Primary angiosarcomas of the anterior mediastinum
7
Original contribution Primary angiosarcomas of the anterior mediastinum: A clinicopathologic and immunohistochemical study of 9 cases Annikka Weissferdt MD a, ⁎ , Neda Kalhor MD a , Saul Suster MD b , Cesar A. Moran MD a a Department of Pathology and Laboratory Medicine, MD Anderson Cancer Center, Houston, TX 77030, USA b Department of Pathology and Laboratory Services, Medical College of Wisconsin, Milwaukee, WI53226, USA Received 3 March 2010; revised 9 May 2010; accepted 12 May 2010 Keywords: Angiosarcoma; Anterior mediastinum; Thymus; Immunohistochemistry Summary We report 9 cases of primary angiosarcomas of the anterior mediastinum. Patient ages ranged from 25 to 62 years (mean, 40.7 years); 5 patients were male and 4 were female. Main presenting symptoms included chest pain, dyspnea, and cough. The tumor size ranged from 3 to 12.5 cm. Macroscopically, the lesions were ill-defined hemorrhagic masses. Histologically, the growth patterns ranged from large vascular spaces to capillary-like proliferations. These were either lined by bland or more pleomorphic endothelial cells. The mitotic activity was variable and corresponded to the degree of differentiation. A rim of thymic tissue was observed in 2 cases suggesting a thymic origin of the tumors. No teratomatous components were identified. Immunohistochemical studies showed that all 9 cases were reactive for vascular markers including factor VIII–related antigen, CD31, and CD34, and negative for cytokeratin CAM5.2. All cases were treated by complete resection and 3 patients received adjuvant chemotherapy. Follow-up information available for 6 patients revealed that 4 were alive and free of disease at intervals ranging from 6 to 36 months after diagnosis and 1 was alive with recurrence at 48 months. One patient had died of the disease 10 months after diagnosis. Primary angiosarcomas of the anterior mediastinum are rare tumors that need to be added to the differential diagnosis of primary anterior mediastinal neoplasms. Despite their histologic similarity to angiosarcomas at other sites, primary angiosarcomas of the anterior mediastinum appear to follow a more protracted clinical course than their counterparts in other organ systems. © 2010 Elsevier Inc. All rights reserved. 1. Introduction Vascular tumors of the anterior mediastinum are scarce and represent approximately 1% to 2% of all tumors in this location [1]. Angiosarcomas are most often encountered as sporadic cutaneous lesions, typically in the scalp or face of an elderly patient. However, angiosarcomas can occur in virtually any anatomic site, including the deep soft tissue, breast, visceral organs, and bone. Although most cases are sporadic, important predisposing conditions include radia- tion exposure, chronic lymphedema, exposure to toxins such as vinyl chloride or thorotrast, or