
Increased Tissue Factor Expression and Poor Nephroblastoma Prognosis
6
Increased Tissue Factor Expression and Poor Nephroblastoma Prognosis Elinês O. Maciel, Gustavo F. Carvalhal,* Vinícius D. da Silva, Eraldo L. Batista, Jr. and Bernardo Garicochea From the Departments of Pediatric Surgery (EOM), Urology (GFC), Pathology (VDS, ELB) and Clinical Oncology (BG), Pontifícia Universidade Católica, Porto Alegre, Brazil Abbreviations and Acronyms NWTS National WT Study SIOP Societé Internationale d’Urologie Pédiatrique TF tissue factor WT Wilms tumor Submitted for publication December 26, 2008. Study received approval from the ethical com- mittee at the 2 university hospitals. * Correspondence: Pontifícia Universidade católica do Rio Grande do Sul, Rua Sto. Inácio 500 Apt. 501, Porto Alegre, RS, Brazil, CEP 90570- 150 (telephone: 55 51 99589025; FAX: 55 51 33463939; e-mail: [email protected]). Purpose: There is potential interaction between malignant cell growth and the coagulation pathway. Recent studies suggest that tissue factor, a primary initi- ator of the extrinsic coagulation pathway, is expressed in various solid tumors in association with increased angiogenesis. To our knowledge we report for the first time the detection of tissue factor expression by immunohistochemistry in Wilms tumors and its correlation with clinical outcomes. Material and Methods: Tissue factor expression detected by immunohistochem- istry was assessed in 41 formalin fixed, paraffin embedded Wilms tumor cases treated at university hospitals. We correlated findings with tumor recurrence and cancer specific survival. Results: Positive immunohistochemistry detection of tissue factor was observed in 88.3% of the tumors analyzed. Tissue factor on immunohistochemistry was associated with tumor recurrence and survival (p 0.01 and 0.02, respectively). Increased immunohistochemical detection of tissue factor was the most impor- tant risk factor for recurrence and mortality in our population on bivariate and multivariate analysis. Conclusions: Tissue factor is a promising research subject as a prognostic factor for Wilms tumor. More studies are needed to clarify the mechanisms by which tissue factor affects cancer progression and outcome, and its potential role as a therapeutic target. Key Words: kidney, Wilms tumor, thromboplastin, prognosis, mortality WILMS tumor or nephroblastoma is the most common renal malignancy and the second most common ab- dominal solid tumor in childhood. 1,2 Known preoperative and postopera- tive factors help define the prognosis in each individual, such as anapla- sia, and clinical and pathological stage. Although the NWTS-V Group stated that overall 4-year survival exceeds 90% for favorable histology tumors, a subgroup of patients expe- riences relapse and responds poorly to second line therapy. 3,4 Therefore, there is a continuous search for novel potential prognostic markers of poor outcomes to improve thera- peutic strategies. 5,6 TF, also known as thromboplas- tin, is a transmembrane glycopro- tein that was originally recognized as important for initiating the ex- trinsic pathway of coagulation. Weak TF expression on immunohis- tochemistry was observed in various tissue lines. 7 However, it is strongly detected in the adventitia of blood vessels and in tissues surrounding 1594 www.jurology.com 0022-5347/09/1824-1594/0 Vol. 182, 1594-1599, October 2009 THE JOURNAL OF UROLOGY ® Printed in U.S.A. Copyright © 2009 by AMERICAN UROLOGICAL ASSOCIATION DOI:10.1016/j.juro.2009.06.011
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Increased Tissue Factor Expression and Poor Nephroblastoma Prognosis

Increased Tissue Factor Expression and PoorNephroblastoma Prognosis
Elinês O. Maciel, Gustavo F. Carvalhal,* Vinícius D. da Silva, Eraldo L. Batista, Jr.and Bernardo GaricocheaFrom the Departments of Pediatric Surgery (EOM), Urology (GFC), Pathology (VDS, ELB) and Clinical Oncology (BG), Pontifícia UniversidadeCatólica, Porto Alegre, Brazil
Abbreviations
and Acronyms
NWTS � National WT Study
SIOP � Societé Internationaled’Urologie Pédiatrique
TF � tissue factor
WT � Wilms tumor
Submitted for publication December 26, 2008.Study received approval from the ethical com-
mittee at the 2 university hospitals.* Correspondence: Pontifícia Universidade
católica do Rio Grande do Sul, Rua Sto. Inácio500 Apt. 501, Porto Alegre, RS, Brazil, CEP 90570-150 (telephone: 55 51 99589025; FAX: 55 5133463939; e-mail: [email protected]).
