OralEnoxacin forInfection Prevention inAdults withAcute Nonlymphocytic Leukemia
10
10.1128/AAC.37.3.474. 1993, 37(3):474. DOI: Antimicrob. Agents Chemother. Bond G H Talbot, P A Cassileth, L Paradiso, R Correa-Coronas and L Enoxacin Prophylaxis Study Group. with acute nonlymphocytic leukemia. The Oral enoxacin for infection prevention in adults http://aac.asm.org/content/37/3/474 Updated information and services can be found at: These include: CONTENT ALERTS more» cite this article), Receive: RSS Feeds, eTOCs, free email alerts (when new articles http://journals.asm.org/site/misc/reprints.xhtml Information about commercial reprint orders: http://journals.asm.org/site/subscriptions/ To subscribe to to another ASM Journal go to: on December 4, 2013 by guest http://aac.asm.org/ Downloaded from on December 4, 2013 by guest http://aac.asm.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of OralEnoxacin forInfection Prevention inAdults withAcute Nonlymphocytic Leukemia

10.1128/AAC.37.3.474.
1993, 37(3):474. DOI:Antimicrob. Agents Chemother. BondG H Talbot, P A Cassileth, L Paradiso, R Correa-Coronas and L Enoxacin Prophylaxis Study Group.with acute nonlymphocytic leukemia. The Oral enoxacin for infection prevention in adults
http://aac.asm.org/content/37/3/474Updated information and services can be found at:
These include:
CONTENT ALERTS more»cite this article),
Receive: RSS Feeds, eTOCs, free email alerts (when new articles
http://journals.asm.org/site/misc/reprints.xhtmlInformation about commercial reprint orders: http://journals.asm.org/site/subscriptions/To subscribe to to another ASM Journal go to:
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from
on D
ecember 4, 2013 by guest
http://aac.asm.org/
Dow
nloaded from

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Mar. 1993, p. 474-4820066-4804/93/030474-09$02.00/0Copyright © 1993, American Society for Microbiology
Oral Enoxacin for Infection Prevention in Adults with AcuteNonlymphocytic Leukemia
GEORGE H. TALBOT,lt* PETER A. CASSILETH,2 LINDA PARADISO,3 RAFAEL CORREA-CORONAS,3LYNNE BOND,3 AND THE ENOXACIN PROPHYLAXIS STUDY GROUPt
Infectious Diseases Section' and Hematology-Oncology Section,2 Department of Medicine,University ofPennsylvania Medical Center, Philadelphia, Pennsylvania, and
Parke-Davis Pharmaceutical Research, Inc., Ann Arbor, Michigan3
Received 10 June 1992/Accepted 23 December 1992
A randomized, double-blind, placebo-controlled trial was conducted in eight hematologic units to determinethe efficacy and safety of oral enoxacin for infection prevention in adult patients with acute nonlymphocyticleukemia. One hundred nineteen patients undergoing remission induction or consolidation chemotherapy wereenrolled; 62 of them received enoxacin (400 mg orally every 12 h). Patients received antifungal prophylaxis withoral mycostatin (1,000,000 U four times daily) or clotrimazole (1 troche five times daily). Analysis was
performed on an intent-to-treat basis. There was no significant difference between groups in race, age, or typeand stage of leukemia, but there were more males in the placebo group (P = 0.073 [Fisher's exact test]). Fewerenoxacin patients had gram-negative bacteremia (1 versus 14 [P < 0.001]), gram-negative infection at any site(2 versus 19 [P < 0.001]), or bacterial and/or fungal infection (17 versus 26 [P = 0.056]). There was no significantdifference in the number of patients with gram-positive infection at any site (12 versus 16), gram-positivebacteremia (9 versus 10), deep fungal infection (6 versus 2), death (2 versus 3), other antimicrobial therapyrequired (48 versus 48), therapy with amphotericin B (15 versus 7 [P = 0.105]), any adverse event (45 versus 36),or any study drug-associated adverse events (13 versus 6). Logistic regression confirmed (odds ratios and 95%confidence intervals are given in parentheses) that enoxacin reduced the risk of gram-negative infection (0.07;0.01 to 0.30), especially gram-negative bacillary bacteremia (0.05; 0.01 to 0.37), without altering the risk ofgram-positive bacterial (0.63; 0.26 to 1.5), deep fungal (2.57; 0.47 to 13.9), or Clostridium difficile (1.16; 0.3 to4.56) infection. The median time to the onset of fever of 102.80F (39.3°C) was 32 days for the enoxacin groupversus 15 days for patients receiving placebo (P = 0.0007 [Wilcoxon test]). In patients with acute nonlymphocyticleukemia, oral enoxacin prevents gram-negative infections, delays the onset of fever, does not alter the incidenceof gram-positive or proven deep fungal infections, and is well tolerated.
Granulocytopenic patients are at a substantial risk ofbacterial infection, which is directly related to the durationand degree of the granulocyte nadir (2). The gastrointestinal(GI) tract is a major source of infecting organisms, withintestinal colonization being the antecedent to bacterialtranslocation across the gut and systemic dissemination (5,18, 35, 39, 43). Recognition of these facts led to trials of oralnonabsorbable antibiotics for infection prevention in granu-locytopenic patients (5, 18, 38, 43). However, oral nonab-sorbable antibiotics such as vancomycin and colistin are
expensive and unpalatable (18, 38, 43). Premature discontin-uation of prophylactic treatment due to lack of tolerability
* Corresponding author.t Present address: Rhone-Poulenc Rorer Central Research, P.O.
Box 1200, Collegeville, PA 19426.t The Enoxacin Prophylaxis Study Group included the following
members: G. H. Talbot and P. A. Cassileth, University of Pennsyl-vania Medical Center, Philadelphia, Pa.; A. Raza and H. Preisler,Roswell Park Memorial Institute, Buffalo, N.Y.; W. R. Vogler,Emory University School of Medicine, Atlanta, Ga.; J. Goldberg,Regional Oncology Center, State University of New York, Syra-cuse, N.Y.; P. Wiernik and R. Gulcalp, Van Etten Hospital, Bronx,N.Y.; J. Mazza, Marshfield Clinic, Marshfield, Wis.; S. BenhamKahn, Hahneman Hospital and University, Philadelphia, Pa.; andJ. Hines, Cleveland Metropolitan General Hospital, Cleveland,Ohio.
has been associated with rebound GI bacterial overgrowthand, on occasion, subsequent infection (38).
Accordingly, focus switched to oral absorbable agentssuch as nalidixic acid and trimethoprim-sulfamethoxazole(TMP-SMX) for selective decontamination of the GI tract (4,8, 16-18, 34, 37, 38, 43). The latter in particular is capable ofpreventing infections in some granulocytopenic patient pop-ulations (4, 18, 37, 38, 43, 44). However, limitations of TMP-SMX include lack of efficacy in some groups studied, defi-cient in vitro activity against Pseudomonas aeruginosa,occasional emergence of bacterial resistance, rash, andpotential prolongation of the granulocyte nadir (5, 18, 29, 34,38, 44).
