Childhood leukemia and lymphoma: time trends and factors affecting survival in five Southern and...
10
1 23 Cancer Causes & Control An International Journal of Studies of Cancer in Human Populations ISSN 0957-5243 Volume 24 Number 6 Cancer Causes Control (2013) 24:1111-1118 DOI 10.1007/s10552-013-0188-y Childhood leukemia and lymphoma: time trends and factors affecting survival in five Southern and Eastern European Cancer Registries Eleni Th. Petridou, Nadya Dimitrova, Sultan Eser, Denis Kachanov, Hulya Karakilinc, Svetlana Varfolomeeva, Maria Belechri, et al.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Childhood leukemia and lymphoma: time trends and factors affecting survival in five Southern and...
1 23
Cancer Causes & ControlAn International Journal of Studies ofCancer in Human Populations ISSN 0957-5243Volume 24Number 6 Cancer Causes Control (2013)24:1111-1118DOI 10.1007/s10552-013-0188-y
Childhood leukemia and lymphoma: timetrends and factors affecting survival in fiveSouthern and Eastern European CancerRegistries
Eleni Th. Petridou, Nadya Dimitrova,Sultan Eser, Denis Kachanov, HulyaKarakilinc, Svetlana Varfolomeeva,Maria Belechri, et al.

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media Dordrecht. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.
ORIGINAL PAPER
Childhood leukemia and lymphoma: time trends and factorsaffecting survival in five Southern and Eastern European CancerRegistries
Eleni Th. Petridou • Nadya Dimitrova • Sultan Eser • Denis Kachanov •
Hulya Karakilinc • Svetlana Varfolomeeva • Maria Belechri • Margarita Baka •
Maria Moschovi • Sofia Polychronopoulou • Fani Athanasiadou-Piperopoulou •
Ioanna Fragandrea • Eftichia Stiakaki • Apostolos Pourtsidis • Christodoulos Stefanadis •
Jan-Willem Coebergh • Theodoros N. Sergentanis
Received: 14 December 2012 / Accepted: 14 March 2013 / Published online: 26 March 2013
� Springer Science+Business Media Dordrecht 2013
Abstract
Purpose Within Europe, incidence and mortality rates of
childhood leukemia and lymphoma are rather heteroge-
neous. The present study comprising data from five
Southern and Eastern European Cancer Registries aims to
compare time trends and examine whether sociodemo-
graphic variables, clinical parameters, and proxies of effi-
cient care affect survival.
Methods Data spanning 1996–2010 were obtained for a
total of 3,041 newly diagnosed childhood leukemia and
1,183 lymphoma cases reported by the Greek Nationwide
Registry for Childhood Hematological Malignancies, Bul-
garian National Cancer Registry, Moscow Region and
Turkey (Antalya and Izmir) Cancer Registries. Poisson
modeling for the evaluation of time trends and multivariate
Cox regression analysis for the assessment of prognostic
factors were performed.
Results The incidence of leukemia was increasing in all
cases, with Bulgaria and Greece presenting statistically
significant annual changes (?3.5, and ?1.7 %, respec-
tively), followed by marginally increasing trends in Izmir
and Moscow; by contrast, there was a remarkable, statis-
tically significant, decreasing mortality trend for leukemia.
Rates for lymphoma remained flat. Greece experienced
almost twofold better survival rates for both leukemia and
lymphoma, probably due to its higher socioeconomic status
during the study period. Overall, patients with leukemia
living in rural areas had a 28 % lower prognosis (RR: 1.28,
95 % CI 1.03–1.59), pointing to effects of remoteness,
when the most privileged country (Greece) was excluded
from the analysis.
Conclusions The favorable mortality trends highlight the
progress in Southern–Eastern European countries alongElectronic supplementary material The online version of thisarticle (doi:10.1007/s10552-013-0188-y) contains supplementarymaterial, which is available to authorized users.
E. Th. Petridou (&) � M. Belechri � T. N. Sergentanis
Department of Hygiene, Epidemiology and Medical Statistics,
Athens University Medical School, 75 M. Asias Str.
Goudi, 115 27 Athens, Greece
e-mail: [email protected]
N. Dimitrova
Bulgarian National Cancer Registry, National Oncology
Hospital, Sofia, Bulgaria
S. Eser
Cancer Control Department, Izmir Public Health Institute,
Izmir, Turkey
D. Kachanov � S. Varfolomeeva
Department of Clinical Oncology, Federal Clinical Research
Center of Pediatric Hematology, Oncology and Immunology,
Moscow, Russian Federation
H. Karakilinc
Provincial Health Directory of Antalya, Antalya Cancer
Registry, Antalya, Turkey
M. Baka � A. Pourtsidis
Department of Pediatric Haematology–Oncology,
‘‘Pan. & Agl. Kyriakou’’ Children’s Hospital, Athens, Greece
M. Moschovi
Haematology–Oncology Unit, First Department of Pediatrics,
Athens University Medical School, ‘‘Aghia Sophia’’
Children’s Hospital, Athens, Greece
S. Polychronopoulou
Department of Pediatric Haematology–Oncology,
‘‘Aghia Sophia’’ Children’s Hospital, Athens, Greece
123
Cancer Causes Control (2013) 24:1111–1118
DOI 10.1007/s10552-013-0188-y
Author's personal copy

their trajectory to converge with Northern–Western EU
counterpart states. Socioeconomic status may act as a
multipotent factor underlying the study findings.
