nal therapies that address the under-lying lesion (1,2). In addition, it hasbeen suggested that gradual, low-pressure reperfusion may offer certainadvantages over sudden, high-pres-sure reperfusion associated withsurgical revascularization (1,3,4). Re-cently, the Food and Drug Adminis-tration recalled urokinase (Abboki-nase; Abbott Laboratories, AbbottPark, IL). As a result, a critical evalu-ation of alternate methods to treatacute limb ischemia with use of otherthrombolytic drug strategies, PATand/or PMT, will be needed.
Reporting standards for the treat-ment of peripheral arterial disease(PAD) and practice guidelines forthrombolytic therapy for acute limbischemia have been published (1,2,5–7). However, there is insufficient evi-dence in the literature to determine the
best therapy in a given case of acutelimb ischemia. This is because the lit-erature is replete with individual orinstitutional reports of surgical andthrombolytic therapy that are eitherbiased or lack concurrent controls andstandardized reporting practices (1).The purpose of this document is toestablish reporting standards for sub-sequent studies pertaining to TRT inthe treatment of acute limb ischemia.Consistent data reporting is needed tohelp precisely define the safety, effi-cacy, and long-term outcome of TRTprocedures (1,8,9). Only then can theappropriate treatment be determinedfor patients presenting with acute limbischemia.
PATIENT SELECTION
Demographic data are important toassess any differences between studygroups, and they also allow a clinicianto determine whether the study is rel-evant to his or her patient population.Useful demographic data includesage, sex, and race.
Thrombus can cause occlusion ofnative arterial segment(s) or surgicalbypass graft(s). For a given occlusion,a clear determination of embolic ver-sus in situ thrombotic etiology maynot be possible. Nevertheless, an at-tempt should be made to distinguishbetween these two etiologies with useof the criteria in the Pretreatment Eval-
This article first appeared in J Vasc Interv Radiol2001; 12:559–570.
Members of the Technology Assessment Committeeare: Curtis W. Bakal, MD, MPH; Gary J. Becker, MD;Dana R. Burke, MD; Patricia E. Cole, PhD, MD;William B. Crenshaw, MD; Michael D. Dake, MD;Alain Drooz, MD; Scott C. Goodwin, MD; MargaretE. Hansen, MD; Ziv Haskal, MD; Thomas B. Kinney,MD; Lindsay Machan, MD; David L. Marinelli, MD;Louis G. Martin, MD; Reed Ali Omary, MD; DouglasC.B. Redd, MD; John H. Rundback, MD; RichardShlansky-Goldberg, MD; James E. Silberzweig, MD;Kenneth S. Rholl, MD; and Robert L. Vogelzang,MD. Address correspondence to SIR, 10201 LeeHighway, Suite 500, Fairfax, VA 22030.
© SIR, 2003
DOI: 10.1097/01.RVI.0000094619.61428.11
S453

uation section. The atheromatous nar-rowing of PAD or the neointimal pro-liferation seen within surgical bypassgrafts may lead to in situ thrombosis.An embolus characteristically lodgesin a vascular bed where there has beenno previous stimulus for collateral de-velopment (1).
Although multiple case series in-clude data on the efficacy and safety ofthrombolytic therapy, most series aresmall and cannot offer definitive con-clusions (3,10–20). Several prospectiverandomized trials have been valuablein determining the patient populationmost likely to benefit from thrombo-lytic therapy (21–27). These studiesalso suggest that a management strat-egy must incorporate definitive cor-rection of any underlying lesion dis-closed after thrombolytic therapy.Patient selection has benefited from animproved understanding of the factorsinfluencing the technical and clinicalsuccess of thrombolytic therapy (28–31).
Recently, in an attempt to expediterestoration of blood flow to an acutelyischemic limb and to reduce the risk ofbleeding complications associatedwith thrombolytic therapy, multiplemechanical devices have been em-ployed (32–38). These devices work byseveral different methods, includingaspiration, pulverization, destruction,and recirculation of the thrombus. Me-chanical devices may allow percutane-ous treatment of more profound isch-emia than is currently possible withthrombolytic therapy alone.
Patients presenting with “blue toesyndrome” (atherothrombotic micro-embolization) usually have transientfixed ischemia, occasionally with mi-nor tissue loss, but without diffuseforefoot ischemia. These patientsshould not be included in reportingexperiences of acute limb ischemiaand are better reported separately.
Recommendations for ReportingStandards
Demographic data, which includesage, sex, and race, must be reported.For categorical variables (ie, sex, race),the proportions of the subjects in eachof the categories must be reported. Forcontinuous variables (ie, age), themean or median (for nonparametricvariables), SD or SEM, and range mustbe reported. The target population of
the study must be relevant to the hy-potheses being tested. The target pop-ulation must be defined and themethod of assigning treatments tosubjects must be described. The num-ber and description of patients consid-ered for but not treated by TRT shouldbe tabulated as a screening log. Thisscreening log should include the rea-son for exclusion in each case. It isimportant to explicitly state the selec-tion (inclusion) criteria for choosingthe study patients and control subjectsfrom the patient population. In addi-tion, the exclusion criteria must be re-ported. Possible exclusions includecontraindications to thrombolytictherapy or profound, progressiveacute limb ischemia that cannot affordthe time needed to undergo thrombo-lytic therapy.
Treatment of acute limb ischemiacaused by in situ thrombus versus em-bolus must be studied and reportedseparately (39). When possible, selec-tion should be stratified according tonative arterial versus graft occlusion,duration of symptoms, and disease se-verity. These are detailed in the Pre-treatment Evaluation section of this ar-ticle.
PRETREATMENTEVALUATION
Clinical Evaluation
Clinical evaluation of revascular-ization procedures, particularly thosethat compare different treatmentmethods, may be difficult to interpretunless differences in factors that canaffect outcome are identified and char-acterized. The history and physical ex-amination will help define risk factors,comorbidities, previous interventionsand operations, and the severity andduration of ischemia. Tobacco use, hy-pertension, diabetes, hyperlipidemia,and hypercoagulable states (protein C,protein S, and antithrombin III defi-ciency, anticardiolipin syndrome, etc.)may affect patency (1,7). Cardiac, pul-monary, renal, and carotid artery dis-ease and malignancy may influencemorbidity and mortality (1,7). To ourknowledge, there are no publishedstudies evaluating the influence of ahistory of PAD or earlier revascular-ization (surgical graft composition,age, and earlier graft interventions) onclinical success and outcome of TRT
and it would therefore be helpful tocollect data on these factors.
A history of claudication, recent di-agnostic catheterization, or lower ex-tremity intervention (ie, percutaneoustransluminal angioplasty [PTA], stentplacement, bypass graft, endarterec-tomy) suggests in situ thrombosis. Thefollowing features may suggest theclinical diagnosis of arterial embolismto the limb: (a) sudden onset of symp-toms, (b) known embolic source, (c) noantecedent claudication, (d) normalpulse and Doppler systolic blood pres-sures in the unaffected extremity (1).
Preintervention anticoagulationwith therapeutic levels of heparin hasbeen shown to reduce morbidity andmortality and is part of the overalltreatment strategy for patients withacute limb ischemia (40,41). Therefore,preprocedural medications affectingthe coagulation pathway or plateletactivity may affect the outcome of in-terventional procedures for thrombusremoval. To our knowledge, there areno published studies evaluating therole of vasoactive drugs in acute limbischemia (1).
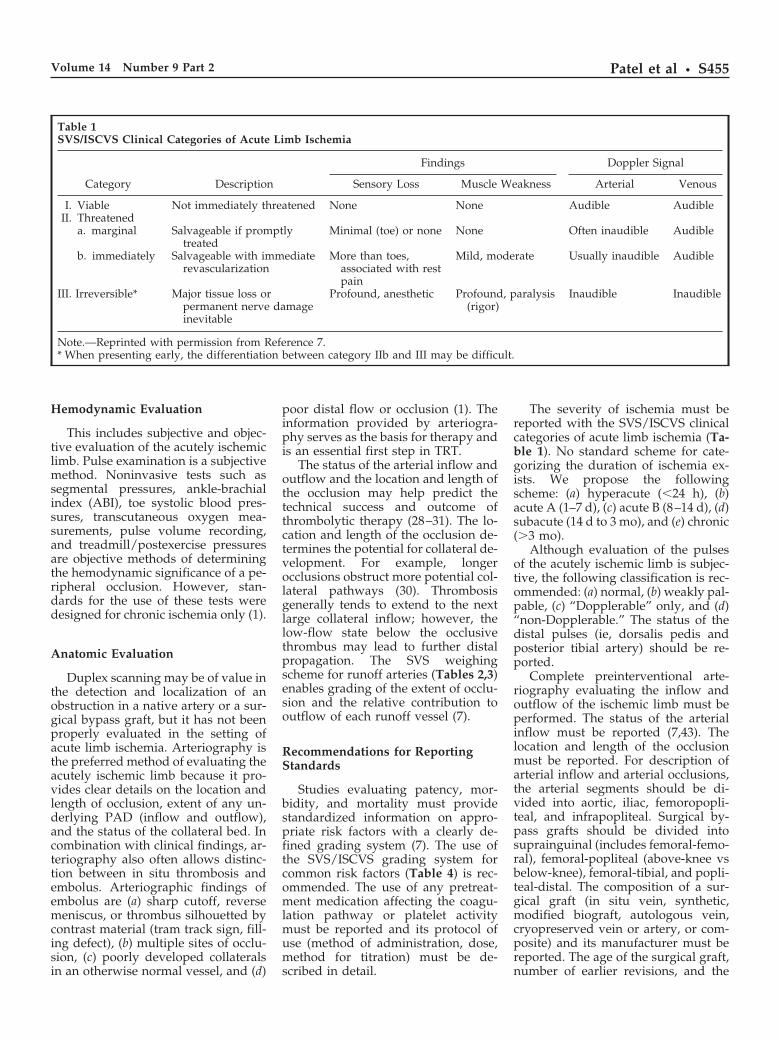
There is a need for objective mea-sures of the severity of acute limb isch-emia to predict outcome more accu-rately. Classification systems for theseverity of acute limb ischemia must(a) be clinically relevant to the diagno-sis and treatment and (b) meaningfullystratify patients for outcome assess-ment (1). The Society of Vascular Sur-gery/International Society of Cardio-vascular Surgery (SVS/ISCVS) clinicalcategory of acute limb ischemia is auseful classification scheme (Table 1).Immediate revascularization is indi-cated in the profoundly ischemic limb(7). The sudden onset of hypoperfu-sion of the lower extremity leadsrapidly to systemic acid-base and elec-trolyte disorders that impair cardio-pulmonary function. Elevated myoglo-bin level is associated with irreversiblerenal failure. Successful revasculariza-tion may induce a severe reperfusioninjury, causing further neuromusculardamage to the extremity (1).