foreign bodies [2]. Primary angiosarcomas of the anterior mediastinum are extremely rare and, to date, less than 25 cases of this entity have been described either as isolated case reports or as part of larger studies investigating angiosarcomas in general [1,3-8]. We herein report a series of 9 cases and present the ⁎ Corresponding author. E-mail address: [email protected] (A. Weissferdt). www.elsevier.com/locate/humpath 0046-8177/$ – see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.humpath.2010.05.003 Human Pathology (2010) 41, 1711–1717
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Primary angiosarcomas of the anterior mediastinum

www.elsevier.com/locate/humpath
Human Pathology (2010) 41, 1711–1717
Original contribution
Primary angiosarcomas of the anterior mediastinum:A clinicopathologic and immunohistochemicalstudy of 9 cases
Annikka Weissferdt MDa,⁎, Neda Kalhor MDa, Saul Suster MDb, Cesar A. Moran MDa
aDepartment of Pathology and Laboratory Medicine, MD Anderson Cancer Center, Houston, TX 77030, USAbDepartment of Pathology and Laboratory Services, Medical College of Wisconsin, Milwaukee, WI53226, USA
Received 3 March 2010; revised 9 May 2010; accepted 12 May 2010
0d
Keywords:Angiosarcoma;Anterior mediastinum;Thymus;Immunohistochemistry
Summary We report 9 cases of primary angiosarcomas of the anterior mediastinum. Patient ages rangedfrom 25 to 62 years (mean, 40.7 years); 5 patients were male and 4 were female. Main presentingsymptoms included chest pain, dyspnea, and cough. The tumor size ranged from 3 to 12.5 cm.Macroscopically, the lesions were ill-defined hemorrhagic masses. Histologically, the growth patternsranged from large vascular spaces to capillary-like proliferations. These were either lined by bland ormore pleomorphic endothelial cells. The mitotic activity was variable and corresponded to the degree ofdifferentiation. A rim of thymic tissue was observed in 2 cases suggesting a thymic origin of the tumors.No teratomatous components were identified. Immunohistochemical studies showed that all 9 caseswere reactive for vascular markers including factor VIII–related antigen, CD31, and CD34, andnegative for cytokeratin CAM5.2. All cases were treated by complete resection and 3 patients receivedadjuvant chemotherapy. Follow-up information available for 6 patients revealed that 4 were alive andfree of disease at intervals ranging from 6 to 36 months after diagnosis and 1 was alive with recurrenceat 48 months. One patient had died of the disease 10 months after diagnosis. Primary angiosarcomas ofthe anterior mediastinum are rare tumors that need to be added to the differential diagnosis of primaryanterior mediastinal neoplasms. Despite their histologic similarity to angiosarcomas at other sites,primary angiosarcomas of the anterior mediastinum appear to follow a more protracted clinical coursethan their counterparts in other organ systems.© 2010 Elsevier Inc. All rights reserved.
