
Thermal characteristics of sapphire contact probe delivery systems for laser angioplasty
Upload
independentCategory
view
0download
0
From Peripheral to Coronary Dynamic Angioplasty: Analysis of Resulting Particles
ABDURRAZZAK ABDULKADER GEHANI, M.B., M.R.C.P., F.A.C.A., *STEPHEN GEOFFRY BALL, F.R.C.P., PHD., KEITH STOODLEY, PHD., SIMON ASHLEY, F.R.C.S., STEPHEN GERALD BROOK, F.R.C.S., and MICHAEL RALPH REES, M.R.C.P., F.R.C.R., F.I.C.A.
From the Cardiac Research Unit, Killingbeck Hospital, und the *Depariment of Curdiovusculur Studies, University nf Leeds, Leeds, United Kingdom
The factors that could reduce the size of particles generated by peripheral (8 Fr) and coronary 15 Fr) Kensey catheters (KC) in calcfied and noncalcified atheroma were investigated. Fresh endarterectomy specimens (72 calcqied, 72 noncalcijied) were inserted in a flow circuit and randomized to iindergo simulated dynamic angioplasty using 5 Fr or 8 Fr KC at a range of predetermined cam speeds (20,000- 80,000 rpm) andflow rates (18-60 mllmin) . Atherectomy as measured by weight loss from the specimen was greater in noncalcified lesions, 21.4 * 4.5 mg and 14.9 ? 3.8 mg, respectively (P < 0.001). In calcified atheroma, the atherectomy was asymmetrical in 38 out of 72 specimens but in onb 12 of 72 noncalcified lesions ( P < 0.01). Overall, 65% ? 3.9% of collected particles were smaller than 5 p m and 86.8% 2 9.1% were smaller than 35 pm. In the remaining 13.2% k 8.9% of particles larger than 35 pm, signijicant differences were detected between the maximum particle size in each group. Larger particles were generated from calcified atheroma. In noncalcified lesions, increasing cam speed re- duced maximum particle size from 890 to 170 pm ( P < 0.001). Although a higher.flow1 rate and the use of 5 Fr catheter have also significantly reduced the particle size, their effect was less than that exerted by cam speed. In calci$ed atheroma, cam speed was the only factor obJrrved to influence the maximal particle size, reducing it f rom 1,260 to 381 pm (P < 0.001). In conclusion, allhorrgh the majority of particles resulting from the use of KC were small, a proportion of large particles was also detected. Their size could br signi5cantly reduced by carefil adju ytment of the operating parameters. These results are important for future application of KC in coronary dynamic angioplasty . However, the impact of reducing particle size on the risk oj embolism in vivo requires jiirther study. (J Interven Cardiol 1991 :4:2)
Introduction
Dynamic angioplasty using Kensey catheter (KC; Kensey Nash Corp., Exton, PA, USA) is a percutaneous technique designed to recanalize chronic arterial occlusions where balloon angio- plasty often fails.’.* It “pulverizes” the occlusive atheroma into “smaller” particle^,^ the size of
Address for reprints: A. A. Gehani, M.B., Cardiac Research Unit, Killingbeck Hospital, York Road, Leeds LS14 6UQ, U.K. Fax: 0532-609483.
Submitted for publication October 10, 1990; accepted with revisions December 18, 1990; revisions returned January 9, 1991.
which has been the subject of some ~ i e b a t e . ~ . ~ This attains further importance as 5 Fr KC is now proposed for coronary use. Investigation into the factors that could reduce particle size is partic- ularly relevant for future application of this tech- nique.
The clinical consequences of embolic debris in vivo will depend on several factors, the size of particles, the vessel’s diameter and tone,’ and efficacy of collateral circulation.6
Can the size of particles generated by KC be reduced? There is no detailed information re- garding the influence of various operating con- ditions on particle size. The manufacturer’s
Vol. 4, No. 2, 1991 Journal of Interventional Cardiology 91

GEHANI, Er AL.
Figure 1. Kensey catheter tip. (A) A circumferential vortex is created by high pressure fluid jet and fast rotating cam. This is thought to pulverise atheroma during atherectomy. (B) Size 8 Fr “peripheral” and 5 Fr “coronary.”
guidelines regarding the use of this device are relatively arbitrary and most operators follow their instinct in the absence of an objective in- vestigation.
Although an in vivo study would be ideal, the catheter does not retrieve generated debris, which makes collection of particles during clin- ical use difficult. An experimental model was de- signed to simulate dynamic angioplasty in vitro. This is the first systematic study into the effect of the operating parameters on the particle size, using peripheral (8 Fr) and coronary (5 Fr) cath- eters.
Material and Methods
The KC has a fast rotating cam at its tip. Fluid is injected under high pressure to exit under the cam as a circumferential jet (Fig. 1A). An 8 Fr
and a 5 Fr size KC were used in this study (Fig. 1B). Fresh samples of occlusive atheroma were obtained from surgical endarterectomy and trans- ported in tissue culture medium with antibiotics at 4°C. They were screened using X rays for evi- dence of calcification. Calcified and noncalcified atheroma were allocated in two groups and used within 1-6 hours.
