MRI-guided biopsy and fine needle aspiration biopsy (FNAB) in the diagnosis of musculoskeletal...
6
European Journal of Radiology 82 (2013) 2328–2333 Contents lists available at ScienceDirect European Journal of Radiology journa l ho me p age: www.elsevier.com/locate/ejrad MRI-guided biopsy and fine needle aspiration biopsy (FNAB) in the diagnosis of musculoskeletal lesions Pekka Kerimaa a,∗ , Antti Marttila a , Pekka Hyvönen b , Risto Ojala a , Elisa Lappi-Blanco c , Osmo Tervonen a , Roberto Blanco Sequeiros a a Department of Radiology, Oulu University Hospital, P.O. Box 50, 90029 OYS, Finland b Department of Surgery, Oulu University Hospital, P.O. Box 50, 90029 OYS, Finland c Department of Pathology, Oulu University Hospital, P.O. Box 50, 90029 OYS, Finland a r t i c l e i n f o Article history: Received 22 January 2013 Received in revised form 2 September 2013 Accepted 6 September 2013 Keywords: MRI guidance Musculoskeletal Biopsy Tumor Interventional MRI a b s t r a c t Objectives: The purpose of this study was to evaluate the diagnostic performance of magnetic resonance imaging (MRI) guided musculoskeletal biopsy and the value of fine needle aspiration biopsy (FNAB) when combined with histologic biopsy. Materials and methods: A total of 172 biopsies were performed under MRI guidance, 170 were histologic biopsies. In 112 cases, a fine needle aspiration biopsy was also performed. In two cases, a stand-alone FNAB was performed. The diagnostic performance was evaluated retrospectively by comparing the histopatho- logic and cytologic diagnosis with the current or final diagnosis after at least one year of clinical and imaging follow-up. A 0.23 T open MRI scanner with an interventional stereotactic guidance system was used. Results: The overall diagnostic accuracy of MRI guided biopsy was 0.95, sensitivity 0.91, specificity 0.98, positive predictive value (ppv) 0.97 and negative predictive value (npv) 0.93. The diagnostic accuracy of trephine biopsy alone was 0.93, sensitivity 0.89, specificity 0.98, ppv 0.97 and npv 0.91 and accuracy for FNAB alone was 0.85, sensitivity 0.80, specificity 0.90, ppv 0.89 and npv 0.82. Conclusions: MRI guidance is a feasible and accurate tool in percutaneous musculoskeletal biopsies. Fine needle biopsy is a useful low-cost supplement to histologic biopsy. © 2013 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Image guided percutaneous biopsy is typically the first invasive step in the diagnostic workup for investigating musculoskeletal lesions. Considering bone lesions, computed tomography and flu- oroscopy are the two most common methods used for guidance [1–5]. As for soft tissue lesions, especially superficially located, ultrasound is usually the preferred modality [6,7,8]. Percutaneous fine-needle aspiration biopsy (FNAB) has an established role in the diagnostic workup of an extremely wide range of soft-tissue lesions [1,9]. Combining FNAB with a percu- taneous trephine biopsy or with a core-needle biopsy through a coaxial needle requires minimal additional effort and causes lit- tle or no additional trauma or cost and it may well increase the diagnostic accuracy of the bone biopsy [2,5]. Magnetic resonance ∗ Corresponding author. Tel.: +358 8 3153737; fax: +358 8 3155420. E-mail addresses: pekka.kerimaa@ppshp.fi (P. Kerimaa), antti.marttila@ppshp.fi (A. Marttila), pekka.hyvonen@ppshp.fi (P. Hyvönen), risto.ojala@ppshp.fi (R. Ojala), elisa.lappi-blanco@ppshp.fi (E. Lappi-Blanco), osmo.tervonen@ppshp.fi (O. Tervonen), roberto.blanco@oulu.fi (R. Blanco Sequeiros). imaging (MRI) guided biopsy has proven its value as a tool for musculoskeletal biopsies and therapeutic procedures [10–14], especially in a situation where the target lesion or its most repre- sentative part is best visualized or accessed by magnetic resonance imaging guidance [15]. However, there are no reports using a large patient population evaluating the diagnostic value of MRI in mus- culoskeletal intervention, especially in bone biopsies. The purpose of this retrospective study was to evaluate the diag- nostic performance of MRI guided percutaneous musculoskeletal biopsy in the clinical context and to assess the value of combined fine-needle aspiration. 2. Materials and methods 2.1. Patients This study has been approved by the ethical board of the hospi- tal. A total of 163 patients were included in this retrospective study. Informed consent was obtained from all patients or their parents before the procedure. The patients underwent 172 percutaneous MRI guided musculoskeletal biopsies. In addition, 114 FNABs were 0720-048X/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ejrad.2013.09.005
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of MRI-guided biopsy and fine needle aspiration biopsy (FNAB) in the diagnosis of musculoskeletal...

