Is extended and saturation biopsy necessary?
16
Review ArticleIs extended and saturation biopsy necessary? Vincenzo Scattoni, Carmen Maccagnano, Giuseppe Zanni, Diego Angiolilli, Marco Raber, Marco Roscigno, Patrizio Rigatti and Francesco Montorsi Department of Urology, University Vita-Salute, Scientific Institute San Raffaele, Milan, Italy Abstract: Prostate biopsy (PBx) techniques have significantly changed since the original Hodge’s ‘sextant scheme’, which should now be considered obsolete. The feasibility of carrying out a biopsy scheme with a high number of cores in an outpatient setting is a result of the great improvement and efficacy of local anesthesia. Peri-prostatic nerve block with lidocaine injection should be considered the ‘gold standard’ because it provides the best pain relief to patients undergoing PBx. The optimal extended protocol should now include the sextant template with an additional 4–6 cores directed laterally (anterior horn) to the base and medially to the apex. Saturation biopsies (i.e. template with 20 cores, including transition zone) should be carried out only when biopsies are repeated in patients where there is a high suspicion of prostate cancer. Complementary imaging methods (such as color- and power-Doppler imaging, with or without contrast enhancement, and elastography) could be used in order to increase the accuracy of biopsy and reduce the number of unnecessary procedures. Nevertheless, the routine use of these methods is still under evaluation. Key words: diagnosis transrectal ultrasound, prostate biopsy, prostatic neoplasms. Introduction Prostate biopsy (PBx) remains one of the most common procedures carried out in the urologist’s office today. It has evolved from the digitally guided transrectal biopsy, described by Astraldi in 1937, to the standard sextant biopsy method, described by Hodge et al. in 1989, with a prostate cancer (PCa) detection rate (DR) between 20% and 35%. 1,2 Over the past years, there has been rising interest in defining more accurate PBx schemes in order to improve PCa DR. Intuitively, this aim could be achieved by adding more biop- sies to prostatic areas not sampled by standard sextant schemes. 3,4 The introduction and refinement of effective local anesthesia has allowed an increase in the number of biopsies taken in the outpatient setting (from 10 to 18 or 20) without increasing the discomfort and pain of the patients. Thus, the concepts of ‘extended biopsy’ (EPBx; 10–12 cores) and ‘saturation biopsy’ (SPBx; 20 cores) have rapidly evolved in the past 10 years, radically changing the general idea of PBx. 5,6 Today, a PBx is not only a method to diagnose PCa, but it has become an informative method for an accurate morphological characterisation of PCa, leading to new follow-up and therapeutic perspectives. Anesthesia Traditional finger-guided PBx was carried out either without any anesthesia or under spinal or general anesthesia, depending on physician preferences. With the diffusion of transrectal ultrasound (TRUS) PBx, local anesthesia has been introduced, and it has been proved to be particularly effective. Nowadays, it is considered mandatory, and carrying out a PBx without anesthesia can be considered as ‘malpractice’, according to the international guidelines (Table 1 and Table 8). 3,7 Furthermore, without the introduc- tion of anesthesia, the diffusion of the EPBx and SPBx schemes should not have taken place. During the past few years, a radical improvement of anes- thetic techniques has become evident, with an increasing number of published trials (Table 2). Discomfort and pain during PBx are not only related to the number of cores; they partly derive both from the introduction and the movements of the TRUS probe into the rectum and they are partly caused by needle passage through the prostate capsule. 16,26–29 The available alternatives in anesthetic techniques in PBx are listed in Table 2. Peri-prostatic nerve block Several randomised studies have shown that the administra- tion of 1% or 2% lidocaine with peri-prostatic nerve block (PPNB) is the best form of pain control and comfort man- agement during TRUS PBx. It remains unclear which is the optimal dosage. A recent study using a placebo and six groups of escalating doses of 1% lidocaine (2.5, 5 and Correspondence: Vincenzo Scattoni MD, Department of Urology, University Vita-Salute, Scientific Institute H San Raf- faele, Via Olgettina 60, 20132 Milan, Italy. Email: [email protected] Received 11 November 2009; accepted 4 January 2010. International Journal of Urology (2010) 17, 432–449 doi: 10.1111/j.1442-2042.2010.02479.x, 10.1111/j.1442-2042.2010.02524.x 432 © 2010 The Japanese Urological Association
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Is extended and saturation biopsy necessary?

Review Articleiju_2479 432..449
Is extended and saturation biopsy necessary?Vincenzo Scattoni, Carmen Maccagnano, Giuseppe Zanni, Diego Angiolilli, Marco Raber,Marco Roscigno, Patrizio Rigatti and Francesco MontorsiDepartment of Urology, University Vita-Salute, Scientific Institute San Raffaele, Milan, Italy
Abstract: Prostate biopsy (PBx) techniques have significantly changed since the original Hodge’s ‘sextant scheme’,which should now be considered obsolete. The feasibility of carrying out a biopsy scheme with a high number of cores inan outpatient setting is a result of the great improvement and efficacy of local anesthesia. Peri-prostatic nerve block withlidocaine injection should be considered the ‘gold standard’ because it provides the best pain relief to patients undergoingPBx. The optimal extended protocol should now include the sextant template with an additional 4–6 cores directedlaterally (anterior horn) to the base and medially to the apex. Saturation biopsies (i.e. template with �20 cores, includingtransition zone) should be carried out only when biopsies are repeated in patients where there is a high suspicion ofprostate cancer. Complementary imaging methods (such as color- and power-Doppler imaging, with or without contrastenhancement, and elastography) could be used in order to increase the accuracy of biopsy and reduce the number ofunnecessary procedures. Nevertheless, the routine use of these methods is still under evaluation.
Key words: diagnosis transrectal ultrasound, prostate biopsy, prostatic neoplasms.
Introduction
Prostate biopsy (PBx) remains one of the most commonprocedures carried out in the urologist’s office today. It hasevolved from the digitally guided transrectal biopsy,described by Astraldi in 1937, to the standard sextant biopsymethod, described by Hodge et al. in 1989, with a prostatecancer (PCa) detection rate (DR) between 20% and 35%.1,2
Over the past years, there has been rising interest in definingmore accurate PBx schemes in order to improve PCa DR.Intuitively, this aim could be achieved by adding more biop-sies to prostatic areas not sampled by standard sextantschemes.3,4 The introduction and refinement of effectivelocal anesthesia has allowed an increase in the number ofbiopsies taken in the outpatient setting (from 10 to 18 or 20)without increasing the discomfort and pain of the patients.Thus, the concepts of ‘extended biopsy’ (EPBx; 10–12cores) and ‘saturation biopsy’ (SPBx; �20 cores) haverapidly evolved in the past 10 years, radically changing thegeneral idea of PBx.5,6 Today, a PBx is not only a method todiagnose PCa, but it has become an informative method foran accurate morphological characterisation of PCa, leadingto new follow-up and therapeutic perspectives.
Anesthesia
Traditional finger-guided PBx was carried out either withoutany anesthesia or under spinal or general anesthesia,depending on physician preferences. With the diffusion oftransrectal ultrasound (TRUS) PBx, local anesthesia hasbeen introduced, and it has been proved to be particularlyeffective. Nowadays, it is considered mandatory, andcarrying out a PBx without anesthesia can be considered as‘malpractice’, according to the international guidelines(Table 1 and Table 8).3,7 Furthermore, without the introduc-tion of anesthesia, the diffusion of the EPBx and SPBxschemes should not have taken place.
During the past few years, a radical improvement of anes-thetic techniques has become evident, with an increasingnumber of published trials (Table 2). Discomfort and painduring PBx are not only related to the number of cores; theypartly derive both from the introduction and the movementsof the TRUS probe into the rectum and they are partlycaused by needle passage through the prostate capsule.16,26–29
The available alternatives in anesthetic techniques in PBxare listed in Table 2.
Peri-prostatic nerve block
Several randomised studies have shown that the administra-tion of 1% or 2% lidocaine with peri-prostatic nerve block(PPNB) is the best form of pain control and comfort man-agement during TRUS PBx. It remains unclear which is theoptimal dosage. A recent study using a placebo and sixgroups of escalating doses of 1% lidocaine (2.5, 5 and
Correspondence: Vincenzo Scattoni MD, Department ofUrology, University Vita-Salute, Scientific Institute H San Raf-faele, Via Olgettina 60, 20132 Milan, Italy. Email:[email protected]
Received 11 November 2009; accepted 4 January 2010.
International Journal of Urology (2010) 17, 432–449 doi: 10.1111/j.1442-2042.2010.02479.x, 10.1111/j.1442-2042.2010.02524.x
432 © 2010 The Japanese Urological Association

Table 1 American Urology Association, European Association of urology and National Comprehensive Cancer Network 2009prostate biopsy guidelines
Topic American UrologyAssociation
European Associationof Urology
National Comprehensive CancerNetwork (early detection program)
Indication for initialbiopsy
• Based primarily on PSAand DRE results.
• The need for prostate biopsies should bedetermined on the basis of the PSA leveland/or a suspicious DRE.
• Positive DRE despite PSA values.
• It should take intoaccount multiple factors:
• PSA and PSA velocity:PSA <2.5 ng/mL and PSA velocity>0.35 ng/mL/y
Patient age• The patient’s biological age, potential
comorbidities (ASA Index and CharlsonComorbidity Index) and the therapeuticconsequences should also be considered.
PSA 2.6–4 ng/mLPSA velocity PSA >4 ng/mL and PSA velocity
>0.75 ng/mL/yPSA densityPSA 4–10 ng/mL or fPSA �10%PSA >10 ng/mL
Family history
• Prior biopsy history: 3–12 monthsafter the first biopsy and PSA>10 ng/mL
Ethnicity• The first elevated PSA level should not
prompt an immediate biopsy.
• Ethnicity (African American families)
Prior biopsy historyComorbidities
• Individualized riskassessment
• Biopsy carried outirrespective of a ‘normal’transrectal ultrasoundexamination
Anesthesia,regardless of thetechnique
• Mandatory • Ultrasound-guided peri-prostatic block isstate-of-the-art without any differencewhether the depot is apical or basal.
Both topical lidocaine gel andinjectable nerve block have beenshown to be safe and efficacious inreducing discomfort. Topicallidocaine was more efficacious inreducing pain during probeinsertion, whereas periprostaticinjection reduced pain during biopsyitself.
• Intrarectal instillation of a local anestheticis clearly inferior to peri-prostaticinfiltration.
For exceptional cases, intravenoussedation or general anaestheicmight be advantageous.
Biopsy approach • Transrectal,ultrasound-guidedprostate biopsy is themost common method.
• Transrectal, ultrasound-guided prostatebiopsy is the most common method.
Transrectal, ultrasound-guidedprostate biopsy is the most commonmethod.
• Transperineal biopsywith transrectalultrasound guidance isconsidered a validalternative.
• The ultrasound-guided perineal approachis a useful alternative in special situations,e.g. after rectal amputation.
Standard biopsy 8–12 cores targeting theperipheral zone at theapex, mid gland , andbase, as well as laterallydirected cores on eachside of the prostate.
• Sextant biopsy is no longer consideredadequate.
12-cores targeting the sextants (6) andthe lateral peripheral zone (6) and ,lesion-directed at palpable nodulesor suspicious imaging (extendedpattern).
• The sample sites should be as far posteriorand lateral in the peripheral gland aspossible.
Extended biopsy Additional tissue might betaken from the anteriorand transition zones ofthe prostate as well.
• Additional cores should be obtained fromsuspect areas by DRE/TRUS, chosen on anindividual basis.
An extended pattern 12-core biopsywith sextant and lateral peripheralzone and lesion-directed palpablenodules or suspicious image.• At a glandular volume of 30–40 mL, at
least eight cores should be sampled. Morethan 12 cores are not significantly moreconclusive.
Transition zonebiopsy
– Transition zone sampling during baselinebiopsies provides a very low detection rateand TZ sampling should therefore beconfined to repeat biopsies.
Transition zone biopsy is notsupported in routine biopsy.However, this can be added to anextended biopsy protocol in arepeat biopsy if PSA is persistentlyelevated.
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 433

