Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases
9
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases. Eur J Radiol (2010), doi:10.1016/j.ejrad.2010.06.055 ARTICLE IN PRESS G Model EURR-4917; No. of Pages 9 European Journal of Radiology xxx (2010) xxx–xxx Contents lists available at ScienceDirect European Journal of Radiology journal homepage: www.elsevier.com/locate/ejrad Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases Eugenio Rimondi a,∗ , Giuseppe Rossi b , Tommaso Bartalena g , Rosanna Ciminari a , Marco Alberghini c , Pietro Ruggieri d , Costantino Errani d , Andrea Angelini d , Teresa Calabrò d , Caterina Novella Abati d , Alba Balladelli e , Cristina Tranfaglia h , Andreas F. Mavrogenis d , Daniel Vanel f , Mario Mercuri d a Radiology Department, Istituto Ortopedico Rizzoli, Bologna, Italy b Interventional Angiography Department, Istituto Ortopedico Rizzoli, Bologna, Italy c Surgical Pathology Department, Istituto Ortopedico Rizzoli, Bologna, Italy d Orthopaedic Oncology Department, Istituto Ortopedico Rizzoli, Bologna, Italy e Laboratory of Experimental Oncology, Istituto Ortopedico Rizzoli, Bologna, Italy f Bone Tumor Center, Istituto Ortopedico Rizzoli, Bologna, Italy g Radiology Department, University of Bologna, Italy h Nuclear Medicine Department, Maggiore Hospital, Bologna, Italy article info Article history: Received 14 June 2010 Accepted 15 June 2010 Keywords: Musculoskeletal system Bone lesions Computed tomography Percutaneous biopsy abstract Introduction: Biopsy of the musculoskeletal system is useful in the management of bone lesions partic- ularly in oncology but they are often challenging procedures with a significant risk of complications. Computed tomography (CT)-guided needle biopsies may decrease these risks but doubts still exist about their diagnostic accuracy. This retrospective analysis of the experience of a single institution with per- cutaneous CT-guided biopsy of musculoskeletal lesions evaluates the results of these biopsies for bone lesions either in the appendicular skeleton or in the spine, and defines indications. Materials and methods: We reviewed the results of 2027 core needle biopsies performed over the past 18 years at the authors’ institution. The results obtained are subject of this paper. Results: In 1567 cases the correct diagnosis was made with the first CT-guided needle biopsy (77.3% accuracy rate), in 408 cases the sample was not diagnostic and in 52 inadequate. Within 30 days these 408 patients underwent another biopsy, which was diagnostic in 340 cases with a final diagnostic accu- racy of 94%. Highest accuracy rates were obtained in primary and secondary malignant lesions. Most false negative results were found in cervical lesions and in benign, pseudotumoral, flogistic, and sys- temic pathologies. There were 22 complications (18 transient paresis, 3 haematomas, 1 retroperitoneal haematoma) which had no influence on the treatment strategy, nor on patient outcome. Conclusion: This technique is reliable and safe and should be considered nowadays the gold standard for biopsies of the musculoskeletal system. © 2010 Elsevier Ireland Ltd. All rights reserved. 1. Introduction An accurate biopsy is essential in the diagnosis of musculoskele- tal lesions particularly in the diagnostic work-up and management of bone tumors, and although modern radiological imaging tech- niques have a good predictive value in differential diagnosis, a histological examination is usually necessary to plan further treat- ment [1,2]. Biopsy is a compromise between the need of significant tissue but must avoid contamination both local or in blood cir- ∗ Corresponding author at: Radiology Department, Rizzoli Orthopaedic Institute, Via Pupilli 1, 40136 Bologna, Italy. Tel.: +39 0516836; fax: +39 0516366280. E-mail address: [email protected] (E. Rimondi). culation [3,4]. To avoid contamination, it is mandatory not to open the tumor capsule, not to violate compartmental barriers, not to contaminate other compartments and extracompartmen- tal areas, not to dissect outside the surgical line and not to cause haematoma. There are different types of biopsy: fine needle, trocar, frozen, incisional, and excisional. Traditionally, open biopsy (incisional/excisional) has been the gold standard for musculoskeletal lesions, providing adequate material for histological and immunohistochemical studies in most cases, resulting in a highly diagnostic procedure. However, in ver- tebral and in deeply seated pelvic bone lesions, performing an open biopsy can be a difficult procedure with a significant risk of com- plications [5,6]. 0720-048X/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2010.06.055
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases

G
E
PR
EPAa
b
c
d
e
f
g
h
a
ARA
KMBCP
1
tonhmt
V
0d
ARTICLE IN PRESSModel
URR-4917; No. of Pages 9
European Journal of Radiology xxx (2010) xxx–xxx
Contents lists available at ScienceDirect
European Journal of Radiology
journa l homepage: www.e lsev ier .com/ locate /e j rad
ercutaneous CT-guided biopsy of the musculoskeletal system:esults of 2027 cases
ugenio Rimondia,∗, Giuseppe Rossib, Tommaso Bartalenag, Rosanna Ciminari a, Marco Alberghini c,ietro Ruggierid, Costantino Erranid, Andrea Angelinid, Teresa Calabròd, Caterina Novella Abatid,lba Balladelli e, Cristina Tranfagliah, Andreas F. Mavrogenisd, Daniel Vanel f, Mario Mercurid
