Musculoskeletal side effects of aromatase inhibitors treatment ...
Upload
independentCategory
view
3download
0
Introduction
CT is an important tool for imaging of the musculo-skeletal system in children. Multidetector row CT(MDRCT), in turn, has been a significant advancecompared to single-detector row CT (SDRCT). Mul-tiplanar reformations (MPR) and three-dimensional (3-D) reformations that can be obtained from MDRCTallow superior volumetric assessment of the musculo-skeletal system. The protocols used for performingthese examinations continue to evolve, incorporatingnew technologies in order to reduce radiation expo-sure.
This review is based on our experience with muscu-loskeletal CT examinations performed at the Massa-chusetts General Hospital in the pediatric populationover a 20-month period. The studies were performed oneight MDRCT scanners. Seven scanners were made byGeneral Electric Medical systems (Waukesha, Wis.,USA) and ranged from 4 to 16 detector rows. One was a16-detector-row scanner built by Siemens MedicalSolutions (Forchheim, Germany). Detector configura-tions varied according to the machines used and at thediscretion of the supervising radiologist. The patientpopulation included inpatients, outpatients, and patientspresenting to the emergency department. One hundred
Hamid Salamipour
Rafael M. Jimenez
Sherry L. Brec
Vernon M. Chapman
Manudeep K. Kalra
Diego Jaramillo
Multidetector row CT in pediatricmusculoskeletal imaging
Received: 9 June 2004Revised: 20 November 2004Accepted: 20 December 2004Published online: 18 March 2005� Springer-Verlag 2005
Abstract The proliferation ofmultidetector row CT (MDRCT)has had a significant effect onimaging of the musculoskeletalsystem. An increasing number ofsuch examinations is being per-formed in children. We reviewed ourexperience using such examinationsin children during a period of20 months. In this review, we discussMDRCT techniques and issuesregarding the radiation dose of theseexaminations. We present the effectof newer scanning techniques andtheir incorporation into ourscanning protocols.
Keywords Pediatric radiology ÆMultidetector row CT ÆMusculoskeletal system
Pediatr Radiol (2005) 35: 555–564DOI 10.1007/s00247-005-1410-1 REVIEW
H. Salamipour Æ R. M. JimenezS. L. Brec Æ V. M. Chapman Æ M. K. KalraDepartment of Pediatric Radiology,Massachusetts General Hospital,Boston, MA, USA
H. Salamipour (&)Department of Radiology, MassachusettsGeneral Hospital, 34 Fruit Street,Boston, MA 02114, USAE-mail:[email protected].: +1-617-7244207
D. JaramilloDepartment of Radiology,Children’s Hospital of Philadelphia,Philadelphia, PA, USA

and fourteen musculoskeletal noncontrast MDRCTexaminations were identified in 99 patients. The age ofthe patients ranged from 4 months to 15 years, with anaverage age of 11.6 years at the time of the examination.None of the studies was performed under sedation, andall were performed without intravenous contrast. Elevenstudies were performed on patients in casts.
Discussion
MDRCT techniques
In MDRCT, multiple helical data streams are simulta-neously and rapidly acquired in each slice. Faster speedslead to thinner collimation, allowing slices thinner than1 mm [1]. In turn, thin-slice volume acquisitions using athickness of 0.5 mm allow nearly isotropic voxels, i.e.,equal in size in all dimensions [1]. The isotropic voxelsobtained by MDRCT can be quite exquisite in spatialresolution and detail, allowing seamless MPR withoutdegrading image quality, eliminating the need for mul-tiplanar scanning [1]. The reformations maintain highspatial resolution in any plane (Fig. 1). In MDRCT,MPR images are an integral part of the examinationitself [1].
Musculoskeletal application of CT often requireslarge areas of anatomic coverage. MDRCT is capable ofsimultaneous rapid acquisition of multiple helical datastreams in each slice, which allows coverage of a largeranatomical part per unit time without resorting toincreasing slice thickness or pitch, both of which can
degrade image quality. This affords multiple advantages,including extended anatomic coverage, reduced scanningand setup times, scanning in nonanatomic positions,decreased need for sedation, and reduced motion artifact[1, 2]. These benefits are especially valuable in theemergency setting, where acutely injured patientssometimes cannot be positioned according to standards.The use of subsecond spiral acquisition limits or elimi-nates even minimal interscan or intrascan motion arti-fact [3], even in the pediatric patient who may notremain motionless.