Introduction of the fluoroquinolones offered the possibilityof achieving selective intestinal decontamination without thedisadvantages of TMP-SMX and oral nonabsorbable antibi-otics (5, 20, 44). Indeed, subsequent to the initiation of our
study, it has been shown that the fluoroquinolones can
prevent gram-negative bacterial infections in granulocytope-nic patients (3, 7, 15, 21, 23, 40-42). However, some studiesincluded patients with a variety of underlying hematologicand oncological diseases (15, 23, 40, 42), which complicatesassessment of efficacy (10). In addition, all studies but one
were not placebo controlled, so that estimation of theabsolute efficacy and tolerability of prophylactic treatmentoften has not been possible (3, 7, 15, 23, 40, 42). To addressthese issues, we report our randomized, double-blind, pla-cebo-controlled multicenter study of oral enoxacin for infec-
474
Vol. 37, No. 3
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ENOXACIN IN ACUTE LEUKEMIA 475
tion prophylaxis in granulocytopenic patients with acutenonlymphocytic leukemia. (This work was presented in partat the 31st Interscience Conference on Antimicrobial Agentsand Chemotherapy, Chicago, Ill., 29 September to 2 October1991 [34a].)
MATERIALS AND METHODS
Eleven institutions across the United States were selectedfor participation. Institutional review board approval wasobtained at each site, and patients were required to givewritten informed consent before enrollment. Eligible pa-tients were males or nonpregnant, nonnursing females, aged18 years or older, diagnosed as having acute nonlymphocyticleukemia (subtypes Ml to M6 in the FAB classification [1]),and undergoing remission induction (either initial or firstrelapse) or consolidation chemotherapy.
Exclusion criteria included existing infection; history ofallergy to quinolones or azoquinolones; antimicrobial ther-apy for suspected infection within the 48 h preceding studyentry; initiation of antileukemia therapy >48 h previously;fever (temperature of >38.0°C [>100.4°F]); hepatic impair-ment (twice the upper limit of normal aspartate aminotrans-ferase level) and renal impairment (twice the upper limit ofnormal serum creatinine level), isolated hepatic impairment(three times the upper limit of normal aspartate aminotrans-ferase level), or isolated renal impairment (three times theupper limit of normal serum creatinine level); diagnosis ofchronic myelogenous leukemia in blast crisis, acute lympho-cytic leukemia, acute undifferentiated leukemia, or leukemiarefractory to chemotherapy; high probability of dying within1 week; concurrent allogeneic or autologous bone marrowtransplantation; participation in a phase II/III study with aninvestigational antileukemic agent; and prior enrollmentunder this protocol.
Identical 200-mg grey gelatin capsules of enoxacin orplacebo were supplied by Parke-Davis Pharmaceutical Re-search, Inc. Patients received 400 mg of enoxacin or placeboin a double-blind fashion every 12 h. Randomization wasstratified at each study center according to whether induc-tion or consolidation chemotherapy was intended. Drugadministration was to continue until the absolute granulo-cyte count (AGC) was 21,000/mm3 or was .500/mm3 con-sistently for 7 days or until 6 weeks of treatment had passed.Patients could extend treatment for another 6 weeks withpermission of P. Cassileth.No other antibacterial prophylaxis was allowed, but pro-
phylactic antiviral agents were permitted. Regimens for oraland rectal care and diet were not standardized so as toincrease the generalizability of the results; however, in nocenter was a life island or its equivalent used. It wasrecommended that systemic antibacterial therapy (an anti-pseudomonal penicillin or cephalosporin plus an antipseudo-monal aminoglycoside) be initiated whenever a granulocyto-penic patient developed a single fever of 238.3°C (101°F) ora temperature of 238.0°C (100.4°F) on two measurements>4 h apart within a 24-h period. Empirical amphotericin Btherapy was recommended for febrile granulocytopenic pa-tients with no apparent source of infection who did notrespond to 7 consecutive days of antibacterial therapy butcould be added sooner at the investigator's discretion.Each febrile episode (fever of >38.0OC [100.40F] from any
cause) was categorized as due to either (i) microbiologicallydocumented infection (a febrile episode accompanied byadditional signs and symptoms of infection including micro-biological confirmation), (ii) clinically documented infection
(a febrile episode accompanied by additional signs andsymptoms of infection, treated with antimicrobial agents butlacking microbiological confirmation), (iii) indeterminatecause (a febrile episode not conforming to the first twocategories above, but in which antimicrobial therapy wasadministered), or (iv) noninfectious cause (a febrile episodein which, a noninfectious cause was documented or sus-pected and in which no antimicrobial therapy was given). Afebrile episode was considered to have ended' when themaximum temperature was below 38°C for .2 days. Infec-tious fever was defined as fever in categories 1 to 3, i.e.,fever for which antibacterial therapy was administered.
Pathogens were tested for susceptibility to enoxacin bothby broth microdilution to determine the MIC and by diskdiffusion in agar to determine the zone diameter of completeinhibition (24, 25). In cases in which the two tests disagreed,the zone diameter was used to determine susceptibility brresistance.The interaction of enoxacin with theophylline has been
shown to raise the levels of theophylline in serum, some-times into the toxic range (22). Patients who were takingtheophylline or its derivatives were to have theophyllinelevels measured regularly and the dosage of theophyllineadjusted appropriately while on concomitant enoxacin.
All adverse events which occurred during the study wererecorded by the investigators, and the dates of onset andcessation, severity, relationship to and management of in-vestigational drug, and clinical outcome were specified foreach event.
Appropriate reasons for discontinuation of prophylaxiswere the following: a clearly drug-related adverse event orlaboratory abnormality interfering with ongoing antileuke-mic treatment, deterioration of hepatic and/or renal functionto the levels noted above, and extreme lack of patientcompliance.Sample size determinations for this study were based on
the assumption that during the entire study period 50% ofpatients receiving placebo would develop a microbiologi-cally proven infection. A sample size of 60 evaluable patientsper treatment group was calculated to guarantee a test thatwould detect a difference of 25 percentage points (i.e., adifference of 50% or more) in the infection rates of enoxacinand placebo with a 0.80 probability at an alpha level of 0.05in a two-sided test (6).An interim analysis was conducted after the enrollment of
approximately 30 patients per treatment group. Criticalvalues were based on the O'Brien-Fleming multiple testingmethod (26). To achieve an overall alpha level of 0.05, thecritical values for the chi-square statistic were estimated tobe 3.928 x 2 (equivalent to P < 0.005) for the midpointinterim analysis and 3.928 (equivalent to P < 0.048) for thefinal analysis. Safety of the treatment groups was alsoconsidered at the interim point. This interim analysis did notreach significance for safety or efficacy, so the study wascontinued to full enrollment.
Efficacy of enoxacin compared with that of placebo wasevaluated on an intent-to-treat basis for the following param-eters: all microbiologically documented infection, micro-biologically documented bacterial and/or fungal infection,gram-positive bacterial infection, gram-positive bacteremia,gram-negative bacterial infection, gram-negative bacillarybacteremia, Clostridium difficile diarrhea, fungal infection,clinically documented infection, infectious fever (febrileepisodes requiring antibacterial therapy), requirement forantimicrobial therapy other than the study drugs, recovery
VOL. 37, 1993
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
of the granulocyte count (AGC > 1,000 cells/mm3), anddeath.The incidence of each of the outcome parameters was
evaluated by using a two-tailed Fisher's exact test at the 5%level of significance. A 95% confidence interval for thedifference in proportions (enoxacin versus placebo) was
computed.Logistic regression was performed by using PROC LO-
GIST (32) in SAS (version 5.18) for each of the outcomeparameters and the following independent variables: treat-ment group, age (<65 or 265 years), sex, race, study center,baseline AGC (0 to 99, 100 to 499, 500 to 999, or .1,000/mm3), number of days with an AGC of <500/mm3, andchemotherapeutic stage (induction versus consolidation). Apreliminary model including all the independent variableswas fitted. Covariates were then retained or removed fromthe model according to their statistical significances, howwell the model fitted, and whether their inclusion in themodel was clinically reasonable.Time to event for each outcome was evaluated by deter-
mining the median and 95% confidence interval for eachtreatment group (33); significance testing was performedwith the Wilcoxon test.