Radiology Department, Istituto Ortopedico Rizzoli, Bologna, ItalyInterventional Angiography Department, Istituto Ortopedico Rizzoli, Bologna, ItalySurgical Pathology Department, Istituto Ortopedico Rizzoli, Bologna, ItalyOrthopaedic Oncology Department, Istituto Ortopedico Rizzoli, Bologna, ItalyLaboratory of Experimental Oncology, Istituto Ortopedico Rizzoli, Bologna, ItalyBone Tumor Center, Istituto Ortopedico Rizzoli, Bologna, ItalyRadiology Department, University of Bologna, ItalyNuclear Medicine Department, Maggiore Hospital, Bologna, Italy
r t i c l e i n f o
rticle history:eceived 14 June 2010ccepted 15 June 2010
eywords:usculoskeletal system
one lesionsomputed tomographyercutaneous biopsy
a b s t r a c t
Introduction: Biopsy of the musculoskeletal system is useful in the management of bone lesions partic-ularly in oncology but they are often challenging procedures with a significant risk of complications.Computed tomography (CT)-guided needle biopsies may decrease these risks but doubts still exist abouttheir diagnostic accuracy. This retrospective analysis of the experience of a single institution with per-cutaneous CT-guided biopsy of musculoskeletal lesions evaluates the results of these biopsies for bonelesions either in the appendicular skeleton or in the spine, and defines indications.Materials and methods: We reviewed the results of 2027 core needle biopsies performed over the past 18years at the authors’ institution. The results obtained are subject of this paper.Results: In 1567 cases the correct diagnosis was made with the first CT-guided needle biopsy (77.3%accuracy rate), in 408 cases the sample was not diagnostic and in 52 inadequate. Within 30 days these408 patients underwent another biopsy, which was diagnostic in 340 cases with a final diagnostic accu-
racy of 94%. Highest accuracy rates were obtained in primary and secondary malignant lesions. Mostfalse negative results were found in cervical lesions and in benign, pseudotumoral, flogistic, and sys-temic pathologies. There were 22 complications (18 transient paresis, 3 haematomas, 1 retroperitonealhaematoma) which had no influence on the treatment strategy, nor on patient outcome.Conclusion: This technique is reliable and safe and should be considered nowadays the gold standard forbiopsies of the musculoskeletal system.. Introduction
An accurate biopsy is essential in the diagnosis of musculoskele-al lesions particularly in the diagnostic work-up and managementf bone tumors, and although modern radiological imaging tech-
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
iques have a good predictive value in differential diagnosis, aistological examination is usually necessary to plan further treat-ent [1,2]. Biopsy is a compromise between the need of significant
issue but must avoid contamination both local or in blood cir-
∗ Corresponding author at: Radiology Department, Rizzoli Orthopaedic Institute,ia Pupilli 1, 40136 Bologna, Italy. Tel.: +39 0516836; fax: +39 0516366280.
E-mail address: [email protected] (E. Rimondi).
720-048X/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2010.06.055
© 2010 Elsevier Ireland Ltd. All rights reserved.
culation [3,4]. To avoid contamination, it is mandatory not toopen the tumor capsule, not to violate compartmental barriers,not to contaminate other compartments and extracompartmen-tal areas, not to dissect outside the surgical line and not to causehaematoma.
There are different types of biopsy: fine needle, trocar, frozen,incisional, and excisional.
Traditionally, open biopsy (incisional/excisional) has been thegold standard for musculoskeletal lesions, providing adequate
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
material for histological and immunohistochemical studies in mostcases, resulting in a highly diagnostic procedure. However, in ver-tebral and in deeply seated pelvic bone lesions, performing an openbiopsy can be a difficult procedure with a significant risk of com-plications [5,6].

IN PRESSG
E
2 rnal of Radiology xxx (2010) xxx–xxx
gphatlgafrbt
ccp
2
bstlT
dw2idobr
sppaosnpCt
awikrw
bIBMwTa
tg(
ARTICLEModel
URR-4917; No. of Pages 9
E. Rimondi et al. / European Jou
Alternatively to open biopsy, percutaneous needle biopsy hasained popularity showing a good accuracy with a less invasiverocedure. It can be performed in an outpatient clinic or in dayospital, since general anesthesia is rarely necessary. Cost and timere lower than those of an open biopsy and there is less risk ofumor spread, infections and/or wound breakdown. In deep lesions,ike in the pelvis or spine, the aid of computed tomography (CT)-uidance has further increased accuracy [7], reduced complicationsnd has therefore, in most instances become a standard procedureor diagnosis [8–11]. Biopsy must be carried out in specialized refer-al centers to reduce the risk of misdiagnosis, non-representativeiospies, related complications and overall consequent changes inreatment and prognosis [12].
Purpose of this paper is to assess diagnostic accuracy andlinical usefulness of percutaneous CT-guided trocar biopsy in mus-uloskeletal system lesions. We reviewed 2027 trocar biopsieserformed at our institution over the last 18 years.
. Materials and methods
From January 1990 to December 2008, 2027 core needle CT-iopsies were performed. All histologic diagnoses and imagingtudies were reviewed. Site of the procedure included spine in 703,horacic cage in 85, upper limb in 141, pelvis in 492 and lowerimb in 606 patients. Patient data and biopsy site are reported inable 1.