10 mL) infiltration showed that the best pain reliefwas obtained with 10 mL of lidocaine infiltrated solely atthe neurovascular bundle region (single site), or to theneurovascular bundle and apical regions (double site).Therefore, the authors recommended single-site,10-mL infiltration in the region of the neurovascularbundle.21
Various infiltration sites have been described, includingthe apex only,18,24 bilateral neurovascular bundle regionsonly (defined variously as basolateral, posterolateral,periprostatic nerve plexus, prostate-vesicular junctioninjections),8–13,16–23 apex and neurovascular bundle,14 threelocations (base, mid and apex) posterolaterally14 and lateral
to the tip of the seminal vesicles.11,16,18 Most of the authorshave reported the best pain relief was obtained with 1%lidocaine 10 mL injected in the neurovascular bundle region(5 mL each side) (Table 2). Effective pain relief has alsobeen described with apical infiltration.14,18,24 The combina-tion of infiltration at both sites is still matter of debate, evenif some studies report that the combination seems to besuperior to PPNB alone in reducing pain during PBx.11,18
Recently, Ashley et al. have shown that mid and apical biop-sies of the prostate are more painful than base biopsies,whereas apical and intraprostatic blockades appear toprovide superior analgesia to the seminal vesical-prostaticbase blockade.24
Table 1 Continued
Topic American UrologyAssociation
European Associationof Urology
National Comprehensive CancerNetwork (early detection program)
Saturation biopsy Saturation biopsy, takingtissue from more than 20locations, might beconsidered in men withpersistently elevated PSAlevels and multipleprevious negativeprostate biopsies.
• The incidence of PCa Dr detected bysaturation repeat biopsy is 30–33% anddepends on the number of cores sampledduring earlier biopsies
In patients with two negative extendedbiopsies, yet persistently rising PSAvalues, a saturation biopsy might beconsidered.
• In special situations, saturation biopsymight be carried out with the transperinealtechnique. This will detect an additional38% of PCa. The high rate of urinaryretention (10%) is a drawback (3-Dstereotactic biopsy).
Repeat biopsy • Indications are: • Indications are:Rising and/or persistent PSA. Patients with prior negative
biopsies, yet persistently rising PSA.Suspicious DRE
Suspicious DRE.ASAP• The optimal timing depends on the
histological outcome of the baseline ASAPbiopsy and the index of a persistentsuspicion of PCa.
• Yield are highest in the laterallydirected cores and the apical cores,including the anterior apical horn.
• The later the repeat biopsy is done, thehigher the detection rate (21).
Previous ASAP andHGPIN diagnosis
• HGPIN is no longer considered anindication for re-biopsy.
• HGPIN. Extended repeat biopsy,including transition zone isindicated if HGPIN is found on TRUSguided biopsy of less than 10 cores.
• Only If PIN is extensive this could be areason for early re-biopsy.
• ASAP. Extended pattern re-biopsy(within 3 months) with increasedsampling of atypia site and adjacentarea is recommended.
• ASAP patients have to undergo repeatbiopsy.
The optimal timing depends on thehistological outcome of the baseline ASAPbiopsy and the index of a persistentsuspicion of PCa.
Doppler imaging role Color Doppler ultrasoundhas been shown to havethe potential forimproving biopsytargeting, but, like grayscale, does not substitutefor a biopsy.
ASA, American Scientific Affiliation; ASAP, atypical small acinar proliferation; DRE, digital rectal examination; fPSA, free prostate-specific antigen;HGPIN, high-grade prostatic intraepithelial neoplasia; PCa, prostate cancer, PIN, intraepithelial neoplasia; PSA, prostate-specific antigen; TRUS,transrectal ultrasound; TZ, transition zone.
V SCATTONI ET AL.
434 © 2010 The Japanese Urological Association

Table 2 Literature review of recent news on anaesthetic techniques in prostate biopsies (2007–2009)
Author Year andjournal
No. pts Anesthetic technique Site of injection in PPNB Conclusion
Yurdakul8 Urol Int 2009 100 Group 1: 25 pts, no local anesthesia Periprostatic IRLA and PPBN have granted bestpain control, independently ofused drug.
Group 2: 25 pts, IRLA with 2% lidocaine gel.Group 3: 25 pts, IRLA with 2% lidocaine gel
PPBN with 5 mL bupivacaine (0.25%).Group 4: 25 pts, IRLA with 2% lidocaine gel
and PPBN 5-mL ropivacaine injection(0.25%).
Ingber9 Int Urol Nephrol2009
50 Group 1: 25 pts, placebo (0.9% salinesolution).
Region between the prostateand the seminal vesiclesjunction laterally near thevascular pedicle.
No significant pain improvementusing PPNB. Pain is welltolerated with no anesthesia.Group 2: 25 pts, PPBN with 1% lidocaine.
MontoliuGarcia10
Arch Espan Urol2009
80 Group 1: 40 pts, intravenous analgesia andIRLA with 12.5 g lidocaine gel.
Intracapsular The injection of intracapsularlidocaine improved toleranceand diminished the painGroup 2: 40 pts, intravenous analgesia and
IRLA with 12.5 g of lidocaine gel andintracapsular injection of 8 mL of 2%lidocaine .
Bingqian11 J Urol 2009 200 Group 1: 100 pts, PPNB and intraprostaticlocal anesthesia with 5 mL 2% lidocaine.
Region of the prostatic vascularpedicle at the prostate basejust lateral to the junctionbetween the seminal vesicleand prostate on each side.
Combining PPNB andintraprostatic local anesthesiaprovided significantly betterpain control than PPNB. Thecombination might be ofmaximum benefit in patientswith a prostate volume �48 mLor younger patients(�66 years).
Group 2: 100 pts PPNB and intraprostaticlocal anesthesia with 5 mL 0.9% NaCl.
Group 3: 100 pts, no anesthesia.
Luján Marco12 Actas UrolEspan 2009
100 Group 1: 50 pts, intravenous meperidine50 mg.
Angle between prostate andseminal vesicles.
Periprostatic plexus blocked withlidocaine does not offeradvantages in respect tomeperidine.
Group 2: 50 pts: PPNB 5 mL lidocaine 2%.
Skriapas13 Minerva UrolNephrol 2009
147 Group 1: 74 pts, IRLA with lidocaine cream2% and PPNB.
Periprostatic IRLA with lidocaine cream 2%significantly reduced analdiscomfort and pain before theprobe insertion for ultrasoundguided biopsies in youngpatients.
Group 2: 73 pts, lubricant gel and PPNB.
Visapää14 Scand J Surg2009
50 Group 1: 25 pts, PPNB with 1% lidocaine andparacetamol 500 mg and codeine 30 mgorally.
Four locations: lateral to theseminal vesicles and apicallyon both sides.
The combination of oralparacetamol, codeine andPPNB significantly relievedbiopsy-related pain.Group 2: 25 pts, PPNB with 1% lidocaine no
oral analgesics.Kandirali15 Urol Int 2009 80 Group 1: 20 pts, no anesthesia. – Perianal anesthesia with
lidocaine-prilocaine creammight solely be sufficient todecrease the pain duringprostate biopsy.
Group 2: 20 pts, 5 mL lidocaine-prilocainecream perianally administered.
Group 3: 20 pts, IRLA with 5 mLlidocaine-prilocaine cream.
Group 4: 20 pts, lidocaine-prilocaine creamperianally and IRLA.
Giannarini16 J Urol 2009 280 Group 1: 70 pts. combinedperianal-intrarectal lidocaine-prilocainecream and 1% lidocaine PPNB.
Area just lateral to the junctionbetween seminal vesicles andthe prostate base, 5 mL pereach side.
The combination ofperianal-intrarectallidocaine-prilocaine cream andPPNB provided better paincontrol than the 2 modalitiesalone. The magnitude of thiseffect is higher in younger men(�65 years), men with aprostate volume �49 mLand men with lower anorectalcompliance.
Group 2: 70 pts, perianal-intrarectallidocaine-prilocaine cream alone.
Group 3: 70 pts, 1% lidocaine PPNB alone.Group 4: 70 pts, no anesthesia.
Cantiello17 BJU Int 2009 200 Group 1: 100 pts, PPNB with solution of 5 mLlidocaine 1% and naropine 0.75% alone.
Into the neurovascular bundlesat the seminal vesicle-bladder-rectum angle oneither side (5 mL per eachside).
Antrolin placed with PPNBhas been better than PNB alonein reducing pain and discomfortGroup 2: 100 pts, previous administration of
the topical anesthetic Antrolin and PPNBwith solution of 5 mL lidocaine 1% andnaropine 0.75% alone.
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 435