Purpose: There is potential interaction between malignant cell growth and thecoagulation pathway. Recent studies suggest that tissue factor, a primary initi-ator of the extrinsic coagulation pathway, is expressed in various solid tumors inassociation with increased angiogenesis. To our knowledge we report for the firsttime the detection of tissue factor expression by immunohistochemistry in Wilmstumors and its correlation with clinical outcomes.Material and Methods: Tissue factor expression detected by immunohistochem-istry was assessed in 41 formalin fixed, paraffin embedded Wilms tumor casestreated at university hospitals. We correlated findings with tumor recurrence andcancer specific survival.Results: Positive immunohistochemistry detection of tissue factor was observedin 88.3% of the tumors analyzed. Tissue factor on immunohistochemistry wasassociated with tumor recurrence and survival (p � 0.01 and 0.02, respectively).Increased immunohistochemical detection of tissue factor was the most impor-tant risk factor for recurrence and mortality in our population on bivariate andmultivariate analysis.Conclusions: Tissue factor is a promising research subject as a prognostic factorfor Wilms tumor. More studies are needed to clarify the mechanisms by whichtissue factor affects cancer progression and outcome, and its potential role as atherapeutic target.
Key Words: kidney, Wilms tumor, thromboplastin, prognosis, mortality
1594 www.jurology.com
WILMS tumor or nephroblastoma isthe most common renal malignancyand the second most common ab-dominal solid tumor in childhood.1,2
Known preoperative and postopera-tive factors help define the prognosisin each individual, such as anapla-sia, and clinical and pathologicalstage. Although the NWTS-V Groupstated that overall 4-year survivalexceeds 90% for favorable histologytumors, a subgroup of patients expe-riences relapse and responds poorly
to second line therapy.3,4 Therefore,0022-5347/09/1824-1594/0THE JOURNAL OF UROLOGY®
Copyright © 2009 by AMERICAN UROLOGICAL ASSOCIATION
there is a continuous search fornovel potential prognostic markersof poor outcomes to improve thera-peutic strategies.5,6
TF, also known as thromboplas-tin, is a transmembrane glycopro-tein that was originally recognizedas important for initiating the ex-trinsic pathway of coagulation.Weak TF expression on immunohis-tochemistry was observed in varioustissue lines.7 However, it is stronglydetected in the adventitia of blood
vessels and in tissues surroundingVol. 182, 1594-1599, October 2009Printed in U.S.A.
DOI:10.1016/j.juro.2009.06.011
TISSUE FACTOR EXPRESSION AND NEPHROBLASTOMA PROGNOSIS 1595
most internal organs, presumably acting as a nat-ural hemostatic barrier. When exposed, TF acts asa specific cofactor for plasma factor VII and sub-sequently TF activated factor VIIa activates fac-tors IX and X, resulting in fibrin formation.8 –10 TFexpression was also identified by immunohisto-chemistry in cells of various tissues during embryo-genesis, when coagulation factors are not presentor are incapable of crossing the placental barrier.8
Studies in knockout mice models revealed that TFdeficiency is lethal to embryos due to defectivedevelopment of the blood vessel subendotheliallayer.7,8,11 More recently TF was related to metas-tasis, possibly due to interference with cell signal-ing pathways and the proteolytic activity of TF/factor VII activated complex.12 TF also correlateswith a worse prognosis of various tumors.
To our knowledge TF expression detected byimmunohistochemistry has not previously beenstudied in WT. We evaluated TF expression de-tected by immunohistochemistry in 41 patientswith WT treated at tertiary hospitals in PortoAlegre, Brazil. We correlated findings with vari-ables such as patient age, stage, histology, tumorrecurrence and cancer specific survival.
MATERIALS AND METHODS
We evaluated the records of 45 patients with WT treatedfrom 1993 to 2003 at 2 university affiliated institutions insouthern Brazil, including Hospital São Lucas and Hospi-tal da Criança Conceição. All patients underwent surgerydespite the use of neoadjuvant or adjuvant treatment andwere followed until death or the latest evaluation up toJune 2007. Three patients were excluded from analysisbecause paraffin blocks were unavailable and 1 missedfollowup evaluations after surgery. Thus, our final studygroup consisted of 41 patients. Variables were patient ageat diagnosis, histology, tumor stage and TF expression onimmunohistochemistry. Tumor recurrence and overallsurvival were chosen as outcome measures.