The duration of ischemia may affectthe duration of infusion and overalldose of thrombolytic drug needed(1,42). Also, clinical and temporal cri-teria may help define the role of me-chanical thrombectomy devices in thetreatment of profound limb ischemia.
S454 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR
Hemodynamic Evaluation
This includes subjective and objec-tive evaluation of the acutely ischemiclimb. Pulse examination is a subjectivemethod. Noninvasive tests such assegmental pressures, ankle-brachialindex (ABI), toe systolic blood pres-sures, transcutaneous oxygen mea-surements, pulse volume recording,and treadmill/postexercise pressuresare objective methods of determiningthe hemodynamic significance of a pe-ripheral occlusion. However, stan-dards for the use of these tests weredesigned for chronic ischemia only (1).
Anatomic Evaluation
Duplex scanning may be of value inthe detection and localization of anobstruction in a native artery or a sur-gical bypass graft, but it has not beenproperly evaluated in the setting ofacute limb ischemia. Arteriography isthe preferred method of evaluating theacutely ischemic limb because it pro-vides clear details on the location andlength of occlusion, extent of any un-derlying PAD (inflow and outflow),and the status of the collateral bed. Incombination with clinical findings, ar-teriography also often allows distinc-tion between in situ thrombosis andembolus. Arteriographic findings ofembolus are (a) sharp cutoff, reversemeniscus, or thrombus silhouetted bycontrast material (tram track sign, fill-ing defect), (b) multiple sites of occlu-sion, (c) poorly developed collateralsin an otherwise normal vessel, and (d)
poor distal flow or occlusion (1). Theinformation provided by arteriogra-phy serves as the basis for therapy andis an essential first step in TRT.
The status of the arterial inflow andoutflow and the location and length ofthe occlusion may help predict thetechnical success and outcome ofthrombolytic therapy (28–31). The lo-cation and length of the occlusion de-termines the potential for collateral de-velopment. For example, longerocclusions obstruct more potential col-lateral pathways (30). Thrombosisgenerally tends to extend to the nextlarge collateral inflow; however, thelow-flow state below the occlusivethrombus may lead to further distalpropagation. The SVS weighingscheme for runoff arteries (Tables 2,3)enables grading of the extent of occlu-sion and the relative contribution tooutflow of each runoff vessel (7).
Recommendations for ReportingStandards
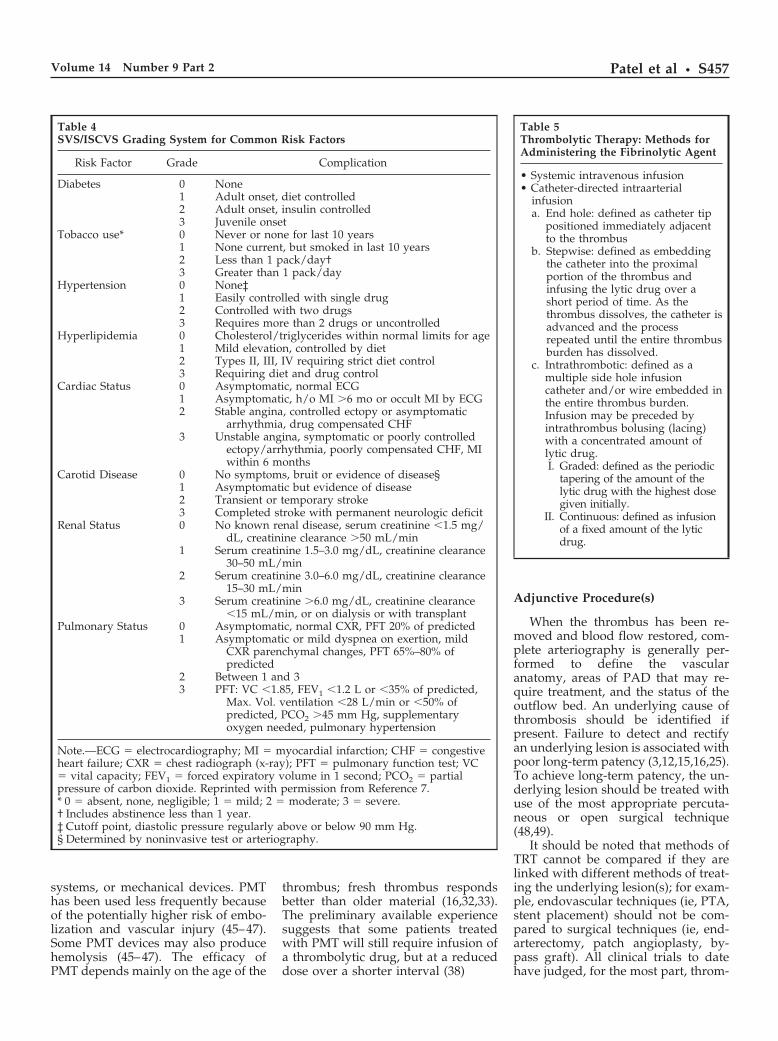
Studies evaluating patency, mor-bidity, and mortality must providestandardized information on appro-priate risk factors with a clearly de-fined grading system (7). The use ofthe SVS/ISCVS grading system forcommon risk factors (Table 4) is rec-ommended. The use of any pretreat-ment medication affecting the coagu-lation pathway or platelet activitymust be reported and its protocol ofuse (method of administration, dose,method for titration) must be de-scribed in detail.
The severity of ischemia must bereported with the SVS/ISCVS clinicalcategories of acute limb ischemia (Ta-ble 1). No standard scheme for cate-gorizing the duration of ischemia ex-ists. We propose the followingscheme: (a) hyperacute (�24 h), (b)acute A (1–7 d), (c) acute B (8–14 d), (d)subacute (14 d to 3 mo), and (e) chronic(�3 mo).
Although evaluation of the pulsesof the acutely ischemic limb is subjec-tive, the following classification is rec-ommended: (a) normal, (b) weakly pal-pable, (c) “Dopplerable” only, and (d)“non-Dopplerable.” The status of thedistal pulses (ie, dorsalis pedis andposterior tibial artery) should be re-ported.
Complete preinterventional arte-riography evaluating the inflow andoutflow of the ischemic limb must beperformed. The status of the arterialinflow must be reported (7,43). Thelocation and length of the occlusionmust be reported. For description ofarterial inflow and arterial occlusions,the arterial segments should be di-vided into aortic, iliac, femoropopli-teal, and infrapopliteal. Surgical by-pass grafts should be divided intosuprainguinal (includes femoral-femo-ral), femoral-popliteal (above-knee vsbelow-knee), femoral-tibial, and popli-teal-distal. The composition of a sur-gical graft (in situ vein, synthetic,modified biograft, autologous vein,cryopreserved vein or artery, or com-posite) and its manufacturer must bereported. The age of the surgical graft,number of earlier revisions, and the
Table 1SVS/ISCVS Clinical Categories of Acute Limb Ischemia
Category Description
Findings Doppler Signal
Sensory Loss Muscle Weakness Arterial Venous
I. Viable Not immediately threatened None None Audible AudibleII. Threatened
a. marginal Salvageable if promptlytreated
Minimal (toe) or none None Often inaudible Audible
b. immediately Salvageable with immediaterevascularization
More than toes,associated with restpain
Mild, moderate Usually inaudible Audible
III. Irreversible* Major tissue loss orpermanent nerve damageinevitable
Profound, anesthetic Profound, paralysis(rigor)
Inaudible Inaudible
Note.—Reprinted with permission from Reference 7.* When presenting early, the differentiation between category IIb and III may be difficult.
