
Is sentinel lymph node biopsy indicated in patients with a ...
10
Review Is sentinel lymph node biopsy indicated in patients with a diagnosis of ductal carcinoma in situ? A systematic literature review and meta-analysis Hiba El Hage Chehade, M.D., M.R.C.S.*, Hannah Headon, M.B.B.S., B.Sc., Umar Wazir, M.B.B.S., M.R.C.S., M.Sc., Houssam Abtar, M.D., Abdul Kasem, M.D., F.R.C.S., Kefah Mokbel, M.S., F.R.C.S. The London Breast Institute, Princess Grace Hospital, 42-52 Nottingham Place, London W1U 5NY, UK KEYWORDS: Sentinel lymph node biopsy; Ductal carcinoma in situ; Breast cancer Abstract BACKGROUND: Recent discussion has suggested that some cases of ductal carcinoma in situ (DCIS) with high risk of invasive disease may require sentinel lymph node biopsy (SLNB). METHODS: Systematic literature review identified 48 studies (9,803 DCIS patients who underwent SLNB). Separate analyses for patients diagnosed preoperatively by core sampling and patients diagnosed postoperatively by specimen pathology were conducted to determine the percentage of patients with axillary nodal involvement. Patient factors were analyzed for associations with risk of nodal involvement. RESULTS: The mean percentage of positive SLNBs was higher in the preoperative group (5.95% vs 3.02%; P 5 .0201). Meta-regression analysis showed a direct association with tumor size (P 5 .0333) and grade (P 5 .00839) but not median age nor tumor upstage rate. CONCLUSIONS: The SLNB should be routinely considered in patients with large (.2 cm) high- grade DCIS after a careful multidisciplinary discussion. In the context of breast conserving surgery, the SLNB is not routinely indicated for low- and intermediate-grade DCIS, high-grade DCIS smaller than 2 cm, or pure DCIS diagnosed by definitive surgical excision. Crown Copyright Ó 2016 Published by Elsevier Inc. All rights reserved. Ductal carcinoma in situ (DCIS) is the predominant noninvasive breast neoplasia in the United Kingdom, comprising 83% of all in situ breast cancers diagnosed. 1 At present, the treatment of DCIS comprises wide local excision or mastectomy to achieve local control of the dis- ease. In patients treated with breast conserving surgery, radiotherapy may be considered to reduce the risk of local recurrence. In breast cancer, the status of the regional lymph nodes has been found to be the most important prognostic factor and predictor of survival and therefore has important implica- tions for future treatment decisions. 2 As DCIS is noninvasive by definition, this implies that there should be no spread to the axillary lymph nodes. Subsequently, omission of axillary dissection is now the standard of treatment since previous This review was funded by grants from the Breast Cancer Hope Foun- dation (London, UK). The authors declare no conflicts of interest. * Corresponding author. Tel.: 144 207 908 2101; fax: 144 207 908 2275. E-mail address: [email protected] Manuscript received February 24, 2016; revised manuscript April 19, 2016 0002-9610/$ - see front matter Crown Copyright Ó 2016 Published by Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.amjsurg.2016.04.019 The American Journal of Surgery (2017) 213, 171-180
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Is sentinel lymph node biopsy indicated in patients with a ...

The American Journal of Surgery (2017) 213, 171-180
Review
Is sentinel lymph node biopsy indicated inpatients with a diagnosis of ductal carcinomain situ? A systematic literature review andmeta-analysis
Hiba El Hage Chehade, M.D., M.R.C.S.*, Hannah Headon, M.B.B.S., B.Sc.,Umar Wazir, M.B.B.S., M.R.C.S., M.Sc., Houssam Abtar, M.D.,Abdul Kasem, M.D., F.R.C.S., Kefah Mokbel, M.S., F.R.C.S.
The London Breast Institute, Princess Grace Hospital, 42-52
Nottingham Place, London W1U 5NY, UKKEYWORDS:Sentinel lymph nodebiopsy;Ductal carcinoma insitu;Breast cancer
This review was funded by grants fro
dation (London, UK).
The authors declare no conflicts of i
* Corresponding author. Tel.: 144 2
2275.
E-mail address: haj_shehadeh_hiba@
Manuscript received February 24, 20
2016
0002-9610/$ - see front matter Crown
http://dx.doi.org/10.1016/j.amjsurg.20
AbstractBACKGROUND: Recent discussion has suggested that some cases of ductal carcinoma in situ (DCIS)
with high risk of invasive disease may require sentinel lymph node biopsy (SLNB).METHODS: Systematic literature review identified 48 studies (9,803 DCIS patients who underwent
SLNB). Separate analyses for patients diagnosed preoperatively by core sampling and patients diagnosedpostoperatively by specimen pathology were conducted to determine the percentage of patients withaxillary nodal involvement. Patient factors were analyzed for associations with risk of nodal involvement.
RESULTS: The mean percentage of positive SLNBs was higher in the preoperative group (5.95% vs3.02%; P 5 .0201). Meta-regression analysis showed a direct association with tumor size (P 5 .0333)and grade (P 5 .00839) but not median age nor tumor upstage rate.
CONCLUSIONS: The SLNB should be routinely considered in patients with large (.2 cm) high-grade DCIS after a careful multidisciplinary discussion. In the context of breast conserving surgery,the SLNB is not routinely indicated for low- and intermediate-grade DCIS, high-grade DCIS smallerthan 2 cm, or pure DCIS diagnosed by definitive surgical excision.Crown Copyright � 2016 Published by Elsevier Inc. All rights reserved.
Ductal carcinoma in situ (DCIS) is the predominantnoninvasive breast neoplasia in the United Kingdom,comprising 83% of all in situ breast cancers diagnosed.1
m the Breast Cancer Hope Foun-
nterest.
07 908 2101; fax: 144 207 908
hotmail.com
16; revised manuscript April 19,
Copyright � 2016 Published by Elsev
16.04.019
At present, the treatment of DCIS comprises wide localexcision or mastectomy to achieve local control of the dis-ease. In patients treated with breast conserving surgery,radiotherapy may be considered to reduce the risk of localrecurrence.
In breast cancer, the status of the regional lymph nodes hasbeen found to be the most important prognostic factor andpredictor of survival and therefore has important implica-tions for future treatment decisions.2 As DCIS is noninvasiveby definition, this implies that there should be no spread to theaxillary lymph nodes. Subsequently, omission of axillarydissection is now the standard of treatment since previous
ier Inc. All rights reserved.