Generation of Particles. All samples were im- mediately rinsed in saline and divided into small specimens of 0.5-1 cm in length. Each was mop dried and weighed before it was gently inserted in a flow circuit (Fig. 2). The circuit was then primed with normal saline for a few minutes to wash all debris resulting from handling of the specimen. A snare was placed on the outside of the sheath below the level of the atheroma to pre- vent its movement during the procedure.
Each specimen was randomized to undergo a simulated dynamic angioplasty using 5 Fr or 8 Fr
Journal of Interventional Cardiology Vol. 4, No. 2, 1991 92

ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
I) Motor (r.P.m) Angio-pump
(mf/min)
(5Fr or 8Fr)
-11 C F I n w
the extent of atherectomy achieved in 10 sec- onds, Each experiment was repeated three times.
A control group of 24 specimens (12 calcified and 12 noncalcifiedj was handled in an identical manner but without activation of the catheter.
Effect of Duration of Reexposure on Particle Size. Does continuing exposure to the rotating cam breakup the particles any further?
When in contact with the occlusive atheroma, the cam creates two distinct populations of par- ticles. While new "large" particles are continu- ously generated from the atheroma, it is claimed that existing debris is broken further. Therefore, to investigate the effect of the duration of ex- posure on ultimate particle size, a population of particles had to be isolated to prevent new and large particles from being constantly added from the atheroma. Twelve specimens (six calcified and six noncalcified) were treated with an 8 Fr KC at a cam speed of 80,000 rpm and a flow rate of 60 mL/min for a control period of 10 seconds. Two mL of the collected debris was used to de-
Particles in suspension Figure 2. The setup used for simulated dynamic angioplasty. To generate particles, the catheter tip is lowered vertically (downward arrow) and engaged into the atheromatous tissue. The snare below the atheroma prevents its progression during the procedure.
catheter at a predetermined cam speed of 20, 40, 60, or 80 thousand rpm. The catheter was also flushed using a high pressure injector pump at a flow rate of 16, 36, or 60 mL/min. The catheter was introduced into the sheath through the valve cap and advanced toward the atheroma. When in contact, the device was activated at the preset speed and flow rate, and gentle forward pressure was applied as in clinical cases. This was contin- ued for 10 seconds.
Clean tubes containing 0.5 mL of 1% buffered gluteraldehyde (pH = 7.4) were used to collect the effluent fluid. At the end of the procedure, the snare was removed and the remaining ath- eroma and debris were flushed out into the col- lecting tube. The atheroma was then removed, rinsed, mop dried, and weighed again to deter- mine the amount of weight loss, which represents
7 L-tube /r I
i
I Glass slide
Direction of centrifugal force
Figure 3. L-tube used to spin the debris. The centrifugal force drives the particles toward glass microscopy slides.
Vol. 4, No. 2, 1991 Journal of Interventional Cardiology 93

GEHANI, ET AL.
Computerised Edge Detection Technique
H . R. Cam era
Acquisition (Im age display)
r===il
Figure 4A. Computerised edge detection technique. The particles on glass slide are filmed by high resolution camera and displayed on a monitor. Satisfactory images were fed into a computer for image analysis.
terminc the particle size at the end of the 10 sec- onds. The rest was then transferred into clean arterial sheaths and reexposed to the catheter for a further 30 or 60 seconds. The final particle size was determined and compared to that at the end of the initial 10 seconds.
Preparation of Particles for Size Measurement. All debris was centrifuged at 50g for 10 minutes and the supernatant separated. The particles in the sediment were resuspended in 2 mL of saline and spread over microscopy glass slides. The su- pernatant (containing smaller particles) was placed in special L-shaped tubes and spun using a dedicated centrifuge (Shandon Cytospin-2; Shandon, Inc., Pittsburgh, PA, USA) at lOOg for 20 minutes. In this device, the centrifugal force
drives all particles to stick on microscopy slides fitted to the side opening of the tube (Fig. 3).
To enhance the adherence of the particles, all slides were pfetreated with aminopropyl trie- thoxy silane7 and sprayed with Cytofix (water soluble wax; Lip Cell-Fix, Ltd., Shipley, UK) before they were left to dry. The particles were stained with Leishman stain and covered with a coverslip.
Particle Size Measurement. The computerized edge detection technique (Magiscan 11, Joyce- Loeble, Dukesway, Gateshead, UK) was used to analyze the size of the particles (Fig. 4A). The slides were placed under a light microscope, which was attached to a high resolution camera. The images were displayed on a computer screen
94 Journal of Interventional Cardiology Vol. 4, No. 2, 1991

ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
To answer the question whether KC abrades the calcified components in the atheroma, debris from calcified lesions was mounted on slides and stained using Van-Kossa (silver nitrate) stain and then examined under a light microscope for evi- dence of calcium crystals.
Statistics. All values were expressed as a range or mean 2 SD. Analysis of variance for a three- way design (catheter size, cam speed, and flow rate) with replications was used to test the sig- nificance of the effect of each on calcified and noncalcified atheroma (Fisher’s F-test). Previ- ously selected comparisons between subgroups within this design were carried out using t- and Chi-square tests. A P value of < 0.05 was con- sidered significant.
