
Mitral valve disruption following percutaneous balloon valvuloplasty

Functional Properties and Performance of New and Reprocessed
Coronary Angioplasty Balloon Catheters
Mariangela Fedel1, Francesco Tessarolo1, Paolo Ferrari2, Christian Lösche3,
Nikou Ghassemieh3, Giovanni Maria Guarrera4 and Giandomenico Nollo2,5
1 Department of Materials Engineering and Industrial Technologies, University of Trento, Trento, Italy
2 Department of Physics, University of Trento, Trento, Italy
3 Department of Research and Development, Vanguard AG, Berlin, Germany
4 Department of Care and Rehabilitation, Azienda Provinciale per i Servizi Sanitari, Trento, Italy
5 ITC-irst, Trento, Italy
Correspondence to:
Mariangela Fedel
Department of Materials Engineering and Industrial Technologies, University of Trento
Via Mesiano, 77
38050 Trento, Italy
Tel +39 0461 881594; Fax +39 0461 883952

Abstract
The need of health costs control has prompted the reuse of devices originally
manufactured for single use only. To assess reprocessing feasibility of disposable
medical devices, hygienic, technical, and functional aspects must be taken into account,
besides economical, ethical, and legal implications. This study aims to characterize
percutaneous transluminal coronary angioplasty catheters and to evaluate performance
changes induced by reprocessing. Multiple testing, including crossing profile,
slipperiness, compliance and burst pressure tests, were performed at different steps of
the protocol on 21 catheters, reprocessed up to two times.
The study highlighted that both clinical use and reprocessing procedures can affect
angioplasty catheters characteristics. Mechanical stress induced on balloon materials by
inflation during clinical practice, and thermal and chemical stresses undergone by
polymers during cleaning and sterilization procedures caused modifications of materials
response, inducing an overall shrinking effect. However, compliance tests showed the
conformity of reprocessed balloons with manufacturers original specifications within
the 10% limit of acceptance. The measured burst pressure of reprocessed devices was
80% higher than the rated burst pressure recommended by manufacturers, thus
removing any concern of breakage during reuse. A strict dependence on device model in
catheters behaviour was found, specifically for balloons crossing profile and
slipperiness. Main changes occurred after the first reprocessing cycle, while a second
cleaning and sterilization did not introduce further alterations. On the whole, the
magnitude of modifications introduced up to two reprocessing cycles did not
compromise in-vitro catheters performance.
Keywords: single use medical devices; PTCA catheters; reuse; reprocessing;
functionality tests.
INTRODUCTION
The rapid development of minimally invasive procedure for diagnosis and
therapy had led to a considerable increase in the cost of medical equipment. Many
medical devices, and in particular devices for interventional cardiology, are nowadays
placed on the market as Single Use Devices (SUDs). However, reuse of SUDs is
common practice in USA and Canada under specific regulatory frameworks by the
Food and Drug Administration (FDA)1,2 and by the Conseil d’Évaluation des
Technologies de la Santé du Quebec (CETS)3 respectively. On the other side, there is a
paucity of European studies on the practicability of reprocessing procedures4 and the
European juridical approach is still quite heterogeneous.
Percutaneous transluminal coronary angioplasty (PTCA) catheters, with more
than one million coronary interventions performed annually worldwide, are an example
of medical devices labelled by manufacturers as SUDs, with significant financial burden
on health services.5,6 Such devices are used to reopen coronary vessels clogged by
atherosclerosis, in order to restore a proper blood flow to the cardiac muscle. Balloon-
tipped catheters are threaded through the skin into the artery to reach the vascular
stenosis and inflated to expand the diameter of the occluded vessel. Although safeness
and efficiency of reused angioplasty catheters is debated, the practice of their
reprocessing is actually of large extent in western countries.7-13
In order to assure the safety of restored devices, the conformity to the intended
use and the equivalence of performance between new and reprocessed devices, both
hygienic and technical requirements must be satisfied.14-17 Possible modifications of
catheter materials and functional properties, that might occur during decontamination

and cleaning procedures with chemical aggressive agents or during EtO sterilization,
must be carefully evaluated.18 In the case of balloon coronary catheters, crossing profile,
balloon compliance, crossability and burst pressure are the most critical parameters that
describe devices functional behaviour.19-21 The assessment of such parameters is
therefore mandatory to certify a qualified reprocessing protocol for angioplasty
catheters.
This work aims to evaluate the functional properties of PTCA restored catheters
and to compare them respect to new devices specifications. With this purpose a
multifaced analysis of performances was carried out on new and reprocessed devices by
using specifically developed instrumentation and testing set-up.
MATERIALS AND METHODS
PTCA catheters
Modern rapid-exchange angioplasty catheters consist of a proximal stainless steel
hypotube and a polymeric (Polyamide/Polyethylene) double-lumen distal portion,
usually covered with an hydrophilic coating,22 ending with a dilating balloon.
Compliant and semi-compliant polymers are employed to produce catheters with
different specifications, such as balloon size (length and nominal diameter), compliance
(diameter vs inflation pressure) and operative pressure. Polymeric guiding catheters and
radio-opaque guide-wires are employed during clinical use to support the advancement
of balloons up to the lesion.
In this study 21 rapid exchange PTCA catheters from different manufacturers,
with variable balloon size (2.0–3.5 mm) and balloon length (10-30 mm), have been
tested. Nine catheters (hereafter referred as “new”) were taken from the shelf in sterile