�
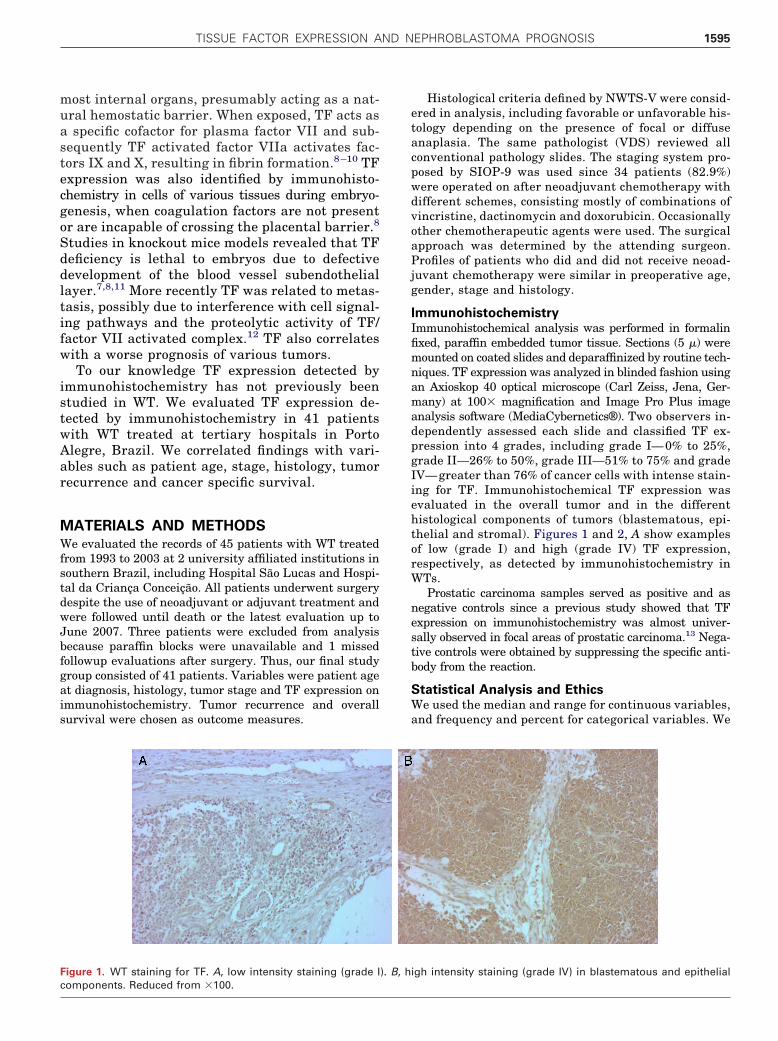
Figure 1. WT staining for TF. A, low intensity staining (grade I
components. Reduced from �100.Histological criteria defined by NWTS-V were consid-ered in analysis, including favorable or unfavorable his-tology depending on the presence of focal or diffuseanaplasia. The same pathologist (VDS) reviewed allconventional pathology slides. The staging system pro-posed by SIOP-9 was used since 34 patients (82.9%)were operated on after neoadjuvant chemotherapy withdifferent schemes, consisting mostly of combinations ofvincristine, dactinomycin and doxorubicin. Occasionallyother chemotherapeutic agents were used. The surgicalapproach was determined by the attending surgeon.Profiles of patients who did and did not receive neoad-juvant chemotherapy were similar in preoperative age,gender, stage and histology.
ImmunohistochemistryImmunohistochemical analysis was performed in formalinfixed, paraffin embedded tumor tissue. Sections (5 �) weremounted on coated slides and deparaffinized by routine tech-niques. TF expression was analyzed in blinded fashion usingan Axioskop 40 optical microscope (Carl Zeiss, Jena, Ger-many) at 100� magnification and Image Pro Plus imageanalysis software (MediaCybernetics®). Two observers in-dependently assessed each slide and classified TF ex-pression into 4 grades, including grade I— 0% to 25%,grade II—26% to 50%, grade III—51% to 75% and gradeIV— greater than 76% of cancer cells with intense stain-ing for TF. Immunohistochemical TF expression wasevaluated in the overall tumor and in the differenthistological components of tumors (blastematous, epi-thelial and stromal). Figures 1 and 2, A show examplesof low (grade I) and high (grade IV) TF expression,respectively, as detected by immunohistochemistry inWTs.
Prostatic carcinoma samples served as positive and asnegative controls since a previous study showed that TFexpression on immunohistochemistry was almost univer-sally observed in focal areas of prostatic carcinoma.13 Nega-tive controls were obtained by suppressing the specific anti-body from the reaction.