RESULTS
A total of 119 patients from eight centers were enrolled,with 62 patients randomly assigned to the enoxacin treat-ment group and 57 patients randomly assigned to the placebotreatment group. Baseline characteristics of the treatmentgroups were similar (Table 1) except for a trend towardsmore males in the placebo group. In addition, there were no
significant differences between the groups with regard toconcurrent medical conditions or antimicrobial treatment inthe month prior to study entry.The dispositions of patients enrolled in the study are
shown in Table 2. Twenty-three (37%) patients in the enox-
acin treatment group and 20 (35%) patients in the placebotreatment group were eliminated from the study beforecompleting the anticipated 6 weeks of treatment. The mostfrequent reason for early withdrawal was the occurrence ofan adverse event.Enoxacin markedly decreased the frequency of gram-
negative bacterial infections, including bacteremia, withoutincreasing the risk of gram-positive bacterial, C. difficile, or
deep fungal infection (Tables 3 to 5). Consequently, enoxa-
cin patients had fewer microbiologically proven infectionsoverall. There was no effect on clinically documented infec-tions or on the number of patients requiring antibacterialtherapy for febrile episodes (infectious fever). Susceptibilitytesting of the pathogens isolated showed no evidence ofemergence of resistance; however, the number of gram-negative isolates in the enoxacin group was too low formeaningful comparisons (Table 3).The results of logistic regression modeling are displayed in
Table 5. Logistic regression confirmed that enoxacin treat-ment was an important independent variable, which de-creased (odds ratios and 95% confidence intervals are givenin parentheses) the risks of microbiologically documentedinfection (0.45; 0.21 to 0.97), gram-negative bacterial infec-tion (0.07; 0.01 to 0.3), and gram-negative bacillary bactere-mia (0.05; 0.01 to 0.37). Enoxacin treatment was not an
independent risk factor for gram-positive bacterial infection,gram-positive bacteremia, C. difficile diarrhea, deep fungalinfection, clinically documented infection, requirement for
TABLE 1. Patient characteristics
Value for groupaCharacteristic Enoxacin Placebo P
(n = 62) (n = 57)Gender 0.073Male 29 (47) 36 (63)Female 33 (53) 21 (37)
Race 0.768White 54 (87) 52 (91)Black 5 (8) 3 (5)Other 3 (5) 2 (4)
Age 0.635<65 yr 48 (77) 42 (74)>65 yr 14 (23) 15 (26)
Leukemia status 0.924Initial episode 27 (44) 25 (44)Postremission treatment 17 (27) 14 (25)Relapse 18 (29) 18 (32)
Acute leukemia type 0.155Myelogenous 26 (42) 30 (53)Promyelocytic 7 (11) 5 (9)Myelomonocytic 19 (31) 15 (26)Monocytic 1 (2) 3 (5)Erythroleukemia 8 (13) 1 (2)Megakaryocytic 1 (20) 1 (2)Not specified 0 (0) 2 (4)
Chemotherapy 0.353Induction 43 (69) 43 (75)Consolidation 17 (27) 14 (25)Not specified 2 (3) 0 (0)
Baseline granulocyte count" 0.1370-99 3 (5) 5 (9)
101-499 13 (21) 8 (14)500-999 9 (16) 8 (14).1,000 33 (53) 24 (42)Not specified 4 (6) 12 (21)
Patient-days of granulocytopeniac 0.9640-99 643 520
100-499 310 245500-999 156 126>1,000 285 240
a Percentages are given in parentheses.b Per cubic millimeter.Total number of days for all patients in a group with the indicated number
of granulocytes per cubic millimeter.
other antimicrobial therapy, or delayed granulocyte recov-ery.The median time to an event could not be calculated for
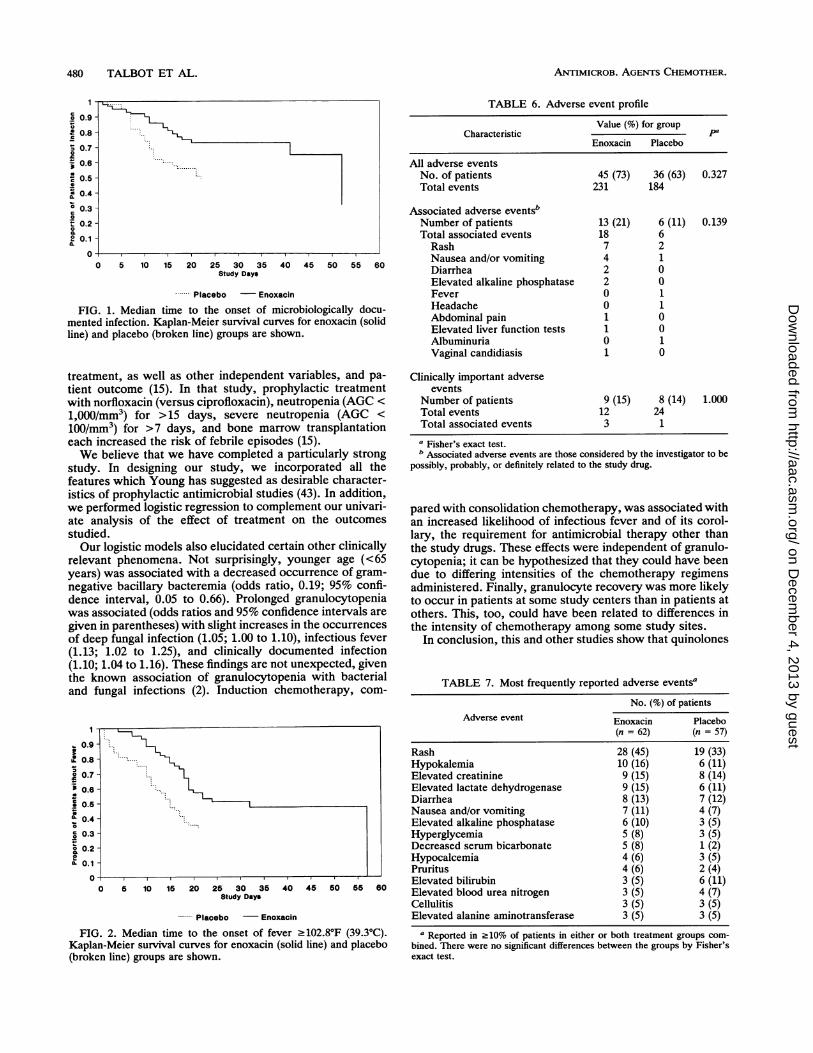
certain outcomes (gram-positive infection, gram-positivebacteremia, gram-negative infection, gram-negative bacil-lary bacteremia, C. difficile infection, and fungal infection)because too few events occurred. A calculable clinicallysignificant difference occurred for microbiologically docu-mented infection, with placebo-treated patients experiencinga median time to event of 22 days versus a median time toevent of 52 days for enoxacin-treated patients (Fig. 1). Inaddition, patients receiving placebo developed their firstmajor fever (temperature, .102.80F [39.3°C]) sooner thandid those receiving enoxacin (medians of 15 and 32 days,respectively [P = 0.0007] [Fig. 2]). Clinically nonsignificantdifferences occurred for infectious fever, clinically docu-mented infection, other antimicrobial therapy required, andgranulocyte recovery (data not shown).The antifungal prophylactic regimen (mycostatin alone,
clotrimazole alone, both mycostatin and clotrimazole, orneither) had no effect on the occurrence of fungal infection