Intra-rectal local anesthesia withlidocaine gelIn several randomised studies, the administration oflidocaine gel versus simple lubricant gel has lead to
controversial results.30,31 Nevertheless, recent trials andTiong’s meta-analysis have shown that intra-rectal localanesthesia, intrarectal local anesthetic (IRLA) alone hasappeared to be inferior to PPNB.32–37
Table 2 Continued
Author Year andjournal
No. pts Anesthetic technique Site of injection in PPNB Conclusion
Akan18 Urology 2009 117 Group 1: 60 pts, PPNB with 5 mL lidocaine. Group 1: Region just lateral tothe junction between thebase of the prostate and theseminal vesicles on bothsides (2.5 mL per each side).
The single apical injection and thebilateral basal injectiontechniques are both effective interms of pain prevention. Themain advantage of the singleapical injection technique is itsease of use and therequirement for one half theamount of local anestheticagent.
Group 2: 57 pts, PPNB 5 mL lidocaine in thesingle apical injection.
Group 2: apex of the prostate toprovide the distribution oflidocaine toward the base ofthe prostate underDenonvilliers fascia.
Cam19 J Urol 2008 200 Group 1: 100 pts, PPNB with 1% lidocaineand intraprostatic lidocaine injection.
Region of the prostatic vascularpedicle at the prostate basejust lateral to the junctionbetween the seminal vesicleand prostate
Adding intraprostatic localanesthesia has provided asignificantly efficient strategy.Group 2: 100 pts, PPNB with 1% lidocaine
and injection of 0.9% NaCl.
Szlauer20 Urol Int 2008 100 Group 1: 25 pts, a suppository containing60 mg of lidocaine 2 h before biopsy.
Periprostatic All lidocaine suppositories haveshown a good analgesic effectalthough a significantly betterpain reduction was achieved byPPNB
Group 2: 25 pts, a 120-mg lidocainesuppository 1 h before biopsy
Group 3: 25 pts, a 120-mg lidocainesuppository 2 h before biopsy
Group 4: 25 pts, PPNB with 5 mL 2%lidocaine
Bhomi21 Urol Int 2007 120 Group 1: 20 pts, no anesthesia. Periprostatic PPNB with 1% lidocainesignificantly decreases painassociated with prostate biopsywhen compared with controland intramuscular diclofenac.
Group 2: 20 pts, intramuscular injection ofdiclofenac sodium.
Group 3: PPNB with 1% lidocaine.
Inal22 Int Urol Nephrol2008
159 Group 1: 64 pts, no anesthesia. Region of the neurovascularbundle and the needle waswithdrawn slowly from thebase of the prostate to theapex.
Using IRLA and PPNB or solelyunilateral pudendal nerve blockhas provided efficient patientcomfort by reducing pain bothduring probe insertion andneedle passing through theprostate gland.
Group 2: 34 pts, PPNB with 3 mL 1%lidocaine.
Group 3: 26 pts, unilateral pudendal nerveblockade.
Group 4: 20 pts, IRLA with lidocaine gel.Group 5: 15 pts; IRLA with lidocaine gel and
PPNB with 3 mL 1% lidocaine.Raber23 Eur Urol 2008 300 Group 1: PPNB with 2% lidocaine. The neurovascular bundle at the
seminal vesicle base on eachside.
Combined prilocaine-lidocainecream topically placed withPPNB is superior to PPNB aloneand might be of maximumbenefit for younger patients(mean: 60 years).
Group 2: topical anesthesia of the anal ring,anal canal, and anterior rectal wallcombined with PPNB
Group 3: Placebo
Ashley24 Cancer 2007 243 PPNB with 1% lidocaine in all groups. Group 1: seminalvesical-prostatic baseblockade
The seminal vesicle-prostatic baseblockade is less effective thanintraprostatic and apical-rectalblockade at controlling pain.Group 2: intraprostatic blockade
Group 3: apical-rectal blockadeLee25 J Urol 2007 152 Group 1: 41 pts, intraprostatic local
anesthesia into the right and left sideswith a total of 2 mL 1% lidocaine and aPPNB injection of 2 mL saline later.
Intraprostatic anaesthesia: into2 sites of the right and leftsides of the prostate at thebase.
A combination of intracapsularanesthesia and PPNB is aneffective and useful techniquethat is well tolerated by thepatient. It decreases the levelof pain and discomfortassociated with the prostaticbiopsy procedure.
Group 2: 49 pts, intraprostatic injection of2 mL saline, followed by PPNB with 2 mL1% lidocaine.
PPBN: region of the prostaticvascular pedicle at the baseof the prostate just lateral tothe junction between theprostate and seminal vesicles.
Group 3: 62 pts, intraprostatic and PPNBwith 2 mL 1% lidocaine.
IRLA, intrarectal local anesthetic; PPNB, peri-prostatic nerve block; pts, patients.
V SCATTONI ET AL.
436 © 2010 The Japanese Urological Association
Association of PPNB with IRLA
Different studies have reported that the association of IRLAwith lidocaine gel and PPNB was superior to PPNB alone inrelieving PBx-related pain by reducing discomfort duringthe introduction of a TRUS probe and peri-prostatic infil-tration. The patients who better benefit from this associationof anesthesia are younger men (�65 years), or patients withlower anorectal compliance (because of haemorrhoids oranal strictures).8,11,13,16,23 The correlation between this benefitand prostate volume is still controversial; Binqian et al.found a direct correlation between prostate volume �49 mLand pain relief during PBx. Giannarini et al. reported theopposite situation; the larger the prostate volume (�49 mL),the bigger advantage in pain control.11,16
There is an increasing interest in experimenting withalternative gels when carrying out IRLA in combinationwith PPNB. In a recent published trial, Cantiello et al.described the intrarectal use of a cream that is a mixture of1.5% lidocaine and 0.3% nifedipine (Antroline; Bracco,Milan, Italy). The authors have reported a reduction ofpain perception during probe insertion 30 min afterPBx, without general or local side-effects or majorcomplications.17
Association of PPNB with oral medications
Diclofenac,38 rofecoxib,39 tramadol,40,41 paracetamol andopioids42 have been proposed and have shown to grant asignificant decrease in pain during the procedure withoutcausing any additional complications.
Despite the variability of location and dosage of infiltra-tion, PPBN with lidocaine is actually the ‘gold standard’ thatgrants comfort and no pain for patients undergoing PBx.
The association with IRLA or oral medication with PPNBis still controversial, even if there are now several trials thatshow the importance of controlling discomfort caused byTRUS probe insertion achieved by IRLA administration.
Prostate biopsy strategy in theinitial setting
Extended biopsy
Since the diffusion of the sextant scheme, several authorshave shown the limitations of PCa detection by 6-corebiopsy and have reported high rates of false negative biop-sies. Over the past few years, there has been increasinginterest in defining more accurate PBx schemes in order toincrease PCa DR and different prostatic schemes with 8, 10or 12 biopsies, the so called extended biopsy (EPBx), havebeen proposed as a new standard of reference.43 Differentauthors have reported that taking more than six cores mightincrease the PCa DR of approximately 5–30%.44–50 Asdefined by the National Comprehensive Cancer Network, an
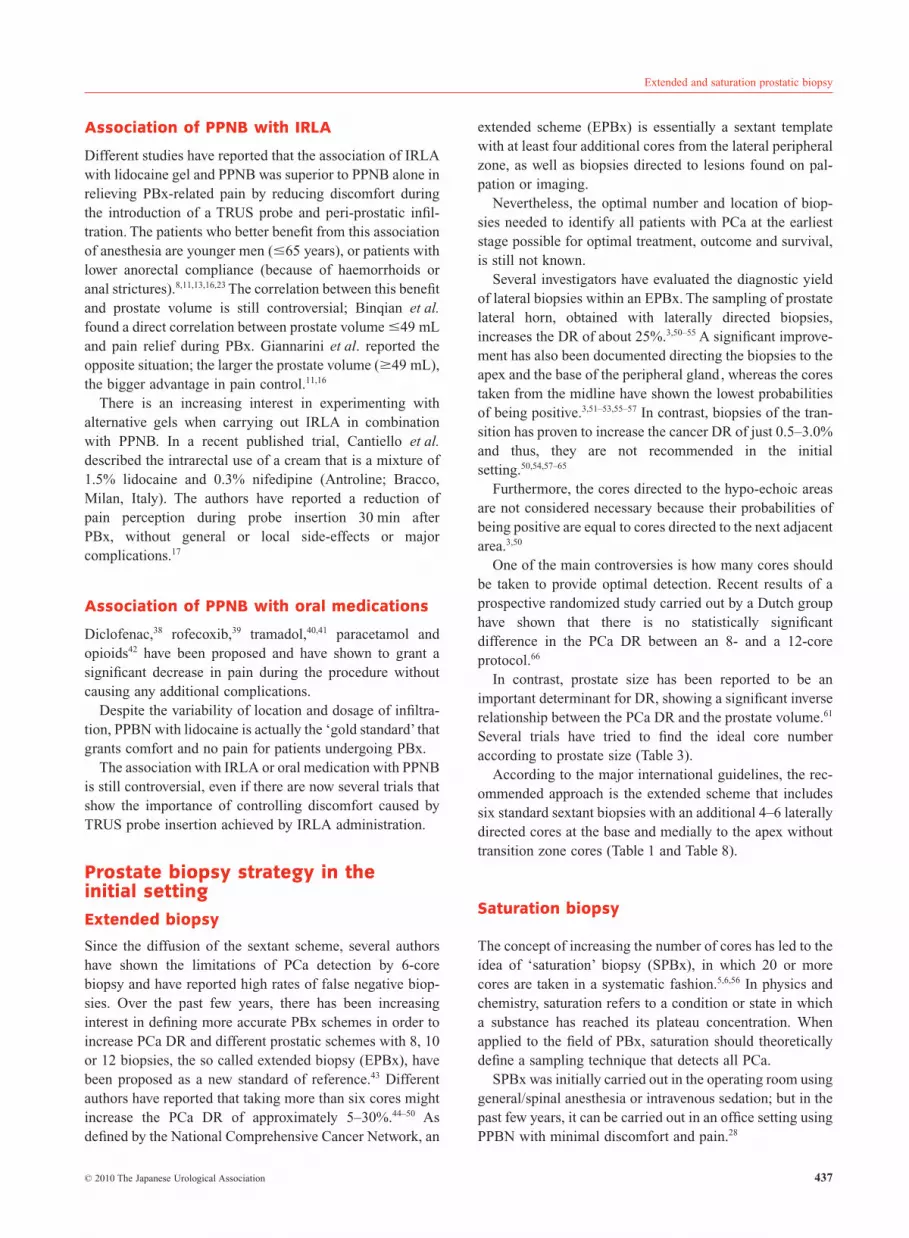
extended scheme (EPBx) is essentially a sextant templatewith at least four additional cores from the lateral peripheralzone, as well as biopsies directed to lesions found on pal-pation or imaging.
Nevertheless, the optimal number and location of biop-sies needed to identify all patients with PCa at the earlieststage possible for optimal treatment, outcome and survival,is still not known.
Several investigators have evaluated the diagnostic yieldof lateral biopsies within an EPBx. The sampling of prostatelateral horn, obtained with laterally directed biopsies,increases the DR of about 25%.3,50–55 A significant improve-ment has also been documented directing the biopsies to theapex and the base of the peripheral gland, whereas the corestaken from the midline have shown the lowest probabilitiesof being positive.3,51–53,55–57 In contrast, biopsies of the tran-sition has proven to increase the cancer DR of just 0.5–3.0%and thus, they are not recommended in the initialsetting.50,54,57–65
Furthermore, the cores directed to the hypo-echoic areasare not considered necessary because their probabilities ofbeing positive are equal to cores directed to the next adjacentarea.3,50
One of the main controversies is how many cores shouldbe taken to provide optimal detection. Recent results of aprospective randomized study carried out by a Dutch grouphave shown that there is no statistically significantdifference in the PCa DR between an 8- and a 12-coreprotocol.66
In contrast, prostate size has been reported to be animportant determinant for DR, showing a significant inverserelationship between the PCa DR and the prostate volume.61
Several trials have tried to find the ideal core numberaccording to prostate size (Table 3).
According to the major international guidelines, the rec-ommended approach is the extended scheme that includessix standard sextant biopsies with an additional 4–6 laterallydirected cores at the base and medially to the apex withouttransition zone cores (Table 1 and Table 8).
Saturation biopsy
The concept of increasing the number of cores has led to theidea of ‘saturation’ biopsy (SPBx), in which 20 or morecores are taken in a systematic fashion.5,6,56 In physics andchemistry, saturation refers to a condition or state in whicha substance has reached its plateau concentration. Whenapplied to the field of PBx, saturation should theoreticallydefine a sampling technique that detects all PCa.
SPBx was initially carried out in the operating room usinggeneral/spinal anesthesia or intravenous sedation; but in thepast few years, it can be carried out in an office setting usingPPBN with minimal discomfort and pain.28
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 437