Thinner slices allow increased contrast resolution ofvolumetric data (Fig. 2) that also improves visualizationof low-contrast resolution examinations [2]. Lowerpitch values can be selected with MDRCT scanners (lessthan 1) compared to the SDRCT. Use of lower pitchwith ‘‘overlapping spirals’’ allows much higher effectivetube current-time product (which is tube current-timeproduct divided by pitch) with MDRCT, which canreduce beam-hardening artifacts caused by photonstarvation. In large patients and those with metallichardware, MDRCT diminishes artifacts and is capableof producing images superior to those produced bySDRCT (Fig. 3) [1]. Recent studies have shown thatincreasing tube current or tube potential does notimprove metal-related streak artifacts [4]. Selection oflower pitch with MDRCT in large patients at higherpeak kilovoltage reduces photon starvation andimproves image quality in these patients [1].
Multidetector row CT also allows construction ofsuperb 3-D rendering models. Superior 3-D renderingcan define dimensions of masses, abscesses, and collec-tions, as well as their relationship to surroundingstructures. These 3-D models also allow a better
Fig. 1 A 13-year-old girl with a history of repeated fractures of theleft clavicle. Curved oblique reformation of MDRCT of the leftclavicle allows visualization of the entire clavicle, showing post-traumatic healing and no acute fracture
Fig. 2 A 12-year-old boy with a history of falling. MDRCT directaxial with thin reconstructions: fracture of first and secondmetatarsals (black arrows) better seen on thinner reconstructions.(Slice thickness 2.5 mm, reconstructed to 0.47 mm)
556

understanding of the relationship between fracturefragments. They can help in presurgical planning as wellas planning of percutaneous procedures such as biopsies,aspirations, and drainages. Enhanced visualization ofthe skeleton using 3-D rendering models is especiallyvaluable in anatomically complex areas such as theelbow and the ankle, and it simplifies demonstration andconveying of such information to our clinical colleagues.
Radiation dose
Substantial increase in CT scanning with availability ofstate-of-the-art MDRCT scanners has generated debateabout its safety, particularly in children and youngadults. MDRCT does not automatically require a sig-nificantly increased amount of radiation compared toSDRCT. MDRCT can decrease the number of times thepatient is scanned. MPR images performed on MDRCTdata sets eliminate the need for multiplanar scanning.Moreover, artifacts necessitating repeat scanning withuse of SDRCT are effectively reduced or eliminated.
Examinations need to be tailored individually tooptimize radiation parameters. In recent years, majortechniques have been developed and incorporated by CTvendors to address radiation dose issues. These tech-niques include prepatient X-ray beam collimation, betterbeam-shaping filters and image-processing algorithms,efficient detector configuration, and automatic exposure-control (AEC) techniques [5].
Automatic exposure-control techniques enable auto-matic adjustment of the tube current in the x–y plane(angular modulation), along the scanning direction or z-axis (z-axis modulation) or both (xyz or combinedmodulation), according to the size and attenuationcharacteristics of the patient. The techniques achieveconstant CT image quality with lower radiation expo-
sure. These techniques adjust the tube current to followchanging patient anatomy so that quantum noise in theprojections can be adjusted to maintain a desired noisein the image and improve dose efficiency. The z-axismodulation uses localizer radiograph data to calculatepatient size and attenuation and adjusts the tube currentto maintain a user-specified quantum noise in the imagedata. Angular modulation adapts the tube current tominimize X-rays in projections (angles) that are lessimportant (for example, anteroposterior direction inshoulders compared to lateral direction) to reduce theoverall image noise content. Combined modulationtechniques combine advantages of both z-axis modula-tion and angular modulation.