Statistical Analysis and EthicsWe used the median and range for continuous variables,and frequency and percent for categorical variables. We
igh intensity staining (grade IV) in blastematous and epithelial
�
). B, h
by SIO
TISSUE FACTOR EXPRESSION AND NEPHROBLASTOMA PROGNOSIS1596
used the nonparametric Wilcoxon/Mann-Whitney test tocompare continuous variables and the chi-square orFisher exact test to compare categorical variables. Forsurvival analysis Kaplan-Meier curves were comparedusing the log rank test. To evaluate the effect of poten-tial confounders on survival curves we used Cox propor-tional hazards model. Significance was considered at� � 5% (p �0.05). Data were analyzed using SPSS®,version 11.5. The study protocol was approved by theethical committee at the 2 university hospitals.
RESULTS
Table 1 lists clinical and pathological variables inour 41 patients. Of the patients 23 (56.1%) werefemale. The tumor affected the left kidney in 22cases (53.7%). Histology was favorable in 38 cases(92.7%) and cases were distributed across allSIOP-9 stages.
Median followup was 4.4 years (range 0 to 12).In 18 patients (43.9%) recurrence developed dur-
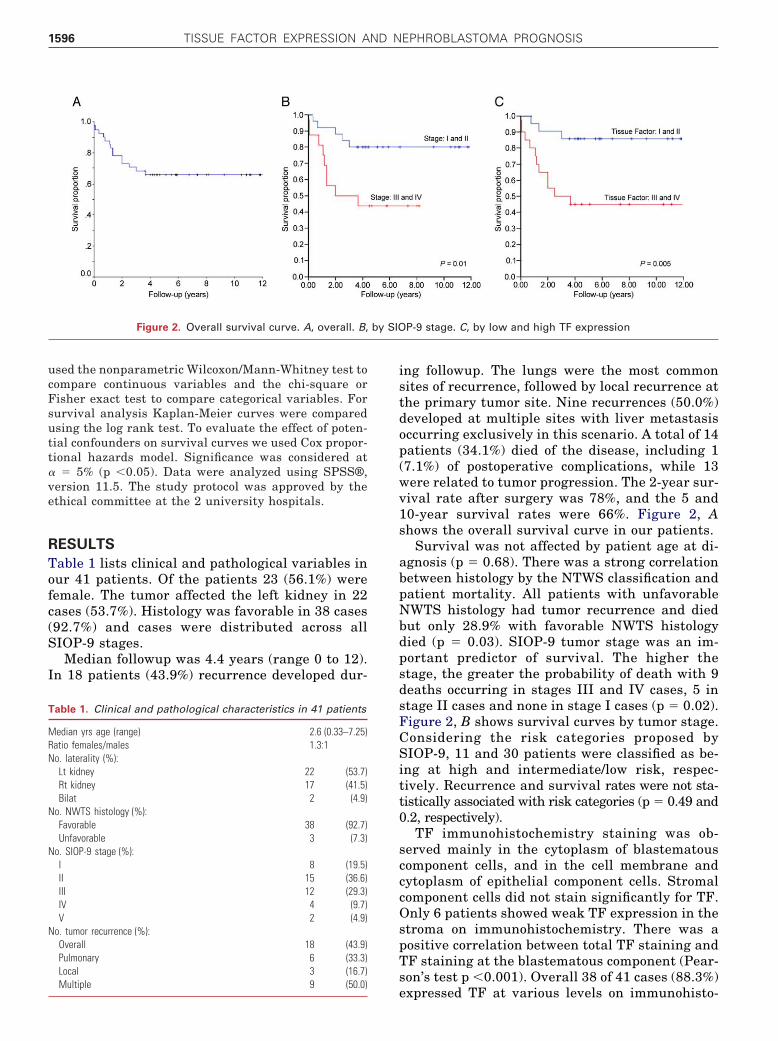
Figure 2. Overall survival curve. A, overall. B,
Table 1. Clinical and pathological characteristics in 41 patients
Median yrs age (range) 2.6 (0.33–7.25)Ratio females/males 1.3:1No. laterality (%):
Lt kidney 22 (53.7)Rt kidney 17 (41.5)Bilat 2 (4.9)
No. NWTS histology (%):Favorable 38 (92.7)Unfavorable 3 (7.3)
No. SIOP-9 stage (%):I 8 (19.5)II 15 (36.6)III 12 (29.3)IV 4 (9.7)V 2 (4.9)
No. tumor recurrence (%):Overall 18 (43.9)Pulmonary 6 (33.3)Local 3 (16.7)
Multiple 9 (50.0)ing followup. The lungs were the most commonsites of recurrence, followed by local recurrence atthe primary tumor site. Nine recurrences (50.0%)developed at multiple sites with liver metastasisoccurring exclusively in this scenario. A total of 14patients (34.1%) died of the disease, including 1(7.1%) of postoperative complications, while 13were related to tumor progression. The 2-year sur-vival rate after surgery was 78%, and the 5 and10-year survival rates were 66%. Figure 2, Ashows the overall survival curve in our patients.