Patel et al • S455Volume 14 Number 9 Part 2
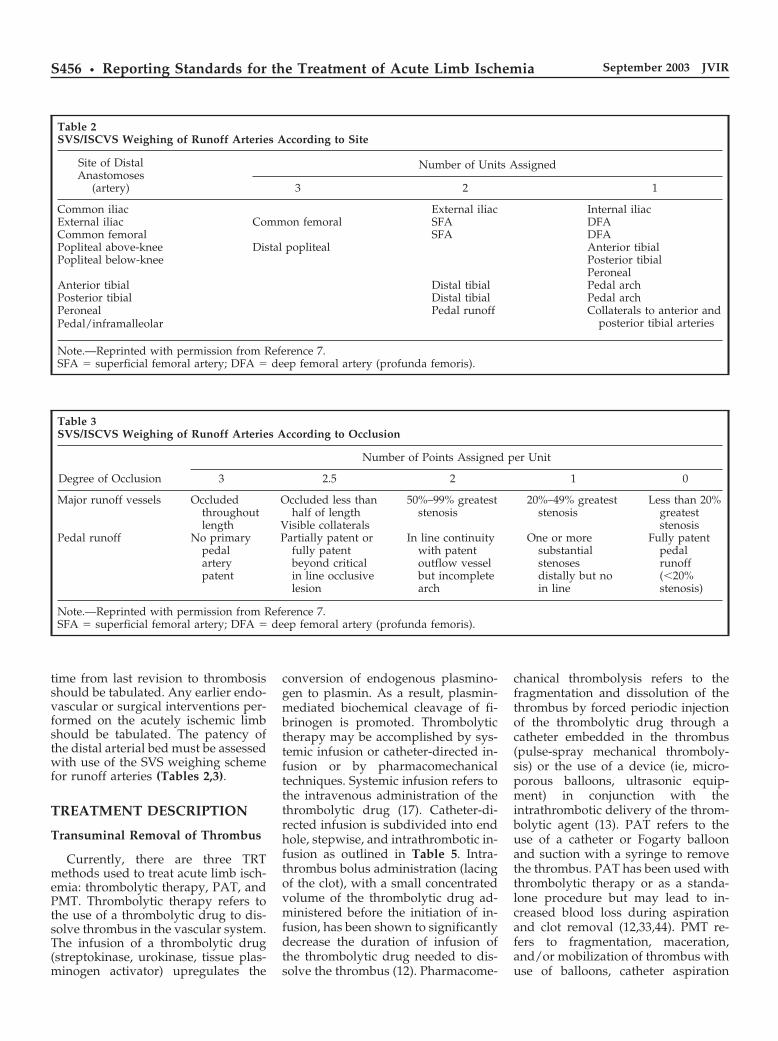
time from last revision to thrombosisshould be tabulated. Any earlier endo-vascular or surgical interventions per-formed on the acutely ischemic limbshould be tabulated. The patency ofthe distal arterial bed must be assessedwith use of the SVS weighing schemefor runoff arteries (Tables 2,3).
TREATMENT DESCRIPTION
Transuminal Removal of Thrombus
Currently, there are three TRTmethods used to treat acute limb isch-emia: thrombolytic therapy, PAT, andPMT. Thrombolytic therapy refers tothe use of a thrombolytic drug to dis-solve thrombus in the vascular system.The infusion of a thrombolytic drug(streptokinase, urokinase, tissue plas-minogen activator) upregulates the
conversion of endogenous plasmino-gen to plasmin. As a result, plasmin-mediated biochemical cleavage of fi-brinogen is promoted. Thrombolytictherapy may be accomplished by sys-temic infusion or catheter-directed in-fusion or by pharmacomechanicaltechniques. Systemic infusion refers tothe intravenous administration of thethrombolytic drug (17). Catheter-di-rected infusion is subdivided into endhole, stepwise, and intrathrombotic in-fusion as outlined in Table 5. Intra-thrombus bolus administration (lacingof the clot), with a small concentratedvolume of the thrombolytic drug ad-ministered before the initiation of in-fusion, has been shown to significantlydecrease the duration of infusion ofthe thrombolytic drug needed to dis-solve the thrombus (12). Pharmacome-
chanical thrombolysis refers to thefragmentation and dissolution of thethrombus by forced periodic injectionof the thrombolytic drug through acatheter embedded in the thrombus(pulse-spray mechanical thromboly-sis) or the use of a device (ie, micro-porous balloons, ultrasonic equip-ment) in conjunction with theintrathrombotic delivery of the throm-bolytic agent (13). PAT refers to theuse of a catheter or Fogarty balloonand suction with a syringe to removethe thrombus. PAT has been used withthrombolytic therapy or as a standa-lone procedure but may lead to in-creased blood loss during aspirationand clot removal (12,33,44). PMT re-fers to fragmentation, maceration,and/or mobilization of thrombus withuse of balloons, catheter aspiration
Table 2SVS/ISCVS Weighing of Runoff Arteries According to Site
Site of DistalAnastomoses
(artery)
Number of Units Assigned
3 2 1
Common iliac External iliac Internal iliacExternal iliac Common femoral SFA DFACommon femoral SFA DFAPopliteal above-knee Distal popliteal Anterior tibialPopliteal below-knee Posterior tibial
PeronealAnterior tibial Distal tibial Pedal archPosterior tibial Distal tibial Pedal archPeroneal Pedal runoff Collaterals to anterior and
posterior tibial arteriesPedal/inframalleolar
Note.—Reprinted with permission from Reference 7.SFA � superficial femoral artery; DFA � deep femoral artery (profunda femoris).
Table 3SVS/ISCVS Weighing of Runoff Arteries According to Occlusion
Degree of Occlusion
Number of Points Assigned per Unit
3 2.5 2 1 0
Major runoff vessels Occludedthroughoutlength
Occluded less thanhalf of length
Visible collaterals
50%–99% greateststenosis
20%–49% greateststenosis
Less than 20%greateststenosis
Pedal runoff No primarypedalarterypatent
Partially patent orfully patentbeyond criticalin line occlusivelesion
In line continuitywith patentoutflow vesselbut incompletearch
One or moresubstantialstenosesdistally but noin line
Fully patentpedalrunoff(�20%stenosis)
Note.—Reprinted with permission from Reference 7.SFA � superficial femoral artery; DFA � deep femoral artery (profunda femoris).
S456 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR
systems, or mechanical devices. PMThas been used less frequently becauseof the potentially higher risk of embo-lization and vascular injury (45–47).Some PMT devices may also producehemolysis (45–47). The efficacy ofPMT depends mainly on the age of the
thrombus; fresh thrombus respondsbetter than older material (16,32,33).The preliminary available experiencesuggests that some patients treatedwith PMT will still require infusion ofa thrombolytic drug, but at a reduceddose over a shorter interval (38)
Adjunctive Procedure(s)
When the thrombus has been re-moved and blood flow restored, com-plete arteriography is generally per-formed to define the vascularanatomy, areas of PAD that may re-quire treatment, and the status of theoutflow bed. An underlying cause ofthrombosis should be identified ifpresent. Failure to detect and rectifyan underlying lesion is associated withpoor long-term patency (3,12,15,16,25).To achieve long-term patency, the un-derlying lesion should be treated withuse of the most appropriate percuta-neous or open surgical technique(48,49).
It should be noted that methods ofTRT cannot be compared if they arelinked with different methods of treat-ing the underlying lesion(s); for exam-ple, endovascular techniques (ie, PTA,stent placement) should not be com-pared to surgical techniques (ie, end-arterectomy, patch angioplasty, by-pass graft). All clinical trials to datehave judged, for the most part, throm-
Table 4SVS/ISCVS Grading System for Common Risk Factors
Risk Factor Grade Complication
Diabetes 0 None1 Adult onset, diet controlled2 Adult onset, insulin controlled3 Juvenile onset
Tobacco use* 0 Never or none for last 10 years1 None current, but smoked in last 10 years2 Less than 1 pack/day†3 Greater than 1 pack/day
Hypertension 0 None‡1 Easily controlled with single drug2 Controlled with two drugs3 Requires more than 2 drugs or uncontrolled
Hyperlipidemia 0 Cholesterol/triglycerides within normal limits for age1 Mild elevation, controlled by diet2 Types II, III, IV requiring strict diet control3 Requiring diet and drug control
Cardiac Status 0 Asymptomatic, normal ECG1 Asymptomatic, h/o MI �6 mo or occult MI by ECG2 Stable angina, controlled ectopy or asymptomatic
arrhythmia, drug compensated CHF3 Unstable angina, symptomatic or poorly controlled
ectopy/arrhythmia, poorly compensated CHF, MIwithin 6 months
Carotid Disease 0 No symptoms, bruit or evidence of disease§1 Asymptomatic but evidence of disease2 Transient or temporary stroke3 Completed stroke with permanent neurologic deficit
Renal Status 0 No known renal disease, serum creatinine �1.5 mg/dL, creatinine clearance �50 mL/min
1 Serum creatinine 1.5–3.0 mg/dL, creatinine clearance30–50 mL/min
2 Serum creatinine 3.0–6.0 mg/dL, creatinine clearance15–30 mL/min
3 Serum creatinine �6.0 mg/dL, creatinine clearance�15 mL/min, or on dialysis or with transplant
Pulmonary Status 0 Asymptomatic, normal CXR, PFT 20% of predicted1 Asymptomatic or mild dyspnea on exertion, mild
CXR parenchymal changes, PFT 65%–80% ofpredicted
2 Between 1 and 33 PFT: VC �1.85, FEV1 �1.2 L or �35% of predicted,
Max. Vol. ventilation �28 L/min or �50% ofpredicted, PCO2 �45 mm Hg, supplementaryoxygen needed, pulmonary hypertension
Note.—ECG � electrocardiography; MI � myocardial infarction; CHF � congestiveheart failure; CXR � chest radiograph (x-ray); PFT � pulmonary function test; VC� vital capacity; FEV1 � forced expiratory volume in 1 second; PCO2 � partialpressure of carbon dioxide. Reprinted with permission from Reference 7.* 0 � absent, none, negligible; 1 � mild; 2 � moderate; 3 � severe.† Includes abstinence less than 1 year.‡ Cutoff point, diastolic pressure regularly above or below 90 mm Hg.§ Determined by noninvasive test or arteriography.