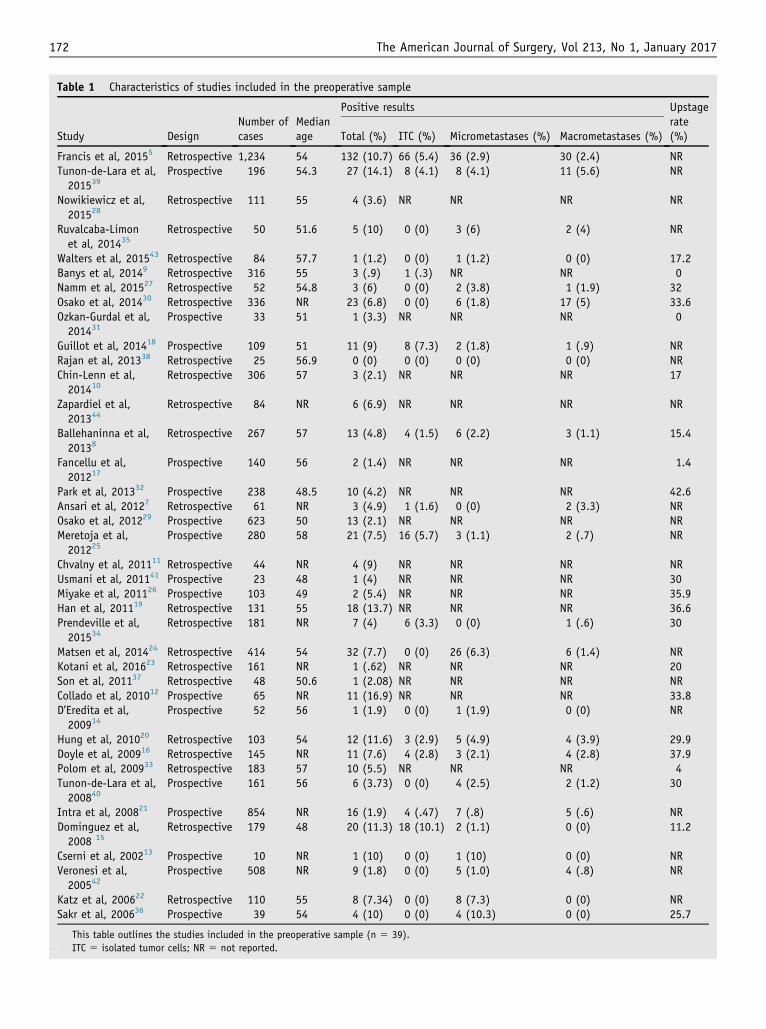
Table 1 Characteristics of studies included in the preoperative sample
Study DesignNumber ofcases
Medianage
Positive results Upstagerate(%)Total (%) ITC (%) Micrometastases (%) Macrometastases (%)
Francis et al, 20155 Retrospective 1,234 54 132 (10.7) 66 (5.4) 36 (2.9) 30 (2.4) NRTunon-de-Lara et al,201539
Prospective 196 54.3 27 (14.1) 8 (4.1) 8 (4.1) 11 (5.6) NR
Nowikiewicz et al,201528
Retrospective 111 55 4 (3.6) NR NR NR NR
Ruvalcaba-Limonet al, 201435
Retrospective 50 51.6 5 (10) 0 (0) 3 (6) 2 (4) NR
Walters et al, 201543 Retrospective 84 57.7 1 (1.2) 0 (0) 1 (1.2) 0 (0) 17.2Banys et al, 20149 Retrospective 316 55 3 (.9) 1 (.3) NR NR 0Namm et al, 201527 Retrospective 52 54.8 3 (6) 0 (0) 2 (3.8) 1 (1.9) 32Osako et al, 201430 Retrospective 336 NR 23 (6.8) 0 (0) 6 (1.8) 17 (5) 33.6Ozkan-Gurdal et al,201431
Prospective 33 51 1 (3.3) NR NR NR 0
Guillot et al, 201418 Prospective 109 51 11 (9) 8 (7.3) 2 (1.8) 1 (.9) NRRajan et al, 201338 Retrospective 25 56.9 0 (0) 0 (0) 0 (0) 0 (0) NRChin-Lenn et al,201410
Retrospective 306 57 3 (2.1) NR NR NR 17
Zapardiel et al,201344
Retrospective 84 NR 6 (6.9) NR NR NR NR
Ballehaninna et al,20138
Retrospective 267 57 13 (4.8) 4 (1.5) 6 (2.2) 3 (1.1) 15.4
Fancellu et al,201217
Prospective 140 56 2 (1.4) NR NR NR 1.4
Park et al, 201332 Prospective 238 48.5 10 (4.2) NR NR NR 42.6Ansari et al, 20127 Retrospective 61 NR 3 (4.9) 1 (1.6) 0 (0) 2 (3.3) NROsako et al, 201229 Prospective 623 50 13 (2.1) NR NR NR NRMeretoja et al,201225
Prospective 280 58 21 (7.5) 16 (5.7) 3 (1.1) 2 (.7) NR
Chvalny et al, 201111 Retrospective 44 NR 4 (9) NR NR NR NRUsmani et al, 201141 Prospective 23 48 1 (4) NR NR NR 30Miyake et al, 201126 Prospective 103 49 2 (5.4) NR NR NR 35.9Han et al, 201119 Retrospective 131 55 18 (13.7) NR NR NR 36.6Prendeville et al,201534
Retrospective 181 NR 7 (4) 6 (3.3) 0 (0) 1 (.6) 30
Matsen et al, 201424 Retrospective 414 54 32 (7.7) 0 (0) 26 (6.3) 6 (1.4) NRKotani et al, 201623 Retrospective 161 NR 1 (.62) NR NR NR 20Son et al, 201137 Retrospective 48 50.6 1 (2.08) NR NR NR NRCollado et al, 201012 Prospective 65 NR 11 (16.9) NR NR NR 33.8D’Eredita et al,200914
Prospective 52 56 1 (1.9) 0 (0) 1 (1.9) 0 (0) NR
Hung et al, 201020 Retrospective 103 54 12 (11.6) 3 (2.9) 5 (4.9) 4 (3.9) 29.9Doyle et al, 200916 Retrospective 145 NR 11 (7.6) 4 (2.8) 3 (2.1) 4 (2.8) 37.9Polom et al, 200933 Retrospective 183 57 10 (5.5) NR NR NR 4Tunon-de-Lara et al,200840
Prospective 161 56 6 (3.73) 0 (0) 4 (2.5) 2 (1.2) 30
Intra et al, 200821 Prospective 854 NR 16 (1.9) 4 (.47) 7 (.8) 5 (.6) NRDominguez et al,2008 15
Retrospective 179 48 20 (11.3) 18 (10.1) 2 (1.1) 0 (0) 11.2
Cserni et al, 200213 Prospective 10 NR 1 (10) 0 (0) 1 (10) 0 (0) NRVeronesi et al,200542
Prospective 508 NR 9 (1.8) 0 (0) 5 (1.0) 4 (.8) NR
Katz et al, 200622 Retrospective 110 55 8 (7.34) 0 (0) 8 (7.3) 0 (0) NRSakr et al, 200636 Prospective 39 54 4 (10) 0 (0) 4 (10.3) 0 (0) 25.7
This table outlines the studies included in the preoperative sample (n 5 39).
ITC 5 isolated tumor cells; NR 5 not reported.