The number of cores for SPBx has varied widely in pub-lished studies, with a range from 23 to 24 to as great as 139cores, as it has been recently reported (Table 4). Despiteseveral investigators having tried to optimize the number ofcores in a single patient, Eichler et al. have shown that nosignificant benefit accrues by taking >12 cores, and Joneset al.47 have suggested that further efforts at EPBx strategiesbeyond 10–12 cores are not appropriate in the initial set-ting.43,47 More recently, Pepe et al. have reported in a retro-spective study that SPBx (range 24–37 cores) does notincrease the PCa DR compared with an 18-core scheme inthe initial setting.13 Descazeaud et al. have reported that theDR of their 21-core biopsy protocol was similar to their 10-to 12-core biopsy scheme as an initial biopsy strategy.44
Recently, Delongchamps et al. have evaluated SPBx (36cores) on autopsied prostates for detecting PCa.45 They con-cluded that the DR of the SPBx protocol was not increasedover an 18-core regimen.45 In a large retrospective study, wehave previously shown that an initial 18-core PBx did notimprove the overall prostate cancer DR compared with a12-core PBx (39.9% vs 38.4%, P = 0.37).46 Furthermore,Lane et al. have shown that the false negative rate on sub-sequent PBx after initial SPBx is equivalent to that aftertraditional PBx.67
In contrast, Guichard et al. have carried out a SPBx (21cores) as their initial PBx in 1000 patients including sextantbiopsies, three additional posterolateral biopsies in eachperipheral zone, three biopsies in each transition zone and
three biopsies in the midline peripheral zone.68 They foundan improvement, although not statistically significant, in theDR when increasing from 12 to 18 or 21 cores (improve-ment of cancer detected of approximately 7%, with anincrease of cancer DR of 2.8%).68
The present study group has recently carried out SPBx inthe initial setting and we have tried to identify the mostadvantageous PBx scheme, defined as the combination ofsampling sites that detected the 95% of all cancers with theminimal number of biopsy cores. We have reported that,despite the fact that the mean cancer DR significantlyincreased with an increasing number of cores, the cancer DRvaried significantly according to the different combinationof sites considered at a given number of cores. Thus, weproposed a user-friendly flow chart to identify the mostadvantageous set of sampling sites, according to patients’characteristics. The analysis showed that the most advanta-geous scheme for patients who were digital rectal examina-tion (DRE) negative, had a prostate volume �60 and aged�65 years was a combination of a 16-core biopsy. Forpatients who were DRE negative, had a prostate volume�60 and aged >65 years or were DRE negative and had aprostate volume >60, two different combinations of a14-core biopsy were the most advantageous. Finally, thesampling that detects 95% of cancers in patients who wereDRE positive was a combination of a 10-core biopsy.82
In conclusion, there is sufficient evidence in the literaturethat SPBx is not necessary in the initial setting and an
Table 3 Relationship between prostate size and number of cores in extended schemes
Author Journal and publication year Prostate size (cc) No. cores recommended
de la Taille52 Urology 2003 �40 �12–14Ficarra62 Eur Urol 2005 �30 8
>30 �12–14Inahara63 Urology 2006 �30 8
�35 12Damiano64 Prostate Cancer Prostatic Dis 2006 �50 8–14
�51 �14
Table 4 Comparison of trials with baseline saturation biopsy (2006–2009)
Author Year No. patients No. cores PCa DR (%)
Jones65 J Urol 2006 139 24 44.6Guichard68 Eur Urol 2007 1000 21 42.5Lane67 J Urol 2008 257 24 42.8Simon82 BJU Int 2008 40 139 45Scattoni69 Eur Urol 2009 617 24 46.8
PCa DR, prostate cancer detection rate.
V SCATTONI ET AL.
438 © 2010 The Japanese Urological Association

individualized approach might optimize cancer DR in asingle patient (Table 8).
Repeat biopsy strategy
Patients with a prior negative PBx but with a persistentsuspicion of PCa on the basis of DRE findings, repeatedprostate-specific antigen (PSA) measurements (such as freePSA percentage, complex PSA, PSA density, PSA velocity)and patients with suspicious histological findings, such asatypical small acinar proliferation and high-grade prostaticintraepithelial neoplasia, should be considered for arepeated biopsy. Based on the findings that even initial10–12 core biopsy schemes miss almost one-third ofcancers, a SPBx has been used to improve PCa DR. It hasbeen reported by different authors that office-based SPBxincreases the DR of PCa in patients with suspicious clinicalfindings after previous negative standard PBx, comparedwith repeat standard biopsy strategies using up to 12 cores.The PCa DR of repeat SPBx has been reported to beapproximately 30%, regardless of the type of previousbiopsy scheme (Table 5).70–77
Furthermore, SPBx might be carried out in patients whoareccandidates for an active surveillance protocol. In fact,SPBx have proved to lead to a more accurate assessment ofthe extent and grade of PCa than traditional sextant biopsy.SPBx have also been proven to be useful when focal therapyis considered.47,78–81
In conclusion, although SPBx has not been shown bebeneficial in men as an initial biopsy strategy, it provides anaccurate prediction of prostate tumor volume and grade, andclearly improves cancer detection if clinical suspicion per-sists after a previous biopsy with negative findings.56,78–82
According to international guidelines, SPBx is now stronglyrecommended in all situations of repeated setting (Table 1and Table 8).
Transperineal approach
Before the 1980s, digital rectal examination or transperinealTRUS PBx was the main method of diagnosing PCa(Table 8).83–88 Nowadays, in the USA the transperineal
approach is uncommon and used by 2% of urologists,whereas it is more common in European and Asiancountries.89
The transperineal and transrectal approach have beenshown to be equivalent in PCa DR when the same numberof cores were used, as shown by Emiliozzi, Watanabe andKawakami, and according to international guidelines(Table 1).90–92 However, in the 2000s, several authorsreported fewer complications and a greater PCa DR usinga transperineal approach. This probably depends on thefact that the biopsy needle enters the prostate apex in alongitudinal direction, allowing efficient sampling of theprostate peripheral zone. Thus, with the help of templates,the direction of the biopsy gun can be controlled andsamples are uniformly distributed in the whole prostate.Recently, there has been rising interest in taking trans-perineal biopsies, through a brachytherapy grid , in order tosaturate the entire gland.94,95 Li et al. have recently carriedout an 11-region template guided transperineal SPBx,obtaining a mean of 23.7 cores. The authors concludedthat the transperineal ultrasound-guided SPBx is safeand feasible, and provides an encouraging cancerDR.96
Different authors have also carried out a scheme with thecombination of transrectal and transperineal 6-core PBx,simultaneously. They have shown that the two approachescombined were better than a single approach.91–93 Geometricconsiderations would dictate that the apex and the anteriorregion of the prostate are best sampled through the trans-perineal route, whereas the base is best sampled using thetransrectal approach. Even if this combination provides ahigh DR, it is not recommended because it requires hospi-talization and major anesthesia.
The role of new imaging methods
The diffusion of EPBx and SPBx is due to the fact thatstandard gray-scale TRUS technology has limited specificityand sensitivity to detect prostate cancer that is isoechoic andnot distinguishable from normal tissue.3 This situation hasled to the development of a new imaging technique suitablefor TRUS, based on neo-angiogenesis in cancer foci.
Table 5 Comparison of trials with saturation biopsy as repeat biopsy (2006–2009)
Author Year No. patients Mean/median PSA,ng/mL
No. cores PCa DR
Walz76 Eur Urol 2006 161 9.4 24.2 41Jones65 J Urol 2006 139 6.3 24 44.6Lane67 J Urol 2008 59 5.5 24 24
PCa DR, prostate cancer detection rate, PSA, prostate-specific antigen.
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 439