The overall size (transverse and cranio-caudaliameters—intra/extracompartmental) of the spinal lesionsas between 0.5 cm and 2.5 cm in 48 lesions, between
.5 cm and 3.5 cm in 584, and 3.5 cm or more in the remain-ng 71 cases. Overall size (transverse and cranio-caudaliameters—intra/extracompartmental) of the lesions of thether skeletal sites were between 0.5 cm and 2.5 cm in 21 lesions,etween 2.5 cm and 3.5 cm in 261 and 3.5 cm or more in theemaining 1042 cases.
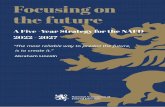
Complete staging of the disease, usually with radiographs, bonecan, CT with contrast media and MRI was carried out. In an allergicatient or in systemic diseases like myeloma a pre-biopsy CT waserformed without contrast media and in these cases an MRI waslways carried out two or three days before the procedure. The rolef CT with contrast media or of MRI is useful to identify site andize of the lesion and to define its features: morphology (sclerotic,ecrotic and/or hemorrhagic, viable part), intra- or also extracom-artmental extension, neurovascular bundles (Fig. 1). By means ofT and MRI three basic operative criteria can be settled: approach,rocar, and where to sample.
The patient’s position (supine, prone, lateral right or left) variedccording to the anatomical region affected. The needle approachas chosen according to a potential future surgical procedure, that
s on the line of an ideal surgical incision to operate the lesion, thuseeping the biopsy tract easily excisable (Table 2). For a suspectecurrence, in patients previously surgically treated, the approachas always performed on the surgical scar.
All biopsies were carried out with three different core needleiopsy sets: Trap System Set (HS-Hospital Services S.p.A., Roma,
taly), Craig-Kogler Set (Chiruma S.r.l., S. Giovanni in Persiceto,ologna, Italy), and the small caliber Bonopty Insertion Set (RadiS, Uppsala, Sweden) (Fig. 2). We used the small caliber set onlyhen site, size or approach did not allow the use of a larger needle.
able 3 summarizes the types and features of the different needles,
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
nd the number of biopsies performed with each set.We always tried to retrieve the sample from the viable part of
he lesion, on the outskirts if a sarcoma was suspected (centripetalrowth pattern), in the depth for carcinoma and systemic diseaseinfiltrating pattern), in both and in the adjacent soft tissues for
Fig. 1. Pre-biopsy CT with contrast. Size, intra and extracompartmental extension,lesion morphology and viable part. Also the neurovascular bundles are clearly iden-tified.
inflammatory lesions; for the latter, a sample for microbiology wascollected. At least two samples were collected. For multiple lesionsthe biopsy was undertaken at the most easily approachable site.
A scout-view radiogram was taken focused on the affectedarea. The setting of the thickness and slice interval wasrelated to site and size of the lesion. Usually in the spine weused 1 mm thickness–1 mm interval for the cervical spine andupper thoracic tract (T1–T6), for lower thoracic tract (T7–T12)1–2 mm thickness–1–2 mm interval, for lumbar and sacral spine3–5 mm thickness–3 mm interval and for coccygeal bone 1–3 mmthickness–1–2 mm interval. In 63 cases, in the thoracic and lumbarspine, in patients with particular cyphosis or lordosis, an angulatedapproach was chosen by tilting the CT-gantry parallel to the upperand lower surface of the vertebral body. Usually in other skeletalsites we used 1 mm thickness and interval for sternum, ribs andclavicle, 3–5 mm thickness–3 mm interval in the remaining skele-tal. Under CT-guidance the best insertion point was selected andmarked on the skin. Then needle insertion, with coaxial or tandemtechnique, was done under sequential scans (Figs. 3–5). A lowerrate of milli-Amperes (mAs) was used to monitor needle approachto the lesion, so as to reduce the dose absorbed by the patient.
Samples were sent to the pathologist in saline solution. A swabsample was obtained for microbiology in 86 suspected infections.
All biopsies were carried out after informed consent wasobtained and all, but 37 biopsies, performed under local anesthesia:infiltration of mepivacaine cloridate at 2% (5–15 cm3). Thirty-sevenchildren, between 5 and 10 years of age, underwent a generalanesthesia. Antibiotics were discontinued 48 h and FANS a weekbefore biopsy. The time required for the complete biopsy pro-cedure, including pre-biopsy CT, varied from 35 min to 70 min(median 30–35).
3. Results
CT-guided biopsy was diagnostic in 1567 of 2027 cases (77.3%):
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
445 malignant bone tumors or systemic diseases, 360 benign,66 pseudotumors, 320 metastases. In 202 patients an acute orchronic inflammatory disease was found, 174 had other diagnoses(metabolic diseases, chronic degenerative arthropathies, Paget’sdisease, gout, etc.). In 771 cases (primary malignant, secondary

Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guided biopsy of the musculoskeletal system: Results of 2027 cases. Eur JRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx 3
Table 1Demographic and detailed spinal location of 2027 CT-guided biopsies.a Males 1091 (54%), females 936 (46%). Median age 46 years (range 3–87 years). 1263 in-patients, 764out-patients.