Md
POa
b
c
a
ARRA
KMMBTI
1
slo[u
ertctd
(e(
0h
European Journal of Radiology 82 (2013) 2328– 2333
Contents lists available at ScienceDirect
European Journal of Radiology
journa l ho me p age: www.elsev ier .com/ locate /e j rad
RI-guided biopsy and fine needle aspiration biopsy (FNAB) in theiagnosis of musculoskeletal lesions
ekka Kerimaaa,∗, Antti Marttilaa, Pekka Hyvönenb, Risto Ojalaa, Elisa Lappi-Blancoc,smo Tervonena, Roberto Blanco Sequeirosa
Department of Radiology, Oulu University Hospital, P.O. Box 50, 90029 OYS, FinlandDepartment of Surgery, Oulu University Hospital, P.O. Box 50, 90029 OYS, FinlandDepartment of Pathology, Oulu University Hospital, P.O. Box 50, 90029 OYS, Finland
r t i c l e i n f o
rticle history:eceived 22 January 2013eceived in revised form 2 September 2013ccepted 6 September 2013
eywords:RI guidanceusculoskeletal
iopsyumor
a b s t r a c t
Objectives: The purpose of this study was to evaluate the diagnostic performance of magnetic resonanceimaging (MRI) guided musculoskeletal biopsy and the value of fine needle aspiration biopsy (FNAB) whencombined with histologic biopsy.Materials and methods: A total of 172 biopsies were performed under MRI guidance, 170 were histologicbiopsies. In 112 cases, a fine needle aspiration biopsy was also performed. In two cases, a stand-alone FNABwas performed. The diagnostic performance was evaluated retrospectively by comparing the histopatho-logic and cytologic diagnosis with the current or final diagnosis after at least one year of clinical andimaging follow-up. A 0.23 T open MRI scanner with an interventional stereotactic guidance system wasused.
nterventional MRI Results: The overall diagnostic accuracy of MRI guided biopsy was 0.95, sensitivity 0.91, specificity 0.98,positive predictive value (ppv) 0.97 and negative predictive value (npv) 0.93. The diagnostic accuracy oftrephine biopsy alone was 0.93, sensitivity 0.89, specificity 0.98, ppv 0.97 and npv 0.91 and accuracy forFNAB alone was 0.85, sensitivity 0.80, specificity 0.90, ppv 0.89 and npv 0.82.Conclusions: MRI guidance is a feasible and accurate tool in percutaneous musculoskeletal biopsies. Fineneedle biopsy is a useful low-cost supplement to histologic biopsy.
. Introduction
Image guided percutaneous biopsy is typically the first invasivetep in the diagnostic workup for investigating musculoskeletalesions. Considering bone lesions, computed tomography and flu-roscopy are the two most common methods used for guidance1–5]. As for soft tissue lesions, especially superficially located,ltrasound is usually the preferred modality [6,7,8].
Percutaneous fine-needle aspiration biopsy (FNAB) has anstablished role in the diagnostic workup of an extremely wideange of soft-tissue lesions [1,9]. Combining FNAB with a percu-aneous trephine biopsy or with a core-needle biopsy through a
oaxial needle requires minimal additional effort and causes lit-le or no additional trauma or cost and it may well increase theiagnostic accuracy of the bone biopsy [2,5]. Magnetic resonance∗ Corresponding author. Tel.: +358 8 3153737; fax: +358 8 3155420.E-mail addresses: [email protected] (P. Kerimaa), [email protected]
A. Marttila), [email protected] (P. Hyvönen), [email protected] (R. Ojala),[email protected] (E. Lappi-Blanco), [email protected]. Tervonen), [email protected] (R. Blanco Sequeiros).
720-048X/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.ejrad.2013.09.005
© 2013 Elsevier Ireland Ltd. All rights reserved.
imaging (MRI) guided biopsy has proven its value as a toolfor musculoskeletal biopsies and therapeutic procedures [10–14],especially in a situation where the target lesion or its most repre-sentative part is best visualized or accessed by magnetic resonanceimaging guidance [15]. However, there are no reports using a largepatient population evaluating the diagnostic value of MRI in mus-culoskeletal intervention, especially in bone biopsies.
The purpose of this retrospective study was to evaluate the diag-nostic performance of MRI guided percutaneous musculoskeletalbiopsy in the clinical context and to assess the value of combinedfine-needle aspiration.
2. Materials and methods
2.1. Patients
This study has been approved by the ethical board of the hospi-
tal. A total of 163 patients were included in this retrospective study.Informed consent was obtained from all patients or their parentsbefore the procedure. The patients underwent 172 percutaneousMRI guided musculoskeletal biopsies. In addition, 114 FNABs were
P. Kerimaa et al. / European Journal of
Table 1The anatomic locations of the target lesions.