476 TALBOT ET AL.
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ENOXACIN IN ACUTE LEUKEMIA 477
TABLE 2. Patient dispositions
No. (%) of patientsCharacteristic
Enoxacin Placebo Total
Randomly assigned to treatment 62 57 119
Withdrawn 23 (37) 20 (35) 43 (36)Adverse event 12 (19) 8 (14) 20 (17)Discharged while granulocytopenic 3 (5) 2 (4) 5 (4)Ineligiblea 3 (5) 2 (4) 5 (4)Noncompliant 2 (3) 2 (4) 4 (3)Personal reasons 0 (0) 3 (5) 3 (3)Error 0 (0) 2 (4) 2 (2)Death 2 (3) 0 (0) 2 (2)Doctor's recommendation 0 (0) 1 (2) 1 (1)Unable to take oral medications 1 (2) 0 (0) 1 (1)
Completed study 39 (63) 37 (65) 76 (64)a Including patient ineligibility, questionableness of the disease, and enroll-
ment in another study.
(incidence in the 111 patients for whom data are available,5.6, 7.0, 7.1, and 0% [0 of 1], respectively).Compliance with the study drug regimens was excellent.
Enoxacin patients missed (means and standard deviations)2.6 + 4.1 (range, 0 to 18) doses compared with 2.5 + 3.4(range, 0 to 15) doses for placebo patients.Adverse events (Tables 6 and 7) were summarized in
terms of both the number of affected patients and the totalnumber of reports. Forty-five (73%) patients in the enoxacingroup had 231 adverse events, while 36 (63%) patients in theplacebo group had 184 adverse events. Table 7 shows themost frequently reported adverse events, including all suchoccurrences and not just those considered to be associatedwith study drug therapy (i.e., considered by the investigatorto be possibly, probably, or definitely related to the studydrug). Six (11%) placebo patients and 13 (21%) enoxacinpatients were reported to have a total of 6 and 18 associatedadverse events, respectively. In the placebo group, therewere two cases of rash and one case each of fever, headache,nausea and/or vomiting, and albuminuria. In the enoxacingroup, there were seven cases of rash, four cases of nauseaand/or vomiting, two cases of diarrhea, two cases of elevatedalkaline phosphatase, one case of abdominal pain, one caseof increased liver function test, and one case of vaginalmoniliasis. One episode of nausea and/or vomiting in eachgroup was considered severe. There were no significantdifferences between groups in age distribution, the numberof deaths, severity of associated adverse events, or thenumber of patients who withdrew because of adverseevents.Two enoxacin-treated and three placebo-treated patients
died during the study. In the former group, causes werefungal infection and refractory leukemia; in the latter, etiol-ogies included fungal infection, infection of unspecified type,and unspecified cause. In no instance was death attributed tostudy drug therapy.Of five patients concurrently receiving theophylline, two
patients were in the enoxacin group and three patients werein the placebo group. The former patients reported 38 totaladverse events, while the latter patients reported 3 adverseevents. Symptoms reported by enoxacin patients includeddry mouth or throat, nausea and/or vomiting, diarrhea,confusion, tremor, twitching, and itching. Of note, however,only four adverse events (three of mild severity in the
TABLE 3. Distribution of causative pathogens among body sitesa
No. of isolatesOrganisms and site
Enoxacin Placebo Total
BacteriaBloodstream
Coagulase-negative staphylococcusAlpha streptococcusStaphylococcus aureusGroup D streptococcusEscherichia coliKiebsiella sp.Pseudomonas aeruginosaEscherichia coli and Staphylococcus
aureus
Gastrointestinal tractClostridium difficileBacteroides corrodens and other
bacteria
Skin and skin structureCoagulase-negative staphylococcusStaphylococcus aureusCoagulase-negative staphylococcusand Pseudomonas aeruginosa
Escherichia coli and Enterococcusfaecalis
Salmonella paratyphi
Urinary tractGroup D streptococcusCitrobacter NOSCorynebacterium sp.
VaginaGardnerella vaginalis and other bac-
teriaMixed gram-negative bacilli
Lower respiratory tractCoagulase-negative staphylococcusMixed gram-negative bacilli
Sinus, Acinetobacter sp. and group Dstreptococcus
FungiBloodstream, Candida sp.
Various sitesAspergillus sp.Alternaia sp.
Sinus and nose, Aspergillus sp.
Vagina, Candida albicans
Virus, oropharynx, herpes simplex
4 5 94 1 5
2 21 1
5 54 4
1 3 42 2
5 4 91 1
2
1
1
3 32
1 1
1 1
1 1
2 21 1
1
1
1 1
1 11 1
1 1
2 1 3
11
1 21
2
1
2
1
2 1 3
a Results (numbers of isolates) of susceptibility testing to enoxacin were asfollows. Coagulase-negative staphylococci: enoxacin group (E), two suscep-tible (S), zero resistant (R), and two not tested (NT); placebo group (P), eightS, zero R, and two NT. S. aureus: E, one S and one NT; P, three S and oneNT. Alpha streptococcus: E, two R and two NT; P, one NT. Group Dstreptococci including E. faecalis: E, one R; P, five R. Corynebacterium sp.:E, one R. E. coli: P, nine S. Klebsiella sp.: P, three S and one NT. P.aeruginosa: E, one NT; P, four S and one NT. Acinetobacter sp.: P, one S.Citrobacter sp.: P, one S. Salmonella sp.: P, one S.
VOL. 37, 1993
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
TABLE 4. Bacteriological and clinical efficacies
No. (%) of patientsOutcome ~~~~~~~~~~~~~~~~~~ConfidenceOutcome Enoxacin Placebo intervala
(n = 62) (n = 57)Infectious fever' 48 (77) 46 (81) -18 to 11 0.822Microbiologically documented infectiond 22 (35) 30 (53) -35 to 0 0.067Microbiologically documented bacterial and/or fungal infection 17 (27) 26 (46) -35 to -1 0.056Gram-positive bacterial infection 12 (19) 16 (28) -24 to 7 0.287Gram-positive bacteremia 9 (15) 10 (18) -16 to 10 0.803Gram-negative bacterial infection 2 (3) 19 (33) -43 to -17 <0.001Gram-negative bacillary bacteremia 1 (2) 14 (25) -35 to -11 <0.001C. difficile diarrhea 5 (8) 4 (7) -8 to 11 1.000Deep fungal infectione 6 (10) 2 (4) -3 to 15 0.276Clinically documented infection 38 (61) 41 (72) -27 to 6 0.248Other antimicrobial therapy required 48 (77) 48 (84) -21 to 7 0.365Amphotericin B therapy 15 (24) 7 (12) -26 to 2 0.105Granulocyte recovery 25 (40) 25 (44) -21 to 14 0.714Death 2 (3) 3 (5) -9 to 5 0.670
a 95% confidence interval for the difference in proportions.b Fisher's exact test.c Any febrile episode requiring antibacterial therapy.d Including all bacterial, viral, and fungal infections.e One enoxacin patient who developed vaginal candidiasis is not included.fAGC, .1,000/mm3.
enoxacin group and one of moderate severity in the placebogroup) in theophylline-treated patients were considered to beassociated with study drug therapy (as defined above).Hemoglobin, platelet count, leukocyte count, and AGC
showed no significant differences between the study groupsfor nadir count, day of nadir, or day of recovery. There wasa nonsignificant trend to prolonged recovery for each param-eter for enoxacin-treated patients.