Table 5Thrombolytic Therapy: Methods forAdministering the Fibrinolytic Agent
• Systemic intravenous infusion• Catheter-directed intraarterial
infusiona. End hole: defined as catheter tip
positioned immediately adjacentto the thrombus
b. Stepwise: defined as embeddingthe catheter into the proximalportion of the thrombus andinfusing the lytic drug over ashort period of time. As thethrombus dissolves, the catheter isadvanced and the processrepeated until the entire thrombusburden has dissolved.
c. Intrathrombotic: defined as amultiple side hole infusioncatheter and/or wire embedded inthe entire thrombus burden.Infusion may be preceded byintrathrombus bolusing (lacing)with a concentrated amount oflytic drug.I. Graded: defined as the periodic
tapering of the amount of thelytic drug with the highest dosegiven initially.
II. Continuous: defined as infusionof a fixed amount of the lyticdrug.
Patel et al • S457Volume 14 Number 9 Part 2

bolytic therapy linked with PTA, sur-gical thrombectomy, endarterectomy,patch angioplasty, and/or bypass. Theonly way TRT methods can be com-pared is if the treatment of the under-lying lesions is standardized in theprotocol.
Recommendations
The method(s) of TRT must be de-scribed. If a thrombolytic drug is used,then the following must be reported:(a) thrombolytic drug (type, manufac-turer, city, state) and its concentration,(b) method of administration as de-fined in Table 5, (c) the total dose ofdrug used, and (d) the total duration ofthe drug infusion. For pharmacome-chanical thrombolysis, the protocol forthe use of the thrombolytic drug andcatheter or device (type, manufacturer,city, state) must also be described. ForPAT and PMT, the device or cathetersystem (type, manufacturer, city,state) and protocol of its use (ie,thrombus aspiration, maceration, mo-bilization performed in conjunctionwith a mechanical device or cathetersystem, application of an external cuffto prevent distal emboli) must be de-scribed in detail. If adjunctive antico-agulant or antiplatelet medications areused with TRT, their protocol of use(method of administration, dose,method of titration) must be describedin detail. The method of patient mon-itoring, both clinical and laboratory,must be described in detail. For stud-ies of techniques designed to shortenrevascularization time (PAT andPMT), total procedure time and fluo-roscopy time should be reported.Blood loss and amount of hemolysisshould be reported for PAT and PMT.
Adjunctive treatment given to pa-tients should be tabulated. The loca-tion, length, and morphology of anyunderlying lesion(s) should be de-scribed. The selection criteria for treat-ment of any underlying lesion by en-dovascular versus surgical methodsshould be outlined and standardized.The method used (Table 6) to treat theunderlying lesion must be reported.The patency of the distal arterial bed,again according to the SVS scheme forweighing of runoff arteries, must beassessed before and after adjunctivetreatment. After intervention, the pro-tocol for use of any adjunctive medicaltherapy (antiplatelet, anticoagulation,
etc.), short- or long-term, must be de-scribed in detail.
POSTTREATMENTEVALUATION
There are multiple single-center re-ports of the short- and long-term re-sults on the revascularization of theacutely ischemic limb. Unfortunately,these studies are difficult to compareand apply directly to patient manage-ment. This problem is attributable todifferences in study populations, dif-ferences in reporting methods, andlack of relevant outcome data. Theevaluation of therapeutic effectivenessrequires patient outcome measuresrather than hemodynamic measuresalone (1).
Immediate success is determinedby technical success, hemodynamicsuccess, and clinical success. Potentialoutcomes such as a decrease in re-quirement of surgical intervention andreplacement of major surgery by a mi-nor surgery or endovascular interven-tion are also relevant in the assessmentof immediate success. The short- andlong-term outcome measures dependon the hypothesis of the study. Out-come endpoints can be gauged by anumber of parameters such as patency(primary, primary-assisted, second-ary), 1-year major amputation-freesurvival, partial limb salvage, recur-rent ischemia, complications, anddeath, or with use of a composite out-come incorporating some or all ofthese elements (“event-free survival”).Standardized definitions are providedherein.
Technical Success of TRT
Technical success of TRT is definedas restoration of antegrade flow andcomplete or near complete (95% byvolume) removal of the thrombus (50).This definition allows evaluation ofTRT separately from the adjunctiveprocedure(s), if needed. Initial failureof TRT should be analyzed as to find acause of failure: (a) inability to cathe-terize, embed an infusion system, oradvance a mechanical device into thethrombosed segment; (b) treatmentaborted as a result of complications; or(c) treatment performed but not tech-nically successful. If the purpose of thestudy is to evaluate the effectivenessof the use of a thrombolytic drug alonefor TRT, removal of any residualthrombus by other methods is re-garded as a technical failure. Similarly,if the intended TRT method involvesonly the use of a device, removal ofany residual thrombus by other meth-ods is regarded as a technical failure.
Hemodynamic Success
The ideal definition of hemody-namic success is the return of the pa-tient to at least his/her preocclusivebaseline ABI. There are several prob-lems with the use of this definition.Pretreatment ABI is frequently not re-corded in the setting of acute limbischemia because its significance, asnoted earlier, is unclear. The posttreat-ment ABI usually includes the TRTand the adjunctive procedure if thereis an underlying lesion, and the finalABI will be largely determined by theadjunctive procedure and may behigher than baseline level. A morequalitative assessment that may be re-ported is the return of pulses distal tothe treated segment, although this de-pends on the presence and treatmentof the underlying lesions. For thesereasons, reporting of hemodynamicsuccess is of limited value. Nonethe-less, it is important to report the finalABI because it will be used to evaluaterecurrent ischemia during follow-up.
Clinical Success of TRT
Clinical success of TRT is defined asrelief of the acute ischemic symptomsor reduction of the level of the subse-quent surgical intervention or ampu-tation needed (Table 7). To comment
Table 6Types of Adjunctive Procedures
• Percutaneous transluminalangioplasty
• Stent• Atherectomy• Surgical
Thrombectomy/embolectomyEndarterectomy � patch angioplastyInsertion of a new graftInsertion of a jump graftGraft revision
Patch angioplastyExcision of diseased segment and
reanastomosis with or without aninterposition graft
Ligation of arteriovenous fistula
S458 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR

on how TRT changed the surgicaltreatment option, it is necessary torecord which surgical treatmentwould have been performed had TRTnot been attempted.
Overall Clinical Success
Overall clinical success, or clinicalsuccess for the TRT procedure plusadjunctive therapy of underlying le-sions, is defined by relief of the acuteischemic symptoms and return of thepatient to at least his/her preocclusiveclinical baseline level after the TRTand adjunctive procedures.
Patency
Patency applies only to the treatedsegment, refers to continued flowthrough the treated segment, andmust be documented. Duplex Dopplerultrasonography, conventional an-giography, or magnetic resonance an-giography can be used to assess pa-tency. Stenosis developing within thetreated segment without reocclusion isnot considered a loss of patency butwill contribute to recurrent ischemia(6).
Primary patency is defined as thetime from the revascularization proce-dure to either revision or the first oc-currence of thrombosis of the treatedsegment. Any treatment to deal withdisease progression in the adjacent na-
tive vessel is not considered a loss ofprimary patency.
Primary assisted patency is definedas the time from the revascularizationprocedure to thrombosis, irrespectiveof any interval therapy to restore ormaintain flow within the treated seg-ment. Patency may be maintained bypercutaneous or surgical proceduresother than bypass (ie, focal endarter-ectomy, PTA, stent placement, patchangioplasty) performed to treat one ormore stenoses in the treated segment.
Secondary patency is defined as thetime from the procedure to the perma-nent loss of flow in the treated seg-ment, irrespective of any interval ther-apies. Patency may be restored andmaintained by percutaneous (ie,thrombolysis, PTA, stent placement,atherectomy) or surgical (thrombecto-my, endarterectomy, patch angio-plasty) interventions. Secondary pa-tency is lost if the treated segment issurgically bypassed.
One-year Major Amputation-freeSurvival
One-year major amputation-freesurvival means a patient has had noamputation or a minor amputationleaving sufficient functional foot rem-nant to allow walking without a pros-thesis for at least 1 year after treat-ment. Minor amputation allows thepatient to ambulate without the use ofa prosthesis and is represented for the
most part by toe or metatarsal ampu-tations. Syme amputation and mosthigh forefoot amputations (ie,Chopart) are included as major ampu-tations. This definition applies only tothe evaluation of therapeutic outcomeof procedures that are intended toavoid major amputation. In a patientwith established tissue loss, a revascu-larization procedure that allows a mi-nor amputation to heal qualifies as asuccess. An unexpected minor ampu-tation as a result of the TRT method isregarded as a major complication.