original packages and twelve devices were collected from the catheterization laboratory
of the Department of Cardiology at S.Chiara Hospital, Trento, after clinical use on
patient (hereafter referred as “used”). As reported in Table I, new and used devices were
grouped according to manufacturer and size features. Seven catheters were reprocessed
once before destructive bursting test, while 14 were reprocessed twice. On the whole, a
total amount of 56 complete testing cycles was carried out.
Reprocessing Protocol
The reprocessing protocol consisted basically of two main steps: preconditioning
(decontamination and cleaning) and sterilization. Catheters were decontaminated by
immersion in Perfektan Endo (3% in water, 15 min), and Instru Plus (5% in water, 15
min). The cleaning was achieved with a special machine that repeatedly injected
detergent and disinfectant solutions at 55°C on catheter lumens and external surface.
Specific chemical agents for thermosensitive instruments, effective against bacteria,
fungi and virus (including HBV and HIV) were employed. Devices were then rinsed
with purified water and, finally, with sterile water. When completely dry, catheters
external surface was cleaned with a gauze soaked in disinfectant solution. Balloons
were then folded with a three-blade folding-machine, covered with a cap of suitable
dimensions, and double-wrapped in standard sterilization packaging. Due to the
complex design of the products, to the presence of long narrow lumens, and to the
thermal sensitivity of polymeric materials, Ethylene Oxide (EtO) was adopted as
elective technique for the sterilization (180 min at 6% EtO concentration, 94% CO2,
42°C, 1.7 bar).

Functional Tests
Crossing Profile. Crossing profile, defined as the diameter of the smallest
aperture that a folded catheter can cross, was measured by means of a laser scan
micrometer (ODAC® 32xy, Zumbach Electronics). The distal portion of the catheter
was positioned on a straight, rigid guide-wire while two perpendicular laser beams
scanned the balloon for the whole length without direct touching. As originary crossing
profile of used balloons could not be assayed, this test was performed only on new
devices (groups A-C) before and after reprocessing. Every device was tested three
times, and the crossing profile was calculated as the mean of the maximum values
registered during each single measurement.
Slipperiness. The sliding behaviour of the catheter during clinical intervention is
influenced by the interaction of the catheter with coronary vessels, guiding catheter and
guide-wire. The quantification of the friction forces exerted by balloon catheters was
accomplished by means of a special coronary vessel model23. This model, realized in
accordance with anatomic considerations, simulated the structure of an healthy right
coronary vessel with a properly shaped polyethylene sleeve (1.5 mm internal diameter).
The coronary model, and associated models of aorta and arteria femoralis, were
constantly maintained in water at body temperature (T=37°C) in order to reproduce
physiologic conditions.
Rapid exchange catheters were mounted on a guide-wire (0.014”, BBraun,
Melsungen AG) fixed at the and of the artificial vessel, and inserted in a guiding
catheter (7FR JR4 100cm, Vista Brite tip®, Cordis) acting as support track. PTCA
catheters were then clamped at their proximal end, advanced for 65mm into the
coronary vessel model by a stepper motor at a speed of 8 mm/sec, and withdrawn at the
same speed. Every catheter was tested three times, with a rotation of 120° over the
guide-wire at every advancement. Force transducers based on strain-gauge technology
were positioned in four critical points of the coronary vessel model (Figure 1) to
evaluate respectively insertion forces, support forces on the tip of the guiding catheter,
wall reaction forces and friction forces exerted on the guide-wire. As for the crossing
profile, slipperiness was measured only on new catheters (groups A-C), comparing data
before and after reprocessing.
Compliance. The compliance curve (balloon diameter vs inflating pressure),
was measured by a laser scan micrometer (ODAC® 32xy, Zumbach Electronics), as
used in crossing profile evaluation. Catheters were filled with water by means of an
automatic inflator at a rate of 0.7 atm/sec up to the nominal pressure and maintained at
this pressure for 15 sec. Balloon material underwent a gradual dilatation, reaching
saturation after some seconds. According to this behaviou,r and considering the mean
clinical inflation time, the experimental working diameter was collected 7 seconds after
the achievement of nominal pressure (Figure 2). As consecutive inflation cycles up to
the nominal pressure induced creeping and plastic deformation of balloon polymers, the
limit-diameter reached at the third inflation was assumed as representative of the
nominal diameter.
Burst Pressure. Manufacturers provide as pressure operative limit value the
rated burst pressure (RBP), defined as the maximum statistically guaranteed pressure
withstood by 99.9% of an inflated balloon with a 95% confidence level. To verify the
absence of leakages and the resistance to high pressure, catheters were inflated ten times