DISCUSSION
Our study has shown that enoxacin prevents gram-nega-tive bacterial infections in granulocytopenic patients receiv-ing chemotherapy for acute nonlymphocytic leukemia. Thereduction in gram-negative bacteremia was especially pro-nounced. Enoxacin did not increase the frequency of gram-positive bacterial, C. difficile, or deep fungal infection inthese patients. Consequently, the rate of microbiologicallydocumented infections overall was lower for patients receiv-ing enoxacin. These successes were reflected in the obser-vation that the median time to development of a microbio-logically documented infection was 52 days for enoxacin-treated patients versus 22 days for placebo recipients.
Logistic regression models confirmed that enoxacin treat-ment independently reduced (odds ratios and 95% confi-dence intervals are given in parentheses) microbiologicallydocumented infection (0.45; 0.21 to 0.97), gram-negativebacterial infection (0.07; 0.01 to 0.30), and gram-negativebacillary bacteremia (0.05; 0.01 to 0.37) but did not affectgram-positive bacterial infection, gram-positive bacteremia,C. difficile diarrhea, deep fungal infection, clinically docu-mented infection, requirement for other antimicrobial ther-apy, or granulocyte recovery.Enoxacin, a new fluoroquinolone, is well absorbed from
the GI tract (20). It is widely distributed in body tissues, hasa half-life of about 6 to 7 h, and is cleared primarily by therenal route (20). Enoxacin is effective in vitro (MIC c 2,ug/ml) against multiply resistant clinical isolates of thefamily Enterobacteriaceae and of P. aeruginosa (19, 31).Henry also demonstrated good activity of enoxacin against
staphylococci but less effectiveness against Pseudomonasspp. and streptococci (19).A variety of studies have addressed the suitability of the
quinolones as agents for selective decontamination of thedigestive tract (9, 11-14, 27, 28, 30, 36). For example,Edlund et al. compared the effects of enoxacin and norflox-acin on colonic microflora in 10 healthy human volunteers(9). By day 7 of administration, both drugs markedly sup-pressed strains of the family Enterobacteriaceae whereasthe gram-positive and anaerobic microfloras were not signif-icantly altered. Pecquet et al. found that norfloxacin elimi-nated intestinal strains of the Enterobacteriaceae in humanvolunteers while the anaerobic flora was not substantiallychanged (27). Colonization resistance of gnotobiotic miceassociated with a human fecal flora was also studied. Nor-floxacin reduced colonization resistance for only 2 of 14strains tested.
Generally similar results have been observed for otherquinolones (12, 28, 30), although in some instances moresubstantial reductions of group D streptococci (12, 28) andBacteroides spp. (12) have been noted. In addition, resistantorganisms (fungi, staphylococci, and gram-negative bacilli)can appear in the feces (12, 28, 30).
Goldstein and Citron attempted to resolve the apparentdiscrepancy between the observation that anaerobic bacteriaare susceptible to norfloxacin and enoxacin at levels achiev-able in feces (13) and the finding that in laboratory animalsand granulocytopenic humans norfloxacin markedly reducesfecal aerobic bacteria while having minimal effect on theanaerobic flora. When antibiotic susceptibility was studiedby using an inoculum of 109 CFU/ml (to approximate actualfecal counts), a dramatic inoculum effect was present formany anaerobic strains but not for the Eschenichia colistrains tested (14).Enoxacin appears to be well suited for selective intestinal
decontamination because it is not highly susceptible to fecalinactivation (36). Studies of the fecal inactivation of thequinolones in vitro have found that the higher the concen-tration of fresh feces the greater the level of inactivation, asmeasured by MBCs (36). Nalidixic acid, pipemidic acid, aind
478 TALBOT ET AL.
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from
ENOXACIN IN ACUTE LEUKEMIA 479
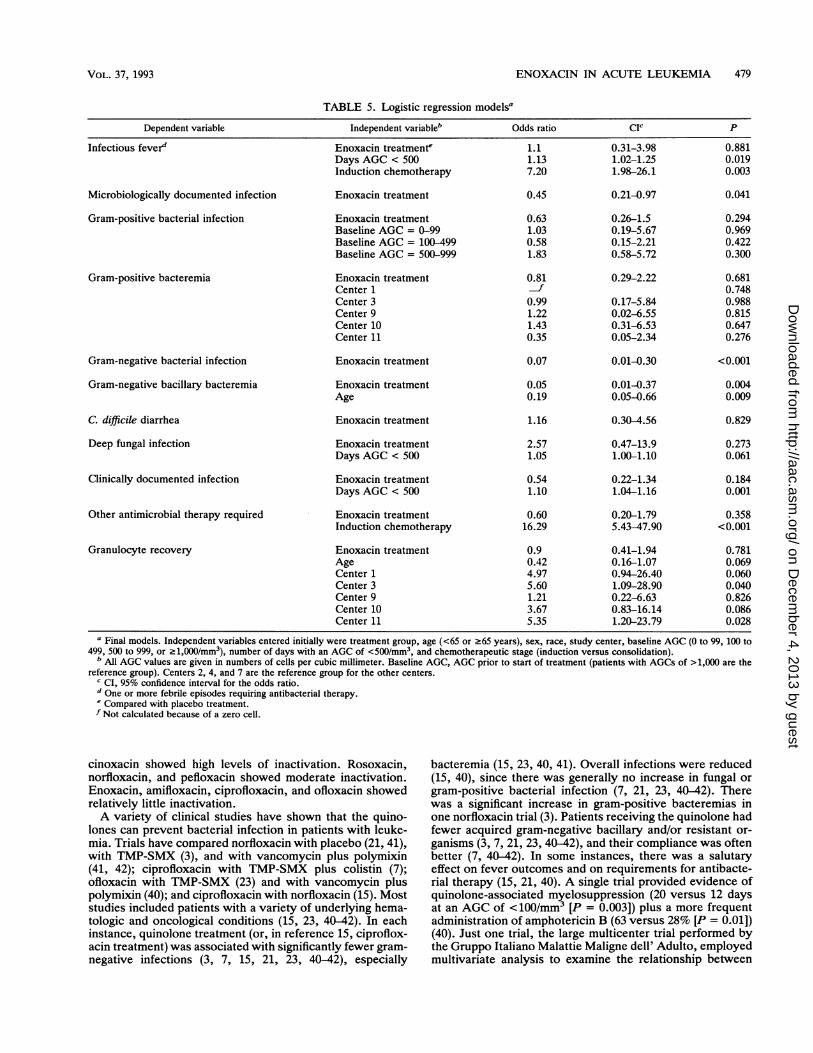
TABLE 5. Logistic regression modelsa
Dependent variable Independent variableb Odds ratio CIC P
Infectious fever" Enoxacin treatmente 1.1 0.31-3.98 0.881Days AGC < 500 1.13 1.02-1.25 0.019Induction chemotherapy 7.20 1.98-26.1 0.003
Microbiologically documented infection Enoxacin treatment 0.45 0.21-0.97 0.041
Gram-positive bacterial infection Enoxacin treatment 0.63 0.26-1.5 0.294Baseline AGC = 0-99 1.03 0.19-5.67 0.969Baseline AGC = 100-499 0.58 0.15-2.21 0.422Baseline AGC = 500-999 1.83 0.58-5.72 0.300
Gram-positive bacteremia Enoxacin treatment 0.81 0.29-2.22 0.681Center 1 f 0.748Center 3 0.99 0.17-5.84 0.988Center 9 1.22 0.02-6.55 0.815Center 10 1.43 0.31-6.53 0.647Center 11 0.35 0.05-2.34 0.276
Gram-negative bacterial infection Enoxacin treatment 0.07 0.01-0.30 <0.001
Gram-negative bacillary bacteremia Enoxacin treatment 0.05 0.01-0.37 0.004Age 0.19 0.05-0.66 0.009
C. difficile diarrhea Enoxacin treatment 1.16 0.30-4.56 0.829
Deep fungal infection Enoxacin treatment 2.57 0.47-13.9 0.273Days AGC < 500 1.05 1.00-1.10 0.061