Anatomic site Frequency Percent
Femur 55 32.0Spine 37 21.5Pelvis 30 17.4Upper extremity 15 8.7Tibia 10 5.8Thorax 5 2.9Foot 4 2.3
t(Fhtaart
mootwmippn
2istlm(tcogce
2
aVf
t
TL
Soft tissue 16 9.3
Total 172 100.0
argeted to the lesion area either as a complementary procedure112 cases) or as a stand-alone procedure (two). One stand-aloneNAB was performed in a case of a paralabral cyst in the gleno-umeral joint. The other case was lymphoma of the spine, wherehe histologic sample was omitted in order to achieve the diagnosiss fast as possible. In 36 cases, a microbiologic culture sample waslso acquired, but these results were largely unavailable for the ret-ospective analysis. A lesion in the soft tissue was targeted in 16 ofhe 172 procedures, leaving 156 lesions in the bone.
The mean age of the patients was 49 years (range 1–87), with 89en and 83 women. All the patients had a musculoskeletal lesion
f an unconfirmed nature detected in a previous radiograph, CTr MRI. The lesion was suspected as being either neoplastic, infec-ious, inflammatory or unknown in nature. A percutaneous biopsyas necessary for diagnostic purposes and MRI was seen as theost suitable method for guidance. Usually the decision-making
nvolved a multidisciplinary group consisting of a radiologist, aathologist, an oncologist and either a plastic surgeon or an ortho-edic surgeon. Most patients were discharged on the same or theext day.
The maximal lesion diameter varied from 0.3 cm to 15 cm (mean.7 cm). Lesions were graded by preoperative or perioperative MR
maging as odematous (n = 83, 48.3%), destructive (n = 33, 19.2%),clerotic (n = 35, 20.3%) or cystic (n = 20, 11.6%) of nature. One (0.6%)arget was determined as normal, when suspected myopathy ofevator scapulae muscle was biopsied. A primary malignancy or a
etastasis of an underlying malignancy was suspected in 70 cases40.1%). In some cases, a biopsy was harvested when conducting aherapeutic procedure of a benign lesion, such as filling of a boneyst, drilling of an osteochondritis dissecans lesion or laser ablationf an osteoid osteoma. The anatomic locations of the lesions areiven in Table 1 with the spine and the extremities being the mostommon sites. The lesions in the soft tissue are grouped into a singlentity because of their heterogeneous anatomic distribution.
.2. Equipment
A 0.23 T open MRI scanner with an instrument tracking systemnd software was used. (Outlook Proview, Philips medical systems,
antaa, Finland.) A surface coil allowing needle placement was usedor all periprocedural imaging.Instrument tracking was performed using an infrared naviga-
or system where a camera detects two reflectors, one of which is
able 2ow-field MR imaging sequences used.
Sequence TE (ms) TR (ms) Slice thickness (mm) Slice interv
T1 FSE 7 95 7.0 7.0
T1 FSE 11 130 10.0 10.0
T1 FSE w. contrast 400 16 7.0 8.0
T2 FSE 3500 150 7.0 8.0
True-FISP GE 4.2 8.4 5.0 5.0
True-FISP GE 4.5 9.2 10.0 10.0
Radiology 82 (2013) 2328– 2333 2329
attached to the biopsy set and the other to the magnet providinga fixed reference frame. The chosen target point, the instrumentand its trajectory are shown in real-time as a graphic overlay in theimage set during the procedure.
Three MRI compatible trephine biopsy sets of different calibers(3 mm and 6 mm diameter, InVivo Philips, Schwerin, Germany and2 mm diameter, Somatex, Berlin, Germany) were used. A 16 gaugecore biopsy gun was used in cases where the target was located inthe soft tissue (InVivo Philips, Schwerin, Germany).
FNAB was performed through a coaxial needle or a cannula ofthe biopsy set with MRI compatible 18–20 gauge needles (MReye,Cook, Bloomington, IN, USA, In vivo-Philips, Somatex, Berlin,Germany).
2.3. The procedure
The preliminary procedural route planning was done using theimages from a previous MRI study but if this was not available, theroute was determined preprocedurally with T1- and T2-weightedfast spin echo and True-FISP gradient echo sequences. The mostviable-appearing part of the lesion was selected as the target. Withbone lesions, the path with the least amount of cortical or other-wise sclerotic bone was preferred and an extraosseous part of thelesion was targeted whenever possible. T1-weighted fast spin echoimaging or True-FISP gradient echo imaging was used to visualizethe biopsy set and the target during the procedure. The detailedspecifics of the used sequences are listed in Table 2.
