Percutaneous transluminal angioplasty for the treatment of limb threatening ischemia: Do the results...
33
Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients (Review) van Zuuren EJ, Fedorowicz Z, Pucci E, Jagannath VA, Robak EW This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2012, Issue 12 http://www.thecochranelibrary.com Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients (Review) Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Percutaneous transluminal angioplasty for the treatment of limb threatening ischemia: Do the results...

Percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis patients (Review)
van Zuuren EJ Fedorowicz Z Pucci E Jagannath VA Robak EW
This is a reprint of a Cochrane review prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2012 Issue 12
httpwwwthecochranelibrarycom
Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
4OBJECTIVES
5METHODS
8RESULTS
Figure 1 9
10DISCUSSION
11AUTHORSrsquo CONCLUSIONS
11ACKNOWLEDGEMENTS
12REFERENCES
16CHARACTERISTICS OF STUDIES
25DATA AND ANALYSES
25ADDITIONAL TABLES
30HISTORY
30CONTRIBUTIONS OF AUTHORS
31DECLARATIONS OF INTEREST
31SOURCES OF SUPPORT
31DIFFERENCES BETWEEN PROTOCOL AND REVIEW
iPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Percutaneous transluminal angioplasty for treatment ofchronic cerebrospinal venous insufficiency (CCSVI) inmultiple sclerosis patients
Esther J van Zuuren1 Zbys Fedorowicz2 Eugenio Pucci3 Vanitha A Jagannath4 Edward W Robak5
1MS Consumer Oegstgeest Netherlands 2UKCC (Bahrain Branch) The Cochrane Collaboration Awali Bahrain 3UO Neurologia
- Ospedale di Macerata ASUR Marche - Zona Territoriale 9 Macerata Italy 4Department of Paediatrics American Mission Hospital
Manama Bahrain 5MS Consumer Fredericton Canada
Contact address Esther J van Zuuren MS Consumer Oegstgeest Netherlands EJvan_Zuurenlumcnl
Editorial group Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous System Group
Publication status and date New published in Issue 12 2012
Review content assessed as up-to-date 3 April 2012
Citation van Zuuren EJ Fedorowicz Z Pucci E Jagannath VA Robak EW Percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients Cochrane Database of Systematic Reviews 2012 Issue
12 Art No CD009903 DOI 10100214651858CD009903pub2
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Multiple sclerosis (MS) is a leading cause of neurological disability in young adults The most widely accepted hypothesis regarding its
pathogenesis is that it is an immune-mediated disease It has been hypothesised more recently that chronic venous congestion may be
an important factor in the pathogenesis of MS This concept has been named rsquochronic cerebrospinal venous insufficiencyrsquo (CCSVI) and
is characterised by stenoses of either the internal jugular or azygos veins or both It is suggested that these stenoses restrict the normal
blood flow from the brain causing the deposition of iron in the brain and the eventual triggering of an auto-immune response The
proposed treatment for CCSVI is percutaneous transluminal angioplasty also known as the rsquoliberation procedurersquo which is claimed to
improve the blood flow in the brain thereby alleviating some of the symptoms of MS
Objectives
To assess the effects of percutaneous transluminal angioplasty for the treatment of CCSVI in people with MS
Search methods
We searched the following databases up to June 2012 The Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous
System Group Specialised Register CENTRAL in The Cochrane Library 2012 Issue 5 MEDLINE (from 1946) EMBASE (from
1974) and reference lists of articles We also searched several online trials registries for ongoing trials
Selection criteria
Randomised controlled trials assessing the effects of percutaneous transluminal angioplasty in adults with multiple sclerosis that have
been diagnosed to have CCSVI
Data collection and analysis
Our searches retrieved 159 references six of which were to ongoing trials Based on assessment of the title or abstract or both we
excluded all of the studies with the exception of one which was evaluated following examination of the full text report However this
study also did not meet our inclusion criteria and was subsequently excluded
1Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
No randomised controlled trials met our inclusion criteria
Authorsrsquo conclusions
There is currently no high level evidence to support or refute the efficacy or safety of percutaneous transluminal angioplasty for treatment
of CCSVI in people with MS Clinical practice should be guided by evidence supported by well-designed randomised controlled trials
closure of some of the gaps in the evidence may be feasible at the time of completion of the six ongoing clinical trials
P L A I N L A N G U A G E S U M M A R Y
The more popularly known rsquoLiberation procedurersquo for treatment of venous stenoses (CCSVI) in the brain of MS sufferers
Multiple sclerosis (MS) is an inflammatory disease of the nervous system and the most frequent cause of neurological disability in
young adults Myelin the material that wraps around and protects the nerves becomes damaged and this results in scarring and the
formation of scar-like plaques
MS is considered to be an immune-mediated disease in which the personrsquos own immune system attacks the nervous system and most
of the current drug therapies are based on this hypothesis
However a new theory has been recently proposed with a suggestion that impaired blood flow in the veins draining the central nervous
system so called chronic cerebrospinal venous insufficiency (CCSVI) may play a role in the cause of MS CCSVI is thought to be
congenital and it may result in iron deposits which in turn trigger the immune system to attack the central nervous system thus
damaging the myelin The proposed treatment for CCSVI is balloon angioplasty which entails the widening of narrowed (stenosed)
veins the commonly named rsquoliberation procedurersquo This theory has gained a lot of attention via the Internet mainly among the patientsrsquo
community and the increased interest by the media has further enhanced the expectations of people suffering with MS We searched
the relevant literature but found no studies that matched the criteria of methodological quality necessary for their inclusion in this
review
There is currently no evidence to support or refute the efficacy and the safety of angioplasty for CCSVI in people with MS Well-
designed and robust studies are warranted
B A C K G R O U N D
Unfamiliar terms are listed in the rsquoGlossary of termsrsquo in Table 1
Description of the condition
Definition signs and symptoms
Multiple sclerosis (MS) is a leading cause of neurological disability
in young adults The disease is characterised by demyelination ax-
onal loss and inflammation (Compston 2008) Four clinical forms
of MS can be distinguished relapsing-remitting (RRMS) sec-
ondary progressive (SPMS) primary progressive (PPMS) and pro-
gressive relapsing (PRMS) MS (Lublin 1996) RRMS and SPMS
are the clinical forms of MS that account for approximately 80
to 85 of sufferers and SPMS evolves from the RRMS form
(Lublin 1996)
MS is heterogeneous both histopathologically and clinically
(Lucchinetti 1996) and the natural history can be difficult to
predict In most cases it begins as RRMS with episodic largely
reversible neurological dysfunction (Nessler 2010) Natural his-
tory studies have shown that after a period of approximately
10 years almost 50 of people with MS gradually develop per-
manent disability (ie SPMS) which may also include acute re-
lapses (Weinshenker 1989) After a median of 15 to 28 years
(Tremlett 2006 Weinshenker 1989) from disease onset a disabil-
ity milestone equivalent to the use of an assistive walking device is
reached Whether current disease-modifying drugs (DMDs) alter
these prognostics is unknown Clinical features include all of the
symptoms caused by the impairment of the central nervous system
2Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(CNS) (eg loss of vision double vision muscle weakness sen-
sory disturbances bladder dysfunction impotence constipation
ataxia vertigo tremor spasticity pain cognitive impairment and
dysarthria) fatigue anxiety and depression are also frequent oc-
currences (Compston 2008) Magnetic resonance imaging (MRI)
can support the clinical diagnosis and it is integrated with clinical
and other para-clinical diagnostic methods (eg examining cere-
brospinal fluid and evoked potentials) to facilitate the diagnosis
of MS (Polman 2011) MRI parameters are also used as surrogate
markers of disease activity and progression
The disease has an adverse impact on the health-related quality of
life (HRQoL) of people with MS and their families and may also
pose a financial burden even when the disease is not physically
disabling
Epidemiology and causes
The most widely accepted hypothesis on the pathogenesis of
MS is that it is an immune-mediated disease characterised by
lymphocytic infiltration leading to damage of myelin and axons
(Compston 2008)
Although the aetiology is largely indeterminate a large propor-
tion of the scientific community considers that MS develops in
genetically predisposed subjects and that environmental factors
play a central role in its pathogenesis based on immune-mediated
mechanisms It is thought that aberrant immune responses to self
or foreign antigens cause and perpetuate inflammation (Frohman
2006) The inflammation leads to demyelination and subsequent
axonal damage However the role of inflammation is considered
to be complex and may include both beneficial and detrimen-
tal effects (Martino 2002) Some researchers also consider that
a cryptic aetiological agent may be the primary cause of axonal
damage and demyelination as well as inducing an inflammatory
response that could play a secondary role (Barnett 2006 Maggs
2004 Trapp 1998)
The age of onset of MS is usually between 20 and 40 years
(Ascherio 2007) Incidence is low in childhood and is rarer at the
age of 50 years or older Female to male ratios vary between 151
and 251 in most populations but this ratio has increased over the
last decade (up to 2011) (Sellner 2011) The incidence and preva-
lence of MS varies geographically (Ebers 2008 Simpson 2011)
High-frequency areas (prevalence in excess of 60 per 100000 peo-
ple) include all of Europe in addition to southern Canada north-
ern US New Zealand and south-east Australia In many of these
areas the prevalence is more than 100 per 100000 people This
geographic variance may be explained in part by racial differences
white populations especially those from northern Europe appear
to be most susceptible People of Asian African or American In-
dian origin have the lowest risk with other groups intermediate
MS is most likely to be caused by a complex interaction between
polygenetic and environmental factors (Hohlfeld 2011) The ma-
jor histocompatibility complex confers the greatest genetic risk
on susceptibility to MS Recent work has highlighted the impor-
tance of both HLA-DR and HLA-DQ in determining risk (Burrell
2011) There is also a widely held belief of an association between
geographical latitude and MS with the risk of MS increasing from
south to north Exceptions to the gradient are likely to be as a
result of genetic and behavioural-cultural variations (Ebers 2008
Simpson 2011) Geographical latitude and sunshine exposure and
the resulting increase in vitamin D levels which are closely related
are major environmental factors associated with the risk of devel-
oping MS (Burrell 2011 Comabella 2012 Simpson 2011) The
involvement of UV light in the production of vitamin D has gen-
erated a perception that vitamin D is itself the latitudinal factor
that influences the risk of developing MS Direct support for this
comes from a prospective study showing that low serum 25-hy-
droxyvitamin D (25-OH-D) (the circulating form of vitamin D)
levels are associated with an increased risk of MS (Munger 2006)
Other factors that have been suggested include exposure to Ep-
stein Barr virus with an almost 100 prevalence in MS patients
and tobacco smoking (Burrell 2011 Ebers 2008)
A more recent hypothesis suggests that chronic venous congestion
may be an important factor in the pathogenesis of MS (Zamboni
2006 Zamboni 2009a Zamboni 2010 Zamboni 2011a) The
predominantly venotopic location of MS lesions in the CNS is
postulated to be a consequence of local erythrocyte extravasation
owing to elevated transmural venous pressure (rsquovenous conges-
tionrsquo ie analogous to lower-limb chronic venous insufficiency)
followed by erythrocyte degradation and iron-driven phagocytosis
and subsequent lymphocytic infiltration (Singh 2009) This con-
cept has been named rsquochronic cerebrospinal venous insufficiencyrsquo
(CCSVI) and is characterised by stenoses of the internal jugular
veins azygos veins or both which restrict the normal blood flow
from the brain along with the appearance of small collateral veins
that may have developed to reduce the impact of the stenoses
(Zamboni 2009a) In his initial study Zamboni found CCSVI
in all subjects in the study group that were diagnosed with MS
and none in the healthy controls (Zamboni 2009a) Zambonirsquos
research group maintained that CCSVI can be non-invasively and
reliably diagnosed through the use of combined transcranial and
extracranial echo colour Doppler (ECD) by individuals trained to
recognise the indicators of CCSVI (Menegatti 2008 Menegatti
2011 Zivadinov 2011b)
ECD is used to measure five variables
1 reflux in the internal jugular veins (IJVs) or in the vertebral
veins (VVs) or both with the head in any position
2 reflux in the deep cerebral veins
3 high-resolution B-mode evidence of IJV stenoses
4 flow not detected by Doppler in the IJVs or VVs or both
5 reverted postural control of the main cerebral venous outflow
pathways
The diagnosis of CCSVI needs to fulfil at least two of these five
ECD indicators (Zamboni 2009a)
There has been some criticism of several of the limitations in the
3Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
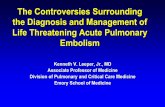
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