Clinically documented infection Enoxacin treatment 0.54 0.22-1.34 0.184Days AGC < 500 1.10 1.04-1.16 0.001
Other antimicrobial therapy required Enoxacin treatment 0.60 0.20-1.79 0.358Induction chemotherapy 16.29 5.43-47.90 <0.001
Granulocyte recovery Enoxacin treatment 0.9 0.41-1.94 0.781Age 0.42 0.16-1.07 0.069Center 1 4.97 0.94-26.40 0.060Center 3 5.60 1.09-28.90 0.040Center 9 1.21 0.22-6.63 0.826Center 10 3.67 0.83-16.14 0.086Center 11 5.35 1.20-23.79 0.028
a Final models. Independent variables entered initially were treatment group, age (<65 or >65 years), sex, race, study center, baseline AGC (0 to 99, 100 to499, 500 to 999, or >1,000/mm3), number of days with an AGC of <500/mm3, and chemotherapeutic stage (induction versus consolidation).
b All AGC values are given in numbers of cells per cubic millimeter. Baseline AGC, AGC prior to start of treatment (patients with AGCs of >1,000 are thereference group). Centers 2, 4, and 7 are the reference group for the other centers.
c CI, 95% confidence interval for the odds ratio.d One or more febrile episodes requiring antibacterial therapy.e Compared with placebo treatment.f Not calculated because of a zero cell.
cinoxacin showed high levels of inactivation. Rosoxacin,norfloxacin, and pefloxacin showed moderate inactivation.Enoxacin, amifloxacin, ciprofloxacin, and ofloxacin showedrelatively little inactivation.A variety of clinical studies have shown that the quino-
lones can prevent bacterial infection in patients with leuke-mia. Trials have compared norfloxacin with placebo (21, 41),with TMP-SMX (3), and with vancomycin plus polymixin(41, 42); ciprofloxacin with TMP-SMX plus colistin (7);ofloxacin with TMP-SMX (23) and with vancomycin pluspolymixin (40); and ciprofloxacin with norfloxacin (15). Moststudies included patients with a variety of underlying hema-tologic and oncological conditions (15, 23, 40-42). In eachinstance, quinolone treatment (or, in reference 15, ciproflox-acin treatment) was associated with significantly fewer gram-negative infections (3, 7, 15, 21, 23, 40-42), especially
bacteremia (15, 23, 40, 41). Overall infections were reduced(15, 40), since there was generally no increase in fungal orgram-positive bacterial infection (7, 21, 23, 40-42). Therewas a significant increase in gram-positive bacteremias inone norfloxacin trial (3). Patients receiving the quinolone hadfewer acquired gram-negative bacillary and/or resistant or-ganisms (3, 7, 21, 23, 40-42), and their compliance was oftenbetter (7, 40-42). In some instances, there was a salutaryeffect on fever outcomes and on requirements for antibacte-rial therapy (15, 21, 40). A single trial provided evidence ofquinolone-associated myelosuppression (20 versus 12 daysat an AGC of <100/mm3 [P = 0.003]) plus a more frequentadministration of amphotericin B (63 versus 28% [P = 0.01])(40). Just one trial, the large multicenter trial performed bythe Gruppo Italiano Malattie Maligne dell' Adulto, employedmultivariate analysis to examine the relationship between
VOL. 37, 1993
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from
ANTIMICROB. AGENTS CHEMOTHER.
1090 .9 -
0.8-
0.7
0.6-....
0.5 -
0.4-
° 0.3-
0.2-
0.1-
0
0 5 10 15 20 25 30 35 40 45 50 55 60Study Days
-- Placebo - Enoxacin
FIG. 1. Median time to the onset of microbiologically docu-mented infection. Kaplan-Meier survival curves for enoxacin (solidline) and placebo (broken line) groups are shown.
treatment, as well as other independent variables, and pa-tient outcome (15). In that study, prophylactic treatmentwith norfloxacin (versus ciprofloxacin), neutropenia (AGC <
1,000/mm3) for >15 days, severe neutropenia (AGC <
100/mm3) for >7 days, and bone marrow transplantationeach increased the risk of febrile episodes (15).We believe that we have completed a particularly strong
study. In designing our study, we incorporated all thefeatures which Young has suggested as desirable character-istics of prophylactic antimicrobial studies (43). In addition,we performed logistic regression to complement our univari-ate analysis of the effect of treatment on the outcomesstudied.Our logistic models also elucidated certain other clinically
relevant phenomena. Not surprisingly, younger age (<65years) was associated with a decreased occurrence of gram-negative bacillary bacteremia (odds ratio, 0.19; 95% confi-dence interval, 0.05 to 0.66). Prolonged granulocytopeniawas associated (odds ratios and 95% confidence intervals are
given in parentheses) with slight increases in the occurrences
of deep fungal infection (1.05; 1.00 to 1.10), infectious fever(1.13; 1.02 to 1.25), and clinically documented infection(1.10; 1.04 to 1.16). These findings are not unexpected, giventhe known association of granulocytopenia with bacterialand fungal infections (2). Induction chemotherapy, com-
I1-
20.8 -
. 0.7
- 0.6-
e 0.5
0.4-
o 0.3 -
0.2-
IL0.1
0
0 5 10 15 20 25 30 36 40 45 50 55 60Study Days
----- Placebo -Enoxacin
FIG. 2. Median time to the onset of fever >102.80F (39.30C).Kaplan-Meier survival curves for enoxacin (solid line) and placebo(broken line) groups are shown.
