
Carotid artery visualization during anterior skull base surgery: a novel protocol for...
8
Carotid artery visualization during anterior skull base surgery: a novel protocol for neuronavigation Brent M. McGrath • William J. Maloney • Stefan Wolfsberger • Ron Hill • Emad Massoud • Syed Ali Imran • David B. Clarke Published online: 12 February 2010 Ó Springer Science+Business Media, LLC 2010 Abstract Detailed knowledge of the vascular anatomy of the anterior skull base is critical to successful surgery in this area. Whereas conventional neuronavigational approaches combine MRI (± contrast) for tumor visuali- zation and CT (± C) for bony and vascular anatomy, we describe the Canadian and Austrian experiences using a novel protocol integrating MR angiography (MRA) into surgical neuronavigation to provide superior visualization of the carotid arteries. The pre-operative imaging protocol employs a T1-weighted, 3D fast spoiled gradient echo MRI (± C) for soft tissue anatomy, a plain CT for bony anat- omy, and a 3D time-of-flight MR angiography for carotid anatomy. The series are imported into the Medtronic StealthStation Ò TREON Ò Treatment Guidance System; during intra-operative neuronavigation, each series (MRI, CT, MRA) can be viewed individually, or layered and viewed as a composite image. Our protocol has important advantages. First, it provides detailed tissue, tumor, vas- cular and bony anatomy. Second, a contrast CT is not necessary; this is important, as numerous reports have highlighted the nephrotoxic nature of radiographic contrast material. Third, visualization of the carotid system is superior than can be obtained from CT angiography. We use this unique imaging protocol routinely for our endo- scopic transsphenoidal surgeries to provide superior visu- alization of the carotid arteries during anterior skull base surgery. Keywords Neuronavigation Á Transsphenoidal surgery Á Carotid artery Á Skull base Á Magnetic resonance angiography Background Guiot and Thibaut [1] repopularized transsphenoidal sur- gery, a procedure whose widespread acceptance as a modern neurosurgical approach was made possible by Hardy’s refinements, including the introduction of micro- surgical techniques and neuroimaging [2–4]. Transsphe- noidal approaches to the skull base are now considered safe, with acceptably low mortality rates [5–7]. Despite low mortality rates, however, the morbidity associated with transsphenoidal surgery remains significant; in a recent B. M. McGrath Á R. Hill Á E. Massoud Á D. B. Clarke (&) Department of Surgery (Neurosurgery), Dalhousie University, 1796 Summer Street, Halifax, NS B3H 3A7, Canada e-mail: [email protected] W. J. Maloney Department of Radiology and Diagnostic Imaging (Neuroradiology), Dalhousie University, 1796 Summer Street, Halifax, NS B3H 3A7, Canada S. Wolfsberger Department of Neurosurgery, Medical University of Vienna, Vienna, Austria E. Massoud Á D. B. Clarke Department of Surgery (Otolaryngology), Dalhousie University, 5820 University Avenue, Halifax, NS B3H 2Y9, Canada S. A. Imran Á D. B. Clarke Department of Medicine (Endocrinology), Dalhousie University, 1276 South Park Street, Halifax, NS B3H 2Y9, Canada E. Massoud Á S. A. Imran Á D. B. Clarke Halifax Neuropituitary Program, Dalhousie University, 1796 Summer Street, Halifax, NS B3H 3A7, Canada D. B. Clarke Department of Anatomy & Neurobiology, Dalhousie University, 1796 Summer Street, Halifax, NS B3H 3A7, Canada 123 Pituitary (2010) 13:215–222 DOI 10.1007/s11102-010-0220-0
Transcript of Carotid artery visualization during anterior skull base surgery: a novel protocol for...