Doppler imaging
Based on the fact that PCa tissue is associated with anincreased density of small and uniform microvessels,several investigators have tried to use Doppler (CDUS) andPower Doppler imaging (PDI) with the aim of increasing theaccuracy of prostate TRUS.97–104 Both of the techniques aregenerally able to identify neovascular foci. CDUS imagingcan also show an increased number of visualized vessels aswell as an increase in flow rate, size and irregularity ofvessels with diffuse flow within PCa lesions greater than5 mm in size, especially in isoechoic tumors.97,105 Unfortu-nately, later studies have shown that the sensitivityand specificity of CDUS for diagnosing PCa mightsignificantly vary and range between 49–87% and 38–93%,respectively.106
PDI is nowadays considered the next generation ofDoppler imaging, because of its increased sensitivity forindividuating small, low flow blood vessels. Halpern et al.have studied the value of gray scale, CDUS and PDI for PCadetection; they concluded that PDI might be useful for tar-geting biopsies when the number of biopsy passes must belimited, but there is no substantial advantage of PDI overCDUS.107 Remzi et al. have recently reported the high nega-tive predictive value of PDI, with the aim of reducing thenumber of unnecessary biopsies.108 As shown by interna-tional guidelines, Doppler ultrasound (US) has been shownto have the potential for improving biopsy targeting, but,like gray scale, is not a substitute for a biopsy (Table 1 andTable 8).
Contrast-enhancement ultrasound
Ultrasound contrast agents are made of different gasmicrobubbles, encapsulated in hard or soft shells that aresmall enough to cross through capillary beds, where theypersist until they dissolve. They are many times morereflective than blood, thus improving flow detection. Fur-thermore, their vibrations generate higher harmonics to amuch greater degree than surrounding tissues and they canbe detected by the probe. Thus, newly developed US con-trast agents are able to delineate the neo-vascularanatomy of PCa foci by enhancing the signal strength fromneovessels.105
Frauscher et al. have reported a sensitivity of 53%, aspecificity of 72% and a positive predictive value of 70% indistinguishing PCa from a benign lesion.109 Bogers et al.have evaluated contrast enhanced 3-D TRUS imaging ofthe prostate vasculature with power Doppler before andafter intravenous administration of US contrast agent.110
Enhanced images have shown a sensitivity of 85% and aspecificity of 85%, allowing scheduling for PBx. A morerecent analysis by the same group has reported that a 3-Dcontrast-enhanced power Doppler ultrasound is a better
diagnostic tool than DRE, PSA level, gray scale US and PDIUS alone. The most suitable diagnostic predictor for PCawas a combination of 3-D contrast enhanced, powerDoppler US and PSA level.111
A new approach to the contrast enhanced imaging of theprostate is phase-inversion, or pulse-inversion technology, touse the non linear behaviour of the bubbles in order todifferentiate blood flow echoes from background tissue withhigh contrast, spatial resolution.112 In a preliminary report,Halpern et al. have shown the usefulness of intermittentcontrast-enhanced ultrasound to obtain selective enhance-ment of malignant tissue.113
The same group have described that contrast enhancedTRUS might improve sensitivity for PCa detection withoutsubstantial loss of specificity.114 They have also reported inanother study that PCa DR of contrast enhanced targetedcore is significantly higher when compared with sextantcores.115
At present, contrast enhanced TRUS is the most promis-ing method that might help to discriminate between benignand malignant tissue, and that might allow target biopsieswith a high cancer DR to be carried out. Nevertheless, thetechnique alone is not sufficient to predict which patient hasbenign versus malignant disease (Table 8).
Elastography
Real-time elastography (RTE) is a new imaging modality ofPCA detection. The differences in tissue stiffness, producedby compression and relaxation of the tissue, can be visual-ized under real-time conditions, as first described by Ophiret al., with a mean sensitivity of approximately 80%.116,117
Thus, several investigators have used RTE as a tool tosupport TRUS-guided PBx. Konig et al. have reported PCaDR enhanced up to 84% in comparison to only 64% withconventional diagnostic modalities.118 The same Austriangroup have reported that, even if the overall PCa DR bypatient was not significantly better than for systematic PBx,RTE targeted biopsy in men with PCa was 2.9-fold morelikely to detect PCa than PBx. Thus, RTE seems to have thepotential to decrease TRUS-guided biopsy cores.119
The major limitation of this technique is the dependenceon the physician’s experience and on the pressure applied onthe probe. This limitation can be decreased using the strainratio, that is, a cut-off value for prostate lesion to achievehigh specificity, sensitivity and accuracy in the differentia-tion between a benign and malignant lesion. Another limi-tation is that benign prostatic hyperplasia and chronicprostatitis mimic hard tissue and can lead to false negativeresults.117
The published trials have shown promising results of RTEin PCa imaging and detection, especially in conjunctionwith TRUS, in order to reduce the number of cores. Never-theless, further clinical studies are necessary (Table 8).
V SCATTONI ET AL.
440 © 2010 The Japanese Urological Association

Pathological issues
In the past few years, pathologists have made considerableefforts to improve their approach in prostate tissue process-ing and reporting, being faced every day with samplessmaller and smaller, and located in areas of the prostate notroutinely sampled. Nowadays, pathologists closely reportnot only the Gleason score of the cancer detected, but alsothe amount of cancer involved in each core.
The use of EPBx has proven to be beneficial in the pre-treatment decision-making process because an increasednumber of biopsies increase the Gleason concordance. SanFrancisco et al.120 have reported an improvement in the con-cordance rate from 63% to 72%. Mian et al.121 have reportedthat the rate of upgrading to a worsening risk category wassignificantly reduced with EPBx. Numao et al.122 haverecently reported that a 26-core systematic biopsy can moreaccurately predict the presence of Gleason pattern 4/5 onsurgical specimens compared with transrectal 12-PBx. Dif-ferent authors have shown that, with more EPBx, the risk ofsignificant upgrading decreases because of higher samplingdensity and more accurate pathological biopsyevaluation.70,122–124
Until recently, the Gleason score was considered as one ofthe most important parameters for predicting the response ofthe PCa to treatment and the patient’s post-therapy diseasecourse, besides the preoperative increase in serum PSAlevels and tumor stage.125,126 Nevertheless, in the era of PSAscreening, it is losing its prognostic value because PCa isdiagnosed at such a low PSA level.127 In this scenario, thequantitative histological features of the cores have gainedimportance as predictive factors for prostate cancer(Table 6). The extent of involvement of needle cores ofprostatic adenocarcinoma has been shown to correlate(albeit not perfectly) with the Gleason score, pathologicalstage, surgical margins, but especially, with tumor vol-ume.120,123 As the number of positive cores and the amount oftumor per core increase, the larger the tumor volume islikely to be. It is easy to understand why EPBx and SPBxmight be necessary in the different settings to provide acorrect diagnosis and evaluation of the prostate cancer thathas been detected125–133 (Table 7).
Conclusion
The course of PBx has changed significantly from randombiopsies to systematic, extended and SPBx schemes. Thesextant biopsy is now considered to be obsolete in favour ofEPBx and SPBx. Nevertheless, despite the number of pub-lished trials, the issue about the number and location of thecores is still a matter of debate. In future, with the develop-ment of new imaging methods that allow targeted biopsies tobe carried out, the role of EPBx and SPBx will probably bereconsidered. At present, EPBx is sufficient to provideadequate diagnosis and prostate cancer characterisation inthe initial setting, whereas SPBx seems to be necessary inmen with persistent suspicion of PCa after negative initialbiopsy and in active surveillance protocols.
Table 6 Quantitative histological features obtained whencarrying out prostate biopsies
• Location of PCa (unilateral or bilateral)• Presence of PCa in both lateral margins of the gland• Total number of positive cores• Greatest percentage of any single core involved by PCa• Total percentage of cancer and Gleason score
PCa, prostate cancer.
Table 7 Quantitative and qualitative histology report
• Each core reported individually• Number and total length of all cores• Number and location of cores with cancer (calculate percentage of biopsy cores involved with cancer: number of involved
cores/total cores as percentage)• Total length of biopsy cores involved with cancer
Calculate percentage of biopsy cores involved with cancer: millimetres involved cores/total length of cores in millimetresExclude those <1 cm and those without epithelial component
• Tumor length in all cores (calculate total tumor length divided by total length of core multiplied by 100, i.e. overallpercentage of cancer in all biopsies)
• Number of cores with peri-neural invasion (extent: focal vs multifocal) and calibre of nerve bundles• Number of cores with lympho-vascular invasion• Gleason score of each core with cancer• Number and location of cores with atypical glands, suspicious for cancer• High-grade prostatic intraepithelial neoplasia: extent and location
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 441

References
1 Astraldi A. Diagnosis of cancer of the prostate: biopsy byrectal route. Urol. Cutan Rev. 1937; 41: 421.
2 Hodge KK, McNeal JE, Terris MK, Stamey TA. Randomsystematic versus directed ultrasound guided trans-rectalcore biopsies of the prostate. J. Urol. 1989; 142: 71–4,discussion 74–5.
3 Scattoni V, Zlotta S, Montironi R, Schulman C, Rigatti P,Montorsi F. Extended and saturation prostatic biopsy inthe diagnosis and characterisation of prostate cancer: acritical analysis of the literature. Eur. Urol. 2007; 52:1309–22.
4 Shariat SF, Roehrborn CG. Using biopsy to detectprostate cancer. Rev. Urol. 2008; 10: 262–79.
5 Stewart CS, Leibovich BC, Weaver AL, Lieber MM.Prostate cancer diagnosis using a saturationneedle biopsy technique after previous negativesextant biopsies. J. Urol. 2001; 166: 86–91, discussion92.
6 Borboroglu PG, Corner SW, Riffenburgh RH, Amling CL.Extensive repeat trans-rectal ultrasound guided prostatebiopsy in patient with previous benign sextant biopsies. J.Urol. 2000; 163: 158–62.
7 Bertaccini A, Fandella A, Prayer-Galetti T et al.Systematic development of clinical practice guidelines forprostate biopsies: a 3-year Italian project. Anticancer Res.2007; 27: 659–66.
8 Yurdakul T, Taspinar B, Kilic O, Kilinc M, Serarslan A.Topical and long-acting local anesthetic for prostate
Table 8 Key points
Indication for biopsyThe need for PBx should be determined on the basis of the PSA level (up to 2.5 ng/mL, repeat exams just twice) and/or a
suspicious DRE.The patient’s biological age, potential comorbidities and the therapeutic consequences should also be considered , calculating
an individualized risk assessment.AnesthesiaIt is mandatory, regardless the technique. PPNB with 1or 2% lidocaine in the region of seminal vesicles junction with the
prostate base is considered the gold standard for anesthesia in PBx. Adding IRLA or oral medication in order to have betterpain relief is increasingly advisable.
Biopsy approachThe most common is TRUS-guided , but a transperineal approach is also feasible. At least 8–12 cores have to be carried out,
targeting the biopsies to the peripheral zone at the apex, mid gland , and base, as well as laterally directed cores on eachside of the prostate
Baseline biopsy strategyEPBx that optimise the DR should include six standard sextant biopsies with additional laterally directed core at the base and
medially to the apex. Thus, the recommended number of cores to carry out in an extended strategy is 12–14, includingsuspect areas at TRUS and without transition zone cores. SPBx as an initial PBx strategy does not improve PCa DR.
Repeat biopsy strategySPBx with a mean of 20 cores is most often carried out in men with a prior negative prostate biopsy but with a persistent
suspicion of PCa on the basis of: DRE findings, repeated PSA measurements (such as free PSA percentage, complex PSA,PSA density, PSA velocity) and suspicious histological findings such as ASAP and HGPIN. Another indication involves patientswho have been diagnosed with PCa and remain on active surveillance protocol or are considering focal therapy. Transitionzone should have to be included.
‘Insignificant cancer’There is no confirmed predictive model or marker to distinguish insignificant from significant carcinomas. Insignificant prostate
carcinomas do exist but cannot be identified reliably with any currently available diagnostic method prior to treatmentRole of new imaging techniquesAs shown by international guidelines, Doppler ultrasound has been shown to have the potential for improving biopsy targeting,
but, like gray scale, is not a substitute for a biopsy (Table 1).Contrast enhanced TRUS with intermittent harmonic imaging provides a statistically significant improvement in discrimination
between benign and malignant biopsy sites, whereas the technique alone might not be sufficient to predict as to whichpatients have benign vs malignant disease.
The published trials have shown promising results of RTE in PCa imaging and detection, especially in conjunction with TRUS, inorder to reduce the number of cores.
ASAP, atypical small acinar proliferation; DRE, digital rectal examination; EPBx, extended biopsy; HGPIN, high-grade prostaticintraepithelial neoplasia; IRLA, intrarectal local anesthetic; PBx, prostate biopsy; PCa, prostate cancer, PPNB, peri-prostatic nerveblock PSA, prostate-specific antigen; RTE, Real-time elastography; SPBx, saturated prostate biopsy; TRUS, transrectal ultrasound.
V SCATTONI ET AL.
442 © 2010 The Japanese Urological Association