Keywords Childhood leukemia � Childhood lymphoma �Survival � Incidence � Mortality � Time trends �Socioeconomic status
Introduction
Childhood leukemia, at least in the developed countries,
seems to exhibit a two-faced pattern regarding incidence
and survival rates, in the sense that survival rates seem to
be impressively and constantly improving, whereas in the
same period increasing incidence trends have been widely
reported [1–3]. Longer survival is reflected upon sizeable
decrease in mortality rates, as reported in the USA [4],
Europe [5], Latin America, Asia, and Oceania [6].
The globally reported impact of survival rates upon
mortality may not seem surprising, given the considerable
therapeutic progress. Indeed, the 5-year survival rates have
climbed from\5 % before the early 1960s [7, 8] to close to
90 % [9] for acute lymphoblastic leukemia (ALL) and
approximately 50 % for acute myeloid leukemia (AML)
[10]. Regarding childhood lymphoma, 5-year survival for
non-Hodgkin lymphoma (NHL) has also increased, reach-
ing 88 % in the USA, whereas steady improvements in 5-
and 10-year survival rates for Hodgkin’s lymphoma (HL)
are approaching figures as high as 95 % [11]. In the
European Union, however, the impressive declines in
mortality rates for childhood leukemia from 1.7 to 0.9/
100,000 for boys and from 1.3 to 0.7/100,000 for girls do
not seem to be equally shared, as the respective figures
were considerably higher in Southern or Eastern European
countries [5].
The present study focuses on the rather less privileged
region of Southern and Eastern Europe, aiming to compar-
atively assess incidence and mortality time trends of child-
hood leukemia and lymphoma in five Registries of four
South-Eastern and Eastern European countries and to
examine whether inherent sociodemographic and clinical
parameters, notably age, gender, country, subtype of leuke-
mia/lymphoma, and place of residence, affect survival in the
cross-national study setting. Specifically, data gathered from
two nationwide Cancer Registries in two adjacent EU
member states [Nationwide Registry for Childhood Hema-
tological Malignancies (NARECHEM) in Greece and the
Bulgarian National Cancer Registry (BNCR)] as well as
from three Regional Registries located in countries sharing
borders with EU, namely Russia (Moscow Region Cancer
Registry) and Turkey (Antalya and Izmir Cancer Registries),
during a period spanning circa 1996–2010 were examined.
Materials and methods
Country (Greece, Bulgaria, Turkey, and Russia) and Reg-
istry (NARECHEM, BNCR, Antalya, Izmir, and Moscow
Region Cancer Registries) characteristics are provided in
the Supplemental Methods file for all five Registries.
Specifically, during a 15-year study period for which data
were available, a total of 1,215 incident leukemia cases and
422 lymphoma cases were retrieved from NARECHEM
(1996–2010); 675 leukemias and 292 lymphomas from
BNCR (1996–2009); 403 leukemias and 158 lymphomas
from the Moscow Region Registry (2000–2010); 323 leu-
kemias and 121 lymphomas from the Antalya Registry
(1998–2008); and 425 leukemias and 190 lymphomas from
the Izmir Cancer Registry (1996–2007) and contributed to
the study dataset.
Data analysis
Details regarding the analysis of incidence and mortality
rates by country as well as the respective time trends are
presented in the Supplemental Methods.
Survival (vital status) data by age, gender, place of resi-
dence at diagnosis, and location of Registry as well by specific
subtypes of the disease (ALL, AML and other leukemia type;
HL, NHL, Burkitt and other lymphoma type) were compared;
the chi-square test was used to identify any differences. In the
survival analyses, only incident cases diagnosed in the Reg-
istries during the study periods were included.
Finally, survival of leukemia or lymphoma was exam-
ined, by modeling the data through Cox proportional hazards
multivariate regression analysis. Independent variables
included age, gender, location of the Registry, disease sub-
type, and place of living. Data for the latter variable were not
F. Athanasiadou-Piperopoulou
2nd Department of Pediatrics, Aristotelian University
of Thessaloniki, AHEPA General Hospital, Thessaloniki, Greece
I. Fragandrea
Pediatric Oncology Department, Hippokration
Hospital, Thessaloniki, Greece
E. Stiakaki
Department of Pediatric Hematology-Oncology,
University of Crete, Heraklion, Crete, Greece
C. Stefanadis
1st Department of Cardiology, Athens University
Medical School, Athens, Greece
J.-W. Coebergh
Eindhoven Cancer Registry of Comprehensive
Cancer Centre South, Eindhoven, The Netherlands
1112 Cancer Causes Control (2013) 24:1111–1118
123
Author's personal copy

available for Moscow Registry, whereas there were some
missing values in the Greek and the Antalya Registry; con-
sequently, it was introduced as an additional variable to the
initial model. Missing cases were due to administrative
reasons and were not considered to introduce any bias in the
results. Follow-up was active for NARECHEM, Izmir, and
Antalya, passive for the BNCR, and both active and passive
for the Moscow Region Registry, with 31 December 2010
being the censoring date. Statistical analyses were carried
out using SAS software, version 9 for Windows (SAS
Institute Inc., Cary, NC, USA).
