
Balloon angioplasty results in increased segmental coronary distensibiliy: A likely mechanism of...
10
1ACCV.A . 23. No. 9 Ape1"1;1017-11 BalloonAngioplastyResultsinIncreasedSegmentalCoronary Distensibility:ALikelyMechanismofPercutaneousTransluminal CoronaryAngioplasty IAVIERnOTAS,MD,DAVIDA .CLARK,MD .FACC .FAUSfOPINTO,MD, ADRIANCHENZDRAIIN,MD,TIMA .FISCHELL .MD,FACC SmA{ond, CaliforodaapedNaslnille . reapeessee Obrabes.TheIsposeofthisso*wasto evaluate the hypa(bslsshottheuscram In lamestuseseducedbypereuhne- Mshaslomhalcoronary .aoplmttyesemdssgaachanpein lesion(sillsdal)duen6Hq . Rahgeuaad, DsplieThewideagodusofcoronaryangio- ph* .theprods nedpolm (de srehuess)Nlumenarm ImprovementremobmPotentunderstaw, MeLbb. QsathafiwossuaryWWWWB*was used in swore sheminimal leantra t long aced) balloondlammers m I Ii 5mm,lae9mlve,duringthefineandfi=1balloonInfatiosin 24 keens smnmldqheadwithceroearyangisplsty.Torule MIpstWesMaMIngefkeerdetodumtaInballommaterial dWeslbggydurhigrepeatedInltkus .Orecontrolballoouswere stalledavlvo. In parallel,loksweadprldtresMdbangingwas uWnudMcorpsethesegmentaldtdaantblfiq(duge In loosen seendaringthecwrdheqds)ofeightdisease-freeandseven .II ispsdorMaq handmmvemesAafter sapmrWIndbspsglopYSy. Rsah.hblamlbellowsdbmdersIncreasedeiguglcanlb belMeethefirsand`dinfadom(46%,33%.26% .14%sad Theprecisemechntdsm(s)ofimprovementinblmeacross- sectionalareaaftersuccessfulperculaneoustranstuminal mennaryangioplastyremainspoorlyunderstood .Early studiesconfirmedthatplaquecompressionandextrusion and distal®bolieationplayaminimalruleinthisprocess (t-3l.Someanimalandcadaverstudieshavesuggestedthat irreversiblemedial igjury with"anmuysmnl"dilationmight FromlIeDivisiondCadiuanenlarMrdrne .%dual Unvotsdy MedialCones.amefad.CSafemaredDtvabnorCsniislauy .Vetrbdl Univmd0Mead Center.Nacvie . Taessee.hiswar-prmdmd a par uthe64thAnmslSdsamkSodas of doAnaiaallime Anodaba.AsheeaCaMaab,Noeembor 1991. It amsuppoardinpail by a13nImIsreaquw Amd14 . FSsrhd4Gnat IKMI1 .mm1-0I, NsdomlHmn.Less .andPloudtmtnme .NadsdIodmNs of Hmab, Blhesd0 .Maryland.R. lams ismereegint d GramIN5220termire Fod9dekvsyacbasChapsedebSmuddadSdcbltflSAaodasaut 6nme FoodMsnMAFFKEModalSpain . MmascdrlreceivedSept-b., 21.1992 : meisednaaseriplno ivd No"sn6arm,1993,aoregedNoraibee A1993. Dr.TinA.Fsel . VaodertalUelveesay titledCake . Divines ofCmdiology. MeitalCenerNorth, CC-227& No&&-Tmmea37232. 0t9M bedo Anelimo CAW arcl,dbks 1043 ID%atL,3,3,4sad5am,telpeedvdy,allp<0 .0001), demonstratingan0temehaarterieldhksuaibhtiityaftersucffusNl coronaryangioplsty.NosignificantchapsInhalloos diameters aceobmneddaftsgamtldNlhlhtlhassat1ad2otm (n=S).tUbttmdIncreasesinhdhM diameters nereobeaed duringrepeatedballoonInhalanththeexvivooldiet(4 .9±It [mesa 3 SEMI . Adhosubllqboles,derivedfromdoiahw- vscularulhamaddata,wassotdiQereibetween lie hdlew. dilatedandtheretinal WPM* billwassigdghwlly lower 3s mildlydiseases .'ails114.7s31n .129 s 1.2vs.6 .9s13, reepecrvely,p<095)despiteawallpsquearea(7.3w1n. 11Js1neon''.prndenllmbNtedvadaredsegmats, svspec. lr~r,P<0.05) . Cdwdsbs,Cmsssydhdsdbilp)Ise sly Impaired In shmnwtenusaydimmedcoronarysegmentadblcresm slgul0canlyalts balloon agloplsq .Thisinareaaeinaegnsentb coronarycompienceaftercoronaryagoplslymayauka largerlumenareabyallowingthevesseltodistendInresponseto normalntraarterial pRmRe. (IAm CONCdrgW 1994;23;1( 43-S2) be aprimarymechanismoflumenenlargement (4-7). More recently (8-10),ithasbeensuggestedthatalargeproportion oftheincreaseInlumencross-sectionalareaaftercoronary angioplastyisrelatedtoanim:reaseinsegmentalcoronary distesibilityafterthemediaisreleasedfromthecicatrizing effectsofthenoncompliatintimalplaque .This"release"of themedia,secondarytoplaquesplitting,mayallowthe vesseltopassivelydistendinresponsetohydrostaticforces (bloodpressure). Thisstudywasconductedtoevaluatetheeffectofballoon dilationonsegmentalcoronarydistensibility.Weusedquail. titativeangiographictechniquestomeasurethedegreeof ro(mnstonofangioplastyballoonsatthesiteofacoronary lesionduringincrementallyincreasinginflationpressures duringthe first andfinalballooninflationduringcoronary angiopasty.Comparisonoftheminimalballoondiameter m eachsequentialpressureduringthetwofoliationprovidesa meantoquantifythechange .if any.in segmental(lesion) coronarydistensibilityinducedbycoronaryangioplsty .In anadditionalseriesof patients twoconsecutiveialbtions oils-1wJ%Sr.m
Transcript of Balloon angioplasty results in increased segmental coronary distensibiliy: A likely mechanism of...

1ACC V.A . 23. No. 9Ape 1"1;1017-11
Balloon Angioplasty Results in Increased Segmental CoronaryDistensibility: A Likely Mechanism of Percutaneous TransluminalCoronary AngioplastyIAVIER nOTAS, MD, DAVID A . CLARK, MD . FACC . FAUSfOPINTO, MD,ADRIAN CHENZDRAIIN, MD, TIM A. FISCHELL . MD, FACCSmA{ond, Califoroda aped Naslnille . reapeessee
Obrabes. The Is pose of this so* was to evaluate thehypa(bsls shot the uscr am In lamest uses educed by pereuhne-Mshaslomhalcoronary .a oplmttyesemdssgaachanpeinlesion (sills dal) duen6Hq .
Rahgeuaad, Dsplie The wideagod us of coronary angio-ph* . the prods nedpolm (de srehuess) N lumen armImprovement remobm Potent understaw,
MeLbb. Qsathafiw ossuary WWWWB* was used inswore she minimal leantra t long aced) balloon dlammers m IIi 5 mm, lae9mlve, during the fine and fi=1 balloon Infatios in24 keens smnm ldq head with ceroeary a ngisplsty. To ruleMI pstWesMaMIng efkeerde to dumt a In ballom materialdWeslbggy durhig repeated Inltkus .Ore control balloouswerestalleda vlvo. In parallel, loksweadpr ldtresMd banging wasuWnud M corpse the segmental dtdaantblfiq (duge In loosenseen daring the cwrdhe qds) of eight disease-free and seven.II ispsd orMaq h and mm vemesA aftersapmrW Indb s psglopYSy.Rsah. hblaml bellows dbmders Increased eiguglcanlb
belMee the firs and `d infadom (46%, 33%. 26% . 14% sad
The precise mechntdsm(s) of improvement in blmea cross-sectional area after successful perculaneous transtuminalmennary angioplasty remains poorly understood . Earlystudies confirmed that plaque compression and extrusionand distal ®bolieation play a minimal rule in this process(t-3l. Some animal and cadaver studies have suggested thatirreversible medial igjury with "anmuysmnl" dilation might
From lIe Division d Cadiuanenlar Mrdrne. %dual UnvotsdyMedial Cones. amefad. CSafema red Dtvabn or Csniislauy . V etrbdlUnivmd0 Mead Center. Nacvie. Ta essee. his war- prmdmda par u the 64th Anmsl Sdsamk Sodas of do Anaiaal limeAnodaba. Asheea CaMaab, Noeembor 1991. It am suppoard in pailby a 13nIm Isreaquw Amd 14. FSsrhd4 Gnat I KM I1 .mm1-0I,Nsdoml Hmn. Less . and Ploud tmtnme . Nadsd IodmNs of Hmab,Blhesd0. Maryland. R. lams is me reegint d Gram IN5220 term ireFod9de kvsyacbasCh apse deb Smuddad Sdcbl tflSAaodasaut6 n me FoodMsn MAFFKE Modal Spain .