172 The American Journal of Surgery, Vol 213, No 1, January 2017
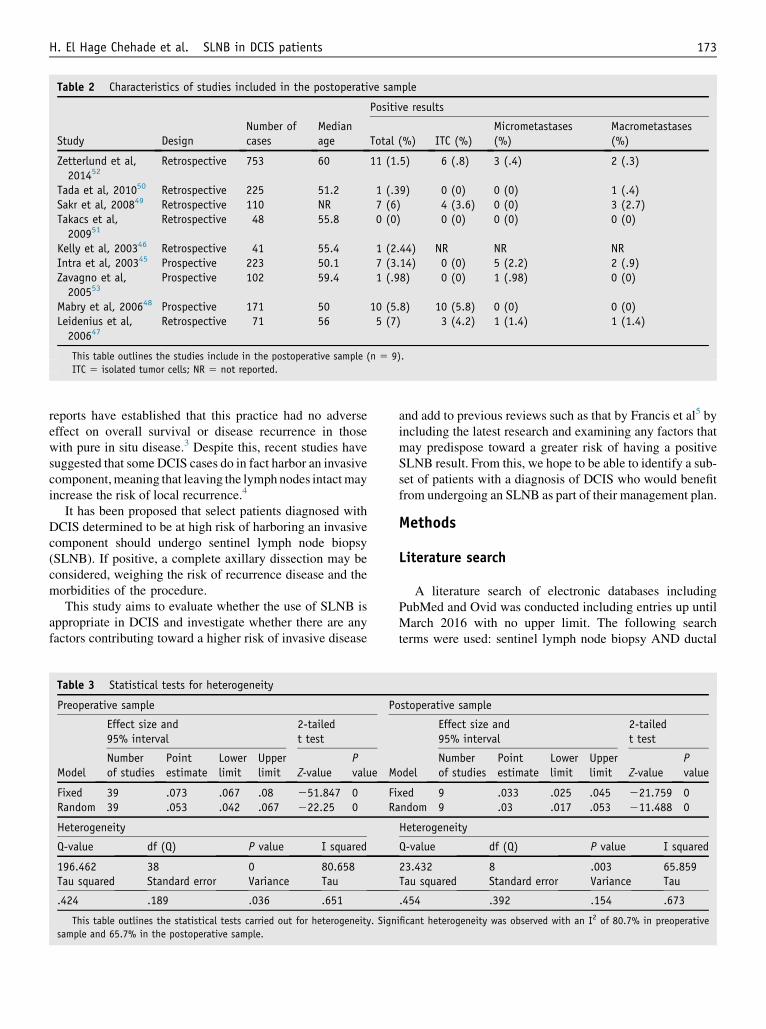
Table 2 Characteristics of studies included in the postoperative sample
Study DesignNumber ofcases
Medianage
Positive results
Total (%) ITC (%)Micrometastases(%)
Macrometastases(%)
Zetterlund et al,201452
Retrospective 753 60 11 (1.5) 6 (.8) 3 (.4) 2 (.3)
Tada et al, 201050 Retrospective 225 51.2 1 (.39) 0 (0) 0 (0) 1 (.4)Sakr et al, 200849 Retrospective 110 NR 7 (6) 4 (3.6) 0 (0) 3 (2.7)Takacs et al,200951
Retrospective 48 55.8 0 (0) 0 (0) 0 (0) 0 (0)
Kelly et al, 200346 Retrospective 41 55.4 1 (2.44) NR NR NRIntra et al, 200345 Prospective 223 50.1 7 (3.14) 0 (0) 5 (2.2) 2 (.9)Zavagno et al,200553
Prospective 102 59.4 1 (.98) 0 (0) 1 (.98) 0 (0)
Mabry et al, 200648 Prospective 171 50 10 (5.8) 10 (5.8) 0 (0) 0 (0)Leidenius et al,200647
Retrospective 71 56 5 (7) 3 (4.2) 1 (1.4) 1 (1.4)
This table outlines the studies include in the postoperative sample (n 5 9).
ITC 5 isolated tumor cells; NR 5 not reported.
H. El Hage Chehade et al. SLNB in DCIS patients 173
reports have established that this practice had no adverseeffect on overall survival or disease recurrence in thosewith pure in situ disease.3 Despite this, recent studies havesuggested that some DCIS cases do in fact harbor an invasivecomponent,meaning that leaving the lymph nodes intactmayincrease the risk of local recurrence.4
It has been proposed that select patients diagnosed withDCIS determined to be at high risk of harboring an invasivecomponent should undergo sentinel lymph node biopsy(SLNB). If positive, a complete axillary dissection may beconsidered, weighing the risk of recurrence disease and themorbidities of the procedure.
This study aims to evaluate whether the use of SLNB isappropriate in DCIS and investigate whether there are anyfactors contributing toward a higher risk of invasive disease
Table 3 Statistical tests for heterogeneity
Preoperative sample Po
Model
Effect size and95% interval
2-tailedt test
MNumberof studies
Pointestimate
Lowerlimit
Upperlimit Z-value
Pvalue
Fixed 39 .073 .067 .08 251.847 0 FiRandom 39 .053 .042 .067 222.25 0 Ra
Heterogeneity
Q-value df (Q) P value I squared
196.462 38 0 80.658Tau squared Standard error Variance Tau
.424 .189 .036 .651
This table outlines the statistical tests carried out for heterogeneity. Sign
sample and 65.7% in the postoperative sample.
and add to previous reviews such as that by Francis et al5 byincluding the latest research and examining any factors thatmay predispose toward a greater risk of having a positiveSLNB result. From this, we hope to be able to identify a sub-set of patients with a diagnosis of DCIS who would benefitfrom undergoing an SLNB as part of their management plan.
Methods
Literature search
A literature search of electronic databases includingPubMed and Ovid was conducted including entries up untilMarch 2016 with no upper limit. The following searchterms were used: sentinel lymph node biopsy AND ductal
stoperative sample
odel
Effect size and95% interval
2-tailedt test
Numberof studies
Pointestimate
Lowerlimit
Upperlimit Z-value
Pvalue
xed 9 .033 .025 .045 221.759 0ndom 9 .03 .017 .053 211.488 0
Heterogeneity
Q-value df (Q) P value I squared
23.432 8 .003 65.859Tau squared Standard error Variance Tau
.454 .392 .154 .673
ificant heterogeneity was observed with an I2 of 80.7% in preoperative
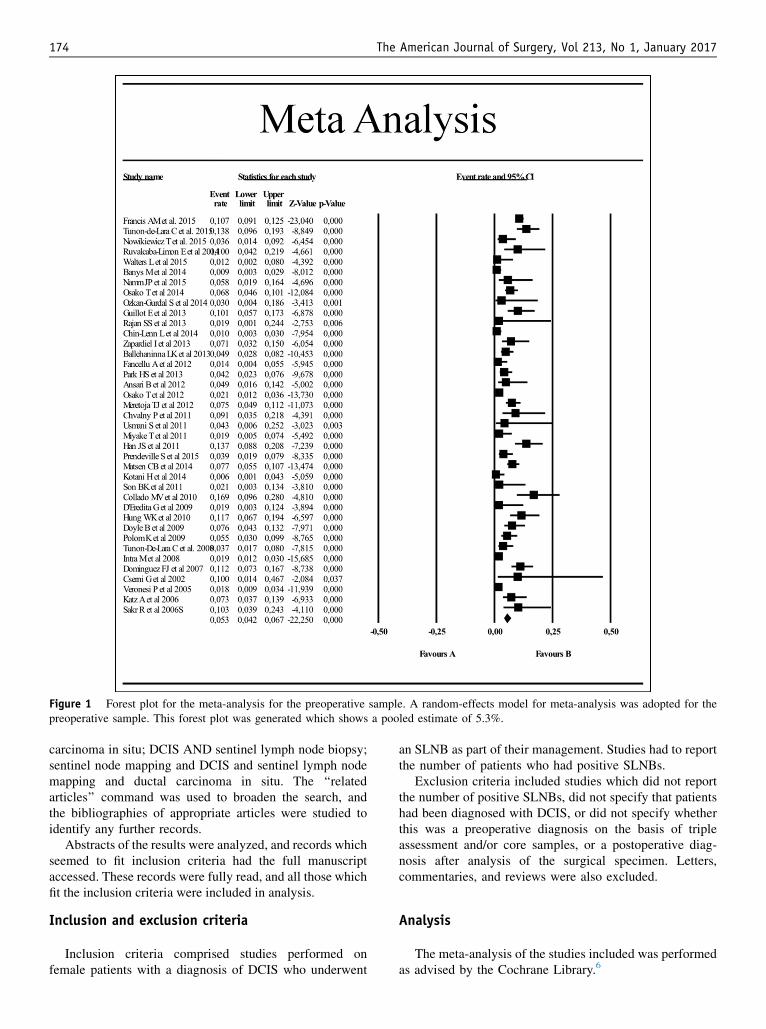
Figure 1 Forest plot for the meta-analysis for the preoperative sample. A random-effects model for meta-analysis was adopted for thepreoperative sample. This forest plot was generated which shows a pooled estimate of 5.3%.