We have used z-axis modulation (AutomA, GE) inCT scanning of adults and children for different clinicalindications, including the musculoskeletal system [6].This technique requires selection of the desired imagequality or user-specified noise index, which is approxi-mately equal to the image noise in the central region ofthe image obtained from scanning a uniform phantom.The noise index varies directly with noise in the recon-structed image and is inversely proportional to radiationdose. To avoid unexpected increase or decrease of tubecurrent with this technique, the radiologist can set arange of milliampere determined by the minimum andmaximum milliampere settings [5, 7].
These advances have allowed us to use lower tubecurrents in imaging the appendicular skeleton. Based onthe research performed in our department, we currentlyuse AutomA techniques to evaluate pediatric elbowtrauma (Fig. 4). These examinations are performed witha 100 kVp, a noise index of 20, and range of 25–200 mA,and scan time of 0.5 s/rotation (Table 1) [8]. Despiteencouraging results in other parts of the body (Fig. 5),AEC techniques have not been adequately studied forscanning pediatric musculoskeletal maladies, and fixedtube current scanning protocols continue to be morecommonly used. We are updating our CT scanningprotocols to investigate and incorporate AECtechniques further, especially in evaluation of theextremities.
The musculoskeletal MDRCT examinations reviewedbelow were performed using less radiation than sug-gested by manufacturers for adult patients (Table 2),and we were still able to achieve excellent quality ofimaging. It should be noted that the recommendationspublished were not specifically designed for pediatricpatients. More recently and even since we concluded thereview of the examinations described below, we havebeen optimizing our low-dose fixed-current techniquesto reduce radiation exposure even further. We are vigi-lant about decreasing radiation dose when possible,because the highest resolution images with high radia-tion doses are not always necessary for diagnosticquality. We are continually changing the CT protocols
Fig. 3 An 11-year-old boy with a history of open left ankle fracturestatus post ORIF. MDRCT coronal reformations show exquisitevisualization of nonunion of medial malleolus fracture (blackarrows) with negligible metallic hardware artifact
557

we design, investigating and incorporating newer imag-ing techniques such as AEC in order to reduce radiationdose even further. Our strategy is to revamp ourMDRCT scanning protocols utilizing AEC techniques,but our attempts are too preliminary to yield recom-mendations to report in this forum.
Applications
Trauma
Skeletal trauma is among the most common reasons forimaging infants and children in the emergency depart-ment [9]. In the setting of trauma, plain radiography is
often of poor quality. Non-MDRCT can be challengingbecause the patient might not be able to cooperate fullywith positioning, and non-MDRCT might be limited by
Fig. 5 MDRCT of the foot using AutomA (noise level 20, 140 kV,12–36 mAs, slice thickness 1.25 mm). Direct axial image (mAs ofthis slice=39) revealing excellent visualization of navicular fracture(black arrow)
Fig. 4 MDRCT of the elbow using AutomA (noise level 20,100 kV, 30–50 mAs, slice thickness 2.5 mm). Direct axial image(mAs of this slice=25) shows Salter-Harris type II fracture of theradial neck (black arrow)
Table 1 Low-dose scanning protocol for elbow trauma withautomatic exposure control (AEC) technique on a 16-slice multi-detector row CT (MDCT) scanner
Noise index 20Minimum 20 mAMaximum 200 mAGantry rotation time 0.5 sVoltage 100 kVpBeam pitch 0.938:1Table speed 18.75 mm/rotationDetector configuration 16·1.25 mmReconstructed slice thickness 1.25–2.5 mm
Table 2 Radiation parameters for musculoskeletal MDRCT: lit-erature suggestions (adults) versus our experience (children); ourprotocols have undergone much revision since these results wereobtained
Parameter Literaturesuggestions (adults)
Our experience(children)
kV 120 a 100–140120–140b 120 (median and mode)
mA 280a 137 (average)190–300+b 120 (median)
(110 (mode)Slice thickness (mm) 1–3 a 1.25–5
0.5–2.5b 2.5 (median and mode)Pitch 1–1.5 a 0.625–1.35
0.6–0.8 b
aPretorius and Fishman [3]bBuckwalter et al. [1]
558

motion artifact and metallic artifact. MDRCT, on theother hand, is capable of producing spectacular high-contrast resolution and seamless MPR, which haverevolutionized the evaluation of musculoskeletal trau-ma. In critically injured patients, MDRCT might replaceradiography altogether. This is particularly true inimaging of cervical spine injuries.