Mmascdrl received Sept-b., 21. 1992 : meised naaseripl no ivdNo"sn6ar m,1993, aoreged Noraibee A 1993.
Dr. Tin A. F sel . Vaodertal Uelveesaytitled Cake. Divines of Cmdiology. Meital Cener North, CC-227&No&&- Tmmea 37232.
0t9M be do Anelimo CAW arcl,dbks
1043
ID % at L, 3, 3, 4 sad 5 am, telpeedvdy, all p < 0 .0001),demonstrating an 0temehaarterieldhksuaibhtiityaftersucffusNlcoronary angioplsty. No significant chaps In halloos diametersace obmned daft sgamtld N lhl htlhass at 1 ad 2 otm(n = S). tUbttmd Increases in hdhM diameters nere obeaedduring repeated balloon Inhalant h the ex vivool diet (4 .9± It[mesa 3 SEMI . A dhosubl lq boles, derived from do iahw-vscular ulhamad data, was sot diQerei between lie hdlew.dilated and the retinal WPM* bill was sigdghwlly lower 3smildly diseases .' ails 114.7 s 31 n . 129 s 1.2 vs. 6 .9 s 13,reepecrvely, p < 095) despite a wall psque area (7.3 w 1 n.11J s 1 neon''. prndenllmbNtedva dared seg mats, svspec.lr~r, P < 0.05).
Cdwdsbs, Cmsssy dhdsdbilp) Is e sly ImpairedIn shmnwtenusay dimmed coronary segment ad blcresmslgul0canly alts balloon a gloplsq . This inareaae in aegnsent bcoronary compience after coronary agoplsly may auk alarger lumen area by allowing the vessel to distend In response tonormal ntraarterial pRmRe.
(I Am CON CdrgW 1994;23;1( 43-S2)
be a primary mechanism of lumen enlargement (4-7). Morerecently (8-10), it has been suggested that a large proportionof the increase In lumen cross-sectional area after coronaryangioplasty is related to an im:rease in segmental coronarydistesibility after the media is released from the cicatrizingeffects of the noncompliat intimal plaque . This "release" ofthe media, secondary to plaque splitting, may allow thevessel to passively distend in response to hydrostatic forces(blood pressure).
This study was conducted to evaluate the effect of balloondilation on segmental coronary distensibility. We used quail.titative angiographic techniques to measure the degree ofro(mnston of angioplasty balloons at the site of a coronarylesion during incrementally increasing inflation pressuresduring the first and final balloon inflation during coronaryangiopasty. Comparison of the minimal balloon diameter meach sequential pressure during the two foliation provides amean to quantify the change . if any. in segmental (lesion)coronary distensibility induced by coronary angioplsty . Inan additional series of patients two consecutive ialbtions
oils-1wJ%Sr.m

If
-~
aN
1Y
.
c
Y
1.