174 The American Journal of Surgery, Vol 213, No 1, January 2017
carcinoma in situ; DCIS AND sentinel lymph node biopsy;sentinel node mapping and DCIS and sentinel lymph nodemapping and ductal carcinoma in situ. The ‘‘relatedarticles’’ command was used to broaden the search, andthe bibliographies of appropriate articles were studied toidentify any further records.
Abstracts of the results were analyzed, and records whichseemed to fit inclusion criteria had the full manuscriptaccessed. These records were fully read, and all those whichfit the inclusion criteria were included in analysis.
Inclusion and exclusion criteria
Inclusion criteria comprised studies performed onfemale patients with a diagnosis of DCIS who underwent
an SLNB as part of their management. Studies had to reportthe number of patients who had positive SLNBs.
Exclusion criteria included studies which did not reportthe number of positive SLNBs, did not specify that patientshad been diagnosed with DCIS, or did not specify whetherthis was a preoperative diagnosis on the basis of tripleassessment and/or core samples, or a postoperative diag-nosis after analysis of the surgical specimen. Letters,commentaries, and reviews were also excluded.
Analysis
The meta-analysis of the studies included was performedas advised by the Cochrane Library.6

Figure 2 Forest plot for the meta-analysis in the postoperative sample. A random-effects model for the meta-analysis was adopted for thepostoperative sample. This forest plot was generated showing a pooled estimate of 3.5%.
H. El Hage Chehade et al. SLNB in DCIS patients 175
Some studies assessed the SLNB-positive rate in defin-itive DCIS, ie, those with a postoperative diagnosis ofDCIS, whereas others reported this as a function of thosewith a preoperative diagnosis of DCIS. We, therefore,performed separate analyses in these groups as thefrequency of a positive SLNB may differ between the 2.
Data on the number of patients, the SLNB technique, thenumber of patients with positive SLNBs, the median age,and the biopsy method were collected, tabulated, andsubsequently analyzed.
An analysis of variance analysis was conducted to lookfor any significant difference in the mean percentage of
Figure 3 A funnel plot from the preoperative sample. A funnel plot wpublication bias. As not all the points are within the prescribed margin
positive SLNBs between preoperative and postoperativediagnoses. To carry out the meta-analysis, we separatedthe included studies depending on whether the diagnosisof DCIS was given preoperatively or postoperatively andthen conducted 2 separate meta-analyses. Pooled estimateswere calculated with 95% confidence intervals. Cochran’sQ test was used to test the null hypothesis, and heteroge-neity was calculated using an I2 index. For both groups, afunnel plot was created to look for publication bias, andboth the Begg and Mazumdar Rank Correlation test andEgger’s test of the intercept were performed to supportthis. Duval and Tweedie’s trim and fill method was used
as generated for the preoperative sample to look for evidence ofs, there is evidence of publication bias in this sample.

Figure 4 A funnel plot from the postoperative sample. A funnel plot was generated for the postoperative sample to look for evidence ofpublication bias. Again, there is some evidence of publication bias.
176 The American Journal of Surgery, Vol 213, No 1, January 2017
to look for differences between observed and adjustedpooled rates.
In addition, a meta-regression analysis was carried out toidentify factors associated with a higher risk of having apositive SLNB result. Statistical significance was consid-ered at P , .05.
Table 4 Statistical tests for publication bias
TestTestresult Preoperative
Classic fail-safeN (per study)
N 581
Begg andMazumdar rankcorrelation test
Tau 2.217z-value for tau 1.948P value (1 tailed) .026P value (2 tailed) .051
Egger’s Test ofthe intercept
Intercept 22.13995% CI lower limit(2 tailed)
23.288
95% CI upper limit(2 tailed)
2.990
P value (1 tailed) .000P value (2 tailed) .001
Duval andTweedie’s Trimand Fill
Observed pooled effect .053Adjusted pooled effect .073Studies trimmed 11.000Missing values To right of
mean
This table outlines the statistical tests carried out to assess for
evidence of publication bias in the preoperative sample. The results are
suggestive of publication bias, resulting in an adjusted pooled
estimate of 7.3%.
Results
Forty-eight articles were identified and analyzedyielding a total of 9,803 patients. This included bothretrospective and prospective studies.
The primary endpoint was the percentage of DCISpatients with positive SLNBs. Studies were divided basedon the time of diagnosis of DCIS (ie, preoperative vspostoperative diagnosis). Characteristics of the includedstudies are shown in Tables 1 and 2. The incidence ofSLNB positivity was significantly higher in the preopera-tive diagnosis group (n 5 39 studies),5,7–44 with a meanof 5.95% (range 5 0% to 16.9%) vs a mean of 3.02%(range 5 0% to 7%) in the postoperative diagnosis group(n 5 9 studies)45–53 (P 5 .0201). Further analysis showedthat axillary nodal metastasis harbored isolated tumor cells(ITCs), micrometastasis, and macrometastasis in 24.4%(median 12.5%), 48.5% (median 43.8%), and 23.1% (me-dian 22.7%), respectively in the preoperative diagnosisstudies, vs 33.95% (median 27.3%), 27.3 (median 10%),and 26.2% (median 19.1%) in the postoperative diagnosisgroup. However, not all studies reported the incidence ofITCs; therefore, this should be interpreted with caution.