Multidetector row CT has advanced the two majorroles of CT in the evaluation of trauma. It can rapidlyand confidently define or exclude a fracture that theradiologist was uncertain about on plain radiography.Clinically suspected fractures that are radiographicallysubtle or occult can be definitively imaged with MDRCT(Fig. 6). If necessary, volume-rendered images can alsoaid in demonstrating complex injuries. Subtle fractures,particularly if axially oriented, are better seen on vol-ume-rendered images [3]. In addition, simultaneousevaluation of associated soft-tissue abnormalities areobtained. IV contrast media allow simultaneous evalu-ation of vascular structures, if clinically indicated [3].
Additionally, MPR and 3-D imaging obtained byMDRCT allow optimal visualization to define the extentof previously diagnosed complex fractures that requirefurther evaluation (Fig. 7). Osseous anatomy can beexquisitely demonstrated using volume-rendered images,especially in anatomically complex areas. Complexspatial information about relative position of the frac-ture fragments can be provided for referring physicians(Fig. 8) [3].
Multidetector row CT is also excellent for the evalua-tion of fracture healing, as well as post-traumaticcomplications such as pseudoarthrosis formation, post-traumatic physeal closure and growth arrest (Fig. 9),myositis ossificans (Fig. 10), and formation of loosebodies. In patients who undergo open reduction internal
fixation, MPR and volume-rendered images obtainedfrom MDRCT are optimally suited to assess hardwarefailure, as the high quality of the images eliminates moststreak artifact from metallic hardware and delineates therelationship of the hardware to the skeleton [3].We followmost of our surgically reduced patients with plain radi-ography and reserve MDRCT to clarify difficult cases.
Our review found that most of our studies (48/114)were performed in patients with a history of trauma.Almost half of these scans (23/48) were of the foot andankle. Only one scan was done for follow-up of trauma.In 10 of the 47 first-time trauma studies, the extremityimaged was in a cast. Overall, 37 scans were positive fortrauma, while 11 scans with a history of trauma werenormal. Most of the positive scans showed multipleanatomic parts of the bone were injured. Radiological
Fig. 6 An 8-year-old girl with ahistory of falling while skiing.a Radiograph of the knee in acast. Fracture is difficult tovisualize. b MDRCT coronalMPR images obtained in a cast.The tibial eminence fracture isclearly visible (black arrows)
Fig. 7 An 11-year-old girl, who fell while snowboarding. MDRCTcoronal and sagittal reformations demonstrate triplane fractureplanes (white arrows) and relationship of bony fragments
559

findings of bony bridges were seen in two scans, onelocated in the femur and the other in the posteriormedial aspect of the distal tibial growth plate. Myositisossificans was diagnosed on one scan.
Congenital/developmental
CT has an established role in imaging of the musculo-skeletal system in congenital and developmental disor-ders of childhood. In the preoperative stage, it is used todemonstrate osseous anatomy and to determine surgi-
cally appropriate assessment. In the thorax, CT is usedfor measurement of the pectus index in the setting ofpectus excavatum. In the lower extremity, measurementsof femoral anteversion angles and tibial torsion can becalculated. Imaging of tarsal coalition is greatly simpli-fied by MDRCT. Where previously two planes wererequired in a single acquisition, with the patient posi-tioned anatomically, MDRCT allows images to be ob-tained in a single plane and reconstructed to otherplanes, eliminating the need for additional scanning. Inthis way, diagnosis of both talocalcaneal and calcaneo-navicular coalition is possible.
CT can be used in the immediate postoperative per-iod to assess the success of the surgery, such as assess-ment of hip location after operative reduction ofdevelopmental dysplasia of the hips (DDH). Follow-upscanning can also demonstrate healing and degree ofmeasurable improvement.
