
Life-threatening presentation of mediastinal neoplasms: report on 7 consecutive pediatric patients
Upload
independentCategory
view
0download
0
The Controversies Surrounding The Controversies Surrounding the Diagnosis and Management of the Diagnosis and Management of Life Threatening Acute Pulmonary Life Threatening Acute Pulmonary
EmbolismEmbolism
Kenneth V Leeper Jr MDKenneth V Leeper Jr MDAssociate Professor of MedicineAssociate Professor of Medicine
Division of Pulmonary and Critical Care MedicineDivision of Pulmonary and Critical Care MedicineEmory School of MedicineEmory School of Medicine
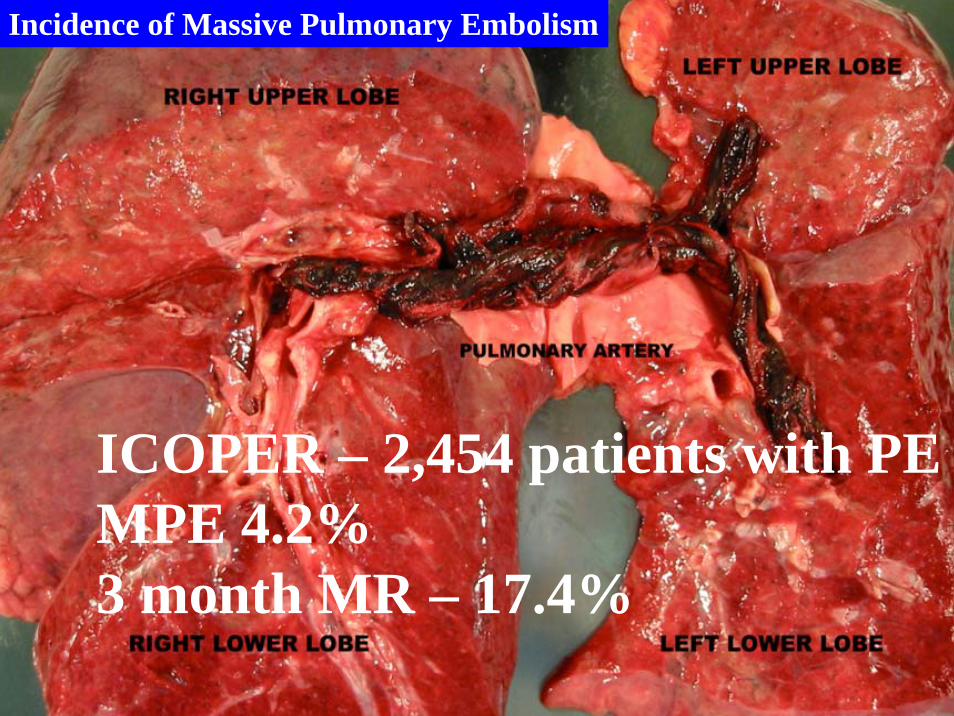
ICOPER ndash 2454 patients with PEMPE 423 month MR ndash 174
Incidence of Massive Pulmonary Embolism
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Massive Pulmonary EmbolismMassive Pulmonary EmbolismDefinitionsDefinitions
gtgt 50 obstruction 50 obstruction -- Dalen NEJM 1969Dalen NEJM 1969
gtgt 50 obstruction 50 obstruction -- Miller Br Heart J 1970Miller Br Heart J 1970
Filling defectobstruction = 2 lobar arteries UPET I + IIFilling defectobstruction = 2 lobar arteries UPET I + II
Shock Dyspnea PaOShock Dyspnea PaO22 lt50 PCOlt50 PCO22 lt30 lt30 acidosis acidosis uarruarr CVP PAP CVP PAP gtgt 3030PA obstruction PA obstruction gtgt 50 50 -- Greenfield 1976Greenfield 1976
RV dysfunction RV dysfunction ++ hypotension hypotension -- Goldhaber 1995Goldhaber 1995
MPE MPE ndashndash Clinical Definition Clinical Definition Overt Respiratory and Hemodynamic Overt Respiratory and Hemodynamic DeteriorationDeterioration
ShockShockCor pulmonaleCor pulmonaleSyncopeSyncope
High Risk of Cardiopulmonary DeteriorationHigh Risk of Cardiopulmonary DeteriorationPersistent tachycardiaPersistent tachycardiaPersistent hypoxemiaPersistent hypoxemiaRelative hypotensionRelative hypotensionEvidence of RV dysfunctionEvidence of RV dysfunction
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
ICOPER ndash 2454 patients with PEMPE 423 month MR ndash 174
Incidence of Massive Pulmonary Embolism
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Massive Pulmonary EmbolismMassive Pulmonary EmbolismDefinitionsDefinitions
gtgt 50 obstruction 50 obstruction -- Dalen NEJM 1969Dalen NEJM 1969
gtgt 50 obstruction 50 obstruction -- Miller Br Heart J 1970Miller Br Heart J 1970
Filling defectobstruction = 2 lobar arteries UPET I + IIFilling defectobstruction = 2 lobar arteries UPET I + II
Shock Dyspnea PaOShock Dyspnea PaO22 lt50 PCOlt50 PCO22 lt30 lt30 acidosis acidosis uarruarr CVP PAP CVP PAP gtgt 3030PA obstruction PA obstruction gtgt 50 50 -- Greenfield 1976Greenfield 1976
RV dysfunction RV dysfunction ++ hypotension hypotension -- Goldhaber 1995Goldhaber 1995
MPE MPE ndashndash Clinical Definition Clinical Definition Overt Respiratory and Hemodynamic Overt Respiratory and Hemodynamic DeteriorationDeterioration
ShockShockCor pulmonaleCor pulmonaleSyncopeSyncope
High Risk of Cardiopulmonary DeteriorationHigh Risk of Cardiopulmonary DeteriorationPersistent tachycardiaPersistent tachycardiaPersistent hypoxemiaPersistent hypoxemiaRelative hypotensionRelative hypotensionEvidence of RV dysfunctionEvidence of RV dysfunction
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Massive Pulmonary EmbolismMassive Pulmonary EmbolismDefinitionsDefinitions
gtgt 50 obstruction 50 obstruction -- Dalen NEJM 1969Dalen NEJM 1969
gtgt 50 obstruction 50 obstruction -- Miller Br Heart J 1970Miller Br Heart J 1970
Filling defectobstruction = 2 lobar arteries UPET I + IIFilling defectobstruction = 2 lobar arteries UPET I + II
Shock Dyspnea PaOShock Dyspnea PaO22 lt50 PCOlt50 PCO22 lt30 lt30 acidosis acidosis uarruarr CVP PAP CVP PAP gtgt 3030PA obstruction PA obstruction gtgt 50 50 -- Greenfield 1976Greenfield 1976
RV dysfunction RV dysfunction ++ hypotension hypotension -- Goldhaber 1995Goldhaber 1995
MPE MPE ndashndash Clinical Definition Clinical Definition Overt Respiratory and Hemodynamic Overt Respiratory and Hemodynamic DeteriorationDeterioration
ShockShockCor pulmonaleCor pulmonaleSyncopeSyncope