In the meta-analysis, significant heterogeneity wasobserved between the studies with an I2 statistic of 80.7%and 65.7% in the preoperative and postoperative groups,respectively (Table 3). Thus, a random-effects model wasadopted, and pooled estimate of positive SLNB of 5.3%and 3.0% were reported in the preoperative and postopera-tive diagnosis, respectively (Figs. 1 and 2). A funnel plotwas subsequently created which showed evidence of publi-cation bias in both groups (Figs. 3 and 4) supported byBegg and Mazumdar rank correlation test and Egger’s

Table 5 Statistical tests for publication bias
Test Test result Postoperative
Classic fail-safeN (per study)
N 105
Begg andMazumdar rankcorrelation test
Tau 2.167z-value for tau .626P value (1 tailed) .266P value (2 tailed) .532
Egger’s Test ofthe intercept
Intercept 21.19195% CI lower limit(2 tailed)
24.266
95% CI upper limit(2 tailed)
1.884
P value (1 tailed) .195P value (2 tailed) .390
Duval andTweedie’s Trimand Fill
Observed pooled effect .030Adjusted pooled effect .037Studies trimmed 2.000Missing values To right of
mean
This table outlines the statistical tests carried out to assess for
evidence of publication bias in the postoperative sample. The results
are suggestive of publication bias, resulting in an adjusted pooled
estimate of 3.7%.
CI 5 confidence interval.
H. El Hage Chehade et al. SLNB in DCIS patients 177
test of the intercept. Subsequently, an adjusted estimate wascomputed using Duval and Tweedie’s trim and fill methodwhich was calculated at 7.3% in the preoperative diagnosisstudies and 3.7% in the postoperative diagnosis ones(Tables 4 and 5).
A meta-regression was also performed to determine thevariables associated with SLNB positivity. Neither themedian age nor the upstage rate was associated withincreased likelihood of positive SLNB (P 5 .303 and.1585, respectively). However, larger tumor size and highergrade were significantly associated with SLNB positivity(P 5 .03333 and P 5 .00839, respectively; Table 6).
Comments
With the development and widespread introduction ofhigh-quality digital mammography, DCIS is now consideredthe most rapidly growing subgroup of breast carcinomas
Table 6 Meta-regression
Covariate Coefficient Standard error 95
Tumor grade vs nodal involvementIntercept .00946 .00359High grade % 22.947 23.28096 2
Tumor sizevs nodalinvolvement
Intercept .08947 .04204Tumor size 22.74722 .13064 2
This table outlines the statistical test for meta-regression which was pe
significantly associated with a higher risk of having a positive SLNB result. Si
accounting for 15.7% of all neoplasia detected through theNationa Health Service (NHS) Breast Screening Programmebetween 2003 and 2011.3 There are several points of conten-tion in the management of DCIS, one of which is the use ofSLNB.
Although SLNB has become the standard treatmentoption in clinically node negative invasive breast cancer, itsroutine use in the current management of DCIS is notwarranted and would not be without its risks: the AxillaryLymphatic Mapping Against Nodal Axillary Clearance(ALMANAC) trial demonstrated that 5% of patients un-dergoing SLNB alone developed arm lymphedema.54
Furthermore, an increasing number of immediate hypersen-sitivity reactions have been reported after the use of PatentBlue V for breast cancer surgery with 1 multicenter trialshowing an incidence of .34% in 1,742 patients, 2 casesof which required admission into the intensive careunit.55 A number of case studies also illustrated cases ofanaphylactic reactions.56–59 However, its use has nowlargely been replaced by methylene blue which is safer.60,61
Other potential complications include seromas, hematomas,and arm pain.62,63
Standard preoperative diagnostic techniques are knownto miss areas of small foci of invasive disease due tosampling and slicing.64 This is acknowledged by the mostrecent guidelines published by the American Society ofClinical Oncology which state that SLNB should be per-formed for DCIS in 2 circumstances: First, in patients un-dergoing mastectomy, as it would technically infeasible toperform an SLNB in the aftermath. Second, as a second-stage SLNB if an invasive component was found on the his-tological analysis of the tumor after breast conservingsurgery.65 However, it is unclear whether there is a rolefor a routine SLNB in DCIS patients undergoing breastconserving surgery.
This meta-analysis has demonstrated a significantlyhigher SLNB positivity in patients with preoperativediagnosis of DCIS than in those with postoperativediagnosis with a reported mean of 5.95% and 3.02%,respectively (P 5 .0201). Especially if the cases with ITCare omitted, the final number of clinically relevant positivenodes is too low to justify the routine use of SLNB in allcases of DCIS. However, identification of factors predictiveof a positive SLNB in the setting of DCIS would be of
% lower 95% upper Z-value P value
.00243 .01649 2.63608 .008393.28096 22.61303 217.29528 0
.00707 .17187 2.12813 .033333.00328 22.49116 221.0284 0
rformed to investigate whether high tumor grade and tumor size was
gnificance was assumed when P , .05 (bold).

178 The American Journal of Surgery, Vol 213, No 1, January 2017
clinical utility. Our meta-analysis has established a signifi-cant association between SLNB positivity and high tumorgrade and large tumor size but not with age at diagnosisnor the upstage rate.
Our finding of positive association between high tumorgrade and positive SLNB in DCIS patients is consistent withfindings in other studies where high-grade disease has beenearmarked as an independent risk factor for clinically occultinvasion.66,67 Boler et al67 reported that patients with high-grade disease were more likely to undergo SLNB althoughother studies failed to demonstrate a correlation betweenthe likelihood of SLN metastases and high tumor grade.22
Likewise, our finding of increased possibility of SLNBpositivity in larger tumors is similar to previous reports.Kondoet al68 observed that tumors larger than 2 cmwere significantlyassociated with upstaging a previous DCIS tumor to invasivedisease. Furthermore, an audit from the UK NHS BreastScreening Programme has suggested that axillary surgery inthe setting of preoperatively diagnosed DCIS was associatedwith larger tumor size.3 Similarly, Chin-Lenn et al10 observedthat in cases where DCIS was diagnosed preoperatively, hav-ing a larger tumor was associated with undergoing a SLNB.This is likely being done in conjunction with a mastectomyperformed in cases where extensive DCIS has made breast-conserving surgery infeasible.
Our analysis did not find an association of positive SLNBwith clinically occult invasion. This is in contrast to severalstudies included in our analysis.5,25,26 Indeed, it stands toreason that patients with large areas of high-grade DCISare more likely to harbor areas of clinically occult microin-vasion, which should account for the increased rate of posi-tive SLNB. Previous studies have found associationsbetween features of high-grade DCIS, such as opacity onmammogram and palpable tumors, and subsequent detectionof invasion.18,42,43 Unfortunately, not all studies included inour meta-analysis reported on upstage rate after a preopera-tive diagnosis of DCIS. Of those that did, the mean upstagerate reported was 23.2% (range 0% to 42.6%).5,9–11,13,16,17,19,20,23,26,27,30,32,33,36,39,41,43 This equated to 714of 3,246 cases (22%) in studies reporting upstage rate. Hope-fully, explicit reporting of the upstage rate in future studieswould resolve this anomaly. Alternatively, it is possiblethat portion of the positive SLNBs may be due to other fac-tors, such as seeding core biopsies, or mechanical displace-ment, and therefore may not be of great clinical import.69,70
Furthermore, we did not observe a significant correlationbetween age at diagnosis and the risk of SLNB positivity inthe present study. However, Yen et al71 reported that an ageof less than 55 years was an independent factor forharboring invasive disease and suggested that youngerpatients with DCIS should be considered for SLNB. Like-wise, Shah et al72 observed that women with DCIS olderthan 56 years were less likely to undergo SLNB.