Partial Limb Salvage
Applies only to the therapeutic out-come of surgical or endovascular in-tervention(s) that are intended tochange the level of an inevitable majoramputation. For example, a revascu-larization procedure qualifies as a suc-cess if it allows healing of a below-knee amputation when an above-kneeamputation was otherwise predicted.
Recurrent Ischemia
Recurrent ischemia is defined as re-currence of ischemic symptoms or adecrease in ABI of �0.15 from theposttreatment (TRT and adjunctive)baseline level (6). Acute limb ischemiacaused by recurrent embolization maybe experienced by as many as 43% ofpatients in the absence of anticoagula-tion therapy (51). Each episode re-duces the likelihood of complete res-toration of blood flow to the limb.Ischemia from in situ thrombosis alsohas a high incidence of recurrence(52,53). If the underlying lesion dis-closed by thrombolytic therapy is nottreated, the recurrence rate may be ashigh as 53% (1). Recurrent ischemiamay also be a result of loss of primarypatency of the adjunctive procedureused to treat the underlying lesion.
Health-related Quality of Life
Health-related quality of life is usedto identify the general well being of apatient through evaluation of overallfunctional status, perceived health,psychologic well-being, and role func-tion. The use of a validated quality-of-life questionnaire is recommended tomeasure the general health status aftertreatment in patients with acute limbischemia (1). The SF-36 is a standard-
Table 7Recommended Scale for Gauging Changes in Clinical Status in Acute LimbIschemia after Thrombolysis
�1 Ischemia is worse (by at least one major or minor category from SVS/ISCVSClinical Categories of Acute Limb Ischemia)
0 No change (failure)�1 Ischemia improved
a. Revascularization with thrombolytic methods aloneI. amputation necessary but at a lesser level‡
b. Adjunctive surgical revascularization necessary but at a lesser level†I. amputation necessary but at a lesser level‡
c. Adjunctive endovascular revascularization necessary (angioplasty, stent,atherectomy, etc.)I. amputation necessary but at a lesser level‡
Note.—Categories a, b, and c do not imply greater or lesser degrees of success.† Levels of surgical revascularization: 1, Major: insertion of new bypass graft,replacement of an existing bypass graft, or excision or repair of an aneurysm. 2,Moderate: graft revision, patch angioplasty, endarterectomy, or profundaplasty. 3,Minor: thrombectomy/embolectomy or fasciotomy‡ Levels of amputation: 1, above the knee; 2, below the knee; 3, transmetatarsal; and4, toe.
Patel et al • S459Volume 14 Number 9 Part 2

ized and validated method for this as-sessment (1).
Functional Status
For patients with chronic limb isch-emia, the Walking Impairment Ques-tionnaire is useful in evaluating theimpact of mild to moderate limb isch-emia on leg function (1). Currently,there is no method for evaluating pa-tients with acute limb ischemia.
Recommendations
The overall success and clinical out-come of the study group(s) must bereported. The study patients must bestratified into native arteries versusgrafts and vein grafts versus prosthet-ic/composite grafts, and analyses ofthe groups must be performed sepa-rately and together. The success andoutcome data must take into accountdifferences in risk factors betweengroups. Therefore, the patients mustalso be sub-stratified by severity ofacute limb ischemia with use of theSVS/ISCVS clinical categories, dura-tion of ischemia, etiology of occlusion(in situ thrombosis vs embolus), andrisk factors/comorbidities accordingto the outline in the Pretreatment Clin-ical Evaluation section of this article.
As stated previously in other SIRdocuments, follow-up periods are de-fined as immediate (1–30 d after theprocedure), short-term (30 d to 12 moafter the procedure), and long-term(�12 mo after the procedure) (5,6). Im-mediate success must be evaluated byintent to treat and by the intended pri-mary method for thrombus removal(“per-protocol analysis”). The imme-diate technical and clinical successmust be reported. Hemodynamic suc-cess may be reported, depending onstudy design. The incidence andcauses of primary treatment failure(before treatment with another modal-ity) must be described.
The primary endpoints that mustbe reported include patency, 1-yearamputation free survival, partial limbsalvage, and mortality. The secondaryendpoints reported will depend on thepurpose of the study. Previous reportsof thrombolytic therapy trials have in-cluded composite outcomes in theirstatistical analysis (22). We recom-mend that composite outcomes shouldnot be used because specific outcomes
of interest tend to be hidden whengrouped together. The number andnature of procedures to maintain pri-mary assisted or secondary patencymust be reported. The secondary end-points that must be reported includeprimary treatment failure, major mor-bidity, and recurrent ischemia. Thirty-day or even 6-month outcomes may beinsufficient, particularly if one treat-ment has a shorter durability of suc-cess than the other. Follow-up shouldbe at least 6 months for meaningfulcomparisons of therapy (1).
COMPLICATIONS
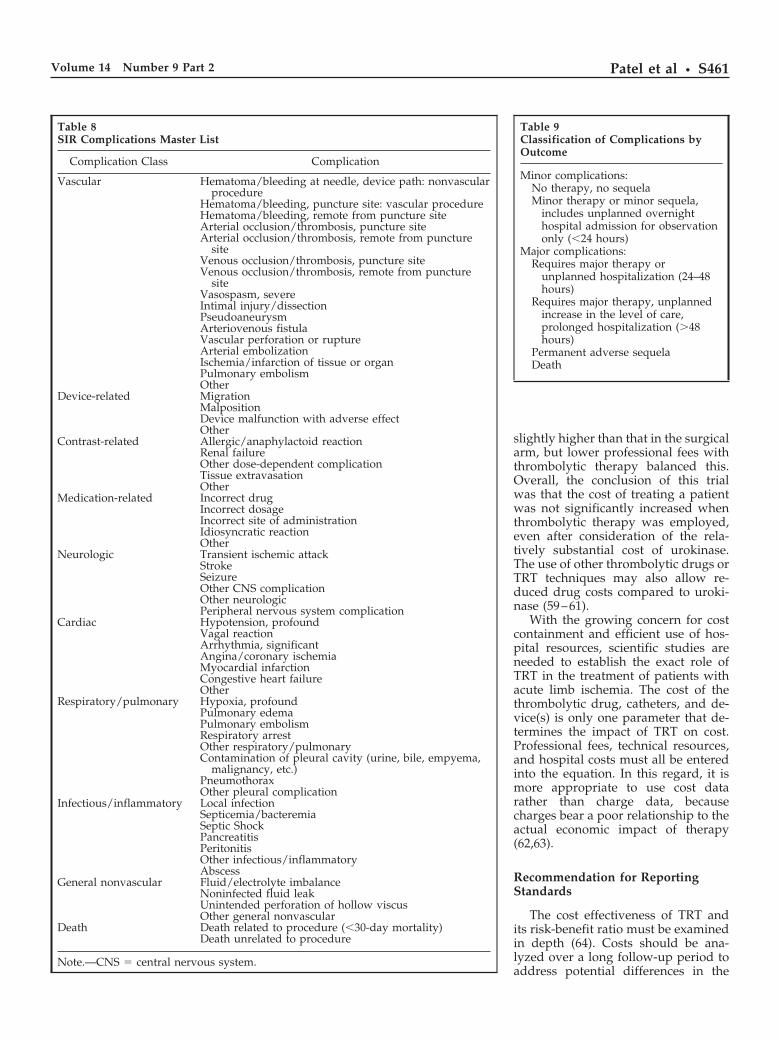
Complications may be hemorrhagicor nonhemorrhagic. The bleeding canbe local or remote and should be di-vided into major and minor. Majorbleeding is defined as an intracranialbleed, bleeding resulting in death, orbleeding requiring transfusion, sur-gery, or cessation of TRT. Minor bleed-ing is defined as less severe bleedingmanaged by local compression, in-creases in vascular sheath size, ordecreases in dose of the lytic, antico-agulant, or antiplatelet drug. Non-bleeding complications include punc-ture-related injury, local arterial injury(perforation, dissection, occlusion),embolization requiring intervention,rethrombosis, pericatheter thrombosisrequiring unexpected additional inter-vention, reperfusion injury, compart-ment syndrome, renal failure, acutemyocardial infarction, etc. The SIRcomplications list is provided in Table8.
Reperfusion injury is one of themost common complications leadingto prolonged morbidity. The suddenreturn of oxygenated blood to theacutely ischemic muscle causes thegeneration and release of oxygen freeradicals and subsequent cellular dam-age. Failure to anticipate or recognizethis complication can lead to the rapiddevelopment of compartment syn-drome and myonecrosis. Treatmentconsists of fasciotomy (1).
An unexpected amputation (ie,caused by distal emboli) or an increasein the level of amputation as a directresult of the revascularization proce-dure is regarded as a major complica-tion. Any adverse effect occurring dur-ing the time period beginning with thediagnostic arteriogram to 24 hours af-ter revascularization is defined as a
procedure-related complication. Otheradverse events that are detected morethan 24 hours after revascularizationmay also be procedure-related (acuterenal failure, delayed embolization, orhematoma from the intervention or ac-cess site, etc.).