High Risk of Cardiopulmonary DeteriorationHigh Risk of Cardiopulmonary DeteriorationPersistent tachycardiaPersistent tachycardiaPersistent hypoxemiaPersistent hypoxemiaRelative hypotensionRelative hypotensionEvidence of RV dysfunctionEvidence of RV dysfunction
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Massive Pulmonary EmbolismMassive Pulmonary EmbolismDefinitionsDefinitions
gtgt 50 obstruction 50 obstruction -- Dalen NEJM 1969Dalen NEJM 1969
gtgt 50 obstruction 50 obstruction -- Miller Br Heart J 1970Miller Br Heart J 1970
Filling defectobstruction = 2 lobar arteries UPET I + IIFilling defectobstruction = 2 lobar arteries UPET I + II
Shock Dyspnea PaOShock Dyspnea PaO22 lt50 PCOlt50 PCO22 lt30 lt30 acidosis acidosis uarruarr CVP PAP CVP PAP gtgt 3030PA obstruction PA obstruction gtgt 50 50 -- Greenfield 1976Greenfield 1976
RV dysfunction RV dysfunction ++ hypotension hypotension -- Goldhaber 1995Goldhaber 1995
MPE MPE ndashndash Clinical Definition Clinical Definition Overt Respiratory and Hemodynamic Overt Respiratory and Hemodynamic DeteriorationDeterioration
ShockShockCor pulmonaleCor pulmonaleSyncopeSyncope
High Risk of Cardiopulmonary DeteriorationHigh Risk of Cardiopulmonary DeteriorationPersistent tachycardiaPersistent tachycardiaPersistent hypoxemiaPersistent hypoxemiaRelative hypotensionRelative hypotensionEvidence of RV dysfunctionEvidence of RV dysfunction
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

MPE MPE ndashndash Clinical Definition Clinical Definition Overt Respiratory and Hemodynamic Overt Respiratory and Hemodynamic DeteriorationDeterioration
ShockShockCor pulmonaleCor pulmonaleSyncopeSyncope
High Risk of Cardiopulmonary DeteriorationHigh Risk of Cardiopulmonary DeteriorationPersistent tachycardiaPersistent tachycardiaPersistent hypoxemiaPersistent hypoxemiaRelative hypotensionRelative hypotensionEvidence of RV dysfunctionEvidence of RV dysfunction
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
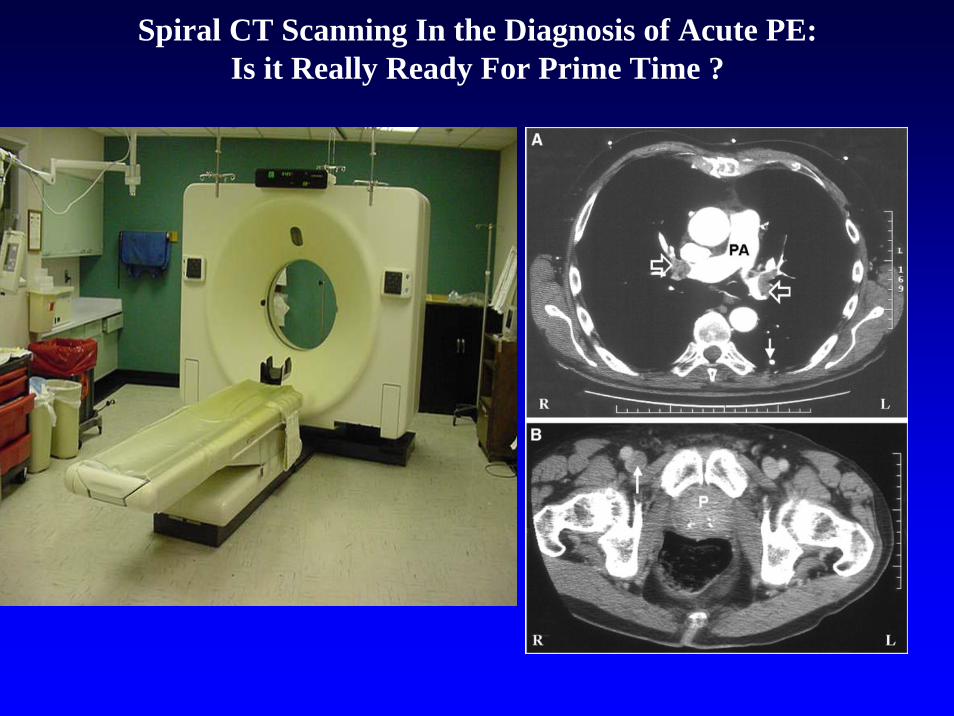
Spiral CT Scanning In the Diagnosis of Acute PEIs it Really Ready For Prime Time
PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

PIOPED II NEJM 20063542317PIOPED II NEJM 20063542317--23272327
BackgroundBackground The accuracy of multidetector computed The accuracy of multidetector computed tomographic angiography (CTA) for the diagnosis of acute tomographic angiography (CTA) for the diagnosis of acute pulmonary embolism has not been determined conclusively pulmonary embolism has not been determined conclusively MethodsMethods The Prospective Investigation of Pulmonary The Prospective Investigation of Pulmonary Embolism Diagnosis II trial was a prospective multicenter Embolism Diagnosis II trial was a prospective multicenter investigation of the accuracy of multidetector CTA alone and investigation of the accuracy of multidetector CTA alone and combined with venouscombined with venous--phase imaging (CTAphase imaging (CTAndashndashCTV) for the CTV) for the diagnosis of acute pulmonary embolism We used a diagnosis of acute pulmonary embolism We used a composite reference test to confirm or rule out the diagnosis composite reference test to confirm or rule out the diagnosis of pulmonary embolism of pulmonary embolism
Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Venous ThromboembolismVenous Thromboembolism
PIOPED II The Bottom Line
CTPA aloneSensitivity 83Specificity 96
CTA-CTVSensitivity 90Specificity 95
PIOPED II JAMA 2006
Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Role of MRA in the Diagnosis of Acute Role of MRA in the Diagnosis of Acute PE PE ndashndash PIOPED IIIPIOPED III
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

ldquoVenous thrombosis is always a severe disease and is often fatal because fragments of the thrombi may detach and occlude branches of the pulmonary artery the occlusion of the main branches of the pulmonary artery causes a striking rise of the blood pressure in these vessels This rise-which the right heart might fight in order to ensure circulation-may sometimes lead to cardiac arrestrdquo
Picot 1884Lecons de Clinique Meacutedicale
Pulmonary Embolism Stratification
Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Pressure loadPressure loadPressure load