This study is not without limitations. Our meta-analysisdid not examine the type of the metastasis (ie, ITC vsmicrometastasis vs macrometastasis) due to the absence ofthis information in many of the included studies. ITCs are
defined as deposits less than .2 mm or less than 200 cellsand have been reported with increasing frequency sincethe introduction of immunohistochemistry. It is notcurrently considered an indication for further treatmentof the axilla.65,73 Micrometastases are defined as depositsbetween .2 and 2 mm and have been found to be associ-ated with a poorer prognosis than negative SLNB. Man-agement should be performed after multidisciplinarydiscussion to identify those patients who have a highrisk of harboring lymphatic spread since axillary lymphnode dissection may be safely omitted.74 ITCs accountedfor a large portion of our data and as the presence of ITCswould not likely change treatment or disease outcomes, abetter reporting of the proportion of cases with ITCswould have provide more clarity regarding the clinicalimplications of a positive SLNB.
Furthermore, the extent of the histological analysis (ie,the number of sections, the technique of specimen slicing,and the use of IHC) of either the core biopsy or thedefinitive histology is likely to be heterogeneous among thestudies; nevertheless, the available data did not allow us toexamine these potentially significant parameters.
Similarly, clinical palpability of the tumor19,38 and re-ceptor status39,68 have been cited as predictors of axillaryinvolvement. However, the lack of data precluded their in-clusion in this study.
Finally, the current data did not permit the study of theassociation between the type of core biopsy (ie, standardcore-needle biopsy [CNB] vs vacuum-assisted biopsy[VAB]) and the incidence of sentinel lymph node metastasis.However, the included studies failed to specify the pre-operative biopsy modality (ie, conventional CNB or VAB).This is a significant limitation since VAB has a greateraccuracy than CNB in identifying invasive disease.75 Kotaniet al23 reported a positive SLNB rate of .6% in 199 DCIS pa-tients who were diagnosed with preoperative stereotacticVAB although 20% of these patients were upstaged on finalpathology. Hence, they recommended avoiding SLNB in thissubgroup of DCIS patients. In contrast, Meijnen et al76
emphasized the importance of SLNB in CNB-diagnosedDCIS patients as they have reported an upstage of 26.2%and SLNB positivity of 12.08%. Similarly, Omranipouret al77 suggested that SLNB should be indicated wheneverthe diagnosis of DCIS is based on CNB.
Moreover, questions arise regarding the optimal manage-ment of patients with positive SLNB results who have apreoperative diagnosis of DCIS: the significance of positivefindings remains unclear. In our study, the most commonfinding was either ITCs or micrometastases. The AmericanSociety of Clinical Oncology guidelines indicate that clini-cians should not recommend axillary lymph node dissectionwith early breast cancer patients who have 1 or 2 sentinellymph node metastases and receive breast conserving therapyand radiotherapy.64 Although SLNB would be inappropriatein most cases of DCIS, the selected use of SLNB in thecase of extensive high-grade DCIS could be considered aftera thorough discussion within the multidisciplinary team.

H. El Hage Chehade et al. SLNB in DCIS patients 179
Conclusions
To our knowledge, this is the largest analysis to date forthe use of the SLNB in DCIS. The SLNB should be routinelyconsidered in patients with large (.2 cm) high-grade DCIS.In the context of breast conserving surgery, the SLNB is notroutinely indicated for low- and intermediate-grade DCIS,high-grade DCIS smaller than 2 cm, or pure DCIS diagnosedby definitive surgical excision. Furthermore, we believe thatthe clinical effect of such selective SLNB for DCIS would bean important area of research for future prospective studiesand randomized trials as this would enable better informeddecisions in the treatment of DCIS.
References
1. Office for National Statistics; 2012 Available at: http://www.ons.gov.
uk/ons/search/index.html?newquery5cancer1registrations. Accessed
December 13, 2015.
2. Al-Hilli Z, Hieken TJ, Boughey JC. Axillary ultrasound in the man-
agement of the newly diagnosed breast cancer patient. Breast J
2015;21:634–41.
3. Nicholson S, Hanby A, Clements K, et al. Variations in the manage-
ment of the axilla in screen-detected ductal carcinoma in situ: evidence
from the UK NHS breast screening programme audit of screen
detected DCIS. Eur J Surg Oncol 2015;41:86–93.
4. Chang WC, Hsu HH, Yu JC, et al. Underestimation of invasive lesions
in patients with ductal carcinoma in situ of the breast diagnosed by
ultrasound-guided biopsy: a comparison between patients with and
without HER2/neu overexpression. Eur J Radiol 2014;83:935–41.
5. Francis AM, Haugen CE, Grimes LM, et al. Is sentinel lymph node
dissection warranted for patients with a diagnosis of ductal carcinoma
in situ? Ann Surg Oncol 2015;22:4270–9.
6. Deeks JJ, Higgins JP. Statistical Algorithms in Review Manager 5. Sta-
tistical Methods Group of the Cochrane Collaboration; 2010. Available
at: http://ims.cochrane.org/revman/documentation/Statistical-methods-
in-RevMan-5.pdf. Accessed August 1, 2016.
7. Ansari B, Boughey JC, Adamczyk DL, et al. Should axillary ultra-
sound be used in patients with a preoperative diagnosis of ductal car-
cinoma in situ? Am J Surg 2012;204:290–3.
8. Ballehaninna UK, Chamberlain RS. Utility of intraoperative frozen
section examination of sentinel lymph nodes in ductal carcinoma in
situ of the breast. Clin Breast Cancer 2013;13:350–8.
9. Banys M, Hahn M, Gruber I, et al. Detection and clinical relevance of
hematogenous tumor cell dissemination in patients with ductal carci-
noma in situ. Breast Cancer Res Treat 2014;144:531–8.
10. Chin-Lenn L, Mack LA, Temple W, et al. Predictors of treatment with
mastectomy, use of sentinel lymph node biopsy and upstaging to inva-
sive cancer in patients diagnosed with breast ductal carcinoma in situ
(DCIS) on core biopsy. Ann Surg Oncol 2014;21:66–73.
11. Chvalny P, Donat R, Dyttert D, et al. Ductal carcinoma in situ (DCIS)
and biopsy of the sentinel lymph node. Rozhl Chir 2011;90:352–60.
12. Collado MV, Ruiz-Tovar J, Garcia-Villanueva A, et al. Sentinel lymph
node biopsy in selected cases of ductal carcinoma in situ. Clin Transl
Oncol 2010;12:499–502.
13. Cserni G. Sentinel lymph node biopsy as a tool for the staging of
ductal carcinoma in situ in patients with breast carcinoma. Surg Today
2002;32:99–103.