-11Mg
p ~
gIts
~Hwu Ifill I
.1411 0-11 -1!
s,1.
x
WT
~
=s$
•su
~
dT
C
T C
3 oE'S
6.9.w
-1A
-114
1
gY
8~
Ya
$'S
'E~^
8 $
g* E5
$~~
~~',°3
E
IH_
•-U$
.11- a
24 i
a'C
2411-81MR
$5
~sy~~
,,,~paq
g~
rsrs5
~3
-i~u'Yw
cr
`d3pm~up Y.~B̀.,
quN ~ i
$~.g
e d~~
•v~
C qq
pa
'''QQQ$3
7 ,7,
q T
• IX
1iJ
fl
ji
a.
ai
'H
"•i
y+
'a
~E'3'~
•,3YF
,p

JACC Vat. 23. No . 5
BOTAS ET AL.no it 1994:t04$42
ANGIOPLASTY INCREASES CORONARY DISTBNSIBILITY
balloon boundaries and minimal and mean diameters werederived for each segment . Only minimal balloon diameterswere used for subsequent data analysis because they werethought to best represent the balloon contact zone with theunderlying diseased segment. in general for a given Lesionthe waist or minimal dimension of the balloon occurred atthe same site, but minimal diameter was objectively deter-mined by a compmer-assistted edge detection algorithm tocomes: objectivity and was not necessarily at en identical sitein the balloon in every terse . The same metaodology wasused to analyze t e reference vessel, the coronary lesionbefore and after coronary angioplasty and the control exvivo balloon inflation . AB me asuremens were performed intwo consecutive frames (end-diastolic for the in viva study) .The data shown represent the average of these two measure-ments. All measurements were performed by the sameinvestigator to minimize variability. The resolution of thissystem for coronary artery analysis has been demonstratedto be ±0.06 mm (11), with a (mean) frame to frame variation-0.15 mm .
Iuamnasrolar nYnmmd procedure& The procedure fornnraemonary ultrasound image acquisition at our institutionhas been described elsewhere (12) . Briefly, intravascularultrasound images were provided by a 5F or 4.3F 30-Miteultrasound catheter (CVIS Inc .). The catheter has a lumenthat accommodates a 0.014-in. (0 .036 em) roronrry guidewire that allows its manipulation in coronary ur eries similarto balloon angioplasty systems . Images were recorded anVisa. videotape for subsequent off-line analysis .
Intravasculatriabousound studies were perforated in sevenadditional patients immediately after successful coronarysngioplasty . Images of the balloon-dilated segment and of amildly diseased pmaimal segment were recorded . In addi-ttan, as a control group. images were obtained at twocoronary sites in font cerdfac transplant recipients who badm evidence of carorary artery disease by either aagiogra-phy or Mmr coronary ultrasound. Images of the balloon-dilated vessels (f.e ., the dilated segreeat and the proximalMildly diseased se(pnent) and the coronary mtmies of dueeardl a transplant recipients were subsequently digitizedonto a 512 x 512 x 8-bit matrix in 34•bmne sequencesobtained at 30 framesis by an image processing computer(Mesira Medical Inc.). The largess (systolic) and smallest(dieatolic) lumens from the digitized cardiac cycle wereobtained for analysis . The hman-vessel interfere ; and theexternal border of the indeed layer (i.e.. imimal-medialinterface) were traced by pla®euy. This allows calculationof the "plaque" area in the proximal and balloon-dilatedsegments in the patients with coronary angioplasty (i.e.,subtracting the lumen area from the arm within the externalbmderordie indeed layer) amd the calculation of afactionalmtimal area defend as the ratio of plaque area to the arm ofthe plaque Red lumen areas. This is refund to as the plaqueinfix . A distensibaiay index was calculated for each segmentas the largest mime the smallest lumen area divided by thesmallest lumen arm multiplied by 100 . A similar definition
1045
has been used by Gedey et al . (13). The data shownrepresent the average of three cardiac cycle measurements .
Statistics. All data am presented as mean value -_ SEM .Comparisons between minimal balloon diameters during thefirst second and final inflations were analyzed by one-wayanalysis of variance using repeated measures (Schefie r test,Stsnview) . Comparisons of intravascular ultrasound mea-surements between groups were performed using theKruskal-Wallis lest. Comparisons between two variablesware performed using a Student Repaired r test or Mann-Whitney f1 test for continuous variables and the chi-squaretest for categoric variables. Analysis of satterO am plotswas performed using a linear regression approach . Data arepleated as mean values for each group, with errors barssignifying tSEM . and p < 0.05 was considered statisticallysignillcsmt .