Spine location 703 (34%)
Cervical (22) Thoracic (206) Lumbar (283) Sacral (192)
C1 (2) T1–T4 (35) L1 (51) S1 (103)C2 (2) T5–T8 (58) L2 (53) S2 (52)C3 (5) T9–T12 (113) L3 (41) S3 (15)C6 (5) L4 (66) SI-joint (17)C7 (8) L5 (72) Tailbone (5)
Other skeletal sites 1324 (66%)
Thoracic cage (85) Upper limb (141) Pelvis (492) Lower limb (606)
Sternum (17) Arm (97) Ilium (301) Thigh (388)Rib (15) Forearm (39) Ischium (117) Leg (193)Scapula and clavicle (53) Wrist–hand (5) Pubis (74) Foot (25)
a January 1990–May 1997: CT Sytec 3000 (General Electric, Milwaukee, USA). June 1997–December 2008: High-Speed Cti (General Electric, Milwaukee, USA).
Table 2Approaches of 2027 CT-guided biopsies.
Spine site Patient position Biopsy approach 703 (34%)
Cervical tract Supine Anterolaterala (11)Prone Transpedicular (7)Prone Midposterior (4)
Dorsal tract Prone Midposterior (5)Prone, lateral left/right Transpedicular (156)Lateral left/right Transcostovertebral (4)Lateral leftb Posterolateral (41)
Lumbar tract Prone Midposterior (17)Prone, lateral right/left Transpedicular (167)Lateral rightb Posterolateral (99)
Sacral tract–SI-joint tailbone Prone Midposterior (192)
Other skeletal sites Patient position Biopsy approach 1324 (66%)
Thoracic cageSternum–rib Supine Anterior (32)Scapula–clavicle Prone Midposterior (53)
Upper limbArm Supine Anterior (97)Forearm Supine Anterior (39)Wrist–hand Supine Anterior (5)
PelvisIlium Supine/prone Anterior/lateral/posterior (301)Ischium Prone Posterior (117)Pubis Anterior Anterior (74)
Lower limbThigh Supine Lateral (388)Leg Supine/pronec Medial (193)Foot Supine Anteromed/lat (25)
a Between windpipe and neurovascular bundle or behind the neurovascular bundle.b Lateral left/right to avoid cava/aorta.c Posterior popliteal in 5 lesions reaching the skin.
Table 3Biopsy set used in 2027 percutaneous CT-guided biopsies.
Trap system Craig-Kogler Bonopty
Trocar calibera 8/4–5 mm with 10/15 cm sharp stylet 8 G/4–5 mm with 19 cm sharp guide 15 G/1.8 mm, 14 G/2.1 mm with 12.2/16 cm drillsTrocar length 10–15 cm 10 cm 9.5 cmExtractor 10/15 cm Flexible steel (9 G) 21 cm Coaxial (12 G) 16 cm Cannula (18 G)Multiple coaxial No Yes Yes
Action systemb
#Biopsies 1927 71 29
a Inner and outer caliber.b With this system the trocar remains positioned inside the lesion while multiple samples can be taken through the needle.

ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
4 E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx
F A–D) CK biopsy
mlscwmeb
IcimW
Fsra
ig. 2. Trocar and core needle used for the 2027 CT-guided percutaneous biopsy. (ogler trocar, (D) Craig-Kogler sample retrieving, (E) Trap System, and (F) Bonopty
alignant, benign and pseudotumoral), a surgical treatment fol-owed, confirming the biopsy diagnosis. The other 796 biopsies (100ystemic malignancies: Hodgkin, non-Hodgkin, myeloma, plasmo-ytoma, 320 metastases, 202 inflammatory diseases and 174 othersere not followed by a surgical treatment. In these cases the treat-ent response (chemo and/or radiotherapy, antibiotics, palliative
mbolization) and the clinical course confirmed the accuracy of theiopsy.
Four hundred and sixty CT-guided biopsies were not diagnostic.n 52 cases (2.6%) the sample was inadequate, in the remaining 408
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
ases (20.1%) the retrieved tissue was atypical (e.g. sclerotic bone,ntramedullary sclerosis/fibrosis, blood clots, intramedullary lipo-
atosis, etc.) and did not lead to a specific histological diagnosis.ithin 30 days these patients all underwent a second diagnos-
ig. 3. Choice of the approach (A–D): pelvic approach on the surgical incisional line forelection of the slice: line 1 represents the slice selected, usually that in which the lesiepresents the surgical line crossed by the slice selected and the skin insertion point;nesthesia (D), the trocar inserted and the measured distance (line 1) to the bottom of th
raig-Kogler system: (A) Craig-Kogler assembled, (B) Craig-Kogler guide, (C) Craig-core set and drills (see Table 3).
tic procedure: 52 patients had an incisional biopsy, 408 anotherpercutaneous biopsy.
The diagnosis of the 52 open biopsies was 2 angiomas, 7 giantcell tumors, 15 aneurysmal bone cysts, 26 systemic diseases (lym-phoma, myeloma, plasmocytoma), 1 primary malignant and 1metastasis.
Three hundred and forty second percutaneous biopsies werediagnostic: 299 revealed 50 malignant bone tumors or systemicdiseases, 63 benign lesions, 39 pseudotumors, 33 metastases, 53acute or chronic inflammatory lesions and 61 had other diagnoses
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
(Table 6). In the remaining 41 of these 340 cases, in which the firstdiagnosis did not lead to a specific pathology, the first diagnosisnot only was confirmed but was further defined (stress or insuffi-ciency fracture, edema in irradiated bone, geode in arthrosis, bone
lateral pelvis (Smith–Petersen line) (A), scout-view and the slices carried out (B),on is largest (see medial to line 1 the femoral neurovascolar bundles); the + signline 2 and line 3 the trocar insertion angle and the length of the trocar (C), locale lesion. Trap System trocar: single coaxial biopsy.

Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx 5
Fig. 4. Technique (A and B): (A) Craig-Kogler: multiple coaxial trocar biopsy at T9level and (B) Trap System trocar biopsy: tandem technique the needle used for anes-thesia is left inside and works as a monorail for the trocar biopsy (single coaxial) atT9 level.
Fig. 5. Samples retrieved (A and B): (A) large sample with trocar (Tr
Table 6Accuracy rates versus histotype regardless site, lesion size and needle gauge.
Histotype I CT-guidedbiopsy
II CT-guidedbiopsy
Open biopsy
1567 (77.3%) 340 (16.8%) 120 (5.9%)
Primary benign 360 63 39Pseudotumoral 66 39 27Primary malignant 334 39 1Systemic malignant 111 11 33Secondary malignant 320 33 1Inflammatory disease 202 53 9Othera,b 174 102b 10
Overall accuracy Percutaneousbiopsy failure
1097 (94.1%) 120 (5.9%)
a Paget’s disease, gout, metabolic disease (e.g. hyperparathyroidism).
Table 4Diagnostic accuracy after the first percutaneous CT-guided biopsy according to different m
Features of the sample Total Thoracic cage
Inadequate 2.6% 1.5%Not diagnostic 20.1% 16.4%Diagnostic 77.3% 82.1%
Table 5Diagnostic accuracy after the second percutaneous CT-guided biopsy according to differe
Diagnosis Total Thoracic cage Low
Open biopsy 120 (5.9%) 4 (4.7%) 8CT-guided biopsy 1907 (94.1%) 81 (95.3%) 598
b 41 Cases further defined by the second percutaneous biopsy included in thisgroup (see text): aspecific non-pathologic diagnoses as stress fractures, osteoporoticfragments with bone resorption, edema in irradiated bone, bone sclerosis or necro-sis, and subchondral cystic lesion in osteoarthritis.
necrosis). These “41 negative cases” were followed-up by clinicaland radiological controls for a period variable from 8 months to 3years and no diagnostic adjustments were made. These “negativecases” were put in the group of other diagnosis.
Cases non-diagnostic at the second percutaneous procedureunderwent a open biopsy which resulted in 17 systemic lesions,11 aneurysmal bone cysts, 5 giant cell tumors, 25 benign latent and10 chronic inflammatory lesions. This gave an overall rate of non-diagnostic procedures of 5.9% and an overall diagnostic accuracy of94.1%.
Table 4 shows the accuracy after the first percutaneousCT-guided biopsies according to the different musculoskeletal seg-ments. There were more inadequate samples in the spine and morenon-diagnostic aspecific results in the upper limb. Table 5 shows
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
ap System) and (B) small sample with core needle (Bonopty).
the accuracy of the percutaneous CT-guided biopsies accordingto the different musculoskeletal segments after the second pro-cedure. Lower accuracy was always in the spine followed by theupper limb. Table 6 shows the accuracy rates based on histologi-cal diagnosis regardless site and size of the lesion. False negative
usculoskeletal segments.
Lower limb Pelvis limb Spine Upper
2.4% 2.1% 3.9% 0.8%19.6% 21.5% 19.8% 30.4%78.0% 76.4% 76.4% 68.8%
nt musculoskeletal segments. Number and percentage.
er limb Pelvis limb Spine Upper
(1%) 15 (3%) 78 (11%) 15 (10.6%)(99%) 477 (97%) 625 (89%) 126 (89.4%)

ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
6 E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx
Table 7Inadequate material versus lesion size regardless site, histotype and needle gauge(2 samples retrieved).
Size Total Diagnostic Inadequate
0.5–2.5 cm 69 34 (49.3%) 35 (50.7%)2.5–3.5 cm 845 820 (97%) 25 (3%)3.5 cm or more 1113 1053 (94.6%) 60 (5.4%)
Table 8Diagnostic accuracy related to morphological features of the lesions regardless site,size, histotype and needle gauge.
Size Total Diagnostic Inadequate
Lytic bone lesions(prevalentlyintracompartmental)
545 515 (94.4%) 30 (5.6%)
Sclerotic bone lesions(prevalentlyintracompartmental)
491 430 (87.6%) 61 (12.4%)
Mixed 991 962 (97%) 29 (3%)
dfassplm
bc
1rvn
4
iiipttdmt
1
2
3
456
cl
(intra/extracompartmentalwith soft tissueinvolvement)
iagnosis was more frequent in benign tumors, systemic malignantorms, pseudotumoral and inflammatory lesions, while in primarynd secondary malignant lesions accuracy was very high. Table 7hows the percentage of inadequate samples according to lesionize regardless site, histotype and needle gauge. Inadequate sam-les were more frequent in small and, but less frequently, in huge
esions. Table 8 shows the percentage of diagnosis depending onorphological features of the lesion, lytic, sclerotic and mixed.Of the 86 cases swab samples were collected, 38 (44.2%) showed
acterial growth (27 tuberculosis, 6 Brucellosis and 3 Escherichiaoli). In 48 cases (55.8%) no bacterial growth was detected.