The inherent speed and enhanced spatial resolutionof MDRCT can be exploited for demonstration ofosseous anatomy in congenital and developmental dis-orders. MDRCT can cover large anatomic areas rapidly,eliminate the need for multiplanar scanning, and reducemotion artifact to study bony deformities. Superior 3-D
Fig. 9 A 13-year-old hockey player with a history of Salter-Harristype III fracture. MDRCT coronal and sagittal reformations showpost-traumatic bony bridging (black arrows) after healing ofphyseal fracture of the distal tibia
Fig. 8 A 13-year-old boy, post-motorcycle accident. a Radiographof partially casted elbow shows displaced olecranon (black arrow)and capitellar (white arrow) fracture. b MDRCT coronal andsagittal reformations reveal the complexity of the fractures. c 3-Drendering models clarify the relationships of the fracture fragments
Fig. 10 A 12-year-old boy 6 weeks after right thigh injury.MDRCT direct axial and coronal reformation shows calcificationin the anterolateral thigh, with a rim of mature ossification (blackarrows) consistent with myositis ossificans
560

imaging of limb deformities allows detailed preoperativeevaluation.
Suspected congenital or developmental abnormalitiescomprised the second-highest group, after trauma, ofcommonly performed examinations (28/114) in our ser-ies. Of these, 23 were positive for such a diagnosis. Theseexaminations were performed most commonly forevaluation of DDH, tarsal coalition (Fig. 11), and pre-operative evaluation of pectus excavatum.
Tumors
Traditionally, plain radiography has been the imaging ofchoice for evaluation of benign bone tumors. MDRCTallows detailed assessment of the criteria used for tumorevaluation, including tumor margin, lesion matrix, and
periosteal reaction. Multiplanar capability of MDRCTprovides a significant advantage over plain radiography,as it eliminates the overlap of structures that occurs onplain radiography (Fig. 12). MDRCT can be used forprimary diagnosis as well as follow-up of bone and soft-tissue tumors. It allows rapid assessment of possible le-sions suggested on plain radiography. Although MRIremains superior toCT for evaluation ofmedullary tumorextent and evaluation of extraosseous soft-tissue masses[1], MDRCT maintains superiority to MRI for detectionof cortical destruction and lesion calcification [3]. In thesetting in whichMRI and CT might be of matched value,MDRCT is also superior to MRI, as it is faster and re-duces or eliminates the need for sedation.
Multidetector row CT can evaluate a variety ofosseous, cartilaginous and fibrous lesions, as well as soft-tissue lesions. MDRCT is ideally suited for evaluation ofassociated abnormalities, such as pathologic fractures,given its detailed assessment of the cortex (Fig. 11).MDRCT is also excellent for follow-up of these lesions.It can evaluate stability, post-treatment response(Fig. 13), and recurrence in patients who undergotreatment (Fig. 14).
We performed 27 MDRCT studies for the evaluationof benign bone tumors. Nineteen were performed for theinitial diagnosis of such tumors, while 11 examinationswere obtained to follow-up previously described benignbone tumors. The most commonly diagnosed benignbone tumors in our series included fibrous cortical de-fect, nonossifying fibroma, and Langerhans’ cell histio-cytosis. Other diagnoses included chondroblastoma andchondromyxofibroma.
Infection
In the setting of infection, MRI is excellent for evalua-tion of bone-marrow edema and soft-tissue findings.However, CT provides reliable detection of cortical
Fig. 11 A 15-year-old girl with 18 months of foot pain. MDRCTof the feet: coronal reformations of the hindfeet show bilateraltalocalcaneal coalition, osseous on the right (black arrow),fibrocartilaginous on the left (white arrow)
Fig. 12 A 16-year-old boy witha 6-week history of right thighpain. a Radiograph of the rightknee shows sclerotic bandacross distal femur (whitearrowhead) and a vague, smalllucent lesion posteromediallywith a sclerotic rim (blackarrowhead). The findings wereinterpreted as a healing patho-logic or stress fracture. Theclinician had ordered metastaticworkup based on outside inter-pretation. b MDRCT of thetibia clearly shows mildly ex-pansile, well-circumscribed fi-brous cortical defect (blackarrowheads) with pathologicfracture (white arrowheads)
561

destruction, periosteal reaction, and associated soft-tis-sue extension of infection. These characteristics can beradiographically occult [10]. MDRCT improves detec-tion of these features with its superior resolution, MPR,and volume-rendering. Bone marrow can be evaluatedon soft-tissue windows. Visualization of the soft tissues
and abscess formation can be improved with use ofintravenous contrast media [3]. MDRCT can betterdefine the extent of the infectious process and com-partment involvement, triage for medical versus surgicalmanagement, and the response to therapy.