biopsy: a prospective randomized placebo-controlledstudy. Urol. Int. 2009; 83: 151–4.
9 Ingber MS, Ibrahim I, Turzewski C, Hollander JB, DioknoAC. Does periprostatic block reduce pain duringtransrectal prostate biopsy? A randomized ,placebo-controlled , double-blinded study. Int. Urol.Nephrol. 2009. Published on line 8 Aug 2009. DOI10.1007/s11255-009-9621-2.
10 Montoliu García A, Juan Escudero J, Ramos de CamposM et al. Prospective randomized study on the use oflidocaine local anesthesia in prostate biopsy. Arch. Esp.Urol. 2009; 62: 339–47.
11 Bingqian L, Peihuan L, Yudong W et al. Intraprostaticlocal anesthesia with periprostatic nerve block fortransrectal ultrasound guided prostate biopsy. J. Urol.2009; 182: 479–83, discussion 483–4.
12 Luján Marco S, Bango García V Arlandis Guzmán S et al.Comparative study between analgesic efficacy and safetyof meperidine compared with lidocaine periprostaticinfiltration in transrectal ultrasound guided prostatebiopsy. Actas Urol. Esp. 2009; 33: 30–4.
13 Skriapas K, Konstandinidis C, Samarinas M et al. Painlevel and anal discomfort during transrectal ultrasound forguided prostate biopsy. Does intrarectal administration oflocal anesthetic before periprostatic anesthesia makes anydifference? Minerva Urol. Nephrol. 2009; 61: 137–42.
14 Visapää H, Taari K. Combination of paracetamol, codeineand lidocaine for pain relief during transrectal ultrasoundguided biopsy of the prostate. Scand. J. Surg. 2009; 98:55–7.
15 Kandirali E, Ulukaradag E, Uysal B et al. Is only perianalanesthesia with lidocaine-prilocaine cream sufficient todecrease the pain during transrectal ultrasound-guidedprostate biopsy? A prospective randomized study. Urol.Int. 2009; 82: 262–5.
16 Giannarini G, Autorino R, Valent F et al. Combination ofperianal-intrarectal lidocaine-prilocaine cream andperiprostatic nerve block for pain control duringtransrectal ultrasound guided prostate biopsy: arandomized , controlled trial. J. Urol. 2009; 181: 585–91,discussion 591–3.
17 Cantiello F, Imperatore V, Iannuzzo M et al. Periprostaticnerve block (PNB) alone vs PNB combined with ananaesthetic-myorelaxant agent cream for prostate biopsy: aprospective, randomized double-arm study. BJU Int. 2009;103: 1195–8.
18 Akan H, Yildiz O, Dalva I, Yücesoy C. Comparison oftwo periprostatic nerve blockade techniques for transrectalultrasound-guided prostate biopsy: bilateral basal injectionand single apical injection. Urology 2009; 73: 23–6.
19 Cam K, Sener M, Kayikci A, Akman Y, Erol A. Combinedperiprostatic and intraprostatic local anesthesia for prostatebiopsy: a double-blind , placebo controlled , randomizedtrial. J. Urol. 2008; 180: 141–4, discussion 144–5.
20 Szlauer R, Gotschl R, Gnad A et al. Comparison oflidocaine suppositories and periprostatic nerve blockduring transrectal prostate biopsy. Urol. Int. 2008; 80:253–6.
21 Bhomi KK, Lim HH, Consigliere DT, Tiong HY. Controlof pain during transrectal ultrasound-guided prostatebiopsy: a prospective study comparing two methods. Urol.Int. 2007; 79: 332–5.
22 Inal G, Adsan O, Ugurlu O et al. Comparison of fourdifferent anesthesia methods for relief of all pain duringtransrectal ultrasound-guided prostate biopsy. Int. Urol.Nephrol. 2008; 40: 335–9.
23 Raber M, Scattoni V, Roscigno M et al. Topicalprilocaine-lidocaine cream combined with peripheralnerve block improves pain control in prostatic biopsy:results from a prospective randomized trial. Eur. Urol.2008; 53: 967–73.
24 Ashley RA, Inman BA, Routh JC et al. Preventing painduring office biopsy of the prostate: a single center,prospective, double-blind , 3-arm, parallel group,randomized clinical trial. Cancer 2007; 110:1708–14.
25 Lee HY, Lee HJ, Byun SS. Effect of intraprostatic localanesthesia during transrectal ultrasound guided prostatebiopsy: comparison of 3 methods in a randomized ,double-blind , placebo controlled trial. J. Urol. 2007; 178:469–72.
26 Naughton CK, Ornstein DK, Smith DS et al. Pain andmorbidity of transrectal ultrasound guided prostate biopsy:a prospective randomised trial of 6 versus 12 cores. J.Urol. 2000; 163: 168–71.
27 Chang SC, Alberts G, Wells N et al. Intrarectal lidocaineduring transrectal prostate biopsy: results of a prospectiverandomized trial. J. Urol. 2001; 166: 2178–80.
28 Nash PA, Bruce JE, Indudhara R et al. Transrectalultrasound guided prostatic nerve blockade easessystematic needle biopsy of the prostate. J. Urol. 1996;155: 607–9.
29 Hollabaugh RS, Smochowski AR, Steiner MS et al.Neuroanatomy of the male rabdmiosphincter. Urology1997; 49: 426.
30 Desgrandchamps F, Meria P, Irani J et al. The rectaladministration of lidocaine gel and tolerance oftransrectak ultrasonography-guided biopsy of the prostate:a prospective randomised placebo-controlled study. BJUInt. 1999; 83: 1007–9.
31 Issa MM, Bux S, Chun T et al. A randomised prospectivetrial of intrarectal lidocaine for pain control duringtransrectal prostate biopsy : the Emory Universityexperience. J. Urol. 2000; 164: 397–9.
32 Lynn NN, Collins GN, Brown SC et al. Periprostatic nerveblock gives better analgesia for prostatic biopsy. BJU Int.2002; 90: 424–6.
33 Matlaga BR, Lovato JF, Hall MC. Randomizedprospective trial of a novel local anaesthetic technique forextensive prosate biopsy. Urology 2003; 61: 972–6.
34 Adamakis I, Mitropoulos D, Haritopoulos K et al. Painduring transrectal ultrasonography guided biopsy : arandomised prospective trial comparing periprostaticinfiltration with lidocaine with the intrarectal instillationof lidocaine-prilocaine cream. World J. Urol. 2004; 22:281–4.
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 443