The necessary precautions were implemented to ensure a sterileand safe procedural condition. This included the usual safety issuesconcerning MRI setup and instrumentation. Antibiotic prophylaxis,most typically a single 1.5 g intravenous dose of cefuroxim, hadbeen administered according to the records in 31 cases and notused in 117 cases. However, this information was missing in theremaining 24 cases.
If previous or periprocedural imaging suggested that the useof contrast agent might help to visualize the most viable partof the lesion, intravenous contrast medium (0.1 ml/kg gadobutrol(Gadovist®, Bayer pharma, Leverkusen, Germany)) was used (eightcases) and T1-weighted fast spin echo imaging was then performed.Contrast enhancement was used in five lesions graded odematous,two graded destructive and one graded sclerotic.
The site of the skin puncture and the final procedural route weredetermined by placing the tracker-mounted instrument close tothe skin at the estimated skin puncture area and acquiring subse-quent image sets in order to visualize the procedure area and theroute. Local anesthetic (lidocaine 10 mg/ml or 20 mg/ml) was usu-ally injected into the soft tissue and along the puncture route. Thiswas performed to reduce any possible postprocedural pain evenin cases when general anesthesia or spinal anesthesia was usedduring the procedure. A small skin incision was made to facilitatethe entry of the biopsy set. The coaxial biopsy set was advancedthrough the incision to the perimeter of the lesion using the tracker
generated graphic overlay and the instrument generated suscepti-bility in repeated MR acquisitions.After lesion contact, the trocar was removed from the coax-ial cannula and sample was collected with a cutting needle or a
al (mm) FOV Matrix No. of Slices Acquisition time (s)
380 × 380 300 × 300 3 12380 × 380 256 × 256 5 18380 × 380 324 × 324 5 23380 × 380 192 × 192 9 35380 × 380 256 × 256 8 24380 × 380 256 × 256 1 1.5

2330 P. Kerimaa et al. / European Journal of Radiology 82 (2013) 2328– 2333
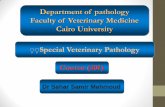
Fig. 1. MRI-guided biopsy of an odematous destructive lesion located in the thirdlumbar vertebra. (A) Sagittal plane (B-FFE3D, TR/TE 8.4/4.2 ms, matrix 256 × 256,resolution 1.5 mm × 1.5 mm) and (B) axial plane (B-FFE2D, TR/TE 9/4.5 ms, matrix216 × 216, resolution 1.8 mm × 1.8 mm). The white arrow illustrates the needle.Images cropped to region of interest. The lesion proved to be a metastasis ofu
t2ni5tmctri
t3w
Fig. 2. MRI-guided biopsy of an odematous lesion in the right tibia with anosteotomy complication. (A) Coronal plane (T1 TSE TR/TE 400/16 ms, matrix288 × 288, resolution 1.0 mm × 1.0 mm) and (B) axial plane (T1 TSE TR/TE 400/16 ms,matrix 288 × 288, resolution 1.0 mm × 1.0 mm). The white arrow shows the needle
least one year of follow-up and classified as true positive, true neg-
nknown origin.
rephine. In the case of a bony lesion, a cylindrical trephine of either, 3 or 6 mm of diameter was advanced into the lesion thru the can-ula (Figs. 1 and 2) and a sample was collected. This was repeated
f the sample seemed insufficient, i.e. sample length was less than mm. A 16 g biopsy gun with a side-cutting needle was used if thearget was located in the soft tissue. Unfortunately detailed infor-
ation was not available about sample numbers and length in allases. The cytologic sample was aspirated through the cannula afterhe initial tissue biopsy or, in case of a stand-alone fine needle aspi-ation biopsy, through a coaxial needle of smaller diameter insertedn a similar fashion.
A total of 87 procedures were performed under general anes-hesia, 56 under spinal anesthesia, 21 under local anesthesia and
under epidural anesthesia. In five cases, the means of anesthesiaas not specified.
next to the fixation material induced artifact. Images cropped to region of interest.Infection was suspected, but only reactive changes were found.
2.4. Classification of the biopsy results
The tissue biopsy samples were fixed in 10% formalin. The FNABmaterial was fixed in 50% alcohol. The samples were then processedand analyzed by experienced pathologists and deemed as eithersufficient or insufficient for diagnostic use. The FNAB findings wererated as follows: C0 = insufficient, C1 = normal, C2 = benign atypia,C3 = possibly malignant, C4 = highly suspicious of malignancy andC5 = malignant. Grades C3, C4 and C5 were interpreted as repre-senting malignant histology.
To determine the diagnostic performance for histology andFNAB, the results were compared with the final diagnosis after at
ative, false positive or false negative. In the absence of technicalfailure, the result “no specific histopathologic findings” was inter-preted as a successful procedure and a true finding when this was

nal of
nowifib
3
swobdobtco
rnftsgop
wapadCfinofsati
i0psm
hsmswT
fitt(bF
P. Kerimaa et al. / European Jour
ot in contradiction with the clinical setting or follow-up, as withsteoid osteomas, hemangiomas and other such benign lesions,here the biopsy often yields normal tissue. In the few cases where
nterpretation of the final outcome between true and false was dif-cult (cytologic class three), the decision was made against theiopsy method.