Figure 4B. Particles on the screen monitor. The edge of each particle is determined before its dimensions are measured.
(Fig. 4B). This allows the exclusion of unsatis- factory images, e.g., artifacts or overlapping par- ticles that may otherwise be counted as one “large” particle.
The approved image was then fed into a com- puter that was programmed to detect the precise edge of each particle and measure its size. Two diameters of each particle were measured at per- pendicular axes (Fig. 5) . This adds valuable in- formation about the geometry of the particles. However, the largest of the two diameters was used to express and compare the particle size in different specimens. Histograms were generated from which calculations of the percentage of par- ticles for each size were made.
The measuring system was calibrated using a scored grid before every session.
Light and Scanning Electron Microscopy. De- bris obtained from four additional specimens (two calcified and two noncalcified) treated at a cam speed of 40,000 rpm and flow rate of 36 mL/ second were dedicated for morphological study. The debris was filtered using 35 km filters that were sequentially dehydrated to absolute alco- hol. After critical point drying, they were splut- ter-coated with colloidal gold (Nanotech Thin Films, Ltd., Manchester, UK) and studied with a scanning electron microscope (GL-JSM T20 Japanese Electron-Optics, Ltd., Tokyo, Japan).
Figure 5. The longest diameters in two perpendicular axes were measured to express the “geometry” of each particle.
Vol. 4, No. 2 , 1991 Journal of Interventional Cardiology 95
GEHANI, ET AL.
Results
One hundred forty-four endarterectomy spec- imens were subjected to simulated dynamic an- gioplasty (72 noncalcified and 72 calcified). Twenty-four control specimens were handled in an identical manner but without the activation of the catheter. The effects of two size catheters (5 Fr and 8 Fr), four cam speeds, and three flow rates were investigated.
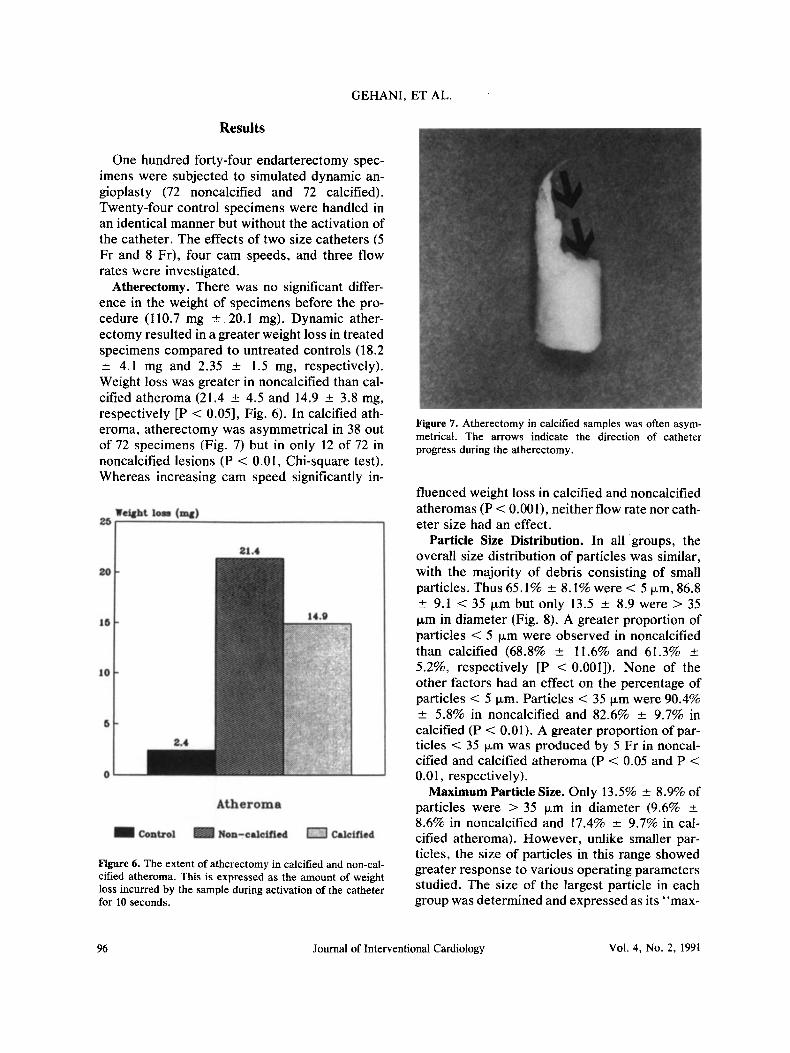
Atherectomy. There was no significant differ- ence in the weight of specimens before the pro- cedure (110.7 mg * 20.1 mg). Dynamic ather- ectomy resulted in a greater weight loss in treated specimens compared to untreated controls (18.2 k 4.1 mg and 2.35 -t 1.5 mg, respectively). Weight loss was greater in noncalcified than cal- cified atheroma (21.4 k 4.5 and 14.9 k 3.8 mg, respectively [P < 0.051, Fig. 6). In calcified ath- eroma, atherectomy was asymmetrical in 38 out of 72 specimens (Fig. 7) but in only 12 of 72 in noncalcified lesions (P < 0.01, Chi-square test). Whereas increasing cam speed significantly in-
Figure 6. The extent of atherectomy in calcified and non-cal- cified atheroma. This is expressed as the amount of weight loss incurred by the sample during activation of the catheter for 10 seconds.