Survival was not affected by patient age at di-agnosis (p � 0.68). There was a strong correlationbetween histology by the NTWS classification andpatient mortality. All patients with unfavorableNWTS histology had tumor recurrence and diedbut only 28.9% with favorable NWTS histologydied (p � 0.03). SIOP-9 tumor stage was an im-portant predictor of survival. The higher thestage, the greater the probability of death with 9deaths occurring in stages III and IV cases, 5 instage II cases and none in stage I cases (p � 0.02).Figure 2, B shows survival curves by tumor stage.Considering the risk categories proposed bySIOP-9, 11 and 30 patients were classified as be-ing at high and intermediate/low risk, respec-tively. Recurrence and survival rates were not sta-tistically associated with risk categories (p � 0.49 and0.2, respectively).
TF immunohistochemistry staining was ob-served mainly in the cytoplasm of blastematouscomponent cells, and in the cell membrane andcytoplasm of epithelial component cells. Stromalcomponent cells did not stain significantly for TF.Only 6 patients showed weak TF expression in thestroma on immunohistochemistry. There was apositive correlation between total TF staining andTF staining at the blastematous component (Pear-son’s test p �0.001). Overall 38 of 41 cases (88.3%)
P-9 stage. C, by low and high TF expression
expressed TF at various levels on immunohisto-
TISSUE FACTOR EXPRESSION AND NEPHROBLASTOMA PROGNOSIS 1597
chemistry. Of the 41 cases TF expression wasgraded by immunohistochemistry staining inten-sity as grades I to IV in 8 (19.5%), 13 (31.7%), 17(41.5%) and 3 (7.3%), respectively.
There was no statistical correlation betweenmedian total TF expression grade on immunohis-tochemistry and patient age (p � 0.64), favorable/unfavorable histology (p � 0.21) or SIOP stage(p � 0.13). There was a positive association be-tween median total TF expression grade on immu-nohistochemistry and tumor recurrence (p � 0.01,table 2). Increased intensity of total TF expressionand of blastematous TF expression were also pos-itively associated with death (p � 0.02 and �0.01,respectively, table 2).
For survival analysis we divided patients into 2main groups according to TF expression on immuno-histochemistry, including low intensity—grades I plusII and high intensity—grades III plus IV. On immu-nohistochemistry low and high TF expression inten-sity was noted in 21 (51.2%) and 20 patients (48.8%),respectively. Increased TF expression on immunohis-tochemistry was statistically associated with de-creased survival (fig. 2, C).
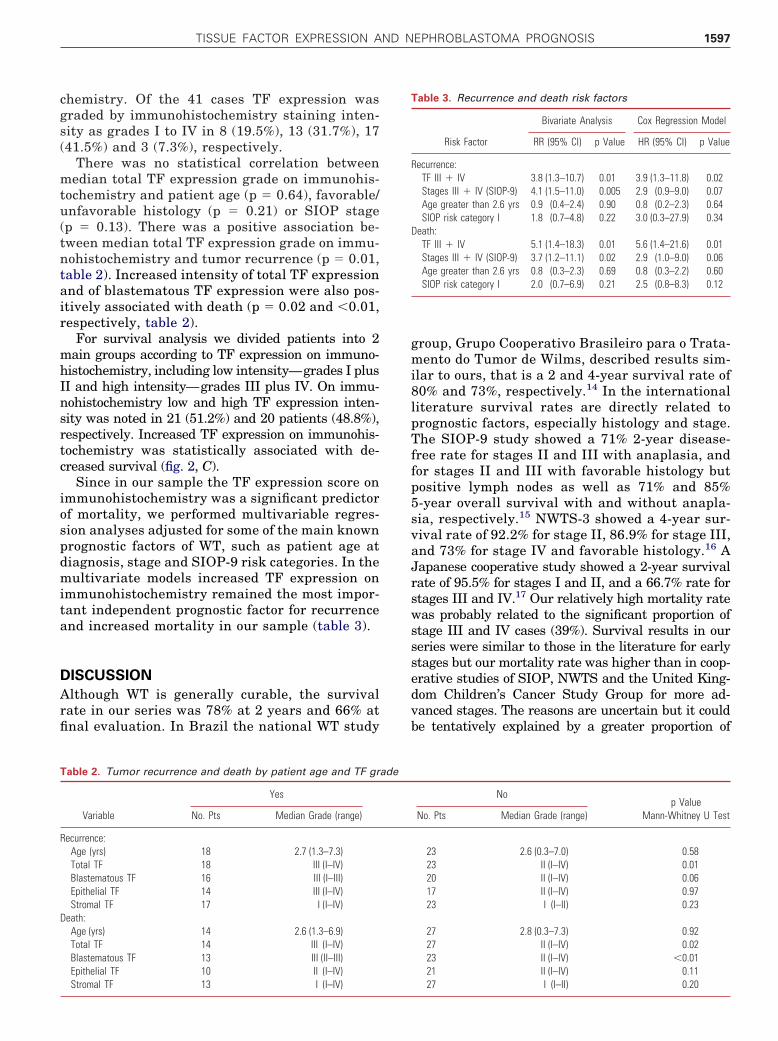
Since in our sample the TF expression score onimmunohistochemistry was a significant predictorof mortality, we performed multivariable regres-sion analyses adjusted for some of the main knownprognostic factors of WT, such as patient age atdiagnosis, stage and SIOP-9 risk categories. In themultivariate models increased TF expression onimmunohistochemistry remained the most impor-tant independent prognostic factor for recurrenceand increased mortality in our sample (table 3).