Carotid artery visualization during anterior skull base surgery:a novel protocol for neuronavigation
Brent M. McGrath • William J. Maloney •
Stefan Wolfsberger • Ron Hill • Emad Massoud •
Syed Ali Imran • David B. Clarke
Published online: 12 February 2010
� Springer Science+Business Media, LLC 2010
Abstract Detailed knowledge of the vascular anatomy
of the anterior skull base is critical to successful surgery
in this area. Whereas conventional neuronavigational
approaches combine MRI (± contrast) for tumor visuali-
zation and CT (± C) for bony and vascular anatomy, we
describe the Canadian and Austrian experiences using a
novel protocol integrating MR angiography (MRA) into
surgical neuronavigation to provide superior visualization
of the carotid arteries. The pre-operative imaging protocol
employs a T1-weighted, 3D fast spoiled gradient echo MRI
(± C) for soft tissue anatomy, a plain CT for bony anat-
omy, and a 3D time-of-flight MR angiography for carotid
anatomy. The series are imported into the Medtronic
StealthStation� TREON� Treatment Guidance System;
during intra-operative neuronavigation, each series (MRI,
CT, MRA) can be viewed individually, or layered and
viewed as a composite image. Our protocol has important
advantages. First, it provides detailed tissue, tumor, vas-
cular and bony anatomy. Second, a contrast CT is not
necessary; this is important, as numerous reports have
highlighted the nephrotoxic nature of radiographic contrast
material. Third, visualization of the carotid system is
superior than can be obtained from CT angiography. We
use this unique imaging protocol routinely for our endo-
scopic transsphenoidal surgeries to provide superior visu-
alization of the carotid arteries during anterior skull base
surgery.
Keywords Neuronavigation � Transsphenoidal surgery �Carotid artery � Skull base �Magnetic resonance angiography
Background
Guiot and Thibaut [1] repopularized transsphenoidal sur-
gery, a procedure whose widespread acceptance as a
modern neurosurgical approach was made possible by
Hardy’s refinements, including the introduction of micro-
surgical techniques and neuroimaging [2–4]. Transsphe-
noidal approaches to the skull base are now considered
safe, with acceptably low mortality rates [5–7]. Despite
low mortality rates, however, the morbidity associated with
transsphenoidal surgery remains significant; in a recent
B. M. McGrath � R. Hill � E. Massoud � D. B. Clarke (&)
Department of Surgery (Neurosurgery), Dalhousie University,
1796 Summer Street, Halifax, NS B3H 3A7, Canada
e-mail: [email protected]
W. J. Maloney
Department of Radiology and Diagnostic Imaging
(Neuroradiology), Dalhousie University, 1796 Summer Street,
Halifax, NS B3H 3A7, Canada
S. Wolfsberger
Department of Neurosurgery, Medical University of Vienna,
Vienna, Austria
E. Massoud � D. B. Clarke
Department of Surgery (Otolaryngology), Dalhousie University,
5820 University Avenue, Halifax, NS B3H 2Y9, Canada
S. A. Imran � D. B. Clarke
Department of Medicine (Endocrinology), Dalhousie University,
1276 South Park Street, Halifax, NS B3H 2Y9, Canada
E. Massoud � S. A. Imran � D. B. Clarke
Halifax Neuropituitary Program, Dalhousie University,
1796 Summer Street, Halifax, NS B3H 3A7, Canada
D. B. Clarke
Department of Anatomy & Neurobiology, Dalhousie University,
1796 Summer Street, Halifax, NS B3H 3A7, Canada
123
Pituitary (2010) 13:215–222
DOI 10.1007/s11102-010-0220-0
large review of more than five thousand cases, 26.8%
morbidity was reported which included neurovascular
complications in 6.9% of patients [6]. The importance of
avoiding carotid or basilar artery injury has been empha-
sized by several authors, and understanding the vascular
relationships in this era of endoscopic approaches is critical
[8–11].
The present technical note reports on Canadian and
Austrian experiences using a novel imaging protocol that
provides excellent bony and high-quality carotid artery
visualization during anterior skull base surgery. This sur-
gical neuronavigation protocol uses a single contrast study,
integrating non-enhanced CT, contrast MRI and MR
angiography (MRA).