Increased RV volumeIncreased RV volumeIncreased RV volume
Decreased LV preload Decreased LV preload Decreased LV preload
Septal shift Septal shift Pericardial restrictionPericardial restriction
SeriesSeriesinteractioninteraction
DecreasedRV outputDecreasedDecreasedRV outputRV output
RV decompensatlonRV decompensatlonRV decompensatlonIschemiaIschemiaIschemia
DecreasedDecreasedCOMAPCOMAP
DecreasedRV CPP
DecreasedDecreasedRV CPPRV CPP
NeurohumoralNeurohumoralObstructionObstruction
Decreased LV distensibility Decreased LV distensibility
uarruarr OO22 demandsdemandsuarruarr WWall tensionall tension
uarruarr WWall tensionall tensionuarruarr OO22 demanddemand
Wood KE Wood KE ChestChest 2002121877 2002121877
Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Respiratory ConsequencesIncrease VDVT
Right to left shuntingVQ inequality
Low MVO2
MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

MPE diagnosis The EKGMPE diagnosis The EKG
Nonspecific
S1
Q3 T3
Sinus tachycardia gt100bmComplete or incomplete RBBBSIQIIITIIIT wave inversion in V2 V3ST segment depressionQr in V1 (pseudoinfarction pattern(RV dilation and dysfunction)ST segment elevation V1
Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Initial Management in Acute PEInitial Management in Acute PEHeparin 10000 U IV bolus and a continous infusion of Heparin 10000 U IV bolus and a continous infusion of 1250Uhr Target PTT of 80 sec1250Uhr Target PTT of 80 secJudicious use of IV fluids in patients with signs of RV Judicious use of IV fluids in patients with signs of RV dysfunction ( patient with JVD)dysfunction ( patient with JVD)
Aggressive fluid volume Aggressive fluid volume ndashndash increase RV stressischemia and increase RV stressischemia and further interventricular septal shift toward the LVfurther interventricular septal shift toward the LVFluids should be used with caution and early consideration Fluids should be used with caution and early consideration should be given to vasopressorsshould be given to vasopressors
NE appears to improve RV function by enhancing RV NE appears to improve RV function by enhancing RV CPPCPPDobutamine Dobutamine ndashndash use in moderate hypotensionuse in moderate hypotension
PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

PE PE mdashmdash Mortality based on Mortality based on hemodynamic presentationhemodynamic presentation
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
81
14
23
60
0 10 20 30 40 50 60 70
Group 1
Group 2
Group 3
Group 4
Mortality rate ()Mortality rate ()
Group 1 Group 1 -- APE + RV dysfunctionAPE + RV dysfunctionGroup 2 Group 2 -- APE + hypotensionAPE + hypotensionGroup 3 Group 3 -- APE + shockAPE + shockGroup 4 Group 4 -- APE + circulatory collapseAPE + circulatory collapse
204 German centers1001 consecutive patients204 German centers1001 consecutive patients
Kasper W et al Kasper W et al J Am Coll CardiolJ Am Coll Cardiol 1997301165 1997301165
Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Right ventricular dysfunction and acute PERight ventricular dysfunction and acute PE
Four PE registriesFour PE registriesInternational Cooperative Pulmonary Embolism Registry International Cooperative Pulmonary Embolism Registry CirculationCirculation 199796(Suppl I)I 199796(Suppl I)I--159159Ribeiro A et al Ribeiro A et al Am Heart JAm Heart J 1997134479 1997134479Kasper W et al Kasper W et al HeartHeart 199777346 199777346Management Strategy and Prognosis of Pulmonary Management Strategy and Prognosis of Pulmonary Embolism Registry (MAPPET)Embolism Registry (MAPPET)
Incidence of RV dysfunction in NAP Incidence of RV dysfunction in NAP ndashndash 4040MR with RVD MR with RVD ndashndash 3x that of patients without RVD3x that of patients without RVDRV hypokinesis in the presence of normal systemic RV hypokinesis in the presence of normal systemic pressure predicts an adverse clinical outcomepressure predicts an adverse clinical outcome
Methodologic LimitationsMethodologic LimitationsbullbullLack of standardized definition of RV dysfunctionLack of standardized definition of RV dysfunctionbullbullLack of information on initial hemodynamic presentationLack of information on initial hemodynamic presentationbullbullPotential patient selection bias Potential patient selection bias bullbullLack of outcome validation of PE related deathsLack of outcome validation of PE related deaths
Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Risk Stratification in APE Risk Stratification in APE -- SignificanceSignificance
Rationale of Risk Rationale of Risk StratificationStratification
Selecting appropriate initial Selecting appropriate initial therapytherapyIdentification of patients Identification of patients suspected pf CTEPHsuspected pf CTEPH
Assessment of RV functionAssessment of RV functionPhysical examPhysical examEchocardiogramEchocardiogramCardiac BiomarkersCardiac BiomarkersEKGEKG
Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Echocardiography in the Echocardiography in the diagnostic evaluation of acute PEdiagnostic evaluation of acute PE
RV pressure overloadRV pressure overloadR V dilationhypokinesisR V dilationhypokinesisIncreased RVLV diameter Increased RVLV diameter ratioratioParadoxical septal shiftParadoxical septal shiftTRTRPA dilationPA dilationLoss of inspiratory collapse Loss of inspiratory collapse (IVC)(IVC)PFOPFO
Alternative Diagnosis AMI tamponadeaortic dissection valvular disease hypovolemia
Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Cardiac Biomarkers and RVD
Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Troponin levels as a cardiac Troponin levels as a cardiac biomarker in acute PE biomarker in acute PE mdashmdash SummarySummaryElevated as a result of acute Elevated as a result of acute myocardial injurymyocardial injuryPrevalence in acute PE Prevalence in acute PE ndashndash 21 to 4421 to 44Elevated troponin levels correlated Elevated troponin levels correlated with RV dysfunctionwith RV dysfunctionElevated troponin levels predict Elevated troponin levels predict adverse outcomes in PEadverse outcomes in PE
Horlander KT Leeper KV Horlander KT Leeper KV Curr Opin Pulm MedCurr Opin Pulm Med 20039374 20039374
Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Risk Stratification In Pulmonary EmbolismRisk Stratification In Pulmonary EmbolismMortality Clinical State
6565 Cardiac ArrestCardiac Arrest
2525 ShockShock
1515 Hypotension Hypotension without without
hypoperfusionhypoperfusion
8181 Normal BP RV Normal BP RV dysfunctiondysfunction
00--11 Normal BP and Normal BP and RVRVData from MAPPET ndash Kasper JACC 1997 30 1165-1171
High Risk
Low Risk
Predictions
HistoryPExamDiagnostic
Studies
bull EKGbull CXRbull ABGbullD-dimerbullTroponinbull BNPbull EchoConfirmatory Studiesbull VQbull CT Angiobull Angio
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

CT Scan ImagesCT Scan Images
7 days after initial presentation 24 hours post-Activase administration
A B
Cases drawn from actual patients Individual results may vary
MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

MPE MPE mdashmdash Management Management ThrombolysisThrombolysis
FDAFDA--approved thrombolytic therapy regimens for PEapproved thrombolytic therapy regimens for PEStreptokinase (1977) Streptokinase (1977) ndashndash IV 250000 IU loading dose IV 250000 IU loading dose over 30 min followed by 100000 IUh for 24 hover 30 min followed by 100000 IUh for 24 hUrokinase (1978) Urokinase (1978) ndashndash IV 2000 IUlb loading dose over IV 2000 IUlb loading dose over 10 10 ndashndash 20 min followed by 2000 IUlbh for 12 or 24 h20 min followed by 2000 IUlbh for 12 or 24 hrtrt--PA (1990) PA (1990) ndashndash 100 mg as a continuous peripheral 100 mg as a continuous peripheral IV over 2 h IV over 2 h
Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Thrombolytic Therapy In Massive ( Major ) Pulmonary Thrombolytic Therapy In Massive ( Major ) Pulmonary Emboli The FactsEmboli The Facts
By various imaging modalities thrombolytic therapy By various imaging modalities thrombolytic therapy promoted more rapid clot lysis when compared to promoted more rapid clot lysis when compared to heparin in all clinical trialsheparin in all clinical trialsNo differnces in the effectiveness of thrombolytic agentsNo differnces in the effectiveness of thrombolytic agentsIV rtPA = intrapulmonary rtPAIV rtPA = intrapulmonary rtPABolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBolus rtPA (6mgkg over 15 min) = 100mg over 2 hrsBleeding complication can be considerableBleeding complication can be considerable