1. Introduction virtually any anatomic site, including the deep soft tissue,
Vascular tumors of the anterior mediastinum are scarceand represent approximately 1% to 2% of all tumors in thislocation [1]. Angiosarcomas are most often encountered assporadic cutaneous lesions, typically in the scalp or face ofan elderly patient. However, angiosarcomas can occur in
⁎ Corresponding author.E-mail address: [email protected] (A. Weissferdt).
046-8177/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2010.05.003
breast, visceral organs, and bone. Although most cases aresporadic, important predisposing conditions include radia-tion exposure, chronic lymphedema, exposure to toxins suchas vinyl chloride or thorotrast, or foreign bodies [2]. Primaryangiosarcomas of the anterior mediastinum are extremelyrare and, to date, less than 25 cases of this entity have beendescribed either as isolated case reports or as part of largerstudies investigating angiosarcomas in general [1,3-8].We herein report a series of 9 cases and present the
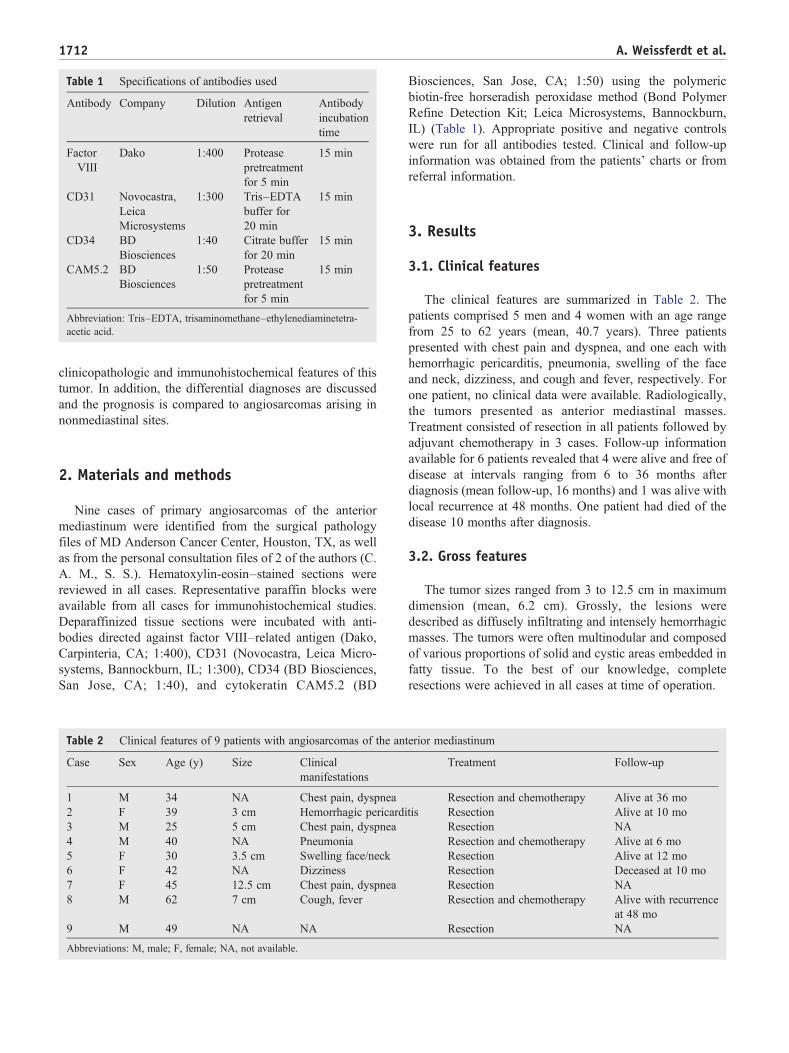
Table 1 Specifications of antibodies used
Antibody Company Dilution Antigenretrieval
Antibodyincubationtime
FactorVIII
Dako 1:400 Proteasepretreatmentfor 5 min
15 min
CD31 Novocastra,LeicaMicrosystems
1:300 Tris–EDTAbuffer for20 min
15 min
CD34 BDBiosciences
1:40 Citrate bufferfor 20 min
15 min
CAM5.2 BDBiosciences
1:50 Proteasepretreatmentfor 5 min
15 min
Abbreviation: Tris–EDTA, trisaminomethane–ethylenediaminetetra-acetic acid.
1712 A. Weissferdt et al.
clinicopathologic and immunohistochemical features of thistumor. In addition, the differential diagnoses are discussedand the prognosis is compared to angiosarcomas arising innonmediastinal sites.
2. Materials and methods
Nine cases of primary angiosarcomas of the anteriormediastinum were identified from the surgical pathologyfiles of MD Anderson Cancer Center, Houston, TX, as wellas from the personal consultation files of 2 of the authors (C.A. M., S. S.). Hematoxylin-eosin–stained sections werereviewed in all cases. Representative paraffin blocks wereavailable from all cases for immunohistochemical studies.Deparaffinized tissue sections were incubated with anti-bodies directed against factor VIII–related antigen (Dako,Carpinteria, CA; 1:400), CD31 (Novocastra, Leica Micro-systems, Bannockburn, IL; 1:300), CD34 (BD Biosciences,San Jose, CA; 1:40), and cytokeratin CAM5.2 (BD
Table 2 Clinical features of 9 patients with angiosarcomas of the an
Case Sex Age (y) Size Clinicalmanifestations
1 M 34 NA Chest pain, dyspnea2 F 39 3 cm Hemorrhagic pericardi3 M 25 5 cm Chest pain, dyspnea4 M 40 NA Pneumonia5 F 30 3.5 cm Swelling face/neck6 F 42 NA Dizziness7 F 45 12.5 cm Chest pain, dyspnea8 M 62 7 cm Cough, fever
9 M 49 NA NA
Abbreviations: M, male; F, female; NA, not available.