ResultsThe patient and procedural data are shown in Table 1 .
Twenty-four lesions were studied in 22 patients . Sinele-vessel coronary angioplasty was performed in 21 patientsand double-vessel angioplasty in 1 . AS of these lesions werenew stenoses. In addition, one of the previously includedlesions restenosed, and a second dilation was performed(lesion 3. Table 2) and included in the study. In one patientwith an intetmal mammary artery bypass to the left anteriordescending coronary artery, angioplasty of the "protected"left main coronary artery was performed . The average lesionlength was 5.6 ± 0.4 mm . Nine lesions were classified aseccentric (lesion centerline in the outer 25% of the lumen) .Nine of the lesions showed tuoroscopic calcifications, but inonly four was the calcification graded as moderate or severe .No lesion was on a bend >45°, and noangiegraphic evidenceof thrombus was observed before or after coronary angio-plasty. A 2.5-mum balloon was used in 14 lesions, a 3 .0-mmballoon in 8 and a 323-end 3.5-min balloon in I each. Theresult was successful (<50% residual diameter stenusis andTIMI Sow grade 3) in all lesions. Clinically insignificantintimal dissections were observed in six patients . There wasno abrupt vessel closure or emergency coronary arterybypass surgery.
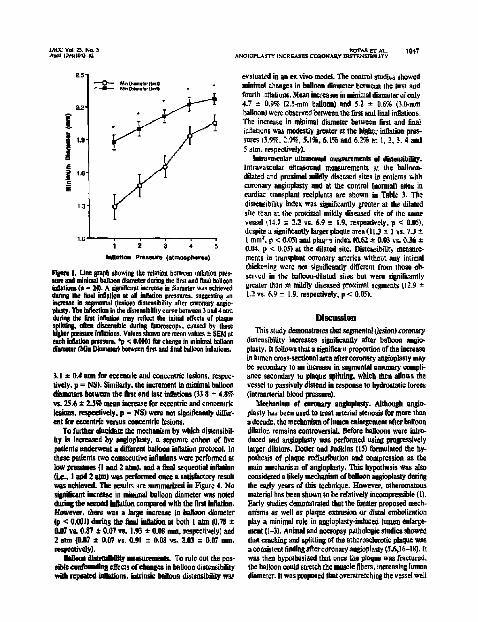
Inertia mnmaow ate of legal dlseodbllily. Minimalballoon diameters us each sequential pressure during the firstand final in vivo inllatons am shown in Table 2 . In Figure Ithe minimal diameter of the balloon at each sequentialpressure is plated for the first and final infations, At allpressures (1 to S amt), there was a significant increase in theminimal balloon diameter achieved after coronary angio-plasty. The increase in minimal balloon diameter was ¢real-est al low inflation pressures (46% at I atm [1.24 to 1.81 tons],33%at2atm(1.48to1.97mol,26%at3start [1 .67to2.11 mm], all p < 0 .0001). Although the increase diminishedat higher pressures, it remained statistically significant (14%increase at 4 arm [1,95 to 2 .21 non], 10% increase at 5 arm12.08 to 2.29 mm/, p < 0.0001). Therefore, a consistently

A
"~2
''s
2~een3rv
.~.n
n1Ir~n4N
V4ILI
jfhjhl~a41
Allis
rv~- - - x'~$NNN
~R-3STAt--R~f§~Sl,~,~,2$~aiye~{$KwiNNN NKµKrvrvn-r n n-
..-rvrvnn
9 3 Bm~n5&~rv~rvi
-
NNN4K56
4-nn-=N-NNNN
iggma;
------------
An
M-OR
Q-0-8465
---
-----------
TRo
.dd
-R16m-s
.ddd^d
^iiF3~
eacc~cc-'a-dea
a
ds sec
IACC van. a. Nn sAprel ILVelcas-n
2.5-
1 .3
1 .e
evaluated in an ex vivo model. The control studies showedminimal changes in balloon diameter between the hrst andfourth inflation. Mean increases in minimal diameter of only4 .7 ± 0 .9% (2.5-mm balloon) and 5.2 ± 0.6% (3 .0-mmballoon) were observed between the first and final infations .The increase in minimal diameter between first and finalinflation was modestly greater at the higher inflation pres-sures (3 .94% 2 .9%, 5.1%. 6.1% and 6 .2% at 1, 2, 3 . 4 and5 atm . respectively).