Results
Table 1 presents the calculated average age-adjusted and
crude incidence rates for the initial and last 3 years as well
as the percentage of the annual change in each Registry.
The incidence of leukemia was increasing in all Registries,
with Bulgaria and Greece presenting statistically signifi-
cant annual changes, followed by Izmir and Moscow
Region with marginally increasing trends (Fig. 1a). Con-
cerning mortality rates, there was a remarkable, decreasing
trend in all Registries with Moscow presenting the highest
annual change (-9.9 %), followed by Greece and Bulgaria
(Fig. 1b). The AMRs in Bulgaria were considerably higher
Table 1 Average first and last 3 years (circa 1996–2010), age-adjusted and crude incidence and mortality rates (AIR, CIR and AMR, CMR) per
1,000,000 in the 5 Cancer Registries, along with corresponding annual change, 95 % confidence intervals (95 % CI), and p values
Country Greece Bulgaria Turkey Turkey Russia
Cancer Registry NARECHEM BNCR Izmir CR Antalya CR Moscow Region CR
Years 3-first 3-last 3-first 3-last 3-first 3-last 3-first 3-last 3-first 3-last
Leukemia
AIR 49.1 56.6 38.7 48.6 46.9 58.2 52.6 60.1 45.7 43.2
CIR 43.7 54.4 35.2 47.2 45.0 53.5 48.2 54.9 37.5 41.8
% annual change
(95 % CI), p value
1.7 (0.4, 3.0), 0.01 3.5 (1.6, 5.5), 0.0002 2.7 (-0.1, 5.6), 0.06 0.9 (-8.7, 11.5), 0.86 2.7 (-0.3, 5.9), 0.08
AMR 12.1 5.6 21.7 12.0 NA NA 16.7 4.0
CMR 11.6 5.6 20.8 12.0 NA NA 14.3 3.8
% annual change
(95 % CI), p value
-4.5 (-8.0, -0.9),
0.02
-3.7 (-6.6, -0.8),
0.01
NA NA -9.9 (-15.5, -4.0),
0.001
Lymphoma
AIR 16.7 17.1 17.0 14.0 17.0 24.8 18.4 17.3 14.6 13.0
Crude IR 18.1 17.8 17.9 14.6 17.9 25.2 17.9 17.0 17.8 13.4
% annual change
(95 % CI), p value
-0.5 (-2.7, 1.7), 0.64 -2.1 (-4.8, 0.8), 0.15 3.7 (-0.5, 8.1), 0.08 2.3 (-12.6, 19.8),
0.78
-3.0 (-7.6, 1.8), 0.22
Average AMR 0.8 2.9 5.2 3.5 NA NA 2.1 2.2
Crude MR 0.7 2.9 5.2 3.3 NA NA 2.9 2.3
% annual change
(95 % CI), p value
8.2 (0.2, 16.9), 0.05 -5.3 (11.0, 0.8), 0.09 NA NA -4.6 (-16.6, 9.2), 0.49
NA Not available
2000-2010
1996-2007
1998-2008
1996-2009
1996-2010
AIR for leukemia -Annual increase (%, 95%CIs) in each Registry
+2.7 (-0.3, +5.9)
+2.7 (-0.1, +5.6)
+0.9 (-8.7, +11.5)
+3.5 (+1.6, +5.5)
+1.7 (+0.4, +3.0)
AMR for leukemia -Annual decrease (%, 95%CIs) in each Registry
-9.9 (-15.5, -4.0) Moscow
Not available
-3.7 (-6.6, -0.8)
-4.5 (-8.0, -0.9)
Izmir /
Antalya
Bulgaria
Greece
2000-2010
1996-2009
1996-2010
a
b
Fig. 1 a AIR for leukemia. Annual increase (%, 95 % CIs) in each
Registry. b AMR for leukemia. Annual decrease (%, 95 % CIs) in
each Registry
Cancer Causes Control (2013) 24:1111–1118 1113
123
Author's personal copy

than the corresponding AMRs for Greece (p = 0.002) and
Moscow Region (p \ 0.001), especially during the last
period.
In contrast to leukemia, results about lymphoma showed no
significant trends in AIRs; Moscow Region displayed the
lowest AIRs (Moscow vs. Izmir p = 0.0015). Concerning
mortality, Bulgaria appeared to have a considerably higher
AMR than the other two Registries with available data for the
initial 3 years, reaching significance versus Greece
(p \ 0.001); the sizably lower starting mortality rate (first
3-year period) in Greece might have resulted in the increasing
trend observed in the most recent period (p = 0.05). Sup-
plemental Figs. 1 and 2 present the comparisons between
countries regarding incidence and mortality rates.