Recommendations for ReportingStandards
All complications must be tabu-lated and reported. Also, the compli-cations must be classified by outcomeas major or minor (Table 9), with themost severe complication incurred bythe patient to be reported for use in theclassification (6). Procedure-relatedand overall complication rates must bereported. The 30-day morbidity andmortality rates must be reported. Also,the overall (beyond 30 d) morbidityand mortality rates must be reportedto gauge the long-term effects of thetreatment.
COSTS
Thrombolytic therapy has been crit-icized because of high costs associatedwith the thrombolytic drug. The costof thrombolytic therapy has been eval-uated in only a few studies (54,55).Van Breda et al (56) examined the costof two thrombolytic drugs, urokinaseand streptokinase, in the treatment ofperipheral arterial occlusive disease.Despite the greater cost of urokinase,the total cost of care was greater withstreptokinase because urokinase ther-apy had greater success with fewercomplications. Janosik et al (57) exam-ined the length of hospital stay in pa-tients treated with surgery or throm-bolytic therapy for peripheral arterialocclusive disease. The length of hospi-tal stay was identical between thegroup treated by surgical revascular-ization and the group treated bythrombolytic therapy with streptoki-nase, averaging 21 hospital days.However, thrombolytic therapy withurokinase was associated with a re-duction in hospital stay, which aver-aged 11.5 hospital days. In the Roch-ester trial, costs were calculated forpatients randomized to undergothrombolytic therapy with urokinaseversus those undergoing primary sur-gical intervention (25,58). The cost ofhospitalization (technical component)in the thrombolytic therapy arm was
S460 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR
slightly higher than that in the surgicalarm, but lower professional fees withthrombolytic therapy balanced this.Overall, the conclusion of this trialwas that the cost of treating a patientwas not significantly increased whenthrombolytic therapy was employed,even after consideration of the rela-tively substantial cost of urokinase.The use of other thrombolytic drugs orTRT techniques may also allow re-duced drug costs compared to uroki-nase (59–61).
With the growing concern for costcontainment and efficient use of hos-pital resources, scientific studies areneeded to establish the exact role ofTRT in the treatment of patients withacute limb ischemia. The cost of thethrombolytic drug, catheters, and de-vice(s) is only one parameter that de-termines the impact of TRT on cost.Professional fees, technical resources,and hospital costs must all be enteredinto the equation. In this regard, it ismore appropriate to use cost datarather than charge data, becausecharges bear a poor relationship to theactual economic impact of therapy(62,63).
Recommendation for ReportingStandards
The cost effectiveness of TRT andits risk-benefit ratio must be examinedin depth (64). Costs should be ana-lyzed over a long follow-up period toaddress potential differences in the
Table 8SIR Complications Master List
Complication Class Complication
Vascular Hematoma/bleeding at needle, device path: nonvascularprocedure
Hematoma/bleeding, puncture site: vascular procedureHematoma/bleeding, remote from puncture siteArterial occlusion/thrombosis, puncture siteArterial occlusion/thrombosis, remote from puncture
siteVenous occlusion/thrombosis, puncture siteVenous occlusion/thrombosis, remote from puncture
siteVasospasm, severeIntimal injury/dissectionPseudoaneurysmArteriovenous fistulaVascular perforation or ruptureArterial embolizationIschemia/infarction of tissue or organPulmonary embolismOther
Device-related MigrationMalpositionDevice malfunction with adverse effectOther
Contrast-related Allergic/anaphylactoid reactionRenal failureOther dose-dependent complicationTissue extravasationOther
Medication-related Incorrect drugIncorrect dosageIncorrect site of administrationIdiosyncratic reactionOther
Neurologic Transient ischemic attackStrokeSeizureOther CNS complicationOther neurologicPeripheral nervous system complication
Cardiac Hypotension, profoundVagal reactionArrhythmia, significantAngina/coronary ischemiaMyocardial infarctionCongestive heart failureOther
Respiratory/pulmonary Hypoxia, profoundPulmonary edemaPulmonary embolismRespiratory arrestOther respiratory/pulmonaryContamination of pleural cavity (urine, bile, empyema,
malignancy, etc.)PneumothoraxOther pleural complication
Infectious/inflammatory Local infectionSepticemia/bacteremiaSeptic ShockPancreatitisPeritonitisOther infectious/inflammatoryAbscess
General nonvascular Fluid/electrolyte imbalanceNoninfected fluid leakUnintended perforation of hollow viscusOther general nonvascular
Death Death related to procedure (�30-day mortality)Death unrelated to procedure
Note.—CNS � central nervous system.
Table 9Classification of Complications byOutcome
Minor complications:No therapy, no sequelaMinor therapy or minor sequela,
includes unplanned overnighthospital admission for observationonly (�24 hours)
Major complications:Requires major therapy or
unplanned hospitalization (24–48hours)
Requires major therapy, unplannedincrease in the level of care,prolonged hospitalization (�48hours)
Permanent adverse sequelaDeath
Patel et al • S461Volume 14 Number 9 Part 2
durability of procedures. Ideally, costsshould be compared with an assess-ment of quality of life so that costs perquality-adjusted life year can be deter-mined (65–67). Cost analysis might bedone best as a separate study.
COMPARISON BETWEENTREATMENT GROUPS
There are two general types of stud-ies that can be used in clinical trials toevaluate TRT (5,68). The first is a ran-domized clinical trial, which involvesthe random assignment of treatmentto each subject (69). The double-blindrandomized clinical trial is the “goldstandard” of clinical research. How-ever, it is often not feasible to conductsuch studies because of cost, patientrecruitment issues, and/or ethical con-siderations. If a clinical trial is eithernot possible or not feasible, much canbe learned from an observationalstudy (ie, case-control study, cross-sectional study, and cohort study) inwhich treatment is not assigned ran-domly. These studies often can be per-formed more easily than randomizedclinical trials and can be very informa-tive. A randomized, prospective studyis the methodology of choice for deter-mining the safety and efficacy of agiven TRT method and for comparingvarious TRT methods to one anotheror to surgical revascularization. Re-ports must indicate whether the studyis single-center, multi-center, spon-sored (if so, by whom), and, if spon-sored, whether it was performed un-der the aegis of the United States Foodand Drug Administration or other reg-ulatory body. The institutional reviewboard status must be provided. Formulti-center trials, the number of casesenrolled by each center and the indi-vidual institutional experience mustbe reported.
The hypothesis must be clearlystated. The primary and secondaryendpoints of the study must be clearlystated. The study design, estimatedSD, significance level, sample size, sta-tistical power, and statistical analysesmust be reported. Depending on thepurpose of the study, there should bea sufficient number of patients treatedso that the descriptive statistics andoutcomes can be reported for eachstratum, each sub-stratum, and thestudy population as a whole. Consul-tation with a statistician in the meth-
Table 10Recommendations for Reporting Standards
Data RequiredHighly
Recommended Recommended
Patient SelectionDefine target population X
Justification of study design XInclusion criteria XDescription of methods of assigning
treatmentX
Exclusion criteria XStratification of study group X
PretreatmentRisk factors/comorbidities XPre-procedure medications XDisease severity XFor surgical bypass graft occlusions:
type of graftX
Recent interventions (endovascular orsurgical) to the ischemic limb
X
Treatment descriptionLevel of operator experience XDetails of thrombolytic method used XLytic drug: type used, total amount used,
duration of useX
Device: type used, protocol of use XMethod of patient monitoring XMethod of treatment assessment (eg,
imaging)X
Regimen of concomitant anticoagulation(dose, titration)
X
Description of underlying lesion(morphology, location, length)
X
Adjunctive treatment (type, location) XAssessment of distal arterial bed
preadjunctive treatment Xpostadjunctive treatment X
Posttreatment pharmacologic management(eg, ASA, ticlid, etc.)
X
Posttreatment evaluationImmediate success XReporting causes for failures XLong-term results
Patency X1-year amputation free survival XMortality XPartial limb salvage XRecurrent ischemia X
StatisticsDemographics XSurvival curves X
Complications48 hours post-TRT
Major XMinor X
30-day and overallMajor XMinor X
BleedingMajor XMinor X
Costs XQuality of life assessment X
Note.—ASA � aspirin.
S462 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR

odology of the study design and sta-tistical analysis is recommendedbefore commencement of the study.
Primary statistical analyses shouldbe reported based on intent-to-treatand per-protocol analyses. With an in-tent-to-treat approach, subjects are an-alyzed with the group to which theywere randomized, even if theydropped out of the study or the treat-ment was not performed. The justifi-cation for this is that the study willthen measure the benefit or harm ofmaking a change in the practice ofmedicine. A per-protocol analysis con-siders only those patients receiving theintended treatment.
There are several statistical meth-ods that could be used for the analysisof data that is generated by a revascu-larization study. Because much of thedata are time-to-event data, survivalanalysis should be performed with useof either life-table or Kaplan-Meiertechniques (70,71). Survival analysiscan easily deal with missing data be-cause it merely treats the missing dataas if it were censored. Most other sta-tistical methods do not handle missinginformation nearly as neatly. If a sub-stantial portion of the data are miss-ing, an adjustment for it should bemade in the analysis (72). Survivalcurves should be compared with useof either the log-rank test or the Wil-coxon test. If the outcome variables arenot time-to-event data, there are otherstatistical methods that would be ap-propriate. If the response is binary (ie,a patient does or does not have a par-ticular adverse event at a specifictime), the different arms of the studycan be compared with either �2 test orlogistic regression. If there are demo-graphic or stratification variables thatshould affect the results of the analy-sis, logistic regression will allow forthe estimated treatment effects to beadjusted for the effects of the othercovariates. It is important to report testresults, even if they are not significant,to reduce the inherent publication biasin the literature.