. Results
A total of 172 MRI guided percutaneous musculoskeletal biop-ies were performed and a successful needle placement at targetas achieved in all but one case. In that particular case, the length
f the trephine biopsy set was not sufficient to allow it to reach theony target lesion in an obese patient and FNAB failed to provide aiagnostic sample. There were no periprocedural conversions tother image modalities or to open surgery. All other histologiciopsies yielded an adequate amount of material and were thusechnically successful (yield 99.4%). FNAB resulted in Papanicolaulass 0, insufficient sample, in a total of fifteen cases (yield 86.8%),f which twelve were bone lesions.
Out of the 171 technically successful biopsies, 74 were ret-ospectively interpreted as true positive findings and 87 as trueegative after at least one year of unstructured clinical and imaging
ollow-up including repeated biopsies in a few cases. There werewo false positive results where both histologic biopsy and FNABuggested a malignancy: one lesion which turned out to be a gan-lion was initially suspected of being a giant cell tumor and thether was a suspected lymphoid neoplasm that subsequently wasroven to be insignificant at open biopsy.
Seven samples were interpreted as false negative. Five of theseere missed malignancies, one was an enchondroma and one was
bone cyst. This results in a sensitivity of 0.91, specificity of 0.98,ositive predictive value of 0.97, negative predictive value of 0.93nd accuracy of 0.95 for the whole material. A conjunctive FNABetected two malignancies that the histologic biopsy had missed.ytology class three was seen with a chondrosarcoma and a classve with a metastasis from an adrenal cancer. There were ten falseegative FNAB’s and the histologic biopsy was true positive in fivef those. Thus, the respective measures of diagnostic performanceor histologic biopsy alone (169 technically successful cases) werelightly lower: sensitivity 0.89, specificity 0.98, PPV 0.97, NPV 0.91nd accuracy 0.93. For FNAB alone (99 technically successful cases),he respective values were 0.80, 0.90, 0.89, 0.82 and 0.85 when thensufficient class zero samples were excluded.
Separate results were calculated for lesions in the bone andn the soft tissue as well. For lesions in the bone, sensitivity was.90, specificity 0.99, positive predictive value 0.99 and negativeredictive value 0.92. The material includes only 16 lesions in theoft tissue, for which the respective measures of diagnostic perfor-ance were 1.00, 0.88, 0.89 and 1.00.Measures of diagnostic performance were also calculated for
istologic biopsy and FNAB on target lesions in the bone and in theoft tissue separately. The low number of lesions in the soft tissueakes these measures less substantial, but it seems that a sufficient
ample is more difficult to harvest from a target in the bone, asould be expected. The diagnostic performance is summarized in
able 3.The cytologic finding was in contradiction with the histologic
nding in ten out of 99 cases (89.9% concurrence). In addition tohe aforementioned two malignancies detected by FNAB alone,
here were three class 3 cytologic findings that proved to be benignan enchondroma, postradiation fibrosis and Paget’s disease of theone). The rest of the inconsistent cases were tumors missed byNAB but detected by histologic biopsy: one enchondroma and fourRadiology 82 (2013) 2328– 2333 2331
malignancies. No false class 4 or 5 cytologic findings were detected,which is noteworthy.
The mean actual procedural time from the introduction of theneedle through the skin to needle retraction was 45 min. The meanoperative time from the patient entering the interventional MRIdepartment to the patient leaving was 87 min and this includedthe time for anesthesia and other preparations. On a few occasions,a therapeutic procedure, such as laser ablation of the lesion, wasconducted at the same time which somewhat prolonged the totalduration.
There were two recorded postprocedural complications in twopatients. A pathologic fracture occurred in the biopsied femur (anenchondroma) seven days after the procedure and necessitatedsurgical bone augmentation in order to achieve structural support.The other case was a 2 cm × 5 cm × 5 cm hematoma that developedafter a biopsy of a pelvic bone metastasis from a breast cancer. Thehematoma resolved on its own without any need for transfusion orintervention. A trephine biopsy had been performed in both cases.
4. Discussion
Percutaneous imaging guided biopsy is a cost-effective, mini-mally invasive and highly accurate technique. It is undoubtedly themethod of choice as the first minimally invasive step in the diagno-sis of musculoskeletal lesions of an uncertain character after clinicaland imaging workup [1,5,15–17]. Biopsy is certainly warranted alsowhenever a simple confirmation or exclusion of malignancy will bedecisive for selected treatment, conservative, palliative or curative.