MAPPETMAPPETMajor hemorrhage Major hemorrhage ndashndash 2222Hemorrhagic stroke Hemorrhagic stroke ndashndash 1212Fatal Hemorrhage Fatal Hemorrhage ndashndash0606
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
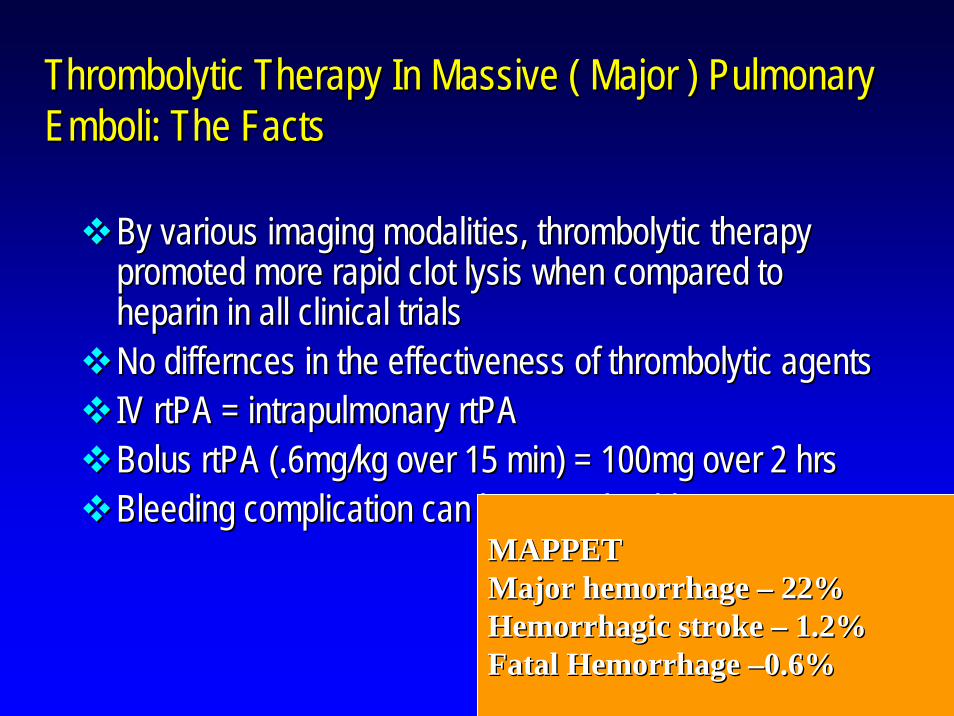
Wan S Thrombolysis vs Heparin a meta Wan S Thrombolysis vs Heparin a meta --analysis analysis ndashndash Subgroup Analyses Circulation Subgroup Analyses Circulation 20042004
94
19
53 48
02468
101214161820
Thrombolysis Heparin
Recurrent PE
or Death
Trials with MPETrials woMPE
511 Trials
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Surgical management of MPE Surgical management of MPE Pulmonary EmbolectomyPulmonary Embolectomy
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
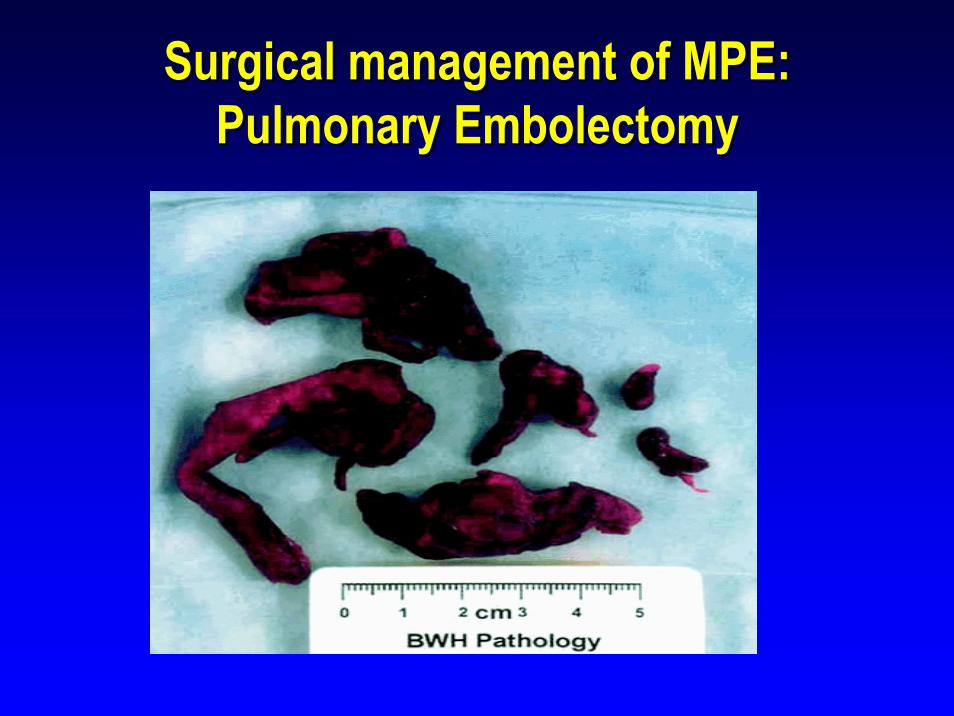
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism results of 47 consecutive patients after rapid diagnosis and results of 47 consecutive patients after rapid diagnosis and aggressive surgical approach Leacche M etal J Thorac aggressive surgical approach Leacche M etal J Thorac Cardiovasc Surg 20051291018Cardiovasc Surg 20051291018--2323
Indications for surgical embolectomy (n=47)Indications for surgical embolectomy (n=47)IndicationIndication N ()N ()
Contraindication to lysis 21 (45)Contraindication to lysis 21 (45)Failed medical treatment 10 (21)Failed medical treatment 10 (21)Large RA Large RA ndashndashRV thrombusRV thrombus 5 (10)5 (10)RV hemodynamic dysfuntion 15 (32)RV hemodynamic dysfuntion 15 (32)Large PFOLarge PFO 1 (2)1 (2)
Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Modern surgical management of massive pulmonary embolism Modern surgical management of massive pulmonary embolism Surgical Technique Leacche M etal J Thorac Cardiovasc Surgical Technique Leacche M etal J Thorac Cardiovasc Surg 20051291018Surg 20051291018--23 Results 23 Results --
Bilateral PE and main trunk Bilateral PE and main trunk 3947 (83)3947 (83)Left PA onlyLeft PA only 247 (4)247 (4)Right PA onlyRight PA only 647 (13)647 (13)Inserted IVC filtersInserted IVC filters 3847 (81)3847 (81)
MortalityMortalityEarly deaths ( within 30days)Early deaths ( within 30days) 347 (6)347 (6)Late actuarial survival Late actuarial survival (1 and 3 years) 86 83(1 and 3 years) 86 83
56 late deaths were diagnosed with cancer at time of embolectom56 late deaths were diagnosed with cancer at time of embolectomyy
CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

CatheterCatheter--Directed Thromboembolism Directed Thromboembolism FragmentationFragmentation
Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Mechanical and Enzymatic Thrombolysis For Massive PulmonarEmbolism De Gregorio etal J Vasc and Inter Rad 2002
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Non - Shock Establish DiagnosisVQ PA SCPT MRI)
Evidence of RV Dysfunctionbullgt30 perfusion defectbullEKG ndash RV strainbullEcho ndash Qualitative and Quantitative abnbullPositive Biomarkers
No evidence of RVD
Heparin
Evidence of RVD
Heparin + IVC vs Lysis
Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Therapeutic Approach Major Therapeutic Approach Major Pulmonary EmbolismPulmonary Embolism
Shock ndash PE Induced
Full Dose IV Heparin
Careful Fluid Adm
Vasopressor Rx
PE Diagnosis EstablishedEcho ndash TTE TEESCPTA
ThrombolysisContraindicated
CatheterSurgery Embolectomy
Thrombolysis
AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

AN 09282006AN 0928200681 yo female sp AVR one month ago81 yo female sp AVR one month agoHx COPD chronic aortic stenosis Hx COPD chronic aortic stenosis smokersmokerUpon discharge immediate SOB and Upon discharge immediate SOB and dyspnea on exertion with no follow updyspnea on exertion with no follow upCame for 30 day fu and admittedCame for 30 day fu and admitted
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
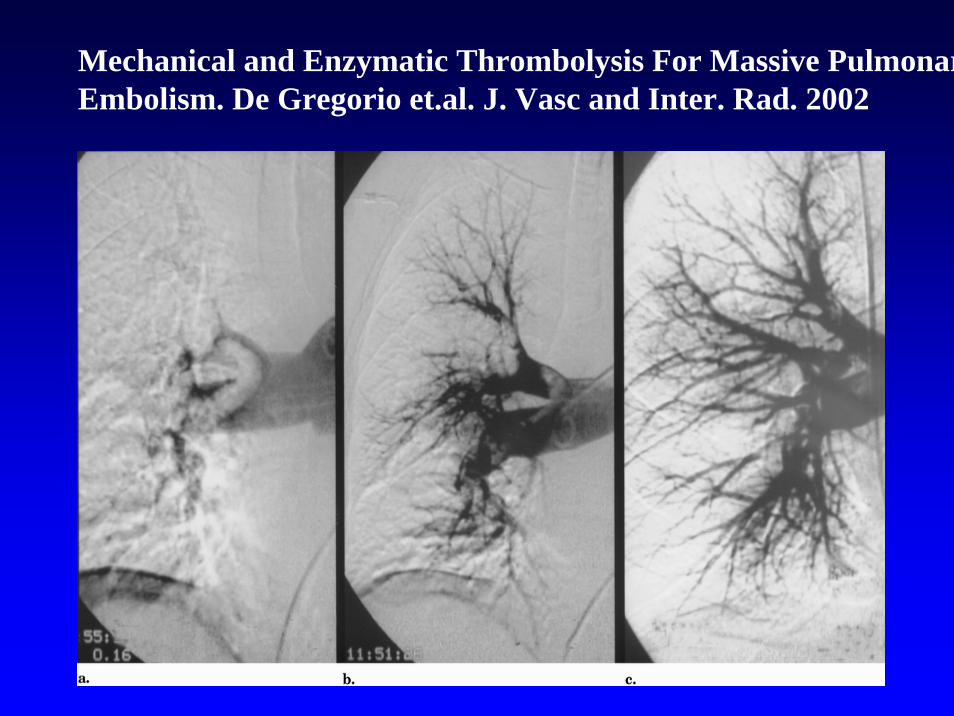