CONCLUSION
Published studies on thrombolytictherapy for the treatment of acute limbischemia have been limited by incon-sistencies in study design, and pub-lished studies on mechanical throm-bectomy are currently lacking. It is the
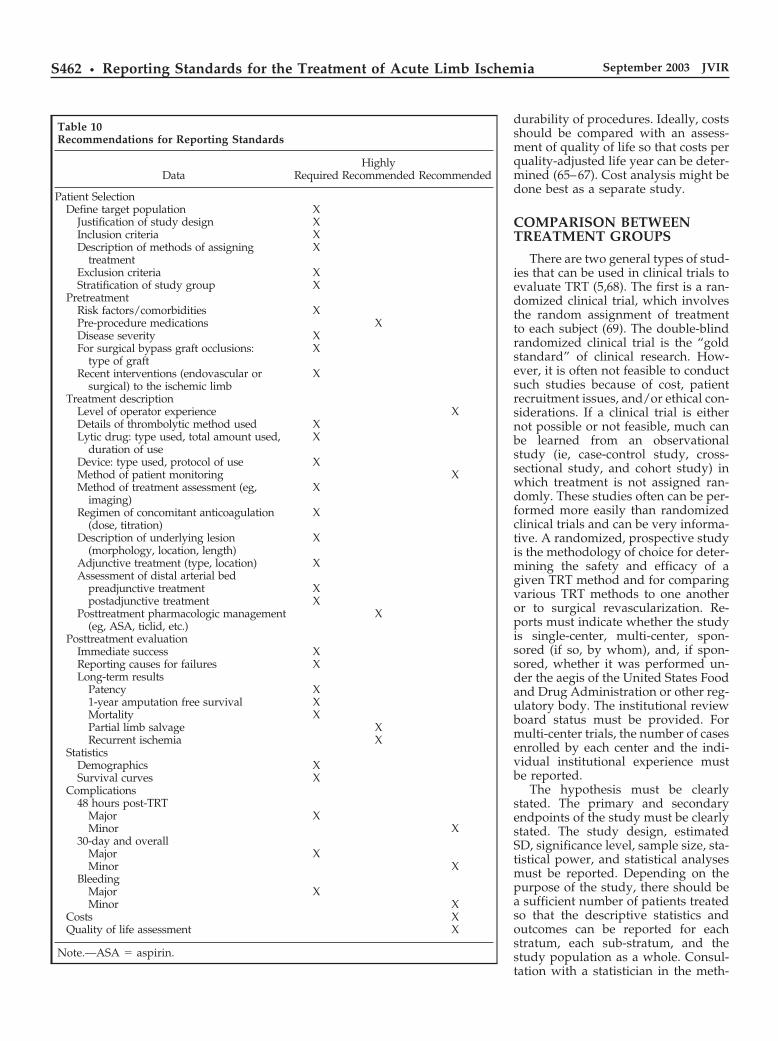
purpose of these reporting standardsto bring greater uniformity to researchon TRT for the treatment of acute limbischemia. A summary of the recom-mendations and requirements for re-porting are provided in Table 10.
References1. Dormandy JA, Rutherford RB. Man-
agement of peripheral arterial disease(PAD). TASC Working Group. J VascSurg 2000; 31(suppl):S1–S296.
2. Working Party on Thrombolysis in theManagement of Limb Ischemia.Thrombolysis in the management oflower limb peripheral arterial occlu-sion—a consensus document. Am JCardiol 1998; 81:207–218.
3. McNamara TO, Fischer JR. Throm-bolysis of peripheral arterial and graftocclusions: improved results usinghigh-dose urokinase. AJR Am J Roent-genol 1985; 144:769–775.
4. Beyersdorf F, Matheis G, Kruger S, etal. Avoiding reperfusion injury afterlimb revascularization: experimentalobservations and recommendations forclinical application. J Vasc Surg 1989;9:757–766.
5. Sacks D, Marinelli DL, Martin LG,Spies JB. General principles for eval-uation of new interventional technolo-gies and devices. Technology Assess-ment Committee. J Vasc Interv Radiol1997; 8:133–136.
6. Sacks D, Marinelli DL, Martin LG,Spies JB. Reporting standards forclinical evaluation of new peripheralarterial revascularization devices.Technology Assessment Committee JVasc Interv Radiol 1997; 8:137–149.
7. Rutherford, et al. Recommendedstandards for reports dealing withlower extremity ischemia: revised ver-sion. J Vasc Surg 1997; 26:517–538.
8. Bettmann MA. The present and thefuture for catheter-directed thrombo-lytic therapy. J Vasc Interv Radiol 1995;6(suppl):1S–2S.
9. Diffin DC, Kandarpa K. Assessmentof peripheral intraarterial thrombolysisversus surgical revascularization inacute lower-limb ischemia: a review oflimb salvage and mortality statistics. JVasc Interv Radiol 1996; 7:57–63.
10. Katzen BT, Van Breda A. Low dosestreptokinase in the treatment of arte-rial occlusions. AJR Am J Roentgenol1981; 136:1171–1178.
11. Hess H, Ingrisch H, Mietaschk A, RathH. Local low-dose thrombolytic ther-apy of peripheral arterial occlusions.N Engl J Med 1982; 307:1627–1630.
12. Sullivan KL, Gardiner GA Jr, ShapiroMJ, Bonn J, Levin DC. Acceleration ofthrombolysis with a high-dose trans-
thrombus bolus technique. Radiology1989; 173:805–808.
13. Valji K, Roberts AC, Davis GB, Book-stein JJ. Pulsed-spray thrombolysis ofarterial and bypass graft occlusions.AJR Am J Roentgenol 1991; 156:617–621.
14. LeBlang SD, Becker GJ, Benenati JF, Ze-mel G, Katzen BT, Sallee SS. Low-dose urokinase regimen for the treat-ment of lower extremity arterial andgraft occlusions: experience in 132cases. J Vasc Interv Radiol 1992; 3:475–483.
15. Sullivan KL, Gardiner GA Jr, KandarpaK, et al. Efficacy of thrombolysis ininfrainguinal bypass grafts. Circulation1991; 83(suppl):99–105.
16. Durham JD, Rutherford RB. Assess-ment of long-term efficacy of fibrino-lytic therapy in the ischemic limb. Se-min Intervent Radiol 1992; 9:166–173.
17. Ward AS, Andaz SK, Bygrave S. Pe-ripheral thrombolysis with tissue plas-minogen activator: results of two treat-ment regimens. Arch Surg 1994; 129:861–865.
18. Decrinis M, Pilger E, Stark G, Lafer M,Obernosterer A, Lammer J. A simpli-fied procedure for intra-arterial throm-bolysis with tissue-type plasminogenactivator in peripheral arterial occlu-sive disease: primary and long-term re-sults. Eur Heart J 1993; 14:297–305.
19. Berridge DC, Gregson RH, HopkinsonBR, Makin GS. Randomized trial ofintra-arterial recombinant tissue plas-minogen activator, intravenous recom-binant tissue plasminogen activatorand intra-arterial streptokinase in pe-ripheral arterial thrombolysis. Br J Surg1991; 78:988–995.
20. Meyerovitz MF, Goldhaber SZ, ReaganK, et al. Recombinant tissue-typeplasminogen activator versus uroki-nase in peripheral arterial and graft oc-clusions: a randomized trial. Radiology1990; 175:75–78.
21. Nilsson L, Albrechtsson U, Jonung T, etal. Surgical treatment versus throm-bolysis in acute arterial occlusion: arandomised controlled study. Eur JVasc Surg 1992; 6:189–193.
22. Graor RA, Comerota AJ, Douville Y, etal. Results of a prospective random-ized trial evaluating surgery versusthrombolysis for ischemia of the lowerextremity. The STILE trial. Ann Surg1994, 220:251–266.
23. Weaver FA, Comerota AJ, YoungbloodM, Froehlich J, Hosking JD, Papanico-laou G. Surgical revascularizationversus thrombolysis for nonemboliclower extremity native artery occlu-sions: results of a prospective random-ized trial. J Vasc Surg 1996; 24:513–521.
24. Comerota AJ, Weaver FA, Hosking JD,et al. Results of a prospective, ran-
Patel et al • S463Volume 14 Number 9 Part 2
domized trial of surgery versus throm-bolysis for occluded lower extremitybypass grafts. Am J Surg 1996; 172:105–112.
25. Ouriel K, Shortell CK, DeWeese JA, etal. A comparison of thrombolytictherapy with operative revasculariza-tion in the initial treatment of acuteperipheral arterial ischemia. J VascSurg 1994; 19:1021–1030.
26. Ouriel K, Veith FJ, Sasahara AA.Thrombolysis or peripheral arterialsurgery: phase I results. TOPAS Inves-tigators. J Vasc Surg 1996, 23:64–73.