DISCUSSION
Although WT is generally curable, the survivalrate in our series was 78% at 2 years and 66% atfinal evaluation. In Brazil the national WT study
Table 2. Tumor recurrence and death by patient age and TF gr
Variable
Yes
No. Pts Median Grade (range)
Recurrence:Age (yrs) 18 2.7 (1.3–7.3)Total TF 18 III (I–IV)Blastematous TF 16 III (I–III)Epithelial TF 14 III (I–IV)Stromal TF 17 I (I–IV)
Death:Age (yrs) 14 2.6 (1.3–6.9)Total TF 14 III (I–IV)Blastematous TF 13 III (II–III)Epithelial TF 10 II (I–IV)
Stromal TF 13 I (I–IV)group, Grupo Cooperativo Brasileiro para o Trata-mento do Tumor de Wilms, described results sim-ilar to ours, that is a 2 and 4-year survival rate of80% and 73%, respectively.14 In the internationalliterature survival rates are directly related toprognostic factors, especially histology and stage.The SIOP-9 study showed a 71% 2-year disease-free rate for stages II and III with anaplasia, andfor stages II and III with favorable histology butpositive lymph nodes as well as 71% and 85%5-year overall survival with and without anapla-sia, respectively.15 NWTS-3 showed a 4-year sur-vival rate of 92.2% for stage II, 86.9% for stage III,and 73% for stage IV and favorable histology.16 AJapanese cooperative study showed a 2-year survivalrate of 95.5% for stages I and II, and a 66.7% rate forstages III and IV.17 Our relatively high mortality ratewas probably related to the significant proportion ofstage III and IV cases (39%). Survival results in ourseries were similar to those in the literature for earlystages but our mortality rate was higher than in coop-erative studies of SIOP, NWTS and the United King-dom Children’s Cancer Study Group for more ad-vanced stages. The reasons are uncertain but it couldbe tentatively explained by a greater proportion of
Nop Value
Mann-Whitney U TestNo. Pts Median Grade (range)
23 2.6 (0.3–7.0) 0.5823 II (I–IV) 0.0120 II (I–IV) 0.0617 II (I–IV) 0.9723 I (I–II) 0.23
27 2.8 (0.3–7.3) 0.9227 II (I–IV) 0.0223 II (I–IV) �0.0121 II (I–IV) 0.11
Table 3. Recurrence and death risk factors
Bivariate Analysis Cox Regression Model
Risk Factor RR (95% CI) p Value HR (95% CI) p Value
Recurrence:TF III � IV 3.8 (1.3–10.7) 0.01 3.9 (1.3–11.8) 0.02Stages III � IV (SIOP-9) 4.1 (1.5–11.0) 0.005 2.9 (0.9–9.0) 0.07Age greater than 2.6 yrs 0.9 (0.4–2.4) 0.90 0.8 (0.2–2.3) 0.64SIOP risk category I 1.8 (0.7–4.8) 0.22 3.0 (0.3–27.9) 0.34
Death:TF III � IV 5.1 (1.4–18.3) 0.01 5.6 (1.4–21.6) 0.01Stages III � IV (SIOP-9) 3.7 (1.2–11.1) 0.02 2.9 (1.0–9.0) 0.06Age greater than 2.6 yrs 0.8 (0.3–2.3) 0.69 0.8 (0.3–2.2) 0.60SIOP risk category I 2.0 (0.7–6.9) 0.21 2.5 (0.8–8.3) 0.12
ade
27 I (I–II) 0.20

TISSUE FACTOR EXPRESSION AND NEPHROBLASTOMA PROGNOSIS1598
malnutrition and delayed diagnosis in our patientssince the chemotherapy and radiotherapy that weused were strictly in accordance with SIOP-9 protocolrecommendations.