up to the RBP. Balloons were then finally brought to rupture and the burst pressure (BP)
value was registered as the maximum inflating pressure reached before bursting.
Statistical Analysis. To compare products with different features, in particular
with different balloon size and RBP, data collected after one and two reprocessing
cycles were normalized to theoretical nominal values when reported on the packaging,
and to measured reference values otherwise. Thus, per cent values were obtained,
assessing the increase or decrease of the physical quantities respect to the values for
new devices.
Continuous data were presented as the mean ± standard deviation. Continuous
variables were analysed using Kruskal-Wallis and Mann-Whitney U-test. P values
<0.05 were considered statistically significant.
RESULTS
Crossing Profile. After one reprocessing cycle, catheters showed a mean
increase in crossing profile of 29±18%. Partial deterioration of balloon folding after
reconditioning was assessed, in particular for larger balloons (Table II), but the degree
of changes was different for the various groups of devices tested. After the second
complete cycle of cleaning and sterilization, the crossing profile did not increase
significantly further on (33±18%).
Slipperiness. Figure 3 reports the typical behaviour of the force intensities
registered by the four different sensors during advancement and withdrawal of the
catheter into the coronary vessel model. Insertion force (Figure 3a) represents the most
important sliding feature, as it characterizes the friction actually felt by the clinician
during catheter positioning and could be related to intervention duration and efficacy.8,13
Each device presents a typical slipperiness curve that carries information about tip
conformation, friction exerted by radio-opaque markers, and materials stiffness and
flexibility.
The maximum force intensities registered during catheter advancement into the
bending artery-model were extrapolated and selected as meaningful parameter. Figure 4
summarizes the results and compares data relative to the different device classes (A, B1,
B2 and C). The maximum intensity of insertion force required to advance the catheter
was generally smaller than 1N, but distinct catheters classes presented different
characteristic values. Changes induced on catheters slipperiness by reprocessing
procedures were also strictly model related. The most significant variations between
new and restored devices occurred after the first reprocessing cycle, with an appreciable
decrease of 21±4% for the group A, and a variable increase up to about 22% for the
other groups. After the second reprocessing cycle, there were no further significant
modifications in the maximum strain applied during catheter insertion.
Support forces exerted on the tip of the guiding catheter, wall reaction forces,
and friction forces exerted on the guide-wire presented a similar trend (Figure 3b-d),
with variable dependence on the class of products tested. Withdrawal forces generally
showed the same behaviour as the relative forces registered during catheters
advancement and are not reported here for sake of brevity.
Compliance. New devices always presented smaller diameters when compared
to nominal values (Figure 5), ranging from –2.3±1.6% to –5.2±1.0%. Used catheters
tested before reprocessing exhibited a greater compliance than the new ones

(+1.5±2.8% ÷ -1.3±2.3% ), probably due to repeated inflation cycles over the nominal
pressure, as commonly performed in clinical practice. Apart from this offset, the
nominal diameter of new and used catheters followed the same trend during
reconditioning. After cleaning procedure balloons diameter experienced a first decrease.
Catheters underwent a further appreciable shrink at the end of the first complete
reprocessing cycle, but they did never exceed original specification limits. Neither new,
nor used balloons changed significantly their diameter at nominal pressure after a
second reprocessing cycle.
Burst Pressure. Three out of 21 catheters underwent fractures in the Luer-Lock,
and couldn’t therefore be tested for burst pressure. The tightness of these products was
compromised either by cracks or leakages in the Luer-Lock.
All the other catheters tolerated repeated inflations up to the RBP without
pressure leakages. The mean pressure required to reach bursting for regenerated
balloons was always largely above the RBP limits recommended by the manufacturers.
On the average, the burst pressure after one and two reprocessing cycles was
respectively 81±21% and 77±32% higher compared to the RBP reference values (Figure
6). No significant differences in burst pressure values between new and used catheters
were registered. PTCA catheters always burst causing long longitudinal fractures on
balloon walls, as previously documented,19,20 but no pinhole ruptures were detected.

DISCUSSION
This study aimed at testing recent models of PTCA catheters currently in use in
clinical practice. Devices from many manufacturers and with different nominal
specification have been selected, thus to consider a wide spectrum of the current market,
even though the number of new catheters tested was limited by the cost of the devices.
Due to the shortage of information from manufacturers about technical characteristics of
original products, and about the exact composition of materials employed, a first
analysis of new catheters was necessary to get a reference baseline for subsequent
comparisons with used and reprocessed devices.
By testing the most crucial functional parameters of PTCA catheters at different
steps of the reprocessing protocol, we evidenced that both use and regeneration process
can affect catheters behaviour and introduce functional changes at different degree. On
the whole, devices functionality up to the second reprocessing cycle was however
preserved.
Balloons refolding represented one of the most critical parameters for quality
control of reconditioned devices. Once deflated, balloons were unlikely to regain the
original crossing profile. The attempt to lower crossing profile by covering the balloon
with a plastic cap of proper diameter during sterilization did not always succeed and
sometimes originated wrinkles in balloon wings. Anyway, higher crossing profile does
not necessarily mean lower catheter crossability or increased difficulty in catheter
positioning. As highlighted by the slipperiness measurements performed in the
coronary-vessel model, no direct correlation seem to exist between the friction forces
registered during catheters advancement/withdrawal and the diameter of folded