In the setting of osteomyelitis, MDRCT can exqui-sitely assess cortical destruction, periosteal reaction,extent of bone expansion, involucrum formation, cloacatracks, and detection of bony sequestra, hyperattenua-tion of the medullary canal [10], and extent of associatedsoft tissue. All these features are more reliably evaluatedwith MDRCT than with SDRCT.
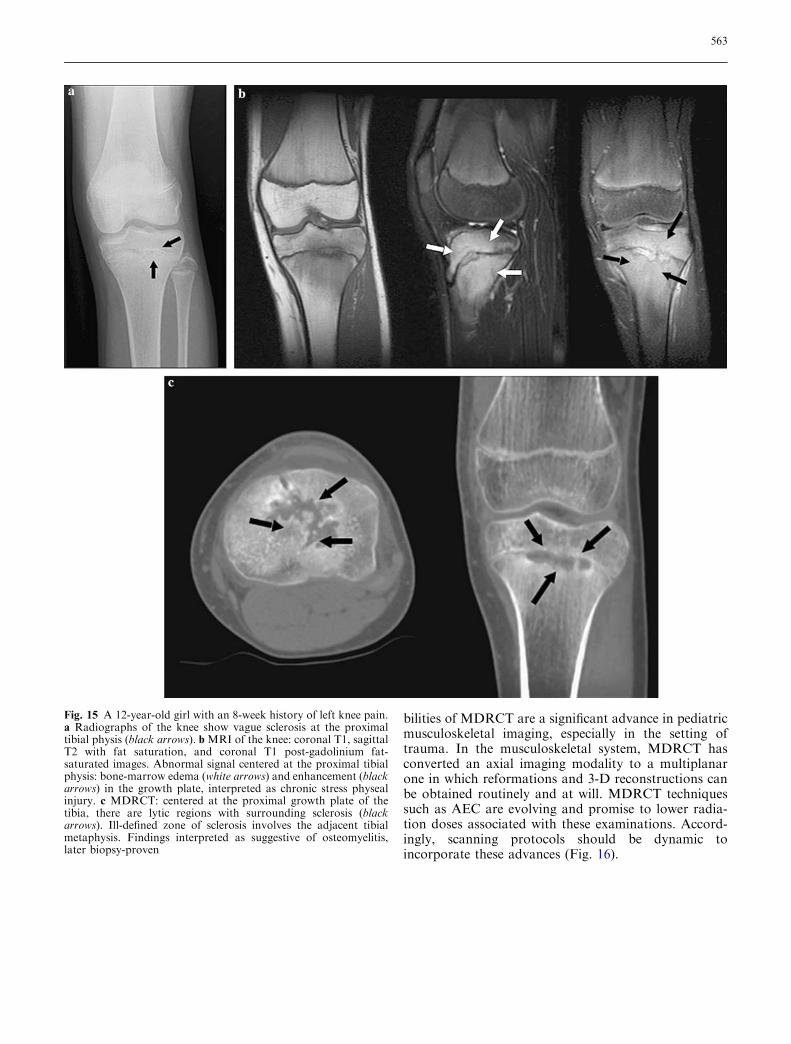
In our series, only one patient was diagnosed withosteomyelitis based on MDRCT. Although MRI is mostcommonly used at our institution to evaluate musculo-skeletal infection, this patient was initially misdiagnosedbased on MRI. The MRI in this case suggested a diag-nosis of chronic physeal stress injury (Fig. 15).