Imaging technique
MR data were acquired with a 1.5 Tesla (T) scanner (GE
HDx Signa). MRI images were obtained using sagittal T1,
coronal T1 and T2 as well as post-gadolinium coronal T1
weighted 3D fast spoiled gradient echo (FSGE) sequences
(TR = 11.21 ms, TE = 4.2 ms, slice thickness = 1.5 mm,
resolution = 256 9 256). During the same scanning
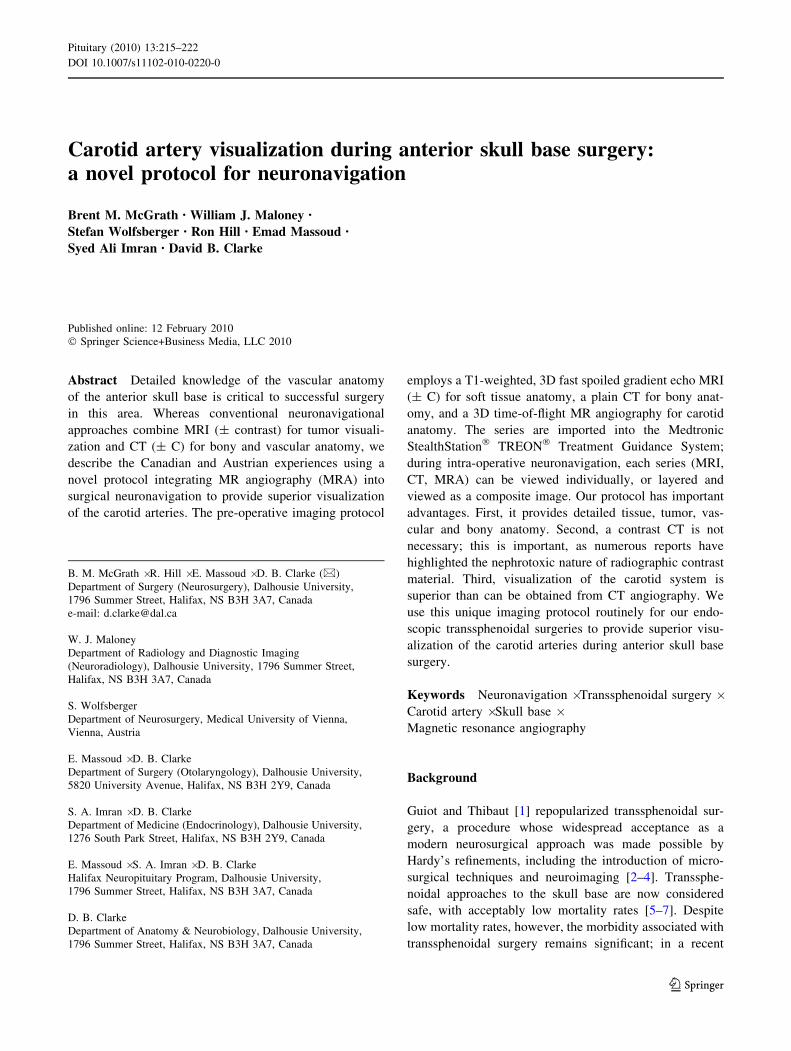
Fig. 1 Pre-operative studies,
Patient 1. a Coronal T1 MRI
with enhancement showing
sellar mass. b Anterior-posterior
MRA showing cerebral arterial
vasculature, including carotid-
basilar arteries. c Axial CT
(plain)
216 Pituitary (2010) 13:215–222
123
session, MRA images were obtained using a 3D vascular
time-of-flight (TOF) SPGR sequence (TR = 24 ms,
TE = 2.3 ms, slice thickness = 1.4 mm, resolution =
256 9 256). Non-enhanced CT data were acquired on a
Siemens Somatom Sensation 64 scanner in contiguous
1 mm thick axial slices. The same skin fiducial markers
were used for both CT and MRI/MRA scanning and served
to verify fusion of the three imaging data series.
Imaging data from all three paradigms were then
integrated and stored in the Medtronic StealthStation�
TREON� Treatment Guidance System for use during
surgery. Intra-operative multiplanar neuronavigation enables
each data series (i.e. MRI, MRA and/or CT) to be viewed
individually, or layered and viewed as a composite of any
combination of the three image series. MRI and CT
images are windowed to be viewed in the standard
radiological fashion, whereas MRA images are viewed in
heat scale so as to highlight the carotid-basilar arterial
system, and to differentiate it from surrounding soft tissue
and bone.
Illustrative cases
The following three cases include examples of the
acquired images and show intra-operative neuronavigation
images obtained by using our MRI/MRA/CT imaging
technique.