Prognostic role of echocardiography among patients with acute Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure4 of 90mm pulmonary embolism and a systolic arterial pressure4 of 90mm Hg or higher Kucher N etal Arch Intern Med 2005Hg or higher Kucher N etal Arch Intern Med 2005
1035 patients with PE from ICOPER with SBP gt90 1035 patients with PE from ICOPER with SBP gt90 mmHgmmHgEchocardiography within 24 hrsEchocardiography within 24 hrsRV hypokinesis RV hypokinesis ndashndash 405 absence of 405 absence of ndashndash 630630Main outcome measure Main outcome measure ndashndash 30 day cumulative 30 day cumulative survival ratesurvival rate
30 day MR 30 day MR ndashndash RV hypokinesis 163RV hypokinesis 163absence of RV Hypokinesis 94 P lt0001absence of RV Hypokinesis 94 P lt0001
RV hypokinesis was an independent predictor of 30 RV hypokinesis was an independent predictor of 30 day morality (HR 194)day morality (HR 194)
AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

AN 9282006AN 9282006
Respiratory distress in 21 ICURespiratory distress in 21 ICUBP 8945 122 resp rate 24BP 8945 122 resp rate 24Lungs clearLungs clearRV heave S1and S2RV heave S1and S2Ext no swellingExt no swelling
AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

AN 09282006AN 09282006
LLE Doppler positive for DVTLLE Doppler positive for DVTEchocardiogram Severe RV dilation Echocardiogram Severe RV dilation with moderate hypokinesiswith moderate hypokinesisTroponin Troponin ndashndash 041ngml041ngml
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
AN 9292006AN 9292006
Early AM underwent Early AM underwent ldquoldquoTrendelenberg Trendelenberg procedureprocedurerdquordquo with IVC filter placementwith IVC filter placementPost Post ndashndash op intubated op intubated ndashndash low dose NE low dose NE and milrinoneand milrinoneExtubated at 1130 AMExtubated at 1130 AMStarted Lovenox and Coumadin Started Lovenox and Coumadin
Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Defining Therapy for Life Threatening Defining Therapy for Life Threatening Pulmonary EmbolismPulmonary Embolism
Definition and prevalence of massive or life Definition and prevalence of massive or life threatening pulmonary embolismthreatening pulmonary embolismDiagnostic approach to major PEDiagnostic approach to major PEHemodynamic and respiratory Hemodynamic and respiratory pathophysiology pathophysiology ndashndash RV dysfunctionRV dysfunctionRole of thrombolysis in LTPERole of thrombolysis in LTPESurgical interventionsSurgical interventions
Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Short Term PE Related Mortality in Short Term PE Related Mortality in Patients with Normal RV on EchoPatients with Normal RV on Echo
Study Mortality PE DeathsPatients
Goldhaber 1993Goldhaber 1993 2323 00 00
Ribeiro 1997Ribeiro 1997 5656 00 00
ViellardViellard--BaronBaron 6363 00 00
Grifoni 2000Grifoni 2000 9797 00 00
TotalsTotals 239239 00 00
Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Outcomes Hemodynamically Stable Confirmed PE Outcomes Hemodynamically Stable Confirmed PE with RV Dysfunction Tx Heparinwith RV Dysfunction Tx Heparin
Study YearPE
Deaths
Mortalityn
GoldhaberGoldhaber 19931993 2323 22 8787GrifoniGrifoni 20002000 6161 33 55HamelHamel 20012001 6464 00 00GiannitsisGiannitsis 20002000 2626 22 7777Viellard BaronViellard Baron 20022002 3232 11 33PruszczykPruszczyk 20032003 6464 88 125125PruszczykPruszczyk 20032003 5151 1010 196196KucherKucher 20032003 1919 22 105105
340340 2828 8282
Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Brain Natriuretic PeptideBrain Natriuretic Peptide
Kucher Circ 2003 1072545-2547
BNP lt 90 BNP lt 90 pgmlpgml
8585 7575 9393 5757
BNP lt 50 BNP lt 50 pgmlpgml
9595 6060 9797 4848
Predictive Value Absent Adverse Event
Sensitivity Specificity Negative Positive
bull BNP gt 90 ngml independent predictor adverse (OR 80)
bull BNP lt 50 ngml rarr highly sensitive excellent negative predictive value
Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Spiral CT scan and RV dysfunctionSpiral CT scan and RV dysfunction431 patients with PE by CT431 patients with PE by CT4 chamber reconstruction4 chamber reconstructionRV enlargement RV enlargement ndashndash RVLV RVLV ratio gt09ratio gt09Prevalence of RV Prevalence of RV enlargement enlargement ndashndash 656530 day MR30 day MR