Biosciences, San Jose, CA; 1:50) using the polymericbiotin-free horseradish peroxidase method (Bond PolymerRefine Detection Kit; Leica Microsystems, Bannockburn,IL) (Table 1). Appropriate positive and negative controlswere run for all antibodies tested. Clinical and follow-upinformation was obtained from the patients' charts or fromreferral information.
3. Results
3.1. Clinical features
The clinical features are summarized in Table 2. Thepatients comprised 5 men and 4 women with an age rangefrom 25 to 62 years (mean, 40.7 years). Three patientspresented with chest pain and dyspnea, and one each withhemorrhagic pericarditis, pneumonia, swelling of the faceand neck, dizziness, and cough and fever, respectively. Forone patient, no clinical data were available. Radiologically,the tumors presented as anterior mediastinal masses.Treatment consisted of resection in all patients followed byadjuvant chemotherapy in 3 cases. Follow-up informationavailable for 6 patients revealed that 4 were alive and free ofdisease at intervals ranging from 6 to 36 months afterdiagnosis (mean follow-up, 16 months) and 1 was alive withlocal recurrence at 48 months. One patient had died of thedisease 10 months after diagnosis.
3.2. Gross features
The tumor sizes ranged from 3 to 12.5 cm in maximumdimension (mean, 6.2 cm). Grossly, the lesions weredescribed as diffusely infiltrating and intensely hemorrhagicmasses. The tumors were often multinodular and composedof various proportions of solid and cystic areas embedded infatty tissue. To the best of our knowledge, completeresections were achieved in all cases at time of operation.
terior mediastinum
Treatment Follow-up
Resection and chemotherapy Alive at 36 motis Resection Alive at 10 mo
Resection NAResection and chemotherapy Alive at 6 moResection Alive at 12 moResection Deceased at 10 moResection NAResection and chemotherapy Alive with recurrence
at 48 moResection NA

Table 3 Histologic features of 9 patients with angiosarcomas of the anterior mediastinum
Case Grade Histologic characteristics Necrosis a
(%)Growthpattern
Mitotic activity(mitoses/10 HPF)
Thymictissueidentified
Presence ofgerm celltumor
1 High grade Cavernous; focal papillary endothelialhyperplasia pattern
20 Infiltrative 3 No No
2 Low grade Capillary 30 Infiltrative 1 No No3 High grade Capillary and cavernous 10 Infiltrative 3 No No4 High grade Capillary and cavernous; focal epithelioid
features10 Infiltrative 1 No No
5 Low grade Capillary and cavernous 30 Infiltrative 2 No No6 High grade Capillary and cavernous; focal papillary
endothelial hyperplasia; epithelioid features70 Infiltrative 3 No No
7 Low grade Capillary 0 Infiltrative 1 Yes No8 High grade Capillary 10 Infiltrative 5 No No9 Low and high
gradeFocal papillary endothelial hyperplasia;calcification, ossification and cysticdegeneration; stromal tumor giant cells
10 Infiltrative 2 Yes No
Abbreviation: HPF, high-power fields.a Percentage of necrosis in material available for review.
1713Primary angiosarcomas of the anterior mediastinum
3.3. Histological features
The histologic features are summarized in Table 3. Themorphologic spectrum ranged from low-grade tumorsmimicking benign vascular lesions to high-grade tumorswith prominent cytologic atypia and high mitotic activity.Overall, 5 cases were considered high grade, 3 low grade,and 1 had mixed high- and low-grade histologic features.Growth patterns included large cavernous vascular struc-tures, irregular interanastomosing channels of varying size,small capillary-like proliferations, and slit-like spaces linedby atypical endothelial cells (Figs. 1-3). Vascular spaceformation was more difficult to identify in areas with moresolid growth patterns. The atypical cells had larger and more
Fig. 1 Angiosarcoma composed of large cavernous vascularspaces (case 1).