)nlrarascnlar alnasopiad mesarements of dislessibllity.Intravascular ultrasound measurements at the balloon-dilated and proximal mildly diseased sites in patients withcoronary angoplasty and at the control (normal) sites incardiac transplant recipients m e shown us Table 3 . Thedistenibility index was significantly greater at the dilatedshe than at the proximal mildly diseased site of the samevessel (14 .7 a 2.2 vs. 6.9 C 1 .9. respectively. p < 0.05) .despite a significantly Foyer plague urea (I L .) T- I vs . 7.3 ±I mm= . p < 0.051 and plag" •s index (0 .62 m 0.03 vs . 0.36 .t0.04, p < 0.0.0 at the dilated site. Disteasibility measure-
hmamm Praawra (atmosplrraa) meets in transplant coronary arteries without any intimalthickening ware am significantly different from those ob-served in the balloon-dilated sites but wine significantlygreater than in mildly diseased proximal segments (12 .9 1.2 vs. 6.9 ± 1 .9. respectively, p < 0.05) .
- -- 0- MTaumNerairsa-.- Matwswrioni
1
2
3
s
5
Flgme 1 . Line graph showing the relation between inflation pr e-,sum and minimal balloon diameter during the first and final ballooninflation (a - 24) . A siani5caot increase in diameter was achievedduring the goal inflation at all inflation pressures. suggesting anincrease in segmental (lesion) disienslbtity after coronary angieplasty. The inflection in the distensibility curve between 3 and 4 atmdating the first inflation may reflect the initial effects of plaquesplitting, often discernible during finoroscop) . caused by thesehigher pressure inauriom . Values shown am mean values ± SEM ateach inflation pressure. °p a 0.0001 for change in minimal balloondiameter (Min Diameter) between first and final balloon inflation .
3.1 * 0.4 atm for eccentric and concentric lesions . respec-tively . p = NS) . Similarly, the increment in minimal balloondieoeters between the first and last inflation (33 .8 t 4.8%vs . 25 .6 s 2.5% mean increase for eccentric and concentriclesions . respectively. p = NS) were net signifleantiy differ-ent for eccentric versus concentric lesions.
To further elucidate the mechaaiam by which distensibil-hy is increased by angioplasty, a sepnmre cohort or fivepatients underwent a different balloon inflation protocol . Inthese patients two consecutive inflation were performed atlow pressure (I and 2 atm). NW a final sequential inflation(i e., I and 2 mm) was performed once a satisfactory resultwas achieved. The results are summarized in Figure 4 . Nosignificant increase in minimal balloon diameter was notedduring the second litigation compared with the Oral inflation.However, there was a large increase in balloon diameter(p < 0 .001) during the hand inflation at both I atm (0.78 ±0.07 vi . 0.87 t 0.07 vs. 1 .93 ± 0.08 mm, respectively) and2 aim (0.07 ± 0.07 vs. 0.91 t 0.08 vs . 2 .03 *- 0.07 mm.respectively).
Orison dlaemlb0gy measurements. To rule out the pos-sible cmdannding effects of changes in balloon distensibilitywith repeated inflation, iaainsic balloon distensibility was
avrA_a ET AL
1047ANGIOPLASTY INCREASES CORONARY O sannssnannsTY
Ulacma®hThis study demonstrates that segmental (lesion) coronary
distensibility increases significantly after balloon angio .plasty . It follows that a significa n proportion of the increasein lumen cross-sectional area after coronary angioplasty maybe secondary to an increase in segmental eotrmary, compli-ance secondary to plaque splitting, which then allows thevessel to passively distend in response to hydrostatic forces(intmsrterial blood pressure) .