In Table 2, the distribution of the sociodemographic and
disease characteristics among the studied regions is dis-
played for the total of 3,041 incident childhood leukemia and
1,183 lymphoma cases. The known preponderance of males
was noted; considerable differentials pertaining to age were
observed (p = 0.003), with infant leukemia occurrence
being higher in Turkey and leukemia in children 10? year
old being more common in Bulgaria. Semi-urban place of
living was the predominant category for leukemia cases
reported from Greece and Bulgaria, whereas in Izmir and
Antalya, the majority of cases were living in urban areas
(p = 0.0001 for place of residence). Of note is the very low
proportion of other than ALL or AML leukemias in Greece,
which should also be interpreted along with the favorable
survival in this country (82.1 %).
As expected, lymphomas were more common among
boys. The high proportion of Burkitt lymphoma in Greece
and Turkey ([21 %) and the disparities in survival from
87 % in Greece and Moscow Region to 70 % in Bulgaria
seem notable.
In Supplemental Table 1, survival (vital) status by soci-
odemographic and disease characteristics are presented;
these results serve descriptive purposes only, as they are not
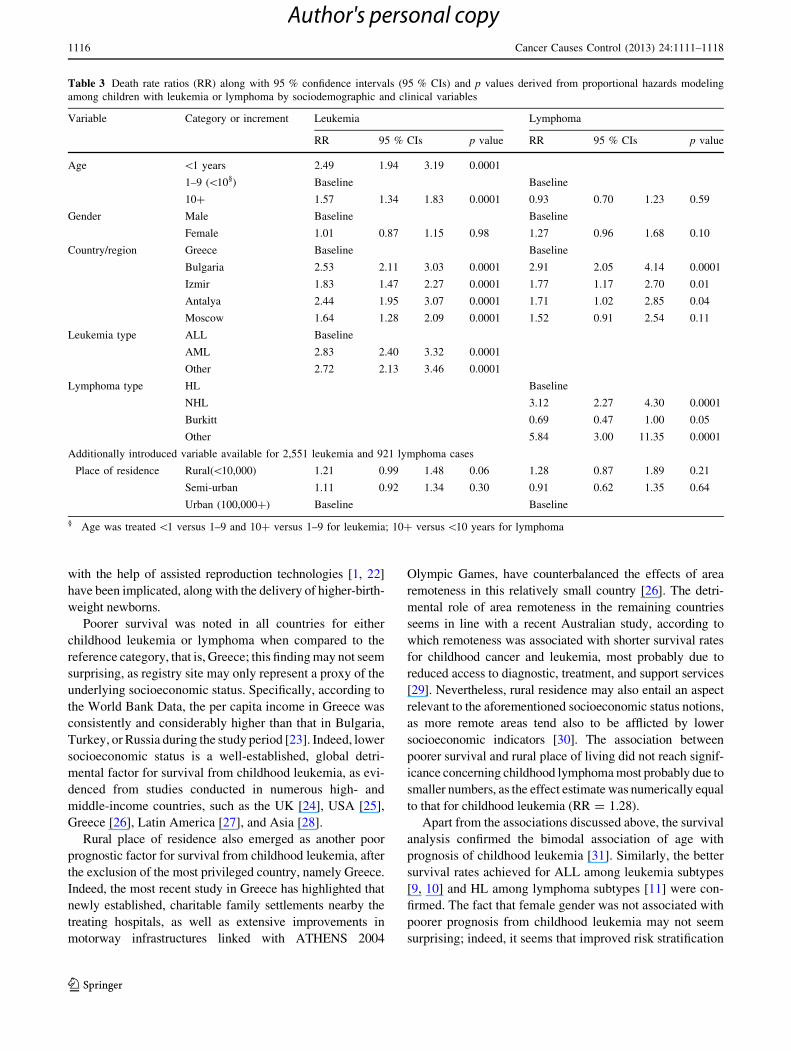
mutually adjusted. Table 3 quantifies these results by age:
indeed, infants (B1 year old) were more than 2 times more
likely to die from leukemia compared with standard age risk
children (1–9 years), the latter having also better survival
compared with older children. Likewise, the risk of death
was more than twofold higher among children diagnosed
with AML and ‘‘other leukemia’’ subtypes, compared with
ALL. It is worth noting that an established risk factor, namely
male gender, did not seem to exert a sizeable role; moreover,
the risk of death in the other four participating sites was
1.5–2.5 times higher compared with that in Greece. Lastly,
rural place of residence seemed to increase marginally the
risk of dying by 21 % (p = 0.06); nevertheless, at a post hoc
sensitivity analysis excluding the best performing country
(Greece), area remoteness reached formal significance as
both semi-urban (RR = 1.28, p = 0.03) and rural (RR =
1.17, p = 0.04) places of residence were associated with
poorer survival (Supplemental Table 2). As a rule, the sub-
analysis on ALL, which comprised over 80 % of the total
leukemias, replicated the overall results (Supplemental
Table 3).