hyperchromatic nuclei than normal endothelial cells andfocally showed crowding or a prominent hobnailing pattern.In 3 cases, papillary projections resembling endothelialpapillary hyperplasia were noted (Fig. 4). In 2 cases, theendothelial cells showed a prominent epithelioid morphol-ogy characterized by cells with abundant cytoplasm,vesicular nuclei, and small eosinophilic nucleoli (Fig. 5).Isolated pleomorphic tumor giant cells were identified in thestromal background of 1 case (Fig. 6). The stroma wascomposed of fibrous or myxoid tissue and in some areasthe tumor was dissecting the preexisting fat. In 8 cases,necrosis was present ranging from 10% to 70% of the tissueavailable for review and the mitotic rate ranged from 1 to 5mitoses per 10 high-power fields. Foci of hemorrhage, red
Fig. 2 Proliferation of capillary-like vessels in low-gradeangiosarcoma (case 2).

Fig. 3 Angiosarcoma forming irregular slit-like vascular spaces(case 2).
Fig. 5 Solid growth pattern of high-grade angiosarcoma withpleomorphic epithelioid cells and increased mitotic activity (case 6).
1714 A. Weissferdt et al.
blood cell extravasation, and hemosiderin deposition wereevident in most cases. Calcification, ossification, and cysticdegeneration were noted in 1 case. Overall, 7 cases showedthe pattern of conventional angiosarcoma, 1 was classified asan epithelioid type, and 1 demonstrated a mixed pattern. Aperipheral rim of thymic tissue was observed in 2 casessuggesting a thymic origin of these tumors. Teratomatous orother germ cell elements were not identified in any of thecases.
3.4. Immunohistochemical features
The immunohistochemical features are summarized inTable 4. All 9 cases showed at least focal cytoplasmicpositivity for factor VIII–related antigen including low- andhigh-grade areas of differentiation (100%) (Fig. 7). Stainingfor CD31 was performed on 6 tumors, 3 of which showedreactivity for this marker (50%). Staining for CD34performed on 5 cases resulted in positive staining in all 5
Fig. 4 Papillary endothelial hyperplasia-like areas (case 9).
tumors (100%). None of the cases were positive forCAM5.2.
4. Discussion
Angiosarcoma is an uncommon tumor representing lessthan 1% of all sarcomas [9]. Although the most commonclinical presentation is as a cutaneous tumor in the scalp andfacial regions of elderly men, angiosarcomas occur in manylocations including soft tissue, breast, visceral organs, andbone [2]. Apart from the sporadic forms, there is a strongassociation of angiosarcomas occurring with radiation,environmental carcinogens such as vinyl chloride orthorotrast, chronic lymphedema, or foreign bodies [2].Median age at presentation is 52 years and the prognosis isgenerally poor with a median survival of 42 months and a
Fig. 6 Irregular vascular spaces with atypical stromal cells(case 9).

Table 4 Immunohistochemical features of angiosarcomas ofthe anterior mediastinum
Case Immunohistochemistry of angiosarcomas of theanterior mediastinum
Factor VIII CD31 CD34 CAM5.2
1 + − + −2 + + + −3 + + + −4 + − + −5 + NA NA −6 + − + −7 + NA NA −8 + NA NA −9 + + NA −
Abbreviation: NA, not available.
1715Primary angiosarcomas of the anterior mediastinum
5-year overall survival of 43% [10]. Angiosarcomas are,however, a heterogeneous group of tumors and apart fromstage at diagnosis, an important prognostic factor is theprimary site. Whereas angiosarcomas of the liver, bone, andheart have a particularly bad outcome with 5-year survivalrates ranging from 0% to 36%, tumors of the breast, softtissue, and skin appear to be associated with a slightly betterprognosis as reflected in 5-year survival rates ranging from43% to 74% [10].