Meelmnism of coronary angioplasty. Although angio-plasty has been used to treat arterial stenosis for more thana decade, the mechanism of lumen enlargement after balloondilation remains controversial . Before balloons were intro-duced and angioplasty was performed using progressivelylarger dilators, Dotter and Judkins (I5) formulated the hy-pothesis of plaque redistribution and compression as themain mechanism of anglopasty . This hypothesis was alsoconsidered a likely mechanism of balloon angioplasty daringthe early years of this technique . However, atheromatousmaterial has been shouts to be relatively incompressible (1) .Early studies demonstrated that the farmer proposed meeh-anisma as well as plagnee exrnsims or distal embolizarionplay a minimal rob in angioplasty-induced baton enlarge-ment (1-3) . Animal and necropsy pathologic studies showedthat cracking and splitting of the atherosclerotic plaque wasa consistent findingaftercoronary angioplasty (5,6,16-18) . Itwas then hypothesized that once the plaque was fractured,the balloon could stretch the muscle fibers, increasing lumendiameter. It was proposed that overstretching the vessel wall

B E 2
9Iw
3
td•iU1
t8 F8 $
16°0
-2
n
i.ii
g
t

JACC VOL 23. No . 5April 19%4.1043-2
6 •
7
00 2
5=St
•
y - 0.5055 . 2.42200
0.4
6.0
00
1 .0
12
1 .1
Minimum Lesion Diameter (mm)
Plgen 3. Seattelgmm showing the relation between the minimalkdat diametertsefore coronary angioplasty and the pl-wre duringthe first inflation needed to achieve two-thirds of the control balloondiamnerat 5 star . This variable provides an estimate of the intrinsi.dlsteaslbllby , of the lesions. By this definition. intrinsic distensibi9tyappears to be Inversely related to lesion severity . Thus . the smallerthe baseline diameter the greater the pressure needed to achievetwo-thirds of the commit balloon diameter during the initial inflation(p < 0.05).
Flgme 4. Bar graph demonstrating the effects of sequential lowpressure (I to 2 alai) inflation on vessel distensibility (n = 5) .Values shown are mass value `- SEM at each inflation pressure.Sequential low pressure inflatium fail to lacrosse segmental (iesien)dislensibIlry, as determined by minimal balloon diameters achievedat I•and 2atm balloon inflation pressure . After successPol coronaryatgioplasty at higher balloon inflation pressures (map S to 8 aim),there is a parked increase in segmental distensibility (p valueseompmmg fiat and second inflation to final inflation n shown) .
I mmesphwe
a stmoapheresInflation Pressure
aoTAS Sr AL.
1049ANGIOF : .1STY INCREASES CORONARY DISTENSIOILITY
14 .29, 50
Cti16.4510.46.73
11 .8917.%
Nom.]
'See test for explanation. PrCA = pereutunmus traoslundnal coronaryrgimplasty.
•
6-
•
a
•
a
damage In a previous study performed under carefullycontrol . : laboratory conditions. it was demonstrated thatrelatively severe degrees of stretching (>50% beyond re-laxed internal medial diameter) were aecessary to inducesmooth muscle paralysis in muscular arteries (8) . In con-trast, it has been estimated that coronary angioplasty moretypically results in only 15% to 30% stretching of the mediabeyond its relaxed diameter (8) . These observations suggestthat the hypothesis of balloon-induced irreversible medialinjury with subsequent smooth muscle paralysis is an un-likely mechanism for lumen improvement after coronaryangioplasty.
Arterial dlsteoslhlkyt m1edograpbfe measurements . Pre-vious studies (28,29) have used balloon pressure-diameterrelations to try to assess different characteristics of theplaque but not specifically to try to evaluate the changesinduced by balloon angioplasty. Our data demonstrate anincrease in arterial distensibility after coronary angioplastyat all sequential balloon inflation pressures. The finding ofonly very small increases in minimal balloon diametersbetween the first and final balloon inflations in the ex vivoprocedures suggest that changes in balloon material disten-sibihty would not explain the large increases in distensibilityobserved in vivo, particularly at low inflation pressures .