Biopsy related complications were reported in 22 cases (1.1%):8 transient paresis of lower limbs, 3 psoas muscle haematomas, 1etroperitoneal haematoma due to accidental puncture of a lumbarein that resolved spontaneously in a day. The 22 complicationseither affected treatment strategy nor overall patient outcome.
. Discussion
The radiological study of musculoskeletal lesions has signif-cantly improved with the use of CT and MR imaging. But thismprovement is essentially morphologic. It offers excellent imag-ng of anatomical extension and a clear identification of the activeart of the lesion after contrast. In fact the low specificity allowshe etiologic diagnosis only in a few cases, for most musculoskele-al lesions, instead, a histological study is required for definitiveiagnosis [8,11]. The indications for a musculoskeletal biopsy are,ainly, primary or secondary tumors, and infections. Biopsy is used
o:
. determine the nature of a solitary bone tissue lesion with non-specific imaging features;
. confirm or exclude musculoskeletal metastasis in patients witha diagnosed primary malignant tumor;
. exclude malignancy in vertebral body compression (metastasesor myeloma);
. evaluate recurrences after surgical and/or medical treatment;
. investigate pathological fractures;
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
. investigate and confirm musculoskeletal infections.
Contraindications are essentially coagulopathy and hydatidyst. We performed biopsies also in thoracic vertebrae (isolatedesions) where a hypervascular lesion was suspected (usually a
Fig. 6. Recurrence of a previously surgically treated chordoma of the sacrum. Lyticlesion (Trap System). Trocar inserted on the surgical scar. Note the big bowel herni-ated out of the pelvis.
secondary malignant lesion from kidney) ready with a foam gelfor checking bleeding, but always in patients with normal hematicdiathesis.
An absolute contraindication is when biopsy does not give addi-tional information or does not change patient management.
All biopsies, regardless of site, lesion size and type of needlesused, were performed with strict adherence to anatomic compart-ments; uninvolved compartments had to be avoided by the needle[13], for already operated patient the needle approach was done on
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
the surgical scar (Fig. 6). With the patient in position for the rightapproach, the needle was inserted on the line of the ideal surgicalincision.
Percutaneous biopsy of a musculoskeletal lesion can be per-formed either by fine needle aspiration (FNA) or trocar needle

ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx 7
F undlel lasmo
bw(TfatOmFpdmamatpa6hsn
Fl
ig. 7. Cervical spine C2 (A and B): (A) lateral approach behind the neurovascular besion (Bonopty). Small needle gauge but medium lesion. More samples retrieved. P
iopsy (TNB). FNA needles have a diameter of less than 1 mm,hereas trocar needles have a diameter of more than 1.5 mm
1.5–5 mm). At our institution we do not perform FNA biopsies.his method of biopsy only provides cells that can be analyzedor ultrastructural abnormalities but does not detect histology forssessment of intracellular relationships, tissue anatomical archi-ecture is not preserved and only cytological studies are possible.nly a very well trained team can use it with reliable results. Thisight make a histological diagnosis more difficult and less accurate.
or primary malignant tumors, anatomical architecture is crucial,articularly in mesenchymal tumors, which are among the mostifficult to diagnose by pathologist. Furthermore, sampling errorsay occur due to the small amount of material obtained [14]. Inrecent review of FNA and trocar biopsies in 359 patients withusculoskeletal lesions the accuracy of fine needle percutaneous
spiration biopsy is reported over 60% but significantly lower thanhat of core needle biopsy (more than 70%) [15]. In a more recentaper (only 50 cases and no biopsies performed in the spine), FNA
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
chieved a diagnostic accuracy rate of 88% for nature of the lesion,4% for specific diagnosis, 78% for histologic grading, and 74% foristologic typing [16]. In an even more recent paper on 155 biop-ies, more in the bone than in the soft tissues, of 145 adult patients,o differences were reported in diagnostic yield (77% for all lesions
ig. 8. Cervical spine C7 (A and B): anterior approach medial to the neurovascular bundlesion (Trap System). Metastases.
and parotid gland and in front of the nervous root and the vertebral artery, (B) lyticcytoma.
but it is not specified if there were biopsies in the spine) whatevergauge used (range of gauge 14–18, usually 15 G used) underliningthe importance not only of more than one sample but also of samplesize [17]. We used a 15 G needle (bonopty-multiple coaxial system)only in 29 cases: in the cervical and thoracic spine 6 times and in thesmall bones of hand and foot in the last 23 cases (all in children andin small lesions 0.5–1.5 cm) but always obtaining more than onesample (Fig. 7). For these 29 cases our accuracy rate was less thanthat of Wu’s series: 3 out 6 in spine, one diagnostic at the secondbiopsy, 17 out of 23 in the other skeletal segments for an overallaccuracy of 69%. However, also in Wu’s study small size lesions hada lower accuracy.
Other authors claim that trocar biopsy achieves an accuracy rateof 93% for nature of lesions, 83% for specific diagnosis, 83% for his-tologic grading, and 90% for histologic typing. Both biopsy methodshave a higher diagnostic accuracy rate for high-grade tumors com-pared to low-grade or benign lesions in determining nature, specificdiagnosis, and histologic grading [6] (Figs. 8–10). Sometimes also
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
larger samples can be inadequate or not diagnostic for differen-tial diagnosis of lesions like osteofibrous dysplasia, monostoticfibrous dysplasia, dedifferentiated chondrosarcoma, hemangioen-dothelioma. In 17 of these cases as first biopsy we used a trocar(Trap System) but we had to repeat it because radiological and
e and lateral to the windpipe and esophagus. (A) Anesthesia and (B) biopsy. Mixed

Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
ARTICLE IN PRESSG Model
EURR-4917; No. of Pages 9
8 E. Rimondi et al. / European Journal of Radiology xxx (2010) xxx–xxx
Fig. 9. Cervical spine C2 posterior approach. Lytic lesion. Chronic ABC (Trap System).