Primary angiosarcomas arising in the anterior mediasti-num are very rare. To date, less than 25 cases of this entityhave been described in this location [1,3-8]. The age of thepatients ranged from 5 to 66 years and most tumors werelocated in the anterior mediastinum [5,8]. Chest pain was themain presenting symptom and, from the limited dataavailable, survival ranged from 2 to 36 months from timeof diagnosis [3,7,8,11]. We have studied a further 9 cases ofangiosarcoma arising in the mediastinum. Clinically, thepatients all presented with the typical symptoms of anteriormediastinal masses, namely, chest pain, dyspnea, and cough.The patients' age ranged from 25 to 62 years with a mean ageof 40.7 years. Radiologically, the tumors presented as
Fig. 7 Immunohistochemical staining with CD34 (case 3).
nonspecific anterior mediastinal masses. Histologically, thetumors displayed the typical spectrum of features seen inother locations, ranging from low-grade neoplasms withdefinitive vasoformation to high-grade lesions with a moresolid growth pattern and vast areas of necrosis. Themalignant endothelial cells lining these structures demon-strated variably atypical features ranging from mild nuclearhyperchromasia to highly pleomorphic cells with atypicalmitotic figures. Immunohistochemically, the tumors did notdiffer from their counterparts in other locations. All lesionsshowed at least focal immunoreactivity with the vascularmarkers factor VIII–related antigen, CD34, and CD31, andall were negative for CAM5.2.
Interestingly, follow-up information available for 6patients revealed that 4 were alive and free of disease atintervals ranging from 6 to 36 months after diagnosis (meanfollow up, 16 months). One patient was alive with localrecurrence at 48 months, whereas another patient had died ofthe disease 10 months after diagnosis. Comparing thesesurvival times to those of angiosarcomas in other locationssuch as the deep soft tissue (median survival, 20 months) orthe heart (median survival, 9-12 months) [6,11,12], angio-sarcomas of the anterior mediastinum seem to pursue a lessaggressive clinical course. Because age of presentation,histology, and treatment modalities do not appear to differmuch from tumors in other locations, alternative explana-tions for this improved prognosis will have to be explored[6,11,13]. One possibility may be that the surgical approachof the anterior mediastinum may facilitate complete surgicalresection and avoid local tumor recurrence. Tumor recur-rence is known to occur in at least 20% of cases ofangiosarcomas of the soft tissue [6] and complete surgicalresection may account for the better outcome in patients withmediastinal tumors.
Because of the rarity of mediastinal angiosarcomas, theseneoplasms need to be differentiated from a variety of othertumors that can occur in this location. The most importantdifferential diagnosis of the epithelioid type of angiosarcomais epithelioid hemangioendothelioma (Table 5). Epithelioidhemangioendothelioma is a vascular neoplasm of low tointermediate malignant potential that follows a nonaggres-sive clinical course. This tumor has been described in the softtissue as well as in various other organ systems includingbone, liver, and lung [14-16]. The anterior mediastinum isless commonly the site of origin [17]. Epithelioid heman-gioendothelioma, regardless of its primary site, is typicallycomposed of nodules with centrally hypocellular andperipherally hypercellular areas. The tumor cells aremonomorphic and contain round to oval pale nuclei withsmall nucleoli and eosinophilic cytoplasm. Intranuclear orintracytoplasmic vacuoles are often present, sometimescontaining erythrocytes. The stroma shows prominentmyxoid or chondroid changes. Mitotic activity, cellularatypia, and tumor cell necrosis are typically not observed,although in isolated cases, foci of necrosis and infarctionmay be seen [17,18]. Immunohistochemical studies do not

Table 5 Common characteristics of angiosarcomas and epithelioid hemangioendotheliomas of the anterior mediastinum
Angiosarcoma of anterior mediastinum Epithelioid hemangioendotheliomaof anterior mediastinum17
Clinical features Chest pain, dyspnea, cough, hemorrhagic pericarditis, pneumonia,dizziness, fever, swollen face/neck; mean age 40.7 y
Chest pain, cough, dyspnea, many timesasymptomatic; mean age 49.4 y
Radiologic features Anterior mediastinal masses Anterior mediastinal masses;often multifocal process
Gross features Multinodular solid-cystic hemorrhagic masses with infiltrativeborders
Often well circumscribed and encapsulatedmasses, rarely locally infiltrative
Cytologic features Enlarged hyperchromatic endothelial cells; epithelioid endothelialcells with vesicular nuclei and eosinophilic nucleoli
Nests and cords of bland epithelioid cellswith inconspicuous nucleoli
Stroma Myxoid, hyalinized, or fibrous background Prominent myxohyaline backgroundMitoses Variable; average 2.3/10 HPF Few; average 1/10 HPFNecrosis Prominent Absent or focalImmunohistochemicalfeatures
Factor VIII–related antigen, CD34, CD31, CK may be positivein epithelioid subtype
Factor VIII–related antigen, CD34, CD31
Prognosis Aggressive (but less aggressive than angiosarcomas at other sites) Low to intermediate malignant behavior
Abbreviation: HPF, high-power fields; CK, cytokeratin.