T A B L E O F C O N T E N T S
1HEADER
1ABSTRACT
2PLAIN LANGUAGE SUMMARY
2BACKGROUND
4OBJECTIVES
5METHODS
8RESULTS
Figure 1 9
10DISCUSSION
11AUTHORSrsquo CONCLUSIONS
11ACKNOWLEDGEMENTS
12REFERENCES
16CHARACTERISTICS OF STUDIES
25DATA AND ANALYSES
25ADDITIONAL TABLES
30HISTORY
30CONTRIBUTIONS OF AUTHORS
31DECLARATIONS OF INTEREST
31SOURCES OF SUPPORT
31DIFFERENCES BETWEEN PROTOCOL AND REVIEW
iPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
[Intervention Review]
Percutaneous transluminal angioplasty for treatment ofchronic cerebrospinal venous insufficiency (CCSVI) inmultiple sclerosis patients
Esther J van Zuuren1 Zbys Fedorowicz2 Eugenio Pucci3 Vanitha A Jagannath4 Edward W Robak5
1MS Consumer Oegstgeest Netherlands 2UKCC (Bahrain Branch) The Cochrane Collaboration Awali Bahrain 3UO Neurologia
- Ospedale di Macerata ASUR Marche - Zona Territoriale 9 Macerata Italy 4Department of Paediatrics American Mission Hospital
Manama Bahrain 5MS Consumer Fredericton Canada
Contact address Esther J van Zuuren MS Consumer Oegstgeest Netherlands EJvan_Zuurenlumcnl
Editorial group Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous System Group
Publication status and date New published in Issue 12 2012
Review content assessed as up-to-date 3 April 2012
Citation van Zuuren EJ Fedorowicz Z Pucci E Jagannath VA Robak EW Percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients Cochrane Database of Systematic Reviews 2012 Issue
12 Art No CD009903 DOI 10100214651858CD009903pub2
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Multiple sclerosis (MS) is a leading cause of neurological disability in young adults The most widely accepted hypothesis regarding its
pathogenesis is that it is an immune-mediated disease It has been hypothesised more recently that chronic venous congestion may be
an important factor in the pathogenesis of MS This concept has been named rsquochronic cerebrospinal venous insufficiencyrsquo (CCSVI) and
is characterised by stenoses of either the internal jugular or azygos veins or both It is suggested that these stenoses restrict the normal
blood flow from the brain causing the deposition of iron in the brain and the eventual triggering of an auto-immune response The
proposed treatment for CCSVI is percutaneous transluminal angioplasty also known as the rsquoliberation procedurersquo which is claimed to
improve the blood flow in the brain thereby alleviating some of the symptoms of MS
Objectives
To assess the effects of percutaneous transluminal angioplasty for the treatment of CCSVI in people with MS
Search methods
We searched the following databases up to June 2012 The Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous
System Group Specialised Register CENTRAL in The Cochrane Library 2012 Issue 5 MEDLINE (from 1946) EMBASE (from
1974) and reference lists of articles We also searched several online trials registries for ongoing trials
Selection criteria
Randomised controlled trials assessing the effects of percutaneous transluminal angioplasty in adults with multiple sclerosis that have
been diagnosed to have CCSVI
Data collection and analysis
Our searches retrieved 159 references six of which were to ongoing trials Based on assessment of the title or abstract or both we
excluded all of the studies with the exception of one which was evaluated following examination of the full text report However this
study also did not meet our inclusion criteria and was subsequently excluded
1Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
No randomised controlled trials met our inclusion criteria
Authorsrsquo conclusions
There is currently no high level evidence to support or refute the efficacy or safety of percutaneous transluminal angioplasty for treatment
of CCSVI in people with MS Clinical practice should be guided by evidence supported by well-designed randomised controlled trials
closure of some of the gaps in the evidence may be feasible at the time of completion of the six ongoing clinical trials
P L A I N L A N G U A G E S U M M A R Y
The more popularly known rsquoLiberation procedurersquo for treatment of venous stenoses (CCSVI) in the brain of MS sufferers
Multiple sclerosis (MS) is an inflammatory disease of the nervous system and the most frequent cause of neurological disability in
young adults Myelin the material that wraps around and protects the nerves becomes damaged and this results in scarring and the
formation of scar-like plaques
MS is considered to be an immune-mediated disease in which the personrsquos own immune system attacks the nervous system and most
of the current drug therapies are based on this hypothesis
However a new theory has been recently proposed with a suggestion that impaired blood flow in the veins draining the central nervous
system so called chronic cerebrospinal venous insufficiency (CCSVI) may play a role in the cause of MS CCSVI is thought to be
congenital and it may result in iron deposits which in turn trigger the immune system to attack the central nervous system thus
damaging the myelin The proposed treatment for CCSVI is balloon angioplasty which entails the widening of narrowed (stenosed)
veins the commonly named rsquoliberation procedurersquo This theory has gained a lot of attention via the Internet mainly among the patientsrsquo
community and the increased interest by the media has further enhanced the expectations of people suffering with MS We searched
the relevant literature but found no studies that matched the criteria of methodological quality necessary for their inclusion in this
review
There is currently no evidence to support or refute the efficacy and the safety of angioplasty for CCSVI in people with MS Well-
designed and robust studies are warranted
B A C K G R O U N D
Unfamiliar terms are listed in the rsquoGlossary of termsrsquo in Table 1
Description of the condition
Definition signs and symptoms
Multiple sclerosis (MS) is a leading cause of neurological disability
in young adults The disease is characterised by demyelination ax-
onal loss and inflammation (Compston 2008) Four clinical forms
of MS can be distinguished relapsing-remitting (RRMS) sec-
ondary progressive (SPMS) primary progressive (PPMS) and pro-
gressive relapsing (PRMS) MS (Lublin 1996) RRMS and SPMS
are the clinical forms of MS that account for approximately 80
to 85 of sufferers and SPMS evolves from the RRMS form
(Lublin 1996)
MS is heterogeneous both histopathologically and clinically
(Lucchinetti 1996) and the natural history can be difficult to
predict In most cases it begins as RRMS with episodic largely
reversible neurological dysfunction (Nessler 2010) Natural his-
tory studies have shown that after a period of approximately
10 years almost 50 of people with MS gradually develop per-
manent disability (ie SPMS) which may also include acute re-
lapses (Weinshenker 1989) After a median of 15 to 28 years
(Tremlett 2006 Weinshenker 1989) from disease onset a disabil-
ity milestone equivalent to the use of an assistive walking device is
reached Whether current disease-modifying drugs (DMDs) alter
these prognostics is unknown Clinical features include all of the
symptoms caused by the impairment of the central nervous system
2Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(CNS) (eg loss of vision double vision muscle weakness sen-
sory disturbances bladder dysfunction impotence constipation
ataxia vertigo tremor spasticity pain cognitive impairment and
dysarthria) fatigue anxiety and depression are also frequent oc-
currences (Compston 2008) Magnetic resonance imaging (MRI)
can support the clinical diagnosis and it is integrated with clinical
and other para-clinical diagnostic methods (eg examining cere-
brospinal fluid and evoked potentials) to facilitate the diagnosis
of MS (Polman 2011) MRI parameters are also used as surrogate
markers of disease activity and progression
The disease has an adverse impact on the health-related quality of
life (HRQoL) of people with MS and their families and may also
pose a financial burden even when the disease is not physically
disabling
Epidemiology and causes
The most widely accepted hypothesis on the pathogenesis of
MS is that it is an immune-mediated disease characterised by
lymphocytic infiltration leading to damage of myelin and axons
(Compston 2008)
Although the aetiology is largely indeterminate a large propor-
tion of the scientific community considers that MS develops in
genetically predisposed subjects and that environmental factors
play a central role in its pathogenesis based on immune-mediated
mechanisms It is thought that aberrant immune responses to self
or foreign antigens cause and perpetuate inflammation (Frohman
2006) The inflammation leads to demyelination and subsequent
axonal damage However the role of inflammation is considered
to be complex and may include both beneficial and detrimen-
tal effects (Martino 2002) Some researchers also consider that
a cryptic aetiological agent may be the primary cause of axonal
damage and demyelination as well as inducing an inflammatory
response that could play a secondary role (Barnett 2006 Maggs
2004 Trapp 1998)
The age of onset of MS is usually between 20 and 40 years
(Ascherio 2007) Incidence is low in childhood and is rarer at the
age of 50 years or older Female to male ratios vary between 151
and 251 in most populations but this ratio has increased over the
last decade (up to 2011) (Sellner 2011) The incidence and preva-
lence of MS varies geographically (Ebers 2008 Simpson 2011)
High-frequency areas (prevalence in excess of 60 per 100000 peo-
ple) include all of Europe in addition to southern Canada north-
ern US New Zealand and south-east Australia In many of these
areas the prevalence is more than 100 per 100000 people This
geographic variance may be explained in part by racial differences
white populations especially those from northern Europe appear
to be most susceptible People of Asian African or American In-
dian origin have the lowest risk with other groups intermediate
MS is most likely to be caused by a complex interaction between
polygenetic and environmental factors (Hohlfeld 2011) The ma-
jor histocompatibility complex confers the greatest genetic risk
on susceptibility to MS Recent work has highlighted the impor-
tance of both HLA-DR and HLA-DQ in determining risk (Burrell
2011) There is also a widely held belief of an association between
geographical latitude and MS with the risk of MS increasing from
south to north Exceptions to the gradient are likely to be as a
result of genetic and behavioural-cultural variations (Ebers 2008
Simpson 2011) Geographical latitude and sunshine exposure and
the resulting increase in vitamin D levels which are closely related
are major environmental factors associated with the risk of devel-
oping MS (Burrell 2011 Comabella 2012 Simpson 2011) The
involvement of UV light in the production of vitamin D has gen-
erated a perception that vitamin D is itself the latitudinal factor
that influences the risk of developing MS Direct support for this
comes from a prospective study showing that low serum 25-hy-
droxyvitamin D (25-OH-D) (the circulating form of vitamin D)
levels are associated with an increased risk of MS (Munger 2006)
Other factors that have been suggested include exposure to Ep-
stein Barr virus with an almost 100 prevalence in MS patients
and tobacco smoking (Burrell 2011 Ebers 2008)
A more recent hypothesis suggests that chronic venous congestion
may be an important factor in the pathogenesis of MS (Zamboni
2006 Zamboni 2009a Zamboni 2010 Zamboni 2011a) The
predominantly venotopic location of MS lesions in the CNS is
postulated to be a consequence of local erythrocyte extravasation
owing to elevated transmural venous pressure (rsquovenous conges-
tionrsquo ie analogous to lower-limb chronic venous insufficiency)
followed by erythrocyte degradation and iron-driven phagocytosis
and subsequent lymphocytic infiltration (Singh 2009) This con-
cept has been named rsquochronic cerebrospinal venous insufficiencyrsquo
(CCSVI) and is characterised by stenoses of the internal jugular
veins azygos veins or both which restrict the normal blood flow
from the brain along with the appearance of small collateral veins
that may have developed to reduce the impact of the stenoses
(Zamboni 2009a) In his initial study Zamboni found CCSVI
in all subjects in the study group that were diagnosed with MS
and none in the healthy controls (Zamboni 2009a) Zambonirsquos
research group maintained that CCSVI can be non-invasively and
reliably diagnosed through the use of combined transcranial and
extracranial echo colour Doppler (ECD) by individuals trained to
recognise the indicators of CCSVI (Menegatti 2008 Menegatti
2011 Zivadinov 2011b)
ECD is used to measure five variables
1 reflux in the internal jugular veins (IJVs) or in the vertebral
veins (VVs) or both with the head in any position
2 reflux in the deep cerebral veins
3 high-resolution B-mode evidence of IJV stenoses
4 flow not detected by Doppler in the IJVs or VVs or both
5 reverted postural control of the main cerebral venous outflow
pathways
The diagnosis of CCSVI needs to fulfil at least two of these five
ECD indicators (Zamboni 2009a)
There has been some criticism of several of the limitations in the
3Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