Fig. 10. Thoracic spine T4 (A and B): (A) patient in lateral left position, transpedicularapproach and (B) lytic lesion (Trap System). Myeloma.
Fig. 11. Cervical Spine C3 posterior approach. 1st Percutaneous biopsy. Failure ofthe percutaneous biopsy. Lytic lesion, inadequate sample (Trap System). The patientunderwent an open biopsy: metastases.
clinical correlation was not consistent with histological results;moreover, also with a big trocar inadequate samples are possiblealso in patients with malignancy (Fig. 11).
At first biopsy we had 52 inadequate samples and 408non-diagnostic samples. All these cases were reviewed in a mul-tidisciplinary way by an orthopaedic surgeon, pathologist andradiologist and since the diagnosis was not consistent with theclinical and radiological findings the biopsy was repeated. Anotherpercutaneous biopsy for the 408 non-diagnostic samples was per-formed targeting a different area of the lesion, instead whensamples were inadequate an open biopsy was done. Although over-all accuracy increased after the second percutaneous biopsy, loweraccuracy was always found in the spine (in particular for the cervi-cal and upper thoracic segment).
This lower accuracy rate can be correlated to the relativelysmaller size of the vertebra and to the difficulties in obtainingmore than one core. The results for the cervical tract, however,were based on a relatively small group of cases. Instead, for theupper limb, we think the cause is probably linked to the nature ofthe lesions, many were elderly patients with arthrosic lesions orsystemic diseases.
Also histotype of the lesion influences accuracy of the percu-taneous CT-guided needle biopsy. Other authors have previouslydescribed a tendency towards higher accuracy in metastatic lesionscompared to primary bone tumors. In our series most false neg-ative results were found in biopsies of benign tumors, systemicmalignant lesions, flogistic lesions, and pseudotumorous lesions.Accuracy in primary and secondary malignant, lesions was veryhigh. Fibrotic, collagenous, deeply vascularized and sometimescolliquative features are usually more typical of benign, flogistic-like colliquative tubercolosis, or systemic lesions, aneurysmal bone
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
cyst, hemangioma, whose thin membrane, endothelium or scat-tered nodules were missed in the first biopsy. Malignant lesions,on the other hand usually contain more cohesive cells and stroma.Careful evaluation of the pre-biopsy imaging studies is necessary to

ING
E
rnal o
oiinbSfiacpl
oosbdrnleti
Foiwlii
iiciyfoa
5
af[[atl[
dtsb
[
[
[
[
[
[
[
[
[
Roentgenol 2006;186:977–80.[19] Wu JS, Gorbachova T, Morrison WB, et al. Imaging guided bone biopsy for
ARTICLEModel
URR-4917; No. of Pages 9
E. Rimondi et al. / European Jou
btain tissue from the viable part of the lesion: from the periphery,f expansile, in depth if infiltrative, in both and in the soft tissues ift seems inflammatory [2]. In systemic malignant disease (Hodgkin,on-Hodgkin lymphoma and myeloma) histological diagnosis cane difficult and is often based on immunohistochemical stainings.ome of our cases were negative for immunohistochemistry at therst needle biopsy but positive at the second. This might be due totechnical error during the needle biopsy, resulting in an insuffi-
ient amount of sample tissue or non-diagnostic tissue. This couldartially explain the false negative results in systemic malignant
esions.If an infection (osteomyelitis, spondylitis) is suspected antibi-
tics should be interrupted at least 24–48 h before biopsy. Accuracyf percutaneous disc biopsy has been reported as low as 47% forpondilodiscitis, both disc and adjacent subchondral bone shoulde included in the specimen. When diagnosis of osteomyelitis andiscitis is obvious, biopsy with the sole purpose of obtaining mate-ial for culture should be performed. Because of the high rate ofegative cultures about 40–60%, both histological and microbio-
ogical assessment are mandatory [18,19]. In our series culturalxaminations were negative in 55% of cases. Wu et al. found thathe collection of at least 2 ml of fluid from large abscess cavitiesncreased culture positivity [19].
Also size and morphological features of the lesions affect results.or size, a higher diagnostic accuracy expressed in percentage wasbtained in medium size lesions (2.5–3.5 cm), in absolute numbers,n large lesions (more than 3.5 cm), and a lower diagnostic accuracy
as seen in small lesions for difficulty in targeting. Paradoxically,arger lesions, due to the rapid growth, for the possibility of target-ng a necrotic or nonviable area. In this case, after reviewing themaging we targeted a different area.
For the morphological features the best results were obtainedn mixed and in osteolytic lesions, the worst in the sclerotic ones. Its therefore useful to retrieve samples from ostelytic or soft tissueomponents of the lesion, as sampling in sclerotic areas may resultn a poor yield. In a recent paper Wu et al. underlined a diagnosticield for medium and large lesions of about 76–85% and a 87% yieldor osteolytic bone lesions compared to 57% yields for the scleroticnes [19]. The goal should be to obtain a sample as homogeneouss possible and in good quantity for ancillary studies.