Concerning the survival analysis for lymphoma, a 27 %
detrimental effect of gender was noted that did not reach
nominal statistical significance (p value: 0.10). The out-
come by disease subtype was better for HL, as expected.
The country of origin seemed to follow the pattern noted in
childhood leukemia. Finally, lymphoma cases living in
rural areas had 28 % increased death rates than those
residing in urban areas, although this result did not reach
significance.
Discussion
The main messages of this study pertain to the uniform
improvement in mortality rates for childhood leukemia,
together with increasing incidence rates, predominantly for
Greece and Bulgaria. On the contrary, regarding childhood
lymphoma, no sizable, consistent patterns were observed
either at the level of mortality or at the level of incidence.
Importantly, predictors modifying survival from childhood
leukemia in this cross-national setting included also rural
place of living and country, apart from the rather well-
established effects of age and leukemia type.
The present, favorable findings regarding the evolution
of mortality rates seem in accordance with the conclusions
of the most recent EU-wide study, pointing to room for
further improvement in the Southern-Eastern European
countries [5] along their trajectory to convergence with
their Northern and Western EU counterpart states. The
background reasons for the globally observed improvement
in mortality and survival trends may encompass the
implementation and administration of multidrug chemo-
therapy protocols, the development of supportive measures
limiting the effects of toxicity, the progress in bone marrow
transplantation, and improved diagnostic methods [6].
The increasing rates in the incidence of childhood leukemia
may be inscribed into the wider context of upward incidence
figures reported in the USA (1992–2004) [3] and the Europe-
wide Automated Childhood Cancer Information System
(ACCIS) project (1978–1997) [1]. Similar data have appeared
from country-specific studies over various periods, such as the
UK (1971–2000) [8], Spain (1983–2002) [12], Germany
(1987–2004) [13], Italy (1967–2001) [14]; nevertheless, the
Nordic countries (1982–2001) [15] and Canada (1999–2006)
[16] have reported stable childhood leukemia rates during the
most recent years. Interestingly, the present study, encom-
passing four additional years, when compared to the previous
NARECHEM Greek study (1996–2006) [17], has allowed the
1114 Cancer Causes Control (2013) 24:1111–1118
123
Author's personal copy

detection of the significant upward trend, most possibly due to
larger statistical power and longer study period. At a patho-
physiological level, the underlying explanation remains elu-
sive; changes in lifestyle habits, decreased crowding index in
the family [18] and day care [13], modifications in maternal
diet [19], decreasing exposure to infectious agents [20] or
underlying trends of atopic disease [21], or even growingly
larger proportion of otherwise infertile women giving birth
Table 2 Distribution of the 3,041 leukemia and 1,183 lymphoma incident cases recorded circa 1996–2010 in the 5 Cancer Registries by study
variables and survival status as of 31 December 2010
Greece Bulgaria Izmir-Turkey Antalya Turkey Moscow Region p value§
N % N % N % N % N %
Leukemia
Age (years) 0.003
\1 47 3.9 31 4.6 30 7.1 19 5.9 14 3.5
1–9 939 77.3 473 70.1 298 70.1 242 74.9 305 75.7
10? 229 18.8 171 25.3 97 22.8 62 19.2 84 20.8
Sex 0.26
Male 688 56.6 365 54.1 220 51.8 191 59.1 224 55.6
Female 527 43.4 310 45.9 205 48.2 132 40.9 179 44.4
Place of residence 0.0001
Rural \10,000 341 29.9 188 27.9 41 9.6 74 23.9 MA MA
Semi-urban 553 48.5 275 40.7 36 8.5 107 34.5
Urban 100,000? 247 21.6 212 31.4 348 81.9 129 41.6
Type 0.0001
ALL 1056 86.9 530 78.5 328 77.2 246 76.2 320 79.4
AML 143 11.8 90 13.3 72 16.9 50 15.5 61 15.1
Other 16 1.3 55 8.2 25 5.9 27 8.3 22 5.5
Status 0.0001
Dead 217 17.9 273 40.4 135 31.8 116 35.9 93 23.1
Alive 998 82.1 402 59.6 290 68.2 207 64.1 310 76.9
Lymphoma
Age (years) 0.0001
\10 215 50.9 149 51.0 111 58.4 85 70.3 53 33.5
10? 207 49.1 143 49.0 79 41.6 36 29.7 105 66.5
Sex 0.01
Male 302 71.6 200 68.5 129 67.9 66 54.6 101 63.9
Female 120 28.4 92 31.5 61 32.1 55 45.4 57 36.1
Place of residence 0.0001
Rural \10,000 96 29.5 83 28.4 19 10.0 37 32.5 MA MA
Semi-urban 179 55.1 111 38.0 18 9.5 35 30.7
Urban 100,000? 50 15.4 98 33.6 153 80.5 42 36.8
Type 0.0001
HL 173 41.0 160 54.8 73 38.4 39 32.2 84 53.2
NHL, non-Burkitt 139 32.9 98 33.5 74 38.9 50 41.3 48 30.4
Burkitt 110 26.1 25 8.6 40 21.1 25 20.7 22 13.9
Other 0 0.0 9 3.1 3 1.6 7 5.8 4 2.5
Status 0.0001
Dead 52 12.3 87 29.8 38 20.0 22 18.2 21 13.3
Alive 370 87.7 205 70.2 152 80.0 99 81.8 137 86.7
Place of residence is missing for 490 leukemia cases (74 for Greece, 13 for Antalya, and 403 for Moscow Region) and for 262 lymphoma cases
(97 for Greece, 7 for Antalya, and 158 for Moscow Region)§ p values derived from chi-square test
Cancer Causes Control (2013) 24:1111–1118 1115
123
Author's personal copy
with the help of assisted reproduction technologies [1, 22]
have been implicated, along with the delivery of higher-birth-
weight newborns.