[Intervention Review]
Percutaneous transluminal angioplasty for treatment ofchronic cerebrospinal venous insufficiency (CCSVI) inmultiple sclerosis patients
Esther J van Zuuren1 Zbys Fedorowicz2 Eugenio Pucci3 Vanitha A Jagannath4 Edward W Robak5
1MS Consumer Oegstgeest Netherlands 2UKCC (Bahrain Branch) The Cochrane Collaboration Awali Bahrain 3UO Neurologia
- Ospedale di Macerata ASUR Marche - Zona Territoriale 9 Macerata Italy 4Department of Paediatrics American Mission Hospital
Manama Bahrain 5MS Consumer Fredericton Canada
Contact address Esther J van Zuuren MS Consumer Oegstgeest Netherlands EJvan_Zuurenlumcnl
Editorial group Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous System Group
Publication status and date New published in Issue 12 2012
Review content assessed as up-to-date 3 April 2012
Citation van Zuuren EJ Fedorowicz Z Pucci E Jagannath VA Robak EW Percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients Cochrane Database of Systematic Reviews 2012 Issue
12 Art No CD009903 DOI 10100214651858CD009903pub2
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
A B S T R A C T
Background
Multiple sclerosis (MS) is a leading cause of neurological disability in young adults The most widely accepted hypothesis regarding its
pathogenesis is that it is an immune-mediated disease It has been hypothesised more recently that chronic venous congestion may be
an important factor in the pathogenesis of MS This concept has been named rsquochronic cerebrospinal venous insufficiencyrsquo (CCSVI) and
is characterised by stenoses of either the internal jugular or azygos veins or both It is suggested that these stenoses restrict the normal
blood flow from the brain causing the deposition of iron in the brain and the eventual triggering of an auto-immune response The
proposed treatment for CCSVI is percutaneous transluminal angioplasty also known as the rsquoliberation procedurersquo which is claimed to
improve the blood flow in the brain thereby alleviating some of the symptoms of MS
Objectives
To assess the effects of percutaneous transluminal angioplasty for the treatment of CCSVI in people with MS
Search methods
We searched the following databases up to June 2012 The Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous
System Group Specialised Register CENTRAL in The Cochrane Library 2012 Issue 5 MEDLINE (from 1946) EMBASE (from
1974) and reference lists of articles We also searched several online trials registries for ongoing trials
Selection criteria
Randomised controlled trials assessing the effects of percutaneous transluminal angioplasty in adults with multiple sclerosis that have
been diagnosed to have CCSVI
Data collection and analysis
Our searches retrieved 159 references six of which were to ongoing trials Based on assessment of the title or abstract or both we
excluded all of the studies with the exception of one which was evaluated following examination of the full text report However this
study also did not meet our inclusion criteria and was subsequently excluded
1Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Main results
No randomised controlled trials met our inclusion criteria
Authorsrsquo conclusions
There is currently no high level evidence to support or refute the efficacy or safety of percutaneous transluminal angioplasty for treatment
of CCSVI in people with MS Clinical practice should be guided by evidence supported by well-designed randomised controlled trials
closure of some of the gaps in the evidence may be feasible at the time of completion of the six ongoing clinical trials
P L A I N L A N G U A G E S U M M A R Y
The more popularly known rsquoLiberation procedurersquo for treatment of venous stenoses (CCSVI) in the brain of MS sufferers
Multiple sclerosis (MS) is an inflammatory disease of the nervous system and the most frequent cause of neurological disability in
young adults Myelin the material that wraps around and protects the nerves becomes damaged and this results in scarring and the
formation of scar-like plaques
MS is considered to be an immune-mediated disease in which the personrsquos own immune system attacks the nervous system and most
of the current drug therapies are based on this hypothesis
However a new theory has been recently proposed with a suggestion that impaired blood flow in the veins draining the central nervous
system so called chronic cerebrospinal venous insufficiency (CCSVI) may play a role in the cause of MS CCSVI is thought to be
congenital and it may result in iron deposits which in turn trigger the immune system to attack the central nervous system thus
damaging the myelin The proposed treatment for CCSVI is balloon angioplasty which entails the widening of narrowed (stenosed)
veins the commonly named rsquoliberation procedurersquo This theory has gained a lot of attention via the Internet mainly among the patientsrsquo
community and the increased interest by the media has further enhanced the expectations of people suffering with MS We searched
the relevant literature but found no studies that matched the criteria of methodological quality necessary for their inclusion in this
review
There is currently no evidence to support or refute the efficacy and the safety of angioplasty for CCSVI in people with MS Well-
designed and robust studies are warranted
B A C K G R O U N D
Unfamiliar terms are listed in the rsquoGlossary of termsrsquo in Table 1
Description of the condition
Definition signs and symptoms
Multiple sclerosis (MS) is a leading cause of neurological disability
in young adults The disease is characterised by demyelination ax-
onal loss and inflammation (Compston 2008) Four clinical forms
of MS can be distinguished relapsing-remitting (RRMS) sec-
ondary progressive (SPMS) primary progressive (PPMS) and pro-
gressive relapsing (PRMS) MS (Lublin 1996) RRMS and SPMS
are the clinical forms of MS that account for approximately 80
to 85 of sufferers and SPMS evolves from the RRMS form
(Lublin 1996)
MS is heterogeneous both histopathologically and clinically
(Lucchinetti 1996) and the natural history can be difficult to
predict In most cases it begins as RRMS with episodic largely
reversible neurological dysfunction (Nessler 2010) Natural his-
tory studies have shown that after a period of approximately
10 years almost 50 of people with MS gradually develop per-
manent disability (ie SPMS) which may also include acute re-
lapses (Weinshenker 1989) After a median of 15 to 28 years
(Tremlett 2006 Weinshenker 1989) from disease onset a disabil-
ity milestone equivalent to the use of an assistive walking device is
reached Whether current disease-modifying drugs (DMDs) alter
these prognostics is unknown Clinical features include all of the
symptoms caused by the impairment of the central nervous system
2Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(CNS) (eg loss of vision double vision muscle weakness sen-
sory disturbances bladder dysfunction impotence constipation
ataxia vertigo tremor spasticity pain cognitive impairment and
dysarthria) fatigue anxiety and depression are also frequent oc-
currences (Compston 2008) Magnetic resonance imaging (MRI)
can support the clinical diagnosis and it is integrated with clinical
and other para-clinical diagnostic methods (eg examining cere-
brospinal fluid and evoked potentials) to facilitate the diagnosis
of MS (Polman 2011) MRI parameters are also used as surrogate
markers of disease activity and progression
The disease has an adverse impact on the health-related quality of
life (HRQoL) of people with MS and their families and may also
pose a financial burden even when the disease is not physically
disabling
Epidemiology and causes
The most widely accepted hypothesis on the pathogenesis of
MS is that it is an immune-mediated disease characterised by
lymphocytic infiltration leading to damage of myelin and axons
(Compston 2008)
Although the aetiology is largely indeterminate a large propor-
tion of the scientific community considers that MS develops in
genetically predisposed subjects and that environmental factors
play a central role in its pathogenesis based on immune-mediated
mechanisms It is thought that aberrant immune responses to self
or foreign antigens cause and perpetuate inflammation (Frohman
2006) The inflammation leads to demyelination and subsequent
axonal damage However the role of inflammation is considered
to be complex and may include both beneficial and detrimen-
tal effects (Martino 2002) Some researchers also consider that
a cryptic aetiological agent may be the primary cause of axonal
damage and demyelination as well as inducing an inflammatory
response that could play a secondary role (Barnett 2006 Maggs
2004 Trapp 1998)
The age of onset of MS is usually between 20 and 40 years
(Ascherio 2007) Incidence is low in childhood and is rarer at the
age of 50 years or older Female to male ratios vary between 151
and 251 in most populations but this ratio has increased over the
last decade (up to 2011) (Sellner 2011) The incidence and preva-
lence of MS varies geographically (Ebers 2008 Simpson 2011)
High-frequency areas (prevalence in excess of 60 per 100000 peo-
ple) include all of Europe in addition to southern Canada north-
ern US New Zealand and south-east Australia In many of these
areas the prevalence is more than 100 per 100000 people This
geographic variance may be explained in part by racial differences
white populations especially those from northern Europe appear
to be most susceptible People of Asian African or American In-
dian origin have the lowest risk with other groups intermediate
MS is most likely to be caused by a complex interaction between
polygenetic and environmental factors (Hohlfeld 2011) The ma-
jor histocompatibility complex confers the greatest genetic risk
on susceptibility to MS Recent work has highlighted the impor-
tance of both HLA-DR and HLA-DQ in determining risk (Burrell
2011) There is also a widely held belief of an association between
geographical latitude and MS with the risk of MS increasing from
south to north Exceptions to the gradient are likely to be as a
result of genetic and behavioural-cultural variations (Ebers 2008
Simpson 2011) Geographical latitude and sunshine exposure and
the resulting increase in vitamin D levels which are closely related
are major environmental factors associated with the risk of devel-
oping MS (Burrell 2011 Comabella 2012 Simpson 2011) The
involvement of UV light in the production of vitamin D has gen-
erated a perception that vitamin D is itself the latitudinal factor
that influences the risk of developing MS Direct support for this
comes from a prospective study showing that low serum 25-hy-
droxyvitamin D (25-OH-D) (the circulating form of vitamin D)
levels are associated with an increased risk of MS (Munger 2006)
Other factors that have been suggested include exposure to Ep-
stein Barr virus with an almost 100 prevalence in MS patients
and tobacco smoking (Burrell 2011 Ebers 2008)
A more recent hypothesis suggests that chronic venous congestion
may be an important factor in the pathogenesis of MS (Zamboni
2006 Zamboni 2009a Zamboni 2010 Zamboni 2011a) The
predominantly venotopic location of MS lesions in the CNS is
postulated to be a consequence of local erythrocyte extravasation
owing to elevated transmural venous pressure (rsquovenous conges-
tionrsquo ie analogous to lower-limb chronic venous insufficiency)
followed by erythrocyte degradation and iron-driven phagocytosis
and subsequent lymphocytic infiltration (Singh 2009) This con-
cept has been named rsquochronic cerebrospinal venous insufficiencyrsquo
(CCSVI) and is characterised by stenoses of the internal jugular
veins azygos veins or both which restrict the normal blood flow
from the brain along with the appearance of small collateral veins
that may have developed to reduce the impact of the stenoses
(Zamboni 2009a) In his initial study Zamboni found CCSVI
in all subjects in the study group that were diagnosed with MS
and none in the healthy controls (Zamboni 2009a) Zambonirsquos
research group maintained that CCSVI can be non-invasively and
reliably diagnosed through the use of combined transcranial and
extracranial echo colour Doppler (ECD) by individuals trained to
recognise the indicators of CCSVI (Menegatti 2008 Menegatti
2011 Zivadinov 2011b)
ECD is used to measure five variables
1 reflux in the internal jugular veins (IJVs) or in the vertebral
veins (VVs) or both with the head in any position
2 reflux in the deep cerebral veins
3 high-resolution B-mode evidence of IJV stenoses
4 flow not detected by Doppler in the IJVs or VVs or both
5 reverted postural control of the main cerebral venous outflow
pathways
The diagnosis of CCSVI needs to fulfil at least two of these five
ECD indicators (Zamboni 2009a)
There has been some criticism of several of the limitations in the
3Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Main results
No randomised controlled trials met our inclusion criteria
Authorsrsquo conclusions
There is currently no high level evidence to support or refute the efficacy or safety of percutaneous transluminal angioplasty for treatment
of CCSVI in people with MS Clinical practice should be guided by evidence supported by well-designed randomised controlled trials
closure of some of the gaps in the evidence may be feasible at the time of completion of the six ongoing clinical trials
P L A I N L A N G U A G E S U M M A R Y
The more popularly known rsquoLiberation procedurersquo for treatment of venous stenoses (CCSVI) in the brain of MS sufferers
Multiple sclerosis (MS) is an inflammatory disease of the nervous system and the most frequent cause of neurological disability in
young adults Myelin the material that wraps around and protects the nerves becomes damaged and this results in scarring and the
formation of scar-like plaques
MS is considered to be an immune-mediated disease in which the personrsquos own immune system attacks the nervous system and most
of the current drug therapies are based on this hypothesis
However a new theory has been recently proposed with a suggestion that impaired blood flow in the veins draining the central nervous
system so called chronic cerebrospinal venous insufficiency (CCSVI) may play a role in the cause of MS CCSVI is thought to be
congenital and it may result in iron deposits which in turn trigger the immune system to attack the central nervous system thus
damaging the myelin The proposed treatment for CCSVI is balloon angioplasty which entails the widening of narrowed (stenosed)
veins the commonly named rsquoliberation procedurersquo This theory has gained a lot of attention via the Internet mainly among the patientsrsquo
community and the increased interest by the media has further enhanced the expectations of people suffering with MS We searched
the relevant literature but found no studies that matched the criteria of methodological quality necessary for their inclusion in this
review
There is currently no evidence to support or refute the efficacy and the safety of angioplasty for CCSVI in people with MS Well-
designed and robust studies are warranted
B A C K G R O U N D
Unfamiliar terms are listed in the rsquoGlossary of termsrsquo in Table 1
Description of the condition
Definition signs and symptoms
Multiple sclerosis (MS) is a leading cause of neurological disability
in young adults The disease is characterised by demyelination ax-
onal loss and inflammation (Compston 2008) Four clinical forms
of MS can be distinguished relapsing-remitting (RRMS) sec-
ondary progressive (SPMS) primary progressive (PPMS) and pro-
gressive relapsing (PRMS) MS (Lublin 1996) RRMS and SPMS
are the clinical forms of MS that account for approximately 80
to 85 of sufferers and SPMS evolves from the RRMS form
(Lublin 1996)
MS is heterogeneous both histopathologically and clinically
(Lucchinetti 1996) and the natural history can be difficult to
predict In most cases it begins as RRMS with episodic largely
reversible neurological dysfunction (Nessler 2010) Natural his-
tory studies have shown that after a period of approximately
10 years almost 50 of people with MS gradually develop per-
manent disability (ie SPMS) which may also include acute re-
lapses (Weinshenker 1989) After a median of 15 to 28 years
(Tremlett 2006 Weinshenker 1989) from disease onset a disabil-
ity milestone equivalent to the use of an assistive walking device is
reached Whether current disease-modifying drugs (DMDs) alter
these prognostics is unknown Clinical features include all of the
symptoms caused by the impairment of the central nervous system
2Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(CNS) (eg loss of vision double vision muscle weakness sen-
sory disturbances bladder dysfunction impotence constipation
ataxia vertigo tremor spasticity pain cognitive impairment and
dysarthria) fatigue anxiety and depression are also frequent oc-
currences (Compston 2008) Magnetic resonance imaging (MRI)
can support the clinical diagnosis and it is integrated with clinical
and other para-clinical diagnostic methods (eg examining cere-
brospinal fluid and evoked potentials) to facilitate the diagnosis
of MS (Polman 2011) MRI parameters are also used as surrogate
markers of disease activity and progression
The disease has an adverse impact on the health-related quality of
life (HRQoL) of people with MS and their families and may also
pose a financial burden even when the disease is not physically
disabling
Epidemiology and causes
The most widely accepted hypothesis on the pathogenesis of
MS is that it is an immune-mediated disease characterised by
lymphocytic infiltration leading to damage of myelin and axons
(Compston 2008)
Although the aetiology is largely indeterminate a large propor-
tion of the scientific community considers that MS develops in
genetically predisposed subjects and that environmental factors
play a central role in its pathogenesis based on immune-mediated
mechanisms It is thought that aberrant immune responses to self
or foreign antigens cause and perpetuate inflammation (Frohman
2006) The inflammation leads to demyelination and subsequent
axonal damage However the role of inflammation is considered
to be complex and may include both beneficial and detrimen-
tal effects (Martino 2002) Some researchers also consider that
a cryptic aetiological agent may be the primary cause of axonal
damage and demyelination as well as inducing an inflammatory
response that could play a secondary role (Barnett 2006 Maggs
2004 Trapp 1998)
The age of onset of MS is usually between 20 and 40 years
(Ascherio 2007) Incidence is low in childhood and is rarer at the
age of 50 years or older Female to male ratios vary between 151
and 251 in most populations but this ratio has increased over the
last decade (up to 2011) (Sellner 2011) The incidence and preva-
lence of MS varies geographically (Ebers 2008 Simpson 2011)
High-frequency areas (prevalence in excess of 60 per 100000 peo-
ple) include all of Europe in addition to southern Canada north-
ern US New Zealand and south-east Australia In many of these
areas the prevalence is more than 100 per 100000 people This
geographic variance may be explained in part by racial differences
white populations especially those from northern Europe appear
to be most susceptible People of Asian African or American In-
dian origin have the lowest risk with other groups intermediate
MS is most likely to be caused by a complex interaction between
polygenetic and environmental factors (Hohlfeld 2011) The ma-
jor histocompatibility complex confers the greatest genetic risk
on susceptibility to MS Recent work has highlighted the impor-
tance of both HLA-DR and HLA-DQ in determining risk (Burrell
2011) There is also a widely held belief of an association between
geographical latitude and MS with the risk of MS increasing from
south to north Exceptions to the gradient are likely to be as a
result of genetic and behavioural-cultural variations (Ebers 2008
Simpson 2011) Geographical latitude and sunshine exposure and
the resulting increase in vitamin D levels which are closely related
are major environmental factors associated with the risk of devel-
oping MS (Burrell 2011 Comabella 2012 Simpson 2011) The
involvement of UV light in the production of vitamin D has gen-
erated a perception that vitamin D is itself the latitudinal factor
that influences the risk of developing MS Direct support for this
comes from a prospective study showing that low serum 25-hy-
droxyvitamin D (25-OH-D) (the circulating form of vitamin D)
levels are associated with an increased risk of MS (Munger 2006)
Other factors that have been suggested include exposure to Ep-
stein Barr virus with an almost 100 prevalence in MS patients
and tobacco smoking (Burrell 2011 Ebers 2008)
A more recent hypothesis suggests that chronic venous congestion
may be an important factor in the pathogenesis of MS (Zamboni
2006 Zamboni 2009a Zamboni 2010 Zamboni 2011a) The
predominantly venotopic location of MS lesions in the CNS is
postulated to be a consequence of local erythrocyte extravasation
owing to elevated transmural venous pressure (rsquovenous conges-
tionrsquo ie analogous to lower-limb chronic venous insufficiency)
followed by erythrocyte degradation and iron-driven phagocytosis
and subsequent lymphocytic infiltration (Singh 2009) This con-
cept has been named rsquochronic cerebrospinal venous insufficiencyrsquo
(CCSVI) and is characterised by stenoses of the internal jugular
veins azygos veins or both which restrict the normal blood flow
from the brain along with the appearance of small collateral veins
that may have developed to reduce the impact of the stenoses
(Zamboni 2009a) In his initial study Zamboni found CCSVI
in all subjects in the study group that were diagnosed with MS
and none in the healthy controls (Zamboni 2009a) Zambonirsquos
research group maintained that CCSVI can be non-invasively and
reliably diagnosed through the use of combined transcranial and
extracranial echo colour Doppler (ECD) by individuals trained to
recognise the indicators of CCSVI (Menegatti 2008 Menegatti
2011 Zivadinov 2011b)
ECD is used to measure five variables
1 reflux in the internal jugular veins (IJVs) or in the vertebral
veins (VVs) or both with the head in any position
2 reflux in the deep cerebral veins
3 high-resolution B-mode evidence of IJV stenoses
4 flow not detected by Doppler in the IJVs or VVs or both
5 reverted postural control of the main cerebral venous outflow
pathways
The diagnosis of CCSVI needs to fulfil at least two of these five
ECD indicators (Zamboni 2009a)
There has been some criticism of several of the limitations in the
3Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