MRI is generally considered as the best modality to diagnosea wide variety of musculoskeletal diseases, including neoplasticprocesses. In particular, oedematous lesions are usually best visu-alized with MRI [12–14,18] and adequate tissue contrast is usuallyachieved even without the need for contrast media. However, thereare results indicating that the use of contrast medium may con-tribute to the accuracy of bone lesion detection in MRI. Especiallythe detection of recurrent malignancies and certain types of car-tilaginous lesions have been reported to benefit from contrastenhancement [19]. Our series did not include many primary malig-nant bone or cartilaginous tumors and thus gadolinium was rarelyused (eight cases of intravenous use, six cases of missing informa-tion in this regard) and thus its possible benefit cannot be evaluated.However, no subjective advantage from contrast use was noted.The key element of MRI is that it provides detailed visualization ofedema in tissue, the hallmark of pathology, and this feature is ofparamount importance in lesion detection.
CT and MRI usually provide better visualization of skeletallesions than fluoroscopy since there is no problem of interferenceby superimposing normal structures and CT has now become estab-lished as a reliable guidance method in skeletal biopsies [1–3,5].With soft tissue lesions, especially in superficial locations, ultra-sound is the primary choice, due to its ready availability, low cost,true real-time imaging and lack of ionizing radiation [6,7]. How-ever, ultrasound does suffer its limitations, such as the lack of highresolution tissue penetration and acoustic shadowing from boneand gas. Newer techniques, such as cone beam CT and image fusionhave been introduced for image guided biopsies [20]; these maysoon be joined by contrast enhanced ultrasound [8].
An open MRI scanner provides unobstructed and instantaneousaccess to the patient during the procedure without having to movethe operating table or the patient. The optical tracking feature,although not a necessity, provides near real-time visualization and
control of the instrument position in relation to the image data atarbitrary angles, potentially speeding up procedures.All lesions detected preoperatively with CT, 1.5 T MRI or scintig-raphy were also detected perioperatively with our 0.23 T scanner.

2332 P. Kerimaa et al. / European Journal of Radiology 82 (2013) 2328– 2333
Table 3Diagnostic performance of MRI guided musculoskeletal biopsies.
Biopsy type ortarget
Number of biopsies
Total Non-diagnostic Truepositive
Truenegative
Falsepositive
Falsenegative
Sensitivity Specificity Positivepredictivevalue
Negativepredictivevalue
Histologic biopsy 170 1 71 87 2 9 0.89 0.98 0.97 0.91FNAB 114 15 40 44 5 10 0.80 0.90 0.89 0.82bone 156 1 66 81 1 7 0.90 0.99 0.99 0.92Soft tissue 16 0 8 7 1 0 1.00 0.88 0.89 1.00HB, bone 154 1 63 80 1 9 0.88 0.99 0.98 0.90HB, soft 16 0 8 7 1 0 1.00 0.88 0.89 1.00
4
1
2
Tplcaamvttc
siFc
ioftts
savmavis
wstccdpctlma
iwFb
FNAB, bone 101 12 34 41
FNAB, soft 13 3 6 3
All 172 1 74 88
he image quality was sufficient to guarantee a safe and successfulrocedure. CT generally has superior spatial resolution and excel-
ent bone to soft tissue contrast, which favors its use, at least inertain complex skeletal regions, such as the cervical spine, or inreas containing fine bony structures or purely sclerotic bone. Inddition to the resolution disadvantage, the MRI-specific instru-entation represents a restriction when operating on small bone
olumes under MRI. Since less ferromagnetic but relatively softitanium alloys are used instead of steel, the thin needles neededo operate in such locations are not ideal for penetrating throughortical bone.
The steady state imaging and parallel imaging substantiallypeed up the MR imaging sequences. In our opinion, the differencen imaging speed when compared to CT guidance is not decisive.urthermore, the visualization of changes in cancellous bone islearly better with MRI than with CT.
MRI does no require the use of ionizing radiation and thiss highly advantageous, especially when performing proceduresn children, adolescents or, should it be necessary, on pregnantemales and of course for the performing physician and the otherheater staff. It must be noted that modern imaging should adhereo the ALARA principle, which requires minimization of unneces-ary exposure to ionizing radiation.
Although most biopsies can be performed under local anesthe-ia, it is our experience that patients do experience more discomfortnd pain when only local anesthesia is used. Spinal anesthesia is aiable option especially when the target is in the lumbar region orore caudally. With children, general anesthesia is almost invari-
bly used, independent of guiding modality. Furthermore, optimalisualization of the thorax region requires minimizing the motionn the target area and thus one must apply apnea during MRI acqui-itions. This is most reliably achieved with mechanical ventilation.