balloons. On the contrary, catheter sliding features proved to be model related, as
recently evidenced by Brown et al.19 In our study, force profiles seemed to be affected
by constructive characteristics, as flexibility of catheter shaft, tip conformation and
lubricious polymer properties, rather than by reprocessing procedures.
Inflation tests proved that semi-compliant polymers used for balloons
manufacturing, slowly adapted to pressure increase and a creeping effect of balloon
materials was registered. The compliance of used catheters showed to depend on the
total strain applied, that is to say, on the number and duration of inflations and on the
maximum pressure sustained during intervention. The need to dilate hard-calcified
atherosclerotic plaques during clinical use may lead to exceede the nominal pressure,
thus causing an overstretching of the balloon, with consequent loss of elasticity of the
polymeric material.
Cleaning and resterilization procedures could, on the other side, introduce
thermal and chemical stresses on materials,24 affecting balloons diameter. Compliance
tests documented an appreciable shrinking of balloons at the first reprocessing, that did
not increase significantly after a second cleaning and sterilization.
Several studies reported the effects of EtO on polymeric biomaterials.25
According to some authors, EtO could generate structural modifications by oxidizing
the polymeric chains.26 Despite this hypotheses, other studies found that repeated
exposure of polyethylene catheters to EtO had no significant effect on their mechanical
strength.27,28 Balloon materials shrinking reported in this work could be caused by
exceeding the glass transition temperature of balloon polymers during automatic
cleaning, or by chemical action of the agents employed in decontamination and
cleaning. Nevertheless, it is noteworthy to report that diameter variations induced by
reprocessing did never exceed the limit of variability given by manufacturers for new

products, (usually certified as 10% of the nominal values). On the average, a maximum
diameter decrease of 5.2±1.0% was reached after reprocessing. By these considerations
we want to underline that compliance tests, if performed regularly on each device, can
provide more precise information about the functionality of the single product, whether
new or reprocessed.
Bursting of both new and used balloons after one or two reprocessing cycles was
achieved at pressure values approximately 80% higher than the RBP certified by
manufacturers. The wide gap between experimental and nominal bursting pressure
seems to assure a large safety margin. Moreover, bursting pressure is a device specific
feature and seems not to be affected by multiple reprocessing. The presence of hard
calcified coronary plaques represents however a possible cause of damages on balloon
surface, that could not be tested in-vitro.
The leakages in the Luer-Lock that affected three devices, underlined the
weakness of this part of the catheter, and could be related to materials quality (intended
for single use only) or to the reprocessing technique.
A first inspection by means of conventional microscopy is fundamental to detect
leaks, kinks or lumen obstructions and to reject macroscopically damaged catheters
before starting reprocessing procedure.
Further clinical trials are required to relate in-vitro and in-vivo performance of
reprocessed catheters and to evaluate the possibility of clinical complications to take
place. The present study for the assessment of PTCA catheters performance was, in fact,
completely conducted in-vitro, thus providing a potential limitation. As reported in
some recent clinical study, there is however little evidence of increased risks related to
balloon catheters reprocessing. According to some authors, reuse strategy is in fact not
associated with increased procedure time or worsening of other procedural
variables.8,9,12,13
CONCLUSIONS
This study aimed to assess PTCA catheters performance before and after
reconditioning. Testing performed during this trial on angioplasty catheters succeeded
in characterizing both new and reprocessed devices. Crossing profile, slipperiness,
compliance and burst pressure proved to be relevant parameters to describe functional
properties of balloon catheters.
Devices response to reprocessing showed to be highly related to the model of
catheter tested. This result supports the statement that, for safe reusing, each product
should undergo individual evaluations to establish the conformity of restored devices
with nominal performance. A reprocessing facility, whether represented by hospital or
third-party reprocessor, should thus hold suitable laboratories to validate regeneration
procedures and to perform methodically adequate and up-to-date testing and quality
controls.
Nevertheless, further clinical trials need to be carried out in order to assess the
degree of importance of the functional changes induced by use and reprocessing, and to
establish whether catheter modifications could negatively affect clinical practice in
terms of procedure time or adverse clinical events.
Acknoledgments
This work was supported by SICC-SIX Project financed by Fondo Unico per la Ricerca
2001, Provincia Autonoma di Trento.

The authors would like to acknowledge the staff of the Hemodynamics Laboratory at
the S. Chiara Hospital, Trento, for catheters retreival.
Running Heads: Functional properties of reprocessed PTCA catheters

REFERENCES
1. U.S. Department of Health and Human Services Food and Drug Administration
Center for Devices and Radiological Health. FDA proposed strategy on reuse of
single-use devices. Updated November 1, 1999. Available at
http://www.fda.gov/cdrh/comp/guidance/1168.pdf
2. U.S. Department of Health and Human Services Food and Drug Administration
Center for Devices and Radiological Health. Medical device user fee and
modernization act of 2002, validation data in premarket notification submissions
(510(k)s) for reprocessed single-use medical devices; Guidance for industry and
FDA staff. Issued June 1, 2004. Available at
http://www.fda.gov/cdrh/ode/guidance/1216.pdf
3. Conseil d’Evaluation des Technologies de la Santé du Québec. The reuse of
single-use cardiac catheters: safety, economical ethical and legal issues. Can J
Cardiol 1994;10:413-421.
4. Fecht G. Requirements for reprocessing single-use medical devices. Zentr Steril.
1998;6:12-27.
5. Milandri M, Saviotti M. Reuse of single-use catheters: a dilemma to be clarified.
G Ital Cardiol. 1994;24:1175-1186.
6. Lesh MD. Cost efficacy modeling of catheter reuse for percutaneous
transluminal coronary angioplasty. J Am Coll Cardiol. 1996 Nov 15;28(6):1640-
1641.
7. Plante S, Strauss BH, Goulet G, Watson RK, Chisholm RJ. Reuse of balloon
catheters for coronary angioplasty: a potential cost-saving strategy? J Am Coll
Cardiol. 1994;24:1475-1481.
8. Mak KH, Eisenberg MJ, Plante S, Strauss BH, Arheart KL, Topol EJ. Absence
of increased in-hospital complications with reused balloon catheters. Am J
Cardiol. 1996;78:717-719.