(CNS) (eg loss of vision double vision muscle weakness sen-
sory disturbances bladder dysfunction impotence constipation
ataxia vertigo tremor spasticity pain cognitive impairment and
dysarthria) fatigue anxiety and depression are also frequent oc-
currences (Compston 2008) Magnetic resonance imaging (MRI)
can support the clinical diagnosis and it is integrated with clinical
and other para-clinical diagnostic methods (eg examining cere-
brospinal fluid and evoked potentials) to facilitate the diagnosis
of MS (Polman 2011) MRI parameters are also used as surrogate
markers of disease activity and progression
The disease has an adverse impact on the health-related quality of
life (HRQoL) of people with MS and their families and may also
pose a financial burden even when the disease is not physically
disabling
Epidemiology and causes
The most widely accepted hypothesis on the pathogenesis of
MS is that it is an immune-mediated disease characterised by
lymphocytic infiltration leading to damage of myelin and axons
(Compston 2008)
Although the aetiology is largely indeterminate a large propor-
tion of the scientific community considers that MS develops in
genetically predisposed subjects and that environmental factors
play a central role in its pathogenesis based on immune-mediated
mechanisms It is thought that aberrant immune responses to self
or foreign antigens cause and perpetuate inflammation (Frohman
2006) The inflammation leads to demyelination and subsequent
axonal damage However the role of inflammation is considered
to be complex and may include both beneficial and detrimen-
tal effects (Martino 2002) Some researchers also consider that
a cryptic aetiological agent may be the primary cause of axonal
damage and demyelination as well as inducing an inflammatory
response that could play a secondary role (Barnett 2006 Maggs
2004 Trapp 1998)
The age of onset of MS is usually between 20 and 40 years
(Ascherio 2007) Incidence is low in childhood and is rarer at the
age of 50 years or older Female to male ratios vary between 151
and 251 in most populations but this ratio has increased over the
last decade (up to 2011) (Sellner 2011) The incidence and preva-
lence of MS varies geographically (Ebers 2008 Simpson 2011)
High-frequency areas (prevalence in excess of 60 per 100000 peo-
ple) include all of Europe in addition to southern Canada north-
ern US New Zealand and south-east Australia In many of these
areas the prevalence is more than 100 per 100000 people This
geographic variance may be explained in part by racial differences
white populations especially those from northern Europe appear
to be most susceptible People of Asian African or American In-
dian origin have the lowest risk with other groups intermediate
MS is most likely to be caused by a complex interaction between
polygenetic and environmental factors (Hohlfeld 2011) The ma-
jor histocompatibility complex confers the greatest genetic risk
on susceptibility to MS Recent work has highlighted the impor-
tance of both HLA-DR and HLA-DQ in determining risk (Burrell
2011) There is also a widely held belief of an association between
geographical latitude and MS with the risk of MS increasing from
south to north Exceptions to the gradient are likely to be as a
result of genetic and behavioural-cultural variations (Ebers 2008
Simpson 2011) Geographical latitude and sunshine exposure and
the resulting increase in vitamin D levels which are closely related
are major environmental factors associated with the risk of devel-
oping MS (Burrell 2011 Comabella 2012 Simpson 2011) The
involvement of UV light in the production of vitamin D has gen-
erated a perception that vitamin D is itself the latitudinal factor
that influences the risk of developing MS Direct support for this
comes from a prospective study showing that low serum 25-hy-
droxyvitamin D (25-OH-D) (the circulating form of vitamin D)
levels are associated with an increased risk of MS (Munger 2006)
Other factors that have been suggested include exposure to Ep-
stein Barr virus with an almost 100 prevalence in MS patients
and tobacco smoking (Burrell 2011 Ebers 2008)
A more recent hypothesis suggests that chronic venous congestion
may be an important factor in the pathogenesis of MS (Zamboni
2006 Zamboni 2009a Zamboni 2010 Zamboni 2011a) The
predominantly venotopic location of MS lesions in the CNS is
postulated to be a consequence of local erythrocyte extravasation
owing to elevated transmural venous pressure (rsquovenous conges-
tionrsquo ie analogous to lower-limb chronic venous insufficiency)
followed by erythrocyte degradation and iron-driven phagocytosis
and subsequent lymphocytic infiltration (Singh 2009) This con-
cept has been named rsquochronic cerebrospinal venous insufficiencyrsquo
(CCSVI) and is characterised by stenoses of the internal jugular
veins azygos veins or both which restrict the normal blood flow
from the brain along with the appearance of small collateral veins
that may have developed to reduce the impact of the stenoses
(Zamboni 2009a) In his initial study Zamboni found CCSVI
in all subjects in the study group that were diagnosed with MS
and none in the healthy controls (Zamboni 2009a) Zambonirsquos
research group maintained that CCSVI can be non-invasively and
reliably diagnosed through the use of combined transcranial and
extracranial echo colour Doppler (ECD) by individuals trained to
recognise the indicators of CCSVI (Menegatti 2008 Menegatti
2011 Zivadinov 2011b)
ECD is used to measure five variables
1 reflux in the internal jugular veins (IJVs) or in the vertebral
veins (VVs) or both with the head in any position
2 reflux in the deep cerebral veins
3 high-resolution B-mode evidence of IJV stenoses
4 flow not detected by Doppler in the IJVs or VVs or both
5 reverted postural control of the main cerebral venous outflow
pathways
The diagnosis of CCSVI needs to fulfil at least two of these five
ECD indicators (Zamboni 2009a)
There has been some criticism of several of the limitations in the
3Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

ultrasound-based investigation used to measure the rather com-
plex and dynamic (ie postural dependent) cerebrospinal venous
outflow These include the wide individual variability operator
dependence and intra- and inter-rater bias the difficulty of stan-
dardising values for diagnostic criteria and the necessity of venog-
raphy as a gold standard (Doepp 2010 Hojnacki 2010 Wattjes
2011 Zivadinov 2011b) A high degree of correlation between
CCSVI and MS was found in a number of studies (Al-Omari 2010
Bavera 2011 Hojnacki 2010 Simka 2010) but this has been con-
tested by other studies (Baracchini 2011 Centonze 2011 Doepp
2010 Krogias 2010 Marder 2011 Mayer 2011 Sundstroumlm 2010
Tsivgoulis 2011 Yamout 2010) More recently it has also been
suggested that CCSVI could be related to MS disability since the
higher frequency of CCSVI found in people with MS was associ-
ated with higher disability longer disease duration and progressive
forms (Patti 2012)
Several reviews have reported that the incidence of CCSVI varies in
people with MS ranging from 0 to 100 and from 0 to 23
in healthy controls (Ghezzi 2011 Zivadinov 2011b) One study of
499 people with MS found an increased prevalence of CCSVI but
with a modest sensitivity and specificity and suggestive of a less
likely primary causative role for CCSVI in the development of MS
(Zivadinov 2011a) A further study found no relationship between
CCSVI and HLA DRB11501 a genetic variation that has been
consistently linked to MS (Weinstock-Guttman 2011) Attempts
have been made to correlate CCSVI with specific symptoms of
MS in particular an association with fatigue (which often severely
affects people with MS) (Malagoni 2010)
The hypothesised association between CCSVI and MS implicates
CCSVI as a treatable cause of MS and hence it has formed the
basis for the so called rsquoliberation procedurersquo (Zamboni 2009c)
which is based on the technique of balloon angioplasty (Zamboni
2009b Zamboni 2011b) Venous stent placement has also been
used to treat CCSVI in people with MS but this treatment has
been associated with a small number of serious adverse events
(AEs) (Anon 2010 Burton 2011 Ludyga 2010 Petrov 2011)
These concerns were addressed by Zamboni and his group who
indicated that stents were not used in the rsquoliberation procedurersquo
that they perform (Giacobbi 2012 Multiple Sclerosis Society of
Canada 2012)
Much of the research on this topic has over recent years generated
a major interest and continuing debate in the scientific community
on the definition of CCSVI as a pathological entity the correlation
between CCSVI and MS the proposed etiopathogenetic mecha-
nisms and as a consequence on the utility of its treatment (Bagert
2011 Drsquohaeseleer 2011 Diaconu 2012 Dorne 2010 Fragoso
2011 Ghezzi 2011 Khan 2010 Lazzaro 2011 Reekers 2011 van
Rensburg 2010 Waschbisch 2011 Zivadinov 2011b)
Description of the intervention
Percutaneous transluminal angioplasty (PTA) involves the inser-
tion of a small catheter with a balloon attachment via the femoral
vein in the groin Initially a venogram is performed so that images
can be obtained to identify the narrowed sections of the veins The
catheter is then inserted and advanced into the right and left IJVs
as well as the azygos veins The balloon is inflated at the narrowed
section of the vein thereby increasing its diameter and improving
the flow of blood The procedure is performed with venographic
control
How the intervention might work
According to Zamboni by reducing the venous pressure the clin-
ical course of MS fatigue and quality of life (QoL) parame-
ters might improve (Malagoni 2010 Zamboni 2009b Zamboni
2009c)
Why it is important to do this review
The MS-CCSVI hypothesis has generated both enthusiasm and
skepticism among people with MS and the specialists who treat
them The rsquoliberation procedurersquo has attracted considerable atten-
tion among people with MS as well as the media and on the Inter-
net (Fragoso 2011 Mayer 2011 Vera 2012) Consumers have been
frequently exposed to media hyperbole with exaggerated claims
that have led to unrealistic expectations (Qiu 2010) As a con-
sequence CCSVI treatment has been offered to MS patients in
many countries mostly not at conventional MS centres or within
research trials in spite of the lack of confirmation of early evi-
dence from Zambonirsquos pivotal trials (Diaconu 2012 Senato della
Repubblica 2010)
Recognising the significant interest of this topic to people with MS
and notwithstanding the lack of consensus in the scientific com-
munity about the relationship between MS and CCSVI a system-
atic review is now needed to examine the potential benefits and
risks of this intervention This review also attempted to highlight
possible methodological issues in existing and proposed clinical
trials in order to provide an evidence-based review of the effect of
treating CCSVI in people with MS Our aim in this review was
to contribute in such a way that the expectations of people with
MS and the claims of efficacy made by clinicians are realistic and
stay within the boundaries of the evidence-based medicine (EBM)
paradigm
O B J E C T I V E S
To assess the effects of percutaneous transluminal angioplasty for
the treatment of CCSVI in people with MS
4Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) Trials were not excluded on
the basis of duration of follow-up
Types of participants
Participants of both genders gt 17 years with a diagnosis of
MS according to the original or the revised McDonald criteria
(McDonald 2001 Polman 2005 Polman 2011) and with diag-
nosis of CCSVI according to Zambonirsquos criteria (Zamboni 2009a)
or other relevant internationally recognised and validated criteria
Types of interventions
PTA alone or in combination with other MS treatments versus
no treatment sham treatment or other MS treatments PTA asso-
ciated with stenting was not considered in this review
Types of outcome measures
Primary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 The number of participants with at least one AE
bull serious AE according to (ICH Expert Working Group
1994)
bull any other AE reported during or after the PTA procedure
2 The number of participants who experienced progression on the
Expanded Disability Status Scale (EDSS) (Kurtzke 1983) Def-
initions of progression reported in the original studies were ac-
cepted However we tried to evaluate this outcome using the def-
inition of progression as a persistent worsening of at least 1 point
in EDSS recorded outside a relapse and confirmed by a follow-up
assessment at six months a persistent half-point increase was to
be adopted if baseline EDSS was 55 or worse
3 Patient reported outcomes (PROs) could include any of the
following if reported
bull change in quality of life (QoL) assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995) MSQLI
(Fischer 1999) MusiQoL (Simeoni 2008)) or generic
instrument (eg short form 36 (SF-36) (Rudick 2007))
bull mean change in well-being as measured with a visual
analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale (MFIS)
(Kos 2005) or other recognised and validated MS-fatigue scale
bull or any other PRO
Secondary outcomes
Assessments at 12 months 24 months and at the end of the sched-
uled follow-up period in the primary studies
1 Restenosis of target vessel primary and secondary patency
Primary patency is the interval following the initial angioplasty
procedure until a re-intervention is performed to preserve patency
Secondary patency is defined as the interval following the initial
angioplasty procedure until treatment of the vein is abandoned
due to an inability to treat the original lesion (Diehm 2007)
2 Mean change in cognitive functions assessment through vali-
dated battery in MS (ie Brief Repeatable Battery of Neuropsy-
chological Tests (BRBNT) (Rao 1991))
3 In the RRMS subgroup only the number of participants expe-
riencing at least one relapse We accepted definitions of relapse as
reported in the original studies
Search methods for identification of studies
Although there were no language restrictions on included studies
we did not retrieve any relevant non-English papers We will not
apply any language restrictions on any studies identified for future
updates of the review and will arrange to translate any studies not
in the English language
Electronic searches
We searched the following databases
bull the Cochrane Multiple Sclerosis and Rare Diseases of the
Central Nervous System Group Specialised Register (to June
2012) (Appendix 1)
bull the Cochrane Central Register of Controlled Trials
(CENTRAL) (The Cochrane Library 2012 Issue 5) (Appendix 2)
bull MEDLINE (PubMed) (1946 to June 2012) (Appendix 3)
bull EMBASE (embasecom) (1974 to June 2012) (Appendix 4)
Searching other resources
References from published studies
We examined the bibliography of one study (Zamboni 2012)
which although it was subsequently excluded did not provide any
further references to potentially eligible RCTs If any of the on-
going studies are included in future updates their bibliographical
references will be examined accordingly
5Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Ongoing trials registers
We searched the following ongoing trials registers
1 the metaRegister of Controlled Trials wwwcontrolled-
trialscom
2 the US National Institutes of Health Ongoing Trials
Register wwwclinicaltrialsgov
3 the Australian and New Zealand Clinical Trials Registry
wwwanzctrorgau
4 the World Health Organization International Clinical Trials
Registry platform wwwwhointtrialsearch
Correspondence
We contacted trial investigators to request missing data or to clarify
study details (see Table 2)
Data collection and analysis
Selection of studies
Three review authors (EvZ VJ and EP) independently assessed
the abstracts of studies resulting from the searches Based on as-
sessments of the titles and abstracts of the other references it was
clear that none of the studies were eligible for inclusion and they
were therefore excluded We obtained a full-text copy of the sin-
gle potentially eligible study (Zamboni 2012) The three review
authors then independently assessed this study resolved any dis-
agreements through discussion and consensus and subsequently
excluded it
Table of methods archived for use in future updates
Issue Method
Data extraction and management Details of eligible trials will be extracted and summarised using structured
data extraction forms by two review authors (EvZ and ZF) Disagreements
will be resolved by discussion The data will be checked for consistency
by the same two review authors Study details will be entered into the
rsquoCharacteristics of included studiesrsquo table in RevMan (RevMan 2011)
The review authors will only include data if there will be an independently
reached consensus and any disagreements will be resolved by discussion
between the review authors
The following details will be extracted
1 trial methods - method of allocation masking of participants and
outcomes assessors and date and setting of study
2 participants - sample size age sex inclusion and exclusion criteria
exclusion of participants after randomisation and proportion of losses at
follow-up
3 intervention and comparison - length of study type and treatment
details
4 outcomes - primary and secondary outcomes reported in the study
5 notes - if our primary outcomes were addressed and other
comments
Assessment of risk of bias in included studies The review authors (EvZ and ZF) will independently assess the risk of
bias using The Cochrane Collaboration tool for assessing risk of bias
as described in Chapter 8 Section 85 in the Cochrane Handbook forSystematic Reviews of Interventions (Higgins 2011) The following domains
will be rated separately for any included study as rsquolow risk of biasrsquo rsquohigh
risk of biasrsquo and rsquounclearrsquo if the risk of bias was uncertain or unknown
1 sequence generation
2 allocation concealment
3 blinding of participants personnel
4 blinding of outcomes assessment
5 incomplete outcome data
6Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

(Continued)
6 selective outcome reporting
7 other bias
These assessments will be reported in the rsquoRisk of biasrsquo table for each
included study
To summarise risk of bias of the included studies for future included
studies we will consider the domains of sequence generation allocation
concealment blinding of outcome assessors and incomplete outcome data
in order to classify the studies into three classes As rsquolow risk of biasrsquo when
all of these criteria will be met rsquohigh risk of biasrsquo when at least one of them
will be unmet and rsquounclear risk of biasrsquo in the remainder
Measures of treatment effect We will present continuous outcomes where possible on the original scale
as reported in each individual study If similar outcomes are reported
using different scales these will be standardised by dividing the estimated
coefficient by its standard deviation (SD) thereby allowing comparisons
to be made between scales
Dichotomous outcomes data will be presented as risk ratios (RR) All
outcomes data will be reported with their associated 95 confidence
intervals and will be analysed in RevMan using the Mantel Haenzel test
unless stated otherwise
Unit of analysis issues The outcomes sought in this review will require studies of long dura-
tion with repeated observations on participants for several time periods
of follow-up and are therefore likely to present unit of analysis issues
Outcomes data will be grouped according to the clinically important time
points specified in the rsquoTypes of outcome measuresrsquo section of the review
and we will follow the recommendations on their analysis and reporting
provided in Section 934 of the Cochrane Handbook for Systematic Reviewsof Interventions (Higgins 2011)
Dealing with missing data We will try to contact the investigators of any included studies to obtain
missing or inadequately reported data If data are unavailable we will
follow the advice provided in Section 1612 of the Cochrane Handbookfor Systematic Reviews of Interventions (Higgins 2011) This may include
sensitivity analyses in which we will impute missing data and compare the
results for the best-worst case scenario with the worst-best case scenario
for the key primary outcomes
Assessment of heterogeneity We will assess clinical heterogeneity by examining the characteristics of the
studies the similarity between the types of participants the interventions
and the outcomes as specified in the criteria for included studies Statistical
heterogeneity will be assessed using a Chi2 test and the I2 statistic We will
report heterogeneity as important if it was at least moderate to substantial
with an I2 statistic gt 50 (Higgins 2011)
Assessment of reporting bias If a sufficient number of trials assessing similar effects are identified for
inclusion in this review publication bias will be assessed according to the
recommendations on testing for funnel plot asymmetry (Egger 1997) as
described in Section 10431 of the Cochrane Handbook for Systematic
7Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