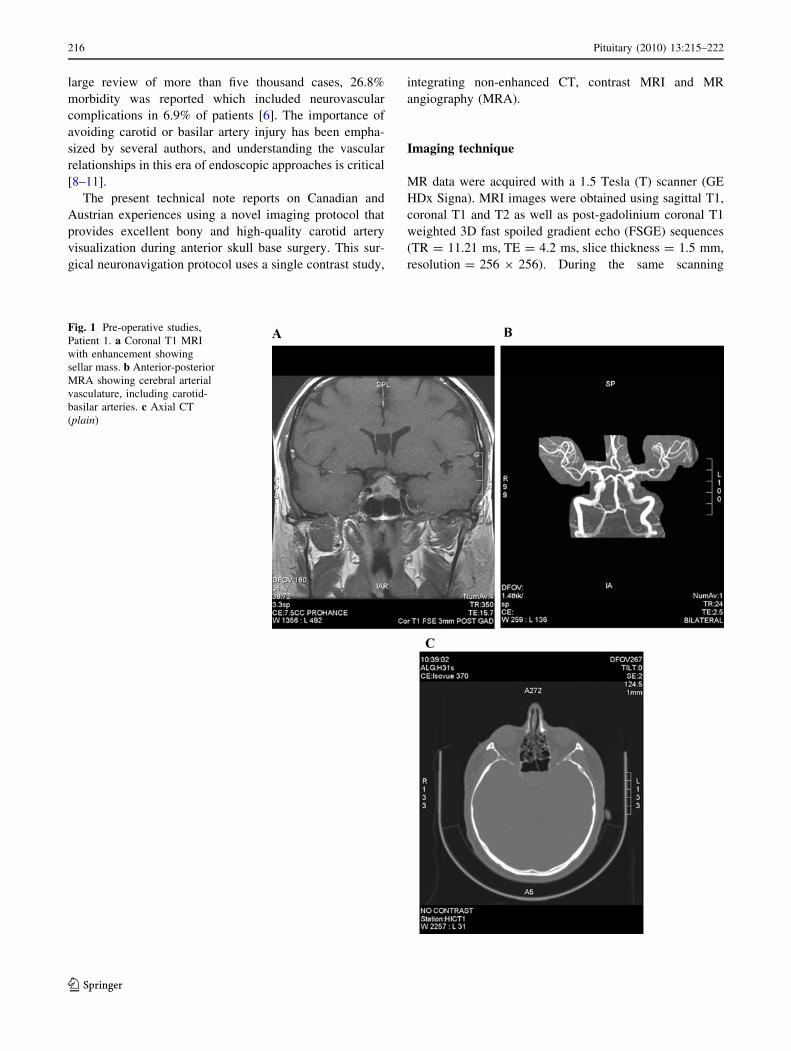
Fig. 2 Intra-operative neuronavigation, Patient 1. MRA/MRI fused
images showing carotid arteries (color) in relation to sellar mass (grayscale) in coronal (a) and sagittal (b) planes. MRA/CT fused images
showing carotid arteries (color) in relation to bony sellar anatomy
(gray scale) in similar coronal (c) and sagittal (d) planes. Crosshairsindicate the inferior border of the left cavernous sinus. (Color figure
online)
Pituitary (2010) 13:215–222 217
123

Patient 1
A 52-year-old man presented with a 3-month history of
headaches and decreased vision in his left eye, revealed by
Goldmann visual field-testing to be a left incomplete
temporal hemianopsia. Endocrine evaluation revealed
secondary hypothyroidism and hypogonadism. Pre-opera-
tive imaging by coronal MRI revealed a sellar mass
(2.5 cm 9 2.1 cm in maximal cross-sectional diameters)
extending superiorly and compressing the left aspect of the
optic chiasm. Clinical evaluation, neuroimaging and hor-
mone studies were consistent with the final diagnosis of a
non-functioning pituitary macroadenoma. See Figs. 1 and 2
for pre- and intra-operative images, respectively.