9. Shaw JP, Eisenberg MJ, Azoulay A, Nguyen N. Reuse of catheters for
percutaneous transluminal coronary angioplasty: effects on procedure time and
clinical outcomes. Cathet Cardiovasc Intervent. 1999;48:54-60.
10. Bourassa MG. The reuse of single-use balloon angioplasty catheters: is it now
legitimate? Am J Cardiol. 1996;78:673-674.
11. Burton J, Tymchak W, Dzavik V, Lucas A, Muzyka T, Hogg N, Yim R,
Montagne T, Teo K. Randomized controlled trial of reuse of PTCA balloon
catheters. Circulation. 1995;92(suppl I):I-661.
12. Zubaid M, Thomas CS, Al-Rashdan I, Hayat N, Habashi A, Abraham MT,
Varghese K, Thalib L. A randomized study of the safety and efficacy of reused
angioplasty balloon catheters. Indian Heart J. 2001;53:167-171.
13. Browne KF, Maldonaldo R, Telatnik M, Vlietstra RE, Brenner AS. Initial
experience with reuse of coronary angioplasty catheters in the United States.
JACC. 1997;30:1735-1740.
14. Mak KH, Eisenberg MJ, Eccleston DS, Cornhill JF, Topol EJ. Reuse of
coronary angioplasty equipement: technical and clinical issues. Editorial. Am
Heart J. 1996;131:624-630.
15. Grimandi G, Sellai O, Grimandi F, Crochet D. Risks of reusing coronary
angioplasty catheters: results of an experimental study. Cathet and Cardiovasc
Diagn. 1996;38:123-130.
16. Robert Koch Institute and Federal German Institute for Medical Drugs and
Medical Products. Hygienic requirements for processing of medical devices.
Hyg Med. 2001;26-Heft 12.
17. Krause G, Dziekan G, Daschner FD. Reuse of coronary angioplasty balloon
catheters: yes or no? Eur Heart J. 2000;21:185-189.

18. Karov J, Chawla AS, Hinberg I. Effect of reuse on surface characteristics of
balloon angioplasty catheters. Art Cells Blood Subs Immob Biotech.
2000;28:229-240.
19. Brown SA, Merritt K, Woods TO, Hitchins VM. The effects of use and
simulated reuse on percutaneous transluminal coronary angioplasty balloons and
catheters. Biomed Intrum Technol. 2001;35:312-322.
20. Unverdorben M, Quaden R, Werner C, Bloss P, Degenhardt R, Ackermann H,
Vallbracht C. Change of the mechanical properties of two different balloon
catheters with increasing numbers of cycles of resterilization. Catheter
Cardiovasc Interv 2003;58:29-33.
21. Marmieri G, Pettenati M, Cassinelli C, Morra M. Evaluation of slipperness of
catheter surfaces. J Biomed Mater Res (Appl Biomater). 1996;33:29-33.
22. Park S, Bearinger JP, Lautenschlager EP, Castner DG, Healy KE. Surface
modifications of Poly(ethylene terephtalate) angioplasty balloons with a
hydrophilic poly(acrylamide-co-ethylene glicol) interpenetrating polymer
network coating. J Biomed Mater Res (Appl Biomater). 2000;53:586-576.
23. Kraft M, Schmitz H, Schulte R, Boenick U. Multifunctional testing of PTCA
catheters. Biomed Tecknik 2000;45:146-153.
24. Granados DL, Jimenez A, Cuadrado TR. Assessment of parameters associated
to the risk of PVC catheter reuse. J Biomed Mater Res. 2001;58:505-510.
25. Hermanson NJ, Navarrete LY, Crittenden P. The effects of high energy and EtO
sterilization on thermoplastics. Med Device Diagn Ind Mag. 1997 (August) 1-9.
26. Zapf S, Thelen M. Possibilities and limitations of preparation for reusing
angiography catheters. Dtsch Med Wochenschr 1988;113:1117-1120.
27. Zapf S, Muller K, Haas L. Reuse of angiography catheters. II - Effect of
multiple sterilization on the properties of the catheter material - Physiochemical
studies. Röntgen-Blätter 1987a;40:154-158.

28. Bentolia P, Jacob R, Roberge F. Effects of reuse on the physical characteristics
of angiographic catheters. J Med Eng Technol. 1990;14:254-259.

