
Accuracy of biopsy sampling for subtyping basal cell carcinoma
6
Accuracy of biopsy sampling for subtyping basal cell carcinoma Andrea L. Haws, MD, MS, a Rafael Rojano, MD, a Steven R. Tahan, MD, b and Thuy L. Phung, MD, PhD a Houston, Texas, and Boston, Massachusetts Background: Basal cell carcinoma (BCC) is a common skin cancer for which the treatment and recurrence risk correlate with the histologic subtype. Limited information is available regarding the accuracy of biopsy in diagnosing BCC subtypes. Objective: We sought to determine the correlation between BCC subtypes present in a biopsy specimen and the actual subtypes present in a tumor. Methods: In this retrospective study, skin biopsy specimens and corresponding excisions were reviewed. All histologic subtypes present in the biopsy specimen were reported and compared with the composite BCC subtype present in the biopsy specimen and excision. Results: A total of 232 biopsy specimens and corresponding wide excisions were examined. The biopsy specimen accuracy rate was 82% for punch and shave biopsy specimens. Mixed histologic subtypes were seen in 54% of the cases, half of which contained an aggressive subtype (infiltrative, morpheaform, or micronodular). There was an 18% discordance rate between the biopsy specimen subtype and the composite subtype. Importantly, 40% of these discordant cases (7% of all cases examined) had an aggressive subtype that was not sampled in the initial biopsy specimen. Furthermore, some cases were misidentified as infiltrative subtype in the biopsy specimen as a result of misinterpretation of surface ulceration and reactive stromal changes. Limitations: The limited number of punch biopsy specimens and the fact that Mohs excisions were not included are limitations. Conclusions: Punch and shave biopsy specimens provided adequate sampling for correct BCC subtyping in 82% of the cases examined. However, 18% of the biopsy specimens were misidentified, some of which missed an aggressive component. Thus, there are potential pitfalls in the identification of BCC subtypes in biopsy specimens, which may have important implications in treatment outcome. ( J Am Acad Dermatol 2012;66:106-11.) Key words: accuracy; basal cell carcinoma; biopsy; excision; histologic subtypes. B asal cell carcinoma (BCC) is one of the most common human cancers and constitutes more than 80% of nonmelanoma skin can- cers. 1,2 Although BCC is a tumor with low metastatic potential, it can be locally destructive and invasive. 2,3 There are multiple known histologic subtypes (ie, growth patterns) of BCC. Each subtype has an associated biological behavior that can affect the likelihood of tumor recurrence and treatment mo- dality. 4-6 Infiltrative, morpheaform, and micronodu- lar BCC are aggressive subtypes and have a high likelihood of incomplete excision and recurrence. 4,7 BCC with mixed histologic subtypes is defined as tumor composed of two or more growth patterns within the same lesion, such as superficial pattern in the epidermis and infiltrative pattern in the dermis. These tumors behave in the manner of the most aggressive subtype present. 6,7 Noninvasive treat- ment may be offered for selected patients with low-risk superficial BCC, 6 whereas Mohs From the Department of Pathology and Immunology, Baylor College of Medicine, Houston, a and Department of Pathology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston. b Funding sources: None. Conflicts of interest: None declared. Reprint requests: Thuy L. Phung, MD, PhD, Baylor College of Medicine, One Baylor Plaza, Mail Stop Code BCM315, Houston, TX 77030. E-mail: [email protected]. Published online July 29, 2011. 0190-9622/$36.00 Ó 2011 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2011.02.042 106
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Accuracy of biopsy sampling for subtyping basal cell carcinoma

Accuracy of biopsy sampling for subtyping basalcell carcinoma
Andrea L. Haws, MD, MS,a Rafael Rojano, MD,a Steven R. Tahan, MD,b and Thuy L. Phung, MD, PhDa
Houston, Texas, and Boston, Massachusetts
From
C
Be
Sc
Fund
Conf
Repr
M
TX
Publ
0190
� 20
doi:1
106
Background: Basal cell carcinoma (BCC) is a common skin cancer for which the treatment and recurrencerisk correlate with the histologic subtype. Limited information is available regarding the accuracy of biopsyin diagnosing BCC subtypes.