The results of our biopsy series are comparable to those obtainedith CT guidance [2,5]. However, in previous MRI bone biopsy
tudies, the patient numbers have been smaller [10,15,21] andhe suboptimal sample quality has lessened the diagnostic effi-acy [22]. Inadvertent packing of a bone sample may occur, whichan result in the destruction of the fine structures. However, weid not observe any such problems in our series with bone sam-les, which may be due to our decision to use a slow penetratingylindrical drill instead of a biopsy gun. On the other hand, a cut-ing, Westcott-type needle or an aspiration needle would mostikely provide better results on soft tissue targets. Detailed infor-
ation of sample number and cylinder length in each case was notvailable.
FNAB in conjunction with bone biopsy has been shown to be
nformative [2,5]. In this series, the cytologic diagnosis concurredith histologic diagnosis in the vast majority of cases (89 of 99).urthermore, it revealed two malignancies that had been missedy histologic biopsy but yielded no false malignant (class 4 or 5)
10 0.77 0.91 0.90 0.800 1.00 0.75 0.86 1.007 0.91 0.98 0.97 0.93
findings. Overall, since FNAB in conjunction with histologic biopsyis fast and straightforward to perform and is responsible for rela-tively minor additional cost and little or no additional trauma, wefeel there is no reason to omit FNAB once the coaxial needle is inplace. It adds certainty to the workup and may occasionally provideadditional information and added value. In some cases, a repeatedprocedure may be avoided. In this series, histologic biopsy alonewas performed in 58 cases of which all but three lesions were inthe bone. FNAB was supposedly omitted in most of these cases dueto the dense nature of the target lesion, but the decision ultimatelywas operator dependent.
Procedural MRI setup may be challenging, even cumbersome.All the equipment used must be MRI compatible. This applies to allinstruments and devices in the room, not only those in the hands ofthe performing physician. Instrument safety is one of the key issuesin interventional MRI. It is a fact that MRI compatible instrumenta-tion is relatively expensive. Although most of the major instrumentmanufacturers do have MRI compatible equipment for sale, noneseem to have a very large selection of instruments for interventionalMRI which in conjunction with the higher prices may discouragethe use of MRI guidance.
MRI guided biopsy is more expensive than CT guided biopsy[23], however it is probably cheaper and certainly less invasivethan open surgery. Ronkainen demonstrated that MRI guided ther-apeutic procedure is a financially viable alternative to surgery [24].Furthermore, those patients that are referred for MRI guided pro-cedures often have no other good options available as the lesionis either not visible or is otherwise less accessible by other means,surgery included.
4.1. Limitations of the study
We had a number (n = 42) of technically successfully acquiredsamples where the histologic and/or cytologic analysis led to eitherinterpretation uncertainty or to nonspecific histopathologic find-ings. This seemed to be clearly associated with benign lesions, suchas osteoid osteomas, osteoblastomas, hemangiomas, cystic bonelesions, osteochondritis dissecans-foci and infectious or inflamma-tory non-tumoural lesions where the representative tissue is eitheractually without any specific histopathologic findings or especiallydifficult to harvest adequately.
The target lesions were classified to reside either in the boneor in the soft tissue. However, a pathologic lesion in the bone canbe all but bone in structure. The density of the target lesion cannotalways be interpreted from MR-images, which among other things
led us to the classification used. Separating target lesions in thebone further to soft tissue lesions and bony lesions would lead todifferent results in this respect, but would not change the overallresult.
nal of
bvriaol
5
lsmpg
C
R
[
[
[
[
[[
[
[
[
[
[
[
[
[analysis of low-field (0.23 T) MRI- and CT-guided bone biopsies. Eur Radiol
P. Kerimaa et al. / European Jour
The study population was rather heterogeneous with respect toiopsy indications and suspected target lesion types. There were aery small number of malignant primary bone tumors, as these areare. This clinical setting is typical of that found in most tertiary carenstitutions. Referrals for musculoskeletal biopsies include a widerray of unspecific bone lesions depicted by MRI, CT, radiographyr ultrasound. MRI is the preferred guidance modality when theesion to be biopsied is occult on CT, fluoroscopy and US.
. Conclusion
We conclude that MRI guided percutaneous biopsy of muscu-oskeletal lesions is accurate and safe. Given its safety profile andimilar accuracy as other more commonly used biopsy guidanceodalities, it can be used to perform most biopsies and is clearly
referable in selected patients. Fine needle biopsy is an advanta-eous low-cost supplement to histologic biopsy.
onflict of interest
None.
eferences
[1] Ghelman B. Biopsies of the musculoskeletal system. Radiol Clin North Am1998;36(3):567–80.
[2] Tikkakoski T, Lahde S, Puranen J, Apaja-Sarkkinen M. Combined CT-guidedbiopsy and cytology in diagnosis of bony lesions. Acta Radiol 1992;33(3):225–9.