FIGURE CAPTIONS
Figure 1.
Simplified schematic representation of the coronary-vessel set-up for the quantification
of catheters slipperiness. The geometrical structure of the coronary-vessel model
simulated the anatomy of an healthy right coronary branch. The four sensors positioned
along the path of the PTCA catheter measured, respectively, the force exerted during
catheter advancement/withdrawal (A), the support force on the tip of the guiding
catheter (B), the reaction force of the coronary-model wall (C), and the friction force on
the guide-wire (D).
Figure 2.
Balloon inflation protocol (lower panel) and typical compliance curve (upper panel).
Catheters were inflated at 0.7 atm/sec up to the nominal pressure and maintained at this
pressure for 15 sec. Subseqent inflating cycles showed shift in compliance curve;
according to this behaviour, experimental diameter values were collected at the third
inflation cycle, 7 sec after the achievement of nominal pressure.
Figure 3.
Forces exerted during advancement (0-65 mm) and withdrawal (65-130 mm) of the
PTCA catheter in the coronary vessel model. As depicted in Figure 1: (a) insertion
forces, (b) support forces on the tip of the guiding catheter, (c) wall reaction forces and
(d) friction forces exerted on the guide-wire. Arrows indicate the maximum values
registered by each sensor, that are summarized in Figure 4.
Figure 4.
Comparison among maximum forces intensity of new and reprocessed catheters for
groups A, B1, B2 and C (Tab 1). Data were measured during catheter advancement in
the coronary-vessel model: (a) insertion force, (b) support force on the tip of the guiding
catheter, (c) wall reaction force, (d) friction force exerted on the guide-wire.
Reprocessing did not seem to critically affect catheters sliding behaviour, but
slipperiness properties show to be highly dependent on device classes.
Figure 5.
Effects of cleaning and reprocessing on balloon working diameter. Experimental
diameters were normalized to the nominal specifications. Data refer to new devices (a),
and to products used once on patients (b). Both new and used catheters underwent a
progressive shrinking, but working diameter changes were always below the 10% error
bar certified by manufacturers.
Figure 6.
Mean burst pressure (BP) of balloon catheters subjected respectively to one and two
reprocessing cycles. Data are normalized to the rated burst pressure (RBP) values
provided by manufacturers. Reprocessing seems not to affect bursting pressure, as the
breaking point value did not change significantly from first to second cycle and was
always markedly higher than the nominal value.
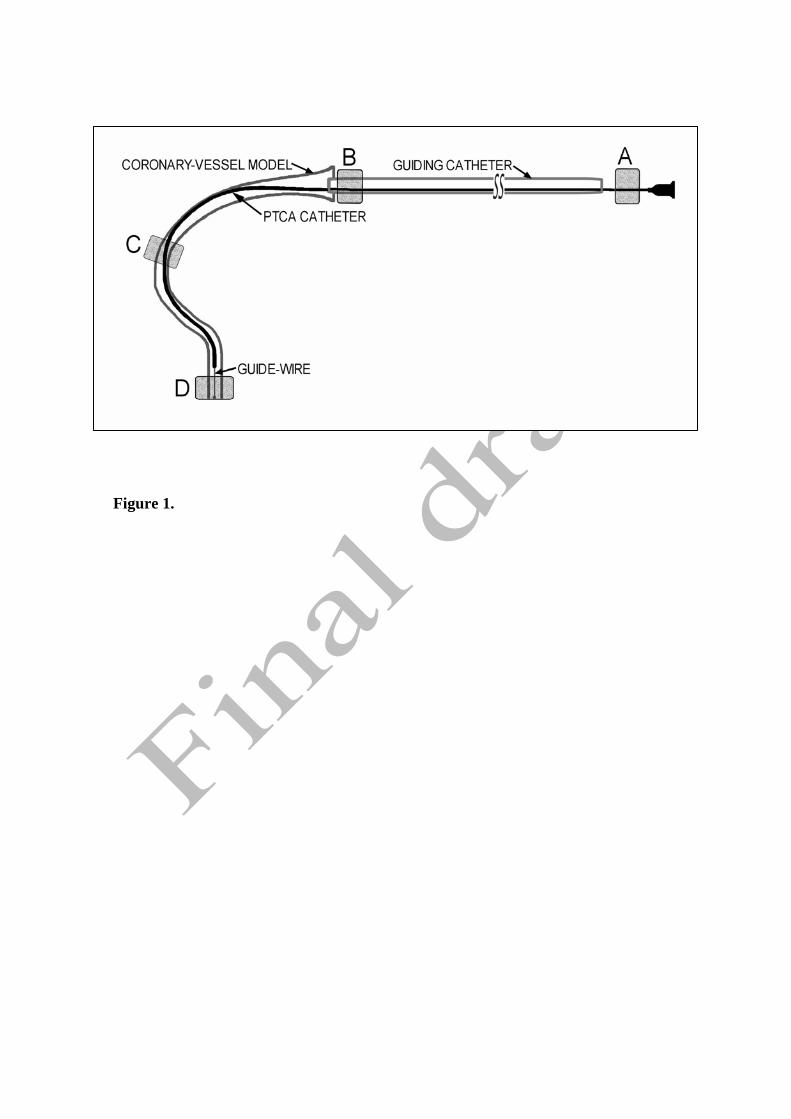
Figure 1.