Objective: We sought to determine the correlation between BCC subtypes present in a biopsy specimenand the actual subtypes present in a tumor.
Methods: In this retrospective study, skin biopsy specimens and corresponding excisions were reviewed.All histologic subtypes present in the biopsy specimen were reported and compared with the compositeBCC subtype present in the biopsy specimen and excision.
Results: A total of 232 biopsy specimens and corresponding wide excisions were examined. The biopsyspecimen accuracy rate was 82% for punch and shave biopsy specimens. Mixed histologic subtypes wereseen in 54% of the cases, half of which contained an aggressive subtype (infiltrative, morpheaform, ormicronodular). There was an 18% discordance rate between the biopsy specimen subtype and thecomposite subtype. Importantly, 40% of these discordant cases (7% of all cases examined) had anaggressive subtype that was not sampled in the initial biopsy specimen. Furthermore, some cases weremisidentified as infiltrative subtype in the biopsy specimen as a result of misinterpretation of surfaceulceration and reactive stromal changes.
Limitations: The limited number of punch biopsy specimens and the fact that Mohs excisions were notincluded are limitations.
Conclusions: Punch and shave biopsy specimens provided adequate sampling for correct BCC subtypingin 82% of the cases examined. However, 18% of the biopsy specimens were misidentified, some of whichmissed an aggressive component. Thus, there are potential pitfalls in the identification of BCC subtypes inbiopsy specimens, which may have important implications in treatment outcome. ( J Am Acad Dermatol2012;66:106-11.)
Key words: accuracy; basal cell carcinoma; biopsy; excision; histologic subtypes.
2,3
Basal cell carcinoma (BCC) is one of the mostcommon human cancers and constitutesmore than 80% of nonmelanoma skin can-
cers.1,2 Although BCC is a tumor with low metastatic
the Department of Pathology and Immunology, Baylor
ollege of Medicine, Houston,a and Department of Pathology,
th Israel Deaconess Medical Center and Harvard Medical
hool, Boston.b
ing sources: None.
licts of interest: None declared.
int requests: Thuy L. Phung, MD, PhD, Baylor College of
edicine, One Baylor Plaza, Mail Stop Code BCM315, Houston,
77030. E-mail: [email protected].
ished online July 29, 2011.
-9622/$36.00
11 by the American Academy of Dermatology, Inc.
0.1016/j.jaad.2011.02.042
potential, it can be locally destructive and invasive.There are multiple known histologic subtypes (ie,growth patterns) of BCC. Each subtype has anassociated biological behavior that can affect thelikelihood of tumor recurrence and treatment mo-dality.4-6 Infiltrative, morpheaform, and micronodu-lar BCC are aggressive subtypes and have a highlikelihood of incomplete excision and recurrence.4,7
BCC with mixed histologic subtypes is defined astumor composed of two or more growth patternswithin the same lesion, such as superficial pattern inthe epidermis and infiltrative pattern in the dermis.These tumors behave in the manner of the mostaggressive subtype present.6,7 Noninvasive treat-ment may be offered for selected patients withlow-risk superficial BCC,6 whereas Mohs

J AM ACAD DERMATOL
VOLUME 66, NUMBER 1Haws et al 107
micrographic surgery is recommended for recurrentfacial BCC and BCC with aggressive subtypes.8
Evaluation of BCC is made on a clinical basis andsupported by a shave or punch skin biopsy to estab-lish the diagnosis. However, only a few studies todate, each with different criteria for determiningbiopsy-excision concordance, have evaluated the
CAPSULE SUMMARY
d Current management of basal cellcarcinoma depends on the tumor’sbiologic behavior, which correlates withits histologic growth pattern.
d Biopsy specimen did not correctlyidentify histologic subtypes in basal cellcarcinoma in 18% of the cases examined;40% of these cases had an aggressivesubtype not sampled in the initial biopsyspecimen.