Figure 7. Atherectomy in calcified samples was often asym- metrical. The arrows indicate the direction of catheter progress during the atherectomy.
fluenced weight loss in calcified and noncalcified atheromas (P < 0.001), neither flow rate nor cath- eter size had an effect.
Particle Size Distribution. In all groups, the overall size distribution of particles was similar, with the majority of debris consisting of small particles. Thus 65.1% 2 8.1% were < 5 pm, 86.8 ? 9.1 < 35 pm but only 13.5 & 8.9 were > 35 pm in diameter (Fig. 8). A greater proportion of particles < 5 pm were observed in noncalcified than calcified (68.8% 2 11.6% and 61.3% 5.2%, respectively [P < O.OOl]). None of the other factors had an effect on the percentage of particles < 5 pm. Particles < 35 pm were 90.4% * 5.8% in noncalcified and 82.6% ? 9.7% in calcified (P < 0.01). A greater proportion of par- ticles < 35 pm was produced by 5 Fr in noncal- cified and calcified atheroma (P < 0.05 and P < 0.01, respectively).
Maximum Particle Size. Only 13.5% -e 8.9% of particles were > 35 Fm in diameter (9.6% 2 8.6% in noncalcified and 17.4% 2 9.7% in cal- cified atheroma). However, unlike smaller par- ticles, the size of particles in this range showed greater response to various operating parameters studied. The size of the largest particle in each group was determined and expressed as its “max-
96 Journal of Interventional Cardiology Vol. 4, No. 2, 1991

ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
Y of particlea 100
90
80
70
60
50
40
30
20
10
0
p <o. 00 1
a5Um
pco.01
(35Um 1
p<O.OOl
335Um
Particle size (Microns)
Non-calcified Calcified atheroma
Figure 8. Overall particle size distribution; p values signify the difference between calcified and non-calcified atheroma. The latter produced smaller particles.
Maximum Particle Size (Urn) 1400
1200
1000
800
600
400
200
0 Non
p < O . O O l
Calcified A th erom
20K 40K
Calcified A th eroma
60K 80K
CAM SPEED (x1000 RPM)
Figure 9. Effect of cam speed on particle size. This was sig- nificant in both types of atheroma.
imum particle size.” This was 1,260 pm in cal- cified and 890 pm in noncalcified atheroma (P < 0.01). In noncalcified atheroma, increasing the cam speed from 20 to 80 thousand rpm reduced the maximum particle size from 890 to 170 pm (P < 0.001). In calcified atheroma, increasing cam speed reduced the maximum particle size from 1,260 to 381 km (P < 0.001) (Fig. 9).
Higher flow rate significantly reduced maxi- mum particle size in noncalcified (P < 0.001) but not in calcified atheroma (Fig. 10). Maximum particle size was significantly smaller using “cor- onary” 5 Fr than 8 Fr KC (P < 0.001); however, this difference was not significant at all cam speeds (Fig. 1 1 ) . The effects of flow rate and cath- eter size on maximum particle size were of smaller magnitude than that exerted by the cam speed.
In both types of atheromas, the effect of in- creasing cam speed and flow rate on maximum particle size was not linear (Figs. 9 and 10). Al- though a minimum speed of 40,000 rpm was re- quired to produce an effect on maximum particle size, a lower cam speed was required to produce
I000
800
600
400
200
0
laximum Particle
p <0.001
ize (Um) I
Non -Calcified Atheroma Calcified Atheroma
Flow Rate
Figure 10. Effect of flow rate on particle size. Flow rate sig- nificantly affected the particle size only in non-calcified ath- eroma.
Vol. 4, No. 2, 1991 Journal of lnterventional Cardiology 97

to00
800
600
400
200
0
GEHANI, ET AL.
Maximum Particle Size (Urn) N. S N. S
20K 40K 60K
N. S
80K
CAM SPEED (x1000 RPM)
8Fr 5Fr Figure 11. 5 Fr “coronary” catheter produced smaller particles than 8 Fr. This difference was dependent on cam speed. N.S = not significant.
an optimal effect by 5 Fr than 8 Fr (60 and 80 thousand rpm, respectively [Fig. 91).