In summary, multidetector row CT allows rapid anddetailed evaluation of the musculoskeletal system. Rapidscanning, increased resolution, and multiplanar capa-
Fig. 13 An 8-year-old girl with a 6-month history of right hip painand limping gait. a Radiograph of the pelvis shows lytic lesion ofthe right acetabular roof (black arrows), with a slight sclerotic,ill-defined border. Biopsy-proven Langerhans’ cell histiocytosis.bMDRCT 7 weeks after intralesional cotricosteroid administrationshows minimal new bone formation (black arrowhead) consistentwith interval early healing. cMDRCT 16 months later shows stablesize of the lesion, with further healing (black arrowheads)
Fig. 14 An 8-year-old girl with a history of knee pain and mass inthe left medial tibia. a Radiograph of the left knee shows mixedlytic and sclerotic lesion of the proximal tibia, known aneurysmalbone cyst status postcurettage, grafting, and packing. b Follow-upMDRCT shows multiple destructive foci within the treated lesionwith fluid-fluid level (arrow) consistent with tumor recurrence.c MPR images demonstrate extent of lytic changes (white arrows)consistent with recurrence
562
bilities of MDRCT are a significant advance in pediatricmusculoskeletal imaging, especially in the setting oftrauma. In the musculoskeletal system, MDRCT hasconverted an axial imaging modality to a multiplanarone in which reformations and 3-D reconstructions canbe obtained routinely and at will. MDRCT techniquessuch as AEC are evolving and promise to lower radia-tion doses associated with these examinations. Accord-ingly, scanning protocols should be dynamic toincorporate these advances (Fig. 16).
Fig. 15 A 12-year-old girl with an 8-week history of left knee pain.a Radiographs of the knee show vague sclerosis at the proximaltibial physis (black arrows). b MRI of the knee: coronal T1, sagittalT2 with fat saturation, and coronal T1 post-gadolinium fat-saturated images. Abnormal signal centered at the proximal tibialphysis: bone-marrow edema (white arrows) and enhancement (blackarrows) in the growth plate, interpreted as chronic stress physealinjury. c MDRCT: centered at the proximal growth plate of thetibia, there are lytic regions with surrounding sclerosis (blackarrows). Ill-defined zone of sclerosis involves the adjacent tibialmetaphysis. Findings interpreted as suggestive of osteomyelitis,later biopsy-proven
563

Fig. 16 A 6-year-old boy with ahistory of unicameral bonecyst of the proximal humerus.a Axial MDRCT imageobtained with fixed tube currentof 140 kV, 88 mAs. Shows bonecyst with pathologic fractureanterolaterally. b Follow-upscan performed 10 months laterwith AutomA (120 kV milli-ampere-second of this particu-lar slice was 54) shows healingfracture
References
1. Buckwalter KA, Rydberg J, KopeckyKK, et al (2001) Musculoskeletalimaging with multislice CT. AJR176:979–986
2. Tanenbaum LN (2003) Multichannelhelical CT of the musculoskeletal sys-tem. Appl Radiol 32:15–24
3. Pretorius ES, Fishman EK (1999) Vol-ume-rendered three-dimensional spiralCT: musculoskeletal applications. Ra-diographics 19:1143–1160
4. Haramati N, Staron RB, Mazel-Sper-ling K, et al (1994) CT scans throughmetal scanning technique versus hard-ware composition. Comput Med Imag-ing Graph 18:429–434
5. Kalra MK, Maher MM, Toth TL, et al(2004) Strategies for CT radiation doseoptimization. Radiology 230:619–628
6. Kalra MK, Maher MM, Toth TL, et al(2004) Techniques and applications ofautomatic tube current modulation forCT. Radiology 230:619–628 (Oct. 21Epub ahead of publication)
7. Kalra MK, Maher MM, Kamath RS,et al (2004) Sixteen-slice multidetector-row CT of abdomen and pelvis: a studyfor optimization of z-axis modulationtechnique in 153 subjects. Radiology (inpress)
8. Chapman VM, Kalra MK, Halpern EF,et al (2004) D16-slice multidetector CTof the post-traumatic pediatric elbow:optimum parameters and associatedradiation dose. AJR (in press)
9. John SD (1999) Trends in pediatricemergency imaging. Radiol Clin NorthAm 37:995–1034, vi
10. Mahboubi S, Morris MC (2001) Imag-ing of spinal infections in children.Radiol Clin North Am 39:215–222
564
Copyright © 2022 FDOKUMEN