Some groups reported that older age at diagnosiscorrelated with a worse WT prognosis.1 Although inour patients age at diagnosis was similar to that inpublished studies, we did not find any correlationbetween age and stage, histology, recurrence ordeath.
In our series there was a slight preponderanceof the female gender (56.1% of patients). This is inagreement with the North American literature, inwhich females are slightly more common thanmales (1.0:0.92 in NWTS). Regarding tumor loca-tion, our findings were also similar to those in thepublished literature with the left kidney affectedslightly more often.17
Traditionally histology is a major prognosticfactor for WT and the NWTS classification is themost widely used. As in NWTS,18 most of ourpatients had favorable histology. Likewise, unfa-vorable histology was an important determinantof poor outcome in our series. However, on multi-variate analysis histology was incorporated intothe SIOP-9 risk categories and was not an inde-pendent predictor of mortality in our study.
We used the SIOP-9 system for tumor stagingbecause most patients received neoadjuvant che-motherapy. Tumor stage remained an importantprognostic factor for recurrence and survival inour series. Of the 18 cases of recurrence 12 werestages III and IV, and only 6 were stages I and II.The higher the stage at diagnosis, the greater theprobability of death with 9 deaths in stages III andIV, 5 in stage II and none in stage I cases. Oursurvival curves show greater than 80% 10-yearsurvival for stages I and II with less than 50%10-year survival for stages III and IV, confirmingthe assumption that stage at diagnosis is a keyprognostic factor for WT. However, tumor stagewas not an independent predictor of mortality onmultivariate analysis. This might be explained bythe important relative weight of other prognosticfactors, eg TF, to predict survival. SIOP-9 riskcategories (low, intermediate or high) were notdeterminants of recurrence or death. Our smallsample size could be a reason.
To our knowledge our study shows for the firsttime the immunohistochemical expression of TF inWT. On immunohistochemistry TF was expressedmore frequently in tumor blastematous and epi-thelial components, and sparsely in the stromalcomponent. Despite the relatively small number ofpatients increased TF expression on immunohis-tochemistry showed a significant association with
recurrence and death. Increased immunohisto-chemistry detection of TF expression was the mostimportant prognostic factor for recurrence anddeath, and the only independent predictor of deathin our series on multivariate analysis.
Increased TF expression on immunohistochemistrywas an adverse prognostic factor in other studies. Ab-dulkadir et al noted increased TF expression on im-munohistochemistry in 73% of 67 patients with pros-tate carcinoma and found that TF expression onimmunohistochemistry correlated positively with pre-operative serum prostate specific antigen.13 Callanderet al reported that at least 60% of epithelial malignantneoplasms expressed TF on immunohistochemistry.19
The percent of gastrointestinal carcinomas expressingTF on immunohistochemistry was particularly high,up to 100% in gastric and pancreatic carcinomas. Morerecently researchers defining a possible role for TF asa tumor marker noted that it can be measured in bloodand urine. Lwaleed et al studied urinary TF in pa-tients with bladder and prostate cancer.20 In that se-ries increased urinary TF was related to poorly differ-entiated tumors and death. Further studies in the fieldmay prove the usefulness of TF as a diagnostic andfollowup tool. Therapies against TF, eg TF proteininhibitor, may be tested in laboratory and clinical set-tings, which could allow advances in the managementof many tumors.