Poorer survival was noted in all countries for either
childhood leukemia or lymphoma when compared to the
reference category, that is, Greece; this finding may not seem
surprising, as registry site may only represent a proxy of the
underlying socioeconomic status. Specifically, according to
the World Bank Data, the per capita income in Greece was
consistently and considerably higher than that in Bulgaria,
Turkey, or Russia during the study period [23]. Indeed, lower
socioeconomic status is a well-established, global detri-
mental factor for survival from childhood leukemia, as evi-
denced from studies conducted in numerous high- and
middle-income countries, such as the UK [24], USA [25],
Greece [26], Latin America [27], and Asia [28].
Rural place of residence also emerged as another poor
prognostic factor for survival from childhood leukemia, after
the exclusion of the most privileged country, namely Greece.
Indeed, the most recent study in Greece has highlighted that
newly established, charitable family settlements nearby the
treating hospitals, as well as extensive improvements in
motorway infrastructures linked with ATHENS 2004
Olympic Games, have counterbalanced the effects of area
remoteness in this relatively small country [26]. The detri-
mental role of area remoteness in the remaining countries
seems in line with a recent Australian study, according to
which remoteness was associated with shorter survival rates
for childhood cancer and leukemia, most probably due to
reduced access to diagnostic, treatment, and support services
[29]. Nevertheless, rural residence may also entail an aspect
relevant to the aforementioned socioeconomic status notions,
as more remote areas tend also to be afflicted by lower
socioeconomic indicators [30]. The association between
poorer survival and rural place of living did not reach signif-
icance concerning childhood lymphoma most probably due to
smaller numbers, as the effect estimate was numerically equal
to that for childhood leukemia (RR = 1.28).
Apart from the associations discussed above, the survival
analysis confirmed the bimodal association of age with
prognosis of childhood leukemia [31]. Similarly, the better
survival rates achieved for ALL among leukemia subtypes
[9, 10] and HL among lymphoma subtypes [11] were con-
firmed. The fact that female gender was not associated with
poorer prognosis from childhood leukemia may not seem
surprising; indeed, it seems that improved risk stratification
Table 3 Death rate ratios (RR) along with 95 % confidence intervals (95 % CIs) and p values derived from proportional hazards modeling
among children with leukemia or lymphoma by sociodemographic and clinical variables
Variable Category or increment Leukemia Lymphoma
RR 95 % CIs p value RR 95 % CIs p value
Age \1 years 2.49 1.94 3.19 0.0001
1–9 (\10§) Baseline Baseline
10? 1.57 1.34 1.83 0.0001 0.93 0.70 1.23 0.59
Gender Male Baseline Baseline
Female 1.01 0.87 1.15 0.98 1.27 0.96 1.68 0.10
Country/region Greece Baseline Baseline
Bulgaria 2.53 2.11 3.03 0.0001 2.91 2.05 4.14 0.0001
Izmir 1.83 1.47 2.27 0.0001 1.77 1.17 2.70 0.01
Antalya 2.44 1.95 3.07 0.0001 1.71 1.02 2.85 0.04
Moscow 1.64 1.28 2.09 0.0001 1.52 0.91 2.54 0.11
Leukemia type ALL Baseline
AML 2.83 2.40 3.32 0.0001
Other 2.72 2.13 3.46 0.0001
Lymphoma type HL Baseline
NHL 3.12 2.27 4.30 0.0001
Burkitt 0.69 0.47 1.00 0.05
Other 5.84 3.00 11.35 0.0001
Additionally introduced variable available for 2,551 leukemia and 921 lymphoma cases
Place of residence Rural(\10,000) 1.21 0.99 1.48 0.06 1.28 0.87 1.89 0.21
Semi-urban 1.11 0.92 1.34 0.30 0.91 0.62 1.35 0.64
Urban (100,000?) Baseline Baseline
§ Age was treated \1 versus 1–9 and 10? versus 1–9 for leukemia; 10? versus \10 years for lymphoma
1116 Cancer Causes Control (2013) 24:1111–1118
123
Author's personal copy

and newer chemotherapy regimens have eliminated the
previous independent prognostic significance of gender, as
observed in the most recent Nordic Society of Paediatric
Haematology and Oncology (NOPHO) data [32].