35 Alawi AS, Soloway MS, Vaidya A et al. Local anesthesiafor ultrasound guided prostate biopsy: a prospectiverandomised trial comparing 2 methods. J. Urol. 2001; 166:1343–5.
36 Stirling BN, Shockley KF, Carothers GG et al.Comparison of local anesthesia techinique duringtransrectal ultrasound guided biopsy. Urology 2002; 60:89–92.
37 Tiong HY, Liew LC, Samuel M, Consigliere D,Esuvaranathan K. A meta analysis of local anaesthesia fortransrectal ultrasound guided biopsy of the prostate.Prostate Cancer Prostatic Dis. 2007; 10: 127–36.
38 Ragavan N, Philip J, Balasubramanian SP et al. Arandomized , controlled trial comparing lidocaineperiprostatic nerve block, diclofenac suppository and bothfor transrectal ultrasound guided biopsy of the prostate. J.Urol. 2005; 174: 510–13.
39 Moinzadeh A, Mourtizinos A, Triaca V, Hamawy KJ. Arandomised double blind prospective study evaluatingpatient tolerance of transrectal ultrasound-guided biopsyof the prostate using prebiopsy rofecoxib. Urology 2003;62: 1054–7.
40 Hirsh I, Kaploun A, Faris G et al. Tramadol improvespatients’ tolerance of transrectal ultrasound-guided biopsyof the prostate. Urology 2007; 69: 491–4.
41 Pendleton J, Costa J, Wludyka P et al. Combination of oraltramadol, acetaminophen and 1% lidocaine inducedperiprostatic nerve block for pain control during transrectalultrasound guided biopsy of the prostate: a prospective ran-domised , controlled trial. J. Urol. 2006; 176: 1372.
42 Visapää H, Taari K. Combination of paracetamol, codeineand lidocaine for pain relief during transrectal ultrasoundguided biopsy of the prostate. Scand. J. Surg. 2009; 98:55–7.
43 Eichler K, Hempel S, Wilby J et al. Diagnostic value ofsystematic biopsy methods in the investigation of prostatecancer: a systematic review. J. Urol. 2006; 175: 1605–12.
44 Descazeaud A, Rubin M, Chemama S et al. Saturationbiopsy protocol enhances prediction of pT3 and surgicalmargin status on prostatectomy specimen. World J. Urol.2006; 24: 676–80.
45 Delongchamps NB, de la Roza G, Jones R, Jumbelic M,Haas GP. Saturation biopsies on autopsied prostates fordetecting and characterizing prostate cancer. BJU Int.2009; 103: 49–54.
46 Scattoni V, Roscigno M, Raber M et al. Initial extendedtransrectal prostate biopsy – are more prostate cancersdetected with 18 cores than with 12 cores? J. Urol. 2008;179: 1327–31.
47 Jones JS. Saturation biopsy for detecting andcharacterizing prostate cancer. BJU Int. 2007; 99: 1340–4.
48 Naughton CK, Miller DC, Mager DE, Ornsetin DK,Catalona WJ. A prospective randomised trial comparing 6versus 12 prostate biopsy cores: impact of cancerdetection. J. Urol. 2000; 164: 388.
49 Gore JL, Shariat S, Miles BJ et al. Optimal combinationsof systematic sextant and laterally directed biopsies for thedetection of prostate cancer. J. Urol. 2001; 165: 1554–9.
50 Siu W, Dunn RL, Shah RB et al. Use of extended patterntechnique for initial prostate biopsy. J. Urol. 2005; 174:505–9.
51 Singh H, Canto EI, Shariat SF et al. Improved detection ofclinically significant, curable prostate cancer withsystematic 12-core biopsy. J. Urol. 2004; 171: 1089–92.
52 de la Taille A, Antiphon P, Salomon L et al. prospectiveevaluation of a 21-sample needle biopsy proceduredesigned to improve the prostate cancer detection rate.Urology 2003; 61: 1181–6.
53 Presti JC Jr, O’Dowd GJ, Miller MC et al. Extendedperipheral zone biopsy schemes increases cancer detectionrates and minimizes variance in prostate specific antigenand age related cancer rates : results of a communitymulti-practice study. J. Urol. 2003; 169: 125–9.
54 Eskew LA, Bare RL, McCullough DL. Systematic 5region prostate biopsy is superior to sextant method fordiagnosing carcinoma of the prostate. J. Urol. 2000; 164:393–6.
55 Meng MV, Franks JH, Presti JC Jr, Shinohara K. Theutility of apical anterior horn biopsies in prostate cancerdetection. Urol. Oncol. 2003; 21: 361–5.
56 Patel AR, Jones JS, Rabets J, DeOreo G, Zippe CD.Parasagittal biopsies add minimal information in repeatsaturation prostate biopsy. Urology 2004; 63: 87–9.
57 Philip J, Hanchanale V, Foster CS, Javle P. Importance ofperipheral biopsies in maximising the detection of earlyprostate cancer in repeat 12-core biopsy protocol. BJU Int.2006; 98: 559–62.
58 Pelzer AE, Bektic J, Berger AP et al. Are transition zonebiopsies still necessary to improve prostate cancerdetection? Results from the Tyrol screening project. Eur.Urol. 2005; 48: 916–21.
59 Peyromaure M, Ravery V, Boccon-Gibod L. The role ofthe biopsy of the transitional zone and of the seminalvesicles in the diagnosis and staging of prostate cancer.Eur. Urol. Suppl. 2002; 1: 40–6.
60 Onur E, Littrup PJ, Pontes JE, Bianco FJ Jr.Contemporary impact of trans-rectal ultrasound lesions forprostate cancer detection. J. Urol. 2004; 172:512–14.
61 Djavan B. Prostate biopsies and Vienna Nomograms. Eur.Urol. Suppl. 2006; 5: 500–10.
62 Ficarra V, Novella G, Novara G et al. The potentialimpact of prostate volume in the planning of optimalnumber of cores in the systematic transperineal prostatebiopsy. Eur. Urol. 2005; 48: 932–7.
63 Inahara M, Suzuki H, Kojima S et al. Improved prostatecancer detection using systematic 14-core biopsy for lagerprostate glands with normal digital rectal examinationfinding. Urology 2006; 68: 815–19.
64 Damiano R, Autorino R, Perdona S et al. Are extendedbiopsies really necessary to improve prostate cancerdetection? Prostate Cancer Prostatic Dis. 2003; 6:250–5.
65 Jones SJ, Patel A, Schoenfield L et al. Saturationtechnique does not improve cancer detection as an initialprostate biopsy strategy. J. Urol. 2006; 175: 485–8.
V SCATTONI ET AL.
444 © 2010 The Japanese Urological Association

66 de La Rosette JMCH, Wink MH, Mamoulakis C et al.Optimizing prostate cancer detection : 8 versus 12 corebiopsy protocol. J. Urol. 2009; 182: 1329–36.
67 Lane BR, Zippe CD, Abouassaly A, Schoenfield L,Magi-Galluzzi C, Stephen Jones L. Saturation Tecniquedoes not decrease cancer detection during follow-up afterinitial prostate biopsy. J. Urol. 2008; 179: 1749–50.
68 Guichard G, Larre S, Gallina A et al. Extended 21-sampleneedle biopsy protocol for diagnosis of prostate cancer in1000 consecutives patients. Eur. Urol. 2007; 52: 430–5.
69 Scattoni V, Raber M, Abdollah F et al. Biopsy schemeswith the fewest cores for detecting 95% of the prostatecancers detected by a 24-core biopsy. Eur. Urol. 2009; 57:1–8.
70 Patel AR, Jones JS. Optimal biopsy strategies for thediagnosis and staging of prostate cancer. Curr. Opin. Urol.2009; 19: 232–7.
71 Presti JC Jr. Repeat biopsy-when, where and how. Urol.Oncol. 2009; 27: 312–14.
72 Ellis WJ, Brawer MK. Repeat prostate needle biopsy: whoneeds it? J. Urol. 1995; 153: 1496–8.
73 Keetch DW, Catalona WJ, Smith DS. Serial prostaticbiopsies in men with persistently elevated serum prostatespecific antigen values. J. Urol. 1994; 151: 1571–4.
74 Fleshner N, Klotz L. Role of ‘saturation biopsy’ in thedetection of prostate cancer among difficult diagnosticcases. Urology 2002; 60: 93–7.
75 Pryor MB, Schellhammer PF. The pursuit of prostatecancer in patients with a rising prostate specific antigenand multiple negative transrectal ultrasound guidedprostate biopsies. Clin. Prostate Cancer 2002; 1: 172–6.
76 Walz J, Graefen M, Chun FK et al. High incidence ofprostate cancer detected by saturation biopsy afterprevious negative biopsy series. Eur. Urol. 2006; 50:498–505.
77 Rabets JC, Jones JS, Patel A et al. Prostate cancerdetection with office based saturation biopsy in a repeatbiopsy population. J. Urol. 2004; 172: 94–7.
78 Epstein JI, Sanderson H, Carter HB et al. Utility ofsaturation biopsy to predict insignificant cancer at radicalprostatectomy. Urology 2005; 66: 356–60.
79 Warlick C, Trock BJ, Landis B et al. Delayed versusimmediate surgical intervention and prostate canceroutcome. J. Natl. Cancer Inst. 2006; 98: 355–7.
80 Abouassaly R, Lane BR, Stephen Jones J. Stagingsaturation biopsy in patients with prostate cancer on activesurveillance protocol. Urology 2008; 71: 573–7.
81 Boccon-Gibod LM, de Longchamps NB, Toublanc Met al. Prostate saturation biopsy in the re-evaluation ofmicrofocal prostate cancer. J. Urol. 2006; 176: 971–3.
82 Simon J, Kuefer R, Bartsch G Jr et al. Intensifying thesaturation biopsy technique for detecting prostate cancerafter previous negative biopsies: a step in the wrongdirection. BJU Int. 2008; 102: 459–62.
83 Epstein JI, Chan DW, Sokoll LJ. Non palpable stage T1cprostate cancer: prediction of insignificant disease usingfree/total prostate specific antigen levels and needle biopsyfindings. J. Urol. 1998; 160: 2407–11.
84 Cooperberg MR, Lubeck DP, Meng MV et al. Thechanging face of low risk prostate cancer: trends inclinical presentation and primary management. J. Clin.Oncol. 2004; 22: 2141–9.
85 Master VA, Chi T, Simko JP et al. The independentimpact of extended pattern biopsy on prostatecancer stage migration. J. Urol. 2005; 174: 1789–93,discussion 1793.
86 Kahl P, Wolf S, Adam A et al. Saturation biopsy improvespreoperative Gleason scoring of prostate cancer. Pathol.Res. Pract. 2009; 205: 259–64.
87 Kaufman JJ, Roenthal M, Godwin WE. Methods ofdiagnosis of carcinoma of the prostate: a comparison ofclinical impression, prostate smear, needle biopsy openperineal biopsy and transurethral biopsy. J. Urol. 1954;72: 450–63.
88 Ritkin MD, Kurtz AB, Goldberg BB. Sonographicallyguided transperineal prostate biopsy: preliminaryexperience with a longitudinal linear array transducer. AJRAm. J. Roentgenol. 1983; 140: 745–7.
89 Shandera KC, Thibault GP, Deshon JE et al. Variability inpatient preparation for prostate biopsy among AmericanUrologists. Urology 1998; 52: 644–6.
90 Emiliozzi P, Corsetti A, Tassi B et al. Best approach forprostate cancer detection: a prospective study ontransperineal versus transrectal six core prostate biopsy.Urology 2003; 61: 961–6.
91 Watanabe M, Hayashi T, Tsushima T et al. Extensivebiopsy using a combined transperineal and transrectalapproach to improve prostate cancer detection. Int. J. Urol.2005; 12: 969–3.
92 Kawakami S, Okuno T, Yonese J et al. Optimal samplingsites for repeat prostate biopsy: a recursive portioninganalysis of three-dimensional 26-core systematic biopsy.Eur. Urol. 2007; 51: 675–83.
93 Emiliozzi P, Maymone S, Paterno A et al. Increasedaccuracy of biopsy Gleason score obtained by extendedneedle biopsy. J. Urol. 2004; 172 (6 Pt 1): 2224–6.
94 Takenaka A, Hara R, Hyodo Y et al. Transperinealextended biopsy improves the clinically significantprostate cancer detection rate: a comparativestudy of 6 and 12 biopsy cores. Int. J. Urol. 2006; 13:10–14.
95 Li H, Yan W, Zhou Y et al. Transperinealultrasound-guided saturation biopsies using 11-regiontemplate of prostate: report of 303 cases. Urology 2007;70: 1157–61.
96 Furuno T, Demura T, Kaneta T et al. Difference of cancercore distribution between first and repeat biopsy in patientdiagnose by extensive transperineal ultrasound guidedtemplate prostate biopsy. Prostate 2004; 58: 76–81.
97 Rifkin MD, Sudakoff GS, Alexander AA. Prostate:techniques, results, and potential applications of colorDoppler US scanning. Radiology 1993; 186: 509–13.
98 Kelly IM, Lees WR, Rickards D. Prostate cancer and therole of color Doppler US. Radiology 1993; 189: 153–6.
99 Newman JS, Bree RL, Rubin JM. Prostate cancer:diagnosis with color Doppler sonography with histologic
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 445