27. Ouriel K, Veith FJ, Sasahara AA. Acomparison of recombinant urokinasewith vascular surgery as initial treat-ment for acute arterial occlusion of thelegs. Thrombolysis or Peripheral Arte-rial Surgery (TOPAS) Investigators.N Engl J Med 1998; 338:1105–1111.
28. Kandarpa K. Technical determinantsof success in catheter-directed throm-bolysis for peripheral arterial occlu-sions. J Vasc Interv Radiol 1995;6(suppl):55S–61S.
29. Shortell CK, Ouriel K. Thrombolysisin acute peripheral arterial occlusion:predictors of immediate success. AnnVasc Surg 1994; 8:59–65.
30. McNamara TO, Gardner KR, Bomb-erger RA, Greaser LE. Clinical andangiographic selection factors forthrombolysis as initial therapy foracute lower limb ischemia. J Vasc In-terv Radiol 1995; 6(suppl):36S–47S.
31. Ouriel K, Veith FJ. Acute lower limbischemia: determinants of outcome.Surgery 1998, 124:336–341.
32. Reekers JA. Kromhout JG, SpithovenHG, et al. Arterial thrombosis belowthe inguinal ligament: percutaneoustreatment with a thrombosuction cath-eter. Radiology 1996; 198:49–53.
33. Wagner HJ, Muller-Hulsbeck S, PittonMB, Weiss W, Wess M. Rapid throm-bectomy with a hydrodynamic cathe-ter: results from a prospective, multi-center trial. Radiology 1997; 205:675–681.
34. Gorich J, Rilinger N, Sokiranski R, et al.Mechanical thrombolysis of acute oc-clusion of both the superficial and thedeep femoral arteries using a throm-bectomy device. AJR Am J Roentgenol1998; 170:1177–1180.
35. Henry M, Amor M, Henry I, TricocheO, Allaoui M. The Hydrolyser throm-bectomy catheter: a single-center expe-rience. J Endovascular Surgery 1998;5:24–31.
36. Tadavarthy SM, Murray PD, InampudiS, Nazarian GK, Amplatz K. Mechan-ical thrombectomy with the Amplatzdevice: human experience. J Vasc In-terv Radiol 1994; 5:715–724.
37. Rousseau H, Sapoval M, Ballini P, et al.Percutaneous recanalization of acutely
thrombosed vessels by hydrodynamicthrombectomy (Hydrolyser). Eur Ra-diol 1997; 7:935–941.
38. Rilinger N, Gorich J, Scharrer-PamlerR, et al. Short-term results with use ofthe Amplatz device in the treatment ofacute lower limb occlusions J Vasc In-terv Radiol 1997; 8:343–348.
39. Huettl EA, Soulen MC. Thrombolysisof lower extremity embolic occlusions:a study of the results of the STAR Reg-istry. Radiology 1995; 197:141–145.
40. Blaisdell FW, Steele M, Allen RE.Management of acute lower extrem-ity arterial ischemia due to embolismand thrombosis. Surgery 1978; 84:822– 834.
41. Jivegard L, Holm J, Schersten T. Ar-terial thromboembolectomy—shouldanticoagulants be administered? ActaChir Scand 1986; 152:493–497.
42. Wholey MH, Maynar MA, WholeyMH, et al. Comparison of thrombo-lytic therapy of lower-extremity acute,subacute, and chronic arterial occlu-sions. Cathet Cardiovasc Diagn 1998;44:159–169.
43. Ikeda Y, Rummel MC, Field CK, et al.Relationship of runoff vessels to resultsfollowing thrombolysis and revascu-larization for synthetic graft occlusion-s.Am Surg 1995; 61:481–485.
44. Starck EE, McDermott JC, CrummyAB, Turnipseed WD, Acher CW, BurgessJH. Percutaneous aspiration thrombo-embolectomy. Radiology 1985; 156:61–66.
45. Sharafuddin MJ, Hicks ME. Currentstatus of percutaneous mechanicalthrombectomy. I. General principles. JVasc Interv Radiol 1997; 8:911–921.
46. Sharafuddin MJ, Hicks ME. Currentstatus of percutaneous mechanicalthrombectomy. II. Devices and mecha-nisms of action. J Vasc Interv Radiol1998; 9:15–31.
47. Sharafuddin MJ, Hicks ME. Currentstatus of percutaneous mechanicalthrombectomy. III. Present and futureapplications. J Vasc Interv Radiol 1998;9:209–224.
48. McNamara TO, Bomberger RA. Fac-tors affecting initial and 6 month pa-tency rates after intraarterial thrombol-ysis with high dose urokinase. Am JSurg 1986; 152:709–712.
49. Gardiner GA Jr, Harrington DP, Kol-tun W, Whittemore A, Mannick JA,Levin DC. Salvage of occluded arte-rial bypass grafts by means of throm-bolysis. J Vasc Surg 1989; 9:426–431.
50. Ouriel K, Kandarpa K, Schuerr DM,Hultquist M, Hodkinson G, Wallin B.Prourokinase versus urokinase for re-canalization of peripheral occlusions,safety and efficacy: the PURPOSE trial.J Vasc Interv Radiol 1999; 10:1083–1091.
51. Elliott JP Jr, Hageman JH, Szilagyi E,Ramakrishnan V, Bravo JJ, Smith RF.Arterial embolization: problems ofsource, multiplicity, recurrence, anddelayed treatment. Surgery 1980; 88:833–845.
52. Jivegard L, Holm J, Schersten T. Theoutcome in arterial thrombosis misdi-agnosed as arterial embolism. ActaChir Scand 1986; 152:251–256.
53. Sicard GA, Schier JJ, Totty WG, et al.Thrombolytic therapy for acute arterialocclusion. J Vasc Surg 1985; 2:65–78.
54. Kaul AF. Pharmacoeconomic consid-erations in peripheral arterial thrombo-lytic therapy. J Vasc Interv Radiol 1995;6(suppl):104S–110S.
55. Patel ST, Haser PB, Bush HL Jr, KentKC. Is thrombolysis of lower extrem-ity acute arterial occlusion cost-effec-tive? J Surg Res 1999; 83:106–112.
56. Van Breda A, Graor RA, Katzen BT,Risius B, Gillings D. Relative cost-ef-fectiveness of urokinase versus strep-tokinase in the treatment of peripheralvascular disease. J Vasc Interv Radiol1991; 2:77–87.
57. Janosik JE, Bettmann MA, Kaul AF,Souney PF. Therapeutic alternativesfor subacute peripheral arterial occlu-sion. Comparison by outcome, lengthof stay, and hospital charges. InvestRadiol 1991; 26:921–925.
58. Ouriel K, Kolassa M, DeWeese JA,Green RM. Economic implications ofthrombolysis or operation as the initialtreatment modality in acute peripheralarterial occlusion. Surgery 1995; 118:810–814.
59. Mark DB, Hlatky MA, Califf RM, et al.Cost effectiveness of thrombolytic ther-apy with tissue plasminogen activatoras compared with streptokinase foracute myocardial infarction. N EnglJ Med 1995; 332:1418–1424.
60. Weber JJ, Chong K. Regional throm-bolytic infusion for peripheral arterialocclusion: is urokinase really the drugof choice? Am J Health Syst Pharm1998; 55:2414–2416.
61. White HD. Selecting a thrombolyticagent. Cardiol Clin 1995; 13:347–354.
62. Perler BA. Cost-efficacy issues in thetreatment of peripheral vascular dis-ease: primary amputation or revascu-larization for limb-threatening isch-emia. J Vasc Interv Radiol 1995;6(suppl):111S–115S.
63. Schwartz JS. Clinical economics andnoncoronary vascular disease. J VascInterv Radiol 1995; 6(suppl):116S–124S.
64. Mark DB. Clinical and economic les-sons from studies of coronary throm-bolysis. J Vasc Interv Radiol 1995;6(suppl):94S–101S.
65. Hunink MG, Wong JB, Donaldson MC,
S464 • Reporting Standards for the Treatment of Acute Limb Ischemia September 2003 JVIR

Meyerovitz MF, de Vries J, HarringtonDP, et al. Revascularization for femo-ropopliteal disease: a decision andcost-effectiveness analysis. JAMA 1995;274:165–171.
66. Yin D, Forman HP, Langlotz CP.Evaluating health services: the impor-tance of patients’ preferences and qual-ity of life. AJR Am J Roentgenol 1995;165:1323–1328.
67. Yin D, Forman HP. Health care cost-
benefit and cost-effectiveness analysis:an overview. J Vasc Interv Radiol 1995;6:311–320.
68. Dawson-Saunders B, Trapp RG. Basicand clinical biostatistics. Norwalk CT:Appleton & Lange, 1994.
69. Begg C, Cho M, Eastwood S, et al. Im-proving the quality of reporting of ran-domized controlled trials: the CON-SORT statement. JAMA 1996; 276:637–639.
70. Collet D. Modelling survival data inmedical research. London: Chapman &Hall, 1994.
71. Wiles A, Atkinson G, Huson L, et al.Good statistical practice in clinical re-search: guideline standard operatingprocedures. Drug Information J 1994;28:615–627.
72. Little RJA, Rubin RB. Statistical anal-ysis with missing data. New York: JohnWiley & Sons, 1987.
Patel et al • S465Volume 14 Number 9 Part 2
Copyright © 2022 FDOKUMEN