(Continued)
Reviews of Interventions (Higgins 2011) If asymmetry is identified we
will try to assess other possible causes and these will be explored in the
discussion if appropriate
Data synthesis Two review authors (EvZ and ZF) will analyse the data in RevMan (
RevMan 2011) and will report them as specified in Chapter 9 of the
Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)
Data synthesis will only carried out if we are able to identify a sufficient
number of studies (N ge three) investigating similar treatments and which
have reported data that could be pooled (Treadwell 2006) We will use
a fixed-effect model to combine the results of individual studies and if
heterogeneity is identified random-effects models will be fitted
Subgroup analysis and investigation of heterogeneity We will only conduct subgroup analyses if a sufficient number of studies
(gt 10) with moderate-to-substantial heterogeneity (as defined above) are
included Although we did not identify a sufficient number of studies
at this time in future updates it will be of clinical relevance to consider
carrying out a subgroup analysis based on the different subtypes of MS
the duration and the baseline EDSS level
Sensitivity analysis If a sufficient number of studies are included in future updates we plan to
conduct sensitivity analyses to assess the robustness of our review results
by repeating the analysis with the following adjustments exclusion of
studies with unclear sequence generation unclear or inadequate allocation
concealment unclear or inadequate blinding of outcomes assessment and
completeness of follow-up
R E S U L T S
Description of studies
See Characteristics of excluded studies Characteristics of ongoing
studies
Results of the search
The electronic searches retrieved 159 references to studies which
included six ongoing clinical trials (see the rsquoCharacteristics of
ongoing studiesrsquo section) After examination of the titles and ab-
stracts four duplicate references were removed and a further 148
references were also subsequently excluded from the review A
full-text copy of the one remaining study (Zamboni 2012) was
obtained assessed independently for eligibility by three authors
(EvZ EP and VJ) and only excluded after consensus was reached
For further details see the rsquoStudy Flow Diagramrsquo (Figure 1)
8Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Figure 1 Flow diagram
9Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Included studies
No studies were included
Excluded studies
One study was excluded after evaluation of a full text copy of the
report (Zamboni 2012) (see Characteristics of excluded studies)
Risk of bias in included studies
No studies were included
Effects of interventions
No randomised controlled trials were found that fulfilled the in-
clusion criteria
D I S C U S S I O N
Summary of main results
Unfortunately at present no randomised controlled trials could
be included in this review (see Table 3) We identified one poten-
tially eligible study but after extensive discussion and consultation
with the other review authors and methodology experts this study
was excluded (Zamboni 2012) The investigators indicated that
in conducting this study they had attempted to address some of
the methodological concerns which had been raised (Khan 2010)
about their earlier study (Zamboni 2009b) ie the lack of a con-
trol group and blinded and objective measurement of MRI How-
ever our own assessments of the risk of bias in their recent study
called into question the methods used to generate the allocation
sequence which were not truly random and largely due to a lack
of clarity in the report we raised concerns as to whether any of
the outcomes assessments were blinded Our attempts to clarify
some of these trial conduct details with the principal investigator
proved unsuccessful
Overall completeness and applicability ofevidence
Several ongoing studies were identified that may eventually help
to fill in some of the gaps in the evidence for the efficacy and safety
of PTA for CCSVI (see the rsquoCharacteristics of ongoing studiesrsquo
section) In view of the lack of evidence there is a pressing need for
well designed randomised controlled trials which can help inform
and guide clinical practice
Quality of the evidence
There is currently no high level evidence to support or refute
the efficacy and safety of PTA for the treatment of CCSVI in
participants with multiple sclerosis
Potential biases in the review process
We made every attempt to limit bias in the review process by
ensuring a comprehensive search for potentially eligible studies
The authorsrsquo independent assessments of eligibility of studies for
inclusion in this review minimised the potential for additional
bias
Agreements and disagreements with otherstudies or reviews
In view of the lack of studies included in this review we are in broad
agreement with the relevant NICE guidance (NICE 2012) that
ldquocurrent evidence on the efficacy of percutaneous venoplasty for
chronic cerebrospinal venous insufficiency (CCSVI) for multiple
sclerosis (MS) is inadequate in quality and quantityrdquo Concurrent
with our implications for research the guidance also recommends
further randomised controlled trials but that these studies should
ldquoclearly define selection criteria and patient characteristicsrdquo as well
as ldquotechnical success which may include measurement of pressure
gradients across treated vein segments before and after venoplasty
Outcomes should include clinical and quality of life measuresrdquo
The findings of a recent systematic review and meta-analysis re-
ported a positive association between CCSVI and MS but also
concluded that poor reporting of the success of blinding and
marked heterogeneity among the included studies precluded any
definitive conclusions (Laupacis 2011) Although this meta-anal-
ysis did not specifically address the effect of percutaneous trans-
luminal angioplasty on CCSVI it does nevertheless help improve
our understanding of a possible association if not causal relation-
ship between CCSVI and MS
The objectives of a further review were to ldquocritically analyse the
scientific basis of CCSVI and the current literature on the rela-
tionship between CCSVI and MS as well as the methodology
of the ultrasound that has been claimed to provide evidence of
impaired cerebral venous drainagerdquo (Baracchini 2012) This was
a classical literature review which although it did not provide
10Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

any evidence that a systematic and complete search of the rele-
vant research had been conducted did nevertheless provide a valu-
able and comprehensive background to the theory surrounding
CCSVI the related diagnostic criteria and the proposed therapy
However in concluding that ldquono piece of the CCSVI puzzle has a
solid supportive scientific evidencerdquo the authors failed to provide
any indication of how studies on which their conclusions appear
to have been based were selected critically evaluated and could
be designated as reliable sources of evidence either for or in their
opinion against the efficacy of the rsquoliberationrsquo procedure or in-
deed were capable of rejecting the CCSVI hypothesis The con-
clusions of their literature review on the CCSVI hypothesis would
also appear to be at some divergence with the systematic review
(Laupacis 2011) which reported evidence of a ldquostrong associationrdquo
between CCSVI and MS Futhermore their caution against any
further ldquocontrolled liberation trials until solid scientific evidence
of a causal relationship between CCSVI and MS has been clearly
demonstratedrdquo would appear to countermand the recommenda-
tions of the systematic review as indeed the recommendations of
our review See rsquoImplications for researchrsquo
A U T H O R S rsquo C O N C L U S I O N S
Implications for practice
There is currently no high level evidence to support or refute
the use of percutaneous transluminal angioplasty for treatment of
chronic cerebrospinal venous insufficiency in people with MS As
MS is a chronic and distressing disease accompanied by increasing
disability and with a huge impact on quality of life the importance
of assessing the efficacy and safety of this intervention should not
be underestimated
The FDA has recently alerted health care professionals and patients
about injuries and death associated with the use of an experimental
procedure called rsquoliberation therapyrsquo in addition to the ldquopotential
dangers of unproven treatment for multiple sclerosisrdquo (FDA news
release 2012) There is a degree of urgency in trying to resolve these
uncertainties which is compounded by the high expectations of
people suffering with MS who are looking for some improvement
in their condition and who might choose to undergo PTA based
on the results of testing for CCSVI (Qiu 2010)
Implications for research
A review of percutaneous transluminal angioplasty for treatment of
CCSVI in people with MS provides an example of the implications
for research when no eligible studies had been found This review
highlights the need for randomised controlled trials to evaluate
the effects of this intervention and which can ultimately provide
reliable evidence to help inform clinical decision making
Any future randomised controlled trials must be well-designed
well-conducted and adequately delivered with subsequent report-
ing including high-quality descriptions of all aspects of methodol-
ogy Reporting should conform to the Consolidated Standards of
Reporting Trials (CONSORT) statement (httpwwwconsort-
statementorg) which will enable appraisal and interpretation of
results and accurate judgements to be made about the risk of bias
and the overall quality of the evidence
Although it is uncertain whether reported quality mirrors actual
study conduct it is noteworthy that studies with unclear method-
ology have been shown to produce biased estimates of treatment
effects (Schulz 1995)
Further small and methodologically unsound studies should be
discouraged as they can be considered unethical and only add
further to the existing confusion about the pros and cons of CCSVI
and the effects of ldquoliberation therapyrdquo in MS
For further research recommendations based on the EPICOT
(evidence population intervention comparison outcomes and
time) format (Brown 2006) see Table 4
A C K N O W L E D G E M E N T S
The review authors would like to thank the Cochrane Multiple
Sclerosis and Rare Diseases of the Central Nervous
System Group and the peer reviewers and referees for their help
in developing this review
11Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