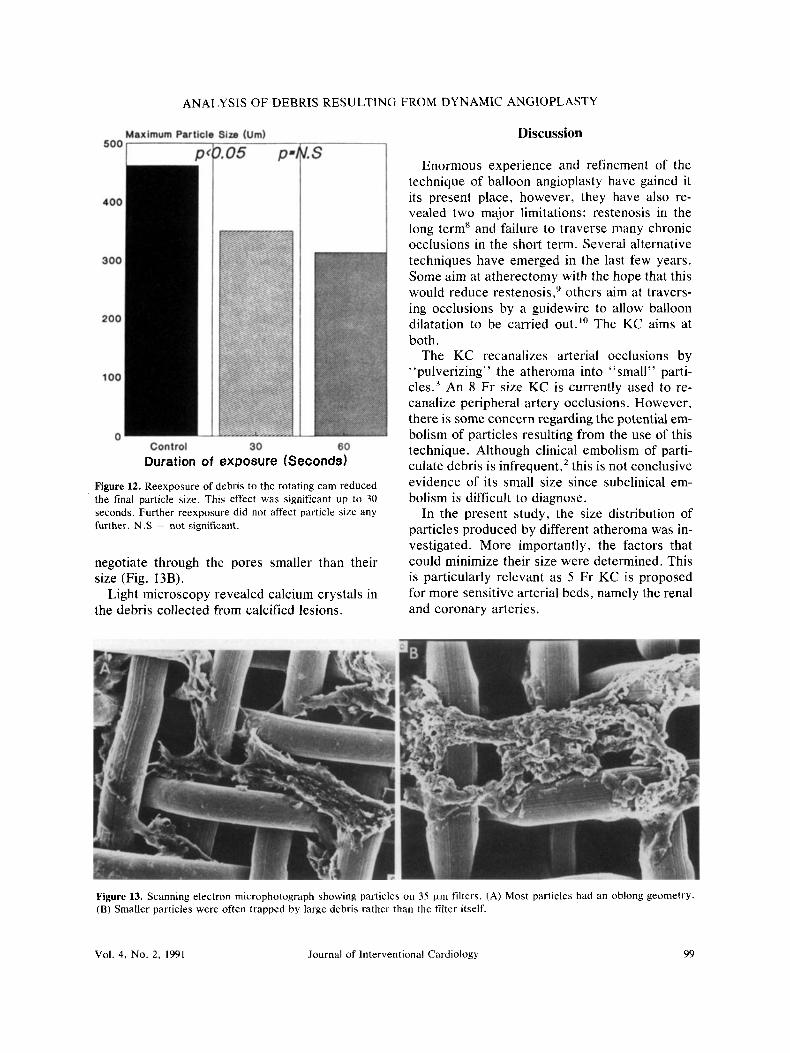
Effect of Duration of Exposure on Particle Size. Two durations were used, 30 and 60 seconds. The ultimate maximum particle size was compared with that after the initial 10 seconds control pe- riod. Reexposure of particles to the rotating cam reduced their size. In noncalcified specimens, the maximum particle size was significantly different between control and 30 seconds (462 5 65 prn and 350 2 73 pm, respectively [P < 0.051). Ex- tending the duration of reexposure to 60 seconds did not significantly reduce the particle size any further (313 f 95 pm [P = 0.41, Fig. 12). In- creased duration had no consistent effect on the size of particles obtained from calcified ather- oma.
Particles larger than 1.5 mm were observed in 8 out 144 specimens (six calcified and two non- calcified). These were larger than the maximum particle size expected from similar aliquots
treated at an identical cam speed and flow rate. All eight were among specimens subjected to 8 Fr catheters and at cam speeds <40,000 rpm but occurred at high and low flow rates. None were observed in the group treated by 5 Fr.
Geometry of Particles. In the majority of the particles, the diameter in one axis was at least twice that in the other. This suggests that most particles were oblong in shape since these two diameters were measured along perpendicular axes (Fig. 5). In the present study, the larger of the two diameters was used to express the par- ticle size unless otherwise indicated.
Light and Scanning Electron Microscopy. Nu- merous fragments were detected. The particles appeared as thin flakes, most were irregular but generally oblong (Fig. 13A). Although large de- bris was trapped by the filter, many small par- ticles were entangled by larger particles rather than by the filter itself. The particles showed a degree of deformability and some were able to
Journal of Interventiondl Cardiology Vol. 4, No. 2, 1991 98
ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
Duration of exposure (Seconds)
Figure 12. Reexposure of debris to the rotating cam reduced the final particle size. This effect was significant up to 30 seconds. Further reexposure did not affect particle s i x any further. N .S not significant.
negotiate through the pores smaller than their size (Fig. 13B).
Light microscopy revealed calcium crystals in the debris collected from calcified lesions.
Discussion
Enormous experience and refinement of the technique of balloon angioplasty have gained it its present place, however, they have also re- vealed two major limitations: restenosis in the long term’ and failure to traverse many chronic occlusions in the short term. Several alternative techniques have emerged in the last few years. Some aim at atherectomy with the hope that this would reduce restenosis,’ others aim at travcrs- ing occlusions by a guidewire to allow balloon dilatation to be carried out.” The KC aims at both.
The KC recanalizes arterial occlusions by “pulverizing” the atheroma into “small” parti- cles.3 An 8 Fr size KC is currently used to re- canalize peripheral artery occlusions. However, there is some concern regarding the potential em- bolism of particles resulting from the use of this technique. Although clinical embolism of parti- culate debris is infrequent,’ this is not conclusive evidence of its small size since subclinical em- bolism is difficult to diagnose.
In the present study, the size distribution of particles produced by different atheroma was in- vestigated. More importantly, the factors that could minimize their size were determined. This is particularly relevant as 5 Fr KC is proposed for more sensitive arterial beds, namely the renal and coronary arteries.
Figure 13. Scanning electron microphotograph showing particles on 3.5 kni filters. (A) Most particles had an ohlong geometry. (B) Smaller particles were often trapped by large debris rather than the filter itself.