d Broad and deep biopsy specimento sample the superficial and deepaspects of basal cell carcinoma wouldimprove tumor subtyping accuracy. Alltumor subtypes present should bereported.
correlation of BCC subtypespresent in the initial biopsyspecimen and the follow-upwide excision. It has beenreported that the accuracyrate of BCC subtyping in bi-opsy specimen is 80%.9
However, studies of patientswho underwent Mohs micro-graphic surgery for BCCreported low correlation be-tween biopsy specimen andMohs excision. One studyreported that only 10% ofthe initial biopsy specimensreported BCC with mixedsubtypes when these tumorswere actually found in 40% ofMohs resections, and a sec-ond study reported 51.1%concordance of biopsy spec-imen with Mohs excision.8,10
Given the limited numbers of published studiesevaluating the adequacy of biopsy specimen for BCCsubtyping and the wide differences found in thesereports, we undertook a study to systematicallycompare the tumor subtypes present in the initialbiopsy specimen with the composite subtypes pre-sent in the biopsy specimen and wide excision. Wedetermined the accuracy rate of biopsy specimen incorrectly identifying all the subtypes present in atumor, and evaluated trends towardmisidentificationof tumor subtypes.
METHODSThe use of pathology archival material was ap-
proved by the Institutional Review Boards at the BethIsrael Deaconess Medical Center, Boston, MA, andBaylor College of Medicine/Ben Taub GeneralHospital, Houston, TX. This retrospective studyincluded a total of 232 cases from these two institu-tions. Inclusion criteria were patients with primarycutaneous BCC and subsequent wide excision. Casesthat had no residual BCC tumor in the excision wereexcluded. Of 232 cases, 128 cases were from theDepartment of Pathology, Beth Israel DeaconessMedical Center, submitted over a 23-month periodfrom January 1, 2001, to November 1, 2002. These
biopsy specimens and excisions were independentlyreviewed by two dermatopathologists who wereblinded to patient identification. An additional 104cases were from the Department of Pathology, BenTaub General Hospital, submitted from October 7,2004, to October 1, 2009. These biopsy specimensand excisions were reviewed by one pathologist
who was blinded to patientidentification.
The BCC subtypes wereidentified based on standardhistopathologic characteris-tics.4,11 Superficial BCC is tu-mor consisting of multiplesmall islands of basaloid cellsattached to the epidermisand confined to the papillarydermis. Nodular BCC hassmall and large roundednests of tumor cells with pe-ripheral palisading present inthe dermis or growing pre-dominantly downward fromthe epidermis into the der-mis. Micronodular BCC re-sembles nodular type butthe nests are much smallerwith wide infiltration in thedermis. Infiltrative BCC has
irregular, thin nests and cords of basaloid cells, someof which may have an irregular outline with pointedspiky projections, interspersed and infiltrating be-tween dermal collagen bundles. Morpheaform BCCconsists of narrow elongated strands and smallislands of tumor cells embedded within a densefibrous stroma. Metatypical BCC is tumor with nestsand strands of basaloid tumor cells that mature intolarger paler cells.
Upon review of biopsy specimens and excisions,every subtype present in the tumor was recorded.The composite BCC subtypes were defined as thecombined subtypes present in the biopsy specimenand thewide excision. BCCwithmixed subtypeswasdefined as tumor consisting of two or more growthpatterns within the same lesion, such as superficialsubtype in the epidermis and infiltrative subtype inthe dermis. Different BCC subtypes were groupedbased on biologic behavior: nonaggressive subtypesconsisting of superficial and nodular patterns; andaggressive subtypes consisting of infiltrative, micro-nodular, morpheaform, or metatypical pattern.Percent concordance was calculated as the percentof cases in which the BCC subtypes present in thebiopsy specimen were the same as the compositesubtypes. Percent discordance was calculated as the

Table I. Distribution of basal cell carcinomasubtypes
Total biopsy specimens 232Shave 88% (205)Punch 12% (27)
BCC subtype Percent of total cases(No. of cases)
Single subtype 46 (107/232)Superficial 12 (28)Nodular 30 (70)Aggressive 4 (9)
Mixed subtypes 54 (125/232)Superficial 1 nodular 27 (62)Mixed with aggressive subtype* 27 (63)
BCC, Basal cell carcinoma.