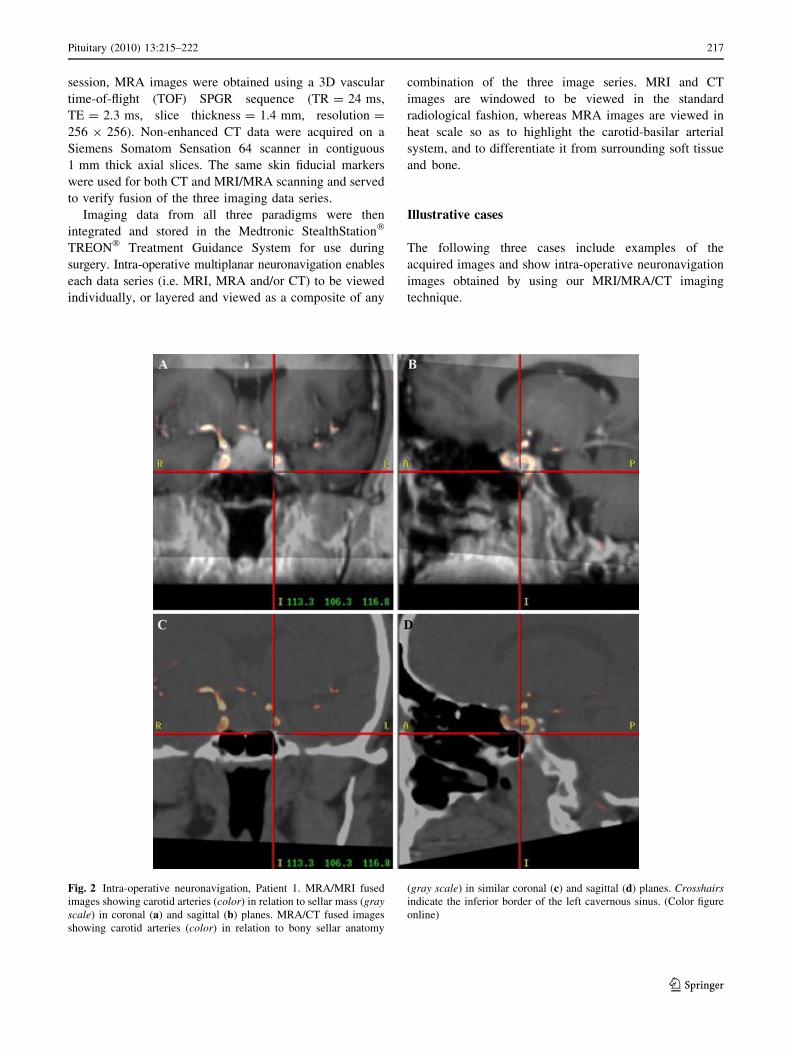
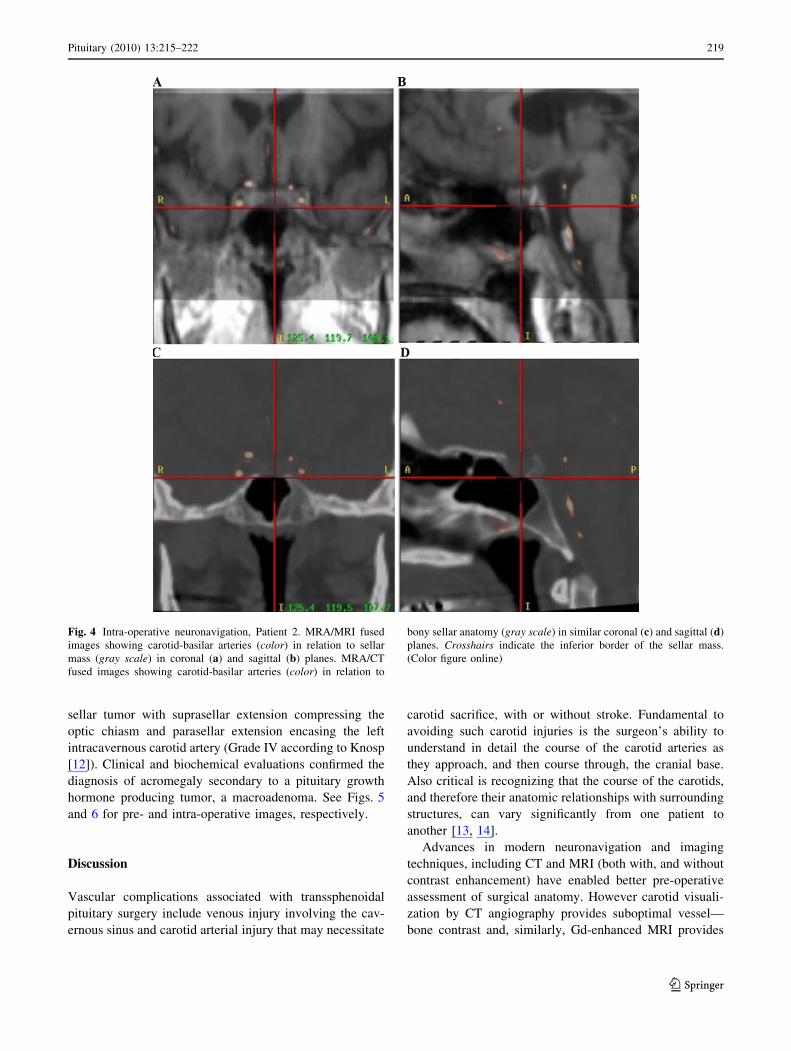
Patient 2
A 32-year-old woman presented with clinical features of
Cushing’s syndrome. Pre-operative coronal MRI revealed a
small, non-enhancing microadenoma and, incidentally, a
hypoplastic left vertebral artery. Clinical evaluation, neu-
roimaging and hormone studies were consistent with the
final diagnosis of Cushing’s disease. See Figs. 3 and 4 for
pre- and intra-operative images, respectively.