14. D’Eredita G, Giardina C, Napoli A, et al. Sentinel lymph node biopsy
in patients with pure and high-risk ductal carcinoma in situ of the
breast. Tumori 2009;95:706–11.
15. Dominguez FJ, Golshan M, Black DM, et al. Sentinel node biopsy is
important in mastectomy for ductal carcinoma in situ. Ann Surg Oncol
2008;15:268–73.
16. Doyle B, Al-Mudhaffer M, Kennedy MM, et al. Sentinel lymph node
biopsy in patients with a needle core biopsy diagnosis of ductal carci-
noma in situ: is it justified? J Clin Pathol 2009;62:534–8.
17. Fancellu A, Cottu P, Feo CF, et al. Sentinel node biopsy in early breast
cancer: lessons learned from more than 1000 cases at a single institu-
tion. Tumori 2012;98:413–20.
18. Guillot E, Vaysse C, Goetgeluck J, et al. Extensive pure ductal carci-
noma in situ of the breast: identification of predictors of associated
infiltrating carcinoma and lymph node metastasis before immediate
reconstructive surgery. Breast 2014;23:97–103.
19. Han JS, Molberg KH, Sarode V. Predictors of invasion and axillary
lymph node metastasis in patients with a core biopsy diagnosis of ductal
carcinoma in situ: an analysis of 255 cases. Breast J 2011;17:223–9.
20. Hung WK, Ying M, Chan M, et al. The impact of sentinel lymph node
biopsy in patients with a core biopsy diagnosis of ductal carcinoma in
situ. Breast Cancer 2010;17:276–80.
21. Intra M, Rotmensz N, Veronesi P, et al. Sentinel node biopsy is not a
standard procedure in ductal carcinoma in situ of the breast: the expe-
rience of the European institute of oncology on 854 patients in 10
years. Ann Surg 2008;247:315–9.
22. Katz A, Gage I, Evans S, et al. Sentinel lymph node positivity of pa-
tients with ductal carcinoma in situ or microinvasive breast cancer. Am
J Surg 2006;191:761–6.
23. Kotani H, Yoshimura A, Adachi Y, et al. Sentinel lymph node biopsy is
not necessary in patients diagnosed with ductal carcinoma in situ of
the breast by stereotactic vacuum-assisted biopsy. Breast Cancer
2016;23:190–4.
24. Matsen CB, Hirsch A, Eaton A, et al. Extent of microinvasion in ductal
carcinoma in situ is not associated with sentinel lymph node metasta-
ses. Ann Surg Oncol 2014;21:3330–5.
25. Meretoja TJ, Heikkila PS, Salmenkivi K, et al. Outcome of patients
with ductal carcinoma in situ and sentinel node biopsy. Ann Surg On-
col 2012;19:2345–51.
26. Miyake T, Shimazu K, Ohashi H, et al. Indication for sentinel lymph
node biopsy for breast cancer when core biopsy shows ductal carci-
noma in situ. Am J Surg 2011;202:59–65.
27. Namm JP, Mueller J, Kocherginsky M, et al. The utility of sentinel
lymph node biopsy in patients with ductal carcinoma in situ suspicious
for microinvasion on core biopsy. Ann Surg Oncol 2015;22:59–65.
28. Nowikiewicz T, Wisniewska M, Wisniewski M, et al. Clinical signif-
icance of Van Nuys Prognostic Index as a qualification criterion to
sentinel lymph node biopsy in patients diagnosed with ductal carci-
noma in situ. Pol Przegl Chir 2015;86:479–85.
29. Osako T, Iwase T, Kimura K, et al. Incidence and possible pathogen-
esis of sentinel node micrometastases in ductal carcinoma in situ of the
breast detected using molecular whole lymph node assay. Br J Cancer
2012;106:1675–81.
30. Osako T, Iwase T, Ushijima M, et al. Incidence and prediction of inva-
sive disease and nodal metastasis in preoperatively diagnosed ductal
carcinoma in situ. Cancer Sci 2014;105:576–82.
31. Ozkan-Gurdal S, Cabioglu N, Ozcinar B, et al. Factors predicting mi-
croinvasion in Ductal Carcinoma in situ. Asian Pac J Cancer Prev
2014;15:55–60.
32. Park HS, Park S, Cho J, et al. Risk predictors of underestimation and
the need for sentinel node biopsy in patients diagnosed with ductal car-
cinoma in situ by preoperative needle biopsy. J Surg Oncol 2013;107:
388–92.
33. Polom K, Murawa D, Wasiewicz J, et al. The role of sentinel node bi-
opsy in ductal carcinoma in situ of the breast. Eur J Surg Oncol 2009;
35:43–7.
34. Prendeville S, Ryan C, Feeley L, et al. Sentinel lymph node biopsy is
not warranted following a core needle biopsy diagnosis of ductal car-
cinoma in situ (DCIS) of the breast. Breast 2015;24:197–200.
35. Ruvalcaba-Limon E, de Jesus Garduno-Raya M, Bautista-Pina V, et al.
Sentinel lymph node metastasis in patients with ductal breast carci-
noma in situ. Cir Cir 2014;82:129–41.
36. Sakr R, Barranger E, Antoine M, et al. Ductal carcinoma in situ: value
of sentinel lymph node biopsy. J Surg Oncol 2006;94:426–30.
180 The American Journal of Surgery, Vol 213, No 1, January 2017
37. Son BK, Bong JG, Park SH, et al. Ductal carcinoma in situ and
sentinel lymph node biopsy. J Breast Cancer 2011;14:301–7.
38. Sundara Rajan S, Verma R, Shaaban AM, et al. Palpable ductal carci-
noma in situ: analysis of radiological and histological features of a
large series with 5-year follow-up. Clin Breast Cancer 2013;13:
486–91.
39. Tunon-de-Lara C, Chauvet MP, Baranzelli MC, et al. The role of
sentinel lymph node biopsy and factors associated with invasion in
extensive DCIS of the breast treated by mastectomy: the Cinnamome
prospective multicenter study. Ann Surg Oncol 2015;22:3853–60.
40. Tunon-de-Lara C, Giard S, Buttarelli M, et al. Sentinel node procedure
is warranted in ductal carcinoma in situ with high risk of occult inva-
sive carcinoma and microinvasive carcinoma treated by mastectomy.
Breast J 2008;14:135–40.
41. Usmani S, Khan HA, Al Saleh N, et al. Selective approach to
radionuclide-guided sentinel lymph node biopsy in high-risk ductal
carcinoma in situ of the breast. Nucl Med Commun 2011;32:
1084–7.
42. Veronesi P, Intra M, Vento AR, et al. Sentinel lymph node biopsy for
localised ductal carcinoma in situ? Breast 2005;14:520–2.
43. Walters LL, Pang JC, Zhao L, et al. Ductal carcinoma in situ with dis-
torting sclerosis on core biopsy may be predictive of upstaging on
excision. Histopathology 2015;66:577–86.
44. Zapardiel I, Llorca J, Xercavins J, et al. Variation among Spanish
teaching hospitals in ductal carcinoma in situ treatment: results of a
national survey. Eur J Obstet Gynecol Reprod Biol 2013;171:128–31.