TABLE 6. Adverse event profile
Value (%) for groupCharacteristic pa
Enoxacin Placebo
All adverse eventsNo. of patients 45 (73) 36 (63) 0.327Total events 231 184
Associated adverse eventsbNumber of patients 13 (21) 6 (11) 0.139Total associated events 18 6Rash 7 2Nausea and/or vomiting 4 1Diarrhea 2 0Elevated alkaline phosphatase 2 0Fever 0 1Headache 0 1Abdominal pain 1 0Elevated liver function tests 1 0Albuminuria 0 1Vaginal candidiasis 1 0
Clinically important adverseevents
Number of patients 9 (15) 8 (14) 1.000Total events 12 24Total associated events 3 1
a Fisher's exact test.b Associated adverse events are those considered by the investigator to be
possibly, probably, or definitely related to the study drug.
pared with consolidation chemotherapy, was associated withan increased likelihood of infectious fever and of its corol-lary, the requirement for antimicrobial therapy other thanthe study drugs. These effects were independent of granulo-cytopenia; it can be hypothesized that they could have beendue to differing intensities of the chemotherapy regimensadministered. Finally, granulocyte recovery was more likelyto occur in patients at some study centers than in patients atothers. This, too, could have been related to differences inthe intensity of chemotherapy among some study sites.
In conclusion, this and other studies show that quinolones
TABLE 7. Most frequently reported adverse eventsaNo. (%) of patients
Adverse event Enoxacin Placebo(n = 62) (n = 57)
Rash 28 (45) 19 (33)Hypokalemia 10 (16) 6 (11)Elevated creatinine 9 (15) 8 (14)Elevated lactate dehydrogenase 9 (15) 6 (11)Diarrhea 8 (13) 7 (12)Nausea and/or vomiting 7 (11) 4 (7)Elevated alkaline phosphatase 6 (10) 3 (5)Hyperglycemia 5 (8) 3 (5)Decreased serum bicarbonate 5 (8) 1 (2)Hypocalcemia 4 (6) 3 (5)Pruritus 4 (6) 2 (4)Elevated bilirubin 3 (5) 6 (11)Elevated blood urea nitrogen 3 (5) 4 (7)Cellulitis 3 (5) 3 (5)Elevated alanine aminotransferase 3 (5) 3 (5)
a Reported in .10% of patients in either or both treatment groups com-bined. There were no significant differences between the groups by Fisher'sexact test.
480 TALBOT ET AL.
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ENOXACIN IN ACUTE LEUKEMIA 481
can successfully prevent gram-negative infection in patientswith acute nonlymphocytic leukemia. The potential for anincreased risk of gram-positive bacterial infection is a con-cern but, at least in the current study, could not be demon-strated. The incidence of confirmed deep fungal infectiondoes not appear to be increased; however, it must be notedthat more quinolone patients required amphotericin B in ourtrial (P = 0.105) and that of Winston and colleagues (40),suggesting that suspected deep fungal infection may be morefrequent. This issue needs further study. Our trial and that ofthe Gruppo Italiano Malattie Maligne dell' Adulto (15) indi-cate that quinolone prophylaxis may reduce the occurrenceof fever; the latter also suggests a decreased need forantibacterial therapy. The quinolones are safe comparedwith either placebo or other antibacterial regimens. In par-ticular, the possibility of a myelosuppressive effect, noted byWinston et al. (40), was not found in other trials or by ourown logistic regression analysis. Remaining issues to beconsidered include the possibility of emergence of bacterialresistance, which was not evident in our study, and thecost-effectiveness of quinolone prophylaxis, which appearslikely but cannot necessarily be inferred from available data.
ACKNOWLEDGMENTSThis work was supported by a grant from Parke-Davis Pharma-
ceutical Research, Inc. G. H. Talbot and P. A. Cassileth served asconsultants to Parke-Davis during the planning and conduct of thisstudy.We thank the many physicians, nurses, and laboratory staff
members who contributed to the successful completion of this work.
REFERENCES1. Bennett, J. M., D. Catovsky, M. T. Daniel, G. Flandrin, D. A.
Galton, H. R. Gralnick, and C. Sultan. 1985. Proposed revisedcriteria for the classification of acute myeloid leukemia. Ann.Intern. Med. 103:620-624.
2. Bodey, G. P., M. Buckley, Y. S. Sathe, et al. 1966. Quantitativerelationships between circulating leukocytes and infection inpatients with acute leukemia. Ann. Intern. Med. 64:328-340.
3. Bow, E. J., E. Rayner, and T. J. Louie. 1988. Comparison ofnorfloxacin with cotrimoxazole for infection prophylaxis inacute leukemia. The trade-off for reduced Gram-negative sepsis.Am. J. Med. 84:847-854.
4. Bow, E. J., E. Rayner, B. A. Scott, and T. J. Louie. 1987.Selective gut decontamination with nalidixic acid or tri-methoprim-sulfamethoxazole for infection prophylaxis in neu-tropenic cancer patients: relationship of efficacy to antimicro-bial spectrum and timing of administration. Antimicrob. AgentsChemother. 31:551-557.
5. Claesner, H. A. L., E. J. Vollaard, and H. K. F. van Saene. 1987.Long-term prophylaxis of infection by selective decontamina-tion in leukopenia and in mechanical ventilation. Rev. Infect.Dis. 9:295-328.
6. Cohen, J. 1977. Statistical power analysis for the behavioralsciences, revised ed., p. 179-185. Academic Press, New York.
7. Dekker, A. W., M. Rosenberg-Arska, and J. Verhoef. 1987.Infection prophylaxis in acute leukemia: a comparison of cipro-floxacin with trimethoprim-sulfamethoxazole and colistin. Ann.Intern. Med. 106:7-12.
8. de Vries-Hospers, H. G., D. T. Sleofer, N. H. Mulder, D. van derWaaU, H. 0. Nieweg, and H. K. F. van Saene. 1981. Bacterio-logical aspects of selective decontamination of the digestivetract as a method of infection prevention in granulocytopenicpatients. Antimicrob. Agents Chemother. 19:813-820.
9. Edlund, C., A. Lidbeck, L. Kager, and C. E. Nord. 1987.Comparative effects of enoxacin and norfloxacin on humancolonic microflora. Antimicrob. Agents Chemother. 31:1846-1848.
10. Elliott, C. R., and J. L. Pater. 1988. The effect of differentmeasures of outcome on the results of studies of empiric
antibiotic therapy in febrile neutropenic patients. Clin. Invest.Med. 11:327-330.
11. Frimodt-Moller, P. C., K. M.-E. Jensen, and P. 0. Madsen.1983. Antibacterial activity of norfloxacin in the gastrointestinaltracts of rats. Antimicrob. Agents Chemother. 24:560-563.
12. Giuliano, M., A. Pantosti, G. Gentile, M. Venditti, W. Arcese,and P. Martino. 1989. Effects on oral and intestinal microflorasof norfloxacin and pefloxacin for selective decontamination inbone marrow transplant patients. Antimicrob. Agents Chemo-ther. 33:1709-1713.
13. Goldstein, E., and D. Citron. 1985. Comparative activity of thequinolones against anaerobic bacteria isolated at communityhospitals. Antimicrob. Agents Chemother. 27:57-59.
14. Goldstein, E. J. C., D. M. Citron, and M. L. Corrado. 1987.Effect of inoculum size on in vitro activity of norfloxacin againstfecal anaerobic bacteria: rationale for selective decontaminationof the digestive tract. Am. J. Med. 82(Suppl. 6B):79-83.
15. Gruppo Italiano Malattie Maligne dell' Adulto Infection Pro-gram. 1991. Prevention of bacterial infection in neutropenicpatients with hematologic malignancies. A randomized, multi-center trial comparing norfloxacin with ciprofloxacin. Ann.Intern. Med. 115:7-12.