*Tumor consisting of more than one subtype, of which at least
one is an aggressive subtype.
J AM ACAD DERMATOL
JANUARY 2012108 Haws et al
percent of cases in which the BCC subtypes in thebiopsy specimen were different from the compositesubtypes.
RESULTSOf the total biopsy specimens examined, 88%
(205/232) were shave biopsy specimens and 12%(27/232) were punch biopsy specimens (Table I).The most common BCC pattern observed was mixedhistologic subtypes, consisting of 54% (125/232) ofall the cases. Of note, 50% (63/125) of the mixedsubtype tumors (27% of total cases) had an aggres-sive component, which was composed of infiltrative,micronodular, morpheaform, or metatypical growthpattern. BCC with a single subtype was seen in 46%(107/232) of the total cases with nodular subtypebeing the most common (30% of total cases),followed by superficial (12%) and aggressive (4%)subtypes.
There was an overall 82% (190/232) concordancerate between the BCC subtypes present in a biopsyspecimen and the composite subtypes (Table II). Theaccuracy rates for shave and punch biopsy speci-mens were 81% and 89%, respectively. High concor-dance rate for biopsy specimen was seen within thefollowing groups of BCC subtypes: 96% (44/46) formixed superficial and nodular subtypes, 90% (28/31)for superficial subtype, 90% (9/10) for aggressivesubtype, and 87% (46/53) for mixed subtypes withaggressive component. The lowest concordance ratewas seen with nodular subtype in which only 68%(63/92) of the biopsy specimen subtype correlatedwith the composite subtype.
There was an overall 18% (42/232) discordance inwhich the subtypes in the initial biopsy specimen didnot entirely correlate with the composite BCC
subtype (Table II). The highest discordance wasseen with nodular subtype, in which 32% (29/92) ofthe initial biopsy specimens showed nodular BCCbut failed to detect the other components of thetumor, namely superficial and aggressive subtypes,which were later identified in the wide excision (Fig1, A to D). Diagnostic discrepancies were also foundin other subtype groups: 13% (7/53) discordance inmixed subtypes with aggressive component, 10%(3/31) in superficial subtype, 10% (1/10) in infiltra-tive subtype, and 4% (2/46) in mixed superficial andnodular subtypes.
Because of themoremalignant biological behaviorof aggressive subtypes, we determined from thegroup of biopsy specimens that were misidentifiedthe number of cases that had missed an aggressivetumor component. We found that in 40% (17/42) ofthe discordant cases (7% of the total cases examined),the initial biopsy specimen failed to correctly identifyan aggressive component that was subsequentlyfound in the corresponding excision, possibly reflect-ing partial sampling. Among the discordant cases,19% (8/42) of these cases were classified as infiltrativesubtype in the biopsy specimen; however, no infil-trative tumor was seen in the final excision (Fig 1, Eand F ). The biopsy specimen typically showed nod-ular BCC with surface ulceration, inflammation, andreactive stromal changes, which could have posed asdiagnostic pitfalls and could have been misinter-preted as infiltrative BCC. Of note, all the 8 misclassi-fied cases were shave biopsy specimens of ulceratedlesions. In contrast, there was no misclassified infil-trative subtype in the punch biopsy specimens.