R E F E R E N C E S
References to studies excluded from this review
Zamboni 2012 published data only
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients
with multiple sclerosis results of a pilot study Journal of
Vascular Surgery 201243(1)116ndash22 [PUBMED PMID
21839654]
References to ongoing studies
ACTRN12612000302853 published and unpublished data
ACTRN12612000302853 A randomised blinded
controlled study of percutaneous transluminal angioplasty
(PTA) for extracranial vein stenoses in patients with multiple
sclerosis (MS) wwwanzctrorgau
NCT01089686 unpublished data only
NCT01089686 Study to evaluate treating chronic
cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis patients wwwclinicaltrialsgov
NCT01201707 unpublished data only
NCT01201707 Evaluation of angioplasty in the treatment
of chronic cerebrospinal venous insufficiency (CCSVI) in
multiple sclerosis wwwclinicaltrialsgov
NCT01371760 unpublished data only
NCT01371760 BRAVE-DREAMS (BRAin VEnous
DRainage Exploited Against Multiple Sclerosis)
wwwclinicaltrialsgov
NCT01450072 unpublished data only
NCT01450072 Prospective randomized endovascular
therapy in multiple sclerosis - PREMiSE
wwwclinicaltrialsgov
NCT01555684 unpublished data only
NCT01555684 Functional changes following
percutaneous venoplasty in multiple sclerosis patients
wwwclinicaltrialsgov
Additional references
Al-Omari 2010
Al-Omari MH Rousan LA Internal jugular vein
morphology and hemodynamics in patients with multiple
sclerosis International Angiology 201029(2)115ndash20
[PUBMED PMID 20351667]
Anon 2010
Anon Experimental multiple sclerosis vascular shunting
procedure halted at Stanford Annals of Neurology 201067
(1)A13ndash5 [PUBMED PMID 20186848]
Ascherio 2007
Ascherio A Munger KL Environmental risk factors for
multiple sclerosis Part I the role of infection Annalsof Neurology 200761(4)288ndash99 [PUBMED PMID
17444504]
Bagert 2011
Bagert BA Marder E Stuumlve O Chronic cerebrospinal
venous insufficiency and multiple sclerosis Archives ofNeurology 201168(11)1379ndash84 [PUBMED PMID
21747006]
Baracchini 2011
Baracchini C Perini P Calabrese M Causin F Rinaldi
F Gallo P No evidence of chronic cerebrospinal venous
insufficiency at multiple sclerosis onset Annals of Neurology201169(1)90ndash9 [PUBMED PMID 21280079]
Baracchini 2012
Baracchini C Atzori M Gallo P CCSVI and MS no
meaning no fact Neurological Sciences 2012May 9Epub
ahead of print [PUBMED PMID 22569567]
Barnett 2006
Barnett MH Sutton I The pathology of multiple sclerosis
a paradigm shift Current Opinion in Neurology 200619(3)
242ndash7 [PUBMED PMID 16702829]
Bavera 2011
Bavera PM Mendozzi L Cavarretta R Agus GB Venous
extracranial Duplex ultrasound and possible correlations
between multiple sclerosis and CCSVI an observational
study after 560 exams Acta Phlebologica 201112(2)
109ndash13
Brown 2006
Brown P Brunnhuber K Chalkidou K Chalmers I Clarke
M Fenton M et alHow to formulate research questions
BMJ 2006333(7572)804ndash6
Burrell 2011
Burrell AM Handel AE Ramagopalan SV Ebers GC
Morahan JM 1 Epigenetic mechanisms in multiple
sclerosis and the major histocompatibility complex (MHC)
Discovery Medicine 201111(58)187ndash96 [PUBMED
PMID 21447278]
Burton 2011
Burton JM Alikhani K Goyal M Costello F White C
Patry D et alComplications in MS patients after CCSVI
procedures abroad (Calgary AB) Canadian Journal ofNeurological Sciences 201138(5)741ndash6 [PUBMED
PMID 21856578]
Centonze 2011
Centonze D Floris R Stefanini M Rossi S Fabiano S
Castelli M et alProposed chronic cerebrospinal venous
insufficiency criteria do not predict multiple sclerosis risk or
severity Annals of Neurology 201170(1)51ndash8 [PUBMED
PMID 21786298]
Comabella 2012
Comabella M Khoury SJ Immunopathogenesis of multiple
sclerosis Clinical Immunology 2012 Vol 142 issue 1
2ndash8 [PUBMED PMID 21458377]
Compston 2008
Compston A Coles A Multiple sclerosis Lancet 2008372
(9648)1502ndash17 [PUBMED PMID 18970977]
12Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Drsquohaeseleer 2011
Drsquohaeseleer M Cambron M Vanopdenbosch L De Keyser
J Vascular aspects of multiple sclerosis Lancet Neurology
201110(7)657-66 [PUBMED PMID 21683931]
Diaconu 2012
Diaconu CI Conway D Fox RJ Rae-Grant A Chronic
cerebrospinal venous insufficiency as a cause of multiple
sclerosis controversy and reality Current TreatmentOptions in Cardiovascular Medicine 201214(2)203ndash14
[PUBMED PMID 22311713]
Diehm 2007
Diehm N Baumgartner I Jaff M Do DD Minar E
Schmidli J et alA call for uniform reporting standards
in studies assessing endovascular treatment for chronic
ischaemia of lower limb arteries European Heart Journal200728(7)798ndash805 [PUBMED PMID 17317699]
Doepp 2010
Doepp F Paul F Valdueza JM Schmierer K Schreiber
SJ No cerebrocervical venous congestion in patients with
multiple sclerosis Annals of Neurology 201068(2)173ndash83
[PUBMED PMID 20695010]
Dorne 2010
Dorne H Zaidat OO Fiorella D Hirsh J Prestigiacomo
C Albuquerque F et alChronic cerebrospinal venous
insufficiency and the doubtful promise of an endovascular
treatment for multiple sclerosis AACN Clinical Issues in
Critical Care Nursing 20102(4)309ndash11
Ebers 2008
Ebers GC Environmental factors and multiple sclerosis
Lancet Neurology 20087(3)268ndash77 [PUBMED PMID
18275928]
Egger 1997
Egger M Davey Smith G Schneider M Minder C Bias
in meta-analysis detected by a simple graphical test BMJ
1997315(7109)629ndash34 [PUBMED PMID 9310563]
FDA news release 2012
FDA FDA issues alert on potential dangers of unproven
treatment for multiple sclerosis httpwwwfdagov
NewsEventsNewsroomPressAnnouncements
ucm303538htm (released 10 May 2012)
Fischer 1999
Fischer JS LaRocca NG Miller DM Ritvo PG Andrews
H Paty D Recent developments in the assessment of
quality of life in multiple sclerosis (MS) Multiple Sclerosis19995(4)251ndash9 [PUBMED PMID10467384]
Fragoso 2011
Fragoso YD The internet racing ahead of the scientific
evidence The case of ldquoliberation treatmentrdquo for multiple
sclerosis Arquivos de Neuro-Psiquiatria 201169(3)525ndash7
[PUBMED PMID 21755134]
Frohman 2006
Frohman EM Racke MK Raine CS Multiple sclerosis
- the plaque and its pathogenesis New England Journalof Medicine 2006354(9)942ndash55 [PUBMED PMID
16510748]
Ghezzi 2011
Ghezzi A Comi G Federico A Chronic cerebro-spinal
venous insufficiency (CCSVI) and multiple sclerosis
Neurological Sciences 201132(1)17ndash21 [PUBMED
PMID 21161309]
Giacobbi 2012
Giacobbi S Zamboni attacks Ottawa - Canadian studies
doomed to failure [Zamboni attacca Ottawa ndash Gli studi
canadesi destinati al fallimento] CCSVI nella Sclerosi
Multipla - Onlus (available at httpwwwccsvi-smorgq=
node425) (accessed 4 May 2012)
Higgins 2011
Higgins JPT Green S (editors) Cochrane Handbook for
Systematic Reviews of Interventions 510 [updated March
2011] Available from wwwcochrane-handbookorg
Hohlfeld 2011
Hohlfeld R Barkhof F Polman C Future clinical challenges
in multiple sclerosis relevance to sphingosine 1-phosphate
receptor modulator therapy Neurology 201176(8 Suppl 3)
S28ndash37 [PUBMED PMID 21339488]
Hojnacki 2010
Hojnacki D Zamboni P Lopez-Soriano A Galleotti R
Menegatti E Weinstock-Guttman B et alUse of neck
magnetic resonance venography Doppler sonography and
selective venography for diagnosis of chronic cerebrospinal
venous insufficiency a pilot study in multiple sclerosis
patients and healthy controls International Angiology 2010
29(2)127ndash39 [PUBMED PMID 20351669]
ICH Expert Working Group 1994
ICH Expert Working Group Clinical Safety
Data Management Definitions and Standards for
Expedited Reporting E2A International Conference on
Harmonisation of Technical Requirements for Registration
of Pharmaceuticals for Human Use 1994 http
wwwichorgproductsguidelinesefficacyarticleefficacy-
guidelineshtml (accessed 30 April 2012)
Khan 2010
Khan O Filippi M Freedman MS Barkhof F Dore-
Duffy P Lassmann H et alChronic cerebrospinal venous
insufficiency and multiple sclerosis Annals of Neurology
201067(3)286ndash90 [PUBMED PMID 20373339]
Kos 2005
Kos D Kerckhofs E Carrea I Verza R Ramos M Jansa J
Evaluation of the Modified Fatigue Impact Scale in four
different European countries Multiple Sclerosis 200511(1)
76ndash80
Krogias 2010
Krogias C Schroumlder A Wiendl H Hohlfeld R Gold R
ldquoChronic cerebrospinal venous insufficiencyrdquo and multiple
sclerosis critical analysis and first observation in an
unselected cohort of MS patients [in German] Nervenarzt201081(6)740ndash6 [PUBMED PMID 20386873]
Kurtzke 1983
Kurtzke JF Rating neurologic impairment in multiple
sclerosis an expanded disability status scale (EDSS)
13Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Neurology 198333(11)1444ndash52 [PUBMED PMID
6685237]
Laupacis 2011
Laupacis A Lillie E Dueck A Straus S Perrier L Burton
JM et alAssociation between chronic cerebrospinal venous
insufficiency and multiple sclerosis a meta-analysis
Canadian Medical Association Journal 2011183(16)
E1203ndash12 [PUBMED PMID 21969411]
Lazzaro 2011
Lazzaro MA Zaidat OO Mueller-Kronast N Taqi MA
Woo D Endovascular therapy for chronic cerebrospinal
venous insufficiency in multiple sclerosis Frontiers in
Neurology 2011244 [PUBMED PMID 21808631]
Lublin 1996
Lublin FD Reingold SC Defining the clinical course
of multiple sclerosis results of an international survey
National Multiple Sclerosis Society (USA) Advisory
Committee on Clinical Trials of New Agents in Multiple
Sclerosis Neurology 199646(4)907ndash11 [PUBMED
PMID 8780061]
Lucchinetti 1996
Lucchinetti CF Bruumlck W Rodriguez M Lassmann H
Distinct patterns of multiple sclerosis pathology indicates
heterogeneity on pathogenesis Brain Pathology 19966(3)
259ndash74 [PUBMED PMID 8864283]
Ludyga 2010
Ludyga T Kazibudzki M Simka M Hartel M Swierad
M Piegza J et alEndovascular treatment for chronic
cerebrospinal venous insufficiency is the procedure safe
Phlebology 201025(6)286ndash95 [PUBMED PMID
21107001]
Maggs 2004
Maggs FG Palace J The pathogenesis of multiple sclerosis
is it really a primary inflammatory process Multiple Sclerosis200410(3)326ndash9 [PUBMED PMID 15222700]
Malagoni 2010
Malagoni AM Galeotti R Menegatti E Manfredini F
Basaglia N Salvi F et alIs chronic fatigue the symptom of
venous insufficiency associated with multiple sclerosis A
longitudinal pilot study International Angiology 201029
(2)176ndash82 [PUBMED PMID 20351673]
Marder 2011
Marder E Gupta P Greenberg BM Frohman EM
Awad AM Bagert B et alNo cerebral or cervical venous
insufficiency in US veterans with multiple sclerosis
Archives of Neurology 2011 Vol 68 issue 121521ndash5
[PUBMED PMID 21825217]
Martino 2002
Martino G Adorini L Rieckmann P Hillert J Kallmann B
Comi G et alInflammation in multiple sclerosis the good
the bad and the complex Lancet Neurology 20021(8)
499ndash509 [PUBMED 12849335]
Mayer 2011
Mayer CA Pfeilschifter W Lorenz MW Nedelmann M
Bechmann I Steinmetz H et alThe perfect crime CCSVI
not leaving a trace in MS Journal of Neurology Neurosurgery
and Psychiatry 201182(4)436ndash40 [PUBMED PMID
21296899]
McDonald 2001
McDonald WI Compston A Edan G Goodkin D Hartung
HP Lublin FD et alRecommended diagnostic criteria for
multiple sclerosis guidelines from the International Panel
on the diagnosis of multiple sclerosis Annals of Neurology
200150(1)121ndash7 [PUBMED PMID 11456302]
Menegatti 2008
Menegatti E Zamboni P Doppler haemodynamics of
cerebral venous return Current Neurovascular Research
20085(4)260ndash5 [PUBMED PMID 18991660]
Menegatti 2011
Menegatti E Genova V Tessari M Malagoni AM
Bartolomei I Zuolo M et alThe reproducibility of colour
Doppler in chronic cerebrospinal venous insufficiency
associated with multiple sclerosis International Angiology201029(2)121ndash6 [PUBMED PMID 20351668]
Multiple Sclerosis Society of Canada 2012
Multiple Sclerosis Society of Canada CCSVI and MS
httpccsvicaprocedurehtml (assessed 4 May 2012)
Munger 2006
Munger KL Levin LI Hollis BW Howard NS Ascherio
A Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis JAMA 2006296(23)2832ndash8 [PUBMED
PMID 17179460]
Nessler 2010
Nessler S Bruumlck W Advances in multiple sclerosis research
in 2009 Journal of Neurology 2010257(9)1590ndash3
[PUBMED PMID 20689961]
NICE 2012
National Institute for Health and Clinical Excellence
Percutaneous venoplasty for chronic cerebrospinal
venous insufficiency for multiple sclerosis guidance
guidanceniceorgukipg420 (accessed on 28 March 2012)
Patti 2012
Patti F Nicoletti A Leone C Messina S DrsquoAmico E Lo
Fermo S et alMultiple Sclerosis and CCSVI A population-
based case control study PLoS One 20127(8)e41227
[PUBMED 22870210]
Petrov 2011
Petrov I Grozdinski L Kaninski G Iliev N Iloska M
Radev A Safety profile of endovascular treatment for
chronic cerebrospinal venous insufficiency in patients with
multiple sclerosis Journal of Endovascular Therapy 201118
(3)314ndash23 [PUBMED PMID 21679067]
Polman 2005
Polman CH Reingold SC Edan G Filippi M Hartung HP
Kappos L et alDiagnostic criteria for multiple sclerosis
2005 revisions to the ldquoMcDonald Criteriardquo Annalsof Neurology 200558(6)840ndash6 [PUBMED PMID
16283615]
Polman 2011
Polman CH Reingold SC Banwell B Clanet M Cohen
JA Filippi M et alDiagnostic criteria for multiple
14Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