Vol. 4, No. 2, 1991 Journal of lnterventional Cardiology 99

GEHANI, ET AL.
Need for an Experimental Model. The KC has no mechanism for retrieving particles that ren- ders in vivo collection of particles difficult. Therefore, this study had to be carried out in vitro. Although this may represent a limitation, the model used allows simulated dynamic angio- plasty to be performed on selected samples of atheroma under controlled conditions. Such con- trol is crucial for any conclusions to be made re- garding the influence of cam speed, flow rate, duration of exposure, and type of atheroma on particle size. Some investigators have used am- putated legs4; however, it is often difficult to ex- clude debris from the surgical field from contam- inating the collected specimens. A similar prob- lem would be faced in vivo.
Atherectomy. The speed of atherectomy was assessed by the amount of weight loss during 10 seconds of catheter activation. Clinically, the ad- vance of the catheter should match the speed of atherectomy to minimize the risk of perforation. Atherectomy was significantly faster in noncal- cified than calcified lesions where the atherec- tomy was often asymmetrical. The cause of this asymmetry is not clear. The presence of calcium crystals in the debris from calcified lesions sug- gest that the catheter does abrade calcified areas. However, the asymmetry may reflect uneven cal- cification. The catheter may bounce off heavily calcified areas and follow the path of least resis-
A similar phenomenon was observed with laser-thermal angioplasty . I ’ These findings may partly explain the relative tendency of these de- vices to cause dissection and perforation in cal- cified occI~sions.~ Higher cam speed resulted in a faster atherectomy, however, the catheter should be advanced at a much slower pace in than in noncalcified lesions. Although there was no significant difference in the amount of atherec- tomy produced by 5 Fr and 8 Fr catheter, the latter is likely to produce a larger channel, which may make subsequent passage of a guidewire eas- ier. Weight loss resulting from KC is comparable to that observed with the laser when delivered for similar duration.’* However, while KC con- verts all atheroma into particles, part of the weight loss observed with laser was due to water evaporation.
Aminopropyl Triethoxy Silane. Secure reten- tion of particles on the slides during preparation
and staining is essential. All slides were pre- treated with 2% aminopropyl triethoxy silane, a technique that was originally used by Van Prooi- jen-Knegt et aI.I3 to enhance chromosome spreading on glass slides. It was modified by Ren- trop et al.’ who found the technique equally ef- fective for frozen and formalin fixed sections. Aminopropyl triethoxy silane provides glass sur- faces with aminoalkyl groups that are capable of forming strong bonds with the appropriate func- tional groups in the tissue section.’ In an initial pilot experiment, we found a significantly greater amount of particles retained on pretreated than ordinary slides.
Clinical Implications. The grouping of particles into < 5 or 35 pm is not entirely arbitrary. Five pm represent the mean capillary size while pre- capillary arterioles are around 35 pm.I4 Particles < 5 pm constituted the largest proportion. These are presumably small enough to pass through all but the smallest of capillaries. Ahn et aI.l5 la- belled particles of 2-20 pm diameter (produced by rotablator) and injected them into canine fem- oral arteries. Lung, liver, and spleen were the sites where most radioactivity was detected. Minimal counts were found in the legs but with- out evidence of ischemia.” About one fifth of analyzed debris was 5-35 pm. Particles in this range are unlikely to pass the capillary net. How- ever, Zacca et a1.I6 have injected debris of up to 180 prn (produced during mechanical atherec- tomy) into porcine coronary arteries in vivo. They detected no evidence of coronary occlusion or myocardial infarction, l6 However, reduction of particle size is likely to reduce the incidence and extent of embolism related infarction.
Although particles larger than 35 pm made up < lo%, reduction of their size is important since they pose the greatest occlusive risk. In noncal- cified lesions, modifying several parameters re- duced particle size including, in order of mag- nitude, increasing cam speed, flow rate, and using 5 Fr instead of 8 Fr size. The 5 Fr catheter did not only produce an overall smaller particles than 8 Fr, but a lower speed was required for an optimal effect. The availability of factors besides cam speed may be important since higher speeds are associated with increased risk of perfora- tion.’’ Using higher flow rate and 5 Fr catheter allows reduction of cam speed, and therefore im-
100 Journal of Interventional Cardiology Vol. 4, No. 2, 1991

ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
proved safety, without an appreciable increase in particle size.
Larger particles were produced by calcified than noncalcified lesions. This is in agreement with the results of other investigator^.^ Although calcification is not under the operator’s control, its identification calls for the manipulation of the only means that could reduce particle size, namely increasing cam speed. However, this should be used with great caution.” Particles larger than 1.5 mm have been r e p ~ r t e d . ~ Their occurrence in our series was rare and unpredict- able. They were unexpectedly large when com- pared to particles produced by aliquot specimens treated in identical manner. The reason for this is not clear, however, they seem lo be associated with the use of low cam speeds in calcified ath- eroma.