45. Intra M, Veronesi P, Mazzarol G, et al. Axillary sentinel lymph node
biopsy in patients with pure ductal carcinoma in situ of the breast.
Arch Surg 2003;138:309–13.
46. Kelly TA, Kim JA, Patrick R, et al. Axillary lymph node metastases in
patients with a final diagnosis of ductal carcinoma in situ. Am J Surg
2003;186:368–70.
47. Leidenius M, Salmenkivi K, von Smitten K, et al. Tumour-positive
sentinel node findings in patients with ductal carcinoma in situ.
J Surg Oncol 2006;94:380–4.
48. Mabry H, Giuliano AE, Silverstein MJ. What is the value of axillary
dissection or sentinel node biopsy in patients with ductal carcinoma
in situ? Am J Surg 2006;192:455–7.
49. Sakr R, Bezu C, Raoust I, et al. The sentinel lymph node procedure for
patients with preoperative diagnosis of ductal carcinoma in situ: risk
factors for unsuspected invasive disease and for metastatic sentinel
lymph nodes. Int J Clin Pract 2008;62:1730–5.
50. Tada K, Ogiya A, Kimura K, et al. Ductal carcinoma in situ and
sentinel lymph node metastasis in breast cancer. World J Surg Oncol
2010;8:6.
51. Takacs T, Paszt A, Szentpali K, et al. Importance of sentinel lymph
node biopsy in surgical therapy of in situ breast cancer. Pathol Oncol
Res 2009;15:329–33.
52. Zetterlund L, Stemme S, Arnrup H, et al. Incidence of and risk factors
for sentinel lymph node metastasis in patients with a postoperative
diagnosis of ductal carcinoma in situ. Br J Surg 2014;101:488–94.
53. Zavagno G, Carcoforo P, Marconato R, et al. Role of axillary sentinel
lymph node biopsy in patients with pure ductal carcinoma in situ of the
breast. BMC Cancer 2005;5:28.
54. Fleissig A, Fallowfield LJ, Langridge CI, et al. Post-operative arm
morbidity and quality of life. Results of the ALMANAC randomised
trial comparing sentinel node biopsy with standard axillary treatment
in the management of patients with early breast cancer. Breast Cancer
Res Treat 2006;95:279–93.
55. Brenet O, Lalourcey L, Queinnec M, et al. Hypersensitivity reactions
to Patent Blue V in breast cancer surgery: a prospective multicentre
study. Acta Anaesthesiol Scand 2013;57:106–11.
56. Iqbal FM, Basit A, Salem F, et al. Feeling blue, going green and
finding other attractive alternatives: a case of biphasic anaphylaxis
to patent blue and a literature review of alternative sentinel node local-
isation methods. BMJ Case Rep 2015;2015. http://dx.doi.org/10.1136/
bcr-2015-213107.
57. Manson AL, Juneja R, Self R, et al. Anaphylaxis to patent blue V: a
case series. Asia Pac Allergy 2012;2:86–9.
58. Maranhao MV, Nobrega DK, Anunciacao CE, et al. Allergic reaction
to patent blue dye in breast surgery - case report. Rev Bras Anestesiol
2016;66:433–6.
59. Wong A, Spillane A, Breast Surgeons of Australia and New Zealand
Incorporated (BreastSurgANZ). Patent Blue V dye anaphylaxis: expe-
rience of Australian and New Zealand surgeons. ANZ J Surg 2014;84:
37–41.
60. Thevarajah S,HustonTL, Simmons RM.A comparison of the adverse re-
actions associated with isosulfan blue versus methylene blue dye in
sentinel lymphnodebiopsy for breast cancer.AmJSurg 2005;189:236–9.
61. Bezu C, Coutant C, Salengro A, et al. Anaphylactic response to blue
dye during sentinel lymph node biopsy. Surg Oncol 2011;20:e55–9.
62. Ronka R, von Smitten K, Tasmuth T, et al. One-year morbidity after
sentinel node biopsy and breast surgery. Breast 2005;14:28–36.
63. Sener SF, Winchester DJ, Martz CH, et al. Lymphedema after sentinel
lymphadenectomy for breast carcinoma. Cancer 2001;92:748–52.
64. Diepstraten SC, van de Ven SM, Pijnappel RM, et al. Development and
evaluation of a prediction model for underestimated invasive breast
cancer in women with ductal carcinoma in situ at stereotactic large
core needle biopsy. PLoS One 2013;8:e77826.
65. Lyman GH, Temin S, Edge SB, et al. Sentinel lymph node biopsy for
patients with early-stage breast cancer: American Society of Clinical
Oncology clinical practice guideline update. J Clin Oncol 2014;32:
1365–83.
66. Tan JC, McCready DR, Easson AM, et al. Role of sentinel lymph node
biopsy in ductal carcinoma-in-situ treated by mastectomy. Ann Surg
Oncol 2007;14:638–45.
67. Boler DE, Cabioglu N, Ince U, et al. Sentinel lymph node biopsy in
pure DCIS: is it necessary? ISRN Surg 2012;2012:394095.
68. Kondo T, Hayashi N, Ohde S, et al. A model to predict upstaging to
invasive carcinoma in patients preoperatively diagnosed with ductal
carcinoma in situ of the breast. J Surg Oncol 2015;112:476–80.
69. Diaz LK, Wiley EL, Venta LA. Are malignant cells displaced by large-
gauge needle core biopsy of the breast? AJR Am J Roentgenol 1999;
173:1303–13.
70. Diaz NM, Cox CE, Ebert M, et al. Benign mechanical transport of
breast epithelial cells to sentinel lymph nodes. Am J Surg Pathol
2004;28:1641–5.
71. Yen TW, Hunt KK, Ross MI, et al. Predictors of invasive breast cancer
in patients with an initial diagnosis of ductal carcinoma in situ: a guide
to selective use of sentinel lymph node biopsy in management of
ductal carcinoma in situ. J Am Coll Surg 2005;200:516–26.
72. Shah DR, Canter RJ, Khatri VP, et al. Utilization of sentinel lymph
node biopsy in patients with ductal carcinoma in situ undergoing mas-
tectomy. Ann Surg Oncol 2013;20:24–30.
73. Patani N, Mokbel K. The clinical significance of sentinel lymph node
micrometastasis in breast cancer. Breast Cancer Res Treat 2009;114:
393–402.
74. Salhab M, Patani N, Mokbel K. Sentinel lymph node micrometastasis
in human breast cancer: an update. Surg Oncol 2011;20:e195–206.
75. Iwase T, Takahashi K, Gomi N, et al. Present state of and problems
with core needle biopsy for non-palpable breast lesions. Breast Cancer
2006;13:32–7.
76. Meijnen P, Oldenburg HS, Loo CE, et al. Risk of invasion and axillary
lymph node metastasis in ductal carcinoma in situ diagnosed by core-
needle biopsy. Br J Surg 2007;94:952–6.
77. Omranipour R, Alipour S, Hadji M, et al. Two decades of experience
with ductal carcinoma in situ of the breast in the Cancer Institute of
Tehran, Iran. Asian Pac J Cancer Prev 2014;15:2771–6.




