Patient 3
A 31-year-old women admitted to hospital due to rapid
visual deterioration. Pre-operative MRI revealed a large
Fig. 3 Pre-operative studies,
Patient 2. a Pre-operative
coronal T1 MRI with
enhancement showing sellar
mass. b Pre-operative anterior-
posterior MRA showing
cerebral arterial vasculature.
c Pre-operative axial CT (plain)
218 Pituitary (2010) 13:215–222
123
sellar tumor with suprasellar extension compressing the
optic chiasm and parasellar extension encasing the left
intracavernous carotid artery (Grade IV according to Knosp
[12]). Clinical and biochemical evaluations confirmed the
diagnosis of acromegaly secondary to a pituitary growth
hormone producing tumor, a macroadenoma. See Figs. 5
and 6 for pre- and intra-operative images, respectively.
Discussion
Vascular complications associated with transsphenoidal
pituitary surgery include venous injury involving the cav-
ernous sinus and carotid arterial injury that may necessitate
carotid sacrifice, with or without stroke. Fundamental to
avoiding such carotid injuries is the surgeon’s ability to
understand in detail the course of the carotid arteries as
they approach, and then course through, the cranial base.
Also critical is recognizing that the course of the carotids,
and therefore their anatomic relationships with surrounding
structures, can vary significantly from one patient to
another [13, 14].
Advances in modern neuronavigation and imaging
techniques, including CT and MRI (both with, and without
contrast enhancement) have enabled better pre-operative
assessment of surgical anatomy. However carotid visuali-
zation by CT angiography provides suboptimal vessel—
bone contrast and, similarly, Gd-enhanced MRI provides
Fig. 4 Intra-operative neuronavigation, Patient 2. MRA/MRI fused
images showing carotid-basilar arteries (color) in relation to sellar
mass (gray scale) in coronal (a) and sagittal (b) planes. MRA/CT
fused images showing carotid-basilar arteries (color) in relation to
bony sellar anatomy (gray scale) in similar coronal (c) and sagittal (d)
planes. Crosshairs indicate the inferior border of the sellar mass.
(Color figure online)
Pituitary (2010) 13:215–222 219
123

poor carotid artery—cavernous sinus distinction. Further-
more, the use of contrast agents in both scans carries
additional cost and potential risk. The use of iodinated
agents and gadolinium have been reported in numerous
studies to cause subsequent renal dysfunction [15, 16], and
to be the third most common cause of renal failure among
hospitalized patients [15, 17]. While there is some recent
evidence [18] to suggest that the nephrotoxic effects of
contrast agents may not be as pervasive as once thought,
employing an imaging method that provides excellent
visualization of the neuro-vasculature while minimizing
the patient’s exposure to potentially toxic substances is a
worthy endeavor.
Utilization of this protocol has several important
advantages. First, it provides the detailed tissue, tumor,
vascular and bony anatomy that is a prerequisite for an
optimal neuronavigational tool. Second, a contrast CT or
catheter-based angiographic approach is not necessary; this
is an important advantage in light of the risks outlined
above. Moreover, catheter angiography carries the added
risk of inducing severe neurologic injury [19]. MRA, like
all MR imaging modalities, has no known adverse effects
and is done as part of the routine pre-operative MR scan.
Third, visualization of the carotid system is superior than
can be obtained from CT angiography; the surgeon is
provided with high quality vascular images having high
spatial resolution. The only foreseeable drawback of uti-
lizing MRA in place of contrast CT is that it requires longer
scan times in the MR imager. At many institutions,
including our own, MR time is at a premium. That said, the
additional scan time is small (less than 6 min) and the
associated cost would likely be offset by reductions in CT
scanning time, the use of contrast agents, incidence of
contrast-induced nephropathies, and vascular injury at the
time of surgery.
In response to the suboptimal neuronavigational visu-
alization of the carotid arteries as they course through the
skull base, we have developed and have now used this
imaging protocol in almost 400 patients; it is now used for
all of our anterior skull base surgeries.