[3] Settle WJ, Ebraheim NA, Coombs R, Saunders RC, Jackson WT. CT-guided biopsyof metastatic sacral tumors. Orthopedics 1990;13(7):753–8.
[4] Jelinek JS, Kransdorf MJ, Gray R, Aboulafia AJ, Malawer MM. Percutaneoustranspedicular biopsy of vertebral body lesions. Spine 1996;21(17):2035–40.
[5] Leffler SG, Chew FS. CT-guided percutaneous biopsy of sclerotic bone lesions:diagnostic yield and accuracy. AJR 1999;172(5):1389–92.
[6] Joines MM, Motamedi K, Seeger LL, DiFiori JP. Musculoskeletal interventionalultrasound. Semin Musculoskelet Radiol 2007;11(2):192–8.
[7] Soudack M, Nachtigal A, Vladovski E, Brook O, Gaitini D. Sonographically guidedpercutaneous needle biopsy of soft tissue masses with histopathologic corre-lation. J Ultrasound Med 2006;25(10):1271–7.
[
Radiology 82 (2013) 2328– 2333 2333
[8] Loizides A, Widmann G, Freuis T, Peer S, Gruber H. Optimizing ultrasound-guided biopsy of musculoskeletal masses by application of an ultrasoundcontrast agent. Ultraschall Med 2011;32(3):307–10.
[9] Welker JA, Henshaw RM, Jelinek J, Shmookler BM, Malawer MM. The per-cutaneous needle biopsy is safe and recommended in the diagnosis ofmusculoskeletal masses. Cancer 2000;89(12):2677–86.
10] Buecker A, Adam G, Neuerburg JM, Glowinski A, van Vaals JJ, Guenther RW.MR-guided biopsy using a T2-weighted single-shot zoom imaging sequence(Local Look technique). J Magn Reson Imaging 1998;8(4):955–9.
11] Ojala R, Vahala E, Karppinen J, et al. Nerve root infiltration of the first sacralroot with MRI guidance. J Magn Reson Imaging 2000;12(4):556–61.
12] Adam G, Bucker A, Nolte-Ernsting C, Tacke J, Gunther RW. Interventional MRimaging: percutaneous abdominal and skeletal biopsies and drainages of theabdomen. Eur Radiol 1999;9(8):1471–8.
13] Hoane BR, Shields AF, Porter BA, Shulman HM. Detection of lymphoma-tous bone marrow involvement with magnetic resonance imaging. Blood1991;78(3):728–38.
14] Gehl HB, Frahm C. MRI-controlled biopsies. Radiologe 1998;38(3):194–9.15] Carrino JA, Khurana B, Ready JE, Silverman SG, Winalski CS. Magnetic resonance
imaging-guided percutaneous biopsy of musculoskeletal lesions. J Bone JointSurg Am 2007;89(10):2179–87.
16] Fraser-Hill MA, Renfrew DL, Hilsenrath PE. Percutaneous needle biopsy of mus-culoskeletal lesions. 2. Cost-effectiveness. AJR 1992;158(4):813–8.
17] Shin HJ, Amaral JG, Armstrong D, et al. Image-guided percutaneous biopsy ofmusculoskeletal lesions in children. Pediatr Radiol 2007;37(4):362–9.
18] Kaplan GR, Saifuddin A, Pringle JA, Noordeen MH, Mehta MH. Langerhans’cell histiocytosis of the spine: use of MRI in guiding biopsy. Skeletal Radiol1998;27(12):673–6.
19] Geirnaerdt MJ, Bloem JL, van der Woude HJ, Taminiau AH, Nooy MA, Hogen-doorn PC. Chondroblastic osteosarcoma: characterisation by gadolinium-enhanced MR imaging correlated with histopathology. Skeletal Radiol1998;27(3):145–53.
20] Abi-Jaoudeh N, Mielekamp P, Noordhoek N, et al. Cone-beam com-puted tomography fusion and navigation for real-time positron emissiontomography-guided biopsies and ablations: a feasibility study. J Vasc IntervRadiol 2012;23(6):737–43.
21] Blanco Sequeiros R, Klemola R, Ojala R, et al. MRI-guided trephine biopsy andfine-needle aspiration in the diagnosis of bone lesions in low-field (0.23 T) MRIsystem using optical instrument tracking. Eur Radiol 2002;12(4):830–5.
22] Neuerburg JM, Adam G, Buecker A, et al. MRI-guided biopsy of bone in a hybridsystem. J Magn Reson Imaging 1998;8(1):85–90.
23] Alanen J, Keski-Nisula L, Blanco-Sequeiros R, Tervonen O. Cost comparison
2004;14(1):123–8.24] Ronkainen J, Blanco Sequeiros R, Tervonen O. Cost comparison of low-field
(0.23 T) MRI-guided laser ablation and surgery in the treatment of osteoidosteoma. Eur Radiol 2006;16(12):2858–65.