Percutaneous angioscopy following dynamic angioplasty has often revealed potential debris in the form of loosely attached intimal fragments.” The embolic potential of these flaps have not been studied; however, when large enough to ob- struct blood flow they occasionally have been successfully ablated using laser energy. l 9
Coleman et al.4 showed that the injection of particles resulting from an 8 Fr catheter into ca- nine coronary and renal arteries lead to focal in- farcts. A 5 Fr rather than 8 Fr KC is the suitable size for these arteries and our results show that 5 Fr catheter produced significantly smaller de- bris. Furthermore, the cam speed and flow rate used were below that required to produce an op- timal reduction of particle size. However, the im- pact of these differences on the extent of focal infarction in vivo remains to be shown.
Computerized edge detection as means of quantitative measurement has been widely used in cellular biology and in quantitative cinean- giography to evaluate coronary stenoses.’*~’’ Computerized edge detection and scanning elec- tron microscopy suggest that most particles were oblong in shape. While all calculations were based on the largest diameter, it could be argued that blood flow would align the particles to ne- gotiate the artery with the smaller of the two di- ameters, thus posing a lower occlusive risk than suggested by our analysis. This may also explain why particles that theoretically should occlude microcirculation have often escaped. l 6 However,
the intention of the present study was to find means that may reduce the maximal embolic po- tential that corresponds to the maximum particle size.
Filters of varying pore diameter have been used to separate particles produced by other an- gioplasty devices. ’’ However, the scanning elec- tron microscopy observations suggest that this may not be an accurate method of classifying par- ticles by size. Particles smaller than the filter pores were often trapped by large debris rather than by the filter itself.
Effect of Duration of Exposure on Particle Size. It has been claimed that the reexposure of the particles to the rotating cam emulsifies the par- ticles f ~ r t h e r . ~ Although this was confirmed, it appears to be related to duration of exposure, possibly due to the way in which the particles interact with the rotating cam. It was observed that particles were initially drawn toward the cam, which lead to significant reduction in par- ticle size. However, as the vortex became estab- lished, the particles were simply spun parallel to the cam. The duration of reexposure of particles in vivo will depend on blood flow and rate of clearance of debris away from the angioplasty site. Both are likely to be slower in occlusions than normal or stenotic segments.
Particles Resulting From Other Angioplasty De- vices. Embolic debris can result from all inter- ventional procedures, including bypass sur- gery.’2 Although balloon angioplasty does not of necessity produce debris similar to KC, down- stream embolization of plaque fragments large enough to occlude arteries has been observed.23 Atheromatous debris and embolism can also re- sult from laser ang i~p las ty .~~ . ’~ However, unlike the results of the present study, there are no re- ports on the effect of the type or the amount of laser energy delivered on the size of particles pro- duced.
For some lasers, the thermal effect on blood is another potential source of embolic debris.I2 Gaseous byproducts have been reported as a re- sult of laser ablation; their effect however, is thought to be in~ignificant.~~
Some atherectomy devices retrieve the ex- cized atheroma. In the Simpson catheter (De- vices for Vascular Intervention, Redwood City, CA, USA), these are stored in a metal housing
Vol. 4, No. 2, 1991 Journal of lnterventional Cardiology 101

GEHANI, ET AL.
while the transluminal extraction catheter uses plasty of total arterial occlusions. Br J Sum 1990: continuous vacuum suction. l o However, using these devices does not entirely eliminate the risk of embolism. The atheroma recovered from re- current lesions by Simpson catheter has provided an important insight into the possible mechanism of restenosis.’
Limitations of the Study. Although it provides an important insight into some basic principles that govern the size of debris produced by KC, this is an in vitro study. There may be other fac- tors that affect the size of particles in vivo. The interaction of these particles with blood may in- crease their size by accumulation of platelets around them.26 However, we have recently dem- onstrated that activation of KC inhibits platelet function. ’’
In addition to size, the rheology of particles may be important. More flexible particles of equal size would negotiate vessels more readily. This aspect has not been addressed by the present study. Finally, although likely, it still remains to be seen whether reduction of particle size in the range described will affect the incidence or the extent of clinical and subclinical embolism.
In conclusion, debris generated by peripheral and coronary KC in calcified and noncalcified atheroma was investigated and the factors that may reduce its size were determined. The ex- perimental model described in this study could be adapted to evaluate particles resulting from other angioplasty devices. While reducing par- ticle size is likely to minimize their occlusive po- tential, this conclusion remains tentative and in vivo investigations are required.
Acknmw/edgment: The authors are grateful for the profes- sional assistance of Dr. A. B. Latif, Dr. R. Shore, and Mr. V. Hawkin. Also to Mr. D. Todd for producing the illustra- tions.
References
I . Safian RD, McCabe CH, Sipperly ME, et al. Initial and long term follow up of percutaneous transluminal cor- onary angioplasty in chronic total occlusions versus con- ventional stenoses. Am J Cardiol 1988; 61:23G-28G. Gehani AA, Sheard K, Ashley S, et al. Dynamic angio- 2.
6 .