Figure 2.
2,5
2,6
2,7
2,8
2,9
3,0
0 5 10 15 20 25 30
t (s)
D (m
m)
1st inflation2nd inflation3rd inflation
0246
0 5 10 15 20 25 30t (s)
P (a
tm)
Inflation Stopping
Data Acquisition
Inflation
2,5
2,6
2,7
2,8
2,9
3,0
0 5 10 15 20 25 30
t (s)
D (m
m)
1st inflation2nd inflation3rd inflation
0246
0 5 10 15 20 25 30t (s)
P (a
tm)
Inflation Stopping
Data Acquisition
Inflation

Figure 3.
(a) (b)
(c) (d)
-1,5
-1,0
-0,5
0,0
0,5
1,0
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,8
-0,4
0,0
0,4
0,8
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,3
-0,2
-0,1
0,0
0,1
0,2
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,4
-0,2
0,0
0,2
0,4
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
(a) (b)
(c) (d)
-1,5
-1,0
-0,5
0,0
0,5
1,0
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,8
-0,4
0,0
0,4
0,8
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,3
-0,2
-0,1
0,0
0,1
0,2
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,4
-0,2
0,0
0,2
0,4
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
(a) (b)
(c) (d)
-1,5
-1,0
-0,5
0,0
0,5
1,0
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,8
-0,4
0,0
0,4
0,8
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,3
-0,2
-0,1
0,0
0,1
0,2
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
-0,4
-0,2
0,0
0,2
0,4
0 20 40 60 80 100 120Displacement (mm): 0-65 advancement / 65-130 withdrawal
F (N
)
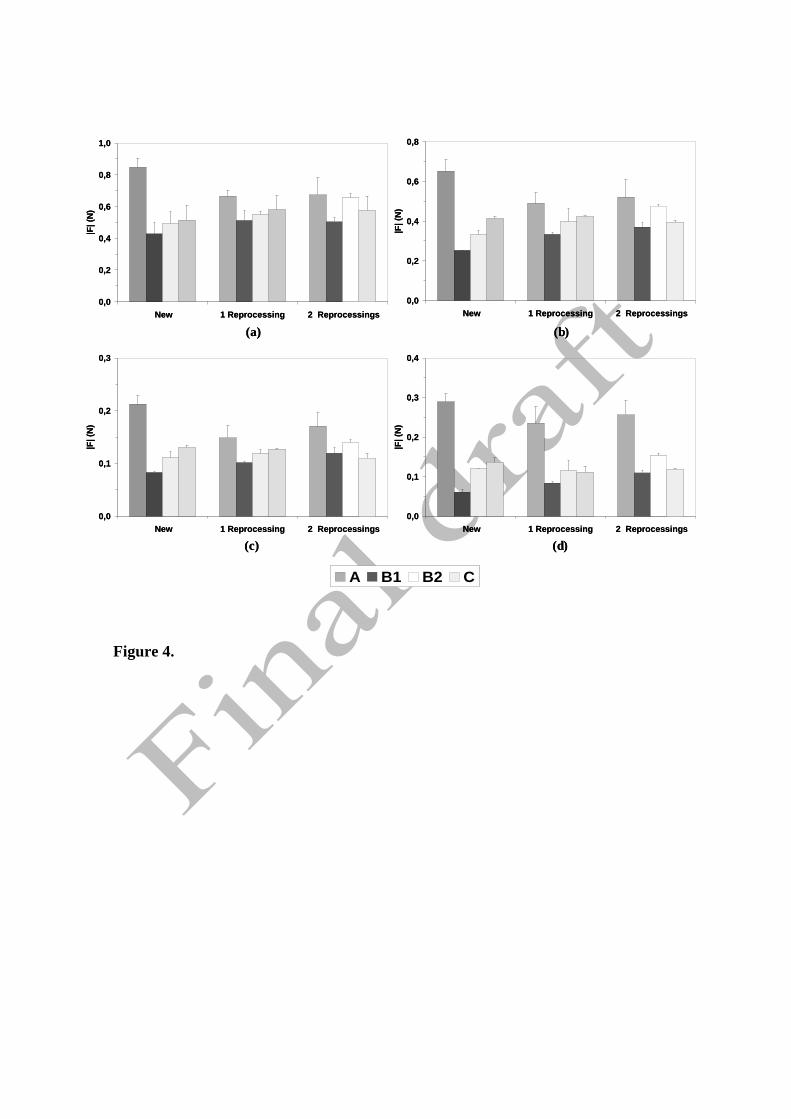
Figure 4.
(a) (b)
(c) (d)
0,0
0,2
0,4
0,6
0,8
1,0
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,2
0,4
0,6
0,8
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,1
0,2
0,3
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,1
0,2
0,3
0,4
New 1 Reprocessing 2 Reprocessings
|F| (
N)
A B1 B2 C
(a) (b)
(c) (d)
0,0
0,2
0,4
0,6
0,8
1,0
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,2
0,4
0,6
0,8
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,1
0,2
0,3
New 1 Reprocessing 2 Reprocessings
|F| (
N)
0,0
0,1
0,2
0,3
0,4
New 1 Reprocessing 2 Reprocessings
|F| (
N)
A B1 B2 C

(a)
(b)
D = experimental working diameter
ND = nominal diameter
Figure 5.
-8
-6
-4
-2
0
New 1 Cleaning 1 Reprocessing 2 Reprocessings
(D-N
D)/N
D %
-4
-2
0
2
4
6
First use 1 Cleaning 1 Reprocessing 2 Reprocessings
(D-N
D)/N
D %