sclerosis 2010 revisions to the McDonald criteria Annals
of Neurology 201169(2)292ndash302 [PUBMED PMID
21387374]
Qiu 2010
Qiu J Venous abnormalities and multiple sclerosis another
breakthrough claim Lancet Neurology 20109(5)464ndash5
[PUBMED PMID 20398855]
Rao 1991
Rao SM Leo GJ Ellington L Nauertz T Bernardin L
Unverzagt F Cognitive dysfunction in multiple sclerosis II
Impact on employment and social functioning Neurology199141(5)692ndash6 [PUBMED PMID 1823781]
Reekers 2011
Reekers JA Lee MJ Belli AM Barkhof F Cardiovascular
and Interventional Radiological Society of Europe
commentary on the treatment of chronic cerebrospinal
venous insufficiency Cardiovascular and Interventional
Radiology 201134(1)1ndash2 [PUBMED PMID 21136256]
RevMan 2011
The Nordic Cochrane Centre The Cochrane Collaboration
Review Manager (RevMan) 51 Copenhagen The Nordic
Cochrane Centre The Cochrane Collaboration 2011
Rudick 2007
Rudick RA Miller D Hass S Hutchinson M Calabresi PA
Confavreux C et alHealth-related quality of life in multiple
sclerosis effects of natalizumab Annals of Neurology 2007
62(4)335ndash46 [PUBMED PMID 17696126]
Schulz 1995
Schulz KF Chalmers I Hayes RJ Altman DG Empirical
evidence of bias Dimensions of methodological quality
associated with estimates of treatment effects in controlled
trials JAMA 1995273(5)408ndash12
Sellner 2011
Sellner J Kraus J Awad A Milo R Hemmer B Stuumlve O
The increasing incidence and prevalence of female multiple
sclerosis - a critical analysis of potential environmental
factors Autoimmunity Reviews 201110(8)495ndash502
[PUBMED PMID 21354338]
Senato della Repubblica 2010
Commissione Parlamentare di inchiesta sullrsquoefficacia e
efficienza del Servizio Sanitario Nazionale Senate of the
Republic XVI Legislature Transcript no 79 Hearing of
Professor Paolo Zamboni and Dr Fabrizio Salvi 82nd
session 22 September 2010 [Senato della Repubblica XVI
Legislatura Resoconto stenografico 79 Audizione del prof
Paolo Zamboni e del Dr Fabrizio Salvi 82deg seduta 2010]
httpwwwsenatoitdocumentirepositorycommissioni
servizio˙sanitario16Stenografici079˙definitivopdf
(accessed 30 April 2012)
Simeoni 2008
Simeoni M Auquier P Fernandez O Flachenecker P
Stecchi S Constantinescu C Validation of the Multiple
Sclerosis International Quality of Life questionnaire
Multiple Sclerosis 200814(2)219ndash30 [PUBMED PMID
17942521]
Simka 2010
Simka M Kostecki J Zaniewski M Majewski E Hartel
M Extracranial Doppler sonographic criteria of chronic
cerebrospinal venous insufficiency in the patients with
multiple sclerosis International Angiology 201029(2)
109ndash14 [PUBMED PMID 20351666]
Simpson 2011
Simpson S Jr Blizzard L Otahal P Van der Mei I Taylor
B Latitude is significantly associated with the prevalence
of multiple sclerosis a meta-analysis Journal of Neurology
Neurosurgery and Psychiatry 201182(10)1132ndash41
[PUBMED PMID 21478203]
Singh 2009
Singh AV Zamboni P Anomalous venous blood flow
and iron deposition in multiple sclerosis Journal of
Cerebral Blood Flow and Metabolism 200929(12)1867ndash78
[PUBMED PMID 19724286]
Sundstroumlm 2010
Sundstroumlm P Waringhlin A Ambarki K Birgander R Eklund
A Malm J Venous and cerebrospinal fluid flow in multiple
sclerosis a case-control study Annals of Neurology 201068
(2)255ndash9 [PUBMED PMID 20695018]
Trapp 1998
Trapp BD Peterson J Ransohoff RM Rudick R Moumlrk S
Bouml L Axonal transection in the lesions of multiple sclerosis
New England Journal of Medicine 1998338(5)278ndash85
[PUBMED PMID 9445407]
Treadwell 2006
Treadwell JT Tregear SJ Reston JT Turkelson CM A
system for rating the stability and strength of medical
evidence BMC Medical Research Methodology 2006652
[DOI 1011861471-2288-6-52]
Tremlett 2006
Tremlett H Devonshire V Is late-onset multiple sclerosis
associated with a worse outcome Neurology 200667(6)
954ndash9 [PUBMED PMID 17000960]
Tsivgoulis 2011
Tsivgoulis G Mantatzis M Bogiatzi C Vadikolias K
Voumvourakis K Prassopoulos P et alExtracranial venous
hemodynamics in multiple sclerosis a case-control study
Neurology 201177(13)1241ndash5 [PUBMED PMID
21849653]
van Rensburg 2010
van Rensburg SJ van Toorn R The controversy of CCSVI
and iron in multiple sclerosis is ferritin the key Neurology
201075(18)1581ndash2 [PUBMED PMID 20881276]
Vera 2012
Vera C Herr A Mandato K Englander M Ginsburg L
Siskin GP Internet-based social networking and its role in
the evolution of chronic cerebrospinal venous insufficiency
Techniques in Vascular and Interventional Radiology 201215
(2)153ndash7 [PUBMED PMID 22640505]
Vickrey 1995
Vickrey BG Hays RD Harooni R Myers LW Ellison GW
A health-related quality of life measure for multiple sclerosis
15Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Quality of life Research 19954(3)187ndash206 [PUBMED
PMID 7613530]
Waschbisch 2011
Waschbisch A Manzel A Linker RA Lee D Vascular
pathology in multiple sclerosis mind boosting or myth
busting Experimental amp Translational Stroke Medicine20113(1)7 [PUBMED PMID 21756314]
Wattjes 2011
Wattjes MP van Oosten BW de Graaf WL Seewann A
Bot JC van den Berg R et alNo association of abnormal
cranial venous drainage with multiple sclerosis a magnetic
resonance venography and flow-quantification study
Journal of Neurology Neurosurgery and Psychiatry 201182
(4)429ndash35 [PUBMED PMID 20980483]
Weinshenker 1989
Weinshenker BG Bass B Rice GP Noseworthy J Carriere
W Baskerville J et alThe natural history of multiple
sclerosis a geographically based study 2 Predictive value of
the early clinical course Brain 1989112 (Pt 6)1419ndash28
[PUBMED PMID 2597989]
Weinstock-Guttman 2011
Weinstock-Guttman B Zivadinov R Cutter G Tamantildeo-
Blanco M Marr K Badgett D et alChronic cerebrospinal
vascular insufficiency is not associated with HLA
DRB11501 status in multiple sclerosis patients PLoS One20116(2)e16802 [PUBMED PMID 21340025]
Yamout 2010
Yamout B Herlopian A Issa Z Habib RH Fawaz A
Salame J et alExtracranial venous stenosis is an unlikely
cause of multiple sclerosis Multiple Sclerosis 201016(11)
1341ndash8 [PUBMED PMID 21041329]
Zamboni 2006
Zamboni P The Big Idea iron-dependent inflammation in
venous disease and proposed parallels in multiple sclerosis
Journal of the Royal Society of Medicine 200699589ndash93
[PUBMED PMID 18045150]
Zamboni 2009a
Zamboni P Galeotti R Menegatti E Malagoni AM
Tacconi G DallrsquoAra S et alChronic cerebrospinal venous
insufficiency in patients with multiple sclerosis Journal ofNeurology Neurosurgery and Psychiatry 200980(4)392ndash9
[PUBMED PMID 19060024]
Zamboni 2009b
Zamboni P Galeotti R Menegatti E Malagoni AM
Gianesini S Bartolomei I et alA prospective open-label
study of endovascular treatment of chronic cerebrospinal
venous insufficiency Journal of Vascular Surgery 200950
(6)1348ndash58 [PUBMED PMID 19958985]
Zamboni 2009c
Zamboni P Galeotti R Menegatti E Malagoni AM Mascoli
F DallrsquoAra S et alRationale and preliminary report of
endovascular treatment of multiple sclerosis the liberation
procedure Vascular and Endovascular Controversies
Update 31st International Symposium Charing Cross
Controversies Challenges Consensus London BIBA
Medical 200971ndash9
Zamboni 2010
Zamboni P Galeotti R The chronic cerebrospinal venous
insufficiency syndrome Phlebology 201025(6)269ndash79
[PUBMED PMID 21106999]
Zamboni 2011a
Zamboni P Menegatti E Weinstock-Guttman B Dwyer
MG Schirda CV Malagoni AM et alHypoperfusion of
brain parenchyma is associated with the severity of chronic
cerebrospinal venous insufficiency in patients with multiple
sclerosis a cross-sectional preliminary report BMCMedicine 2011922 [PUBMED PMID 21385345]
Zamboni 2011b
Zamboni P Galeotti R Weinstock-Guttman B Kennedy
C Salvi F Zivadinov R Venous angioplasty in patients with
multiple sclerosis results of a pilot study European Journal
of Vascular and Endovascular Surgery 2012 Vol 43 issue
1116ndash22 [PUBMED PMID 21839654]
Zivadinov 2011a
Zivadinov R Marr K Cutter G Ramanathan M Benedict
RH Kennedy C et alPrevalence sensitivity and specificity
of chronic cerebrospinal venous insufficiency in MS
Neurology 201177(2)138ndash44 [PUBMED PMID
21490322]
Zivadinov 2011b
Zivadinov R Ramanathan M Dolic K Marr K Karmon
Y Siddiqui AH et alChronic cerebrospinal venous
insufficiency in multiple sclerosis diagnostic pathogenetic
clinical and treatment perspectives Expert Review of
Neurotherapeutics 201111(9)1277ndash94 [PUBMED
21864074]lowast Indicates the major publication for the study
16Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Zamboni 2012 Non RCT the sequence generation was not random but based on availability of a passport by participants recruited
in Buffalo and in Italy on alphabetical order Not designed to compare PTA versus no treatment sham treatment
or other MS treatment
RCT = randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12612000302853
Trial name or title A randomised blinded controlled study of percutaneous transluminal angioplasty (PTA) for extracranial vein
stenoses in patients with multiple sclerosis (MS)
Methods Randomised controlled trial
Participants Inclusion criteria
bull signed Participant Information and Consent Form
bull age 18 to 65 years
bull Expanded Disability Disease Scale Score (EDSS) ranging from 0 to 75
bull diagnosis of MS according to the revised McDonald criteria
bull therapy with currently approved disease-modifying treatments
bull normal renal function or pre-hydration
bull no allergy to contrast media or pre-treatment
bull abnormal extracranial vein venogram
stenosis at any level
abnormal filling of vertebral veins following a jugular bulb injection
delayed emptying of the internal jugular vein in the supine position
persistent filling of the internal jugular vein in the erect position
abnormal appearance of the internal jugular valve
stenosis of the thoracic azygos vein
delayed emptying of the thoracic azygos vein
Exclusion criteria
bull pregnancy or planning a pregnancy within the next two years
bull relapse disease progression and steroid treatment in the 30 days preceding study entry (all conditions
significantly modify clinical parameters rendering unreliable any postoperative assessment)
bull pre-existing medical conditions known to be associated with brain pathology including
neurodegenerative disorder cerebrovascular disease and history of alcohol abuse Abnormal renal function
with a calculated e-GFR (estimated glomerular filtration rate) lt 60 and pre-hydration not possible
bull allergy to contrast and pre-treatment not possible
bull refusal to undergo the endovascular treatment or randomisation
17Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

ACTRN12612000302853 (Continued)
bull previous PTA on extracranial veins
bull unable to adequately perform the CogState cognitive assessment tool because of visual or manual
dexterity impairment
Interventions PTA procedure compared to the control group The control group will get a sham PTA procedure (the
angiogram without the ballooning) at the beginning of the study
Outcomes Primary outcomes of the trial
bull Change in clinical parameters and disease progression as measured by Kurtzke Extended Disability
Status Scale (EDSS) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by the Multiple Sclerosis Functional
Composite Score (MSFC) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in clinical parameters and disease progression as measured by Cognitive Assessment Tool
(CogState) at 1 week 1 3 6 and 12 months compared to baseline
Secondary outcomes of the trial
bull Composite number of procedural and post-procedural adverse events (to 12 months) measured
Common Terminology Criteria for Adverse Events v 4 (CTCAE) at 1 week 1 3 6 and 12 months
compared to baseline
bull Restoration of venous outflow (to 75 from normal outflow) as measured by venogram US
(ultrasound) and MRV (Magnetic Resonance Venography) at 6 and 12 months
bull Change in patient reported quality of life measured by the Multiple Sclerosis Quality of Life-54
Instrument (MSQoL-54) at 1 week 1 3 6 and 12 months compared to baseline
bull Change in patient reported fatigue as measured by the Fatigue Severity Scale (FSS) at 1 week 1 3 6
and 12 months compared to baseline
Starting date April 2012
Contact information Helen Kavnoudias
Radiology Research Unit
Radiology Department
The Alfred
Level 1 Phillip Block
55 Commercial Road
Melbourne Vic 3004 Australia
Tel +61 3 9076 3606
hkavnoudiasalfredorgau
Notes Website assessed 9 July 2012
NCT01089686
Trial name or title Study to evaluate treating chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull must be 18 years old or greater and less than or equal to 65 years of age
bull core of 0 to 7 on the EDSS (Expanded Disability Disease Scale Score) scale
18Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01089686 (Continued)
bull diagnosis of relapsing remitting or secondary progressive MSby a neurologist and confirmed by one of
the independent study neurologists
bull presence of greater than or equal to 50 percent stenosis of the extracranial veins as determined by
venogram
bull informed consent signed by patient
Exclusion criteria
bull patient is unwilling to comply with the follow-up
bull patient is pregnant
bull diagnosis of primary progressive MS by a certified neurologist confirmed by one of the study
neurologists
bull presence of less than 50 stenosis of the extracranial veins as determined by venogram
bull presence of other medical illnesses or a psychiatric condition that in the opinion of the investigator
may cause the subject to be non-compliant with the protocol requirements
bull life expectancy is less than 1 year
bull lack of mental capacity to consent
bull creatinine level of greater than 25 or is dialysis dependent
bull enrollment in another clinical study
Interventions Venoplasty versus sham procedure (non-treatment)
Outcomes Primary outcomes of the trial
bull Incidence of major adverse events
The evaluation of safety will be defined as the incidence of major adverse events at 30 days following the
index procedure The evaluation of feasibility and efficacy will be determined by those patients that do not
have more than 50 restenosis within the 30 day time frame
bull Neurological assessment of MS
An independent neurologist will assess the number of MS attacks that have occurred during 1 year follow-up
period
bull MRIMRA (Magnetic Resonance ImagingMagnetic Resonance Angiography)(evaluation of MS
lesions)
Evaluation of imaging to reveal local iron content change in MS lesions and oxygen saturation changes using
conventional MRAMRI methods by an independent radiologist
Secondary outcomes of the trial
bull Mortality
All cause mortality will be evaluated through 1 year
bull Major adverse events
Incidence of all major adverse events will be collected for 1 year
bull Identification of central venous stenosis
Evaluation of the correlation between MRV (Magnetic Resonance Venography) Duplex Ultrasound and
Venogram in identifying central venous stenosis
Starting date August 2010
Contact information Manish Mehta MD
The Center for Vascular Awareness Albany New York US
5 Pine West Plaza Suite 501
Washington Avenue Extension Albany NY 12205
Tel (518) 452-1048
19Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01089686 (Continued)
Notes Website assessed 9 July 2012
NCT01201707
Trial name or title Evaluation of angioplasty in the treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple
sclerosis
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients who are willing to comply with the protocol requirements and can be contacted by telephone
bull 18 to 60 years of age
bull clinically defined MS by Polman criteria
bull history of MS as defined above with an EDSS (Expanded Disability Disease Scale Score) between 3
and 6
bull significant stenosis of the internal jugular or azygos vein on the basis of magnetic resonance
venography or Doppler ultrasound
Exclusion criteria
bull renal insufficiency based on an estimated GFR lt 45
bull known severe allergy to iodine or gadolinium-based contrast agents which cannot be adequately pre-
medicated
bull known allergy to nickel
bull pregnancy
bull contraindication to anticoagulation or anti-platelet medication
bull contraindication to drugs used for conscious sedation during interventional procedures including
Versed and Fentanyl
bull history of deep venous thrombosis of the lower extremities
bull occlusion of the right and left common femoral veins
bull any changes in their disease modifying drug regimen for MS during the 6 months prior to enrolment
in this trial This would include the addition of any new medications a change in the dosage of any
medications or the removal of any medications from a patientrsquos drug regimen
bull life expectancy lt 18 months
bull currently enrolled or who plan to enroll in other investigations that conflict with follow-up testing or
confounds data in this trial
Interventions Angioplasty versus no treatment (observation)
Outcomes Primary outcomes of the trial
bull Impact of CCSVI treatment on quality of life in patients with MS at 1 3 6 12 18 and 24 months
This will be assessed using the Multiple Sclerosis Quality of Life-54 (MSQOL-54) which is a health-related
quality of life measure that combines generic and MS-specific items into a single self-report questionnaire
Secondary outcomes of the trial
bull Clinical significance of CCSVI in MS patients at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates Expanded Disability Status Scale (EDSS) change
and change in the timed 25-foot walk
bull Superiority of angioplasty to observation for treatment of CCSVI at 1 6 12 18 and 24 months
This will be assessed clinically using annualised relapse rates EDSS change and change in the timed 25-foot
20Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01201707 (Continued)
walk
bull Incidence of CCSVI in patients with MS at baseline
This will be assessed on the basis of the findings on diagnostic venography of the internal jugular and azygos
veins which is the initial procedure performed in these patients
bull Safety of endovascular treatment of CCSVI at 1 3 6 12 18 and 24 months
This is defined as the number and nature of any procedure-related adverse effects
bull Target vessel primary and secondary patency at 1 3 6 12 18 and 24 months
Primary patency is the interval following the initial angioplasty procedure until a re-intervention is performed
to preserve patency Secondary patency is defined as the interval following the initial angioplasty procedure
until treatment of the vein is abandoned due to an inability to treat the original lesion
Starting date August 2010
Contact information Barbara MacDowell
Albany Medical Center
Albany New York United States 12208
Tel (518) -262-5356
macdowbmailamcedu
Katy Regan
Tel (518) -262-5938
regankmailamcedu
Notes Website assessed 9 July 2012
NCT01371760
Trial name or title BRAVE-DREAMS (BRAin VEnous DRainage Exploited Against Multiple Sclerosis)
Methods Randomised controlled trial
Participants Inclusion criteria
bull patients affected by CCSVI associated with MS
bull relapsing-remitting or secondary progressive or both
bull 18to 65 years old
bull EDSS (Expanded Disability Disease Scale Score) 2 to 5
bull disease duration lt 10 yrs
bull no relapse in the 30 days preceding the procedure
bull clinical stability in the last 6 months with disease modifying treatments
bull patients under the best available therapy
Exclusion criteria
bull patients previously treated for CCSVI or inserted in other clinical trials in the last 3 months
bull under treatment with natalizumab
bull pregnant or refusing to adopt contraception
bull presence of significant comorbidities
bull alcohol-drug abuse
bull thrombophilia
bull contraindication to MR
21Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01371760 (Continued)
Interventions Venous percutaneous transluminal angioplasty versus sham treatment (catheter venography)
Outcomes Primary outcomes of the trial
bull Clinical parameters in an integrated functional score from baseline to 12 months
Five neurological parameters will be measured by the means of proper validated tools along 1 year follow-up
The evaluation leads to a score respectively expressed as improved stable fluctuant worsened
bull MRI outcome measures T1Gad active lesion T2 lesion volume MRI evaluation at baseline 6 and 12
months
Standard MRI parameters will be assessed by the means of a blinded centre of lecture
Secondary outcomes
bull EDSS from baseline to 12 months
EDSS will be assessed along 1 year follow-up
bull Chronic fatigue from baseline to 12 months
This highly disabling symptom completely orphan of effective therapy will be measured by M-FIS (Modified-
Fatigue Impact Scale)
bull Cognitive function from baseline to 12 months
Cognitive functions will be measured by the means of MoCA mental state questionnaire
bull Annualized relapse rate from baseline to 12 months
In the sub population affected by the RR clinical form the number of relapses will be assessed
bull Patency rate from baseline to 12 months
The rate of successful PTA will be assessed by the means of postoperative Doppler sonography
bull Emotional status from baseline to 12 months
Anxiety and Depression Scale for use with multiple sclerosis patients will be administered
bull Memory and cognition from baseline to 12 months
The assessment will be performed by the means of PASAT - Paced Auditory Serial Addition Test
bull Overactive Bladder from baseline to 12 months
Overactive Bladder symptom will be measured by the means of validated Overactive Bladder Questionnaire-
b
Starting date July 2011
Contact information Graziella Filippini MD
S Anna Hospital University of Ferrara Ferrara Italy 44100
Tel 0039 0223941
gfilippiniinstituto-bestait
Paolo Zamboni MD
Tel 0039 0532237694
Notes Website assessed 9 July 2012
NCT01450072
Trial name or title Prospective randomized endovascular therapy in multiple sclerosis - PREMiSE
Methods Randomised controlled trial
22Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01450072 (Continued)
Participants Inclusion criteria
bull age 18 to 65 years
bull EDSS (Expanded Disability Disease Scale Score) 0 to 65 (0 to 55 in the phase II of the study)
bull diagnosis of relapsing MS according to the McDonald criteria (Polman 2005)
bull 1 relapse within the past 12 months or GAD positive lesion on an MRI within the past 3 months (only
for phase II of the study)
bull be on treatment with currently FDA approved disease-modifying treatments (excluding Tysabri or
steroids (within the last 30 days prior to enrolment)
bull evidence of ge 2 sonographic parameters of suspicious abnormal extracranial cerebral venous outflow
(see Table 1 background and 15 section)
bull normal renal function creatinine clearance level of gt 60
Exclusion criteria
bull relapse disease progression and Tysabri and steroid treatment in the 30 days preceding study entry
bull pre-existing medical conditions known to be associated with brain pathology (eg neurodegenerative
disorder cerebrovascular disease positive history of alcohol abuse)
bull severe peripheral chronic venous insufficiency
bull abnormal renal function
bull contrast allergy (anaphylaxis)
bull not willing to undergo the endovascular treatment
bull peripheral vascular disease
Interventions Selective venography followed by therapeutic balloon angioplasty versus venography and sham angioplasty
Outcomes Primary outcomes of the trial
bull Safety at 24 hours and at 1 month
Percent () of patients with Severe Adverse Events (SAE) post-surgical safety outcome in MS patients diag-
nosed with CCSVI that underwent therapeutic angioplasty
Secondary outcomes of the trial
bull Preliminary efficacy at 1 3 6 and 12 months
Restoration of venous outflow (more than 75 of normal outflow) as measured by the combined ECDTCD
(Extracranial Venous DopplerTranscranial Doppler) and and MRV following the angioplasty as compared
to baseline as well as compared to a parallel control group of MS patients that will undergo only selective
venography without balloon angioplasty (sham-angioplasty)
Starting date June 2010
Contact information Cheryl Kennedy LMSW MPH
University at Buffalo Neurosurgery
Buffalo New York United States 14209
Tel 716-859-7068
Jennifer Gay
Tel 716-887-5200
jgayubnscom
Notes Website assessed 9 July 2012
23Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