16. Guiot, H. F. L., P. J. van den Broek, J. W. M. van der Meer, andR. van Furth. 1983. Selective antimicrobial modulation of theintestinal flora of patients with acute nonlymphocytic leukemia:a double-blind, placebo-controlled study. J. Infect. Dis. 147:615-623.
17. Guiot, H. F. L., J. W. M. van der Meer, and R. van Furth. 1981.Selective antimicrobial modulation of human microbial flora:infection prevention in patients with decreased host defensemechanisms by selective elimination of potentially pathogenicbacteria. J. Infect. Dis. 143:644 654.
18. Henry, D., A. G. Skidmor, J. Ngui-Yen, A. Smith, and J. A.Smith. 1985. In vitro activities of enoxacin, ticarcillin plusclavulanic acid, aztreonam, piperacillin, and imipenem andcomparison with commonly used antimicrobial agents. Antimi-crob. Agents Chemother. 28:259-264.
19. Henry, S. A. 1984. Chemoprophylaxis of bacterial infections ingranulocytopenic patients. Am. J. Med. 76:645-651.
20. Hooper, D. C., and J. S. Wolfson. 1985. The fluoroquinolones:pharmacology, clinical uses, and toxicities in humans. Antimi-crob. Agents Chemother. 28:716-721.
21. Karp, J. E., W. G. Merz, C. Hendricksen, B. Laughon, T.Redden, B. J. Bamberger, J. G. Bartlett, R. Saral, and P. J.Burke. 1987. Oral norfloxacin for prevention of gram-negativebacterial infections in patients with acute leukemia and granu-locytopenia. Ann. Intern. Med. 106:1-7.
22. Koup, J. R., R. D. Toothaker, E. Posvar, A. J. Sedman, andW. A. Colburn. 1990. Theophylline dosage adjustment duringenoxacin coadministration. Antimicrob. Agents Chemother. 34:803-807.
23. Liang, R. H. S., R. W. H. Yung, T.-K. Chan, P.-Y. Chau, W.-K.Lam, S.-Y. So, and D. Todd. 1990. Ofloxacin versus co-trimox-azole for prevention of infection in neutropenic patients follow-ing cytotoxic chemotherapy. Antimicrob. Agents Chemother.34:215-218.
24. National Committee for Clinical Laboratory Standards. 1984.Performance standards for antimicrobial disk susceptibilitytests, 3rd ed. Approved standard M2-A3. National Committeefor Clinical Laboratory Standards, Villanova, Pa.
25. National Committee for Clinical Laboratory Standards. 1985.Methods for dilution antimicrobial susceptibility tests for bac-teria that grow aerobically. Approved standards M7-A. NationalCommittee for Clinical Laboratory Standards, Villanova, Pa.
26. O'Brien, P. C., and T. R. Fleming. 1979. A multiple testingprocedure for clinical trials. Biometrics 35:549-556.
27. Pecquet, S., A. Andremont, and C. Tancrede. 1986. Selectiveantimicrobial modulation of the intestinal tract by norfloxacin inhuman volunteers and in gnotobiotic mice associated with ahuman fecal flora. Antimicrob. Agents Chemother. 29:1047-1052.
28. Pecquet, S., A. Andremont, and C. Tancrede. 1987. Effect of oralofloxacin on fecal bacteria in human volunteers. Antimicrob.
VOL. 37, 1993
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
Agents Chemother. 31:124-125.29. Riou, B., C. Richard, A. Rimailho, and P. Auzepy. 1985.
Potential risks of trimethoprim-sulfamethoxazole prophylaxis inneutropenic patients. J. Infect. Dis. 151:969. (Letter.)
30. Rosenberg-Arska, M., A. W. Dekker, and J. Verhoef. 1985.Ciprofloxacin for selective decontamination of the alimentarytract in patients with acute leukemia during remission inductiontreatment: the effect on fecal flora. J. Infect. Dis. 152:104-107.
31. Rudrik, J. T., S. J. Cavalieri, and E. M. Britt. 1984. In vitroactivities of enoxacin and 17 other antimicrobial agents againstmultiply resistant, gram-negative bacteria. Antimicrob. AgentsChemother. 26:97-100.
32. SAS Institute, Inc. 1985. SAS user's guide: statistics, version 5ed. SAS Institute Inc., Carey, N.C.
33. SAS Institute, Inc. 1986. SUGI supplemental library user'sguide: statistics, version 5 ed. SAS Institute Inc., Carey, N.C.
34. Sleijfer, D. T., H. H. Mulder, H. G. de Vries-Hospers, et al. 1980.Infection prevention in granulocytopenic patients by selectivedecontamination of the digestive tract. Eur. J. Cancer 16:859-869.
34a.Talbot, G. H., P. A. Cassileth, L. Paradiso, R. Correa-Coronas,and The Enoxacin Prophylaxis Study Group. 1991. ProgramAbstr. 31st Intersci. Conf. Antimicrob. Agents Chemother.,abstr. 1162.
35. Tancrede, C. H., and A. 0. Andremont. 1985. Bacterial trans-location and gram-negative bacteremia in patients with hemato-logical malignancies. J. Infect. Dis. 152:99-103.
36. van Saene, J. J. M., H. K. F. van Saene, and C. F. Lerk. 1986.Inactivation of quinolones by feces. J. Infect. Dis. 153:999-1000. (Letter.)
37. Wade, J. C., C. A. de Jongh, K. A. Newman, J. Crowley, P. H.Wiernik, and S. C. Schimpif. 1983. Selective antimicrobialmodulation as prophylaxis against infection during granulocyto-penia: trimethoprim-sulfamethoxazole vs. nalidixic acid. J. In-fect. Dis. 147:624-634.
38. Wade, J. C., and S. C. Schimpff. 1988. Epidemiology andprevention of infection in the compromised host, p. 5-40. InR. H. Rubin and L. S. Young (ed.), Clinical approach toinfection in the compromised host, 2nd ed. Plenum MedicalBook Company, New York.
39. Wells, C., M. A. Maddaus, and R. L. Simmons. 1988. Proposedmechanisms for the translocation of intestinal bacteria. Rev.Infect. Dis. 10:958-978.
40. Winston, D. J., W. G. Ho, D. A. Bruckner, R. P. Gale, and R. E.Champlin. 1990. Ofloxacin versus vancomycin/polymyxin forprevention of infections in granulocytopenic patients. Am. J.Med. 88:36-42.
41. Winston, D. J., W. G. Ho, R. E. Champlin, J. M. Joshi, J. C.Wade, J. Karp, J. Bartlett, G. Talbot, L. Levitt, S. Drezinski,and M. Corrado. 1987. Norfloxacin for prevention of bacterialinfections in granulocytopenic patients. Am. J. Med. 82(Suppl.6B):40-46.
42. Winston, D. J., W. G. Ho, S. L. Nakao, R. P. Gale, and R. E.Champlin. 1986. Norfloxacin versus vancomycin/polymixin forprevention of infections in granulocytopenic patients. Am. J.Med. 80:884-890.
43. Young, L. S. 1983. Antimicrobial prophylaxis against infectionin neutropenic patients. J. Infect. Dis. 147:611-614.
44. Young, L. S. 1987. The new fluorinated quinolones for infectionprevention in acute leukemia. Ann. Intern. Med. 106:144-146.
482 TALBOT ET AL.
on Decem
ber 4, 2013 by guesthttp://aac.asm
.org/D
ownloaded from