DISCUSSIONOur studies showed that BCC with mixed histo-
logic subtypes was the most common variant con-sisting of 54% of the total cases examined.Importantly, half of the mixed subtypes containedan aggressive growth pattern. Other studies havereported a wide range of incidence of mixed sub-types from 11% to 39%.7,12-16 In particular, studies ofMohs excisions of BCC found even a higher inci-dence (43%) of mixed subtypes.8 The high incidenceof mixed subtype BCC in our studies may be a resultof differences in the patient population, tissue sam-pling, and diagnostic criteria. The samples in ourstudy came from dermatology practices at two majoracademic medical institutions where patients mayhave presented with more advanced lesions andwould have a higher likelihood of having an aggres-sive component. Superficial sampling could poten-tially miss a component present deeper in the dermisin a mixed subtype BCC. Furthermore, pathologistsmay use different criteria to diagnose an infiltrative

Table II. Correlation of basal cell carcinoma subtypes in biopsy specimen and excision
Subtype in biopsy specimen (N) Composite BCC subtypes (N) Concordance Discordance
Single subtypeSuperficial (31) Superficial (28) 90% (28/31)
Superficial 1 nodular (2)Mixed with aggressive subtype (1)
10% (3/31)
Nodular (92) Nodular (63) 68% (63/92)Nodular 1 superficial (15)Mixed with aggressive subtype* (14)
32% (29/92)
Aggressive subtype (10)Micronodular (2) Micronodular (2)
Morpheaform (1)Infiltrative (6)
Morpheaform (1) 90% (9/10)Infiltrative (7)
Superficial 1 nodular (1) 10% (1/10)Mixed subtypesSuperficial 1 nodular (46) Superficial 1 nodular (44) 96% (44/46)
Mixed with aggressive subtype* (2) 4% (2/46)Mixed with aggressive subtype (53) Mixed with aggressive subtype* (46) 87% (46/53)
Nodular (7) 13% (7/53)Total 82% (190/232) 18% (42/232)
BCC, Basal cell carcinoma; N, number of cases.
*Tumor consisting of more than one subtype, of which at least one is an aggressive subtype.
J AM ACAD DERMATOL
VOLUME 66, NUMBER 1Haws et al 109
or micronodular pattern, some requiring that thesepatterns occupy most of the tumor to make suchdiagnoses, whereas others report only the predom-inant subtype seen in the tissue specimen. BecauseMohsmicrographic surgery is typically performed onmore aggressive lesions, Mohs cases were not in-cluded in our study to avoid skewing the samplepopulation in the study, which primarily examinedbiopsy samples from general dermatology clinics.
To date, only a few studies have examined theaccuracy of biopsy in diagnosing the true histologicsubtype of BCC, which is important in predicting thetumor’s clinical behavior. We found an accuracy rateof 82% in the biopsy diagnosis. These findings areconsistent with previous studies in which the accur-acy rates for shave and punch biopsy specimenswere 80%.9 However, studies of Mohs resectionspecimens reported much lower accuracy rates inthe biopsy specimen. One study reported only 10%accuracy rate, which was attributed mainly to lack ofspecification of BCC subtypes in the pathologyreport (ie, either no subtype or only a single subtypewas reported).8 A more recent study showed a 51.1%accuracy rate between biopsy specimen and intra-operative examination of nonmelanoma skin can-cers (BCC and squamous cell carcinoma).10
A major and clinically important finding in ourstudy is an overall 18% discordance rate betweentumor subtype identification in the biopsy specimenand the composite BCC subtype. Sampling errorsinherent in a small biopsy specimen of a large tumorwould in part account for the observed discrepancy.