156 156 -- RVERVE77 77 -- NRVENRVEHR for predicting death HR for predicting death ndashndash517 fold for RVLVgt09517 fold for RVLVgt09
Schoepf UJ et al Cardiology 2004
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
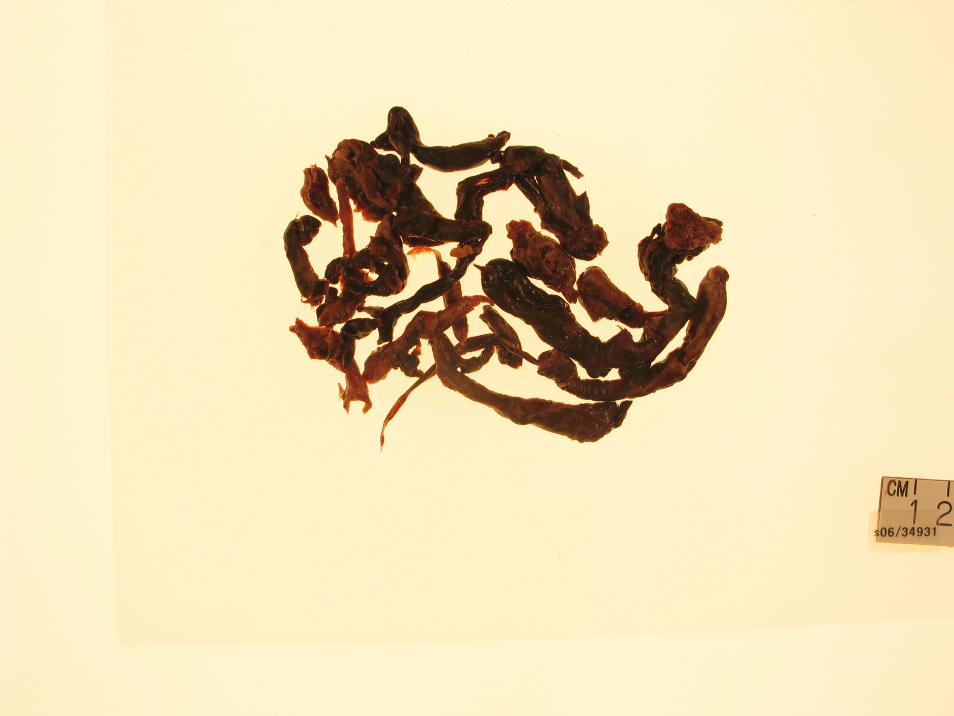
Concerns about Thrombolysis in APEConcerns about Thrombolysis in APE
The hemodynamic benefits of thrombolysis are The hemodynamic benefits of thrombolysis are fleetingfleetingThrombolysis potentially can be associated with Thrombolysis potentially can be associated with lifelife--threatening bleeding ratethreatening bleeding rateMaybe with the exception of massive PE with Maybe with the exception of massive PE with shock there is no direct evidence that thrombolytic shock there is no direct evidence that thrombolytic therapy reduces intherapy reduces in--hospital or longhospital or long--term mortality term mortality or rate of complications compared with heparin or rate of complications compared with heparin alonealone
Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Review of the recent literatureReview of the recent literaturethrombolytic therapy for acute PEthrombolytic therapy for acute PE
Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Should thrombolytic therapy be used in patients Should thrombolytic therapy be used in patients with RV dysfunction but hemodynamically stablewith RV dysfunction but hemodynamically stable
MAPPET Registry MAPPET Registry ndashndash HemodynamicallyHemodynamicallystable patients with RV dysfunctionstable patients with RV dysfunctionThrombolysis vs HeparinThrombolysis vs Heparin
Lower MR Lower MR ndashndash 47 vs 11147 vs 111Reduced rate of recurrent PE Reduced rate of recurrent PE ndashndash 77 vs 18777 vs 187Increase frequency of bleeding Increase frequency of bleeding ndashndash 219 vs 78219 vs 78
Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Heparin plus alteplase compared with heparin alone in Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolismpatients with submassive pulmonary embolism
Objective To compare thrombolytic therapy with Objective To compare thrombolytic therapy with heparin alone in patients with submassive PE PE heparin alone in patients with submassive PE PE with RV dysfunction without arterial hypotension or with RV dysfunction without arterial hypotension or shockshock256 patients Random assignment to 256 patients Random assignment to H + P (n = 138) vs H + A (n = 118)H + P (n = 138) vs H + A (n = 118)RV dysfunction One of the following RV dysfunction One of the following ndashndash RVE without RVE without inspiratory collapse of IVC or PH inspiratory collapse of IVC or PH ndashndash TRJV TRJV ndashndash 28 msec28 msecConfirmation of PE Confirmation of PE ndashndash VQ CT PAVQ CT PA
Konstantinides S et al Konstantinides S et al N Engl J MedN Engl J Med 20023471143 20023471143
Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Inhospital clinical eventsInhospital clinical eventsHeparin plusHeparin plus Heparin plusHeparin plus
alteplasealteplase placeboplaceboEventEvent (n = 118)(n = 118) (n = 138)(n = 138) PP valuevalue
n ()n ()Primary endpointPrimary endpoint 13 (110)13 (110) 34 (246)34 (246) 00060006Death from all causesDeath from all causes 4 (34)4 (34) 3 (22)3 (22) 071071Escalation of treatmentEscalation of treatment 12 (102)12 (102) 34 (246)34 (246) 00040004
Catecholamine infusionCatecholamine infusion 3 (25)3 (25) 8 (58)8 (58) 033033(for persistent hypotension or shock)(for persistent hypotension or shock)
Secondary thrombolysisSecondary thrombolysis 9 (76)9 (76) 32 (232) 32 (232) 00010001Endotracheal intubationEndotracheal intubation 3 (25)3 (25) 3 (22)3 (22) 085085Cardiopulmonary resuscitationCardiopulmonary resuscitation 00 1 (07)1 (07) 1010Embolectomy orEmbolectomy or 00 1 (07)1 (07) 10 10
thrombus fragmentationthrombus fragmentationSecondary endpointsSecondary endpointsRecurrent PERecurrent PE 4 (34)4 (34) 4 (29)4 (29) 089089Major bleedingMajor bleeding 1 (08)1 (08) 5 (36)5 (36) 029029