1716 A. Weissferdt et al.
differentiate between the lesions as both demonstrate avascular phenotype with immunoreactivity for factor VIII–related antigen, CD31, and CD34 [6,19]. Distinctionbetween the 2 lesions, however, is vital as epithelioidhemangioendothelioma may run a less aggressive clinicalcourse, whereas epithelioid angiosarcoma has a much higherpotential for progression and metastasis [6,14,17].
Epithelioid angiosarcomas also need to be differentiatedfrom carcinoma. Carcinomas, whether primary or metastatic,lack a vasoformative component and express an epithelialimmunohistochemical phenotype; they show no reactivityfor vascular markers. On the other hand, low-gradeangiosarcoma may resemble benign vascular lesions suchas a hemangioma. Cytologic atypia, increased mitoticactivity, and especially infiltrative margins in the formermay be the only features distinguishing these lesions [20].
Another important diagnostic consideration is the possi-bility that angiosarcomas may occur in association withmediastinal germ cell tumors. The presence of this so-calledsarcomatous transformation in these tumors carries a graveprognosis with early local recurrence and metastasis andsurvival times that range from 9 to 33 months [21-23].Distinction of pure mediastinal angiosarcomas from the lattertumors through thorough sampling is therefore vital giventhe difference in outcome.
In summary, we have presented the clinicopathologic andimmunohistochemical features of 9 cases of primaryangiosarcomas of the anterior mediastinum. Despite theaggressive behavior of these tumors in other sites, angio-sarcomas of the anterior mediastinum appear to have a betterprognosis. Whether this is due to easier surgical access at thissite resulting in a higher rate of complete surgical resectionremains to be determined. Primary angiosarcomas need to beincluded in the differential diagnosis of anterior mediastinalneoplasms, and distinction from other tumors at this site isimportant given the potential difference in prognosis.
References[1] Wychulis AR, PayneWS, Clagett OT, Woolner LB. Surgical treatment
of mediastinal tumors: a 40 year experience. J Thorac Cardiovasc Surg1971;62:379-92.
[2] Lucas DR. Angiosarcoma, radiation-associated angiosarcoma, andatypical vascular lesion. Arch Pathol Lab Med 2009;133:1804-9.
[3] Pachter MR, Lattes R. Mesenchymal tumors of the mediastinum. II.Tumors of blood vascular origin. Cancer 1963;16:95-105.
[4] Gibbs AR, Johnson NF, Giddings JC, Powell DE, Jasani B. Primaryangiosarcoma of the mediastinum: light and electron microscopicdemonstration of factor VIII–related antigen in neoplastic cells. HUM
PATHOL 1984;15:687-91.[5] Kardamakis D, Bouboulis N, Ravazoula P, Dimopoulos P, Dougenis
D. Primary hemangiosarcoma of the mediastinum. Lung Cancer 1996;16:81-6.
[6] Meis-Kindblom JM, Kindblom LG. Angiosarcoma of soft tissue: astudy of 80 cases. Am J Surg Pathol 1998;22:683-97.