Importantly, 40% of the discordant cases (7% of thetotal cases examined) were found to have an aggres-sive subtype that was not identified in the initialbiopsy specimen. Nodular subtype was found tohave the highest discrepancy (32%) between biopsyspecimen and excision, in which the initial biopsyspecimen showed nodular BCC but failed to detectthe other components of the tumor. The intrinsicgrowth patterns of the subtypes involved may affecttumor sampling. For example, superficial subtypehas a broad peripheral growth pattern with multiplenests of tumor cells; some arewidely separated nests.Likewise, aggressive subtypes are infiltrative andoften grow in the deep portion of the tumor.Hence, small biopsy specimens centered topograph-ically on the central nodular componentmaymiss theperipherally extending superficial or deeper infiltra-tive component. Similar failure to detect aggressivetumor subtypes has also been reported in Mohsexcision specimens where 21.1% of the cases exam-ined intraoperatively revealed an aggressive subtypethat was not diagnosed by biopsy specimen.10
Another notable finding is that 19% of the discor-dant cases weremisidentified as infiltrative BCC in thebiopsy specimen as a result of surface ulceration andreactive stromal changes. In these cases, we observedthat the biopsy specimen showed nodular BCC withulceration and stromal reaction that could have al-tered tumor morphology and mimicked an infiltrativegrowth pattern. This type of misidentification oc-curred in shave biopsy specimens in which only asuperficial portion of the tumor was sampled, and
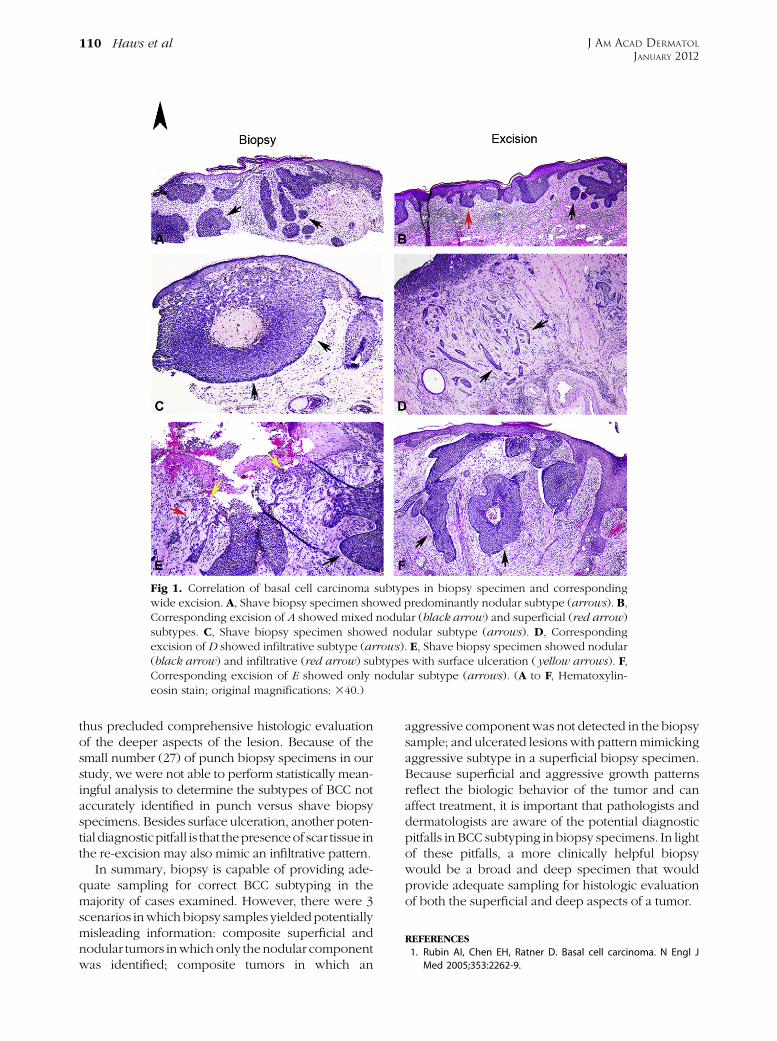
Fig 1. Correlation of basal cell carcinoma subtypes in biopsy specimen and correspondingwide excision. A, Shave biopsy specimen showed predominantly nodular subtype (arrows). B,Corresponding excision of A showed mixed nodular (black arrow) and superficial (red arrow)subtypes. C, Shave biopsy specimen showed nodular subtype (arrows). D, Correspondingexcision of D showed infiltrative subtype (arrows). E, Shave biopsy specimen showed nodular(black arrow) and infiltrative (red arrow) subtypes with surface ulceration ( yellow arrows). F,Corresponding excision of E showed only nodular subtype (arrows). (A to F, Hematoxylin-eosin stain; original magnifications: 340.)
J AM ACAD DERMATOL
JANUARY 2012110 Haws et al
thus precluded comprehensive histologic evaluationof the deeper aspects of the lesion. Because of thesmall number (27) of punch biopsy specimens in ourstudy, we were not able to perform statistically mean-ingful analysis to determine the subtypes of BCC notaccurately identified in punch versus shave biopsyspecimens. Besides surface ulceration, another poten-tial diagnosticpitfall is that thepresenceof scar tissue inthe re-excision may also mimic an infiltrative pattern.