BP = Burst Pressure
RBP = Rated Burst Pressure
Figure 6.
76,6 %81,5 %
0
20
40
60
80
100
120
1 Reprocessing 2 Reprocessings
((BP-
RB
P)/R
BP)
%
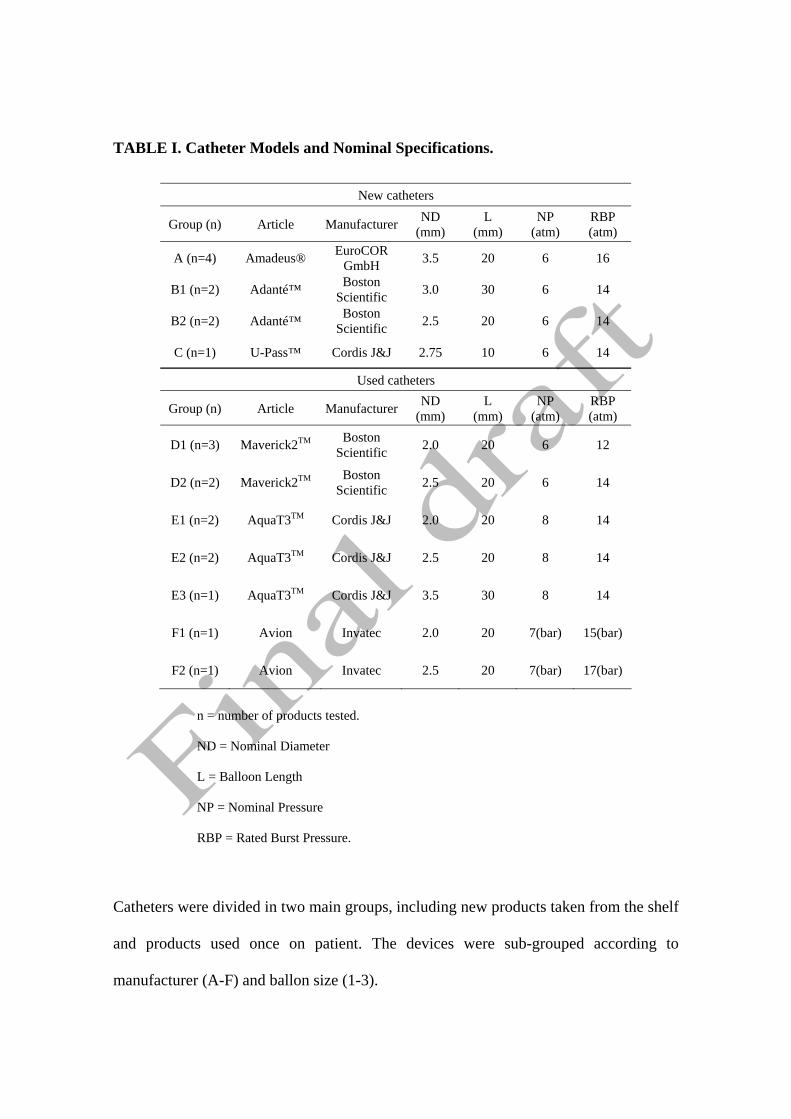
TABLE I. Catheter Models and Nominal Specifications.
n = number of products tested.
ND = Nominal Diameter
L = Balloon Length
NP = Nominal Pressure
RBP = Rated Burst Pressure.
Catheters were divided in two main groups, including new products taken from the shelf
and products used once on patient. The devices were sub-grouped according to
manufacturer (A-F) and ballon size (1-3).
New catheters
Group (n) Article Manufacturer ND (mm)
L (mm)
NP (atm)
RBP (atm)
A (n=4) Amadeus® EuroCOR GmbH 3.5 20 6 16
B1 (n=2) Adanté™ Boston Scientific 3.0 30 6 14
B2 (n=2) Adanté™ Boston Scientific 2.5 20 6 14
C (n=1) U-Pass™ Cordis J&J 2.75 10 6 14
Used catheters
Group (n) Article Manufacturer ND (mm)
L (mm)
NP (atm)
RBP (atm)
D1 (n=3) Maverick2TM Boston Scientific 2.0 20 6 12
D2 (n=2) Maverick2TM Boston Scientific 2.5 20 6 14
E1 (n=2) AquaT3TM Cordis J&J 2.0 20 8 14
E2 (n=2) AquaT3TM Cordis J&J 2.5 20 8 14
E3 (n=1) AquaT3TM Cordis J&J 3.5 30 8 14
F1 (n=1) Avion Invatec 2.0 20 7(bar) 15(bar)
F2 (n=1) Avion Invatec 2.5 20 7(bar) 17(bar)

TABLE II. Crossing Profile of New and Reprocessed Devices.
Group New (mm)
1 Reprocessing (mm)
2 Reprocessings (mm)
A 1.02±0.05 1.50±0.02* 1.57±0.10*
B1 0.99±0.05 1.02±0.01 1.16±0.05
B2 1.07±0.01 1.44±0.12 1.37±0.01*
C 0.94±0.01 1.24±0.02* 1.25±0.01*
* P<0.05 vs new balloon (U-test)
Crossing profile of PTCA catheters reprocessed once and twice, compared to new
devices. P values <0.05 were considered statistically significant.
Running Heads:
Functional properties of new and reprocessed PTCA catheters.
Copyright © 2022 FDOKUMEN




