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
4 1 :@2-9O5. Kensey KR, Nash JE, Abrahams, C, et al. Recanalis- ation of obstructed arteries with a flexible, rotating tip catheter. Radiology 1987; 165:387-389. Coleman CC, Poaslasky IP, Robinson JD, et al. Ath- eroablation with the Kensey Catheter: A pathologic study. Radiology 1989; 170:391-394. Wilson RF, Lesser JR, Laxson DD, et al. Intense mi- crovascular constriction after angioplasty of acute thrombotic coronary arterial lesions. Lancet 1989;
Kolibash AJ, Bush CA, Wespic RA, el al. Coronary col- lateral vessels: Spectrum of physiologic capabilities with respect to providing rest and stress myocardial perfu- sioh, maintenance of left ventricular function and pro- tection against infarction. Am J Cardiol 1985; 50:230- 238. Rentrop M, Knapp B, Winter H, et al. Aminoalkylsaline- treated glass slides as support for in situ hyperidization of keratin DNA to frozen sections under varying fixation and pretreatment conditions. Histochem J 1986; 18:271- 276. Giraldo AA, Esposo OM, Meis JM. lntimal hyperplasia as a cause of restenosis after percutaneous transluminal coronary angioplasty. Arch Pathol Lab Med 1985;
Simpson JB, Selmon MR, Robertson GC, et al. Trans- luminal atherectomy for occlusive peripheral vascular disease. Am J Cardiol 1988; 61:96G-101G. Wholey MH, Jarmolowski CR. New Reperfusion De- vices: The Kensey catheter, the atherolytic reperfusion wire device, and the transluminal extraction catheter. Radiology 1989; 172:947-952. Isner JM, Donalson RF, Funai JT, et al. Factors con- tributing to perforations resulting from argon laser cor- onary angioplasty: Observations in an intact human postmortem preparation of intraoperative laser coronary angioplasty. (abstract) Circulation 1985; 72(Suppl 11): 191. Keoh BE, Crea F, Bull T, et al. Intravascular delivery of laser energy with metal-capped optical fibre: The po- tential hazard of distal embolism. Am Heart J 1989;
Van Prooijen-Knegt AC, Raap AK, Van Der Burg MJM, et al. Spreading and staining of human metaphase chro- mosomes on aminoalkyisaline-treated glass slides. His- tochem J 1982; 14:333-344. Ganong WF. In: Review of Medical Physiology, 11th edition. Los Altos: Lang Medical Publications, 1983: 462. Ahn SS, Auth D, Marcus DR, et al. Removal of focal atheromatous lesions by angioscopically guided high speed rotary atherectomy: Preliminary experimental ob- servations. J Vasc Surg 1988; 7:292-300. Zacca NM, Raizner AE, Noon GP, et al. Short term follow up of patients treated with a recently developed rotational atherectomy device and in vivo assessment of particles generated. (abstract) J Am Coll Cardiol 1988; 11 (2): 109A. Gehani AA, Latif AB, Ashley S, et al. Dynamic angio- plasty in normal and abnormal coronary arteries. (ab- stract) Br Heart J 1989; 61:85. Gehani AA, Ball SG, Latif AB, et al. Experimental and clinical percutaneous angioscopy experience with dy- namic angioplasty. Angiology 1990; 77: 1139-1 141.
-
1 SO7-81 I .
6:173-175.
1 18~47-52.
102 Journal of Interventional Cardiology Vol. 4, No. 2, 1991

ANALYSIS OF DEBRIS RESULTING FROM DYNAMIC ANGIOPLASTY
19.
20.
21.
22.
23.
Gehani AA, Ashley S, Brooks S, et al. Percutaneous angioscopy and lasing of intirnal flaps following angio- plasty. (abstract) Heart and Vessels 1988; 4(1):53. Foster J. Medical application of image analysis with the magiscan 2. Analytical and quantitative cytology and histology 1985; 7(3): 192-196. Wiesel J, Grunwald AM, Tobiasz C, et al. Quantitation of absolute area of a coronary arterial stenosis: Exper- imental validation with preparation in vivo. Circulation 1986: 5: 1099-1 106. 26. Weitz Z, Gafter U , Chagnac A, el al. Cholesterol emboli in atherosclerotic patients: Report of four cases occur- ring spontaneously or complicating angioplasty and aorto-renal bypass. J Am Geriatr SOC 1987; 35:357-359. Saenz CB, Harrell RR, Swayer JA, et al. Acute per-
24.
25.
27.
cutaneous coronary angioplasty complicated by embo- lism to a coronary artery remote from the site of in- farction. Cath Cardiovasc Diagn 1987; 13:266-268. Crewe DD, Castaneda-Zuniga WR, Nordstrom LA, et al. Debris analysis after photorecanalisation of athero- sclerotic plaque. Sem lnterven Radio1 1986; 3(1):53-60. Lammer J. Karnel F. Percutaneous transluminal laser angioplasty with contact probes. Radiology 1988; 168:733-737. Scriven AJI, Nathan AW. The effect of laser generated tissue debris on platelet function in vitro. Lasers in Med- ical Sciences 1988; 7:310. Gehani AA, Latif AB, Ashley SG, et al. The influence of two laser and dynamic angioplasty devices on platelet reactivity. (abstract) Br Heart J 1990; 64(1):58.
Vol. 4, No. 2, 1991 Journal of lnterventional Cardiology 103
Copyright © 2022 FDOKUMEN




