In summary, biopsy is capable of providing ade-quate sampling for correct BCC subtyping in themajority of cases examined. However, there were 3scenarios inwhich biopsy samples yieldedpotentiallymisleading information: composite superficial andnodular tumors inwhich only thenodular componentwas identified; composite tumors in which an
aggressive componentwas not detected in the biopsysample; and ulcerated lesionswith patternmimickingaggressive subtype in a superficial biopsy specimen.Because superficial and aggressive growth patternsreflect the biologic behavior of the tumor and canaffect treatment, it is important that pathologists anddermatologists are aware of the potential diagnosticpitfalls in BCC subtyping in biopsy specimens. In lightof these pitfalls, a more clinically helpful biopsywould be a broad and deep specimen that wouldprovide adequate sampling for histologic evaluationof both the superficial and deep aspects of a tumor.
REFERENCES
1. Rubin AI, Chen EH, Ratner D. Basal cell carcinoma. N Engl J
Med 2005;353:2262-9.

J AM ACAD DERMATOL
VOLUME 66, NUMBER 1Haws et al 111
2. Miller SJ. Biology of basal cell carcinoma (part I). J Am Acad
Dermatol 1991;24:1-13.
3. Snow SN, Sahl W, Lo JS, Mohs FE, Warner T, Dekkinga JA, et al.
Metastatic basal cell carcinoma: report of five cases. Cancer
1994;73:328-35.
4. Crowson AN. Basal cell carcinoma: biology, morphology
and clinical implications. Mod Pathol 2006;19(Suppl):
S127-47.
5. Dixon AY, Lee SH, McGregor DH. Histologic features predictive
of basal cell carcinoma recurrence: results of a multivariate
analysis. J Cutan Pathol 1993;20:137-42.
6. Mosterd K, Arits AH, Thissen MR, Kelleners-Smeets NW.
Histology-based treatment of basal cell carcinoma. Acta
Derm Venereol 2009;89:454-8.
7. Sexton M, Jones DB, Maloney ME. Histologic pattern analysis
of basal cell carcinoma: study of a series of 1039 consecutive
neoplasms. J Am Acad Dermatol 1990;23:1118-26.
8. Cohen PR, Schulze KE, Nelson BR. Basal cell carcinoma with
mixed histology: a possible pathogenesis for recurrent skin
cancer. Dermatol Surg 2006;32:542-51.
9. Russell EB, Carrington PR, Smoller BR. Basal cell carcinoma: a
comparison of shave biopsy versus punch biopsy
techniques in subtype diagnosis. J Am Acad Dermatol
1999;41:69-71.
10. Izikson L, Seyler M, Zeitouni NC. Prevalence of underdiag-
nosed aggressive non-melanoma skin cancers treated with
Mohs micrographic surgery: analysis of 513 cases. Dermatol
Surg 2010;36:1769-72.
11. Rippey JJ. Why classify basal cell carcinomas? Histopathology
1998;32:393-8.
12. Freeman RG, Duncan C. Recurrent skin cancer. Arch Dermatol
1973;107:395-9.
13. Sloane JP. The value of typingbasal cell carcinomas inpredicting
recurrence after surgical excision. Br J Dermatol 1977;96:127-32.
14. Lang PG Jr, Maize JC. Histologic evolution of recurrent basal
cell carcinoma and treatment implications. J Am Acad
Dermatol 1986;14:186-96.
15. Swetter SM, Yaghmai D, Egbert BM. Infiltrative basal cell
carcinoma occurring in sites of biopsy-proven nodular basal
cell carcinoma. J Cutan Pathol 1998;25:420-5.
16. Wrone DA, Swetter SM, Egbert BM, Smoller BR, Khavari PA.
Increased proportion of aggressive-growth basal cell carci-
noma in the Veterans Affairs population of Palo Alto,
California. J Am Acad Dermatol 1996;35:907-10.




