Regarding limitations of this study, the fact that the survival
analysis comprised data from all five Registries, whereas the
figures on mortality rates did not include data from Izmir and
Antalya, may not seem mutually contradictory. Specifically,
the survival analysis included data from incident cases during
the study period, whereas mortality data were based on cases
dying during the study period; inconsistencies regarding the
follow-up of earlier cases in the Turkish Registries did not
allow the inclusion of the latter in the analysis of mortality
trends. Other limitations of the present effort include the fact
that more sophisticated models, such as joint-point regression
analysis, were not implemented, whereas the fact that the
study periods for each Registry did not absolutely coincide
should also be declared. Moreover, time trends in the validity
of the registration process could theoretically represent a key
limitation affecting the observed trends; nevertheless, the fact
that all five included Registries provide data to International
Association for Research on Cancer (IARC)-related databases
may underline the validity and quality of the included Registries.
In conclusion, this study points to a uniform improve-
ment in mortality rates from childhood leukemia and
lymphoma in Southern–Eastern Europe, although of dif-
ferent size. The increasing incidence trends follow soci-
odemographic trends seen elsewhere, whereas the nature of
the underlying pathophysiological mechanisms remains to
be explored. Socioeconomic status consistently as a mul-
tipotent factor underlies the study findings about inequality
in survival between and within countries, which seemed
also of special interest, as constantly changing financial
conditions and local economic crises in the region may
modify the picture portrayed herein in the future.
Acknowledgments This study has been supported in part by the
National and Kapodistrian University of Athens. Special thanks are
due to Nick Dessypris for his contribution in the collection and
analysis of the data.
References
1. Kaatsch P, Steliarova-Foucher E, Crocetti E, Magnani C, Spix C,
Zambon P (2006) Time trends of cancer incidence in European
children (1978–1997): report from the Automated Childhood
Cancer Information System project. Eur J Cancer 42:1961–1971
2. Coebergh JW, Reedijk AM, de Vries E, Martos C, Jakab Z,
Steliarova-Foucher E, Kamps WA (2006) Leukaemia incidence
and survival in children and adolescents in Europe during
1978–1997. Report from the Automated Childhood Cancer
Information System project. Eur J Cancer 42:2019–2036
3. Linabery AM, Ross JA (2008) Trends in childhood cancer inci-
dence in the U.S. (1992–2004). Cancer 112:416–432
4. Centers for Disease Control and Prevention (CDC) (2007) Trends
in childhood cancer mortality–United States, 1990–2004.
MMWR Morb Mortal Wkly Rep 56:1257–1261
5. Bosetti C, Bertuccio P, Chatenoud L, Negri E, Levi F, La Vecchia
C (2010) Childhood cancer mortality in Europe, 1970–2007. Eur
J Cancer 46:384–394
6. Chatenoud L, Bertuccio P, Bosetti C, Levi F, Negri E, La Vecchia
C (2010) Childhood cancer mortality in America, Asia, and
Oceania, 1970 through 2007. Cancer 116:5063–5074
7. Thames Cancer Registry (1994) Cancer in South East England,
1991: cancer incidence, prevalence and survival in residents of
the district health authorities in South East England. Thames
Cancer Registry, Sutton, p 43
8. Shah A, Coleman MP (2007) Increasing incidence of childhood
leukaemia: a controversy re-examined. Br J Cancer 97:1009–1012
9. Pui CH, Mullighan CG, Evans WE, Relling MV (2012) Pediatric
acute lymphoblastic leukemia: where are we going and how do
we get there? Blood 120:1165–1174
10. Colby-Graham MF, Chordas C (2003) The childhood leukemias.
J Pediatr Nurs 18:87–95
11. Pulte D, Gondos A, Brenner H (2008) Trends in 5- and 10-year
survival after diagnosis with childhood hematologic malignancies
in the United States, 1990–2004. J Natl Cancer Inst 100:
1301–1309
12. Peris-Bonet R, Salmeron D, Martinez-Beneito MA, Galceran J,
Marcos-Gragera R, Felipe S, Gonzalez V, Sanchez de Toledo
Codina J (2010) Childhood cancer incidence and survival in
Spain. Ann Oncol 21(Suppl 3):iii103–iii110
13. Spix C, Eletr D, Blettner M, Kaatsch P (2008) Temporal trends in
the incidence rate of childhood cancer in Germany 1987–2004.