Table 3. 'ntravascular Ultrasound Data'Didussbility Plaque Lumen,{leaOccupied
Ivdvs Ana (mar) by Plaque 1331
PrCA Sine17.10 63.15
d s3 7.16 06.-wIO?1 11.14 61 .2211225 13 .57 64.93
2 .70 12.0 64.022.56 7.4 ea.01343 15.0 69 .12
btadly Disemcd
6 .66 11.6 44 .616 .66 6.4 . 5 .3
5 .36 s .2 36.3108 4 .23 21 .560.43 5 .23 24.37'.41 5 .80 33.337.60 9.70 40,63

HO
.1P.9
NJ - m
v
L,
W:t
H a
All
a]
1
li t
w e
IMi
IUlf
allMIS
I'sI
IS
all11
14
,141j,111
*41

tACC Vol 23. No . 5Apse $9410os2
cacao ma LImeIALarose aeetrcanLAeEA
ARTERY BEFOREANGIOPLASTY
Lslen (Dotter e(hct), making it anon difficult to assess theresponse of the lesion to the first dilation .
h Is recoga cad that engiogmphk : measurement of mini-msl balloon preen diameter is a relatively indirect techniquefor precise determinutiat of the physical characteristics(dlstendbihy) of the underlying arterial segment . For exam-ple, in a number of eases the minimal balloon lumen diam-eter at I arm was slightly smaller Then the measured post-agioplesty minimal lesion diameter. 'These are severalpotential enplnnations for this : 1) Balloon diameter is amname of the contrast column inside the inflated balloonand his to take into account the thickness (m two sides) cithe balloon mawrial (i .e., two sides of Pdyethylene 600 is010 mm thick (Advanced Cardiovascular Systems . personalcommmieatlon . October 19931). 2) In cases where there ismarked segmental dilation after high pressure (therapeutic)miktions, the minimal lumen diameter at physiologic bloodpressure my h larger than the inlased balloon diameter atlow Measure such that the balloon does tea contact theastesial wall and will srtderesdmate the segmental compli-ance . 3) The contrast density of Coeray 60 used in theballoon Is leas don that used (Omeipaque 3501 duringpootighplasty angiogrnphy. 4) Small air bubbles in theballoon could lead to underestimation of the balloon diame-ter, psRiculatly at low pressures. 5) Extaluminal (subin6-map contrast tray be detected during the quantitative mea-
EOTAS or AL.
1051ANOIOPtSSrY tb-CReases CORONARY 1RSTENSnMY
DURING BALLOONINFLATION
AFTER SUCCESSFULPTCA
1Warm. 1340%1
Ft0ams. Schematicillsladruthemarked increase intrsioulumencmss-sectianal area expected, who modest increases in segmentaldiatettsi40hy. Asslagnga 101 increase in segaenatdistensitildy at60rnm He perfusion (mean anesia) pressure ever successful plaquesplteing. There wpold be a 340% increase in mono cross section,assuming that the plaque is completely mcan presoote and is neitherexmded em embalaed . PTCA m pereuaneous tmnalumiml camnary angioplany.
surements or minimal lumen diameter after coronaryangioplasty. and this may lead to overestimation of theactual diameter mediating the balloore-vessel wall contact .overall, the mining tureen diameter of the balloon was only0.12 m 0.05 ran analler than the minimal lumen diameter ofthe postangioplasty segment at s-atm balloon inflation pres-sure and was 0.05 0:0.04 mm larger than the lesion minimallumen diameter at 2 atm . Thus, it is possible that thepostangioplasty (lesion) segmental distensibility was slightlyunderestimated by the balloon diameter measurements atI am (i .e., the lumen was larger m a physiologic distendingpressure of 70 to 100 mm Hg than at the balloon Inflationpressure of 160 mm Hg1I atm). However, this underestima-tion appears to be modest and would not alter the mainconclusions of this study .
Implications and conclusions. To explain how increasedlesion disteusibility, may account for successful coronary
Met11A
PLAQUE
BEFORE AFTER
EL000Paeaua aware- w mnq- mmman
PLAmiAR4a_ _ ll.amm~- . .. 11.amma
cetpLUacc( }_g g.ammnM,map- =0.025 mMnmaalaaemrmslat
1LtaeRAL _ n •pamna a.. Doe coma -- a •lsamala-1L70a- I&42
mm2 latoraecnnnal1%

-d0111
Ila I-*
jib]~
~ '
e
..
-It~
•
`
Sa
zs
eg-
-Ijow
all.MR
-N
..i'.
.nd
.- - d
- - d




