[7] Chen TJ, Chiou CC, Chen CH, Kuo TT, Hong HS. Metastasis ofmediastinal epithelioid angiosarcoma to the finger. Am J ClinDermatol 2008;9:181-3.
[8] Deyrup AT, Miettinen M, North PE, et al. Angiosarcomas arising inthe viscera and soft tissue of children and young adults: aclinicopathologic study of 15 cases. Am J Surg Pathol 2009;33:264-9.
[9] Enzinger FM, Weiss SW. Malignant vascular tumors. In: Weiss SW,Goldblum JR, editors. Soft tissue tumors. Philadelphia, PA: MosbyElsevier; 2008. p. 703-20.
[10] Fayette J, Martin E, Piperno-Neumann S, et al. Angiosarcomas, aheterogeneous group of sarcomas with specific behavior depending onprimary site: a retrospective study of 161 cases. Ann Oncol 2007;18:2030-6.
[11] Fong Y, Coit DG, Woodruff JM, Brennan MF. Lymph node metastasisfrom soft tissue sarcoma in adults. Analysis of data from a prospectivedatabase of 1772 sarcoma patients. Ann Surg 1993;217:72-7.
[12] Pigott C, Welker M, Khosla P, Higgins RS. Improved outcome withmultimodality therapy in primary cardiac angiosarcoma. Nat Clin PractOncol 2008;5:112-5.
[13] Reardon MJ, Walkes JC, Benjamin R. Therapy insight: malignantprimary cardiac tumors. Nat Clin Pract Cardiovasc Med 2006;3:548-53.
[14] Weiss SW, Enzinger FM. Epithelioid hemangioendothelioma: avascular tumor often mistaken for a carcinoma. Cancer 1982;50:970-81.

1717Primary angiosarcomas of the anterior mediastinum
[15] Dail DH, Liebow AA, Gmelich JT, et al. Intravascular, bronchiolar,and alveolar tumor of the lung (IVBAT). An analysis of twenty casesof a peculiar sclerosing endothelial tumor. Cancer 1983;51:453-64.
[16] Dietze O, Davies SE, Williams R, Portmann B. Malignant epithelioidhaemangioendothelioma of the liver: a clinicopathological andhistochemical study of 12 cases. Histopathology 1989;15:225-37.
[17] Suster S, Moran CA, Koss MN. Epithelioid hemangioendothelioma ofthe anterior mediastinum. Clinicopathologic, immunohistochemical,and ultrastructural analysis of 12 cases. Am J Surg Pathol 1994;18:871-81.
[18] Allen PW, Ramakrishna B, MacCormac LB. The histiocytoidhemangiomas and other controversies. Pathol Annu 1992;27:51-87.
[19] Mentzel T, Beham A, Calonje E, Katenkamp D, Fletcher CD.Epithelioid hemangioendothelioma of skin and soft tissues: clinico-
pathologic and immunohistochemical study of 30 cases. Am J SurgPathol 1997;21:363-74.
[20] Moran CA, Suster S. Mediastinal hemangiomas: a study of 18 caseswith emphasis on the spectrum of morphological features. HUM PATHOL1995;26:416-21.
[21] Gonzalez-Vela JL, Savage PD, Manivel JC, Torkelson JL, KennedyBJ. Poor prognosis of mediastinal germ cell cancers containingsarcomatous components. Cancer 1990;66:1114-6.
[22] Malagón HD, Valdez AM,Moran CA, Suster S. Germ cell tumors withsarcomatous components: a clinicopathologic and immunohistochem-ical study of 46 cases. Am J Surg Pathol 2007;31:1356-62.
[23] Contreras AL, Punar M, Tamboli P, et al. Mediastinal germ cell tumorswith an angiosarcomatous component: a report of 12 cases. HUM
PATHOL 2010;41:832-7.