NCT01555684
Trial name or title Functional changes following percutaneous venoplasty in multiple sclerosis patients
Methods Randomised controlled trial
Participants Inclusion criteria
bull Diagnosis of CCSVI using transcranial and extracranial colour Doppler sonography in both supine
and sitting positions The diagnosis requires that 2 or more of the following 5 criteria are met reflux in the
internal jugular or vertebral veins or both with the head in any position reflux in the deep cerebral veins
high-resolution B-mode evidence of internal jugular vein stenosis absence of Doppler-detectable flow in the
internal jugular veins andor vertebral veins loss of postural control of the main cerebral venous outflow
pathways
Exclusion criteria
bull Non ambulatory
Interventions Percutaneous venoplasty versus no treatment
Outcomes Primary outcomes of the trial
bull Neuromuscular function at 52 days
The venoplasty procedure will be performed at 8 days
Secondary outcomes of the trial
bull Free living activity from 0 to 7 days and from 9 to 52 days
Measured by accelerometry
Starting date April 2012
Contact information Angus Hunter PhD
amhunter1stiracuk
University of Stirling Stirling UK FK9 4LA
Notes Website assessed 9 July 2012
24Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

D A T A A N D A N A L Y S E S
This review has no analyses
A D D I T I O N A L T A B L E S
Table 1 Glossary of terms
Antigen Substance or molecule that when introduced into the body triggers the production of
an antibody by the immune system which will then kill or neutralise the antigen that
is recognised as a foreign and potentially harmful invader
Autoreactive Immune response acting against own tissue
Ataxia Neurological sign and symptom that consists of gross lack of coordination of muscle
movements
Axon Part of the neuron that conducts electrical impulses away from the neuronrsquos cell body
Central nervous system Part of the nervous system that integrates the information that it receives from and
coordinates the activity of all parts of the body It includes the brain and the spinal
cord
Cognitive impairment Condition associated with confusion forgetfulness difficulty concentrating and plan-
ning and so on
Congestion Accumulation or overfilling of the blood vessels
Demyelination Loss of the myelin sheath insulating the nerves
Dysarthria Having a problem with articulating
Erythrocyte extravasation Leakage of red blood cells into the surrounding tissue
Gliosis Proliferation of astrocytes (glial cells) in damaged areas of the central nervous system
HLA-DR Major histocompatability complex (MHC) class II cell surface receptor encoded by
the human leukocyte antigen complex on chromosome 6 region 6p2131 HLA-DR
is also involved in several autoimmune conditions disease susceptibility and disease
resistance It is also closely linked to HLA-DQ and this linkage often makes it difficult
to resolve the more causative factor in disease
HLA-DQ A cell surface receptor type protein (MHC class II type) found on antigen presenting
cells The DQ loci are in close genetic linkage to HLA-DR When tolerance to self
proteins is lost DQ may become involved in autoimmune disease
Immuno-mediated disease Conditions that result from abnormal activity of the bodyrsquos immune system
25Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Table 1 Glossary of terms (Continued)
Inflammation Response of vascular tissues to harmful stimuli and a protective attempt to remove the
injurious stimuli and to initiate the healing process A cascade of biochemical events
propagates and matures the inflammatory response involving the local vascular system
the immune system and various cells within the injured tissue
Major histocompatability complex (MHC) A large genomic region or gene family found in most vertebrates that encodes MHC
molecules MHC molecules play an important role in the immune system and autoim-
munity
Neuron An electrically excitable cell that processes and transmits information by electrical and
chemical signalling Chemical signalling occurs via synapses specialised connections
with other cells Neurons connect to each other to form networks Neurons are the
core components of the nervous system
Pathological Altered or caused by disease
Pathogenesis The mechanism by which the disease is caused
Phagocytosis Mechanism used to remove pathogens and cell debris
Polygenic disease Disease controlled by several genes at once
Relapse An objective newre-emerging neurological abnormality present for at least 24 hours
in the absence of feverinfection
Reversible Capable of returning to an original conditionsituation
Stenosis Abnormal narrowing in a blood vessel
Tremor Involuntary somewhat rhythmic muscle contraction and relaxation involving to-and-
fro movements of one or more body parts
Venogram An X-ray test that takes pictures of blood flow through the veins in a certain area of
the body
Venotopic Located in the veins
Venous angioplasty A procedure that can be performed during a venogram to open or bypass veins It can
also be used for placement of a stent which keeps a vessel or tissue in an open position
to allow for improved blood flow
Venous congestion Dilation of veins and capillaries due to impaired venous drainage
Vertigo Type of dizziness where there is a feeling of motion when one is stationary
26Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Table 2 Contact with investigators
Study ID Response Additional Comment
Zamboni 2012 Nil e-mail zmpunifeit on 24 July 2012 4 August 2012
Dear Professor Zamboni
My colleagues and I are conducting a Cochrane review on
rdquoPercutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous
insufficiency (CCSVI) in multiple sclerosis patientsrdquo and your study ldquoZamboni P Ga-
leotti R Weinstock-Guttman B Kennedy C Salvi F Zivadinov R Venous angioplasty
in patients with multiple sclerosis results of a pilot study Journal of Vascular Surgery
201243(1)116-22rdquo has been identified as potentially eligible for inclusion
To enable us to further assess this trial for inclusion I would be obliged if you could
kindly provide us with the following missing trial details
bull Can we receive the protocol of this study
bull Did restenosis occur in the first 6 months after PTA in the immediate group or
later
bull When exactly did the relapses occur in both groups (time after start of the study)
bull In which group occurred the vasovagal collapse (immediate PTA or delayed
PTA)
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis
Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for participants
with multiple sclerosis
Patient or population participants with multiple sclerosis
Intervention percutaneous transluminal angioplasty
Comparison no treatment sham treatment or other MS treatment
Outcomes Illustrative comparative risks
(95 CI)
Relative effect
(95 CI)
No of Partici-
pants
(studies)
Quality of the
evidence
(GRADE)
Comments
Assumed risk Corresponding
risk
No treatment
sham treatment
or other MS
treatment
Percu-
taneous trans-
luminal angio-
plasty
Serious ad-
verse events ac-
cording to ICH
Expert Working
Group 1994
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
27Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Table 3 Percutaneous transluminal angioplasty compared to no treatment sham treatment or other MS treatment for
participants with multiple sclerosis (Continued)
Any other ad-
verse events
reported during
or after the PTA
procedure
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Change in QoL
assessed using
any validated
disease specific
or generic in-
strument
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
well-being as
measured with a
visual analogue
scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Mean change in
Modified
Fatigue Impact
Scale (MFIS) (
Kos 2005)
or other recog-
nised and vali-
dated MS-
fatigue scale
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
Any
other patient re-
ported outcome
- - Not estimable 0
(0)
No evidence
from RCTs1
No RCT
included
The basis for the assumed risk (eg the median control group risk across studies) is provided in footnotes The corresponding risk
(and its 95 confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention
(and its 95 CI)
CI Confidence interval RR Risk ratio
GRADE Working Group grades of evidence
High quality Further research is very unlikely to change our confidence in the estimate of effect
Moderate quality Further research is likely to have an important impact on our confidence in the estimate of effect and may change
the estimate
Low quality Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to
change the estimate
Very low quality We are very uncertain about the estimate
1 We did not address study designs other than RCT the current evidence is mainly based on observational studies and the quality of
this evidence should be considered low to very low
28Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients
Core elements Issues to consider Status of research for this review
Evidence (E) What is the current state of the evidence This systematic review identified no RCTs No evi-
dence of effectiveness of percutaneous transluminal an-
gioplasty (PTA) for treatment of chronic cerebrospinal
insufficiency (CCSVI) in MS patients
Population (P) Diagnosis disease stage comorbidity risk factors gen-
der age ethnic group specific inclusion or exclusion
criteria clinical setting
Inclusion criteria
bull participants of both genders gt 17 years with a
diagnosis of MS according to the original or the
revised McDonald criteria (McDonald 2001Polman
2005Polman 2011)
bull diagnosis of CCSVI according to Zambonirsquos
criteria (Zamboni 2009a) or other relevant
internationally recognised and validated criteria
Exclusion criteria
bull pregnancy
bull relapse
bull corticosteroid treatment 30 days before study
entry
bull pre-existing medical conditions known to be
associated with brain pathology
bull allergy to contrast media
bull disease progression
bull previous PTA treatment
bull patients with renal insufficiency
bull patients with a contraindication to
anticoagulation or anti-platelet medication
bull patients with a history of deep venous thrombosis
of the lower extremities
bull patients with occlusion of the right and left
common femoral veins
bull patients with a life expectancy lt 18 months
Intervention (I) Type frequency dose duration prognostic factor The study duration should be at least 12 months as-
sessing percutaneous transluminal angioplasty alone or
in combination with other MS treatments
Comparison (C) Type frequency dose duration prognostic factor No treatment sham treatment or other MS treatments
Outcome (O) Which clinical or patient-related outcomes will the re-
searcher need to measure improve influence or accom-
plish Which methods of
measurement should be used
1 The number of patients with at least one AE
bull serious AE according to ICH Expert Working
Group 1994
bull any other AE reported during or after the PTA
procedure
2 The number of participants who experienced progres-
sion on the Expanded Disability Status Scale (EDSS)
(Kurtzke 1983)
29Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

Table 4 Research recommendations based on a gap in the evidence of the effects of percutaneous transluminal angioplasty
for treatment of chronic cerebrospinal venous insufficiency in multiple sclerosis patients (Continued)
3 Patient reported outcomes (PROs) to include any of
the following if reported
bull change in QoL assessed using any validated
disease specific (eg MSQOL-54 (Vickrey 1995)
MSQLI (Fischer 1999) MusiQoL (Simeoni 2008)) or
generic instrument (eg short form 36 (SF-36)
(Rudick 2007))
bull mean change in well-being as measured with a
visual analogue scale (VAS)
bull mean change in Modified Fatigue Impact Scale
(MFIS) (Kos 2005) or other recognised and validated
MS-fatigue scale
bull or any other PRO
4 Restenosis of target vessel primary and secondary pa-
tency
5 Mean change in cognitive functions assessment
through validated battery of tests in MS (ie Brief Re-
peatable Battery of Neuropsychological Tests (BRBNT)
(Rao 1991))
3 In the RRMS subgroup only the number of partici-
pants experiencing at least one relapse
Time stamp (T) Date of literature search or recommendation July 2012
Study type What is the most appropriate study design to address
the proposed question
bull Randomised controlled trial (adequately
poweredmulti-centred)
bull Methods concealment of allocation sequence
bull Blinding because blinding of participants and
trialists may not be feasible outcomes assessors and
data analysts should be blinded to the intervention
received by the participants
bull Setting hospitaluniversity with adequate follow-
up (at least 12 months)
H I S T O R Y
Protocol first published Issue 6 2012
Review first published Issue 12 2012
30Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd
C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd

C O N T R I B U T I O N S O F A U T H O R S
The trial search coordinator of the Cochrane MSRDCNS Group was responsible for running the search
Esther van Zuuren (EvZ) was responsible for organising the retrieval of papers writing to authors of papers for additional information
screening search results screening retrieved papers against inclusion criteria appraising the quality of papers obtaining and screening
data on unpublished studies
Zbys Fedorowicz (ZF) and EvZ will be responsible in future updates for reviewing the studies and extracting outcome data assessing
risk of bias from the papers and entering it into RevMan
ZF EvZ and Eugenio Pucci (EP) will be responsible in future updates for writing the effects of intervention analysis and interpretation
of the data
All review authors contributed to writing the review
EvZ ZF VJ and Edward Robak (ER) conceived the idea for the review and are the guarantors for the review
ZF and EvZ will update the review
D E C L A R A T I O N S O F I N T E R E S T
EP has received funds from a non-profit association the ldquoAssociazione Marchigiana sclerosi multipla e altre malattie neurologicherdquo
this association has received donations from Biogen Dompeacute Merck-Serono and Bayer-Schering In the last five years (2007 to 2012)
EP has also received honoraria reimbursement for attending congresses and grant support for organising scientific activities from the
above-mentioned drug industries and from Aventis UCB Lundbeck and Novartis The other review authors have no financial conflicts
of interest and they do not have any associations with any parties who may have vested interests in the results of this review One of the
authors (ER) has undergone the procedure under consideration in this review
S O U R C E S O F S U P P O R T
Internal sources
bull No sources of support Netherlands
External sources
bull No sources of support Netherlands
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
There are no differences between the protocol and the review
31Percutaneous transluminal angioplasty for treatment of chronic cerebrospinal venous insufficiency (CCSVI) in multiple sclerosis patients
(Review)
Copyright copy 2012 The Cochrane Collaboration Published by John Wiley amp Sons Ltd




