correlation of each biopsy site. Radiology 1995; 195:86–90.
100 Littrup PJ, Klein RM, Gross ML et al. Color Doppler ofthe prostate: histologic and racial correlations. Radiology1995; 197: 365.
101 Ismail M, Petersen RO, Alexander AA et al. ColorDoppler imaging in predicting the biologic behavior ofprostate cancer: correlation with disease- free survival.Urology 1997; 50: 906–12.
102 Ismail M, Gomella LG, Alexander AA. Color Dopplersonography of the prostate. Tech. Urol. 1997; 3: 140–6.
103 Alexander AA. To color Doppler image the prostate ornot: that is the question. Radiology 1995; 195: 11–13.
104 Rifkin MD, Alexander AA, Helinek TG, Merton DA.Color Doppler as an adjunct to prostate ultrasound. Scand.J. Urol. Nephrol. Suppl. 1991; 137: 85–9.
105 Pallwein L, Mitterberger M, Gradl J. Value ofcontrast-enhanced ultrasound and elastography inimaging of prostate cancer. Curr. Opin. Urol. 2007; 17:39–47.
106 Amiel GE, Slawin KM. Newer modalities of ultrasoundimaging and treatment of the prostate. Urol. Clin. NorthAm. 2006; 33: 329–37.
107 Halpern EJ, Strup SE. Using gray-scale and color andpower Doppler sonography to detect prostatic cancer. AJRAm. J. Roetntgenol. 2000; 174: 623–7.
108 Remzi M, Dobrovits M, Reissigl A et al. EuropeanSociety for Oncological Urology (ESOU). Can powerDoppler enhanced transrectal ultrasound guided biopsyimprove prostate cancer detection on first and repeatbiopsy? Eur. Urol. 2004; 46: 451–6.
109 Frauscher E, Helweg G, Gotwald TF et al. The value ofcontrast-enhanced color Doppler ultrasonography in thediagnosis of prostate cancer. Radiology 1998; 209: 417,abstract.
110 Bogers HA, Sedelaar JP, Beerlage HP et al. Contrastenhanced three dimensional power Doppler angiographyof the human prostate: correlation with biopsy outcome.Urology 1999; 54: 97–104.
111 Unal D, Sedelaar JP, Aarnink RG et al.Three-dimensional contrast-enhanced power Dopplerultrasonography and conventional examination methods:the value of diagnostic predictors of prostate cancer. BJUInt. 2000; 86: 58–64.
112 Albrecht T, Hoffmann CW, Schettler S et al. B-modeenhancement at phase inversion US with air-basedmicrobubble contrast agent: initial experience in humans.Radiology 2000; 216: 273–8.
113 Halpern EJ, Verkh L, Forsberg F et al. Initial experiencewith contrast enhanced sonography of the prostate. AJRAm. J. Roentgenol. 2000; 174: 1575–80.
114 Halpern EJ, Rosenberg M, Gomolla LG. Contrastenhanced sonography of the prostate. Radiology 2001;219: 219–25.
115 Halpern EJ, Ramey JR, Strup SE et al. Detection ofprostate carcinoma with contrast-enhanced sonographyusing intermittent harmonic imaging. Cancer 2005; 104:2373–83.
116 Ophir J, Cespedes I, Ponnekanti H et al. Elastography: aquantitative method for imaging the elasticity of biologicaltissue. Ultrason. Imaging 1991; 13: 111–34.
117 Pallwein L, Aigner F, Faschingbauer R et al. Prostatecancer diagnosis: value of real-time elastography. Abdom.Imaging 2008; 33: 729–35.
118 Konig K, Scheipers U, Pesavento A et al. Initialexperiences with real-time elastography guided biopsies ofthe prostate. J. Urol. 2005; 174: 115–7.
119 Pallwein L, Mitterberger M, Pinggera G et al.Sonoelastography of the prostate: comparison withsystematic biopsy findings in 492 patients. Eur. J. Radiol.2008; 65: 304–10. Epub 2007 May 23.
120 San Francisco IF, DeWolf WC, Rosen S, Upton M, OlumiAF. Extended prostate needle biopsy improvesconcordance of Gleason grading between prostate needlebiopsy and radical prostatectomy. J. Urol. 2003; 169:136–40.
121 Mian BM, Lehr DJ, Moore CK et al. Role of prostatebiopsy schemes in accurate prediction of Gleason scores.Urology 2006; 67: 379–83.
122 Numao N, Kawakami S, Yonese J et al. Three-dimensional26-core biopsy-based patient selection criteria fornerve-sparing radical prostatectomy. Int. J. Urol. 2008; 15:1061–6.
123 Davis JW, Kim J, Ward JF et al. Radical prostatectomyfindings in patients predicted to havelow-volume/low-grade prostate cancer diagnosed byextended-core biopsies: an analysis of volume and zonaldistribution of tumour foci. BJU Int. 2009. Published online 3 Nov 2009; doi:10.1111/j.1464-410X.2009.08964.x.
124 Moussa AS, Kattan MW, Berglund R, Yu C, Fareed K,Jones JS. A nomogram for predicting upgrading inpatients with low- and intermediate-grade prostate cancerin the era of extended prostate sampling. BJU Int. 2009;105: 352–8.
125 Babaain RJ, Troncoso P, Bhadkamkar DA, Johston DA.Analysis of clinico-pathologic factors predicting outcomeafter radical prostatectomy. Cancer 2001; 91: 1414–22.
126 Mian BM, Naya Y, Okihara F et al. Role of the prostatebiopsy schemes in accurate prediction of Gleason score.Urology 2006; 67: 379–83.
127 Stamey TA, Caldwell M, McNeal JE. The prostate specificantigen era in the United States is over for prostate cancer:what happened in the last 20 years? J. Urol. 2004; 172:1297–301.
128 Thickman D, Speers WC, Philpott PJ, Shapiro H. effect ofthe number of core biopsies of the prostate on predictingGleason score of prostate cancer. J. Urol. 1996; 156:110–13.
129 Fugakai T, Namiki T, Namiki H et al. Discrepanciesbetween Gleason score of needle biopsy and radicalprostatetcomy specimes. Pathol. Int. 2001; 51:364–70.
130 Cecchi R, Minervini R, Sepich CA et al. Correlationbetween Gleason score of needle biopsy and radicalprostatectomy tissue. Int. Urol. Nephrol. 1998; 30:575–80.
V SCATTONI ET AL.
446 © 2010 The Japanese Urological Association

131 Epstein JI, Walsh PC, Sauvageot J, Carter HB. Use ofrepeat sextant and transition zone biopsies forassessing extent of prostate cancer. J. Urol. 1997; 158:1886–90.
132 Divrik RT, Eroglu A, Sahin A et al. Increasing the numberof biopsies increases the concordance of Gleason scores
of needle biopsies and prostatectomy specimens. Urol.Oncol. 2007; 25: 376–82.
133 Pepe P, Galia A, Fraggetta F et al. Prediction byquantitative histology on pathological stage in prostatecancer. Eur. J. Surg. Oncol. 2005; 31: 309–13.
Editorial Commentiju_2524 447..464
Editorial Comment to Is extended and saturationbiopsy necessary?
Amongst a global trend from non-extended to extendedprostate biopsy, no standard extended biopsy scheme hasbeen established yet. In this well organized review article, theauthors are addressing controversial issues in the diagnosis ofprostate cancer with an updated literature review.1 Among all,Tables 6 and 7. How to use the information along withclinical information for precise risk assessment is the mostcritical point in the treatment decision-making process ofprostate cancer. Some issues, however, should be addressed.
Ambiguity in the definition ofsaturation biopsy
My first concern is what the term saturation biopsy means.As was the case in the majority of previous literature, theauthors adopted a somewhat arbitrary definition of satura-tion biopsy, a biopsy protocol in which 20 or more cores aretaken in a systematic fashion. Unfortunately, there is ambi-guity associated with this kind of definition. After the pio-neering work by Stewart et al.,2 several investigators havereported the diagnostic performance of saturation biopsyprotocols.3–7 However, saturation biopsy was defined assimply taking a larger number of cores in most reports andless attention has been paid on how to locate sampling siteswithin the gland effectively. For example, Jones and hisco-workers reported that a transrectal 24-core biopsy did notimprove cancer detection compared with a transrectal10-core biopsy and suggested that extended transrectalbiopsy beyond 10–12 cores does not appear to be appropri-ate at the initial biopsy.3 Pepe et al. demonstrated that tran-srectal 24–37 core biopsy offers no advantage over atransrectal 12-core biopsy at the initial biopsy setting.4 Inthe analysis of a large cohort including more than 3000 men,Scattoni and his co-workers revealed that a diagnosticadvantage of a transrectal 18-core biopsy over a transrectal12-core biopsy was seen only in men with a prostate largerthan 55 mL.5 In contrast, Ravery et al. found that the cancerdetection rate of a transrectal 20-core biopsy was signifi-cantly better than that of a transrectal 10-core biopsy.6
Although Guichard et al. showed the superiority of a tran-
srectal 21-core biopsy over a transrectal 12-core biopsy, thereported increment of the cancer detection rate was no morethan 9.8%.7 These studies illustrate that additional transrec-tal sampling to the conventional transrectal 12-core biopsymight not lead to a significant improvement in cancer detec-tion.8 Altogether, these saturation biopsy strategies, taking alarge number of cores through a single approach, seemneither efficient nor practical. A recent editorial entitled‘Saturation biopsy of the prostate. Why saturation does notsaturate’ addressed this issue very clearly and concluded thatthe term saturation biopsy would be rightfully used onlywhen a biopsy protocol that associates maximized diagnos-tic yield is devised.9
Saturation of the cancerdetection rate
From a practical point of view, the optimal extended biopsyscheme should yield a maximum cancer detection rate witha minimal number of biopsy cores.10,11 To this end, tissuesampling sites are to be located to cover the entire peripheralzone with special attention to the anterior portion.10–13 Inprinciple, the more biopsy cores that are taken the morecancers would be detected by prostate biopsy. However, itshould be noted that the relationship between the number ofbiopsy cores and the resultant cancer detection rate does notcorrelate linearly. Instead, the cancer detection rate wouldbecome saturated when increasing the number of biopsycores.10,11,14
We analyzed the saturation phenomena in the cancerdetection rate of extended prostate biopsy by using a 3-D26-core systematic super-extended biopsy protocol.10,11 Inthese analyses, subset biopsy schemes were determined byrecursive partitioning to achieve maximum a cancer detec-tion rate at given number of biopsy cores through singletransrectal, single transperineal or 3-D combination of tran-srectal and transperineal approaches. When cancer detectionrates of biopsy schemes were plotted against the number ofbiopsy cores, saturation in the cancer detection rate wasclearly demonstrated either in the initial (Fig. 1)10 or in the
Extended and saturation prostatic biopsy
© 2010 The Japanese Urological Association 447