Fatal bleedingFatal bleeding 00 1 (07)1 (07) 1010Hemorrhagic strokeHemorrhagic stroke 00 00 mdashmdash
Ischemic strokeIschemic stroke 00 1 (07)1 (07) 1010
00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

00 55 1010 1515 2020 2525 3030
Number at riskNumber at riskHeparin + alteplaseHeparin + alteplase 118118 107107 9696 5757 2626 1111 66Heparin + placeboHeparin + placebo 137137 105105 8787 5353 2424 33 22
Days after randomizationDays after randomization
00
100100
9090
8080
7070
6060
5050
Prob
abilit
y of e
vent
Prob
abilit
y of e
vent
-- free
surv
ival (
)
free s
urviv
al (
)
Heparin + placeboHeparin + placebo
Heparin + alteplaseHeparin + alteplase
KaplanKaplan--Meier estimates of probability of eventMeier estimates of probability of event--free survival free survival among patients with acute submassive PE according to among patients with acute submassive PE according to
treatment with heparin plus alteplase or heparin plus placebotreatment with heparin plus alteplase or heparin plus placebo
Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Determination of the risk of inhospital Determination of the risk of inhospital death or escalation of treatmentdeath or escalation of treatment
Relative riskRelative riskVariableVariable (95 CI)(95 CI) PP valuevalue
Treatment with heparin + placeboTreatment with heparin + placebo 263 (132 263 (132 ndashndash 526)526) 00060006(vs heparin + alteplase)(vs heparin + alteplase)
Age gt 70 years (vs Age gt 70 years (vs lele 70 years)70 years) 229 (114 229 (114 ndashndash 460)460) 002002Female sex (vs male)Female sex (vs male) 268 (134 268 (134 ndashndash 536)536) 00050005Presence of previous or concomitant disease (vs absence)Presence of previous or concomitant disease (vs absence)
Cardiac diseaseCardiac disease 172 (082 172 (082 ndashndash 361)361) 015015Pulmonary diseasePulmonary disease 126 (065 126 (065 ndashndash 243)243) 048048Diabetes mellitusDiabetes mellitus 070 (036 070 (036 ndashndash 137)137) 030030
Systolic BP Systolic BP lele 100 mm Hg (vs gt 100 mm Hg)100 mm Hg (vs gt 100 mm Hg) 150 (032 150 (032 ndashndash 700)700) 060060Heart rate gt 100 beatsmin (vs Heart rate gt 100 beatsmin (vs lele 100 beatsmin)100 beatsmin) 142 (075 142 (075 ndashndash 268)268) 028028Respiratory rate gt 24 breathsminRespiratory rate gt 24 breathsmin 150 (078 150 (078 ndashndash 285)285) 022 022
(vs (vs lele 24 breathsmin)24 breathsmin)Presence of arterial hypoxemia (vs absence)Presence of arterial hypoxemia (vs absence) 357 (155 357 (155 ndashndash 820)820) 00030003
Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Heparin vs Lysis in Submassive PEHeparin vs Lysis in Submassive PE
70 70 NONO RV dysfunction via echoRV dysfunction via echo
No difference in mortality or recurrenceNo difference in mortality or recurrence
Escalation Tx Escalation Tx rarrrarr Heparin 25 vs lysis 102Heparin 25 vs lysis 102NOT catecholaminesNOT catecholaminesNOT intubationNOT intubationNOT CPRNOT CPRNOT embolectomyNOT embolectomySecondary thrombolysis for worsening respiratory Secondary thrombolysis for worsening respiratory symptomssymptoms
Konstantinides NEJM 2002 3471143Konstantinides NEJM 2002 3471143--5050
Selection bias Selection bias rarrrarr 256 pts49ctrs4yrs = 256 pts49ctrs4yrs = 125125 ptsctryrptsctryr
Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk

Role of Role of thrombolyticthrombolytic therapy in therapy in acute PEacute PE
PE with severe respiratory and PE with severe respiratory and hemodynamichemodynamicdeterioration should undergo deterioration should undergo thrombolysisthrombolysis if no if no contraindicationscontraindicationsConvincing evidence to suggest that the presence Convincing evidence to suggest that the presence of RV dysfunction identifies a subgroup of of RV dysfunction identifies a subgroup of normotensivenormotensive patients who potentially may have patients who potentially may have increase morbidity and mortalityincrease morbidity and mortalityPE PE thrombolysisthrombolysis rapidly improves PE rapidly improves PE ndashndash induced RV induced RV dysfunction dysfunction ndashndash benefit benefit vsvs riskrisk
Copyright © 2022 FDOKUMEN




