. Conclusions
CT-guided percutaneous core needle biopsy is a fast, economic,nd safe procedure. Diagnostic accuracy is influenced by severalactors: the needle used [15,16,20], site, size, nature of the lesions17] and almost of all the institute where the biopsy is performed12]. Success rate is higher with big trocar and in malignant lesions,nd lower with small needles and in benign, pseudotumoral, sys-emic and inflammatory lesions, especially when chronic. In spineesions, particularly in the cervical segment, accuracy rate is lower11].
Please cite this article in press as: Rimondi E, et al. Percutaneous CT-guideRadiol (2010), doi:10.1016/j.ejrad.2010.06.055
If the histological diagnosis after percutaneous biopsy is stilloubtful or the result is not consistent with the clinical and/orhe imaging suspected diagnosis, the percutaneous needle biopsyhould be repeated. Only in a few cases an incisional biopsy shoulde necessary.
[
PRESSf Radiology xxx (2010) xxx–xxx 9
Therefore CT-guided biopsy should be recommended for most ofthe bone lesions, namely deeply located and spinal lesions. Failuresof this procedure can be minimized in experienced hands with acareful previous evaluation of the case and a team approach.
Conflict of interest
There are no conflicts of interest with any author.
Acknowledgements
Authors acknowledge Ms. Cristina Ghinelli, medical artist, forthe graphics.
References
[1] Campanacci M, Mercuri M, Gamberini G. Biopsy. Chir Organi Mov1995;80(2):113–23.
[2] Bickels J, Jelinek J, ShmooklerB, et al. Biopsy of muscoluloskeletal tumors. Cur-rent concepts. Cinical Orthop Relat Res 2001;368:212–9.
[3] Schwartz HS, Sprengler DM. Needle tract recurrences after closed biopsyfor sarcoma: three cases and review of the literature. Ann Sur Oncol1997;4(3):228–36.
[4] Zoubek A, Kovar H, Kronberger M, et al. Mobilization of tumour cells dur-ing biopsy in an infant with Ewing sarcoma. Eur J Pediatry 1996;155(5):373–6.
[5] Skrzynski MC, Biermann JS, Montag A, et al. Diagnostic accuracy and chargesavings of outpatient core needle biopsy compared with open biopsy of mus-culoskeletal tumors. J Bone Joint Surg Am 1996;78(5):644–9.
[6] Puri A, Shingade V, Agarwal M, et al. CT-guided percutaneous core needlebiopsy in deep seated musculoskeletal lesions: a prospective study of 128 cases.Skeletal Radiol 2006;35(3):138–43.
[7] Issakov J, Flusser G, Kollender Y, et al. Computed tomography-guided coreneedle biopsy for bone and soft tissue tumors. Isr Med Assoc J 2003;5:28–30.
[8] Rimondi E, Busacca M, Moio A, et al. Computerized tomography guided biopsyin the diagnosis of neoplastic and inflammatory lesions of the pelvis. RadiolMed 2001;101(1–2):60–5.
[9] Monti C, Rimondi E, Rollo G, et al. Percutaneous computed tomography-guidedbiopsy in spinal diseases. Radiol Med 1994;87(3):299–304.
10] Lis E, Bilsky MH, Pisinski L, et al. Percutaneous CT-guided biopsy of osseouslesion of the spine in patients with known or suspected malignancy. Am JNeuroradiol 2004;25(9):1583–8.
11] Rimondi E, Staals EL, Errani C, et al. Percutaneous CT-guided biopsy of the spine:results of 430 biopsies. Eur Spine J 2008;17:975–81.
12] Mankin HJ, Mankin CJ, Simon MA. The hazards of biopsy, revisited. J Bone JointSurg Am 1996;78(5):656–63.
13] Liu PT, Valadez SD, Chivers FS, et al. Anatomically based guidelines for core nee-dle biopsy of bone tumors: implications for limb sparing surgery. Radiographics2007;27:189–205.
14] Ward WG, Kilpatrick S. Fine needle aspiration biopsy of primary bone tumors.Clin Orthop Relat Res 2000;373:30–7.
15] Hau MA, Kim JI, Kattapuram S, et al. Accuracy of CT-guided biopsies in 359patient with musculoskeletal lesions. Skeletal Radiol 2002;31(6):349–53.
16] Yang YJ, Damron TA. Comparison of needle core biopsy and fine needle aspi-ration for diagnostic accuracy in musculoskeletal lesions. Arch Pathol Lab Med2004;128(7):759–64.
17] Wu JS, Goldsmith GD, Horwich PJ, et al. Bone and soft tissue lesions: what fac-tors affect the diagnostic yield of image-guided core needle biopsy. Radiology2008;248(3):962–70.
18] Michel SC, Pfirmann CW, Boss N, et al. CT-guided core biopsy of subchon-dral bone and intervertebral space in suspected spondylodiskitis. AJR Am J
d biopsy of the musculoskeletal system: Results of 2027 cases. Eur J
osteomyelitis: Are there factors associated with positive or negative cultures?AJR Am J Roentgenol 2007;188(6):1529–34.
20] Altuntas AO, Slavin J, Smith PJ, et al. Accuracy of computed guided core needlebiopsy of musculoskeletal tumors. ANZ J Surg 2005;75(4):187–91.