Fig. 5 Pre-operative studies, Patient 3. a Coronal T1 MRI with enhancement showing sellar mass with supra- and left para-sellar extension.
b Sagittal MRA showing cerebral arterial vasculature. Note the elongated left carotid siphon. c Axial CT (plain)
220 Pituitary (2010) 13:215–222
123

Acknowledgments The authors would like to thank Carla Roberts
for her assistance in the preparation of this manuscript.
References
1. Guiot G, Thibaut B (1959) L’extirpation des adenomas hypo-
physaires par voie trans-sphenoidale. Neurochirurgia (Stuttg)
1:133–150
2. Hardy J (1969) Transsphenoidal microsurgery of the normal and
pathological pituitary. Clin Neurosurg 16:185–217
3. Hardy J (1971) Transsphenoidal hypophysectomy. J Neurosurg
34:582–594
4. Hardy J, Wigser SM (1965) Transsphenoidal surgery of the
pituitary fossa tumors with televised radiofluoroscopic control.
J Neurosurg 23:612–619
5. Black PM, Zervas N, Candia GL (1987) Incidence and manage-
ment of complications of transsphenoidal operation for pituitary
adenomas. Neurosurgery 20:920–924
6. Barker FG, Klibanski A, Swearingen B (2003) Transsphenoidal
surgery for pituitary tumors in the United States, 1996–2000:
mortality, morbidity, and the effects of hospital and surgeon
volume. J Clin Endocrinol Metabol 88:4709–4719
7. Senior BA, Ebert CS, Bednarski KK, Bassim MK, Younes M,
Sigounas D, Ewend MG (2008) Minimally invasive pituitary
surgery. Laryngoscope 118:1842–1855
8. Couldwell WT, Weiss MH, Rabb C, Liu JK, Apfelbaum RI,
Fukushima T (2004) Variations on the standard transsphenoidal
approach to the sellar region, with emphasis on the extended
approaches and parasellar approaches: surgical experience in 105
cases. Neurosurgery 55:539–547
9. de Divitiis E, Cappabianca P, Cavallo LM (2002) Endoscopic
transsphenoidal approach: adaptability of the procedure to dif-
ferent sellar lesions. Neurosurgery 51:699–705
Fig. 6 Intra-operative neuronavigation, Patient 3. MRA/MRI/CT fused images showing carotid arteries (color) in relation to sellar mass and
bone (gray scale) in coronal (a), sagittal (b) and axial (c) planes. (Color figure online)
Pituitary (2010) 13:215–222 221
123

10. Cappabianca P, Briganti F, Cavallo LM, de Divitiis E (2001)
Pseudoaneurysm of the intracavernous carotid artery following
endoscopic endonasal transsphenoidal surgery, treated by endo-
vascular approach. Acta Neurochir (Wien) 143:95–96
11. Kassam A, Snyderman CH, Carrau RL, Gardner P, Mintz A
(2005) Endoneurosurgical hemostasis techniques: lessons learned
from 400 cases. Neurosurg Focus 19:E7
12. Knosp E, Steiner E, Kitz K, Matula C (1993) Pituitary adenomas
with invasion of the cavernous sinus space: a magnetic resonance
imaging classification compared with surgical findings. Neuro-
surgery 33:610–617
13. Bedford MA (1966) The ‘‘cavernous’’ sinus. Br J Ophthal 50:
41–46
14. Bull JWD, Schunk H (1962) The significance of displacement of
the cavernous portion of the internal carotid artery. Br J Radiol
35:801–814
15. Nash K, Hafeez A, Hou S (2002) Hospital-acquired renal insuf-
ficiency. Am J Kidney Dis 39:930–936
16. Gleeson TG, Bulugahapitiya S (2004) Contrast-induced
nephropathy. AJR 183:1673–1689
17. Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT
(1983) Hospital-acquired renal insufficiency: a prospective study.
Am J Med 74:243–248
18. Newhouse JH, Kho D, Rao QA, Starren J (2008) Frequency of
serum creatinine changes in the absence of iodinated contrast
material: implications for studies of contrast nephrotoxicity. AJR
Am J Roentgenol 191:376–382
19. Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G,
Montanera W (2003) Neurologic complications of cerebral
angiography: prospective analysis of 2,899 procedures and
review of the literature. Radiology 227:522–528
222 Pituitary (2010) 13:215–222
123




