Despite the interesting positive correlation betweenincreased TF expression on immunohistochemistryand prognosis in our study we acknowledge some ca-veats that may limit the generalization of our findings.1) We performed a retrospective study in a relativelysmall sample, which should be put into perspective.2) Our patients were treated at 2 university hospitalsby different groups of pediatric surgeons. Al-though all surgeons who treated these childrenwere experienced with pediatric oncology, we can-not truly ascertain the importance of this fact.3) Most patients received chemotherapy preoper-atively and at this time it is impossible to evaluatethe effects of this treatment on TF expression, asdetected by immunohistochemistry. 4) We cannotoveremphasize the limitations of immunohisto-chemistry. TF staining intensity was measuredaccording to a semiquantitative score based onquartiles with the problems of subjectivity inher-ent to this methodology. We also must considerthat many slides were obtained from paraffin em-bedded samples in stock more than 10 years at thepathology laboratory. A prospective study would the-oretically be more useful since it could minimize techni-cal biases.
CONCLUSIONS
TF expression on immunohistochemistry was the most
important independent prognostic factor for survival
TISSUE FACTOR EXPRESSION AND NEPHROBLASTOMA PROGNOSIS 1599
in a cohort of patients with WT. However, the limita-tions of our study do not allow us to do more than
generate hypotheses. Further studies are needed toREFERENCES
Urol Clin North Am 2000; 27: 455. neiro: Revinter 1998; pp 10
determine the real usefulness of these findings andidentify possible roles of TF as a clinical marker and a
therapeutic target.1. Breslow NE, Beckwith JB, Ciol M et al: Agedistribution of Wilms tumor: report from the Na-tional Wilms= Tumor Study. Cancer Res 1988; 48:1653.
2. Pastore G, Carli M, Lemerle J et al: Epidemiologicfeatures of Wilms= tumor: results of studies bythe International Society of Pediatric Oncology(SIOP). Med Pediatr Oncol 1988; 16: 7.
3. Abramson LP, Grundy PE, Rademaker AW et al:Increased microvascular density predicts relapsein Wilms= tumor. J Pediatr Surg 2003; 38: 325.
4. Williams RD, Hing SN, Greer BT et al: Prognosticclassification of relapsing favorable histologyWilms tumor using cDNA microarray expressionprofiling and support vector machines. GenesChromosomes Cancer 2004; 41: 65.
5. Blakely ML and Ritchey ML: Controversies in themanagement of Wilms= tumor. Semin PediatrSurg 2001; 10: 127.
6. Farhat W, McLorie G and Capolicchio G: Wilms’tumor: surgical considerations and controversies.
7. Carmeliet P, Mackmann N, Moons L et al: Role oftissue factor in embryonic blood vessel develop-ment. Nature 1996; 383: 73.
8. Carmeliet P and Collen D: Tissue factor. Int J Bio-chem Cell Biol 1998; 30: 661.
9. Banner DW: The factor VIIa/tissue factor com-plex. Thromb Haemost 1997; 78: 512.
10. Higashi S and Iwanaga S: Molecular interactionbetween factor VII and tissue factor. Int J Hema-tol 1998; 67: 229.
11. Mackman N: Role of tissue factor in hemostasis,thrombosis, and vascular development. Arterio-scler Thromb Vasc Biol 2004; 24: 1015.
12. Rickles FR, Patierno S and Fernandez PM: Tissuefactor, thrombin, and cancer. Chest, suppl., 2003;124: 58S.
13. Abdulkadir AS, Carvalhal GF, Kaleem Z et al:Tissue factor expression and angiogenesis in hu-man prostate carcinoma. Hum Pathol 2000; 31:443.
14. de Camargo B: Tumor de Wilms. In: CirurgiaPediátrica. Edited by JG Maksoud. Rio de Ja-
05–1018.
15. Delemarre JF, Sandstedt B, Harms D et al: Thenew SIOP (Stockholm) working classification ofrenal tumors of childhood. International Societyof Pediatric Oncology. Med Pediatr Oncol 1996;26: 145.
16. Takamizawa S, Okamoto S, Bishop W et al: Dif-ferential apoptosis gene expression in pediatrictumors of the kidney. J Pediatr Surg 2000; 35:390.
17. Suita A, Kinoshita Y, Tajiri T et al: Clinical char-acteristics and outcome of Wilms tumors with afavorable histology in Japan: a report from theStudy Group for pediatric Solid Malignant Tumorsin the Kyushu area. Japan J Pediatr Surg 2006;41: 1501.
18. Beckwith JB: National Wilms Tumor Study: anupdate for pathologists. Pediatr Dev Pathol 1998;1: 79.
19. Callander NS, Varki N and Rao VM: Immunohis-tochemical identification of tissue factor in solidtumors. Cancer 1992; 70: 1194.
20. Lwaleed BA, Francis JL and Chisholm M: Urinarytissue factor levels in patients with bladder and
prostate cancer. Eur J Surg Oncol 2000; 26: 44.



