Int J Cancer 122:1859–1867
14. Dalmasso P, Pastore G, Zuccolo L, Maule MM, Pearce N, Mer-
letti F, Magnani C (2005) Temporal trends in the incidence of
childhood leukemia, lymphomas and solid tumors in north-west
Italy, 1967–2001. A report of the Childhood Cancer Registry of
Piedmont. Haematologica 90:1197–1204
15. Hjalgrim LL, Rostgaard K, Schmiegelow K, Soderhall S, Kol-
mannskog S, Vettenranta K, Kristinsson J, Clausen N, Melbye M,
Hjalgrim H, Gustafsson G (2003) Age- and sex-specific incidence
of childhood leukemia by immunophenotype in the Nordic
countries. J Natl Cancer Inst 95:1539–1544
16. Mitra D, Shaw AK, Hutchings K (2012) Trends in incidence of
childhood cancer in Canada, 1992–2006. Chronic Dis Inj Can
32:131–139
17. Petridou ET, Pourtsidis A, Dessypris N, Katsiardanis K, Baka M,
Moschovi M, Polychronopoulou S, Koliouskas D, Sidi V, Atha-
nasiadou-Piperopoulou F, Kalmanti M, Belechri M, La Vecchia
C, Curado MP, Skalkidis I (2008) Childhood leukaemias and
lymphomas in Greece (1996–2006): a nationwide registration
study. Arch Dis Child 93:1027–1032
18. Petridou E, Trichopoulos D, Kalapothaki V, Pourtsidis A, Ko-
gevinas M, Kalmanti M, Koliouskas D, Kosmidis H, Panagiotou
JP, Piperopoulou F, Tzortzatou F (1997) The risk profile of
childhood leukaemia in Greece: a nationwide case–control study.
Br J Cancer 76:1241–1247
19. Petridou E, Ntouvelis E, Dessypris N, Terzidis A, Trichopoulos D
(2005) Maternal diet and acute lymphoblastic leukemia in young
children. Cancer Epidemiol Biomarkers Prev 14:1935–1939
20. Greaves MF, Alexander FE (1993) An infectious etiology for
common acute lymphoblastic leukemia in childhood? Leukemia
7:349–360
21. Schuz J, Morgan G, Bohler E, Kaatsch P, Michaelis J (2003)
Atopic disease and childhood acute lymphoblastic leukemia. Int J
Cancer 105:255–260
22. Petridou ET, Sergentanis TN, Panagopoulou P, Moschovi M,
Polychronopoulou S, Baka M, Pourtsidis A, Athanassiadou F,
Cancer Causes Control (2013) 24:1111–1118 1117
123
Author's personal copy

Kalmanti M, Sidi V, Dessypris N, Frangakis C, Matsoukis IL,
Stefanadis C, Skalkidou A, Stephansson O, Adami HO, Kieler H
(2012) In vitro fertilization and risk of childhood leukemia in
Greece and Sweden. Pediatr Blood Cancer 58:930–936
23. The World Bank. GNI per capita, Atlas method (current US$)
24. Lightfoot TJ, Johnston WT, Simpson J, Smith AG, Ansell P,
Crouch S, Roman E, Kinsey SE (2012) Survival from childhood
acute lymphoblastic leukaemia: the impact of social inequality in
the United Kingdom. Eur J Cancer 48:263–269
25. Kent EE, Sender LS, Largent JA, Anton-Culver H (2009) Leu-
kemia survival in children, adolescents, and young adults: influ-
ence of socioeconomic status and other demographic factors.
Cancer Causes Control 20:1409–1420
26. Sergentanis TN, Dessypris N, Kanavidis P, Skalkidis I, Baka M,
Polychronopoulou S, Athanassiadou F, Stiakaki E, Fragandrea I,
Moschovi M, Petridou ET (2012) Socio-economic status, area
remoteness and survival from childhood leukemia: results from
the Nationwide Registry for Childhood Hematological Malig-
nancies (NARECHEM) in Greece. Eur J Cancer Prev 12 Dec
2012 [Epub ahead of print]
27. Bonilla M, Gupta S, Vasquez R, Fuentes SL, deReyes G, Ribeiro
R, Sung L (2010) Predictors of outcome and methodological
issues in children with acute lymphoblastic leukaemia in El
Salvador. Eur J Cancer 46:3280–3286
28. Tang Y, Xu X, Song H, Yang S, Shi S, Wei J (2008) Long-term
outcome of childhood acute lymphoblastic leukemia treated in
China. Pediatr Blood Cancer 51:380–386
29. Youlden DR, Baade PD, Valery PC, Ward LJ, Green AC, Aitken
JF (2011) Differentials in survival for childhood cancer in Aus-
tralia by remoteness of residence and area disadvantage. Cancer
Epidemiol Biomarkers Prev 20:1649–1656
30. Eurostat. Regional gross domestic product (PPS per inhabitant)
by NUTS 2 regions
31. Donadieu J, Auclerc MF, Baruchel A, Perel Y, Bordigoni P,
Landman-Parker J, Leblanc T, Cornu G, Sommelet D, Leverger
G, Schaison G, Hill C (2000) Prognostic study of continuous
variables (white blood cell count, peripheral blast cell count,
haemoglobin level, platelet count and age) in childhood acute
lymphoblastic leukaemia. Analysis of a population of 1545
children treated by the French Acute Lymphoblastic Leukaemia
Group (FRALLE). Br J Cancer 83:1617–1622
32. Schmiegelow K, Forestier E, Hellebostad M, Heyman M, Kris-
tinsson J, Soderhall S, Taskinen M (2010) Long-term results of
NOPHO ALL-92 and ALL-2000 studies of childhood acute
lymphoblastic leukemia. Leukemia 24:345–354
1118 Cancer Causes Control (2013) 24:1111–1118
123
Author's personal copy